User login
‘Alarming’ worldwide decline in mental health
The Mental Health Million project of Sapien Labs issued its second report, published online March 15, encompassing 34 countries and over 220,000 Internet-enabled adults. It found a continued decline in mental health in all age groups and genders, with English-speaking countries having the lowest mental well-being.
The decline was significantly correlated with the stringency of COVID-19 lockdown measures in each country and was directionally correlated to the cases and deaths per million.

The youngest age group (18-24 years) reported the poorest mental well-being, with better mental health scores rising in every successively older age group.
“Some of our findings, especially regarding mental health in young adults, are alarming,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, told this news organization.
“Our data, which are continually updated in real time, are freely available for nonprofit, noncommercial use and research, and we hope that researchers will get involved in an interdisciplinary way that spans sociology, economics, psychiatry, and other fields,” she said.
Pioneering research
Dr. Thiagarajan and her team pioneered the Mental Health Million project, an ongoing research initiative utilizing a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability.”
The MHQ consists of 47 “elements of mental well-being,” with scores ranging from –100 to +200. (Negative scores indicate poorer mental well-being.) The MHQ categorizes respondents as “clinical, at-risk, enduring, managing, succeeding, and thriving” and computes scores on the basis of six broad dimensions of mental health: core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
As reported by this news organization, Sapien Lab’s first Mental Health State of the World report (n = 49,000 adults) was conducted in eight English-speaking countries in 2020. Participants were compared to a smaller sample of people from the same countries polled in 2019.
In this year’s report, “we expanded quite substantially,” Dr. Thiagarajan said. The project added Spanish, French, and Arabic and recruited participants from 34 countries on six continents (n = 223,087) via advertising on Google and Facebook.

Economic prosperity not protective
Across the eight English-speaking countries, there was a decline in mental well-being of 3% from 2020 to 2021, which was smaller than the 8% decline from 2019 to 2020. The percentage of people who were “distressed or struggling” increased from 26% to 30% in 2021.
“Now that a lot of pandemic issue seems to be easing up, I hope we’ll see mental well-being coming back up, but at least it’s a smaller decline than we saw between 2019 and 2020,” said Dr. Thiagarajan.
The decline across countries from 2019 to 2021 was significantly correlated with the stringency of governmental COVID-19-related measures (based on the Oxford COVID-19 Government Response Tracker, 2022; r = .54) and directionally correlated to the cases and deaths per million.
In total, 30% of respondents in English-speaking countries had mental well-being scores in the “distressed” or “struggling” range – higher than the Middle Eastern countries, North Africa, Latin America, and Europe (23%, 23%, 24%, and 18%, respectively).
Only 36% of participants in the English-speaking countries, the Middle East, and North Africa reported “thriving or succeeding,” vs. 45% and 46% in Latin America and Europe, respectively. Venezuela topped the list with an average MHQ of 91, while the United Kingdom and South Africa had the lowest scores, at 46 each.
Mental well-being was slightly higher in males than in females but was dramatically lower in nonbinary/third-gender respondents. In fact, those identifying as nonbinary/third gender had the lowest mental well-being of any group.
Across all countries and languages, higher education was associated with better mental well-being. Employment was also associated with superior mental well-being, compared with being unemployed – particularly in core English-speaking countries.
However, “country indicators of economic prosperity were negatively correlated with mental well-being, particularly for young adults and males, belying the commonly held belief that national economic prosperity translates into greater mental well-being,” said Dr. Thiagarajan.
‘Stark’ contrast
The most dramatic finding was the difference in mental well-being between younger and older adults, which was two- to threefold larger than differences in other dimensions (for example, age, gender, employment). Even the maximum difference between countries overall (15%) was still smaller than the generational gap within any region.
While only 7% (6%- 9%) of participants aged ≥65 years were “distressed and struggling” with their mental well-being to a “clinical” extent, 44% (38%-50%) of those aged 18-24 years reported mental well-being scores in the “distressed or struggling” range – representing a “growing gap between generations that, while present prior to the COVID-19 pandemic, has since been exacerbated,” the authors state.
With every successive decrement in age group, mental well-being “plummeted,” Dr. Thiagarajan said. She noted that research conducted prior to 2010 in several regions of the world showed that young adults typically had the highest well-being. “Our findings stand in stark contrast to these previous patterns.”
The relationship between lockdown stringency and poorer mental health could play a role. “The impact of social isolation may be most strongly felt in younger people,” she said.
Internet a culprit?
“Within almost every region, scores for cognition and drive and motivation were highest while mood and outlook and social self were the lowest,” the authors report.
The aggregate percentage of respondents who reported being “distressed or struggling” in the various MHQ dimensions is shown in the following table.
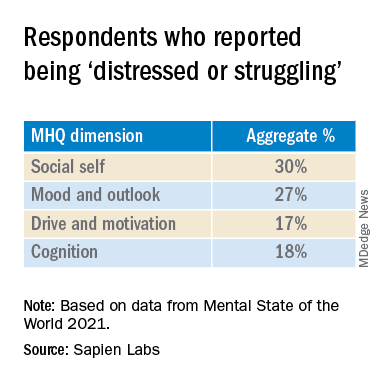
In particular, English-speaking countries scored lowest on the social self scale.
The sense of social self is “how you see yourself with respect to others, how you relate to others and the ability to form strong, stable relationships and maintain them with other people,” said Dr. Thiagarajan.
Internet use might account for the “massive” difference between the youngest and the oldest generations, she suggested. “Following 2010, mobile phone penetration picked up and rose rapidly. ... Mobile phones took over the world.”
Time spent on the Internet – an estimated 7-10 hours per day – “eats into the time people in older generations used in building the social self. Kids who grow up on the Internet are losing thousands of hours in social interactions, which is challenging their ability to form relationships, how they see themselves, and how they fit into the social fabric,” Dr. Thiagarajan added
Sedentary time
Commenting for this news organization, Bernardo Ng, MD, a member of the American Psychiatric Association’s Council on International Psychiatry and Global Health and medical director of Sun Valley Research Center, Imperial, Calif., called the report “interesting, with an impressive sample size” and an “impressive geographic distribution.”

Dr. Ng, who was not involved in the report, said, “I did not think the impact of Internet use on mental health was as dramatic before looking at this report.
“On the other hand, I have personally been interested in the impact of sedentarism in mental health – not only emotionally but also biologically. Sedentarism, which is directly related to screen use time, produces inflammation that worsens brain function.”

Also commenting, Ken Duckworth, MD, chief medical officer of the National Alliance of Mental Illness, called the survey “extremely well timed and creative, although it looked only at Internet-enabled populations, so one cannot make too many overall pronouncements, because a lot of people don’t have access to the Internet.”
The data regarding young people are particularly powerful. “The idea that young people are having a decrease in their experience of mental health across the world is something I haven’t seen before.”
Dr. Duckworth suggested the reason might “have to do with the impact of the COVID lockdown on normal development that young people go through, while older people don’t struggle with these developmental challenges in the same way.”
A version of this article first appeared on Medscape.com.
The Mental Health Million project of Sapien Labs issued its second report, published online March 15, encompassing 34 countries and over 220,000 Internet-enabled adults. It found a continued decline in mental health in all age groups and genders, with English-speaking countries having the lowest mental well-being.
The decline was significantly correlated with the stringency of COVID-19 lockdown measures in each country and was directionally correlated to the cases and deaths per million.
The youngest age group (18-24 years) reported the poorest mental well-being, with better mental health scores rising in every successively older age group.
“Some of our findings, especially regarding mental health in young adults, are alarming,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, told this news organization.
“Our data, which are continually updated in real time, are freely available for nonprofit, noncommercial use and research, and we hope that researchers will get involved in an interdisciplinary way that spans sociology, economics, psychiatry, and other fields,” she said.
Pioneering research
Dr. Thiagarajan and her team pioneered the Mental Health Million project, an ongoing research initiative utilizing a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability.”
The MHQ consists of 47 “elements of mental well-being,” with scores ranging from –100 to +200. (Negative scores indicate poorer mental well-being.) The MHQ categorizes respondents as “clinical, at-risk, enduring, managing, succeeding, and thriving” and computes scores on the basis of six broad dimensions of mental health: core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
As reported by this news organization, Sapien Lab’s first Mental Health State of the World report (n = 49,000 adults) was conducted in eight English-speaking countries in 2020. Participants were compared to a smaller sample of people from the same countries polled in 2019.
In this year’s report, “we expanded quite substantially,” Dr. Thiagarajan said. The project added Spanish, French, and Arabic and recruited participants from 34 countries on six continents (n = 223,087) via advertising on Google and Facebook.
Economic prosperity not protective
Across the eight English-speaking countries, there was a decline in mental well-being of 3% from 2020 to 2021, which was smaller than the 8% decline from 2019 to 2020. The percentage of people who were “distressed or struggling” increased from 26% to 30% in 2021.
“Now that a lot of pandemic issue seems to be easing up, I hope we’ll see mental well-being coming back up, but at least it’s a smaller decline than we saw between 2019 and 2020,” said Dr. Thiagarajan.
