User login
Parent-led intervention linked with decreased autism symptoms in at-risk infants
These findings, which were published in JAMA Pediatrics, were the first evidence worldwide that a preemptive intervention during infancy could lead to such a significant improvement in children’s social development, resulting in “three times fewer diagnoses of autism at age 3,” said lead author Andrew Whitehouse, PhD, in a statement.
“No trial of a preemptive infant intervention, applied prior to diagnosis, has to date shown such an effect to impact diagnostic outcomes – until now,” he said.
Study intervention is a nontraditonal approach
Dr. Whitehouse, who is professor of Autism Research at Telethon Kids and University of Western Australia, and Director of CliniKids in Perth, said the intervention is a departure from traditional approaches. “Traditionally, therapy seeks to train children to learn ‘typical’ behaviors,” he said in an email. “The difference of this therapy is that we help parents understand the unique abilities of their baby, and to use these strengths as a foundation for future development.”
Dr. Whitehouse’s study included 103 children (aged approximately 12 months), who displayed at least three of five behaviors indicating a high likelihood of ASD as defined by the Social Attention and Communication Surveillance–Revised (SACS-R) 12-month checklist. The infants were randomized to receive either usual care or the intervention, which is called the iBASIS–Video Interaction to Promote Positive Parenting (iBASIS-VIPP). Usual care was delivered by community physicians, whereas the intervention involved 10 sessions delivered at home by a trained therapist.
“The iBASIS-VIPP uses video-feedback as a means of helping parents recognize their baby’s communication cues so they can respond in a way that builds their social communication development,” Dr. Whitehouse explained in an interview. “The therapist then provides guidance to the parent as to how their baby is communicating with them, and they can communicate back to have back-and-forth conversations.”
“We know these back-and-forth conversations are crucial to support early social communication development, and are a precursor to more complex skills, such as verbal language,” he added.
Reassessment of the children at age 3 years showed a “small but enduring” benefit of the intervention, noted the authors. Children in the intervention group had a reduction in ASD symptom severity (P = .04), and reduced odds of ASD classification, compared with children receiving usual care (6.7% vs. 20.5%; odds ratio, 0.18; P = .02).
The findings provide “initial evidence of efficacy for a new clinical model that uses a specific developmentally focused intervention,” noted the authors. “The children falling below the diagnostic threshold still had developmental difficulties, but by working with each child’s unique differences, rather than trying to counter them, the therapy has effectively supported their development through the early childhood years,” noted Dr. Whitehouse in a statement.
Other research has shown benefits of new study approach
This is a “solid” study, “but, as acknowledged by the authors, the main effects are small in magnitude, and longer-term outcomes will be important to capture,” said Jessica Brian, PhD, C Psych, associate professor in the department of pediatrics at the University of Toronto, colead at the Autism Research Centre, and psychologist and clinician-investigator at Holland Bloorview Kids Rehab Hospital in Toronto.
Dr. Brian said she and her coauthors of a paper published in Autism Research and others have shown that the kind of approach used in the new study can be helpful for enhancing different areas of toddler development, but “the specific finding of reduced likelihood of a clinical ASD diagnosis is a bit different.”
The goal of reducing the likelihood of an ASD diagnosis “needs to be considered carefully, from the perspective of autism acceptance,” she added. “From an acceptance lens, the primary objective of early intervention in ASD might be better positioned as aiming to enhance or support a young child’s development, help them make developmental progress, build on their strengths, optimize outcomes, or reduce impairment. … I think the authors do a good job of balancing this perspective.”
New study shows value of parent-mediated interventions
Overall, Dr. Brian, who coauthored the Canadian Paediatric Society’s position statement on ASD diagnosis, lauded the findings as good news.
“It shows the value of using parent-mediated interventions, which are far less costly and are more resource-efficient than most therapist-delivered models.”
“In cases where parent-mediated approaches are made available to families prior to diagnosis, there is potential for strong effects, when the brain is most amenable to learning. Such models may also be an ideal fit before diagnosis, since they are less resource-intensive than therapist-delivered models, which may only be funded by governments once a diagnosis is confirmed,” she said.
“Finally, parent-mediated programs have the potential to support parents during what, for many families, is a particularly challenging time as they identify their child’s developmental differences or receive a diagnosis. Such programs have potential to increase parents’ confidence in parenting a young child with unique learning needs.”
What Dr. Brian thought was missing from the paper was acknowledgment that, “despite early developmental gains from parent-mediated interventions, it is likely that most children with ASD will need additional supports throughout development.”
This study was sponsored by the Telethon Kids Institute. Dr. Whitehouse reported no conflicts of interest. Dr. Brian codeveloped a parent-mediated intervention for toddlers with probable or confirmed ASD (the Social ABCs), for which she does not receive any royalties.
These findings, which were published in JAMA Pediatrics, were the first evidence worldwide that a preemptive intervention during infancy could lead to such a significant improvement in children’s social development, resulting in “three times fewer diagnoses of autism at age 3,” said lead author Andrew Whitehouse, PhD, in a statement.
“No trial of a preemptive infant intervention, applied prior to diagnosis, has to date shown such an effect to impact diagnostic outcomes – until now,” he said.
Study intervention is a nontraditonal approach
Dr. Whitehouse, who is professor of Autism Research at Telethon Kids and University of Western Australia, and Director of CliniKids in Perth, said the intervention is a departure from traditional approaches. “Traditionally, therapy seeks to train children to learn ‘typical’ behaviors,” he said in an email. “The difference of this therapy is that we help parents understand the unique abilities of their baby, and to use these strengths as a foundation for future development.”
Dr. Whitehouse’s study included 103 children (aged approximately 12 months), who displayed at least three of five behaviors indicating a high likelihood of ASD as defined by the Social Attention and Communication Surveillance–Revised (SACS-R) 12-month checklist. The infants were randomized to receive either usual care or the intervention, which is called the iBASIS–Video Interaction to Promote Positive Parenting (iBASIS-VIPP). Usual care was delivered by community physicians, whereas the intervention involved 10 sessions delivered at home by a trained therapist.
“The iBASIS-VIPP uses video-feedback as a means of helping parents recognize their baby’s communication cues so they can respond in a way that builds their social communication development,” Dr. Whitehouse explained in an interview. “The therapist then provides guidance to the parent as to how their baby is communicating with them, and they can communicate back to have back-and-forth conversations.”
“We know these back-and-forth conversations are crucial to support early social communication development, and are a precursor to more complex skills, such as verbal language,” he added.
Reassessment of the children at age 3 years showed a “small but enduring” benefit of the intervention, noted the authors. Children in the intervention group had a reduction in ASD symptom severity (P = .04), and reduced odds of ASD classification, compared with children receiving usual care (6.7% vs. 20.5%; odds ratio, 0.18; P = .02).
The findings provide “initial evidence of efficacy for a new clinical model that uses a specific developmentally focused intervention,” noted the authors. “The children falling below the diagnostic threshold still had developmental difficulties, but by working with each child’s unique differences, rather than trying to counter them, the therapy has effectively supported their development through the early childhood years,” noted Dr. Whitehouse in a statement.
Other research has shown benefits of new study approach
This is a “solid” study, “but, as acknowledged by the authors, the main effects are small in magnitude, and longer-term outcomes will be important to capture,” said Jessica Brian, PhD, C Psych, associate professor in the department of pediatrics at the University of Toronto, colead at the Autism Research Centre, and psychologist and clinician-investigator at Holland Bloorview Kids Rehab Hospital in Toronto.
Dr. Brian said she and her coauthors of a paper published in Autism Research and others have shown that the kind of approach used in the new study can be helpful for enhancing different areas of toddler development, but “the specific finding of reduced likelihood of a clinical ASD diagnosis is a bit different.”
The goal of reducing the likelihood of an ASD diagnosis “needs to be considered carefully, from the perspective of autism acceptance,” she added. “From an acceptance lens, the primary objective of early intervention in ASD might be better positioned as aiming to enhance or support a young child’s development, help them make developmental progress, build on their strengths, optimize outcomes, or reduce impairment. … I think the authors do a good job of balancing this perspective.”
New study shows value of parent-mediated interventions
Overall, Dr. Brian, who coauthored the Canadian Paediatric Society’s position statement on ASD diagnosis, lauded the findings as good news.
“It shows the value of using parent-mediated interventions, which are far less costly and are more resource-efficient than most therapist-delivered models.”
“In cases where parent-mediated approaches are made available to families prior to diagnosis, there is potential for strong effects, when the brain is most amenable to learning. Such models may also be an ideal fit before diagnosis, since they are less resource-intensive than therapist-delivered models, which may only be funded by governments once a diagnosis is confirmed,” she said.
“Finally, parent-mediated programs have the potential to support parents during what, for many families, is a particularly challenging time as they identify their child’s developmental differences or receive a diagnosis. Such programs have potential to increase parents’ confidence in parenting a young child with unique learning needs.”
What Dr. Brian thought was missing from the paper was acknowledgment that, “despite early developmental gains from parent-mediated interventions, it is likely that most children with ASD will need additional supports throughout development.”
This study was sponsored by the Telethon Kids Institute. Dr. Whitehouse reported no conflicts of interest. Dr. Brian codeveloped a parent-mediated intervention for toddlers with probable or confirmed ASD (the Social ABCs), for which she does not receive any royalties.
These findings, which were published in JAMA Pediatrics, were the first evidence worldwide that a preemptive intervention during infancy could lead to such a significant improvement in children’s social development, resulting in “three times fewer diagnoses of autism at age 3,” said lead author Andrew Whitehouse, PhD, in a statement.
“No trial of a preemptive infant intervention, applied prior to diagnosis, has to date shown such an effect to impact diagnostic outcomes – until now,” he said.
Study intervention is a nontraditonal approach
Dr. Whitehouse, who is professor of Autism Research at Telethon Kids and University of Western Australia, and Director of CliniKids in Perth, said the intervention is a departure from traditional approaches. “Traditionally, therapy seeks to train children to learn ‘typical’ behaviors,” he said in an email. “The difference of this therapy is that we help parents understand the unique abilities of their baby, and to use these strengths as a foundation for future development.”
Dr. Whitehouse’s study included 103 children (aged approximately 12 months), who displayed at least three of five behaviors indicating a high likelihood of ASD as defined by the Social Attention and Communication Surveillance–Revised (SACS-R) 12-month checklist. The infants were randomized to receive either usual care or the intervention, which is called the iBASIS–Video Interaction to Promote Positive Parenting (iBASIS-VIPP). Usual care was delivered by community physicians, whereas the intervention involved 10 sessions delivered at home by a trained therapist.
“The iBASIS-VIPP uses video-feedback as a means of helping parents recognize their baby’s communication cues so they can respond in a way that builds their social communication development,” Dr. Whitehouse explained in an interview. “The therapist then provides guidance to the parent as to how their baby is communicating with them, and they can communicate back to have back-and-forth conversations.”
“We know these back-and-forth conversations are crucial to support early social communication development, and are a precursor to more complex skills, such as verbal language,” he added.
Reassessment of the children at age 3 years showed a “small but enduring” benefit of the intervention, noted the authors. Children in the intervention group had a reduction in ASD symptom severity (P = .04), and reduced odds of ASD classification, compared with children receiving usual care (6.7% vs. 20.5%; odds ratio, 0.18; P = .02).
The findings provide “initial evidence of efficacy for a new clinical model that uses a specific developmentally focused intervention,” noted the authors. “The children falling below the diagnostic threshold still had developmental difficulties, but by working with each child’s unique differences, rather than trying to counter them, the therapy has effectively supported their development through the early childhood years,” noted Dr. Whitehouse in a statement.
Other research has shown benefits of new study approach
This is a “solid” study, “but, as acknowledged by the authors, the main effects are small in magnitude, and longer-term outcomes will be important to capture,” said Jessica Brian, PhD, C Psych, associate professor in the department of pediatrics at the University of Toronto, colead at the Autism Research Centre, and psychologist and clinician-investigator at Holland Bloorview Kids Rehab Hospital in Toronto.
Dr. Brian said she and her coauthors of a paper published in Autism Research and others have shown that the kind of approach used in the new study can be helpful for enhancing different areas of toddler development, but “the specific finding of reduced likelihood of a clinical ASD diagnosis is a bit different.”
The goal of reducing the likelihood of an ASD diagnosis “needs to be considered carefully, from the perspective of autism acceptance,” she added. “From an acceptance lens, the primary objective of early intervention in ASD might be better positioned as aiming to enhance or support a young child’s development, help them make developmental progress, build on their strengths, optimize outcomes, or reduce impairment. … I think the authors do a good job of balancing this perspective.”
New study shows value of parent-mediated interventions
Overall, Dr. Brian, who coauthored the Canadian Paediatric Society’s position statement on ASD diagnosis, lauded the findings as good news.
“It shows the value of using parent-mediated interventions, which are far less costly and are more resource-efficient than most therapist-delivered models.”
“In cases where parent-mediated approaches are made available to families prior to diagnosis, there is potential for strong effects, when the brain is most amenable to learning. Such models may also be an ideal fit before diagnosis, since they are less resource-intensive than therapist-delivered models, which may only be funded by governments once a diagnosis is confirmed,” she said.
“Finally, parent-mediated programs have the potential to support parents during what, for many families, is a particularly challenging time as they identify their child’s developmental differences or receive a diagnosis. Such programs have potential to increase parents’ confidence in parenting a young child with unique learning needs.”
What Dr. Brian thought was missing from the paper was acknowledgment that, “despite early developmental gains from parent-mediated interventions, it is likely that most children with ASD will need additional supports throughout development.”
This study was sponsored by the Telethon Kids Institute. Dr. Whitehouse reported no conflicts of interest. Dr. Brian codeveloped a parent-mediated intervention for toddlers with probable or confirmed ASD (the Social ABCs), for which she does not receive any royalties.
FROM JAMA PEDIATRICS
Higher than standard vitamin D dose provides no added benefits to children’s neurodevelopment
Prescribing higher doses of vitamin D may not provide any additional benefits to children’s brain development, a new study suggests.
New research published online in JAMA found that there were no differences in children’s developmental milestones or social-emotional problems when given a higher daily dose of 1,200 IU of vitamin D versus the standard dose of 400 IU.
Although past studies have looked into the relationship between vitamin D and neurodevelopment in children, the findings were inconsistent. A 2019 study published in Psychoneuroendocrinology found that vitamin D deficiency could be a biological risk factor for psychiatric disorders and that vitamin D acts as a neurosteroid with direct effect on brain development. However, a 2021 study published in Global Pediatric Health found no significant association between vitamin D levels and neurodevelopmental status in children at 2 years old.
Researchers of the current study said they expected to find a positive association between higher vitamin D levels and neurodevelopment.
“Our results highlight that the current recommendations, set forth mainly on the basis of bone health, also support healthy brain development,” said study author Kati Heinonen, PhD, associate professor of psychology and welfare sciences at Tampere (Finland) University. “Our results also point out that higher than currently recommended levels do not add to the benefits received from the vitamin D supplements.”
For the study, Dr. Heinonen and colleagues analyzed data from a double-blind, randomized clinical trial involving healthy infants born full-term between Jan. 1, 2013, and June 30, 2014, at a maternity hospital in Helsinki. They got follow-up information on 404 infants who were randomized to receive 400 IU of oral vitamin D supplements daily and 397 infants who received 1,200 IU of vitamin D supplements from 2 weeks to 24 months of age.
Researchers found no differences between the 400-IU group and the 1,200-IU group in the mean adjusted Ages and Stages Questionnaire total score at 12 months, a questionnaire that’s used to measure communication, problem solving, gross motor skills, fine motor skills, and personal and social skills. However, they did find that children receiving 1,200 IU of vitamin D supplementation had better developmental milestone scores in communication and problem-solving skills at 12 months.
Furthermore, they also found that higher vitamin D concentrations were associated with fewer sleeping problems at 24 months.
The researcher’s findings did not surprise Francis E. Rushton Jr., MD, a clinical professor of pediatrics at the University of South Carolina, Columbia, who was not involved in the study. “This study reveals that more is not always better,” Dr. Rushton said in an interview.
Dr. Rushton, who is also the medical director of the Quality Through Innovation in Pediatrics network, said other ways to enhance early brain development include initiatives like infant home visitation and language enrichment programs like Reach Out and Read.
Dr. Heinonen noted that the study’s findings might be different if it had been conducted on infants from a different country.
“We have to remember that the participants were from northern European countries where several food products are also fortified by vitamin D,” Dr. Heinonen explained. “Thus, direct recommendations of the amount of the supplementation given for children from 2 weeks to 2 years in other countries should not be done on the basis of our study.”
Researchers also observed that the children receiving 1,200 IU of vitamin D supplementation had a risk of scoring higher on the externalizing symptoms scale at 24 months, meaning these infants are more likely to lose their temper and become physically aggressive.
“We could not fully exclude potential disadvantageous effects of higher doses. Even if minimal, the potential nonbeneficial effects of higher than standard doses warrant further studies,” she said.
Researchers said more studies are needed that follow children up to school age and adolescence, when higher cognitive abilities develop, to understand the long-term outcomes of early vitamin D supplementation.
Prescribing higher doses of vitamin D may not provide any additional benefits to children’s brain development, a new study suggests.
New research published online in JAMA found that there were no differences in children’s developmental milestones or social-emotional problems when given a higher daily dose of 1,200 IU of vitamin D versus the standard dose of 400 IU.
Although past studies have looked into the relationship between vitamin D and neurodevelopment in children, the findings were inconsistent. A 2019 study published in Psychoneuroendocrinology found that vitamin D deficiency could be a biological risk factor for psychiatric disorders and that vitamin D acts as a neurosteroid with direct effect on brain development. However, a 2021 study published in Global Pediatric Health found no significant association between vitamin D levels and neurodevelopmental status in children at 2 years old.
Researchers of the current study said they expected to find a positive association between higher vitamin D levels and neurodevelopment.
