User login
Intranasal oxytocin for autism promising – then came the data
When parents of children with autism spectrum disorder (ASD) participating in the largest clinical trial of intranasal oxytocin to date came in for follow-up visits with investigators, they reported marked improvement in the children’s social functioning.
Kids who rarely communicated with their families began to interact more. Those who usually preferred to isolate themselves started joining their parents for meals. It all seemed so promising – until the data came in.
“Those sounded like real improvements to me, and it seemed like they increased over the period of the study,” lead investigator Linmarie Sikich, MD, an associate clinical professor of psychiatry with Duke University School of Medicine and the Duke Center for Autism and Brain Development, Durham, N.C., told this news organization. “Turns out it wasn’t oxytocin that was making that difference.”
Researchers found that after 24 weeks of daily treatment with intranasal oxytocin, there were no significant differences in social functioning between children who received active treatment and those in the placebo group.
The much-anticipated results were published online in The New England Journal of Medicine. To say that they are disappointing, Dr. Sikich said, is an understatement.
Increase in off-label use
Most studies in mouse models of ASD and small trials in children produced conflicting results, although there were modest improvements in social functioning associated with the use of intranasal oxytocin. Some clinicians were already prescribing it off label.
On the basis of this research and early feedback from parents of children, Dr. Sikich and colleagues were hopeful.
However, results from a rigorous, 5-year, $11.4 million randomized trial were negative. Yet, parents were convinced their child improved during the study, and there was a significant increase in off-label prescribing of a treatment her research says doesn’t work. What’s next for oxytocin?
Known as the “love hormone,” oxytocin is a neurotransmitter that is primarily synthesized in the hypothalamus. It plays a role in childbirth and lactation and is also involved in the regulation of social functioning and emotions. Research suggests low oxytocin levels are associated with diminished social functioning, regardless of ASD status.
Its potential as an autism therapy for children has been under study for a decade. Some findings link its use to improvements in core deficits associated with ASD, including repetitive behaviors, fixated or restricted interest, and social communication. A study published in 2020 showed that the treatment improved symptoms in high-functioning adults with ASD.
These were mostly small studies and were underpowered to reliably detect an effect of the therapy on social functioning. They often involved only a single dose of oxytocin. Some studies showed improvements, but others did not.
Still, interest in the treatment grew. Physicians began prescribing it for children with ASD, and parents began buying products containing oxytocin on the internet. Researchers feared this off-label use was becoming widespread, despite inconclusive evidence of efficacy.
High hopes
With support from a National Institutes of Health grant, Dr. Sikich and her team designed a phase 2, multicenter, randomized, double-blind, placebo-controlled study to determine whether the use of oxytocin in children with ASD works and is safe.
The challenges began before they even enrolled a single child. A number of behavioral assessment tools are used to measure social function in ASD, but there is no consensus on which one is best.
A simple blood test could determine how much oxytocin from the nasal spray was absorbed in the blood, but identifying how much made it to the brain would require fMRI, which is expensive and is challenging to use in this study population. Then there was the acquisition of the drug itself.
The Food and Drug Administration has approved intravenous oxytocin for inducing labor. Intranasal oxytocin is not approved for any indication and isn’t available commercially in the United States. Patients or researchers must secure the drug from a manufacturer in a country where it is approved or order it from a U.S. pharmacy that is capable of compounding IV oxytocin into an intranasal formulation.
The pharmacy in Switzerland Dr. Sikich planned to use couldn’t make enough for the study. Contracting with a compounding pharmacy in the United States was significantly more expensive and time consuming, but it was the researchers’ only option.
“If it hadn’t been something we expected to have a major benefit, I think we would have given up the project at multiple points along the line due to all of these challenges,” said Dr. Sikich.
In August 2014, with all the pieces finally in place, researchers began enrolling children aged 3-17 years. The final cohort included 290 participants with ASD, 146 in the oxytocin group and 144 in the placebo group. Of these, 48% had minimal verbal fluency, and 52% had fluent verbal speech.
Participants received daily synthetic oxytocin or placebo via a nasal spray for 24 weeks. The daily oxytocin dose was 48 IU for the first 7 weeks. After that, the dosage could be titrated to a maximum of 80 IU/d. The mean maximal total daily dose of oxytocin throughout the study was 67.6 ± 16.9 IU.
‘It just didn’t work’
Both study groups showed improvement in social withdrawal beginning at 4 weeks and continuing throughout the trial, as determined on the basis of caretakers’ responses on the Aberrant Behavior Checklist Modified Social Withdrawal Subscale, the study’s primary outcome measure.
Sociability and social motivation also improved in both groups, as measured by the Pervasive Developmental Disorders Behavior Inventory and the Social Responsiveness Scale.
But by the end of the trial, the difference between the groups in improvement of social function wasn’t significant (difference, -0.2 points; P = .61) after adjusting for age, verbal fluency, and baseline oxytocin level.
“We were so convinced that it would work,” Dr. Sikich said, “but it just didn’t.”
From observation, parents were also convinced the therapy was working. At the trial’s conclusion, fewer than half of caregivers correctly guessed whether their child was in the treatment group or the placebo group.
A lot of development changes can happen in a child over 6 months. It’s possible the improvements would have occurred regardless of the trial, Dr. Sikich said. Parents’ perceptions could also be a placebo effect. Their child was in a clinical trial of a drug they believed could improve social functioning, so in their mind, it did.
Caregivers received training in how to identify certain behavioral changes, which may have helped them spot an existing positive change they had previously overlooked. Or they may have worked with their child more intently as a result of their participation in the trial.
“People may start doing more things or doing them more intensively or purposefully, consciously or subconsciously, to try to help their child improve the skills or behaviors targeted by the active therapy in the study,” Dr. Sikich said. “These are things that might really help the child move forward which are completely separate from the medication being studied.”
The safety analysis offered more hopeful results. Only one serious adverse event from the treatment was reported: A 17-year-old participant taking a daily dose of 48 IU experienced a sedating effect while driving and had an accident.
Too soon to walk away?
Perhaps the most important take-away from the study is that even if it’s safe, intranasal oxytocin as it is currently used doesn’t work and clinicians shouldn’t prescribe it, said Daniel Geschwind, MD, PhD, director of the University of California, Los Angeles (UCLA) Center for Autism Research, who penned a commentary on the study and discussed the findings with this news organization.
“This study shows that using oxytocin the way it’s used in the community right now is not helping anybody, so why put a child through that?” added Dr. Geschwind, who also is a professor of genetics, neurology, and psychiatry at UCLA.
The trial highlights areas that need to be addressed in order to improve research in the field, he said. Establishing a consensus process to measure social functioning and figuring out a better way to access intranasal oxytocin would lead to studies that are more conclusive, comparable, and less expensive. Dr. Sikich agrees.
Despite the findings, Dr. Geschwind and other autism researchers say it’s too soon to walk away from oxytocin altogether, although it may be time to change the approach to autism research.
“We have to take a page from the playbook of modern medicine in other areas and begin to recognize that these syndromes are incredibly heterogeneous,” Dr. Geschwind says. “We can surmise, although we don’t know, that there might be different biological forms of autism that have different pathways involved that are going to respond differently to different medications.”
Calling the researchers’ efforts “heroic,” Karen Parker, PhD, an associate professor and associate chair of psychiatry and behavioral sciences at Stanford (Calif.) University, says efficacy trials such as this one are critical. However, Dr. Parker said in an interview, there are a number of questions that the study didn’t address.
The majority of medication dispensed in a standard intranasal device is sprayed into the back of the throat. Regular blood tests confirmed that oxytocin was getting into participants’ system, but, given how quickly oxytocin degrades in the blood, Dr. Parker said it’s hard to know just how much reached the brain.
It’s also unclear whether the results would have been different had the treatment been paired with behavioral therapy, an approach Dr. Parker suggests might benefit a subset of children with ASD.
A 2017 study from Dr. Parker’s lab found that children with ASD whose use of oxytocin at baseline was low derived greater benefit from synthetic oxytocin, something the new study failed to find. Still, Dr. Parker said, it’s possible oxytocin might increase social motivation and increase a child’s receptiveness to behavioral therapy.
“When you see a negative trial like this, it decreases enthusiasm for the therapy for autism in this context,” Dr. Parker said. “I hope people who are studying these syndromes will continue to explore oxytocin as a therapy.”
The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development through the Autism Centers of Excellence Program and the Department of Psychiatry and Behavioral Sciences at Duke University. Full disclosures of the authors’ possible conflicts of interest are available online.
A version of this article first appeared on Medscape.com.
When parents of children with autism spectrum disorder (ASD) participating in the largest clinical trial of intranasal oxytocin to date came in for follow-up visits with investigators, they reported marked improvement in the children’s social functioning.
Kids who rarely communicated with their families began to interact more. Those who usually preferred to isolate themselves started joining their parents for meals. It all seemed so promising – until the data came in.
“Those sounded like real improvements to me, and it seemed like they increased over the period of the study,” lead investigator Linmarie Sikich, MD, an associate clinical professor of psychiatry with Duke University School of Medicine and the Duke Center for Autism and Brain Development, Durham, N.C., told this news organization. “Turns out it wasn’t oxytocin that was making that difference.”
Researchers found that after 24 weeks of daily treatment with intranasal oxytocin, there were no significant differences in social functioning between children who received active treatment and those in the placebo group.
The much-anticipated results were published online in The New England Journal of Medicine. To say that they are disappointing, Dr. Sikich said, is an understatement.
Increase in off-label use
Most studies in mouse models of ASD and small trials in children produced conflicting results, although there were modest improvements in social functioning associated with the use of intranasal oxytocin. Some clinicians were already prescribing it off label.
On the basis of this research and early feedback from parents of children, Dr. Sikich and colleagues were hopeful.
However, results from a rigorous, 5-year, $11.4 million randomized trial were negative. Yet, parents were convinced their child improved during the study, and there was a significant increase in off-label prescribing of a treatment her research says doesn’t work. What’s next for oxytocin?
Known as the “love hormone,” oxytocin is a neurotransmitter that is primarily synthesized in the hypothalamus. It plays a role in childbirth and lactation and is also involved in the regulation of social functioning and emotions. Research suggests low oxytocin levels are associated with diminished social functioning, regardless of ASD status.
Its potential as an autism therapy for children has been under study for a decade. Some findings link its use to improvements in core deficits associated with ASD, including repetitive behaviors, fixated or restricted interest, and social communication. A study published in 2020 showed that the treatment improved symptoms in high-functioning adults with ASD.
These were mostly small studies and were underpowered to reliably detect an effect of the therapy on social functioning. They often involved only a single dose of oxytocin. Some studies showed improvements, but others did not.
Still, interest in the treatment grew. Physicians began prescribing it for children with ASD, and parents began buying products containing oxytocin on the internet. Researchers feared this off-label use was becoming widespread, despite inconclusive evidence of efficacy.
High hopes
With support from a National Institutes of Health grant, Dr. Sikich and her team designed a phase 2, multicenter, randomized, double-blind, placebo-controlled study to determine whether the use of oxytocin in children with ASD works and is safe.
The challenges began before they even enrolled a single child. A number of behavioral assessment tools are used to measure social function in ASD, but there is no consensus on which one is best.
A simple blood test could determine how much oxytocin from the nasal spray was absorbed in the blood, but identifying how much made it to the brain would require fMRI, which is expensive and is challenging to use in this study population. Then there was the acquisition of the drug itself.
The Food and Drug Administration has approved intravenous oxytocin for inducing labor. Intranasal oxytocin is not approved for any indication and isn’t available commercially in the United States. Patients or researchers must secure the drug from a manufacturer in a country where it is approved or order it from a U.S. pharmacy that is capable of compounding IV oxytocin into an intranasal formulation.
The pharmacy in Switzerland Dr. Sikich planned to use couldn’t make enough for the study. Contracting with a compounding pharmacy in the United States was significantly more expensive and time consuming, but it was the researchers’ only option.
“If it hadn’t been something we expected to have a major benefit, I think we would have given up the project at multiple points along the line due to all of these challenges,” said Dr. Sikich.
In August 2014, with all the pieces finally in place, researchers began enrolling children aged 3-17 years. The final cohort included 290 participants with ASD, 146 in the oxytocin group and 144 in the placebo group. Of these, 48% had minimal verbal fluency, and 52% had fluent verbal speech.
Participants received daily synthetic oxytocin or placebo via a nasal spray for 24 weeks. The daily oxytocin dose was 48 IU for the first 7 weeks. After that, the dosage could be titrated to a maximum of 80 IU/d. The mean maximal total daily dose of oxytocin throughout the study was 67.6 ± 16.9 IU.
‘It just didn’t work’
Both study groups showed improvement in social withdrawal beginning at 4 weeks and continuing throughout the trial, as determined on the basis of caretakers’ responses on the Aberrant Behavior Checklist Modified Social Withdrawal Subscale, the study’s primary outcome measure.
Sociability and social motivation also improved in both groups, as measured by the Pervasive Developmental Disorders Behavior Inventory and the Social Responsiveness Scale.
But by the end of the trial, the difference between the groups in improvement of social function wasn’t significant (difference, -0.2 points; P = .61) after adjusting for age, verbal fluency, and baseline oxytocin level.
“We were so convinced that it would work,” Dr. Sikich said, “but it just didn’t.”
From observation, parents were also convinced the therapy was working. At the trial’s conclusion, fewer than half of caregivers correctly guessed whether their child was in the treatment group or the placebo group.
A lot of development changes can happen in a child over 6 months. It’s possible the improvements would have occurred regardless of the trial, Dr. Sikich said. Parents’ perceptions could also be a placebo effect. Their child was in a clinical trial of a drug they believed could improve social functioning, so in their mind, it did.
Caregivers received training in how to identify certain behavioral changes, which may have helped them spot an existing positive change they had previously overlooked. Or they may have worked with their child more intently as a result of their participation in the trial.
“People may start doing more things or doing them more intensively or purposefully, consciously or subconsciously, to try to help their child improve the skills or behaviors targeted by the active therapy in the study,” Dr. Sikich said. “These are things that might really help the child move forward which are completely separate from the medication being studied.”
The safety analysis offered more hopeful results. Only one serious adverse event from the treatment was reported: A 17-year-old participant taking a daily dose of 48 IU experienced a sedating effect while driving and had an accident.
Too soon to walk away?
Perhaps the most important take-away from the study is that even if it’s safe, intranasal oxytocin as it is currently used doesn’t work and clinicians shouldn’t prescribe it, said Daniel Geschwind, MD, PhD, director of the University of California, Los Angeles (UCLA) Center for Autism Research, who penned a commentary on the study and discussed the findings with this news organization.
“This study shows that using oxytocin the way it’s used in the community right now is not helping anybody, so why put a child through that?” added Dr. Geschwind, who also is a professor of genetics, neurology, and psychiatry at UCLA.
The trial highlights areas that need to be addressed in order to improve research in the field, he said. Establishing a consensus process to measure social functioning and figuring out a better way to access intranasal oxytocin would lead to studies that are more conclusive, comparable, and less expensive. Dr. Sikich agrees.
Despite the findings, Dr. Geschwind and other autism researchers say it’s too soon to walk away from oxytocin altogether, although it may be time to change the approach to autism research.
“We have to take a page from the playbook of modern medicine in other areas and begin to recognize that these syndromes are incredibly heterogeneous,” Dr. Geschwind says. “We can surmise, although we don’t know, that there might be different biological forms of autism that have different pathways involved that are going to respond differently to different medications.”
Calling the researchers’ efforts “heroic,” Karen Parker, PhD, an associate professor and associate chair of psychiatry and behavioral sciences at Stanford (Calif.) University, says efficacy trials such as this one are critical. However, Dr. Parker said in an interview, there are a number of questions that the study didn’t address.
The majority of medication dispensed in a standard intranasal device is sprayed into the back of the throat. Regular blood tests confirmed that oxytocin was getting into participants’ system, but, given how quickly oxytocin degrades in the blood, Dr. Parker said it’s hard to know just how much reached the brain.
It’s also unclear whether the results would have been different had the treatment been paired with behavioral therapy, an approach Dr. Parker suggests might benefit a subset of children with ASD.
A 2017 study from Dr. Parker’s lab found that children with ASD whose use of oxytocin at baseline was low derived greater benefit from synthetic oxytocin, something the new study failed to find. Still, Dr. Parker said, it’s possible oxytocin might increase social motivation and increase a child’s receptiveness to behavioral therapy.
“When you see a negative trial like this, it decreases enthusiasm for the therapy for autism in this context,” Dr. Parker said. “I hope people who are studying these syndromes will continue to explore oxytocin as a therapy.”
The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development through the Autism Centers of Excellence Program and the Department of Psychiatry and Behavioral Sciences at Duke University. Full disclosures of the authors’ possible conflicts of interest are available online.
A version of this article first appeared on Medscape.com.
When parents of children with autism spectrum disorder (ASD) participating in the largest clinical trial of intranasal oxytocin to date came in for follow-up visits with investigators, they reported marked improvement in the children’s social functioning.
Kids who rarely communicated with their families began to interact more. Those who usually preferred to isolate themselves started joining their parents for meals. It all seemed so promising – until the data came in.
“Those sounded like real improvements to me, and it seemed like they increased over the period of the study,” lead investigator Linmarie Sikich, MD, an associate clinical professor of psychiatry with Duke University School of Medicine and the Duke Center for Autism and Brain Development, Durham, N.C., told this news organization. “Turns out it wasn’t oxytocin that was making that difference.”
Researchers found that after 24 weeks of daily treatment with intranasal oxytocin, there were no significant differences in social functioning between children who received active treatment and those in the placebo group.
The much-anticipated results were published online in The New England Journal of Medicine. To say that they are disappointing, Dr. Sikich said, is an understatement.
Increase in off-label use
Most studies in mouse models of ASD and small trials in children produced conflicting results, although there were modest improvements in social functioning associated with the use of intranasal oxytocin. Some clinicians were already prescribing it off label.
On the basis of this research and early feedback from parents of children, Dr. Sikich and colleagues were hopeful.
However, results from a rigorous, 5-year, $11.4 million randomized trial were negative. Yet, parents were convinced their child improved during the study, and there was a significant increase in off-label prescribing of a treatment her research says doesn’t work. What’s next for oxytocin?
Known as the “love hormone,” oxytocin is a neurotransmitter that is primarily synthesized in the hypothalamus. It plays a role in childbirth and lactation and is also involved in the regulation of social functioning and emotions. Research suggests low oxytocin levels are associated with diminished social functioning, regardless of ASD status.
Its potential as an autism therapy for children has been under study for a decade. Some findings link its use to improvements in core deficits associated with ASD, including repetitive behaviors, fixated or restricted interest, and social communication. A study published in 2020 showed that the treatment improved symptoms in high-functioning adults with ASD.
These were mostly small studies and were underpowered to reliably detect an effect of the therapy on social functioning. They often involved only a single dose of oxytocin. Some studies showed improvements, but others did not.
Still, interest in the treatment grew. Physicians began prescribing it for children with ASD, and parents began buying products containing oxytocin on the internet. Researchers feared this off-label use was becoming widespread, despite inconclusive evidence of efficacy.
High hopes
With support from a National Institutes of Health grant, Dr. Sikich and her team designed a phase 2, multicenter, randomized, double-blind, placebo-controlled study to determine whether the use of oxytocin in children with ASD works and is safe.
The challenges began before they even enrolled a single child. A number of behavioral assessment tools are used to measure social function in ASD, but there is no consensus on which one is best.
A simple blood test could determine how much oxytocin from the nasal spray was absorbed in the blood, but identifying how much made it to the brain would require fMRI, which is expensive and is challenging to use in this study population. Then there was the acquisition of the drug itself.
The Food and Drug Administration has approved intravenous oxytocin for inducing labor. Intranasal oxytocin is not approved for any indication and isn’t available commercially in the United States. Patients or researchers must secure the drug from a manufacturer in a country where it is approved or order it from a U.S. pharmacy that is capable of compounding IV oxytocin into an intranasal formulation.
The pharmacy in Switzerland Dr. Sikich planned to use couldn’t make enough for the study. Contracting with a compounding pharmacy in the United States was significantly more expensive and time consuming, but it was the researchers’ only option.
“If it hadn’t been something we expected to have a major benefit, I think we would have given up the project at multiple points along the line due to all of these challenges,” said Dr. Sikich.
In August 2014, with all the pieces finally in place, researchers began enrolling children aged 3-17 years. The final cohort included 290 participants with ASD, 146 in the oxytocin group and 144 in the placebo group. Of these, 48% had minimal verbal fluency, and 52% had fluent verbal speech.
Participants received daily synthetic oxytocin or placebo via a nasal spray for 24 weeks. The daily oxytocin dose was 48 IU for the first 7 weeks. After that, the dosage could be titrated to a maximum of 80 IU/d. The mean maximal total daily dose of oxytocin throughout the study was 67.6 ± 16.9 IU.
‘It just didn’t work’
Both study groups showed improvement in social withdrawal beginning at 4 weeks and continuing throughout the trial, as determined on the basis of caretakers’ responses on the Aberrant Behavior Checklist Modified Social Withdrawal Subscale, the study’s primary outcome measure.
Sociability and social motivation also improved in both groups, as measured by the Pervasive Developmental Disorders Behavior Inventory and the Social Responsiveness Scale.
But by the end of the trial, the difference between the groups in improvement of social function wasn’t significant (difference, -0.2 points; P = .61) after adjusting for age, verbal fluency, and baseline oxytocin level.
“We were so convinced that it would work,” Dr. Sikich said, “but it just didn’t.”
From observation, parents were also convinced the therapy was working. At the trial’s conclusion, fewer than half of caregivers correctly guessed whether their child was in the treatment group or the placebo group.
A lot of development changes can happen in a child over 6 months. It’s possible the improvements would have occurred regardless of the trial, Dr. Sikich said. Parents’ perceptions could also be a placebo effect. Their child was in a clinical trial of a drug they believed could improve social functioning, so in their mind, it did.
Caregivers received training in how to identify certain behavioral changes, which may have helped them spot an existing positive change they had previously overlooked. Or they may have worked with their child more intently as a result of their participation in the trial.
“People may start doing more things or doing them more intensively or purposefully, consciously or subconsciously, to try to help their child improve the skills or behaviors targeted by the active therapy in the study,” Dr. Sikich said. “These are things that might really help the child move forward which are completely separate from the medication being studied.”
The safety analysis offered more hopeful results. Only one serious adverse event from the treatment was reported: A 17-year-old participant taking a daily dose of 48 IU experienced a sedating effect while driving and had an accident.
Too soon to walk away?
Perhaps the most important take-away from the study is that even if it’s safe, intranasal oxytocin as it is currently used doesn’t work and clinicians shouldn’t prescribe it, said Daniel Geschwind, MD, PhD, director of the University of California, Los Angeles (UCLA) Center for Autism Research, who penned a commentary on the study and discussed the findings with this news organization.
“This study shows that using oxytocin the way it’s used in the community right now is not helping anybody, so why put a child through that?” added Dr. Geschwind, who also is a professor of genetics, neurology, and psychiatry at UCLA.
The trial highlights areas that need to be addressed in order to improve research in the field, he said. Establishing a consensus process to measure social functioning and figuring out a better way to access intranasal oxytocin would lead to studies that are more conclusive, comparable, and less expensive. Dr. Sikich agrees.
Despite the findings, Dr. Geschwind and other autism researchers say it’s too soon to walk away from oxytocin altogether, although it may be time to change the approach to autism research.
“We have to take a page from the playbook of modern medicine in other areas and begin to recognize that these syndromes are incredibly heterogeneous,” Dr. Geschwind says. “We can surmise, although we don’t know, that there might be different biological forms of autism that have different pathways involved that are going to respond differently to different medications.”
Calling the researchers’ efforts “heroic,” Karen Parker, PhD, an associate professor and associate chair of psychiatry and behavioral sciences at Stanford (Calif.) University, says efficacy trials such as this one are critical. However, Dr. Parker said in an interview, there are a number of questions that the study didn’t address.
The majority of medication dispensed in a standard intranasal device is sprayed into the back of the throat. Regular blood tests confirmed that oxytocin was getting into participants’ system, but, given how quickly oxytocin degrades in the blood, Dr. Parker said it’s hard to know just how much reached the brain.
It’s also unclear whether the results would have been different had the treatment been paired with behavioral therapy, an approach Dr. Parker suggests might benefit a subset of children with ASD.
A 2017 study from Dr. Parker’s lab found that children with ASD whose use of oxytocin at baseline was low derived greater benefit from synthetic oxytocin, something the new study failed to find. Still, Dr. Parker said, it’s possible oxytocin might increase social motivation and increase a child’s receptiveness to behavioral therapy.
“When you see a negative trial like this, it decreases enthusiasm for the therapy for autism in this context,” Dr. Parker said. “I hope people who are studying these syndromes will continue to explore oxytocin as a therapy.”
The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development through the Autism Centers of Excellence Program and the Department of Psychiatry and Behavioral Sciences at Duke University. Full disclosures of the authors’ possible conflicts of interest are available online.
A version of this article first appeared on Medscape.com.
U.S. overdose deaths hit an all-time high
a 28.5% increase from the previous year.
Deaths in some states rose even more precipitously. Vermont saw an almost 70% increase, and drug overdose deaths in West Virginia increased by 62%. Many states, including Alabama, California, Kansas, Kentucky, Louisiana, Tennessee, and Washington, had a 45%-50% rise in overdose deaths.
The data released by the CDC was provisional, as there is generally a lag between a reported overdose and confirmation of the death to the National Vital Statistics System. The agency uses statistical models that render the counts almost 100% accurate, the CDC says.
The vast majority (73,757) of overdose deaths involved opioids – with most of those (62,338) involving synthetic opioids such as fentanyl. Federal officials said that one American died every 5 minutes from an overdose, or 265 a day.
“We have to acknowledge what this is – it is a crisis,” Department of Health & Human Services Secretary Xavier Becerra told reporters on a call.
“As much as the numbers speak so vividly, they don’t tell the whole story. We see it in the faces of grieving families and all those overworked caregivers. You hear it every time you get that panicked 911 phone call, you read it in obituaries of sons and daughters who left us way too soon,” Mr. Becerra said.
Rahul Gupta, MD, director of the White House Office of National Drug Control Policy, said that “this is unacceptable, and it requires an unprecedented response.”
Dr. Gupta, who noted that he has a waiver to treat substance use disorder patients with buprenorphine, said he’s seen “first-hand the heartbreak of the overdose epidemic,” adding that, with 23 years in practice, “I’ve learned that an overdose is a cry for help and for far too many people that cry goes unanswered.”
Both Mr. Becerra and Dr. Gupta called on Congress to pass President Joe Biden’s fiscal 2022 budget request, noting that it calls for $41 billion – a $669 million increase from fiscal year 2021 – to go to agencies working on drug interdiction and substance use prevention, treatment, and recovery support.
Dr. Gupta also announced that the administration was releasing a model law that could be used by state legislatures to help standardize policies on making the overdose antidote naloxone more accessible. Currently, such policies are a patchwork across the nation.
