User login
Key driver of fish oil’s antidepressant effects revealed
A key molecular mechanism underpinning the anti-inflammatory, antidepressant, and neuroprotective effects of omega-3 fatty acids has been identified. In findings that could lead to the development of new treatments for depression, the research provides the “first evidence” that hippocampal neurons are able to produce two key lipid metabolites of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) – lipoxygenase and cytochrome P450, lead investigator Alessandra Borsini, PhD, told this news organization.
This is how EPA and DHA exert their anti-inflammatory and neurogenic properties in vitro, as well as antidepressant properties in patients with depression, said Dr. Borsini, from King’s College London.
“Indeed, we found evidence for a correlation between increased levels of these metabolites and a decrease in severity of depressive symptoms in patients with major depressive disorder,” Dr. Borsini said.
The study was published online June 16 in Molecular Psychiatry.
‘Depression in a dish’
Despite the known role of inflammation in depression, there remains a lack of data showing anti-inflammatory strategies that are effective, safe for everyday use, and with a clear mechanism of action, the researchers note.
Dr. Borsini and colleagues tested the theory that when EPA and DHA are metabolized, some of their metabolites, or lipid mediators, can protect the brain from the harmful effects of inflammation. They used a validated “depression in a dish” in vitro human hippocampal cell model to test their theory.
They found that treating human hippocampal cells with EPA or DHA before exposing them to cytokines prevented increased cell death and decreased neurogenesis. Both these impacts had been previously observed in cells exposed to cytokines alone.
They confirmed that these effects were mediated by the formation of several key lipid mediators produced by EPA and DHA – namely hydroxyeicosapentaenoic acid, hydroxydocosahexaenoic acid, epoxyeicosatetraenoic acid (EpETE), and epoxydocosapentaenoic acid (EpDPA).
It’s the first time these lipid mediators were detected in human hippocampal neurons, the researchers say.
They also found that treating the neurons with an enzyme inhibitor increased the availability of two of these metabolites (EpETE and EpDPA), suggesting a possible way by which future treatments could be optimized.
The findings were replicated in 22 patients with major depression given either EPA (3 g/day) or DHA (1.4 g/day) for 12 weeks. In both groups, EPA or DHA treatment was associated with an increase in their respective metabolites and significant improvement in depressive symptoms.
The average reduction in symptom scores was 64% and 71% in the EPA and DHA groups, respectively, and there was some evidence that higher levels of the same metabolites correlated with less severe depressive symptoms.
“For some time we have known that omega-3 [polyunsaturated fatty acid (PUFA)] can induce antidepressant and anti-inflammatory effects, but, without further understanding of how this happens in the human brain, it has been difficult to develop treatments,” Dr. Borsini said in a news release.
“ which can inform the development of potential new treatments for depression using omega-3 PUFA,” Dr. Borsini added.
“We need to be cautious when interpreting data generated from the correlation between levels of metabolites and depressive symptoms as findings require further validation in a bigger sample of patients,” Dr. Borsini said.
“It is important to highlight that our research has not shown that by simply increasing omega-3 fatty acids in our diets or through taking nutritional supplements we can reduce inflammation or depression,” study author Carmine Pariante, MD, PhD, from King’s College London, said in the news release.
“The mechanisms behind the associations between depression and omega-3 PUFA are complicated and require further research and clinical trials to fully understand how they work and inform future therapeutic approaches,” Dr. Pariante said.
No clinical implications
Weighing in on this research in a Science Media Centre statement, Kevin McConway, emeritus professor of applied statistics, The Open University, Milton Keynes, United Kingdom, said, “The point of the study was to throw some light on the mechanisms in the body by which omega-3 fatty acids might work to reduce inflammation or depression.”
“The research mostly involved cells in laboratory dishes, but it also involved treating a small sample of patients with major depression by giving them supplements of one or other of the two omega-3 acids under investigation for 12 weeks,” he noted.
“The researchers found that the patients’ average scores on a standard set of questions, used to diagnose and measure depression, improved over that 12-week period, for each of the two fatty acids.
While depression symptoms improved over 12 weeks with omega-3 fatty acid treatment, “depression symptoms change over time anyway, for many reasons,” and depressive symptoms might have improved over 12 weeks even if the patients had not been given the omega-3 acids, Dr. McConway said.
“We just can’t tell since every patient got omega-3 fatty acids. So these results can hint that omega-3 fatty acids might help in depression, but it comes nowhere near showing that this is the case with a reasonable degree of certainty,” he cautioned.
“Indeed the researchers did not carry out this part of their study to see whether the omega-3 supplements help with depression – they did it to see whether the biochemical changes that they had seen in cell cultures in the lab might also occur in human bodies,” he noted.
This research was funded in part by grants to the investigators from the U.K. Medical Research Council, the European Commission Horizon 2020, and the National Institute for Health Research (NIHR), Maudsley Biomedical Research Centre (BRC) at South London and Maudsley NHS Foundation Trust and King’s College London. Dr. Borsini has received research funding from Johnson & Johnson for research on depression and inflammation. Dr. McConway is a trustee of the Science Media Centre and a member of its advisory committee.
A version of this article first appeared on Medscape.com.
A key molecular mechanism underpinning the anti-inflammatory, antidepressant, and neuroprotective effects of omega-3 fatty acids has been identified. In findings that could lead to the development of new treatments for depression, the research provides the “first evidence” that hippocampal neurons are able to produce two key lipid metabolites of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) – lipoxygenase and cytochrome P450, lead investigator Alessandra Borsini, PhD, told this news organization.
This is how EPA and DHA exert their anti-inflammatory and neurogenic properties in vitro, as well as antidepressant properties in patients with depression, said Dr. Borsini, from King’s College London.
“Indeed, we found evidence for a correlation between increased levels of these metabolites and a decrease in severity of depressive symptoms in patients with major depressive disorder,” Dr. Borsini said.
The study was published online June 16 in Molecular Psychiatry.
‘Depression in a dish’
Despite the known role of inflammation in depression, there remains a lack of data showing anti-inflammatory strategies that are effective, safe for everyday use, and with a clear mechanism of action, the researchers note.
Dr. Borsini and colleagues tested the theory that when EPA and DHA are metabolized, some of their metabolites, or lipid mediators, can protect the brain from the harmful effects of inflammation. They used a validated “depression in a dish” in vitro human hippocampal cell model to test their theory.
They found that treating human hippocampal cells with EPA or DHA before exposing them to cytokines prevented increased cell death and decreased neurogenesis. Both these impacts had been previously observed in cells exposed to cytokines alone.
They confirmed that these effects were mediated by the formation of several key lipid mediators produced by EPA and DHA – namely hydroxyeicosapentaenoic acid, hydroxydocosahexaenoic acid, epoxyeicosatetraenoic acid (EpETE), and epoxydocosapentaenoic acid (EpDPA).
It’s the first time these lipid mediators were detected in human hippocampal neurons, the researchers say.
They also found that treating the neurons with an enzyme inhibitor increased the availability of two of these metabolites (EpETE and EpDPA), suggesting a possible way by which future treatments could be optimized.
The findings were replicated in 22 patients with major depression given either EPA (3 g/day) or DHA (1.4 g/day) for 12 weeks. In both groups, EPA or DHA treatment was associated with an increase in their respective metabolites and significant improvement in depressive symptoms.
The average reduction in symptom scores was 64% and 71% in the EPA and DHA groups, respectively, and there was some evidence that higher levels of the same metabolites correlated with less severe depressive symptoms.
“For some time we have known that omega-3 [polyunsaturated fatty acid (PUFA)] can induce antidepressant and anti-inflammatory effects, but, without further understanding of how this happens in the human brain, it has been difficult to develop treatments,” Dr. Borsini said in a news release.
“ which can inform the development of potential new treatments for depression using omega-3 PUFA,” Dr. Borsini added.
“We need to be cautious when interpreting data generated from the correlation between levels of metabolites and depressive symptoms as findings require further validation in a bigger sample of patients,” Dr. Borsini said.
“It is important to highlight that our research has not shown that by simply increasing omega-3 fatty acids in our diets or through taking nutritional supplements we can reduce inflammation or depression,” study author Carmine Pariante, MD, PhD, from King’s College London, said in the news release.
“The mechanisms behind the associations between depression and omega-3 PUFA are complicated and require further research and clinical trials to fully understand how they work and inform future therapeutic approaches,” Dr. Pariante said.
No clinical implications
Weighing in on this research in a Science Media Centre statement, Kevin McConway, emeritus professor of applied statistics, The Open University, Milton Keynes, United Kingdom, said, “The point of the study was to throw some light on the mechanisms in the body by which omega-3 fatty acids might work to reduce inflammation or depression.”
“The research mostly involved cells in laboratory dishes, but it also involved treating a small sample of patients with major depression by giving them supplements of one or other of the two omega-3 acids under investigation for 12 weeks,” he noted.
“The researchers found that the patients’ average scores on a standard set of questions, used to diagnose and measure depression, improved over that 12-week period, for each of the two fatty acids.
While depression symptoms improved over 12 weeks with omega-3 fatty acid treatment, “depression symptoms change over time anyway, for many reasons,” and depressive symptoms might have improved over 12 weeks even if the patients had not been given the omega-3 acids, Dr. McConway said.
“We just can’t tell since every patient got omega-3 fatty acids. So these results can hint that omega-3 fatty acids might help in depression, but it comes nowhere near showing that this is the case with a reasonable degree of certainty,” he cautioned.
“Indeed the researchers did not carry out this part of their study to see whether the omega-3 supplements help with depression – they did it to see whether the biochemical changes that they had seen in cell cultures in the lab might also occur in human bodies,” he noted.
This research was funded in part by grants to the investigators from the U.K. Medical Research Council, the European Commission Horizon 2020, and the National Institute for Health Research (NIHR), Maudsley Biomedical Research Centre (BRC) at South London and Maudsley NHS Foundation Trust and King’s College London. Dr. Borsini has received research funding from Johnson & Johnson for research on depression and inflammation. Dr. McConway is a trustee of the Science Media Centre and a member of its advisory committee.
A version of this article first appeared on Medscape.com.
A key molecular mechanism underpinning the anti-inflammatory, antidepressant, and neuroprotective effects of omega-3 fatty acids has been identified. In findings that could lead to the development of new treatments for depression, the research provides the “first evidence” that hippocampal neurons are able to produce two key lipid metabolites of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) – lipoxygenase and cytochrome P450, lead investigator Alessandra Borsini, PhD, told this news organization.
This is how EPA and DHA exert their anti-inflammatory and neurogenic properties in vitro, as well as antidepressant properties in patients with depression, said Dr. Borsini, from King’s College London.
“Indeed, we found evidence for a correlation between increased levels of these metabolites and a decrease in severity of depressive symptoms in patients with major depressive disorder,” Dr. Borsini said.
The study was published online June 16 in Molecular Psychiatry.
‘Depression in a dish’
Despite the known role of inflammation in depression, there remains a lack of data showing anti-inflammatory strategies that are effective, safe for everyday use, and with a clear mechanism of action, the researchers note.
Dr. Borsini and colleagues tested the theory that when EPA and DHA are metabolized, some of their metabolites, or lipid mediators, can protect the brain from the harmful effects of inflammation. They used a validated “depression in a dish” in vitro human hippocampal cell model to test their theory.
They found that treating human hippocampal cells with EPA or DHA before exposing them to cytokines prevented increased cell death and decreased neurogenesis. Both these impacts had been previously observed in cells exposed to cytokines alone.
They confirmed that these effects were mediated by the formation of several key lipid mediators produced by EPA and DHA – namely hydroxyeicosapentaenoic acid, hydroxydocosahexaenoic acid, epoxyeicosatetraenoic acid (EpETE), and epoxydocosapentaenoic acid (EpDPA).
It’s the first time these lipid mediators were detected in human hippocampal neurons, the researchers say.
They also found that treating the neurons with an enzyme inhibitor increased the availability of two of these metabolites (EpETE and EpDPA), suggesting a possible way by which future treatments could be optimized.
The findings were replicated in 22 patients with major depression given either EPA (3 g/day) or DHA (1.4 g/day) for 12 weeks. In both groups, EPA or DHA treatment was associated with an increase in their respective metabolites and significant improvement in depressive symptoms.
The average reduction in symptom scores was 64% and 71% in the EPA and DHA groups, respectively, and there was some evidence that higher levels of the same metabolites correlated with less severe depressive symptoms.
“For some time we have known that omega-3 [polyunsaturated fatty acid (PUFA)] can induce antidepressant and anti-inflammatory effects, but, without further understanding of how this happens in the human brain, it has been difficult to develop treatments,” Dr. Borsini said in a news release.
“ which can inform the development of potential new treatments for depression using omega-3 PUFA,” Dr. Borsini added.
“We need to be cautious when interpreting data generated from the correlation between levels of metabolites and depressive symptoms as findings require further validation in a bigger sample of patients,” Dr. Borsini said.
“It is important to highlight that our research has not shown that by simply increasing omega-3 fatty acids in our diets or through taking nutritional supplements we can reduce inflammation or depression,” study author Carmine Pariante, MD, PhD, from King’s College London, said in the news release.
“The mechanisms behind the associations between depression and omega-3 PUFA are complicated and require further research and clinical trials to fully understand how they work and inform future therapeutic approaches,” Dr. Pariante said.
No clinical implications
Weighing in on this research in a Science Media Centre statement, Kevin McConway, emeritus professor of applied statistics, The Open University, Milton Keynes, United Kingdom, said, “The point of the study was to throw some light on the mechanisms in the body by which omega-3 fatty acids might work to reduce inflammation or depression.”
“The research mostly involved cells in laboratory dishes, but it also involved treating a small sample of patients with major depression by giving them supplements of one or other of the two omega-3 acids under investigation for 12 weeks,” he noted.
“The researchers found that the patients’ average scores on a standard set of questions, used to diagnose and measure depression, improved over that 12-week period, for each of the two fatty acids.
While depression symptoms improved over 12 weeks with omega-3 fatty acid treatment, “depression symptoms change over time anyway, for many reasons,” and depressive symptoms might have improved over 12 weeks even if the patients had not been given the omega-3 acids, Dr. McConway said.