“Our results highlight that the current recommendations, set forth mainly on the basis of bone health, also support healthy brain development,” said study author Kati Heinonen, PhD, associate professor of psychology and welfare sciences at Tampere (Finland) University. “Our results also point out that higher than currently recommended levels do not add to the benefits received from the vitamin D supplements.”
For the study, Dr. Heinonen and colleagues analyzed data from a double-blind, randomized clinical trial involving healthy infants born full-term between Jan. 1, 2013, and June 30, 2014, at a maternity hospital in Helsinki. They got follow-up information on 404 infants who were randomized to receive 400 IU of oral vitamin D supplements daily and 397 infants who received 1,200 IU of vitamin D supplements from 2 weeks to 24 months of age.
Researchers found no differences between the 400-IU group and the 1,200-IU group in the mean adjusted Ages and Stages Questionnaire total score at 12 months, a questionnaire that’s used to measure communication, problem solving, gross motor skills, fine motor skills, and personal and social skills. However, they did find that children receiving 1,200 IU of vitamin D supplementation had better developmental milestone scores in communication and problem-solving skills at 12 months.
Furthermore, they also found that higher vitamin D concentrations were associated with fewer sleeping problems at 24 months.
The researcher’s findings did not surprise Francis E. Rushton Jr., MD, a clinical professor of pediatrics at the University of South Carolina, Columbia, who was not involved in the study. “This study reveals that more is not always better,” Dr. Rushton said in an interview.
Dr. Rushton, who is also the medical director of the Quality Through Innovation in Pediatrics network, said other ways to enhance early brain development include initiatives like infant home visitation and language enrichment programs like Reach Out and Read.
Dr. Heinonen noted that the study’s findings might be different if it had been conducted on infants from a different country.
“We have to remember that the participants were from northern European countries where several food products are also fortified by vitamin D,” Dr. Heinonen explained. “Thus, direct recommendations of the amount of the supplementation given for children from 2 weeks to 2 years in other countries should not be done on the basis of our study.”
Researchers also observed that the children receiving 1,200 IU of vitamin D supplementation had a risk of scoring higher on the externalizing symptoms scale at 24 months, meaning these infants are more likely to lose their temper and become physically aggressive.
“We could not fully exclude potential disadvantageous effects of higher doses. Even if minimal, the potential nonbeneficial effects of higher than standard doses warrant further studies,” she said.
Researchers said more studies are needed that follow children up to school age and adolescence, when higher cognitive abilities develop, to understand the long-term outcomes of early vitamin D supplementation.
Prescribing higher doses of vitamin D may not provide any additional benefits to children’s brain development, a new study suggests.
New research published online in JAMA found that there were no differences in children’s developmental milestones or social-emotional problems when given a higher daily dose of 1,200 IU of vitamin D versus the standard dose of 400 IU.
Although past studies have looked into the relationship between vitamin D and neurodevelopment in children, the findings were inconsistent. A 2019 study published in Psychoneuroendocrinology found that vitamin D deficiency could be a biological risk factor for psychiatric disorders and that vitamin D acts as a neurosteroid with direct effect on brain development. However, a 2021 study published in Global Pediatric Health found no significant association between vitamin D levels and neurodevelopmental status in children at 2 years old.
Researchers of the current study said they expected to find a positive association between higher vitamin D levels and neurodevelopment.
“Our results highlight that the current recommendations, set forth mainly on the basis of bone health, also support healthy brain development,” said study author Kati Heinonen, PhD, associate professor of psychology and welfare sciences at Tampere (Finland) University. “Our results also point out that higher than currently recommended levels do not add to the benefits received from the vitamin D supplements.”
For the study, Dr. Heinonen and colleagues analyzed data from a double-blind, randomized clinical trial involving healthy infants born full-term between Jan. 1, 2013, and June 30, 2014, at a maternity hospital in Helsinki. They got follow-up information on 404 infants who were randomized to receive 400 IU of oral vitamin D supplements daily and 397 infants who received 1,200 IU of vitamin D supplements from 2 weeks to 24 months of age.
Researchers found no differences between the 400-IU group and the 1,200-IU group in the mean adjusted Ages and Stages Questionnaire total score at 12 months, a questionnaire that’s used to measure communication, problem solving, gross motor skills, fine motor skills, and personal and social skills. However, they did find that children receiving 1,200 IU of vitamin D supplementation had better developmental milestone scores in communication and problem-solving skills at 12 months.
Furthermore, they also found that higher vitamin D concentrations were associated with fewer sleeping problems at 24 months.
The researcher’s findings did not surprise Francis E. Rushton Jr., MD, a clinical professor of pediatrics at the University of South Carolina, Columbia, who was not involved in the study. “This study reveals that more is not always better,” Dr. Rushton said in an interview.
Dr. Rushton, who is also the medical director of the Quality Through Innovation in Pediatrics network, said other ways to enhance early brain development include initiatives like infant home visitation and language enrichment programs like Reach Out and Read.
Dr. Heinonen noted that the study’s findings might be different if it had been conducted on infants from a different country.
“We have to remember that the participants were from northern European countries where several food products are also fortified by vitamin D,” Dr. Heinonen explained. “Thus, direct recommendations of the amount of the supplementation given for children from 2 weeks to 2 years in other countries should not be done on the basis of our study.”
Researchers also observed that the children receiving 1,200 IU of vitamin D supplementation had a risk of scoring higher on the externalizing symptoms scale at 24 months, meaning these infants are more likely to lose their temper and become physically aggressive.
“We could not fully exclude potential disadvantageous effects of higher doses. Even if minimal, the potential nonbeneficial effects of higher than standard doses warrant further studies,” she said.
Researchers said more studies are needed that follow children up to school age and adolescence, when higher cognitive abilities develop, to understand the long-term outcomes of early vitamin D supplementation.
FROM JAMA
Assessing headache severity via migraine symptoms can help predict outcomes
according to an analysis of data from thousands of headache sufferers who recorded variables like pain and duration in a daily digital diary.
“Our hope is that this work serves as foundational basis for better understanding the complexity of headache as a symptom-based condition,” James S. McGinley, PhD, of Vector Psychometric Group in Chapel Hill, N.C., and coauthors wrote. The study was published in Cephalalgia.
To evaluate whether keeping track of daily headache features can produce a useful, predictive score, the researchers reviewed data from migraine patients that were collected via N1‑Headache, a commercial digital health platform. Ultimately, information from 4,380 adults with a self-reported migraine diagnosis was analyzed; the sample was 90% female and their mean age was 37 years. Study participants reported an average of 33 headaches per month over the last 3 months. Nine patient-reported variables were initially considered in calculating the Headache Day Severity (HDS) score: pain intensity, headache duration, aura, pulsating/throbbing pain, unilateral pain, pain aggravation by activity, nausea/vomiting, photophobia, and phonophobia.
After determining that unilateral pain was not a meaningful variable, the researchers’ model found that, for every 1 standard deviation increase in HDS, the patient’s odds of physician visit increased by 71% (odds ratio, 1.71; 95% confidence interval, 1.32-2.21) and the odds of an ED visit increased by 342% (OR, 4.42; 95% CI, 2.23-7.60). They also found that the likelihood of missed work or school increased by 190% (OR, 2.90; 95% CI, 2.56-3.29), the chances of missing household work increased by 237% (OR, 3.37; 95% CI, 3.06-3.72) and the odds of missing other leisure or social activity increased by 228% (OR, 3.28; 95% CI, 2.97-3.64).
Tracking multiple variables
“We encourage all of our patients to monitor their headaches; there are just too many variables to try to keep it in your head,” Robert Cowan, MD, professor of neurology and chief of the division of headache medicine at Stanford (Calif.) University, said in an interview. He referenced a previous study from the University of Washington where patients were asked to track their headaches; that data was then compared against their self-reported headaches at a quarterly physician visit.
“What they found was there was absolutely no correlation with reported frequency of headache at the visit and what was seen in the tracker,” he said. “If patients had a headache in the previous 3 days before their visit, they felt that their headaches were poorly controlled. If they hadn’t, they thought their headaches were under good control. So the value of tracking is pretty clear.”
He added that, while not every headache sufferer needs to track their daily routines and symptoms, once those symptoms interfere with your life on a day-to-day basis, it’s probably time to consider keeping tabs on yourself with a tool of some sort. And while this study’s calculated HDS score supports the idea of migraine’s complexity, it also leaves unanswered the question of how to treat patients with severe symptoms.
“Frequently,” he said, “we’ll see patients who say: ‘I can deal with the pain, but the nausea makes it impossible to work, or the light sensitivity makes it impossible to go outside.’ The big question within the headache community is, can you treat migraine and have it address the whole spectrum, from dizziness to light sensitivity to sound sensitivity to vertigo, or should you be going after individual symptoms? That’s a controversy that rages on; I think most of us go for a combination. We’re in a polypharmacy phase: ‘If nausea is a big problem, take this, but we also try to prevent the whole migraine complex, so take this as well.’ ”
The authors acknowledged their study’s limitations, including the inability to determine how many participants’ migraines were formally diagnosed by a trained medical professional and the lack of generalizability of data from a convenience sample, though they added that patients who independently track their own headaches “may be representative of those who would participate in a clinical trial.” In addition, as seven of the nine features were collected in N1‑Headache on a yes/no scale, they recognized that “increasing the number of response options for each item may improve our ability to measure HDS.”
The study was funded by Amgen through the Competitive Grant Program in Migraine Research. The authors declared several potential conflicts of interest, including receiving funding, research support, salary, and honoraria from various pharmaceutical companies.
according to an analysis of data from thousands of headache sufferers who recorded variables like pain and duration in a daily digital diary.
“Our hope is that this work serves as foundational basis for better understanding the complexity of headache as a symptom-based condition,” James S. McGinley, PhD, of Vector Psychometric Group in Chapel Hill, N.C., and coauthors wrote. The study was published in Cephalalgia.
To evaluate whether keeping track of daily headache features can produce a useful, predictive score, the researchers reviewed data from migraine patients that were collected via N1‑Headache, a commercial digital health platform. Ultimately, information from 4,380 adults with a self-reported migraine diagnosis was analyzed; the sample was 90% female and their mean age was 37 years. Study participants reported an average of 33 headaches per month over the last 3 months. Nine patient-reported variables were initially considered in calculating the Headache Day Severity (HDS) score: pain intensity, headache duration, aura, pulsating/throbbing pain, unilateral pain, pain aggravation by activity, nausea/vomiting, photophobia, and phonophobia.
After determining that unilateral pain was not a meaningful variable, the researchers’ model found that, for every 1 standard deviation increase in HDS, the patient’s odds of physician visit increased by 71% (odds ratio, 1.71; 95% confidence interval, 1.32-2.21) and the odds of an ED visit increased by 342% (OR, 4.42; 95% CI, 2.23-7.60). They also found that the likelihood of missed work or school increased by 190% (OR, 2.90; 95% CI, 2.56-3.29), the chances of missing household work increased by 237% (OR, 3.37; 95% CI, 3.06-3.72) and the odds of missing other leisure or social activity increased by 228% (OR, 3.28; 95% CI, 2.97-3.64).
Tracking multiple variables
“We encourage all of our patients to monitor their headaches; there are just too many variables to try to keep it in your head,” Robert Cowan, MD, professor of neurology and chief of the division of headache medicine at Stanford (Calif.) University, said in an interview. He referenced a previous study from the University of Washington where patients were asked to track their headaches; that data was then compared against their self-reported headaches at a quarterly physician visit.
“What they found was there was absolutely no correlation with reported frequency of headache at the visit and what was seen in the tracker,” he said. “If patients had a headache in the previous 3 days before their visit, they felt that their headaches were poorly controlled. If they hadn’t, they thought their headaches were under good control. So the value of tracking is pretty clear.”
He added that, while not every headache sufferer needs to track their daily routines and symptoms, once those symptoms interfere with your life on a day-to-day basis, it’s probably time to consider keeping tabs on yourself with a tool of some sort. And while this study’s calculated HDS score supports the idea of migraine’s complexity, it also leaves unanswered the question of how to treat patients with severe symptoms.
“Frequently,” he said, “we’ll see patients who say: ‘I can deal with the pain, but the nausea makes it impossible to work, or the light sensitivity makes it impossible to go outside.’ The big question within the headache community is, can you treat migraine and have it address the whole spectrum, from dizziness to light sensitivity to sound sensitivity to vertigo, or should you be going after individual symptoms? That’s a controversy that rages on; I think most of us go for a combination. We’re in a polypharmacy phase: ‘If nausea is a big problem, take this, but we also try to prevent the whole migraine complex, so take this as well.’ ”
The authors acknowledged their study’s limitations, including the inability to determine how many participants’ migraines were formally diagnosed by a trained medical professional and the lack of generalizability of data from a convenience sample, though they added that patients who independently track their own headaches “may be representative of those who would participate in a clinical trial.” In addition, as seven of the nine features were collected in N1‑Headache on a yes/no scale, they recognized that “increasing the number of response options for each item may improve our ability to measure HDS.”
The study was funded by Amgen through the Competitive Grant Program in Migraine Research. The authors declared several potential conflicts of interest, including receiving funding, research support, salary, and honoraria from various pharmaceutical companies.
according to an analysis of data from thousands of headache sufferers who recorded variables like pain and duration in a daily digital diary.
“Our hope is that this work serves as foundational basis for better understanding the complexity of headache as a symptom-based condition,” James S. McGinley, PhD, of Vector Psychometric Group in Chapel Hill, N.C., and coauthors wrote. The study was published in Cephalalgia.
To evaluate whether keeping track of daily headache features can produce a useful, predictive score, the researchers reviewed data from migraine patients that were collected via N1‑Headache, a commercial digital health platform. Ultimately, information from 4,380 adults with a self-reported migraine diagnosis was analyzed; the sample was 90% female and their mean age was 37 years. Study participants reported an average of 33 headaches per month over the last 3 months. Nine patient-reported variables were initially considered in calculating the Headache Day Severity (HDS) score: pain intensity, headache duration, aura, pulsating/throbbing pain, unilateral pain, pain aggravation by activity, nausea/vomiting, photophobia, and phonophobia.
After determining that unilateral pain was not a meaningful variable, the researchers’ model found that, for every 1 standard deviation increase in HDS, the patient’s odds of physician visit increased by 71% (odds ratio, 1.71; 95% confidence interval, 1.32-2.21) and the odds of an ED visit increased by 342% (OR, 4.42; 95% CI, 2.23-7.60). They also found that the likelihood of missed work or school increased by 190% (OR, 2.90; 95% CI, 2.56-3.29), the chances of missing household work increased by 237% (OR, 3.37; 95% CI, 3.06-3.72) and the odds of missing other leisure or social activity increased by 228% (OR, 3.28; 95% CI, 2.97-3.64).
Tracking multiple variables
“We encourage all of our patients to monitor their headaches; there are just too many variables to try to keep it in your head,” Robert Cowan, MD, professor of neurology and chief of the division of headache medicine at Stanford (Calif.) University, said in an interview. He referenced a previous study from the University of Washington where patients were asked to track their headaches; that data was then compared against their self-reported headaches at a quarterly physician visit.
“What they found was there was absolutely no correlation with reported frequency of headache at the visit and what was seen in the tracker,” he said. “If patients had a headache in the previous 3 days before their visit, they felt that their headaches were poorly controlled. If they hadn’t, they thought their headaches were under good control. So the value of tracking is pretty clear.”
He added that, while not every headache sufferer needs to track their daily routines and symptoms, once those symptoms interfere with your life on a day-to-day basis, it’s probably time to consider keeping tabs on yourself with a tool of some sort. And while this study’s calculated HDS score supports the idea of migraine’s complexity, it also leaves unanswered the question of how to treat patients with severe symptoms.
“Frequently,” he said, “we’ll see patients who say: ‘I can deal with the pain, but the nausea makes it impossible to work, or the light sensitivity makes it impossible to go outside.’ The big question within the headache community is, can you treat migraine and have it address the whole spectrum, from dizziness to light sensitivity to sound sensitivity to vertigo, or should you be going after individual symptoms? That’s a controversy that rages on; I think most of us go for a combination. We’re in a polypharmacy phase: ‘If nausea is a big problem, take this, but we also try to prevent the whole migraine complex, so take this as well.’ ”
The authors acknowledged their study’s limitations, including the inability to determine how many participants’ migraines were formally diagnosed by a trained medical professional and the lack of generalizability of data from a convenience sample, though they added that patients who independently track their own headaches “may be representative of those who would participate in a clinical trial.” In addition, as seven of the nine features were collected in N1‑Headache on a yes/no scale, they recognized that “increasing the number of response options for each item may improve our ability to measure HDS.”
The study was funded by Amgen through the Competitive Grant Program in Migraine Research. The authors declared several potential conflicts of interest, including receiving funding, research support, salary, and honoraria from various pharmaceutical companies.
FROM CEPHALALGIA
Aspirin and heparin increase bleeding risk during EVT
Treatment with acetylsalicylic acid (ASA) or heparin is associated with an increased risk for symptomatic intracranial hemorrhage (sICH) in patients with ischemic stroke who are undergoing endovascular therapy (EVT), new data show.
In this population, ASA and heparin are each associated with an approximately doubled risk for sICH when administered during EVT.
“We did not find any evidence for a beneficial effect on functional outcome,” investigator Wouter van der Steen, MD, research physician and PhD student at Erasmus University Medical Center, Rotterdam, the Netherlands, told this news organization. The possibility that a positive effect would be observed if the trial were continued was considered negligible, he added.
The researchers stopped the trial for safety reasons and recommend avoiding the evaluated dosages of both medications during EVT for ischemic stroke, said Dr. van der Steen.
He presented the findings from the MR CLEAN-MED trial at the European Stroke Organisation Conference (ESOC) 2021, which was held online.