The decline across countries from 2019 to 2021 was significantly correlated with the stringency of governmental COVID-19-related measures (based on the Oxford COVID-19 Government Response Tracker, 2022; r = .54) and directionally correlated to the cases and deaths per million.
In total, 30% of respondents in English-speaking countries had mental well-being scores in the “distressed” or “struggling” range – higher than the Middle Eastern countries, North Africa, Latin America, and Europe (23%, 23%, 24%, and 18%, respectively).
Only 36% of participants in the English-speaking countries, the Middle East, and North Africa reported “thriving or succeeding,” vs. 45% and 46% in Latin America and Europe, respectively. Venezuela topped the list with an average MHQ of 91, while the United Kingdom and South Africa had the lowest scores, at 46 each.
Mental well-being was slightly higher in males than in females but was dramatically lower in nonbinary/third-gender respondents. In fact, those identifying as nonbinary/third gender had the lowest mental well-being of any group.
Across all countries and languages, higher education was associated with better mental well-being. Employment was also associated with superior mental well-being, compared with being unemployed – particularly in core English-speaking countries.
However, “country indicators of economic prosperity were negatively correlated with mental well-being, particularly for young adults and males, belying the commonly held belief that national economic prosperity translates into greater mental well-being,” said Dr. Thiagarajan.
‘Stark’ contrast
The most dramatic finding was the difference in mental well-being between younger and older adults, which was two- to threefold larger than differences in other dimensions (for example, age, gender, employment). Even the maximum difference between countries overall (15%) was still smaller than the generational gap within any region.
While only 7% (6%- 9%) of participants aged ≥65 years were “distressed and struggling” with their mental well-being to a “clinical” extent, 44% (38%-50%) of those aged 18-24 years reported mental well-being scores in the “distressed or struggling” range – representing a “growing gap between generations that, while present prior to the COVID-19 pandemic, has since been exacerbated,” the authors state.
With every successive decrement in age group, mental well-being “plummeted,” Dr. Thiagarajan said. She noted that research conducted prior to 2010 in several regions of the world showed that young adults typically had the highest well-being. “Our findings stand in stark contrast to these previous patterns.”
The relationship between lockdown stringency and poorer mental health could play a role. “The impact of social isolation may be most strongly felt in younger people,” she said.
Internet a culprit?
“Within almost every region, scores for cognition and drive and motivation were highest while mood and outlook and social self were the lowest,” the authors report.
The aggregate percentage of respondents who reported being “distressed or struggling” in the various MHQ dimensions is shown in the following table.
In particular, English-speaking countries scored lowest on the social self scale.
The sense of social self is “how you see yourself with respect to others, how you relate to others and the ability to form strong, stable relationships and maintain them with other people,” said Dr. Thiagarajan.
Internet use might account for the “massive” difference between the youngest and the oldest generations, she suggested. “Following 2010, mobile phone penetration picked up and rose rapidly. ... Mobile phones took over the world.”
Time spent on the Internet – an estimated 7-10 hours per day – “eats into the time people in older generations used in building the social self. Kids who grow up on the Internet are losing thousands of hours in social interactions, which is challenging their ability to form relationships, how they see themselves, and how they fit into the social fabric,” Dr. Thiagarajan added
Sedentary time
Commenting for this news organization, Bernardo Ng, MD, a member of the American Psychiatric Association’s Council on International Psychiatry and Global Health and medical director of Sun Valley Research Center, Imperial, Calif., called the report “interesting, with an impressive sample size” and an “impressive geographic distribution.”
Dr. Ng, who was not involved in the report, said, “I did not think the impact of Internet use on mental health was as dramatic before looking at this report.
“On the other hand, I have personally been interested in the impact of sedentarism in mental health – not only emotionally but also biologically. Sedentarism, which is directly related to screen use time, produces inflammation that worsens brain function.”
Also commenting, Ken Duckworth, MD, chief medical officer of the National Alliance of Mental Illness, called the survey “extremely well timed and creative, although it looked only at Internet-enabled populations, so one cannot make too many overall pronouncements, because a lot of people don’t have access to the Internet.”
The data regarding young people are particularly powerful. “The idea that young people are having a decrease in their experience of mental health across the world is something I haven’t seen before.”
Dr. Duckworth suggested the reason might “have to do with the impact of the COVID lockdown on normal development that young people go through, while older people don’t struggle with these developmental challenges in the same way.”
A version of this article first appeared on Medscape.com.
The Mental Health Million project of Sapien Labs issued its second report, published online March 15, encompassing 34 countries and over 220,000 Internet-enabled adults. It found a continued decline in mental health in all age groups and genders, with English-speaking countries having the lowest mental well-being.
The decline was significantly correlated with the stringency of COVID-19 lockdown measures in each country and was directionally correlated to the cases and deaths per million.
The youngest age group (18-24 years) reported the poorest mental well-being, with better mental health scores rising in every successively older age group.
“Some of our findings, especially regarding mental health in young adults, are alarming,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, told this news organization.
“Our data, which are continually updated in real time, are freely available for nonprofit, noncommercial use and research, and we hope that researchers will get involved in an interdisciplinary way that spans sociology, economics, psychiatry, and other fields,” she said.
Pioneering research
Dr. Thiagarajan and her team pioneered the Mental Health Million project, an ongoing research initiative utilizing a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability.”
The MHQ consists of 47 “elements of mental well-being,” with scores ranging from –100 to +200. (Negative scores indicate poorer mental well-being.) The MHQ categorizes respondents as “clinical, at-risk, enduring, managing, succeeding, and thriving” and computes scores on the basis of six broad dimensions of mental health: core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
As reported by this news organization, Sapien Lab’s first Mental Health State of the World report (n = 49,000 adults) was conducted in eight English-speaking countries in 2020. Participants were compared to a smaller sample of people from the same countries polled in 2019.
In this year’s report, “we expanded quite substantially,” Dr. Thiagarajan said. The project added Spanish, French, and Arabic and recruited participants from 34 countries on six continents (n = 223,087) via advertising on Google and Facebook.
Economic prosperity not protective
Across the eight English-speaking countries, there was a decline in mental well-being of 3% from 2020 to 2021, which was smaller than the 8% decline from 2019 to 2020. The percentage of people who were “distressed or struggling” increased from 26% to 30% in 2021.
“Now that a lot of pandemic issue seems to be easing up, I hope we’ll see mental well-being coming back up, but at least it’s a smaller decline than we saw between 2019 and 2020,” said Dr. Thiagarajan.
The decline across countries from 2019 to 2021 was significantly correlated with the stringency of governmental COVID-19-related measures (based on the Oxford COVID-19 Government Response Tracker, 2022; r = .54) and directionally correlated to the cases and deaths per million.
In total, 30% of respondents in English-speaking countries had mental well-being scores in the “distressed” or “struggling” range – higher than the Middle Eastern countries, North Africa, Latin America, and Europe (23%, 23%, 24%, and 18%, respectively).
Only 36% of participants in the English-speaking countries, the Middle East, and North Africa reported “thriving or succeeding,” vs. 45% and 46% in Latin America and Europe, respectively. Venezuela topped the list with an average MHQ of 91, while the United Kingdom and South Africa had the lowest scores, at 46 each.
Mental well-being was slightly higher in males than in females but was dramatically lower in nonbinary/third-gender respondents. In fact, those identifying as nonbinary/third gender had the lowest mental well-being of any group.
Across all countries and languages, higher education was associated with better mental well-being. Employment was also associated with superior mental well-being, compared with being unemployed – particularly in core English-speaking countries.
However, “country indicators of economic prosperity were negatively correlated with mental well-being, particularly for young adults and males, belying the commonly held belief that national economic prosperity translates into greater mental well-being,” said Dr. Thiagarajan.
‘Stark’ contrast
The most dramatic finding was the difference in mental well-being between younger and older adults, which was two- to threefold larger than differences in other dimensions (for example, age, gender, employment). Even the maximum difference between countries overall (15%) was still smaller than the generational gap within any region.
While only 7% (6%- 9%) of participants aged ≥65 years were “distressed and struggling” with their mental well-being to a “clinical” extent, 44% (38%-50%) of those aged 18-24 years reported mental well-being scores in the “distressed or struggling” range – representing a “growing gap between generations that, while present prior to the COVID-19 pandemic, has since been exacerbated,” the authors state.
With every successive decrement in age group, mental well-being “plummeted,” Dr. Thiagarajan said. She noted that research conducted prior to 2010 in several regions of the world showed that young adults typically had the highest well-being. “Our findings stand in stark contrast to these previous patterns.”
The relationship between lockdown stringency and poorer mental health could play a role. “The impact of social isolation may be most strongly felt in younger people,” she said.
Internet a culprit?
“Within almost every region, scores for cognition and drive and motivation were highest while mood and outlook and social self were the lowest,” the authors report.
The aggregate percentage of respondents who reported being “distressed or struggling” in the various MHQ dimensions is shown in the following table.
In particular, English-speaking countries scored lowest on the social self scale.
The sense of social self is “how you see yourself with respect to others, how you relate to others and the ability to form strong, stable relationships and maintain them with other people,” said Dr. Thiagarajan.
Internet use might account for the “massive” difference between the youngest and the oldest generations, she suggested. “Following 2010, mobile phone penetration picked up and rose rapidly. ... Mobile phones took over the world.”
