User login
Obesity-related cancers increasing in younger adults
The incidence of obesity-related cancers such as kidney and gallbladder cancer has increased significantly in young adults over the past two decades in the United States, according to an analysis of data from 25 population-based state registries in the United States.
The incidence of 6 of the 12 obesity-related cancers increased among individuals aged 25-49 years, Hyuna Sung, PhD, of the American Cancer Society, Atlanta, and her colleagues reported Feb. 4 in the Lancet Public Health.
Among more than 14.6 million incident cases of cancer diagnosed in adults aged 25-84 years between 1995 and 2014, the greatest increase in incidence, 6.23% annually, was seen with kidney cancer among the 25- to 29-year age group. Incidence, however, also increased by at least 6.17% in those aged 30-34 years, by 5.23% in those aged 35-39 years, and by 3.88% in those aged 40-44 years.
The incidence rate for kidney cancer among individuals born around 1985 was nearly fivefold higher than in individuals born in 1950, the investigators said (Lancet Public Health. 2019 Feb 4. doi: 10.1016/S2468-2667(18)30267-6).
The analysis also showed significant increases from 1995 to 2014 in the incidence of cancer of the gallbladder among younger adults: 3.71% per year among those aged 25-29 years and 2.58% per year in those aged 30-34 years.
Similarly, the incidence of uterine corpus cancer increased in the 25- to 29-year age group by 3.34% per year and by 3.22% in the 30- to 34-year age group. The incidence of colorectal cancer increased by 2.41% among those aged 25-29 years and by 2.38% in those aged 30-34 years, Dr. Sung and her associates said.
The greatest annual increase in the incidence of multiple myeloma was seen in individuals aged 30-34 years (2.21%), but significant annual increases in incidence were seen in individuals aged 30-44 years.
For pancreatic cancer, significant annual increases in incidence were seen among individuals aged 25-29 years (4.34%) and 30-34 years (2.47%).
The study also showed increases in the same obesity-related cancers – except for colorectal cancer – among adults aged 50 years and older. The incidence of colorectal cancer actually decreased annually in older adults, while the incidence of uterine corpus cancer increased among women aged 50-69 years but decreased in those over 75 years.
Dr. Sung and her coauthors suggested that these trends may be related to the rise of obesity and overweight in the United States, noting that excess body weight could be responsible for up to 60% of all endometrial cancers, 36% of gallbladder cancers, and 33% of kidney cancers in adults aged over 30 years.
“Because most epidemiological studies have primarily focused on older populations, the effect of excess bodyweight in early life or of weight change from young adulthood on cancer risk in different stages of the life course is not well characterized,” they wrote. “In concert with excess bodyweight, obesity-related health conditions and lifestyle factors can contribute to the increasing burden of obesity-related cancers in young adults, which include diabetes, gallstones, inflammatory bowel disease, and poor diet.”
The incidences of breast cancer and gastric cardia cancer were relatively stable in all age groups over the study period, and the incidence of ovarian cancer decreased in all age groups.
Researchers looked at the incidence of 30 cancers in total, including 18 cancers not related to obesity. Here they saw increases among younger adults only in the incidence of gastric noncardiac cancer – which showed a 2.16% annual increase in incidence among those aged 30-34 years – and leukemia, where there was a 1.33% annual increase in incidence in the same age group.
But the incidence of eight cancers, including those related to smoking and infection, decreased each year among younger adults.
“Our findings expose a recent change that could serve as a warning of an increased burden of obesity-related cancers to come in older adults,” study senior author Ahmedin Jemal, PhD, of the American Cancer Society, said in a statement. “Most cancers occur in older adults, which means that as the young people in our study age, the burden of obesity-related cancer cases and deaths are likely to increase even more. On the eve of World Cancer Day, it’s timely to consider what can be done to avert the impending rise.”
The future burden of these cancers could halt or even reverse the reductions in cancer mortality achieved over the past several decades, the investigators warned.
The study was funded by the American Cancer Society and the National Cancer Institute. No conflicts of interest were declared.
SOURCE: Sung H et al. Lancet Public Health. 2019 Feb 4 doi: 10.1016/ S2468-2667(18)30267-6.
Cancer was long thought of as a disease of aging, but the increase in incidence of some cancers in younger age groups has driven a recent reexamination of risk factors. This study’s most striking finding is the disproportionate increase in obesity-related cancer incidence among successively younger cohorts. Coupled with the rising incidence of obesity over the same period, it provides compelling evidence of a possible causal role for obesity in the increased incidence of these cancers.
Not all obesity-related cancers, however, show this pattern of age-specific increase in incidence, which could reflect the influence of other risk factors.
The hypothesis suggested by the study’s authors is plausible but needs to be tested more directly in experimental and population-based studies.
Catherine R. Marinac, PhD, is with the department of medical oncology at the Dana-Farber Cancer Institute, Boston, and Brenda M. Birmann, ScD, is with the department of medicine at Brigham and Women’s Hospital, Boston. These comments are taken from an accompanying editorial (Lancet Public Health. 2019 Feb 4. doi: 10.1016/S2468-2667(19)30017-9). No conflicts of interest were declared.
Cancer was long thought of as a disease of aging, but the increase in incidence of some cancers in younger age groups has driven a recent reexamination of risk factors. This study’s most striking finding is the disproportionate increase in obesity-related cancer incidence among successively younger cohorts. Coupled with the rising incidence of obesity over the same period, it provides compelling evidence of a possible causal role for obesity in the increased incidence of these cancers.
Not all obesity-related cancers, however, show this pattern of age-specific increase in incidence, which could reflect the influence of other risk factors.
The hypothesis suggested by the study’s authors is plausible but needs to be tested more directly in experimental and population-based studies.
Catherine R. Marinac, PhD, is with the department of medical oncology at the Dana-Farber Cancer Institute, Boston, and Brenda M. Birmann, ScD, is with the department of medicine at Brigham and Women’s Hospital, Boston. These comments are taken from an accompanying editorial (Lancet Public Health. 2019 Feb 4. doi: 10.1016/S2468-2667(19)30017-9). No conflicts of interest were declared.
Cancer was long thought of as a disease of aging, but the increase in incidence of some cancers in younger age groups has driven a recent reexamination of risk factors. This study’s most striking finding is the disproportionate increase in obesity-related cancer incidence among successively younger cohorts. Coupled with the rising incidence of obesity over the same period, it provides compelling evidence of a possible causal role for obesity in the increased incidence of these cancers.
Not all obesity-related cancers, however, show this pattern of age-specific increase in incidence, which could reflect the influence of other risk factors.
The hypothesis suggested by the study’s authors is plausible but needs to be tested more directly in experimental and population-based studies.
Catherine R. Marinac, PhD, is with the department of medical oncology at the Dana-Farber Cancer Institute, Boston, and Brenda M. Birmann, ScD, is with the department of medicine at Brigham and Women’s Hospital, Boston. These comments are taken from an accompanying editorial (Lancet Public Health. 2019 Feb 4. doi: 10.1016/S2468-2667(19)30017-9). No conflicts of interest were declared.
The incidence of obesity-related cancers such as kidney and gallbladder cancer has increased significantly in young adults over the past two decades in the United States, according to an analysis of data from 25 population-based state registries in the United States.
The incidence of 6 of the 12 obesity-related cancers increased among individuals aged 25-49 years, Hyuna Sung, PhD, of the American Cancer Society, Atlanta, and her colleagues reported Feb. 4 in the Lancet Public Health.
Among more than 14.6 million incident cases of cancer diagnosed in adults aged 25-84 years between 1995 and 2014, the greatest increase in incidence, 6.23% annually, was seen with kidney cancer among the 25- to 29-year age group. Incidence, however, also increased by at least 6.17% in those aged 30-34 years, by 5.23% in those aged 35-39 years, and by 3.88% in those aged 40-44 years.
The incidence rate for kidney cancer among individuals born around 1985 was nearly fivefold higher than in individuals born in 1950, the investigators said (Lancet Public Health. 2019 Feb 4. doi: 10.1016/S2468-2667(18)30267-6).
The analysis also showed significant increases from 1995 to 2014 in the incidence of cancer of the gallbladder among younger adults: 3.71% per year among those aged 25-29 years and 2.58% per year in those aged 30-34 years.
Similarly, the incidence of uterine corpus cancer increased in the 25- to 29-year age group by 3.34% per year and by 3.22% in the 30- to 34-year age group. The incidence of colorectal cancer increased by 2.41% among those aged 25-29 years and by 2.38% in those aged 30-34 years, Dr. Sung and her associates said.
The greatest annual increase in the incidence of multiple myeloma was seen in individuals aged 30-34 years (2.21%), but significant annual increases in incidence were seen in individuals aged 30-44 years.
For pancreatic cancer, significant annual increases in incidence were seen among individuals aged 25-29 years (4.34%) and 30-34 years (2.47%).
The study also showed increases in the same obesity-related cancers – except for colorectal cancer – among adults aged 50 years and older. The incidence of colorectal cancer actually decreased annually in older adults, while the incidence of uterine corpus cancer increased among women aged 50-69 years but decreased in those over 75 years.
Dr. Sung and her coauthors suggested that these trends may be related to the rise of obesity and overweight in the United States, noting that excess body weight could be responsible for up to 60% of all endometrial cancers, 36% of gallbladder cancers, and 33% of kidney cancers in adults aged over 30 years.
“Because most epidemiological studies have primarily focused on older populations, the effect of excess bodyweight in early life or of weight change from young adulthood on cancer risk in different stages of the life course is not well characterized,” they wrote. “In concert with excess bodyweight, obesity-related health conditions and lifestyle factors can contribute to the increasing burden of obesity-related cancers in young adults, which include diabetes, gallstones, inflammatory bowel disease, and poor diet.”
The incidences of breast cancer and gastric cardia cancer were relatively stable in all age groups over the study period, and the incidence of ovarian cancer decreased in all age groups.
Researchers looked at the incidence of 30 cancers in total, including 18 cancers not related to obesity. Here they saw increases among younger adults only in the incidence of gastric noncardiac cancer – which showed a 2.16% annual increase in incidence among those aged 30-34 years – and leukemia, where there was a 1.33% annual increase in incidence in the same age group.
But the incidence of eight cancers, including those related to smoking and infection, decreased each year among younger adults.
“Our findings expose a recent change that could serve as a warning of an increased burden of obesity-related cancers to come in older adults,” study senior author Ahmedin Jemal, PhD, of the American Cancer Society, said in a statement. “Most cancers occur in older adults, which means that as the young people in our study age, the burden of obesity-related cancer cases and deaths are likely to increase even more. On the eve of World Cancer Day, it’s timely to consider what can be done to avert the impending rise.”
The future burden of these cancers could halt or even reverse the reductions in cancer mortality achieved over the past several decades, the investigators warned.
The study was funded by the American Cancer Society and the National Cancer Institute. No conflicts of interest were declared.
SOURCE: Sung H et al. Lancet Public Health. 2019 Feb 4 doi: 10.1016/ S2468-2667(18)30267-6.
The incidence of obesity-related cancers such as kidney and gallbladder cancer has increased significantly in young adults over the past two decades in the United States, according to an analysis of data from 25 population-based state registries in the United States.
The incidence of 6 of the 12 obesity-related cancers increased among individuals aged 25-49 years, Hyuna Sung, PhD, of the American Cancer Society, Atlanta, and her colleagues reported Feb. 4 in the Lancet Public Health.
Among more than 14.6 million incident cases of cancer diagnosed in adults aged 25-84 years between 1995 and 2014, the greatest increase in incidence, 6.23% annually, was seen with kidney cancer among the 25- to 29-year age group. Incidence, however, also increased by at least 6.17% in those aged 30-34 years, by 5.23% in those aged 35-39 years, and by 3.88% in those aged 40-44 years.
The incidence rate for kidney cancer among individuals born around 1985 was nearly fivefold higher than in individuals born in 1950, the investigators said (Lancet Public Health. 2019 Feb 4. doi: 10.1016/S2468-2667(18)30267-6).
The analysis also showed significant increases from 1995 to 2014 in the incidence of cancer of the gallbladder among younger adults: 3.71% per year among those aged 25-29 years and 2.58% per year in those aged 30-34 years.
Similarly, the incidence of uterine corpus cancer increased in the 25- to 29-year age group by 3.34% per year and by 3.22% in the 30- to 34-year age group. The incidence of colorectal cancer increased by 2.41% among those aged 25-29 years and by 2.38% in those aged 30-34 years, Dr. Sung and her associates said.
The greatest annual increase in the incidence of multiple myeloma was seen in individuals aged 30-34 years (2.21%), but significant annual increases in incidence were seen in individuals aged 30-44 years.
For pancreatic cancer, significant annual increases in incidence were seen among individuals aged 25-29 years (4.34%) and 30-34 years (2.47%).
The study also showed increases in the same obesity-related cancers – except for colorectal cancer – among adults aged 50 years and older. The incidence of colorectal cancer actually decreased annually in older adults, while the incidence of uterine corpus cancer increased among women aged 50-69 years but decreased in those over 75 years.
Dr. Sung and her coauthors suggested that these trends may be related to the rise of obesity and overweight in the United States, noting that excess body weight could be responsible for up to 60% of all endometrial cancers, 36% of gallbladder cancers, and 33% of kidney cancers in adults aged over 30 years.
“Because most epidemiological studies have primarily focused on older populations, the effect of excess bodyweight in early life or of weight change from young adulthood on cancer risk in different stages of the life course is not well characterized,” they wrote. “In concert with excess bodyweight, obesity-related health conditions and lifestyle factors can contribute to the increasing burden of obesity-related cancers in young adults, which include diabetes, gallstones, inflammatory bowel disease, and poor diet.”
The incidences of breast cancer and gastric cardia cancer were relatively stable in all age groups over the study period, and the incidence of ovarian cancer decreased in all age groups.
Researchers looked at the incidence of 30 cancers in total, including 18 cancers not related to obesity. Here they saw increases among younger adults only in the incidence of gastric noncardiac cancer – which showed a 2.16% annual increase in incidence among those aged 30-34 years – and leukemia, where there was a 1.33% annual increase in incidence in the same age group.
But the incidence of eight cancers, including those related to smoking and infection, decreased each year among younger adults.
“Our findings expose a recent change that could serve as a warning of an increased burden of obesity-related cancers to come in older adults,” study senior author Ahmedin Jemal, PhD, of the American Cancer Society, said in a statement. “Most cancers occur in older adults, which means that as the young people in our study age, the burden of obesity-related cancer cases and deaths are likely to increase even more. On the eve of World Cancer Day, it’s timely to consider what can be done to avert the impending rise.”
The future burden of these cancers could halt or even reverse the reductions in cancer mortality achieved over the past several decades, the investigators warned.
The study was funded by the American Cancer Society and the National Cancer Institute. No conflicts of interest were declared.
SOURCE: Sung H et al. Lancet Public Health. 2019 Feb 4 doi: 10.1016/ S2468-2667(18)30267-6.
FROM THE LANCET PUBLIC HEALTH
Key clinical point: The incidence of obesity-related cancers has increased in younger adults.
Major finding: The incidence of kidney cancer has increased by more than 6% per year in younger adults since 1995.
Study details: Analysis of data from 14,672,409 cases of cancer diagnosed between 1995 and 2014.
Disclosures: The study was funded by the American Cancer Society and the National Cancer Institute. No conflicts of interest were declared.
Source: Sung H et al. Lancet Public Health. 2019 Feb 4.

The other side of activity
While the increasing prevalence of obesity has been obvious for nearly half a century, it is only in the last decade or two that the focus has broadened to include the associated decline in physical activity.

A recent paper attempts to sharpen that focus by examining the timeline of that decline (Pediatrics 2019 Jan. doi: 10.1542/peds.2018-0994.). Using a device incorporating five sensors, one of which was an accelerometer, the investigators collected data from 600 children from five European countries accumulating more than 1,200 observations. What they discovered was that their subjects’ physical activity declined by 75 minutes per day from ages 6 to 11 years of age while sedentary behavior increased more than 100 minutes over that same interval. This observation is concerning because previous attention has focused intervention on adolescents assuming that the erosion of physical activity was occurring primarily during the teen years.
Not surprisingly the authors suggest that more studies should be performed to aid in the design of more sharply targeted interventions. While more information may be helpful, their current findings and an abundance of anecdotal observations suggest that to be effective that intervention must begin well before children reach school age.
What should this intervention look like? Currently, the emphasis seems to have been on programs that encourage activity. The National Football League is promoting its NFL Play 60 initiative. The Afterschool Alliance has its Kids on the Move programs. Former First Lady Michelle Obama has been the spokesperson and driving force behind Let’s Move. And, the American Academy of Pediatrics has recently been encouraging both parents and pediatricians to appreciate The Power of Play to encourage children to get into more physical activity. All of these initiatives are well meaning, but I suspect their effectiveness is usually limited to the public awareness they generate.
We seem to have forgotten that there are two sides to the equation. The accelerometer study from Europe should remind us that our initiatives should also be addressing the problem of epidemic inactivity with equal vigor. Creating programs that focus on increasing activity can be expensive. There may be costs for equipment, spaces to be maintained, and staff to be paid. On the other hand, curbing sedentary behavior requires only an adult with the courage to say, “No.” “No, we will have the television for only an hour today.” “No, you can’t play your video game until after dinner.”
While addressing the disciplinary side of the activity-inactivity dichotomy may be relatively inexpensive, it does seem to have a cost on parents. It requires them to buy into the idea that, given even the most-limited supply of objects and infrastructure, most children can keep themselves entertained and active. There does seem to be a small subset of children who enter the world with a sedentary mindset, possibly inherited from their parents. This unfortunate minority will require some creative intervention to achieve a healthy level of activity.

However, most young children who have become accustomed to being amused by sedentary “activities” such as television and video games still retain their innate creativity and natural inclination to be physically active. Unfortunately, unmasking these health-sustaining attributes may require a long and unpleasant weaning period that many parents don’t seem to have the patience to endure. The longer the child has been allowed to engage in sedentary behaviors, the longer this adjustment period will be, yet another argument for early intervention.
Encouraging physical activity is something we should be doing every day in our offices, but it must go hand in hand with an equivalent emphasis on helping parents create a discipline framework that discourages sedentary behavior.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
While the increasing prevalence of obesity has been obvious for nearly half a century, it is only in the last decade or two that the focus has broadened to include the associated decline in physical activity.
A recent paper attempts to sharpen that focus by examining the timeline of that decline (Pediatrics 2019 Jan. doi: 10.1542/peds.2018-0994.). Using a device incorporating five sensors, one of which was an accelerometer, the investigators collected data from 600 children from five European countries accumulating more than 1,200 observations. What they discovered was that their subjects’ physical activity declined by 75 minutes per day from ages 6 to 11 years of age while sedentary behavior increased more than 100 minutes over that same interval. This observation is concerning because previous attention has focused intervention on adolescents assuming that the erosion of physical activity was occurring primarily during the teen years.
Not surprisingly the authors suggest that more studies should be performed to aid in the design of more sharply targeted interventions. While more information may be helpful, their current findings and an abundance of anecdotal observations suggest that to be effective that intervention must begin well before children reach school age.
What should this intervention look like? Currently, the emphasis seems to have been on programs that encourage activity. The National Football League is promoting its NFL Play 60 initiative. The Afterschool Alliance has its Kids on the Move programs. Former First Lady Michelle Obama has been the spokesperson and driving force behind Let’s Move. And, the American Academy of Pediatrics has recently been encouraging both parents and pediatricians to appreciate The Power of Play to encourage children to get into more physical activity. All of these initiatives are well meaning, but I suspect their effectiveness is usually limited to the public awareness they generate.
We seem to have forgotten that there are two sides to the equation. The accelerometer study from Europe should remind us that our initiatives should also be addressing the problem of epidemic inactivity with equal vigor. Creating programs that focus on increasing activity can be expensive. There may be costs for equipment, spaces to be maintained, and staff to be paid. On the other hand, curbing sedentary behavior requires only an adult with the courage to say, “No.” “No, we will have the television for only an hour today.” “No, you can’t play your video game until after dinner.”
While addressing the disciplinary side of the activity-inactivity dichotomy may be relatively inexpensive, it does seem to have a cost on parents. It requires them to buy into the idea that, given even the most-limited supply of objects and infrastructure, most children can keep themselves entertained and active. There does seem to be a small subset of children who enter the world with a sedentary mindset, possibly inherited from their parents. This unfortunate minority will require some creative intervention to achieve a healthy level of activity.