Trial stopped for safety
Previous research has supported the safety and efficacy of EVT for ischemic stroke. Still, more than 30% of patients do not recover, despite fast and complete recanalization. Incomplete microvascular reperfusion (IMR) could explain this incomplete recovery, the researchers note.
Microthrombi, which occlude distal vessels, and neutrophil extracellular traps can cause IMR. This problem can be reduced through treatment with ASA, which has an antithrombotic effect, or with heparin, which dissolves neutrophil extracellular traps, they add. Although these drugs are associated with good clinical outcomes, they entail an increased risk for sICH.
The investigators conducted the multicenter, randomized controlled MR CLEAN-MED trial to evaluate the effect of intravenous (IV) ASA and heparin, alone or in combination, during EVT for acute ischemic stroke. Treatment was open label, but outcome assessment was blinded. Eligible participants were adults with a National Institutes of Health Stroke Scale (NIHSS) score of greater than or equal to 2 and an anterior circulation large-vessel occlusion for whom EVT could be initiated in fewer than 6 hours.
Investigators randomly assigned patients to receive or not to receive ASA. Within each of these two treatment groups, patients were randomly assigned to receive no heparin, low-dose heparin, or moderate-dose heparin.
ASA was given in a loading dose of 300 mg. Patients who were given low-dose heparin received a loading dose of 5,000 IU followed by 500 IU/h for 6 hours. Patients who received moderate-dose heparin were given a loading dose of 5,000 IU followed by 1,250 IU/h for 6 hours.
The study’s primary outcome was Modified Rankin Scale (mRS) score at 90 days. Secondary outcomes were NIHSS score at 24 hours, NIHSS score at 5 to 7 days, and recanalization grade at 24 hours on CT angiography or MRI. The primary safety outcomes were sICH and death within 90 days.
An independent, unblinded data and safety monitoring board (DSMB) assessed the risk for the primary safety outcomes throughout the trial. The board performed interim analyses of safety and efficacy for every 300 patients.
After the fourth safety assessment, the DSMB recommended that enrollment in the moderate-dose heparin arm be discontinued for safety reasons. Enrollment in other arms continued.
After the second interim analysis, the DSMB advised that the trial steering committee be unblinded to decide whether to stop or continue the trial. The steering committee decided to stop the trial for reasons of safety.
Increased risk for sICH
In all, 628 patients were included in the study. The ASA groups included 310 patients, and the no-ASA groups included 318 patients. In all, 332 participants received heparin, and 296 received no heparin.
The demographic characteristics were well balanced between groups. The population’s median age was 73 years, and about 53% were men. The median baseline NIHSS score was approximately 15. About 74% of patients received IV thrombolysis. The median baseline Alberta Stroke Program Early CT Scan score was 9.
The investigators observed a slight shift toward worse outcome in the ASA group, compared with the no-ASA group (adjusted OR, 0.91). In addition, the ASA group had a significantly increased risk for sICH, compared with the no-ASA group (14% vs. 7.2%; aOR, 1.95).
Patients in the ASA group were less likely to have good functional outcome (mRS of 0 to 2; aOR, 0.76), and the mortality rate tended to be higher.
The researchers found a nonsignificant shift toward a worse functional outcome in the heparin group, compared with the no-heparin group (aOR, 0.81). The risk for sICH was significantly higher in the heparin group, compared with the no-heparin group (13% vs. 7.4%; aOR, 2.00).
Patients in the heparin group were also less likely to have a good functional outcome (aOR, 0.78), and there was a nonsignificant increase in risk for death among those patients.
The rate of sICH was 11% in the group that received low-dose heparin; it was 26% in the group that received moderate-dose heparin (aOR, 6.05). The mortality rate was 23% in the low-dose group and 47% in the moderate-dose group (aOR, 5.45).
There was no significant interaction between ASA and heparin on the primary outcome and on sICH occurrence.
‘A unique trial’
“MR CLEAN-MED is a unique trial because it investigated a widely used treatment but until now without any proof of effectiveness,” said Dr. van der Steen. The researchers expect that their findings will have a strong impact on the management of patients with acute ischemic stroke. They suggest that the administration of antithrombotic agents during EVT be avoided.
“We consider it probable that the increased risk of sICH explains at least a part of the nonsignificant shift towards a worse functional outcome,” co-investigator Bob Roozenbeek, MD, PhD, a neurologist at the Erasmus Medical Center, said in an interview. “However, to make more definite statements, we will have to do more in-depth analyses.”
It remains unclear whether the periprocedural use of lower dosages of antithrombotic agents or of a single bolus of heparin could be safe and effective, said Dr. van der Steen.
To gain insight into these questions, the investigators will evaluate the effect of the medications and dosages examined in this trial on primary hemostasis and coagulation activity in the trial population. They also plan to examine the effect of primary hemostasis and coagulation activity on risk for sICH and functional outcome.
Enhancing the effectiveness of thrombectomy for acute ischemic stroke continues to be an important goal for stroke therapy, said Mark Fisher, MD, professor of neurology and pathology and laboratory medicine at the University of California, Irvine, who commented on the findings for this news organization.
At least three strategies are available: The use of ancillary antithrombotic medications, neuroprotection, and modulation of the vasoconstrictive properties of the microcirculation.
“Results of MR CLEAN-MED argue against the antithrombotic strategy,” said Dr. Fisher. “The alternate strategies remain viable, and results of interventions using those approaches are awaited with great interest.”
The study was funded by the CONTRAST consortium, which is supported by the Netherlands Cardiovascular Research Initiative and the Brain Foundation Netherlands. Funding also was provided by Stryker, Medtronic, and Cerenovus. Dr. van der Steen and Dr. Fisher have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Treatment with acetylsalicylic acid (ASA) or heparin is associated with an increased risk for symptomatic intracranial hemorrhage (sICH) in patients with ischemic stroke who are undergoing endovascular therapy (EVT), new data show.
In this population, ASA and heparin are each associated with an approximately doubled risk for sICH when administered during EVT.
“We did not find any evidence for a beneficial effect on functional outcome,” investigator Wouter van der Steen, MD, research physician and PhD student at Erasmus University Medical Center, Rotterdam, the Netherlands, told this news organization. The possibility that a positive effect would be observed if the trial were continued was considered negligible, he added.
The researchers stopped the trial for safety reasons and recommend avoiding the evaluated dosages of both medications during EVT for ischemic stroke, said Dr. van der Steen.
He presented the findings from the MR CLEAN-MED trial at the European Stroke Organisation Conference (ESOC) 2021, which was held online.
Trial stopped for safety
Previous research has supported the safety and efficacy of EVT for ischemic stroke. Still, more than 30% of patients do not recover, despite fast and complete recanalization. Incomplete microvascular reperfusion (IMR) could explain this incomplete recovery, the researchers note.
Microthrombi, which occlude distal vessels, and neutrophil extracellular traps can cause IMR. This problem can be reduced through treatment with ASA, which has an antithrombotic effect, or with heparin, which dissolves neutrophil extracellular traps, they add. Although these drugs are associated with good clinical outcomes, they entail an increased risk for sICH.
The investigators conducted the multicenter, randomized controlled MR CLEAN-MED trial to evaluate the effect of intravenous (IV) ASA and heparin, alone or in combination, during EVT for acute ischemic stroke. Treatment was open label, but outcome assessment was blinded. Eligible participants were adults with a National Institutes of Health Stroke Scale (NIHSS) score of greater than or equal to 2 and an anterior circulation large-vessel occlusion for whom EVT could be initiated in fewer than 6 hours.
Investigators randomly assigned patients to receive or not to receive ASA. Within each of these two treatment groups, patients were randomly assigned to receive no heparin, low-dose heparin, or moderate-dose heparin.
ASA was given in a loading dose of 300 mg. Patients who were given low-dose heparin received a loading dose of 5,000 IU followed by 500 IU/h for 6 hours. Patients who received moderate-dose heparin were given a loading dose of 5,000 IU followed by 1,250 IU/h for 6 hours.
The study’s primary outcome was Modified Rankin Scale (mRS) score at 90 days. Secondary outcomes were NIHSS score at 24 hours, NIHSS score at 5 to 7 days, and recanalization grade at 24 hours on CT angiography or MRI. The primary safety outcomes were sICH and death within 90 days.
An independent, unblinded data and safety monitoring board (DSMB) assessed the risk for the primary safety outcomes throughout the trial. The board performed interim analyses of safety and efficacy for every 300 patients.
After the fourth safety assessment, the DSMB recommended that enrollment in the moderate-dose heparin arm be discontinued for safety reasons. Enrollment in other arms continued.
After the second interim analysis, the DSMB advised that the trial steering committee be unblinded to decide whether to stop or continue the trial. The steering committee decided to stop the trial for reasons of safety.
Increased risk for sICH
In all, 628 patients were included in the study. The ASA groups included 310 patients, and the no-ASA groups included 318 patients. In all, 332 participants received heparin, and 296 received no heparin.
The demographic characteristics were well balanced between groups. The population’s median age was 73 years, and about 53% were men. The median baseline NIHSS score was approximately 15. About 74% of patients received IV thrombolysis. The median baseline Alberta Stroke Program Early CT Scan score was 9.
The investigators observed a slight shift toward worse outcome in the ASA group, compared with the no-ASA group (adjusted OR, 0.91). In addition, the ASA group had a significantly increased risk for sICH, compared with the no-ASA group (14% vs. 7.2%; aOR, 1.95).
Patients in the ASA group were less likely to have good functional outcome (mRS of 0 to 2; aOR, 0.76), and the mortality rate tended to be higher.
The researchers found a nonsignificant shift toward a worse functional outcome in the heparin group, compared with the no-heparin group (aOR, 0.81). The risk for sICH was significantly higher in the heparin group, compared with the no-heparin group (13% vs. 7.4%; aOR, 2.00).
Patients in the heparin group were also less likely to have a good functional outcome (aOR, 0.78), and there was a nonsignificant increase in risk for death among those patients.
The rate of sICH was 11% in the group that received low-dose heparin; it was 26% in the group that received moderate-dose heparin (aOR, 6.05). The mortality rate was 23% in the low-dose group and 47% in the moderate-dose group (aOR, 5.45).
There was no significant interaction between ASA and heparin on the primary outcome and on sICH occurrence.
‘A unique trial’
“MR CLEAN-MED is a unique trial because it investigated a widely used treatment but until now without any proof of effectiveness,” said Dr. van der Steen. The researchers expect that their findings will have a strong impact on the management of patients with acute ischemic stroke. They suggest that the administration of antithrombotic agents during EVT be avoided.
“We consider it probable that the increased risk of sICH explains at least a part of the nonsignificant shift towards a worse functional outcome,” co-investigator Bob Roozenbeek, MD, PhD, a neurologist at the Erasmus Medical Center, said in an interview. “However, to make more definite statements, we will have to do more in-depth analyses.”
It remains unclear whether the periprocedural use of lower dosages of antithrombotic agents or of a single bolus of heparin could be safe and effective, said Dr. van der Steen.
To gain insight into these questions, the investigators will evaluate the effect of the medications and dosages examined in this trial on primary hemostasis and coagulation activity in the trial population. They also plan to examine the effect of primary hemostasis and coagulation activity on risk for sICH and functional outcome.
Enhancing the effectiveness of thrombectomy for acute ischemic stroke continues to be an important goal for stroke therapy, said Mark Fisher, MD, professor of neurology and pathology and laboratory medicine at the University of California, Irvine, who commented on the findings for this news organization.
At least three strategies are available: The use of ancillary antithrombotic medications, neuroprotection, and modulation of the vasoconstrictive properties of the microcirculation.
“Results of MR CLEAN-MED argue against the antithrombotic strategy,” said Dr. Fisher. “The alternate strategies remain viable, and results of interventions using those approaches are awaited with great interest.”
The study was funded by the CONTRAST consortium, which is supported by the Netherlands Cardiovascular Research Initiative and the Brain Foundation Netherlands. Funding also was provided by Stryker, Medtronic, and Cerenovus. Dr. van der Steen and Dr. Fisher have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Treatment with acetylsalicylic acid (ASA) or heparin is associated with an increased risk for symptomatic intracranial hemorrhage (sICH) in patients with ischemic stroke who are undergoing endovascular therapy (EVT), new data show.
In this population, ASA and heparin are each associated with an approximately doubled risk for sICH when administered during EVT.
“We did not find any evidence for a beneficial effect on functional outcome,” investigator Wouter van der Steen, MD, research physician and PhD student at Erasmus University Medical Center, Rotterdam, the Netherlands, told this news organization. The possibility that a positive effect would be observed if the trial were continued was considered negligible, he added.
The researchers stopped the trial for safety reasons and recommend avoiding the evaluated dosages of both medications during EVT for ischemic stroke, said Dr. van der Steen.
He presented the findings from the MR CLEAN-MED trial at the European Stroke Organisation Conference (ESOC) 2021, which was held online.
Trial stopped for safety
Previous research has supported the safety and efficacy of EVT for ischemic stroke. Still, more than 30% of patients do not recover, despite fast and complete recanalization. Incomplete microvascular reperfusion (IMR) could explain this incomplete recovery, the researchers note.
Microthrombi, which occlude distal vessels, and neutrophil extracellular traps can cause IMR. This problem can be reduced through treatment with ASA, which has an antithrombotic effect, or with heparin, which dissolves neutrophil extracellular traps, they add. Although these drugs are associated with good clinical outcomes, they entail an increased risk for sICH.
The investigators conducted the multicenter, randomized controlled MR CLEAN-MED trial to evaluate the effect of intravenous (IV) ASA and heparin, alone or in combination, during EVT for acute ischemic stroke. Treatment was open label, but outcome assessment was blinded. Eligible participants were adults with a National Institutes of Health Stroke Scale (NIHSS) score of greater than or equal to 2 and an anterior circulation large-vessel occlusion for whom EVT could be initiated in fewer than 6 hours.
Investigators randomly assigned patients to receive or not to receive ASA. Within each of these two treatment groups, patients were randomly assigned to receive no heparin, low-dose heparin, or moderate-dose heparin.
ASA was given in a loading dose of 300 mg. Patients who were given low-dose heparin received a loading dose of 5,000 IU followed by 500 IU/h for 6 hours. Patients who received moderate-dose heparin were given a loading dose of 5,000 IU followed by 1,250 IU/h for 6 hours.
The study’s primary outcome was Modified Rankin Scale (mRS) score at 90 days. Secondary outcomes were NIHSS score at 24 hours, NIHSS score at 5 to 7 days, and recanalization grade at 24 hours on CT angiography or MRI. The primary safety outcomes were sICH and death within 90 days.
An independent, unblinded data and safety monitoring board (DSMB) assessed the risk for the primary safety outcomes throughout the trial. The board performed interim analyses of safety and efficacy for every 300 patients.
After the fourth safety assessment, the DSMB recommended that enrollment in the moderate-dose heparin arm be discontinued for safety reasons. Enrollment in other arms continued.
After the second interim analysis, the DSMB advised that the trial steering committee be unblinded to decide whether to stop or continue the trial. The steering committee decided to stop the trial for reasons of safety.
Increased risk for sICH
In all, 628 patients were included in the study. The ASA groups included 310 patients, and the no-ASA groups included 318 patients. In all, 332 participants received heparin, and 296 received no heparin.
The demographic characteristics were well balanced between groups. The population’s median age was 73 years, and about 53% were men. The median baseline NIHSS score was approximately 15. About 74% of patients received IV thrombolysis. The median baseline Alberta Stroke Program Early CT Scan score was 9.
The investigators observed a slight shift toward worse outcome in the ASA group, compared with the no-ASA group (adjusted OR, 0.91). In addition, the ASA group had a significantly increased risk for sICH, compared with the no-ASA group (14% vs. 7.2%; aOR, 1.95).
Patients in the ASA group were less likely to have good functional outcome (mRS of 0 to 2; aOR, 0.76), and the mortality rate tended to be higher.
The researchers found a nonsignificant shift toward a worse functional outcome in the heparin group, compared with the no-heparin group (aOR, 0.81). The risk for sICH was significantly higher in the heparin group, compared with the no-heparin group (13% vs. 7.4%; aOR, 2.00).
Patients in the heparin group were also less likely to have a good functional outcome (aOR, 0.78), and there was a nonsignificant increase in risk for death among those patients.
The rate of sICH was 11% in the group that received low-dose heparin; it was 26% in the group that received moderate-dose heparin (aOR, 6.05). The mortality rate was 23% in the low-dose group and 47% in the moderate-dose group (aOR, 5.45).
There was no significant interaction between ASA and heparin on the primary outcome and on sICH occurrence.
‘A unique trial’
“MR CLEAN-MED is a unique trial because it investigated a widely used treatment but until now without any proof of effectiveness,” said Dr. van der Steen. The researchers expect that their findings will have a strong impact on the management of patients with acute ischemic stroke. They suggest that the administration of antithrombotic agents during EVT be avoided.
“We consider it probable that the increased risk of sICH explains at least a part of the nonsignificant shift towards a worse functional outcome,” co-investigator Bob Roozenbeek, MD, PhD, a neurologist at the Erasmus Medical Center, said in an interview. “However, to make more definite statements, we will have to do more in-depth analyses.”
It remains unclear whether the periprocedural use of lower dosages of antithrombotic agents or of a single bolus of heparin could be safe and effective, said Dr. van der Steen.
To gain insight into these questions, the investigators will evaluate the effect of the medications and dosages examined in this trial on primary hemostasis and coagulation activity in the trial population. They also plan to examine the effect of primary hemostasis and coagulation activity on risk for sICH and functional outcome.
Enhancing the effectiveness of thrombectomy for acute ischemic stroke continues to be an important goal for stroke therapy, said Mark Fisher, MD, professor of neurology and pathology and laboratory medicine at the University of California, Irvine, who commented on the findings for this news organization.
At least three strategies are available: The use of ancillary antithrombotic medications, neuroprotection, and modulation of the vasoconstrictive properties of the microcirculation.