Time spent on the Internet – an estimated 7-10 hours per day – “eats into the time people in older generations used in building the social self. Kids who grow up on the Internet are losing thousands of hours in social interactions, which is challenging their ability to form relationships, how they see themselves, and how they fit into the social fabric,” Dr. Thiagarajan added
Sedentary time
Commenting for this news organization, Bernardo Ng, MD, a member of the American Psychiatric Association’s Council on International Psychiatry and Global Health and medical director of Sun Valley Research Center, Imperial, Calif., called the report “interesting, with an impressive sample size” and an “impressive geographic distribution.”
Dr. Ng, who was not involved in the report, said, “I did not think the impact of Internet use on mental health was as dramatic before looking at this report.
“On the other hand, I have personally been interested in the impact of sedentarism in mental health – not only emotionally but also biologically. Sedentarism, which is directly related to screen use time, produces inflammation that worsens brain function.”
Also commenting, Ken Duckworth, MD, chief medical officer of the National Alliance of Mental Illness, called the survey “extremely well timed and creative, although it looked only at Internet-enabled populations, so one cannot make too many overall pronouncements, because a lot of people don’t have access to the Internet.”
The data regarding young people are particularly powerful. “The idea that young people are having a decrease in their experience of mental health across the world is something I haven’t seen before.”
Dr. Duckworth suggested the reason might “have to do with the impact of the COVID lockdown on normal development that young people go through, while older people don’t struggle with these developmental challenges in the same way.”
A version of this article first appeared on Medscape.com.
Standard of care in suicide prevention in pediatrics: A review of the Blueprint for Youth Suicide Prevention
In March, an unprecedented collaboration between the American Academy of Pediatrics (AAP), American Foundation for Suicide Prevention (AFSP), and National Institute of Mental Health (NIMH) resulted in the development of the Blueprint for Youth Suicide Prevention. The blueprint comprises a consensus summary of expert recommendations, educational resources, and specific and practical strategies for pediatricians and other health care providers to support youth at risk for suicide in pediatric primary care settings. It is ambitious and far-reaching in scope and speaks to the growing understanding that suicide care pathways offer a clear ray of hope toward a shared “zero suicide” goal.
Following the declaration of a national emergency for child and adolescent mental health, the blueprint represents a resource to help us move forward during this national emergency. It offers practically focused suggestions at the clinic site and individual level, in addition to community and school levels, to tackle the deeply concerning and alarming increasing rate of emergency department visits by 30% in the last 2 pandemic years for youth suicide attempts. A reflexive visit for an emergency mental health evaluation in an emergency department after a disclosure of suicidal ideation isn’t always the next best step in a pathway to care, nor a sustainable community solution with the dearth of mental health and crisis resources nationally.

With this new tool, let’s proceed through a case of how one would approach a patient in the office setting with a concerning disclosure.
Case
Emily is a 12-year-old girl who presents for a routine well-check in your practice. Her mother shared with you before your examination that she has wondered if Emily may need more support. Since the pandemic, Emily had increasingly spent time using social media and watching television. When you meet with Emily on her own, she says, “I know that life is getting back to normal, and I am supposed to be excited for that, but now I have some anxiety about doing what I used to do. I’ve had some thoughts that it would be better to sleep forever and not wake up ...”
Case discussion
The blueprint recommends universal screening for suicide in all youths aged 12 and over. Not all children, like Emily, will be as open about their inner thoughts. The blueprint provides a link to the ASQ, which comprises questions to ascertain suicide risk and takes 20 seconds to complete with a patient. It is recommended as a first-line screening tool by the NIMH: Suicide Risk Screening Tool. This tool can guide one’s clinical thinking beyond the question of whether or not a child feels “suicidal” after a disclosure such as Emily’s. The blueprint also provides a tip sheet on how to frame these screenings to ensure their thoroughness and interpersonal effectiveness.
Case continued
You go through the ASQ with Emily and she revealed that she has had thoughts about suicide but not currently and without further plans. According to the ASQ, this screening falls into the category of a “non-acute positive screen (potential risk identified),” and now the patient requires a brief suicide safety assessment to determine if an emergency mental health evaluation is needed.
Case discussion
An initial screen (ASQ) should be followed by a Brief Suicide Safety Assessment (BSSA). Two common ones are the ASQ-BSSA (created by the same group that created the ASQ) or the C-SSRS (Columbia suicide severity rating scale).
The blueprint suggests adding this level of depth to one’s investigation in a pediatrics office for a divulged concern with suicidal ideation and following the algorithm to ensure safety.
The complete screening process is also described, in detail, in this instructional video: Suicide Risk Screening Training: How to Manage Patients at Risk for Suicide.
Case continued
Following the ASQ-BSSA, you determine that a referral to more immediate mental health resources would be most helpful and discuss your concerns with Emily and her family. You connect her via a “warm handoff” to a therapist in the office available from the newly adopted primary care mental health integration model. Emily completes further screening for anxiety and depressive disorders and begins a course of cognitive-behavioral therapy. You feel reassured that the therapist can connect with the consulting psychiatrist in the model who can offer a comprehensive psychiatric evaluation if needed. A referral to the emergency department to complete this screening has been avoided. You also plan for a “caring contact” from the office in a day to check in on Emily and her family and, before they go, provide them with crisis services and resources.
The blueprint represents a thoughtful means to know when emergency department visits are necessary and when other forms of support such as robust safety planning, a connection to other nonemergency services, and “caring contacts” from the office within 24-48 hours are actually of more benefit. “Caring contacts,” in particular, have been lauded as having a significant impact in modifying the course of a patient with suicidal ideation. Data show that differences such as follow-up phone calls by any staff member or even postcards from the clinic over 6-12 months can affect suicide risk.
Beyond outlining suicide care pathways, the blueprint also shares clinical algorithms from the National Network of Child Psychiatry Access Programs (NNCPAP). These algorithms help clinicians assess common issues in pediatrics and reserve referrals to psychiatry and escalations of care to the emergency department for certain high-risk circumstances.
The blueprint seeks to provide a “one-stop-shop” for accessible and usable resources in the clinic workflow for suicide prevention. It is inspiring to see our professional organizations pursuing practical and practice-based solutions to our children’s mental health crisis in unison.
Dr. Pawlowski is a child and adolescent consulting psychiatrist. She is a division chief at the University of Vermont Medical Center where she focuses on primary care mental health integration within primary care pediatrics, internal medicine, and family medicine. Email her at pdnews@mdedge.com.
In March, an unprecedented collaboration between the American Academy of Pediatrics (AAP), American Foundation for Suicide Prevention (AFSP), and National Institute of Mental Health (NIMH) resulted in the development of the Blueprint for Youth Suicide Prevention. The blueprint comprises a consensus summary of expert recommendations, educational resources, and specific and practical strategies for pediatricians and other health care providers to support youth at risk for suicide in pediatric primary care settings. It is ambitious and far-reaching in scope and speaks to the growing understanding that suicide care pathways offer a clear ray of hope toward a shared “zero suicide” goal.
Following the declaration of a national emergency for child and adolescent mental health, the blueprint represents a resource to help us move forward during this national emergency. It offers practically focused suggestions at the clinic site and individual level, in addition to community and school levels, to tackle the deeply concerning and alarming increasing rate of emergency department visits by 30% in the last 2 pandemic years for youth suicide attempts. A reflexive visit for an emergency mental health evaluation in an emergency department after a disclosure of suicidal ideation isn’t always the next best step in a pathway to care, nor a sustainable community solution with the dearth of mental health and crisis resources nationally.
With this new tool, let’s proceed through a case of how one would approach a patient in the office setting with a concerning disclosure.
Case
Emily is a 12-year-old girl who presents for a routine well-check in your practice. Her mother shared with you before your examination that she has wondered if Emily may need more support. Since the pandemic, Emily had increasingly spent time using social media and watching television. When you meet with Emily on her own, she says, “I know that life is getting back to normal, and I am supposed to be excited for that, but now I have some anxiety about doing what I used to do. I’ve had some thoughts that it would be better to sleep forever and not wake up ...”
Case discussion
The blueprint recommends universal screening for suicide in all youths aged 12 and over. Not all children, like Emily, will be as open about their inner thoughts. The blueprint provides a link to the ASQ, which comprises questions to ascertain suicide risk and takes 20 seconds to complete with a patient. It is recommended as a first-line screening tool by the NIMH: Suicide Risk Screening Tool. This tool can guide one’s clinical thinking beyond the question of whether or not a child feels “suicidal” after a disclosure such as Emily’s. The blueprint also provides a tip sheet on how to frame these screenings to ensure their thoroughness and interpersonal effectiveness.
Case continued
You go through the ASQ with Emily and she revealed that she has had thoughts about suicide but not currently and without further plans. According to the ASQ, this screening falls into the category of a “non-acute positive screen (potential risk identified),” and now the patient requires a brief suicide safety assessment to determine if an emergency mental health evaluation is needed.
Case discussion
An initial screen (ASQ) should be followed by a Brief Suicide Safety Assessment (BSSA). Two common ones are the ASQ-BSSA (created by the same group that created the ASQ) or the C-SSRS (Columbia suicide severity rating scale).