“We just can’t tell since every patient got omega-3 fatty acids. So these results can hint that omega-3 fatty acids might help in depression, but it comes nowhere near showing that this is the case with a reasonable degree of certainty,” he cautioned.
“Indeed the researchers did not carry out this part of their study to see whether the omega-3 supplements help with depression – they did it to see whether the biochemical changes that they had seen in cell cultures in the lab might also occur in human bodies,” he noted.
This research was funded in part by grants to the investigators from the U.K. Medical Research Council, the European Commission Horizon 2020, and the National Institute for Health Research (NIHR), Maudsley Biomedical Research Centre (BRC) at South London and Maudsley NHS Foundation Trust and King’s College London. Dr. Borsini has received research funding from Johnson & Johnson for research on depression and inflammation. Dr. McConway is a trustee of the Science Media Centre and a member of its advisory committee.
A version of this article first appeared on Medscape.com.
AI-based software demonstrates accuracy in diagnosis of autism
A software program based on artificial intelligence (AI) is effective for distinguishing young children with autism spectrum disorder (ASD) from those with other conditions, according to results of a pivotal trial presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
The AI-based software, which will be submitted to regulatory approval as a device, employs an algorithm that assembles inputs from a caregiver questionnaire, a video, and a clinician questionnaire, according to Sharief Taraman, MD, a pediatric neurologist at CHOC, a pediatric health care system in Orange County, Calif.
Although the device could be employed in a variety of settings, it is envisioned for use by primary care physicians. This will circumvent the need for specialist evaluation except in challenging cases. Currently, nearly all children with ASD are diagnosed in specialty care, according to data cited by Dr. Taraman.
“The lack of diagnostic tools for ASD in primary care settings contributes to an average delay of 3 years between first parental concern and diagnosis and to long wait lists for specialty evaluation,” he reported at the virtual meeting, presented by MedscapeLive.
When used with clinical judgment and criteria from the American Psychiatric Association’s 5th edition of the Diagnostic and Statistical Manual (DSM-5), the data from the trial suggest the diagnostic tool in the hands of primary care physicians “could efficiently and accurately assess ASD in children 18 to 72 months old,” said Dr. Taraman, also an associate clinical professor of pediatrics at the University of California, Irvine.*
The AI-assisted software was evaluated in 425 children at 14 sites in 6 states. The study population was reflective of U.S. demographics. Although only 36% of the children were female, this is consistent with ASD prevalence. Only 60% of the subjects were White. Nearly 30% were Black or Latinx and other populations, such as those of Asian heritage, were represented.
Children between the ages of 18 and 72 months were eligible if both a caregiver and a health care professional were concerned that the child had ASD. About the same time that a caregiver completed a 20-item questionnaire and the primary care physician completed a 15-item questionnaire on a mobile device, the caregiver uploaded two videos of 1-2 minutes in length.
This information, along with a 33-item questionnaire completed by an analyst of the submitted videos, was then processed by the software algorithm. It provided a patient status of positive or negative for ASD, or it concluded that the status was indeterminate.
“To reduce the risk of false classifications, the indeterminate status was included as a safety feature,” Dr. Taraman explained. However, Dr. Taraman considers an indeterminate designation potentially actionable. Rather than a negative result, this status suggests a complex neurodevelopmental disorder and indicates the need for further evaluation.
The reference standard diagnosis, completed in all participants in this study, was a specialist evaluation completed independently by two experts. The presence or absence of ASD was confirmed if the experts agreed. If they did not, a third specialist made the final determination.
In comparison to the specialist determinations, all were correctly classified except for one child, in which the software was determined to have made a false-negative diagnosis. A diagnosis of ASD was reached in 29% of the study participants.
For those with a determinate designation, the sensitivity was 98.4% and the specificity was 78.9%. This translated into positive predictive and negative predictive values of 80.8% and 98.3%, respectively.
Of those identified as indeterminate by the AI-assisted algorithm, 91% were ultimately considered by specialist evaluation to have complex issues. In this group, ASD was part of the complex clinical picture in 20%. The others had non-ASD neurodevelopmental conditions, according to Dr. Taraman.
When the accuracy was evaluated across ages, ethnicity, and factors such as parent education or family income, the tool performed consistently, Dr. Taraman reported. This is important, he said, because the presence or absence of ASD is misdiagnosed in many underserved populations.
The focus on developing a methodology specific for use in primary care was based on evidence that the delay in the diagnosis of ASD is attributable to long wait times for specialty evaluations.
“There will never be enough specialists. There is a need for a way to streamline the diagnosis of ASD,” Dr. Taraman maintained. This is helpful not only to parents concerned about their children, he said, but also there are data to suggest that early intervention improves outcomes.
A specialist in ASD, Paul Carbone, MD, medical director of the child development program at the University of Utah, Salt Lake City, agreed. He said early diagnosis and intervention should be a goal.
“Reducing the age of ASD diagnosis is a priority because early entry into autism-specific interventions is a strong predictor of optimal developmental outcomes for children,” Dr. Carbone said.
Although he is not familiar with this experimental AI-assisted diagnostic program, he has published on the feasibility of ASD diagnosis at the primary care level. In his study, Dr. Carbone examined the Modified Checklist for Autism in Toddlers (M-CHAT) as one of several methodologies that might be considered.
Diagnosis of ASD “can be achieved through systematic processes within primary care that facilitate universal development surveillance and autism screening followed by prompt and timely diagnostic evaluations of at-risk children,” Dr. Carbone said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Taraman reported a financial relationship with Cognoa, the company that is developing the ASD software for clinical use. Dr. Carbone reported that he has no conflicts of interest.
*Updated, 7/7/21
A software program based on artificial intelligence (AI) is effective for distinguishing young children with autism spectrum disorder (ASD) from those with other conditions, according to results of a pivotal trial presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
The AI-based software, which will be submitted to regulatory approval as a device, employs an algorithm that assembles inputs from a caregiver questionnaire, a video, and a clinician questionnaire, according to Sharief Taraman, MD, a pediatric neurologist at CHOC, a pediatric health care system in Orange County, Calif.
Although the device could be employed in a variety of settings, it is envisioned for use by primary care physicians. This will circumvent the need for specialist evaluation except in challenging cases. Currently, nearly all children with ASD are diagnosed in specialty care, according to data cited by Dr. Taraman.
“The lack of diagnostic tools for ASD in primary care settings contributes to an average delay of 3 years between first parental concern and diagnosis and to long wait lists for specialty evaluation,” he reported at the virtual meeting, presented by MedscapeLive.
When used with clinical judgment and criteria from the American Psychiatric Association’s 5th edition of the Diagnostic and Statistical Manual (DSM-5), the data from the trial suggest the diagnostic tool in the hands of primary care physicians “could efficiently and accurately assess ASD in children 18 to 72 months old,” said Dr. Taraman, also an associate clinical professor of pediatrics at the University of California, Irvine.*
The AI-assisted software was evaluated in 425 children at 14 sites in 6 states. The study population was reflective of U.S. demographics. Although only 36% of the children were female, this is consistent with ASD prevalence. Only 60% of the subjects were White. Nearly 30% were Black or Latinx and other populations, such as those of Asian heritage, were represented.
Children between the ages of 18 and 72 months were eligible if both a caregiver and a health care professional were concerned that the child had ASD. About the same time that a caregiver completed a 20-item questionnaire and the primary care physician completed a 15-item questionnaire on a mobile device, the caregiver uploaded two videos of 1-2 minutes in length.
This information, along with a 33-item questionnaire completed by an analyst of the submitted videos, was then processed by the software algorithm. It provided a patient status of positive or negative for ASD, or it concluded that the status was indeterminate.
“To reduce the risk of false classifications, the indeterminate status was included as a safety feature,” Dr. Taraman explained. However, Dr. Taraman considers an indeterminate designation potentially actionable. Rather than a negative result, this status suggests a complex neurodevelopmental disorder and indicates the need for further evaluation.
The reference standard diagnosis, completed in all participants in this study, was a specialist evaluation completed independently by two experts. The presence or absence of ASD was confirmed if the experts agreed. If they did not, a third specialist made the final determination.
In comparison to the specialist determinations, all were correctly classified except for one child, in which the software was determined to have made a false-negative diagnosis. A diagnosis of ASD was reached in 29% of the study participants.
For those with a determinate designation, the sensitivity was 98.4% and the specificity was 78.9%. This translated into positive predictive and negative predictive values of 80.8% and 98.3%, respectively.
Of those identified as indeterminate by the AI-assisted algorithm, 91% were ultimately considered by specialist evaluation to have complex issues. In this group, ASD was part of the complex clinical picture in 20%. The others had non-ASD neurodevelopmental conditions, according to Dr. Taraman.
When the accuracy was evaluated across ages, ethnicity, and factors such as parent education or family income, the tool performed consistently, Dr. Taraman reported. This is important, he said, because the presence or absence of ASD is misdiagnosed in many underserved populations.
The focus on developing a methodology specific for use in primary care was based on evidence that the delay in the diagnosis of ASD is attributable to long wait times for specialty evaluations.
“There will never be enough specialists. There is a need for a way to streamline the diagnosis of ASD,” Dr. Taraman maintained. This is helpful not only to parents concerned about their children, he said, but also there are data to suggest that early intervention improves outcomes.
A specialist in ASD, Paul Carbone, MD, medical director of the child development program at the University of Utah, Salt Lake City, agreed. He said early diagnosis and intervention should be a goal.
“Reducing the age of ASD diagnosis is a priority because early entry into autism-specific interventions is a strong predictor of optimal developmental outcomes for children,” Dr. Carbone said.
Although he is not familiar with this experimental AI-assisted diagnostic program, he has published on the feasibility of ASD diagnosis at the primary care level. In his study, Dr. Carbone examined the Modified Checklist for Autism in Toddlers (M-CHAT) as one of several methodologies that might be considered.
Diagnosis of ASD “can be achieved through systematic processes within primary care that facilitate universal development surveillance and autism screening followed by prompt and timely diagnostic evaluations of at-risk children,” Dr. Carbone said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Taraman reported a financial relationship with Cognoa, the company that is developing the ASD software for clinical use. Dr. Carbone reported that he has no conflicts of interest.
*Updated, 7/7/21
A software program based on artificial intelligence (AI) is effective for distinguishing young children with autism spectrum disorder (ASD) from those with other conditions, according to results of a pivotal trial presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
The AI-based software, which will be submitted to regulatory approval as a device, employs an algorithm that assembles inputs from a caregiver questionnaire, a video, and a clinician questionnaire, according to Sharief Taraman, MD, a pediatric neurologist at CHOC, a pediatric health care system in Orange County, Calif.
Although the device could be employed in a variety of settings, it is envisioned for use by primary care physicians. This will circumvent the need for specialist evaluation except in challenging cases. Currently, nearly all children with ASD are diagnosed in specialty care, according to data cited by Dr. Taraman.
“The lack of diagnostic tools for ASD in primary care settings contributes to an average delay of 3 years between first parental concern and diagnosis and to long wait lists for specialty evaluation,” he reported at the virtual meeting, presented by MedscapeLive.
When used with clinical judgment and criteria from the American Psychiatric Association’s 5th edition of the Diagnostic and Statistical Manual (DSM-5), the data from the trial suggest the diagnostic tool in the hands of primary care physicians “could efficiently and accurately assess ASD in children 18 to 72 months old,” said Dr. Taraman, also an associate clinical professor of pediatrics at the University of California, Irvine.*
The AI-assisted software was evaluated in 425 children at 14 sites in 6 states. The study population was reflective of U.S. demographics. Although only 36% of the children were female, this is consistent with ASD prevalence. Only 60% of the subjects were White. Nearly 30% were Black or Latinx and other populations, such as those of Asian heritage, were represented.
Children between the ages of 18 and 72 months were eligible if both a caregiver and a health care professional were concerned that the child had ASD. About the same time that a caregiver completed a 20-item questionnaire and the primary care physician completed a 15-item questionnaire on a mobile device, the caregiver uploaded two videos of 1-2 minutes in length.
This information, along with a 33-item questionnaire completed by an analyst of the submitted videos, was then processed by the software algorithm. It provided a patient status of positive or negative for ASD, or it concluded that the status was indeterminate.
“To reduce the risk of false classifications, the indeterminate status was included as a safety feature,” Dr. Taraman explained. However, Dr. Taraman considers an indeterminate designation potentially actionable. Rather than a negative result, this status suggests a complex neurodevelopmental disorder and indicates the need for further evaluation.
The reference standard diagnosis, completed in all participants in this study, was a specialist evaluation completed independently by two experts. The presence or absence of ASD was confirmed if the experts agreed. If they did not, a third specialist made the final determination.
In comparison to the specialist determinations, all were correctly classified except for one child, in which the software was determined to have made a false-negative diagnosis. A diagnosis of ASD was reached in 29% of the study participants.
For those with a determinate designation, the sensitivity was 98.4% and the specificity was 78.9%. This translated into positive predictive and negative predictive values of 80.8% and 98.3%, respectively.
Of those identified as indeterminate by the AI-assisted algorithm, 91% were ultimately considered by specialist evaluation to have complex issues. In this group, ASD was part of the complex clinical picture in 20%. The others had non-ASD neurodevelopmental conditions, according to Dr. Taraman.
When the accuracy was evaluated across ages, ethnicity, and factors such as parent education or family income, the tool performed consistently, Dr. Taraman reported. This is important, he said, because the presence or absence of ASD is misdiagnosed in many underserved populations.
The focus on developing a methodology specific for use in primary care was based on evidence that the delay in the diagnosis of ASD is attributable to long wait times for specialty evaluations.
“There will never be enough specialists. There is a need for a way to streamline the diagnosis of ASD,” Dr. Taraman maintained. This is helpful not only to parents concerned about their children, he said, but also there are data to suggest that early intervention improves outcomes.
A specialist in ASD, Paul Carbone, MD, medical director of the child development program at the University of Utah, Salt Lake City, agreed. He said early diagnosis and intervention should be a goal.
“Reducing the age of ASD diagnosis is a priority because early entry into autism-specific interventions is a strong predictor of optimal developmental outcomes for children,” Dr. Carbone said.
Although he is not familiar with this experimental AI-assisted diagnostic program, he has published on the feasibility of ASD diagnosis at the primary care level. In his study, Dr. Carbone examined the Modified Checklist for Autism in Toddlers (M-CHAT) as one of several methodologies that might be considered.