“Results of MR CLEAN-MED argue against the antithrombotic strategy,” said Dr. Fisher. “The alternate strategies remain viable, and results of interventions using those approaches are awaited with great interest.”
The study was funded by the CONTRAST consortium, which is supported by the Netherlands Cardiovascular Research Initiative and the Brain Foundation Netherlands. Funding also was provided by Stryker, Medtronic, and Cerenovus. Dr. van der Steen and Dr. Fisher have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
ADHD a new risk factor for Alzheimer’s?
results from a large, multigenerational study show.
“The findings suggest there are common genetic and/or environmental contributions to the association between ADHD and dementia,” study investigator Zheng Chang, PhD, from the department of medical epidemiology and biostatistics at Karolinska Institute, Stockholm, said in a statement.
“There have been few studies previously on the link between ADHD and dementia, all with limited sample size,” Dr. Chang said in an interview.
“This is the first study to look at ADHD and dementia within extended families. It’s a large population-based study including over 2 million individuals and their over 5 million biological relatives,” he noted.
The study was published online Sept. 9, 2021, in the journal Alzheimer’s & Dementia.
Shared familial risk
The researchers identified roughly 2.1 million people born in Sweden between 1980 and 2001. Overall, 3.2% of the cohort had a diagnosis of ADHD.
Using national registries, they linked these individuals to more than 5 million of their biological relatives including parents, grandparents, uncles, and aunts and determined which of these relatives developed dementia over time.
In adjusted analyses, parents of individuals with ADHD had 34% higher risk for any dementia than parents of those without ADHD (hazard ratio, 1.34; 95% CI, 1.11-1.63).
The risk for AD, the most common type of dementia, was 55% higher in parents of individuals with ADHD (HR, 1.55; 95% CI, 1.26-1.89).
Individuals with ADHD were more likely to have parents with early-onset dementia rather than late-onset dementia. However, the absolute risk for dementia was low for the parent cohort: Only 0.17% of the parents were diagnosed with dementia during follow-up.
The association between ADHD and dementia was not as strong for second-degree relatives of individuals with ADHD. For example, grandparents of individuals with ADHD had a 10% increased risk for dementia, compared with grandparents of individuals without ADHD.
The finding of attenuated associations with decreasing genetic relatedness (parents > grandparents and uncles/aunts), points to shared familial risk between ADHD and AD, the researchers said.
There could be “undiscovered genetic variants that contribute to either traits or family-wide environmental risk factors, such as socioeconomic status, that may have an impact on the association,” Dr. Chang said in the news release.
“There are no direct clinical implications from this study, but research like this could lead to further research with goals for improved detection, prevention, and treatment,” he said in an interview.
More questions than answers
Heather Snyder, PhD, vice president of medical and scientific relations for the Alzheimer’s Association that the way different brain diseases are linked “is a question the Alzheimer’s Association is often asked, and it is a part of our funding portfolio to get that question answered.”
This study looking at ADHD and dementia is “intriguing,” Dr. Snyder said, “because, right now, there is limited information available. That said, this is an association study; it shows that two things are somehow connected. Because of how the study was conducted, it does not – and cannot – prove causation,” Dr. Snyder said. “But it is interesting all the same. More research is needed to uncover specifically why and how these two diseases are related. That might eventually give us insight into how to manage risk or even improve treatment.”
The study was supported by grants from the Swedish Council for Health, Working Life and Welfare, the Swedish Research Council, the Swedish Brain Foundation, the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie, the Fredrik & Ingrid Thurings Stiftelse, and the Karolinska Institutet Research Foundation. Dr. Chang and Dr. Snyder disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
results from a large, multigenerational study show.
“The findings suggest there are common genetic and/or environmental contributions to the association between ADHD and dementia,” study investigator Zheng Chang, PhD, from the department of medical epidemiology and biostatistics at Karolinska Institute, Stockholm, said in a statement.
“There have been few studies previously on the link between ADHD and dementia, all with limited sample size,” Dr. Chang said in an interview.
“This is the first study to look at ADHD and dementia within extended families. It’s a large population-based study including over 2 million individuals and their over 5 million biological relatives,” he noted.
The study was published online Sept. 9, 2021, in the journal Alzheimer’s & Dementia.
Shared familial risk
The researchers identified roughly 2.1 million people born in Sweden between 1980 and 2001. Overall, 3.2% of the cohort had a diagnosis of ADHD.
Using national registries, they linked these individuals to more than 5 million of their biological relatives including parents, grandparents, uncles, and aunts and determined which of these relatives developed dementia over time.
In adjusted analyses, parents of individuals with ADHD had 34% higher risk for any dementia than parents of those without ADHD (hazard ratio, 1.34; 95% CI, 1.11-1.63).
The risk for AD, the most common type of dementia, was 55% higher in parents of individuals with ADHD (HR, 1.55; 95% CI, 1.26-1.89).
Individuals with ADHD were more likely to have parents with early-onset dementia rather than late-onset dementia. However, the absolute risk for dementia was low for the parent cohort: Only 0.17% of the parents were diagnosed with dementia during follow-up.
The association between ADHD and dementia was not as strong for second-degree relatives of individuals with ADHD. For example, grandparents of individuals with ADHD had a 10% increased risk for dementia, compared with grandparents of individuals without ADHD.
The finding of attenuated associations with decreasing genetic relatedness (parents > grandparents and uncles/aunts), points to shared familial risk between ADHD and AD, the researchers said.
There could be “undiscovered genetic variants that contribute to either traits or family-wide environmental risk factors, such as socioeconomic status, that may have an impact on the association,” Dr. Chang said in the news release.
“There are no direct clinical implications from this study, but research like this could lead to further research with goals for improved detection, prevention, and treatment,” he said in an interview.
More questions than answers
Heather Snyder, PhD, vice president of medical and scientific relations for the Alzheimer’s Association that the way different brain diseases are linked “is a question the Alzheimer’s Association is often asked, and it is a part of our funding portfolio to get that question answered.”
This study looking at ADHD and dementia is “intriguing,” Dr. Snyder said, “because, right now, there is limited information available. That said, this is an association study; it shows that two things are somehow connected. Because of how the study was conducted, it does not – and cannot – prove causation,” Dr. Snyder said. “But it is interesting all the same. More research is needed to uncover specifically why and how these two diseases are related. That might eventually give us insight into how to manage risk or even improve treatment.”
The study was supported by grants from the Swedish Council for Health, Working Life and Welfare, the Swedish Research Council, the Swedish Brain Foundation, the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie, the Fredrik & Ingrid Thurings Stiftelse, and the Karolinska Institutet Research Foundation. Dr. Chang and Dr. Snyder disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
results from a large, multigenerational study show.
“The findings suggest there are common genetic and/or environmental contributions to the association between ADHD and dementia,” study investigator Zheng Chang, PhD, from the department of medical epidemiology and biostatistics at Karolinska Institute, Stockholm, said in a statement.
“There have been few studies previously on the link between ADHD and dementia, all with limited sample size,” Dr. Chang said in an interview.
“This is the first study to look at ADHD and dementia within extended families. It’s a large population-based study including over 2 million individuals and their over 5 million biological relatives,” he noted.
The study was published online Sept. 9, 2021, in the journal Alzheimer’s & Dementia.
Shared familial risk
The researchers identified roughly 2.1 million people born in Sweden between 1980 and 2001. Overall, 3.2% of the cohort had a diagnosis of ADHD.
Using national registries, they linked these individuals to more than 5 million of their biological relatives including parents, grandparents, uncles, and aunts and determined which of these relatives developed dementia over time.
In adjusted analyses, parents of individuals with ADHD had 34% higher risk for any dementia than parents of those without ADHD (hazard ratio, 1.34; 95% CI, 1.11-1.63).
The risk for AD, the most common type of dementia, was 55% higher in parents of individuals with ADHD (HR, 1.55; 95% CI, 1.26-1.89).
Individuals with ADHD were more likely to have parents with early-onset dementia rather than late-onset dementia. However, the absolute risk for dementia was low for the parent cohort: Only 0.17% of the parents were diagnosed with dementia during follow-up.
The association between ADHD and dementia was not as strong for second-degree relatives of individuals with ADHD. For example, grandparents of individuals with ADHD had a 10% increased risk for dementia, compared with grandparents of individuals without ADHD.
The finding of attenuated associations with decreasing genetic relatedness (parents > grandparents and uncles/aunts), points to shared familial risk between ADHD and AD, the researchers said.
There could be “undiscovered genetic variants that contribute to either traits or family-wide environmental risk factors, such as socioeconomic status, that may have an impact on the association,” Dr. Chang said in the news release.
“There are no direct clinical implications from this study, but research like this could lead to further research with goals for improved detection, prevention, and treatment,” he said in an interview.
More questions than answers
Heather Snyder, PhD, vice president of medical and scientific relations for the Alzheimer’s Association that the way different brain diseases are linked “is a question the Alzheimer’s Association is often asked, and it is a part of our funding portfolio to get that question answered.”
This study looking at ADHD and dementia is “intriguing,” Dr. Snyder said, “because, right now, there is limited information available. That said, this is an association study; it shows that two things are somehow connected. Because of how the study was conducted, it does not – and cannot – prove causation,” Dr. Snyder said. “But it is interesting all the same. More research is needed to uncover specifically why and how these two diseases are related. That might eventually give us insight into how to manage risk or even improve treatment.”
The study was supported by grants from the Swedish Council for Health, Working Life and Welfare, the Swedish Research Council, the Swedish Brain Foundation, the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie, the Fredrik & Ingrid Thurings Stiftelse, and the Karolinska Institutet Research Foundation. Dr. Chang and Dr. Snyder disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
78-year-old man • tail bone pain • unintended weight loss • history of diabetes and hypertension • Dx?
THE CASE
A 78-year-old man with a history of diabetes and hypertension was referred to the outpatient surgical office with a chief complaint of “tail bone pain” that had started after a fall a year earlier. The patient complained that the pain was worse when sitting and at nighttime. He also admitted to a 7-lb weight loss over the past 2 months without change in diet or appetite. He denied symptoms of incontinence, urinary retention, sharp stabbing pains in the lower extremities, night sweats, or anorexia.
The patient first visited an urgent care facility on the day after the fall because he was experiencing pain in his “tail bone” region while riding his lawn mower. A pelvic x-ray was performed at that time and showed no coccyx fracture. He received a steroid injection in the right sacroiliac joint, which provided some relief for a month. Throughout the course of the year, he was given 6 steroid injections into his sacroiliac joint by his primary care provider (PCP) and clinicians at his local urgent care facility. One year after the fall, the patient’s PCP ordered a computed tomography (CT) scan of the abdomen and pelvis, which revealed a 4.6 x 7.5–cm soft-tissue mass with bony destruction of the lower sacrum and coccyx that extended into the sacral and coccygeal canal (FIGURE 1).
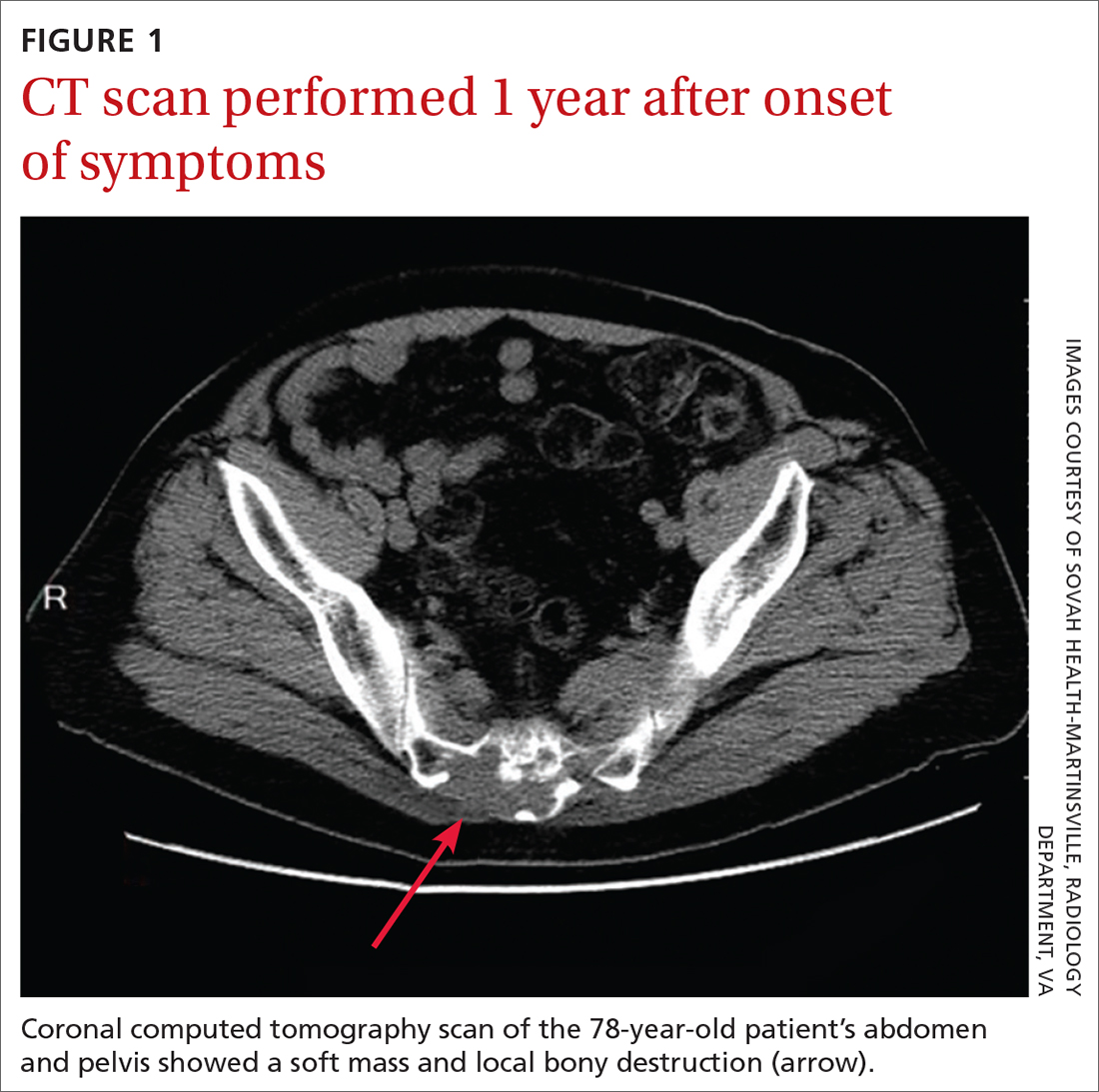
On exam in our surgical office, the patient was found to be alert and oriented. His neurologic exam was unremarkable, with an intact motor and sensory exam and no symptoms of cauda equina syndrome. During palpation over the lower sacrum and coccyx, both tenderness and a boggy, soft mass were observed. Nerve impingement was most likely caused by the size of the mass.
THE DIAGNOSIS
Biopsy revealed a large tan-gray, gelatinous, soft-tissue mass that was necrotizing through the lower sacrum. The diagnosis of a sacral chordoma was confirmed with magnetic resonance imaging of the pelvis, which demonstrated a 4.6 × 8.1–cm destructive expansile sacrococcygeal tumor with an exophytic soft-tissue component (FIGURE 2). The tumor also involved the piriformis and gluteus maximus muscles bilaterally.
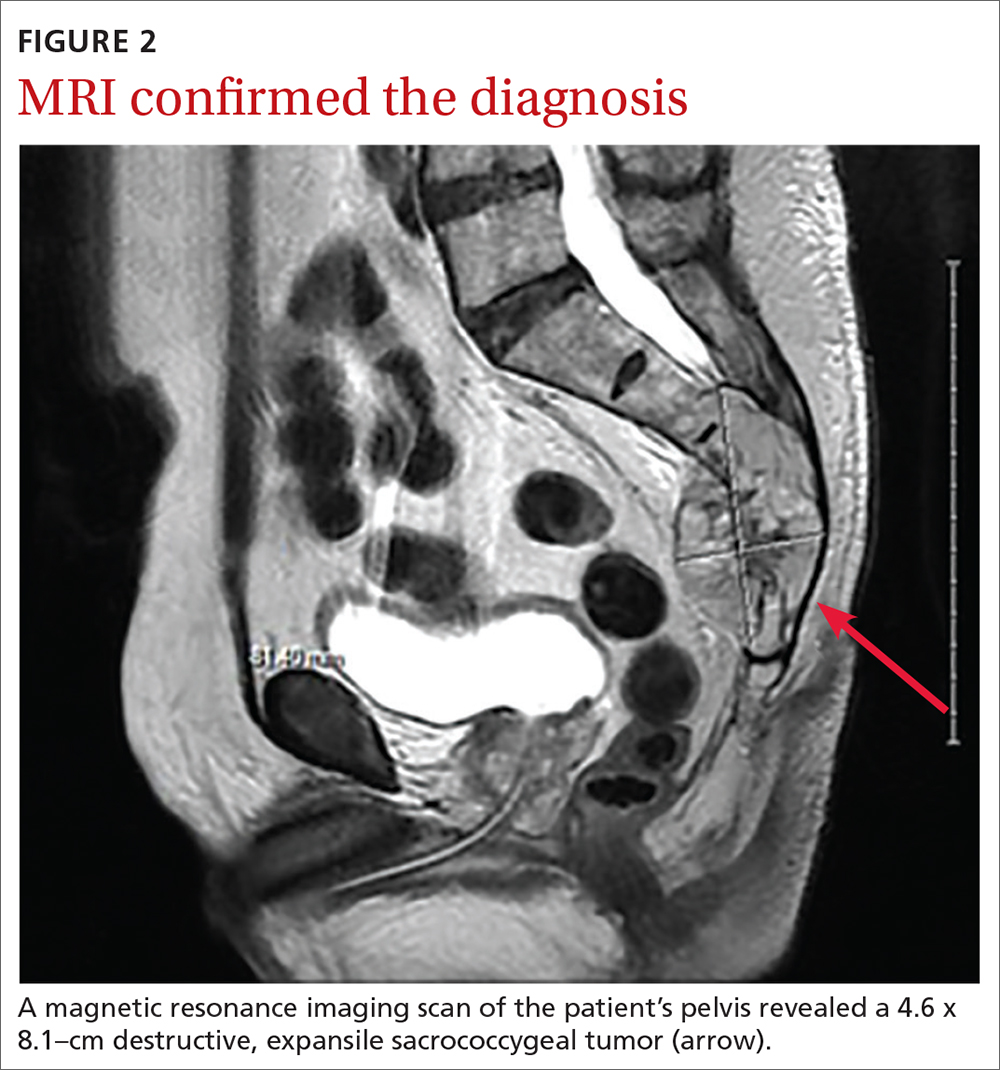
DISCUSSION
Chordomas are rare, malignant bone tumors that grow slowly and originate from embryonic remnants of the notochord.1 They are most commonly seen in the sacrococcygeal segment (50%) but are also seen in the spheno-occipital synchondrosis (30%-35%) and other spinal segments such as C2 and lumbar spine.2 Chordomas are typically seen in middle-aged patients, with sacral chordomas occurring predominantly in men compared to women (3:1).2
Slow to grow, slow to diagnose
The difficulty with diagnosing sacral chordomas lies in the tendency for these tumors to grow extremely slowly, making detection challenging due to a lack of symptoms in the early clinical course. Once the tumors cause noticeable symptoms, they are usually large and extensively locally invasive. As a result, most patients experience delayed diagnosis, with an average symptom duration of 2.3 years prior to diagnosis.3
Reexamining a common problem as a symptom of a rare condition
The most commonly manifesting symptom of sacral chordomas is lower back pain that is typically dull and worse with sitting.3,4 Since lower back pain is the leading cause of disability, it is difficult to determine when back pain is simply a benign consequence of aging or muscular pain and when it is, in fact, pathologic.5 A thorough history and physical are crucial in making the distinction.