The blueprint suggests adding this level of depth to one’s investigation in a pediatrics office for a divulged concern with suicidal ideation and following the algorithm to ensure safety.
The complete screening process is also described, in detail, in this instructional video: Suicide Risk Screening Training: How to Manage Patients at Risk for Suicide.
Case continued
Following the ASQ-BSSA, you determine that a referral to more immediate mental health resources would be most helpful and discuss your concerns with Emily and her family. You connect her via a “warm handoff” to a therapist in the office available from the newly adopted primary care mental health integration model. Emily completes further screening for anxiety and depressive disorders and begins a course of cognitive-behavioral therapy. You feel reassured that the therapist can connect with the consulting psychiatrist in the model who can offer a comprehensive psychiatric evaluation if needed. A referral to the emergency department to complete this screening has been avoided. You also plan for a “caring contact” from the office in a day to check in on Emily and her family and, before they go, provide them with crisis services and resources.
The blueprint represents a thoughtful means to know when emergency department visits are necessary and when other forms of support such as robust safety planning, a connection to other nonemergency services, and “caring contacts” from the office within 24-48 hours are actually of more benefit. “Caring contacts,” in particular, have been lauded as having a significant impact in modifying the course of a patient with suicidal ideation. Data show that differences such as follow-up phone calls by any staff member or even postcards from the clinic over 6-12 months can affect suicide risk.
Beyond outlining suicide care pathways, the blueprint also shares clinical algorithms from the National Network of Child Psychiatry Access Programs (NNCPAP). These algorithms help clinicians assess common issues in pediatrics and reserve referrals to psychiatry and escalations of care to the emergency department for certain high-risk circumstances.
The blueprint seeks to provide a “one-stop-shop” for accessible and usable resources in the clinic workflow for suicide prevention. It is inspiring to see our professional organizations pursuing practical and practice-based solutions to our children’s mental health crisis in unison.
Dr. Pawlowski is a child and adolescent consulting psychiatrist. She is a division chief at the University of Vermont Medical Center where she focuses on primary care mental health integration within primary care pediatrics, internal medicine, and family medicine. Email her at pdnews@mdedge.com.
In March, an unprecedented collaboration between the American Academy of Pediatrics (AAP), American Foundation for Suicide Prevention (AFSP), and National Institute of Mental Health (NIMH) resulted in the development of the Blueprint for Youth Suicide Prevention. The blueprint comprises a consensus summary of expert recommendations, educational resources, and specific and practical strategies for pediatricians and other health care providers to support youth at risk for suicide in pediatric primary care settings. It is ambitious and far-reaching in scope and speaks to the growing understanding that suicide care pathways offer a clear ray of hope toward a shared “zero suicide” goal.
Following the declaration of a national emergency for child and adolescent mental health, the blueprint represents a resource to help us move forward during this national emergency. It offers practically focused suggestions at the clinic site and individual level, in addition to community and school levels, to tackle the deeply concerning and alarming increasing rate of emergency department visits by 30% in the last 2 pandemic years for youth suicide attempts. A reflexive visit for an emergency mental health evaluation in an emergency department after a disclosure of suicidal ideation isn’t always the next best step in a pathway to care, nor a sustainable community solution with the dearth of mental health and crisis resources nationally.
With this new tool, let’s proceed through a case of how one would approach a patient in the office setting with a concerning disclosure.
Case
Emily is a 12-year-old girl who presents for a routine well-check in your practice. Her mother shared with you before your examination that she has wondered if Emily may need more support. Since the pandemic, Emily had increasingly spent time using social media and watching television. When you meet with Emily on her own, she says, “I know that life is getting back to normal, and I am supposed to be excited for that, but now I have some anxiety about doing what I used to do. I’ve had some thoughts that it would be better to sleep forever and not wake up ...”
Case discussion
The blueprint recommends universal screening for suicide in all youths aged 12 and over. Not all children, like Emily, will be as open about their inner thoughts. The blueprint provides a link to the ASQ, which comprises questions to ascertain suicide risk and takes 20 seconds to complete with a patient. It is recommended as a first-line screening tool by the NIMH: Suicide Risk Screening Tool. This tool can guide one’s clinical thinking beyond the question of whether or not a child feels “suicidal” after a disclosure such as Emily’s. The blueprint also provides a tip sheet on how to frame these screenings to ensure their thoroughness and interpersonal effectiveness.
Case continued
You go through the ASQ with Emily and she revealed that she has had thoughts about suicide but not currently and without further plans. According to the ASQ, this screening falls into the category of a “non-acute positive screen (potential risk identified),” and now the patient requires a brief suicide safety assessment to determine if an emergency mental health evaluation is needed.
Case discussion
An initial screen (ASQ) should be followed by a Brief Suicide Safety Assessment (BSSA). Two common ones are the ASQ-BSSA (created by the same group that created the ASQ) or the C-SSRS (Columbia suicide severity rating scale).
The blueprint suggests adding this level of depth to one’s investigation in a pediatrics office for a divulged concern with suicidal ideation and following the algorithm to ensure safety.
The complete screening process is also described, in detail, in this instructional video: Suicide Risk Screening Training: How to Manage Patients at Risk for Suicide.
Case continued
Following the ASQ-BSSA, you determine that a referral to more immediate mental health resources would be most helpful and discuss your concerns with Emily and her family. You connect her via a “warm handoff” to a therapist in the office available from the newly adopted primary care mental health integration model. Emily completes further screening for anxiety and depressive disorders and begins a course of cognitive-behavioral therapy. You feel reassured that the therapist can connect with the consulting psychiatrist in the model who can offer a comprehensive psychiatric evaluation if needed. A referral to the emergency department to complete this screening has been avoided. You also plan for a “caring contact” from the office in a day to check in on Emily and her family and, before they go, provide them with crisis services and resources.
The blueprint represents a thoughtful means to know when emergency department visits are necessary and when other forms of support such as robust safety planning, a connection to other nonemergency services, and “caring contacts” from the office within 24-48 hours are actually of more benefit. “Caring contacts,” in particular, have been lauded as having a significant impact in modifying the course of a patient with suicidal ideation. Data show that differences such as follow-up phone calls by any staff member or even postcards from the clinic over 6-12 months can affect suicide risk.
Beyond outlining suicide care pathways, the blueprint also shares clinical algorithms from the National Network of Child Psychiatry Access Programs (NNCPAP). These algorithms help clinicians assess common issues in pediatrics and reserve referrals to psychiatry and escalations of care to the emergency department for certain high-risk circumstances.
The blueprint seeks to provide a “one-stop-shop” for accessible and usable resources in the clinic workflow for suicide prevention. It is inspiring to see our professional organizations pursuing practical and practice-based solutions to our children’s mental health crisis in unison.
Dr. Pawlowski is a child and adolescent consulting psychiatrist. She is a division chief at the University of Vermont Medical Center where she focuses on primary care mental health integration within primary care pediatrics, internal medicine, and family medicine. Email her at pdnews@mdedge.com.
Diagnosing adolescent ADHD
Pediatricians are increasingly expert in the assessment and treatment of attention-deficit/hyperactivity disorder. But what do you do when adolescents present to your office saying they think they have ADHD? While ADHD is a common and treatable disorder of youth, it is important to take special care when assessing an adolescent. Difficulties with attention and concentration are common symptoms for many different challenges of adolescence, and for ADHD to be the underlying cause, those symptoms must have started prior to adolescence (according to DSM-5, prior to the age of 12). When your adolescent patients or their parents come to your office complaining of inattention, it is important to consider the full range of possible explanations.
Sleep
We have written in this column previously about the challenges that adolescents face in getting adequate sleep consistently. Teenagers, on average, need more than 9 hours of sleep nightly and American teenagers get fewer than 6. This mismatch is because of physiologic shifts that move their natural sleep onset time significantly later, while school still starts early. It’s often compounded by other demands on their time, including homework, extracurricular activities, and the gravitational pull of social connections. Independent teenagers make their own decisions about how to manage their time and may feel sleep is optional, or manage their fatigue with naps and caffeine, both of which will further compromise the quality and efficiency of sleep.

Chronic sleep deprivation will present with difficulties with focus, attention, memory, and cognitive performance. Treatment of this problem with stimulants is likely to make the underlying poor sleep habits even worse. When your patient presents complaining of difficulty concentrating and worsening school performance, be sure to start with a thorough sleep history, and always provide guidance about the body’s need for sleep and healthy sleep habits.
Anxiety
Anxiety disorders are the most common psychiatric illnesses of youth, with estimates of as many as 30% of children and adolescents experiencing one. The true prevalence of ADHD is estimated to be about 4% of the population. Whether social phobia, generalized anxiety disorder, or even posttraumatic stress disorder, anxiety disorders interfere with attention as ruminative worry tends to distract those experiencing it. It can also affect attention and focus indirectly by interfering with restful sleep. Anxiety disorders can be difficult to identify, as the sufferers typically internalize their symptoms. But inquire about specific worries (such as speaking in front of others, meeting new people, or an illness or accident striking themselves or a loved one) and how much time they take up. Explore if worries fill their thoughts during quiet or downtime, and explore more about their worries. You may use a screening instrument such as the Pediatric Symptom Checklist or the SCARED, both of which will indicate a likely problem with anxiety. While it is possible to have comorbid ADHD with an anxiety disorder, the anxiety disorder will likely worsen with stimulants and should be treated first. These are usually curable illnesses and you may find that remission of anxiety symptoms resolves the attentional problems.