In addition, the federal government is newly supporting harm reduction, Mr. Becerra said. This means federal money can be used by clinics and outreach programs to buy fentanyl test strips, which they can then distribute to drug users.
“It’s important for Americans to have the ability to make sure that they can test for fentanyl in the substance,” Dr. Gupta said.
Fake pills, fentanyl a huge issue
Federal officials said that both fentanyl and methamphetamine are contributing to rising numbers of fatalities.
“Drug cartels in Mexico are mass-producing fentanyl and methamphetamine largely sourced from chemicals in China and they are distributing these substances throughout the United States,” Anne Milgram, administrator of the Drug Enforcement Administration, said on the call.
Ms. Milgram said the agency had seized 12,000 pounds of fentanyl in 2021, enough to provide every American with a lethal dose. Fentanyl is also mixed in with cocaine, heroin, methamphetamine, and marijuana – often in counterfeit pills, Ms. Milgram said.
The DEA and other law enforcement agencies have seized more than 14 million such pills in 2021. “These types of pills are easily accessible today on social media and e-commerce platforms, Ms. Milgram said.
“Drug dealers are now in our homes,” she said. “Wherever there is a smart phone or a computer, a dealer is one click away,” Ms. Milgram said.

National Institute on Drug Abuse Director Nora D. Volkow, MD, said that dealers will continue to push both fentanyl and methamphetamine because they are among the most addictive substances. They also are more profitable because they don’t require cultivation and harvesting, she said on the call.
Dr. Volkow also noted that naloxone is not as effective in reversing fentanyl overdoses because fentanyl is more potent than heroin and other opioids, and “it gets into the brain extremely rapidly.”
Ongoing research is aimed at developing a faster delivery mechanism and a longer-lasting formulation to counter overdoses, Dr. Volkow said.
A version of this article first appeared on Medscape.com.
a 28.5% increase from the previous year.
Deaths in some states rose even more precipitously. Vermont saw an almost 70% increase, and drug overdose deaths in West Virginia increased by 62%. Many states, including Alabama, California, Kansas, Kentucky, Louisiana, Tennessee, and Washington, had a 45%-50% rise in overdose deaths.
The data released by the CDC was provisional, as there is generally a lag between a reported overdose and confirmation of the death to the National Vital Statistics System. The agency uses statistical models that render the counts almost 100% accurate, the CDC says.
The vast majority (73,757) of overdose deaths involved opioids – with most of those (62,338) involving synthetic opioids such as fentanyl. Federal officials said that one American died every 5 minutes from an overdose, or 265 a day.
“We have to acknowledge what this is – it is a crisis,” Department of Health & Human Services Secretary Xavier Becerra told reporters on a call.
“As much as the numbers speak so vividly, they don’t tell the whole story. We see it in the faces of grieving families and all those overworked caregivers. You hear it every time you get that panicked 911 phone call, you read it in obituaries of sons and daughters who left us way too soon,” Mr. Becerra said.
Rahul Gupta, MD, director of the White House Office of National Drug Control Policy, said that “this is unacceptable, and it requires an unprecedented response.”
Dr. Gupta, who noted that he has a waiver to treat substance use disorder patients with buprenorphine, said he’s seen “first-hand the heartbreak of the overdose epidemic,” adding that, with 23 years in practice, “I’ve learned that an overdose is a cry for help and for far too many people that cry goes unanswered.”
Both Mr. Becerra and Dr. Gupta called on Congress to pass President Joe Biden’s fiscal 2022 budget request, noting that it calls for $41 billion – a $669 million increase from fiscal year 2021 – to go to agencies working on drug interdiction and substance use prevention, treatment, and recovery support.
Dr. Gupta also announced that the administration was releasing a model law that could be used by state legislatures to help standardize policies on making the overdose antidote naloxone more accessible. Currently, such policies are a patchwork across the nation.
In addition, the federal government is newly supporting harm reduction, Mr. Becerra said. This means federal money can be used by clinics and outreach programs to buy fentanyl test strips, which they can then distribute to drug users.
“It’s important for Americans to have the ability to make sure that they can test for fentanyl in the substance,” Dr. Gupta said.
Fake pills, fentanyl a huge issue
Federal officials said that both fentanyl and methamphetamine are contributing to rising numbers of fatalities.
“Drug cartels in Mexico are mass-producing fentanyl and methamphetamine largely sourced from chemicals in China and they are distributing these substances throughout the United States,” Anne Milgram, administrator of the Drug Enforcement Administration, said on the call.
Ms. Milgram said the agency had seized 12,000 pounds of fentanyl in 2021, enough to provide every American with a lethal dose. Fentanyl is also mixed in with cocaine, heroin, methamphetamine, and marijuana – often in counterfeit pills, Ms. Milgram said.
The DEA and other law enforcement agencies have seized more than 14 million such pills in 2021. “These types of pills are easily accessible today on social media and e-commerce platforms, Ms. Milgram said.
“Drug dealers are now in our homes,” she said. “Wherever there is a smart phone or a computer, a dealer is one click away,” Ms. Milgram said.
National Institute on Drug Abuse Director Nora D. Volkow, MD, said that dealers will continue to push both fentanyl and methamphetamine because they are among the most addictive substances. They also are more profitable because they don’t require cultivation and harvesting, she said on the call.
Dr. Volkow also noted that naloxone is not as effective in reversing fentanyl overdoses because fentanyl is more potent than heroin and other opioids, and “it gets into the brain extremely rapidly.”
Ongoing research is aimed at developing a faster delivery mechanism and a longer-lasting formulation to counter overdoses, Dr. Volkow said.
A version of this article first appeared on Medscape.com.
a 28.5% increase from the previous year.
Deaths in some states rose even more precipitously. Vermont saw an almost 70% increase, and drug overdose deaths in West Virginia increased by 62%. Many states, including Alabama, California, Kansas, Kentucky, Louisiana, Tennessee, and Washington, had a 45%-50% rise in overdose deaths.
The data released by the CDC was provisional, as there is generally a lag between a reported overdose and confirmation of the death to the National Vital Statistics System. The agency uses statistical models that render the counts almost 100% accurate, the CDC says.
The vast majority (73,757) of overdose deaths involved opioids – with most of those (62,338) involving synthetic opioids such as fentanyl. Federal officials said that one American died every 5 minutes from an overdose, or 265 a day.
“We have to acknowledge what this is – it is a crisis,” Department of Health & Human Services Secretary Xavier Becerra told reporters on a call.
“As much as the numbers speak so vividly, they don’t tell the whole story. We see it in the faces of grieving families and all those overworked caregivers. You hear it every time you get that panicked 911 phone call, you read it in obituaries of sons and daughters who left us way too soon,” Mr. Becerra said.
Rahul Gupta, MD, director of the White House Office of National Drug Control Policy, said that “this is unacceptable, and it requires an unprecedented response.”
Dr. Gupta, who noted that he has a waiver to treat substance use disorder patients with buprenorphine, said he’s seen “first-hand the heartbreak of the overdose epidemic,” adding that, with 23 years in practice, “I’ve learned that an overdose is a cry for help and for far too many people that cry goes unanswered.”
Both Mr. Becerra and Dr. Gupta called on Congress to pass President Joe Biden’s fiscal 2022 budget request, noting that it calls for $41 billion – a $669 million increase from fiscal year 2021 – to go to agencies working on drug interdiction and substance use prevention, treatment, and recovery support.
Dr. Gupta also announced that the administration was releasing a model law that could be used by state legislatures to help standardize policies on making the overdose antidote naloxone more accessible. Currently, such policies are a patchwork across the nation.
In addition, the federal government is newly supporting harm reduction, Mr. Becerra said. This means federal money can be used by clinics and outreach programs to buy fentanyl test strips, which they can then distribute to drug users.
“It’s important for Americans to have the ability to make sure that they can test for fentanyl in the substance,” Dr. Gupta said.
Fake pills, fentanyl a huge issue
Federal officials said that both fentanyl and methamphetamine are contributing to rising numbers of fatalities.
“Drug cartels in Mexico are mass-producing fentanyl and methamphetamine largely sourced from chemicals in China and they are distributing these substances throughout the United States,” Anne Milgram, administrator of the Drug Enforcement Administration, said on the call.
Ms. Milgram said the agency had seized 12,000 pounds of fentanyl in 2021, enough to provide every American with a lethal dose. Fentanyl is also mixed in with cocaine, heroin, methamphetamine, and marijuana – often in counterfeit pills, Ms. Milgram said.
The DEA and other law enforcement agencies have seized more than 14 million such pills in 2021. “These types of pills are easily accessible today on social media and e-commerce platforms, Ms. Milgram said.
“Drug dealers are now in our homes,” she said. “Wherever there is a smart phone or a computer, a dealer is one click away,” Ms. Milgram said.
National Institute on Drug Abuse Director Nora D. Volkow, MD, said that dealers will continue to push both fentanyl and methamphetamine because they are among the most addictive substances. They also are more profitable because they don’t require cultivation and harvesting, she said on the call.
Dr. Volkow also noted that naloxone is not as effective in reversing fentanyl overdoses because fentanyl is more potent than heroin and other opioids, and “it gets into the brain extremely rapidly.”
Ongoing research is aimed at developing a faster delivery mechanism and a longer-lasting formulation to counter overdoses, Dr. Volkow said.
A version of this article first appeared on Medscape.com.
Two-thirds of preschoolers correctly identified emotions of masked adults
Some are concerned about the effects of adults working in preschools wearing face masks on the ability of young children to learn to recognize emotions, study author Juliane Schneider, MD, of University Hospital Lausanne (Switzerland), and colleagues wrote. Previous studies using photographs of faces with digitally added masks have suggested that young children’s emotional recognition was worse with masked faces.
In the study published in JAMA Pediatrics, the researchers tested the impact of masks on the ability of preschool children to identify joy, anger, and sadness. The study included 135 girls and 141 boys aged 36-72 months with a mean age of 52.4 months. The tests were conducted at nine daycare centers.
Children were shown photographs of 15 actors (5 men and 10 women) with and without surgical face masks. The total data set included 90 pictures illustrating joy, anger, and sadness. The children were shown the pictures at random, and they could either name the emotion, point to a card with emoticons showing the three emotions, or respond “I don’t know” or “quit the experiment.” Test sessions lasted approximately 7 minutes per child. Effect sizes were calculated using X2 and Cramer V tests.
Overall, 68.8% of the children correctly identified the emotion portrayed; the correct response rate was 70.6% for faces without face masks and 66.9% for those with face masks. Correct recognition of joy was significantly higher for faces without masks than for those with masks (94.8% vs. 87.3), as was correct recognition of sadness (54.1% vs. 48.9%; P < .001 for both). Recognition of anger was not significantly different for unmasked and masked faces (62.2% vs. 64.6%, P = .10).
No significant differences in correct responses appeared between boys and girls and the rate of correct responses increased significantly with age. The rates of “I don’t know,” and “quit the experiment” responses were 3.1% and 2.2%, respectively. In an analysis of incorrect responses, approximately 25% of the children confused anger and sadness, and 21% misidentified joy for images of anger or sadness.
“Overall, participants in this study, who had been exposed to face masks for nearly a year, recognized emotions on pictures better than has been reported in previous research, even with face masks,” the researchers wrote.
The study findings were limited by several factors including the use of static pictures versus real individuals, which limits generalizability, and the lack of data on children with developmental issues, the researchers noted.
Despite relatively small differences and weak effect size (Cramer V scores of 0.2 or less for all), the results show a stronger recognition of emotion, compared with other studies, and highlight the importance of investigating the impact of face masks on other aspects of child development as the COVID-19 pandemic persists, the researchers concluded.
The study received no outside funding. The researchers had no relevant financial conflicts to disclose.
Some are concerned about the effects of adults working in preschools wearing face masks on the ability of young children to learn to recognize emotions, study author Juliane Schneider, MD, of University Hospital Lausanne (Switzerland), and colleagues wrote. Previous studies using photographs of faces with digitally added masks have suggested that young children’s emotional recognition was worse with masked faces.
In the study published in JAMA Pediatrics, the researchers tested the impact of masks on the ability of preschool children to identify joy, anger, and sadness. The study included 135 girls and 141 boys aged 36-72 months with a mean age of 52.4 months. The tests were conducted at nine daycare centers.
Children were shown photographs of 15 actors (5 men and 10 women) with and without surgical face masks. The total data set included 90 pictures illustrating joy, anger, and sadness. The children were shown the pictures at random, and they could either name the emotion, point to a card with emoticons showing the three emotions, or respond “I don’t know” or “quit the experiment.” Test sessions lasted approximately 7 minutes per child. Effect sizes were calculated using X2 and Cramer V tests.
Overall, 68.8% of the children correctly identified the emotion portrayed; the correct response rate was 70.6% for faces without face masks and 66.9% for those with face masks. Correct recognition of joy was significantly higher for faces without masks than for those with masks (94.8% vs. 87.3), as was correct recognition of sadness (54.1% vs. 48.9%; P < .001 for both). Recognition of anger was not significantly different for unmasked and masked faces (62.2% vs. 64.6%, P = .10).
No significant differences in correct responses appeared between boys and girls and the rate of correct responses increased significantly with age. The rates of “I don’t know,” and “quit the experiment” responses were 3.1% and 2.2%, respectively. In an analysis of incorrect responses, approximately 25% of the children confused anger and sadness, and 21% misidentified joy for images of anger or sadness.
“Overall, participants in this study, who had been exposed to face masks for nearly a year, recognized emotions on pictures better than has been reported in previous research, even with face masks,” the researchers wrote.
The study findings were limited by several factors including the use of static pictures versus real individuals, which limits generalizability, and the lack of data on children with developmental issues, the researchers noted.
Despite relatively small differences and weak effect size (Cramer V scores of 0.2 or less for all), the results show a stronger recognition of emotion, compared with other studies, and highlight the importance of investigating the impact of face masks on other aspects of child development as the COVID-19 pandemic persists, the researchers concluded.
The study received no outside funding. The researchers had no relevant financial conflicts to disclose.
Some are concerned about the effects of adults working in preschools wearing face masks on the ability of young children to learn to recognize emotions, study author Juliane Schneider, MD, of University Hospital Lausanne (Switzerland), and colleagues wrote. Previous studies using photographs of faces with digitally added masks have suggested that young children’s emotional recognition was worse with masked faces.
In the study published in JAMA Pediatrics, the researchers tested the impact of masks on the ability of preschool children to identify joy, anger, and sadness. The study included 135 girls and 141 boys aged 36-72 months with a mean age of 52.4 months. The tests were conducted at nine daycare centers.
Children were shown photographs of 15 actors (5 men and 10 women) with and without surgical face masks. The total data set included 90 pictures illustrating joy, anger, and sadness. The children were shown the pictures at random, and they could either name the emotion, point to a card with emoticons showing the three emotions, or respond “I don’t know” or “quit the experiment.” Test sessions lasted approximately 7 minutes per child. Effect sizes were calculated using X2 and Cramer V tests.
Overall, 68.8% of the children correctly identified the emotion portrayed; the correct response rate was 70.6% for faces without face masks and 66.9% for those with face masks. Correct recognition of joy was significantly higher for faces without masks than for those with masks (94.8% vs. 87.3), as was correct recognition of sadness (54.1% vs. 48.9%; P < .001 for both). Recognition of anger was not significantly different for unmasked and masked faces (62.2% vs. 64.6%, P = .10).
No significant differences in correct responses appeared between boys and girls and the rate of correct responses increased significantly with age. The rates of “I don’t know,” and “quit the experiment” responses were 3.1% and 2.2%, respectively. In an analysis of incorrect responses, approximately 25% of the children confused anger and sadness, and 21% misidentified joy for images of anger or sadness.
“Overall, participants in this study, who had been exposed to face masks for nearly a year, recognized emotions on pictures better than has been reported in previous research, even with face masks,” the researchers wrote.
The study findings were limited by several factors including the use of static pictures versus real individuals, which limits generalizability, and the lack of data on children with developmental issues, the researchers noted.
Despite relatively small differences and weak effect size (Cramer V scores of 0.2 or less for all), the results show a stronger recognition of emotion, compared with other studies, and highlight the importance of investigating the impact of face masks on other aspects of child development as the COVID-19 pandemic persists, the researchers concluded.
The study received no outside funding. The researchers had no relevant financial conflicts to disclose.
FROM JAMA PEDIATRICS
What to do about pandemic PTSD
When the COVID-19 pandemic engulfed the nation well over a year ago, Rebecca Hendrickson, MD, PhD, immersed herself in the shell-shocking revelations that clinicians began posting on social media. The accounts offered just a snapshot of the pandemic’s heavy psychological toll, and Dr. Hendrickson, a psychiatrist at the University of Washington in Seattle and an expert in posttraumatic stress disorder (PTSD), wanted to know more.

She and her colleagues devised a survey to assess the impact of several pandemic-related factors, including increased work hours, social distancing restrictions, and lack of adequate personal protective equipment.
What began as a survey of health care workers soon expanded in scope. Of the more than 600 survey respondents to date, health care workers account for about 60%, while the rest are first responders – police officers, firefighters, paramedics, and emergency medical technicians – and nonclinical personnel, such as security guards and office staff, in health care settings. The respondents range in age from 19 to 72, and hail from all regions of the country.
“Our findings were really striking,” Dr. Hendrickson said, “including very high rates of thoughts of suicide and thoughts of leaving one’s current field, which were both strongly linked to COVID-19–related occupational stress exposure.”
The distress stemmed from a multitude of factors. Among the most demoralizing: witnessing patients die in isolation and being stretched thin to provide optimal care for all patients amid an unrelenting onslaught of COVID-19 cases, she said. For some health care workers, living in the garage or basement – to avoid infecting family members with the virus – also wore on their psyches.
Of all health care workers in the study, more than three-quarters reported symptoms that fell within the clinical range for depression (76%) and anxiety (78%). More than 25% noted that they had lost a family member or close colleague to the virus.
Dr. Hendrickson, who works with military veterans at the VA Puget Sound Hospital System’s Mental Illness Research, Education, and Clinical Center and its PTSD outpatient clinic, hadn’t expected the experience of loss to be so pervasive. She said the sheer number of people who “crossed the threshold” into despair concerned her deeply.
Signs and symptoms of PTSD
PTSD’s prevalence among health care workers has always been variable, said Jessica Gold, MD, assistant professor and director of wellness, engagement, and outreach in the department of psychiatry at Washington University in St. Louis.

As a psychiatrist who sees health care workers in her clinical practice, Dr. Gold has noted poor baseline mental health, including depression and trauma. Significant data have pointed to a relatively higher suicide rate among physicians than among the general population. These problems have been compounded by COVID-19.
“It has been an unrelenting series of new stressors,” she said, citing lack of resources; a feeling of being unable to help; and the high frequency of risk of death to patients, family and friends, and the caregivers themselves as just as few examples. “It is very likely going to increase our baseline trauma, and honestly, I don’t know that we can predict how. To me, ”
PTSD can manifest itself in health care workers in several different ways. A few commonalities Dr. Gold has observed are sleep disruption (including insomnia and nightmares), work avoidance by taking disability or quitting, irritability or other changes in mood, trouble concentrating, and hypervigilance.
She said she has seen physical manifestations of trauma – such as body pain, stomachaches, and teeth grinding, which “you might not realize are at all related to trauma but ultimately are.” Sometimes, she added, “people have panic attacks on the way to work or right when they get to work, or are thinking about work.”
Dr. Gold noted that different types of treatment, such as cognitive-behavioral therapy and eye movement desensitization and reprocessing (EMDR), can be effective for PTSD. Medication is often necessary because of comorbid anxiety, depression, or eating disorders, said Dr. Gold, who is conducting a study on the pandemic’s effects on medical students.
The difficulties in isolating COVID-19 as a contributor
Not all researchers are convinced that a causal relationship has been established between the pandemic and worsening mental health among those in the health care sector.
With provider burnout being a long-standing concern in medicine, Ankur A. Butala, MD, assistant professor of neurology, psychiatry, and behavioral sciences at the Johns Hopkins University, Baltimore, said he remains a bit skeptical that acute stressors during the pandemic amounted to a uniquely potent driving force that can be extrapolated and quantified in a study.
“It’s hard to interpret a chronic, rolling, ongoing trauma like COVID-19 against tools or scales developed to investigate symptoms from a singular and acute trauma, like a school shooting or a [military] firefight,” Dr. Butala said.
In addition, he noted a reluctance to generalizing results from a study in which participants were recruited via social media as opposed to research methods involving more rigorous selection protocols.
Although Dr. Hendrickson acknowledged the study’s limitations, she said her team nonetheless found strong correlations between COVID-19-related stressors and self-reported struggles in completing work-related tasks, as well as increasing thoughts of leaving one’s current field. They adjusted for previous lifetime trauma exposure, age, gender, and a personal history of contracting COVID-19.
The underlying premise of the study could be confirmed with repeated surveys over time, Dr. Butala said, as the COVID-19 pandemic evolves and the vaccination effort unfolds.
Follow-up surveys are being sent to participants every 2 weeks and every 3 months to gauge their mood, for a total follow-up period of 9 months per individual. New participants are still welcome. “We will continue to enroll as long as it seems relevant,” Dr. Hendrickson said.
Carol S. North, MD, MPE, who has added to the growing research on the pandemic’s toll on mental health, noted that because symptom scales do not provide psychiatric diagnoses, it is difficult to attribute the prevalence of psychiatric disorders to the pandemic. Dr. North is chair and professor of crisis psychiatry at UT Southwestern Medical Center in Dallas, and director of the program in trauma and disaster at VA North Texas Health Care System.
The DSM-5 criteria exclude naturally occurring illness, such as a virus (even during a pandemic) as a qualifying trauma for the diagnosis of PTSD. According to current criteria by the American Psychiatric Association, COVID-19 and the pandemic are not defined as trauma, Dr. North said, while noting that “just because it’s not trauma or PTSD does not mean that the pandemic should be discounted as not stressful; people are finding it very stressful.”
Identifying the exact source of distress would still be difficult, Dr. North said, as the pandemic has produced severe economic consequences and prolonged social isolation, as well as occurring alongside nationwide protests over racial and ethnic divisions. Studies to date haven’t effectively separated out for these stressors, making it impossible to weigh their relative impact.
Furthermore, “most of us face many other stressors in our daily lives, such as grief, losses, broken relationships, and personal failures,” she said. “All of these may contribute to psychological distress, and research is needed to determine how much was a product of the virus, other aspects of the pandemic, or unrelated life stressors.”
A rallying cry for new interventions
Despite such doubts, a growing number of studies are reporting that health care workers and first responders are experiencing intensified PTSD, depression, anxiety, and insomnia as a result of the pandemic, said Hrayr Pierre Attarian, MD, professor of neurology at Northwestern University, Chicago. These results should act as a rallying cry for implementing more policies tailored to prevent burnout, he said.
“What we are seeing during this terrible pandemic is burnout on steroids,” said Dr. Attarian, medical director of Northwestern’s Center for Sleep Disorders. There are already high burnout rates, “so this should be doubly important.”
Rooting out this problem starts at the institutional level, but merely advising providers to “be well” wouldn’t make inroads. “There needs to be fluid dialogue between health care workers and the leadership,” he said.
Among his proposed remedies: Access to confidential and free mental health resources, increased administrative support, flexible hours, respect for work-life balance, and forgiveness for occasional errors that don’t result in harm.
“Sometimes even the perception that a mistake has been made is taken as proof of guilt,” Dr. Attarian said. “It is not conducive to wellness. Extra income does not replace a nurturing work environment.”
Furthermore, “as a profession, we must stop glorifying ‘overwork.’ We must stop wearing ‘lack of sleep’ as badge of honor,” he said. “Sleep is a biological imperative like self-preservation, hunger, and thirst. When we don’t sleep anxiety, pain, and depression get amplified. Our perception of distress is off, as is our judgment.”
The Federation of State Physician Health Programs provides a directory that physicians can use for referrals to confidential consultation or treatment.
Christopher Bundy, MD, MPH, executive medical director of Washington Physicians Health Program in Seattle, has been following Dr. Hendrickson’s longitudinal study with keen interest. As president of the Federation of State Physician Health Programs, he hopes to translate the findings into practice.
“Obviously, the COVID-19 pandemic has been a ‘black swan’ in terms of workforce sustainability issues,” Dr. Bundy said, citing “high rates of burnout, disillusionment, and dissatisfaction.” He sees some similarities with his former role in treating war veterans.
“The invisible wounds of combat, the psychological scars don’t really become apparent until after you’re out of the war zone,” said Dr. Bundy, clinical associate professor of psychiatry at the University of Washington.
Likewise, he expects the “emotional chickens will come home to roost as the pandemic subsides.” Until then, “people are just focused on survival, and in doing their jobs and protecting their patients.” Eventually, “their own wounds inside the pandemic will take hold.”
A version of this article first appeared on Medscape.com.
When the COVID-19 pandemic engulfed the nation well over a year ago, Rebecca Hendrickson, MD, PhD, immersed herself in the shell-shocking revelations that clinicians began posting on social media. The accounts offered just a snapshot of the pandemic’s heavy psychological toll, and Dr. Hendrickson, a psychiatrist at the University of Washington in Seattle and an expert in posttraumatic stress disorder (PTSD), wanted to know more.
She and her colleagues devised a survey to assess the impact of several pandemic-related factors, including increased work hours, social distancing restrictions, and lack of adequate personal protective equipment.
What began as a survey of health care workers soon expanded in scope. Of the more than 600 survey respondents to date, health care workers account for about 60%, while the rest are first responders – police officers, firefighters, paramedics, and emergency medical technicians – and nonclinical personnel, such as security guards and office staff, in health care settings. The respondents range in age from 19 to 72, and hail from all regions of the country.
“Our findings were really striking,” Dr. Hendrickson said, “including very high rates of thoughts of suicide and thoughts of leaving one’s current field, which were both strongly linked to COVID-19–related occupational stress exposure.”
The distress stemmed from a multitude of factors. Among the most demoralizing: witnessing patients die in isolation and being stretched thin to provide optimal care for all patients amid an unrelenting onslaught of COVID-19 cases, she said. For some health care workers, living in the garage or basement – to avoid infecting family members with the virus – also wore on their psyches.
Of all health care workers in the study, more than three-quarters reported symptoms that fell within the clinical range for depression (76%) and anxiety (78%). More than 25% noted that they had lost a family member or close colleague to the virus.
Dr. Hendrickson, who works with military veterans at the VA Puget Sound Hospital System’s Mental Illness Research, Education, and Clinical Center and its PTSD outpatient clinic, hadn’t expected the experience of loss to be so pervasive. She said the sheer number of people who “crossed the threshold” into despair concerned her deeply.
Signs and symptoms of PTSD
PTSD’s prevalence among health care workers has always been variable, said Jessica Gold, MD, assistant professor and director of wellness, engagement, and outreach in the department of psychiatry at Washington University in St. Louis.