Continue to: Clinical red flags...
Clinical red flags include pain with neurologic symptoms (including paresthesia, urinary or bowel disturbances, and weakness in the lower limbs), pain in the lower back with or without coccyx pain that persists and gradually worsens over time, and pain that fails to resolve.3 These symptoms are collectively strong indicators of underlying sacral pathology and should warrant further investigation, including a CT and MRI of the involved area.
Survival rate is improved by surgery
The gold standard for treatment of sacral chordomas is surgical resection with adequate margins, as these tumors are both radio- and chemo-insensitive.6 It is generally accepted that achieving a wide surgical margin is the most important predictor of survival and of reducing local recurrence in patients with sacrococcygeal chordoma.7-9
The survival rate varies after a posterior-only surgical approach; some studies cite the 5-year survival rate as 100% and others state the 7-year survival rate as 5%.4 The wide variation is likely due to small trial size, a lack of evidence, and how invasive the disease is at the time of surgery.
The recurrence rate 5 years after surgery is approximately 20%.4 The rate of urinary and fecal incontinence after surgery using a posterior-only approach is between 20% and 100%; some of this variation may be due to which spinal level is involved.4 If S3 is affected, there is almost always perineal anesthesia along with bowel and bladder incontinence.4
This patient was referred to Neurosurgery and underwent resection. He recovered well from surgery but suffered from some residual urinary incontinence. The patient did not receive chemotherapy or radiation, and further work-up revealed no evidence of metastasis.
Continue to: THE TAKEAWAY
THE TAKEAWAY
The diagnosis of sacral chordoma remains challenging. A history of clinical red flags, especially persistent lower back pain with neuropathy, should prompt an aggressive investigation to rule out underlying pathology. Other signs on physical exam could include urinary or bowel disturbances, weakness in the lower limbs, saddle anesthesia, new foot drop, and/or laxity of the anal sphincter.5 Early detection and surgical intervention are crucial for these patients to experience a better prognosis and preserve maximum function.
CORRESPONDENCE
Ginger Poulton, MD, 123 Hendersonville Road, Asheville, NC 28803; ginger.poulton@mahec.net
1. Zabel-du Bois A, Nikoghosyan A, Schwahofer A, et al. Intensity modulated radiotherapy in the management of sacral chordoma in primary versus recurrent disease. Radiother Oncol. 2010;97:408-412. doi: 10.1016/j.radonc.2010.10.008
2. Murphey MD, Andrews CL, Flemming DJ, et al. Primary tumors of the spine: radiologic pathologic correlation. Radiographics. 1996;1131-1158. doi: 10.1148/radiographics.16.5.8888395
3. Jeys L, Gibbins R, Evans G, et al. Sacral chordoma: a diagnosis not to be sat on? Int Orthopaedics. 2008;32:269-272. doi: 10.1007/s00264-006-0296-3
4. Pillai S, Govender, S. Sacral chordoma: a review of literature. J Orthop. 2018;15:679-684. doi: 10.1016/j.jor.2018.04.001
5. Traeger A, Buchbinder R, Harris I, et al. Diagnosis and management of low-back pain in primary care. CMAJ. 2017;189:E1386-E1395. doi: 10.1503/cmaj.170527
6. Walcott BP, Nahed BV, Mohyeldin A, et al. Chordoma: current concepts, management, and future directions. Lancet Oncol. 2012;13:e69-76. doi: 10.1016/S1470-2045(11)70337-0
7. Bergh P, Kindblom LG, Gunterberg B, et al. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer. 2000;88:2122-2134. doi: 10.1002/(sici)1097-0142(20000501)88:9<2122::aid-cncr19>3.0.co;2-1
8. Boriani S, Bandiera S, Biagini R, et al. Chordoma of the mobile spine: fifty years of experience. Spine. 2006;31:493-503. doi: 10.1097/01.brs.0000200038.30869.27
9. Hanna SA, Aston WJ, Briggs TW, et al. Sacral chordoma: can local recurrence after sacrectomy be predicted? Clin Orthop Relat Res. 2008;466:2217-2223. doi: 10.1007/s11999-008-0356-7
THE CASE
A 78-year-old man with a history of diabetes and hypertension was referred to the outpatient surgical office with a chief complaint of “tail bone pain” that had started after a fall a year earlier. The patient complained that the pain was worse when sitting and at nighttime. He also admitted to a 7-lb weight loss over the past 2 months without change in diet or appetite. He denied symptoms of incontinence, urinary retention, sharp stabbing pains in the lower extremities, night sweats, or anorexia.
The patient first visited an urgent care facility on the day after the fall because he was experiencing pain in his “tail bone” region while riding his lawn mower. A pelvic x-ray was performed at that time and showed no coccyx fracture. He received a steroid injection in the right sacroiliac joint, which provided some relief for a month. Throughout the course of the year, he was given 6 steroid injections into his sacroiliac joint by his primary care provider (PCP) and clinicians at his local urgent care facility. One year after the fall, the patient’s PCP ordered a computed tomography (CT) scan of the abdomen and pelvis, which revealed a 4.6 x 7.5–cm soft-tissue mass with bony destruction of the lower sacrum and coccyx that extended into the sacral and coccygeal canal (FIGURE 1).
On exam in our surgical office, the patient was found to be alert and oriented. His neurologic exam was unremarkable, with an intact motor and sensory exam and no symptoms of cauda equina syndrome. During palpation over the lower sacrum and coccyx, both tenderness and a boggy, soft mass were observed. Nerve impingement was most likely caused by the size of the mass.
THE DIAGNOSIS
Biopsy revealed a large tan-gray, gelatinous, soft-tissue mass that was necrotizing through the lower sacrum. The diagnosis of a sacral chordoma was confirmed with magnetic resonance imaging of the pelvis, which demonstrated a 4.6 × 8.1–cm destructive expansile sacrococcygeal tumor with an exophytic soft-tissue component (FIGURE 2). The tumor also involved the piriformis and gluteus maximus muscles bilaterally.
DISCUSSION
Chordomas are rare, malignant bone tumors that grow slowly and originate from embryonic remnants of the notochord.1 They are most commonly seen in the sacrococcygeal segment (50%) but are also seen in the spheno-occipital synchondrosis (30%-35%) and other spinal segments such as C2 and lumbar spine.2 Chordomas are typically seen in middle-aged patients, with sacral chordomas occurring predominantly in men compared to women (3:1).2
Slow to grow, slow to diagnose
The difficulty with diagnosing sacral chordomas lies in the tendency for these tumors to grow extremely slowly, making detection challenging due to a lack of symptoms in the early clinical course. Once the tumors cause noticeable symptoms, they are usually large and extensively locally invasive. As a result, most patients experience delayed diagnosis, with an average symptom duration of 2.3 years prior to diagnosis.3
Reexamining a common problem as a symptom of a rare condition
The most commonly manifesting symptom of sacral chordomas is lower back pain that is typically dull and worse with sitting.3,4 Since lower back pain is the leading cause of disability, it is difficult to determine when back pain is simply a benign consequence of aging or muscular pain and when it is, in fact, pathologic.5 A thorough history and physical are crucial in making the distinction.
Continue to: Clinical red flags...
Clinical red flags include pain with neurologic symptoms (including paresthesia, urinary or bowel disturbances, and weakness in the lower limbs), pain in the lower back with or without coccyx pain that persists and gradually worsens over time, and pain that fails to resolve.3 These symptoms are collectively strong indicators of underlying sacral pathology and should warrant further investigation, including a CT and MRI of the involved area.
Survival rate is improved by surgery
The gold standard for treatment of sacral chordomas is surgical resection with adequate margins, as these tumors are both radio- and chemo-insensitive.6 It is generally accepted that achieving a wide surgical margin is the most important predictor of survival and of reducing local recurrence in patients with sacrococcygeal chordoma.7-9
The survival rate varies after a posterior-only surgical approach; some studies cite the 5-year survival rate as 100% and others state the 7-year survival rate as 5%.4 The wide variation is likely due to small trial size, a lack of evidence, and how invasive the disease is at the time of surgery.
The recurrence rate 5 years after surgery is approximately 20%.4 The rate of urinary and fecal incontinence after surgery using a posterior-only approach is between 20% and 100%; some of this variation may be due to which spinal level is involved.4 If S3 is affected, there is almost always perineal anesthesia along with bowel and bladder incontinence.4
This patient was referred to Neurosurgery and underwent resection. He recovered well from surgery but suffered from some residual urinary incontinence. The patient did not receive chemotherapy or radiation, and further work-up revealed no evidence of metastasis.
Continue to: THE TAKEAWAY
THE TAKEAWAY
The diagnosis of sacral chordoma remains challenging. A history of clinical red flags, especially persistent lower back pain with neuropathy, should prompt an aggressive investigation to rule out underlying pathology. Other signs on physical exam could include urinary or bowel disturbances, weakness in the lower limbs, saddle anesthesia, new foot drop, and/or laxity of the anal sphincter.5 Early detection and surgical intervention are crucial for these patients to experience a better prognosis and preserve maximum function.
CORRESPONDENCE
Ginger Poulton, MD, 123 Hendersonville Road, Asheville, NC 28803; ginger.poulton@mahec.net
THE CASE
A 78-year-old man with a history of diabetes and hypertension was referred to the outpatient surgical office with a chief complaint of “tail bone pain” that had started after a fall a year earlier. The patient complained that the pain was worse when sitting and at nighttime. He also admitted to a 7-lb weight loss over the past 2 months without change in diet or appetite. He denied symptoms of incontinence, urinary retention, sharp stabbing pains in the lower extremities, night sweats, or anorexia.
The patient first visited an urgent care facility on the day after the fall because he was experiencing pain in his “tail bone” region while riding his lawn mower. A pelvic x-ray was performed at that time and showed no coccyx fracture. He received a steroid injection in the right sacroiliac joint, which provided some relief for a month. Throughout the course of the year, he was given 6 steroid injections into his sacroiliac joint by his primary care provider (PCP) and clinicians at his local urgent care facility. One year after the fall, the patient’s PCP ordered a computed tomography (CT) scan of the abdomen and pelvis, which revealed a 4.6 x 7.5–cm soft-tissue mass with bony destruction of the lower sacrum and coccyx that extended into the sacral and coccygeal canal (FIGURE 1).
On exam in our surgical office, the patient was found to be alert and oriented. His neurologic exam was unremarkable, with an intact motor and sensory exam and no symptoms of cauda equina syndrome. During palpation over the lower sacrum and coccyx, both tenderness and a boggy, soft mass were observed. Nerve impingement was most likely caused by the size of the mass.
THE DIAGNOSIS
Biopsy revealed a large tan-gray, gelatinous, soft-tissue mass that was necrotizing through the lower sacrum. The diagnosis of a sacral chordoma was confirmed with magnetic resonance imaging of the pelvis, which demonstrated a 4.6 × 8.1–cm destructive expansile sacrococcygeal tumor with an exophytic soft-tissue component (FIGURE 2). The tumor also involved the piriformis and gluteus maximus muscles bilaterally.
DISCUSSION
Chordomas are rare, malignant bone tumors that grow slowly and originate from embryonic remnants of the notochord.1 They are most commonly seen in the sacrococcygeal segment (50%) but are also seen in the spheno-occipital synchondrosis (30%-35%) and other spinal segments such as C2 and lumbar spine.2 Chordomas are typically seen in middle-aged patients, with sacral chordomas occurring predominantly in men compared to women (3:1).2
Slow to grow, slow to diagnose
The difficulty with diagnosing sacral chordomas lies in the tendency for these tumors to grow extremely slowly, making detection challenging due to a lack of symptoms in the early clinical course. Once the tumors cause noticeable symptoms, they are usually large and extensively locally invasive. As a result, most patients experience delayed diagnosis, with an average symptom duration of 2.3 years prior to diagnosis.3
Reexamining a common problem as a symptom of a rare condition
The most commonly manifesting symptom of sacral chordomas is lower back pain that is typically dull and worse with sitting.3,4 Since lower back pain is the leading cause of disability, it is difficult to determine when back pain is simply a benign consequence of aging or muscular pain and when it is, in fact, pathologic.5 A thorough history and physical are crucial in making the distinction.
Continue to: Clinical red flags...
Clinical red flags include pain with neurologic symptoms (including paresthesia, urinary or bowel disturbances, and weakness in the lower limbs), pain in the lower back with or without coccyx pain that persists and gradually worsens over time, and pain that fails to resolve.3 These symptoms are collectively strong indicators of underlying sacral pathology and should warrant further investigation, including a CT and MRI of the involved area.
Survival rate is improved by surgery
The gold standard for treatment of sacral chordomas is surgical resection with adequate margins, as these tumors are both radio- and chemo-insensitive.6 It is generally accepted that achieving a wide surgical margin is the most important predictor of survival and of reducing local recurrence in patients with sacrococcygeal chordoma.7-9
The survival rate varies after a posterior-only surgical approach; some studies cite the 5-year survival rate as 100% and others state the 7-year survival rate as 5%.4 The wide variation is likely due to small trial size, a lack of evidence, and how invasive the disease is at the time of surgery.
The recurrence rate 5 years after surgery is approximately 20%.4 The rate of urinary and fecal incontinence after surgery using a posterior-only approach is between 20% and 100%; some of this variation may be due to which spinal level is involved.4 If S3 is affected, there is almost always perineal anesthesia along with bowel and bladder incontinence.4
This patient was referred to Neurosurgery and underwent resection. He recovered well from surgery but suffered from some residual urinary incontinence. The patient did not receive chemotherapy or radiation, and further work-up revealed no evidence of metastasis.
Continue to: THE TAKEAWAY
THE TAKEAWAY
The diagnosis of sacral chordoma remains challenging. A history of clinical red flags, especially persistent lower back pain with neuropathy, should prompt an aggressive investigation to rule out underlying pathology. Other signs on physical exam could include urinary or bowel disturbances, weakness in the lower limbs, saddle anesthesia, new foot drop, and/or laxity of the anal sphincter.5 Early detection and surgical intervention are crucial for these patients to experience a better prognosis and preserve maximum function.