Diagnosis of ASD “can be achieved through systematic processes within primary care that facilitate universal development surveillance and autism screening followed by prompt and timely diagnostic evaluations of at-risk children,” Dr. Carbone said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Taraman reported a financial relationship with Cognoa, the company that is developing the ASD software for clinical use. Dr. Carbone reported that he has no conflicts of interest.
*Updated, 7/7/21
FROM CP/AACP PSYCHIATRY UPDATE
Risk to infant may warrant drug treatment for postpartum depression
If moderate to severe postpartum depression poses a risk to child development, that argues in favor of pharmacologic therapy, according to a detailed risk-benefit assessment presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.

“It is important to consider that there are potential risks of antidepressant drugs, but there are also potential risks from not providing effective treatment,” reported Neha Hudepohl, MD, at the virtual meeting, presented by MedscapeLive.
On a website maintained by the Centers for Disease Control and Prevention, the question of whether antidepressants pose a risk to breast-feeding children is answered with a “maybe.” Although many of these drugs can be detected in breast milk, according to the CDC, “most have little or no effect on milk supply or on infant well-being.”
This is enough uncertainty that antidepressants are not first-line intervention when postpartum depression is mild, said Dr. Hudepohl, director of women’s mental health at Prisma Health Upstate, Greenville, S.C. However, she noted that the American College of Obstetricians and Gynecologists is among the organizations that recommend drug treatment if symptoms are moderate to severe.
“Depression in the mother affects interactions in feeding practices, sleep routines and patterns, and safety practices,” said Dr. Hudepohl, citing published studies supporting each of these consequences.
For the child, there is some degree of uncertainty about risk from untreated maternal depression as well as from breast mild exposure to antidepressants. Conclusive statements are not offered by ACOG and others.
“Some but not all studies have shown an impact of either antenatal or postnatal depression on speech recognition in infancy of native versus nonnative languages, IQ, and cognitive development, and reduction in left frontal brain electrical activity associated with impaired positive emotions,” Dr. Hudepohl reported.
Sifting through published data, Dr. Hudepohl cited studies associating persistent postpartum depression with a more than fourfold risk of behavioral problems at the age of 3.5 years, lower grades in mathematics at age 16, and a higher prevalence of depression at age 18. Among children who had depressed mothers in infancy, there have also been studies showing a higher reactivity to stressors and higher baseline cortisol levels.
“The good news is that Dr. Hudepohl said. In fact, she cited evidence of a correlation between improvement in maternal symptoms and a reduction in the complications in children, such as behavioral problems.
Postpartum depression, which can develop anytime in the first 12 months after childbirth, is not uncommon, occurring in approximately 15% of women, according to Dr. Hudepohl. Risk factors include personal or family history of depression, anxiety or depression during pregnancy, and a prior history of postpartum depression.
Postpartum depression increases the risk of maternal suicide by about 70-fold, Dr. Hudepohl reported. She noted that the peaks in suicide attempts in the 1st and 12th month after delivery. Adverse infant outcomes are not a predictor of increase risk of attempts, but fetal or infant death are.
According to one study, about 40% of mothers with postpartum depression have intrusive thoughts that involve harming their child. About 15% fear being alone with their infant. Behaviors such as decreased playfulness, less talking, or other interactions with the child, and inconsistent response to the child are all likely to contribute to impaired maternal-child bonding, Dr. Hudepohl reported.
For women who discontinued antidepressants for pregnancy but have now developed significant postpartum depression, Dr. Hudepohl recommended using “what has worked in the past.” She considered monotherapy preferable if possible, but severe symptoms warrant more aggressive intervention. Dr. Hudepohl pointed out that the risks of antidepressants taken by the breast-feeding mother to the infant remain unclear despite multiple studies attempting to establish and quantify risk.
“Antidepressants are the most researched medication in pregnancy,” she said.
Conversely, the risks of untreated symptoms to the mother are significant, and the potential risks to the infant and family – if variable – are not insignificant.
Overall, “nonpharmacologic treatment is preferred first line for mild symptoms,” Dr. Hudepohl, but she and others consider a risk-benefit ratio growing increasingly in favor of drug therapy when this approach is the best option for bringing moderate to severe symptoms under control.
Whether depression arises during pregnancy or in the postpartum period, “psychotherapy is generally considered first-line treatment,” agreed Nancy Byatt, DO, MS, MBA, professor of psychiatry and of obstetrics and gynecology at the University of Massachusetts, Worcester.
Dr. Byatt, who has published frequently on this topic, further agreed that risks to the mother and the child increase with uncontrolled depression in the postpartum period. With symptoms of greater intensity, the uncertain risks of medication are outweighed by substantial potential benefits.
“When a pregnant or postpartum individual has moderate to severe illness, treatment with medication is typically recommended, because the benefits are thought to outweigh the risks,” she said, echoing a consensus opinion among experts and organized medicine.
MedscapeLive and this news organization are owned by the same parent company. Dr. Hudepohl and Dr. Byatt reported no potential financial conflicts of interest.
If moderate to severe postpartum depression poses a risk to child development, that argues in favor of pharmacologic therapy, according to a detailed risk-benefit assessment presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“It is important to consider that there are potential risks of antidepressant drugs, but there are also potential risks from not providing effective treatment,” reported Neha Hudepohl, MD, at the virtual meeting, presented by MedscapeLive.
On a website maintained by the Centers for Disease Control and Prevention, the question of whether antidepressants pose a risk to breast-feeding children is answered with a “maybe.” Although many of these drugs can be detected in breast milk, according to the CDC, “most have little or no effect on milk supply or on infant well-being.”
This is enough uncertainty that antidepressants are not first-line intervention when postpartum depression is mild, said Dr. Hudepohl, director of women’s mental health at Prisma Health Upstate, Greenville, S.C. However, she noted that the American College of Obstetricians and Gynecologists is among the organizations that recommend drug treatment if symptoms are moderate to severe.
“Depression in the mother affects interactions in feeding practices, sleep routines and patterns, and safety practices,” said Dr. Hudepohl, citing published studies supporting each of these consequences.
For the child, there is some degree of uncertainty about risk from untreated maternal depression as well as from breast mild exposure to antidepressants. Conclusive statements are not offered by ACOG and others.
“Some but not all studies have shown an impact of either antenatal or postnatal depression on speech recognition in infancy of native versus nonnative languages, IQ, and cognitive development, and reduction in left frontal brain electrical activity associated with impaired positive emotions,” Dr. Hudepohl reported.
Sifting through published data, Dr. Hudepohl cited studies associating persistent postpartum depression with a more than fourfold risk of behavioral problems at the age of 3.5 years, lower grades in mathematics at age 16, and a higher prevalence of depression at age 18. Among children who had depressed mothers in infancy, there have also been studies showing a higher reactivity to stressors and higher baseline cortisol levels.
“The good news is that Dr. Hudepohl said. In fact, she cited evidence of a correlation between improvement in maternal symptoms and a reduction in the complications in children, such as behavioral problems.
Postpartum depression, which can develop anytime in the first 12 months after childbirth, is not uncommon, occurring in approximately 15% of women, according to Dr. Hudepohl. Risk factors include personal or family history of depression, anxiety or depression during pregnancy, and a prior history of postpartum depression.
Postpartum depression increases the risk of maternal suicide by about 70-fold, Dr. Hudepohl reported. She noted that the peaks in suicide attempts in the 1st and 12th month after delivery. Adverse infant outcomes are not a predictor of increase risk of attempts, but fetal or infant death are.
According to one study, about 40% of mothers with postpartum depression have intrusive thoughts that involve harming their child. About 15% fear being alone with their infant. Behaviors such as decreased playfulness, less talking, or other interactions with the child, and inconsistent response to the child are all likely to contribute to impaired maternal-child bonding, Dr. Hudepohl reported.
For women who discontinued antidepressants for pregnancy but have now developed significant postpartum depression, Dr. Hudepohl recommended using “what has worked in the past.” She considered monotherapy preferable if possible, but severe symptoms warrant more aggressive intervention. Dr. Hudepohl pointed out that the risks of antidepressants taken by the breast-feeding mother to the infant remain unclear despite multiple studies attempting to establish and quantify risk.
“Antidepressants are the most researched medication in pregnancy,” she said.
Conversely, the risks of untreated symptoms to the mother are significant, and the potential risks to the infant and family – if variable – are not insignificant.
Overall, “nonpharmacologic treatment is preferred first line for mild symptoms,” Dr. Hudepohl, but she and others consider a risk-benefit ratio growing increasingly in favor of drug therapy when this approach is the best option for bringing moderate to severe symptoms under control.
Whether depression arises during pregnancy or in the postpartum period, “psychotherapy is generally considered first-line treatment,” agreed Nancy Byatt, DO, MS, MBA, professor of psychiatry and of obstetrics and gynecology at the University of Massachusetts, Worcester.
Dr. Byatt, who has published frequently on this topic, further agreed that risks to the mother and the child increase with uncontrolled depression in the postpartum period. With symptoms of greater intensity, the uncertain risks of medication are outweighed by substantial potential benefits.
“When a pregnant or postpartum individual has moderate to severe illness, treatment with medication is typically recommended, because the benefits are thought to outweigh the risks,” she said, echoing a consensus opinion among experts and organized medicine.
MedscapeLive and this news organization are owned by the same parent company. Dr. Hudepohl and Dr. Byatt reported no potential financial conflicts of interest.
If moderate to severe postpartum depression poses a risk to child development, that argues in favor of pharmacologic therapy, according to a detailed risk-benefit assessment presented by Current Psychiatry and the American Academy of Clinical Psychiatrists.
“It is important to consider that there are potential risks of antidepressant drugs, but there are also potential risks from not providing effective treatment,” reported Neha Hudepohl, MD, at the virtual meeting, presented by MedscapeLive.
On a website maintained by the Centers for Disease Control and Prevention, the question of whether antidepressants pose a risk to breast-feeding children is answered with a “maybe.” Although many of these drugs can be detected in breast milk, according to the CDC, “most have little or no effect on milk supply or on infant well-being.”
This is enough uncertainty that antidepressants are not first-line intervention when postpartum depression is mild, said Dr. Hudepohl, director of women’s mental health at Prisma Health Upstate, Greenville, S.C. However, she noted that the American College of Obstetricians and Gynecologists is among the organizations that recommend drug treatment if symptoms are moderate to severe.
“Depression in the mother affects interactions in feeding practices, sleep routines and patterns, and safety practices,” said Dr. Hudepohl, citing published studies supporting each of these consequences.
For the child, there is some degree of uncertainty about risk from untreated maternal depression as well as from breast mild exposure to antidepressants. Conclusive statements are not offered by ACOG and others.
“Some but not all studies have shown an impact of either antenatal or postnatal depression on speech recognition in infancy of native versus nonnative languages, IQ, and cognitive development, and reduction in left frontal brain electrical activity associated with impaired positive emotions,” Dr. Hudepohl reported.
Sifting through published data, Dr. Hudepohl cited studies associating persistent postpartum depression with a more than fourfold risk of behavioral problems at the age of 3.5 years, lower grades in mathematics at age 16, and a higher prevalence of depression at age 18. Among children who had depressed mothers in infancy, there have also been studies showing a higher reactivity to stressors and higher baseline cortisol levels.
“The good news is that Dr. Hudepohl said. In fact, she cited evidence of a correlation between improvement in maternal symptoms and a reduction in the complications in children, such as behavioral problems.
Postpartum depression, which can develop anytime in the first 12 months after childbirth, is not uncommon, occurring in approximately 15% of women, according to Dr. Hudepohl. Risk factors include personal or family history of depression, anxiety or depression during pregnancy, and a prior history of postpartum depression.
Postpartum depression increases the risk of maternal suicide by about 70-fold, Dr. Hudepohl reported. She noted that the peaks in suicide attempts in the 1st and 12th month after delivery. Adverse infant outcomes are not a predictor of increase risk of attempts, but fetal or infant death are.
According to one study, about 40% of mothers with postpartum depression have intrusive thoughts that involve harming their child. About 15% fear being alone with their infant. Behaviors such as decreased playfulness, less talking, or other interactions with the child, and inconsistent response to the child are all likely to contribute to impaired maternal-child bonding, Dr. Hudepohl reported.
For women who discontinued antidepressants for pregnancy but have now developed significant postpartum depression, Dr. Hudepohl recommended using “what has worked in the past.” She considered monotherapy preferable if possible, but severe symptoms warrant more aggressive intervention. Dr. Hudepohl pointed out that the risks of antidepressants taken by the breast-feeding mother to the infant remain unclear despite multiple studies attempting to establish and quantify risk.
“Antidepressants are the most researched medication in pregnancy,” she said.
Conversely, the risks of untreated symptoms to the mother are significant, and the potential risks to the infant and family – if variable – are not insignificant.
Overall, “nonpharmacologic treatment is preferred first line for mild symptoms,” Dr. Hudepohl, but she and others consider a risk-benefit ratio growing increasingly in favor of drug therapy when this approach is the best option for bringing moderate to severe symptoms under control.
Whether depression arises during pregnancy or in the postpartum period, “psychotherapy is generally considered first-line treatment,” agreed Nancy Byatt, DO, MS, MBA, professor of psychiatry and of obstetrics and gynecology at the University of Massachusetts, Worcester.
Dr. Byatt, who has published frequently on this topic, further agreed that risks to the mother and the child increase with uncontrolled depression in the postpartum period. With symptoms of greater intensity, the uncertain risks of medication are outweighed by substantial potential benefits.
“When a pregnant or postpartum individual has moderate to severe illness, treatment with medication is typically recommended, because the benefits are thought to outweigh the risks,” she said, echoing a consensus opinion among experts and organized medicine.
MedscapeLive and this news organization are owned by the same parent company. Dr. Hudepohl and Dr. Byatt reported no potential financial conflicts of interest.
FROM CP/AACP PSYCHIATRY UPDATE
Polypharmacy remains common for autism spectrum patients
Approximately one-third of individuals with autism spectrum disorder (ASD) are prescribed multiple medications to manage comorbidities and symptoms, according to data from a retrospective cohort study of more than 26,000 patients.