As a psychiatrist who sees health care workers in her clinical practice, Dr. Gold has noted poor baseline mental health, including depression and trauma. Significant data have pointed to a relatively higher suicide rate among physicians than among the general population. These problems have been compounded by COVID-19.
“It has been an unrelenting series of new stressors,” she said, citing lack of resources; a feeling of being unable to help; and the high frequency of risk of death to patients, family and friends, and the caregivers themselves as just as few examples. “It is very likely going to increase our baseline trauma, and honestly, I don’t know that we can predict how. To me, ”
PTSD can manifest itself in health care workers in several different ways. A few commonalities Dr. Gold has observed are sleep disruption (including insomnia and nightmares), work avoidance by taking disability or quitting, irritability or other changes in mood, trouble concentrating, and hypervigilance.
She said she has seen physical manifestations of trauma – such as body pain, stomachaches, and teeth grinding, which “you might not realize are at all related to trauma but ultimately are.” Sometimes, she added, “people have panic attacks on the way to work or right when they get to work, or are thinking about work.”
Dr. Gold noted that different types of treatment, such as cognitive-behavioral therapy and eye movement desensitization and reprocessing (EMDR), can be effective for PTSD. Medication is often necessary because of comorbid anxiety, depression, or eating disorders, said Dr. Gold, who is conducting a study on the pandemic’s effects on medical students.
The difficulties in isolating COVID-19 as a contributor
Not all researchers are convinced that a causal relationship has been established between the pandemic and worsening mental health among those in the health care sector.
With provider burnout being a long-standing concern in medicine, Ankur A. Butala, MD, assistant professor of neurology, psychiatry, and behavioral sciences at the Johns Hopkins University, Baltimore, said he remains a bit skeptical that acute stressors during the pandemic amounted to a uniquely potent driving force that can be extrapolated and quantified in a study.
“It’s hard to interpret a chronic, rolling, ongoing trauma like COVID-19 against tools or scales developed to investigate symptoms from a singular and acute trauma, like a school shooting or a [military] firefight,” Dr. Butala said.
In addition, he noted a reluctance to generalizing results from a study in which participants were recruited via social media as opposed to research methods involving more rigorous selection protocols.
Although Dr. Hendrickson acknowledged the study’s limitations, she said her team nonetheless found strong correlations between COVID-19-related stressors and self-reported struggles in completing work-related tasks, as well as increasing thoughts of leaving one’s current field. They adjusted for previous lifetime trauma exposure, age, gender, and a personal history of contracting COVID-19.
The underlying premise of the study could be confirmed with repeated surveys over time, Dr. Butala said, as the COVID-19 pandemic evolves and the vaccination effort unfolds.
Follow-up surveys are being sent to participants every 2 weeks and every 3 months to gauge their mood, for a total follow-up period of 9 months per individual. New participants are still welcome. “We will continue to enroll as long as it seems relevant,” Dr. Hendrickson said.
Carol S. North, MD, MPE, who has added to the growing research on the pandemic’s toll on mental health, noted that because symptom scales do not provide psychiatric diagnoses, it is difficult to attribute the prevalence of psychiatric disorders to the pandemic. Dr. North is chair and professor of crisis psychiatry at UT Southwestern Medical Center in Dallas, and director of the program in trauma and disaster at VA North Texas Health Care System.
The DSM-5 criteria exclude naturally occurring illness, such as a virus (even during a pandemic) as a qualifying trauma for the diagnosis of PTSD. According to current criteria by the American Psychiatric Association, COVID-19 and the pandemic are not defined as trauma, Dr. North said, while noting that “just because it’s not trauma or PTSD does not mean that the pandemic should be discounted as not stressful; people are finding it very stressful.”
Identifying the exact source of distress would still be difficult, Dr. North said, as the pandemic has produced severe economic consequences and prolonged social isolation, as well as occurring alongside nationwide protests over racial and ethnic divisions. Studies to date haven’t effectively separated out for these stressors, making it impossible to weigh their relative impact.
Furthermore, “most of us face many other stressors in our daily lives, such as grief, losses, broken relationships, and personal failures,” she said. “All of these may contribute to psychological distress, and research is needed to determine how much was a product of the virus, other aspects of the pandemic, or unrelated life stressors.”
A rallying cry for new interventions
Despite such doubts, a growing number of studies are reporting that health care workers and first responders are experiencing intensified PTSD, depression, anxiety, and insomnia as a result of the pandemic, said Hrayr Pierre Attarian, MD, professor of neurology at Northwestern University, Chicago. These results should act as a rallying cry for implementing more policies tailored to prevent burnout, he said.
“What we are seeing during this terrible pandemic is burnout on steroids,” said Dr. Attarian, medical director of Northwestern’s Center for Sleep Disorders. There are already high burnout rates, “so this should be doubly important.”
Rooting out this problem starts at the institutional level, but merely advising providers to “be well” wouldn’t make inroads. “There needs to be fluid dialogue between health care workers and the leadership,” he said.
Among his proposed remedies: Access to confidential and free mental health resources, increased administrative support, flexible hours, respect for work-life balance, and forgiveness for occasional errors that don’t result in harm.
“Sometimes even the perception that a mistake has been made is taken as proof of guilt,” Dr. Attarian said. “It is not conducive to wellness. Extra income does not replace a nurturing work environment.”
Furthermore, “as a profession, we must stop glorifying ‘overwork.’ We must stop wearing ‘lack of sleep’ as badge of honor,” he said. “Sleep is a biological imperative like self-preservation, hunger, and thirst. When we don’t sleep anxiety, pain, and depression get amplified. Our perception of distress is off, as is our judgment.”
The Federation of State Physician Health Programs provides a directory that physicians can use for referrals to confidential consultation or treatment.
Christopher Bundy, MD, MPH, executive medical director of Washington Physicians Health Program in Seattle, has been following Dr. Hendrickson’s longitudinal study with keen interest. As president of the Federation of State Physician Health Programs, he hopes to translate the findings into practice.
“Obviously, the COVID-19 pandemic has been a ‘black swan’ in terms of workforce sustainability issues,” Dr. Bundy said, citing “high rates of burnout, disillusionment, and dissatisfaction.” He sees some similarities with his former role in treating war veterans.
“The invisible wounds of combat, the psychological scars don’t really become apparent until after you’re out of the war zone,” said Dr. Bundy, clinical associate professor of psychiatry at the University of Washington.
Likewise, he expects the “emotional chickens will come home to roost as the pandemic subsides.” Until then, “people are just focused on survival, and in doing their jobs and protecting their patients.” Eventually, “their own wounds inside the pandemic will take hold.”
A version of this article first appeared on Medscape.com.
When the COVID-19 pandemic engulfed the nation well over a year ago, Rebecca Hendrickson, MD, PhD, immersed herself in the shell-shocking revelations that clinicians began posting on social media. The accounts offered just a snapshot of the pandemic’s heavy psychological toll, and Dr. Hendrickson, a psychiatrist at the University of Washington in Seattle and an expert in posttraumatic stress disorder (PTSD), wanted to know more.
She and her colleagues devised a survey to assess the impact of several pandemic-related factors, including increased work hours, social distancing restrictions, and lack of adequate personal protective equipment.
What began as a survey of health care workers soon expanded in scope. Of the more than 600 survey respondents to date, health care workers account for about 60%, while the rest are first responders – police officers, firefighters, paramedics, and emergency medical technicians – and nonclinical personnel, such as security guards and office staff, in health care settings. The respondents range in age from 19 to 72, and hail from all regions of the country.
“Our findings were really striking,” Dr. Hendrickson said, “including very high rates of thoughts of suicide and thoughts of leaving one’s current field, which were both strongly linked to COVID-19–related occupational stress exposure.”
The distress stemmed from a multitude of factors. Among the most demoralizing: witnessing patients die in isolation and being stretched thin to provide optimal care for all patients amid an unrelenting onslaught of COVID-19 cases, she said. For some health care workers, living in the garage or basement – to avoid infecting family members with the virus – also wore on their psyches.
Of all health care workers in the study, more than three-quarters reported symptoms that fell within the clinical range for depression (76%) and anxiety (78%). More than 25% noted that they had lost a family member or close colleague to the virus.
Dr. Hendrickson, who works with military veterans at the VA Puget Sound Hospital System’s Mental Illness Research, Education, and Clinical Center and its PTSD outpatient clinic, hadn’t expected the experience of loss to be so pervasive. She said the sheer number of people who “crossed the threshold” into despair concerned her deeply.
Signs and symptoms of PTSD
PTSD’s prevalence among health care workers has always been variable, said Jessica Gold, MD, assistant professor and director of wellness, engagement, and outreach in the department of psychiatry at Washington University in St. Louis.
As a psychiatrist who sees health care workers in her clinical practice, Dr. Gold has noted poor baseline mental health, including depression and trauma. Significant data have pointed to a relatively higher suicide rate among physicians than among the general population. These problems have been compounded by COVID-19.
“It has been an unrelenting series of new stressors,” she said, citing lack of resources; a feeling of being unable to help; and the high frequency of risk of death to patients, family and friends, and the caregivers themselves as just as few examples. “It is very likely going to increase our baseline trauma, and honestly, I don’t know that we can predict how. To me, ”
PTSD can manifest itself in health care workers in several different ways. A few commonalities Dr. Gold has observed are sleep disruption (including insomnia and nightmares), work avoidance by taking disability or quitting, irritability or other changes in mood, trouble concentrating, and hypervigilance.
She said she has seen physical manifestations of trauma – such as body pain, stomachaches, and teeth grinding, which “you might not realize are at all related to trauma but ultimately are.” Sometimes, she added, “people have panic attacks on the way to work or right when they get to work, or are thinking about work.”
Dr. Gold noted that different types of treatment, such as cognitive-behavioral therapy and eye movement desensitization and reprocessing (EMDR), can be effective for PTSD. Medication is often necessary because of comorbid anxiety, depression, or eating disorders, said Dr. Gold, who is conducting a study on the pandemic’s effects on medical students.
The difficulties in isolating COVID-19 as a contributor
Not all researchers are convinced that a causal relationship has been established between the pandemic and worsening mental health among those in the health care sector.
With provider burnout being a long-standing concern in medicine, Ankur A. Butala, MD, assistant professor of neurology, psychiatry, and behavioral sciences at the Johns Hopkins University, Baltimore, said he remains a bit skeptical that acute stressors during the pandemic amounted to a uniquely potent driving force that can be extrapolated and quantified in a study.
“It’s hard to interpret a chronic, rolling, ongoing trauma like COVID-19 against tools or scales developed to investigate symptoms from a singular and acute trauma, like a school shooting or a [military] firefight,” Dr. Butala said.
In addition, he noted a reluctance to generalizing results from a study in which participants were recruited via social media as opposed to research methods involving more rigorous selection protocols.
Although Dr. Hendrickson acknowledged the study’s limitations, she said her team nonetheless found strong correlations between COVID-19-related stressors and self-reported struggles in completing work-related tasks, as well as increasing thoughts of leaving one’s current field. They adjusted for previous lifetime trauma exposure, age, gender, and a personal history of contracting COVID-19.
The underlying premise of the study could be confirmed with repeated surveys over time, Dr. Butala said, as the COVID-19 pandemic evolves and the vaccination effort unfolds.
Follow-up surveys are being sent to participants every 2 weeks and every 3 months to gauge their mood, for a total follow-up period of 9 months per individual. New participants are still welcome. “We will continue to enroll as long as it seems relevant,” Dr. Hendrickson said.
Carol S. North, MD, MPE, who has added to the growing research on the pandemic’s toll on mental health, noted that because symptom scales do not provide psychiatric diagnoses, it is difficult to attribute the prevalence of psychiatric disorders to the pandemic. Dr. North is chair and professor of crisis psychiatry at UT Southwestern Medical Center in Dallas, and director of the program in trauma and disaster at VA North Texas Health Care System.
The DSM-5 criteria exclude naturally occurring illness, such as a virus (even during a pandemic) as a qualifying trauma for the diagnosis of PTSD. According to current criteria by the American Psychiatric Association, COVID-19 and the pandemic are not defined as trauma, Dr. North said, while noting that “just because it’s not trauma or PTSD does not mean that the pandemic should be discounted as not stressful; people are finding it very stressful.”
Identifying the exact source of distress would still be difficult, Dr. North said, as the pandemic has produced severe economic consequences and prolonged social isolation, as well as occurring alongside nationwide protests over racial and ethnic divisions. Studies to date haven’t effectively separated out for these stressors, making it impossible to weigh their relative impact.
Furthermore, “most of us face many other stressors in our daily lives, such as grief, losses, broken relationships, and personal failures,” she said. “All of these may contribute to psychological distress, and research is needed to determine how much was a product of the virus, other aspects of the pandemic, or unrelated life stressors.”
A rallying cry for new interventions
Despite such doubts, a growing number of studies are reporting that health care workers and first responders are experiencing intensified PTSD, depression, anxiety, and insomnia as a result of the pandemic, said Hrayr Pierre Attarian, MD, professor of neurology at Northwestern University, Chicago. These results should act as a rallying cry for implementing more policies tailored to prevent burnout, he said.
“What we are seeing during this terrible pandemic is burnout on steroids,” said Dr. Attarian, medical director of Northwestern’s Center for Sleep Disorders. There are already high burnout rates, “so this should be doubly important.”
Rooting out this problem starts at the institutional level, but merely advising providers to “be well” wouldn’t make inroads. “There needs to be fluid dialogue between health care workers and the leadership,” he said.
Among his proposed remedies: Access to confidential and free mental health resources, increased administrative support, flexible hours, respect for work-life balance, and forgiveness for occasional errors that don’t result in harm.
“Sometimes even the perception that a mistake has been made is taken as proof of guilt,” Dr. Attarian said. “It is not conducive to wellness. Extra income does not replace a nurturing work environment.”
Furthermore, “as a profession, we must stop glorifying ‘overwork.’ We must stop wearing ‘lack of sleep’ as badge of honor,” he said. “Sleep is a biological imperative like self-preservation, hunger, and thirst. When we don’t sleep anxiety, pain, and depression get amplified. Our perception of distress is off, as is our judgment.”
The Federation of State Physician Health Programs provides a directory that physicians can use for referrals to confidential consultation or treatment.
Christopher Bundy, MD, MPH, executive medical director of Washington Physicians Health Program in Seattle, has been following Dr. Hendrickson’s longitudinal study with keen interest. As president of the Federation of State Physician Health Programs, he hopes to translate the findings into practice.
“Obviously, the COVID-19 pandemic has been a ‘black swan’ in terms of workforce sustainability issues,” Dr. Bundy said, citing “high rates of burnout, disillusionment, and dissatisfaction.” He sees some similarities with his former role in treating war veterans.
“The invisible wounds of combat, the psychological scars don’t really become apparent until after you’re out of the war zone,” said Dr. Bundy, clinical associate professor of psychiatry at the University of Washington.
Likewise, he expects the “emotional chickens will come home to roost as the pandemic subsides.” Until then, “people are just focused on survival, and in doing their jobs and protecting their patients.” Eventually, “their own wounds inside the pandemic will take hold.”
A version of this article first appeared on Medscape.com.
Single infusion of ketamine rapidly reduces suicidal thoughts
A single infusion of ketamine rapidly improves distorted thinking and reasoning to reduce suicidal thoughts, independent of the drug’s effect on severe depression, new research shows.

“Previously it was shown that ketamine rapidly improved depression and that explained part of the rapid improvement in suicidal ideation,” senior author J. John Mann, MD, with Columbia University, New York, said in an interview.
“What was unclear was what else changed that could decrease suicidal ideation and the risk for suicidal behavior. This study identifies a second new domain of improvement – namely rapid improvement in several cognitive functions that can potentially reduce suicide risk,” said Dr. Mann.
The study was published online Nov. 2, 2021, in the Journal of Clinical Psychiatry.
Boosts cognitive function
A total of 78 adults with major depressive disorder and clinically significant suicidal ideation underwent neuropsychological testing before, and 1 day after, double-blind treatment with a single intravenous infusion of ketamine or midazolam.
“Ketamine produced rapid improvement in suicidal ideation and mood” compared with midazolam, the authors reported.
Ketamine was linked to specific improvement in reaction time and cognitive control/interference processing – a measure that has been associated with previous suicide attempt in depression.
A subgroup of patients whose suicidal ideation did not remit on midazolam were later treated with unblinded ketamine and retested. In these individuals, reaction time and cognitive control/interference processing also improved relative to preketamine assessments.
Neurocognitive improvement, however, was not correlated with changes in depression, suicidal thinking, or general mood, the researchers noted.
Nonetheless, they say ketamine had a “positive therapeutic effect” on neurocognition 1 day after treatment on at least one measure associated with suicidal behavior in the context of depression.
The results suggest “additional independent therapeutic effects for ketamine in the treatment of depressed patients at risk for suicidal behavior,” they wrote.
“Ketamine modulates many neurotransmitter systems including glutamate transmission which is crucial for learning and memory. It increases the number of synapses or connections between neurons. These effects are fundamental to cognition and are logical explanations of the beneficial effects observed in this study,” Dr. Mann said in an interview.
“Our study helped us gain a better understanding of how ketamine works in the brain and how quickly it can improve distorted thinking. study investigator Ravi. N. Shah, MD, chief innovation officer, Columbia Psychiatry, said in a news release.
Important research with caveats
In a comment, James Murrough, MD, PhD, director of the Depression and Anxiety Center for Discovery and Treatment at Mount Sinai in New York, said the study is important and “adds to a growing understanding of how ketamine affects brain systems and thinking in the context of depression and suicide risk.”
“One reason this study is significant is that prior studies have shown that ketamine can have harmful effects on cognitive functioning in the context of ketamine misuse and exposures to high doses for long periods of time,” Dr. Murrough, who wasn’t involved in the study, said in an interview.
“In contrast in this study, a single low-dose treatment of ketamine can have the opposite effects, actually boosting some markers of cognitive functioning, at least in the short-term,” he noted.
Dr. Murrough said one caveat to the study is that it only examined the effect of ketamine on cognition once, 1 day after a single treatment.
“While this is an important initial observation, we don’t yet have any understanding of how persistent this effect on cognition is, or how this observed change may be related to any benefit ketamine may have on depression or suicide risk,” Dr. Murrough said.
“In fact, the researchers found that there was no association between change in cognitive functioning following ketamine and change in depression or suicidal thinking. The patients who showed improved cognitive function following ketamine did not differ in terms of mood or suicide risk compared to patients who did not show an improvement in cognition,” Dr. Murrough noted.
“This raises the important question of what is the relevance of change in cognition to the potential benefits of ketamine. This is an important area and should be the focus of future research in order to improve outcomes for patients with depression and who are at risk for suicide,” he added.

Also weighing in, Roger S. McIntyre, MD, professor of psychiatry and pharmacology and head of the mood disorders psychopharmacology unit, University of Toronto, said the study is “very interesting and in keeping” with some previous work that he and his colleagues have done showing that ketamine “seems to benefit aspects of cognition which is a core element in depression.”
“It’s a testable hypothesis that the improvement in cognition now being reported and replicated could play some role in the improved quality of life and functioning with this treatment and as well reduce reducing suicide,” said Dr. McIntyre.
This study was supported by the National Institute of Mental Health. Dr. Mann receives royalties for commercial use of the Columbia-Suicide Severity Rating Scale, which was not used in this study. Dr. Murrough’s institution was involved in research involving esketamine (Spravato) for treatment-resistant depression and receives financial remuneration from the manufacturer of esketamine. Dr. McIntyre has received research grant support from the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation and speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, Eisai, Minerva, Intra-Cellular, and AbbVie. Dr. McIntyre is also CEO of AltMed.
A version of this article first appeared on Medscape.com.
A single infusion of ketamine rapidly improves distorted thinking and reasoning to reduce suicidal thoughts, independent of the drug’s effect on severe depression, new research shows.
“Previously it was shown that ketamine rapidly improved depression and that explained part of the rapid improvement in suicidal ideation,” senior author J. John Mann, MD, with Columbia University, New York, said in an interview.
“What was unclear was what else changed that could decrease suicidal ideation and the risk for suicidal behavior. This study identifies a second new domain of improvement – namely rapid improvement in several cognitive functions that can potentially reduce suicide risk,” said Dr. Mann.
The study was published online Nov. 2, 2021, in the Journal of Clinical Psychiatry.
Boosts cognitive function
A total of 78 adults with major depressive disorder and clinically significant suicidal ideation underwent neuropsychological testing before, and 1 day after, double-blind treatment with a single intravenous infusion of ketamine or midazolam.
“Ketamine produced rapid improvement in suicidal ideation and mood” compared with midazolam, the authors reported.
Ketamine was linked to specific improvement in reaction time and cognitive control/interference processing – a measure that has been associated with previous suicide attempt in depression.
A subgroup of patients whose suicidal ideation did not remit on midazolam were later treated with unblinded ketamine and retested. In these individuals, reaction time and cognitive control/interference processing also improved relative to preketamine assessments.
Neurocognitive improvement, however, was not correlated with changes in depression, suicidal thinking, or general mood, the researchers noted.
Nonetheless, they say ketamine had a “positive therapeutic effect” on neurocognition 1 day after treatment on at least one measure associated with suicidal behavior in the context of depression.
The results suggest “additional independent therapeutic effects for ketamine in the treatment of depressed patients at risk for suicidal behavior,” they wrote.
“Ketamine modulates many neurotransmitter systems including glutamate transmission which is crucial for learning and memory. It increases the number of synapses or connections between neurons. These effects are fundamental to cognition and are logical explanations of the beneficial effects observed in this study,” Dr. Mann said in an interview.
“Our study helped us gain a better understanding of how ketamine works in the brain and how quickly it can improve distorted thinking. study investigator Ravi. N. Shah, MD, chief innovation officer, Columbia Psychiatry, said in a news release.
Important research with caveats
In a comment, James Murrough, MD, PhD, director of the Depression and Anxiety Center for Discovery and Treatment at Mount Sinai in New York, said the study is important and “adds to a growing understanding of how ketamine affects brain systems and thinking in the context of depression and suicide risk.”
“One reason this study is significant is that prior studies have shown that ketamine can have harmful effects on cognitive functioning in the context of ketamine misuse and exposures to high doses for long periods of time,” Dr. Murrough, who wasn’t involved in the study, said in an interview.
“In contrast in this study, a single low-dose treatment of ketamine can have the opposite effects, actually boosting some markers of cognitive functioning, at least in the short-term,” he noted.
Dr. Murrough said one caveat to the study is that it only examined the effect of ketamine on cognition once, 1 day after a single treatment.
“While this is an important initial observation, we don’t yet have any understanding of how persistent this effect on cognition is, or how this observed change may be related to any benefit ketamine may have on depression or suicide risk,” Dr. Murrough said.
“In fact, the researchers found that there was no association between change in cognitive functioning following ketamine and change in depression or suicidal thinking. The patients who showed improved cognitive function following ketamine did not differ in terms of mood or suicide risk compared to patients who did not show an improvement in cognition,” Dr. Murrough noted.
“This raises the important question of what is the relevance of change in cognition to the potential benefits of ketamine. This is an important area and should be the focus of future research in order to improve outcomes for patients with depression and who are at risk for suicide,” he added.
Also weighing in, Roger S. McIntyre, MD, professor of psychiatry and pharmacology and head of the mood disorders psychopharmacology unit, University of Toronto, said the study is “very interesting and in keeping” with some previous work that he and his colleagues have done showing that ketamine “seems to benefit aspects of cognition which is a core element in depression.”
“It’s a testable hypothesis that the improvement in cognition now being reported and replicated could play some role in the improved quality of life and functioning with this treatment and as well reduce reducing suicide,” said Dr. McIntyre.
This study was supported by the National Institute of Mental Health. Dr. Mann receives royalties for commercial use of the Columbia-Suicide Severity Rating Scale, which was not used in this study. Dr. Murrough’s institution was involved in research involving esketamine (Spravato) for treatment-resistant depression and receives financial remuneration from the manufacturer of esketamine. Dr. McIntyre has received research grant support from the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation and speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, Eisai, Minerva, Intra-Cellular, and AbbVie. Dr. McIntyre is also CEO of AltMed.
A version of this article first appeared on Medscape.com.
A single infusion of ketamine rapidly improves distorted thinking and reasoning to reduce suicidal thoughts, independent of the drug’s effect on severe depression, new research shows.
“Previously it was shown that ketamine rapidly improved depression and that explained part of the rapid improvement in suicidal ideation,” senior author J. John Mann, MD, with Columbia University, New York, said in an interview.
“What was unclear was what else changed that could decrease suicidal ideation and the risk for suicidal behavior. This study identifies a second new domain of improvement – namely rapid improvement in several cognitive functions that can potentially reduce suicide risk,” said Dr. Mann.
The study was published online Nov. 2, 2021, in the Journal of Clinical Psychiatry.
Boosts cognitive function
A total of 78 adults with major depressive disorder and clinically significant suicidal ideation underwent neuropsychological testing before, and 1 day after, double-blind treatment with a single intravenous infusion of ketamine or midazolam.
“Ketamine produced rapid improvement in suicidal ideation and mood” compared with midazolam, the authors reported.
Ketamine was linked to specific improvement in reaction time and cognitive control/interference processing – a measure that has been associated with previous suicide attempt in depression.
A subgroup of patients whose suicidal ideation did not remit on midazolam were later treated with unblinded ketamine and retested. In these individuals, reaction time and cognitive control/interference processing also improved relative to preketamine assessments.
Neurocognitive improvement, however, was not correlated with changes in depression, suicidal thinking, or general mood, the researchers noted.
Nonetheless, they say ketamine had a “positive therapeutic effect” on neurocognition 1 day after treatment on at least one measure associated with suicidal behavior in the context of depression.
The results suggest “additional independent therapeutic effects for ketamine in the treatment of depressed patients at risk for suicidal behavior,” they wrote.
“Ketamine modulates many neurotransmitter systems including glutamate transmission which is crucial for learning and memory. It increases the number of synapses or connections between neurons. These effects are fundamental to cognition and are logical explanations of the beneficial effects observed in this study,” Dr. Mann said in an interview.
“Our study helped us gain a better understanding of how ketamine works in the brain and how quickly it can improve distorted thinking. study investigator Ravi. N. Shah, MD, chief innovation officer, Columbia Psychiatry, said in a news release.
Important research with caveats
In a comment, James Murrough, MD, PhD, director of the Depression and Anxiety Center for Discovery and Treatment at Mount Sinai in New York, said the study is important and “adds to a growing understanding of how ketamine affects brain systems and thinking in the context of depression and suicide risk.”
“One reason this study is significant is that prior studies have shown that ketamine can have harmful effects on cognitive functioning in the context of ketamine misuse and exposures to high doses for long periods of time,” Dr. Murrough, who wasn’t involved in the study, said in an interview.
“In contrast in this study, a single low-dose treatment of ketamine can have the opposite effects, actually boosting some markers of cognitive functioning, at least in the short-term,” he noted.