CORRESPONDENCE
Ginger Poulton, MD, 123 Hendersonville Road, Asheville, NC 28803; ginger.poulton@mahec.net
1. Zabel-du Bois A, Nikoghosyan A, Schwahofer A, et al. Intensity modulated radiotherapy in the management of sacral chordoma in primary versus recurrent disease. Radiother Oncol. 2010;97:408-412. doi: 10.1016/j.radonc.2010.10.008
2. Murphey MD, Andrews CL, Flemming DJ, et al. Primary tumors of the spine: radiologic pathologic correlation. Radiographics. 1996;1131-1158. doi: 10.1148/radiographics.16.5.8888395
3. Jeys L, Gibbins R, Evans G, et al. Sacral chordoma: a diagnosis not to be sat on? Int Orthopaedics. 2008;32:269-272. doi: 10.1007/s00264-006-0296-3
4. Pillai S, Govender, S. Sacral chordoma: a review of literature. J Orthop. 2018;15:679-684. doi: 10.1016/j.jor.2018.04.001
5. Traeger A, Buchbinder R, Harris I, et al. Diagnosis and management of low-back pain in primary care. CMAJ. 2017;189:E1386-E1395. doi: 10.1503/cmaj.170527
6. Walcott BP, Nahed BV, Mohyeldin A, et al. Chordoma: current concepts, management, and future directions. Lancet Oncol. 2012;13:e69-76. doi: 10.1016/S1470-2045(11)70337-0
7. Bergh P, Kindblom LG, Gunterberg B, et al. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer. 2000;88:2122-2134. doi: 10.1002/(sici)1097-0142(20000501)88:9<2122::aid-cncr19>3.0.co;2-1
8. Boriani S, Bandiera S, Biagini R, et al. Chordoma of the mobile spine: fifty years of experience. Spine. 2006;31:493-503. doi: 10.1097/01.brs.0000200038.30869.27
9. Hanna SA, Aston WJ, Briggs TW, et al. Sacral chordoma: can local recurrence after sacrectomy be predicted? Clin Orthop Relat Res. 2008;466:2217-2223. doi: 10.1007/s11999-008-0356-7
1. Zabel-du Bois A, Nikoghosyan A, Schwahofer A, et al. Intensity modulated radiotherapy in the management of sacral chordoma in primary versus recurrent disease. Radiother Oncol. 2010;97:408-412. doi: 10.1016/j.radonc.2010.10.008
2. Murphey MD, Andrews CL, Flemming DJ, et al. Primary tumors of the spine: radiologic pathologic correlation. Radiographics. 1996;1131-1158. doi: 10.1148/radiographics.16.5.8888395
3. Jeys L, Gibbins R, Evans G, et al. Sacral chordoma: a diagnosis not to be sat on? Int Orthopaedics. 2008;32:269-272. doi: 10.1007/s00264-006-0296-3
4. Pillai S, Govender, S. Sacral chordoma: a review of literature. J Orthop. 2018;15:679-684. doi: 10.1016/j.jor.2018.04.001
5. Traeger A, Buchbinder R, Harris I, et al. Diagnosis and management of low-back pain in primary care. CMAJ. 2017;189:E1386-E1395. doi: 10.1503/cmaj.170527
6. Walcott BP, Nahed BV, Mohyeldin A, et al. Chordoma: current concepts, management, and future directions. Lancet Oncol. 2012;13:e69-76. doi: 10.1016/S1470-2045(11)70337-0
7. Bergh P, Kindblom LG, Gunterberg B, et al. Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer. 2000;88:2122-2134. doi: 10.1002/(sici)1097-0142(20000501)88:9<2122::aid-cncr19>3.0.co;2-1
8. Boriani S, Bandiera S, Biagini R, et al. Chordoma of the mobile spine: fifty years of experience. Spine. 2006;31:493-503. doi: 10.1097/01.brs.0000200038.30869.27
9. Hanna SA, Aston WJ, Briggs TW, et al. Sacral chordoma: can local recurrence after sacrectomy be predicted? Clin Orthop Relat Res. 2008;466:2217-2223. doi: 10.1007/s11999-008-0356-7

Seizure a first sign of COVID in kids?
Unlike in adults, seizures, including status epilepticus (SE), may be the first and main manifestation of COVID-19 in children, new research suggests.
Seizures may occur even in children with no history of epilepsy and in the absence of fever or severe COVID-19 illness, necessitating a “high index” of suspicion for the virus to make an early diagnosis and allow for appropriate infection control measures, say the researchers.
“We hope to increase physicians’ awareness of noninfluenza-like presentations of COVID in children. In areas with a high prevalence of COVID, we suggest that children with seizures be tested for COVID,” Tal Gilboa, MD, director of the child neurology unit and codirector of epilepsy, Hadassah Medical Center, Jerusalem, told this news organization.
The study was published online August 27 in the journal Seizure.
Presenting symptom
Among 175 children diagnosed with acute SARS-CoV-2 infection in the emergency department over 10 months in 2020, 11 (6%) presented with seizures. Studies in adults with COVID-19 have reported seizures in 0% to 2% of cases, the investigators note.
The 11 children with seizures (seven boys) ranged in age from 6 months to 17 years (median age, 11.5 years). All of them had seizures as the presenting sign of infection and none had severe COVID-19 requiring ventilatory or hemodynamic support. Six of the 11 children presented with fever.
Seven of the children had a prior history of neurological disorder: Five had epilepsy, one had a single unprovoked seizure 3 years before admission, and one had an intellectual disability. Three of the children had uncontrolled seizures despite appropriate treatment with antiseizure medication.
Nine of the 11 children presented with generalized tonic-clonic seizures. One child with a prior history of uncontrolled epilepsy with multiple seizure types had a focal tonic seizure. The youngest patient, a 5-month-old infant, presented with bilateral asymmetrical tonic-clonic seizure.
Of note, say the investigators, five of the 11 children presented with convulsive SE; none had a history of prior SE, and one had no history of seizures.
Although young age, especially under 12 months, is a known risk factor for SE, four of the five patients with SE were between 5 and 17 years old. All five children with SE responded to treatment with antiseizure medications.
All 11 children made a full recovery while in hospital, although further follow-up is essential to determine long-term outcomes, the researchers report.
“Children with no prior history of epilepsy and those with well-controlled epilepsy who present with breakthrough seizures, regardless of their body temperature, should be considered as potentially infected by SARS-CoV-2,” said Dr. Gilboa.
“It is possible, however unlikely, that a child, especially with prior epilepsy, may have an unprovoked seizure while being asymptomatically infected by SARS-CoV-2; in any case, infection control measures should be taken,” Dr. Gilboa added.
Need for replication
Weighing in on the study, Carl E. Stafstrom, MD, PhD, professor of neurology and pediatrics, Johns Hopkins University, Baltimore, said it’s important to note that “about half of the children had had epilepsy already, and for whatever reason, had a seizure, which required an ED visit, and then they found COVID.”
“Nevertheless, this article is interesting and surprising in what they found because nobody else has found nearly as frequent a seizure presentation,” said Dr. Stafstrom, director of the John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medicine.
“We would want to see some replication from other institutions and other populations,” he added.
The study had no specific funding. Dr. Gilboa and Dr. Stafstrom have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unlike in adults, seizures, including status epilepticus (SE), may be the first and main manifestation of COVID-19 in children, new research suggests.
Seizures may occur even in children with no history of epilepsy and in the absence of fever or severe COVID-19 illness, necessitating a “high index” of suspicion for the virus to make an early diagnosis and allow for appropriate infection control measures, say the researchers.
“We hope to increase physicians’ awareness of noninfluenza-like presentations of COVID in children. In areas with a high prevalence of COVID, we suggest that children with seizures be tested for COVID,” Tal Gilboa, MD, director of the child neurology unit and codirector of epilepsy, Hadassah Medical Center, Jerusalem, told this news organization.
The study was published online August 27 in the journal Seizure.
Presenting symptom
Among 175 children diagnosed with acute SARS-CoV-2 infection in the emergency department over 10 months in 2020, 11 (6%) presented with seizures. Studies in adults with COVID-19 have reported seizures in 0% to 2% of cases, the investigators note.
The 11 children with seizures (seven boys) ranged in age from 6 months to 17 years (median age, 11.5 years). All of them had seizures as the presenting sign of infection and none had severe COVID-19 requiring ventilatory or hemodynamic support. Six of the 11 children presented with fever.
Seven of the children had a prior history of neurological disorder: Five had epilepsy, one had a single unprovoked seizure 3 years before admission, and one had an intellectual disability. Three of the children had uncontrolled seizures despite appropriate treatment with antiseizure medication.
Nine of the 11 children presented with generalized tonic-clonic seizures. One child with a prior history of uncontrolled epilepsy with multiple seizure types had a focal tonic seizure. The youngest patient, a 5-month-old infant, presented with bilateral asymmetrical tonic-clonic seizure.
Of note, say the investigators, five of the 11 children presented with convulsive SE; none had a history of prior SE, and one had no history of seizures.
Although young age, especially under 12 months, is a known risk factor for SE, four of the five patients with SE were between 5 and 17 years old. All five children with SE responded to treatment with antiseizure medications.
All 11 children made a full recovery while in hospital, although further follow-up is essential to determine long-term outcomes, the researchers report.
“Children with no prior history of epilepsy and those with well-controlled epilepsy who present with breakthrough seizures, regardless of their body temperature, should be considered as potentially infected by SARS-CoV-2,” said Dr. Gilboa.
“It is possible, however unlikely, that a child, especially with prior epilepsy, may have an unprovoked seizure while being asymptomatically infected by SARS-CoV-2; in any case, infection control measures should be taken,” Dr. Gilboa added.
Need for replication
Weighing in on the study, Carl E. Stafstrom, MD, PhD, professor of neurology and pediatrics, Johns Hopkins University, Baltimore, said it’s important to note that “about half of the children had had epilepsy already, and for whatever reason, had a seizure, which required an ED visit, and then they found COVID.”
“Nevertheless, this article is interesting and surprising in what they found because nobody else has found nearly as frequent a seizure presentation,” said Dr. Stafstrom, director of the John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medicine.
“We would want to see some replication from other institutions and other populations,” he added.
The study had no specific funding. Dr. Gilboa and Dr. Stafstrom have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unlike in adults, seizures, including status epilepticus (SE), may be the first and main manifestation of COVID-19 in children, new research suggests.
Seizures may occur even in children with no history of epilepsy and in the absence of fever or severe COVID-19 illness, necessitating a “high index” of suspicion for the virus to make an early diagnosis and allow for appropriate infection control measures, say the researchers.
“We hope to increase physicians’ awareness of noninfluenza-like presentations of COVID in children. In areas with a high prevalence of COVID, we suggest that children with seizures be tested for COVID,” Tal Gilboa, MD, director of the child neurology unit and codirector of epilepsy, Hadassah Medical Center, Jerusalem, told this news organization.
The study was published online August 27 in the journal Seizure.
Presenting symptom
Among 175 children diagnosed with acute SARS-CoV-2 infection in the emergency department over 10 months in 2020, 11 (6%) presented with seizures. Studies in adults with COVID-19 have reported seizures in 0% to 2% of cases, the investigators note.
The 11 children with seizures (seven boys) ranged in age from 6 months to 17 years (median age, 11.5 years). All of them had seizures as the presenting sign of infection and none had severe COVID-19 requiring ventilatory or hemodynamic support. Six of the 11 children presented with fever.
Seven of the children had a prior history of neurological disorder: Five had epilepsy, one had a single unprovoked seizure 3 years before admission, and one had an intellectual disability. Three of the children had uncontrolled seizures despite appropriate treatment with antiseizure medication.
Nine of the 11 children presented with generalized tonic-clonic seizures. One child with a prior history of uncontrolled epilepsy with multiple seizure types had a focal tonic seizure. The youngest patient, a 5-month-old infant, presented with bilateral asymmetrical tonic-clonic seizure.
Of note, say the investigators, five of the 11 children presented with convulsive SE; none had a history of prior SE, and one had no history of seizures.
Although young age, especially under 12 months, is a known risk factor for SE, four of the five patients with SE were between 5 and 17 years old. All five children with SE responded to treatment with antiseizure medications.
All 11 children made a full recovery while in hospital, although further follow-up is essential to determine long-term outcomes, the researchers report.
“Children with no prior history of epilepsy and those with well-controlled epilepsy who present with breakthrough seizures, regardless of their body temperature, should be considered as potentially infected by SARS-CoV-2,” said Dr. Gilboa.
“It is possible, however unlikely, that a child, especially with prior epilepsy, may have an unprovoked seizure while being asymptomatically infected by SARS-CoV-2; in any case, infection control measures should be taken,” Dr. Gilboa added.
Need for replication
Weighing in on the study, Carl E. Stafstrom, MD, PhD, professor of neurology and pediatrics, Johns Hopkins University, Baltimore, said it’s important to note that “about half of the children had had epilepsy already, and for whatever reason, had a seizure, which required an ED visit, and then they found COVID.”
“Nevertheless, this article is interesting and surprising in what they found because nobody else has found nearly as frequent a seizure presentation,” said Dr. Stafstrom, director of the John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medicine.
“We would want to see some replication from other institutions and other populations,” he added.
The study had no specific funding. Dr. Gilboa and Dr. Stafstrom have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Data supporting cannabis for childhood epilepsy remain scarce
, according to two leading experts.
In a recent invited review article, Martin Kirkpatrick, MD, of the University of Dundee (Scotland), and Finbar O’Callaghan, MD, PhD, of University College London suggested that childhood epilepsy may be easy terrain for commercial interests to break ground, and from there, build their presence.
“Children with epilepsy are at risk of being used as the ‘Trojan horse’ for the cannabis industry,” Dr. Kirkpatrick and Dr. O’Callaghan wrote in Developmental Medicine & Child Neurology.
They noted that some of the first publicized success stories involving cannabis oil for epilepsy coincided with the rise of the medicinal and recreational cannabis markets, which will constitute an estimated 55-billion-dollar industry by 2027.
“Pediatric neurologists, imbued with the need to practice evidence-based medicine and wary of prescribing unlicensed medicines that had inadequate safety data, suddenly found themselves at odds with an array of vested interests and, most unfortunately, with the families of patients who were keen to try anything that would alleviate the effects of their child’s seizures,” the investigators wrote.
According to the review, fundamental questions about cannabis remain unanswered, including concerns about safety with long-term use, and the medicinal value of various plant components, such as myrcene, a terpene that gives cannabis its characteristic smell.
“A widely discussed issue is whether the terpenes add any therapeutic benefit, contributing to the so-called entourage effect of ‘whole-plant’ medicines,” the investigators wrote. “The concept is that all the constituents of the plant together create ‘the sum of all the parts that leads to the magic or power of cannabis.’ Although commonly referred to, there is little or no robust evidence to support the entourage effect as a credible clinical concept.”
Clinical evidence for treatment of pediatric epilepsy is also lacking, according to Dr. Kirkpatrick and Dr. O’Callaghan.
“Unfortunately, apart from the studies of pure cannabidiol (CBD) in Lennox–Gastaut and Dravet syndromes and tuberous sclerosis complex, level I evidence in the field of CBMPs and refractory epilepsy is lacking,” they wrote.
While other experts have pointed out that lower-level evidence – such as patient-reported outcomes and observational data – have previously been sufficient for drug licensing, Dr. Kirkpatrick and Dr. O’Callaghan noted that such exceptions “almost always” involve conditions without any effective treatments, or drugs that are undeniably effective.
“This is not the scenario with CBMPs,” they wrote, referring to current clinical data as “low-level” evidence “suggesting … possible efficacy.”
They highlighted concerns about placebo effect with open-label epilepsy studies, citing a randomized controlled trial for Dravet syndrome, in which 27% of patients given placebo had a 50% reduction in seizure frequency.
“We need carefully designed, good-quality CBMP studies that produce results on which we can rely,” Dr. Kirkpatrick and Dr. O’Callaghan concluded. “We can then work with families to choose the best treatments for children and young people with epilepsy. We owe this to them.”
A therapy of last resort
Jerzy P. Szaflarski, MD, PhD, of the University of Alabama at Birmingham, agreed that data are lacking for the use of CBMPs with patients who have epilepsy and other neurologic conditions; however, he also suggested that Dr. Kirkpatrick and Dr. O’Callaghan did not provide adequate real-world clinical context.
“Medical cannabis is not used as a first-, second-, or third-line therapy,” Dr. Szaflarski said. “It’s mostly used as a last resort in the sense that patients have already failed multiple other therapies.” In that respect, patients and parents are desperate to try anything that might work. “We have medical cannabis, and our patients want to try it, and at the point when multiple therapies have failed, it’s a reasonable option.”
While Dr. Szaflarski agreed that more high-quality clinical trials are needed, he also noted the practical challenges involved in such trials, largely because of variations in cannabis plants.
“The content of the cannabis plant changes depending on the day that it’s collected and the exposure to sun and how much water it has and what’s in the soil and many other things,” Dr. Szaflarski said. “It’s hard to get a very good, standardized product, and that’s why there needs to be a good-quality product delivered by the industry, which I have not seen thus far.”
For this reason, Dr. Szaflarski steers parents and patients away from over-the-counter CBMPs and toward Epidiolex, the only FDA-approved form of CBD.
“There is evidence that Epidiolex works,” he said. “I don’t know whether the products that are sold in a local cannabis store have the same high purity as Epidiolex. I tell [parents] that we should try Epidiolex first because it’s the one that is approved. But if it doesn’t work, we can go in that [other] direction.”
For those going the commercial route, Dr. Szaflarski advised close attention to product ingredients, to ensure that CBMPs are “devoid of any impurities, pesticides, fungicides, and other products that could be potentially dangerous.”
Parents considering CBMPs for their children also need to weigh concerns about long-term neurological safety, he added, noting that, on one hand, commercial products lack data, while on the other, epilepsy itself may cause harm.
“They need to consider the potential effects [of CBMPs] on their child’s brain and development versus … the effects of seizures on the brain,” Dr. Szaflarski said.
Dr. Kirkpatrick and Dr. O’Callaghan disclosed an application for a National Institute for Health Research–funded randomized controlled trial on CBMPs and joint authorship of British Paediatric Neurology Association Guidance on the use of CBMPs in children and young people with epilepsy. Dr. Szaflarski disclosed a relationship with Greenwich Biosciences and several other cannabis companies.
, according to two leading experts.
In a recent invited review article, Martin Kirkpatrick, MD, of the University of Dundee (Scotland), and Finbar O’Callaghan, MD, PhD, of University College London suggested that childhood epilepsy may be easy terrain for commercial interests to break ground, and from there, build their presence.
“Children with epilepsy are at risk of being used as the ‘Trojan horse’ for the cannabis industry,” Dr. Kirkpatrick and Dr. O’Callaghan wrote in Developmental Medicine & Child Neurology.
They noted that some of the first publicized success stories involving cannabis oil for epilepsy coincided with the rise of the medicinal and recreational cannabis markets, which will constitute an estimated 55-billion-dollar industry by 2027.
“Pediatric neurologists, imbued with the need to practice evidence-based medicine and wary of prescribing unlicensed medicines that had inadequate safety data, suddenly found themselves at odds with an array of vested interests and, most unfortunately, with the families of patients who were keen to try anything that would alleviate the effects of their child’s seizures,” the investigators wrote.
According to the review, fundamental questions about cannabis remain unanswered, including concerns about safety with long-term use, and the medicinal value of various plant components, such as myrcene, a terpene that gives cannabis its characteristic smell.