“Clinicians caring for patients with ASD are tasked with the challenges of managing the primary disease, as well as co-occurring medical conditions, and coordinating with educational and social service professionals to provide holistic care,” wrote Aliya G. Feroe of Harvard Medical School, Boston, and colleagues.
The medication classes used to treat individuals with ASD include ADHD medications, antipsychotics, antidepressants, mood stabilizers, benzodiazepines, anxiolytics, and hypnotics, but the prescription rates of these medications in ASD patients have not been examined in large studies, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 26,722 individuals with ASD using a United States health care database from Jan. 1, 2014, to Dec. 31, 2019. Data included records of inpatient and outpatient claims, and records of prescriptions filled through commercial pharmacies. Individuals received at least 1 of 24 of the most common medication groups for ASD or comorbidities. The average age of the study participants was 14 years, and 78% were male. Diagnostic codes for ASD were based on the International Classification of Diseases, Ninth Revision, and International Statistical Classification of Diseases and Related Health Problems, Tenth Revision.
Over the 6-year study period, approximately one-third of the participants were taking three or more medications at once, ranging from 28.6% to 31.5%. In any 1 year, approximately 41% of children were prescribed a single medication, 17% received two prescriptions, 7.9% received four, and 3.4% received five. Medication changes occurred more frequently within classes than between classes, and reasons for these changes may include patient preference, adverse effects, and cost, the researchers noted.
The overall number of children prescribed particular drugs remained consistent, the researchers noted. “For example, the total number of individuals prescribed methylphenidate shifted from 832 in 2014 to 850 in 2015, 899 in 2016, 863 in 2017, and 838 in 2018,” they wrote.
In 15 of the 24 medication groups included in the study, at least 15% of the individuals had unspecified anxiety disorder, anxiety neurosis, or major depressive disorder; in 11 of the medication groups, at least 15% had some form of ADHD. ADHD prevalence in patients taking stimulants varied based on ADHD type, the researchers said.
The most common comorbidities in patients taking antipsychotics were combined type ADHD (11.6%-17.8%) and anxiety disorder (13.1%-30.1%). The study findings suggest that many clinicians are incorporating medications into ASD management, the researchers said.
“Although there is no medical treatment for the core deficits of social communication and repetitive behavioral patterns in ASD, the American Academy of Pediatrics recommends that clinicians consider medications in the management of common comorbid conditions, including seizures, ADHD, anxiety disorders, mood disorders, and disruptive behavior disorders,” they said.
The findings were limited by several factors including the potential for inconsistent reporting of diagnoses and pharmacy claims, the researchers noted. Other limitations included a lack of direct clinical assessment to validate diagnoses and the absence of validated diagnostic instruments to screen for comorbidities, they added.
“Our findings suggest that clinicians may be increasingly using integrated approaches to treating patients with ASD and co-occurring conditions, and further work is necessary to determine the relative effects of pharmacotherapy vs. behavioral interventions on outcomes in patients with ASD,” the researchers concluded.
Many reasons for multiple medications
“The researchers put in a lot of effort to provide data on a large scale,” Herschel Lessin, MD, of Children’s Medical Group, Poughkeepsie, N.Y., said in an interview.
“The findings illustrate the reality that autistic children are prescribed a lot of medications for a lot of reasons, some of which are not entirely clear,” Dr. Lessin said. The study also reflects the chronic lack of behavioral health services for children, he noted. Many children with ASD are referred for services they are unable to access, he said. “As a result, they see doctors who can only prescribe medications to try to control behavior or symptoms for which the cause is unclear,” and which could be ASD or other comorbidities, he emphasized.
The large sample size strengthens the study findings, but some of the challenges include the use of claims data, which do not indicate how diagnoses were made, said Dr. Lessin. An additional limitation is the fact that many medications for children with autism are used off label, so the specific reason for their use may be unknown, he said.
The take-home message for clinicians is that children with ASD are getting a lot of medications, and pediatricians are not usually responsible for multiple medications,” Dr. Lessin said. Ultimately, the study is “a plea for more research,” to tease out details of what medications are indicated and helpful, he said.
The study received no outside funding. The researchers and Dr. Lessin had no financial conflicts to disclose. Dr. Lessin serves on the Pediatric News editorial advisory board.
Approximately one-third of individuals with autism spectrum disorder (ASD) are prescribed multiple medications to manage comorbidities and symptoms, according to data from a retrospective cohort study of more than 26,000 patients.
“Clinicians caring for patients with ASD are tasked with the challenges of managing the primary disease, as well as co-occurring medical conditions, and coordinating with educational and social service professionals to provide holistic care,” wrote Aliya G. Feroe of Harvard Medical School, Boston, and colleagues.
The medication classes used to treat individuals with ASD include ADHD medications, antipsychotics, antidepressants, mood stabilizers, benzodiazepines, anxiolytics, and hypnotics, but the prescription rates of these medications in ASD patients have not been examined in large studies, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 26,722 individuals with ASD using a United States health care database from Jan. 1, 2014, to Dec. 31, 2019. Data included records of inpatient and outpatient claims, and records of prescriptions filled through commercial pharmacies. Individuals received at least 1 of 24 of the most common medication groups for ASD or comorbidities. The average age of the study participants was 14 years, and 78% were male. Diagnostic codes for ASD were based on the International Classification of Diseases, Ninth Revision, and International Statistical Classification of Diseases and Related Health Problems, Tenth Revision.
Over the 6-year study period, approximately one-third of the participants were taking three or more medications at once, ranging from 28.6% to 31.5%. In any 1 year, approximately 41% of children were prescribed a single medication, 17% received two prescriptions, 7.9% received four, and 3.4% received five. Medication changes occurred more frequently within classes than between classes, and reasons for these changes may include patient preference, adverse effects, and cost, the researchers noted.
The overall number of children prescribed particular drugs remained consistent, the researchers noted. “For example, the total number of individuals prescribed methylphenidate shifted from 832 in 2014 to 850 in 2015, 899 in 2016, 863 in 2017, and 838 in 2018,” they wrote.
In 15 of the 24 medication groups included in the study, at least 15% of the individuals had unspecified anxiety disorder, anxiety neurosis, or major depressive disorder; in 11 of the medication groups, at least 15% had some form of ADHD. ADHD prevalence in patients taking stimulants varied based on ADHD type, the researchers said.
The most common comorbidities in patients taking antipsychotics were combined type ADHD (11.6%-17.8%) and anxiety disorder (13.1%-30.1%). The study findings suggest that many clinicians are incorporating medications into ASD management, the researchers said.
“Although there is no medical treatment for the core deficits of social communication and repetitive behavioral patterns in ASD, the American Academy of Pediatrics recommends that clinicians consider medications in the management of common comorbid conditions, including seizures, ADHD, anxiety disorders, mood disorders, and disruptive behavior disorders,” they said.
The findings were limited by several factors including the potential for inconsistent reporting of diagnoses and pharmacy claims, the researchers noted. Other limitations included a lack of direct clinical assessment to validate diagnoses and the absence of validated diagnostic instruments to screen for comorbidities, they added.
“Our findings suggest that clinicians may be increasingly using integrated approaches to treating patients with ASD and co-occurring conditions, and further work is necessary to determine the relative effects of pharmacotherapy vs. behavioral interventions on outcomes in patients with ASD,” the researchers concluded.
Many reasons for multiple medications
“The researchers put in a lot of effort to provide data on a large scale,” Herschel Lessin, MD, of Children’s Medical Group, Poughkeepsie, N.Y., said in an interview.
“The findings illustrate the reality that autistic children are prescribed a lot of medications for a lot of reasons, some of which are not entirely clear,” Dr. Lessin said. The study also reflects the chronic lack of behavioral health services for children, he noted. Many children with ASD are referred for services they are unable to access, he said. “As a result, they see doctors who can only prescribe medications to try to control behavior or symptoms for which the cause is unclear,” and which could be ASD or other comorbidities, he emphasized.
The large sample size strengthens the study findings, but some of the challenges include the use of claims data, which do not indicate how diagnoses were made, said Dr. Lessin. An additional limitation is the fact that many medications for children with autism are used off label, so the specific reason for their use may be unknown, he said.
The take-home message for clinicians is that children with ASD are getting a lot of medications, and pediatricians are not usually responsible for multiple medications,” Dr. Lessin said. Ultimately, the study is “a plea for more research,” to tease out details of what medications are indicated and helpful, he said.
The study received no outside funding. The researchers and Dr. Lessin had no financial conflicts to disclose. Dr. Lessin serves on the Pediatric News editorial advisory board.
Approximately one-third of individuals with autism spectrum disorder (ASD) are prescribed multiple medications to manage comorbidities and symptoms, according to data from a retrospective cohort study of more than 26,000 patients.
“Clinicians caring for patients with ASD are tasked with the challenges of managing the primary disease, as well as co-occurring medical conditions, and coordinating with educational and social service professionals to provide holistic care,” wrote Aliya G. Feroe of Harvard Medical School, Boston, and colleagues.
The medication classes used to treat individuals with ASD include ADHD medications, antipsychotics, antidepressants, mood stabilizers, benzodiazepines, anxiolytics, and hypnotics, but the prescription rates of these medications in ASD patients have not been examined in large studies, the researchers said.
In a study published in JAMA Pediatrics, the researchers identified 26,722 individuals with ASD using a United States health care database from Jan. 1, 2014, to Dec. 31, 2019. Data included records of inpatient and outpatient claims, and records of prescriptions filled through commercial pharmacies. Individuals received at least 1 of 24 of the most common medication groups for ASD or comorbidities. The average age of the study participants was 14 years, and 78% were male. Diagnostic codes for ASD were based on the International Classification of Diseases, Ninth Revision, and International Statistical Classification of Diseases and Related Health Problems, Tenth Revision.
Over the 6-year study period, approximately one-third of the participants were taking three or more medications at once, ranging from 28.6% to 31.5%. In any 1 year, approximately 41% of children were prescribed a single medication, 17% received two prescriptions, 7.9% received four, and 3.4% received five. Medication changes occurred more frequently within classes than between classes, and reasons for these changes may include patient preference, adverse effects, and cost, the researchers noted.
The overall number of children prescribed particular drugs remained consistent, the researchers noted. “For example, the total number of individuals prescribed methylphenidate shifted from 832 in 2014 to 850 in 2015, 899 in 2016, 863 in 2017, and 838 in 2018,” they wrote.
In 15 of the 24 medication groups included in the study, at least 15% of the individuals had unspecified anxiety disorder, anxiety neurosis, or major depressive disorder; in 11 of the medication groups, at least 15% had some form of ADHD. ADHD prevalence in patients taking stimulants varied based on ADHD type, the researchers said.
The most common comorbidities in patients taking antipsychotics were combined type ADHD (11.6%-17.8%) and anxiety disorder (13.1%-30.1%). The study findings suggest that many clinicians are incorporating medications into ASD management, the researchers said.
“Although there is no medical treatment for the core deficits of social communication and repetitive behavioral patterns in ASD, the American Academy of Pediatrics recommends that clinicians consider medications in the management of common comorbid conditions, including seizures, ADHD, anxiety disorders, mood disorders, and disruptive behavior disorders,” they said.
The findings were limited by several factors including the potential for inconsistent reporting of diagnoses and pharmacy claims, the researchers noted. Other limitations included a lack of direct clinical assessment to validate diagnoses and the absence of validated diagnostic instruments to screen for comorbidities, they added.
“Our findings suggest that clinicians may be increasingly using integrated approaches to treating patients with ASD and co-occurring conditions, and further work is necessary to determine the relative effects of pharmacotherapy vs. behavioral interventions on outcomes in patients with ASD,” the researchers concluded.
Many reasons for multiple medications
“The researchers put in a lot of effort to provide data on a large scale,” Herschel Lessin, MD, of Children’s Medical Group, Poughkeepsie, N.Y., said in an interview.
“The findings illustrate the reality that autistic children are prescribed a lot of medications for a lot of reasons, some of which are not entirely clear,” Dr. Lessin said. The study also reflects the chronic lack of behavioral health services for children, he noted. Many children with ASD are referred for services they are unable to access, he said. “As a result, they see doctors who can only prescribe medications to try to control behavior or symptoms for which the cause is unclear,” and which could be ASD or other comorbidities, he emphasized.
The large sample size strengthens the study findings, but some of the challenges include the use of claims data, which do not indicate how diagnoses were made, said Dr. Lessin. An additional limitation is the fact that many medications for children with autism are used off label, so the specific reason for their use may be unknown, he said.
The take-home message for clinicians is that children with ASD are getting a lot of medications, and pediatricians are not usually responsible for multiple medications,” Dr. Lessin said. Ultimately, the study is “a plea for more research,” to tease out details of what medications are indicated and helpful, he said.
The study received no outside funding. The researchers and Dr. Lessin had no financial conflicts to disclose. Dr. Lessin serves on the Pediatric News editorial advisory board.
FROM JAMA PEDIATRICS
Depression remains common among dystonia patients
About one-third of individuals with adult-onset idiopathic dystonia experience major depression or dysthymia, data from a meta-analysis of 54 studies show.
Adult-onset idiopathic dystonia (AOID) is the third-most common movement disorder after essential tremor and Parkinson’s disease, and data show that depression and anxiety are the largest contributors to reduced quality of life in these patients, wrote Alex Medina Escobar, MD, of the University of Calgary (Alta.), and colleagues. However, “the pathogenic mechanisms of depression and anxiety in AOID remain unclear” and might involve a combination of biologic factors, as well as social stigma.
In the meta-analysis, published in Neuroscience and Biobehavioral Reviews, the researchers examined the point prevalence of supraclinical threshold depressive symptoms/depressive disorders in AOID using 54 studies. The resulting study population included 12,635 patients: 6,977 with cervical dystonia, 732 with cranial dystonia, 4,504 with mixed forms, 303 with laryngeal dystonia, and 119 with upper-limb dystonia. The studies were published between 1988 and 2020, and included patients from 21 countries in 52 single-center studies and 2 multicenter studies.
Overall, the pooled prevalence of either supraclinical threshold depressive symptoms or depressive disorders was 31.5% for cervical dystonia, 29.2 % for cranial dystonia, and 33.6 % for clinical samples with mixed forms of AOID.
