User login
As demand for mental health care spikes, budget ax set to strike
When the pandemic hit, health officials in Montana’s Beaverhead County had barely begun to fill a hole left by the 2017 closure of the local public assistance office, mental health clinic, chemical dependency center and job placement office after the state’s last budget shortfall.
Now, those health officials worry more cuts are coming, even as they brace for a spike in demand for substance abuse and mental health services. That would be no small challenge in a poor farming and ranching region where stigma often prevents people from admitting they need help, said Katherine Buckley-Patton, who chairs the county’s Mental Health Local Advisory Council.
“I find it very challenging to find the words that will not make one of my hard-nosed cowboys turn around and walk away,” Ms. Buckley-Patton said.
States across the U.S. are still stinging after businesses closed and millions of people lost jobs because of COVID-related shutdowns and restrictions. Meanwhile, the pandemic has led to a dramatic increase in the number of people who say their mental health has suffered, rising from one in three people in March to more than half of people polled by KFF in July. (KHN is an editorially independent program of KFF.)
The full extent of the mental health crisis and the demand for behavioral health services may not be known until after the pandemic is over, mental health experts said. That could add costs that budget writers haven’t anticipated.

“It usually takes a while before people feel comfortable seeking care from a specialty behavioral health organization,” said Chuck Ingoglia, president and CEO of the nonprofit National Council for Behavioral Health in Washington, D.C. “We are not likely to see the results of that either in terms of people seeking care – or suicide rates going up – until we’re on the other side of the pandemic.”
Last year, states slashed agency budgets, froze pay, furloughed workers, borrowed money, and tapped into rainy-day funds to make ends meet. Health programs, often among the most expensive part of a state’s budget, were targeted for cuts in several states even as health officials led efforts to stem the spread of the coronavirus.
This year, the outlook doesn’t seem quite so bleak, partly because of relief packages passed by Congress last spring and in December that buoyed state economies. Another major advantage was that income increased or held steady for people with well-paying jobs and investment income, which boosted states’ tax revenues even as millions of lower-income workers were laid off.
“It has turned out to be not as bad as it might have been in terms of state budgets,” said Mike Leachman, vice president for state fiscal policy for the nonpartisan Center on Budget and Policy Priorities.
But many states still face cash shortfalls that will be made worse if additional federal aid doesn’t come, Mr. Leachman said. President Joe Biden has pledged to push through Congress a $1.9 billion relief package that includes aid to states, while congressional Republicans are proposing a package worth about a third of that amount. States are banking on federal help.

New York Gov. Andrew Cuomo, a Democrat, predicted his state would have to plug a $15 billion deficit with spending cuts and tax increases if a fresh round of aid doesn’t materialize. Some states, such as New Jersey, borrowed to make their budgets whole, and they’re going to have to start paying that money back. Tourism states such as Hawaii and energy-producing states such as Alaska and Wyoming continue to face grim economic outlooks with oil, gas, and coal prices down and tourists cutting back on travel, Mr. Leachman said.
Even states with a relatively rosy economic outlook are being cautious. In Colorado, for example, Democratic Gov. Jared Polis proposed a budget that restores the cuts made last year to Medicaid and substance abuse programs. But health providers are doubtful the legislature will approve any significant spending increases in this economy.
“Everybody right now is just trying to protect and make sure we don’t have additional cuts,” said Doyle Forrestal, CEO of the Colorado Behavioral Healthcare Council.
That’s also what Ms. Buckley-Patton wants for Montana’s Beaverhead County, where most of the 9,400 residents live in poverty or earn low incomes.
She led the county’s effort to recover from the loss in 2017 of a wide range of behavioral health services, along with offices to help poor people receive Medicaid health services, plus cash and food assistance.
Through persuasive grant writing and donations coaxed from elected officials, Ms. Buckley-Patton and her team secured office space, equipment, and a part-time employee for a resource center that’s open once a week in the county in the southwestern corner of the state, she said. They also convinced the state health department to send two people every other week on a 120-mile round trip from the Butte office to help county residents with their Medicaid and public assistance applications.
But now Ms. Buckley-Patton worries even those modest gains will be threatened in this year’s budget. Montana is one of the few states with a budget on a 2-year cycle, so this is the first time lawmakers have had to craft a spending plan since the pandemic began.
Revenue forecasts predict healthy tax collections over the next 2 years.
In January, at the start of the legislative session, the panel in charge of building the state health department’s budget proposed starting with nearly $1 billion in cuts. The panel’s chairperson, Republican Rep. Matt Regier, pledged to add back programs and services on their merits during the months-long budget process.
It’s a strategy Ms. Buckley-Patton worries will lead to a net loss of funding for Beaverhead County, which covers more land than Connecticut.
“I have grave concerns about this legislative session,” she said. “We’re not digging out of the hole; we’re only going deeper.”
Republicans, who are in control of the Montana House, Senate, and governor’s office for the first time in 16 years, are considering reducing the income tax level for the state’s top earners. Such a measure that could affect state revenue in an uncertain economy has some observers concerned, particularly when an increased need for health services is expected.
“Are legislators committed to building back up that budget in a way that works for communities and for health providers, or are we going to see tax cuts that reduce revenue that put us yet again in another really tight budget?” asked Heather O’Loughlin, codirector of the Montana Budget and Policy Center.
Mary Windecker, executive director of the Behavioral Health Alliance of Montana, said that health providers across the state are still clawing back from more than $100 million in budget cuts in 2017, and that she worries more cuts are on the horizon.

But one bright spot, she said, is a proposal by new Gov. Greg Gianforte to create a fund that would put $23 million a year toward community substance abuse prevention and treatment programs. It would be partially funded by tax revenue the state will receive from recreational marijuana, which voters approved in November, with sales to begin next year.
Ms. Windecker cautioned, though, that mental health and substance use are linked, and the governor and lawmakers should plan with that in mind.
“In the public’s mind, there’s drug addicts and there’s the mentally ill,” she said. “Quite often, the same people who have a substance use disorder are using it to treat a mental health issue that is underlying that substance use. So, you can never split the two out.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
When the pandemic hit, health officials in Montana’s Beaverhead County had barely begun to fill a hole left by the 2017 closure of the local public assistance office, mental health clinic, chemical dependency center and job placement office after the state’s last budget shortfall.
Now, those health officials worry more cuts are coming, even as they brace for a spike in demand for substance abuse and mental health services. That would be no small challenge in a poor farming and ranching region where stigma often prevents people from admitting they need help, said Katherine Buckley-Patton, who chairs the county’s Mental Health Local Advisory Council.
“I find it very challenging to find the words that will not make one of my hard-nosed cowboys turn around and walk away,” Ms. Buckley-Patton said.
States across the U.S. are still stinging after businesses closed and millions of people lost jobs because of COVID-related shutdowns and restrictions. Meanwhile, the pandemic has led to a dramatic increase in the number of people who say their mental health has suffered, rising from one in three people in March to more than half of people polled by KFF in July. (KHN is an editorially independent program of KFF.)
The full extent of the mental health crisis and the demand for behavioral health services may not be known until after the pandemic is over, mental health experts said. That could add costs that budget writers haven’t anticipated.
“It usually takes a while before people feel comfortable seeking care from a specialty behavioral health organization,” said Chuck Ingoglia, president and CEO of the nonprofit National Council for Behavioral Health in Washington, D.C. “We are not likely to see the results of that either in terms of people seeking care – or suicide rates going up – until we’re on the other side of the pandemic.”
Last year, states slashed agency budgets, froze pay, furloughed workers, borrowed money, and tapped into rainy-day funds to make ends meet. Health programs, often among the most expensive part of a state’s budget, were targeted for cuts in several states even as health officials led efforts to stem the spread of the coronavirus.
This year, the outlook doesn’t seem quite so bleak, partly because of relief packages passed by Congress last spring and in December that buoyed state economies. Another major advantage was that income increased or held steady for people with well-paying jobs and investment income, which boosted states’ tax revenues even as millions of lower-income workers were laid off.
“It has turned out to be not as bad as it might have been in terms of state budgets,” said Mike Leachman, vice president for state fiscal policy for the nonpartisan Center on Budget and Policy Priorities.
But many states still face cash shortfalls that will be made worse if additional federal aid doesn’t come, Mr. Leachman said. President Joe Biden has pledged to push through Congress a $1.9 billion relief package that includes aid to states, while congressional Republicans are proposing a package worth about a third of that amount. States are banking on federal help.
New York Gov. Andrew Cuomo, a Democrat, predicted his state would have to plug a $15 billion deficit with spending cuts and tax increases if a fresh round of aid doesn’t materialize. Some states, such as New Jersey, borrowed to make their budgets whole, and they’re going to have to start paying that money back. Tourism states such as Hawaii and energy-producing states such as Alaska and Wyoming continue to face grim economic outlooks with oil, gas, and coal prices down and tourists cutting back on travel, Mr. Leachman said.
Even states with a relatively rosy economic outlook are being cautious. In Colorado, for example, Democratic Gov. Jared Polis proposed a budget that restores the cuts made last year to Medicaid and substance abuse programs. But health providers are doubtful the legislature will approve any significant spending increases in this economy.
“Everybody right now is just trying to protect and make sure we don’t have additional cuts,” said Doyle Forrestal, CEO of the Colorado Behavioral Healthcare Council.
That’s also what Ms. Buckley-Patton wants for Montana’s Beaverhead County, where most of the 9,400 residents live in poverty or earn low incomes.
She led the county’s effort to recover from the loss in 2017 of a wide range of behavioral health services, along with offices to help poor people receive Medicaid health services, plus cash and food assistance.
Through persuasive grant writing and donations coaxed from elected officials, Ms. Buckley-Patton and her team secured office space, equipment, and a part-time employee for a resource center that’s open once a week in the county in the southwestern corner of the state, she said. They also convinced the state health department to send two people every other week on a 120-mile round trip from the Butte office to help county residents with their Medicaid and public assistance applications.
But now Ms. Buckley-Patton worries even those modest gains will be threatened in this year’s budget. Montana is one of the few states with a budget on a 2-year cycle, so this is the first time lawmakers have had to craft a spending plan since the pandemic began.
Revenue forecasts predict healthy tax collections over the next 2 years.
In January, at the start of the legislative session, the panel in charge of building the state health department’s budget proposed starting with nearly $1 billion in cuts. The panel’s chairperson, Republican Rep. Matt Regier, pledged to add back programs and services on their merits during the months-long budget process.
It’s a strategy Ms. Buckley-Patton worries will lead to a net loss of funding for Beaverhead County, which covers more land than Connecticut.
“I have grave concerns about this legislative session,” she said. “We’re not digging out of the hole; we’re only going deeper.”
Republicans, who are in control of the Montana House, Senate, and governor’s office for the first time in 16 years, are considering reducing the income tax level for the state’s top earners. Such a measure that could affect state revenue in an uncertain economy has some observers concerned, particularly when an increased need for health services is expected.
“Are legislators committed to building back up that budget in a way that works for communities and for health providers, or are we going to see tax cuts that reduce revenue that put us yet again in another really tight budget?” asked Heather O’Loughlin, codirector of the Montana Budget and Policy Center.
Mary Windecker, executive director of the Behavioral Health Alliance of Montana, said that health providers across the state are still clawing back from more than $100 million in budget cuts in 2017, and that she worries more cuts are on the horizon.
But one bright spot, she said, is a proposal by new Gov. Greg Gianforte to create a fund that would put $23 million a year toward community substance abuse prevention and treatment programs. It would be partially funded by tax revenue the state will receive from recreational marijuana, which voters approved in November, with sales to begin next year.
Ms. Windecker cautioned, though, that mental health and substance use are linked, and the governor and lawmakers should plan with that in mind.
“In the public’s mind, there’s drug addicts and there’s the mentally ill,” she said. “Quite often, the same people who have a substance use disorder are using it to treat a mental health issue that is underlying that substance use. So, you can never split the two out.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
When the pandemic hit, health officials in Montana’s Beaverhead County had barely begun to fill a hole left by the 2017 closure of the local public assistance office, mental health clinic, chemical dependency center and job placement office after the state’s last budget shortfall.
Now, those health officials worry more cuts are coming, even as they brace for a spike in demand for substance abuse and mental health services. That would be no small challenge in a poor farming and ranching region where stigma often prevents people from admitting they need help, said Katherine Buckley-Patton, who chairs the county’s Mental Health Local Advisory Council.
“I find it very challenging to find the words that will not make one of my hard-nosed cowboys turn around and walk away,” Ms. Buckley-Patton said.
States across the U.S. are still stinging after businesses closed and millions of people lost jobs because of COVID-related shutdowns and restrictions. Meanwhile, the pandemic has led to a dramatic increase in the number of people who say their mental health has suffered, rising from one in three people in March to more than half of people polled by KFF in July. (KHN is an editorially independent program of KFF.)
The full extent of the mental health crisis and the demand for behavioral health services may not be known until after the pandemic is over, mental health experts said. That could add costs that budget writers haven’t anticipated.
“It usually takes a while before people feel comfortable seeking care from a specialty behavioral health organization,” said Chuck Ingoglia, president and CEO of the nonprofit National Council for Behavioral Health in Washington, D.C. “We are not likely to see the results of that either in terms of people seeking care – or suicide rates going up – until we’re on the other side of the pandemic.”
Last year, states slashed agency budgets, froze pay, furloughed workers, borrowed money, and tapped into rainy-day funds to make ends meet. Health programs, often among the most expensive part of a state’s budget, were targeted for cuts in several states even as health officials led efforts to stem the spread of the coronavirus.
This year, the outlook doesn’t seem quite so bleak, partly because of relief packages passed by Congress last spring and in December that buoyed state economies. Another major advantage was that income increased or held steady for people with well-paying jobs and investment income, which boosted states’ tax revenues even as millions of lower-income workers were laid off.
“It has turned out to be not as bad as it might have been in terms of state budgets,” said Mike Leachman, vice president for state fiscal policy for the nonpartisan Center on Budget and Policy Priorities.
But many states still face cash shortfalls that will be made worse if additional federal aid doesn’t come, Mr. Leachman said. President Joe Biden has pledged to push through Congress a $1.9 billion relief package that includes aid to states, while congressional Republicans are proposing a package worth about a third of that amount. States are banking on federal help.
New York Gov. Andrew Cuomo, a Democrat, predicted his state would have to plug a $15 billion deficit with spending cuts and tax increases if a fresh round of aid doesn’t materialize. Some states, such as New Jersey, borrowed to make their budgets whole, and they’re going to have to start paying that money back. Tourism states such as Hawaii and energy-producing states such as Alaska and Wyoming continue to face grim economic outlooks with oil, gas, and coal prices down and tourists cutting back on travel, Mr. Leachman said.
Even states with a relatively rosy economic outlook are being cautious. In Colorado, for example, Democratic Gov. Jared Polis proposed a budget that restores the cuts made last year to Medicaid and substance abuse programs. But health providers are doubtful the legislature will approve any significant spending increases in this economy.
“Everybody right now is just trying to protect and make sure we don’t have additional cuts,” said Doyle Forrestal, CEO of the Colorado Behavioral Healthcare Council.
That’s also what Ms. Buckley-Patton wants for Montana’s Beaverhead County, where most of the 9,400 residents live in poverty or earn low incomes.
She led the county’s effort to recover from the loss in 2017 of a wide range of behavioral health services, along with offices to help poor people receive Medicaid health services, plus cash and food assistance.
Through persuasive grant writing and donations coaxed from elected officials, Ms. Buckley-Patton and her team secured office space, equipment, and a part-time employee for a resource center that’s open once a week in the county in the southwestern corner of the state, she said. They also convinced the state health department to send two people every other week on a 120-mile round trip from the Butte office to help county residents with their Medicaid and public assistance applications.
But now Ms. Buckley-Patton worries even those modest gains will be threatened in this year’s budget. Montana is one of the few states with a budget on a 2-year cycle, so this is the first time lawmakers have had to craft a spending plan since the pandemic began.
Revenue forecasts predict healthy tax collections over the next 2 years.
In January, at the start of the legislative session, the panel in charge of building the state health department’s budget proposed starting with nearly $1 billion in cuts. The panel’s chairperson, Republican Rep. Matt Regier, pledged to add back programs and services on their merits during the months-long budget process.
It’s a strategy Ms. Buckley-Patton worries will lead to a net loss of funding for Beaverhead County, which covers more land than Connecticut.
“I have grave concerns about this legislative session,” she said. “We’re not digging out of the hole; we’re only going deeper.”
Republicans, who are in control of the Montana House, Senate, and governor’s office for the first time in 16 years, are considering reducing the income tax level for the state’s top earners. Such a measure that could affect state revenue in an uncertain economy has some observers concerned, particularly when an increased need for health services is expected.
“Are legislators committed to building back up that budget in a way that works for communities and for health providers, or are we going to see tax cuts that reduce revenue that put us yet again in another really tight budget?” asked Heather O’Loughlin, codirector of the Montana Budget and Policy Center.
Mary Windecker, executive director of the Behavioral Health Alliance of Montana, said that health providers across the state are still clawing back from more than $100 million in budget cuts in 2017, and that she worries more cuts are on the horizon.
But one bright spot, she said, is a proposal by new Gov. Greg Gianforte to create a fund that would put $23 million a year toward community substance abuse prevention and treatment programs. It would be partially funded by tax revenue the state will receive from recreational marijuana, which voters approved in November, with sales to begin next year.
Ms. Windecker cautioned, though, that mental health and substance use are linked, and the governor and lawmakers should plan with that in mind.
“In the public’s mind, there’s drug addicts and there’s the mentally ill,” she said. “Quite often, the same people who have a substance use disorder are using it to treat a mental health issue that is underlying that substance use. So, you can never split the two out.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Study tests ways to increase autism screening and referrals
To improve autism screening rates, researchers in Utah tried a range of interventions.
They added automatic reminders to the electronic health record (EHR). They started using a shorter, more sensitive screening instrument. And they trained clinicians to perform autism-specific evaluations in a primary care clinic.

The researchers found that these interventions were associated with increased rates of autism screening and referrals.
At the same time, they looked at screening and referral rates at other community clinics in their health care system. These clinics incorporated EHR reminders but not all of the other changes.
“The community clinics had an increase in screening frequency with only automatic reminders,” the researchers reported. At the two intervention clinics, however, screening rates increased more than they did at the community clinics. Referrals did not significantly increase at the community clinics.
Kathleen Campbell, MD, MHSc, a pediatric resident at the University of Utah in Salt Lake City, and colleagues described their research in a study published in Pediatrics.
Three phases
They examined more than 12,000 well-child visits for children aged 16-30 months between July 2017 and June 2019.
In all, 4,155 visits occurred at the 2 intervention clinics, and 8,078 visits occurred at the 27 community clinics in the University of Utah health care system.
From baseline through the interventions, the proportion of visits with screening increased by 51% in the intervention clinics (from 58.6% to 88.8%), and by 21% in the community clinics (from 43.4% to 52.4%). The proportion of referrals increased 1.5-fold in intervention clinics, from 1.3% to 3.3%, the authors said.
The American Academy of Pediatrics (AAP) supports screening for autism in all children starting at age 18 months, but “only 44% of children with autism have had a comprehensive autism evaluation before age 36 months,” Dr. Campbell and colleagues wrote.
In their system, about half of the children were being screened for autism, and 0.5% had autism diagnosed.
In an effort to increase the proportion of visits with screening for autism and the proportion of visits with referrals for autism evaluation, Dr. Campbell and colleagues designed a quality improvement study.
Following a baseline period, they implemented interventions in three phases.
Initially, all clinics used the Modified Checklist for Autism in Toddlers, Revised (M-CHAT-R) for autism screening. For the first phase starting in July 2018, the researchers changed the screening instrument at the two intervention clinics to the Parent’s Observation of Social Interaction (POSI). This instrument “is embedded in a broadband developmental screen, is shorter than the M-CHAT-R, and includes questions about the consistency of the child’s behavior,” the authors said. “The POSI has greater sensitivity than the M-CHAT-R ... and similar, although somewhat lower, specificity.”
In intervention phase 2 starting in November 2018, the researchers “added an automatic reminder for autism screening to the EHR health maintenance screen.” Both the intervention clinics and the community clinics received the automatic reminders.
In intervention phase 3 starting in February 2019, they “added a referral option that clinicians could use for rapid access to autism-specific evaluation ... for children who had a POSI result suggestive of autism and for whom the clinician had sufficient concerns about autism that would indicate the need for referral for autism evaluation,” the researchers said.
“Using an online tutorial, we trained three clinicians in the intervention clinics to administer an observational assessment known as the Screening Tool for Autism in Toddlers (STAT),” which requires a 30-minute visit, they said. “Children who had a STAT result suggestive of autism were referred for expedited autism diagnostic evaluation, which was performed by a multidisciplinary team in our university-based developmental assessment clinic. Children who had a STAT result that did not suggest autism did not receive further autism evaluations unless the clinician felt they still needed further evaluation at the developmental clinic.”
After the switch to POSI, the percentage of visits with a positive screen result increased from 4.7% to 13.5% in the intervention clinics.
Furthermore, referrals were 3.4 times more frequent for visits during phase 3 in the intervention clinics, relative to the baseline period.
Potential to overwhelm
“The change to a more sensitive screening instrument increased the frequency of screening results suggestive of autism and informed our improvement team of the need to implement autism evaluation in primary care to avoid overwhelming our referral system,” Dr. Campbell and coauthors reported.
Future studies may assess whether increased screening and referrals speed the time to diagnosis and treatment and improve long-term functional abilities of children with autism. Some children in the study have received an autism diagnosis, while others have not yet been evaluated.
The use of STAT in primary care may be limited by “the barriers of training providers and purchasing materials,” the authors noted. “However, the time-based billing for lengthier appointments and billing for developmental testing help to cover cost.”
The intervention clinics and community clinics were staffed by pediatric providers, including residents and attendings, said Dr. Campbell.
“The staffing is similar at the community and intervention clinics, with mostly pediatricians and some nurse practitioners,” Dr. Campbell said. “One difference is that there are a few family medicine physicians in the community clinics, but we did not study whether that made a difference in screening. At the beginning of the study the approach to screening was the same.”
From the start, the community clinics were screening for autism and referring for further autism evaluation less often than the intervention clinics. “I don’t know why they were screening less, but they did improve with the automatic reminders,” said Dr. Campbell. “We didn’t examine type of provider or type of practice in this study, but the literature suggests that family physicians do not screen for autism as often as pediatricians.”
Payment and referral challenges
In theory, the approach in the study is a great idea, but it may not be feasible to implement for many private practices, said Herschel Lessin, MD. Dr. Lessin is a senior partner of the Children’s Medical Group in New York.