However, most young children who have become accustomed to being amused by sedentary “activities” such as television and video games still retain their innate creativity and natural inclination to be physically active. Unfortunately, unmasking these health-sustaining attributes may require a long and unpleasant weaning period that many parents don’t seem to have the patience to endure. The longer the child has been allowed to engage in sedentary behaviors, the longer this adjustment period will be, yet another argument for early intervention.
Encouraging physical activity is something we should be doing every day in our offices, but it must go hand in hand with an equivalent emphasis on helping parents create a discipline framework that discourages sedentary behavior.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
While the increasing prevalence of obesity has been obvious for nearly half a century, it is only in the last decade or two that the focus has broadened to include the associated decline in physical activity.
A recent paper attempts to sharpen that focus by examining the timeline of that decline (Pediatrics 2019 Jan. doi: 10.1542/peds.2018-0994.). Using a device incorporating five sensors, one of which was an accelerometer, the investigators collected data from 600 children from five European countries accumulating more than 1,200 observations. What they discovered was that their subjects’ physical activity declined by 75 minutes per day from ages 6 to 11 years of age while sedentary behavior increased more than 100 minutes over that same interval. This observation is concerning because previous attention has focused intervention on adolescents assuming that the erosion of physical activity was occurring primarily during the teen years.
Not surprisingly the authors suggest that more studies should be performed to aid in the design of more sharply targeted interventions. While more information may be helpful, their current findings and an abundance of anecdotal observations suggest that to be effective that intervention must begin well before children reach school age.
What should this intervention look like? Currently, the emphasis seems to have been on programs that encourage activity. The National Football League is promoting its NFL Play 60 initiative. The Afterschool Alliance has its Kids on the Move programs. Former First Lady Michelle Obama has been the spokesperson and driving force behind Let’s Move. And, the American Academy of Pediatrics has recently been encouraging both parents and pediatricians to appreciate The Power of Play to encourage children to get into more physical activity. All of these initiatives are well meaning, but I suspect their effectiveness is usually limited to the public awareness they generate.
We seem to have forgotten that there are two sides to the equation. The accelerometer study from Europe should remind us that our initiatives should also be addressing the problem of epidemic inactivity with equal vigor. Creating programs that focus on increasing activity can be expensive. There may be costs for equipment, spaces to be maintained, and staff to be paid. On the other hand, curbing sedentary behavior requires only an adult with the courage to say, “No.” “No, we will have the television for only an hour today.” “No, you can’t play your video game until after dinner.”
While addressing the disciplinary side of the activity-inactivity dichotomy may be relatively inexpensive, it does seem to have a cost on parents. It requires them to buy into the idea that, given even the most-limited supply of objects and infrastructure, most children can keep themselves entertained and active. There does seem to be a small subset of children who enter the world with a sedentary mindset, possibly inherited from their parents. This unfortunate minority will require some creative intervention to achieve a healthy level of activity.
However, most young children who have become accustomed to being amused by sedentary “activities” such as television and video games still retain their innate creativity and natural inclination to be physically active. Unfortunately, unmasking these health-sustaining attributes may require a long and unpleasant weaning period that many parents don’t seem to have the patience to endure. The longer the child has been allowed to engage in sedentary behaviors, the longer this adjustment period will be, yet another argument for early intervention.
Encouraging physical activity is something we should be doing every day in our offices, but it must go hand in hand with an equivalent emphasis on helping parents create a discipline framework that discourages sedentary behavior.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
A skeptic’s view of bariatric surgery
Like JFP’s Editor-in-Chief, Dr. John Hickner, I have been skeptical about bariatric surgery (A [former] skeptic’s view of bariatric surgery. J Fam Pract. 2018;67:600), but I will recommend it for a select few patients who are unable or unwilling to undergo significant lifestyle changes. My experience in clinic has done nothing to change this skeptical view. I have many patients who opted for bariatric surgery, but did not change their lifestyle habits. These patients often regain weight and accumulate chronic diseases 2 to 7 years postop. In the end, if a patient does not change their lifestyle, bariatric surgery can push the consequences of obesity out 5 to 10 years, but at a very significant risk.
The most significant problem I see is that many primary care providers do not feel qualified to impart meaningful lifestyle recommendations to patients, which often leads to guidance that is inadequate and, in some cases, inaccurate. Furthermore, assuming patients have received evidence-based instructions, they often lack the support and means to apply these lifestyle changes. I would be very hesitant to recommend bariatric surgery before addressing all of these concerns.
An interesting study done by Lingvay et al1 showed that postsurgical starvation (600 kcal/d) without the bariatric surgery had better short-term outcomes than surgery with calorie restriction, which suggests that a period of starvation is better than surgery.
In general, the results of evidence-based lifestyle changes far surpass any medical or surgical treatment for obesity and its associated chronic diseases. The evidence for this is overwhelming. (See books by Drs. Joel Fuhrman, Michael Greger, Neal Barnard, Dean Ornish, and Garth Davis, as well as the hundreds of peer-reviewed studies cited in these books.) Yet most patients under-going bariatric surgery never receive proper instructions or attempt any meaningful lifestyle changes.
I think it is far more prudent to refer potential surgical candidates to someone who understands good nutrition and lifestyle changes, such as a doctor certified by the American College of Lifestyle Medicine (lifestylemedicine.org). Surgery, in my opinion, is a very poor and dangerous second choice.
John Reed, MD
Fishersville, Va
1. Lingvay I, GuthE, Eslam A, et al. Rapid improvement in diabetes after gastric bypass surgery: Is it the diet or surgery? Diabetes Care. 2013;36:2741-2747.
Like JFP’s Editor-in-Chief, Dr. John Hickner, I have been skeptical about bariatric surgery (A [former] skeptic’s view of bariatric surgery. J Fam Pract. 2018;67:600), but I will recommend it for a select few patients who are unable or unwilling to undergo significant lifestyle changes. My experience in clinic has done nothing to change this skeptical view. I have many patients who opted for bariatric surgery, but did not change their lifestyle habits. These patients often regain weight and accumulate chronic diseases 2 to 7 years postop. In the end, if a patient does not change their lifestyle, bariatric surgery can push the consequences of obesity out 5 to 10 years, but at a very significant risk.
The most significant problem I see is that many primary care providers do not feel qualified to impart meaningful lifestyle recommendations to patients, which often leads to guidance that is inadequate and, in some cases, inaccurate. Furthermore, assuming patients have received evidence-based instructions, they often lack the support and means to apply these lifestyle changes. I would be very hesitant to recommend bariatric surgery before addressing all of these concerns.
An interesting study done by Lingvay et al1 showed that postsurgical starvation (600 kcal/d) without the bariatric surgery had better short-term outcomes than surgery with calorie restriction, which suggests that a period of starvation is better than surgery.
In general, the results of evidence-based lifestyle changes far surpass any medical or surgical treatment for obesity and its associated chronic diseases. The evidence for this is overwhelming. (See books by Drs. Joel Fuhrman, Michael Greger, Neal Barnard, Dean Ornish, and Garth Davis, as well as the hundreds of peer-reviewed studies cited in these books.) Yet most patients under-going bariatric surgery never receive proper instructions or attempt any meaningful lifestyle changes.
I think it is far more prudent to refer potential surgical candidates to someone who understands good nutrition and lifestyle changes, such as a doctor certified by the American College of Lifestyle Medicine (lifestylemedicine.org). Surgery, in my opinion, is a very poor and dangerous second choice.
John Reed, MD
Fishersville, Va
Like JFP’s Editor-in-Chief, Dr. John Hickner, I have been skeptical about bariatric surgery (A [former] skeptic’s view of bariatric surgery. J Fam Pract. 2018;67:600), but I will recommend it for a select few patients who are unable or unwilling to undergo significant lifestyle changes. My experience in clinic has done nothing to change this skeptical view. I have many patients who opted for bariatric surgery, but did not change their lifestyle habits. These patients often regain weight and accumulate chronic diseases 2 to 7 years postop. In the end, if a patient does not change their lifestyle, bariatric surgery can push the consequences of obesity out 5 to 10 years, but at a very significant risk.
The most significant problem I see is that many primary care providers do not feel qualified to impart meaningful lifestyle recommendations to patients, which often leads to guidance that is inadequate and, in some cases, inaccurate. Furthermore, assuming patients have received evidence-based instructions, they often lack the support and means to apply these lifestyle changes. I would be very hesitant to recommend bariatric surgery before addressing all of these concerns.
An interesting study done by Lingvay et al1 showed that postsurgical starvation (600 kcal/d) without the bariatric surgery had better short-term outcomes than surgery with calorie restriction, which suggests that a period of starvation is better than surgery.
In general, the results of evidence-based lifestyle changes far surpass any medical or surgical treatment for obesity and its associated chronic diseases. The evidence for this is overwhelming. (See books by Drs. Joel Fuhrman, Michael Greger, Neal Barnard, Dean Ornish, and Garth Davis, as well as the hundreds of peer-reviewed studies cited in these books.) Yet most patients under-going bariatric surgery never receive proper instructions or attempt any meaningful lifestyle changes.
I think it is far more prudent to refer potential surgical candidates to someone who understands good nutrition and lifestyle changes, such as a doctor certified by the American College of Lifestyle Medicine (lifestylemedicine.org). Surgery, in my opinion, is a very poor and dangerous second choice.
John Reed, MD
Fishersville, Va
1. Lingvay I, GuthE, Eslam A, et al. Rapid improvement in diabetes after gastric bypass surgery: Is it the diet or surgery? Diabetes Care. 2013;36:2741-2747.
1. Lingvay I, GuthE, Eslam A, et al. Rapid improvement in diabetes after gastric bypass surgery: Is it the diet or surgery? Diabetes Care. 2013;36:2741-2747.
Oral GLP-1 receptor agonist pioneered in T2DM trial
BERLIN – An investigational oral formulation of the glucagonlike peptide–1 receptor agonist (GLP-1 RA) semaglutide reduced glycated hemoglobin (HbA1c) to a greater extent than did placebo at all doses tested in patients with type 2 diabetes mellitus (T2DM) in the phase 3a PIONEER 1 trial.
The estimated mean change in HbA1c from baseline to week 26 – the primary endpoint – using an on-treatment analysis was –0.8% with a once-daily dose of 3 mg, –1.3% with a once-daily dose of 7 mg, and –1.5% with a once-daily dose of 14 mg. The corresponding value for placebo was –0.1%, with all comparisons statistically significant (P less than .001).
The on-treatment analysis evaluated treatment effects for all randomized patients (n = 703) and assumed that all subjects remained on-treatment and excluded the effect of any rescue medication. Results for an intention-to-treat (ITT) analysis provided similar results, however, with estimated mean changes in HbA1c of –0.9%, –1.2%, and –1.4% for the three respective semaglutide doses and –0.3% for placebo.
“There was a very nice dose-dependent decrease in HbA1c, which was superior to placebo for all doses of semaglutide” said study investigator Martin Haluzík, MD, at the annual meeting of the European Association for the Study of Diabetes.
“I think it’s quite important to stress the magnitude of the decrease of HbA1c, because with the highest dose it was –1.5% from a baseline of 8%, which I believe is something that hasn’t ever really been seen with any other oral antidiabetic medication,” added Dr. Haluzík, professor of internal medicine at the 1st Faculty of Medicine at Charles University and deputy head of the Institute for Clinical and Experimental Medicine, both in Prague.
Currently, GLP-1 RAs are available only in a subcutaneous formulation, Dr. Haluzík reminded his audience, adding that oral semaglutide was the first GLP-1 RA to be developed in a tablet formulation and was in the late stages of clinical development.
PIONEER 1 is the first of 10 phase 3a trials with oral semaglutide to be reported. “Additional studies, across the full spectrum of diabetes care, in special populations, comparing it with active comparators with varied trial duration, have been completed or will be completed in 2018,” said coinvestigator for the study Vanita Aroda, MD, during a separate presentation at a dedicated symposium on the PIONEER program.
Dr. Aroda, the director of the diabetes research program at Brigham and Women’s Hospital in Boston, observed that oral semaglutide was being evaluated from early care as monotherapy in the PIONEER 1 study. The other trials, such as PIONEER 2, PIONEER 3, PIONEER 4, and PIONEER 7 were looking at oral semaglutide in combination with oral antidiabetic agents versus various active comparators; PIONEER 5 and PIONEER 6 were in special populations; and PIONEER 8 was looking at its use on top of basal insulin. Two further trials are also part of the study program.
“I think this is the first time that we actually have completed data of an entire program, including cardiovascular data, all within the same year,” Dr. Aroda said. “All of the studies are in the process of data analysis or data reporting.”
PIONEER 1 was a multicenter, randomized, double-blind, placebo-controlled trial examining efficacy and safety of semaglutide versus placebo in 703 adults with drug-naive T2DM who were being treated with diet and exercise only.
Three doses of oral semaglutide – 3 mg, 7 mg, and 14 mg – were assessed and compared with placebo. There was a fixed 4-week dose escalation period, with all patients starting treatment with 3 mg of semaglutide and then increasing to 7 mg by week 4 and 14 mg by week 8. This was to try to reduce the risk of gastrointestinal side effects, which are known to occur with GLP-1 RAs.
Secondary outcome measures were change in body weight, fasting plasma glucose, HbA1c below a target of 7% (53 mmol/mol), which were all measured from baseline to week 26; adverse events, including severe and blood glucose–confirmed symptomatic hypoglycemic episodes, were assessed out to week 31.
The average age of patients in the trial was around 55 years, around half were female, and the starting HbA1c was approximately 8%.The mean body weight ranged from 86.9 kg to 89 kg in the different treatment groups, with a similar body mass index of about 32 kg/m2.
Clinically meaningful weight loss, compared with placebo, was only achieved with the highest dose of oral semaglutide, with a –4.1 kg reduction versus –1.5 kg for placebo from baseline to week 26 (P less than .001, on-treatment analysis). Reductions in body weight for the 3-mg and 7-mg oral semaglutide doses were a respective –1.7 kg and –2.5 kg. ITT results were again similar, with weight losses of –1.5, –2.3, and –3.7 kg for the 3-, 7-, and 14-mg doses of oral semaglutide, respectively, and –1.4 kg for placebo.
More patients treated with oral semaglutide 3, 7, or 14 mg versus placebo achieved an HbA1c of below 7% (59.1%, 71.9%, and 80.3%, respectively, vs. 33.8%) or a body weight loss of 5% or more (21.3%, 28.7%, and 44.3% vs. 15.7%).
Furthermore, more patients treated with oral semaglutide achieved an HbA1c of or below 7% without hypoglycemic episodes or body weight gain than did those given placebo. There were also more patients who achieved an HbA1c reduction of at least 1% and a weight loss of 3% or higher.
“Oral semaglutide demonstrated a safety and tolerability profile consistent with that of [injectable] GLP-1 RAs,” Dr. Haluzík reported. Adverse events were seen in 57.7%, 53.1%, and 56.6%of patients treated with 3, 7, and 14 mg of oral semaglutide and 55.6% of those treated with placebo.
The most common adverse events seen with oral semaglutide affected the gastrointestinal tract, with nausea affecting 8%, 5.1%, and 16% of 3, 7, and 14 mg–treated patients versus 5.6% of placebo-treated patients. Vomiting affected a respective 2.9%, 4.6%, 6.9%, and 2.1%, and diarrhea a respective 8.6%, 5.1%, 5.1%, and 2.2%.
Severe or blood glucose–confirmed, symptomatic hypoglycemia was reported in 2.9%, 1.1%, and 0.6%of those treated with 3, 7, 14 mg of oral semaglutide and 0.6% of placebo-treated patients.
PIONEER 1 represents a “step change in GLP-1 receptor agonist therapy”, said Cliff Bailey, MD, who discussed the trial aa the EASD’s independent commentator during a symposium on the PIONEER program. These data are “leading to a new delivery route for GLP-1 receptor agonists, from injection to oral,” and “this can be done with good metabolic efficacy, with substantial reductions in A1c and body weight, and with a safety profile that’s comparable to the subcutaneous injection.”
Dr. Bailey, who is professor of clinical science at Aston University in Birmingham, England, noted, however, the oral dosing of semaglutide “requires patient commitment because it needs to be taken before breakfast time, and it may also, to some extent, affect the timing of some of the other medications.”
The study was sponsored by Novo Nordisk. Dr. Haluzík disclosed acting as a consultant to AstraZeneca, Eli Lilly, Johnson & Johnson, Mundipharma, Novatin, Novo Nordisk, and Sanofi Aventis. Dr. Aroda was an investigator in the PIONEER 1 study and disclosed acting as a consultant to Novo Nordisk; she also disclosed relationships with multiple other pharmaceutical companies, including AstraZeneca, BMS, Calbra, Eisai, Elcelyx Therapeutics, Janssen, and Sanofi Aventis. Dr. Bailey acknowledged attending advisory boards, undertaking ad hoc consultancy work, and receiving research and travel support from several pharmaceutical companies that included Novo Nordisk.
SOURCES: Haluzík M et al. EASD 2018, Abstract 38; Aroda V. EASD 2018, Session S18 - PIONEER Trial; Bailey C. EASD 2018, Session S18 - PIONEER Trial.
BERLIN – An investigational oral formulation of the glucagonlike peptide–1 receptor agonist (GLP-1 RA) semaglutide reduced glycated hemoglobin (HbA1c) to a greater extent than did placebo at all doses tested in patients with type 2 diabetes mellitus (T2DM) in the phase 3a PIONEER 1 trial.
The estimated mean change in HbA1c from baseline to week 26 – the primary endpoint – using an on-treatment analysis was –0.8% with a once-daily dose of 3 mg, –1.3% with a once-daily dose of 7 mg, and –1.5% with a once-daily dose of 14 mg. The corresponding value for placebo was –0.1%, with all comparisons statistically significant (P less than .001).
The on-treatment analysis evaluated treatment effects for all randomized patients (n = 703) and assumed that all subjects remained on-treatment and excluded the effect of any rescue medication. Results for an intention-to-treat (ITT) analysis provided similar results, however, with estimated mean changes in HbA1c of –0.9%, –1.2%, and –1.4% for the three respective semaglutide doses and –0.3% for placebo.
“There was a very nice dose-dependent decrease in HbA1c, which was superior to placebo for all doses of semaglutide” said study investigator Martin Haluzík, MD, at the annual meeting of the European Association for the Study of Diabetes.
“I think it’s quite important to stress the magnitude of the decrease of HbA1c, because with the highest dose it was –1.5% from a baseline of 8%, which I believe is something that hasn’t ever really been seen with any other oral antidiabetic medication,” added Dr. Haluzík, professor of internal medicine at the 1st Faculty of Medicine at Charles University and deputy head of the Institute for Clinical and Experimental Medicine, both in Prague.
Currently, GLP-1 RAs are available only in a subcutaneous formulation, Dr. Haluzík reminded his audience, adding that oral semaglutide was the first GLP-1 RA to be developed in a tablet formulation and was in the late stages of clinical development.
PIONEER 1 is the first of 10 phase 3a trials with oral semaglutide to be reported. “Additional studies, across the full spectrum of diabetes care, in special populations, comparing it with active comparators with varied trial duration, have been completed or will be completed in 2018,” said coinvestigator for the study Vanita Aroda, MD, during a separate presentation at a dedicated symposium on the PIONEER program.
Dr. Aroda, the director of the diabetes research program at Brigham and Women’s Hospital in Boston, observed that oral semaglutide was being evaluated from early care as monotherapy in the PIONEER 1 study. The other trials, such as PIONEER 2, PIONEER 3, PIONEER 4, and PIONEER 7 were looking at oral semaglutide in combination with oral antidiabetic agents versus various active comparators; PIONEER 5 and PIONEER 6 were in special populations; and PIONEER 8 was looking at its use on top of basal insulin. Two further trials are also part of the study program.
“I think this is the first time that we actually have completed data of an entire program, including cardiovascular data, all within the same year,” Dr. Aroda said. “All of the studies are in the process of data analysis or data reporting.”
PIONEER 1 was a multicenter, randomized, double-blind, placebo-controlled trial examining efficacy and safety of semaglutide versus placebo in 703 adults with drug-naive T2DM who were being treated with diet and exercise only.
Three doses of oral semaglutide – 3 mg, 7 mg, and 14 mg – were assessed and compared with placebo. There was a fixed 4-week dose escalation period, with all patients starting treatment with 3 mg of semaglutide and then increasing to 7 mg by week 4 and 14 mg by week 8. This was to try to reduce the risk of gastrointestinal side effects, which are known to occur with GLP-1 RAs.