Among patients with cervical dystonia, major depressive disorder was more prevalent than dysthymia, but among patients with cranial dystonia, dysthymia was more prevalent. Among patients with mixed forms, the prevalence of major depressive disorder was higher than dysthymia. Heterogeneity varied among the studies but was higher in studies that used rating scales.
Treatment of patients with AOID does not take into account the impact of depression on quality of life, Dr. Escobar and colleagues reported.
“ Such model appears to be inefficient to guarantee resources to address these comorbidities within secondary or tertiary care, or through shared care pathways engaging both primary and hospital-based care.” They also said the use of antidepressants and cognitive-behavioral therapy as a way to target negative body concept or social stigma among these patients are “underexplored and underutilized.”
The study findings were limited by several factors, including the inclusion only of studies published in English. In addition, most of the studies were conducted at movement disorders clinics, which may have yielded a patient population with more severe AOID. Further limitations included the inability to perform subgroup analysis based on demographic and clinical factors, and the insufficient number of studies for meta-analysis of laryngeal and hand dystonia, Dr. Escobar and colleagues added.
However, the results represent the first pooled estimate of depression prevalence in AOID and confirm a high prevalence across different clinical forms, the researchers said. The heterogeneity across studies highlights the need for standardized screening for depression and improved diagnosis of mood disorders in AOID.
“The meta-analytic estimates provided here will be highly useful for the planning of future mechanistic and interventional studies, as well as for the redefinition of current models of care,” they concluded.
The study received no outside funding. Dr. Escobar and colleagues had no disclosures.
About one-third of individuals with adult-onset idiopathic dystonia experience major depression or dysthymia, data from a meta-analysis of 54 studies show.
Adult-onset idiopathic dystonia (AOID) is the third-most common movement disorder after essential tremor and Parkinson’s disease, and data show that depression and anxiety are the largest contributors to reduced quality of life in these patients, wrote Alex Medina Escobar, MD, of the University of Calgary (Alta.), and colleagues. However, “the pathogenic mechanisms of depression and anxiety in AOID remain unclear” and might involve a combination of biologic factors, as well as social stigma.
In the meta-analysis, published in Neuroscience and Biobehavioral Reviews, the researchers examined the point prevalence of supraclinical threshold depressive symptoms/depressive disorders in AOID using 54 studies. The resulting study population included 12,635 patients: 6,977 with cervical dystonia, 732 with cranial dystonia, 4,504 with mixed forms, 303 with laryngeal dystonia, and 119 with upper-limb dystonia. The studies were published between 1988 and 2020, and included patients from 21 countries in 52 single-center studies and 2 multicenter studies.
Overall, the pooled prevalence of either supraclinical threshold depressive symptoms or depressive disorders was 31.5% for cervical dystonia, 29.2 % for cranial dystonia, and 33.6 % for clinical samples with mixed forms of AOID.
Among patients with cervical dystonia, major depressive disorder was more prevalent than dysthymia, but among patients with cranial dystonia, dysthymia was more prevalent. Among patients with mixed forms, the prevalence of major depressive disorder was higher than dysthymia. Heterogeneity varied among the studies but was higher in studies that used rating scales.
Treatment of patients with AOID does not take into account the impact of depression on quality of life, Dr. Escobar and colleagues reported.
“ Such model appears to be inefficient to guarantee resources to address these comorbidities within secondary or tertiary care, or through shared care pathways engaging both primary and hospital-based care.” They also said the use of antidepressants and cognitive-behavioral therapy as a way to target negative body concept or social stigma among these patients are “underexplored and underutilized.”
The study findings were limited by several factors, including the inclusion only of studies published in English. In addition, most of the studies were conducted at movement disorders clinics, which may have yielded a patient population with more severe AOID. Further limitations included the inability to perform subgroup analysis based on demographic and clinical factors, and the insufficient number of studies for meta-analysis of laryngeal and hand dystonia, Dr. Escobar and colleagues added.
However, the results represent the first pooled estimate of depression prevalence in AOID and confirm a high prevalence across different clinical forms, the researchers said. The heterogeneity across studies highlights the need for standardized screening for depression and improved diagnosis of mood disorders in AOID.
“The meta-analytic estimates provided here will be highly useful for the planning of future mechanistic and interventional studies, as well as for the redefinition of current models of care,” they concluded.
The study received no outside funding. Dr. Escobar and colleagues had no disclosures.
About one-third of individuals with adult-onset idiopathic dystonia experience major depression or dysthymia, data from a meta-analysis of 54 studies show.
Adult-onset idiopathic dystonia (AOID) is the third-most common movement disorder after essential tremor and Parkinson’s disease, and data show that depression and anxiety are the largest contributors to reduced quality of life in these patients, wrote Alex Medina Escobar, MD, of the University of Calgary (Alta.), and colleagues. However, “the pathogenic mechanisms of depression and anxiety in AOID remain unclear” and might involve a combination of biologic factors, as well as social stigma.
In the meta-analysis, published in Neuroscience and Biobehavioral Reviews, the researchers examined the point prevalence of supraclinical threshold depressive symptoms/depressive disorders in AOID using 54 studies. The resulting study population included 12,635 patients: 6,977 with cervical dystonia, 732 with cranial dystonia, 4,504 with mixed forms, 303 with laryngeal dystonia, and 119 with upper-limb dystonia. The studies were published between 1988 and 2020, and included patients from 21 countries in 52 single-center studies and 2 multicenter studies.
Overall, the pooled prevalence of either supraclinical threshold depressive symptoms or depressive disorders was 31.5% for cervical dystonia, 29.2 % for cranial dystonia, and 33.6 % for clinical samples with mixed forms of AOID.
Among patients with cervical dystonia, major depressive disorder was more prevalent than dysthymia, but among patients with cranial dystonia, dysthymia was more prevalent. Among patients with mixed forms, the prevalence of major depressive disorder was higher than dysthymia. Heterogeneity varied among the studies but was higher in studies that used rating scales.
Treatment of patients with AOID does not take into account the impact of depression on quality of life, Dr. Escobar and colleagues reported.
“ Such model appears to be inefficient to guarantee resources to address these comorbidities within secondary or tertiary care, or through shared care pathways engaging both primary and hospital-based care.” They also said the use of antidepressants and cognitive-behavioral therapy as a way to target negative body concept or social stigma among these patients are “underexplored and underutilized.”
The study findings were limited by several factors, including the inclusion only of studies published in English. In addition, most of the studies were conducted at movement disorders clinics, which may have yielded a patient population with more severe AOID. Further limitations included the inability to perform subgroup analysis based on demographic and clinical factors, and the insufficient number of studies for meta-analysis of laryngeal and hand dystonia, Dr. Escobar and colleagues added.
However, the results represent the first pooled estimate of depression prevalence in AOID and confirm a high prevalence across different clinical forms, the researchers said. The heterogeneity across studies highlights the need for standardized screening for depression and improved diagnosis of mood disorders in AOID.
“The meta-analytic estimates provided here will be highly useful for the planning of future mechanistic and interventional studies, as well as for the redefinition of current models of care,” they concluded.
The study received no outside funding. Dr. Escobar and colleagues had no disclosures.
FROM NEUROSCIENCE AND BIOBEHAVIORAL REVIEWS
New data on COVID-19’s cognitive fallout
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
High rates of work-related trauma, PTSD in intern physicians
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.

Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”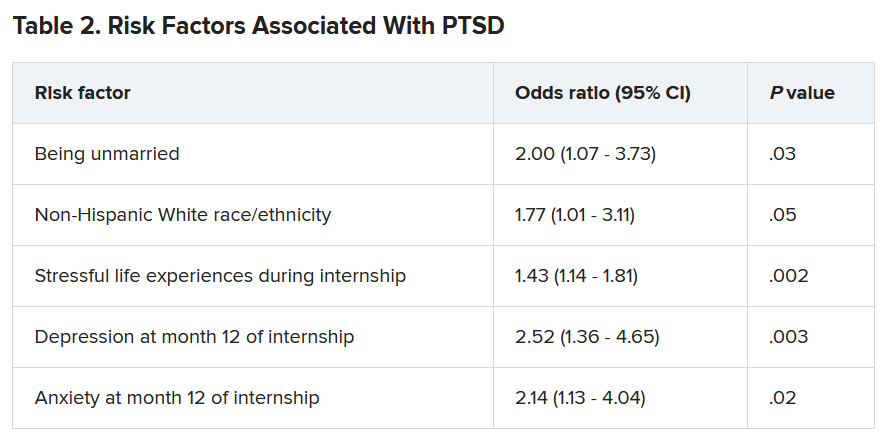
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.
Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Work-related posttraumatic stress disorder is three times higher in interns than the general population, new research shows.
Investigators assessed PTSD in more than 1,100 physicians at the end of their internship year and found that a little over half reported work-related trauma exposure, and of these, 20% screened positive for PTSD.
Overall, 10% of participants screened positive for PTSD by the end of the internship year, compared with a 12-month PTSD prevalence of 3.6% in the general population.
“Work-related trauma exposure and PTSD are common and underdiscussed phenomena among intern physicians,” lead author Mary Vance, MD, assistant professor of psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Md., said in an interview.
“I urge medical educators and policy makers to include this topic in their discussions about physician well-being and to implement effective interventions to mitigate the impact of work-related trauma and PTSD among physician trainees,” she said.
The study was published online June 8 in JAMA Network Open.
Burnout, depression, suicide
“Burnout, depression, and suicide are increasingly recognized as occupational mental health hazards among health care professionals, including physicians,” Dr. Vance said.
“However, in my professional experience as a physician and educator, despite observing anecdotal evidence among my peers and trainees that this is also an issue,” she added.
This gap prompted her “to investigate rates of work-related trauma exposure and PTSD among physicians.”
The researchers sent emails to 4,350 individuals during academic year 2018-2019, 2 months prior to starting internships. Of these, 2,129 agreed to participate and 1,134 (58.6% female, 61.6% non-Hispanic White; mean age, 27.52) completed the study.
Prior to beginning internship, participants completed a baseline survey that assessed demographic characteristics as well as medical education and psychological and psychosocial factors.
Participants completed follow-up surveys sent by email at 3, 6, 9, and 12 months of the internship year. The surveys assessed stressful life events, concern over perceived medical errors in the past 3 months, and number of hours worked over the past week.
At month 12, current PTSD and symptoms of depression and anxiety were also assessed using the Primary Care PTSD Screen for DSM-5, the 9-item Patient Health Questionnaire, and the Generalized Anxiety Disorder 7-item scale, respectively.
Participants were asked to self-report whether they ever had an episode of depression and to complete the Risky Families Questionnaire to assess if they had experienced childhood abuse, neglect, and family conflict. Additionally, they completed an 11-item scale developed specifically for the study regarding recent stressful events.
‘Crucible’ year
A total of 56.4% of respondents reported work-related trauma exposure, and among these, 19.0% screened positive for PTSD. One-tenth (10.8%) of the entire sample screened positive for PTSD by the end of internship year, which is three times higher than the 12-month prevalence of PTSD in the general population (3.6%), the authors noted.
Trauma exposure differed by specialty, ranging from 43.1% in anesthesiology to 72.4% in emergency medicine. Of the respondents in internal medicine, surgery, and medicine/pediatrics, 56.6%, 63.3%, and 71%, respectively, reported work-related trauma exposure.
Work-related PTSD also differed by specialty, ranging from 7.5% in ob.gyn. to 30.0% in pediatrics. Of respondents in internal medicine and family practice, 23.9% and 25.9%, respectively, reported work-related PTSD.
Dr. Vance called the intern year “a crucible, during which newly minted doctors receive intensive on-the-job training at the front lines of patient care [and] work long hours in rapidly shifting environments, often caring for critically ill patients.”
Work-related trauma exposure “is more likely to occur during this high-stress internship year than during the same year in the general population,” she said.
She noted that the “issue of workplace trauma and PTSD among health care workers became even more salient during the height of COVID,” adding that she expects it “to remain a pressure issue for healthcare workers in the post-COVID era.”
Call to action
Commenting on the study David A. Marcus, MD, chair, GME Physician Well-Being Committee, Northwell Health, New Hyde Park, N.Y., noted the study’s “relatively low response rate” is a “significant limitation” of the study.
An additional limitation is the lack of a baseline PTSD assessment, said Dr. Marcus, an assistant professor at Hofstra University, Hempstead, N.Y., who was not involved in the research.
Nevertheless, the “overall prevalence [of work-related PTSD] should serve as a call to action for physician leaders and for leaders in academic medicine,” he said.
Additionally, the study “reminds us that trauma-informed care should be an essential part of mental health support services provided to trainees and to physicians in general,” Dr. Marcus stated.
Also commenting on the study, Lotte N. Dyrbye, MD, professor of medicine and medical education, Mayo Clinic, Rochester, Minn., agreed.
“Organizational strategies should include system-level interventions to reduce the risk of frightening, horrible, or traumatic events from occurring in the workplace in the first place, as well as faculty development efforts to upskill teaching faculty in their ability to support trainees when such events do occur,” she said.
These approaches “should coincide with organizational efforts to support individual trainees by providing adequate time off after traumatic events, ensuring trainees can access affordable mental healthcare, and reducing other barriers to appropriate help-seeking, such as stigma, and efforts to build a culture of well-being,” suggested Dr. Dyrbye, who is codirector of the Mayo Clinic Program on Physician Wellbeing and was not involved in the study.
The study was supported by grants from the Blue Cross Blue Shield Foundation of Michigan and National Institutes of Health. Dr. Vance and coauthors, Dr. Marcus, and Dr. Dyrbye reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Memory benefit seen with antihypertensives crossing blood-brain barrier
Over a 3-year period, cognitively normal older adults taking BBB-crossing antihypertensives demonstrated superior verbal memory, compared with similar individuals receiving non–BBB-crossing antihypertensives, reported lead author Jean K. Ho, PhD, of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, and colleagues.
According to the investigators, the findings add color to a known link between hypertension and neurologic degeneration, and may aid the search for new therapeutic targets.
“Hypertension is a well-established risk factor for cognitive decline and dementia, possibly through its effects on both cerebrovascular disease and Alzheimer’s disease,” Dr. Ho and colleagues wrote in Hypertension. “Studies of antihypertensive treatments have reported possible salutary effects on cognition and cerebrovascular disease, as well as Alzheimer’s disease neuropathology.”