“We desperately need autism screening in a primary care setting,” Dr. Lessin said. “These authors found that wasn’t being done as recommended by the AAP Bright Futures, which is a problem.”
However, the researchers incorporated the interventions in a health care system with “far more resources than most people in practice would ever have” and substituted a less familiar screening tool.
In addition, the ability to use confirmatory STAT for primary care evaluations may be limited. “Unless you can find pediatricians willing to commit 30 to 45 minutes on one of these evaluations ... few are going to do that,” he said.
“The whole problem is that there are no referrals available or very few referrals available, and that insurance payments so underpay for developmental screening and evaluation that it does not justify the time doing it, so a lot of doctors are unable to do it,” said Dr. Lessin. When a referral is warranted, developmental pediatricians may have 6- to 12-month waiting lists, he said.
“For people in clinical practice, this is not news,” Dr. Lessin said. “We know we should screen for autism. The problem is it’s time consuming. Nobody pays for it. We have no place to send them even when we are suspicious.”
From screening to diagnosis to treatment
“Autism screen approaches vary but with educational efforts on the part of the AAP, CDC, and family organizations the rates for autism screening have dramatically improved,” said Susan L. Hyman, MD, professor of pediatrics at the University of Rochester in New York. “I do not know if screening rates have been impacted by COVID.”
Dr. Hyman and coauthors wrote an AAP clinical report on the identification, evaluation, and management of children with autism spectrum disorder. The report was published in the January 2020 issue of Pediatrics.
After screening and diagnostic testing, patients most importantly need to be able to access “timely and equitable evidence-based intervention,” which should be available, said Dr. Hyman.
Although researchers have proposed training primary care providers in autism diagnostics, “older, more complex patients with co-occurring behavioral health or other developmental disorders may need more specialized diagnostic assessment than could be accomplished in a primary care setting,” Dr. Hyman added.
“However, it is very important to identify children with therapeutic needs as early as possible and move them through the continuum from screening to diagnosis to treatment in a timely fashion. It would be wonderful if symptoms could be addressed without the need for diagnosis in the very youngest children,” Dr. Hyman said. “Early symptoms, even if not autism, are likely to be appropriate for intervention – whether it is speech therapy, attention to food selectivity, sleep problems – things that impact quality of life and potential future symptoms.”
The research was supported by the Utah Stimulating Access to Research in Residency Transition Scholar award, which is funded by the National Institutes of Health.
Dr. Campbell is an inventor on a patent related to screening for autism. The study authors otherwise had no disclosures. Dr. Lessin is on the editorial advisory board for Pediatric News and is on an advisory board for Cognoa, which is developing a medical device to diagnose autism and he is also the co-editor of the AAP's current ADHD Toolkit. Dr. Hyman had no relevant financial disclosures.
*This story was updated on Feb. 11, 2021.
To improve autism screening rates, researchers in Utah tried a range of interventions.
They added automatic reminders to the electronic health record (EHR). They started using a shorter, more sensitive screening instrument. And they trained clinicians to perform autism-specific evaluations in a primary care clinic.
The researchers found that these interventions were associated with increased rates of autism screening and referrals.
At the same time, they looked at screening and referral rates at other community clinics in their health care system. These clinics incorporated EHR reminders but not all of the other changes.
“The community clinics had an increase in screening frequency with only automatic reminders,” the researchers reported. At the two intervention clinics, however, screening rates increased more than they did at the community clinics. Referrals did not significantly increase at the community clinics.
Kathleen Campbell, MD, MHSc, a pediatric resident at the University of Utah in Salt Lake City, and colleagues described their research in a study published in Pediatrics.
Three phases
They examined more than 12,000 well-child visits for children aged 16-30 months between July 2017 and June 2019.
In all, 4,155 visits occurred at the 2 intervention clinics, and 8,078 visits occurred at the 27 community clinics in the University of Utah health care system.
From baseline through the interventions, the proportion of visits with screening increased by 51% in the intervention clinics (from 58.6% to 88.8%), and by 21% in the community clinics (from 43.4% to 52.4%). The proportion of referrals increased 1.5-fold in intervention clinics, from 1.3% to 3.3%, the authors said.
The American Academy of Pediatrics (AAP) supports screening for autism in all children starting at age 18 months, but “only 44% of children with autism have had a comprehensive autism evaluation before age 36 months,” Dr. Campbell and colleagues wrote.
In their system, about half of the children were being screened for autism, and 0.5% had autism diagnosed.
In an effort to increase the proportion of visits with screening for autism and the proportion of visits with referrals for autism evaluation, Dr. Campbell and colleagues designed a quality improvement study.
Following a baseline period, they implemented interventions in three phases.
Initially, all clinics used the Modified Checklist for Autism in Toddlers, Revised (M-CHAT-R) for autism screening. For the first phase starting in July 2018, the researchers changed the screening instrument at the two intervention clinics to the Parent’s Observation of Social Interaction (POSI). This instrument “is embedded in a broadband developmental screen, is shorter than the M-CHAT-R, and includes questions about the consistency of the child’s behavior,” the authors said. “The POSI has greater sensitivity than the M-CHAT-R ... and similar, although somewhat lower, specificity.”
In intervention phase 2 starting in November 2018, the researchers “added an automatic reminder for autism screening to the EHR health maintenance screen.” Both the intervention clinics and the community clinics received the automatic reminders.
In intervention phase 3 starting in February 2019, they “added a referral option that clinicians could use for rapid access to autism-specific evaluation ... for children who had a POSI result suggestive of autism and for whom the clinician had sufficient concerns about autism that would indicate the need for referral for autism evaluation,” the researchers said.
“Using an online tutorial, we trained three clinicians in the intervention clinics to administer an observational assessment known as the Screening Tool for Autism in Toddlers (STAT),” which requires a 30-minute visit, they said. “Children who had a STAT result suggestive of autism were referred for expedited autism diagnostic evaluation, which was performed by a multidisciplinary team in our university-based developmental assessment clinic. Children who had a STAT result that did not suggest autism did not receive further autism evaluations unless the clinician felt they still needed further evaluation at the developmental clinic.”
After the switch to POSI, the percentage of visits with a positive screen result increased from 4.7% to 13.5% in the intervention clinics.
Furthermore, referrals were 3.4 times more frequent for visits during phase 3 in the intervention clinics, relative to the baseline period.
Potential to overwhelm
“The change to a more sensitive screening instrument increased the frequency of screening results suggestive of autism and informed our improvement team of the need to implement autism evaluation in primary care to avoid overwhelming our referral system,” Dr. Campbell and coauthors reported.
Future studies may assess whether increased screening and referrals speed the time to diagnosis and treatment and improve long-term functional abilities of children with autism. Some children in the study have received an autism diagnosis, while others have not yet been evaluated.
The use of STAT in primary care may be limited by “the barriers of training providers and purchasing materials,” the authors noted. “However, the time-based billing for lengthier appointments and billing for developmental testing help to cover cost.”
The intervention clinics and community clinics were staffed by pediatric providers, including residents and attendings, said Dr. Campbell.
“The staffing is similar at the community and intervention clinics, with mostly pediatricians and some nurse practitioners,” Dr. Campbell said. “One difference is that there are a few family medicine physicians in the community clinics, but we did not study whether that made a difference in screening. At the beginning of the study the approach to screening was the same.”
From the start, the community clinics were screening for autism and referring for further autism evaluation less often than the intervention clinics. “I don’t know why they were screening less, but they did improve with the automatic reminders,” said Dr. Campbell. “We didn’t examine type of provider or type of practice in this study, but the literature suggests that family physicians do not screen for autism as often as pediatricians.”
Payment and referral challenges
In theory, the approach in the study is a great idea, but it may not be feasible to implement for many private practices, said Herschel Lessin, MD. Dr. Lessin is a senior partner of the Children’s Medical Group in New York.
“We desperately need autism screening in a primary care setting,” Dr. Lessin said. “These authors found that wasn’t being done as recommended by the AAP Bright Futures, which is a problem.”
However, the researchers incorporated the interventions in a health care system with “far more resources than most people in practice would ever have” and substituted a less familiar screening tool.
In addition, the ability to use confirmatory STAT for primary care evaluations may be limited. “Unless you can find pediatricians willing to commit 30 to 45 minutes on one of these evaluations ... few are going to do that,” he said.
“The whole problem is that there are no referrals available or very few referrals available, and that insurance payments so underpay for developmental screening and evaluation that it does not justify the time doing it, so a lot of doctors are unable to do it,” said Dr. Lessin. When a referral is warranted, developmental pediatricians may have 6- to 12-month waiting lists, he said.
“For people in clinical practice, this is not news,” Dr. Lessin said. “We know we should screen for autism. The problem is it’s time consuming. Nobody pays for it. We have no place to send them even when we are suspicious.”
From screening to diagnosis to treatment
“Autism screen approaches vary but with educational efforts on the part of the AAP, CDC, and family organizations the rates for autism screening have dramatically improved,” said Susan L. Hyman, MD, professor of pediatrics at the University of Rochester in New York. “I do not know if screening rates have been impacted by COVID.”
Dr. Hyman and coauthors wrote an AAP clinical report on the identification, evaluation, and management of children with autism spectrum disorder. The report was published in the January 2020 issue of Pediatrics.
After screening and diagnostic testing, patients most importantly need to be able to access “timely and equitable evidence-based intervention,” which should be available, said Dr. Hyman.
Although researchers have proposed training primary care providers in autism diagnostics, “older, more complex patients with co-occurring behavioral health or other developmental disorders may need more specialized diagnostic assessment than could be accomplished in a primary care setting,” Dr. Hyman added.
“However, it is very important to identify children with therapeutic needs as early as possible and move them through the continuum from screening to diagnosis to treatment in a timely fashion. It would be wonderful if symptoms could be addressed without the need for diagnosis in the very youngest children,” Dr. Hyman said. “Early symptoms, even if not autism, are likely to be appropriate for intervention – whether it is speech therapy, attention to food selectivity, sleep problems – things that impact quality of life and potential future symptoms.”
The research was supported by the Utah Stimulating Access to Research in Residency Transition Scholar award, which is funded by the National Institutes of Health.
Dr. Campbell is an inventor on a patent related to screening for autism. The study authors otherwise had no disclosures. Dr. Lessin is on the editorial advisory board for Pediatric News and is on an advisory board for Cognoa, which is developing a medical device to diagnose autism and he is also the co-editor of the AAP's current ADHD Toolkit. Dr. Hyman had no relevant financial disclosures.
*This story was updated on Feb. 11, 2021.
To improve autism screening rates, researchers in Utah tried a range of interventions.
They added automatic reminders to the electronic health record (EHR). They started using a shorter, more sensitive screening instrument. And they trained clinicians to perform autism-specific evaluations in a primary care clinic.
The researchers found that these interventions were associated with increased rates of autism screening and referrals.
At the same time, they looked at screening and referral rates at other community clinics in their health care system. These clinics incorporated EHR reminders but not all of the other changes.
“The community clinics had an increase in screening frequency with only automatic reminders,” the researchers reported. At the two intervention clinics, however, screening rates increased more than they did at the community clinics. Referrals did not significantly increase at the community clinics.
Kathleen Campbell, MD, MHSc, a pediatric resident at the University of Utah in Salt Lake City, and colleagues described their research in a study published in Pediatrics.
Three phases
They examined more than 12,000 well-child visits for children aged 16-30 months between July 2017 and June 2019.
In all, 4,155 visits occurred at the 2 intervention clinics, and 8,078 visits occurred at the 27 community clinics in the University of Utah health care system.
From baseline through the interventions, the proportion of visits with screening increased by 51% in the intervention clinics (from 58.6% to 88.8%), and by 21% in the community clinics (from 43.4% to 52.4%). The proportion of referrals increased 1.5-fold in intervention clinics, from 1.3% to 3.3%, the authors said.
The American Academy of Pediatrics (AAP) supports screening for autism in all children starting at age 18 months, but “only 44% of children with autism have had a comprehensive autism evaluation before age 36 months,” Dr. Campbell and colleagues wrote.
In their system, about half of the children were being screened for autism, and 0.5% had autism diagnosed.
In an effort to increase the proportion of visits with screening for autism and the proportion of visits with referrals for autism evaluation, Dr. Campbell and colleagues designed a quality improvement study.
Following a baseline period, they implemented interventions in three phases.
Initially, all clinics used the Modified Checklist for Autism in Toddlers, Revised (M-CHAT-R) for autism screening. For the first phase starting in July 2018, the researchers changed the screening instrument at the two intervention clinics to the Parent’s Observation of Social Interaction (POSI). This instrument “is embedded in a broadband developmental screen, is shorter than the M-CHAT-R, and includes questions about the consistency of the child’s behavior,” the authors said. “The POSI has greater sensitivity than the M-CHAT-R ... and similar, although somewhat lower, specificity.”
In intervention phase 2 starting in November 2018, the researchers “added an automatic reminder for autism screening to the EHR health maintenance screen.” Both the intervention clinics and the community clinics received the automatic reminders.
In intervention phase 3 starting in February 2019, they “added a referral option that clinicians could use for rapid access to autism-specific evaluation ... for children who had a POSI result suggestive of autism and for whom the clinician had sufficient concerns about autism that would indicate the need for referral for autism evaluation,” the researchers said.
“Using an online tutorial, we trained three clinicians in the intervention clinics to administer an observational assessment known as the Screening Tool for Autism in Toddlers (STAT),” which requires a 30-minute visit, they said. “Children who had a STAT result suggestive of autism were referred for expedited autism diagnostic evaluation, which was performed by a multidisciplinary team in our university-based developmental assessment clinic. Children who had a STAT result that did not suggest autism did not receive further autism evaluations unless the clinician felt they still needed further evaluation at the developmental clinic.”
After the switch to POSI, the percentage of visits with a positive screen result increased from 4.7% to 13.5% in the intervention clinics.
Furthermore, referrals were 3.4 times more frequent for visits during phase 3 in the intervention clinics, relative to the baseline period.
Potential to overwhelm
“The change to a more sensitive screening instrument increased the frequency of screening results suggestive of autism and informed our improvement team of the need to implement autism evaluation in primary care to avoid overwhelming our referral system,” Dr. Campbell and coauthors reported.
Future studies may assess whether increased screening and referrals speed the time to diagnosis and treatment and improve long-term functional abilities of children with autism. Some children in the study have received an autism diagnosis, while others have not yet been evaluated.
The use of STAT in primary care may be limited by “the barriers of training providers and purchasing materials,” the authors noted. “However, the time-based billing for lengthier appointments and billing for developmental testing help to cover cost.”
The intervention clinics and community clinics were staffed by pediatric providers, including residents and attendings, said Dr. Campbell.
“The staffing is similar at the community and intervention clinics, with mostly pediatricians and some nurse practitioners,” Dr. Campbell said. “One difference is that there are a few family medicine physicians in the community clinics, but we did not study whether that made a difference in screening. At the beginning of the study the approach to screening was the same.”
From the start, the community clinics were screening for autism and referring for further autism evaluation less often than the intervention clinics. “I don’t know why they were screening less, but they did improve with the automatic reminders,” said Dr. Campbell. “We didn’t examine type of provider or type of practice in this study, but the literature suggests that family physicians do not screen for autism as often as pediatricians.”
Payment and referral challenges
In theory, the approach in the study is a great idea, but it may not be feasible to implement for many private practices, said Herschel Lessin, MD. Dr. Lessin is a senior partner of the Children’s Medical Group in New York.
“We desperately need autism screening in a primary care setting,” Dr. Lessin said. “These authors found that wasn’t being done as recommended by the AAP Bright Futures, which is a problem.”
However, the researchers incorporated the interventions in a health care system with “far more resources than most people in practice would ever have” and substituted a less familiar screening tool.
In addition, the ability to use confirmatory STAT for primary care evaluations may be limited. “Unless you can find pediatricians willing to commit 30 to 45 minutes on one of these evaluations ... few are going to do that,” he said.
“The whole problem is that there are no referrals available or very few referrals available, and that insurance payments so underpay for developmental screening and evaluation that it does not justify the time doing it, so a lot of doctors are unable to do it,” said Dr. Lessin. When a referral is warranted, developmental pediatricians may have 6- to 12-month waiting lists, he said.
“For people in clinical practice, this is not news,” Dr. Lessin said. “We know we should screen for autism. The problem is it’s time consuming. Nobody pays for it. We have no place to send them even when we are suspicious.”
From screening to diagnosis to treatment
“Autism screen approaches vary but with educational efforts on the part of the AAP, CDC, and family organizations the rates for autism screening have dramatically improved,” said Susan L. Hyman, MD, professor of pediatrics at the University of Rochester in New York. “I do not know if screening rates have been impacted by COVID.”
Dr. Hyman and coauthors wrote an AAP clinical report on the identification, evaluation, and management of children with autism spectrum disorder. The report was published in the January 2020 issue of Pediatrics.
After screening and diagnostic testing, patients most importantly need to be able to access “timely and equitable evidence-based intervention,” which should be available, said Dr. Hyman.
Although researchers have proposed training primary care providers in autism diagnostics, “older, more complex patients with co-occurring behavioral health or other developmental disorders may need more specialized diagnostic assessment than could be accomplished in a primary care setting,” Dr. Hyman added.
“However, it is very important to identify children with therapeutic needs as early as possible and move them through the continuum from screening to diagnosis to treatment in a timely fashion. It would be wonderful if symptoms could be addressed without the need for diagnosis in the very youngest children,” Dr. Hyman said. “Early symptoms, even if not autism, are likely to be appropriate for intervention – whether it is speech therapy, attention to food selectivity, sleep problems – things that impact quality of life and potential future symptoms.”
The research was supported by the Utah Stimulating Access to Research in Residency Transition Scholar award, which is funded by the National Institutes of Health.
Dr. Campbell is an inventor on a patent related to screening for autism. The study authors otherwise had no disclosures. Dr. Lessin is on the editorial advisory board for Pediatric News and is on an advisory board for Cognoa, which is developing a medical device to diagnose autism and he is also the co-editor of the AAP's current ADHD Toolkit. Dr. Hyman had no relevant financial disclosures.
*This story was updated on Feb. 11, 2021.
FROM PEDIATRICS
A Stepwise Approach for Preventing Suicide by Lethal Poisoning
Suicide is a global phenomenon and a worldwide public health concern.1 The World Health Organization estimates that > 800,000 people die by suicide every year. In the US, suicide is the 10th leading cause of death, and on average, 129 Americans die by suicide each day.2 In 2018, the suicide rate for all veterans was 1.5 times higher than the rate for nonveterans, after adjusting for population differences in age and sex. Among female veterans, the rate of suicide was 2.1 times higher than the rate for female nonveterans.3
In light of this disparity, suicide prevention is one of the highest priorities for the US Department of Veterans Affairs (VA). In 2018, the VA developed and published the National Strategy for Preventing Veteran Suicide.4 One major goal of this strategy is to reduce access to lethal means (ie, firearms, medications, chemicals, or poisons) among veterans at high risk for suicide. Reducing access to lethal means has been found to decrease suicide rates.4,5
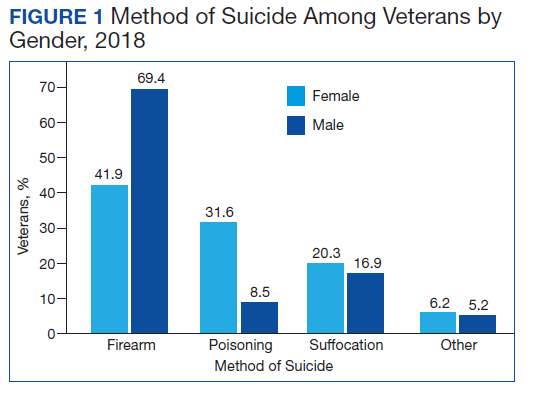
Drug overdose is a leading method for suicide attempts, especially for female veterans.3,6 Although the overall case fatality ratio for overdose is < 2%, drug overdose accounted for 59.4% of suicide attempts and 13.5% of deaths by suicide from 2007 to 2014.6,7 Within the veteran population, the majority of suicide deaths in 2018 were due to self-inflicted firearm injury for both male and female veterans, followed by poisoning via substances and pharmaceutical agents for female veterans (Figure 1).3 Notably, when compared with men, women were more likely to choose drug overdose as a method for suicide. One study found that women aged < 45 years used drug and poison ingestion in 9 out of 10 suicide attempts.6 Since some medications are more lethal than others, interventions to limit the availability of lethal medications may prevent deaths and reduce the severity of suicide attempts. This article will provide a stepwise approach to help clinicians identify and limit lethal medications for patients at high risk for suicide.
Step 1: Determine Suicide Risk
Although it is impossible to predict with certainty an individual’s risk of suicide, several patient characteristics and life circumstances have been identified as risk factors. The strongest predictor of suicide is the presence of psychiatric disease.8 More than 90% of those who have had a death by suicide have a psychiatric diagnosis at the time of death, and suicide rates in those with mental illness are at least 10 times as high as in the general population.9,10 Depression is the leading cause of death by suicide worldwide, followed by substance-related disorders (22.4%), personality disorders (11.6%), schizophrenia (10.6%), and anxiety/somatoform disorders (6.1%).8,11-13
Clinicians also can use various risk assessment tools to identify patients at high risk for suicide. The Veterans Health Administration (VHA) Stratification Tool for Opioid Risk Mitigation (STORM) calculates patients’ risk based on data extracted from the electronic health record and is less time intensive, more easily refined, and may be more powerful than standard risk assessment tools because it can be deployed on a large scale.14,15 The VHA also developed the Suicide Prevention Population Risk Identification and Tracking for Exigencies (SPPRITE) tool to assist clinicians in tracking patients with current (or recent) high levels of suicide risk. This tool unifies specific patient information gathered from the patient’s electronic health record and from other predictive model dashboards (such as STORM).
Step 2: Identify Substances Strongly Associated With Fatalities
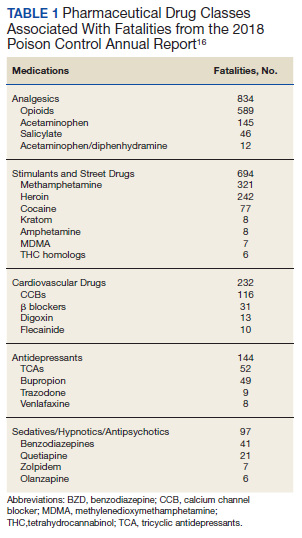
According to the American Association of Poison Control Centers (AAPCC), the pharmaceutical classes associated with the largest number of fatalities are analgesics, followed by stimulants and street drugs, cardiovascular agents, antidepressants, antipsychotics, and sedatives/hypnotics (Table 1).16 Stimulants and street drugs accounted for 694 fatalities of 39,238 single-substance exposures (mortality rate: 1.8%).16 Drugs of abuse, including cocaine, hallucinogenic amphetamines, heroin, and kratom, have shown an increased trend in use.16
In 2018 there were 834 fatalities from 174,269 single-substance exposure to analgesics, which include opioids and acetaminophen, for a mortality rate of 0.5%.16 The opioid epidemic is one of the main drivers of the increase in drug overdose deaths in the US.16,17 The opioid with the highest drug overdose fatality rate is illicitly manufactured fentanyl, which often is combined with other substances, such as heroin, to increase its potency at a low cost.18 These combinations also increase the risk of overdose fatality.
Acetaminophen is unique among the top substances associated with fatalities because it is obtained easily without a prescription. An acetaminophen overdose can cause hepatic injury, which may progress to fulminant hepatic failure and death.19 The recommended maximum dose of acetaminophen is 4 g/d in an adult and 50 to 75 mg/kg/d in children. A single acute ingestion of > 7.5 g in an adult or 150 mg/kg in children has been considered potentially toxic.19,20 The use of combination analgesics that contain both an opioid and acetaminophen can pose an even greater risk due to the potential for respiratory depression and hepatotoxicity.
Cardiovascular drugs accounted for 232 fatalities from 46,499 single-substance exposures (mortality rate: 0.5%).16 According to the AAPCC, calcium channel blockers (CCB) and β-blockers accounted for 63% of overdose deaths by cardiovascular drugs because they can cause severe hypotension, bradycardia, and hemodynamic collapse.16,21,22
In the past, the nondihydropyridine CCBs verapamil and diltiazem were associated with increased overdose fatalities. However, the most recent data show that dihydropyridine CCBs such as amlodipine also have significant risk for lethality.16 Metoprolol was associated with more overdose deaths in the past year among β-blockers. However, caution also should be used with agents such as propranolol and labetalol, which can antagonize sodium channels in overdose and may be associated with a higher risk of mortality than other β-blockers.22
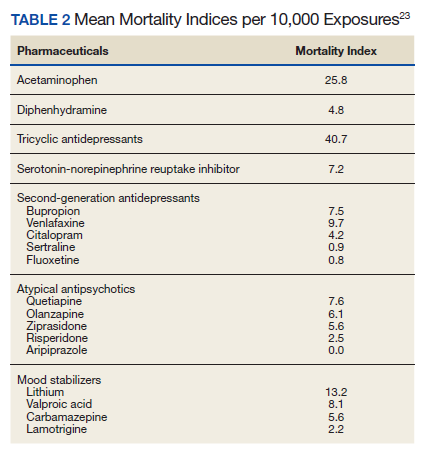
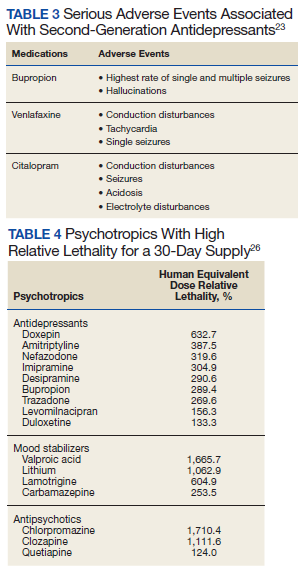
Antidepressants accounted for 144 fatalities from 56,891 single-substance exposures (mortality rate: 0.3%).16 Nelson and Spyker performed a study to determine the morbidity and mortality index for psychotropic agents based on exposure reports from the National Poison Data system and found that tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) had the highest morbidity and mortality rates among all drugs used to treat depression.23 As a class, TCAs have a mortality index of 40.7 per 10,000 exposures and are associated with higher rates of acidosis, cardiac conduction problems, respiratory depression, and seizures (Table 2).23 Amitriptyline accounted for 39.5% of deaths from antidepressants.23 Among newer antidepressants, citalopram, venlafaxine, and bupropion have been found to be the most hazardous.23 Citalopram and venlafaxine have morbidity indices that are 4- to 5-fold higher than sertraline. Adverse events associated with bupropion, venlafaxine, and citalopram, such as seizures, conduction disturbances, hallucinations, and tachycardia contribute to the morbidity and mortality related to these medications (Table 3).
Of the atypical antipsychotics, olanzapine, quetiapine, and ziprasidone have the highest mortality rates.23 Cardiac conduction problems were more frequent with olanzapine and ziprasidone, and respiratory depression was more frequent with olanzapine and quetiapine. Aripiprazole had the lowest rates of morbidity and mortality.23
Of the mood stabilizers, lithium, valproic acid, and carbamazepine have narrow therapeutic indices and, therefore, moderately high mortality rates.23 Lithium was associated with higher rates of bradycardia, confusion, and renal problems. Valproic acid had relatively high levels of acidosis and coma. Carbamazepine had high rates of coma and the highest rate of nystagmus.
Sedatives and hypnotics accounted for 97 fatalities of 51,495 single-substance exposures (mortality rate 0.2%).16 Within this category, benzodiazepines (BZDs), particularly alprazolam, clonazepam, and diazepam, were associated with the highest number of overdose deaths.16 Although fatalities from single-substance exposure to this category are low, it should be noted that BZDs are primarily metabolized by the CYP2C19 and CYP3A4 enzymes. Interactions with other drugs also metabolized by the same CYP enzymes may lead to prolonged effects of BZDs, such as sedation, and respiratory depression, which significantly increase the risk of overdose death. Furthermore, lipophilic BZDs, such as diazepam, can accumulate in the tissue after multiple doses and have impaired clearance in older patients.
Step 3: Consider Potential Drug-Drug Interactions
Suicide attempts involving multiple substances carry increased risk. Only 12.1% of all fatal overdoses, according to AAPCC, involved single-substance exposure, whereas 56.3% were attributed to multiple substance exposures.16 It is important for clinicians to be aware of and avoid possibly fatal drug-drug interactions, such as the combination of opioids and sedative-hypnotics, like BZDs, which can lead to fatal respiratory depression. Clinicians also should be aware of a patient’s history of illicit opioid and alcohol use before prescribing opioids and BZDs. Clinicians can use various online databases to detect potential drug-drug interactions.
Step 4: Address Risks
If a patient is deemed to be at high risk for suicide, but it is not imminent and the patient will be managed as an outpatient, then it may be preferential to prescribe medications that are less lethal, such as SSRIs, instead of TCAs or MAOIs. If a potentially lethal medication is indicated, such as lithium or clozapine, both of which have been found to reduce suicidal behavior, then dispensing a limited quantity of pills and having more frequent follow-up visits are some ways to lessen risk.24,25 A clinical pearl published in Current Psychiatry provided an equation to determine the lethality of a 30-day supply of medications.26 This equation uses lethal dose 50 (LD50), which is the dose of a medication that results in the death of 50% of the animals used in a controlled experiment, and the maximum daily dose of the medication (D) to find the human equivalent dose (HED) relative lethality. The HED relative lethality calculation may help prescribers determine which medications should have a limited quantity dispensed to patients at risk of medication-related suicide. Any value for the HED relative lethality that is > 100% is considered a lethal dose for humans. Therefore, it would be appropriate to avoid or limit the quantity of medications with a HED relative lethality > 100%. Table 4 lists the psychotropic agents with the highest relative lethality for a 30-day supply. The psychotropic agents with the lowest HED relative lethality are SSRIs: desvenlafaxine, mirtazapine, topiramate, and aripiprazole.26
![]()
Limiting drugs with a narrow therapeutic index should be considered when aiming to reduce the risk of medication-related suicide. These drugs present a high risk in the event of an overdose. Clinicians can monitor the levels of lithium, clozapine, or TCAs to ensure that a patient is taking the medication as prescribed rather than stockpiling it at home. If the patient is in a monitored setting, such as a partial hospital program or intensive outpatient program, then the medication can be given while under direct observation.
Clinicians should obtain an accurate and detailed medication and illicit drug use history from patients. It also is important to review the prescription drug monitoring program to limit access to potentially lethal combinations of medications.27 Clinicians can additionally employ risk mitigation strategies (eg, providing naloxone kits) for patients who are prescribed or abuse opioids.
Finally, all patients with a high risk of suicide should receive lethal means counseling, which involves first determining whether patients have access to lethal means, such as firearms or medications with high lethality, then limiting their access to these lethal means. This includes advising patients and family members to safely dispose medications that are no longer in use and in some cases recommending that a family member keep medications locked and dispense them on a daily basis.
Conclusions
Suicide is a major public health concern that affects tens of thousands of Americans annually. Furthermore, veterans are more likely to die by suicide than those in the general population. Firearms continue to be the most lethal means for suicide. However, intentional poisoning with medications or substances also is a common method for suicide, especially in female veterans. Having knowledge of medications with high lethality and limiting access to these agents can be a successful strategy for reducing suicide deaths.
1. World Health Organization. Preventing suicide: a global imperative. Published 2014. Accessed January 16, 2021. https://apps.who.int/iris/bitstream/handle/10665/131056/9789241564779_eng.pdf
2. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention. National Violent Death Reporting System (NVDRS). Updated November 7, 2019. Accessed January 7, 2021. https://www.cdc.gov/violenceprevention/datasources/nvdrs/
3. US Department of Veteran Affairs, Office of Mental Health and Suicide Prevention. 2020 national veteran suicide prevention annual report. Accessed January 16, 2021. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
4. US Department of Veteran Affairs. National strategy for preventing veteran suicide 2018-2028. Accessed January 7, 2021. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
5. Zalsman G, Hawton K, Wasserman D, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. 2016;3(7):646-659. doi:10.1016/S2215-0366(16)30030-X
6. Spicer RS, Miller TR. Suicide acts in 8 states: incidence and case fatality rates by demographics and method. Am J Public Health. 2000;90(12):1885-1891. doi:10.2105/ajph.90.12.1885
7. Conner A, Azrael D, Miller M. Suicide Case-Fatality Rates in the United States, 2007 to 2014: A Nationwide Population-Based Study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
8. Bertolote JM, Fleischmann A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry. 2002;1(3):181-185.
9. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics. 1999;40(1):18-27. doi:10.1016/S0033-3182(99)71267-3
10. Bachmann S. Epidemiology of Suicide and the Psychiatric Perspective. Int J Environ Res Public Health. 2018;15(7):1425. Published 2018 Jul 6. doi:10.3390/ijerph15071425
11. Hoertel N, Franco S, Wall MM, et al. Mental disorders and risk of suicide attempt: a national prospective study. Mol Psychiatry. 2015;20(6):718-726. doi:10.1038/mp.2015.19
12. Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013;10(11):e1001547. doi:10.1371/journal.pmed.1001547
13. World Health Organization. Mental health atlas. Accessed January 7, 2021. https://apps.who.int/iris/bitstream/handle/10665/178879/9789241565011_eng.pdf
14. Velupillai S, Hadlaczky G, Baca-Garcia E, et al. Risk assessment tools and data-driven approaches for predicting and preventing suicidal behavior. Front Psychiatry. 2019;10:36. Published 2019 Feb 13. doi:10.3389/fpsyt.2019.00036
15. Oliva EM, Bowe T, Tavakoli S, et al. Development and applications of the Veterans Health Administration’s Stratification Tool for Opioid Risk Mitigation (STORM) to improve opioid safety and prevent overdose and suicide. Psychol Serv. 2017;14(1):34-49. doi:10.1037/ser0000099
16. Gummin DD, Mowry JB, Spyker DA, et al. 2018 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 36th Annual Report [published correction appears in Clin Toxicol (Phila). 2019 Dec;57(12):e1]. Clin Toxicol (Phila). 2019;57(12):1220-1413. doi:10.1080/15563650.2019.1677022
17. Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999–2018. NCHS Data Brief. 2020(356).
18. Kuczyn´ska K, Grzonkowski P, Kacprzak Ł, Zawilska JB. Abuse of fentanyl: An emerging problem to face. Forensic Sci Int. 2018;289:207-214. doi:10.1016/j.forsciint.2018.05.042
19. Hodgman MJ, Garrard AR. A review of acetaminophen poisoning. Crit Care Clin. 2012;28(4):499-516. doi:10.1016/j.ccc.2012.07.006
20. Chiew AL, Gluud C, Brok J, Buckley NA. Interventions for paracetamol (acetaminophen) overdose. Cochrane Database Syst Rev. 2018;2(2):CD003328. Published 2018 Feb 23. doi:10.1002/14651858.CD003328.pub3
21. Graudins A, Lee HM, Druda D. Calcium channel antagonist and beta-blocker overdose: antidotes and adjunct therapies. Br J Clin Pharmacol. 2016;81(3):453-461. doi:10.1111/bcp.12763
22. DeWitt CR, Waksman JC. Pharmacology, pathophysiology and management of calcium channel blocker and beta-blocker toxicity. Toxicol Rev. 2004;23(4):223-238. doi:10.2165/00139709-200423040-00003
23. Nelson JC, Spyker DA. Morbidity and mortality associated with medications used in the treatment of depression: an analysis of cases reported to U.S. Poison Control Centers, 2000-2014. Am J Psychiatry. 2017;174(5):438-450. doi:10.1176/appi.ajp.2016.16050523
24. Sarai SK, Mekala HM, Lippmann S. Lithium suicide prevention: a brief review and reminder. Innov Clin Neurosci. 2018;15(11-12):30-32.
25. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) [published correction appears in Arch Gen Psychiatry. 2003 Jul;60(7):735]. Arch Gen Psychiatry. 2003;60(1):82-91. doi:10.1001/archpsyc.60.1.82
26. Giurca D. Decreasing suicide risk with math. Curr Psychiatry. 2018;17(2):57-61.
27. Malte CA, Berger D, Saxon AJ, et al. Electronic medical record alert associated with reduced opioid and benzodiazepine coprescribing in high-risk veteran patients. Med Care. 2018;56(2):171-178. doi:10.1097/MLR.0000000000000861
Suicide is a global phenomenon and a worldwide public health concern.1 The World Health Organization estimates that > 800,000 people die by suicide every year. In the US, suicide is the 10th leading cause of death, and on average, 129 Americans die by suicide each day.2 In 2018, the suicide rate for all veterans was 1.5 times higher than the rate for nonveterans, after adjusting for population differences in age and sex. Among female veterans, the rate of suicide was 2.1 times higher than the rate for female nonveterans.3
In light of this disparity, suicide prevention is one of the highest priorities for the US Department of Veterans Affairs (VA). In 2018, the VA developed and published the National Strategy for Preventing Veteran Suicide.4 One major goal of this strategy is to reduce access to lethal means (ie, firearms, medications, chemicals, or poisons) among veterans at high risk for suicide. Reducing access to lethal means has been found to decrease suicide rates.4,5
Drug overdose is a leading method for suicide attempts, especially for female veterans.3,6 Although the overall case fatality ratio for overdose is < 2%, drug overdose accounted for 59.4% of suicide attempts and 13.5% of deaths by suicide from 2007 to 2014.6,7 Within the veteran population, the majority of suicide deaths in 2018 were due to self-inflicted firearm injury for both male and female veterans, followed by poisoning via substances and pharmaceutical agents for female veterans (Figure 1).3 Notably, when compared with men, women were more likely to choose drug overdose as a method for suicide. One study found that women aged < 45 years used drug and poison ingestion in 9 out of 10 suicide attempts.6 Since some medications are more lethal than others, interventions to limit the availability of lethal medications may prevent deaths and reduce the severity of suicide attempts. This article will provide a stepwise approach to help clinicians identify and limit lethal medications for patients at high risk for suicide.
Step 1: Determine Suicide Risk
Although it is impossible to predict with certainty an individual’s risk of suicide, several patient characteristics and life circumstances have been identified as risk factors. The strongest predictor of suicide is the presence of psychiatric disease.8 More than 90% of those who have had a death by suicide have a psychiatric diagnosis at the time of death, and suicide rates in those with mental illness are at least 10 times as high as in the general population.9,10 Depression is the leading cause of death by suicide worldwide, followed by substance-related disorders (22.4%), personality disorders (11.6%), schizophrenia (10.6%), and anxiety/somatoform disorders (6.1%).8,11-13
Clinicians also can use various risk assessment tools to identify patients at high risk for suicide. The Veterans Health Administration (VHA) Stratification Tool for Opioid Risk Mitigation (STORM) calculates patients’ risk based on data extracted from the electronic health record and is less time intensive, more easily refined, and may be more powerful than standard risk assessment tools because it can be deployed on a large scale.14,15 The VHA also developed the Suicide Prevention Population Risk Identification and Tracking for Exigencies (SPPRITE) tool to assist clinicians in tracking patients with current (or recent) high levels of suicide risk. This tool unifies specific patient information gathered from the patient’s electronic health record and from other predictive model dashboards (such as STORM).
Step 2: Identify Substances Strongly Associated With Fatalities
According to the American Association of Poison Control Centers (AAPCC), the pharmaceutical classes associated with the largest number of fatalities are analgesics, followed by stimulants and street drugs, cardiovascular agents, antidepressants, antipsychotics, and sedatives/hypnotics (Table 1).16 Stimulants and street drugs accounted for 694 fatalities of 39,238 single-substance exposures (mortality rate: 1.8%).16 Drugs of abuse, including cocaine, hallucinogenic amphetamines, heroin, and kratom, have shown an increased trend in use.16
In 2018 there were 834 fatalities from 174,269 single-substance exposure to analgesics, which include opioids and acetaminophen, for a mortality rate of 0.5%.16 The opioid epidemic is one of the main drivers of the increase in drug overdose deaths in the US.16,17 The opioid with the highest drug overdose fatality rate is illicitly manufactured fentanyl, which often is combined with other substances, such as heroin, to increase its potency at a low cost.18 These combinations also increase the risk of overdose fatality.
Acetaminophen is unique among the top substances associated with fatalities because it is obtained easily without a prescription. An acetaminophen overdose can cause hepatic injury, which may progress to fulminant hepatic failure and death.19 The recommended maximum dose of acetaminophen is 4 g/d in an adult and 50 to 75 mg/kg/d in children. A single acute ingestion of > 7.5 g in an adult or 150 mg/kg in children has been considered potentially toxic.19,20 The use of combination analgesics that contain both an opioid and acetaminophen can pose an even greater risk due to the potential for respiratory depression and hepatotoxicity.
Cardiovascular drugs accounted for 232 fatalities from 46,499 single-substance exposures (mortality rate: 0.5%).16 According to the AAPCC, calcium channel blockers (CCB) and β-blockers accounted for 63% of overdose deaths by cardiovascular drugs because they can cause severe hypotension, bradycardia, and hemodynamic collapse.16,21,22
In the past, the nondihydropyridine CCBs verapamil and diltiazem were associated with increased overdose fatalities. However, the most recent data show that dihydropyridine CCBs such as amlodipine also have significant risk for lethality.16 Metoprolol was associated with more overdose deaths in the past year among β-blockers. However, caution also should be used with agents such as propranolol and labetalol, which can antagonize sodium channels in overdose and may be associated with a higher risk of mortality than other β-blockers.22
Antidepressants accounted for 144 fatalities from 56,891 single-substance exposures (mortality rate: 0.3%).16 Nelson and Spyker performed a study to determine the morbidity and mortality index for psychotropic agents based on exposure reports from the National Poison Data system and found that tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) had the highest morbidity and mortality rates among all drugs used to treat depression.23 As a class, TCAs have a mortality index of 40.7 per 10,000 exposures and are associated with higher rates of acidosis, cardiac conduction problems, respiratory depression, and seizures (Table 2).23 Amitriptyline accounted for 39.5% of deaths from antidepressants.23 Among newer antidepressants, citalopram, venlafaxine, and bupropion have been found to be the most hazardous.23 Citalopram and venlafaxine have morbidity indices that are 4- to 5-fold higher than sertraline. Adverse events associated with bupropion, venlafaxine, and citalopram, such as seizures, conduction disturbances, hallucinations, and tachycardia contribute to the morbidity and mortality related to these medications (Table 3).
Of the atypical antipsychotics, olanzapine, quetiapine, and ziprasidone have the highest mortality rates.23 Cardiac conduction problems were more frequent with olanzapine and ziprasidone, and respiratory depression was more frequent with olanzapine and quetiapine. Aripiprazole had the lowest rates of morbidity and mortality.23
Of the mood stabilizers, lithium, valproic acid, and carbamazepine have narrow therapeutic indices and, therefore, moderately high mortality rates.23 Lithium was associated with higher rates of bradycardia, confusion, and renal problems. Valproic acid had relatively high levels of acidosis and coma. Carbamazepine had high rates of coma and the highest rate of nystagmus.
Sedatives and hypnotics accounted for 97 fatalities of 51,495 single-substance exposures (mortality rate 0.2%).16 Within this category, benzodiazepines (BZDs), particularly alprazolam, clonazepam, and diazepam, were associated with the highest number of overdose deaths.16 Although fatalities from single-substance exposure to this category are low, it should be noted that BZDs are primarily metabolized by the CYP2C19 and CYP3A4 enzymes. Interactions with other drugs also metabolized by the same CYP enzymes may lead to prolonged effects of BZDs, such as sedation, and respiratory depression, which significantly increase the risk of overdose death. Furthermore, lipophilic BZDs, such as diazepam, can accumulate in the tissue after multiple doses and have impaired clearance in older patients.
Step 3: Consider Potential Drug-Drug Interactions
Suicide attempts involving multiple substances carry increased risk. Only 12.1% of all fatal overdoses, according to AAPCC, involved single-substance exposure, whereas 56.3% were attributed to multiple substance exposures.16 It is important for clinicians to be aware of and avoid possibly fatal drug-drug interactions, such as the combination of opioids and sedative-hypnotics, like BZDs, which can lead to fatal respiratory depression. Clinicians also should be aware of a patient’s history of illicit opioid and alcohol use before prescribing opioids and BZDs. Clinicians can use various online databases to detect potential drug-drug interactions.
Step 4: Address Risks
If a patient is deemed to be at high risk for suicide, but it is not imminent and the patient will be managed as an outpatient, then it may be preferential to prescribe medications that are less lethal, such as SSRIs, instead of TCAs or MAOIs. If a potentially lethal medication is indicated, such as lithium or clozapine, both of which have been found to reduce suicidal behavior, then dispensing a limited quantity of pills and having more frequent follow-up visits are some ways to lessen risk.24,25 A clinical pearl published in Current Psychiatry provided an equation to determine the lethality of a 30-day supply of medications.26 This equation uses lethal dose 50 (LD50), which is the dose of a medication that results in the death of 50% of the animals used in a controlled experiment, and the maximum daily dose of the medication (D) to find the human equivalent dose (HED) relative lethality. The HED relative lethality calculation may help prescribers determine which medications should have a limited quantity dispensed to patients at risk of medication-related suicide. Any value for the HED relative lethality that is > 100% is considered a lethal dose for humans. Therefore, it would be appropriate to avoid or limit the quantity of medications with a HED relative lethality > 100%. Table 4 lists the psychotropic agents with the highest relative lethality for a 30-day supply. The psychotropic agents with the lowest HED relative lethality are SSRIs: desvenlafaxine, mirtazapine, topiramate, and aripiprazole.26
![]()
Limiting drugs with a narrow therapeutic index should be considered when aiming to reduce the risk of medication-related suicide. These drugs present a high risk in the event of an overdose. Clinicians can monitor the levels of lithium, clozapine, or TCAs to ensure that a patient is taking the medication as prescribed rather than stockpiling it at home. If the patient is in a monitored setting, such as a partial hospital program or intensive outpatient program, then the medication can be given while under direct observation.
Clinicians should obtain an accurate and detailed medication and illicit drug use history from patients. It also is important to review the prescription drug monitoring program to limit access to potentially lethal combinations of medications.27 Clinicians can additionally employ risk mitigation strategies (eg, providing naloxone kits) for patients who are prescribed or abuse opioids.
Finally, all patients with a high risk of suicide should receive lethal means counseling, which involves first determining whether patients have access to lethal means, such as firearms or medications with high lethality, then limiting their access to these lethal means. This includes advising patients and family members to safely dispose medications that are no longer in use and in some cases recommending that a family member keep medications locked and dispense them on a daily basis.
Conclusions
Suicide is a major public health concern that affects tens of thousands of Americans annually. Furthermore, veterans are more likely to die by suicide than those in the general population. Firearms continue to be the most lethal means for suicide. However, intentional poisoning with medications or substances also is a common method for suicide, especially in female veterans. Having knowledge of medications with high lethality and limiting access to these agents can be a successful strategy for reducing suicide deaths.
Suicide is a global phenomenon and a worldwide public health concern.1 The World Health Organization estimates that > 800,000 people die by suicide every year. In the US, suicide is the 10th leading cause of death, and on average, 129 Americans die by suicide each day.2 In 2018, the suicide rate for all veterans was 1.5 times higher than the rate for nonveterans, after adjusting for population differences in age and sex. Among female veterans, the rate of suicide was 2.1 times higher than the rate for female nonveterans.3
In light of this disparity, suicide prevention is one of the highest priorities for the US Department of Veterans Affairs (VA). In 2018, the VA developed and published the National Strategy for Preventing Veteran Suicide.4 One major goal of this strategy is to reduce access to lethal means (ie, firearms, medications, chemicals, or poisons) among veterans at high risk for suicide. Reducing access to lethal means has been found to decrease suicide rates.4,5
Drug overdose is a leading method for suicide attempts, especially for female veterans.3,6 Although the overall case fatality ratio for overdose is < 2%, drug overdose accounted for 59.4% of suicide attempts and 13.5% of deaths by suicide from 2007 to 2014.6,7 Within the veteran population, the majority of suicide deaths in 2018 were due to self-inflicted firearm injury for both male and female veterans, followed by poisoning via substances and pharmaceutical agents for female veterans (Figure 1).3 Notably, when compared with men, women were more likely to choose drug overdose as a method for suicide. One study found that women aged < 45 years used drug and poison ingestion in 9 out of 10 suicide attempts.6 Since some medications are more lethal than others, interventions to limit the availability of lethal medications may prevent deaths and reduce the severity of suicide attempts. This article will provide a stepwise approach to help clinicians identify and limit lethal medications for patients at high risk for suicide.
Step 1: Determine Suicide Risk
Although it is impossible to predict with certainty an individual’s risk of suicide, several patient characteristics and life circumstances have been identified as risk factors. The strongest predictor of suicide is the presence of psychiatric disease.8 More than 90% of those who have had a death by suicide have a psychiatric diagnosis at the time of death, and suicide rates in those with mental illness are at least 10 times as high as in the general population.9,10 Depression is the leading cause of death by suicide worldwide, followed by substance-related disorders (22.4%), personality disorders (11.6%), schizophrenia (10.6%), and anxiety/somatoform disorders (6.1%).8,11-13
Clinicians also can use various risk assessment tools to identify patients at high risk for suicide. The Veterans Health Administration (VHA) Stratification Tool for Opioid Risk Mitigation (STORM) calculates patients’ risk based on data extracted from the electronic health record and is less time intensive, more easily refined, and may be more powerful than standard risk assessment tools because it can be deployed on a large scale.14,15 The VHA also developed the Suicide Prevention Population Risk Identification and Tracking for Exigencies (SPPRITE) tool to assist clinicians in tracking patients with current (or recent) high levels of suicide risk. This tool unifies specific patient information gathered from the patient’s electronic health record and from other predictive model dashboards (such as STORM).
Step 2: Identify Substances Strongly Associated With Fatalities
According to the American Association of Poison Control Centers (AAPCC), the pharmaceutical classes associated with the largest number of fatalities are analgesics, followed by stimulants and street drugs, cardiovascular agents, antidepressants, antipsychotics, and sedatives/hypnotics (Table 1).16 Stimulants and street drugs accounted for 694 fatalities of 39,238 single-substance exposures (mortality rate: 1.8%).16 Drugs of abuse, including cocaine, hallucinogenic amphetamines, heroin, and kratom, have shown an increased trend in use.16
In 2018 there were 834 fatalities from 174,269 single-substance exposure to analgesics, which include opioids and acetaminophen, for a mortality rate of 0.5%.16 The opioid epidemic is one of the main drivers of the increase in drug overdose deaths in the US.16,17 The opioid with the highest drug overdose fatality rate is illicitly manufactured fentanyl, which often is combined with other substances, such as heroin, to increase its potency at a low cost.18 These combinations also increase the risk of overdose fatality.
Acetaminophen is unique among the top substances associated with fatalities because it is obtained easily without a prescription. An acetaminophen overdose can cause hepatic injury, which may progress to fulminant hepatic failure and death.19 The recommended maximum dose of acetaminophen is 4 g/d in an adult and 50 to 75 mg/kg/d in children. A single acute ingestion of > 7.5 g in an adult or 150 mg/kg in children has been considered potentially toxic.19,20 The use of combination analgesics that contain both an opioid and acetaminophen can pose an even greater risk due to the potential for respiratory depression and hepatotoxicity.
Cardiovascular drugs accounted for 232 fatalities from 46,499 single-substance exposures (mortality rate: 0.5%).16 According to the AAPCC, calcium channel blockers (CCB) and β-blockers accounted for 63% of overdose deaths by cardiovascular drugs because they can cause severe hypotension, bradycardia, and hemodynamic collapse.16,21,22
In the past, the nondihydropyridine CCBs verapamil and diltiazem were associated with increased overdose fatalities. However, the most recent data show that dihydropyridine CCBs such as amlodipine also have significant risk for lethality.16 Metoprolol was associated with more overdose deaths in the past year among β-blockers. However, caution also should be used with agents such as propranolol and labetalol, which can antagonize sodium channels in overdose and may be associated with a higher risk of mortality than other β-blockers.22
Antidepressants accounted for 144 fatalities from 56,891 single-substance exposures (mortality rate: 0.3%).16 Nelson and Spyker performed a study to determine the morbidity and mortality index for psychotropic agents based on exposure reports from the National Poison Data system and found that tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) had the highest morbidity and mortality rates among all drugs used to treat depression.23 As a class, TCAs have a mortality index of 40.7 per 10,000 exposures and are associated with higher rates of acidosis, cardiac conduction problems, respiratory depression, and seizures (Table 2).23 Amitriptyline accounted for 39.5% of deaths from antidepressants.23 Among newer antidepressants, citalopram, venlafaxine, and bupropion have been found to be the most hazardous.23 Citalopram and venlafaxine have morbidity indices that are 4- to 5-fold higher than sertraline. Adverse events associated with bupropion, venlafaxine, and citalopram, such as seizures, conduction disturbances, hallucinations, and tachycardia contribute to the morbidity and mortality related to these medications (Table 3).
Of the atypical antipsychotics, olanzapine, quetiapine, and ziprasidone have the highest mortality rates.23 Cardiac conduction problems were more frequent with olanzapine and ziprasidone, and respiratory depression was more frequent with olanzapine and quetiapine. Aripiprazole had the lowest rates of morbidity and mortality.23
Of the mood stabilizers, lithium, valproic acid, and carbamazepine have narrow therapeutic indices and, therefore, moderately high mortality rates.23 Lithium was associated with higher rates of bradycardia, confusion, and renal problems. Valproic acid had relatively high levels of acidosis and coma. Carbamazepine had high rates of coma and the highest rate of nystagmus.
Sedatives and hypnotics accounted for 97 fatalities of 51,495 single-substance exposures (mortality rate 0.2%).16 Within this category, benzodiazepines (BZDs), particularly alprazolam, clonazepam, and diazepam, were associated with the highest number of overdose deaths.16 Although fatalities from single-substance exposure to this category are low, it should be noted that BZDs are primarily metabolized by the CYP2C19 and CYP3A4 enzymes. Interactions with other drugs also metabolized by the same CYP enzymes may lead to prolonged effects of BZDs, such as sedation, and respiratory depression, which significantly increase the risk of overdose death. Furthermore, lipophilic BZDs, such as diazepam, can accumulate in the tissue after multiple doses and have impaired clearance in older patients.
Step 3: Consider Potential Drug-Drug Interactions
Suicide attempts involving multiple substances carry increased risk. Only 12.1% of all fatal overdoses, according to AAPCC, involved single-substance exposure, whereas 56.3% were attributed to multiple substance exposures.16 It is important for clinicians to be aware of and avoid possibly fatal drug-drug interactions, such as the combination of opioids and sedative-hypnotics, like BZDs, which can lead to fatal respiratory depression. Clinicians also should be aware of a patient’s history of illicit opioid and alcohol use before prescribing opioids and BZDs. Clinicians can use various online databases to detect potential drug-drug interactions.
Step 4: Address Risks
If a patient is deemed to be at high risk for suicide, but it is not imminent and the patient will be managed as an outpatient, then it may be preferential to prescribe medications that are less lethal, such as SSRIs, instead of TCAs or MAOIs. If a potentially lethal medication is indicated, such as lithium or clozapine, both of which have been found to reduce suicidal behavior, then dispensing a limited quantity of pills and having more frequent follow-up visits are some ways to lessen risk.24,25 A clinical pearl published in Current Psychiatry provided an equation to determine the lethality of a 30-day supply of medications.26 This equation uses lethal dose 50 (LD50), which is the dose of a medication that results in the death of 50% of the animals used in a controlled experiment, and the maximum daily dose of the medication (D) to find the human equivalent dose (HED) relative lethality. The HED relative lethality calculation may help prescribers determine which medications should have a limited quantity dispensed to patients at risk of medication-related suicide. Any value for the HED relative lethality that is > 100% is considered a lethal dose for humans. Therefore, it would be appropriate to avoid or limit the quantity of medications with a HED relative lethality > 100%. Table 4 lists the psychotropic agents with the highest relative lethality for a 30-day supply. The psychotropic agents with the lowest HED relative lethality are SSRIs: desvenlafaxine, mirtazapine, topiramate, and aripiprazole.26
![]()
Limiting drugs with a narrow therapeutic index should be considered when aiming to reduce the risk of medication-related suicide. These drugs present a high risk in the event of an overdose. Clinicians can monitor the levels of lithium, clozapine, or TCAs to ensure that a patient is taking the medication as prescribed rather than stockpiling it at home. If the patient is in a monitored setting, such as a partial hospital program or intensive outpatient program, then the medication can be given while under direct observation.
Clinicians should obtain an accurate and detailed medication and illicit drug use history from patients. It also is important to review the prescription drug monitoring program to limit access to potentially lethal combinations of medications.27 Clinicians can additionally employ risk mitigation strategies (eg, providing naloxone kits) for patients who are prescribed or abuse opioids.
Finally, all patients with a high risk of suicide should receive lethal means counseling, which involves first determining whether patients have access to lethal means, such as firearms or medications with high lethality, then limiting their access to these lethal means. This includes advising patients and family members to safely dispose medications that are no longer in use and in some cases recommending that a family member keep medications locked and dispense them on a daily basis.
Conclusions
Suicide is a major public health concern that affects tens of thousands of Americans annually. Furthermore, veterans are more likely to die by suicide than those in the general population. Firearms continue to be the most lethal means for suicide. However, intentional poisoning with medications or substances also is a common method for suicide, especially in female veterans. Having knowledge of medications with high lethality and limiting access to these agents can be a successful strategy for reducing suicide deaths.
1. World Health Organization. Preventing suicide: a global imperative. Published 2014. Accessed January 16, 2021. https://apps.who.int/iris/bitstream/handle/10665/131056/9789241564779_eng.pdf
2. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention. National Violent Death Reporting System (NVDRS). Updated November 7, 2019. Accessed January 7, 2021. https://www.cdc.gov/violenceprevention/datasources/nvdrs/
3. US Department of Veteran Affairs, Office of Mental Health and Suicide Prevention. 2020 national veteran suicide prevention annual report. Accessed January 16, 2021. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
4. US Department of Veteran Affairs. National strategy for preventing veteran suicide 2018-2028. Accessed January 7, 2021. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
5. Zalsman G, Hawton K, Wasserman D, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. 2016;3(7):646-659. doi:10.1016/S2215-0366(16)30030-X
6. Spicer RS, Miller TR. Suicide acts in 8 states: incidence and case fatality rates by demographics and method. Am J Public Health. 2000;90(12):1885-1891. doi:10.2105/ajph.90.12.1885
7. Conner A, Azrael D, Miller M. Suicide Case-Fatality Rates in the United States, 2007 to 2014: A Nationwide Population-Based Study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
8. Bertolote JM, Fleischmann A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry. 2002;1(3):181-185.
9. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics. 1999;40(1):18-27. doi:10.1016/S0033-3182(99)71267-3
10. Bachmann S. Epidemiology of Suicide and the Psychiatric Perspective. Int J Environ Res Public Health. 2018;15(7):1425. Published 2018 Jul 6. doi:10.3390/ijerph15071425
11. Hoertel N, Franco S, Wall MM, et al. Mental disorders and risk of suicide attempt: a national prospective study. Mol Psychiatry. 2015;20(6):718-726. doi:10.1038/mp.2015.19
12. Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013;10(11):e1001547. doi:10.1371/journal.pmed.1001547
13. World Health Organization. Mental health atlas. Accessed January 7, 2021. https://apps.who.int/iris/bitstream/handle/10665/178879/9789241565011_eng.pdf
14. Velupillai S, Hadlaczky G, Baca-Garcia E, et al. Risk assessment tools and data-driven approaches for predicting and preventing suicidal behavior. Front Psychiatry. 2019;10:36. Published 2019 Feb 13. doi:10.3389/fpsyt.2019.00036
15. Oliva EM, Bowe T, Tavakoli S, et al. Development and applications of the Veterans Health Administration’s Stratification Tool for Opioid Risk Mitigation (STORM) to improve opioid safety and prevent overdose and suicide. Psychol Serv. 2017;14(1):34-49. doi:10.1037/ser0000099
16. Gummin DD, Mowry JB, Spyker DA, et al. 2018 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 36th Annual Report [published correction appears in Clin Toxicol (Phila). 2019 Dec;57(12):e1]. Clin Toxicol (Phila). 2019;57(12):1220-1413. doi:10.1080/15563650.2019.1677022
17. Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999–2018. NCHS Data Brief. 2020(356).
18. Kuczyn´ska K, Grzonkowski P, Kacprzak Ł, Zawilska JB. Abuse of fentanyl: An emerging problem to face. Forensic Sci Int. 2018;289:207-214. doi:10.1016/j.forsciint.2018.05.042
19. Hodgman MJ, Garrard AR. A review of acetaminophen poisoning. Crit Care Clin. 2012;28(4):499-516. doi:10.1016/j.ccc.2012.07.006
20. Chiew AL, Gluud C, Brok J, Buckley NA. Interventions for paracetamol (acetaminophen) overdose. Cochrane Database Syst Rev. 2018;2(2):CD003328. Published 2018 Feb 23. doi:10.1002/14651858.CD003328.pub3
21. Graudins A, Lee HM, Druda D. Calcium channel antagonist and beta-blocker overdose: antidotes and adjunct therapies. Br J Clin Pharmacol. 2016;81(3):453-461. doi:10.1111/bcp.12763
22. DeWitt CR, Waksman JC. Pharmacology, pathophysiology and management of calcium channel blocker and beta-blocker toxicity. Toxicol Rev. 2004;23(4):223-238. doi:10.2165/00139709-200423040-00003
23. Nelson JC, Spyker DA. Morbidity and mortality associated with medications used in the treatment of depression: an analysis of cases reported to U.S. Poison Control Centers, 2000-2014. Am J Psychiatry. 2017;174(5):438-450. doi:10.1176/appi.ajp.2016.16050523
24. Sarai SK, Mekala HM, Lippmann S. Lithium suicide prevention: a brief review and reminder. Innov Clin Neurosci. 2018;15(11-12):30-32.
25. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) [published correction appears in Arch Gen Psychiatry. 2003 Jul;60(7):735]. Arch Gen Psychiatry. 2003;60(1):82-91. doi:10.1001/archpsyc.60.1.82
26. Giurca D. Decreasing suicide risk with math. Curr Psychiatry. 2018;17(2):57-61.
27. Malte CA, Berger D, Saxon AJ, et al. Electronic medical record alert associated with reduced opioid and benzodiazepine coprescribing in high-risk veteran patients. Med Care. 2018;56(2):171-178. doi:10.1097/MLR.0000000000000861
1. World Health Organization. Preventing suicide: a global imperative. Published 2014. Accessed January 16, 2021. https://apps.who.int/iris/bitstream/handle/10665/131056/9789241564779_eng.pdf
2. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention. National Violent Death Reporting System (NVDRS). Updated November 7, 2019. Accessed January 7, 2021. https://www.cdc.gov/violenceprevention/datasources/nvdrs/
3. US Department of Veteran Affairs, Office of Mental Health and Suicide Prevention. 2020 national veteran suicide prevention annual report. Accessed January 16, 2021. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
4. US Department of Veteran Affairs. National strategy for preventing veteran suicide 2018-2028. Accessed January 7, 2021. https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
5. Zalsman G, Hawton K, Wasserman D, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. 2016;3(7):646-659. doi:10.1016/S2215-0366(16)30030-X
6. Spicer RS, Miller TR. Suicide acts in 8 states: incidence and case fatality rates by demographics and method. Am J Public Health. 2000;90(12):1885-1891. doi:10.2105/ajph.90.12.1885
7. Conner A, Azrael D, Miller M. Suicide Case-Fatality Rates in the United States, 2007 to 2014: A Nationwide Population-Based Study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
8. Bertolote JM, Fleischmann A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry. 2002;1(3):181-185.
9. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics. 1999;40(1):18-27. doi:10.1016/S0033-3182(99)71267-3
10. Bachmann S. Epidemiology of Suicide and the Psychiatric Perspective. Int J Environ Res Public Health. 2018;15(7):1425. Published 2018 Jul 6. doi:10.3390/ijerph15071425
11. Hoertel N, Franco S, Wall MM, et al. Mental disorders and risk of suicide attempt: a national prospective study. Mol Psychiatry. 2015;20(6):718-726. doi:10.1038/mp.2015.19
12. Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013;10(11):e1001547. doi:10.1371/journal.pmed.1001547
13. World Health Organization. Mental health atlas. Accessed January 7, 2021. https://apps.who.int/iris/bitstream/handle/10665/178879/9789241565011_eng.pdf
14. Velupillai S, Hadlaczky G, Baca-Garcia E, et al. Risk assessment tools and data-driven approaches for predicting and preventing suicidal behavior. Front Psychiatry. 2019;10:36. Published 2019 Feb 13. doi:10.3389/fpsyt.2019.00036
15. Oliva EM, Bowe T, Tavakoli S, et al. Development and applications of the Veterans Health Administration’s Stratification Tool for Opioid Risk Mitigation (STORM) to improve opioid safety and prevent overdose and suicide. Psychol Serv. 2017;14(1):34-49. doi:10.1037/ser0000099
16. Gummin DD, Mowry JB, Spyker DA, et al. 2018 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 36th Annual Report [published correction appears in Clin Toxicol (Phila). 2019 Dec;57(12):e1]. Clin Toxicol (Phila). 2019;57(12):1220-1413. doi:10.1080/15563650.2019.1677022
17. Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999–2018. NCHS Data Brief. 2020(356).
18. Kuczyn´ska K, Grzonkowski P, Kacprzak Ł, Zawilska JB. Abuse of fentanyl: An emerging problem to face. Forensic Sci Int. 2018;289:207-214. doi:10.1016/j.forsciint.2018.05.042
19. Hodgman MJ, Garrard AR. A review of acetaminophen poisoning. Crit Care Clin. 2012;28(4):499-516. doi:10.1016/j.ccc.2012.07.006
20. Chiew AL, Gluud C, Brok J, Buckley NA. Interventions for paracetamol (acetaminophen) overdose. Cochrane Database Syst Rev. 2018;2(2):CD003328. Published 2018 Feb 23. doi:10.1002/14651858.CD003328.pub3
21. Graudins A, Lee HM, Druda D. Calcium channel antagonist and beta-blocker overdose: antidotes and adjunct therapies. Br J Clin Pharmacol. 2016;81(3):453-461. doi:10.1111/bcp.12763
22. DeWitt CR, Waksman JC. Pharmacology, pathophysiology and management of calcium channel blocker and beta-blocker toxicity. Toxicol Rev. 2004;23(4):223-238. doi:10.2165/00139709-200423040-00003
23. Nelson JC, Spyker DA. Morbidity and mortality associated with medications used in the treatment of depression: an analysis of cases reported to U.S. Poison Control Centers, 2000-2014. Am J Psychiatry. 2017;174(5):438-450. doi:10.1176/appi.ajp.2016.16050523
24. Sarai SK, Mekala HM, Lippmann S. Lithium suicide prevention: a brief review and reminder. Innov Clin Neurosci. 2018;15(11-12):30-32.
25. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) [published correction appears in Arch Gen Psychiatry. 2003 Jul;60(7):735]. Arch Gen Psychiatry. 2003;60(1):82-91. doi:10.1001/archpsyc.60.1.82
26. Giurca D. Decreasing suicide risk with math. Curr Psychiatry. 2018;17(2):57-61.
27. Malte CA, Berger D, Saxon AJ, et al. Electronic medical record alert associated with reduced opioid and benzodiazepine coprescribing in high-risk veteran patients. Med Care. 2018;56(2):171-178. doi:10.1097/MLR.0000000000000861
The journey from burnout to wellbeing
A check-in for you and your peers
COVID-19 did not discriminate when it came to the impact it imposed on our hospitalist community. As the nomenclature moves away from the negative connotations of ‘burnout’ to ‘wellbeing,’ the pandemic has taught us something important about being intentional about our personal health: we must secure our own oxygen masks before helping others.