Dr. Murrough said one caveat to the study is that it only examined the effect of ketamine on cognition once, 1 day after a single treatment.
“While this is an important initial observation, we don’t yet have any understanding of how persistent this effect on cognition is, or how this observed change may be related to any benefit ketamine may have on depression or suicide risk,” Dr. Murrough said.
“In fact, the researchers found that there was no association between change in cognitive functioning following ketamine and change in depression or suicidal thinking. The patients who showed improved cognitive function following ketamine did not differ in terms of mood or suicide risk compared to patients who did not show an improvement in cognition,” Dr. Murrough noted.
“This raises the important question of what is the relevance of change in cognition to the potential benefits of ketamine. This is an important area and should be the focus of future research in order to improve outcomes for patients with depression and who are at risk for suicide,” he added.
Also weighing in, Roger S. McIntyre, MD, professor of psychiatry and pharmacology and head of the mood disorders psychopharmacology unit, University of Toronto, said the study is “very interesting and in keeping” with some previous work that he and his colleagues have done showing that ketamine “seems to benefit aspects of cognition which is a core element in depression.”
“It’s a testable hypothesis that the improvement in cognition now being reported and replicated could play some role in the improved quality of life and functioning with this treatment and as well reduce reducing suicide,” said Dr. McIntyre.
This study was supported by the National Institute of Mental Health. Dr. Mann receives royalties for commercial use of the Columbia-Suicide Severity Rating Scale, which was not used in this study. Dr. Murrough’s institution was involved in research involving esketamine (Spravato) for treatment-resistant depression and receives financial remuneration from the manufacturer of esketamine. Dr. McIntyre has received research grant support from the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation and speaker/consultation fees from Lundbeck, Janssen, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, Eisai, Minerva, Intra-Cellular, and AbbVie. Dr. McIntyre is also CEO of AltMed.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Adding questions in primary care may help predict suicide risk
Craig J. Bryan, PsyD, ABPP, with the department of psychiatry and behavioral health at Ohio State University Wexner Medical Center, Columbus, led the study, published online on Nov. 8, 2021, in Annals of Family Medicine.
The authors cited the urgency highlighted by statistics showing that, from 1999 to 2017, the U.S. suicide rate increased by more than 33% and was particularly high among military personnel and veterans.
Primary care offices are seen as a prime target for prevention efforts as nearly one-half of people who die by suicide in the United States visit a primary care office in the months before their deaths.
A common approach to screening for suicide risk has been to use the Patient Health Questionnaire–9 (PHQ-9). The first two questions assess the frequency of depressed mood and anhedonia in the past 2 weeks. If patients screen positive on those two questions, they are given the remaining seven questions.
A single item – question 9 – asks about how often a patient has “thoughts that you would be better off dead, or of hurting yourself in some way” during the past 2 weeks.
Yet, more that 95% of patients who screen positive on the PHQ-9 suicide risk question do not attempt or die by suicide, the authors noted.
Two methods tested for improving screening
Dr. Bryan and colleagues wanted to assess whether suicide risk screening could be improved in primary care and evaluated two methods.
One was to see whether using any of the other PHQ-9 items could be better than just using item 9 alone to identify the patients who were most likely to attempt suicide in the near future. Researchers found that method was not significantly beneficial. The second was to evaluate the performance of the 16 items on the Suicide Cognitions Scale (SCS), a questionnaire that asks patients to rate the extent to which they agree or disagree with statements that are commonly endorsed by suicidal people.
Patients who were eligible for medical treatment from the Department of Defense medical system were recruited from six large and small military primary care clinics across the United States from July 2015 to August 2018.
Patients answered questions on the PHQ-9 and 16 items from the SCS during routine primary care visits. Evaluators, who were blind to screening results, assessed postbaseline suicide attempts, interrupted attempts and aborted attempts by interviewing patients.
The study included 2,744 primary care patients, ranging from 18 to 89 years of age, with an average age of 40.
Adding at least one question may help
Researchers found that the accuracy of suicide risk screening using the PHQ-9 can be significantly improved by adding one or more questions from the SCS. Three items from SCS contributed most to meaningful improvements in identifying patients who went on to exhibit suicidal behaviors within 30-90 days of screening.
One question was item 16: “I don’t deserve to live another moment.”
Two SCS items improved specificity and positive predictive value without reducing sensitivity, the authors wrote. They are: “It is unbearable when I get this upset” (item 8) and “I can’t imagine anyone being able to withstand this kind of pain” (item 13).
“For example,” the authors wrote, “only 4.1% of patients who screened positive on the PHQ-9 suicide risk item 9 engaged in suicidal behavior within the next 30 days, but when the PHQ-9 suicide risk item 9 was combined with SCS item 13 (the best-performing SCS item), this percentage nearly doubled, to 7.6% of patients.”
Adding one of these SCS items to the PHQ-9 “could provide a simple, accessible, and low-cost method for more accurately identifying primary care patients who require more immediate clinical intervention,” the authors wrote.
Outside expert perspective
Meredith Williamson, PhD, a mental health diagnosis and psychotherapy expert and clinical assistant professor at Texas A&M University, Bryan, said that, though the SCS questions are valuable, neither they nor the PHQ-9 question get to the direct question of whether the person is likely to act on their thoughts and attempt or complete suicide.
“Someone with depression may have thought of wishing they were dead or wishing they weren’t here but that doesn’t always mean they necessarily want to kill themselves,” she said in an interview. “It’s our responsibility as providers to really clarify the meaning of that item.”
Dr. Williamson noted the PHQ-9 is a very accessible method to screen for depression in primary care settings and is a way to catch large numbers of people screening positive, but its shortcomings are well known and additional information is needed.
She said that, in her practice, if a patient screens positive on PHQ-9, clinicians ask more about their intentions, how frequently they occur and whether patients have developed a plan for killing themselves.
The challenge is that “we have yet to predict who is and who is not going to kill themselves.”
Dr. Williamson said she finds the Columbia-Suicide Severity Rating Scale a valuable tool used in research settings that looks at prior attempts and current desire to engage in an attempt in more detail.
“It doesn’t stop people from killing themselves, but helps to better understand their suicidal behavior,” she explained.
This project was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Defense Medical Research and Development Program. Dr. Williamson has no relevant financial disclosures. Dr. Bryan is a paid consultant to Oui Therapeutics and Neurostat Analytical Solutions. He is a principal of Anduril, which conducts training workshops and provides mental health consultation focused on suicide prevention and PTSD.
Craig J. Bryan, PsyD, ABPP, with the department of psychiatry and behavioral health at Ohio State University Wexner Medical Center, Columbus, led the study, published online on Nov. 8, 2021, in Annals of Family Medicine.
The authors cited the urgency highlighted by statistics showing that, from 1999 to 2017, the U.S. suicide rate increased by more than 33% and was particularly high among military personnel and veterans.
Primary care offices are seen as a prime target for prevention efforts as nearly one-half of people who die by suicide in the United States visit a primary care office in the months before their deaths.
A common approach to screening for suicide risk has been to use the Patient Health Questionnaire–9 (PHQ-9). The first two questions assess the frequency of depressed mood and anhedonia in the past 2 weeks. If patients screen positive on those two questions, they are given the remaining seven questions.
A single item – question 9 – asks about how often a patient has “thoughts that you would be better off dead, or of hurting yourself in some way” during the past 2 weeks.
Yet, more that 95% of patients who screen positive on the PHQ-9 suicide risk question do not attempt or die by suicide, the authors noted.
Two methods tested for improving screening
Dr. Bryan and colleagues wanted to assess whether suicide risk screening could be improved in primary care and evaluated two methods.
One was to see whether using any of the other PHQ-9 items could be better than just using item 9 alone to identify the patients who were most likely to attempt suicide in the near future. Researchers found that method was not significantly beneficial. The second was to evaluate the performance of the 16 items on the Suicide Cognitions Scale (SCS), a questionnaire that asks patients to rate the extent to which they agree or disagree with statements that are commonly endorsed by suicidal people.
Patients who were eligible for medical treatment from the Department of Defense medical system were recruited from six large and small military primary care clinics across the United States from July 2015 to August 2018.
Patients answered questions on the PHQ-9 and 16 items from the SCS during routine primary care visits. Evaluators, who were blind to screening results, assessed postbaseline suicide attempts, interrupted attempts and aborted attempts by interviewing patients.
The study included 2,744 primary care patients, ranging from 18 to 89 years of age, with an average age of 40.
Adding at least one question may help
Researchers found that the accuracy of suicide risk screening using the PHQ-9 can be significantly improved by adding one or more questions from the SCS. Three items from SCS contributed most to meaningful improvements in identifying patients who went on to exhibit suicidal behaviors within 30-90 days of screening.
One question was item 16: “I don’t deserve to live another moment.”
Two SCS items improved specificity and positive predictive value without reducing sensitivity, the authors wrote. They are: “It is unbearable when I get this upset” (item 8) and “I can’t imagine anyone being able to withstand this kind of pain” (item 13).
“For example,” the authors wrote, “only 4.1% of patients who screened positive on the PHQ-9 suicide risk item 9 engaged in suicidal behavior within the next 30 days, but when the PHQ-9 suicide risk item 9 was combined with SCS item 13 (the best-performing SCS item), this percentage nearly doubled, to 7.6% of patients.”
Adding one of these SCS items to the PHQ-9 “could provide a simple, accessible, and low-cost method for more accurately identifying primary care patients who require more immediate clinical intervention,” the authors wrote.
Outside expert perspective
Meredith Williamson, PhD, a mental health diagnosis and psychotherapy expert and clinical assistant professor at Texas A&M University, Bryan, said that, though the SCS questions are valuable, neither they nor the PHQ-9 question get to the direct question of whether the person is likely to act on their thoughts and attempt or complete suicide.
“Someone with depression may have thought of wishing they were dead or wishing they weren’t here but that doesn’t always mean they necessarily want to kill themselves,” she said in an interview. “It’s our responsibility as providers to really clarify the meaning of that item.”
Dr. Williamson noted the PHQ-9 is a very accessible method to screen for depression in primary care settings and is a way to catch large numbers of people screening positive, but its shortcomings are well known and additional information is needed.
She said that, in her practice, if a patient screens positive on PHQ-9, clinicians ask more about their intentions, how frequently they occur and whether patients have developed a plan for killing themselves.
The challenge is that “we have yet to predict who is and who is not going to kill themselves.”
Dr. Williamson said she finds the Columbia-Suicide Severity Rating Scale a valuable tool used in research settings that looks at prior attempts and current desire to engage in an attempt in more detail.
“It doesn’t stop people from killing themselves, but helps to better understand their suicidal behavior,” she explained.
This project was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Defense Medical Research and Development Program. Dr. Williamson has no relevant financial disclosures. Dr. Bryan is a paid consultant to Oui Therapeutics and Neurostat Analytical Solutions. He is a principal of Anduril, which conducts training workshops and provides mental health consultation focused on suicide prevention and PTSD.
Craig J. Bryan, PsyD, ABPP, with the department of psychiatry and behavioral health at Ohio State University Wexner Medical Center, Columbus, led the study, published online on Nov. 8, 2021, in Annals of Family Medicine.
The authors cited the urgency highlighted by statistics showing that, from 1999 to 2017, the U.S. suicide rate increased by more than 33% and was particularly high among military personnel and veterans.
Primary care offices are seen as a prime target for prevention efforts as nearly one-half of people who die by suicide in the United States visit a primary care office in the months before their deaths.
A common approach to screening for suicide risk has been to use the Patient Health Questionnaire–9 (PHQ-9). The first two questions assess the frequency of depressed mood and anhedonia in the past 2 weeks. If patients screen positive on those two questions, they are given the remaining seven questions.
A single item – question 9 – asks about how often a patient has “thoughts that you would be better off dead, or of hurting yourself in some way” during the past 2 weeks.
Yet, more that 95% of patients who screen positive on the PHQ-9 suicide risk question do not attempt or die by suicide, the authors noted.
Two methods tested for improving screening
Dr. Bryan and colleagues wanted to assess whether suicide risk screening could be improved in primary care and evaluated two methods.
One was to see whether using any of the other PHQ-9 items could be better than just using item 9 alone to identify the patients who were most likely to attempt suicide in the near future. Researchers found that method was not significantly beneficial. The second was to evaluate the performance of the 16 items on the Suicide Cognitions Scale (SCS), a questionnaire that asks patients to rate the extent to which they agree or disagree with statements that are commonly endorsed by suicidal people.
Patients who were eligible for medical treatment from the Department of Defense medical system were recruited from six large and small military primary care clinics across the United States from July 2015 to August 2018.
Patients answered questions on the PHQ-9 and 16 items from the SCS during routine primary care visits. Evaluators, who were blind to screening results, assessed postbaseline suicide attempts, interrupted attempts and aborted attempts by interviewing patients.
The study included 2,744 primary care patients, ranging from 18 to 89 years of age, with an average age of 40.
Adding at least one question may help
Researchers found that the accuracy of suicide risk screening using the PHQ-9 can be significantly improved by adding one or more questions from the SCS. Three items from SCS contributed most to meaningful improvements in identifying patients who went on to exhibit suicidal behaviors within 30-90 days of screening.
One question was item 16: “I don’t deserve to live another moment.”
Two SCS items improved specificity and positive predictive value without reducing sensitivity, the authors wrote. They are: “It is unbearable when I get this upset” (item 8) and “I can’t imagine anyone being able to withstand this kind of pain” (item 13).
“For example,” the authors wrote, “only 4.1% of patients who screened positive on the PHQ-9 suicide risk item 9 engaged in suicidal behavior within the next 30 days, but when the PHQ-9 suicide risk item 9 was combined with SCS item 13 (the best-performing SCS item), this percentage nearly doubled, to 7.6% of patients.”
Adding one of these SCS items to the PHQ-9 “could provide a simple, accessible, and low-cost method for more accurately identifying primary care patients who require more immediate clinical intervention,” the authors wrote.
Outside expert perspective
Meredith Williamson, PhD, a mental health diagnosis and psychotherapy expert and clinical assistant professor at Texas A&M University, Bryan, said that, though the SCS questions are valuable, neither they nor the PHQ-9 question get to the direct question of whether the person is likely to act on their thoughts and attempt or complete suicide.
“Someone with depression may have thought of wishing they were dead or wishing they weren’t here but that doesn’t always mean they necessarily want to kill themselves,” she said in an interview. “It’s our responsibility as providers to really clarify the meaning of that item.”
Dr. Williamson noted the PHQ-9 is a very accessible method to screen for depression in primary care settings and is a way to catch large numbers of people screening positive, but its shortcomings are well known and additional information is needed.
She said that, in her practice, if a patient screens positive on PHQ-9, clinicians ask more about their intentions, how frequently they occur and whether patients have developed a plan for killing themselves.
The challenge is that “we have yet to predict who is and who is not going to kill themselves.”
Dr. Williamson said she finds the Columbia-Suicide Severity Rating Scale a valuable tool used in research settings that looks at prior attempts and current desire to engage in an attempt in more detail.
“It doesn’t stop people from killing themselves, but helps to better understand their suicidal behavior,” she explained.
This project was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Defense Medical Research and Development Program. Dr. Williamson has no relevant financial disclosures. Dr. Bryan is a paid consultant to Oui Therapeutics and Neurostat Analytical Solutions. He is a principal of Anduril, which conducts training workshops and provides mental health consultation focused on suicide prevention and PTSD.
FROM ANNALS OF FAMILY MEDICINE
A pediatrician’s guide to screening for and treating depression
On Oct. 19, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association jointly declared a “national emergency in children’s mental health,” calling upon policy makers to take actions that could help address “soaring rates” of anxiety and depression.
Knowing that increasing the work force or creating new programs will come slowly if at all, they called for the integration of mental health care into primary care pediatrics and efforts to reduce the risk of suicide in children and adolescents.

Our clinical experience suggests that adolescent depression, which can lead to profoundly impaired function, impaired development, and even suicide, is a major concern in your practice. We hope to do our part by reviewing the screening, diagnosis, and management of depression that can reasonably happen in the pediatrician’s office.
Depression
Depression affects as many as 20% of adolescents, with girls experiencing major depressive disorder (MDD) twice as often as boys. The incidence of depression increases fourfold after puberty, and there is substantial evidence, but no clear cause, that it has increased by nearly 50% over the past decade, rising from a rate of 8% of U.S. adolescents in 2007 to 13% in 2017.1 In that same time period, the rate of completed suicides among U.S. youth aged 10-24 increased 57.4%, after being stable for the prior decade.2 Adolescent depression is also linked to increased substance use and high-risk behaviors such as drunk driving. In 2020, mental health–related emergency department visits by adolescents aged 12-17 increased by 31%. Visits for suicide attempts among adolescent girls in 2021 jumped by 51% from 2019.3 Clearly, MDD in adolescence is a common, potentially life-threatening problem
.

Screening and assessment
At annual checkups with patients 12 and older or at sick visits of patients with emotional, sleep, or vague somatic concerns, it should be standard practice to screen for depression. The Patient Health Questionnaire 9 modified for Adolescents (PHQ9-A) is a reliable, validated, and free screening instrument that your patients can fill out in the waiting room. (The PHQ9 can be used for your patients who are 18 and older.) It takes only 5 minutes to complete and is very easy to score. It establishes whether your patient meets DSM-5 criteria for MDD, and the degree of severity (5-9 is mild, 10-14 is moderate, 15-19 is moderately severe, and 20-27 is severe). It also screens for thoughts about suicide and past suicide attempts. You might add the more comprehensive parent-completed Pediatric Symptom Checklist, which includes a depression screen.4
These screening instruments can be completed electronically prior to or at the visit and should have a preamble explaining why depression screening is relevant. If screening is positive, interview your adolescent patients alone. This will give you the time to gather more detail about how impaired their function is at school, with friends, and in family relationships. Have they been missing school? Have their grades changed? Are they failing to hand in homework? Have they withdrawn from sports or activities? Are they less likely to hang out with friends? Do they participate in family activities? Have others noticed any changes? You should also check for associated anxiety symptoms (ruminative worries, panic attacks) and drug and alcohol use. Of course, you should ask about any suicidal thoughts (from vague morbid thoughts to specific plans, with intent and factors that have prevented them) and actual attempts. Remember, asking about suicidal thoughts and attempts will not cause or worsen them. On the contrary, your patients may feel shame, but will be relieved to not be alone with these thoughts. And this knowledge will be essential as you decide what to do next. When you meet with the parents, ask them about a family history of depression or suicide attempts, and then offer supportive interventions.
Supportive interventions
For all adolescents with depression, supportive interventions are helpful, and for those with mild symptoms, they are often adequate treatment. This begins with education for your patient and their parents about depression. It is an illness, not a problem of character or discipline. Advise your patients that adequate, restful sleep every night is critical to recovery. Regular exercise (daily is best, but at least three times weekly for 30 minutes) is often effective in mild to moderate depression. Patience and compassion for feelings of sadness, irritability, or disinterest are important at home, and maintaining connections with those people who offer support (friends, coaches, parents, etc.) is essential. They should also be told that “depression lies.” Feelings of guilt and self-reproach are a normal part of the illness, not facts. Organizations such as the National Alliance on Mental Illness (NAMI) and the American Academy of Child and Adolescent Psychiatry (AACAP) offer written materials through their websites that are very helpful educational resources. Connect them with sources of counseling support (through school, for example). For those with mild, brief, and uncomplicated depression, supportive interventions alone should offer relief within 4-6 weeks. It is hard to predict the trajectory of depression, so follow-up visits are relevant to determine if they are improving or worsening.
Psychotherapy
For your patients with moderate depression, or with hopelessness or suicidality, a referral for evidence-based psychotherapy is indicated. Both cognitive behavioral therapy and interpersonal therapy have demonstrated efficacy in treating depression in adolescents. If there is a history of trauma or high family conflict, supportive psychotherapy that will enhance communication skills within the family is very important to recovery. Identify various sources for high-quality psychotherapy services (individual, family, and group) in your community. While this may sound easier said than done, online services such as Psychology Today’s therapist locator can help. If your local university has a graduate program in social work or psychology, connect with them as they may have easier access to high-quality services through their training programs. If there is a group practice of therapists in your community, invite them to meet with your team to learn about whether they use evidence-based therapies and can support families as well as individual youth.
Pharmacologic options
For those adolescents with moderate to severe depression, psychotherapy alone is usually inadequate. Indeed, they may be so impaired that they simply cannot meaningfully engage in the work of psychotherapy. These patients require psychopharmacologic treatment first. First-line treatment is with selective serotonin reuptake inhibitors (SSRIs) (both fluoxetine and escitalopram are approved for use in adolescent depression). While many pediatricians remain reluctant about initiating SSRI treatment of depression since the Food and Drug Administration’s 2004 boxed warning was issued, the risks of untreated severe depression are more marked than are the risks of SSRI treatment. As prescription rates dipped in the following decade, rates of suicide attempts in adolescents with severe depression climbed. Subsequent research on the nature of the risk of “increased suicidality” indicated it is substantially lower than originally thought.
The AAP’s Guidelines for Adolescent Depression in Primary Care offer reassuring guidance: They recommend that pediatricians initiate treatment at a very low dose of SSRI (5 mg of fluoxetine, 12.5 mg of sertraline, or 5 mg of escitalopram) and aim to get to a therapeutic dose within 4 weeks.5 Educate the patient and parent about likely side effects (gastrointestinal upset, sleep disruption, akathisia or restlessness, and activation), which indicate the dose should be held steady until the side effects subside. Patients should be seen weekly until they get to a therapeutic dose, then biweekly to monitor for response. At these regular check-ins, the PHQ9A can follow symptom severity. You should monitor changes in function and for any change in suicidal thoughts. If your patient does not respond with at least energy improvement within 4 weeks, you should cross-taper to a different SSRI.
Managing risk
Suicidal thoughts are a common symptom of depression and an important marker of severity. Adolescents have more limited impulse control than do adults, elevating their risk for impulsively acting on these thoughts. Adolescents who are using alcohol or other substances, or who have a history of impulsivity, are at higher risk. Further compounding the degree of risk are a history of suicide attempts, impulsive aggression or psychotic symptoms, or a family history of completed suicide. In managing risk, it is critical that you assess and discuss these risk factors and discuss the need to have a safety plan.
This planning should include both patient and parent. Help the parent to identify lethal means at home (guns, rope, medications, and knives or box cutters) and make plans to secure or remove them. It includes helping your patient list those strategies that can be helpful if they are feeling more distressed (distracting with music or television, exercise, or connecting with select friends). A safety plan is not a promise or a contract to not do something, rather it is a practical set of strategies the patient and family can employ if they are feeling worse. It depends on the adolescent having a secure, trusting connection with the adults at home and with your office.
If your patient fails to improve, if the diagnosis appears complicated, or if you feel the patient is not safe, you should refer to child psychiatry or, if needed, a local emergency department. If you cannot find access to a psychiatrist, start with your state’s child psychiatric consultation hotline for access to telephone support: www.nncpap.org.
Although the suggestions outlined above are grounded in evidence and need, treating moderate to severe depression is likely a new challenge for many pediatricians. Managing the risk of suicide can be stressful, without a doubt. In our own work as child psychiatrists, we recognize that there is no single, reliable method to predict suicide and therefore no specific approach to ensuring prevention. We appreciate this burden of worry when treating a severely depressed adolescent, and follow the rule, “never worry alone” – share your concerns with parents and/or a mental health consultant (hopefully co-located in your office), or obtain a second opinion, even consult a child psychiatrist on a hotline. Offering supportive care for those with mild depression can prevent it from becoming severe, and beginning treatment for those with severe depression can make a profound difference in the course of a young person’s illness.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Pew Research Center. National Survey on Drug Use and Health (2017).
2. Curtin SC. Natl Vital Stat Rep. 2020 Sep;69(11):1-10.
3. Yard E et al. MMWR Morb Mortal Wkly Rep. 2021 Jun 18;70(24):888-94.
4. Jellinek M et al. J Pediatr. 2021 Jun;233:220-6.e1.
5. Zuckerbrot RA et al. Pediatrics. 2018 Mar;141(3):e20174081.
On Oct. 19, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association jointly declared a “national emergency in children’s mental health,” calling upon policy makers to take actions that could help address “soaring rates” of anxiety and depression.
Knowing that increasing the work force or creating new programs will come slowly if at all, they called for the integration of mental health care into primary care pediatrics and efforts to reduce the risk of suicide in children and adolescents.
Our clinical experience suggests that adolescent depression, which can lead to profoundly impaired function, impaired development, and even suicide, is a major concern in your practice. We hope to do our part by reviewing the screening, diagnosis, and management of depression that can reasonably happen in the pediatrician’s office.
Depression
Depression affects as many as 20% of adolescents, with girls experiencing major depressive disorder (MDD) twice as often as boys. The incidence of depression increases fourfold after puberty, and there is substantial evidence, but no clear cause, that it has increased by nearly 50% over the past decade, rising from a rate of 8% of U.S. adolescents in 2007 to 13% in 2017.1 In that same time period, the rate of completed suicides among U.S. youth aged 10-24 increased 57.4%, after being stable for the prior decade.2 Adolescent depression is also linked to increased substance use and high-risk behaviors such as drunk driving. In 2020, mental health–related emergency department visits by adolescents aged 12-17 increased by 31%. Visits for suicide attempts among adolescent girls in 2021 jumped by 51% from 2019.3 Clearly, MDD in adolescence is a common, potentially life-threatening problem
.
Screening and assessment
At annual checkups with patients 12 and older or at sick visits of patients with emotional, sleep, or vague somatic concerns, it should be standard practice to screen for depression. The Patient Health Questionnaire 9 modified for Adolescents (PHQ9-A) is a reliable, validated, and free screening instrument that your patients can fill out in the waiting room. (The PHQ9 can be used for your patients who are 18 and older.) It takes only 5 minutes to complete and is very easy to score. It establishes whether your patient meets DSM-5 criteria for MDD, and the degree of severity (5-9 is mild, 10-14 is moderate, 15-19 is moderately severe, and 20-27 is severe). It also screens for thoughts about suicide and past suicide attempts. You might add the more comprehensive parent-completed Pediatric Symptom Checklist, which includes a depression screen.4
These screening instruments can be completed electronically prior to or at the visit and should have a preamble explaining why depression screening is relevant. If screening is positive, interview your adolescent patients alone. This will give you the time to gather more detail about how impaired their function is at school, with friends, and in family relationships. Have they been missing school? Have their grades changed? Are they failing to hand in homework? Have they withdrawn from sports or activities? Are they less likely to hang out with friends? Do they participate in family activities? Have others noticed any changes? You should also check for associated anxiety symptoms (ruminative worries, panic attacks) and drug and alcohol use. Of course, you should ask about any suicidal thoughts (from vague morbid thoughts to specific plans, with intent and factors that have prevented them) and actual attempts. Remember, asking about suicidal thoughts and attempts will not cause or worsen them. On the contrary, your patients may feel shame, but will be relieved to not be alone with these thoughts. And this knowledge will be essential as you decide what to do next. When you meet with the parents, ask them about a family history of depression or suicide attempts, and then offer supportive interventions.