In a previous study, individuals younger than 75 years exposed to antihypertensives had an 8% decreased risk of dementia per year of use, while another trial showed that intensive blood pressure–lowering therapy reduced mild cognitive impairment by 19%.
“Despite these encouraging findings ... larger meta-analytic studies have been hampered by the fact that pharmacokinetic properties are typically not considered in existing studies or routine clinical practice,” wrote Dr. Ho and colleagues. “The present study sought to fill this gap [in that it was] a large and longitudinal meta-analytic study of existing data recoded to assess the effects of BBB-crossing potential in renin-angiotensin system [RAS] treatments among hypertensive adults.”
Methods and results
The meta-analysis included randomized clinical trials, prospective cohort studies, and retrospective observational studies. The researchers assessed data on 12,849 individuals from 14 cohorts that received either BBB-crossing or non–BBB-crossing antihypertensives.
The BBB-crossing properties of RAS treatments were identified by a literature review. Of ACE inhibitors, captopril, fosinopril, lisinopril, perindopril, ramipril, and trandolapril were classified as BBB crossing, and benazepril, enalapril, moexipril, and quinapril were classified as non–BBB-crossing. Of ARBs, telmisartan and candesartan were considered BBB-crossing, and olmesartan, eprosartan, irbesartan, and losartan were tagged as non–BBB-crossing.
Cognition was assessed via the following seven domains: executive function, attention, verbal memory learning, language, mental status, recall, and processing speed.
Compared with individuals taking non–BBB-crossing antihypertensives, those taking BBB-crossing agents had significantly superior verbal memory (recall), with a maximum effect size of 0.07 (P = .03).
According to the investigators, this finding was particularly noteworthy, as the BBB-crossing group had relatively higher vascular risk burden and lower mean education level.
“These differences make it all the more remarkable that the BBB-crossing group displayed better memory ability over time despite these cognitive disadvantages,” the investigators wrote.
Still, not all the findings favored BBB-crossing agents. Individuals in the BBB-crossing group had relatively inferior attention ability, with a minimum effect size of –0.17 (P = .02).
The other cognitive measures were not significantly different between groups.
Clinicians may consider findings after accounting for other factors
Principal investigator Daniel A. Nation, PhD, associate professor of psychological science and a faculty member of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, suggested that the small difference in verbal memory between groups could be clinically significant over a longer period of time.
“Although the overall effect size was pretty small, if you look at how long it would take for someone [with dementia] to progress over many years of decline, it would actually end up being a pretty big effect,” Dr. Nation said in an interview. “Small effect sizes could actually end up preventing a lot of cases of dementia,” he added.
The conflicting results in the BBB-crossing group – better verbal memory but worse attention ability – were “surprising,” he noted.
“I sort of didn’t believe it at first,” Dr. Nation said, “because the memory finding is sort of replication – we’d observed the same exact effect on memory in a smaller sample in another study. ... The attention [finding], going another way, was a new thing.”
Dr. Nation suggested that the intergroup differences in attention ability may stem from idiosyncrasies of the tests used to measure that domain, which can be impacted by cardiovascular or brain vascular disease. Or it could be caused by something else entirely, he said, noting that further investigation is needed.
He added that the improvements in verbal memory within the BBB-crossing group could be caused by direct effects on the brain. He pointed out that certain ACE polymorphisms have been linked with Alzheimer’s disease risk, and those same polymorphisms, in animal models, lead to neurodegeneration, with reversal possible through administration of ACE inhibitors.
“It could be that what we’re observing has nothing really to do with blood pressure,” Dr. Nation explained. “This could be a neuronal effect on learning memory systems.”
He went on to suggest that clinicians may consider these findings when selecting antihypertensive agents for their patients, with the caveat that all other prescribing factors have already been taking to account.
“In the event that you’re going to give an ACE inhibitor or an angiotensin receptor blocker anyway, and it ends up being a somewhat arbitrary decision in terms of which specific drug you’re going to give, then perhaps this is a piece of information you would take into account – that one gets in the brain and one doesn’t – in somebody at risk for cognitive decline,” Dr. Nation said.
Exact mechanisms of action unknown
Hélène Girouard, PhD, assistant professor of pharmacology and physiology at the University of Montreal, said in an interview that the findings are “of considerable importance, knowing that brain alterations could begin as much as 30 years before manifestation of dementia.”

Since 2003, Dr. Girouard has been studying the cognitive effects of antihypertensive medications. She noted that previous studies involving rodents “have shown beneficial effects [of BBB-crossing antihypertensive drugs] on cognition independent of their effects on blood pressure.”
The drugs’ exact mechanisms of action, however, remain elusive, according to Dr. Girouard, who offered several possible explanations, including amelioration of BBB disruption, brain inflammation, cerebral blood flow dysregulation, cholinergic dysfunction, and neurologic deficits. “Whether these mechanisms may explain Ho and colleagues’ observations remains to be established,” she added.
Andrea L. Schneider, MD, PhD, assistant professor of neurology at the University of Pennsylvania, Philadelphia, applauded the study, but ultimately suggested that more research is needed to impact clinical decision-making.
“The results of this important and well-done study suggest that further investigation into targeted mechanism-based approaches to selecting hypertension treatment agents, with a specific focus on cognitive outcomes, is warranted,” Dr. Schneider said in an interview. “Before changing clinical practice, further work is necessary to disentangle contributions of medication mechanism, comorbid vascular risk factors, and achieved blood pressure reduction, among others.”
The investigators disclosed support from the National Institutes of Health, the Alzheimer’s Association, the Waksman Foundation of Japan, and others. The interviewees reported no relevant conflicts of interest.
Over a 3-year period, cognitively normal older adults taking BBB-crossing antihypertensives demonstrated superior verbal memory, compared with similar individuals receiving non–BBB-crossing antihypertensives, reported lead author Jean K. Ho, PhD, of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, and colleagues.
According to the investigators, the findings add color to a known link between hypertension and neurologic degeneration, and may aid the search for new therapeutic targets.
“Hypertension is a well-established risk factor for cognitive decline and dementia, possibly through its effects on both cerebrovascular disease and Alzheimer’s disease,” Dr. Ho and colleagues wrote in Hypertension. “Studies of antihypertensive treatments have reported possible salutary effects on cognition and cerebrovascular disease, as well as Alzheimer’s disease neuropathology.”
In a previous study, individuals younger than 75 years exposed to antihypertensives had an 8% decreased risk of dementia per year of use, while another trial showed that intensive blood pressure–lowering therapy reduced mild cognitive impairment by 19%.
“Despite these encouraging findings ... larger meta-analytic studies have been hampered by the fact that pharmacokinetic properties are typically not considered in existing studies or routine clinical practice,” wrote Dr. Ho and colleagues. “The present study sought to fill this gap [in that it was] a large and longitudinal meta-analytic study of existing data recoded to assess the effects of BBB-crossing potential in renin-angiotensin system [RAS] treatments among hypertensive adults.”
Methods and results
The meta-analysis included randomized clinical trials, prospective cohort studies, and retrospective observational studies. The researchers assessed data on 12,849 individuals from 14 cohorts that received either BBB-crossing or non–BBB-crossing antihypertensives.
The BBB-crossing properties of RAS treatments were identified by a literature review. Of ACE inhibitors, captopril, fosinopril, lisinopril, perindopril, ramipril, and trandolapril were classified as BBB crossing, and benazepril, enalapril, moexipril, and quinapril were classified as non–BBB-crossing. Of ARBs, telmisartan and candesartan were considered BBB-crossing, and olmesartan, eprosartan, irbesartan, and losartan were tagged as non–BBB-crossing.
Cognition was assessed via the following seven domains: executive function, attention, verbal memory learning, language, mental status, recall, and processing speed.
Compared with individuals taking non–BBB-crossing antihypertensives, those taking BBB-crossing agents had significantly superior verbal memory (recall), with a maximum effect size of 0.07 (P = .03).
According to the investigators, this finding was particularly noteworthy, as the BBB-crossing group had relatively higher vascular risk burden and lower mean education level.
“These differences make it all the more remarkable that the BBB-crossing group displayed better memory ability over time despite these cognitive disadvantages,” the investigators wrote.
Still, not all the findings favored BBB-crossing agents. Individuals in the BBB-crossing group had relatively inferior attention ability, with a minimum effect size of –0.17 (P = .02).
The other cognitive measures were not significantly different between groups.
Clinicians may consider findings after accounting for other factors
Principal investigator Daniel A. Nation, PhD, associate professor of psychological science and a faculty member of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, suggested that the small difference in verbal memory between groups could be clinically significant over a longer period of time.
“Although the overall effect size was pretty small, if you look at how long it would take for someone [with dementia] to progress over many years of decline, it would actually end up being a pretty big effect,” Dr. Nation said in an interview. “Small effect sizes could actually end up preventing a lot of cases of dementia,” he added.
The conflicting results in the BBB-crossing group – better verbal memory but worse attention ability – were “surprising,” he noted.
“I sort of didn’t believe it at first,” Dr. Nation said, “because the memory finding is sort of replication – we’d observed the same exact effect on memory in a smaller sample in another study. ... The attention [finding], going another way, was a new thing.”
Dr. Nation suggested that the intergroup differences in attention ability may stem from idiosyncrasies of the tests used to measure that domain, which can be impacted by cardiovascular or brain vascular disease. Or it could be caused by something else entirely, he said, noting that further investigation is needed.
He added that the improvements in verbal memory within the BBB-crossing group could be caused by direct effects on the brain. He pointed out that certain ACE polymorphisms have been linked with Alzheimer’s disease risk, and those same polymorphisms, in animal models, lead to neurodegeneration, with reversal possible through administration of ACE inhibitors.
“It could be that what we’re observing has nothing really to do with blood pressure,” Dr. Nation explained. “This could be a neuronal effect on learning memory systems.”
He went on to suggest that clinicians may consider these findings when selecting antihypertensive agents for their patients, with the caveat that all other prescribing factors have already been taking to account.
“In the event that you’re going to give an ACE inhibitor or an angiotensin receptor blocker anyway, and it ends up being a somewhat arbitrary decision in terms of which specific drug you’re going to give, then perhaps this is a piece of information you would take into account – that one gets in the brain and one doesn’t – in somebody at risk for cognitive decline,” Dr. Nation said.
Exact mechanisms of action unknown
Hélène Girouard, PhD, assistant professor of pharmacology and physiology at the University of Montreal, said in an interview that the findings are “of considerable importance, knowing that brain alterations could begin as much as 30 years before manifestation of dementia.”
Since 2003, Dr. Girouard has been studying the cognitive effects of antihypertensive medications. She noted that previous studies involving rodents “have shown beneficial effects [of BBB-crossing antihypertensive drugs] on cognition independent of their effects on blood pressure.”
The drugs’ exact mechanisms of action, however, remain elusive, according to Dr. Girouard, who offered several possible explanations, including amelioration of BBB disruption, brain inflammation, cerebral blood flow dysregulation, cholinergic dysfunction, and neurologic deficits. “Whether these mechanisms may explain Ho and colleagues’ observations remains to be established,” she added.
Andrea L. Schneider, MD, PhD, assistant professor of neurology at the University of Pennsylvania, Philadelphia, applauded the study, but ultimately suggested that more research is needed to impact clinical decision-making.
“The results of this important and well-done study suggest that further investigation into targeted mechanism-based approaches to selecting hypertension treatment agents, with a specific focus on cognitive outcomes, is warranted,” Dr. Schneider said in an interview. “Before changing clinical practice, further work is necessary to disentangle contributions of medication mechanism, comorbid vascular risk factors, and achieved blood pressure reduction, among others.”
The investigators disclosed support from the National Institutes of Health, the Alzheimer’s Association, the Waksman Foundation of Japan, and others. The interviewees reported no relevant conflicts of interest.
Over a 3-year period, cognitively normal older adults taking BBB-crossing antihypertensives demonstrated superior verbal memory, compared with similar individuals receiving non–BBB-crossing antihypertensives, reported lead author Jean K. Ho, PhD, of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, and colleagues.
According to the investigators, the findings add color to a known link between hypertension and neurologic degeneration, and may aid the search for new therapeutic targets.
“Hypertension is a well-established risk factor for cognitive decline and dementia, possibly through its effects on both cerebrovascular disease and Alzheimer’s disease,” Dr. Ho and colleagues wrote in Hypertension. “Studies of antihypertensive treatments have reported possible salutary effects on cognition and cerebrovascular disease, as well as Alzheimer’s disease neuropathology.”
In a previous study, individuals younger than 75 years exposed to antihypertensives had an 8% decreased risk of dementia per year of use, while another trial showed that intensive blood pressure–lowering therapy reduced mild cognitive impairment by 19%.
“Despite these encouraging findings ... larger meta-analytic studies have been hampered by the fact that pharmacokinetic properties are typically not considered in existing studies or routine clinical practice,” wrote Dr. Ho and colleagues. “The present study sought to fill this gap [in that it was] a large and longitudinal meta-analytic study of existing data recoded to assess the effects of BBB-crossing potential in renin-angiotensin system [RAS] treatments among hypertensive adults.”
Methods and results
The meta-analysis included randomized clinical trials, prospective cohort studies, and retrospective observational studies. The researchers assessed data on 12,849 individuals from 14 cohorts that received either BBB-crossing or non–BBB-crossing antihypertensives.
The BBB-crossing properties of RAS treatments were identified by a literature review. Of ACE inhibitors, captopril, fosinopril, lisinopril, perindopril, ramipril, and trandolapril were classified as BBB crossing, and benazepril, enalapril, moexipril, and quinapril were classified as non–BBB-crossing. Of ARBs, telmisartan and candesartan were considered BBB-crossing, and olmesartan, eprosartan, irbesartan, and losartan were tagged as non–BBB-crossing.
Cognition was assessed via the following seven domains: executive function, attention, verbal memory learning, language, mental status, recall, and processing speed.
Compared with individuals taking non–BBB-crossing antihypertensives, those taking BBB-crossing agents had significantly superior verbal memory (recall), with a maximum effect size of 0.07 (P = .03).