In February 2020, the Society of Hospital Medicine’s Wellbeing Taskforce efforts quickly changed focus from addressing general wellbeing, to wellbeing during COVID-19. Our Taskforce was commissioned by SHM’s Board with a new charge: Address immediate and ongoing needs of well-being and resiliency support for hospitalists during the COVID-19 pandemic. In this essay, I will discuss how our SHM Wellbeing Taskforce approached the overall topic of wellbeing for hospitalists during the COVID-19 pandemic, including some of our Taskforce group experiences.
The Taskforce started with a framework to aide in cultivating open and authentic conversations within hospital medicine groups. Creating spaces for honest sharing around how providers are doing is a crucial first step to reducing stigma, building mutual support within a group, and elevating issues of wellbeing to the level where structural change can take place. The Taskforce established two objectives for normalizing and mitigating stressors we face as hospitalists during the COVID-19 pandemic:
- Provide a framework for hospitalists to take their own emotional pulse
- Provide an approach to reduce stigma of hospitalists who are suffering from pandemic stress
While a more typical approach to fix stress and burnout is using formal institutional interventions, we used the value and insight provided by SHM’s 7 Drivers of Burnout in Hospital Medicine to help guide the creation of SHM resources in addressing the severe emotional strain being felt across the country by hospitalists. The 7 Drivers support the idea that the social role peers and hospital leaders can make a crucial difference in mitigating stress and burnout. Two examples of social support come to mind from the Wellbeing Taskforce experience:
- Participate in your meetings. One example comes from a member of our group who had underestimated the “healing power” that our group meetings had provided to his psyche. The simple act of participating in our Taskforce meeting and being in the presence of our group had provided such a positive impact that he was better able to face the “death and misery” in his unit with a smile on his face.
- Share what is stressful. The second example of social support comes from an hour of Zoom-based facilitation meetings between the SHM’s Wellbeing Taskforce members and Chapter Leaders in late October. During our Taskforce debrief after the meeting, we came to realize the enormous burden of grief our peers were carrying as one hospitalist had lost a group colleague the previous week due to suicide. Our member who led this meeting was moved – as were we – at how this had impacted his small team, and he was reminded he was not alone.
To form meaningful relationships that foster support, there needs to be a space where people can safely come together at times that initially might feel awkward. After taking steps toward your peers, these conversations can become normalized and contribute to meaningful relationships, providing the opportunity for healthy exchanges on vulnerable topics like emotional and psychological wellbeing. A printable guide for this specific purpose (“HM COVID-19 Check-In Guide for Self and Peers”) was designed to help hospitalists move into safe and supportive conversations with each other. While it is difficult to place a value on the importance these types of conversations have on individual wellbeing, it is known that the quality of a positive work environment where people feel supported can moderate stress, morale, and depression. In other words, hospitalist groups can positively contribute to their social environment during stressful times by sharing meaningful and difficult experiences with one another.
Second, the Taskforce created a social media campaign to provide a public social space for sharing hospitalists’ COVID-19 experiences. We believed that sharing collective experiences with the theme of #YouAreNotAlone and a complementary social media campaign, SHM Cares, on SHM’s social media channels, would further connect the national hospitalist community and provide a different communication pathway to decrease a sense of isolation. This idea came from the second social support idea mentioned earlier to share what is stressful with others in a safe space. We understood that some hospitalists would be more comfortable sharing publicly their comments, photos, and videos in achieving a sense of hospitalist unity.
Using our shared experiences, we identified three pillars for the final structure of the HM COVID-19 Check-In Guide for Self and Peers:
- Pillar 1. Recognize your issues. Recall our oxygen mask metaphor and this is what we mean by recognizing symptoms of new stressors (e.g., sleeplessness, irritability, forgetfulness).
- Pillar 2. Know what to say. A simple open-ended question about how the other person is working through the pandemic is an easy way to start a connection. We learned from a mental health perspective that it is unlikely that you could say anything to make a situation worse by offering a listening ear.
- Pillar 3. Check in with others. Listen to others without trying to fix the person or the situation. When appropriate, offer humorous reflections without diminishing the problem. Be a partner and commit to check in regularly with the other person.
Cultivating human connections outside of your immediate peer group can be valuable and offer additional perspective to stressful situations. For instance, one of my roles as a hospitalist administrator has been offering support by regularly listening as my physicians ‘talk out’ their day confidentially for as long as they needed. Offering open conversation in a safe and confidential way can have a healing effect. As one of my former hospitalists used to say, if issues are not addressed, they will “ooze out somewhere else.”
The HM COVID-19 Check-In Guide for Self and Peers and the SHM Cares social media campaign was the result of the Taskforce’s collective observations to help others normalize the feeling that ‘it’s OK not to be OK.’ Using the pandemic as context, the 7 Drivers of Hospitalist Burnout reminded us that the increased burnout issues we face will require continued attention past the pandemic. The value in cultivating human connections has never been more important. The SHM Wellbeing Taskforce is committed to provide continued resources. Checking in with others and listening to peers are all part of a personal wellbeing and resilience strategy. On behalf of the SHM Wellbeing Taskforce, we hope the information in this article will highlight the importance of continued attention to personal wellbeing during and after the pandemic.
Dr. Robinson received her PhD in organizational learning, performance and change from Colorado State University in 2019. Her dissertation topic was exploring hospitalist burnout, engagement, and social support. She is administrative director of inpatient medicine at St. Mary’s Medical Center in Grand Junction, Colo., a part of SCL Health. She has volunteered in numerous SHM committees, and currently serves on the SHM Wellbeing Taskforce.
A check-in for you and your peers
A check-in for you and your peers
COVID-19 did not discriminate when it came to the impact it imposed on our hospitalist community. As the nomenclature moves away from the negative connotations of ‘burnout’ to ‘wellbeing,’ the pandemic has taught us something important about being intentional about our personal health: we must secure our own oxygen masks before helping others.
In February 2020, the Society of Hospital Medicine’s Wellbeing Taskforce efforts quickly changed focus from addressing general wellbeing, to wellbeing during COVID-19. Our Taskforce was commissioned by SHM’s Board with a new charge: Address immediate and ongoing needs of well-being and resiliency support for hospitalists during the COVID-19 pandemic. In this essay, I will discuss how our SHM Wellbeing Taskforce approached the overall topic of wellbeing for hospitalists during the COVID-19 pandemic, including some of our Taskforce group experiences.
The Taskforce started with a framework to aide in cultivating open and authentic conversations within hospital medicine groups. Creating spaces for honest sharing around how providers are doing is a crucial first step to reducing stigma, building mutual support within a group, and elevating issues of wellbeing to the level where structural change can take place. The Taskforce established two objectives for normalizing and mitigating stressors we face as hospitalists during the COVID-19 pandemic:
- Provide a framework for hospitalists to take their own emotional pulse
- Provide an approach to reduce stigma of hospitalists who are suffering from pandemic stress
While a more typical approach to fix stress and burnout is using formal institutional interventions, we used the value and insight provided by SHM’s 7 Drivers of Burnout in Hospital Medicine to help guide the creation of SHM resources in addressing the severe emotional strain being felt across the country by hospitalists. The 7 Drivers support the idea that the social role peers and hospital leaders can make a crucial difference in mitigating stress and burnout. Two examples of social support come to mind from the Wellbeing Taskforce experience:
- Participate in your meetings. One example comes from a member of our group who had underestimated the “healing power” that our group meetings had provided to his psyche. The simple act of participating in our Taskforce meeting and being in the presence of our group had provided such a positive impact that he was better able to face the “death and misery” in his unit with a smile on his face.
- Share what is stressful. The second example of social support comes from an hour of Zoom-based facilitation meetings between the SHM’s Wellbeing Taskforce members and Chapter Leaders in late October. During our Taskforce debrief after the meeting, we came to realize the enormous burden of grief our peers were carrying as one hospitalist had lost a group colleague the previous week due to suicide. Our member who led this meeting was moved – as were we – at how this had impacted his small team, and he was reminded he was not alone.
To form meaningful relationships that foster support, there needs to be a space where people can safely come together at times that initially might feel awkward. After taking steps toward your peers, these conversations can become normalized and contribute to meaningful relationships, providing the opportunity for healthy exchanges on vulnerable topics like emotional and psychological wellbeing. A printable guide for this specific purpose (“HM COVID-19 Check-In Guide for Self and Peers”) was designed to help hospitalists move into safe and supportive conversations with each other. While it is difficult to place a value on the importance these types of conversations have on individual wellbeing, it is known that the quality of a positive work environment where people feel supported can moderate stress, morale, and depression. In other words, hospitalist groups can positively contribute to their social environment during stressful times by sharing meaningful and difficult experiences with one another.
Second, the Taskforce created a social media campaign to provide a public social space for sharing hospitalists’ COVID-19 experiences. We believed that sharing collective experiences with the theme of #YouAreNotAlone and a complementary social media campaign, SHM Cares, on SHM’s social media channels, would further connect the national hospitalist community and provide a different communication pathway to decrease a sense of isolation. This idea came from the second social support idea mentioned earlier to share what is stressful with others in a safe space. We understood that some hospitalists would be more comfortable sharing publicly their comments, photos, and videos in achieving a sense of hospitalist unity.
Using our shared experiences, we identified three pillars for the final structure of the HM COVID-19 Check-In Guide for Self and Peers:
- Pillar 1. Recognize your issues. Recall our oxygen mask metaphor and this is what we mean by recognizing symptoms of new stressors (e.g., sleeplessness, irritability, forgetfulness).
- Pillar 2. Know what to say. A simple open-ended question about how the other person is working through the pandemic is an easy way to start a connection. We learned from a mental health perspective that it is unlikely that you could say anything to make a situation worse by offering a listening ear.
- Pillar 3. Check in with others. Listen to others without trying to fix the person or the situation. When appropriate, offer humorous reflections without diminishing the problem. Be a partner and commit to check in regularly with the other person.
Cultivating human connections outside of your immediate peer group can be valuable and offer additional perspective to stressful situations. For instance, one of my roles as a hospitalist administrator has been offering support by regularly listening as my physicians ‘talk out’ their day confidentially for as long as they needed. Offering open conversation in a safe and confidential way can have a healing effect. As one of my former hospitalists used to say, if issues are not addressed, they will “ooze out somewhere else.”
The HM COVID-19 Check-In Guide for Self and Peers and the SHM Cares social media campaign was the result of the Taskforce’s collective observations to help others normalize the feeling that ‘it’s OK not to be OK.’ Using the pandemic as context, the 7 Drivers of Hospitalist Burnout reminded us that the increased burnout issues we face will require continued attention past the pandemic. The value in cultivating human connections has never been more important. The SHM Wellbeing Taskforce is committed to provide continued resources. Checking in with others and listening to peers are all part of a personal wellbeing and resilience strategy. On behalf of the SHM Wellbeing Taskforce, we hope the information in this article will highlight the importance of continued attention to personal wellbeing during and after the pandemic.
Dr. Robinson received her PhD in organizational learning, performance and change from Colorado State University in 2019. Her dissertation topic was exploring hospitalist burnout, engagement, and social support. She is administrative director of inpatient medicine at St. Mary’s Medical Center in Grand Junction, Colo., a part of SCL Health. She has volunteered in numerous SHM committees, and currently serves on the SHM Wellbeing Taskforce.
COVID-19 did not discriminate when it came to the impact it imposed on our hospitalist community. As the nomenclature moves away from the negative connotations of ‘burnout’ to ‘wellbeing,’ the pandemic has taught us something important about being intentional about our personal health: we must secure our own oxygen masks before helping others.
In February 2020, the Society of Hospital Medicine’s Wellbeing Taskforce efforts quickly changed focus from addressing general wellbeing, to wellbeing during COVID-19. Our Taskforce was commissioned by SHM’s Board with a new charge: Address immediate and ongoing needs of well-being and resiliency support for hospitalists during the COVID-19 pandemic. In this essay, I will discuss how our SHM Wellbeing Taskforce approached the overall topic of wellbeing for hospitalists during the COVID-19 pandemic, including some of our Taskforce group experiences.
The Taskforce started with a framework to aide in cultivating open and authentic conversations within hospital medicine groups. Creating spaces for honest sharing around how providers are doing is a crucial first step to reducing stigma, building mutual support within a group, and elevating issues of wellbeing to the level where structural change can take place. The Taskforce established two objectives for normalizing and mitigating stressors we face as hospitalists during the COVID-19 pandemic:
- Provide a framework for hospitalists to take their own emotional pulse
- Provide an approach to reduce stigma of hospitalists who are suffering from pandemic stress
While a more typical approach to fix stress and burnout is using formal institutional interventions, we used the value and insight provided by SHM’s 7 Drivers of Burnout in Hospital Medicine to help guide the creation of SHM resources in addressing the severe emotional strain being felt across the country by hospitalists. The 7 Drivers support the idea that the social role peers and hospital leaders can make a crucial difference in mitigating stress and burnout. Two examples of social support come to mind from the Wellbeing Taskforce experience:
- Participate in your meetings. One example comes from a member of our group who had underestimated the “healing power” that our group meetings had provided to his psyche. The simple act of participating in our Taskforce meeting and being in the presence of our group had provided such a positive impact that he was better able to face the “death and misery” in his unit with a smile on his face.
- Share what is stressful. The second example of social support comes from an hour of Zoom-based facilitation meetings between the SHM’s Wellbeing Taskforce members and Chapter Leaders in late October. During our Taskforce debrief after the meeting, we came to realize the enormous burden of grief our peers were carrying as one hospitalist had lost a group colleague the previous week due to suicide. Our member who led this meeting was moved – as were we – at how this had impacted his small team, and he was reminded he was not alone.
To form meaningful relationships that foster support, there needs to be a space where people can safely come together at times that initially might feel awkward. After taking steps toward your peers, these conversations can become normalized and contribute to meaningful relationships, providing the opportunity for healthy exchanges on vulnerable topics like emotional and psychological wellbeing. A printable guide for this specific purpose (“HM COVID-19 Check-In Guide for Self and Peers”) was designed to help hospitalists move into safe and supportive conversations with each other. While it is difficult to place a value on the importance these types of conversations have on individual wellbeing, it is known that the quality of a positive work environment where people feel supported can moderate stress, morale, and depression. In other words, hospitalist groups can positively contribute to their social environment during stressful times by sharing meaningful and difficult experiences with one another.
Second, the Taskforce created a social media campaign to provide a public social space for sharing hospitalists’ COVID-19 experiences. We believed that sharing collective experiences with the theme of #YouAreNotAlone and a complementary social media campaign, SHM Cares, on SHM’s social media channels, would further connect the national hospitalist community and provide a different communication pathway to decrease a sense of isolation. This idea came from the second social support idea mentioned earlier to share what is stressful with others in a safe space. We understood that some hospitalists would be more comfortable sharing publicly their comments, photos, and videos in achieving a sense of hospitalist unity.
Using our shared experiences, we identified three pillars for the final structure of the HM COVID-19 Check-In Guide for Self and Peers:
- Pillar 1. Recognize your issues. Recall our oxygen mask metaphor and this is what we mean by recognizing symptoms of new stressors (e.g., sleeplessness, irritability, forgetfulness).
- Pillar 2. Know what to say. A simple open-ended question about how the other person is working through the pandemic is an easy way to start a connection. We learned from a mental health perspective that it is unlikely that you could say anything to make a situation worse by offering a listening ear.
- Pillar 3. Check in with others. Listen to others without trying to fix the person or the situation. When appropriate, offer humorous reflections without diminishing the problem. Be a partner and commit to check in regularly with the other person.
Cultivating human connections outside of your immediate peer group can be valuable and offer additional perspective to stressful situations. For instance, one of my roles as a hospitalist administrator has been offering support by regularly listening as my physicians ‘talk out’ their day confidentially for as long as they needed. Offering open conversation in a safe and confidential way can have a healing effect. As one of my former hospitalists used to say, if issues are not addressed, they will “ooze out somewhere else.”
The HM COVID-19 Check-In Guide for Self and Peers and the SHM Cares social media campaign was the result of the Taskforce’s collective observations to help others normalize the feeling that ‘it’s OK not to be OK.’ Using the pandemic as context, the 7 Drivers of Hospitalist Burnout reminded us that the increased burnout issues we face will require continued attention past the pandemic. The value in cultivating human connections has never been more important. The SHM Wellbeing Taskforce is committed to provide continued resources. Checking in with others and listening to peers are all part of a personal wellbeing and resilience strategy. On behalf of the SHM Wellbeing Taskforce, we hope the information in this article will highlight the importance of continued attention to personal wellbeing during and after the pandemic.
Dr. Robinson received her PhD in organizational learning, performance and change from Colorado State University in 2019. Her dissertation topic was exploring hospitalist burnout, engagement, and social support. She is administrative director of inpatient medicine at St. Mary’s Medical Center in Grand Junction, Colo., a part of SCL Health. She has volunteered in numerous SHM committees, and currently serves on the SHM Wellbeing Taskforce.
Antidepressant may help COVID-19 patients avoid serious illness
The antidepressant fluvoxamine shows promise in preventing people infected with coronavirus from developing serious symptoms and having to be hospitalized, according to a nonrandomized study of California racetrack workers.