“A widely discussed issue is whether the terpenes add any therapeutic benefit, contributing to the so-called entourage effect of ‘whole-plant’ medicines,” the investigators wrote. “The concept is that all the constituents of the plant together create ‘the sum of all the parts that leads to the magic or power of cannabis.’ Although commonly referred to, there is little or no robust evidence to support the entourage effect as a credible clinical concept.”
Clinical evidence for treatment of pediatric epilepsy is also lacking, according to Dr. Kirkpatrick and Dr. O’Callaghan.
“Unfortunately, apart from the studies of pure cannabidiol (CBD) in Lennox–Gastaut and Dravet syndromes and tuberous sclerosis complex, level I evidence in the field of CBMPs and refractory epilepsy is lacking,” they wrote.
While other experts have pointed out that lower-level evidence – such as patient-reported outcomes and observational data – have previously been sufficient for drug licensing, Dr. Kirkpatrick and Dr. O’Callaghan noted that such exceptions “almost always” involve conditions without any effective treatments, or drugs that are undeniably effective.
“This is not the scenario with CBMPs,” they wrote, referring to current clinical data as “low-level” evidence “suggesting … possible efficacy.”
They highlighted concerns about placebo effect with open-label epilepsy studies, citing a randomized controlled trial for Dravet syndrome, in which 27% of patients given placebo had a 50% reduction in seizure frequency.
“We need carefully designed, good-quality CBMP studies that produce results on which we can rely,” Dr. Kirkpatrick and Dr. O’Callaghan concluded. “We can then work with families to choose the best treatments for children and young people with epilepsy. We owe this to them.”
A therapy of last resort
Jerzy P. Szaflarski, MD, PhD, of the University of Alabama at Birmingham, agreed that data are lacking for the use of CBMPs with patients who have epilepsy and other neurologic conditions; however, he also suggested that Dr. Kirkpatrick and Dr. O’Callaghan did not provide adequate real-world clinical context.
“Medical cannabis is not used as a first-, second-, or third-line therapy,” Dr. Szaflarski said. “It’s mostly used as a last resort in the sense that patients have already failed multiple other therapies.” In that respect, patients and parents are desperate to try anything that might work. “We have medical cannabis, and our patients want to try it, and at the point when multiple therapies have failed, it’s a reasonable option.”
While Dr. Szaflarski agreed that more high-quality clinical trials are needed, he also noted the practical challenges involved in such trials, largely because of variations in cannabis plants.
“The content of the cannabis plant changes depending on the day that it’s collected and the exposure to sun and how much water it has and what’s in the soil and many other things,” Dr. Szaflarski said. “It’s hard to get a very good, standardized product, and that’s why there needs to be a good-quality product delivered by the industry, which I have not seen thus far.”
For this reason, Dr. Szaflarski steers parents and patients away from over-the-counter CBMPs and toward Epidiolex, the only FDA-approved form of CBD.
“There is evidence that Epidiolex works,” he said. “I don’t know whether the products that are sold in a local cannabis store have the same high purity as Epidiolex. I tell [parents] that we should try Epidiolex first because it’s the one that is approved. But if it doesn’t work, we can go in that [other] direction.”
For those going the commercial route, Dr. Szaflarski advised close attention to product ingredients, to ensure that CBMPs are “devoid of any impurities, pesticides, fungicides, and other products that could be potentially dangerous.”
Parents considering CBMPs for their children also need to weigh concerns about long-term neurological safety, he added, noting that, on one hand, commercial products lack data, while on the other, epilepsy itself may cause harm.
“They need to consider the potential effects [of CBMPs] on their child’s brain and development versus … the effects of seizures on the brain,” Dr. Szaflarski said.
Dr. Kirkpatrick and Dr. O’Callaghan disclosed an application for a National Institute for Health Research–funded randomized controlled trial on CBMPs and joint authorship of British Paediatric Neurology Association Guidance on the use of CBMPs in children and young people with epilepsy. Dr. Szaflarski disclosed a relationship with Greenwich Biosciences and several other cannabis companies.
, according to two leading experts.
In a recent invited review article, Martin Kirkpatrick, MD, of the University of Dundee (Scotland), and Finbar O’Callaghan, MD, PhD, of University College London suggested that childhood epilepsy may be easy terrain for commercial interests to break ground, and from there, build their presence.
“Children with epilepsy are at risk of being used as the ‘Trojan horse’ for the cannabis industry,” Dr. Kirkpatrick and Dr. O’Callaghan wrote in Developmental Medicine & Child Neurology.
They noted that some of the first publicized success stories involving cannabis oil for epilepsy coincided with the rise of the medicinal and recreational cannabis markets, which will constitute an estimated 55-billion-dollar industry by 2027.
“Pediatric neurologists, imbued with the need to practice evidence-based medicine and wary of prescribing unlicensed medicines that had inadequate safety data, suddenly found themselves at odds with an array of vested interests and, most unfortunately, with the families of patients who were keen to try anything that would alleviate the effects of their child’s seizures,” the investigators wrote.
According to the review, fundamental questions about cannabis remain unanswered, including concerns about safety with long-term use, and the medicinal value of various plant components, such as myrcene, a terpene that gives cannabis its characteristic smell.
“A widely discussed issue is whether the terpenes add any therapeutic benefit, contributing to the so-called entourage effect of ‘whole-plant’ medicines,” the investigators wrote. “The concept is that all the constituents of the plant together create ‘the sum of all the parts that leads to the magic or power of cannabis.’ Although commonly referred to, there is little or no robust evidence to support the entourage effect as a credible clinical concept.”
Clinical evidence for treatment of pediatric epilepsy is also lacking, according to Dr. Kirkpatrick and Dr. O’Callaghan.
“Unfortunately, apart from the studies of pure cannabidiol (CBD) in Lennox–Gastaut and Dravet syndromes and tuberous sclerosis complex, level I evidence in the field of CBMPs and refractory epilepsy is lacking,” they wrote.
While other experts have pointed out that lower-level evidence – such as patient-reported outcomes and observational data – have previously been sufficient for drug licensing, Dr. Kirkpatrick and Dr. O’Callaghan noted that such exceptions “almost always” involve conditions without any effective treatments, or drugs that are undeniably effective.
“This is not the scenario with CBMPs,” they wrote, referring to current clinical data as “low-level” evidence “suggesting … possible efficacy.”
They highlighted concerns about placebo effect with open-label epilepsy studies, citing a randomized controlled trial for Dravet syndrome, in which 27% of patients given placebo had a 50% reduction in seizure frequency.
“We need carefully designed, good-quality CBMP studies that produce results on which we can rely,” Dr. Kirkpatrick and Dr. O’Callaghan concluded. “We can then work with families to choose the best treatments for children and young people with epilepsy. We owe this to them.”
A therapy of last resort
Jerzy P. Szaflarski, MD, PhD, of the University of Alabama at Birmingham, agreed that data are lacking for the use of CBMPs with patients who have epilepsy and other neurologic conditions; however, he also suggested that Dr. Kirkpatrick and Dr. O’Callaghan did not provide adequate real-world clinical context.
“Medical cannabis is not used as a first-, second-, or third-line therapy,” Dr. Szaflarski said. “It’s mostly used as a last resort in the sense that patients have already failed multiple other therapies.” In that respect, patients and parents are desperate to try anything that might work. “We have medical cannabis, and our patients want to try it, and at the point when multiple therapies have failed, it’s a reasonable option.”
While Dr. Szaflarski agreed that more high-quality clinical trials are needed, he also noted the practical challenges involved in such trials, largely because of variations in cannabis plants.
“The content of the cannabis plant changes depending on the day that it’s collected and the exposure to sun and how much water it has and what’s in the soil and many other things,” Dr. Szaflarski said. “It’s hard to get a very good, standardized product, and that’s why there needs to be a good-quality product delivered by the industry, which I have not seen thus far.”
For this reason, Dr. Szaflarski steers parents and patients away from over-the-counter CBMPs and toward Epidiolex, the only FDA-approved form of CBD.
“There is evidence that Epidiolex works,” he said. “I don’t know whether the products that are sold in a local cannabis store have the same high purity as Epidiolex. I tell [parents] that we should try Epidiolex first because it’s the one that is approved. But if it doesn’t work, we can go in that [other] direction.”
For those going the commercial route, Dr. Szaflarski advised close attention to product ingredients, to ensure that CBMPs are “devoid of any impurities, pesticides, fungicides, and other products that could be potentially dangerous.”
Parents considering CBMPs for their children also need to weigh concerns about long-term neurological safety, he added, noting that, on one hand, commercial products lack data, while on the other, epilepsy itself may cause harm.
“They need to consider the potential effects [of CBMPs] on their child’s brain and development versus … the effects of seizures on the brain,” Dr. Szaflarski said.
Dr. Kirkpatrick and Dr. O’Callaghan disclosed an application for a National Institute for Health Research–funded randomized controlled trial on CBMPs and joint authorship of British Paediatric Neurology Association Guidance on the use of CBMPs in children and young people with epilepsy. Dr. Szaflarski disclosed a relationship with Greenwich Biosciences and several other cannabis companies.
FROM DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY
Growing proportion of cardiac arrests in U.S. considered opioid related
Observational data indicate that the number of hospitalizations for cardiac arrests linked to opioid use roughly doubled from 2012 to 2018.
“This was an observational study, so we cannot conclude that all of the arrests were caused by opioids, but the findings do suggest the opioid epidemic is a contributor to increasing rates,” Senada S. Malik, of the University of New England, Portland, Maine, reported at the virtual annual congress of the European Society of Cardiology.
The data were drawn from the Nationwide Inpatient Sample (NIS) from 2012 to 2018, the most recent period available. Cardiac arrests were considered opioid related if there was a secondary diagnosis of opioid disease. The rates of opioid-associated hospitalizations for these types of cardiac arrests climbed from about 800 per year in 2012 to 1,500 per year in 2018, a trend that was statistically significant (P < .05).
The profile of patients with an opioid-associated cardiac arrest was different from those without secondary diagnosis of opioid disease. This included a younger age and lower rates of comorbidities: heart failure (21.2% vs. 40.6%; P < .05), renal failure (14.3% vs. 30.2%; P < .05), diabetes (19.5% vs. 35.4%; P < .05), and hypertension (43.4% vs. 64.9%; P < .05).
Mortality from opioid-associated cardiac arrest is lower
These features might explain the lower rate of in-hospital mortality for opioid-associated cardiac arrests (56.7% vs. 61.2%), according to Ms. Malik, who performed this research in collaboration with Wilbert S. Aronow, MD, director of cardiology research, Westchester Medical Center, Valhalla, N.Y.
When compared to those without a history of opioid use on admission, those with opioid-associated cardiac arrest were more likely to be depressed (18.8% vs. 9.0%), to smoke (37.0% vs. 21.8%) and to abuse alcohol (16.9% vs. 7.1%), according to the NIS data.
While these findings are based on cardiac arrests brought to a hospital, some opioid-induced cardiac arrests never result in hospital admission, according to data included in a recently issued scientific statement from the American Heart Association.
Rate of opioid-associated cardiac arrests underestimated
In that statement, which was focused on opioid-associated out-of-hospital cardiac arrests (OA-OHCA), numerous studies were cited to support the conclusion that these events are common and underestimated. One problem is that opioid-induced cardiac arrests are not always accurately differentiated from cardiac arrests induced by use of other substances, such as barbiturates, cocaine, or alcohol.
For this and other reasons, the data are inconsistent. One study based on emergency medical service (EMS) response data concluded that 9% of all out-of-hospital cardiac arrests are opioid associated.
In another study using potentially more accurate autopsy data, 60% of the non–cardiac-associated cardiac arrests were found to occur in individuals with potentially lethal serum concentrations of opioids. As 40% of out-of-hospital cardiac arrests were considered non–cardiac related, this suggested that 15% of all out-of-hospital cardiac arrests are opioid related.
In the NIS data, the incident curves of opioid-related cardiac arrests appeared to be flattening in 2018, the last year of data collection, but there was no indication they were declining.
Patterns of opioid-induced cardiac arrests evolving
The patterns of opioid-induced cardiac arrest have changed and are likely to continue to change in response to the evolving opioid epidemic, according to the AHA scientific statement. The authors described three waves of opioid abuse. The first, which was related to the promotion of prescription opioids to treat chronic pain that ultimately led to high rates of opioid addiction, peaked in 2012 when rates of these prescriptions began to fall. At that time a second wave, attributed to patients switching to less expensive nonprescription heroin, was already underway. A third wave, attributed to growth in the use of synthetic opioids, such as fentanyl, began in 2013 and is ongoing, according to data cited in the AHA statement.
Recognizing the role of opioids in rising rates of cardiac arrest is important for promoting strategies of effective treatment and prevention, according to Cameron Dezfulian, MD, medical director of the adult congenital heart disease program at Texas Children’s Hospital, Houston. Dr. Dezfulian was vice chair and leader of the writing committee for the AHA scientific statement on OA-OHCA. He said there are plenty of data to support the need for greater attention to the role of opioids in cardiac arrest.
“The recent data affirms the trends many of us have observed without our emergency rooms and ICUs: a steady increase in the proportion of OA-OHCA, primarily in young and otherwise healthy individuals,” he said.
He calls not only for more awareness at the front lines of health are but also for a more comprehensive approach.
“Public health policies and community- and hospital-based interventions are needed to reduce the mortality due to OA-OHCA, which is distinct from the traditional cardiac etiology,” Dr. Dezfulian said.
In opioid-induced cardiac arrest, as in other types of cardiac arrest, prompt initiation of cardiopulmonary resuscitation is essential, but early administration of the opioid antagonist naloxone can also be lifesaving, according to treatment strategies outlined in the AHA scientific statement. The fact that OA-OHCA typically occur in patients with structurally and electrophysiologically normal hearts is emphasized in the AHA statement. So is the enormous public health toll of OA-OHCA.
Death due to opioid overdose, which includes cardiac arrests, is now the leading cause of mortality in the U.S. among individuals between the ages of 25 and 64 years, according to the statement.
Ms. Malik reports no potential conflicts of interest. Dr. Dezfulian reports a financial relationship with Mallinckrodt.
Observational data indicate that the number of hospitalizations for cardiac arrests linked to opioid use roughly doubled from 2012 to 2018.
“This was an observational study, so we cannot conclude that all of the arrests were caused by opioids, but the findings do suggest the opioid epidemic is a contributor to increasing rates,” Senada S. Malik, of the University of New England, Portland, Maine, reported at the virtual annual congress of the European Society of Cardiology.
The data were drawn from the Nationwide Inpatient Sample (NIS) from 2012 to 2018, the most recent period available. Cardiac arrests were considered opioid related if there was a secondary diagnosis of opioid disease. The rates of opioid-associated hospitalizations for these types of cardiac arrests climbed from about 800 per year in 2012 to 1,500 per year in 2018, a trend that was statistically significant (P < .05).
The profile of patients with an opioid-associated cardiac arrest was different from those without secondary diagnosis of opioid disease. This included a younger age and lower rates of comorbidities: heart failure (21.2% vs. 40.6%; P < .05), renal failure (14.3% vs. 30.2%; P < .05), diabetes (19.5% vs. 35.4%; P < .05), and hypertension (43.4% vs. 64.9%; P < .05).
Mortality from opioid-associated cardiac arrest is lower
These features might explain the lower rate of in-hospital mortality for opioid-associated cardiac arrests (56.7% vs. 61.2%), according to Ms. Malik, who performed this research in collaboration with Wilbert S. Aronow, MD, director of cardiology research, Westchester Medical Center, Valhalla, N.Y.
When compared to those without a history of opioid use on admission, those with opioid-associated cardiac arrest were more likely to be depressed (18.8% vs. 9.0%), to smoke (37.0% vs. 21.8%) and to abuse alcohol (16.9% vs. 7.1%), according to the NIS data.
While these findings are based on cardiac arrests brought to a hospital, some opioid-induced cardiac arrests never result in hospital admission, according to data included in a recently issued scientific statement from the American Heart Association.
Rate of opioid-associated cardiac arrests underestimated
In that statement, which was focused on opioid-associated out-of-hospital cardiac arrests (OA-OHCA), numerous studies were cited to support the conclusion that these events are common and underestimated. One problem is that opioid-induced cardiac arrests are not always accurately differentiated from cardiac arrests induced by use of other substances, such as barbiturates, cocaine, or alcohol.
For this and other reasons, the data are inconsistent. One study based on emergency medical service (EMS) response data concluded that 9% of all out-of-hospital cardiac arrests are opioid associated.
In another study using potentially more accurate autopsy data, 60% of the non–cardiac-associated cardiac arrests were found to occur in individuals with potentially lethal serum concentrations of opioids. As 40% of out-of-hospital cardiac arrests were considered non–cardiac related, this suggested that 15% of all out-of-hospital cardiac arrests are opioid related.
In the NIS data, the incident curves of opioid-related cardiac arrests appeared to be flattening in 2018, the last year of data collection, but there was no indication they were declining.
Patterns of opioid-induced cardiac arrests evolving
The patterns of opioid-induced cardiac arrest have changed and are likely to continue to change in response to the evolving opioid epidemic, according to the AHA scientific statement. The authors described three waves of opioid abuse. The first, which was related to the promotion of prescription opioids to treat chronic pain that ultimately led to high rates of opioid addiction, peaked in 2012 when rates of these prescriptions began to fall. At that time a second wave, attributed to patients switching to less expensive nonprescription heroin, was already underway. A third wave, attributed to growth in the use of synthetic opioids, such as fentanyl, began in 2013 and is ongoing, according to data cited in the AHA statement.
Recognizing the role of opioids in rising rates of cardiac arrest is important for promoting strategies of effective treatment and prevention, according to Cameron Dezfulian, MD, medical director of the adult congenital heart disease program at Texas Children’s Hospital, Houston. Dr. Dezfulian was vice chair and leader of the writing committee for the AHA scientific statement on OA-OHCA. He said there are plenty of data to support the need for greater attention to the role of opioids in cardiac arrest.