Supportive interventions
For all adolescents with depression, supportive interventions are helpful, and for those with mild symptoms, they are often adequate treatment. This begins with education for your patient and their parents about depression. It is an illness, not a problem of character or discipline. Advise your patients that adequate, restful sleep every night is critical to recovery. Regular exercise (daily is best, but at least three times weekly for 30 minutes) is often effective in mild to moderate depression. Patience and compassion for feelings of sadness, irritability, or disinterest are important at home, and maintaining connections with those people who offer support (friends, coaches, parents, etc.) is essential. They should also be told that “depression lies.” Feelings of guilt and self-reproach are a normal part of the illness, not facts. Organizations such as the National Alliance on Mental Illness (NAMI) and the American Academy of Child and Adolescent Psychiatry (AACAP) offer written materials through their websites that are very helpful educational resources. Connect them with sources of counseling support (through school, for example). For those with mild, brief, and uncomplicated depression, supportive interventions alone should offer relief within 4-6 weeks. It is hard to predict the trajectory of depression, so follow-up visits are relevant to determine if they are improving or worsening.
Psychotherapy
For your patients with moderate depression, or with hopelessness or suicidality, a referral for evidence-based psychotherapy is indicated. Both cognitive behavioral therapy and interpersonal therapy have demonstrated efficacy in treating depression in adolescents. If there is a history of trauma or high family conflict, supportive psychotherapy that will enhance communication skills within the family is very important to recovery. Identify various sources for high-quality psychotherapy services (individual, family, and group) in your community. While this may sound easier said than done, online services such as Psychology Today’s therapist locator can help. If your local university has a graduate program in social work or psychology, connect with them as they may have easier access to high-quality services through their training programs. If there is a group practice of therapists in your community, invite them to meet with your team to learn about whether they use evidence-based therapies and can support families as well as individual youth.
Pharmacologic options
For those adolescents with moderate to severe depression, psychotherapy alone is usually inadequate. Indeed, they may be so impaired that they simply cannot meaningfully engage in the work of psychotherapy. These patients require psychopharmacologic treatment first. First-line treatment is with selective serotonin reuptake inhibitors (SSRIs) (both fluoxetine and escitalopram are approved for use in adolescent depression). While many pediatricians remain reluctant about initiating SSRI treatment of depression since the Food and Drug Administration’s 2004 boxed warning was issued, the risks of untreated severe depression are more marked than are the risks of SSRI treatment. As prescription rates dipped in the following decade, rates of suicide attempts in adolescents with severe depression climbed. Subsequent research on the nature of the risk of “increased suicidality” indicated it is substantially lower than originally thought.
The AAP’s Guidelines for Adolescent Depression in Primary Care offer reassuring guidance: They recommend that pediatricians initiate treatment at a very low dose of SSRI (5 mg of fluoxetine, 12.5 mg of sertraline, or 5 mg of escitalopram) and aim to get to a therapeutic dose within 4 weeks.5 Educate the patient and parent about likely side effects (gastrointestinal upset, sleep disruption, akathisia or restlessness, and activation), which indicate the dose should be held steady until the side effects subside. Patients should be seen weekly until they get to a therapeutic dose, then biweekly to monitor for response. At these regular check-ins, the PHQ9A can follow symptom severity. You should monitor changes in function and for any change in suicidal thoughts. If your patient does not respond with at least energy improvement within 4 weeks, you should cross-taper to a different SSRI.
Managing risk
Suicidal thoughts are a common symptom of depression and an important marker of severity. Adolescents have more limited impulse control than do adults, elevating their risk for impulsively acting on these thoughts. Adolescents who are using alcohol or other substances, or who have a history of impulsivity, are at higher risk. Further compounding the degree of risk are a history of suicide attempts, impulsive aggression or psychotic symptoms, or a family history of completed suicide. In managing risk, it is critical that you assess and discuss these risk factors and discuss the need to have a safety plan.
This planning should include both patient and parent. Help the parent to identify lethal means at home (guns, rope, medications, and knives or box cutters) and make plans to secure or remove them. It includes helping your patient list those strategies that can be helpful if they are feeling more distressed (distracting with music or television, exercise, or connecting with select friends). A safety plan is not a promise or a contract to not do something, rather it is a practical set of strategies the patient and family can employ if they are feeling worse. It depends on the adolescent having a secure, trusting connection with the adults at home and with your office.
If your patient fails to improve, if the diagnosis appears complicated, or if you feel the patient is not safe, you should refer to child psychiatry or, if needed, a local emergency department. If you cannot find access to a psychiatrist, start with your state’s child psychiatric consultation hotline for access to telephone support: www.nncpap.org.
Although the suggestions outlined above are grounded in evidence and need, treating moderate to severe depression is likely a new challenge for many pediatricians. Managing the risk of suicide can be stressful, without a doubt. In our own work as child psychiatrists, we recognize that there is no single, reliable method to predict suicide and therefore no specific approach to ensuring prevention. We appreciate this burden of worry when treating a severely depressed adolescent, and follow the rule, “never worry alone” – share your concerns with parents and/or a mental health consultant (hopefully co-located in your office), or obtain a second opinion, even consult a child psychiatrist on a hotline. Offering supportive care for those with mild depression can prevent it from becoming severe, and beginning treatment for those with severe depression can make a profound difference in the course of a young person’s illness.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Pew Research Center. National Survey on Drug Use and Health (2017).
2. Curtin SC. Natl Vital Stat Rep. 2020 Sep;69(11):1-10.
3. Yard E et al. MMWR Morb Mortal Wkly Rep. 2021 Jun 18;70(24):888-94.
4. Jellinek M et al. J Pediatr. 2021 Jun;233:220-6.e1.
5. Zuckerbrot RA et al. Pediatrics. 2018 Mar;141(3):e20174081.
On Oct. 19, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association jointly declared a “national emergency in children’s mental health,” calling upon policy makers to take actions that could help address “soaring rates” of anxiety and depression.
Knowing that increasing the work force or creating new programs will come slowly if at all, they called for the integration of mental health care into primary care pediatrics and efforts to reduce the risk of suicide in children and adolescents.
Our clinical experience suggests that adolescent depression, which can lead to profoundly impaired function, impaired development, and even suicide, is a major concern in your practice. We hope to do our part by reviewing the screening, diagnosis, and management of depression that can reasonably happen in the pediatrician’s office.
Depression
Depression affects as many as 20% of adolescents, with girls experiencing major depressive disorder (MDD) twice as often as boys. The incidence of depression increases fourfold after puberty, and there is substantial evidence, but no clear cause, that it has increased by nearly 50% over the past decade, rising from a rate of 8% of U.S. adolescents in 2007 to 13% in 2017.1 In that same time period, the rate of completed suicides among U.S. youth aged 10-24 increased 57.4%, after being stable for the prior decade.2 Adolescent depression is also linked to increased substance use and high-risk behaviors such as drunk driving. In 2020, mental health–related emergency department visits by adolescents aged 12-17 increased by 31%. Visits for suicide attempts among adolescent girls in 2021 jumped by 51% from 2019.3 Clearly, MDD in adolescence is a common, potentially life-threatening problem
.
Screening and assessment
At annual checkups with patients 12 and older or at sick visits of patients with emotional, sleep, or vague somatic concerns, it should be standard practice to screen for depression. The Patient Health Questionnaire 9 modified for Adolescents (PHQ9-A) is a reliable, validated, and free screening instrument that your patients can fill out in the waiting room. (The PHQ9 can be used for your patients who are 18 and older.) It takes only 5 minutes to complete and is very easy to score. It establishes whether your patient meets DSM-5 criteria for MDD, and the degree of severity (5-9 is mild, 10-14 is moderate, 15-19 is moderately severe, and 20-27 is severe). It also screens for thoughts about suicide and past suicide attempts. You might add the more comprehensive parent-completed Pediatric Symptom Checklist, which includes a depression screen.4
These screening instruments can be completed electronically prior to or at the visit and should have a preamble explaining why depression screening is relevant. If screening is positive, interview your adolescent patients alone. This will give you the time to gather more detail about how impaired their function is at school, with friends, and in family relationships. Have they been missing school? Have their grades changed? Are they failing to hand in homework? Have they withdrawn from sports or activities? Are they less likely to hang out with friends? Do they participate in family activities? Have others noticed any changes? You should also check for associated anxiety symptoms (ruminative worries, panic attacks) and drug and alcohol use. Of course, you should ask about any suicidal thoughts (from vague morbid thoughts to specific plans, with intent and factors that have prevented them) and actual attempts. Remember, asking about suicidal thoughts and attempts will not cause or worsen them. On the contrary, your patients may feel shame, but will be relieved to not be alone with these thoughts. And this knowledge will be essential as you decide what to do next. When you meet with the parents, ask them about a family history of depression or suicide attempts, and then offer supportive interventions.
Supportive interventions
For all adolescents with depression, supportive interventions are helpful, and for those with mild symptoms, they are often adequate treatment. This begins with education for your patient and their parents about depression. It is an illness, not a problem of character or discipline. Advise your patients that adequate, restful sleep every night is critical to recovery. Regular exercise (daily is best, but at least three times weekly for 30 minutes) is often effective in mild to moderate depression. Patience and compassion for feelings of sadness, irritability, or disinterest are important at home, and maintaining connections with those people who offer support (friends, coaches, parents, etc.) is essential. They should also be told that “depression lies.” Feelings of guilt and self-reproach are a normal part of the illness, not facts. Organizations such as the National Alliance on Mental Illness (NAMI) and the American Academy of Child and Adolescent Psychiatry (AACAP) offer written materials through their websites that are very helpful educational resources. Connect them with sources of counseling support (through school, for example). For those with mild, brief, and uncomplicated depression, supportive interventions alone should offer relief within 4-6 weeks. It is hard to predict the trajectory of depression, so follow-up visits are relevant to determine if they are improving or worsening.
Psychotherapy
For your patients with moderate depression, or with hopelessness or suicidality, a referral for evidence-based psychotherapy is indicated. Both cognitive behavioral therapy and interpersonal therapy have demonstrated efficacy in treating depression in adolescents. If there is a history of trauma or high family conflict, supportive psychotherapy that will enhance communication skills within the family is very important to recovery. Identify various sources for high-quality psychotherapy services (individual, family, and group) in your community. While this may sound easier said than done, online services such as Psychology Today’s therapist locator can help. If your local university has a graduate program in social work or psychology, connect with them as they may have easier access to high-quality services through their training programs. If there is a group practice of therapists in your community, invite them to meet with your team to learn about whether they use evidence-based therapies and can support families as well as individual youth.
Pharmacologic options
For those adolescents with moderate to severe depression, psychotherapy alone is usually inadequate. Indeed, they may be so impaired that they simply cannot meaningfully engage in the work of psychotherapy. These patients require psychopharmacologic treatment first. First-line treatment is with selective serotonin reuptake inhibitors (SSRIs) (both fluoxetine and escitalopram are approved for use in adolescent depression). While many pediatricians remain reluctant about initiating SSRI treatment of depression since the Food and Drug Administration’s 2004 boxed warning was issued, the risks of untreated severe depression are more marked than are the risks of SSRI treatment. As prescription rates dipped in the following decade, rates of suicide attempts in adolescents with severe depression climbed. Subsequent research on the nature of the risk of “increased suicidality” indicated it is substantially lower than originally thought.
The AAP’s Guidelines for Adolescent Depression in Primary Care offer reassuring guidance: They recommend that pediatricians initiate treatment at a very low dose of SSRI (5 mg of fluoxetine, 12.5 mg of sertraline, or 5 mg of escitalopram) and aim to get to a therapeutic dose within 4 weeks.5 Educate the patient and parent about likely side effects (gastrointestinal upset, sleep disruption, akathisia or restlessness, and activation), which indicate the dose should be held steady until the side effects subside. Patients should be seen weekly until they get to a therapeutic dose, then biweekly to monitor for response. At these regular check-ins, the PHQ9A can follow symptom severity. You should monitor changes in function and for any change in suicidal thoughts. If your patient does not respond with at least energy improvement within 4 weeks, you should cross-taper to a different SSRI.
Managing risk
Suicidal thoughts are a common symptom of depression and an important marker of severity. Adolescents have more limited impulse control than do adults, elevating their risk for impulsively acting on these thoughts. Adolescents who are using alcohol or other substances, or who have a history of impulsivity, are at higher risk. Further compounding the degree of risk are a history of suicide attempts, impulsive aggression or psychotic symptoms, or a family history of completed suicide. In managing risk, it is critical that you assess and discuss these risk factors and discuss the need to have a safety plan.
This planning should include both patient and parent. Help the parent to identify lethal means at home (guns, rope, medications, and knives or box cutters) and make plans to secure or remove them. It includes helping your patient list those strategies that can be helpful if they are feeling more distressed (distracting with music or television, exercise, or connecting with select friends). A safety plan is not a promise or a contract to not do something, rather it is a practical set of strategies the patient and family can employ if they are feeling worse. It depends on the adolescent having a secure, trusting connection with the adults at home and with your office.
If your patient fails to improve, if the diagnosis appears complicated, or if you feel the patient is not safe, you should refer to child psychiatry or, if needed, a local emergency department. If you cannot find access to a psychiatrist, start with your state’s child psychiatric consultation hotline for access to telephone support: www.nncpap.org.
Although the suggestions outlined above are grounded in evidence and need, treating moderate to severe depression is likely a new challenge for many pediatricians. Managing the risk of suicide can be stressful, without a doubt. In our own work as child psychiatrists, we recognize that there is no single, reliable method to predict suicide and therefore no specific approach to ensuring prevention. We appreciate this burden of worry when treating a severely depressed adolescent, and follow the rule, “never worry alone” – share your concerns with parents and/or a mental health consultant (hopefully co-located in your office), or obtain a second opinion, even consult a child psychiatrist on a hotline. Offering supportive care for those with mild depression can prevent it from becoming severe, and beginning treatment for those with severe depression can make a profound difference in the course of a young person’s illness.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Pew Research Center. National Survey on Drug Use and Health (2017).
2. Curtin SC. Natl Vital Stat Rep. 2020 Sep;69(11):1-10.
3. Yard E et al. MMWR Morb Mortal Wkly Rep. 2021 Jun 18;70(24):888-94.
4. Jellinek M et al. J Pediatr. 2021 Jun;233:220-6.e1.
5. Zuckerbrot RA et al. Pediatrics. 2018 Mar;141(3):e20174081.
Aaron Beck: An appreciation
He always dressed the same at conferences: dark suit, white shirt, bright red bow tie.
For all his fame, he was very kind, warmly greeting those who wanted to see him and immediately turning attention toward their research rather than his own. Aaron Beck actually didn’t lecture much; he preferred to roleplay cognitive therapy with an audience member acting as the patient. He would engage in what he called Socratic questioning, or more formally, cognitive restructuring, with warmth and true curiosity:
- What might be another explanation or viewpoint?
- What are the effects of thinking this way?
- Can you think of any evidence that supports the opposite view?
The audience member/patient would benefit not only from thinking about things differently, but also from the captivating interaction with the man, Aaron Temkin Beck, MD, (who went by Tim), youngest child of Jewish immigrants from the Ukraine.
When written up in treatment manuals, cognitive restructuring can seem cold and overly logical, but in person, Dr. Beck made it come to life. This ability to nurture curiosity was a special talent; his friend and fellow cognitive psychologist Donald Meichenbaum, PhD, recalls that even over lunch, he never stopped asking questions, personal and professional, on a wide range of topics.
It is widely accepted that Dr. Beck, who died Nov. 1 at the age of 100 in suburban Philadelphia, was the most important figure in the field of cognitive-behavioral therapy (CBT).
He didn’t invent the field. Behaviorism predated him by generations, founded by figures such as John Watson and B.F. Skinner. Those psychologists set up behaviorism as an alternative to the reigning power of Freudian psychoanalysis, but they ran a distant second.
It wasn’t until Dr. Beck added a new approach, cognitive therapy, to the behavioristic movement that the new mélange, CBT, began to gain traction with clinicians and researchers. Dr. Beck, who had trained in psychiatry, developed his ideas in the 1960s while observing what he believed were limitations in the classic Freudian methods. He recognized that patients had “automatic thoughts,” not just unconscious emotions, when they engaged in Freudian free association, saying whatever came to their minds.
These thoughts often distorted reality, he observed; they were “maladaptive beliefs,” and when they changed, patients’ emotional states improved.
Dr. Beck wasn’t alone. The psychologist Albert Ellis, PhD, in New York, had come to similar conclusions a decade earlier, though with a more coldly logical and challenging style. The prominent British psychologist Hans Eysenck, PhD, had argued strongly that Freudian psychoanalysis was ineffective and that behavioral approaches were better.
Dr. Beck turned the Freudian equation around: Instead of emotion as cause and thought as effect, it was thought which affected emotion, for better or worse. Once you connected behavior as the outcome, you had the essence of CBT: thought, emotion, and behavior – each affecting the other, with thought being the strongest axis of change.
The process wasn’t bloodless. Behaviorists defended their turf against cognitivists, just as much as Freudians rejected both. At one point the behaviorists in the Association for the Advancement of Behavior Therapy tried to expel the advocates of a cognitive approach. Dr. Beck responded by leading the cognitivists in creating a new journal; he emphasized the importance of research being the main mechanism to decide what treatments worked the best.
Putting these ideas out in the 1960s and 1970s, Dr. Beck garnered support from researchers when he manualized the approach. Freudian psychoanalysis was idiosyncratic; it was almost impossible to study empirically, because the therapist would be responding to the unpredictable dreams and memories of patients engaged in free association. Each case was unique.
But CBT was systematic: The same general approach was taken to all patients; the same negative cognitions were found in depression, for instance, like all-or-nothing thinking or overgeneralization. Once manualized, CBT became the standard method of psychotherapy studied with the newly developed method of randomized controlled trials (RCTs).
By the 1980s, RCTs had proven the efficacy of CBT in depression, and the approach took off.
Dr. Beck already had developed a series of rating scales: the Beck Depression Inventory, the Beck Scale for Suicidal Ideation, the Beck Anxiety Inventory, the Beck Hopelessness Scale. Widely used, these scales extended his influence enormously. Copyrighted, they created a new industry of psychological research.
Dr. Beck’s own work was mainly in depression, but his followers extended it everywhere else: anxiety disorders and phobias, eating disorders, substance abuse, bipolar illness, even schizophrenia. Meanwhile, Freudian psychoanalysis fell into a steep decline from which it never recovered.
Some argued that it was abetted by insurance restrictions on psychotherapy, which favored shorter-term CBT; others that its research was biased in its favor because psychotherapy treatments, unlike medications, cannot be blinded; others that its efficacy could not be shown to be specific to its theory, as opposed to the interpersonal relationship between therapist and client.
Still, CBT has transformed psychotherapy and continues to expand its influence. Computer-based CBT has been proven effective, and digital CBT has become a standard approach in many smartphone applications and is central to the claims of multiple new biotechnology companies advocating for digital psychotherapy.
Aaron Beck continued publishing scientific articles to age 98. His last papers reviewed his life’s work. He characteristically gave credit to others, calmly recollected how he traveled away from psychoanalysis, described how his work started and ended in schizophrenia, and noted that the “working relationship with the therapist” remained a key factor for the success of CBT.
That parting comment reminds us that behind all the technology and research stands the kindly man in the dark suit, white shirt, and bright red bow tie, looking at you warmly, asking about your thoughts, and curiously wondering what might be another explanation or viewpoint you hadn’t considered.
Nassir Ghaemi, MD, MPH, is a professor of psychiatry at Tufts Medical Center and a lecturer in psychiatry at Harvard Medical School. He is the author of several general-interest books on psychiatry. A version of this article first appeared on Medscape.com.
He always dressed the same at conferences: dark suit, white shirt, bright red bow tie.
For all his fame, he was very kind, warmly greeting those who wanted to see him and immediately turning attention toward their research rather than his own. Aaron Beck actually didn’t lecture much; he preferred to roleplay cognitive therapy with an audience member acting as the patient. He would engage in what he called Socratic questioning, or more formally, cognitive restructuring, with warmth and true curiosity:
- What might be another explanation or viewpoint?
- What are the effects of thinking this way?
- Can you think of any evidence that supports the opposite view?
The audience member/patient would benefit not only from thinking about things differently, but also from the captivating interaction with the man, Aaron Temkin Beck, MD, (who went by Tim), youngest child of Jewish immigrants from the Ukraine.
When written up in treatment manuals, cognitive restructuring can seem cold and overly logical, but in person, Dr. Beck made it come to life. This ability to nurture curiosity was a special talent; his friend and fellow cognitive psychologist Donald Meichenbaum, PhD, recalls that even over lunch, he never stopped asking questions, personal and professional, on a wide range of topics.
It is widely accepted that Dr. Beck, who died Nov. 1 at the age of 100 in suburban Philadelphia, was the most important figure in the field of cognitive-behavioral therapy (CBT).
He didn’t invent the field. Behaviorism predated him by generations, founded by figures such as John Watson and B.F. Skinner. Those psychologists set up behaviorism as an alternative to the reigning power of Freudian psychoanalysis, but they ran a distant second.
It wasn’t until Dr. Beck added a new approach, cognitive therapy, to the behavioristic movement that the new mélange, CBT, began to gain traction with clinicians and researchers. Dr. Beck, who had trained in psychiatry, developed his ideas in the 1960s while observing what he believed were limitations in the classic Freudian methods. He recognized that patients had “automatic thoughts,” not just unconscious emotions, when they engaged in Freudian free association, saying whatever came to their minds.
These thoughts often distorted reality, he observed; they were “maladaptive beliefs,” and when they changed, patients’ emotional states improved.
Dr. Beck wasn’t alone. The psychologist Albert Ellis, PhD, in New York, had come to similar conclusions a decade earlier, though with a more coldly logical and challenging style. The prominent British psychologist Hans Eysenck, PhD, had argued strongly that Freudian psychoanalysis was ineffective and that behavioral approaches were better.
Dr. Beck turned the Freudian equation around: Instead of emotion as cause and thought as effect, it was thought which affected emotion, for better or worse. Once you connected behavior as the outcome, you had the essence of CBT: thought, emotion, and behavior – each affecting the other, with thought being the strongest axis of change.
The process wasn’t bloodless. Behaviorists defended their turf against cognitivists, just as much as Freudians rejected both. At one point the behaviorists in the Association for the Advancement of Behavior Therapy tried to expel the advocates of a cognitive approach. Dr. Beck responded by leading the cognitivists in creating a new journal; he emphasized the importance of research being the main mechanism to decide what treatments worked the best.
Putting these ideas out in the 1960s and 1970s, Dr. Beck garnered support from researchers when he manualized the approach. Freudian psychoanalysis was idiosyncratic; it was almost impossible to study empirically, because the therapist would be responding to the unpredictable dreams and memories of patients engaged in free association. Each case was unique.
But CBT was systematic: The same general approach was taken to all patients; the same negative cognitions were found in depression, for instance, like all-or-nothing thinking or overgeneralization. Once manualized, CBT became the standard method of psychotherapy studied with the newly developed method of randomized controlled trials (RCTs).
By the 1980s, RCTs had proven the efficacy of CBT in depression, and the approach took off.
Dr. Beck already had developed a series of rating scales: the Beck Depression Inventory, the Beck Scale for Suicidal Ideation, the Beck Anxiety Inventory, the Beck Hopelessness Scale. Widely used, these scales extended his influence enormously. Copyrighted, they created a new industry of psychological research.
Dr. Beck’s own work was mainly in depression, but his followers extended it everywhere else: anxiety disorders and phobias, eating disorders, substance abuse, bipolar illness, even schizophrenia. Meanwhile, Freudian psychoanalysis fell into a steep decline from which it never recovered.
Some argued that it was abetted by insurance restrictions on psychotherapy, which favored shorter-term CBT; others that its research was biased in its favor because psychotherapy treatments, unlike medications, cannot be blinded; others that its efficacy could not be shown to be specific to its theory, as opposed to the interpersonal relationship between therapist and client.
Still, CBT has transformed psychotherapy and continues to expand its influence. Computer-based CBT has been proven effective, and digital CBT has become a standard approach in many smartphone applications and is central to the claims of multiple new biotechnology companies advocating for digital psychotherapy.
Aaron Beck continued publishing scientific articles to age 98. His last papers reviewed his life’s work. He characteristically gave credit to others, calmly recollected how he traveled away from psychoanalysis, described how his work started and ended in schizophrenia, and noted that the “working relationship with the therapist” remained a key factor for the success of CBT.
That parting comment reminds us that behind all the technology and research stands the kindly man in the dark suit, white shirt, and bright red bow tie, looking at you warmly, asking about your thoughts, and curiously wondering what might be another explanation or viewpoint you hadn’t considered.
Nassir Ghaemi, MD, MPH, is a professor of psychiatry at Tufts Medical Center and a lecturer in psychiatry at Harvard Medical School. He is the author of several general-interest books on psychiatry. A version of this article first appeared on Medscape.com.
He always dressed the same at conferences: dark suit, white shirt, bright red bow tie.
For all his fame, he was very kind, warmly greeting those who wanted to see him and immediately turning attention toward their research rather than his own. Aaron Beck actually didn’t lecture much; he preferred to roleplay cognitive therapy with an audience member acting as the patient. He would engage in what he called Socratic questioning, or more formally, cognitive restructuring, with warmth and true curiosity:
- What might be another explanation or viewpoint?
- What are the effects of thinking this way?
- Can you think of any evidence that supports the opposite view?
The audience member/patient would benefit not only from thinking about things differently, but also from the captivating interaction with the man, Aaron Temkin Beck, MD, (who went by Tim), youngest child of Jewish immigrants from the Ukraine.
When written up in treatment manuals, cognitive restructuring can seem cold and overly logical, but in person, Dr. Beck made it come to life. This ability to nurture curiosity was a special talent; his friend and fellow cognitive psychologist Donald Meichenbaum, PhD, recalls that even over lunch, he never stopped asking questions, personal and professional, on a wide range of topics.
It is widely accepted that Dr. Beck, who died Nov. 1 at the age of 100 in suburban Philadelphia, was the most important figure in the field of cognitive-behavioral therapy (CBT).
He didn’t invent the field. Behaviorism predated him by generations, founded by figures such as John Watson and B.F. Skinner. Those psychologists set up behaviorism as an alternative to the reigning power of Freudian psychoanalysis, but they ran a distant second.
It wasn’t until Dr. Beck added a new approach, cognitive therapy, to the behavioristic movement that the new mélange, CBT, began to gain traction with clinicians and researchers. Dr. Beck, who had trained in psychiatry, developed his ideas in the 1960s while observing what he believed were limitations in the classic Freudian methods. He recognized that patients had “automatic thoughts,” not just unconscious emotions, when they engaged in Freudian free association, saying whatever came to their minds.
These thoughts often distorted reality, he observed; they were “maladaptive beliefs,” and when they changed, patients’ emotional states improved.