“What we observed was that of all the patients who received fluvoxamine, none of them had a severe COVID infection that affected their lungs or their respiratory status,” Caline Mattar, MD, told KNBC in Los Angeles. Dr. Mattar is an infectious disease researcher at Washington University in St. Louis who helped conduct the study that was published in Open Forum Infectious Diseases.
Fluvoxamine, which is sold under the brand name Luvox, is a selective serotonin reuptake inhibitor (SSRI) often prescribed for people diagnosed with obsessive-compulsive disorder. It’s been on the market for over a decade.
Two-hundred employees at Golden Gate Fields Racetrack in Berkeley, Calif., tested positive for COVID-19 last November. Track physician David Seftel, MD, offered fluvoxamine to 113 of them, having learned of a previous randomized study of COVID-19 patients that indicated fluvoxamine helped ward off serious illness, Science News said.
The 65 workers who took a 2-week course of the drug didn’t have to be hospitalized, didn’t have serious symptoms, and felt better after 2 weeks, the study said. Six of the 48 workers who turned down fluvoxamine had to be hospitalized, two required intensive care, and one died, the study said.
“Overall, fluvoxamine appears promising as early treatment for COVID-19 to prevent clinical deterioration requiring hospitalization and to prevent possible long haul symptoms persisting beyond 2 weeks,” the study said.
They said their research needed verification from a randomized, controlled trial. Such a study is now being conducted by Washington University and other schools, KNBC said.
The track workers who were infected were predominantly male and Latino, and 30% had chronic medical problems such as diabetes or high blood pressure, Science News said.
A version of this article first appeared on WebMD.com.
The antidepressant fluvoxamine shows promise in preventing people infected with coronavirus from developing serious symptoms and having to be hospitalized, according to a nonrandomized study of California racetrack workers.
“What we observed was that of all the patients who received fluvoxamine, none of them had a severe COVID infection that affected their lungs or their respiratory status,” Caline Mattar, MD, told KNBC in Los Angeles. Dr. Mattar is an infectious disease researcher at Washington University in St. Louis who helped conduct the study that was published in Open Forum Infectious Diseases.
Fluvoxamine, which is sold under the brand name Luvox, is a selective serotonin reuptake inhibitor (SSRI) often prescribed for people diagnosed with obsessive-compulsive disorder. It’s been on the market for over a decade.
Two-hundred employees at Golden Gate Fields Racetrack in Berkeley, Calif., tested positive for COVID-19 last November. Track physician David Seftel, MD, offered fluvoxamine to 113 of them, having learned of a previous randomized study of COVID-19 patients that indicated fluvoxamine helped ward off serious illness, Science News said.
The 65 workers who took a 2-week course of the drug didn’t have to be hospitalized, didn’t have serious symptoms, and felt better after 2 weeks, the study said. Six of the 48 workers who turned down fluvoxamine had to be hospitalized, two required intensive care, and one died, the study said.
“Overall, fluvoxamine appears promising as early treatment for COVID-19 to prevent clinical deterioration requiring hospitalization and to prevent possible long haul symptoms persisting beyond 2 weeks,” the study said.
They said their research needed verification from a randomized, controlled trial. Such a study is now being conducted by Washington University and other schools, KNBC said.
The track workers who were infected were predominantly male and Latino, and 30% had chronic medical problems such as diabetes or high blood pressure, Science News said.
A version of this article first appeared on WebMD.com.
The antidepressant fluvoxamine shows promise in preventing people infected with coronavirus from developing serious symptoms and having to be hospitalized, according to a nonrandomized study of California racetrack workers.
“What we observed was that of all the patients who received fluvoxamine, none of them had a severe COVID infection that affected their lungs or their respiratory status,” Caline Mattar, MD, told KNBC in Los Angeles. Dr. Mattar is an infectious disease researcher at Washington University in St. Louis who helped conduct the study that was published in Open Forum Infectious Diseases.
Fluvoxamine, which is sold under the brand name Luvox, is a selective serotonin reuptake inhibitor (SSRI) often prescribed for people diagnosed with obsessive-compulsive disorder. It’s been on the market for over a decade.
Two-hundred employees at Golden Gate Fields Racetrack in Berkeley, Calif., tested positive for COVID-19 last November. Track physician David Seftel, MD, offered fluvoxamine to 113 of them, having learned of a previous randomized study of COVID-19 patients that indicated fluvoxamine helped ward off serious illness, Science News said.
The 65 workers who took a 2-week course of the drug didn’t have to be hospitalized, didn’t have serious symptoms, and felt better after 2 weeks, the study said. Six of the 48 workers who turned down fluvoxamine had to be hospitalized, two required intensive care, and one died, the study said.
“Overall, fluvoxamine appears promising as early treatment for COVID-19 to prevent clinical deterioration requiring hospitalization and to prevent possible long haul symptoms persisting beyond 2 weeks,” the study said.
They said their research needed verification from a randomized, controlled trial. Such a study is now being conducted by Washington University and other schools, KNBC said.
The track workers who were infected were predominantly male and Latino, and 30% had chronic medical problems such as diabetes or high blood pressure, Science News said.
A version of this article first appeared on WebMD.com.
Higher dietary fiber tied to lower depression risk in young women
Higher fiber intake may be associated with decreased risk of depression in premenopausal women, new research suggests.