Secondary outcome measures were change in body weight, fasting plasma glucose, HbA1c below a target of 7% (53 mmol/mol), which were all measured from baseline to week 26; adverse events, including severe and blood glucose–confirmed symptomatic hypoglycemic episodes, were assessed out to week 31.
The average age of patients in the trial was around 55 years, around half were female, and the starting HbA1c was approximately 8%.The mean body weight ranged from 86.9 kg to 89 kg in the different treatment groups, with a similar body mass index of about 32 kg/m2.
Clinically meaningful weight loss, compared with placebo, was only achieved with the highest dose of oral semaglutide, with a –4.1 kg reduction versus –1.5 kg for placebo from baseline to week 26 (P less than .001, on-treatment analysis). Reductions in body weight for the 3-mg and 7-mg oral semaglutide doses were a respective –1.7 kg and –2.5 kg. ITT results were again similar, with weight losses of –1.5, –2.3, and –3.7 kg for the 3-, 7-, and 14-mg doses of oral semaglutide, respectively, and –1.4 kg for placebo.
More patients treated with oral semaglutide 3, 7, or 14 mg versus placebo achieved an HbA1c of below 7% (59.1%, 71.9%, and 80.3%, respectively, vs. 33.8%) or a body weight loss of 5% or more (21.3%, 28.7%, and 44.3% vs. 15.7%).
Furthermore, more patients treated with oral semaglutide achieved an HbA1c of or below 7% without hypoglycemic episodes or body weight gain than did those given placebo. There were also more patients who achieved an HbA1c reduction of at least 1% and a weight loss of 3% or higher.
“Oral semaglutide demonstrated a safety and tolerability profile consistent with that of [injectable] GLP-1 RAs,” Dr. Haluzík reported. Adverse events were seen in 57.7%, 53.1%, and 56.6%of patients treated with 3, 7, and 14 mg of oral semaglutide and 55.6% of those treated with placebo.
The most common adverse events seen with oral semaglutide affected the gastrointestinal tract, with nausea affecting 8%, 5.1%, and 16% of 3, 7, and 14 mg–treated patients versus 5.6% of placebo-treated patients. Vomiting affected a respective 2.9%, 4.6%, 6.9%, and 2.1%, and diarrhea a respective 8.6%, 5.1%, 5.1%, and 2.2%.
Severe or blood glucose–confirmed, symptomatic hypoglycemia was reported in 2.9%, 1.1%, and 0.6%of those treated with 3, 7, 14 mg of oral semaglutide and 0.6% of placebo-treated patients.
PIONEER 1 represents a “step change in GLP-1 receptor agonist therapy”, said Cliff Bailey, MD, who discussed the trial aa the EASD’s independent commentator during a symposium on the PIONEER program. These data are “leading to a new delivery route for GLP-1 receptor agonists, from injection to oral,” and “this can be done with good metabolic efficacy, with substantial reductions in A1c and body weight, and with a safety profile that’s comparable to the subcutaneous injection.”
Dr. Bailey, who is professor of clinical science at Aston University in Birmingham, England, noted, however, the oral dosing of semaglutide “requires patient commitment because it needs to be taken before breakfast time, and it may also, to some extent, affect the timing of some of the other medications.”
The study was sponsored by Novo Nordisk. Dr. Haluzík disclosed acting as a consultant to AstraZeneca, Eli Lilly, Johnson & Johnson, Mundipharma, Novatin, Novo Nordisk, and Sanofi Aventis. Dr. Aroda was an investigator in the PIONEER 1 study and disclosed acting as a consultant to Novo Nordisk; she also disclosed relationships with multiple other pharmaceutical companies, including AstraZeneca, BMS, Calbra, Eisai, Elcelyx Therapeutics, Janssen, and Sanofi Aventis. Dr. Bailey acknowledged attending advisory boards, undertaking ad hoc consultancy work, and receiving research and travel support from several pharmaceutical companies that included Novo Nordisk.
SOURCES: Haluzík M et al. EASD 2018, Abstract 38; Aroda V. EASD 2018, Session S18 - PIONEER Trial; Bailey C. EASD 2018, Session S18 - PIONEER Trial.
BERLIN – An investigational oral formulation of the glucagonlike peptide–1 receptor agonist (GLP-1 RA) semaglutide reduced glycated hemoglobin (HbA1c) to a greater extent than did placebo at all doses tested in patients with type 2 diabetes mellitus (T2DM) in the phase 3a PIONEER 1 trial.
The estimated mean change in HbA1c from baseline to week 26 – the primary endpoint – using an on-treatment analysis was –0.8% with a once-daily dose of 3 mg, –1.3% with a once-daily dose of 7 mg, and –1.5% with a once-daily dose of 14 mg. The corresponding value for placebo was –0.1%, with all comparisons statistically significant (P less than .001).
The on-treatment analysis evaluated treatment effects for all randomized patients (n = 703) and assumed that all subjects remained on-treatment and excluded the effect of any rescue medication. Results for an intention-to-treat (ITT) analysis provided similar results, however, with estimated mean changes in HbA1c of –0.9%, –1.2%, and –1.4% for the three respective semaglutide doses and –0.3% for placebo.
“There was a very nice dose-dependent decrease in HbA1c, which was superior to placebo for all doses of semaglutide” said study investigator Martin Haluzík, MD, at the annual meeting of the European Association for the Study of Diabetes.
“I think it’s quite important to stress the magnitude of the decrease of HbA1c, because with the highest dose it was –1.5% from a baseline of 8%, which I believe is something that hasn’t ever really been seen with any other oral antidiabetic medication,” added Dr. Haluzík, professor of internal medicine at the 1st Faculty of Medicine at Charles University and deputy head of the Institute for Clinical and Experimental Medicine, both in Prague.
Currently, GLP-1 RAs are available only in a subcutaneous formulation, Dr. Haluzík reminded his audience, adding that oral semaglutide was the first GLP-1 RA to be developed in a tablet formulation and was in the late stages of clinical development.
PIONEER 1 is the first of 10 phase 3a trials with oral semaglutide to be reported. “Additional studies, across the full spectrum of diabetes care, in special populations, comparing it with active comparators with varied trial duration, have been completed or will be completed in 2018,” said coinvestigator for the study Vanita Aroda, MD, during a separate presentation at a dedicated symposium on the PIONEER program.
Dr. Aroda, the director of the diabetes research program at Brigham and Women’s Hospital in Boston, observed that oral semaglutide was being evaluated from early care as monotherapy in the PIONEER 1 study. The other trials, such as PIONEER 2, PIONEER 3, PIONEER 4, and PIONEER 7 were looking at oral semaglutide in combination with oral antidiabetic agents versus various active comparators; PIONEER 5 and PIONEER 6 were in special populations; and PIONEER 8 was looking at its use on top of basal insulin. Two further trials are also part of the study program.
“I think this is the first time that we actually have completed data of an entire program, including cardiovascular data, all within the same year,” Dr. Aroda said. “All of the studies are in the process of data analysis or data reporting.”
PIONEER 1 was a multicenter, randomized, double-blind, placebo-controlled trial examining efficacy and safety of semaglutide versus placebo in 703 adults with drug-naive T2DM who were being treated with diet and exercise only.
Three doses of oral semaglutide – 3 mg, 7 mg, and 14 mg – were assessed and compared with placebo. There was a fixed 4-week dose escalation period, with all patients starting treatment with 3 mg of semaglutide and then increasing to 7 mg by week 4 and 14 mg by week 8. This was to try to reduce the risk of gastrointestinal side effects, which are known to occur with GLP-1 RAs.
Secondary outcome measures were change in body weight, fasting plasma glucose, HbA1c below a target of 7% (53 mmol/mol), which were all measured from baseline to week 26; adverse events, including severe and blood glucose–confirmed symptomatic hypoglycemic episodes, were assessed out to week 31.
The average age of patients in the trial was around 55 years, around half were female, and the starting HbA1c was approximately 8%.The mean body weight ranged from 86.9 kg to 89 kg in the different treatment groups, with a similar body mass index of about 32 kg/m2.
Clinically meaningful weight loss, compared with placebo, was only achieved with the highest dose of oral semaglutide, with a –4.1 kg reduction versus –1.5 kg for placebo from baseline to week 26 (P less than .001, on-treatment analysis). Reductions in body weight for the 3-mg and 7-mg oral semaglutide doses were a respective –1.7 kg and –2.5 kg. ITT results were again similar, with weight losses of –1.5, –2.3, and –3.7 kg for the 3-, 7-, and 14-mg doses of oral semaglutide, respectively, and –1.4 kg for placebo.
More patients treated with oral semaglutide 3, 7, or 14 mg versus placebo achieved an HbA1c of below 7% (59.1%, 71.9%, and 80.3%, respectively, vs. 33.8%) or a body weight loss of 5% or more (21.3%, 28.7%, and 44.3% vs. 15.7%).
Furthermore, more patients treated with oral semaglutide achieved an HbA1c of or below 7% without hypoglycemic episodes or body weight gain than did those given placebo. There were also more patients who achieved an HbA1c reduction of at least 1% and a weight loss of 3% or higher.
“Oral semaglutide demonstrated a safety and tolerability profile consistent with that of [injectable] GLP-1 RAs,” Dr. Haluzík reported. Adverse events were seen in 57.7%, 53.1%, and 56.6%of patients treated with 3, 7, and 14 mg of oral semaglutide and 55.6% of those treated with placebo.
The most common adverse events seen with oral semaglutide affected the gastrointestinal tract, with nausea affecting 8%, 5.1%, and 16% of 3, 7, and 14 mg–treated patients versus 5.6% of placebo-treated patients. Vomiting affected a respective 2.9%, 4.6%, 6.9%, and 2.1%, and diarrhea a respective 8.6%, 5.1%, 5.1%, and 2.2%.
Severe or blood glucose–confirmed, symptomatic hypoglycemia was reported in 2.9%, 1.1%, and 0.6%of those treated with 3, 7, 14 mg of oral semaglutide and 0.6% of placebo-treated patients.
PIONEER 1 represents a “step change in GLP-1 receptor agonist therapy”, said Cliff Bailey, MD, who discussed the trial aa the EASD’s independent commentator during a symposium on the PIONEER program. These data are “leading to a new delivery route for GLP-1 receptor agonists, from injection to oral,” and “this can be done with good metabolic efficacy, with substantial reductions in A1c and body weight, and with a safety profile that’s comparable to the subcutaneous injection.”
Dr. Bailey, who is professor of clinical science at Aston University in Birmingham, England, noted, however, the oral dosing of semaglutide “requires patient commitment because it needs to be taken before breakfast time, and it may also, to some extent, affect the timing of some of the other medications.”
The study was sponsored by Novo Nordisk. Dr. Haluzík disclosed acting as a consultant to AstraZeneca, Eli Lilly, Johnson & Johnson, Mundipharma, Novatin, Novo Nordisk, and Sanofi Aventis. Dr. Aroda was an investigator in the PIONEER 1 study and disclosed acting as a consultant to Novo Nordisk; she also disclosed relationships with multiple other pharmaceutical companies, including AstraZeneca, BMS, Calbra, Eisai, Elcelyx Therapeutics, Janssen, and Sanofi Aventis. Dr. Bailey acknowledged attending advisory boards, undertaking ad hoc consultancy work, and receiving research and travel support from several pharmaceutical companies that included Novo Nordisk.
SOURCES: Haluzík M et al. EASD 2018, Abstract 38; Aroda V. EASD 2018, Session S18 - PIONEER Trial; Bailey C. EASD 2018, Session S18 - PIONEER Trial.
REPORTING FROM EASD 2018
Key clinical point: A novel oral formulation of semaglutide proved better than placebo for diabetes control and weight loss in patients with T2DM.
Major finding: Mean change in hemoglobin A1c (baseline to week 26) – the primary endpoint – using an on-treatment analysis was –0.8% with a once-daily dose of 3 mg, –1.3% with a once-daily dose of 7 mg, and –1.5% with a once-daily dose of 14 mg. The corresponding value for placebo was –0.1%.
Study details: Phase 3a, multicenter, randomized, double-blind, placebo-controlled trial examining efficacy and safety of semaglutide versus placebo in 703 individuals with T2DM being treated with diet and exercise only.
Disclosures: The study was sponsored by Novo Nordisk. Dr. Haluzík disclosed acting as a consultant to AstraZeneca, Eli Lilly, Johnson & Johnson, Mundipharma, Novatin, Novo Nordisk, and Sanofi Aventis. Dr. Aroda was an investigator in the PIONEER 1 study and disclosed acting as a consultant to Novo Nordisk. She also disclosed relationships with multiple other pharmaceutical companies, including AstraZeneca, BMS, Calbra, Eisai, Elcelyx Therapeutics, Janssen, and Sanofi Aventis. Dr. Bailey acknowledged attending advisory boards of, undertaking ad hoc consultancy work for, and receiving research and travel support from several pharmaceutical companies that included Novo Nordisk.
Source: Haluzík M et al. EASD 2018, Abstract 38; Aroda V. EASD 2018, Session S18 – PIONEER Trial; Bailey C. EASD 2018, Session S18 – PIONEER Trial.
Diet low in free sugars shows promise for adolescent NAFLD
after 8 weeks, compared with boys on a usual diet.
“Because of growing evidence implicating dietary sugars in NAFLD, well-controlled studies in children with NAFLD are needed to inform clinical practice and public policy,” wrote Jeffrey B. Schwimmer, MD, of the University of California, San Diego, La Jolla, and colleagues in JAMA.
The researchers randomized 40 boys aged 11-16 years with active NAFLD to a diet low in free sugars or their usual diet. The intervention diet involved personalized menu planning and provision of meals for the boys’ entire households that were designed to restrict free sugar intake to less than 3% of daily calories. Adherence to the diet was assessed by twice-weekly phone calls.
In the intervention group, hepatic steatosis decreased from an average of 25% at baseline to 17% after 8 weeks, compared with a change from 21% to 20% in the control group. The adjusted mean difference at 8 weeks was −6.23%, which was statistically significant (P less than .001).
The average age of the participants was 13 years, 95% were Hispanic. All 40 completed the study, and 18 of the 20 boys in the intervention group reported less than 3% of calories from free sugar during the study period. No adverse events were reported related to study participation.
The results were limited by several factors, including the small sample size and homogeneous population. In addition, neither hepatic steatosis or serum alanine aminotransferase (ALT) levels decreased enough to enter the normal range, the researchers noted. The findings, though preliminary, support the value of reducing free sugars, including glucose, fructose, and sucrose, to help manage NAFLD in adolescents, and “further research is required to assess long-term and clinical outcomes,” they said.
The study was supported by grants from multiple foundations and organizations, including the Nutrition Science Initiative, the University of California, San Diego, the National Institutes of Health, Children’s Healthcare of Atlanta and Emory University Pediatric Biostatistics Core, and the Georgia Clinical and Translational Science Alliance. Dr. Schwimmer reported receiving research support from Galmed and Intercept.
SOURCE: Schwimmer JB et al. JAMA. 2019;321(3):256-265.
after 8 weeks, compared with boys on a usual diet.
“Because of growing evidence implicating dietary sugars in NAFLD, well-controlled studies in children with NAFLD are needed to inform clinical practice and public policy,” wrote Jeffrey B. Schwimmer, MD, of the University of California, San Diego, La Jolla, and colleagues in JAMA.
The researchers randomized 40 boys aged 11-16 years with active NAFLD to a diet low in free sugars or their usual diet. The intervention diet involved personalized menu planning and provision of meals for the boys’ entire households that were designed to restrict free sugar intake to less than 3% of daily calories. Adherence to the diet was assessed by twice-weekly phone calls.
In the intervention group, hepatic steatosis decreased from an average of 25% at baseline to 17% after 8 weeks, compared with a change from 21% to 20% in the control group. The adjusted mean difference at 8 weeks was −6.23%, which was statistically significant (P less than .001).
The average age of the participants was 13 years, 95% were Hispanic. All 40 completed the study, and 18 of the 20 boys in the intervention group reported less than 3% of calories from free sugar during the study period. No adverse events were reported related to study participation.
The results were limited by several factors, including the small sample size and homogeneous population. In addition, neither hepatic steatosis or serum alanine aminotransferase (ALT) levels decreased enough to enter the normal range, the researchers noted. The findings, though preliminary, support the value of reducing free sugars, including glucose, fructose, and sucrose, to help manage NAFLD in adolescents, and “further research is required to assess long-term and clinical outcomes,” they said.
The study was supported by grants from multiple foundations and organizations, including the Nutrition Science Initiative, the University of California, San Diego, the National Institutes of Health, Children’s Healthcare of Atlanta and Emory University Pediatric Biostatistics Core, and the Georgia Clinical and Translational Science Alliance. Dr. Schwimmer reported receiving research support from Galmed and Intercept.
SOURCE: Schwimmer JB et al. JAMA. 2019;321(3):256-265.
after 8 weeks, compared with boys on a usual diet.
“Because of growing evidence implicating dietary sugars in NAFLD, well-controlled studies in children with NAFLD are needed to inform clinical practice and public policy,” wrote Jeffrey B. Schwimmer, MD, of the University of California, San Diego, La Jolla, and colleagues in JAMA.
The researchers randomized 40 boys aged 11-16 years with active NAFLD to a diet low in free sugars or their usual diet. The intervention diet involved personalized menu planning and provision of meals for the boys’ entire households that were designed to restrict free sugar intake to less than 3% of daily calories. Adherence to the diet was assessed by twice-weekly phone calls.
In the intervention group, hepatic steatosis decreased from an average of 25% at baseline to 17% after 8 weeks, compared with a change from 21% to 20% in the control group. The adjusted mean difference at 8 weeks was −6.23%, which was statistically significant (P less than .001).
The average age of the participants was 13 years, 95% were Hispanic. All 40 completed the study, and 18 of the 20 boys in the intervention group reported less than 3% of calories from free sugar during the study period. No adverse events were reported related to study participation.
The results were limited by several factors, including the small sample size and homogeneous population. In addition, neither hepatic steatosis or serum alanine aminotransferase (ALT) levels decreased enough to enter the normal range, the researchers noted. The findings, though preliminary, support the value of reducing free sugars, including glucose, fructose, and sucrose, to help manage NAFLD in adolescents, and “further research is required to assess long-term and clinical outcomes,” they said.
The study was supported by grants from multiple foundations and organizations, including the Nutrition Science Initiative, the University of California, San Diego, the National Institutes of Health, Children’s Healthcare of Atlanta and Emory University Pediatric Biostatistics Core, and the Georgia Clinical and Translational Science Alliance. Dr. Schwimmer reported receiving research support from Galmed and Intercept.
SOURCE: Schwimmer JB et al. JAMA. 2019;321(3):256-265.
FROM JAMA
Key clinical point: After 8 weeks, adolescent boys on a diet low in free sugars showed significant improvement in hepatic steatosis, compared with those on a usual diet.
Major finding: Hepatic steatosis decreased from an average of 25% at baseline to 17% after 8 weeks in the modified diet group, compared with a decrease from 21% to 20% in the usual diet group.
Study details: The data come from an open-label, randomized trial of 40 adolescent boys aged 11 to 16 years with active NAFLD.
Disclosures: The study was supported by grants from multiple foundations and organizations, including the Nutrition Science Initiative, the University of California, San Diego, the National Institutes of Health, Children’s Healthcare of Atlanta and Emory University Pediatric Biostatistics Core, and the Georgia Clinical and Translational Science Alliance. Dr. Schwimmer reported receiving research support from Galmed and Intercept.
Source: Schwimmer JB et al. JAMA. 2019;321(3):256-265.
Confidential, parent-free discussion should occur by age 13
Discussing confidentiality is essential to the appropriate health care of adolescents, especially prior to discussing sensitive subjects, reported John S. Santelli, MD, MPH, of Mailman School of Public Health, Columbia University, New York, N.Y., and his associates.

“Previous research has shown that when adolescents and young adults (AYAs) are not assured of confidentiality, they are less willing to discuss sensitive topics with their providers,” they wrote. The report is in Pediatrics.
According to national guidelines, although discussions concerning confidentiality can begin with parents in early adolescence, over time, the goal should be to allow fully for alone time for the AYA with you without parents present in the room.
You have a unique opportunity to help parents understand confidentiality and aid them in transitioning over time, with full respect and support for the developing adolescent-provider relationship, so that it can be fully realized by the time the adolescent reaches 13 years of age.