Depression
Mood disorders are less common than anxiety disorders in youth, but far more prevalent than ADHD. And depression is usually marked by serious difficulty concentrating across settings (including for things that were previously very interesting). A sullen teenager who is deeply self-critical about school performance would benefit from exploration of associated changes in mood, interests, energy, appetite, sleep, and for feelings of worthlessness, guilt, and suicidal thoughts. The PHQ9A is a simple, free screening instrument that is reasonable to use with every sick visit (and well-check) with your adolescent patients, given the risks of undetected and untreated depression. If your patient presents complaining of poor school performance, always screen for depression. As with anxiety disorders, comorbid ADHD is possible, but it is always recommended to treat the mood disorder first and then to assess for residual ADHD symptoms once the mood disorder is in remission.
Substance abuse
Adolescence is a time of exploration, and drug and alcohol use is common. While attentional impairment will happen with intoxication, occasional or rare use should not lead to consistent impairment in school. But when parents are more worried than their children about a significant change in school performance, it is important to screen for substance abuse. A child with a secret substance use disorder will often present with behavioral changes and deteriorating school performance and might deny any drug or alcohol use to parents. Indeed, stimulants have some street value and some patients may be seeking a stimulant prescription to sell or trade for other drugs. Regular marijuana use may present with only deteriorating school performance and no irritability or other noticeable behavioral changes. Marijuana is seen as safe and even healthy by many teenagers (and even many parents), and some youth may be using it recreationally or to manage difficulties with sleep, anxiety, or mood symptoms.

But there is compelling evidence that marijuana use causes cognitive impairment, including difficulty with sustaining attention, short-term memory, and processing speed, for as long as 24 hours after use. If a teenager is using marijuana daily after school, it is certainly going to interfere, in a dose-dependent manner, with attention and cognitive function. Sustained heavy use can lead to permanent cognitive deficits. It can also trigger or worsen anxiety or mood symptoms (contrary to much popular opinion).
Gathering a thorough substance use history is essential when assessing a teenager for difficulties with focus or attention, especially when these are accompanied by change in behavior and school performance. Remember, it is critical to interview these children without their parents present to invite them to be forthcoming with you.
History
While true ADHD should have been present throughout childhood, it is possible that the symptoms have become noticeable only in adolescence. For patients with very high intelligence and lower levels of impulsivity and hyperactivity, they might easily have “flown under the radar” during their elementary and even middle school years. Their difficulties with attention and focus might become apparent only when the volume and difficulty of schoolwork both are great enough that their intelligence is not enough to get good grades. That is, their problems with executive function, prioritizing, shifting sets, and completing tasks in a timely way make it impossible to keep up good grades when the work gets harder.
Your history should reveal a long history of dreaminess or distractibility, a tendency to lose and forget things, and the other symptoms of inattention. Did they often seem to not be listening when they were younger? Forget to hand in homework? Leave chores unfinished? Leave messes behind everywhere they went? These will not be definitive, but they do reassure that symptoms may have been present for a long time, even if school performance was considered fine until the workload got too large. If such problems were not present before puberty, consider whether a subtle learning disability could be impairing them as they face more challenging academic subjects.
If you have ruled out anxiety, mood, and substance use concerns, and helped them to address a sleep deficit, then you can proceed. It is worthwhile to get Vanderbilt Assessments as you would for a younger child. If they meet criteria, discuss the risks and benefits of medication, executive skills coaching, and environmental adjustments (extra time for tests, a less stimulating environment) that can help them explore academic challenges without the discouragement that ADHD can bring.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Pediatricians are increasingly expert in the assessment and treatment of attention-deficit/hyperactivity disorder. But what do you do when adolescents present to your office saying they think they have ADHD? While ADHD is a common and treatable disorder of youth, it is important to take special care when assessing an adolescent. Difficulties with attention and concentration are common symptoms for many different challenges of adolescence, and for ADHD to be the underlying cause, those symptoms must have started prior to adolescence (according to DSM-5, prior to the age of 12). When your adolescent patients or their parents come to your office complaining of inattention, it is important to consider the full range of possible explanations.
Sleep
We have written in this column previously about the challenges that adolescents face in getting adequate sleep consistently. Teenagers, on average, need more than 9 hours of sleep nightly and American teenagers get fewer than 6. This mismatch is because of physiologic shifts that move their natural sleep onset time significantly later, while school still starts early. It’s often compounded by other demands on their time, including homework, extracurricular activities, and the gravitational pull of social connections. Independent teenagers make their own decisions about how to manage their time and may feel sleep is optional, or manage their fatigue with naps and caffeine, both of which will further compromise the quality and efficiency of sleep.
Chronic sleep deprivation will present with difficulties with focus, attention, memory, and cognitive performance. Treatment of this problem with stimulants is likely to make the underlying poor sleep habits even worse. When your patient presents complaining of difficulty concentrating and worsening school performance, be sure to start with a thorough sleep history, and always provide guidance about the body’s need for sleep and healthy sleep habits.
Anxiety
Anxiety disorders are the most common psychiatric illnesses of youth, with estimates of as many as 30% of children and adolescents experiencing one. The true prevalence of ADHD is estimated to be about 4% of the population. Whether social phobia, generalized anxiety disorder, or even posttraumatic stress disorder, anxiety disorders interfere with attention as ruminative worry tends to distract those experiencing it. It can also affect attention and focus indirectly by interfering with restful sleep. Anxiety disorders can be difficult to identify, as the sufferers typically internalize their symptoms. But inquire about specific worries (such as speaking in front of others, meeting new people, or an illness or accident striking themselves or a loved one) and how much time they take up. Explore if worries fill their thoughts during quiet or downtime, and explore more about their worries. You may use a screening instrument such as the Pediatric Symptom Checklist or the SCARED, both of which will indicate a likely problem with anxiety. While it is possible to have comorbid ADHD with an anxiety disorder, the anxiety disorder will likely worsen with stimulants and should be treated first. These are usually curable illnesses and you may find that remission of anxiety symptoms resolves the attentional problems.
Depression
Mood disorders are less common than anxiety disorders in youth, but far more prevalent than ADHD. And depression is usually marked by serious difficulty concentrating across settings (including for things that were previously very interesting). A sullen teenager who is deeply self-critical about school performance would benefit from exploration of associated changes in mood, interests, energy, appetite, sleep, and for feelings of worthlessness, guilt, and suicidal thoughts. The PHQ9A is a simple, free screening instrument that is reasonable to use with every sick visit (and well-check) with your adolescent patients, given the risks of undetected and untreated depression. If your patient presents complaining of poor school performance, always screen for depression. As with anxiety disorders, comorbid ADHD is possible, but it is always recommended to treat the mood disorder first and then to assess for residual ADHD symptoms once the mood disorder is in remission.
Substance abuse
Adolescence is a time of exploration, and drug and alcohol use is common. While attentional impairment will happen with intoxication, occasional or rare use should not lead to consistent impairment in school. But when parents are more worried than their children about a significant change in school performance, it is important to screen for substance abuse. A child with a secret substance use disorder will often present with behavioral changes and deteriorating school performance and might deny any drug or alcohol use to parents. Indeed, stimulants have some street value and some patients may be seeking a stimulant prescription to sell or trade for other drugs. Regular marijuana use may present with only deteriorating school performance and no irritability or other noticeable behavioral changes. Marijuana is seen as safe and even healthy by many teenagers (and even many parents), and some youth may be using it recreationally or to manage difficulties with sleep, anxiety, or mood symptoms.
But there is compelling evidence that marijuana use causes cognitive impairment, including difficulty with sustaining attention, short-term memory, and processing speed, for as long as 24 hours after use. If a teenager is using marijuana daily after school, it is certainly going to interfere, in a dose-dependent manner, with attention and cognitive function. Sustained heavy use can lead to permanent cognitive deficits. It can also trigger or worsen anxiety or mood symptoms (contrary to much popular opinion).
Gathering a thorough substance use history is essential when assessing a teenager for difficulties with focus or attention, especially when these are accompanied by change in behavior and school performance. Remember, it is critical to interview these children without their parents present to invite them to be forthcoming with you.
History
While true ADHD should have been present throughout childhood, it is possible that the symptoms have become noticeable only in adolescence. For patients with very high intelligence and lower levels of impulsivity and hyperactivity, they might easily have “flown under the radar” during their elementary and even middle school years. Their difficulties with attention and focus might become apparent only when the volume and difficulty of schoolwork both are great enough that their intelligence is not enough to get good grades. That is, their problems with executive function, prioritizing, shifting sets, and completing tasks in a timely way make it impossible to keep up good grades when the work gets harder.