Investigators analyzed data from close to 6,000 pre- and postmenopausal women. They found that, in premenopausal women, dietary fiber intake was higher among those without depression versus their counterparts with the disorder in a dose-dependent manner. However, there appeared to be no relationship between higher fiber intake and depression risk in postmenopausal women.
“We think the most important finding of our study is that dietary fiber intake was inversely associated with depression in premenopausal but not postmenopausal women,” lead author Yunsun Kim, MD, resident, department of family medicine, Chung-Ang University Hospital, Seoul, South Korea, said in an interview.
“We hope that the findings of this study could form the basis of future investigations to determine the causal relationship between dietary fiber intake and depression,” she added.
The study was published online Dec. 21, 2020, in Menopause.
Gut-brain interaction
The prevalence of depression is twice as high in women, compared with men, which may be attributable to a number of factors, including hormonal status – especially during menstruation and menopause, the authors wrote.
Previous research suggests a potential association between dietary fiber and depression in premenopausal women and between estrogen and gut microbiota. Fiber intake has an impact on gut microbiota, Dr. Kim said.
“We are motivated by the fact that depression provokes disease burden internationally and we would like to find modifiable factors that could prevent depression, especially in women, who are more vulnerable to depression,” she noted.
To investigate, the researchers drew on data from the Korea National Health and Nutrition Examination Survey for 2014, 2016, and 2018. Of the total number of women who met inclusion criteria (n = 5807; mean age, 47.11), roughly half were premenopausal and half were postmenopausal (n = 2,949 [mean age, 36.23 years] and n = 2,868 [mean age, 62.73], respectively).
Dietary fiber intake was assessed using the 24-hour dietary recall method, while depression was assessed using the Patient Health Questionnaire-9. The researchers used the Dietary Reference Intakes for Koreans to define a sufficient intake of dietary fiber (i.e., 12 g/1,000 kcal).
Covariates included chronic diseases, body mass index, medications, smoking status, alcohol use, physical activity, and sociodemographic factors.
When the researchers looked at all participants, they found that the estimated mean dietary fiber intake was significantly higher in women without depression, compared with those with depression (14.07 g/1,000 kcal/d; 95% confidence interval, 13.85-14.29 vs. 12.67 g/1,000 kcal/d; 95% CI, 11.79-13.55; P = .003).
Although the relationship remained significant in premenopausal women, it lost significance in postmenopausal women.
A 5% decrease in the prevalence of depression in premenopausal (but not postmenopausal) women was found in those with an increased intake of dietary fiber – i..e, there was a 1-g increase for every 1,000 kcal of daily energy intake, after adjusting for potential confounders in premenopausal women (OR, 0.949; 95% CI, 0.906-0.993]).
“The inverse relationship between dietary fiber intake and depression could be explained by the gut-brain interactions,” said Dr. Kim.
“Changes in the gut microbiota composition may affect neurotransmission and various neuropsychiatric phenomena in the brain,” she said, noting that previous studies have suggested that dietary fiber intake “may modulate the richness and diversity of the gut microbiota, and this change may promote brain health by affecting neurotransmission.”
Because postmenopausal women experience estrogen depletion, “the decreased interaction between estrogen and the gut microbiota may be related to the insignificant association between dietary fiber intake and depression in postmenopausal women,” she said.
Despite the lack of a significant association between postmenopausal depression and fiber intake, Dr. Kim said she “advises middle-aged women to have dietary fiber–rich diets, regardless of their menopausal status.”
Link between food and mood
In a comment, Stephanie S. Faubion, MD, MBA, a professor and chair of the department of medicine and the Penny and Bill George director of the Mayo Clinic’s Center for Women’s Health in Rochester, Minn., noted the study was cross-sectional and therefore the direction of the association could not be determined and “causality cannot be assumed.”
It is possible that “depressed women are less likely to eat fiber than women without depression. For example, a depressed woman may be more likely to sit on the couch eating Cheetos than shopping for and preparing a healthy meal,” said Dr. Faubion, who is also the medical director of the North American Menopause Society and was not involved with the study.
She noted that other potential confounders, including access to fresh fruits and vegetables or geographic locations could also “impact the findings and .”
Nevertheless, the study does “add to the body of evidence suggesting a link between diet and overall health, including brain health,” Dr. Faubion said.
One take-home message for practicing clinicians is that a healthy diet that includes fiber may benefit women (and men) for a number of reasons and “appears to be linked to mood.”
More research is needed “to determine the pathophysiologic mechanisms (such as potential brain-gut connection that involves the microbiome) that may explain this association,” Dr. Faubion added.
No source of funding listed. Dr. Kim and coauthors, as well as Dr. Faubion, disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Higher fiber intake may be associated with decreased risk of depression in premenopausal women, new research suggests.
Investigators analyzed data from close to 6,000 pre- and postmenopausal women. They found that, in premenopausal women, dietary fiber intake was higher among those without depression versus their counterparts with the disorder in a dose-dependent manner. However, there appeared to be no relationship between higher fiber intake and depression risk in postmenopausal women.
“We think the most important finding of our study is that dietary fiber intake was inversely associated with depression in premenopausal but not postmenopausal women,” lead author Yunsun Kim, MD, resident, department of family medicine, Chung-Ang University Hospital, Seoul, South Korea, said in an interview.
“We hope that the findings of this study could form the basis of future investigations to determine the causal relationship between dietary fiber intake and depression,” she added.
The study was published online Dec. 21, 2020, in Menopause.
Gut-brain interaction
The prevalence of depression is twice as high in women, compared with men, which may be attributable to a number of factors, including hormonal status – especially during menstruation and menopause, the authors wrote.
Previous research suggests a potential association between dietary fiber and depression in premenopausal women and between estrogen and gut microbiota. Fiber intake has an impact on gut microbiota, Dr. Kim said.
“We are motivated by the fact that depression provokes disease burden internationally and we would like to find modifiable factors that could prevent depression, especially in women, who are more vulnerable to depression,” she noted.
To investigate, the researchers drew on data from the Korea National Health and Nutrition Examination Survey for 2014, 2016, and 2018. Of the total number of women who met inclusion criteria (n = 5807; mean age, 47.11), roughly half were premenopausal and half were postmenopausal (n = 2,949 [mean age, 36.23 years] and n = 2,868 [mean age, 62.73], respectively).
Dietary fiber intake was assessed using the 24-hour dietary recall method, while depression was assessed using the Patient Health Questionnaire-9. The researchers used the Dietary Reference Intakes for Koreans to define a sufficient intake of dietary fiber (i.e., 12 g/1,000 kcal).
Covariates included chronic diseases, body mass index, medications, smoking status, alcohol use, physical activity, and sociodemographic factors.
When the researchers looked at all participants, they found that the estimated mean dietary fiber intake was significantly higher in women without depression, compared with those with depression (14.07 g/1,000 kcal/d; 95% confidence interval, 13.85-14.29 vs. 12.67 g/1,000 kcal/d; 95% CI, 11.79-13.55; P = .003).
Although the relationship remained significant in premenopausal women, it lost significance in postmenopausal women.
A 5% decrease in the prevalence of depression in premenopausal (but not postmenopausal) women was found in those with an increased intake of dietary fiber – i..e, there was a 1-g increase for every 1,000 kcal of daily energy intake, after adjusting for potential confounders in premenopausal women (OR, 0.949; 95% CI, 0.906-0.993]).
“The inverse relationship between dietary fiber intake and depression could be explained by the gut-brain interactions,” said Dr. Kim.
“Changes in the gut microbiota composition may affect neurotransmission and various neuropsychiatric phenomena in the brain,” she said, noting that previous studies have suggested that dietary fiber intake “may modulate the richness and diversity of the gut microbiota, and this change may promote brain health by affecting neurotransmission.”
Because postmenopausal women experience estrogen depletion, “the decreased interaction between estrogen and the gut microbiota may be related to the insignificant association between dietary fiber intake and depression in postmenopausal women,” she said.
Despite the lack of a significant association between postmenopausal depression and fiber intake, Dr. Kim said she “advises middle-aged women to have dietary fiber–rich diets, regardless of their menopausal status.”
Link between food and mood
In a comment, Stephanie S. Faubion, MD, MBA, a professor and chair of the department of medicine and the Penny and Bill George director of the Mayo Clinic’s Center for Women’s Health in Rochester, Minn., noted the study was cross-sectional and therefore the direction of the association could not be determined and “causality cannot be assumed.”
It is possible that “depressed women are less likely to eat fiber than women without depression. For example, a depressed woman may be more likely to sit on the couch eating Cheetos than shopping for and preparing a healthy meal,” said Dr. Faubion, who is also the medical director of the North American Menopause Society and was not involved with the study.
She noted that other potential confounders, including access to fresh fruits and vegetables or geographic locations could also “impact the findings and .”
Nevertheless, the study does “add to the body of evidence suggesting a link between diet and overall health, including brain health,” Dr. Faubion said.
One take-home message for practicing clinicians is that a healthy diet that includes fiber may benefit women (and men) for a number of reasons and “appears to be linked to mood.”
More research is needed “to determine the pathophysiologic mechanisms (such as potential brain-gut connection that involves the microbiome) that may explain this association,” Dr. Faubion added.
No source of funding listed. Dr. Kim and coauthors, as well as Dr. Faubion, disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Higher fiber intake may be associated with decreased risk of depression in premenopausal women, new research suggests.
Investigators analyzed data from close to 6,000 pre- and postmenopausal women. They found that, in premenopausal women, dietary fiber intake was higher among those without depression versus their counterparts with the disorder in a dose-dependent manner. However, there appeared to be no relationship between higher fiber intake and depression risk in postmenopausal women.
“We think the most important finding of our study is that dietary fiber intake was inversely associated with depression in premenopausal but not postmenopausal women,” lead author Yunsun Kim, MD, resident, department of family medicine, Chung-Ang University Hospital, Seoul, South Korea, said in an interview.
“We hope that the findings of this study could form the basis of future investigations to determine the causal relationship between dietary fiber intake and depression,” she added.
The study was published online Dec. 21, 2020, in Menopause.
Gut-brain interaction
The prevalence of depression is twice as high in women, compared with men, which may be attributable to a number of factors, including hormonal status – especially during menstruation and menopause, the authors wrote.
Previous research suggests a potential association between dietary fiber and depression in premenopausal women and between estrogen and gut microbiota. Fiber intake has an impact on gut microbiota, Dr. Kim said.
“We are motivated by the fact that depression provokes disease burden internationally and we would like to find modifiable factors that could prevent depression, especially in women, who are more vulnerable to depression,” she noted.
To investigate, the researchers drew on data from the Korea National Health and Nutrition Examination Survey for 2014, 2016, and 2018. Of the total number of women who met inclusion criteria (n = 5807; mean age, 47.11), roughly half were premenopausal and half were postmenopausal (n = 2,949 [mean age, 36.23 years] and n = 2,868 [mean age, 62.73], respectively).
Dietary fiber intake was assessed using the 24-hour dietary recall method, while depression was assessed using the Patient Health Questionnaire-9. The researchers used the Dietary Reference Intakes for Koreans to define a sufficient intake of dietary fiber (i.e., 12 g/1,000 kcal).
Covariates included chronic diseases, body mass index, medications, smoking status, alcohol use, physical activity, and sociodemographic factors.
When the researchers looked at all participants, they found that the estimated mean dietary fiber intake was significantly higher in women without depression, compared with those with depression (14.07 g/1,000 kcal/d; 95% confidence interval, 13.85-14.29 vs. 12.67 g/1,000 kcal/d; 95% CI, 11.79-13.55; P = .003).
Although the relationship remained significant in premenopausal women, it lost significance in postmenopausal women.
A 5% decrease in the prevalence of depression in premenopausal (but not postmenopausal) women was found in those with an increased intake of dietary fiber – i..e, there was a 1-g increase for every 1,000 kcal of daily energy intake, after adjusting for potential confounders in premenopausal women (OR, 0.949; 95% CI, 0.906-0.993]).
“The inverse relationship between dietary fiber intake and depression could be explained by the gut-brain interactions,” said Dr. Kim.
“Changes in the gut microbiota composition may affect neurotransmission and various neuropsychiatric phenomena in the brain,” she said, noting that previous studies have suggested that dietary fiber intake “may modulate the richness and diversity of the gut microbiota, and this change may promote brain health by affecting neurotransmission.”
Because postmenopausal women experience estrogen depletion, “the decreased interaction between estrogen and the gut microbiota may be related to the insignificant association between dietary fiber intake and depression in postmenopausal women,” she said.
Despite the lack of a significant association between postmenopausal depression and fiber intake, Dr. Kim said she “advises middle-aged women to have dietary fiber–rich diets, regardless of their menopausal status.”
Link between food and mood
In a comment, Stephanie S. Faubion, MD, MBA, a professor and chair of the department of medicine and the Penny and Bill George director of the Mayo Clinic’s Center for Women’s Health in Rochester, Minn., noted the study was cross-sectional and therefore the direction of the association could not be determined and “causality cannot be assumed.”
It is possible that “depressed women are less likely to eat fiber than women without depression. For example, a depressed woman may be more likely to sit on the couch eating Cheetos than shopping for and preparing a healthy meal,” said Dr. Faubion, who is also the medical director of the North American Menopause Society and was not involved with the study.
She noted that other potential confounders, including access to fresh fruits and vegetables or geographic locations could also “impact the findings and .”
Nevertheless, the study does “add to the body of evidence suggesting a link between diet and overall health, including brain health,” Dr. Faubion said.
One take-home message for practicing clinicians is that a healthy diet that includes fiber may benefit women (and men) for a number of reasons and “appears to be linked to mood.”
More research is needed “to determine the pathophysiologic mechanisms (such as potential brain-gut connection that involves the microbiome) that may explain this association,” Dr. Faubion added.
No source of funding listed. Dr. Kim and coauthors, as well as Dr. Faubion, disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Cannabis tied to self-harm, death in youth with mood disorders
Adolescents and young adults with mood disorders and cannabis use disorder (CUD) are at significantly increased risk for self-harm, all-cause mortality, homicide, and death by unintentional overdose, new research suggests.