Using a nationally representative age-, race/ethnicity-, and income-matched sample of AYAs, the authors surveyed youth aged 13-26 years concerning preventive services received and discussions held with health care providers. Of the 1,918 individuals who completed the survey, the authors’ analysis was limited to the 1,509 (79%) youth who had seen their providers in the past 2 years.
The study focused on 11 youth-provider discussion topics. For 10 of the 11 topics, less than half of the young people said they had a discussion on the topic with a health care provider on their last visit. The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%). There were more discussions concerning birth control among young women (from 26% at ages 13-14 to 54% by ages 23-26) compared with young men (13% at ages 13-14 to 12% by ages 23-26).
On average, young women reported discussing just 3.7 of the 11 topics during their last preventive care visit; young men similarly reported an average of 3.6 topics. Overall, the mean number of youth-provider discussions declined over time from 4.1 at ages 13-14 and 4.4 at ages 15-18 to 2.6 by ages 23-26.
Compared with white youth, who reported 3.3 topics at their last visit, Hispanic and African American youth reported discussing 4.2 topics. Similar differences were seen when comparing rural (2.7 topics) and urban or suburban youth (3.8 topics) or incomes greater than $75,000 (3.6 topics) compared with incomes of $25,000 or less (4.2 topics).
Youth who previously discussed confidentiality also reported discussing more topics (4.4), compared with those who had not talked about confidentiality (2.9).
Before the implementation of the Patient Protection and Affordable Care Act (ACA), which requires the provision of prevention services without cost sharing, less than half of adolescents visited a medical provider for annual preventive care visits, other studies have shown.
Although professional guidelines for adolescent preventive care recommend youth access to confidential services, “young people report that health care encounters often do not include an explanation of confidentiality by their health care provider.” Without the assurance of confidentiality, adolescents are more likely to not seek care or to opt not to disclose risky behaviors.
Current systems tend to rely on parent reporting regarding uses of services, and there is no mechanism in place for collection of data on discussion of sensitive health topics. The authors also noted a lack of time available for dialogue during visits as well as an absence of screening questionnaires prior to visits that might invite opportunities to disclose information on sensitive topics.
“Young people who reported ever having talked about confidentiality with their regular provider were more likely to engage in health discussions with providers,” emphasized Dr. Santelli and his associates. “The use of a health checklist and/or questionnaire and having spent more time with their provider during the visit were consistently associated with more of these discussions.”
You can build rapport with AYAs during preventive care visits that include screening and counseling. Immunizations, screening, and treatment of sexually transmitted infections, and dispensing of reproductive and sexual health services, including contraception, offer good opportunities for these discussions. Other sensitive topics are tobacco, alcohol, and drug use; depression and mental health; and obesity and physical activity.
Dr. Santelli and his associates consider the results of their research to serve as a “valuable addition to the literature.” They did, however, note several limitations. Because the data are cross-sectional, they cannot demonstrate causality. The use of self-report data may have contributed to underreporting of risk behaviors because adolescents were interviewed directly following parents on the same computer. Survey questions did account for the existence of youth-provider discussions, but the researchers were not able to measure the impact or quality of the resulting conversations.
It is important to note that because providers were not interviewed, the time pressures and other expected barriers were not fully accounted for in this research, Dr. Santelli and his colleagues cautioned. “Future research should ask specifically about provider-level barriers to providing preventive care to better understand their impact,” they advised.
Ultimately, the clinicians who are providing care to youth and their families will need support in implementing such changes, especially where education in the importance of discussion confidentiality and private time are concerned, they added.
The authors had no relevant financial disclosures. The study was funded by an unrestricted research grant from the Merck Foundation.
SOURCE: Santelli J et. al. Pediatrics. 2019. doi: 10.1542/peds.2018-1403.
Passage of the Affordable Care Act “provides a rich opportunity to improve the delivery of adolescent preventive services,” by lowering the financial barriers that had impeded preventive care, Jeanne Van Cleave, MD, wrote in an editorial published with the study. The findings in Santelli et al. “provide important direction for efforts to improve the delivery of adolescent preventive care.”
Specifically, changing office culture to ensure consistent screening, private time with providers, and policies that ensure discussion of confidentiality, can be accomplished by incorporating new roles for office staff, establishing team-based care, and requiring performance measurement. “By involving the whole practice, the burden of ensuring the elements of adolescent preventive care that facilitate discussion of potentially sensitive topics is lifted from individual providers,” advised Dr. Van Cleave.
Essential to the success of such a revised model of care is the practice-wide implementation and understanding of confidentiality. Dr. Van Cleave envisions a partnership between front-desk staff, medical assistants, and providers for administering screening tools and explaining to families the role of private time as well as confidentiality policies. Also essential is routine measurement of performance; the success of such a system would depend upon identifying where the gaps in care exist and what the options are for improving those gaps, she explained.
The use of alternative providers, such as nurses, social workers, or even properly trained parents, is a concept that has been tested previously. They afford greater flexibility, both during and outside of regular office hours, and they have been shown to raise the level of comfort among some youth who might otherwise be reluctant to discuss sensitive topics with their regular providers. These providers can be contacted by families outside of office visits when there are questions, giving advice and counseling by phone and electronic communication.
Dr. Van Cleave points out that while adolescents have many resources at their disposal for researching sensitive topics, including parents, social media, and even school health programs, such sources have been known to provide less accurate or incomplete information, compared with the specific, individually-tailored advice that only the primary care provider can give.
The important take-away message from the Santelli et al. report is that regular discussion of potentially sensitive topics in pediatric primary care leads to “positive patterns for seeking help later in adulthood,” Dr. Van Cleave observed. Their research offers important evidence concerning what needs to change in the practice care environment to facilitate these improvements.
What comes next, namely development and testing of appropriate interventions, will determine whether we can effectively change the role health care has to play in mitigating health risks for this population, she concluded.
Dr. Van Cleave is affiliated with Children’s Hospital Colorado and adult and child consortium for health outcomes research and delivery science, University of Colorado, Aurora. These comments are excerpted from an editorial by Dr. Van Cleave on the study by Santelli et al. (Pediatrics. 2019. doi: 10.1542/peds.2018-3618). She had no relevant financial disclosures and received no external funding.
Passage of the Affordable Care Act “provides a rich opportunity to improve the delivery of adolescent preventive services,” by lowering the financial barriers that had impeded preventive care, Jeanne Van Cleave, MD, wrote in an editorial published with the study. The findings in Santelli et al. “provide important direction for efforts to improve the delivery of adolescent preventive care.”
Specifically, changing office culture to ensure consistent screening, private time with providers, and policies that ensure discussion of confidentiality, can be accomplished by incorporating new roles for office staff, establishing team-based care, and requiring performance measurement. “By involving the whole practice, the burden of ensuring the elements of adolescent preventive care that facilitate discussion of potentially sensitive topics is lifted from individual providers,” advised Dr. Van Cleave.
Essential to the success of such a revised model of care is the practice-wide implementation and understanding of confidentiality. Dr. Van Cleave envisions a partnership between front-desk staff, medical assistants, and providers for administering screening tools and explaining to families the role of private time as well as confidentiality policies. Also essential is routine measurement of performance; the success of such a system would depend upon identifying where the gaps in care exist and what the options are for improving those gaps, she explained.
The use of alternative providers, such as nurses, social workers, or even properly trained parents, is a concept that has been tested previously. They afford greater flexibility, both during and outside of regular office hours, and they have been shown to raise the level of comfort among some youth who might otherwise be reluctant to discuss sensitive topics with their regular providers. These providers can be contacted by families outside of office visits when there are questions, giving advice and counseling by phone and electronic communication.
Dr. Van Cleave points out that while adolescents have many resources at their disposal for researching sensitive topics, including parents, social media, and even school health programs, such sources have been known to provide less accurate or incomplete information, compared with the specific, individually-tailored advice that only the primary care provider can give.
The important take-away message from the Santelli et al. report is that regular discussion of potentially sensitive topics in pediatric primary care leads to “positive patterns for seeking help later in adulthood,” Dr. Van Cleave observed. Their research offers important evidence concerning what needs to change in the practice care environment to facilitate these improvements.
What comes next, namely development and testing of appropriate interventions, will determine whether we can effectively change the role health care has to play in mitigating health risks for this population, she concluded.
Dr. Van Cleave is affiliated with Children’s Hospital Colorado and adult and child consortium for health outcomes research and delivery science, University of Colorado, Aurora. These comments are excerpted from an editorial by Dr. Van Cleave on the study by Santelli et al. (Pediatrics. 2019. doi: 10.1542/peds.2018-3618). She had no relevant financial disclosures and received no external funding.
Passage of the Affordable Care Act “provides a rich opportunity to improve the delivery of adolescent preventive services,” by lowering the financial barriers that had impeded preventive care, Jeanne Van Cleave, MD, wrote in an editorial published with the study. The findings in Santelli et al. “provide important direction for efforts to improve the delivery of adolescent preventive care.”
Specifically, changing office culture to ensure consistent screening, private time with providers, and policies that ensure discussion of confidentiality, can be accomplished by incorporating new roles for office staff, establishing team-based care, and requiring performance measurement. “By involving the whole practice, the burden of ensuring the elements of adolescent preventive care that facilitate discussion of potentially sensitive topics is lifted from individual providers,” advised Dr. Van Cleave.
Essential to the success of such a revised model of care is the practice-wide implementation and understanding of confidentiality. Dr. Van Cleave envisions a partnership between front-desk staff, medical assistants, and providers for administering screening tools and explaining to families the role of private time as well as confidentiality policies. Also essential is routine measurement of performance; the success of such a system would depend upon identifying where the gaps in care exist and what the options are for improving those gaps, she explained.
The use of alternative providers, such as nurses, social workers, or even properly trained parents, is a concept that has been tested previously. They afford greater flexibility, both during and outside of regular office hours, and they have been shown to raise the level of comfort among some youth who might otherwise be reluctant to discuss sensitive topics with their regular providers. These providers can be contacted by families outside of office visits when there are questions, giving advice and counseling by phone and electronic communication.
Dr. Van Cleave points out that while adolescents have many resources at their disposal for researching sensitive topics, including parents, social media, and even school health programs, such sources have been known to provide less accurate or incomplete information, compared with the specific, individually-tailored advice that only the primary care provider can give.
The important take-away message from the Santelli et al. report is that regular discussion of potentially sensitive topics in pediatric primary care leads to “positive patterns for seeking help later in adulthood,” Dr. Van Cleave observed. Their research offers important evidence concerning what needs to change in the practice care environment to facilitate these improvements.
What comes next, namely development and testing of appropriate interventions, will determine whether we can effectively change the role health care has to play in mitigating health risks for this population, she concluded.
Dr. Van Cleave is affiliated with Children’s Hospital Colorado and adult and child consortium for health outcomes research and delivery science, University of Colorado, Aurora. These comments are excerpted from an editorial by Dr. Van Cleave on the study by Santelli et al. (Pediatrics. 2019. doi: 10.1542/peds.2018-3618). She had no relevant financial disclosures and received no external funding.
Discussing confidentiality is essential to the appropriate health care of adolescents, especially prior to discussing sensitive subjects, reported John S. Santelli, MD, MPH, of Mailman School of Public Health, Columbia University, New York, N.Y., and his associates.
“Previous research has shown that when adolescents and young adults (AYAs) are not assured of confidentiality, they are less willing to discuss sensitive topics with their providers,” they wrote. The report is in Pediatrics.
According to national guidelines, although discussions concerning confidentiality can begin with parents in early adolescence, over time, the goal should be to allow fully for alone time for the AYA with you without parents present in the room.
You have a unique opportunity to help parents understand confidentiality and aid them in transitioning over time, with full respect and support for the developing adolescent-provider relationship, so that it can be fully realized by the time the adolescent reaches 13 years of age.
Using a nationally representative age-, race/ethnicity-, and income-matched sample of AYAs, the authors surveyed youth aged 13-26 years concerning preventive services received and discussions held with health care providers. Of the 1,918 individuals who completed the survey, the authors’ analysis was limited to the 1,509 (79%) youth who had seen their providers in the past 2 years.
The study focused on 11 youth-provider discussion topics. For 10 of the 11 topics, less than half of the young people said they had a discussion on the topic with a health care provider on their last visit. The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%). There were more discussions concerning birth control among young women (from 26% at ages 13-14 to 54% by ages 23-26) compared with young men (13% at ages 13-14 to 12% by ages 23-26).
On average, young women reported discussing just 3.7 of the 11 topics during their last preventive care visit; young men similarly reported an average of 3.6 topics. Overall, the mean number of youth-provider discussions declined over time from 4.1 at ages 13-14 and 4.4 at ages 15-18 to 2.6 by ages 23-26.
Compared with white youth, who reported 3.3 topics at their last visit, Hispanic and African American youth reported discussing 4.2 topics. Similar differences were seen when comparing rural (2.7 topics) and urban or suburban youth (3.8 topics) or incomes greater than $75,000 (3.6 topics) compared with incomes of $25,000 or less (4.2 topics).
Youth who previously discussed confidentiality also reported discussing more topics (4.4), compared with those who had not talked about confidentiality (2.9).
Before the implementation of the Patient Protection and Affordable Care Act (ACA), which requires the provision of prevention services without cost sharing, less than half of adolescents visited a medical provider for annual preventive care visits, other studies have shown.
Although professional guidelines for adolescent preventive care recommend youth access to confidential services, “young people report that health care encounters often do not include an explanation of confidentiality by their health care provider.” Without the assurance of confidentiality, adolescents are more likely to not seek care or to opt not to disclose risky behaviors.
Current systems tend to rely on parent reporting regarding uses of services, and there is no mechanism in place for collection of data on discussion of sensitive health topics. The authors also noted a lack of time available for dialogue during visits as well as an absence of screening questionnaires prior to visits that might invite opportunities to disclose information on sensitive topics.
“Young people who reported ever having talked about confidentiality with their regular provider were more likely to engage in health discussions with providers,” emphasized Dr. Santelli and his associates. “The use of a health checklist and/or questionnaire and having spent more time with their provider during the visit were consistently associated with more of these discussions.”
You can build rapport with AYAs during preventive care visits that include screening and counseling. Immunizations, screening, and treatment of sexually transmitted infections, and dispensing of reproductive and sexual health services, including contraception, offer good opportunities for these discussions. Other sensitive topics are tobacco, alcohol, and drug use; depression and mental health; and obesity and physical activity.
Dr. Santelli and his associates consider the results of their research to serve as a “valuable addition to the literature.” They did, however, note several limitations. Because the data are cross-sectional, they cannot demonstrate causality. The use of self-report data may have contributed to underreporting of risk behaviors because adolescents were interviewed directly following parents on the same computer. Survey questions did account for the existence of youth-provider discussions, but the researchers were not able to measure the impact or quality of the resulting conversations.
It is important to note that because providers were not interviewed, the time pressures and other expected barriers were not fully accounted for in this research, Dr. Santelli and his colleagues cautioned. “Future research should ask specifically about provider-level barriers to providing preventive care to better understand their impact,” they advised.
Ultimately, the clinicians who are providing care to youth and their families will need support in implementing such changes, especially where education in the importance of discussion confidentiality and private time are concerned, they added.
The authors had no relevant financial disclosures. The study was funded by an unrestricted research grant from the Merck Foundation.
SOURCE: Santelli J et. al. Pediatrics. 2019. doi: 10.1542/peds.2018-1403.
Discussing confidentiality is essential to the appropriate health care of adolescents, especially prior to discussing sensitive subjects, reported John S. Santelli, MD, MPH, of Mailman School of Public Health, Columbia University, New York, N.Y., and his associates.
“Previous research has shown that when adolescents and young adults (AYAs) are not assured of confidentiality, they are less willing to discuss sensitive topics with their providers,” they wrote. The report is in Pediatrics.
According to national guidelines, although discussions concerning confidentiality can begin with parents in early adolescence, over time, the goal should be to allow fully for alone time for the AYA with you without parents present in the room.
You have a unique opportunity to help parents understand confidentiality and aid them in transitioning over time, with full respect and support for the developing adolescent-provider relationship, so that it can be fully realized by the time the adolescent reaches 13 years of age.
Using a nationally representative age-, race/ethnicity-, and income-matched sample of AYAs, the authors surveyed youth aged 13-26 years concerning preventive services received and discussions held with health care providers. Of the 1,918 individuals who completed the survey, the authors’ analysis was limited to the 1,509 (79%) youth who had seen their providers in the past 2 years.
The study focused on 11 youth-provider discussion topics. For 10 of the 11 topics, less than half of the young people said they had a discussion on the topic with a health care provider on their last visit. The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%). There were more discussions concerning birth control among young women (from 26% at ages 13-14 to 54% by ages 23-26) compared with young men (13% at ages 13-14 to 12% by ages 23-26).
On average, young women reported discussing just 3.7 of the 11 topics during their last preventive care visit; young men similarly reported an average of 3.6 topics. Overall, the mean number of youth-provider discussions declined over time from 4.1 at ages 13-14 and 4.4 at ages 15-18 to 2.6 by ages 23-26.
Compared with white youth, who reported 3.3 topics at their last visit, Hispanic and African American youth reported discussing 4.2 topics. Similar differences were seen when comparing rural (2.7 topics) and urban or suburban youth (3.8 topics) or incomes greater than $75,000 (3.6 topics) compared with incomes of $25,000 or less (4.2 topics).
Youth who previously discussed confidentiality also reported discussing more topics (4.4), compared with those who had not talked about confidentiality (2.9).
Before the implementation of the Patient Protection and Affordable Care Act (ACA), which requires the provision of prevention services without cost sharing, less than half of adolescents visited a medical provider for annual preventive care visits, other studies have shown.
Although professional guidelines for adolescent preventive care recommend youth access to confidential services, “young people report that health care encounters often do not include an explanation of confidentiality by their health care provider.” Without the assurance of confidentiality, adolescents are more likely to not seek care or to opt not to disclose risky behaviors.
Current systems tend to rely on parent reporting regarding uses of services, and there is no mechanism in place for collection of data on discussion of sensitive health topics. The authors also noted a lack of time available for dialogue during visits as well as an absence of screening questionnaires prior to visits that might invite opportunities to disclose information on sensitive topics.
“Young people who reported ever having talked about confidentiality with their regular provider were more likely to engage in health discussions with providers,” emphasized Dr. Santelli and his associates. “The use of a health checklist and/or questionnaire and having spent more time with their provider during the visit were consistently associated with more of these discussions.”
You can build rapport with AYAs during preventive care visits that include screening and counseling. Immunizations, screening, and treatment of sexually transmitted infections, and dispensing of reproductive and sexual health services, including contraception, offer good opportunities for these discussions. Other sensitive topics are tobacco, alcohol, and drug use; depression and mental health; and obesity and physical activity.
Dr. Santelli and his associates consider the results of their research to serve as a “valuable addition to the literature.” They did, however, note several limitations. Because the data are cross-sectional, they cannot demonstrate causality. The use of self-report data may have contributed to underreporting of risk behaviors because adolescents were interviewed directly following parents on the same computer. Survey questions did account for the existence of youth-provider discussions, but the researchers were not able to measure the impact or quality of the resulting conversations.
It is important to note that because providers were not interviewed, the time pressures and other expected barriers were not fully accounted for in this research, Dr. Santelli and his colleagues cautioned. “Future research should ask specifically about provider-level barriers to providing preventive care to better understand their impact,” they advised.
Ultimately, the clinicians who are providing care to youth and their families will need support in implementing such changes, especially where education in the importance of discussion confidentiality and private time are concerned, they added.
The authors had no relevant financial disclosures. The study was funded by an unrestricted research grant from the Merck Foundation.
SOURCE: Santelli J et. al. Pediatrics. 2019. doi: 10.1542/peds.2018-1403.
FROM PEDIATRICS
Key clinical point:
Major finding: The most commonly discussed topics overall included mental health/emotional issues (55%), drug or alcohol use (46%), tobacco use (44%), and school performance (43%); the least common were gun safety (14%), sexual orientation (20%), and sexual or physical abuse (21%).
Study details: Self-report survey.
Disclosures: The authors had no financial relationships relevant to this article to disclose. The study was funded by an unrestricted research grant from the Merck Foundation.
Source: Santelli J. et. al. Pediatrics. 2019;143(2):e20181403.