Your history should reveal a long history of dreaminess or distractibility, a tendency to lose and forget things, and the other symptoms of inattention. Did they often seem to not be listening when they were younger? Forget to hand in homework? Leave chores unfinished? Leave messes behind everywhere they went? These will not be definitive, but they do reassure that symptoms may have been present for a long time, even if school performance was considered fine until the workload got too large. If such problems were not present before puberty, consider whether a subtle learning disability could be impairing them as they face more challenging academic subjects.
If you have ruled out anxiety, mood, and substance use concerns, and helped them to address a sleep deficit, then you can proceed. It is worthwhile to get Vanderbilt Assessments as you would for a younger child. If they meet criteria, discuss the risks and benefits of medication, executive skills coaching, and environmental adjustments (extra time for tests, a less stimulating environment) that can help them explore academic challenges without the discouragement that ADHD can bring.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Pediatricians are increasingly expert in the assessment and treatment of attention-deficit/hyperactivity disorder. But what do you do when adolescents present to your office saying they think they have ADHD? While ADHD is a common and treatable disorder of youth, it is important to take special care when assessing an adolescent. Difficulties with attention and concentration are common symptoms for many different challenges of adolescence, and for ADHD to be the underlying cause, those symptoms must have started prior to adolescence (according to DSM-5, prior to the age of 12). When your adolescent patients or their parents come to your office complaining of inattention, it is important to consider the full range of possible explanations.
Sleep
We have written in this column previously about the challenges that adolescents face in getting adequate sleep consistently. Teenagers, on average, need more than 9 hours of sleep nightly and American teenagers get fewer than 6. This mismatch is because of physiologic shifts that move their natural sleep onset time significantly later, while school still starts early. It’s often compounded by other demands on their time, including homework, extracurricular activities, and the gravitational pull of social connections. Independent teenagers make their own decisions about how to manage their time and may feel sleep is optional, or manage their fatigue with naps and caffeine, both of which will further compromise the quality and efficiency of sleep.
Chronic sleep deprivation will present with difficulties with focus, attention, memory, and cognitive performance. Treatment of this problem with stimulants is likely to make the underlying poor sleep habits even worse. When your patient presents complaining of difficulty concentrating and worsening school performance, be sure to start with a thorough sleep history, and always provide guidance about the body’s need for sleep and healthy sleep habits.
Anxiety
Anxiety disorders are the most common psychiatric illnesses of youth, with estimates of as many as 30% of children and adolescents experiencing one. The true prevalence of ADHD is estimated to be about 4% of the population. Whether social phobia, generalized anxiety disorder, or even posttraumatic stress disorder, anxiety disorders interfere with attention as ruminative worry tends to distract those experiencing it. It can also affect attention and focus indirectly by interfering with restful sleep. Anxiety disorders can be difficult to identify, as the sufferers typically internalize their symptoms. But inquire about specific worries (such as speaking in front of others, meeting new people, or an illness or accident striking themselves or a loved one) and how much time they take up. Explore if worries fill their thoughts during quiet or downtime, and explore more about their worries. You may use a screening instrument such as the Pediatric Symptom Checklist or the SCARED, both of which will indicate a likely problem with anxiety. While it is possible to have comorbid ADHD with an anxiety disorder, the anxiety disorder will likely worsen with stimulants and should be treated first. These are usually curable illnesses and you may find that remission of anxiety symptoms resolves the attentional problems.
Depression
Mood disorders are less common than anxiety disorders in youth, but far more prevalent than ADHD. And depression is usually marked by serious difficulty concentrating across settings (including for things that were previously very interesting). A sullen teenager who is deeply self-critical about school performance would benefit from exploration of associated changes in mood, interests, energy, appetite, sleep, and for feelings of worthlessness, guilt, and suicidal thoughts. The PHQ9A is a simple, free screening instrument that is reasonable to use with every sick visit (and well-check) with your adolescent patients, given the risks of undetected and untreated depression. If your patient presents complaining of poor school performance, always screen for depression. As with anxiety disorders, comorbid ADHD is possible, but it is always recommended to treat the mood disorder first and then to assess for residual ADHD symptoms once the mood disorder is in remission.
Substance abuse
Adolescence is a time of exploration, and drug and alcohol use is common. While attentional impairment will happen with intoxication, occasional or rare use should not lead to consistent impairment in school. But when parents are more worried than their children about a significant change in school performance, it is important to screen for substance abuse. A child with a secret substance use disorder will often present with behavioral changes and deteriorating school performance and might deny any drug or alcohol use to parents. Indeed, stimulants have some street value and some patients may be seeking a stimulant prescription to sell or trade for other drugs. Regular marijuana use may present with only deteriorating school performance and no irritability or other noticeable behavioral changes. Marijuana is seen as safe and even healthy by many teenagers (and even many parents), and some youth may be using it recreationally or to manage difficulties with sleep, anxiety, or mood symptoms.
But there is compelling evidence that marijuana use causes cognitive impairment, including difficulty with sustaining attention, short-term memory, and processing speed, for as long as 24 hours after use. If a teenager is using marijuana daily after school, it is certainly going to interfere, in a dose-dependent manner, with attention and cognitive function. Sustained heavy use can lead to permanent cognitive deficits. It can also trigger or worsen anxiety or mood symptoms (contrary to much popular opinion).
Gathering a thorough substance use history is essential when assessing a teenager for difficulties with focus or attention, especially when these are accompanied by change in behavior and school performance. Remember, it is critical to interview these children without their parents present to invite them to be forthcoming with you.
History
While true ADHD should have been present throughout childhood, it is possible that the symptoms have become noticeable only in adolescence. For patients with very high intelligence and lower levels of impulsivity and hyperactivity, they might easily have “flown under the radar” during their elementary and even middle school years. Their difficulties with attention and focus might become apparent only when the volume and difficulty of schoolwork both are great enough that their intelligence is not enough to get good grades. That is, their problems with executive function, prioritizing, shifting sets, and completing tasks in a timely way make it impossible to keep up good grades when the work gets harder.
Your history should reveal a long history of dreaminess or distractibility, a tendency to lose and forget things, and the other symptoms of inattention. Did they often seem to not be listening when they were younger? Forget to hand in homework? Leave chores unfinished? Leave messes behind everywhere they went? These will not be definitive, but they do reassure that symptoms may have been present for a long time, even if school performance was considered fine until the workload got too large. If such problems were not present before puberty, consider whether a subtle learning disability could be impairing them as they face more challenging academic subjects.
If you have ruled out anxiety, mood, and substance use concerns, and helped them to address a sleep deficit, then you can proceed. It is worthwhile to get Vanderbilt Assessments as you would for a younger child. If they meet criteria, discuss the risks and benefits of medication, executive skills coaching, and environmental adjustments (extra time for tests, a less stimulating environment) that can help them explore academic challenges without the discouragement that ADHD can bring.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Pollution levels linked to physical and mental health problems
Other analyses of data have found environmental air pollution from sources such as car exhaust and factory output can trigger an inflammatory response in the body. What’s new about a study published in RMD Open is that it explored an association between long-term exposure to pollution and risk of autoimmune diseases, wrote Giovanni Adami, MD, of the University of Verona (Italy) and colleagues.
“Environmental air pollution, according to the World Health Organization, is a major risk to health and 99% of the population worldwide is living in places where recommendations for air quality are not met,” said Dr. Adami in an interview. The limited data on the precise role of air pollution on rheumatic diseases in particular prompted the study, he said.
To explore the potential link between air pollution exposure and autoimmune disease, the researchers reviewed medical information from 81,363 adults via a national medical database in Italy; the data were submitted between June 2016 and November 2020.
The average age of the study population was 65 years, and 92% were women; 22% had at least one coexisting health condition. Each study participant was linked to local environmental monitoring via their residential postcode.
The researchers obtained details about concentrations of particulate matter in the environment from the Italian Institute of Environmental Protection that included 617 monitoring stations in 110 Italian provinces. They focused on concentrations of 10 and 2.5 (PM10 and PM2.5).
Exposure thresholds of 30 mcg/m3 for PM10 and 20 mcg/m3 for PM2.5 are generally considered harmful to health, they noted. On average, the long-term exposure was 16 mcg/m3 for PM2.5 and 25 mcg/m3 for PM10 between 2013 and 2019.
Overall, 9,723 individuals (12%) were diagnosed with an autoimmune disease between 2016 and 2020.
Exposure to PM10 was associated with a 7% higher risk of diagnosis with any autoimmune disease for every 10 mcg/m3 increase in concentration, but no association appeared between PM2.5 exposure and increased risk of autoimmune diseases.
However, in an adjusted model, chronic exposure to PM10 above 30 mcg/m3 and to PM2.5 above 20 mcg/m3 were associated with a 12% and 13% higher risk, respectively, of any autoimmune disease.
Chronic exposure to high levels of PM10 was specifically associated with a higher risk of rheumatoid arthritis, but no other autoimmune diseases. Chronic exposure to high levels of PM2.5 was associated with a higher risk of rheumatoid arthritis, connective tissue diseases, and inflammatory bowel diseases.
In their discussion, the researchers noted that the smaller diameter of PM2.5 molecules fluctuate less in response to rain and other weather, compared with PM10 molecules, which might make them a more accurate predictor of exposure to chronic air pollution.