Investigators found the risk for self-harm was three times higher, all-cause mortality was 59% higher, unintentional overdose was 2.5 times higher, and homicide was more than three times higher in those with versus without CUD.
“The take-home message of these findings is that we need to be aware of the perception that cannabis use is harmless, when it’s actually not,” lead author Cynthia Fontanella, PhD, associate professor of psychiatry, Ohio State University Wexner Medical Center, Columbus, said in an interview.
“We need to educate parents and clinicians that there are risks associated with cannabis, including increased risk for self-harm and death, and we need to effectively treat both cannabis use disorder and mood disorders,” she said.
The study was published online Jan. 19, 2021, in JAMA Pediatrics.
Little research in youth
“There has been very little research conducted on CUD in the adolescent population, and most studies have been conducted with adults,” Dr. Fontanella said.
Research on adults has shown that, even in people without mood disorders, cannabis use is associated with the early onset of mood disorders, psychosis, and anxiety disorders and has also been linked with suicidal behavior and increased risk for motor vehicle accidents, Dr. Fontanella said.
“We were motivated to conduct this study because we treat kids with depression and bipolar disorder and we noticed a high prevalence of CUD in this population, so we were curious about what its negative effects might be,” Dr. Fontanella recounted.
The researchers analyzed 7-year data drawn from Ohio Medicaid claims and linked to data from death certificates in 204,780 youths between the ages of 10 and 24 years (mean age was 17.2 years at the time of mood disorder diagnosis). Most were female, non-Hispanic White, enrolled in Medicaid because of poverty, and living in a metropolitan area (65.0%, 66.9%, 87.6%, and 77.1%, respectively).
Participants were followed up to 1 year from diagnosis until the end of enrollment, a self-harm event, or death.
Researchers included demographic, clinical, and treatment factors as covariates.
Close to three-quarters (72.7%) of the cohort had a depressive disorder, followed by unspecified/persistent mood disorder and bipolar disorder (14.9% and 12.4%, respectively). Comorbidities included ADHD (12.4%), anxiety disorder (12.3%), and other mental disorders (13.1%).
One -tenth of the cohort (10.3%) were diagnosed with CUD.
CUD treatment referrals
“Although CUD was associated with suicide in the unadjusted model, it was not significantly associated in adjusted models,” the authors reported.
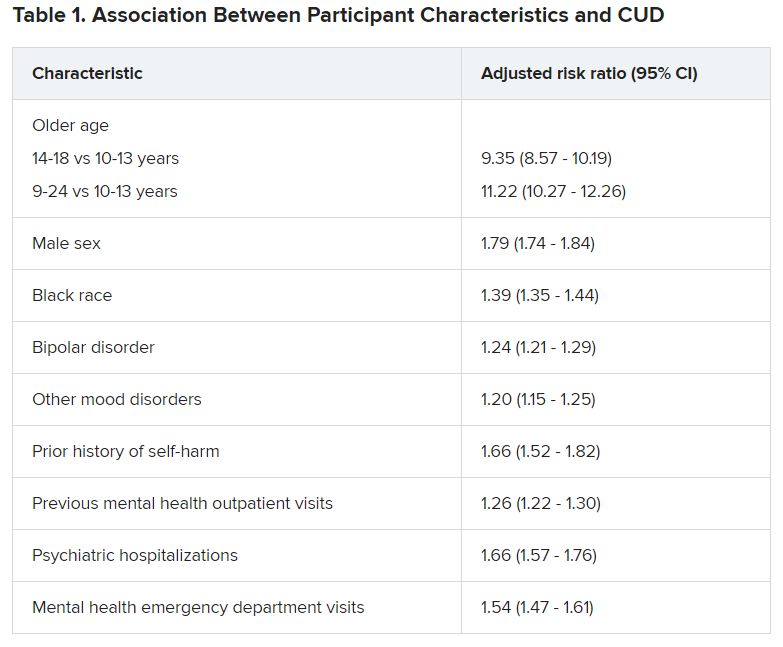
Dr. Fontanella noted that the risk for these adverse outcomes is greater among those who engage in heavy, frequent use or who use cannabis that has higher-potency tetrahydrocannabinol (THC) content.
Reasons why CUD might be associated with these adverse outcomes are that it can increase impulsivity, poor judgment, and clouded thinking, which may in turn increase the risk for self-harm behaviors, she said.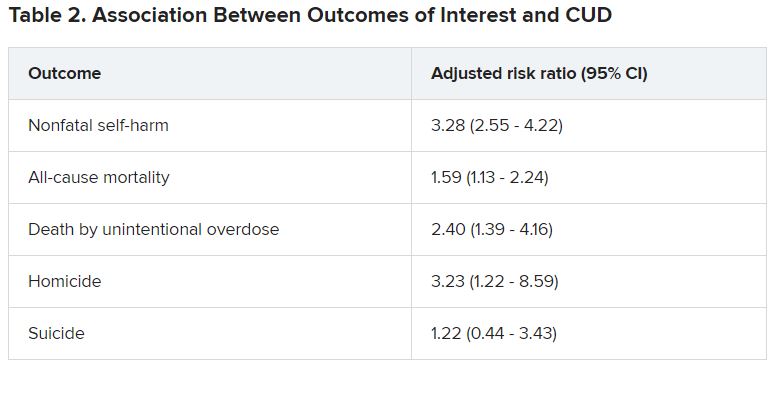
She recommended that clinicians refer youth with CUD for “effective treatments,” including family-based models and individual approaches, such as cognitive behavioral therapy and motivational enhancement therapy.
Open dialogue
In a comment, Wilfrid Noel Raby, MD, PhD, adjunct clinical professor, Albert Einstein College of Medicine, New York, noted that psychosis can occur in patients with CUD and mood disorders – especially bipolar disorder – but was not included as a study outcome. “I would have liked to see more data about that,” he said.
However, “The trend is that cannabis use is starting at younger and younger ages, which has all kinds of ramifications in terms of cerebral development.”
Christopher Hammond, MD, PhD, assistant professor of psychiatry, Johns Hopkins University, Baltimore, said: “Three major strengths of the study are the size of the sample, its longitudinal analysis, and that the authors controlled for a number of potential confounding variables.”
In light of the findings, Dr. Hammond recommended clinicians and other health professionals who work with young people “should screen for cannabis-related problems in youth with mood disorders.”
Dr. Hammond, who is the director of the Co-occurring Disorders in Adolescents and Young Adults Clinical and Research Program, Johns Hopkins Bayview Medical Center, Baltimore, and was not involved with the study, recommended counseling youth with mood disorders and their parents and families “regarding the potential adverse health effects related to cannabis use.”
He also recommended “open dialogue with youth with and without mental health conditions about misleading reports in the national media and advertising about cannabis’ health benefits.”
The study was funded by the National Institute of Mental Health. Dr. Fontanella reported receiving grants from the National Institute of Mental Health during the conduct of the study. Dr. Raby reported no relevant financial relationships. Dr. Hammond reported receiving research grant funding from the National Institutes of Health, the American Academy of Child & Adolescent Psychiatry, Substance Abuse Mental Health Services Administration, the National Network of Depression Centers, and the Armstrong Institute at Johns Hopkins Bayview and serves as a scientific adviser for the National Courts and Science Institute and as a subject matter expert for SAMHSA related to co-occurring substance use disorders and severe emotional disturbance in youth.
A version of this article first appeared on Medscape.com.
Adolescents and young adults with mood disorders and cannabis use disorder (CUD) are at significantly increased risk for self-harm, all-cause mortality, homicide, and death by unintentional overdose, new research suggests.
Investigators found the risk for self-harm was three times higher, all-cause mortality was 59% higher, unintentional overdose was 2.5 times higher, and homicide was more than three times higher in those with versus without CUD.
“The take-home message of these findings is that we need to be aware of the perception that cannabis use is harmless, when it’s actually not,” lead author Cynthia Fontanella, PhD, associate professor of psychiatry, Ohio State University Wexner Medical Center, Columbus, said in an interview.
“We need to educate parents and clinicians that there are risks associated with cannabis, including increased risk for self-harm and death, and we need to effectively treat both cannabis use disorder and mood disorders,” she said.
The study was published online Jan. 19, 2021, in JAMA Pediatrics.
Little research in youth
“There has been very little research conducted on CUD in the adolescent population, and most studies have been conducted with adults,” Dr. Fontanella said.
Research on adults has shown that, even in people without mood disorders, cannabis use is associated with the early onset of mood disorders, psychosis, and anxiety disorders and has also been linked with suicidal behavior and increased risk for motor vehicle accidents, Dr. Fontanella said.
“We were motivated to conduct this study because we treat kids with depression and bipolar disorder and we noticed a high prevalence of CUD in this population, so we were curious about what its negative effects might be,” Dr. Fontanella recounted.
The researchers analyzed 7-year data drawn from Ohio Medicaid claims and linked to data from death certificates in 204,780 youths between the ages of 10 and 24 years (mean age was 17.2 years at the time of mood disorder diagnosis). Most were female, non-Hispanic White, enrolled in Medicaid because of poverty, and living in a metropolitan area (65.0%, 66.9%, 87.6%, and 77.1%, respectively).
Participants were followed up to 1 year from diagnosis until the end of enrollment, a self-harm event, or death.
Researchers included demographic, clinical, and treatment factors as covariates.
Close to three-quarters (72.7%) of the cohort had a depressive disorder, followed by unspecified/persistent mood disorder and bipolar disorder (14.9% and 12.4%, respectively). Comorbidities included ADHD (12.4%), anxiety disorder (12.3%), and other mental disorders (13.1%).
One -tenth of the cohort (10.3%) were diagnosed with CUD.
CUD treatment referrals
“Although CUD was associated with suicide in the unadjusted model, it was not significantly associated in adjusted models,” the authors reported.
Dr. Fontanella noted that the risk for these adverse outcomes is greater among those who engage in heavy, frequent use or who use cannabis that has higher-potency tetrahydrocannabinol (THC) content.
Reasons why CUD might be associated with these adverse outcomes are that it can increase impulsivity, poor judgment, and clouded thinking, which may in turn increase the risk for self-harm behaviors, she said.
She recommended that clinicians refer youth with CUD for “effective treatments,” including family-based models and individual approaches, such as cognitive behavioral therapy and motivational enhancement therapy.
Open dialogue
In a comment, Wilfrid Noel Raby, MD, PhD, adjunct clinical professor, Albert Einstein College of Medicine, New York, noted that psychosis can occur in patients with CUD and mood disorders – especially bipolar disorder – but was not included as a study outcome. “I would have liked to see more data about that,” he said.
However, “The trend is that cannabis use is starting at younger and younger ages, which has all kinds of ramifications in terms of cerebral development.”
Christopher Hammond, MD, PhD, assistant professor of psychiatry, Johns Hopkins University, Baltimore, said: “Three major strengths of the study are the size of the sample, its longitudinal analysis, and that the authors controlled for a number of potential confounding variables.”
In light of the findings, Dr. Hammond recommended clinicians and other health professionals who work with young people “should screen for cannabis-related problems in youth with mood disorders.”
Dr. Hammond, who is the director of the Co-occurring Disorders in Adolescents and Young Adults Clinical and Research Program, Johns Hopkins Bayview Medical Center, Baltimore, and was not involved with the study, recommended counseling youth with mood disorders and their parents and families “regarding the potential adverse health effects related to cannabis use.”
He also recommended “open dialogue with youth with and without mental health conditions about misleading reports in the national media and advertising about cannabis’ health benefits.”
The study was funded by the National Institute of Mental Health. Dr. Fontanella reported receiving grants from the National Institute of Mental Health during the conduct of the study. Dr. Raby reported no relevant financial relationships. Dr. Hammond reported receiving research grant funding from the National Institutes of Health, the American Academy of Child & Adolescent Psychiatry, Substance Abuse Mental Health Services Administration, the National Network of Depression Centers, and the Armstrong Institute at Johns Hopkins Bayview and serves as a scientific adviser for the National Courts and Science Institute and as a subject matter expert for SAMHSA related to co-occurring substance use disorders and severe emotional disturbance in youth.
A version of this article first appeared on Medscape.com.
Adolescents and young adults with mood disorders and cannabis use disorder (CUD) are at significantly increased risk for self-harm, all-cause mortality, homicide, and death by unintentional overdose, new research suggests.
Investigators found the risk for self-harm was three times higher, all-cause mortality was 59% higher, unintentional overdose was 2.5 times higher, and homicide was more than three times higher in those with versus without CUD.
“The take-home message of these findings is that we need to be aware of the perception that cannabis use is harmless, when it’s actually not,” lead author Cynthia Fontanella, PhD, associate professor of psychiatry, Ohio State University Wexner Medical Center, Columbus, said in an interview.
“We need to educate parents and clinicians that there are risks associated with cannabis, including increased risk for self-harm and death, and we need to effectively treat both cannabis use disorder and mood disorders,” she said.
The study was published online Jan. 19, 2021, in JAMA Pediatrics.
Little research in youth
“There has been very little research conducted on CUD in the adolescent population, and most studies have been conducted with adults,” Dr. Fontanella said.
Research on adults has shown that, even in people without mood disorders, cannabis use is associated with the early onset of mood disorders, psychosis, and anxiety disorders and has also been linked with suicidal behavior and increased risk for motor vehicle accidents, Dr. Fontanella said.
“We were motivated to conduct this study because we treat kids with depression and bipolar disorder and we noticed a high prevalence of CUD in this population, so we were curious about what its negative effects might be,” Dr. Fontanella recounted.
The researchers analyzed 7-year data drawn from Ohio Medicaid claims and linked to data from death certificates in 204,780 youths between the ages of 10 and 24 years (mean age was 17.2 years at the time of mood disorder diagnosis). Most were female, non-Hispanic White, enrolled in Medicaid because of poverty, and living in a metropolitan area (65.0%, 66.9%, 87.6%, and 77.1%, respectively).
Participants were followed up to 1 year from diagnosis until the end of enrollment, a self-harm event, or death.
Researchers included demographic, clinical, and treatment factors as covariates.
Close to three-quarters (72.7%) of the cohort had a depressive disorder, followed by unspecified/persistent mood disorder and bipolar disorder (14.9% and 12.4%, respectively). Comorbidities included ADHD (12.4%), anxiety disorder (12.3%), and other mental disorders (13.1%).
One -tenth of the cohort (10.3%) were diagnosed with CUD.
CUD treatment referrals
“Although CUD was associated with suicide in the unadjusted model, it was not significantly associated in adjusted models,” the authors reported.
Dr. Fontanella noted that the risk for these adverse outcomes is greater among those who engage in heavy, frequent use or who use cannabis that has higher-potency tetrahydrocannabinol (THC) content.
Reasons why CUD might be associated with these adverse outcomes are that it can increase impulsivity, poor judgment, and clouded thinking, which may in turn increase the risk for self-harm behaviors, she said.
She recommended that clinicians refer youth with CUD for “effective treatments,” including family-based models and individual approaches, such as cognitive behavioral therapy and motivational enhancement therapy.
Open dialogue
In a comment, Wilfrid Noel Raby, MD, PhD, adjunct clinical professor, Albert Einstein College of Medicine, New York, noted that psychosis can occur in patients with CUD and mood disorders – especially bipolar disorder – but was not included as a study outcome. “I would have liked to see more data about that,” he said.
However, “The trend is that cannabis use is starting at younger and younger ages, which has all kinds of ramifications in terms of cerebral development.”
Christopher Hammond, MD, PhD, assistant professor of psychiatry, Johns Hopkins University, Baltimore, said: “Three major strengths of the study are the size of the sample, its longitudinal analysis, and that the authors controlled for a number of potential confounding variables.”
In light of the findings, Dr. Hammond recommended clinicians and other health professionals who work with young people “should screen for cannabis-related problems in youth with mood disorders.”
Dr. Hammond, who is the director of the Co-occurring Disorders in Adolescents and Young Adults Clinical and Research Program, Johns Hopkins Bayview Medical Center, Baltimore, and was not involved with the study, recommended counseling youth with mood disorders and their parents and families “regarding the potential adverse health effects related to cannabis use.”
He also recommended “open dialogue with youth with and without mental health conditions about misleading reports in the national media and advertising about cannabis’ health benefits.”
The study was funded by the National Institute of Mental Health. Dr. Fontanella reported receiving grants from the National Institute of Mental Health during the conduct of the study. Dr. Raby reported no relevant financial relationships. Dr. Hammond reported receiving research grant funding from the National Institutes of Health, the American Academy of Child & Adolescent Psychiatry, Substance Abuse Mental Health Services Administration, the National Network of Depression Centers, and the Armstrong Institute at Johns Hopkins Bayview and serves as a scientific adviser for the National Courts and Science Institute and as a subject matter expert for SAMHSA related to co-occurring substance use disorders and severe emotional disturbance in youth.
A version of this article first appeared on Medscape.com.
Afternoon napping associated with better cognition in elderly, study shows
according to a new study in General Psychiatry.
The findings add to those seen in other observational studies showing afternoon napping promotes cognitive function, said the authors of the paper, published in General Psychiatry.
“The prevalence of afternoon napping has been increasing in older adults much more than in younger individuals,” wrote Han Cai, MS, of the department of geriatrics at The Fourth People’s Hospital of Wuhu, Anhui, China, and coauthors. “The elderly individuals who took afternoon naps showed significantly higher cognitive performance compared with those who did not nap.”
The researchers enrolled 2,214 people in the study – all Han Chinese and aged 60 or older. Afternoon napping was considered any period of inactivity of at least 5 minutes but less than 2 hours after lunch and outside of the person’s main sleep schedule. Those who reported ever napping – 1,534 subjects – were included in the napping group, and the others – 680 – in the nonnapping group. Patients with major physical conditions were excluded.
The Montreal Cognitive Assessment (MoCA), the Mini-Mental State Examination (MMSE), and the Neuropsychological Test Battery (NTB) were used to measure cognitive function, and 739 patients agreed to blood tests for lipid values.
The average total MMSE score was higher for the napping group at 25.3 points out of 30, than for the nonnapping group, at 24.56 (P = .003). Those in the napping group also had significantly higher scores in the orientation portion of the MoCA test, at 5.55 out of 6 points, compared with 5.41 for the nonnapping group (P = .006).
Those in the napping group scored significantly higher on the digit span and language fluency parts of the Neuropsychological Test Battery (P = .009 and .020, respectively).
Dementia was assessed with face-to-face visits with clinicians, but diagnoses of dementia were not different between the groups.
Triglycerides were found to be higher – though still in the normal range – in the napping group compared with the nonnapping group, 1.80 mmol/L to 1.75 mmol/L, the researchers found (P = .001). No differences were seen for HDL or LDL cholesterol levels, or in hypertension or diabetes, the researchers reported.
The authors noted that inflammation is likely an important feature in the relationship between napping and cognitive function. Inflammatory cytokines have been found to play a role in sleep disorders, and strong inflammatory responses can lead to adverse events, including cognitive impairment.
“Sleep is known to be a regulator of the immune response that counters these inflammatory mediators, whereas napping, in particular, is thought to be an evolved response to inflammation,” they said.
The average age of patients in the napping group was 72.8 years, slightly older than those in the nonnapping group at 71.3 years, and this was a significant difference (P = .016).
The researchers acknowledged that the study “could not show direct causality of napping, whether beneficial or harmful,” and that “a lack of detailed information regarding napping duration ... also limited the description of napping status.”
Junxin Li, PhD, RN, assistant professor at Johns Hopkins School of Nursing, Baltimore, who has studied napping and cognition, said that previous research generally supports a U-shaped relationship between napping and mental acuity, with shorter or medium-length naps benefiting cognition and no naps or naps that are too long being detrimental.