Obesity paradox applies to post-stroke mortality
CHICAGO – Overweight and obese military veterans who experienced an in-hospital stroke had a lower 30-day and 1-year all-cause mortality than did those who were normal weight in a large national study, Lauren Costa reported at the American Heart Association scientific sessions.
Underweight patients had a significantly increased mortality risk, added Ms. Costa of the VA Boston Healthcare System.
It’s yet another instance of what is known as the obesity paradox, which has also been described in patients with heart failure, acute coronary syndrome, MI, chronic obstructive pulmonary disease, and other conditions.
Ms. Costa presented a retrospective study of 26,267 patients in the Veterans Health Administration database who had a first stroke in-hospital during 2002-2012. There were subsequently 14,166 deaths, including 2,473 within the first 30 days and 5,854 in the first year post stroke.
Each patient’s body mass index was calculated based on the average of all BMI measurements obtained 1-24 months prior to the stroke. The analysis of the relationship between BMI and poststroke mortality included extensive statistical adjustment for potential confounders, including age, sex, smoking, cancer, dementia, peripheral artery disease, diabetes, coronary heart disease, atrial fibrillation, chronic kidney disease, use of statins, and antihypertensive therapy.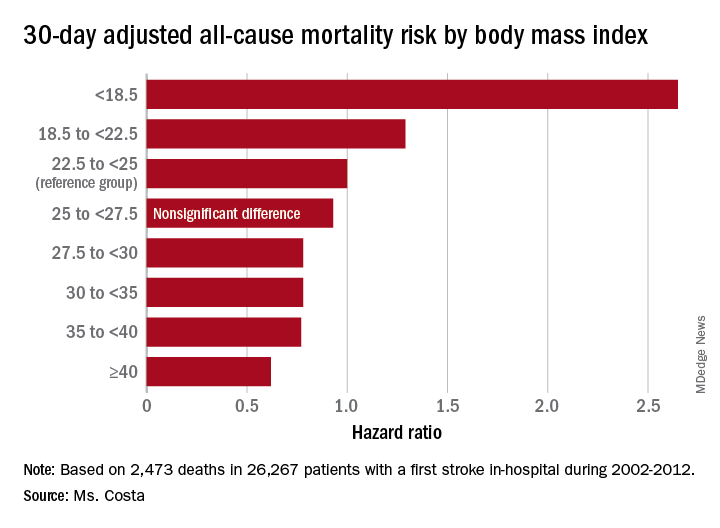
Breaking down the study population into eight BMI categories, Ms. Costa found that the adjusted risk of 30-day all-cause mortality post stroke was reduced by 22%-38% in patients in the overweight or obese groupings, compared with the reference population with a normal-weight BMI of 22.5 to less than 25 kg/m2.
One-year, all-cause mortality showed the same pattern of BMI-based significant differences.
Of deaths within 30 days post stroke, 34% were stroke-related. In an analysis restricted to that group, the evidence of an obesity paradox was attenuated. Indeed, the only BMI group with an adjusted 30-day stroke-related mortality significantly different from the normal-weight reference group were patients with Class III obesity, defined as a BMI of 40 or more. Their risk was reduced by 45%.
The obesity paradox remains a controversial issue among epidemiologists. The increased mortality associated with being underweight among patients with diseases where the obesity paradox has been documented is widely thought to be caused by frailty and/or an underlying illness not adjusted for in analyses. But the mechanism for the reduced mortality risk in overweight and obese patients seen in the VA stroke study and other studies remains unknown despite much speculation.
Ms. Costa reported having no financial conflicts regarding her study, which was supported by the Department of Veterans Affairs.
SOURCE: Costa L. Circulation. 2018;138(suppl 1): Abstract 14288.
CHICAGO – Overweight and obese military veterans who experienced an in-hospital stroke had a lower 30-day and 1-year all-cause mortality than did those who were normal weight in a large national study, Lauren Costa reported at the American Heart Association scientific sessions.
Underweight patients had a significantly increased mortality risk, added Ms. Costa of the VA Boston Healthcare System.
It’s yet another instance of what is known as the obesity paradox, which has also been described in patients with heart failure, acute coronary syndrome, MI, chronic obstructive pulmonary disease, and other conditions.
Ms. Costa presented a retrospective study of 26,267 patients in the Veterans Health Administration database who had a first stroke in-hospital during 2002-2012. There were subsequently 14,166 deaths, including 2,473 within the first 30 days and 5,854 in the first year post stroke.
Each patient’s body mass index was calculated based on the average of all BMI measurements obtained 1-24 months prior to the stroke. The analysis of the relationship between BMI and poststroke mortality included extensive statistical adjustment for potential confounders, including age, sex, smoking, cancer, dementia, peripheral artery disease, diabetes, coronary heart disease, atrial fibrillation, chronic kidney disease, use of statins, and antihypertensive therapy.
Breaking down the study population into eight BMI categories, Ms. Costa found that the adjusted risk of 30-day all-cause mortality post stroke was reduced by 22%-38% in patients in the overweight or obese groupings, compared with the reference population with a normal-weight BMI of 22.5 to less than 25 kg/m2.
One-year, all-cause mortality showed the same pattern of BMI-based significant differences.
Of deaths within 30 days post stroke, 34% were stroke-related. In an analysis restricted to that group, the evidence of an obesity paradox was attenuated. Indeed, the only BMI group with an adjusted 30-day stroke-related mortality significantly different from the normal-weight reference group were patients with Class III obesity, defined as a BMI of 40 or more. Their risk was reduced by 45%.
The obesity paradox remains a controversial issue among epidemiologists. The increased mortality associated with being underweight among patients with diseases where the obesity paradox has been documented is widely thought to be caused by frailty and/or an underlying illness not adjusted for in analyses. But the mechanism for the reduced mortality risk in overweight and obese patients seen in the VA stroke study and other studies remains unknown despite much speculation.
Ms. Costa reported having no financial conflicts regarding her study, which was supported by the Department of Veterans Affairs.
SOURCE: Costa L. Circulation. 2018;138(suppl 1): Abstract 14288.
CHICAGO – Overweight and obese military veterans who experienced an in-hospital stroke had a lower 30-day and 1-year all-cause mortality than did those who were normal weight in a large national study, Lauren Costa reported at the American Heart Association scientific sessions.
Underweight patients had a significantly increased mortality risk, added Ms. Costa of the VA Boston Healthcare System.
It’s yet another instance of what is known as the obesity paradox, which has also been described in patients with heart failure, acute coronary syndrome, MI, chronic obstructive pulmonary disease, and other conditions.
Ms. Costa presented a retrospective study of 26,267 patients in the Veterans Health Administration database who had a first stroke in-hospital during 2002-2012. There were subsequently 14,166 deaths, including 2,473 within the first 30 days and 5,854 in the first year post stroke.
Each patient’s body mass index was calculated based on the average of all BMI measurements obtained 1-24 months prior to the stroke. The analysis of the relationship between BMI and poststroke mortality included extensive statistical adjustment for potential confounders, including age, sex, smoking, cancer, dementia, peripheral artery disease, diabetes, coronary heart disease, atrial fibrillation, chronic kidney disease, use of statins, and antihypertensive therapy.
Breaking down the study population into eight BMI categories, Ms. Costa found that the adjusted risk of 30-day all-cause mortality post stroke was reduced by 22%-38% in patients in the overweight or obese groupings, compared with the reference population with a normal-weight BMI of 22.5 to less than 25 kg/m2.
One-year, all-cause mortality showed the same pattern of BMI-based significant differences.
Of deaths within 30 days post stroke, 34% were stroke-related. In an analysis restricted to that group, the evidence of an obesity paradox was attenuated. Indeed, the only BMI group with an adjusted 30-day stroke-related mortality significantly different from the normal-weight reference group were patients with Class III obesity, defined as a BMI of 40 or more. Their risk was reduced by 45%.
The obesity paradox remains a controversial issue among epidemiologists. The increased mortality associated with being underweight among patients with diseases where the obesity paradox has been documented is widely thought to be caused by frailty and/or an underlying illness not adjusted for in analyses. But the mechanism for the reduced mortality risk in overweight and obese patients seen in the VA stroke study and other studies remains unknown despite much speculation.
Ms. Costa reported having no financial conflicts regarding her study, which was supported by the Department of Veterans Affairs.
SOURCE: Costa L. Circulation. 2018;138(suppl 1): Abstract 14288.
REPORTING FROM THE AHA SCIENTIFIC SESSIONS
Key clinical point: Heavier stroke patients have lower 30-day and 1-year all-cause mortality.
Major finding: The 30-day stroke-related mortality rate after in-hospital stroke was reduced by 45% in VA patients with Class III obesity.
Study details: This retrospective study looked at the relationship between body mass index and post-stroke mortality in more than 26,000 veterans who had an inpatient stroke, with extensive adjustments made for potential confounders.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was sponsored by the Department of Veterans Affairs.
Source: Costa L. Circulation. 2018;138(suppl 1): Abstract 14288.
Tic disorders are associated with obesity and diabetes
The movement disorders are associated with cardiometabolic problems “even after taking into account a number of covariates and shared familial confounders and excluding relevant psychiatric comorbidities,” the researchers wrote. “The results highlight the importance of carefully monitoring cardiometabolic health in patients with Tourette syndrome or chronic tic disorder across the lifespan, particularly in those with comorbid attention-deficit/hyperactivity disorder (ADHD).”
Gustaf Brander, a researcher in the department of clinical neuroscience at Karolinska Institutet in Stockholm, and his colleagues conducted a longitudinal population-based cohort study of individuals living in Sweden between Jan. 1, 1973, and Dec. 31, 2013. The researchers assessed outcomes for patients with previously validated diagnoses of Tourette syndrome or chronic tic disorder in the Swedish National Patient Register. Main outcomes included obesity, dyslipidemia, hypertension, T2DM, and cardiovascular diseases, including ischemic heart diseases, arrhythmia, cerebrovascular diseases, transient ischemic attack, and arteriosclerosis. In addition, the researchers identified families with full siblings discordant for Tourette syndrome or chronic tic disorder.
Of the more than 14 million individuals in the cohort, 7,804 (76.4% male; median age at first diagnosis, 13.3 years) had a diagnosis of Tourette syndrome or chronic tic disorder in specialist care. Furthermore, the cohort included 5,141 families with full siblings who were discordant for these disorders.
Individuals with Tourette syndrome or chronic tic disorder had a higher risk for any metabolic or cardiovascular disorder, compared with the general population (hazard ratio adjusted by sex and birth year [aHR], 1.99) and sibling controls (aHR, 1.37). Specifically, individuals with Tourette syndrome or chronic tic disorder had higher risks for obesity (aHR, 2.76), T2DM(aHR, 1.67), and circulatory system diseases (aHR, 1.76).
The increased risk of any cardiometabolic disorder was significantly greater for males than it was for females (aHRs, 2.13 vs. 1.79), as was the risk of obesity (aHRs, 3.24 vs. 1.97).
The increased risk for cardiometabolic disorders in this patient population was evident by age 8 years. Exclusion of those patients with comorbid ADHD reduced but did not eliminate the risk (aHR, 1.52). The exclusion of other comorbidities did not significantly affect the results. Among patients with Tourette syndrome or chronic tic disorder, those who had received antipsychotic treatment for more than 1 year were significantly less likely to have metabolic and cardiovascular disorders, compared with patients not taking antipsychotic medication. This association may be related to “greater medical vigilance” and “should not be taken as evidence that antipsychotics are free from cardiometabolic adverse effects,” the authors noted.
The study was supported by a research grant from Tourettes Action. In addition, authors reported support from the Swedish Research Council and a Karolinska Institutet PhD stipend. Two authors disclosed personal fees from publishers, and one author disclosed grants and other funding from Shire.
jremaly@mdedge.com
SOURCE: Brander G et al. JAMA Neurol. 2019 Jan 14. doi: 10.1001/jamaneurol.2018.4279.
The movement disorders are associated with cardiometabolic problems “even after taking into account a number of covariates and shared familial confounders and excluding relevant psychiatric comorbidities,” the researchers wrote. “The results highlight the importance of carefully monitoring cardiometabolic health in patients with Tourette syndrome or chronic tic disorder across the lifespan, particularly in those with comorbid attention-deficit/hyperactivity disorder (ADHD).”
Gustaf Brander, a researcher in the department of clinical neuroscience at Karolinska Institutet in Stockholm, and his colleagues conducted a longitudinal population-based cohort study of individuals living in Sweden between Jan. 1, 1973, and Dec. 31, 2013. The researchers assessed outcomes for patients with previously validated diagnoses of Tourette syndrome or chronic tic disorder in the Swedish National Patient Register. Main outcomes included obesity, dyslipidemia, hypertension, T2DM, and cardiovascular diseases, including ischemic heart diseases, arrhythmia, cerebrovascular diseases, transient ischemic attack, and arteriosclerosis. In addition, the researchers identified families with full siblings discordant for Tourette syndrome or chronic tic disorder.
Of the more than 14 million individuals in the cohort, 7,804 (76.4% male; median age at first diagnosis, 13.3 years) had a diagnosis of Tourette syndrome or chronic tic disorder in specialist care. Furthermore, the cohort included 5,141 families with full siblings who were discordant for these disorders.
Individuals with Tourette syndrome or chronic tic disorder had a higher risk for any metabolic or cardiovascular disorder, compared with the general population (hazard ratio adjusted by sex and birth year [aHR], 1.99) and sibling controls (aHR, 1.37). Specifically, individuals with Tourette syndrome or chronic tic disorder had higher risks for obesity (aHR, 2.76), T2DM(aHR, 1.67), and circulatory system diseases (aHR, 1.76).
The increased risk of any cardiometabolic disorder was significantly greater for males than it was for females (aHRs, 2.13 vs. 1.79), as was the risk of obesity (aHRs, 3.24 vs. 1.97).
The increased risk for cardiometabolic disorders in this patient population was evident by age 8 years. Exclusion of those patients with comorbid ADHD reduced but did not eliminate the risk (aHR, 1.52). The exclusion of other comorbidities did not significantly affect the results. Among patients with Tourette syndrome or chronic tic disorder, those who had received antipsychotic treatment for more than 1 year were significantly less likely to have metabolic and cardiovascular disorders, compared with patients not taking antipsychotic medication. This association may be related to “greater medical vigilance” and “should not be taken as evidence that antipsychotics are free from cardiometabolic adverse effects,” the authors noted.
The study was supported by a research grant from Tourettes Action. In addition, authors reported support from the Swedish Research Council and a Karolinska Institutet PhD stipend. Two authors disclosed personal fees from publishers, and one author disclosed grants and other funding from Shire.
jremaly@mdedge.com
SOURCE: Brander G et al. JAMA Neurol. 2019 Jan 14. doi: 10.1001/jamaneurol.2018.4279.
The movement disorders are associated with cardiometabolic problems “even after taking into account a number of covariates and shared familial confounders and excluding relevant psychiatric comorbidities,” the researchers wrote. “The results highlight the importance of carefully monitoring cardiometabolic health in patients with Tourette syndrome or chronic tic disorder across the lifespan, particularly in those with comorbid attention-deficit/hyperactivity disorder (ADHD).”
Gustaf Brander, a researcher in the department of clinical neuroscience at Karolinska Institutet in Stockholm, and his colleagues conducted a longitudinal population-based cohort study of individuals living in Sweden between Jan. 1, 1973, and Dec. 31, 2013. The researchers assessed outcomes for patients with previously validated diagnoses of Tourette syndrome or chronic tic disorder in the Swedish National Patient Register. Main outcomes included obesity, dyslipidemia, hypertension, T2DM, and cardiovascular diseases, including ischemic heart diseases, arrhythmia, cerebrovascular diseases, transient ischemic attack, and arteriosclerosis. In addition, the researchers identified families with full siblings discordant for Tourette syndrome or chronic tic disorder.
Of the more than 14 million individuals in the cohort, 7,804 (76.4% male; median age at first diagnosis, 13.3 years) had a diagnosis of Tourette syndrome or chronic tic disorder in specialist care. Furthermore, the cohort included 5,141 families with full siblings who were discordant for these disorders.
Individuals with Tourette syndrome or chronic tic disorder had a higher risk for any metabolic or cardiovascular disorder, compared with the general population (hazard ratio adjusted by sex and birth year [aHR], 1.99) and sibling controls (aHR, 1.37). Specifically, individuals with Tourette syndrome or chronic tic disorder had higher risks for obesity (aHR, 2.76), T2DM(aHR, 1.67), and circulatory system diseases (aHR, 1.76).
The increased risk of any cardiometabolic disorder was significantly greater for males than it was for females (aHRs, 2.13 vs. 1.79), as was the risk of obesity (aHRs, 3.24 vs. 1.97).
The increased risk for cardiometabolic disorders in this patient population was evident by age 8 years. Exclusion of those patients with comorbid ADHD reduced but did not eliminate the risk (aHR, 1.52). The exclusion of other comorbidities did not significantly affect the results. Among patients with Tourette syndrome or chronic tic disorder, those who had received antipsychotic treatment for more than 1 year were significantly less likely to have metabolic and cardiovascular disorders, compared with patients not taking antipsychotic medication. This association may be related to “greater medical vigilance” and “should not be taken as evidence that antipsychotics are free from cardiometabolic adverse effects,” the authors noted.
The study was supported by a research grant from Tourettes Action. In addition, authors reported support from the Swedish Research Council and a Karolinska Institutet PhD stipend. Two authors disclosed personal fees from publishers, and one author disclosed grants and other funding from Shire.
jremaly@mdedge.com
SOURCE: Brander G et al. JAMA Neurol. 2019 Jan 14. doi: 10.1001/jamaneurol.2018.4279.
FROM JAMA NEUROLOGY
Key clinical point: Monitor cardiometabolic health in patients with Tourette syndrome or chronic tic disorder.
Major finding: Patients with Tourette syndrome or chronic tic disorder have a higher risk of metabolic or cardiovascular disorders, compared with the general population (adjusted hazard ratio, 1.99) and sibling controls (adjusted hazard ratio, 1.37).
Study details: A Swedish longitudinal, population-based cohort study of 7,804 individuals with Tourette syndrome or chronic tic disorder.
Disclosures: The study was supported by a research grant from Tourettes Action. Authors reported support from the Swedish Research Council and a Karolinska Institutet PhD stipend. Two authors disclosed personal fees from publishers, and one author disclosed grants and other funding from Shire.
Source: Brander G et al. JAMA Neurol. 2019 Jan 14. doi: 10.1001/jamaneurol.2018.4279.
Robotic sleeve gastrectomy may heighten organ space infection risk
While most outcomes are similar between robotic surgery and laparoscopic surgery for sleeve gastrectomy, the robotic approach carried a greater risk of organ space infection, according to the findings from a large clinical trial of more than 100,000 patients.
The study’s authors analyzed 107,726 sleeve gastrectomy operations in the Metabolic and Bariatric Surgery Association and Quality Improvement Program data registry (MBSAQIP), 7,385 of which were robotic sleeve gastrectomy (RSG). Peter William Lundberg, MD, and his coauthors of St. Luke’s University Health Network, Bethlehem, Pa., evaluated the safety of RSG vs. laparoscopic sleeve gastrectomy (LSG). The study was the first and largest comparing the two approaches to sleeve gastrectomy, the researchers noted.
“According to the MBSAQIP database, the robotic approach demonstrates a significantly higher rate of organ space infection while trending toward a lower rate of bleeding and 30-day reoperation and intervention,” Dr. Lundberg and his coauthors said.
Overall mortality was 0.07% in both groups (P = .49). The overall rates of significant adverse events were similar in both groups – 1.3% for LSG and 1.1% for RSG (P = .14) – as were bleeding rates – 0.5% and 0.4% (P = .003), respectively. The investigators characterized the slightly lower rates for RSG as “insignificant.”
RSG, however, had three times the rate of organ space infection than did the laparoscopic approach, 0.3% vs. 0.1% (P = .79). “Considering the enthusiasm with which robotics has been adopted by some bariatric surgeons, this is a sobering finding,” Dr. Lundberg noted.
The study determined that the use of staple-line reinforcement (SLR) alone significantly reduced the rate of bleeding regardless of approach by 31% on average (P = .0005). “This risk reduction was enhanced when SLR was combined with oversewing of the staple line,” Dr. Lundberg and his colleagues noted – an average reduction of 42% (P = .0009).
RSG took longer on average, 89 minutes vs. 63 minutes (P less than .0001), and the average length of stay was almost identical, 1.7 for RSG vs. 1.6 days for LSG. Reoperation rates within 30 days were also similar: 0.7% for RSG vs. 0.8% for LSG (P = .003).