Dr. Beck wasn’t alone. The psychologist Albert Ellis, PhD, in New York, had come to similar conclusions a decade earlier, though with a more coldly logical and challenging style. The prominent British psychologist Hans Eysenck, PhD, had argued strongly that Freudian psychoanalysis was ineffective and that behavioral approaches were better.
Dr. Beck turned the Freudian equation around: Instead of emotion as cause and thought as effect, it was thought which affected emotion, for better or worse. Once you connected behavior as the outcome, you had the essence of CBT: thought, emotion, and behavior – each affecting the other, with thought being the strongest axis of change.
The process wasn’t bloodless. Behaviorists defended their turf against cognitivists, just as much as Freudians rejected both. At one point the behaviorists in the Association for the Advancement of Behavior Therapy tried to expel the advocates of a cognitive approach. Dr. Beck responded by leading the cognitivists in creating a new journal; he emphasized the importance of research being the main mechanism to decide what treatments worked the best.
Putting these ideas out in the 1960s and 1970s, Dr. Beck garnered support from researchers when he manualized the approach. Freudian psychoanalysis was idiosyncratic; it was almost impossible to study empirically, because the therapist would be responding to the unpredictable dreams and memories of patients engaged in free association. Each case was unique.
But CBT was systematic: The same general approach was taken to all patients; the same negative cognitions were found in depression, for instance, like all-or-nothing thinking or overgeneralization. Once manualized, CBT became the standard method of psychotherapy studied with the newly developed method of randomized controlled trials (RCTs).
By the 1980s, RCTs had proven the efficacy of CBT in depression, and the approach took off.
Dr. Beck already had developed a series of rating scales: the Beck Depression Inventory, the Beck Scale for Suicidal Ideation, the Beck Anxiety Inventory, the Beck Hopelessness Scale. Widely used, these scales extended his influence enormously. Copyrighted, they created a new industry of psychological research.
Dr. Beck’s own work was mainly in depression, but his followers extended it everywhere else: anxiety disorders and phobias, eating disorders, substance abuse, bipolar illness, even schizophrenia. Meanwhile, Freudian psychoanalysis fell into a steep decline from which it never recovered.
Some argued that it was abetted by insurance restrictions on psychotherapy, which favored shorter-term CBT; others that its research was biased in its favor because psychotherapy treatments, unlike medications, cannot be blinded; others that its efficacy could not be shown to be specific to its theory, as opposed to the interpersonal relationship between therapist and client.
Still, CBT has transformed psychotherapy and continues to expand its influence. Computer-based CBT has been proven effective, and digital CBT has become a standard approach in many smartphone applications and is central to the claims of multiple new biotechnology companies advocating for digital psychotherapy.
Aaron Beck continued publishing scientific articles to age 98. His last papers reviewed his life’s work. He characteristically gave credit to others, calmly recollected how he traveled away from psychoanalysis, described how his work started and ended in schizophrenia, and noted that the “working relationship with the therapist” remained a key factor for the success of CBT.
That parting comment reminds us that behind all the technology and research stands the kindly man in the dark suit, white shirt, and bright red bow tie, looking at you warmly, asking about your thoughts, and curiously wondering what might be another explanation or viewpoint you hadn’t considered.
Nassir Ghaemi, MD, MPH, is a professor of psychiatry at Tufts Medical Center and a lecturer in psychiatry at Harvard Medical School. He is the author of several general-interest books on psychiatry. A version of this article first appeared on Medscape.com.
Twice exceptionality: A hidden diagnosis in primary care
THE CASE
Michael T,* a 20-year-old cisgender male, visited one of our clinic’s primary care physicians (PCPs). He was reserved and quiet and spoke of his concerns about depression and social anxiety that had been present for several years. He also spoke of his inability to succeed at work and school. Following a thorough PCP review leading to diagnoses of major depressive disorder and social anxiety, the patient agreed to try medication. Over a period of 15 months, trials of medications including fluoxetine, sertraline, aripiprazole, and duloxetine did little to improve the patient’s mood. The PCP decided to consult with our clinic’s integrated health team.
The team reviewed several diagnostic possibilities (TABLE 1) and agreed with the PCP’s diagnoses of major depression and social anxiety. But these disorders alone did not explain the full picture. Team members noted the patient’s unusual communication style, characterized by remarkably long response times and slow processing speed. In particular, when discussing mood, he took several seconds to respond but would respond thoughtfully and with few words.

We administered the Wechsler Adult Intelligence Scale (WAIS-IV). Due to differences between the 4 indices within the WAIS-IV, the Full Scale Intelligence Quotient may under- or overestimate abilities across domains; this was the case for this patient. His General Ability Index (GAI) score was 130, in the very superior range and at the 98th percentile, placing him in the category of gifted intelligence. The patient’s processing speed, however, was at the 18th percentile, which explained his delayed response style and presence of developmental asynchrony, a concept occasionally reported when interpreting socio-emotional and educational maladjustment in gifted individuals.
We determined that Mr. T was twice exceptional—intellectually gifted and also having one or more areas of disability.
●
* The patient’s name has been changed to protect his identity .
In individuals with gifted intelligence, a discrepancy between cognitive and emotional development can make them vulnerable to behavioral and emotional challenges. It is not uncommon for gifted individuals to experience co-occurring distress, anxiety, depression, social withdrawal, difficulty coping with challenging tasks and experiences, low self-esteem, and excessive perfectionism.1-6 Giftedness accompanied by a delay in general abilities and processing speed (significant verbal-performance discrepancy) places an individual in the category of twice-exceptionality, or “2E”—having the potential for high achievement while displaying evidence of 1 or more disabilities including emotional or behavioral difficulties.7
2E Individuals: Prevalence, characteristics, and outcomes
Reported prevalence of twice-exceptionality varies, from approximately 180,000 to 360,000 students in the United States.7 In 2009, the National Commission on Twice Exceptional Students provided the following definition of twice exceptionality:7,8
“Twice-exceptional learners are students who demonstrate the potential for high achievement or creative productivity in one or more domains such as math, science, technology, the social arts, the visual, spatial, or performing arts or other areas of human productivity AND who manifest one or more disabilities as defined by federal or state eligibility criteria. These disabilities include specific learning disabilities; speech and language disorders; emotional/behavioral disorders; physical disabilities; Autism Spectrum Disorders (ASD); or other health impairments, such as Attention Deficit/Hyperactivity Disorder (ADHD).”
How twice-exceptionality might manifest. The literature describes 3 unique groupings of 2E children: those who excel early due to strong language abilities, but later show signs of disability, often when curricular demands rise in junior high, high school, or even college; students diagnosed with disability, but who show exceptional gifts in some areas that may be masked by their learning difficulties; and highly intelligent students who seem to be average, because their disabilities mask their giftedness or their talents mask their difficulties.9,10
Unique behavioral and emotional challenges of 2E individuals may include lower motivation and academic self-efficacy, low self-worth and feelings of failure, or disruptive behaviors.7,11,12 Anxiety and depression often result from the functional impact of twice-exceptionality as well as resultant withdrawal, social isolation, and delay or hindrance of social skills (such as difficulty interpreting social cues).13,14 The individual in our case displayed many of these challenges, including lower motivation, self-worth, and self-esteem, and comorbid anxiety and depression (TABLE 1), further clouding diagnostic clarity.
Continue to: The need for improved recognition
The need for improved recognition. Twice-exceptionality commonly manifests as children reach grade-school age, but they are underrepresented in programs for the gifted due to misunderstanding and misdiagnosis by professionals.15,16 Best practices in identifying 2E children incorporate multidimensional assessments including pre-referral and screening, preliminary intervention, evaluation procedures, and educational planning.16 Despite research asserting that 2E individuals need more support services, knowing how to best identify and support individuals across various settings can prove difficult.7,17-19
Primary care, as we will discuss in a bit, is an interdisciplinary setting in which identification and comprehensive and collaborative support can occur. Historically, though, mental and physical health care have been “siloed” and mental health professionals’ functions in medical settings have often been circumscribed.20,21
A lesson from how our case unfolded
Our integrated health team, known as Integrated Behavioral Health Plus (IBH+), was developed at the University of Colorado School of Medicine, and is a system-level integration of behavioral health professionals working with medical providers to improve outcomes and satisfaction.22 Psychology supervisors and trainees, telepsychiatrists and psychiatry residents, social workers, and pharmacists work together with PCPs and residents to deliver comprehensive patient care. Our model includes a range of behavioral health access points for patients (TABLE 2) and the use of complex patient databases and care team meetings.
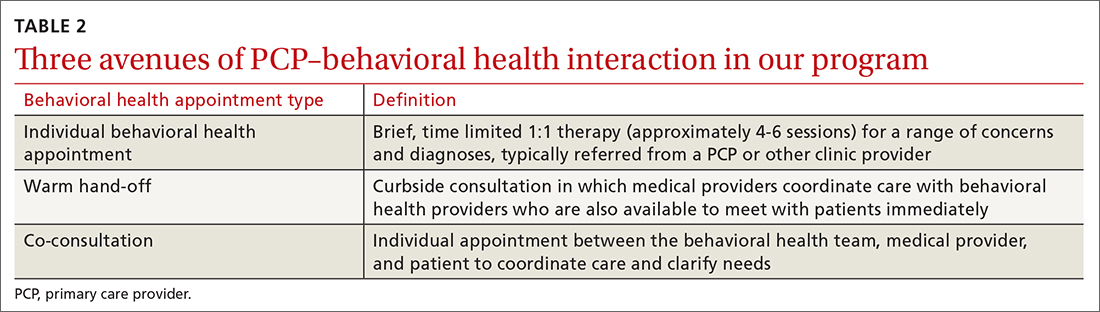
In the case we have described here, the nature of the patient’s presentation did not trigger any of the clinical procedures described in TABLE 2, and he fell under the radar of complex patient cases in the clinic. Instead, informal, asynchronous clinical conversations between providers were what eventually lead to diagnostic clarification. Team consultation and psychometric testing provided by IBH+ helped uncover the “hidden diagnosis” of this patient in primary care and identified him as twice-exceptional, experiencing both giftedness and significant emotional suffering (major depression and social anxiety, low self-esteem and self-worth).
Takeaways for primary care
Not all PCPs, of course, have immediate onsite access to a program such as ours. However, innovative ways to tap into available resources might include establishing a partnership with 1 or more behavioral health professionals or bridging less formal relationships with such providers in the community and schools to more easily share patient records.
Continue to: Other presentations within 2E populations
Other presentations within 2E populations. 2E individuals may have other presentations coupled with high cognitive ability7: symptoms of hyperactivity disorders; specific learning disabilities; a diagnosis of autism spectrum disorder (previously termed Asperger type); attention, organizational, social, and behavioral issues; and impulsivity or emotional volatility.
Of note, the perspective of our care team shifted from a “bugs and drugs” perspective of diagnosis and treatment—biological explanations and pharmaceutical solutions—to an approach that explored the underlying interplay between cognitive and emotional functioning for this individual. Our treatment focused on a strengths-based and patient-centered approach. Even without the resources of a full IBH+ model, primary care practices may be able to adapt our experience to their ever-growing complex populations.
Our team shifted treatment planning to the needs of the patient. The 2E identification changed the patient’s perspective about himself. After learning of his giftedness, the patient was able to reframe himself as a highly intelligent, capable individual in need of treatment for depression and social anxiety, as opposed to questioning his intelligence and experiencing confusion and hopelessness within the medical system. His PCP collaborated with the team via telecommunication to maintain an efficacious antidepressant plan and to use a strengths-based approach focused on increasing the patient’s self-view and changing the illness narrative. This narrative was changed by practicing skills, such as challenging unhelpful thought patterns, setting beneficial boundaries, and supporting assertive communication to oppose thoughts and relationships that perpetuated old, negative beliefs and assumptions.
CORRESPONDENCE
Kathryn S. Saldaña, PhD, University of Colorado, 12631 East 17th Avenue, AO1 L15, 3rd Floor, Aurora, CO 80045; kathryn. saldana@ucdenver.edu.
ACKNOWLEDGEMENTS
Our thanks to A.F. Williams Family Medicine Clinic and the University of Colorado Anschutz Medical Campus School of Medicine for their unparalleled models of resident training and multidisciplinary care.
1. Guénolé F, Louis J, Creveuil C, et al. Behavioral profiles of clinically referred children with intellectual giftedness. BioMed Res Int. 2013;2013:540153.
2. Alesi M, Rappo G, Pepi A. Emotional profile and intellectual functioning: A comparison among children with borderline intellectual functioning, average intellectual functioning, and gifted intellectual functioning. SAGE Open. 2015;5:2158244015589995.
3. Alsop G. Asynchrony: intuitively valid and theoretically reliable. Roeper Rev. 2003;25:118-127.
4. Guignard J-H, Jacquet A-Y, Lubart TI. Perfectionism and anxiety: a paradox in intellectual giftedness? PloS One. 2012;7:e41043.
5. Reis SM, McCoach DB. The underachievement of gifted students: What do we know and where do we go? Gifted Child Quarterly. 2000;44:152-170.
6. Barchmann H, Kinze W. Behaviour and achievement disorders in children with high intelligence. Acta Paedopsychiatr. 1990;53:168-172.
7. Reis SM, Baum SM, Burke E. An operational definition of twice-exceptional learners: implications and applications. Gifted Child Quarterly. 2014;58:217-230.
8. NAGC Position Statements & White Papers. Accessed September 18, 2021. http://www.nagc.org/index.aspx?id=5094
9. Neihart M. Identifying and providing services to twice exceptional children. In: Handbook of Giftedness in Children. Pfeiffer SI, ed. Springer; 2008:115-137.
10. Baum SM, Owen SV. To Be Gifted & Learning Disabled: Strategies for Helping Bright Students with Learning & Attention Difficulties. Prufrock Press Inc; 2004.
11. Reis SM. Talents in two places: case studies of high ability students with learning disabilities who have achieved. [Research Monograph 95114]. 1995.
12. Schiff MM, Kaufman AS, Kaufman NL. Scatter analysis of WISC-R profiles for learning disabled children with superior intelligence. J Learn Disabil. 1981;14:400-404.
13. King EW. Addressing the social and emotional needs of twice-exceptional students. Teaching Exceptional Child. 2005;38:16-21.
14. Stormont M, Stebbins MS, Holliday G. Characteristics and educational support needs of underrepresented gifted adolescents. Psychol Schools. 2001;38:413-423.
15. Morrison WF, Rizza MG. Creating a toolkit for identifying twice-exceptional students. J Educ Gifted. 2007;31:57-76.
16. Rizza MG, Morrison WF. Identifying twice exceptional children: a toolkit for success. Accessed September 17, 2021. https://files.eric.ed.gov/fulltext/EJ967126.pdf
17. Cohen SS, Vaughn S. Gifted students with learning disabilities: what does the research say? Learn Disabil. 1994;5:87-94.
18. National Center for Education Statistics. Students with disabilities. Accessed September 18, 2021. https://nces.ed.gov/programs/coe/indicator_cgg.asp
19. The Hechinger Report. Twice exceptional, doubly disadvantaged? How schools struggle to serve gifted students with disabilities. Accessed September 18, 2021. https://hechingerreport.org/twice-exceptional-doubly-disadvantaged-how-schools-struggle-to-serve-gifted-students-with-disabilities
20. Mendaglio S. Heightened multifaceted sensitivity of gifted students: implications for counseling. J Secondary Gifted Educ. 2002;14:72-82.
21. Pereles DA, Omdal S, Baldwin L. Response to intervention and twice-exceptional learners: a promising fit. Gifted Child Today. 2009;32:40-51.
22. Gerrity M. Evolving models of behavioral health integration: evidence update 2010-2015. Milbank Memorial Fund. 2016. Accessed September 18, 2021. www.milbank.org/wp-content/uploads/2016/05/Evolving-Models-of-BHI.pdf
THE CASE
Michael T,* a 20-year-old cisgender male, visited one of our clinic’s primary care physicians (PCPs). He was reserved and quiet and spoke of his concerns about depression and social anxiety that had been present for several years. He also spoke of his inability to succeed at work and school. Following a thorough PCP review leading to diagnoses of major depressive disorder and social anxiety, the patient agreed to try medication. Over a period of 15 months, trials of medications including fluoxetine, sertraline, aripiprazole, and duloxetine did little to improve the patient’s mood. The PCP decided to consult with our clinic’s integrated health team.
The team reviewed several diagnostic possibilities (TABLE 1) and agreed with the PCP’s diagnoses of major depression and social anxiety. But these disorders alone did not explain the full picture. Team members noted the patient’s unusual communication style, characterized by remarkably long response times and slow processing speed. In particular, when discussing mood, he took several seconds to respond but would respond thoughtfully and with few words.
We administered the Wechsler Adult Intelligence Scale (WAIS-IV). Due to differences between the 4 indices within the WAIS-IV, the Full Scale Intelligence Quotient may under- or overestimate abilities across domains; this was the case for this patient. His General Ability Index (GAI) score was 130, in the very superior range and at the 98th percentile, placing him in the category of gifted intelligence. The patient’s processing speed, however, was at the 18th percentile, which explained his delayed response style and presence of developmental asynchrony, a concept occasionally reported when interpreting socio-emotional and educational maladjustment in gifted individuals.
We determined that Mr. T was twice exceptional—intellectually gifted and also having one or more areas of disability.
●
* The patient’s name has been changed to protect his identity .
In individuals with gifted intelligence, a discrepancy between cognitive and emotional development can make them vulnerable to behavioral and emotional challenges. It is not uncommon for gifted individuals to experience co-occurring distress, anxiety, depression, social withdrawal, difficulty coping with challenging tasks and experiences, low self-esteem, and excessive perfectionism.1-6 Giftedness accompanied by a delay in general abilities and processing speed (significant verbal-performance discrepancy) places an individual in the category of twice-exceptionality, or “2E”—having the potential for high achievement while displaying evidence of 1 or more disabilities including emotional or behavioral difficulties.7
2E Individuals: Prevalence, characteristics, and outcomes
Reported prevalence of twice-exceptionality varies, from approximately 180,000 to 360,000 students in the United States.7 In 2009, the National Commission on Twice Exceptional Students provided the following definition of twice exceptionality:7,8
“Twice-exceptional learners are students who demonstrate the potential for high achievement or creative productivity in one or more domains such as math, science, technology, the social arts, the visual, spatial, or performing arts or other areas of human productivity AND who manifest one or more disabilities as defined by federal or state eligibility criteria. These disabilities include specific learning disabilities; speech and language disorders; emotional/behavioral disorders; physical disabilities; Autism Spectrum Disorders (ASD); or other health impairments, such as Attention Deficit/Hyperactivity Disorder (ADHD).”
How twice-exceptionality might manifest. The literature describes 3 unique groupings of 2E children: those who excel early due to strong language abilities, but later show signs of disability, often when curricular demands rise in junior high, high school, or even college; students diagnosed with disability, but who show exceptional gifts in some areas that may be masked by their learning difficulties; and highly intelligent students who seem to be average, because their disabilities mask their giftedness or their talents mask their difficulties.9,10
Unique behavioral and emotional challenges of 2E individuals may include lower motivation and academic self-efficacy, low self-worth and feelings of failure, or disruptive behaviors.7,11,12 Anxiety and depression often result from the functional impact of twice-exceptionality as well as resultant withdrawal, social isolation, and delay or hindrance of social skills (such as difficulty interpreting social cues).13,14 The individual in our case displayed many of these challenges, including lower motivation, self-worth, and self-esteem, and comorbid anxiety and depression (TABLE 1), further clouding diagnostic clarity.
Continue to: The need for improved recognition
The need for improved recognition. Twice-exceptionality commonly manifests as children reach grade-school age, but they are underrepresented in programs for the gifted due to misunderstanding and misdiagnosis by professionals.15,16 Best practices in identifying 2E children incorporate multidimensional assessments including pre-referral and screening, preliminary intervention, evaluation procedures, and educational planning.16 Despite research asserting that 2E individuals need more support services, knowing how to best identify and support individuals across various settings can prove difficult.7,17-19
Primary care, as we will discuss in a bit, is an interdisciplinary setting in which identification and comprehensive and collaborative support can occur. Historically, though, mental and physical health care have been “siloed” and mental health professionals’ functions in medical settings have often been circumscribed.20,21
A lesson from how our case unfolded
Our integrated health team, known as Integrated Behavioral Health Plus (IBH+), was developed at the University of Colorado School of Medicine, and is a system-level integration of behavioral health professionals working with medical providers to improve outcomes and satisfaction.22 Psychology supervisors and trainees, telepsychiatrists and psychiatry residents, social workers, and pharmacists work together with PCPs and residents to deliver comprehensive patient care. Our model includes a range of behavioral health access points for patients (TABLE 2) and the use of complex patient databases and care team meetings.
In the case we have described here, the nature of the patient’s presentation did not trigger any of the clinical procedures described in TABLE 2, and he fell under the radar of complex patient cases in the clinic. Instead, informal, asynchronous clinical conversations between providers were what eventually lead to diagnostic clarification. Team consultation and psychometric testing provided by IBH+ helped uncover the “hidden diagnosis” of this patient in primary care and identified him as twice-exceptional, experiencing both giftedness and significant emotional suffering (major depression and social anxiety, low self-esteem and self-worth).
Takeaways for primary care
Not all PCPs, of course, have immediate onsite access to a program such as ours. However, innovative ways to tap into available resources might include establishing a partnership with 1 or more behavioral health professionals or bridging less formal relationships with such providers in the community and schools to more easily share patient records.
Continue to: Other presentations within 2E populations
Other presentations within 2E populations. 2E individuals may have other presentations coupled with high cognitive ability7: symptoms of hyperactivity disorders; specific learning disabilities; a diagnosis of autism spectrum disorder (previously termed Asperger type); attention, organizational, social, and behavioral issues; and impulsivity or emotional volatility.
Of note, the perspective of our care team shifted from a “bugs and drugs” perspective of diagnosis and treatment—biological explanations and pharmaceutical solutions—to an approach that explored the underlying interplay between cognitive and emotional functioning for this individual. Our treatment focused on a strengths-based and patient-centered approach. Even without the resources of a full IBH+ model, primary care practices may be able to adapt our experience to their ever-growing complex populations.
Our team shifted treatment planning to the needs of the patient. The 2E identification changed the patient’s perspective about himself. After learning of his giftedness, the patient was able to reframe himself as a highly intelligent, capable individual in need of treatment for depression and social anxiety, as opposed to questioning his intelligence and experiencing confusion and hopelessness within the medical system. His PCP collaborated with the team via telecommunication to maintain an efficacious antidepressant plan and to use a strengths-based approach focused on increasing the patient’s self-view and changing the illness narrative. This narrative was changed by practicing skills, such as challenging unhelpful thought patterns, setting beneficial boundaries, and supporting assertive communication to oppose thoughts and relationships that perpetuated old, negative beliefs and assumptions.
CORRESPONDENCE
Kathryn S. Saldaña, PhD, University of Colorado, 12631 East 17th Avenue, AO1 L15, 3rd Floor, Aurora, CO 80045; kathryn. saldana@ucdenver.edu.
ACKNOWLEDGEMENTS
Our thanks to A.F. Williams Family Medicine Clinic and the University of Colorado Anschutz Medical Campus School of Medicine for their unparalleled models of resident training and multidisciplinary care.
THE CASE
Michael T,* a 20-year-old cisgender male, visited one of our clinic’s primary care physicians (PCPs). He was reserved and quiet and spoke of his concerns about depression and social anxiety that had been present for several years. He also spoke of his inability to succeed at work and school. Following a thorough PCP review leading to diagnoses of major depressive disorder and social anxiety, the patient agreed to try medication. Over a period of 15 months, trials of medications including fluoxetine, sertraline, aripiprazole, and duloxetine did little to improve the patient’s mood. The PCP decided to consult with our clinic’s integrated health team.
The team reviewed several diagnostic possibilities (TABLE 1) and agreed with the PCP’s diagnoses of major depression and social anxiety. But these disorders alone did not explain the full picture. Team members noted the patient’s unusual communication style, characterized by remarkably long response times and slow processing speed. In particular, when discussing mood, he took several seconds to respond but would respond thoughtfully and with few words.
We administered the Wechsler Adult Intelligence Scale (WAIS-IV). Due to differences between the 4 indices within the WAIS-IV, the Full Scale Intelligence Quotient may under- or overestimate abilities across domains; this was the case for this patient. His General Ability Index (GAI) score was 130, in the very superior range and at the 98th percentile, placing him in the category of gifted intelligence. The patient’s processing speed, however, was at the 18th percentile, which explained his delayed response style and presence of developmental asynchrony, a concept occasionally reported when interpreting socio-emotional and educational maladjustment in gifted individuals.
We determined that Mr. T was twice exceptional—intellectually gifted and also having one or more areas of disability.
●
* The patient’s name has been changed to protect his identity .
In individuals with gifted intelligence, a discrepancy between cognitive and emotional development can make them vulnerable to behavioral and emotional challenges. It is not uncommon for gifted individuals to experience co-occurring distress, anxiety, depression, social withdrawal, difficulty coping with challenging tasks and experiences, low self-esteem, and excessive perfectionism.1-6 Giftedness accompanied by a delay in general abilities and processing speed (significant verbal-performance discrepancy) places an individual in the category of twice-exceptionality, or “2E”—having the potential for high achievement while displaying evidence of 1 or more disabilities including emotional or behavioral difficulties.7
2E Individuals: Prevalence, characteristics, and outcomes
Reported prevalence of twice-exceptionality varies, from approximately 180,000 to 360,000 students in the United States.7 In 2009, the National Commission on Twice Exceptional Students provided the following definition of twice exceptionality:7,8
“Twice-exceptional learners are students who demonstrate the potential for high achievement or creative productivity in one or more domains such as math, science, technology, the social arts, the visual, spatial, or performing arts or other areas of human productivity AND who manifest one or more disabilities as defined by federal or state eligibility criteria. These disabilities include specific learning disabilities; speech and language disorders; emotional/behavioral disorders; physical disabilities; Autism Spectrum Disorders (ASD); or other health impairments, such as Attention Deficit/Hyperactivity Disorder (ADHD).”
How twice-exceptionality might manifest. The literature describes 3 unique groupings of 2E children: those who excel early due to strong language abilities, but later show signs of disability, often when curricular demands rise in junior high, high school, or even college; students diagnosed with disability, but who show exceptional gifts in some areas that may be masked by their learning difficulties; and highly intelligent students who seem to be average, because their disabilities mask their giftedness or their talents mask their difficulties.9,10
Unique behavioral and emotional challenges of 2E individuals may include lower motivation and academic self-efficacy, low self-worth and feelings of failure, or disruptive behaviors.7,11,12 Anxiety and depression often result from the functional impact of twice-exceptionality as well as resultant withdrawal, social isolation, and delay or hindrance of social skills (such as difficulty interpreting social cues).13,14 The individual in our case displayed many of these challenges, including lower motivation, self-worth, and self-esteem, and comorbid anxiety and depression (TABLE 1), further clouding diagnostic clarity.