“This study looked at no nap versus naps of less than 2 hours and may not be able to capture this potential U-shaped association,” she said.
For clinicians, the duration, timing, frequency, and purpose of naps are important factors in making recommendations to patients, she said.
“For example, timing – napping in the early evening close to older adult’s bedtime may delay their bedtime and interfere with their nighttime sleep quality. Taking naps after lunchtime is hypothesized to provide the most therapeutic values to the health and usually recommended,” she said. Regular napping is better than “randomly dozing off,” Dr. Li added.
There are also cultural considerations – in east Asia, napping tends to be considered part of a healthy lifestyle, while in western countries it is not – and this could impact napping behaviors and how these behaviors affect cognition, she said.
Phyllis C. Zee, MD, PhD, director of the Center for Circadian and Sleep Medicine at the Northwestern University, Chicago, said the results are consistent with early cross-sectional studies that showed that regular, scheduled naps in the afternoon were associated with positive cognitive performance and lower cardiometabolic disease risk.
Dr. Zee noted that it’s important to recognize that the positive data are associated with naps that are planned, while older adults napping because of excess sleepiness are at a higher risk for cognitive impairment and other health issues.
The study authors, Dr. Li, and Dr. Zee reported no relevant financial disclosures.
according to a new study in General Psychiatry.
The findings add to those seen in other observational studies showing afternoon napping promotes cognitive function, said the authors of the paper, published in General Psychiatry.
“The prevalence of afternoon napping has been increasing in older adults much more than in younger individuals,” wrote Han Cai, MS, of the department of geriatrics at The Fourth People’s Hospital of Wuhu, Anhui, China, and coauthors. “The elderly individuals who took afternoon naps showed significantly higher cognitive performance compared with those who did not nap.”
The researchers enrolled 2,214 people in the study – all Han Chinese and aged 60 or older. Afternoon napping was considered any period of inactivity of at least 5 minutes but less than 2 hours after lunch and outside of the person’s main sleep schedule. Those who reported ever napping – 1,534 subjects – were included in the napping group, and the others – 680 – in the nonnapping group. Patients with major physical conditions were excluded.
The Montreal Cognitive Assessment (MoCA), the Mini-Mental State Examination (MMSE), and the Neuropsychological Test Battery (NTB) were used to measure cognitive function, and 739 patients agreed to blood tests for lipid values.
The average total MMSE score was higher for the napping group at 25.3 points out of 30, than for the nonnapping group, at 24.56 (P = .003). Those in the napping group also had significantly higher scores in the orientation portion of the MoCA test, at 5.55 out of 6 points, compared with 5.41 for the nonnapping group (P = .006).
Those in the napping group scored significantly higher on the digit span and language fluency parts of the Neuropsychological Test Battery (P = .009 and .020, respectively).
Dementia was assessed with face-to-face visits with clinicians, but diagnoses of dementia were not different between the groups.
Triglycerides were found to be higher – though still in the normal range – in the napping group compared with the nonnapping group, 1.80 mmol/L to 1.75 mmol/L, the researchers found (P = .001). No differences were seen for HDL or LDL cholesterol levels, or in hypertension or diabetes, the researchers reported.
The authors noted that inflammation is likely an important feature in the relationship between napping and cognitive function. Inflammatory cytokines have been found to play a role in sleep disorders, and strong inflammatory responses can lead to adverse events, including cognitive impairment.
“Sleep is known to be a regulator of the immune response that counters these inflammatory mediators, whereas napping, in particular, is thought to be an evolved response to inflammation,” they said.
The average age of patients in the napping group was 72.8 years, slightly older than those in the nonnapping group at 71.3 years, and this was a significant difference (P = .016).
The researchers acknowledged that the study “could not show direct causality of napping, whether beneficial or harmful,” and that “a lack of detailed information regarding napping duration ... also limited the description of napping status.”
Junxin Li, PhD, RN, assistant professor at Johns Hopkins School of Nursing, Baltimore, who has studied napping and cognition, said that previous research generally supports a U-shaped relationship between napping and mental acuity, with shorter or medium-length naps benefiting cognition and no naps or naps that are too long being detrimental.
“This study looked at no nap versus naps of less than 2 hours and may not be able to capture this potential U-shaped association,” she said.
For clinicians, the duration, timing, frequency, and purpose of naps are important factors in making recommendations to patients, she said.
“For example, timing – napping in the early evening close to older adult’s bedtime may delay their bedtime and interfere with their nighttime sleep quality. Taking naps after lunchtime is hypothesized to provide the most therapeutic values to the health and usually recommended,” she said. Regular napping is better than “randomly dozing off,” Dr. Li added.
There are also cultural considerations – in east Asia, napping tends to be considered part of a healthy lifestyle, while in western countries it is not – and this could impact napping behaviors and how these behaviors affect cognition, she said.
Phyllis C. Zee, MD, PhD, director of the Center for Circadian and Sleep Medicine at the Northwestern University, Chicago, said the results are consistent with early cross-sectional studies that showed that regular, scheduled naps in the afternoon were associated with positive cognitive performance and lower cardiometabolic disease risk.
Dr. Zee noted that it’s important to recognize that the positive data are associated with naps that are planned, while older adults napping because of excess sleepiness are at a higher risk for cognitive impairment and other health issues.
The study authors, Dr. Li, and Dr. Zee reported no relevant financial disclosures.
according to a new study in General Psychiatry.
The findings add to those seen in other observational studies showing afternoon napping promotes cognitive function, said the authors of the paper, published in General Psychiatry.
“The prevalence of afternoon napping has been increasing in older adults much more than in younger individuals,” wrote Han Cai, MS, of the department of geriatrics at The Fourth People’s Hospital of Wuhu, Anhui, China, and coauthors. “The elderly individuals who took afternoon naps showed significantly higher cognitive performance compared with those who did not nap.”
The researchers enrolled 2,214 people in the study – all Han Chinese and aged 60 or older. Afternoon napping was considered any period of inactivity of at least 5 minutes but less than 2 hours after lunch and outside of the person’s main sleep schedule. Those who reported ever napping – 1,534 subjects – were included in the napping group, and the others – 680 – in the nonnapping group. Patients with major physical conditions were excluded.
The Montreal Cognitive Assessment (MoCA), the Mini-Mental State Examination (MMSE), and the Neuropsychological Test Battery (NTB) were used to measure cognitive function, and 739 patients agreed to blood tests for lipid values.
The average total MMSE score was higher for the napping group at 25.3 points out of 30, than for the nonnapping group, at 24.56 (P = .003). Those in the napping group also had significantly higher scores in the orientation portion of the MoCA test, at 5.55 out of 6 points, compared with 5.41 for the nonnapping group (P = .006).
Those in the napping group scored significantly higher on the digit span and language fluency parts of the Neuropsychological Test Battery (P = .009 and .020, respectively).
Dementia was assessed with face-to-face visits with clinicians, but diagnoses of dementia were not different between the groups.
Triglycerides were found to be higher – though still in the normal range – in the napping group compared with the nonnapping group, 1.80 mmol/L to 1.75 mmol/L, the researchers found (P = .001). No differences were seen for HDL or LDL cholesterol levels, or in hypertension or diabetes, the researchers reported.
The authors noted that inflammation is likely an important feature in the relationship between napping and cognitive function. Inflammatory cytokines have been found to play a role in sleep disorders, and strong inflammatory responses can lead to adverse events, including cognitive impairment.
“Sleep is known to be a regulator of the immune response that counters these inflammatory mediators, whereas napping, in particular, is thought to be an evolved response to inflammation,” they said.
The average age of patients in the napping group was 72.8 years, slightly older than those in the nonnapping group at 71.3 years, and this was a significant difference (P = .016).
The researchers acknowledged that the study “could not show direct causality of napping, whether beneficial or harmful,” and that “a lack of detailed information regarding napping duration ... also limited the description of napping status.”
Junxin Li, PhD, RN, assistant professor at Johns Hopkins School of Nursing, Baltimore, who has studied napping and cognition, said that previous research generally supports a U-shaped relationship between napping and mental acuity, with shorter or medium-length naps benefiting cognition and no naps or naps that are too long being detrimental.
“This study looked at no nap versus naps of less than 2 hours and may not be able to capture this potential U-shaped association,” she said.
For clinicians, the duration, timing, frequency, and purpose of naps are important factors in making recommendations to patients, she said.
“For example, timing – napping in the early evening close to older adult’s bedtime may delay their bedtime and interfere with their nighttime sleep quality. Taking naps after lunchtime is hypothesized to provide the most therapeutic values to the health and usually recommended,” she said. Regular napping is better than “randomly dozing off,” Dr. Li added.
There are also cultural considerations – in east Asia, napping tends to be considered part of a healthy lifestyle, while in western countries it is not – and this could impact napping behaviors and how these behaviors affect cognition, she said.
Phyllis C. Zee, MD, PhD, director of the Center for Circadian and Sleep Medicine at the Northwestern University, Chicago, said the results are consistent with early cross-sectional studies that showed that regular, scheduled naps in the afternoon were associated with positive cognitive performance and lower cardiometabolic disease risk.
Dr. Zee noted that it’s important to recognize that the positive data are associated with naps that are planned, while older adults napping because of excess sleepiness are at a higher risk for cognitive impairment and other health issues.
The study authors, Dr. Li, and Dr. Zee reported no relevant financial disclosures.
Opioid-related deaths lower in counties with active cannabis dispensaries
Areas with active cannabis dispensaries have seen a decrease in opioid-related mortalities, recent research has shown.

“Our findings suggest that higher storefront cannabis dispensary counts are associated with reduced opioid related mortality rates at the county level,” wrote Greta Hsu, PhD, professor of management, University of California, Davis, and Balázs Kovács, PhD, associate professor of organizational behavior, Yale University, New Haven, Conn. “, which include the highly potent synthetic opioid fentanyl and its analogs.”

In the study, published in BMJ, the researchers evaluated the prevalence of medical and recreational cannabis dispensaries in 812 U.S. counties within 23 states with some degree of cannabis legalization between 2014 and 2018. Overall, dispensaries located in counties in eight U.S. states and the District of Columbia that sold cannabis recreationally and an additional 15 states that contained medical cannabis dispensaries were included.
Dr. Hsu and Dr. Kovács performed their analysis by examining dispensaries that were operating storefronts by the end of 2017 at the county level using panel-regression methods, combining data obtained from the consumer-facing website Weedmaps.com, Centers for Disease Control and Prevention U.S. mortality data, and data from the U.S. Census Bureau.
To measure opioid-related mortality, the researchers measured ICD-10 codes specific to natural opioid analgesics and semisynthetic opioids, methadone, heroin, nonmethadone synthetic opioid analgesics, and fentanyl-related deaths.
The analysis showed a negative association between the number of cannabis dispensaries at the county level and overall opioid-related mortality rates (95% confidence interval, −0.23 to −0.11), with an increase from one to two dispensaries in a county resulting in a 17% decrease in opioid-related mortality rates and an increase from two to three dispensaries resulting in another decrease in opioid-related mortality of 8.5%.
When evaluating mortality by specific opioid type, the researchers found a negative association between the number of dispensaries and synthetic nonmethadone opioids, with an increase from one to two dispensaries resulting in a 21% decrease in mortality attributable to synthetic nonmethadone opioids (95% CI, −0.27 to −0.14; P = .002). There were also negative associations between the number of dispensaries and prescription opioid-related mortality rates (95% CI, −0.13 to −0.03) and heroin-related mortality rates (95% CI, −0.13 to −0.02). The negative association was similar in comparisons between synthetic nonmethadone opioid-related mortality and the number of dispensaries for medical cannabis (95% CI, −0.21 to −0.09; P = .002) and recreational cannabis (95% CI, −0.17 to −0.04; P = .01).
Evidence of a negative association between legalization of medical or recreational cannabis and opioid-related mortality has been mixed in the literature, with some studies also showing a “spurious or nonsignificant” association, according to Dr. Hsu and Dr. Kovács.
While previous studies have looked at the legalization of cannabis for medical or recreational use, legalization on its own is an “incomplete picture,” they said, which might offer one explanation for these mixed findings. Some states that legalize medical cannabis, for example, might not allow dispensaries to legally sell cannabis, and there may be a delay of 1-2 years between the time a state legalizes cannabis for recreational use and when dispensaries are open and available to the public.
“These results were obtained after controlling for county level population characteristics, yearly effects, whether recreational dispensaries were legal or not in the focal county’s state, and opioid-related state policies,” the authors wrote.
Results ‘may be even stronger’ than reported
Christopher G. Fichtner, MD, clinical professor of psychiatry and neuroscience at the University of California, Riverside, said in an interview that the evidence for using cannabis as an opioid substitution for pain management has not been balanced, but noted “the bulk of it suggests that there is some harm reduction benefit by having liberalized access to cannabis.”

One strength of the study by Dr. Hsu and Dr. Kovács was how they were able to examine implementation of legalization of medical or recreational cannabis, rather than simply a change in the law, he said.
“By looking at dispensary count, it’s actually looking at a better measure of on-the-ground implementation than just change in policy,” Dr. Fichtner explained. “You’re looking at what was actually accomplished in terms of making cannabis legally available.”
The choice to evaluate storefront dispensaries only and not include delivery services in their data, “probably makes it a relatively conservative estimate. I think that would be a strength, that their findings may be even stronger than what it is they’re reporting,” Dr. Fichtner said.
“I do think, if anything, the paper is relatively tentative about advancing its conclusions, which I think is a weakness in a lot of these studies,” he added. In 2017, the National Academy of Sciences released a report that found evidence cannabis or cannabinoids can significantly reduce pain symptoms. In that report, “one of their strongest conclusions is that there’s conclusive or substantial evidence that cannabis or cannabinoids are effective management of chronic pain,” Dr. Fichtner said.
He said that digging deeper into what kinds of pain cannabis can treat is one area for future research. “Certainly, it seems that it’s unlikely that cannabis is going to be good for every kind of pain,” he said. “What kinds of pain is it better for than others? Is it some benefit for many kinds of pain, or only a few types of pain?”
The authors reported no relevant financial disclosures. Dr. Fichtner is the author of a book on cannabis policy in the United States, but reported no other financial disclosures.
Areas with active cannabis dispensaries have seen a decrease in opioid-related mortalities, recent research has shown.
“Our findings suggest that higher storefront cannabis dispensary counts are associated with reduced opioid related mortality rates at the county level,” wrote Greta Hsu, PhD, professor of management, University of California, Davis, and Balázs Kovács, PhD, associate professor of organizational behavior, Yale University, New Haven, Conn. “, which include the highly potent synthetic opioid fentanyl and its analogs.”
In the study, published in BMJ, the researchers evaluated the prevalence of medical and recreational cannabis dispensaries in 812 U.S. counties within 23 states with some degree of cannabis legalization between 2014 and 2018. Overall, dispensaries located in counties in eight U.S. states and the District of Columbia that sold cannabis recreationally and an additional 15 states that contained medical cannabis dispensaries were included.
Dr. Hsu and Dr. Kovács performed their analysis by examining dispensaries that were operating storefronts by the end of 2017 at the county level using panel-regression methods, combining data obtained from the consumer-facing website Weedmaps.com, Centers for Disease Control and Prevention U.S. mortality data, and data from the U.S. Census Bureau.
To measure opioid-related mortality, the researchers measured ICD-10 codes specific to natural opioid analgesics and semisynthetic opioids, methadone, heroin, nonmethadone synthetic opioid analgesics, and fentanyl-related deaths.
The analysis showed a negative association between the number of cannabis dispensaries at the county level and overall opioid-related mortality rates (95% confidence interval, −0.23 to −0.11), with an increase from one to two dispensaries in a county resulting in a 17% decrease in opioid-related mortality rates and an increase from two to three dispensaries resulting in another decrease in opioid-related mortality of 8.5%.
When evaluating mortality by specific opioid type, the researchers found a negative association between the number of dispensaries and synthetic nonmethadone opioids, with an increase from one to two dispensaries resulting in a 21% decrease in mortality attributable to synthetic nonmethadone opioids (95% CI, −0.27 to −0.14; P = .002). There were also negative associations between the number of dispensaries and prescription opioid-related mortality rates (95% CI, −0.13 to −0.03) and heroin-related mortality rates (95% CI, −0.13 to −0.02). The negative association was similar in comparisons between synthetic nonmethadone opioid-related mortality and the number of dispensaries for medical cannabis (95% CI, −0.21 to −0.09; P = .002) and recreational cannabis (95% CI, −0.17 to −0.04; P = .01).
Evidence of a negative association between legalization of medical or recreational cannabis and opioid-related mortality has been mixed in the literature, with some studies also showing a “spurious or nonsignificant” association, according to Dr. Hsu and Dr. Kovács.
While previous studies have looked at the legalization of cannabis for medical or recreational use, legalization on its own is an “incomplete picture,” they said, which might offer one explanation for these mixed findings. Some states that legalize medical cannabis, for example, might not allow dispensaries to legally sell cannabis, and there may be a delay of 1-2 years between the time a state legalizes cannabis for recreational use and when dispensaries are open and available to the public.
“These results were obtained after controlling for county level population characteristics, yearly effects, whether recreational dispensaries were legal or not in the focal county’s state, and opioid-related state policies,” the authors wrote.
Results ‘may be even stronger’ than reported
Christopher G. Fichtner, MD, clinical professor of psychiatry and neuroscience at the University of California, Riverside, said in an interview that the evidence for using cannabis as an opioid substitution for pain management has not been balanced, but noted “the bulk of it suggests that there is some harm reduction benefit by having liberalized access to cannabis.”
One strength of the study by Dr. Hsu and Dr. Kovács was how they were able to examine implementation of legalization of medical or recreational cannabis, rather than simply a change in the law, he said.
“By looking at dispensary count, it’s actually looking at a better measure of on-the-ground implementation than just change in policy,” Dr. Fichtner explained. “You’re looking at what was actually accomplished in terms of making cannabis legally available.”
The choice to evaluate storefront dispensaries only and not include delivery services in their data, “probably makes it a relatively conservative estimate. I think that would be a strength, that their findings may be even stronger than what it is they’re reporting,” Dr. Fichtner said.
“I do think, if anything, the paper is relatively tentative about advancing its conclusions, which I think is a weakness in a lot of these studies,” he added. In 2017, the National Academy of Sciences released a report that found evidence cannabis or cannabinoids can significantly reduce pain symptoms. In that report, “one of their strongest conclusions is that there’s conclusive or substantial evidence that cannabis or cannabinoids are effective management of chronic pain,” Dr. Fichtner said.
He said that digging deeper into what kinds of pain cannabis can treat is one area for future research. “Certainly, it seems that it’s unlikely that cannabis is going to be good for every kind of pain,” he said. “What kinds of pain is it better for than others? Is it some benefit for many kinds of pain, or only a few types of pain?”
The authors reported no relevant financial disclosures. Dr. Fichtner is the author of a book on cannabis policy in the United States, but reported no other financial disclosures.
Areas with active cannabis dispensaries have seen a decrease in opioid-related mortalities, recent research has shown.
“Our findings suggest that higher storefront cannabis dispensary counts are associated with reduced opioid related mortality rates at the county level,” wrote Greta Hsu, PhD, professor of management, University of California, Davis, and Balázs Kovács, PhD, associate professor of organizational behavior, Yale University, New Haven, Conn. “, which include the highly potent synthetic opioid fentanyl and its analogs.”
In the study, published in BMJ, the researchers evaluated the prevalence of medical and recreational cannabis dispensaries in 812 U.S. counties within 23 states with some degree of cannabis legalization between 2014 and 2018. Overall, dispensaries located in counties in eight U.S. states and the District of Columbia that sold cannabis recreationally and an additional 15 states that contained medical cannabis dispensaries were included.
Dr. Hsu and Dr. Kovács performed their analysis by examining dispensaries that were operating storefronts by the end of 2017 at the county level using panel-regression methods, combining data obtained from the consumer-facing website Weedmaps.com, Centers for Disease Control and Prevention U.S. mortality data, and data from the U.S. Census Bureau.
To measure opioid-related mortality, the researchers measured ICD-10 codes specific to natural opioid analgesics and semisynthetic opioids, methadone, heroin, nonmethadone synthetic opioid analgesics, and fentanyl-related deaths.
The analysis showed a negative association between the number of cannabis dispensaries at the county level and overall opioid-related mortality rates (95% confidence interval, −0.23 to −0.11), with an increase from one to two dispensaries in a county resulting in a 17% decrease in opioid-related mortality rates and an increase from two to three dispensaries resulting in another decrease in opioid-related mortality of 8.5%.
When evaluating mortality by specific opioid type, the researchers found a negative association between the number of dispensaries and synthetic nonmethadone opioids, with an increase from one to two dispensaries resulting in a 21% decrease in mortality attributable to synthetic nonmethadone opioids (95% CI, −0.27 to −0.14; P = .002). There were also negative associations between the number of dispensaries and prescription opioid-related mortality rates (95% CI, −0.13 to −0.03) and heroin-related mortality rates (95% CI, −0.13 to −0.02). The negative association was similar in comparisons between synthetic nonmethadone opioid-related mortality and the number of dispensaries for medical cannabis (95% CI, −0.21 to −0.09; P = .002) and recreational cannabis (95% CI, −0.17 to −0.04; P = .01).
Evidence of a negative association between legalization of medical or recreational cannabis and opioid-related mortality has been mixed in the literature, with some studies also showing a “spurious or nonsignificant” association, according to Dr. Hsu and Dr. Kovács.
While previous studies have looked at the legalization of cannabis for medical or recreational use, legalization on its own is an “incomplete picture,” they said, which might offer one explanation for these mixed findings. Some states that legalize medical cannabis, for example, might not allow dispensaries to legally sell cannabis, and there may be a delay of 1-2 years between the time a state legalizes cannabis for recreational use and when dispensaries are open and available to the public.
“These results were obtained after controlling for county level population characteristics, yearly effects, whether recreational dispensaries were legal or not in the focal county’s state, and opioid-related state policies,” the authors wrote.
Results ‘may be even stronger’ than reported
Christopher G. Fichtner, MD, clinical professor of psychiatry and neuroscience at the University of California, Riverside, said in an interview that the evidence for using cannabis as an opioid substitution for pain management has not been balanced, but noted “the bulk of it suggests that there is some harm reduction benefit by having liberalized access to cannabis.”
One strength of the study by Dr. Hsu and Dr. Kovács was how they were able to examine implementation of legalization of medical or recreational cannabis, rather than simply a change in the law, he said.
“By looking at dispensary count, it’s actually looking at a better measure of on-the-ground implementation than just change in policy,” Dr. Fichtner explained. “You’re looking at what was actually accomplished in terms of making cannabis legally available.”
The choice to evaluate storefront dispensaries only and not include delivery services in their data, “probably makes it a relatively conservative estimate. I think that would be a strength, that their findings may be even stronger than what it is they’re reporting,” Dr. Fichtner said.
“I do think, if anything, the paper is relatively tentative about advancing its conclusions, which I think is a weakness in a lot of these studies,” he added. In 2017, the National Academy of Sciences released a report that found evidence cannabis or cannabinoids can significantly reduce pain symptoms. In that report, “one of their strongest conclusions is that there’s conclusive or substantial evidence that cannabis or cannabinoids are effective management of chronic pain,” Dr. Fichtner said.
He said that digging deeper into what kinds of pain cannabis can treat is one area for future research. “Certainly, it seems that it’s unlikely that cannabis is going to be good for every kind of pain,” he said. “What kinds of pain is it better for than others? Is it some benefit for many kinds of pain, or only a few types of pain?”
The authors reported no relevant financial disclosures. Dr. Fichtner is the author of a book on cannabis policy in the United States, but reported no other financial disclosures.
FROM BMJ
Kids already coping with mental disorders spiral as pandemic topples vital support systems
A bag of Doritos, that’s all Princess wanted.