“As surgeons continue to adopt and develop new technology, ongoing monitoring and reporting of safety and outcomes data are advised to maintain the high standards for outcomes in bariatric surgery,” Dr. Lundberg and his coauthors said.
The study researchers had no financial conflicts.
SOURCE: Lundberg PW et al. Surg Obes Relat Dis. 2018 Oct 25. doi:10.1016/j.soard.2018.10.015.
While most outcomes are similar between robotic surgery and laparoscopic surgery for sleeve gastrectomy, the robotic approach carried a greater risk of organ space infection, according to the findings from a large clinical trial of more than 100,000 patients.
The study’s authors analyzed 107,726 sleeve gastrectomy operations in the Metabolic and Bariatric Surgery Association and Quality Improvement Program data registry (MBSAQIP), 7,385 of which were robotic sleeve gastrectomy (RSG). Peter William Lundberg, MD, and his coauthors of St. Luke’s University Health Network, Bethlehem, Pa., evaluated the safety of RSG vs. laparoscopic sleeve gastrectomy (LSG). The study was the first and largest comparing the two approaches to sleeve gastrectomy, the researchers noted.
“According to the MBSAQIP database, the robotic approach demonstrates a significantly higher rate of organ space infection while trending toward a lower rate of bleeding and 30-day reoperation and intervention,” Dr. Lundberg and his coauthors said.
Overall mortality was 0.07% in both groups (P = .49). The overall rates of significant adverse events were similar in both groups – 1.3% for LSG and 1.1% for RSG (P = .14) – as were bleeding rates – 0.5% and 0.4% (P = .003), respectively. The investigators characterized the slightly lower rates for RSG as “insignificant.”
RSG, however, had three times the rate of organ space infection than did the laparoscopic approach, 0.3% vs. 0.1% (P = .79). “Considering the enthusiasm with which robotics has been adopted by some bariatric surgeons, this is a sobering finding,” Dr. Lundberg noted.
The study determined that the use of staple-line reinforcement (SLR) alone significantly reduced the rate of bleeding regardless of approach by 31% on average (P = .0005). “This risk reduction was enhanced when SLR was combined with oversewing of the staple line,” Dr. Lundberg and his colleagues noted – an average reduction of 42% (P = .0009).
RSG took longer on average, 89 minutes vs. 63 minutes (P less than .0001), and the average length of stay was almost identical, 1.7 for RSG vs. 1.6 days for LSG. Reoperation rates within 30 days were also similar: 0.7% for RSG vs. 0.8% for LSG (P = .003).
“As surgeons continue to adopt and develop new technology, ongoing monitoring and reporting of safety and outcomes data are advised to maintain the high standards for outcomes in bariatric surgery,” Dr. Lundberg and his coauthors said.
The study researchers had no financial conflicts.
SOURCE: Lundberg PW et al. Surg Obes Relat Dis. 2018 Oct 25. doi:10.1016/j.soard.2018.10.015.
While most outcomes are similar between robotic surgery and laparoscopic surgery for sleeve gastrectomy, the robotic approach carried a greater risk of organ space infection, according to the findings from a large clinical trial of more than 100,000 patients.
The study’s authors analyzed 107,726 sleeve gastrectomy operations in the Metabolic and Bariatric Surgery Association and Quality Improvement Program data registry (MBSAQIP), 7,385 of which were robotic sleeve gastrectomy (RSG). Peter William Lundberg, MD, and his coauthors of St. Luke’s University Health Network, Bethlehem, Pa., evaluated the safety of RSG vs. laparoscopic sleeve gastrectomy (LSG). The study was the first and largest comparing the two approaches to sleeve gastrectomy, the researchers noted.
“According to the MBSAQIP database, the robotic approach demonstrates a significantly higher rate of organ space infection while trending toward a lower rate of bleeding and 30-day reoperation and intervention,” Dr. Lundberg and his coauthors said.
Overall mortality was 0.07% in both groups (P = .49). The overall rates of significant adverse events were similar in both groups – 1.3% for LSG and 1.1% for RSG (P = .14) – as were bleeding rates – 0.5% and 0.4% (P = .003), respectively. The investigators characterized the slightly lower rates for RSG as “insignificant.”
RSG, however, had three times the rate of organ space infection than did the laparoscopic approach, 0.3% vs. 0.1% (P = .79). “Considering the enthusiasm with which robotics has been adopted by some bariatric surgeons, this is a sobering finding,” Dr. Lundberg noted.
The study determined that the use of staple-line reinforcement (SLR) alone significantly reduced the rate of bleeding regardless of approach by 31% on average (P = .0005). “This risk reduction was enhanced when SLR was combined with oversewing of the staple line,” Dr. Lundberg and his colleagues noted – an average reduction of 42% (P = .0009).
RSG took longer on average, 89 minutes vs. 63 minutes (P less than .0001), and the average length of stay was almost identical, 1.7 for RSG vs. 1.6 days for LSG. Reoperation rates within 30 days were also similar: 0.7% for RSG vs. 0.8% for LSG (P = .003).
“As surgeons continue to adopt and develop new technology, ongoing monitoring and reporting of safety and outcomes data are advised to maintain the high standards for outcomes in bariatric surgery,” Dr. Lundberg and his coauthors said.
The study researchers had no financial conflicts.
SOURCE: Lundberg PW et al. Surg Obes Relat Dis. 2018 Oct 25. doi:10.1016/j.soard.2018.10.015.
FROM SURGERY FOR OBESITY AND RELATED DISEASES
Key clinical point: Robotic sleeve gastrectomy carries a higher risk of organ space infection than does the laparoscopic approach.
Major finding: Rate of OSI was 0.3% with RSG and 0.1% with laparoscopic surgery.
Study details: An analysis of 107,726 patients who had sleeve gastrectomy in 2016 in the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program registry.
Disclosures: Dr. Lundberg and his coauthors reported having no conflicts.
Source: Lundberg PW et al. Surg Obes Related Dis. 2018 Oct. 25. doi:10.1016/j.soard.2018.10.015.
Glucocorticoid Treatment of Symptomatic Sarcoidosis in 2 Morbidly Obese Patients
Corticosteroid management for patients with sarcoidosis requires the need for close monitoring to detect and manage any complications that may arise during treatment.
Sarcoidosis is a systemic inflammatory condition with pulmonary and extrapulmonary manifestations. The etiology of sarcoidosis remains unknown. Iannuzzi and colleagues hypothesize that an unknown antigen sets off a cycle of chronic granulomatous inflammation in a genetically susceptible host.1
Diagnosis
A diagnosis of sarcoidosis is typically based on a patient having an appropriate clinical presentation and a biopsy, often of lungs or skin, showing noncaseating granulomas.
Symptoms
Of the protean manifestations of sarcoidosis, respiratory symptoms are the most common and typically include subacute or chronic cough and progressive dyspnea on exertion.2 Chest imaging may show only hilar or mediastinal lymphadenopathy, diffuse micronodular lung disease, or signs of chronic inflammation and fibrosis.2 Upper airway involvement and progressive lung disease may lead to increased risk of sleep-disordered breathing, particularly obstructive sleep apnea (OSA).3
Sarcoidosis also can develop in the skin, neurologic system, heart, and other systems. It typically presents as areas of patchy, infiltrative inflammation. In the heart, this can lead to heart failure, often with reduced ejection fraction (EF) and ventricular arrhythmias.1 Pulmonary hypertension (PH) may result from multiple possible mechanisms, including left-heart disease, parenchymal lung disease, sleep-disordered breathing, and possibly direct inflammation and compression of the pulmonary vasculature.2-4
Sarcoidosis in Obese Patients
Emerging evidence shows that sarcoidosis occurs at higher rates in obese patients, suggesting that obesity may be a risk factor for the disease.5-7 Rates of morbid obesity are increasing in the US. From 2000 to 2010, the prevalence of morbid obesity, defined as body mass index (BMI) > 40, increased by 70%, with even larger relative increases in the number of patients with BMI > 50.8 Among veterans who receive health care at the US Department of Veterans Affairs (VA) medical centers, 28% are obese.9 As a result, VA physicians will encounter more patients with morbid obesity and another significant comorbid condition.
Managing symptomatic sarcoidosis in patients with morbid obesity poses a dilemma. Typical treatment for symptomatic pulmonary sarcoidosis is prednisone 20 mg to 40 mg daily.10,11 Higher doses are suggested for involvement of other organs, such as the heart.2,12 Associated weight gain from corticosteroid treatment with possible sleep-disordered breathing increases an already high risk of metabolic complications in morbidly obese patients.13 No clear consensus exists on how corticosteroid doses should be adjusted. We present 2 cases that highlight the complexity of corticosteroid management in the obese sarcoidosis patient.
Case 1: Pulmonary Sarcoidosis
A 43-year-old morbidly obese man presented to his primary care provider with subacute onset of dyspnea. He had a history of OSA that was diagnosed empirically at another institution without polysomnogram and treated with autotitrating continuous positive airway pressure (CPAP).
The patient was admitted for expedited evaluation. His BMI was 63.2 with declining exercise tolerance and hypoxemia on ambulation. His oxyhemoglobin saturation rate was 85% after walking a short distance. Ongoing CPAP therapy for sleep-disordered breathing made laboratory evaluation for obesity hypoventilation syndrome (OHS) challenging. The patient’s serum bicarbonate test result was normal. Serum markers as well as induced sputum stains and cultures were negative for evidence of mycobacterial or fungal infections. A chest radiograph showed bilateral hilar adenopathy and miliary nodularity. Pulmonary function testing revealed severe obstruction and restriction as well as a moderate diffusion impairment. Bronchoscopy with biopsy revealed noncaseating granulomas consistent with sarcoidosis. An electrocardiogram (ECG) was normal. Transthoracic echocardiogram showed evidence of diastolic dysfunction and a mildly dilated right ventricle with normal function, suggestive of possible PH. We were unable to assess his pulmonary artery pressure.
Upon release, the patient began a course of 50 mg (0.24 mg/kg actual body weight) oral prednisone daily and home oxygen.
Six weeks after initiation of steroids, the patient reported that his dyspnea had improved. However, after 6 months of steroid treatment, his weight increased from 462 pounds to 503 pounds. He was evaluated for possible neurosarcoidosis with hypothalamic or pituitary involvement as a possible cause for the weight gain. Brain magnetic resonance imaging and hormonal testing were normal. We considered starting him on a steroid-sparing agent. However, after early efficacy, prednisone was gradually tapered and, after 1 year of treatment, discontinued. At that time, symptoms had substantially improved: His pulmonary function tests had normalized, and he was weaned off oxygen; repeat chest imaging showed only residual enlargement of the hilar lymph nodes. After cessation of steroids, the patient was able to lose 20 pounds.
Case 2: Cardiac Sarcoidosis
A 57-year-old morbidly obese man presented to the emergency department with subacute increasing dyspnea on exertion. He had a known history of sarcoidosis diagnosed by skin biopsy 28 years earlier but had been without treatment for decades. His history also included prediabetes, heart failure with preserved ejection fraction (HFpEF), OSA with an apnea hypopnea index (AHI) of 114.7 per hour, PH diagnosed by prior echocardiogram, and paroxysmal atrial fibrillation (AF). He required 2 L/m home oxygen and bilevel positive airway pressure (PAP) of 22/17 cm H2O while sleeping.
On physical examination, the patient’s BMI was 54.6. He was tachycardic and hypoxemic on his usual oxygen flow rate. His serum bicarbonate, arterial blood pH, and PaCO2 blood levels were normal. We heard bibasilar crackles over the lungs. Chest radiograph revealed an enlarged cardiac silhouette and bilateral infiltrates concerning for cardiogenic pulmonary edema. An echocardiogram showed a restrictive filling pattern with preserved EF and moderate dilation and dysfunction of the right ventricle, consistent with PH. A positron emission tomography (PET)/computed tomography scan, the preferred study for cardiac sarcoidosis, suggested active infiltrative septal cardiac disease and active hilar and mediastinal adenopathy. This was concerning for both cardiac and pulmonary sarcoidosis. Ongoing treatment of sleep-disordered breathing made laboratory assessment for OHS challenging. Given his intact EF, the absence of ventricular arrhythmias, and improvement with diuretics and bilevel PAP, specific treatment of sarcoidosis was not initiated. He was discharged home with a plan to re-evaluate sarcoidosis symptoms and initiate treatment as an outpatient.
The patient was readmitted 2 weeks later with worsened dyspnea, hypoxemia, and volume overload. A right heart catheterization confirmed PH with a mean pulmonary artery pressure of 44 mm Hg (68/32 mm Hg) and pulmonary vascular resistance of 4.6 Wood units. We also found evidence of left-heart dysfunction with a pulmonary capillary wedge pressure of 16 mm Hg.
Given his recurrent symptoms, evidence of active myocardial inflammation on recent PET, and prior biopsy-proven sarcoidosis, we made the decision to pursue treatment for symptomatic sarcoidosis. He began a course of 40 mg (0.20 mg/kg actual body weight) oral prednisone daily. He now required 6 L/m supplemental oxygen. After IV diuretic therapy during his hospitalization, the patient was discharged on his preadmission oral diuretic dose. Pulmonary vasodilator therapy was not initiated for PH as left heart disease and sleep-disordered breathing needed to be managed first.
One month after steroid initiation, the patient reported that the dyspnea and hypoxemia had markedly improved. His oxygen flow rate was reduced to 2 L/m. He remained normotensive and had no further difficulties with fluid retention or volume overload on a stable dose of oral diuretics. He had elevated blood glucose with a glycated hemoglobin (HbA1c) of 6.4%. He began treatment with glipizide 5 mg daily.
After 3 months, he returned to the emergency department with hyperosmolar nonketotic hyperglycemia due to steroid-induced diabetes mellitus (DM). His HbA1c was now 17.1%. The patient was started on a home insulin regimen, and his blood sugar values subsequently improved. He remained symptomatically better and lost 40 pounds with a guided weight management program and a stable diuretic regimen. He underwent arrhythmia evaluation with a Holter monitor that showed AF without ventricular arrhythmias.
Unfortunately, he did not return for cardiac or pulmonary reevaluation, and was lost to follow-up. Nine months after initiation of treatment, the patient died after an out-of-hospital cardiac arrest.
Discussion
These 2 cases highlight therapeutic challenges that may arise in the management of sarcoidosis with symptomatic vital organ involvement and coexistent extreme obesity. Both patients showed symptom improvement with moderate doses of prednisone (40 mg to 50 mg daily), but serious treatment-related complications developed: further weight gain in the first patient, and severe DM in the second. Although DM may have been a direct treatment complication in our second patient, his HFpEF and PH were high-risk comorbidities; he did not present with acute symptomatic worsening after treatment initiation. His symptoms were never reassessed when he was lost to follow-up.
Sarcoidosis/Obesity Relationship
Recent evidence suggests that patients with obesity are at increased risk of developing sarcoidosis.5-7 Although the mechanism of association is unclear, several possibilities have been proposed.
Neurosarcoidosis. One known but rare cause of obesity is neurosarcoidosis of the hypothalamus or pituitary.14 This was investigated in one of our patients.
Proinflammatory responses. Another possible mechanism for the association of sarcoidosis and obesity is the proinflammatory properties of increased fat and adipose tissue.15 Obesity has been linked to an aberrant expansion of inflammatory cells and mediators, including macrophages, proinflammatory cytokines, T cells, and B cells.15 Leptin, produced primarily by adipocytes, also is higher in obese patients and has been found to be proinflammatory.16 These seem to underlie the link between obesity and other inflammatory diseases, including type 2 DM, gout, and atherosclerosis.15
Behavioral link. There also is a possible behavioral link between sarcoidosis and obesity: A patient might develop symptomatic sarcoidosis and later become less active due to dyspnea, which could predispose to weight gain.5
Management of Comorbid Sarcoidosis and Obesity
Regardless of the exact mechanism of this association, management of the co-occurrence of sarcoidosis and obesity poses a clinical problem, especially in cases of extreme obesity. Corticosteroids are generally considered the treatment of choice for symptomatic sarcoidosis. The initial treatment of symptomatic pulmonary sarcoidosis is 20 mg to 40 mg prednisone daily.10,11 Higher daily doses such as 60 mg to 80 mg or 0.5 mg/kg are typically used to treat cardiac sarcoidosis, although no clear consensus exists on the appropriate dose.12,17 One recent study showed no difference in cardiac outcomes in patients treated with high- and low-dose prednisone.18
For patients who are obese and require steroids to treat a medical condition, there is conflicting evidence on whether steroid doses should be increased in proportion to total body weight. Milsap and colleagues found clearance of prednisolone correlated strongly with degree of obesity, suggesting steroid dose should be increased in accordance with actual weight.19 In contrast, Dunn and colleagues found decreased clearance of methylprednisolone in obese patients, suggesting that ideal body weight dosing is appropriate.20
Identifying the appropriate steroid dose is important because corticosteroids place obese patients at higher risk of developing complications. Treatment-related comorbidities include DM, hypertension, fluid retention, osteoporosis, and infection. Further weight gain due to steroid use is a risk for progressive OSA and, even though not generally associated with sarcoidosis alone, OHS. For patients with sarcoidosis, these complications (DM, fluid retention, hypertension, sleep-disordered breathing) may increase the risk of cardiovascular disease and PH.21-23 Cardiomyopathy, especially with reduced EF and increased PH, can be associated with a poor prognosis in sarcoidosis.4,24-26 PH also can be challenging to treat patients with sarcoidosis because the response of PH to steroids is unclear.27 Small trials have shown the benefit of pulmonary vasodilators on hemodynamics, but these have generally been used in patients with stable sarcoidosis who do not have left-heart disease.28-30
Our Prescription Model
We empirically prescribed moderate total doses of prednisone—although low on a mg/kg basis—to balance efficacy and the risk of adverse effects in these 2 morbidly obese patients. We also managed treatment-related complications with guided weight-management programs, CPAP, or noninvasive ventilation for sleep-disordered breathing, and DM treatment.
Our cases demonstrate the need for close monitoring of weight, blood pressure, and blood glucose to detect and treat any complications that may arise during corticosteroid treatment. Aggressive treatment of hyperglycemia with insulin or oral alternatives associated with weight loss such as metformin, sulfonylureas, dipeptidyl peptidase 4 inhibitors, or glucagon-like peptide 1 receptor agonists, may help prevent further DM complications. Sleep-disordered breathing should be assessed and treated. Bariatric surgery may be an option to treat obesity and minimize resultant complications. In our patients, and likely many others, the degree of respiratory and cardiac disease coupled with poor wound healing due to chronic prednisone, may increase the procedural risks.
Conclusion
Our experiences with these patients illustrate that symptomatic and objective improvement in sarcoidosis may be achieved in morbidly obese patients with doses of prednisone that are generally considered moderate, though quite low on a mg/kg basis.
We believe ours is the first report to describe the use of corticosteroids for the treatment of sarcoidosis in patients with morbid obesity. That 2 patients were treated at a single VA medical center within 1-year likely reflects the rising incidence of morbid obesity in the US veteran population and suggests that other federal practitioners might encounter similar patients.
Further study may show that, as an alternative to initial moderate-dose prednisone, patients with symptomatic sarcoidosis and extreme obesity might be started on antimetabolite or antitumor necrosis factor medication or on low-dose prednisone and a second steroid-sparing agent.
1. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007;357(21):2153-2165.
2. Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet PY, Muller-Quernheim J. Sarcoidosis. Lancet. 2014;383 (9923):1155-1167.
3. Lal C, Medarov BI, Judson MA. Interrelationship between sleep-disordered breathing and sarcoidosis. Chest. 2015;148(4):1105-1114.
4. Dobarro D, Schreiber BE, Handler C, Beynon H, Denton CP, Coghlan JG. Clinical characteristics, haemodynamics and treatment of pulmonary hypertension in sarcoidosis in a single centre, and meta-analysis of the published data. Am J Cardiol. 2013;111(2):278-285.
5. Cozier YC, Coogan PF, Govender P, Berman JS, Palmer JR, Rosenberg L. Obesity and weight gain in relation to incidence of sarcoidosis in US black women: data from the Black Women’s Health Study. Chest. 2015;147(4):1086-1093.
6. Harpsoe MC, Basit S, Andersson M, et al. Body mass index and risk of autoimmune diseases: a study within the Danish National Birth Cohort. Int J Epidemiol. 2014;43(3):843-855.