Continue to: The need for improved recognition
The need for improved recognition. Twice-exceptionality commonly manifests as children reach grade-school age, but they are underrepresented in programs for the gifted due to misunderstanding and misdiagnosis by professionals.15,16 Best practices in identifying 2E children incorporate multidimensional assessments including pre-referral and screening, preliminary intervention, evaluation procedures, and educational planning.16 Despite research asserting that 2E individuals need more support services, knowing how to best identify and support individuals across various settings can prove difficult.7,17-19
Primary care, as we will discuss in a bit, is an interdisciplinary setting in which identification and comprehensive and collaborative support can occur. Historically, though, mental and physical health care have been “siloed” and mental health professionals’ functions in medical settings have often been circumscribed.20,21
A lesson from how our case unfolded
Our integrated health team, known as Integrated Behavioral Health Plus (IBH+), was developed at the University of Colorado School of Medicine, and is a system-level integration of behavioral health professionals working with medical providers to improve outcomes and satisfaction.22 Psychology supervisors and trainees, telepsychiatrists and psychiatry residents, social workers, and pharmacists work together with PCPs and residents to deliver comprehensive patient care. Our model includes a range of behavioral health access points for patients (TABLE 2) and the use of complex patient databases and care team meetings.
In the case we have described here, the nature of the patient’s presentation did not trigger any of the clinical procedures described in TABLE 2, and he fell under the radar of complex patient cases in the clinic. Instead, informal, asynchronous clinical conversations between providers were what eventually lead to diagnostic clarification. Team consultation and psychometric testing provided by IBH+ helped uncover the “hidden diagnosis” of this patient in primary care and identified him as twice-exceptional, experiencing both giftedness and significant emotional suffering (major depression and social anxiety, low self-esteem and self-worth).
Takeaways for primary care
Not all PCPs, of course, have immediate onsite access to a program such as ours. However, innovative ways to tap into available resources might include establishing a partnership with 1 or more behavioral health professionals or bridging less formal relationships with such providers in the community and schools to more easily share patient records.
Continue to: Other presentations within 2E populations
Other presentations within 2E populations. 2E individuals may have other presentations coupled with high cognitive ability7: symptoms of hyperactivity disorders; specific learning disabilities; a diagnosis of autism spectrum disorder (previously termed Asperger type); attention, organizational, social, and behavioral issues; and impulsivity or emotional volatility.
Of note, the perspective of our care team shifted from a “bugs and drugs” perspective of diagnosis and treatment—biological explanations and pharmaceutical solutions—to an approach that explored the underlying interplay between cognitive and emotional functioning for this individual. Our treatment focused on a strengths-based and patient-centered approach. Even without the resources of a full IBH+ model, primary care practices may be able to adapt our experience to their ever-growing complex populations.
Our team shifted treatment planning to the needs of the patient. The 2E identification changed the patient’s perspective about himself. After learning of his giftedness, the patient was able to reframe himself as a highly intelligent, capable individual in need of treatment for depression and social anxiety, as opposed to questioning his intelligence and experiencing confusion and hopelessness within the medical system. His PCP collaborated with the team via telecommunication to maintain an efficacious antidepressant plan and to use a strengths-based approach focused on increasing the patient’s self-view and changing the illness narrative. This narrative was changed by practicing skills, such as challenging unhelpful thought patterns, setting beneficial boundaries, and supporting assertive communication to oppose thoughts and relationships that perpetuated old, negative beliefs and assumptions.
CORRESPONDENCE
Kathryn S. Saldaña, PhD, University of Colorado, 12631 East 17th Avenue, AO1 L15, 3rd Floor, Aurora, CO 80045; kathryn. saldana@ucdenver.edu.
ACKNOWLEDGEMENTS
Our thanks to A.F. Williams Family Medicine Clinic and the University of Colorado Anschutz Medical Campus School of Medicine for their unparalleled models of resident training and multidisciplinary care.
1. Guénolé F, Louis J, Creveuil C, et al. Behavioral profiles of clinically referred children with intellectual giftedness. BioMed Res Int. 2013;2013:540153.
2. Alesi M, Rappo G, Pepi A. Emotional profile and intellectual functioning: A comparison among children with borderline intellectual functioning, average intellectual functioning, and gifted intellectual functioning. SAGE Open. 2015;5:2158244015589995.
3. Alsop G. Asynchrony: intuitively valid and theoretically reliable. Roeper Rev. 2003;25:118-127.
4. Guignard J-H, Jacquet A-Y, Lubart TI. Perfectionism and anxiety: a paradox in intellectual giftedness? PloS One. 2012;7:e41043.
5. Reis SM, McCoach DB. The underachievement of gifted students: What do we know and where do we go? Gifted Child Quarterly. 2000;44:152-170.
6. Barchmann H, Kinze W. Behaviour and achievement disorders in children with high intelligence. Acta Paedopsychiatr. 1990;53:168-172.
7. Reis SM, Baum SM, Burke E. An operational definition of twice-exceptional learners: implications and applications. Gifted Child Quarterly. 2014;58:217-230.
8. NAGC Position Statements & White Papers. Accessed September 18, 2021. http://www.nagc.org/index.aspx?id=5094
9. Neihart M. Identifying and providing services to twice exceptional children. In: Handbook of Giftedness in Children. Pfeiffer SI, ed. Springer; 2008:115-137.
10. Baum SM, Owen SV. To Be Gifted & Learning Disabled: Strategies for Helping Bright Students with Learning & Attention Difficulties. Prufrock Press Inc; 2004.
11. Reis SM. Talents in two places: case studies of high ability students with learning disabilities who have achieved. [Research Monograph 95114]. 1995.
12. Schiff MM, Kaufman AS, Kaufman NL. Scatter analysis of WISC-R profiles for learning disabled children with superior intelligence. J Learn Disabil. 1981;14:400-404.
13. King EW. Addressing the social and emotional needs of twice-exceptional students. Teaching Exceptional Child. 2005;38:16-21.
14. Stormont M, Stebbins MS, Holliday G. Characteristics and educational support needs of underrepresented gifted adolescents. Psychol Schools. 2001;38:413-423.
15. Morrison WF, Rizza MG. Creating a toolkit for identifying twice-exceptional students. J Educ Gifted. 2007;31:57-76.
16. Rizza MG, Morrison WF. Identifying twice exceptional children: a toolkit for success. Accessed September 17, 2021. https://files.eric.ed.gov/fulltext/EJ967126.pdf
17. Cohen SS, Vaughn S. Gifted students with learning disabilities: what does the research say? Learn Disabil. 1994;5:87-94.
18. National Center for Education Statistics. Students with disabilities. Accessed September 18, 2021. https://nces.ed.gov/programs/coe/indicator_cgg.asp
19. The Hechinger Report. Twice exceptional, doubly disadvantaged? How schools struggle to serve gifted students with disabilities. Accessed September 18, 2021. https://hechingerreport.org/twice-exceptional-doubly-disadvantaged-how-schools-struggle-to-serve-gifted-students-with-disabilities
20. Mendaglio S. Heightened multifaceted sensitivity of gifted students: implications for counseling. J Secondary Gifted Educ. 2002;14:72-82.
21. Pereles DA, Omdal S, Baldwin L. Response to intervention and twice-exceptional learners: a promising fit. Gifted Child Today. 2009;32:40-51.
22. Gerrity M. Evolving models of behavioral health integration: evidence update 2010-2015. Milbank Memorial Fund. 2016. Accessed September 18, 2021. www.milbank.org/wp-content/uploads/2016/05/Evolving-Models-of-BHI.pdf
1. Guénolé F, Louis J, Creveuil C, et al. Behavioral profiles of clinically referred children with intellectual giftedness. BioMed Res Int. 2013;2013:540153.
2. Alesi M, Rappo G, Pepi A. Emotional profile and intellectual functioning: A comparison among children with borderline intellectual functioning, average intellectual functioning, and gifted intellectual functioning. SAGE Open. 2015;5:2158244015589995.
3. Alsop G. Asynchrony: intuitively valid and theoretically reliable. Roeper Rev. 2003;25:118-127.
4. Guignard J-H, Jacquet A-Y, Lubart TI. Perfectionism and anxiety: a paradox in intellectual giftedness? PloS One. 2012;7:e41043.
5. Reis SM, McCoach DB. The underachievement of gifted students: What do we know and where do we go? Gifted Child Quarterly. 2000;44:152-170.
6. Barchmann H, Kinze W. Behaviour and achievement disorders in children with high intelligence. Acta Paedopsychiatr. 1990;53:168-172.
7. Reis SM, Baum SM, Burke E. An operational definition of twice-exceptional learners: implications and applications. Gifted Child Quarterly. 2014;58:217-230.
8. NAGC Position Statements & White Papers. Accessed September 18, 2021. http://www.nagc.org/index.aspx?id=5094
9. Neihart M. Identifying and providing services to twice exceptional children. In: Handbook of Giftedness in Children. Pfeiffer SI, ed. Springer; 2008:115-137.
10. Baum SM, Owen SV. To Be Gifted & Learning Disabled: Strategies for Helping Bright Students with Learning & Attention Difficulties. Prufrock Press Inc; 2004.
11. Reis SM. Talents in two places: case studies of high ability students with learning disabilities who have achieved. [Research Monograph 95114]. 1995.
12. Schiff MM, Kaufman AS, Kaufman NL. Scatter analysis of WISC-R profiles for learning disabled children with superior intelligence. J Learn Disabil. 1981;14:400-404.
13. King EW. Addressing the social and emotional needs of twice-exceptional students. Teaching Exceptional Child. 2005;38:16-21.
14. Stormont M, Stebbins MS, Holliday G. Characteristics and educational support needs of underrepresented gifted adolescents. Psychol Schools. 2001;38:413-423.
15. Morrison WF, Rizza MG. Creating a toolkit for identifying twice-exceptional students. J Educ Gifted. 2007;31:57-76.
16. Rizza MG, Morrison WF. Identifying twice exceptional children: a toolkit for success. Accessed September 17, 2021. https://files.eric.ed.gov/fulltext/EJ967126.pdf
17. Cohen SS, Vaughn S. Gifted students with learning disabilities: what does the research say? Learn Disabil. 1994;5:87-94.
18. National Center for Education Statistics. Students with disabilities. Accessed September 18, 2021. https://nces.ed.gov/programs/coe/indicator_cgg.asp
19. The Hechinger Report. Twice exceptional, doubly disadvantaged? How schools struggle to serve gifted students with disabilities. Accessed September 18, 2021. https://hechingerreport.org/twice-exceptional-doubly-disadvantaged-how-schools-struggle-to-serve-gifted-students-with-disabilities
20. Mendaglio S. Heightened multifaceted sensitivity of gifted students: implications for counseling. J Secondary Gifted Educ. 2002;14:72-82.
21. Pereles DA, Omdal S, Baldwin L. Response to intervention and twice-exceptional learners: a promising fit. Gifted Child Today. 2009;32:40-51.
22. Gerrity M. Evolving models of behavioral health integration: evidence update 2010-2015. Milbank Memorial Fund. 2016. Accessed September 18, 2021. www.milbank.org/wp-content/uploads/2016/05/Evolving-Models-of-BHI.pdf

Unmasking Our Grief
Since the start of the pandemic, health care systems have requested many in-services for staff on self-care and stress management to help health care workers (HCWs) cope with the heavy toll of COVID-19. The pandemic has set off a global mental health crisis, with unprecedented numbers of individuals meeting criteria for anxiety, depression, and other mental health disorders in response to the intense stressors of living through a pandemic. These calls to assist staff with self-care and burnout prevention have been especially salient for psychologists working in palliative care and geriatrics, where fears of COVID-19 infection and numbers of patient deaths have been high.
Throughout these painful times, we have been grateful for an online community of palliative care psychologists within the US Department of Veterans Affairs (VA) from across the continuum of care and across the country. This community brought together many of us who were both struggling ourselves and striving to support the teams and HCWs around us. We are psychologists who provide home-care services in North Carolina, inpatient hospice and long-term care services in California, and long-term care and outpatient palliative care services in Massachusetts. Through our shared struggles and challenges navigating the pandemic, we realized that our respective teams requested similar services, all focused on staff support.
The psychological impact of COVID-19 on HCWs was clear from the beginning. Early in the pandemic our respective teams requested us to provide staff support and education about coping to our local HCWs. Soon national groups for long-term care staff requested education programs. Through this work, we realized that the emotional needs of HCWs ran much deeper than simple self-care. At the onset of the pandemic, before realizing its chronicity, the trainings we offered focused on stress and coping strategies. We cited several frameworks for staff support and eagerly shared anything that might help us, and our colleagues, survive the immediate anxiety and tumult surrounding us.1-3 In this paper, we briefly discuss the distress affecting the geriatric care workforce, reflect on our efforts to cope as HCWs, and offer recommendations at individual and organization levels to help address our collective grief.
Impact of COVID-19
As the death toll mounted and hospitals were pushed to the brink, we saw the suffering of our fellow HCWs. The lack of personal protective equipment (PPE) and testing supplies led to evolving and increasing anxiety for HCWs about contracting COVID-19, potentially spreading it to one’s social circle or family, fears of becoming sick and dying, and fears of inadvertently spreading the virus to medically-vulnerable patients. Increasing demands on staff required many to work outside their areas of expertise. Clinical practice guidelines changed frequently as information emerged about the virus. Staff members struggled to keep pace with the increasing number of patients, many of whom died despite heroic efforts to save them.
As the medical crisis grew, so too did social uprisings as the general public gained a strengthened awareness of the legacy and ongoing effects of systemic oppression, racism, and social inequities in the United States. Individuals grappled with their own privileges, which often hid such disparities from view. Many HCWs and clinicians of color had to navigate unsolicited questions and discussions about racial injustices while also trying to survive. As psychologists, we strove to support the HCWs around us while also struggling with our own stressors. As the magnitude of the pandemic and ongoing social injustices came into view, we realized that presentations on self-care and burnout prevention did not suffice. We needed discussions on unmasking our grief, acknowledging our traumas, and working toward collective healing.
Geriatric Care Workers
Experiences of grief and trauma hit the geriatric care workforce and especially long-term care facilities particularly hard given the high morbidity and mortality rates of COVID-19.4 The geriatric care workforce itself suffers from institutional vulnerabilities. Individuals are often underpaid, undertrained, and work within a system that continually experiences staffing shortages, high burnout, and consequently high levels of turnover.5,6 Recent immigrants and racial/ethnic minorities disproportionately make up this workforce, who often live in multigenerational households and work in multiple facilities to get by.7,8 Amid the pandemic these HCWs continued to work despite demoralizing negative media coverage of nursing homes.9 Notably, facilities with unionized staff were less likely to need second or third jobs to survive, thus reducing spread across facilities. This along with better access to PPE may have contributed to their lower COVID-19 infection and mortality rates relative to non-unionized staff.10
Similar to long-term care workers, home-care staff had related fears and anxieties, magnified by the need to enter multiple homes. This often overlooked but growing sector of the geriatric care workforce faced the added anxiety of the unknown as they entered multiple homes to provide care to their patients. These staff have little control over who may be in the home when they arrive, the sanitation/PPE practices of the patient/family, and therefore little control over their potential exposure to COVID-19. This also applies to home health aides who, although not providing medical services, are a critical part of home-care services and allow older adults to remain living independently in their home.
Reflection on Grief
As we witnessed the interactive effects of the pandemic and social inequities in geriatrics and palliative care, we frequently sought solace in online communities of psychologists working in similar settings. Over time, our regular community meetings developed a different tone: discussions about caring for others shifted to caring for ourselves. It seemed that in holding others’ pain, many of us neglected to address our own. We needed emotional support. We needed to acknowledge that we were not all okay; that the masks we wear for protection also reveal our vulnerabilities; and that protective equipment in hospitals do not protect us from the hate and bias targeting many of us face everywhere we go.
As we let ourselves be vulnerable with each other, we saw the true face of our pain: it was not stress, it was grief. We were sad, broken, mourning innumerable losses, and grieving, mostly alone. It felt overwhelming. Our minds and hearts often grew numb to find respite from pain. At times we found ourselves seeking haven in our offices, convincing ourselves that paperwork needed to be done when in reality we had no space to hold anyone else’s pain; we could barely contain our own. We could only take so much.
Without space to process, grief festers and eats away at our remaining compassion. How do we hold grace for ourselves, dare to be vulnerable, and allow ourselves to feel, when doing so opens the door to our own grief? How do we allow room for emotional processing when we learned to numb-out in order to function? And as women with diverse intersectional identities, how do we honor our humanity when we live in a society that reflects its indifference? We needed to process our pain in order to heal in the slow and uneven way that grief heals.
Caring During Tough Times
The pain we feel is real and it tears at us over time. Pushing it away disenfranchises ourselves of the opportunity to heal and grow. Our collective grief and trauma demand collective healing and acknowledgment of our individual suffering. We must honor our shared humanity and find commonality amid our differences. Typical self-care (healthy eating, sleep, basic hygiene) may not be enough to mitigate the enormity of these stressors. A glass of wine or a virtual dinner with friends may distract but does not heal our wounds.
Self-care, by definition, centers the self and ignores the larger systemic factors that maintain our struggles. It keeps the focus on the individual and in so doing, risks inducing self-blame should we continue feeling burnout. We must do more. We can advocate that systems acknowledge our grief and suffering as well as our strengths and resiliencies. We can demand that organizations recognize human limits and provide support, rather than promote environments that encourage silent perseverance. And we can deconstruct the cultural narrative that vulnerability is weakness or that we are the “heroes.” Heroism suggests superhuman qualities or extreme courage and often negates the fear and trepidation in its midst.11,12 We can also recognize how intersectional aspects of our identities make navigating the pandemic and systemic racism harder and more dangerous for some than for others.
As noted by President Biden in a speech honoring those lost to COVID-19, “We have to resist becoming numb to the sorrow.”13 The nature of our work (and that of most clinicians) is that it is expected and sometimes necessary to compartmentalize and turn off the emotions so that we can function in a professional manner. But this way of being also serves to hold us back. It does not make space for the very real emotions of trauma and grief that have pervaded HCWs during this pandemic. We must learn a different way of functioning—one where grief is acknowledged and even actively processed while still going about our work. Grief therapist Megan Devine proposes to “tend to pain and grief by bearing witness” and notes that “when we allow the reality of grief to exist, we can focus on helping ourselves—and one another—survive inside pain.”14 She advocates for self-compassion and directs us to “find ways to show our grief to others, in ways that honor the truth of our experience” saying, “we have to be willing to stop diminishing our own pain so that others can be comfortable around us.” But what does this look like among health care teams who are traumatized and grieving?
In our experience, caring for ourselves and our teams in times of prolonged stress, trauma, and grief is essential to maintain functioning over time. We strongly believe that it must occur at both the organizational and individual levels. In the throes of a crisis, teams need support immediately. To offer a timely response, we gathered knowledge of team-based care and collaboration to develop practical strategies that can be implemented swiftly to provide support across the team.15-19
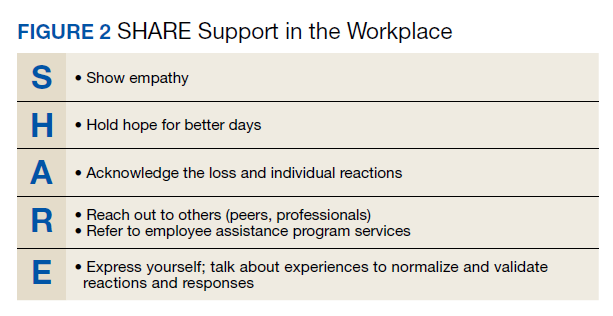
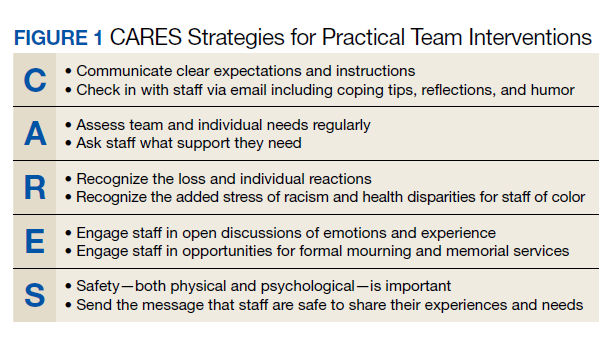
The strategies we developed offer steps for creating and maintaining a supportive, compassionate, and psychologically safe work environment. First, the CARES Strategies for Practical Team Intervention highlights the importance of clear communication, assessing team needs regularly, recognizing the stress that is occurring, engaging staff in discussions, and ensuring psychological safety and comfort (Figure 1). Next, the SHARE approach is laid out to allow for interpersonal support among team members (Figure 2). Showing each other empathy, hoping for better days, acknowledging each other’s pain, reaching out for assistance, and expressing our needs allow HCWs to open up about their grief, stress, and trauma. Of note, we found these sets of strategies interdependent: a team that does not believe the leader/organization CARES is not likely to SHARE. Therefore, we also feel that it is especially important that team leaders work to create or enhance the sense of psychological safety for the team. If team members do not feel safe, they will not disclose their grief and remain stuck in the old mode of suffering in silence.
Conclusions
This pandemic and the collective efforts toward social justice advocacy have revealed our vulnerabilities as well as our strengths. These experiences have forced us to reckon with our past and consider possible futures. It has revealed the inequities in our health care system, including our failure to protect those on the ground who keep our systems running, and prompted us to consider new ways of operating in low-resourced and high-demand environments. These experiences also present us with opportunities to be better and do better as both professionals and people; to reflect on our past and consider what we want different in our lives. As we yearn for better days and brace ourselves for what is to come, we hope that teams and organizations will take advantage of these opportunities for self-reflection and continue unmasking our grief, healing our wounds, and honoring our shared humanity.
1. Blake H, Bermingham F. Psychological wellbeing for health care workers: mitigating the impact of covid-19. Version 2.0. Updated June 18, 2020. Accessed October 12, 2021. https://www.nottingham.ac.uk/toolkits/play_22794
2. Harris R. FACE COVID: how to respond effectively to the corona crisis. Published 2020. Accessed October 12, 2021. http://louisville.edu/counseling/coping-with-covid-19/face-covid-by-dr-russ-harris/view
3. Norcross JC, Phillips CM. Psychologist self-care during the pandemic: now more than ever [published online ahead of print, 2020 May 2]. J Health Serv Psychol. 2020;1-5. doi:10.1007/s42843-020-00010-5
4. Kaiser Family Foundation. State reports of long-term care facility cases and deaths related to COVID-19. 2020. Published April 23, 2020. Accessed October 12, 2021. https://www.kff.org/coronavirus-covid-19/issue-brief/state-reporting-of-cases-and-deaths-due-to-covid-19-in-long-term-care-facilities
5. Sterling MR, Tseng E, Poon A, et al. Experiences of home health care workers in New York City during the coronavirus disease 2019 pandemic: a qualitative analysis. JAMA Intern Med. 2020;180(11):1453-1459. doi:10.1001/jamainternmed.2020.3930
6. Stone R, Wilhelm J, Bishop CE, Bryant NS, Hermer L, Squillace MR. Predictors of intent to leave the job among home health workers: analysis of the National Home Health Aide Survey. Gerontologist. 2017;57(5):890-899. doi:10.1093/geront/gnw075
7. Scales K. It’s time to care: a detailed profile of America’s direct care workforce. PHI. 2020. Published January 21, 2020. Accessed October 12, 2021. https://phinational.org/wp-content/uploads/2020/01/Its-Time-to-Care-2020-PHI.pdf
8. Wolfe R, Harknett K, Schneider D. Inequities at work and the toll of COVID-19. Health Aff Health Policy Brief. Published June 4, 2021. doi: 10.1377/hpb20210428.863621
9. White EM, Wetle TF, Reddy A, Baier RR. Front-line nursing home staff experiences during the COVID-19 pandemic [published correction appears in J Am Med Dir Assoc. 2021 May;22(5):1123]. J Am Med Dir Assoc. 2021;22(1):199-203. doi:10.1016/j.jamda.2020.11.022
10. Dean A, Venkataramani A, Kimmel S. Mortality rates from COVID-19 are lower In unionized nursing homes. Health Aff (Millwood). 2020;39(11):1993-2001.doi:10.1377/hlthaff.2020.01011
11. Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. 2020;46(8):510-513. doi:10.1136/medethics-2020-106398
12. Stokes-Parish J, Elliott R, Rolls K, Massey D. Angels and heroes: the unintended consequence of the hero narrative. J Nurs Scholarsh. 2020;52(5):462-466. doi:10.1111/jnu.12591
13. Biden J. Remarks by President Biden on the more than 500,000 American lives lost to COVID-19. Published February 22, 2021. Accessed October 12, 2021. https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/02/22/remarks-by-president-biden-on-the-more-than-500000-american-lives-lost-to-covid-19
14. Devine M. It’s Okay That You’re Not Okay: Meeting Grief and Loss in a Culture That Doesn’t Understand. Sounds True; 2017.
15. Center for the Study of Traumatic Stress. Grief leadership during COVID-19. Accessed October 12, 2021. https://www.cstsonline.org/assets/media/documents/CSTS_FS_Grief_Leadership_During_COVID19.pdf
16. Center for the Study of Traumatic Stress. Sustaining the well-being of healthcare personnel during coronavirus and other infectious disease outbreaks. Accessed October 12, 2021. https://www.cstsonline.org/assets/media/documents/CSTS_FS_Sustaining_Well_Being_Health care_Personnel_during.pdf
17. Fessell D, Cherniss C. Coronavirus disease 2019 (COVID-19) and beyond: micropractices for burnout prevention and emotional wellness. J Am Coll Radiol. 2020;17(6):746-748. doi:10.1016/j.jacr.2020.03.013
18. US Department of Veterans Affairs, National Center for PTSD. Managing healthcare workers’ stress associated with the COVID-19 virus outbreak. Updated March 25, 2020, Accessed October 12, 2021. https://www.ptsd.va.gov/covid/COVID_healthcare_workers.asp
19. US Department of Veterans Affairs, Veterans Health Administration, National Center for Organization Development (NCOD). Team Development Guide. 2017. https://vaww.va.gov/NCOD/docs/Team_Development_Guide.docx [Nonpublic source, not verified.]
Since the start of the pandemic, health care systems have requested many in-services for staff on self-care and stress management to help health care workers (HCWs) cope with the heavy toll of COVID-19. The pandemic has set off a global mental health crisis, with unprecedented numbers of individuals meeting criteria for anxiety, depression, and other mental health disorders in response to the intense stressors of living through a pandemic. These calls to assist staff with self-care and burnout prevention have been especially salient for psychologists working in palliative care and geriatrics, where fears of COVID-19 infection and numbers of patient deaths have been high.