Her mom calls her Princess, but her real name is Lindsey. She’s 17 and lives with her mom, Sandra, a nurse, outside Atlanta. On May 17, 2020, a Sunday, Lindsey decided she didn’t want breakfast; she wanted Doritos. So she left home and walked to Family Dollar, taking her pants off on the way, while her mom followed on foot, talking to the police on her phone as they went.
Lindsey has autism. It can be hard for her to communicate and navigate social situations. She thrives on routine and gets special help at school. Or got help, before the coronavirus pandemic closed schools and forced tens of millions of children to stay home. Sandra said that’s when their living hell started.
“It’s like her brain was wired,” she said. “She’d just put on her jacket, and she’s out the door. And I’m chasing her.”
On May 17, Sandra chased her all the way to Family Dollar. Hours later, Lindsey was in jail, charged with assaulting her mom. (KHN and NPR are not using the family’s last name.)
Lindsey is 1 of almost 3 million children in the United States who have a serious emotional or behavioral health condition. When the pandemic forced schools and doctors’ offices to close last spring, it also cut children off from the trained teachers and therapists who understand their needs.
As a result, many, like Lindsey, spiraled into EDs and even police custody. Federal data shows a nationwide surge of children in mental health crisis during the pandemic – a surge that’s further taxing an already overstretched safety net.
‘Take her’
Even after schools closed, Lindsey continued to wake up early, get dressed and wait for the bus. When she realized it had stopped coming, Sandra said, her daughter just started walking out of the house, wandering, a few times a week.
In those situations, Sandra did what many families in crisis report they’ve had to do since the pandemic began: Race through the short list of places she could call for help.
First, her state’s mental health crisis hotline. But they often put Sandra on hold.
“This is ridiculous,” she said of the wait. “It’s supposed to be a crisis team. But I’m on hold for 40, 50 minutes. And by the time you get on the phone, [the crisis] is done!”
Then there’s the local hospital’s ED, but Sandra said she had taken Lindsey there for previous crises and been told there isn’t much they can do.
That’s why, on May 17, when Lindsey walked to Family Dollar in just a red T-shirt and underwear to get that bag of Doritos, Sandra called the last option on her list: the police.
Sandra arrived at the store before the police and paid for the chips. According to Sandra and police records, when an officer approached, Lindsey grew agitated and hit her mom on the back, hard.
Sandra said she explained to the officer: “‘She’s autistic. You know, I’m okay. I’m a nurse. I just need to take her home and give her her medication.’ ”
Lindsey takes a mood stabilizer, but because she left home before breakfast, she hadn’t taken it that morning. The officer asked if Sandra wanted to take her to the nearest hospital.
The hospital wouldn’t be able to help Lindsey, Sandra said. It hadn’t before. “They already told me: ‘Ma’am, there’s nothing we can do.’ They just check her labs, it’s fine, and they ship her back home. There’s nothing [the hospital] can do,” she recalled telling the officer.
Sandra asked if the police could drive her daughter home so the teen could take her medication, but the officer said no, they couldn’t. The only other thing they could do, the officer said, was take Lindsey to jail for hitting her mom.
“I’ve tried everything,” Sandra said, exasperated. She paced the parking lot, feeling hopeless, sad and out of options. Finally, in tears, she told the officers: “Take her.”
Lindsey does not like to be touched and fought back when authorities tried to handcuff her. Several officers wrestled her to the ground. At that point, Sandra protested and said an officer threatened to arrest her, too, if she didn’t back away. Lindsey was taken to jail, where she spent much of the night until Sandra was able to post bail.
Clayton County Solicitor-General Charles Brooks denied that Sandra was threatened with arrest and said that, while Lindsey’s case is still pending, his office “is working to ensure that the resolution in this matter involves a plan for medication compliance and not punitive action.”
Sandra isn’t alone in her experience. Multiple families interviewed for this story reported similar experiences of calling in the police when a child was in crisis because caretakers didn’t feel they had any other option.
‘The whole system is really grinding to a halt’
Roughly 6% of U.S. children ages 6-17 years are living with serious emotional or behavioral difficulties, including children with autism, severe anxiety, depression and trauma-related mental health conditions.
Many of these children depend on schools for access to vital therapies. When schools and doctors’ offices stopped providing in-person services last spring, kids were untethered from the people and supports they rely on.

“The lack of in-person services is really detrimental,” said Susan Duffy, MD,a pediatrician and professor of emergency medicine at Brown University, Providence, R.I.
Marjorie, a mother in Florida, said her 15-year-old son has suffered during these disruptions. He has ADHD and oppositional defiant disorder, a condition marked by frequent and persistent hostility. Little things – like being asked to do schoolwork – can send him into a rage, leading to holes punched in walls, broken doors and violent threats. (The family’s last name or her son’s first name are not used to protect her son’s privacy and future prospects.)
The pandemic has shifted both school and her son’s therapy sessions online. But Marjorie said virtual therapy isn’t working because her son doesn’t focus well during sessions and tries to watch television instead. Lately, she has simply been canceling them.
“I was paying for appointments and there was no therapeutic value,” Marjorie said.
The issues cut across socioeconomic lines – affecting families with private insurance, like Marjorie, as well as those who receive coverage through Medicaid, a federal-state program that provides health insurance to low-income people and those with disabilities.
In the first few months of the pandemic, between March and May, children on Medicaid received 44% fewer outpatient mental health services – including therapy and in-home support – compared with the same time period in 2019, according to the Centers for Medicare & Medicaid Services. That’s even after accounting for increased telehealth appointments.
And while the nation’s EDs have seen a decline in overall visits, there was a relative increase in mental health visits for kids in 2020, compared with 2019.
The Centers for Disease Control and Prevention found that, from April to October 2020, hospitals across the United States saw a 24% increase in the proportion of mental health emergency visits for children aged 5-11 years, and a 31% increase for children aged 12-17.
“Not only are we seeing more children, more children are being admitted” to inpatient care.
That’s because there are fewer outpatient services now available to children, she said, and because the conditions of the children showing up at EDs “are more serious.”
This crisis is not only making life harder for these kids and their families, but it’s also stressing the entire health care system.
Child and adolescent psychiatrists working in hospitals around the country said children are increasingly “boarding” in EDs for days, waiting for inpatient admission to a regular hospital or psychiatric hospital.

Before the pandemic, there was already a shortage of inpatient psychiatric beds for children, said Christopher Bellonci, MD, a child psychiatrist at Judge Baker Children’s Center in Boston. That shortage has only gotten worse as hospitals cut capacity to allow for more physical distancing within psychiatric units.
“The whole system is really grinding to a halt at a time when we have unprecedented need,” Dr. Bellonci said.
‘A signal that the rest of your system doesn’t work’
Psychiatrists on the front lines share the frustrations of parents struggling to find help for their children.
Part of the problem is there have never been enough psychiatrists and therapists trained to work with children, intervening in the early stages of their illness, said Jennifer Havens, MD, a child psychiatrist at New York University.
“Tons of people showing up in emergency rooms in bad shape is a signal that the rest of your system doesn’t work,” she said.
Too often, Dr. Havens said, services aren’t available until children are older – and in crisis. “Often for people who don’t have access to services, we wait until they’re too big to be managed.”
While the pandemic has made life harder for Marjorie and her son in Florida, she said it has always been difficult to find the support and care he needs. Last fall, he needed a psychiatric evaluation, but the nearest specialist who would accept her commercial insurance was 100 miles away, in Alabama.
“Even when you have the money or you have the insurance, it is still a travesty,” Marjorie said. “You cannot get help for these kids.”
Parents are frustrated, and so are psychiatrists on the front lines. C.J. Glawe, MD, who leads the psychiatric crisis department at Nationwide Children’s Hospital in Columbus, Ohio, said that once a child is stabilized after a crisis it can be hard to explain to parents that they may not be able to find follow-up care anywhere near their home.
“Especially when I can clearly tell you I know exactly what you need, I just can’t give it to you,” Dr. Glawe said. “It’s demoralizing.”
When states and communities fail to provide children the services they need to live at home, kids can deteriorate and even wind up in jail, like Lindsey. At that point, Dr. Glawe said, the cost and level of care required will be even higher, whether that’s hospitalization or long stays in residential treatment facilities.
That’s exactly the scenario Sandra, Lindsey’s mom, is hoping to avoid for her Princess.
“For me, as a nurse and as a provider, that will be the last thing for my daughter,” she said. “It’s like [state and local leaders] leave it to the school and the parent to deal with, and they don’t care. And that’s the problem. It’s sad because, if I’m not here...”
Her voice trailed off as tears welled.
“She didn’t ask to have autism.”
To help families like Sandra’s and Marjorie’s, advocates said, all levels of government need to invest in creating a mental health system that’s accessible to anyone who needs it.
But given that many states have seen their revenues drop because of the pandemic, there’s a concern services will instead be cut – at a time when the need has never been greater.
This story is part of a reporting partnership that includes NPR, Illinois Public Media and Kaiser Health News. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
A bag of Doritos, that’s all Princess wanted.
Her mom calls her Princess, but her real name is Lindsey. She’s 17 and lives with her mom, Sandra, a nurse, outside Atlanta. On May 17, 2020, a Sunday, Lindsey decided she didn’t want breakfast; she wanted Doritos. So she left home and walked to Family Dollar, taking her pants off on the way, while her mom followed on foot, talking to the police on her phone as they went.
Lindsey has autism. It can be hard for her to communicate and navigate social situations. She thrives on routine and gets special help at school. Or got help, before the coronavirus pandemic closed schools and forced tens of millions of children to stay home. Sandra said that’s when their living hell started.
“It’s like her brain was wired,” she said. “She’d just put on her jacket, and she’s out the door. And I’m chasing her.”
On May 17, Sandra chased her all the way to Family Dollar. Hours later, Lindsey was in jail, charged with assaulting her mom. (KHN and NPR are not using the family’s last name.)
Lindsey is 1 of almost 3 million children in the United States who have a serious emotional or behavioral health condition. When the pandemic forced schools and doctors’ offices to close last spring, it also cut children off from the trained teachers and therapists who understand their needs.
As a result, many, like Lindsey, spiraled into EDs and even police custody. Federal data shows a nationwide surge of children in mental health crisis during the pandemic – a surge that’s further taxing an already overstretched safety net.
‘Take her’
Even after schools closed, Lindsey continued to wake up early, get dressed and wait for the bus. When she realized it had stopped coming, Sandra said, her daughter just started walking out of the house, wandering, a few times a week.
In those situations, Sandra did what many families in crisis report they’ve had to do since the pandemic began: Race through the short list of places she could call for help.
First, her state’s mental health crisis hotline. But they often put Sandra on hold.
“This is ridiculous,” she said of the wait. “It’s supposed to be a crisis team. But I’m on hold for 40, 50 minutes. And by the time you get on the phone, [the crisis] is done!”
Then there’s the local hospital’s ED, but Sandra said she had taken Lindsey there for previous crises and been told there isn’t much they can do.
That’s why, on May 17, when Lindsey walked to Family Dollar in just a red T-shirt and underwear to get that bag of Doritos, Sandra called the last option on her list: the police.
Sandra arrived at the store before the police and paid for the chips. According to Sandra and police records, when an officer approached, Lindsey grew agitated and hit her mom on the back, hard.
Sandra said she explained to the officer: “‘She’s autistic. You know, I’m okay. I’m a nurse. I just need to take her home and give her her medication.’ ”
Lindsey takes a mood stabilizer, but because she left home before breakfast, she hadn’t taken it that morning. The officer asked if Sandra wanted to take her to the nearest hospital.
The hospital wouldn’t be able to help Lindsey, Sandra said. It hadn’t before. “They already told me: ‘Ma’am, there’s nothing we can do.’ They just check her labs, it’s fine, and they ship her back home. There’s nothing [the hospital] can do,” she recalled telling the officer.
Sandra asked if the police could drive her daughter home so the teen could take her medication, but the officer said no, they couldn’t. The only other thing they could do, the officer said, was take Lindsey to jail for hitting her mom.
“I’ve tried everything,” Sandra said, exasperated. She paced the parking lot, feeling hopeless, sad and out of options. Finally, in tears, she told the officers: “Take her.”
Lindsey does not like to be touched and fought back when authorities tried to handcuff her. Several officers wrestled her to the ground. At that point, Sandra protested and said an officer threatened to arrest her, too, if she didn’t back away. Lindsey was taken to jail, where she spent much of the night until Sandra was able to post bail.
Clayton County Solicitor-General Charles Brooks denied that Sandra was threatened with arrest and said that, while Lindsey’s case is still pending, his office “is working to ensure that the resolution in this matter involves a plan for medication compliance and not punitive action.”
Sandra isn’t alone in her experience. Multiple families interviewed for this story reported similar experiences of calling in the police when a child was in crisis because caretakers didn’t feel they had any other option.
‘The whole system is really grinding to a halt’
Roughly 6% of U.S. children ages 6-17 years are living with serious emotional or behavioral difficulties, including children with autism, severe anxiety, depression and trauma-related mental health conditions.
Many of these children depend on schools for access to vital therapies. When schools and doctors’ offices stopped providing in-person services last spring, kids were untethered from the people and supports they rely on.
“The lack of in-person services is really detrimental,” said Susan Duffy, MD,a pediatrician and professor of emergency medicine at Brown University, Providence, R.I.
Marjorie, a mother in Florida, said her 15-year-old son has suffered during these disruptions. He has ADHD and oppositional defiant disorder, a condition marked by frequent and persistent hostility. Little things – like being asked to do schoolwork – can send him into a rage, leading to holes punched in walls, broken doors and violent threats. (The family’s last name or her son’s first name are not used to protect her son’s privacy and future prospects.)
The pandemic has shifted both school and her son’s therapy sessions online. But Marjorie said virtual therapy isn’t working because her son doesn’t focus well during sessions and tries to watch television instead. Lately, she has simply been canceling them.
“I was paying for appointments and there was no therapeutic value,” Marjorie said.
The issues cut across socioeconomic lines – affecting families with private insurance, like Marjorie, as well as those who receive coverage through Medicaid, a federal-state program that provides health insurance to low-income people and those with disabilities.
In the first few months of the pandemic, between March and May, children on Medicaid received 44% fewer outpatient mental health services – including therapy and in-home support – compared with the same time period in 2019, according to the Centers for Medicare & Medicaid Services. That’s even after accounting for increased telehealth appointments.
And while the nation’s EDs have seen a decline in overall visits, there was a relative increase in mental health visits for kids in 2020, compared with 2019.
The Centers for Disease Control and Prevention found that, from April to October 2020, hospitals across the United States saw a 24% increase in the proportion of mental health emergency visits for children aged 5-11 years, and a 31% increase for children aged 12-17.
“Not only are we seeing more children, more children are being admitted” to inpatient care.
That’s because there are fewer outpatient services now available to children, she said, and because the conditions of the children showing up at EDs “are more serious.”
This crisis is not only making life harder for these kids and their families, but it’s also stressing the entire health care system.
Child and adolescent psychiatrists working in hospitals around the country said children are increasingly “boarding” in EDs for days, waiting for inpatient admission to a regular hospital or psychiatric hospital.
Before the pandemic, there was already a shortage of inpatient psychiatric beds for children, said Christopher Bellonci, MD, a child psychiatrist at Judge Baker Children’s Center in Boston. That shortage has only gotten worse as hospitals cut capacity to allow for more physical distancing within psychiatric units.
“The whole system is really grinding to a halt at a time when we have unprecedented need,” Dr. Bellonci said.
‘A signal that the rest of your system doesn’t work’
Psychiatrists on the front lines share the frustrations of parents struggling to find help for their children.
Part of the problem is there have never been enough psychiatrists and therapists trained to work with children, intervening in the early stages of their illness, said Jennifer Havens, MD, a child psychiatrist at New York University.
“Tons of people showing up in emergency rooms in bad shape is a signal that the rest of your system doesn’t work,” she said.
Too often, Dr. Havens said, services aren’t available until children are older – and in crisis. “Often for people who don’t have access to services, we wait until they’re too big to be managed.”
While the pandemic has made life harder for Marjorie and her son in Florida, she said it has always been difficult to find the support and care he needs. Last fall, he needed a psychiatric evaluation, but the nearest specialist who would accept her commercial insurance was 100 miles away, in Alabama.
“Even when you have the money or you have the insurance, it is still a travesty,” Marjorie said. “You cannot get help for these kids.”
Parents are frustrated, and so are psychiatrists on the front lines. C.J. Glawe, MD, who leads the psychiatric crisis department at Nationwide Children’s Hospital in Columbus, Ohio, said that once a child is stabilized after a crisis it can be hard to explain to parents that they may not be able to find follow-up care anywhere near their home.
“Especially when I can clearly tell you I know exactly what you need, I just can’t give it to you,” Dr. Glawe said. “It’s demoralizing.”
When states and communities fail to provide children the services they need to live at home, kids can deteriorate and even wind up in jail, like Lindsey. At that point, Dr. Glawe said, the cost and level of care required will be even higher, whether that’s hospitalization or long stays in residential treatment facilities.
That’s exactly the scenario Sandra, Lindsey’s mom, is hoping to avoid for her Princess.
“For me, as a nurse and as a provider, that will be the last thing for my daughter,” she said. “It’s like [state and local leaders] leave it to the school and the parent to deal with, and they don’t care. And that’s the problem. It’s sad because, if I’m not here...”
Her voice trailed off as tears welled.
“She didn’t ask to have autism.”
To help families like Sandra’s and Marjorie’s, advocates said, all levels of government need to invest in creating a mental health system that’s accessible to anyone who needs it.
But given that many states have seen their revenues drop because of the pandemic, there’s a concern services will instead be cut – at a time when the need has never been greater.
This story is part of a reporting partnership that includes NPR, Illinois Public Media and Kaiser Health News. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
A bag of Doritos, that’s all Princess wanted.
Her mom calls her Princess, but her real name is Lindsey. She’s 17 and lives with her mom, Sandra, a nurse, outside Atlanta. On May 17, 2020, a Sunday, Lindsey decided she didn’t want breakfast; she wanted Doritos. So she left home and walked to Family Dollar, taking her pants off on the way, while her mom followed on foot, talking to the police on her phone as they went.
Lindsey has autism. It can be hard for her to communicate and navigate social situations. She thrives on routine and gets special help at school. Or got help, before the coronavirus pandemic closed schools and forced tens of millions of children to stay home. Sandra said that’s when their living hell started.
“It’s like her brain was wired,” she said. “She’d just put on her jacket, and she’s out the door. And I’m chasing her.”
On May 17, Sandra chased her all the way to Family Dollar. Hours later, Lindsey was in jail, charged with assaulting her mom. (KHN and NPR are not using the family’s last name.)
Lindsey is 1 of almost 3 million children in the United States who have a serious emotional or behavioral health condition. When the pandemic forced schools and doctors’ offices to close last spring, it also cut children off from the trained teachers and therapists who understand their needs.
As a result, many, like Lindsey, spiraled into EDs and even police custody. Federal data shows a nationwide surge of children in mental health crisis during the pandemic – a surge that’s further taxing an already overstretched safety net.
‘Take her’
Even after schools closed, Lindsey continued to wake up early, get dressed and wait for the bus. When she realized it had stopped coming, Sandra said, her daughter just started walking out of the house, wandering, a few times a week.
In those situations, Sandra did what many families in crisis report they’ve had to do since the pandemic began: Race through the short list of places she could call for help.
First, her state’s mental health crisis hotline. But they often put Sandra on hold.
“This is ridiculous,” she said of the wait. “It’s supposed to be a crisis team. But I’m on hold for 40, 50 minutes. And by the time you get on the phone, [the crisis] is done!”
Then there’s the local hospital’s ED, but Sandra said she had taken Lindsey there for previous crises and been told there isn’t much they can do.
That’s why, on May 17, when Lindsey walked to Family Dollar in just a red T-shirt and underwear to get that bag of Doritos, Sandra called the last option on her list: the police.
Sandra arrived at the store before the police and paid for the chips. According to Sandra and police records, when an officer approached, Lindsey grew agitated and hit her mom on the back, hard.
Sandra said she explained to the officer: “‘She’s autistic. You know, I’m okay. I’m a nurse. I just need to take her home and give her her medication.’ ”
Lindsey takes a mood stabilizer, but because she left home before breakfast, she hadn’t taken it that morning. The officer asked if Sandra wanted to take her to the nearest hospital.
The hospital wouldn’t be able to help Lindsey, Sandra said. It hadn’t before. “They already told me: ‘Ma’am, there’s nothing we can do.’ They just check her labs, it’s fine, and they ship her back home. There’s nothing [the hospital] can do,” she recalled telling the officer.
Sandra asked if the police could drive her daughter home so the teen could take her medication, but the officer said no, they couldn’t. The only other thing they could do, the officer said, was take Lindsey to jail for hitting her mom.
“I’ve tried everything,” Sandra said, exasperated. She paced the parking lot, feeling hopeless, sad and out of options. Finally, in tears, she told the officers: “Take her.”
Lindsey does not like to be touched and fought back when authorities tried to handcuff her. Several officers wrestled her to the ground. At that point, Sandra protested and said an officer threatened to arrest her, too, if she didn’t back away. Lindsey was taken to jail, where she spent much of the night until Sandra was able to post bail.
Clayton County Solicitor-General Charles Brooks denied that Sandra was threatened with arrest and said that, while Lindsey’s case is still pending, his office “is working to ensure that the resolution in this matter involves a plan for medication compliance and not punitive action.”
Sandra isn’t alone in her experience. Multiple families interviewed for this story reported similar experiences of calling in the police when a child was in crisis because caretakers didn’t feel they had any other option.
‘The whole system is really grinding to a halt’
Roughly 6% of U.S. children ages 6-17 years are living with serious emotional or behavioral difficulties, including children with autism, severe anxiety, depression and trauma-related mental health conditions.
Many of these children depend on schools for access to vital therapies. When schools and doctors’ offices stopped providing in-person services last spring, kids were untethered from the people and supports they rely on.
“The lack of in-person services is really detrimental,” said Susan Duffy, MD,a pediatrician and professor of emergency medicine at Brown University, Providence, R.I.
Marjorie, a mother in Florida, said her 15-year-old son has suffered during these disruptions. He has ADHD and oppositional defiant disorder, a condition marked by frequent and persistent hostility. Little things – like being asked to do schoolwork – can send him into a rage, leading to holes punched in walls, broken doors and violent threats. (The family’s last name or her son’s first name are not used to protect her son’s privacy and future prospects.)
The pandemic has shifted both school and her son’s therapy sessions online. But Marjorie said virtual therapy isn’t working because her son doesn’t focus well during sessions and tries to watch television instead. Lately, she has simply been canceling them.
“I was paying for appointments and there was no therapeutic value,” Marjorie said.
The issues cut across socioeconomic lines – affecting families with private insurance, like Marjorie, as well as those who receive coverage through Medicaid, a federal-state program that provides health insurance to low-income people and those with disabilities.
In the first few months of the pandemic, between March and May, children on Medicaid received 44% fewer outpatient mental health services – including therapy and in-home support – compared with the same time period in 2019, according to the Centers for Medicare & Medicaid Services. That’s even after accounting for increased telehealth appointments.
And while the nation’s EDs have seen a decline in overall visits, there was a relative increase in mental health visits for kids in 2020, compared with 2019.
The Centers for Disease Control and Prevention found that, from April to October 2020, hospitals across the United States saw a 24% increase in the proportion of mental health emergency visits for children aged 5-11 years, and a 31% increase for children aged 12-17.
“Not only are we seeing more children, more children are being admitted” to inpatient care.
That’s because there are fewer outpatient services now available to children, she said, and because the conditions of the children showing up at EDs “are more serious.”
This crisis is not only making life harder for these kids and their families, but it’s also stressing the entire health care system.
Child and adolescent psychiatrists working in hospitals around the country said children are increasingly “boarding” in EDs for days, waiting for inpatient admission to a regular hospital or psychiatric hospital.
Before the pandemic, there was already a shortage of inpatient psychiatric beds for children, said Christopher Bellonci, MD, a child psychiatrist at Judge Baker Children’s Center in Boston. That shortage has only gotten worse as hospitals cut capacity to allow for more physical distancing within psychiatric units.
“The whole system is really grinding to a halt at a time when we have unprecedented need,” Dr. Bellonci said.
‘A signal that the rest of your system doesn’t work’
Psychiatrists on the front lines share the frustrations of parents struggling to find help for their children.
Part of the problem is there have never been enough psychiatrists and therapists trained to work with children, intervening in the early stages of their illness, said Jennifer Havens, MD, a child psychiatrist at New York University.
“Tons of people showing up in emergency rooms in bad shape is a signal that the rest of your system doesn’t work,” she said.
Too often, Dr. Havens said, services aren’t available until children are older – and in crisis. “Often for people who don’t have access to services, we wait until they’re too big to be managed.”
While the pandemic has made life harder for Marjorie and her son in Florida, she said it has always been difficult to find the support and care he needs. Last fall, he needed a psychiatric evaluation, but the nearest specialist who would accept her commercial insurance was 100 miles away, in Alabama.
“Even when you have the money or you have the insurance, it is still a travesty,” Marjorie said. “You cannot get help for these kids.”
Parents are frustrated, and so are psychiatrists on the front lines. C.J. Glawe, MD, who leads the psychiatric crisis department at Nationwide Children’s Hospital in Columbus, Ohio, said that once a child is stabilized after a crisis it can be hard to explain to parents that they may not be able to find follow-up care anywhere near their home.
“Especially when I can clearly tell you I know exactly what you need, I just can’t give it to you,” Dr. Glawe said. “It’s demoralizing.”
When states and communities fail to provide children the services they need to live at home, kids can deteriorate and even wind up in jail, like Lindsey. At that point, Dr. Glawe said, the cost and level of care required will be even higher, whether that’s hospitalization or long stays in residential treatment facilities.
That’s exactly the scenario Sandra, Lindsey’s mom, is hoping to avoid for her Princess.
“For me, as a nurse and as a provider, that will be the last thing for my daughter,” she said. “It’s like [state and local leaders] leave it to the school and the parent to deal with, and they don’t care. And that’s the problem. It’s sad because, if I’m not here...”
Her voice trailed off as tears welled.
“She didn’t ask to have autism.”
To help families like Sandra’s and Marjorie’s, advocates said, all levels of government need to invest in creating a mental health system that’s accessible to anyone who needs it.
But given that many states have seen their revenues drop because of the pandemic, there’s a concern services will instead be cut – at a time when the need has never been greater.
This story is part of a reporting partnership that includes NPR, Illinois Public Media and Kaiser Health News. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.