7. Ungprasert P, Crowson CS, Matteson EL. Smoking, obesity and risk of sarcoidosis: a population-based nested case-control study. Respir Med. 2016;120:87-90.
8. Sturm R, Hattori A. Morbid obesity rates continue to rise rapidly in the United States. Int J Obes (Lond). 2013;37(6):889-891.
9. Nelson KM. The burden of obesity among a national probability sample of veterans. J Gen Intern Med. 2006; 21(9):915-919.
10. Moller DR, Chen ES. Systemic sarcoidosis. In: Grippi MA, Elias JA, Fishman et al, eds. Fishman’s Pulmonary Diseases and Disorders. 5th ed. New York, NY: McGraw-Hill; 2015: 823-841
11. Judson MA, Morgenthau AS, Baughman RP. Sarcoidosis. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel’s Textbook of Respiratory Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:1188-1206.
12. Patel D, Hamzeh NY. Immunosuppressive management of cardiac sarcoidosis. In: Freeman AM, Weinberger HD, eds. Cardiac Sarcoidosis. New York, NY: Springer; 2015:103-112.
13. Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract. 2010;89(3):309-319.
14. Anthony J, Esper GJ, Ioachimescu A. Hypothalamic-pituitary sarcoidosis with vision loss and hypopituitarism: case series and literature review. Pituitary. 2016;19(1):19-29.
15. Kanneganti TD, Dixit VD. Immunological complications of obesity. Nat Immunol. 2012;13(8):707-712.
16. Matarese G, Leiter EH, La Cava A. Leptin in autoimmunity: many questions, some answers. Tissue Antigens. 2007;70(2):87-95.
17. Doughan AR, Williams BR. Cardiac sarcoidosis. Heart. 2006;92(2):282-288.
18. Yazaki Y, Isobe M, Hiroe M, et al. Prognostic determinants of long-term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am J Cardiol. 2001;88(9):1006-1010.
19. Milsap RL, Plaisance KI, Jusko WJ. Prednisolone disposition in obese men. Clin Pharmacol Ther. 1984;36(6):824-831.
20. Dunn TE, Ludwig EA, Slaughter RL, Camara DS, Jusko WJ. Pharmacokinetics and pharmacodynamics of methylprednisolone in obesity. Clin Pharmacol Ther. 1991;49(5):536-549.
21. Eastwood PR, Malhotra A, Palmer LJ, et al. Obstructive sleep apnoea: from pathogenesis to treatment: current controversies and future directions. Respirology. 2010;15(4):587-595.
22. Wong HS, Williams AJ, Mok Y. The relationship between pulmonary hypertension and obstructive sleep apnea. Curr Opin Pulm Med. 2017;23(6):517-521.
23. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82-93.
24. Handa T, Nagai S, Miki S, et al. Incidence of pulmonary hypertension and its clinical relevance in patients with sarcoidosis. Chest. 2006;129(5):1246-1252.
25. Baughman RP, Engel PJ, Taylor L, Lower EE. Survival in sarcoidosis-associated pulmonary hypertension: the importance of hemodynamic evaluation. Chest. 2010;138(5):1078-1085.
26. Birnie DH, Kandolin R, Nery PB, Kupari M. Cardiac manifestations of sarcoidosis: diagnosis and management. Eur Heart J. 2017;38(35):2663-2670.
27. Nunes H, Humbert M, Capron F, et al. Pulmonary hypertension associated with sarcoidosis: mechanisms, haemodynamics and prognosis. Thorax. 2006;61(1):68-74.
28. Judson MA, Highland KB, Kwon S, et al. Ambrisentan for sarcoidosis associated pulmonary hypertension. Sarcoidosis Vasc Diffuse Lung Dis. 2011;28(2):139-145.
29. Baughman RP, Culver DA, Cordova FC, et al. Bosentan for sarcoidosis-associated pulmonary hypertension: a double-blind placebo controlled randomized trial. Chest. 2014;145(4):810-817.
30. Baughman RP, Judson MA, Lower EE, et al. Inhaled iloprost for sarcoidosis associated pulmonary hypertension. Sarcoidosis Vasc Diffuse Lung Dis. 2009;26(2):110-120.
Corticosteroid management for patients with sarcoidosis requires the need for close monitoring to detect and manage any complications that may arise during treatment.
Corticosteroid management for patients with sarcoidosis requires the need for close monitoring to detect and manage any complications that may arise during treatment.
Sarcoidosis is a systemic inflammatory condition with pulmonary and extrapulmonary manifestations. The etiology of sarcoidosis remains unknown. Iannuzzi and colleagues hypothesize that an unknown antigen sets off a cycle of chronic granulomatous inflammation in a genetically susceptible host.1
Diagnosis
A diagnosis of sarcoidosis is typically based on a patient having an appropriate clinical presentation and a biopsy, often of lungs or skin, showing noncaseating granulomas.
Symptoms
Of the protean manifestations of sarcoidosis, respiratory symptoms are the most common and typically include subacute or chronic cough and progressive dyspnea on exertion.2 Chest imaging may show only hilar or mediastinal lymphadenopathy, diffuse micronodular lung disease, or signs of chronic inflammation and fibrosis.2 Upper airway involvement and progressive lung disease may lead to increased risk of sleep-disordered breathing, particularly obstructive sleep apnea (OSA).3
Sarcoidosis also can develop in the skin, neurologic system, heart, and other systems. It typically presents as areas of patchy, infiltrative inflammation. In the heart, this can lead to heart failure, often with reduced ejection fraction (EF) and ventricular arrhythmias.1 Pulmonary hypertension (PH) may result from multiple possible mechanisms, including left-heart disease, parenchymal lung disease, sleep-disordered breathing, and possibly direct inflammation and compression of the pulmonary vasculature.2-4
Sarcoidosis in Obese Patients
Emerging evidence shows that sarcoidosis occurs at higher rates in obese patients, suggesting that obesity may be a risk factor for the disease.5-7 Rates of morbid obesity are increasing in the US. From 2000 to 2010, the prevalence of morbid obesity, defined as body mass index (BMI) > 40, increased by 70%, with even larger relative increases in the number of patients with BMI > 50.8 Among veterans who receive health care at the US Department of Veterans Affairs (VA) medical centers, 28% are obese.9 As a result, VA physicians will encounter more patients with morbid obesity and another significant comorbid condition.
Managing symptomatic sarcoidosis in patients with morbid obesity poses a dilemma. Typical treatment for symptomatic pulmonary sarcoidosis is prednisone 20 mg to 40 mg daily.10,11 Higher doses are suggested for involvement of other organs, such as the heart.2,12 Associated weight gain from corticosteroid treatment with possible sleep-disordered breathing increases an already high risk of metabolic complications in morbidly obese patients.13 No clear consensus exists on how corticosteroid doses should be adjusted. We present 2 cases that highlight the complexity of corticosteroid management in the obese sarcoidosis patient.
Case 1: Pulmonary Sarcoidosis
A 43-year-old morbidly obese man presented to his primary care provider with subacute onset of dyspnea. He had a history of OSA that was diagnosed empirically at another institution without polysomnogram and treated with autotitrating continuous positive airway pressure (CPAP).
The patient was admitted for expedited evaluation. His BMI was 63.2 with declining exercise tolerance and hypoxemia on ambulation. His oxyhemoglobin saturation rate was 85% after walking a short distance. Ongoing CPAP therapy for sleep-disordered breathing made laboratory evaluation for obesity hypoventilation syndrome (OHS) challenging. The patient’s serum bicarbonate test result was normal. Serum markers as well as induced sputum stains and cultures were negative for evidence of mycobacterial or fungal infections. A chest radiograph showed bilateral hilar adenopathy and miliary nodularity. Pulmonary function testing revealed severe obstruction and restriction as well as a moderate diffusion impairment. Bronchoscopy with biopsy revealed noncaseating granulomas consistent with sarcoidosis. An electrocardiogram (ECG) was normal. Transthoracic echocardiogram showed evidence of diastolic dysfunction and a mildly dilated right ventricle with normal function, suggestive of possible PH. We were unable to assess his pulmonary artery pressure.
Upon release, the patient began a course of 50 mg (0.24 mg/kg actual body weight) oral prednisone daily and home oxygen.
Six weeks after initiation of steroids, the patient reported that his dyspnea had improved. However, after 6 months of steroid treatment, his weight increased from 462 pounds to 503 pounds. He was evaluated for possible neurosarcoidosis with hypothalamic or pituitary involvement as a possible cause for the weight gain. Brain magnetic resonance imaging and hormonal testing were normal. We considered starting him on a steroid-sparing agent. However, after early efficacy, prednisone was gradually tapered and, after 1 year of treatment, discontinued. At that time, symptoms had substantially improved: His pulmonary function tests had normalized, and he was weaned off oxygen; repeat chest imaging showed only residual enlargement of the hilar lymph nodes. After cessation of steroids, the patient was able to lose 20 pounds.
Case 2: Cardiac Sarcoidosis
A 57-year-old morbidly obese man presented to the emergency department with subacute increasing dyspnea on exertion. He had a known history of sarcoidosis diagnosed by skin biopsy 28 years earlier but had been without treatment for decades. His history also included prediabetes, heart failure with preserved ejection fraction (HFpEF), OSA with an apnea hypopnea index (AHI) of 114.7 per hour, PH diagnosed by prior echocardiogram, and paroxysmal atrial fibrillation (AF). He required 2 L/m home oxygen and bilevel positive airway pressure (PAP) of 22/17 cm H2O while sleeping.
On physical examination, the patient’s BMI was 54.6. He was tachycardic and hypoxemic on his usual oxygen flow rate. His serum bicarbonate, arterial blood pH, and PaCO2 blood levels were normal. We heard bibasilar crackles over the lungs. Chest radiograph revealed an enlarged cardiac silhouette and bilateral infiltrates concerning for cardiogenic pulmonary edema. An echocardiogram showed a restrictive filling pattern with preserved EF and moderate dilation and dysfunction of the right ventricle, consistent with PH. A positron emission tomography (PET)/computed tomography scan, the preferred study for cardiac sarcoidosis, suggested active infiltrative septal cardiac disease and active hilar and mediastinal adenopathy. This was concerning for both cardiac and pulmonary sarcoidosis. Ongoing treatment of sleep-disordered breathing made laboratory assessment for OHS challenging. Given his intact EF, the absence of ventricular arrhythmias, and improvement with diuretics and bilevel PAP, specific treatment of sarcoidosis was not initiated. He was discharged home with a plan to re-evaluate sarcoidosis symptoms and initiate treatment as an outpatient.
The patient was readmitted 2 weeks later with worsened dyspnea, hypoxemia, and volume overload. A right heart catheterization confirmed PH with a mean pulmonary artery pressure of 44 mm Hg (68/32 mm Hg) and pulmonary vascular resistance of 4.6 Wood units. We also found evidence of left-heart dysfunction with a pulmonary capillary wedge pressure of 16 mm Hg.
Given his recurrent symptoms, evidence of active myocardial inflammation on recent PET, and prior biopsy-proven sarcoidosis, we made the decision to pursue treatment for symptomatic sarcoidosis. He began a course of 40 mg (0.20 mg/kg actual body weight) oral prednisone daily. He now required 6 L/m supplemental oxygen. After IV diuretic therapy during his hospitalization, the patient was discharged on his preadmission oral diuretic dose. Pulmonary vasodilator therapy was not initiated for PH as left heart disease and sleep-disordered breathing needed to be managed first.
One month after steroid initiation, the patient reported that the dyspnea and hypoxemia had markedly improved. His oxygen flow rate was reduced to 2 L/m. He remained normotensive and had no further difficulties with fluid retention or volume overload on a stable dose of oral diuretics. He had elevated blood glucose with a glycated hemoglobin (HbA1c) of 6.4%. He began treatment with glipizide 5 mg daily.
After 3 months, he returned to the emergency department with hyperosmolar nonketotic hyperglycemia due to steroid-induced diabetes mellitus (DM). His HbA1c was now 17.1%. The patient was started on a home insulin regimen, and his blood sugar values subsequently improved. He remained symptomatically better and lost 40 pounds with a guided weight management program and a stable diuretic regimen. He underwent arrhythmia evaluation with a Holter monitor that showed AF without ventricular arrhythmias.
Unfortunately, he did not return for cardiac or pulmonary reevaluation, and was lost to follow-up. Nine months after initiation of treatment, the patient died after an out-of-hospital cardiac arrest.
Discussion
These 2 cases highlight therapeutic challenges that may arise in the management of sarcoidosis with symptomatic vital organ involvement and coexistent extreme obesity. Both patients showed symptom improvement with moderate doses of prednisone (40 mg to 50 mg daily), but serious treatment-related complications developed: further weight gain in the first patient, and severe DM in the second. Although DM may have been a direct treatment complication in our second patient, his HFpEF and PH were high-risk comorbidities; he did not present with acute symptomatic worsening after treatment initiation. His symptoms were never reassessed when he was lost to follow-up.
Sarcoidosis/Obesity Relationship
Recent evidence suggests that patients with obesity are at increased risk of developing sarcoidosis.5-7 Although the mechanism of association is unclear, several possibilities have been proposed.
Neurosarcoidosis. One known but rare cause of obesity is neurosarcoidosis of the hypothalamus or pituitary.14 This was investigated in one of our patients.
Proinflammatory responses. Another possible mechanism for the association of sarcoidosis and obesity is the proinflammatory properties of increased fat and adipose tissue.15 Obesity has been linked to an aberrant expansion of inflammatory cells and mediators, including macrophages, proinflammatory cytokines, T cells, and B cells.15 Leptin, produced primarily by adipocytes, also is higher in obese patients and has been found to be proinflammatory.16 These seem to underlie the link between obesity and other inflammatory diseases, including type 2 DM, gout, and atherosclerosis.15
Behavioral link. There also is a possible behavioral link between sarcoidosis and obesity: A patient might develop symptomatic sarcoidosis and later become less active due to dyspnea, which could predispose to weight gain.5
Management of Comorbid Sarcoidosis and Obesity
Regardless of the exact mechanism of this association, management of the co-occurrence of sarcoidosis and obesity poses a clinical problem, especially in cases of extreme obesity. Corticosteroids are generally considered the treatment of choice for symptomatic sarcoidosis. The initial treatment of symptomatic pulmonary sarcoidosis is 20 mg to 40 mg prednisone daily.10,11 Higher daily doses such as 60 mg to 80 mg or 0.5 mg/kg are typically used to treat cardiac sarcoidosis, although no clear consensus exists on the appropriate dose.12,17 One recent study showed no difference in cardiac outcomes in patients treated with high- and low-dose prednisone.18
For patients who are obese and require steroids to treat a medical condition, there is conflicting evidence on whether steroid doses should be increased in proportion to total body weight. Milsap and colleagues found clearance of prednisolone correlated strongly with degree of obesity, suggesting steroid dose should be increased in accordance with actual weight.19 In contrast, Dunn and colleagues found decreased clearance of methylprednisolone in obese patients, suggesting that ideal body weight dosing is appropriate.20
Identifying the appropriate steroid dose is important because corticosteroids place obese patients at higher risk of developing complications. Treatment-related comorbidities include DM, hypertension, fluid retention, osteoporosis, and infection. Further weight gain due to steroid use is a risk for progressive OSA and, even though not generally associated with sarcoidosis alone, OHS. For patients with sarcoidosis, these complications (DM, fluid retention, hypertension, sleep-disordered breathing) may increase the risk of cardiovascular disease and PH.21-23 Cardiomyopathy, especially with reduced EF and increased PH, can be associated with a poor prognosis in sarcoidosis.4,24-26 PH also can be challenging to treat patients with sarcoidosis because the response of PH to steroids is unclear.27 Small trials have shown the benefit of pulmonary vasodilators on hemodynamics, but these have generally been used in patients with stable sarcoidosis who do not have left-heart disease.28-30
Our Prescription Model
We empirically prescribed moderate total doses of prednisone—although low on a mg/kg basis—to balance efficacy and the risk of adverse effects in these 2 morbidly obese patients. We also managed treatment-related complications with guided weight-management programs, CPAP, or noninvasive ventilation for sleep-disordered breathing, and DM treatment.
Our cases demonstrate the need for close monitoring of weight, blood pressure, and blood glucose to detect and treat any complications that may arise during corticosteroid treatment. Aggressive treatment of hyperglycemia with insulin or oral alternatives associated with weight loss such as metformin, sulfonylureas, dipeptidyl peptidase 4 inhibitors, or glucagon-like peptide 1 receptor agonists, may help prevent further DM complications. Sleep-disordered breathing should be assessed and treated. Bariatric surgery may be an option to treat obesity and minimize resultant complications. In our patients, and likely many others, the degree of respiratory and cardiac disease coupled with poor wound healing due to chronic prednisone, may increase the procedural risks.
Conclusion
Our experiences with these patients illustrate that symptomatic and objective improvement in sarcoidosis may be achieved in morbidly obese patients with doses of prednisone that are generally considered moderate, though quite low on a mg/kg basis.
We believe ours is the first report to describe the use of corticosteroids for the treatment of sarcoidosis in patients with morbid obesity. That 2 patients were treated at a single VA medical center within 1-year likely reflects the rising incidence of morbid obesity in the US veteran population and suggests that other federal practitioners might encounter similar patients.
Further study may show that, as an alternative to initial moderate-dose prednisone, patients with symptomatic sarcoidosis and extreme obesity might be started on antimetabolite or antitumor necrosis factor medication or on low-dose prednisone and a second steroid-sparing agent.
Sarcoidosis is a systemic inflammatory condition with pulmonary and extrapulmonary manifestations. The etiology of sarcoidosis remains unknown. Iannuzzi and colleagues hypothesize that an unknown antigen sets off a cycle of chronic granulomatous inflammation in a genetically susceptible host.1
Diagnosis
A diagnosis of sarcoidosis is typically based on a patient having an appropriate clinical presentation and a biopsy, often of lungs or skin, showing noncaseating granulomas.
Symptoms
Of the protean manifestations of sarcoidosis, respiratory symptoms are the most common and typically include subacute or chronic cough and progressive dyspnea on exertion.2 Chest imaging may show only hilar or mediastinal lymphadenopathy, diffuse micronodular lung disease, or signs of chronic inflammation and fibrosis.2 Upper airway involvement and progressive lung disease may lead to increased risk of sleep-disordered breathing, particularly obstructive sleep apnea (OSA).3
Sarcoidosis also can develop in the skin, neurologic system, heart, and other systems. It typically presents as areas of patchy, infiltrative inflammation. In the heart, this can lead to heart failure, often with reduced ejection fraction (EF) and ventricular arrhythmias.1 Pulmonary hypertension (PH) may result from multiple possible mechanisms, including left-heart disease, parenchymal lung disease, sleep-disordered breathing, and possibly direct inflammation and compression of the pulmonary vasculature.2-4
Sarcoidosis in Obese Patients
Emerging evidence shows that sarcoidosis occurs at higher rates in obese patients, suggesting that obesity may be a risk factor for the disease.5-7 Rates of morbid obesity are increasing in the US. From 2000 to 2010, the prevalence of morbid obesity, defined as body mass index (BMI) > 40, increased by 70%, with even larger relative increases in the number of patients with BMI > 50.8 Among veterans who receive health care at the US Department of Veterans Affairs (VA) medical centers, 28% are obese.9 As a result, VA physicians will encounter more patients with morbid obesity and another significant comorbid condition.
Managing symptomatic sarcoidosis in patients with morbid obesity poses a dilemma. Typical treatment for symptomatic pulmonary sarcoidosis is prednisone 20 mg to 40 mg daily.10,11 Higher doses are suggested for involvement of other organs, such as the heart.2,12 Associated weight gain from corticosteroid treatment with possible sleep-disordered breathing increases an already high risk of metabolic complications in morbidly obese patients.13 No clear consensus exists on how corticosteroid doses should be adjusted. We present 2 cases that highlight the complexity of corticosteroid management in the obese sarcoidosis patient.
Case 1: Pulmonary Sarcoidosis
A 43-year-old morbidly obese man presented to his primary care provider with subacute onset of dyspnea. He had a history of OSA that was diagnosed empirically at another institution without polysomnogram and treated with autotitrating continuous positive airway pressure (CPAP).