According to the investigators, this finding was particularly noteworthy, as the BBB-crossing group had relatively higher vascular risk burden and lower mean education level.
“These differences make it all the more remarkable that the BBB-crossing group displayed better memory ability over time despite these cognitive disadvantages,” the investigators wrote.
Still, not all the findings favored BBB-crossing agents. Individuals in the BBB-crossing group had relatively inferior attention ability, with a minimum effect size of –0.17 (P = .02).
The other cognitive measures were not significantly different between groups.
Clinicians may consider findings after accounting for other factors
Principal investigator Daniel A. Nation, PhD, associate professor of psychological science and a faculty member of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, suggested that the small difference in verbal memory between groups could be clinically significant over a longer period of time.
“Although the overall effect size was pretty small, if you look at how long it would take for someone [with dementia] to progress over many years of decline, it would actually end up being a pretty big effect,” Dr. Nation said in an interview. “Small effect sizes could actually end up preventing a lot of cases of dementia,” he added.
The conflicting results in the BBB-crossing group – better verbal memory but worse attention ability – were “surprising,” he noted.
“I sort of didn’t believe it at first,” Dr. Nation said, “because the memory finding is sort of replication – we’d observed the same exact effect on memory in a smaller sample in another study. ... The attention [finding], going another way, was a new thing.”
Dr. Nation suggested that the intergroup differences in attention ability may stem from idiosyncrasies of the tests used to measure that domain, which can be impacted by cardiovascular or brain vascular disease. Or it could be caused by something else entirely, he said, noting that further investigation is needed.
He added that the improvements in verbal memory within the BBB-crossing group could be caused by direct effects on the brain. He pointed out that certain ACE polymorphisms have been linked with Alzheimer’s disease risk, and those same polymorphisms, in animal models, lead to neurodegeneration, with reversal possible through administration of ACE inhibitors.
“It could be that what we’re observing has nothing really to do with blood pressure,” Dr. Nation explained. “This could be a neuronal effect on learning memory systems.”
He went on to suggest that clinicians may consider these findings when selecting antihypertensive agents for their patients, with the caveat that all other prescribing factors have already been taking to account.
“In the event that you’re going to give an ACE inhibitor or an angiotensin receptor blocker anyway, and it ends up being a somewhat arbitrary decision in terms of which specific drug you’re going to give, then perhaps this is a piece of information you would take into account – that one gets in the brain and one doesn’t – in somebody at risk for cognitive decline,” Dr. Nation said.
Exact mechanisms of action unknown
Hélène Girouard, PhD, assistant professor of pharmacology and physiology at the University of Montreal, said in an interview that the findings are “of considerable importance, knowing that brain alterations could begin as much as 30 years before manifestation of dementia.”
Since 2003, Dr. Girouard has been studying the cognitive effects of antihypertensive medications. She noted that previous studies involving rodents “have shown beneficial effects [of BBB-crossing antihypertensive drugs] on cognition independent of their effects on blood pressure.”
The drugs’ exact mechanisms of action, however, remain elusive, according to Dr. Girouard, who offered several possible explanations, including amelioration of BBB disruption, brain inflammation, cerebral blood flow dysregulation, cholinergic dysfunction, and neurologic deficits. “Whether these mechanisms may explain Ho and colleagues’ observations remains to be established,” she added.
Andrea L. Schneider, MD, PhD, assistant professor of neurology at the University of Pennsylvania, Philadelphia, applauded the study, but ultimately suggested that more research is needed to impact clinical decision-making.
“The results of this important and well-done study suggest that further investigation into targeted mechanism-based approaches to selecting hypertension treatment agents, with a specific focus on cognitive outcomes, is warranted,” Dr. Schneider said in an interview. “Before changing clinical practice, further work is necessary to disentangle contributions of medication mechanism, comorbid vascular risk factors, and achieved blood pressure reduction, among others.”
The investigators disclosed support from the National Institutes of Health, the Alzheimer’s Association, the Waksman Foundation of Japan, and others. The interviewees reported no relevant conflicts of interest.
FROM HYPERTENSION

Insomnia in children tied to mood and anxiety disorders in adulthood
, new research indicates. However, insomnia symptoms in childhood that remit in the transition to adolescence do not confer increased risk of mood or anxiety disorders later on, the study found.
“As insomnia symptoms may precipitate or maintain internalizing disorders, our findings further reinforce the need for early sleep interventions to prevent future mental health disorders,” said lead investigator Julio Fernandez-Mendoza, PhD, associate professor at Penn State University, Hershey.
He presented his research at Virtual SLEEP 2021, the 35th annual meeting of the Associated Professional Sleep Societies.
Results ‘very clear’
The findings are based on data from the Penn State Child Cohort, a longitudinal, population-based sample of 700 children with a median age of 9 years, including 421 who were followed up 8 years later as adolescents (median age, 16 years) and 502 who were followed up 15 years later as young adults (median age, 24 years).
The data are “very clear that the risk of having internalizing disorders in young adulthood associated with having persistent insomnia symptoms, since childhood through adolescence into young adulthood,” Dr. Fernandez-Mendoza said in his presentation.
A persistent developmental trajectory was associated with a threefold increased risk of adult internalizing disorder (hazard ratio, 3.19).
The risk of having an internalizing disorder in young adulthood associated with newly developing (incident) insomnia symptoms is about twofold higher (HR, 1.94), whereas the risk associated with the waxing and waning pattern of insomnia is 1.5-fold (HR, 1.53) higher and only marginally significant, he reported.
An equally important finding, said Dr. Fernandez-Mendoza, is that those who had remitted insomnia symptoms in the transition to adolescence and throughout young adulthood were not at increased risk of having an internalizing disorder in young adulthood.
“Insomnia symptoms in a persistent manner associated with long-term adverse mental health outcomes, but remission of those insomnia symptoms associated with a good prognosis,” he said.
It’s also important to note, he said, that about 40% of children do not outgrow their insomnia symptoms in the transition to adolescence and are at risk of developing mental health disorders later on during early adulthood.
Reached for comment, Nitun Verma, MD, a spokesperson for the American Academy of Sleep Medicine, said: “There is a connection with mood and anxiety disorders with sleep, especially insomnia. This is a good reminder that reviewing someone’s sleep habits should always be a part of assessing someone’s mental health.”
A version of this article first appeared on Medscape.com.
, new research indicates. However, insomnia symptoms in childhood that remit in the transition to adolescence do not confer increased risk of mood or anxiety disorders later on, the study found.
“As insomnia symptoms may precipitate or maintain internalizing disorders, our findings further reinforce the need for early sleep interventions to prevent future mental health disorders,” said lead investigator Julio Fernandez-Mendoza, PhD, associate professor at Penn State University, Hershey.
He presented his research at Virtual SLEEP 2021, the 35th annual meeting of the Associated Professional Sleep Societies.
Results ‘very clear’
The findings are based on data from the Penn State Child Cohort, a longitudinal, population-based sample of 700 children with a median age of 9 years, including 421 who were followed up 8 years later as adolescents (median age, 16 years) and 502 who were followed up 15 years later as young adults (median age, 24 years).
The data are “very clear that the risk of having internalizing disorders in young adulthood associated with having persistent insomnia symptoms, since childhood through adolescence into young adulthood,” Dr. Fernandez-Mendoza said in his presentation.
A persistent developmental trajectory was associated with a threefold increased risk of adult internalizing disorder (hazard ratio, 3.19).
The risk of having an internalizing disorder in young adulthood associated with newly developing (incident) insomnia symptoms is about twofold higher (HR, 1.94), whereas the risk associated with the waxing and waning pattern of insomnia is 1.5-fold (HR, 1.53) higher and only marginally significant, he reported.
An equally important finding, said Dr. Fernandez-Mendoza, is that those who had remitted insomnia symptoms in the transition to adolescence and throughout young adulthood were not at increased risk of having an internalizing disorder in young adulthood.
“Insomnia symptoms in a persistent manner associated with long-term adverse mental health outcomes, but remission of those insomnia symptoms associated with a good prognosis,” he said.
It’s also important to note, he said, that about 40% of children do not outgrow their insomnia symptoms in the transition to adolescence and are at risk of developing mental health disorders later on during early adulthood.
Reached for comment, Nitun Verma, MD, a spokesperson for the American Academy of Sleep Medicine, said: “There is a connection with mood and anxiety disorders with sleep, especially insomnia. This is a good reminder that reviewing someone’s sleep habits should always be a part of assessing someone’s mental health.”
A version of this article first appeared on Medscape.com.
, new research indicates. However, insomnia symptoms in childhood that remit in the transition to adolescence do not confer increased risk of mood or anxiety disorders later on, the study found.
“As insomnia symptoms may precipitate or maintain internalizing disorders, our findings further reinforce the need for early sleep interventions to prevent future mental health disorders,” said lead investigator Julio Fernandez-Mendoza, PhD, associate professor at Penn State University, Hershey.
He presented his research at Virtual SLEEP 2021, the 35th annual meeting of the Associated Professional Sleep Societies.
Results ‘very clear’
The findings are based on data from the Penn State Child Cohort, a longitudinal, population-based sample of 700 children with a median age of 9 years, including 421 who were followed up 8 years later as adolescents (median age, 16 years) and 502 who were followed up 15 years later as young adults (median age, 24 years).
The data are “very clear that the risk of having internalizing disorders in young adulthood associated with having persistent insomnia symptoms, since childhood through adolescence into young adulthood,” Dr. Fernandez-Mendoza said in his presentation.
A persistent developmental trajectory was associated with a threefold increased risk of adult internalizing disorder (hazard ratio, 3.19).
The risk of having an internalizing disorder in young adulthood associated with newly developing (incident) insomnia symptoms is about twofold higher (HR, 1.94), whereas the risk associated with the waxing and waning pattern of insomnia is 1.5-fold (HR, 1.53) higher and only marginally significant, he reported.
An equally important finding, said Dr. Fernandez-Mendoza, is that those who had remitted insomnia symptoms in the transition to adolescence and throughout young adulthood were not at increased risk of having an internalizing disorder in young adulthood.
“Insomnia symptoms in a persistent manner associated with long-term adverse mental health outcomes, but remission of those insomnia symptoms associated with a good prognosis,” he said.
It’s also important to note, he said, that about 40% of children do not outgrow their insomnia symptoms in the transition to adolescence and are at risk of developing mental health disorders later on during early adulthood.
Reached for comment, Nitun Verma, MD, a spokesperson for the American Academy of Sleep Medicine, said: “There is a connection with mood and anxiety disorders with sleep, especially insomnia. This is a good reminder that reviewing someone’s sleep habits should always be a part of assessing someone’s mental health.”
A version of this article first appeared on Medscape.com.
Low-dose nitrous oxide shows benefit for resistant depression
A 1-hour treatment with a low concentration of nitrous oxide, commonly known as “laughing gas,” appears to relieve symptoms of treatment-resistant major depression (TRMD), with effects lasting as long as several weeks, new research suggests.

In a trial with a crossover design, investigators randomly assigned 28 patients with severe TRMD to receive a single 1-hour inhalation of placebo or nitrous oxide once a month over a 3-month period. Participants received an inhalation of placebo; a 25% concentration of nitrous oxide; and a 50% concentration of nitrous oxide. Sessions were conducted 4 weeks apart.
Both doses of nitrous oxide were associated with substantial improvement in depressive symptoms for roughly 85% of participants. However, the 25% concentration had a lower risk for adverse effects, which included sedation, nausea, and mild dissociation, compared to the 50% concentration.
“Twenty-five percent nitrous oxide has similar efficacy, compared to 50% nitrous oxide, and reduced side effects fourfold,” lead author Peter Nagele, MD, MSc, chair and professor of anesthesia and critical care, University of Chicago, said in an interview.
“We also observed that many patients had a 2-week improvement of depressive symptoms after a nitrous oxide treatment,” said Dr. Nagele, who also is professor of psychiatry and behavioral neuroscience.
The study was published online June 9 in Science Translational Medicine.
Further refinement
A previous proof-of-principle study conducted by the same researchers demonstrated that a 1-hour inhalation of 50% nitrous oxide had rapid antidepressant effects for patients with TRMD.
The current phase 2 trial “is a follow-up study to our earlier 2015 pilot trial and was designed to further refine the dose of nitrous oxide needed for antidepressant efficacy,” Dr. Nagele said.
“An important secondary aim [of the current study] was to determine whether a lower dose – 25% – would reduce side effects, and a third aim was to determine how long the antidepressants effects last,” he explained.
To investigate, the researchers enrolled 28 patients (median [interquartile range (IQR)] age 39 years [26-68 years]; 71% women; 96% White) to have three inhalation sessions (placebo, 25%, and 50% nitrous oxide) at 4-week intervals. Twenty patients completed all three inhalation sessions, and four completed ≥1 treatment.
Participants had “sustained and refractory depressive illness,” with a mean illness lifetime duration of 17.5 years and an extensive history of antidepressant drug failure (median, 4.5 [2-10] adequate-dose/duration antidepressants).
Some patients had undergone vagus nerve stimulation, electroconvulsive therapy, or repetitive transcranial magnetic stimulation, or had received ketamine (4%, 8%, 13%, and 8%, respectively).
The primary outcome was improvement on the 21-item Hamilton Depression rating Scale (HDRS-21) score over a 2-week observation period.
‘Stronger evidence’
Compared to placebo, nitrous oxide significantly improved depressive symptoms (P = .01). There was no significant difference between the 25% and the 50% concentrations (P = .58).
The estimated difference in HDRS-21 scores between the placebo and various treatment groups are shown in the following table.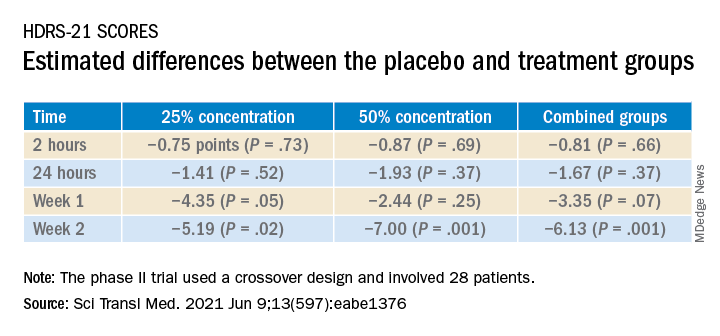
To ensure there where were carryover effects between the two doses, the researchers performed an analysis to ascertain whether order of receipt of the higher dose was related to the 2-week HDRS-21 score; they found no significant effect of trial order (P = .22).