The study findings were limited by several factors including the observational design, which prohibits the establishment of cause, and a lack of data on the start of symptoms and dates of diagnoses for autoimmune diseases, the researchers noted. Other limitations include the high percentage of older women in the study, which may limit generalizability, and the inability to account for additional personal exposure to pollutants outside of the environmental exposure, they said.
However, the results were strengthened by the large sample size and wide geographic distribution with variable pollution exposure, they said.
“Unfortunately, we were not surprised at all,” by the findings, Dr. Adami said in an interview.
“The biological rationale underpinning our findings is strong. Nevertheless, the magnitude of the effect was overwhelming. In addition, we saw an effect even at threshold of exposure that is widely considered as safe,” Dr. Adami noted.
Clinicians have been taught to consider cigarette smoking or other lifestyle behaviors as major risk factors for the development of several autoimmune diseases, said Dr. Adami. “In the future, we probably should include air pollution exposure as a risk factor as well. Interestingly, there is also accumulating evidence linking acute exposure to environmental air pollution with flares of chronic arthritis,” he said.
“Our study could have direct societal and political consequences,” and might help direct policy makers’ decisions on addressing strategies aimed to reduce fossil emissions, he said. As for additional research, “we certainly need multination studies to confirm our results on a larger scale,” Dr. Adami emphasized. “In addition, it is time to take action and start designing interventions aimed to reduce acute and chronic exposure to air pollution in patients suffering from RMDs.”
Consider the big picture of air quality
The Italian study is especially timely “given our evolving and emerging understanding of environmental risk factors for acute and chronic diseases, which we must first understand before we can address,” said Eileen Barrett, MD, of the University of New Mexico, Albuquerque, in an interview.

“I am largely surprised about the findings, as most physicians aren’t studying ambient air quality and risk for autoimmune disease,” said Dr. Barrett. “More often we think of air quality when we think of risk for respiratory diseases than autoimmune diseases, per se,” she said.
“There are several take-home messages from this study,” said Dr. Barrett. “The first is that we need more research to understand the consequences of air pollutants on health. Second, this study reminds us to think broadly about how air quality and our environment can affect health. And third, all clinicians should be committed to promoting science that can improve public health and reduce death and disability,” she emphasized.
The findings do not specifically reflect associations between pollution and other conditions such as chronic obstructive pulmonary disease and asthma although previous studies have shown an association between asthma and COPD exacerbations and air pollution, Dr. Barrett said.
“Further research will be needed to confirm the associations reported in this study,” Dr. Barrett said.
More research in other countries, including research related to other autoimmune diseases, and with other datasets on population and community level risks from poor air quality, would be helpful, and that information could be used to advise smart public policy, Dr. Barrett added.
Air pollution’s mental health impact
Air pollution’s effects extend beyond physical to the psychological, a new study of depression in teenagers showed. This study was published in Developmental Psychology.
Previous research on the environmental factors associated with depressive symptoms in teens has focused mainly on individual and family level contributors; the impact of the physical environment has not been well studied, the investigators, Erika M. Manczak, PhD, of the University of Denver and colleagues, wrote.
In their paper, the authors found a significant impact of neighborhood ozone exposure on the trajectory of depressive symptoms in teens over a 4-year period.
“Given that inhaling pollution activates biological pathways implicated in the development of depression, including immune, cardiovascular, and neurodevelopmental processes, exposure to ambient air pollution may influence the development and/or trajectory of depressive symptoms in youth,” they said.
The researchers recruited 213 adolescents in the San Francisco Bay area through local advertisements. The participants were aged 9-13 years at baseline, with an average age of 11 years. A total of 121 were female, 47% were white, 8.5% were African American, 12.3% were Asian, 10.4% were nonwhite Latin, and 21.7% were biracial or another ethnicity. The participants self-reported depressive symptoms and other psychopathology symptoms up to three times during the study period. Ozone exposure was calculated based on home addresses.
After controlling for other personal, family, and neighborhood variables, the researchers found that higher levels of ozone exposure were significantly associated with increased depressive symptoms over time, and the slope of trajectory of depressive symptoms became steeper as the ozone levels increased (P less than .001). Ozone did not significantly predict the trajectory of any other psychopathology symptoms.
“The results of this study provide preliminary support for the possibility that ozone is an overlooked contributor to the development or course of youth depressive symptoms,” the researchers wrote in their discussion.
“Interestingly, the association between ozone and symptom trajectories as measured by Anxious/Depressed subscale of the [Youth Self-Report] was not as strong as it was for the [Children’s Depression Inventory-Short Version] or Withdrawn/Depressed scales, suggesting that associations are more robust for behavioral withdrawal symptoms of depression than for other types of symptoms,” they noted.
The study findings were limited by the use of self-reports and by the inability of the study design to show causality, the researchers said. Other limitations include the use of average assessments of ozone that are less precise, lack of assessment of biological pathways for risk, lack of formal psychiatric diagnoses, and the small geographic region included in the study, they said.
However, the results provide preliminary evidence that ozone exposure is a potential contributing factor to depressive symptoms in youth, and serve as a jumping-off point for future research, they noted. Future studies should address changes in systemic inflammation, neurodevelopment, or stress reactivity, as well as concurrent psychosocial or biological factors, and temporal associations between air pollution and mental health symptoms, they concluded.
Environmental factors drive inflammatory responses
Peter L. Loper Jr., MD, considers the findings of the Developmental Psychology study to be unsurprising but important – because air pollution is simply getting worse.

“As the study authors cite, there is sufficient data correlating ozone to negative physical health outcomes in youth, but a paucity of data exploring the impact of poor air quality on mental health outcomes in this demographic,” noted Dr. Loper, of the University of South Carolina, Columbia, in an interview.
“As discussed by the study researchers, any environmental exposure that increases immune-mediated inflammation can result in negative health outcomes. In fact, there is already data to suggest that similar cytokines, or immune cell signalers, that get released by our immune system due to environmental exposures and that contribute to asthma, may also be implicated in depression and other mental health problems,” he noted.
“Just like downstream symptom indicators of physical illnesses such as asthma are secondary to immune-mediated pulmonary inflammation, downstream symptom indicators of mental illness, such as depression, are secondary to immune-mediated neuroinflammation,” Dr. Loper emphasized. “The most well-characterized upstream phenomenon perpetuating the downstream symptom indicators of depression involve neuroinflammatory states due to psychosocial and relational factors such as chronic stress, poor relationships, or substance use. However, any environmental factor that triggers an immune response and inflammation can promote neuroinflammation that manifests as symptoms of mental illness.”
The message for teens with depression and their families is that “we are a product of our environment,” Dr. Loper said. “When our environments are proinflammatory, or cause our immune system to become overactive, then we will develop illness; however, the most potent mediator of inflammation in the brain, and the downstream symptoms of depression, is our relationships with those we love most,” he said.
Dr. Loper suggested research aimed at identifying other sources of immune-mediated inflammation caused by physical environments and better understanding how environmental phenomenon like ozone may compound previously established risk factors for mental illness could be useful.
The RMD Open study received no outside funding, and its authors had no financial conflicts.
The Developmental Psychology study was supported by the National Institute of Mental Health and the Stanford University Precision Health and Integrated Diagnostics Center. The researchers for that report, and Dr. Loper and Dr. Barrett had no conflicts to disclose.
Other analyses of data have found environmental air pollution from sources such as car exhaust and factory output can trigger an inflammatory response in the body. What’s new about a study published in RMD Open is that it explored an association between long-term exposure to pollution and risk of autoimmune diseases, wrote Giovanni Adami, MD, of the University of Verona (Italy) and colleagues.
“Environmental air pollution, according to the World Health Organization, is a major risk to health and 99% of the population worldwide is living in places where recommendations for air quality are not met,” said Dr. Adami in an interview. The limited data on the precise role of air pollution on rheumatic diseases in particular prompted the study, he said.
To explore the potential link between air pollution exposure and autoimmune disease, the researchers reviewed medical information from 81,363 adults via a national medical database in Italy; the data were submitted between June 2016 and November 2020.
The average age of the study population was 65 years, and 92% were women; 22% had at least one coexisting health condition. Each study participant was linked to local environmental monitoring via their residential postcode.
The researchers obtained details about concentrations of particulate matter in the environment from the Italian Institute of Environmental Protection that included 617 monitoring stations in 110 Italian provinces. They focused on concentrations of 10 and 2.5 (PM10 and PM2.5).
Exposure thresholds of 30 mcg/m3 for PM10 and 20 mcg/m3 for PM2.5 are generally considered harmful to health, they noted. On average, the long-term exposure was 16 mcg/m3 for PM2.5 and 25 mcg/m3 for PM10 between 2013 and 2019.
Overall, 9,723 individuals (12%) were diagnosed with an autoimmune disease between 2016 and 2020.
Exposure to PM10 was associated with a 7% higher risk of diagnosis with any autoimmune disease for every 10 mcg/m3 increase in concentration, but no association appeared between PM2.5 exposure and increased risk of autoimmune diseases.
However, in an adjusted model, chronic exposure to PM10 above 30 mcg/m3 and to PM2.5 above 20 mcg/m3 were associated with a 12% and 13% higher risk, respectively, of any autoimmune disease.