“The recent data affirms the trends many of us have observed without our emergency rooms and ICUs: a steady increase in the proportion of OA-OHCA, primarily in young and otherwise healthy individuals,” he said.
He calls not only for more awareness at the front lines of health are but also for a more comprehensive approach.
“Public health policies and community- and hospital-based interventions are needed to reduce the mortality due to OA-OHCA, which is distinct from the traditional cardiac etiology,” Dr. Dezfulian said.
In opioid-induced cardiac arrest, as in other types of cardiac arrest, prompt initiation of cardiopulmonary resuscitation is essential, but early administration of the opioid antagonist naloxone can also be lifesaving, according to treatment strategies outlined in the AHA scientific statement. The fact that OA-OHCA typically occur in patients with structurally and electrophysiologically normal hearts is emphasized in the AHA statement. So is the enormous public health toll of OA-OHCA.
Death due to opioid overdose, which includes cardiac arrests, is now the leading cause of mortality in the U.S. among individuals between the ages of 25 and 64 years, according to the statement.
Ms. Malik reports no potential conflicts of interest. Dr. Dezfulian reports a financial relationship with Mallinckrodt.
Observational data indicate that the number of hospitalizations for cardiac arrests linked to opioid use roughly doubled from 2012 to 2018.
“This was an observational study, so we cannot conclude that all of the arrests were caused by opioids, but the findings do suggest the opioid epidemic is a contributor to increasing rates,” Senada S. Malik, of the University of New England, Portland, Maine, reported at the virtual annual congress of the European Society of Cardiology.
The data were drawn from the Nationwide Inpatient Sample (NIS) from 2012 to 2018, the most recent period available. Cardiac arrests were considered opioid related if there was a secondary diagnosis of opioid disease. The rates of opioid-associated hospitalizations for these types of cardiac arrests climbed from about 800 per year in 2012 to 1,500 per year in 2018, a trend that was statistically significant (P < .05).
The profile of patients with an opioid-associated cardiac arrest was different from those without secondary diagnosis of opioid disease. This included a younger age and lower rates of comorbidities: heart failure (21.2% vs. 40.6%; P < .05), renal failure (14.3% vs. 30.2%; P < .05), diabetes (19.5% vs. 35.4%; P < .05), and hypertension (43.4% vs. 64.9%; P < .05).
Mortality from opioid-associated cardiac arrest is lower
These features might explain the lower rate of in-hospital mortality for opioid-associated cardiac arrests (56.7% vs. 61.2%), according to Ms. Malik, who performed this research in collaboration with Wilbert S. Aronow, MD, director of cardiology research, Westchester Medical Center, Valhalla, N.Y.
When compared to those without a history of opioid use on admission, those with opioid-associated cardiac arrest were more likely to be depressed (18.8% vs. 9.0%), to smoke (37.0% vs. 21.8%) and to abuse alcohol (16.9% vs. 7.1%), according to the NIS data.
While these findings are based on cardiac arrests brought to a hospital, some opioid-induced cardiac arrests never result in hospital admission, according to data included in a recently issued scientific statement from the American Heart Association.
Rate of opioid-associated cardiac arrests underestimated
In that statement, which was focused on opioid-associated out-of-hospital cardiac arrests (OA-OHCA), numerous studies were cited to support the conclusion that these events are common and underestimated. One problem is that opioid-induced cardiac arrests are not always accurately differentiated from cardiac arrests induced by use of other substances, such as barbiturates, cocaine, or alcohol.
For this and other reasons, the data are inconsistent. One study based on emergency medical service (EMS) response data concluded that 9% of all out-of-hospital cardiac arrests are opioid associated.
In another study using potentially more accurate autopsy data, 60% of the non–cardiac-associated cardiac arrests were found to occur in individuals with potentially lethal serum concentrations of opioids. As 40% of out-of-hospital cardiac arrests were considered non–cardiac related, this suggested that 15% of all out-of-hospital cardiac arrests are opioid related.
In the NIS data, the incident curves of opioid-related cardiac arrests appeared to be flattening in 2018, the last year of data collection, but there was no indication they were declining.
Patterns of opioid-induced cardiac arrests evolving
The patterns of opioid-induced cardiac arrest have changed and are likely to continue to change in response to the evolving opioid epidemic, according to the AHA scientific statement. The authors described three waves of opioid abuse. The first, which was related to the promotion of prescription opioids to treat chronic pain that ultimately led to high rates of opioid addiction, peaked in 2012 when rates of these prescriptions began to fall. At that time a second wave, attributed to patients switching to less expensive nonprescription heroin, was already underway. A third wave, attributed to growth in the use of synthetic opioids, such as fentanyl, began in 2013 and is ongoing, according to data cited in the AHA statement.
Recognizing the role of opioids in rising rates of cardiac arrest is important for promoting strategies of effective treatment and prevention, according to Cameron Dezfulian, MD, medical director of the adult congenital heart disease program at Texas Children’s Hospital, Houston. Dr. Dezfulian was vice chair and leader of the writing committee for the AHA scientific statement on OA-OHCA. He said there are plenty of data to support the need for greater attention to the role of opioids in cardiac arrest.
“The recent data affirms the trends many of us have observed without our emergency rooms and ICUs: a steady increase in the proportion of OA-OHCA, primarily in young and otherwise healthy individuals,” he said.
He calls not only for more awareness at the front lines of health are but also for a more comprehensive approach.
“Public health policies and community- and hospital-based interventions are needed to reduce the mortality due to OA-OHCA, which is distinct from the traditional cardiac etiology,” Dr. Dezfulian said.
In opioid-induced cardiac arrest, as in other types of cardiac arrest, prompt initiation of cardiopulmonary resuscitation is essential, but early administration of the opioid antagonist naloxone can also be lifesaving, according to treatment strategies outlined in the AHA scientific statement. The fact that OA-OHCA typically occur in patients with structurally and electrophysiologically normal hearts is emphasized in the AHA statement. So is the enormous public health toll of OA-OHCA.
Death due to opioid overdose, which includes cardiac arrests, is now the leading cause of mortality in the U.S. among individuals between the ages of 25 and 64 years, according to the statement.
Ms. Malik reports no potential conflicts of interest. Dr. Dezfulian reports a financial relationship with Mallinckrodt.
FROM ESC 2021
‘Lopioid protocol’ – low-dose opioids – proposed for fracture surgery
In a paper presented at the annual meeting of the American Academy of Orthopaedic Surgeons, researchers from NYU reported on the implementation of their multimodal strategy, dubbed the “lopioid protocol.”
According to the 2019 National Survey on Drug Use and Health, orthopedic surgeons are the third-highest opioid prescribers in the United States.
Kennneth A. Egol, MD, vice chair of the department of orthopedic surgery at NYU, who is the first author of the study, was motivated to help create the protocol following misconceptions that orthopedic surgeons were helping to fuel the opioid epidemic.
Dr. Egol pointed to the year 1995, when pain became the fifth vital sign after body temperature, pulse rate, respiratory rate, and blood pressure.
Since then, in light of the opioid epidemic, the focus of physicians has shifted away from prescribing strong pain medication and reducing pain scores to zero to instead reducing pain to a manageable level.
Reducing opioid prescriptions can be challenging when patients are prescribed an anti-inflammatory and they subsequently ask their physician for a “pain pill.” Patients sometimes don’t understand that inflammation is what causes pain.
It can also be difficult to convince patients that medications that they can buy over the counter can adequately control their pain, as confirmed in numerous studies.
Multimodal pain therapy aims to reduce the need for opioids by supplementing their use with other oral medications and, at times, long-lasting regional nerve blocks.
Anti-inflammatories act at the site of injury or surgery where inflammation is occurring. Nerves then carry the pain signal to the brain. These signals can be dampened by medications such as gabapentin that act on the nerves themselves. The pain signal is received in the brain, where opioids act by binding to receptors in the brain.
The so-called lopioid protocol does not eliminate opioids completely but rather uses “safer” opioids, such as tramadol, in lieu of stronger narcotics.
The protocol began at NYU on Jan. 1, 2019. It consists in the prescribing of tramadol, meloxicam, gabapentin, and acetaminophen.
The study presented at the AAOS meeting demonstrated statistically significant reductions in visual analogue pain scores at discharge and subsequent medication refills for the 931 patients in the lopioid group, compared with a group of 848 patients who received narcotic prescriptions containing oxycodone from the year prior to the protocol initiation.
Educating patients on the rationale for the prescription combination can help to allay their fears. Dr. Egol thinks it’s important for physicians to explain the dangers of opioids to patients. He said in an interview that he also believes surgeons need to “give [patients] an understanding of why we are pursuing these protocols. They also need to know we will not ignore their pain and concerns.”
Brannon Orton, MD, is an orthopedic surgeon at Confluence Health, in Moses Lake, Wash. He sees a large number of trauma patients and thinks NYU is doing a good job of addressing a difficult problem in orthopedics – especially in the field of trauma.
He said in an interview: “Managing narcotics postoperatively can be challenging due to the fact that many people come into these fractures with a history of narcotic use.” Not only are they used to turning to opioids for pain relief, but they also may have built up a tolerance to them.
Although he hasn’t been using the lopioid protocol specifically, he has been following a multimodal approach regarding the postoperative use of narcotics. Of the study by Dr. Egol and colleagues, he said, “I think their paper presents an effective way of decreasing use of oral narcotics and still adequately managing patients’ pain postoperatively.” Dr. Orton’s own practice utilizes tramadol, acetaminophen, and ibuprofen after fracture surgery.
From Dr. Orton’s perspective, a significant challenge in implementing the lopioid protocol in practice is simply sticking to the plan. “It can become difficult when patients are pressuring staff or physicians for more narcotics. However, I feel that if everybody is on the same page with the plan, then it can be very doable.”
Dr. Egol and NYU try to limit narcotic prescriptions beginning with the patient’s initial visit to the ED. The ED physicians at his institution only “prescribe small amounts of narcotics. Our ED people really limit the amount of opioids prescribed.”
Dr. Egol recommends that all practitioners begin with nonnarcotic medication, even if treating a fracture nonoperatively. “Start low and go higher. I always try to start with NSAIDs and Tylenol,” he said.
Dr. Egol and Dr. Orton reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
In a paper presented at the annual meeting of the American Academy of Orthopaedic Surgeons, researchers from NYU reported on the implementation of their multimodal strategy, dubbed the “lopioid protocol.”
According to the 2019 National Survey on Drug Use and Health, orthopedic surgeons are the third-highest opioid prescribers in the United States.
Kennneth A. Egol, MD, vice chair of the department of orthopedic surgery at NYU, who is the first author of the study, was motivated to help create the protocol following misconceptions that orthopedic surgeons were helping to fuel the opioid epidemic.
Dr. Egol pointed to the year 1995, when pain became the fifth vital sign after body temperature, pulse rate, respiratory rate, and blood pressure.
Since then, in light of the opioid epidemic, the focus of physicians has shifted away from prescribing strong pain medication and reducing pain scores to zero to instead reducing pain to a manageable level.
Reducing opioid prescriptions can be challenging when patients are prescribed an anti-inflammatory and they subsequently ask their physician for a “pain pill.” Patients sometimes don’t understand that inflammation is what causes pain.
It can also be difficult to convince patients that medications that they can buy over the counter can adequately control their pain, as confirmed in numerous studies.
Multimodal pain therapy aims to reduce the need for opioids by supplementing their use with other oral medications and, at times, long-lasting regional nerve blocks.
Anti-inflammatories act at the site of injury or surgery where inflammation is occurring. Nerves then carry the pain signal to the brain. These signals can be dampened by medications such as gabapentin that act on the nerves themselves. The pain signal is received in the brain, where opioids act by binding to receptors in the brain.
The so-called lopioid protocol does not eliminate opioids completely but rather uses “safer” opioids, such as tramadol, in lieu of stronger narcotics.
The protocol began at NYU on Jan. 1, 2019. It consists in the prescribing of tramadol, meloxicam, gabapentin, and acetaminophen.
The study presented at the AAOS meeting demonstrated statistically significant reductions in visual analogue pain scores at discharge and subsequent medication refills for the 931 patients in the lopioid group, compared with a group of 848 patients who received narcotic prescriptions containing oxycodone from the year prior to the protocol initiation.
Educating patients on the rationale for the prescription combination can help to allay their fears. Dr. Egol thinks it’s important for physicians to explain the dangers of opioids to patients. He said in an interview that he also believes surgeons need to “give [patients] an understanding of why we are pursuing these protocols. They also need to know we will not ignore their pain and concerns.”
Brannon Orton, MD, is an orthopedic surgeon at Confluence Health, in Moses Lake, Wash. He sees a large number of trauma patients and thinks NYU is doing a good job of addressing a difficult problem in orthopedics – especially in the field of trauma.
He said in an interview: “Managing narcotics postoperatively can be challenging due to the fact that many people come into these fractures with a history of narcotic use.” Not only are they used to turning to opioids for pain relief, but they also may have built up a tolerance to them.
Although he hasn’t been using the lopioid protocol specifically, he has been following a multimodal approach regarding the postoperative use of narcotics. Of the study by Dr. Egol and colleagues, he said, “I think their paper presents an effective way of decreasing use of oral narcotics and still adequately managing patients’ pain postoperatively.” Dr. Orton’s own practice utilizes tramadol, acetaminophen, and ibuprofen after fracture surgery.
From Dr. Orton’s perspective, a significant challenge in implementing the lopioid protocol in practice is simply sticking to the plan. “It can become difficult when patients are pressuring staff or physicians for more narcotics. However, I feel that if everybody is on the same page with the plan, then it can be very doable.”
Dr. Egol and NYU try to limit narcotic prescriptions beginning with the patient’s initial visit to the ED. The ED physicians at his institution only “prescribe small amounts of narcotics. Our ED people really limit the amount of opioids prescribed.”
Dr. Egol recommends that all practitioners begin with nonnarcotic medication, even if treating a fracture nonoperatively. “Start low and go higher. I always try to start with NSAIDs and Tylenol,” he said.
Dr. Egol and Dr. Orton reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
In a paper presented at the annual meeting of the American Academy of Orthopaedic Surgeons, researchers from NYU reported on the implementation of their multimodal strategy, dubbed the “lopioid protocol.”
According to the 2019 National Survey on Drug Use and Health, orthopedic surgeons are the third-highest opioid prescribers in the United States.
Kennneth A. Egol, MD, vice chair of the department of orthopedic surgery at NYU, who is the first author of the study, was motivated to help create the protocol following misconceptions that orthopedic surgeons were helping to fuel the opioid epidemic.
Dr. Egol pointed to the year 1995, when pain became the fifth vital sign after body temperature, pulse rate, respiratory rate, and blood pressure.
Since then, in light of the opioid epidemic, the focus of physicians has shifted away from prescribing strong pain medication and reducing pain scores to zero to instead reducing pain to a manageable level.
Reducing opioid prescriptions can be challenging when patients are prescribed an anti-inflammatory and they subsequently ask their physician for a “pain pill.” Patients sometimes don’t understand that inflammation is what causes pain.
It can also be difficult to convince patients that medications that they can buy over the counter can adequately control their pain, as confirmed in numerous studies.
Multimodal pain therapy aims to reduce the need for opioids by supplementing their use with other oral medications and, at times, long-lasting regional nerve blocks.
Anti-inflammatories act at the site of injury or surgery where inflammation is occurring. Nerves then carry the pain signal to the brain. These signals can be dampened by medications such as gabapentin that act on the nerves themselves. The pain signal is received in the brain, where opioids act by binding to receptors in the brain.
The so-called lopioid protocol does not eliminate opioids completely but rather uses “safer” opioids, such as tramadol, in lieu of stronger narcotics.
The protocol began at NYU on Jan. 1, 2019. It consists in the prescribing of tramadol, meloxicam, gabapentin, and acetaminophen.
The study presented at the AAOS meeting demonstrated statistically significant reductions in visual analogue pain scores at discharge and subsequent medication refills for the 931 patients in the lopioid group, compared with a group of 848 patients who received narcotic prescriptions containing oxycodone from the year prior to the protocol initiation.
Educating patients on the rationale for the prescription combination can help to allay their fears. Dr. Egol thinks it’s important for physicians to explain the dangers of opioids to patients. He said in an interview that he also believes surgeons need to “give [patients] an understanding of why we are pursuing these protocols. They also need to know we will not ignore their pain and concerns.”
Brannon Orton, MD, is an orthopedic surgeon at Confluence Health, in Moses Lake, Wash. He sees a large number of trauma patients and thinks NYU is doing a good job of addressing a difficult problem in orthopedics – especially in the field of trauma.
He said in an interview: “Managing narcotics postoperatively can be challenging due to the fact that many people come into these fractures with a history of narcotic use.” Not only are they used to turning to opioids for pain relief, but they also may have built up a tolerance to them.
Although he hasn’t been using the lopioid protocol specifically, he has been following a multimodal approach regarding the postoperative use of narcotics. Of the study by Dr. Egol and colleagues, he said, “I think their paper presents an effective way of decreasing use of oral narcotics and still adequately managing patients’ pain postoperatively.” Dr. Orton’s own practice utilizes tramadol, acetaminophen, and ibuprofen after fracture surgery.
From Dr. Orton’s perspective, a significant challenge in implementing the lopioid protocol in practice is simply sticking to the plan. “It can become difficult when patients are pressuring staff or physicians for more narcotics. However, I feel that if everybody is on the same page with the plan, then it can be very doable.”
Dr. Egol and NYU try to limit narcotic prescriptions beginning with the patient’s initial visit to the ED. The ED physicians at his institution only “prescribe small amounts of narcotics. Our ED people really limit the amount of opioids prescribed.”
Dr. Egol recommends that all practitioners begin with nonnarcotic medication, even if treating a fracture nonoperatively. “Start low and go higher. I always try to start with NSAIDs and Tylenol,” he said.
Dr. Egol and Dr. Orton reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.