Throughout these painful times, we have been grateful for an online community of palliative care psychologists within the US Department of Veterans Affairs (VA) from across the continuum of care and across the country. This community brought together many of us who were both struggling ourselves and striving to support the teams and HCWs around us. We are psychologists who provide home-care services in North Carolina, inpatient hospice and long-term care services in California, and long-term care and outpatient palliative care services in Massachusetts. Through our shared struggles and challenges navigating the pandemic, we realized that our respective teams requested similar services, all focused on staff support.
The psychological impact of COVID-19 on HCWs was clear from the beginning. Early in the pandemic our respective teams requested us to provide staff support and education about coping to our local HCWs. Soon national groups for long-term care staff requested education programs. Through this work, we realized that the emotional needs of HCWs ran much deeper than simple self-care. At the onset of the pandemic, before realizing its chronicity, the trainings we offered focused on stress and coping strategies. We cited several frameworks for staff support and eagerly shared anything that might help us, and our colleagues, survive the immediate anxiety and tumult surrounding us.1-3 In this paper, we briefly discuss the distress affecting the geriatric care workforce, reflect on our efforts to cope as HCWs, and offer recommendations at individual and organization levels to help address our collective grief.
Impact of COVID-19
As the death toll mounted and hospitals were pushed to the brink, we saw the suffering of our fellow HCWs. The lack of personal protective equipment (PPE) and testing supplies led to evolving and increasing anxiety for HCWs about contracting COVID-19, potentially spreading it to one’s social circle or family, fears of becoming sick and dying, and fears of inadvertently spreading the virus to medically-vulnerable patients. Increasing demands on staff required many to work outside their areas of expertise. Clinical practice guidelines changed frequently as information emerged about the virus. Staff members struggled to keep pace with the increasing number of patients, many of whom died despite heroic efforts to save them.
As the medical crisis grew, so too did social uprisings as the general public gained a strengthened awareness of the legacy and ongoing effects of systemic oppression, racism, and social inequities in the United States. Individuals grappled with their own privileges, which often hid such disparities from view. Many HCWs and clinicians of color had to navigate unsolicited questions and discussions about racial injustices while also trying to survive. As psychologists, we strove to support the HCWs around us while also struggling with our own stressors. As the magnitude of the pandemic and ongoing social injustices came into view, we realized that presentations on self-care and burnout prevention did not suffice. We needed discussions on unmasking our grief, acknowledging our traumas, and working toward collective healing.
Geriatric Care Workers
Experiences of grief and trauma hit the geriatric care workforce and especially long-term care facilities particularly hard given the high morbidity and mortality rates of COVID-19.4 The geriatric care workforce itself suffers from institutional vulnerabilities. Individuals are often underpaid, undertrained, and work within a system that continually experiences staffing shortages, high burnout, and consequently high levels of turnover.5,6 Recent immigrants and racial/ethnic minorities disproportionately make up this workforce, who often live in multigenerational households and work in multiple facilities to get by.7,8 Amid the pandemic these HCWs continued to work despite demoralizing negative media coverage of nursing homes.9 Notably, facilities with unionized staff were less likely to need second or third jobs to survive, thus reducing spread across facilities. This along with better access to PPE may have contributed to their lower COVID-19 infection and mortality rates relative to non-unionized staff.10
Similar to long-term care workers, home-care staff had related fears and anxieties, magnified by the need to enter multiple homes. This often overlooked but growing sector of the geriatric care workforce faced the added anxiety of the unknown as they entered multiple homes to provide care to their patients. These staff have little control over who may be in the home when they arrive, the sanitation/PPE practices of the patient/family, and therefore little control over their potential exposure to COVID-19. This also applies to home health aides who, although not providing medical services, are a critical part of home-care services and allow older adults to remain living independently in their home.
Reflection on Grief
As we witnessed the interactive effects of the pandemic and social inequities in geriatrics and palliative care, we frequently sought solace in online communities of psychologists working in similar settings. Over time, our regular community meetings developed a different tone: discussions about caring for others shifted to caring for ourselves. It seemed that in holding others’ pain, many of us neglected to address our own. We needed emotional support. We needed to acknowledge that we were not all okay; that the masks we wear for protection also reveal our vulnerabilities; and that protective equipment in hospitals do not protect us from the hate and bias targeting many of us face everywhere we go.
As we let ourselves be vulnerable with each other, we saw the true face of our pain: it was not stress, it was grief. We were sad, broken, mourning innumerable losses, and grieving, mostly alone. It felt overwhelming. Our minds and hearts often grew numb to find respite from pain. At times we found ourselves seeking haven in our offices, convincing ourselves that paperwork needed to be done when in reality we had no space to hold anyone else’s pain; we could barely contain our own. We could only take so much.
Without space to process, grief festers and eats away at our remaining compassion. How do we hold grace for ourselves, dare to be vulnerable, and allow ourselves to feel, when doing so opens the door to our own grief? How do we allow room for emotional processing when we learned to numb-out in order to function? And as women with diverse intersectional identities, how do we honor our humanity when we live in a society that reflects its indifference? We needed to process our pain in order to heal in the slow and uneven way that grief heals.
Caring During Tough Times
The pain we feel is real and it tears at us over time. Pushing it away disenfranchises ourselves of the opportunity to heal and grow. Our collective grief and trauma demand collective healing and acknowledgment of our individual suffering. We must honor our shared humanity and find commonality amid our differences. Typical self-care (healthy eating, sleep, basic hygiene) may not be enough to mitigate the enormity of these stressors. A glass of wine or a virtual dinner with friends may distract but does not heal our wounds.
Self-care, by definition, centers the self and ignores the larger systemic factors that maintain our struggles. It keeps the focus on the individual and in so doing, risks inducing self-blame should we continue feeling burnout. We must do more. We can advocate that systems acknowledge our grief and suffering as well as our strengths and resiliencies. We can demand that organizations recognize human limits and provide support, rather than promote environments that encourage silent perseverance. And we can deconstruct the cultural narrative that vulnerability is weakness or that we are the “heroes.” Heroism suggests superhuman qualities or extreme courage and often negates the fear and trepidation in its midst.11,12 We can also recognize how intersectional aspects of our identities make navigating the pandemic and systemic racism harder and more dangerous for some than for others.
As noted by President Biden in a speech honoring those lost to COVID-19, “We have to resist becoming numb to the sorrow.”13 The nature of our work (and that of most clinicians) is that it is expected and sometimes necessary to compartmentalize and turn off the emotions so that we can function in a professional manner. But this way of being also serves to hold us back. It does not make space for the very real emotions of trauma and grief that have pervaded HCWs during this pandemic. We must learn a different way of functioning—one where grief is acknowledged and even actively processed while still going about our work. Grief therapist Megan Devine proposes to “tend to pain and grief by bearing witness” and notes that “when we allow the reality of grief to exist, we can focus on helping ourselves—and one another—survive inside pain.”14 She advocates for self-compassion and directs us to “find ways to show our grief to others, in ways that honor the truth of our experience” saying, “we have to be willing to stop diminishing our own pain so that others can be comfortable around us.” But what does this look like among health care teams who are traumatized and grieving?
In our experience, caring for ourselves and our teams in times of prolonged stress, trauma, and grief is essential to maintain functioning over time. We strongly believe that it must occur at both the organizational and individual levels. In the throes of a crisis, teams need support immediately. To offer a timely response, we gathered knowledge of team-based care and collaboration to develop practical strategies that can be implemented swiftly to provide support across the team.15-19
The strategies we developed offer steps for creating and maintaining a supportive, compassionate, and psychologically safe work environment. First, the CARES Strategies for Practical Team Intervention highlights the importance of clear communication, assessing team needs regularly, recognizing the stress that is occurring, engaging staff in discussions, and ensuring psychological safety and comfort (Figure 1). Next, the SHARE approach is laid out to allow for interpersonal support among team members (Figure 2). Showing each other empathy, hoping for better days, acknowledging each other’s pain, reaching out for assistance, and expressing our needs allow HCWs to open up about their grief, stress, and trauma. Of note, we found these sets of strategies interdependent: a team that does not believe the leader/organization CARES is not likely to SHARE. Therefore, we also feel that it is especially important that team leaders work to create or enhance the sense of psychological safety for the team. If team members do not feel safe, they will not disclose their grief and remain stuck in the old mode of suffering in silence.
Conclusions
This pandemic and the collective efforts toward social justice advocacy have revealed our vulnerabilities as well as our strengths. These experiences have forced us to reckon with our past and consider possible futures. It has revealed the inequities in our health care system, including our failure to protect those on the ground who keep our systems running, and prompted us to consider new ways of operating in low-resourced and high-demand environments. These experiences also present us with opportunities to be better and do better as both professionals and people; to reflect on our past and consider what we want different in our lives. As we yearn for better days and brace ourselves for what is to come, we hope that teams and organizations will take advantage of these opportunities for self-reflection and continue unmasking our grief, healing our wounds, and honoring our shared humanity.
Since the start of the pandemic, health care systems have requested many in-services for staff on self-care and stress management to help health care workers (HCWs) cope with the heavy toll of COVID-19. The pandemic has set off a global mental health crisis, with unprecedented numbers of individuals meeting criteria for anxiety, depression, and other mental health disorders in response to the intense stressors of living through a pandemic. These calls to assist staff with self-care and burnout prevention have been especially salient for psychologists working in palliative care and geriatrics, where fears of COVID-19 infection and numbers of patient deaths have been high.
Throughout these painful times, we have been grateful for an online community of palliative care psychologists within the US Department of Veterans Affairs (VA) from across the continuum of care and across the country. This community brought together many of us who were both struggling ourselves and striving to support the teams and HCWs around us. We are psychologists who provide home-care services in North Carolina, inpatient hospice and long-term care services in California, and long-term care and outpatient palliative care services in Massachusetts. Through our shared struggles and challenges navigating the pandemic, we realized that our respective teams requested similar services, all focused on staff support.
The psychological impact of COVID-19 on HCWs was clear from the beginning. Early in the pandemic our respective teams requested us to provide staff support and education about coping to our local HCWs. Soon national groups for long-term care staff requested education programs. Through this work, we realized that the emotional needs of HCWs ran much deeper than simple self-care. At the onset of the pandemic, before realizing its chronicity, the trainings we offered focused on stress and coping strategies. We cited several frameworks for staff support and eagerly shared anything that might help us, and our colleagues, survive the immediate anxiety and tumult surrounding us.1-3 In this paper, we briefly discuss the distress affecting the geriatric care workforce, reflect on our efforts to cope as HCWs, and offer recommendations at individual and organization levels to help address our collective grief.
Impact of COVID-19
As the death toll mounted and hospitals were pushed to the brink, we saw the suffering of our fellow HCWs. The lack of personal protective equipment (PPE) and testing supplies led to evolving and increasing anxiety for HCWs about contracting COVID-19, potentially spreading it to one’s social circle or family, fears of becoming sick and dying, and fears of inadvertently spreading the virus to medically-vulnerable patients. Increasing demands on staff required many to work outside their areas of expertise. Clinical practice guidelines changed frequently as information emerged about the virus. Staff members struggled to keep pace with the increasing number of patients, many of whom died despite heroic efforts to save them.
As the medical crisis grew, so too did social uprisings as the general public gained a strengthened awareness of the legacy and ongoing effects of systemic oppression, racism, and social inequities in the United States. Individuals grappled with their own privileges, which often hid such disparities from view. Many HCWs and clinicians of color had to navigate unsolicited questions and discussions about racial injustices while also trying to survive. As psychologists, we strove to support the HCWs around us while also struggling with our own stressors. As the magnitude of the pandemic and ongoing social injustices came into view, we realized that presentations on self-care and burnout prevention did not suffice. We needed discussions on unmasking our grief, acknowledging our traumas, and working toward collective healing.
Geriatric Care Workers
Experiences of grief and trauma hit the geriatric care workforce and especially long-term care facilities particularly hard given the high morbidity and mortality rates of COVID-19.4 The geriatric care workforce itself suffers from institutional vulnerabilities. Individuals are often underpaid, undertrained, and work within a system that continually experiences staffing shortages, high burnout, and consequently high levels of turnover.5,6 Recent immigrants and racial/ethnic minorities disproportionately make up this workforce, who often live in multigenerational households and work in multiple facilities to get by.7,8 Amid the pandemic these HCWs continued to work despite demoralizing negative media coverage of nursing homes.9 Notably, facilities with unionized staff were less likely to need second or third jobs to survive, thus reducing spread across facilities. This along with better access to PPE may have contributed to their lower COVID-19 infection and mortality rates relative to non-unionized staff.10
Similar to long-term care workers, home-care staff had related fears and anxieties, magnified by the need to enter multiple homes. This often overlooked but growing sector of the geriatric care workforce faced the added anxiety of the unknown as they entered multiple homes to provide care to their patients. These staff have little control over who may be in the home when they arrive, the sanitation/PPE practices of the patient/family, and therefore little control over their potential exposure to COVID-19. This also applies to home health aides who, although not providing medical services, are a critical part of home-care services and allow older adults to remain living independently in their home.
Reflection on Grief
As we witnessed the interactive effects of the pandemic and social inequities in geriatrics and palliative care, we frequently sought solace in online communities of psychologists working in similar settings. Over time, our regular community meetings developed a different tone: discussions about caring for others shifted to caring for ourselves. It seemed that in holding others’ pain, many of us neglected to address our own. We needed emotional support. We needed to acknowledge that we were not all okay; that the masks we wear for protection also reveal our vulnerabilities; and that protective equipment in hospitals do not protect us from the hate and bias targeting many of us face everywhere we go.
As we let ourselves be vulnerable with each other, we saw the true face of our pain: it was not stress, it was grief. We were sad, broken, mourning innumerable losses, and grieving, mostly alone. It felt overwhelming. Our minds and hearts often grew numb to find respite from pain. At times we found ourselves seeking haven in our offices, convincing ourselves that paperwork needed to be done when in reality we had no space to hold anyone else’s pain; we could barely contain our own. We could only take so much.
Without space to process, grief festers and eats away at our remaining compassion. How do we hold grace for ourselves, dare to be vulnerable, and allow ourselves to feel, when doing so opens the door to our own grief? How do we allow room for emotional processing when we learned to numb-out in order to function? And as women with diverse intersectional identities, how do we honor our humanity when we live in a society that reflects its indifference? We needed to process our pain in order to heal in the slow and uneven way that grief heals.
Caring During Tough Times
The pain we feel is real and it tears at us over time. Pushing it away disenfranchises ourselves of the opportunity to heal and grow. Our collective grief and trauma demand collective healing and acknowledgment of our individual suffering. We must honor our shared humanity and find commonality amid our differences. Typical self-care (healthy eating, sleep, basic hygiene) may not be enough to mitigate the enormity of these stressors. A glass of wine or a virtual dinner with friends may distract but does not heal our wounds.
Self-care, by definition, centers the self and ignores the larger systemic factors that maintain our struggles. It keeps the focus on the individual and in so doing, risks inducing self-blame should we continue feeling burnout. We must do more. We can advocate that systems acknowledge our grief and suffering as well as our strengths and resiliencies. We can demand that organizations recognize human limits and provide support, rather than promote environments that encourage silent perseverance. And we can deconstruct the cultural narrative that vulnerability is weakness or that we are the “heroes.” Heroism suggests superhuman qualities or extreme courage and often negates the fear and trepidation in its midst.11,12 We can also recognize how intersectional aspects of our identities make navigating the pandemic and systemic racism harder and more dangerous for some than for others.
As noted by President Biden in a speech honoring those lost to COVID-19, “We have to resist becoming numb to the sorrow.”13 The nature of our work (and that of most clinicians) is that it is expected and sometimes necessary to compartmentalize and turn off the emotions so that we can function in a professional manner. But this way of being also serves to hold us back. It does not make space for the very real emotions of trauma and grief that have pervaded HCWs during this pandemic. We must learn a different way of functioning—one where grief is acknowledged and even actively processed while still going about our work. Grief therapist Megan Devine proposes to “tend to pain and grief by bearing witness” and notes that “when we allow the reality of grief to exist, we can focus on helping ourselves—and one another—survive inside pain.”14 She advocates for self-compassion and directs us to “find ways to show our grief to others, in ways that honor the truth of our experience” saying, “we have to be willing to stop diminishing our own pain so that others can be comfortable around us.” But what does this look like among health care teams who are traumatized and grieving?
In our experience, caring for ourselves and our teams in times of prolonged stress, trauma, and grief is essential to maintain functioning over time. We strongly believe that it must occur at both the organizational and individual levels. In the throes of a crisis, teams need support immediately. To offer a timely response, we gathered knowledge of team-based care and collaboration to develop practical strategies that can be implemented swiftly to provide support across the team.15-19
The strategies we developed offer steps for creating and maintaining a supportive, compassionate, and psychologically safe work environment. First, the CARES Strategies for Practical Team Intervention highlights the importance of clear communication, assessing team needs regularly, recognizing the stress that is occurring, engaging staff in discussions, and ensuring psychological safety and comfort (Figure 1). Next, the SHARE approach is laid out to allow for interpersonal support among team members (Figure 2). Showing each other empathy, hoping for better days, acknowledging each other’s pain, reaching out for assistance, and expressing our needs allow HCWs to open up about their grief, stress, and trauma. Of note, we found these sets of strategies interdependent: a team that does not believe the leader/organization CARES is not likely to SHARE. Therefore, we also feel that it is especially important that team leaders work to create or enhance the sense of psychological safety for the team. If team members do not feel safe, they will not disclose their grief and remain stuck in the old mode of suffering in silence.
Conclusions
This pandemic and the collective efforts toward social justice advocacy have revealed our vulnerabilities as well as our strengths. These experiences have forced us to reckon with our past and consider possible futures. It has revealed the inequities in our health care system, including our failure to protect those on the ground who keep our systems running, and prompted us to consider new ways of operating in low-resourced and high-demand environments. These experiences also present us with opportunities to be better and do better as both professionals and people; to reflect on our past and consider what we want different in our lives. As we yearn for better days and brace ourselves for what is to come, we hope that teams and organizations will take advantage of these opportunities for self-reflection and continue unmasking our grief, healing our wounds, and honoring our shared humanity.
1. Blake H, Bermingham F. Psychological wellbeing for health care workers: mitigating the impact of covid-19. Version 2.0. Updated June 18, 2020. Accessed October 12, 2021. https://www.nottingham.ac.uk/toolkits/play_22794
2. Harris R. FACE COVID: how to respond effectively to the corona crisis. Published 2020. Accessed October 12, 2021. http://louisville.edu/counseling/coping-with-covid-19/face-covid-by-dr-russ-harris/view
3. Norcross JC, Phillips CM. Psychologist self-care during the pandemic: now more than ever [published online ahead of print, 2020 May 2]. J Health Serv Psychol. 2020;1-5. doi:10.1007/s42843-020-00010-5
4. Kaiser Family Foundation. State reports of long-term care facility cases and deaths related to COVID-19. 2020. Published April 23, 2020. Accessed October 12, 2021. https://www.kff.org/coronavirus-covid-19/issue-brief/state-reporting-of-cases-and-deaths-due-to-covid-19-in-long-term-care-facilities
5. Sterling MR, Tseng E, Poon A, et al. Experiences of home health care workers in New York City during the coronavirus disease 2019 pandemic: a qualitative analysis. JAMA Intern Med. 2020;180(11):1453-1459. doi:10.1001/jamainternmed.2020.3930
6. Stone R, Wilhelm J, Bishop CE, Bryant NS, Hermer L, Squillace MR. Predictors of intent to leave the job among home health workers: analysis of the National Home Health Aide Survey. Gerontologist. 2017;57(5):890-899. doi:10.1093/geront/gnw075
7. Scales K. It’s time to care: a detailed profile of America’s direct care workforce. PHI. 2020. Published January 21, 2020. Accessed October 12, 2021. https://phinational.org/wp-content/uploads/2020/01/Its-Time-to-Care-2020-PHI.pdf
8. Wolfe R, Harknett K, Schneider D. Inequities at work and the toll of COVID-19. Health Aff Health Policy Brief. Published June 4, 2021. doi: 10.1377/hpb20210428.863621
9. White EM, Wetle TF, Reddy A, Baier RR. Front-line nursing home staff experiences during the COVID-19 pandemic [published correction appears in J Am Med Dir Assoc. 2021 May;22(5):1123]. J Am Med Dir Assoc. 2021;22(1):199-203. doi:10.1016/j.jamda.2020.11.022
10. Dean A, Venkataramani A, Kimmel S. Mortality rates from COVID-19 are lower In unionized nursing homes. Health Aff (Millwood). 2020;39(11):1993-2001.doi:10.1377/hlthaff.2020.01011
11. Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. 2020;46(8):510-513. doi:10.1136/medethics-2020-106398
12. Stokes-Parish J, Elliott R, Rolls K, Massey D. Angels and heroes: the unintended consequence of the hero narrative. J Nurs Scholarsh. 2020;52(5):462-466. doi:10.1111/jnu.12591
13. Biden J. Remarks by President Biden on the more than 500,000 American lives lost to COVID-19. Published February 22, 2021. Accessed October 12, 2021. https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/02/22/remarks-by-president-biden-on-the-more-than-500000-american-lives-lost-to-covid-19
14. Devine M. It’s Okay That You’re Not Okay: Meeting Grief and Loss in a Culture That Doesn’t Understand. Sounds True; 2017.
15. Center for the Study of Traumatic Stress. Grief leadership during COVID-19. Accessed October 12, 2021. https://www.cstsonline.org/assets/media/documents/CSTS_FS_Grief_Leadership_During_COVID19.pdf
16. Center for the Study of Traumatic Stress. Sustaining the well-being of healthcare personnel during coronavirus and other infectious disease outbreaks. Accessed October 12, 2021. https://www.cstsonline.org/assets/media/documents/CSTS_FS_Sustaining_Well_Being_Health care_Personnel_during.pdf
17. Fessell D, Cherniss C. Coronavirus disease 2019 (COVID-19) and beyond: micropractices for burnout prevention and emotional wellness. J Am Coll Radiol. 2020;17(6):746-748. doi:10.1016/j.jacr.2020.03.013
18. US Department of Veterans Affairs, National Center for PTSD. Managing healthcare workers’ stress associated with the COVID-19 virus outbreak. Updated March 25, 2020, Accessed October 12, 2021. https://www.ptsd.va.gov/covid/COVID_healthcare_workers.asp
19. US Department of Veterans Affairs, Veterans Health Administration, National Center for Organization Development (NCOD). Team Development Guide. 2017. https://vaww.va.gov/NCOD/docs/Team_Development_Guide.docx [Nonpublic source, not verified.]
1. Blake H, Bermingham F. Psychological wellbeing for health care workers: mitigating the impact of covid-19. Version 2.0. Updated June 18, 2020. Accessed October 12, 2021. https://www.nottingham.ac.uk/toolkits/play_22794
2. Harris R. FACE COVID: how to respond effectively to the corona crisis. Published 2020. Accessed October 12, 2021. http://louisville.edu/counseling/coping-with-covid-19/face-covid-by-dr-russ-harris/view
3. Norcross JC, Phillips CM. Psychologist self-care during the pandemic: now more than ever [published online ahead of print, 2020 May 2]. J Health Serv Psychol. 2020;1-5. doi:10.1007/s42843-020-00010-5
4. Kaiser Family Foundation. State reports of long-term care facility cases and deaths related to COVID-19. 2020. Published April 23, 2020. Accessed October 12, 2021. https://www.kff.org/coronavirus-covid-19/issue-brief/state-reporting-of-cases-and-deaths-due-to-covid-19-in-long-term-care-facilities
5. Sterling MR, Tseng E, Poon A, et al. Experiences of home health care workers in New York City during the coronavirus disease 2019 pandemic: a qualitative analysis. JAMA Intern Med. 2020;180(11):1453-1459. doi:10.1001/jamainternmed.2020.3930
6. Stone R, Wilhelm J, Bishop CE, Bryant NS, Hermer L, Squillace MR. Predictors of intent to leave the job among home health workers: analysis of the National Home Health Aide Survey. Gerontologist. 2017;57(5):890-899. doi:10.1093/geront/gnw075
7. Scales K. It’s time to care: a detailed profile of America’s direct care workforce. PHI. 2020. Published January 21, 2020. Accessed October 12, 2021. https://phinational.org/wp-content/uploads/2020/01/Its-Time-to-Care-2020-PHI.pdf
8. Wolfe R, Harknett K, Schneider D. Inequities at work and the toll of COVID-19. Health Aff Health Policy Brief. Published June 4, 2021. doi: 10.1377/hpb20210428.863621
9. White EM, Wetle TF, Reddy A, Baier RR. Front-line nursing home staff experiences during the COVID-19 pandemic [published correction appears in J Am Med Dir Assoc. 2021 May;22(5):1123]. J Am Med Dir Assoc. 2021;22(1):199-203. doi:10.1016/j.jamda.2020.11.022
10. Dean A, Venkataramani A, Kimmel S. Mortality rates from COVID-19 are lower In unionized nursing homes. Health Aff (Millwood). 2020;39(11):1993-2001.doi:10.1377/hlthaff.2020.01011
11. Cox CL. ‘Healthcare Heroes’: problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. J Med Ethics. 2020;46(8):510-513. doi:10.1136/medethics-2020-106398
12. Stokes-Parish J, Elliott R, Rolls K, Massey D. Angels and heroes: the unintended consequence of the hero narrative. J Nurs Scholarsh. 2020;52(5):462-466. doi:10.1111/jnu.12591
13. Biden J. Remarks by President Biden on the more than 500,000 American lives lost to COVID-19. Published February 22, 2021. Accessed October 12, 2021. https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/02/22/remarks-by-president-biden-on-the-more-than-500000-american-lives-lost-to-covid-19
14. Devine M. It’s Okay That You’re Not Okay: Meeting Grief and Loss in a Culture That Doesn’t Understand. Sounds True; 2017.
15. Center for the Study of Traumatic Stress. Grief leadership during COVID-19. Accessed October 12, 2021. https://www.cstsonline.org/assets/media/documents/CSTS_FS_Grief_Leadership_During_COVID19.pdf
16. Center for the Study of Traumatic Stress. Sustaining the well-being of healthcare personnel during coronavirus and other infectious disease outbreaks. Accessed October 12, 2021. https://www.cstsonline.org/assets/media/documents/CSTS_FS_Sustaining_Well_Being_Health care_Personnel_during.pdf
17. Fessell D, Cherniss C. Coronavirus disease 2019 (COVID-19) and beyond: micropractices for burnout prevention and emotional wellness. J Am Coll Radiol. 2020;17(6):746-748. doi:10.1016/j.jacr.2020.03.013
18. US Department of Veterans Affairs, National Center for PTSD. Managing healthcare workers’ stress associated with the COVID-19 virus outbreak. Updated March 25, 2020, Accessed October 12, 2021. https://www.ptsd.va.gov/covid/COVID_healthcare_workers.asp
19. US Department of Veterans Affairs, Veterans Health Administration, National Center for Organization Development (NCOD). Team Development Guide. 2017. https://vaww.va.gov/NCOD/docs/Team_Development_Guide.docx [Nonpublic source, not verified.]