The patient was admitted for expedited evaluation. His BMI was 63.2 with declining exercise tolerance and hypoxemia on ambulation. His oxyhemoglobin saturation rate was 85% after walking a short distance. Ongoing CPAP therapy for sleep-disordered breathing made laboratory evaluation for obesity hypoventilation syndrome (OHS) challenging. The patient’s serum bicarbonate test result was normal. Serum markers as well as induced sputum stains and cultures were negative for evidence of mycobacterial or fungal infections. A chest radiograph showed bilateral hilar adenopathy and miliary nodularity. Pulmonary function testing revealed severe obstruction and restriction as well as a moderate diffusion impairment. Bronchoscopy with biopsy revealed noncaseating granulomas consistent with sarcoidosis. An electrocardiogram (ECG) was normal. Transthoracic echocardiogram showed evidence of diastolic dysfunction and a mildly dilated right ventricle with normal function, suggestive of possible PH. We were unable to assess his pulmonary artery pressure.
Upon release, the patient began a course of 50 mg (0.24 mg/kg actual body weight) oral prednisone daily and home oxygen.
Six weeks after initiation of steroids, the patient reported that his dyspnea had improved. However, after 6 months of steroid treatment, his weight increased from 462 pounds to 503 pounds. He was evaluated for possible neurosarcoidosis with hypothalamic or pituitary involvement as a possible cause for the weight gain. Brain magnetic resonance imaging and hormonal testing were normal. We considered starting him on a steroid-sparing agent. However, after early efficacy, prednisone was gradually tapered and, after 1 year of treatment, discontinued. At that time, symptoms had substantially improved: His pulmonary function tests had normalized, and he was weaned off oxygen; repeat chest imaging showed only residual enlargement of the hilar lymph nodes. After cessation of steroids, the patient was able to lose 20 pounds.
Case 2: Cardiac Sarcoidosis
A 57-year-old morbidly obese man presented to the emergency department with subacute increasing dyspnea on exertion. He had a known history of sarcoidosis diagnosed by skin biopsy 28 years earlier but had been without treatment for decades. His history also included prediabetes, heart failure with preserved ejection fraction (HFpEF), OSA with an apnea hypopnea index (AHI) of 114.7 per hour, PH diagnosed by prior echocardiogram, and paroxysmal atrial fibrillation (AF). He required 2 L/m home oxygen and bilevel positive airway pressure (PAP) of 22/17 cm H2O while sleeping.
On physical examination, the patient’s BMI was 54.6. He was tachycardic and hypoxemic on his usual oxygen flow rate. His serum bicarbonate, arterial blood pH, and PaCO2 blood levels were normal. We heard bibasilar crackles over the lungs. Chest radiograph revealed an enlarged cardiac silhouette and bilateral infiltrates concerning for cardiogenic pulmonary edema. An echocardiogram showed a restrictive filling pattern with preserved EF and moderate dilation and dysfunction of the right ventricle, consistent with PH. A positron emission tomography (PET)/computed tomography scan, the preferred study for cardiac sarcoidosis, suggested active infiltrative septal cardiac disease and active hilar and mediastinal adenopathy. This was concerning for both cardiac and pulmonary sarcoidosis. Ongoing treatment of sleep-disordered breathing made laboratory assessment for OHS challenging. Given his intact EF, the absence of ventricular arrhythmias, and improvement with diuretics and bilevel PAP, specific treatment of sarcoidosis was not initiated. He was discharged home with a plan to re-evaluate sarcoidosis symptoms and initiate treatment as an outpatient.
The patient was readmitted 2 weeks later with worsened dyspnea, hypoxemia, and volume overload. A right heart catheterization confirmed PH with a mean pulmonary artery pressure of 44 mm Hg (68/32 mm Hg) and pulmonary vascular resistance of 4.6 Wood units. We also found evidence of left-heart dysfunction with a pulmonary capillary wedge pressure of 16 mm Hg.
Given his recurrent symptoms, evidence of active myocardial inflammation on recent PET, and prior biopsy-proven sarcoidosis, we made the decision to pursue treatment for symptomatic sarcoidosis. He began a course of 40 mg (0.20 mg/kg actual body weight) oral prednisone daily. He now required 6 L/m supplemental oxygen. After IV diuretic therapy during his hospitalization, the patient was discharged on his preadmission oral diuretic dose. Pulmonary vasodilator therapy was not initiated for PH as left heart disease and sleep-disordered breathing needed to be managed first.
One month after steroid initiation, the patient reported that the dyspnea and hypoxemia had markedly improved. His oxygen flow rate was reduced to 2 L/m. He remained normotensive and had no further difficulties with fluid retention or volume overload on a stable dose of oral diuretics. He had elevated blood glucose with a glycated hemoglobin (HbA1c) of 6.4%. He began treatment with glipizide 5 mg daily.
After 3 months, he returned to the emergency department with hyperosmolar nonketotic hyperglycemia due to steroid-induced diabetes mellitus (DM). His HbA1c was now 17.1%. The patient was started on a home insulin regimen, and his blood sugar values subsequently improved. He remained symptomatically better and lost 40 pounds with a guided weight management program and a stable diuretic regimen. He underwent arrhythmia evaluation with a Holter monitor that showed AF without ventricular arrhythmias.
Unfortunately, he did not return for cardiac or pulmonary reevaluation, and was lost to follow-up. Nine months after initiation of treatment, the patient died after an out-of-hospital cardiac arrest.
Discussion
These 2 cases highlight therapeutic challenges that may arise in the management of sarcoidosis with symptomatic vital organ involvement and coexistent extreme obesity. Both patients showed symptom improvement with moderate doses of prednisone (40 mg to 50 mg daily), but serious treatment-related complications developed: further weight gain in the first patient, and severe DM in the second. Although DM may have been a direct treatment complication in our second patient, his HFpEF and PH were high-risk comorbidities; he did not present with acute symptomatic worsening after treatment initiation. His symptoms were never reassessed when he was lost to follow-up.
Sarcoidosis/Obesity Relationship
Recent evidence suggests that patients with obesity are at increased risk of developing sarcoidosis.5-7 Although the mechanism of association is unclear, several possibilities have been proposed.
Neurosarcoidosis. One known but rare cause of obesity is neurosarcoidosis of the hypothalamus or pituitary.14 This was investigated in one of our patients.
Proinflammatory responses. Another possible mechanism for the association of sarcoidosis and obesity is the proinflammatory properties of increased fat and adipose tissue.15 Obesity has been linked to an aberrant expansion of inflammatory cells and mediators, including macrophages, proinflammatory cytokines, T cells, and B cells.15 Leptin, produced primarily by adipocytes, also is higher in obese patients and has been found to be proinflammatory.16 These seem to underlie the link between obesity and other inflammatory diseases, including type 2 DM, gout, and atherosclerosis.15
Behavioral link. There also is a possible behavioral link between sarcoidosis and obesity: A patient might develop symptomatic sarcoidosis and later become less active due to dyspnea, which could predispose to weight gain.5
Management of Comorbid Sarcoidosis and Obesity
Regardless of the exact mechanism of this association, management of the co-occurrence of sarcoidosis and obesity poses a clinical problem, especially in cases of extreme obesity. Corticosteroids are generally considered the treatment of choice for symptomatic sarcoidosis. The initial treatment of symptomatic pulmonary sarcoidosis is 20 mg to 40 mg prednisone daily.10,11 Higher daily doses such as 60 mg to 80 mg or 0.5 mg/kg are typically used to treat cardiac sarcoidosis, although no clear consensus exists on the appropriate dose.12,17 One recent study showed no difference in cardiac outcomes in patients treated with high- and low-dose prednisone.18
For patients who are obese and require steroids to treat a medical condition, there is conflicting evidence on whether steroid doses should be increased in proportion to total body weight. Milsap and colleagues found clearance of prednisolone correlated strongly with degree of obesity, suggesting steroid dose should be increased in accordance with actual weight.19 In contrast, Dunn and colleagues found decreased clearance of methylprednisolone in obese patients, suggesting that ideal body weight dosing is appropriate.20
Identifying the appropriate steroid dose is important because corticosteroids place obese patients at higher risk of developing complications. Treatment-related comorbidities include DM, hypertension, fluid retention, osteoporosis, and infection. Further weight gain due to steroid use is a risk for progressive OSA and, even though not generally associated with sarcoidosis alone, OHS. For patients with sarcoidosis, these complications (DM, fluid retention, hypertension, sleep-disordered breathing) may increase the risk of cardiovascular disease and PH.21-23 Cardiomyopathy, especially with reduced EF and increased PH, can be associated with a poor prognosis in sarcoidosis.4,24-26 PH also can be challenging to treat patients with sarcoidosis because the response of PH to steroids is unclear.27 Small trials have shown the benefit of pulmonary vasodilators on hemodynamics, but these have generally been used in patients with stable sarcoidosis who do not have left-heart disease.28-30
Our Prescription Model
We empirically prescribed moderate total doses of prednisone—although low on a mg/kg basis—to balance efficacy and the risk of adverse effects in these 2 morbidly obese patients. We also managed treatment-related complications with guided weight-management programs, CPAP, or noninvasive ventilation for sleep-disordered breathing, and DM treatment.
Our cases demonstrate the need for close monitoring of weight, blood pressure, and blood glucose to detect and treat any complications that may arise during corticosteroid treatment. Aggressive treatment of hyperglycemia with insulin or oral alternatives associated with weight loss such as metformin, sulfonylureas, dipeptidyl peptidase 4 inhibitors, or glucagon-like peptide 1 receptor agonists, may help prevent further DM complications. Sleep-disordered breathing should be assessed and treated. Bariatric surgery may be an option to treat obesity and minimize resultant complications. In our patients, and likely many others, the degree of respiratory and cardiac disease coupled with poor wound healing due to chronic prednisone, may increase the procedural risks.
Conclusion
Our experiences with these patients illustrate that symptomatic and objective improvement in sarcoidosis may be achieved in morbidly obese patients with doses of prednisone that are generally considered moderate, though quite low on a mg/kg basis.
We believe ours is the first report to describe the use of corticosteroids for the treatment of sarcoidosis in patients with morbid obesity. That 2 patients were treated at a single VA medical center within 1-year likely reflects the rising incidence of morbid obesity in the US veteran population and suggests that other federal practitioners might encounter similar patients.
Further study may show that, as an alternative to initial moderate-dose prednisone, patients with symptomatic sarcoidosis and extreme obesity might be started on antimetabolite or antitumor necrosis factor medication or on low-dose prednisone and a second steroid-sparing agent.
1. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007;357(21):2153-2165.
2. Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet PY, Muller-Quernheim J. Sarcoidosis. Lancet. 2014;383 (9923):1155-1167.
3. Lal C, Medarov BI, Judson MA. Interrelationship between sleep-disordered breathing and sarcoidosis. Chest. 2015;148(4):1105-1114.
4. Dobarro D, Schreiber BE, Handler C, Beynon H, Denton CP, Coghlan JG. Clinical characteristics, haemodynamics and treatment of pulmonary hypertension in sarcoidosis in a single centre, and meta-analysis of the published data. Am J Cardiol. 2013;111(2):278-285.
5. Cozier YC, Coogan PF, Govender P, Berman JS, Palmer JR, Rosenberg L. Obesity and weight gain in relation to incidence of sarcoidosis in US black women: data from the Black Women’s Health Study. Chest. 2015;147(4):1086-1093.
6. Harpsoe MC, Basit S, Andersson M, et al. Body mass index and risk of autoimmune diseases: a study within the Danish National Birth Cohort. Int J Epidemiol. 2014;43(3):843-855.
7. Ungprasert P, Crowson CS, Matteson EL. Smoking, obesity and risk of sarcoidosis: a population-based nested case-control study. Respir Med. 2016;120:87-90.
8. Sturm R, Hattori A. Morbid obesity rates continue to rise rapidly in the United States. Int J Obes (Lond). 2013;37(6):889-891.
9. Nelson KM. The burden of obesity among a national probability sample of veterans. J Gen Intern Med. 2006; 21(9):915-919.
10. Moller DR, Chen ES. Systemic sarcoidosis. In: Grippi MA, Elias JA, Fishman et al, eds. Fishman’s Pulmonary Diseases and Disorders. 5th ed. New York, NY: McGraw-Hill; 2015: 823-841
11. Judson MA, Morgenthau AS, Baughman RP. Sarcoidosis. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel’s Textbook of Respiratory Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:1188-1206.
12. Patel D, Hamzeh NY. Immunosuppressive management of cardiac sarcoidosis. In: Freeman AM, Weinberger HD, eds. Cardiac Sarcoidosis. New York, NY: Springer; 2015:103-112.
13. Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract. 2010;89(3):309-319.
14. Anthony J, Esper GJ, Ioachimescu A. Hypothalamic-pituitary sarcoidosis with vision loss and hypopituitarism: case series and literature review. Pituitary. 2016;19(1):19-29.
15. Kanneganti TD, Dixit VD. Immunological complications of obesity. Nat Immunol. 2012;13(8):707-712.
16. Matarese G, Leiter EH, La Cava A. Leptin in autoimmunity: many questions, some answers. Tissue Antigens. 2007;70(2):87-95.
17. Doughan AR, Williams BR. Cardiac sarcoidosis. Heart. 2006;92(2):282-288.
18. Yazaki Y, Isobe M, Hiroe M, et al. Prognostic determinants of long-term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am J Cardiol. 2001;88(9):1006-1010.
19. Milsap RL, Plaisance KI, Jusko WJ. Prednisolone disposition in obese men. Clin Pharmacol Ther. 1984;36(6):824-831.
20. Dunn TE, Ludwig EA, Slaughter RL, Camara DS, Jusko WJ. Pharmacokinetics and pharmacodynamics of methylprednisolone in obesity. Clin Pharmacol Ther. 1991;49(5):536-549.
21. Eastwood PR, Malhotra A, Palmer LJ, et al. Obstructive sleep apnoea: from pathogenesis to treatment: current controversies and future directions. Respirology. 2010;15(4):587-595.
22. Wong HS, Williams AJ, Mok Y. The relationship between pulmonary hypertension and obstructive sleep apnea. Curr Opin Pulm Med. 2017;23(6):517-521.
23. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82-93.
24. Handa T, Nagai S, Miki S, et al. Incidence of pulmonary hypertension and its clinical relevance in patients with sarcoidosis. Chest. 2006;129(5):1246-1252.
25. Baughman RP, Engel PJ, Taylor L, Lower EE. Survival in sarcoidosis-associated pulmonary hypertension: the importance of hemodynamic evaluation. Chest. 2010;138(5):1078-1085.
26. Birnie DH, Kandolin R, Nery PB, Kupari M. Cardiac manifestations of sarcoidosis: diagnosis and management. Eur Heart J. 2017;38(35):2663-2670.
27. Nunes H, Humbert M, Capron F, et al. Pulmonary hypertension associated with sarcoidosis: mechanisms, haemodynamics and prognosis. Thorax. 2006;61(1):68-74.
28. Judson MA, Highland KB, Kwon S, et al. Ambrisentan for sarcoidosis associated pulmonary hypertension. Sarcoidosis Vasc Diffuse Lung Dis. 2011;28(2):139-145.
29. Baughman RP, Culver DA, Cordova FC, et al. Bosentan for sarcoidosis-associated pulmonary hypertension: a double-blind placebo controlled randomized trial. Chest. 2014;145(4):810-817.
30. Baughman RP, Judson MA, Lower EE, et al. Inhaled iloprost for sarcoidosis associated pulmonary hypertension. Sarcoidosis Vasc Diffuse Lung Dis. 2009;26(2):110-120.
1. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007;357(21):2153-2165.
2. Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet PY, Muller-Quernheim J. Sarcoidosis. Lancet. 2014;383 (9923):1155-1167.
3. Lal C, Medarov BI, Judson MA. Interrelationship between sleep-disordered breathing and sarcoidosis. Chest. 2015;148(4):1105-1114.
4. Dobarro D, Schreiber BE, Handler C, Beynon H, Denton CP, Coghlan JG. Clinical characteristics, haemodynamics and treatment of pulmonary hypertension in sarcoidosis in a single centre, and meta-analysis of the published data. Am J Cardiol. 2013;111(2):278-285.
5. Cozier YC, Coogan PF, Govender P, Berman JS, Palmer JR, Rosenberg L. Obesity and weight gain in relation to incidence of sarcoidosis in US black women: data from the Black Women’s Health Study. Chest. 2015;147(4):1086-1093.
6. Harpsoe MC, Basit S, Andersson M, et al. Body mass index and risk of autoimmune diseases: a study within the Danish National Birth Cohort. Int J Epidemiol. 2014;43(3):843-855.
7. Ungprasert P, Crowson CS, Matteson EL. Smoking, obesity and risk of sarcoidosis: a population-based nested case-control study. Respir Med. 2016;120:87-90.
8. Sturm R, Hattori A. Morbid obesity rates continue to rise rapidly in the United States. Int J Obes (Lond). 2013;37(6):889-891.
9. Nelson KM. The burden of obesity among a national probability sample of veterans. J Gen Intern Med. 2006; 21(9):915-919.
10. Moller DR, Chen ES. Systemic sarcoidosis. In: Grippi MA, Elias JA, Fishman et al, eds. Fishman’s Pulmonary Diseases and Disorders. 5th ed. New York, NY: McGraw-Hill; 2015: 823-841
11. Judson MA, Morgenthau AS, Baughman RP. Sarcoidosis. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel’s Textbook of Respiratory Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:1188-1206.
12. Patel D, Hamzeh NY. Immunosuppressive management of cardiac sarcoidosis. In: Freeman AM, Weinberger HD, eds. Cardiac Sarcoidosis. New York, NY: Springer; 2015:103-112.
13. Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract. 2010;89(3):309-319.
14. Anthony J, Esper GJ, Ioachimescu A. Hypothalamic-pituitary sarcoidosis with vision loss and hypopituitarism: case series and literature review. Pituitary. 2016;19(1):19-29.
15. Kanneganti TD, Dixit VD. Immunological complications of obesity. Nat Immunol. 2012;13(8):707-712.
16. Matarese G, Leiter EH, La Cava A. Leptin in autoimmunity: many questions, some answers. Tissue Antigens. 2007;70(2):87-95.
17. Doughan AR, Williams BR. Cardiac sarcoidosis. Heart. 2006;92(2):282-288.
18. Yazaki Y, Isobe M, Hiroe M, et al. Prognostic determinants of long-term survival in Japanese patients with cardiac sarcoidosis treated with prednisone. Am J Cardiol. 2001;88(9):1006-1010.
19. Milsap RL, Plaisance KI, Jusko WJ. Prednisolone disposition in obese men. Clin Pharmacol Ther. 1984;36(6):824-831.
20. Dunn TE, Ludwig EA, Slaughter RL, Camara DS, Jusko WJ. Pharmacokinetics and pharmacodynamics of methylprednisolone in obesity. Clin Pharmacol Ther. 1991;49(5):536-549.
21. Eastwood PR, Malhotra A, Palmer LJ, et al. Obstructive sleep apnoea: from pathogenesis to treatment: current controversies and future directions. Respirology. 2010;15(4):587-595.
22. Wong HS, Williams AJ, Mok Y. The relationship between pulmonary hypertension and obstructive sleep apnea. Curr Opin Pulm Med. 2017;23(6):517-521.
23. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82-93.
24. Handa T, Nagai S, Miki S, et al. Incidence of pulmonary hypertension and its clinical relevance in patients with sarcoidosis. Chest. 2006;129(5):1246-1252.
25. Baughman RP, Engel PJ, Taylor L, Lower EE. Survival in sarcoidosis-associated pulmonary hypertension: the importance of hemodynamic evaluation. Chest. 2010;138(5):1078-1085.
26. Birnie DH, Kandolin R, Nery PB, Kupari M. Cardiac manifestations of sarcoidosis: diagnosis and management. Eur Heart J. 2017;38(35):2663-2670.
27. Nunes H, Humbert M, Capron F, et al. Pulmonary hypertension associated with sarcoidosis: mechanisms, haemodynamics and prognosis. Thorax. 2006;61(1):68-74.
28. Judson MA, Highland KB, Kwon S, et al. Ambrisentan for sarcoidosis associated pulmonary hypertension. Sarcoidosis Vasc Diffuse Lung Dis. 2011;28(2):139-145.
29. Baughman RP, Culver DA, Cordova FC, et al. Bosentan for sarcoidosis-associated pulmonary hypertension: a double-blind placebo controlled randomized trial. Chest. 2014;145(4):810-817.
30. Baughman RP, Judson MA, Lower EE, et al. Inhaled iloprost for sarcoidosis associated pulmonary hypertension. Sarcoidosis Vasc Diffuse Lung Dis. 2009;26(2):110-120.