The 20 patients who completed the entire course of treatment “experienced a clinically significant improvement in depressive symptoms from a median baseline HDRS-21 score of 20.5 (IQR, 19.0 to 25.5) to 8.5 (IQR, 2.0 to 16.0) at study completion, corresponding to a median change of −11.0 points (IQR, −3.3 to −14.0 points; P < .0001) after the 3-month study period,” the investigators noted.
The types of treatment response and improvement in depressive symptoms from baseline to study completion are listed in the table below.
There were statistically significant differences in adverse events between the two treatment doses; 47 events occurred following inhalation of the 50% concentration, compared to 11 after inhalation of the 25% concentration. There were six adverse events after inhalation of placebo (P < .0001).
“None of the adverse events were serious, and nearly all occurred either during or immediately after the treatment session and resolved within several hours,” the authors reported.
“We need to be remindful that – despite the exciting results of the study – the study was small and cannot be considered definitive evidence; as such, it is too early to advocate for the use of nitrous oxide in everyday clinical practice,” Dr. Nagele said.
Nevertheless, on the basis of the current findings, he stated.
Rapid-acting antidepressants
Commenting on the study in an interview, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit at Toronto Western Hospital, noted that the research into nitrous oxide is “part of an interest in rapid-acting antidepressants.”
Dr. McIntyre, also the chairman and executive director of the Brain and Cognition Discovery Foundation, Toronto, who was not involved with the study, found it “interesting” that “almost 20% of the sample had previously had suboptimal outcomes to ketamine and/or neurostimulation, meaning these patients had serious refractory illness, but the benefit [of nitrous oxide] was sustained at 2 weeks.”
Studies of the use of nitrous oxide for patients with bipolar depression “would be warranted, since it appears generally safe and well tolerated,” said Dr. McIntyre, director of the Depression and Bipolar Support Alliance.
The study was sponsored by an award to Dr. Nagele from the NARSAD Independent Investigator Award from the Brain and Behavior Research Foundation and an award to Dr. Nagele and other coauthors from the Taylor Family Institute for Innovative Psychiatric Research at Washington University in St. Louis. Dr. Nagele receives funding from the National Institute of Mental Health the American Foundation for Prevention of Suicide, and the Brain and Behavior Research Foundation; has received research funding and honoraria from Roche Diagnostics and Abbott Diagnostics; and has previously filed for intellectual property protection related to the use of nitrous oxide in major depression. The other authors’ disclosures are listed on the original article. Dr. McIntyre has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation; speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, Eisai, Minerva, Intra-Cellular, and Abbvie. Dr. McIntyre is also CEO of AltMed.
A version of this article first appeared on Medscape.com.
A 1-hour treatment with a low concentration of nitrous oxide, commonly known as “laughing gas,” appears to relieve symptoms of treatment-resistant major depression (TRMD), with effects lasting as long as several weeks, new research suggests.
In a trial with a crossover design, investigators randomly assigned 28 patients with severe TRMD to receive a single 1-hour inhalation of placebo or nitrous oxide once a month over a 3-month period. Participants received an inhalation of placebo; a 25% concentration of nitrous oxide; and a 50% concentration of nitrous oxide. Sessions were conducted 4 weeks apart.
Both doses of nitrous oxide were associated with substantial improvement in depressive symptoms for roughly 85% of participants. However, the 25% concentration had a lower risk for adverse effects, which included sedation, nausea, and mild dissociation, compared to the 50% concentration.
“Twenty-five percent nitrous oxide has similar efficacy, compared to 50% nitrous oxide, and reduced side effects fourfold,” lead author Peter Nagele, MD, MSc, chair and professor of anesthesia and critical care, University of Chicago, said in an interview.
“We also observed that many patients had a 2-week improvement of depressive symptoms after a nitrous oxide treatment,” said Dr. Nagele, who also is professor of psychiatry and behavioral neuroscience.
The study was published online June 9 in Science Translational Medicine.
Further refinement
A previous proof-of-principle study conducted by the same researchers demonstrated that a 1-hour inhalation of 50% nitrous oxide had rapid antidepressant effects for patients with TRMD.
The current phase 2 trial “is a follow-up study to our earlier 2015 pilot trial and was designed to further refine the dose of nitrous oxide needed for antidepressant efficacy,” Dr. Nagele said.
“An important secondary aim [of the current study] was to determine whether a lower dose – 25% – would reduce side effects, and a third aim was to determine how long the antidepressants effects last,” he explained.
To investigate, the researchers enrolled 28 patients (median [interquartile range (IQR)] age 39 years [26-68 years]; 71% women; 96% White) to have three inhalation sessions (placebo, 25%, and 50% nitrous oxide) at 4-week intervals. Twenty patients completed all three inhalation sessions, and four completed ≥1 treatment.
Participants had “sustained and refractory depressive illness,” with a mean illness lifetime duration of 17.5 years and an extensive history of antidepressant drug failure (median, 4.5 [2-10] adequate-dose/duration antidepressants).
Some patients had undergone vagus nerve stimulation, electroconvulsive therapy, or repetitive transcranial magnetic stimulation, or had received ketamine (4%, 8%, 13%, and 8%, respectively).
The primary outcome was improvement on the 21-item Hamilton Depression rating Scale (HDRS-21) score over a 2-week observation period.
‘Stronger evidence’
Compared to placebo, nitrous oxide significantly improved depressive symptoms (P = .01). There was no significant difference between the 25% and the 50% concentrations (P = .58).
The estimated difference in HDRS-21 scores between the placebo and various treatment groups are shown in the following table.
To ensure there where were carryover effects between the two doses, the researchers performed an analysis to ascertain whether order of receipt of the higher dose was related to the 2-week HDRS-21 score; they found no significant effect of trial order (P = .22).
The 20 patients who completed the entire course of treatment “experienced a clinically significant improvement in depressive symptoms from a median baseline HDRS-21 score of 20.5 (IQR, 19.0 to 25.5) to 8.5 (IQR, 2.0 to 16.0) at study completion, corresponding to a median change of −11.0 points (IQR, −3.3 to −14.0 points; P < .0001) after the 3-month study period,” the investigators noted.
The types of treatment response and improvement in depressive symptoms from baseline to study completion are listed in the table below.
There were statistically significant differences in adverse events between the two treatment doses; 47 events occurred following inhalation of the 50% concentration, compared to 11 after inhalation of the 25% concentration. There were six adverse events after inhalation of placebo (P < .0001).
“None of the adverse events were serious, and nearly all occurred either during or immediately after the treatment session and resolved within several hours,” the authors reported.
“We need to be remindful that – despite the exciting results of the study – the study was small and cannot be considered definitive evidence; as such, it is too early to advocate for the use of nitrous oxide in everyday clinical practice,” Dr. Nagele said.
Nevertheless, on the basis of the current findings, he stated.
Rapid-acting antidepressants
Commenting on the study in an interview, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit at Toronto Western Hospital, noted that the research into nitrous oxide is “part of an interest in rapid-acting antidepressants.”
Dr. McIntyre, also the chairman and executive director of the Brain and Cognition Discovery Foundation, Toronto, who was not involved with the study, found it “interesting” that “almost 20% of the sample had previously had suboptimal outcomes to ketamine and/or neurostimulation, meaning these patients had serious refractory illness, but the benefit [of nitrous oxide] was sustained at 2 weeks.”
Studies of the use of nitrous oxide for patients with bipolar depression “would be warranted, since it appears generally safe and well tolerated,” said Dr. McIntyre, director of the Depression and Bipolar Support Alliance.
The study was sponsored by an award to Dr. Nagele from the NARSAD Independent Investigator Award from the Brain and Behavior Research Foundation and an award to Dr. Nagele and other coauthors from the Taylor Family Institute for Innovative Psychiatric Research at Washington University in St. Louis. Dr. Nagele receives funding from the National Institute of Mental Health the American Foundation for Prevention of Suicide, and the Brain and Behavior Research Foundation; has received research funding and honoraria from Roche Diagnostics and Abbott Diagnostics; and has previously filed for intellectual property protection related to the use of nitrous oxide in major depression. The other authors’ disclosures are listed on the original article. Dr. McIntyre has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation; speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, Eisai, Minerva, Intra-Cellular, and Abbvie. Dr. McIntyre is also CEO of AltMed.
A version of this article first appeared on Medscape.com.
A 1-hour treatment with a low concentration of nitrous oxide, commonly known as “laughing gas,” appears to relieve symptoms of treatment-resistant major depression (TRMD), with effects lasting as long as several weeks, new research suggests.
In a trial with a crossover design, investigators randomly assigned 28 patients with severe TRMD to receive a single 1-hour inhalation of placebo or nitrous oxide once a month over a 3-month period. Participants received an inhalation of placebo; a 25% concentration of nitrous oxide; and a 50% concentration of nitrous oxide. Sessions were conducted 4 weeks apart.
Both doses of nitrous oxide were associated with substantial improvement in depressive symptoms for roughly 85% of participants. However, the 25% concentration had a lower risk for adverse effects, which included sedation, nausea, and mild dissociation, compared to the 50% concentration.
“Twenty-five percent nitrous oxide has similar efficacy, compared to 50% nitrous oxide, and reduced side effects fourfold,” lead author Peter Nagele, MD, MSc, chair and professor of anesthesia and critical care, University of Chicago, said in an interview.
“We also observed that many patients had a 2-week improvement of depressive symptoms after a nitrous oxide treatment,” said Dr. Nagele, who also is professor of psychiatry and behavioral neuroscience.
The study was published online June 9 in Science Translational Medicine.
Further refinement
A previous proof-of-principle study conducted by the same researchers demonstrated that a 1-hour inhalation of 50% nitrous oxide had rapid antidepressant effects for patients with TRMD.
The current phase 2 trial “is a follow-up study to our earlier 2015 pilot trial and was designed to further refine the dose of nitrous oxide needed for antidepressant efficacy,” Dr. Nagele said.
“An important secondary aim [of the current study] was to determine whether a lower dose – 25% – would reduce side effects, and a third aim was to determine how long the antidepressants effects last,” he explained.
To investigate, the researchers enrolled 28 patients (median [interquartile range (IQR)] age 39 years [26-68 years]; 71% women; 96% White) to have three inhalation sessions (placebo, 25%, and 50% nitrous oxide) at 4-week intervals. Twenty patients completed all three inhalation sessions, and four completed ≥1 treatment.
Participants had “sustained and refractory depressive illness,” with a mean illness lifetime duration of 17.5 years and an extensive history of antidepressant drug failure (median, 4.5 [2-10] adequate-dose/duration antidepressants).
Some patients had undergone vagus nerve stimulation, electroconvulsive therapy, or repetitive transcranial magnetic stimulation, or had received ketamine (4%, 8%, 13%, and 8%, respectively).
The primary outcome was improvement on the 21-item Hamilton Depression rating Scale (HDRS-21) score over a 2-week observation period.
‘Stronger evidence’
Compared to placebo, nitrous oxide significantly improved depressive symptoms (P = .01). There was no significant difference between the 25% and the 50% concentrations (P = .58).
The estimated difference in HDRS-21 scores between the placebo and various treatment groups are shown in the following table.
To ensure there where were carryover effects between the two doses, the researchers performed an analysis to ascertain whether order of receipt of the higher dose was related to the 2-week HDRS-21 score; they found no significant effect of trial order (P = .22).
The 20 patients who completed the entire course of treatment “experienced a clinically significant improvement in depressive symptoms from a median baseline HDRS-21 score of 20.5 (IQR, 19.0 to 25.5) to 8.5 (IQR, 2.0 to 16.0) at study completion, corresponding to a median change of −11.0 points (IQR, −3.3 to −14.0 points; P < .0001) after the 3-month study period,” the investigators noted.
The types of treatment response and improvement in depressive symptoms from baseline to study completion are listed in the table below.
There were statistically significant differences in adverse events between the two treatment doses; 47 events occurred following inhalation of the 50% concentration, compared to 11 after inhalation of the 25% concentration. There were six adverse events after inhalation of placebo (P < .0001).
“None of the adverse events were serious, and nearly all occurred either during or immediately after the treatment session and resolved within several hours,” the authors reported.
“We need to be remindful that – despite the exciting results of the study – the study was small and cannot be considered definitive evidence; as such, it is too early to advocate for the use of nitrous oxide in everyday clinical practice,” Dr. Nagele said.
Nevertheless, on the basis of the current findings, he stated.
Rapid-acting antidepressants
Commenting on the study in an interview, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit at Toronto Western Hospital, noted that the research into nitrous oxide is “part of an interest in rapid-acting antidepressants.”
Dr. McIntyre, also the chairman and executive director of the Brain and Cognition Discovery Foundation, Toronto, who was not involved with the study, found it “interesting” that “almost 20% of the sample had previously had suboptimal outcomes to ketamine and/or neurostimulation, meaning these patients had serious refractory illness, but the benefit [of nitrous oxide] was sustained at 2 weeks.”
Studies of the use of nitrous oxide for patients with bipolar depression “would be warranted, since it appears generally safe and well tolerated,” said Dr. McIntyre, director of the Depression and Bipolar Support Alliance.
The study was sponsored by an award to Dr. Nagele from the NARSAD Independent Investigator Award from the Brain and Behavior Research Foundation and an award to Dr. Nagele and other coauthors from the Taylor Family Institute for Innovative Psychiatric Research at Washington University in St. Louis. Dr. Nagele receives funding from the National Institute of Mental Health the American Foundation for Prevention of Suicide, and the Brain and Behavior Research Foundation; has received research funding and honoraria from Roche Diagnostics and Abbott Diagnostics; and has previously filed for intellectual property protection related to the use of nitrous oxide in major depression. The other authors’ disclosures are listed on the original article. Dr. McIntyre has received research grant support from CIHR/GACD/Chinese National Natural Research Foundation; speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, Eisai, Minerva, Intra-Cellular, and Abbvie. Dr. McIntyre is also CEO of AltMed.
A version of this article first appeared on Medscape.com.