Chronic exposure to high levels of PM10 was specifically associated with a higher risk of rheumatoid arthritis, but no other autoimmune diseases. Chronic exposure to high levels of PM2.5 was associated with a higher risk of rheumatoid arthritis, connective tissue diseases, and inflammatory bowel diseases.
In their discussion, the researchers noted that the smaller diameter of PM2.5 molecules fluctuate less in response to rain and other weather, compared with PM10 molecules, which might make them a more accurate predictor of exposure to chronic air pollution.
The study findings were limited by several factors including the observational design, which prohibits the establishment of cause, and a lack of data on the start of symptoms and dates of diagnoses for autoimmune diseases, the researchers noted. Other limitations include the high percentage of older women in the study, which may limit generalizability, and the inability to account for additional personal exposure to pollutants outside of the environmental exposure, they said.
However, the results were strengthened by the large sample size and wide geographic distribution with variable pollution exposure, they said.
“Unfortunately, we were not surprised at all,” by the findings, Dr. Adami said in an interview.
“The biological rationale underpinning our findings is strong. Nevertheless, the magnitude of the effect was overwhelming. In addition, we saw an effect even at threshold of exposure that is widely considered as safe,” Dr. Adami noted.
Clinicians have been taught to consider cigarette smoking or other lifestyle behaviors as major risk factors for the development of several autoimmune diseases, said Dr. Adami. “In the future, we probably should include air pollution exposure as a risk factor as well. Interestingly, there is also accumulating evidence linking acute exposure to environmental air pollution with flares of chronic arthritis,” he said.
“Our study could have direct societal and political consequences,” and might help direct policy makers’ decisions on addressing strategies aimed to reduce fossil emissions, he said. As for additional research, “we certainly need multination studies to confirm our results on a larger scale,” Dr. Adami emphasized. “In addition, it is time to take action and start designing interventions aimed to reduce acute and chronic exposure to air pollution in patients suffering from RMDs.”
Consider the big picture of air quality
The Italian study is especially timely “given our evolving and emerging understanding of environmental risk factors for acute and chronic diseases, which we must first understand before we can address,” said Eileen Barrett, MD, of the University of New Mexico, Albuquerque, in an interview.
“I am largely surprised about the findings, as most physicians aren’t studying ambient air quality and risk for autoimmune disease,” said Dr. Barrett. “More often we think of air quality when we think of risk for respiratory diseases than autoimmune diseases, per se,” she said.
“There are several take-home messages from this study,” said Dr. Barrett. “The first is that we need more research to understand the consequences of air pollutants on health. Second, this study reminds us to think broadly about how air quality and our environment can affect health. And third, all clinicians should be committed to promoting science that can improve public health and reduce death and disability,” she emphasized.
The findings do not specifically reflect associations between pollution and other conditions such as chronic obstructive pulmonary disease and asthma although previous studies have shown an association between asthma and COPD exacerbations and air pollution, Dr. Barrett said.
“Further research will be needed to confirm the associations reported in this study,” Dr. Barrett said.
More research in other countries, including research related to other autoimmune diseases, and with other datasets on population and community level risks from poor air quality, would be helpful, and that information could be used to advise smart public policy, Dr. Barrett added.
Air pollution’s mental health impact
Air pollution’s effects extend beyond physical to the psychological, a new study of depression in teenagers showed. This study was published in Developmental Psychology.
Previous research on the environmental factors associated with depressive symptoms in teens has focused mainly on individual and family level contributors; the impact of the physical environment has not been well studied, the investigators, Erika M. Manczak, PhD, of the University of Denver and colleagues, wrote.
In their paper, the authors found a significant impact of neighborhood ozone exposure on the trajectory of depressive symptoms in teens over a 4-year period.
“Given that inhaling pollution activates biological pathways implicated in the development of depression, including immune, cardiovascular, and neurodevelopmental processes, exposure to ambient air pollution may influence the development and/or trajectory of depressive symptoms in youth,” they said.
The researchers recruited 213 adolescents in the San Francisco Bay area through local advertisements. The participants were aged 9-13 years at baseline, with an average age of 11 years. A total of 121 were female, 47% were white, 8.5% were African American, 12.3% were Asian, 10.4% were nonwhite Latin, and 21.7% were biracial or another ethnicity. The participants self-reported depressive symptoms and other psychopathology symptoms up to three times during the study period. Ozone exposure was calculated based on home addresses.
After controlling for other personal, family, and neighborhood variables, the researchers found that higher levels of ozone exposure were significantly associated with increased depressive symptoms over time, and the slope of trajectory of depressive symptoms became steeper as the ozone levels increased (P less than .001). Ozone did not significantly predict the trajectory of any other psychopathology symptoms.
“The results of this study provide preliminary support for the possibility that ozone is an overlooked contributor to the development or course of youth depressive symptoms,” the researchers wrote in their discussion.
“Interestingly, the association between ozone and symptom trajectories as measured by Anxious/Depressed subscale of the [Youth Self-Report] was not as strong as it was for the [Children’s Depression Inventory-Short Version] or Withdrawn/Depressed scales, suggesting that associations are more robust for behavioral withdrawal symptoms of depression than for other types of symptoms,” they noted.
The study findings were limited by the use of self-reports and by the inability of the study design to show causality, the researchers said. Other limitations include the use of average assessments of ozone that are less precise, lack of assessment of biological pathways for risk, lack of formal psychiatric diagnoses, and the small geographic region included in the study, they said.
However, the results provide preliminary evidence that ozone exposure is a potential contributing factor to depressive symptoms in youth, and serve as a jumping-off point for future research, they noted. Future studies should address changes in systemic inflammation, neurodevelopment, or stress reactivity, as well as concurrent psychosocial or biological factors, and temporal associations between air pollution and mental health symptoms, they concluded.
Environmental factors drive inflammatory responses
Peter L. Loper Jr., MD, considers the findings of the Developmental Psychology study to be unsurprising but important – because air pollution is simply getting worse.
“As the study authors cite, there is sufficient data correlating ozone to negative physical health outcomes in youth, but a paucity of data exploring the impact of poor air quality on mental health outcomes in this demographic,” noted Dr. Loper, of the University of South Carolina, Columbia, in an interview.
“As discussed by the study researchers, any environmental exposure that increases immune-mediated inflammation can result in negative health outcomes. In fact, there is already data to suggest that similar cytokines, or immune cell signalers, that get released by our immune system due to environmental exposures and that contribute to asthma, may also be implicated in depression and other mental health problems,” he noted.
“Just like downstream symptom indicators of physical illnesses such as asthma are secondary to immune-mediated pulmonary inflammation, downstream symptom indicators of mental illness, such as depression, are secondary to immune-mediated neuroinflammation,” Dr. Loper emphasized. “The most well-characterized upstream phenomenon perpetuating the downstream symptom indicators of depression involve neuroinflammatory states due to psychosocial and relational factors such as chronic stress, poor relationships, or substance use. However, any environmental factor that triggers an immune response and inflammation can promote neuroinflammation that manifests as symptoms of mental illness.”
The message for teens with depression and their families is that “we are a product of our environment,” Dr. Loper said. “When our environments are proinflammatory, or cause our immune system to become overactive, then we will develop illness; however, the most potent mediator of inflammation in the brain, and the downstream symptoms of depression, is our relationships with those we love most,” he said.
Dr. Loper suggested research aimed at identifying other sources of immune-mediated inflammation caused by physical environments and better understanding how environmental phenomenon like ozone may compound previously established risk factors for mental illness could be useful.
The RMD Open study received no outside funding, and its authors had no financial conflicts.
The Developmental Psychology study was supported by the National Institute of Mental Health and the Stanford University Precision Health and Integrated Diagnostics Center. The researchers for that report, and Dr. Loper and Dr. Barrett had no conflicts to disclose.
Other analyses of data have found environmental air pollution from sources such as car exhaust and factory output can trigger an inflammatory response in the body. What’s new about a study published in RMD Open is that it explored an association between long-term exposure to pollution and risk of autoimmune diseases, wrote Giovanni Adami, MD, of the University of Verona (Italy) and colleagues.
“Environmental air pollution, according to the World Health Organization, is a major risk to health and 99% of the population worldwide is living in places where recommendations for air quality are not met,” said Dr. Adami in an interview. The limited data on the precise role of air pollution on rheumatic diseases in particular prompted the study, he said.
To explore the potential link between air pollution exposure and autoimmune disease, the researchers reviewed medical information from 81,363 adults via a national medical database in Italy; the data were submitted between June 2016 and November 2020.
The average age of the study population was 65 years, and 92% were women; 22% had at least one coexisting health condition. Each study participant was linked to local environmental monitoring via their residential postcode.
The researchers obtained details about concentrations of particulate matter in the environment from the Italian Institute of Environmental Protection that included 617 monitoring stations in 110 Italian provinces. They focused on concentrations of 10 and 2.5 (PM10 and PM2.5).
Exposure thresholds of 30 mcg/m3 for PM10 and 20 mcg/m3 for PM2.5 are generally considered harmful to health, they noted. On average, the long-term exposure was 16 mcg/m3 for PM2.5 and 25 mcg/m3 for PM10 between 2013 and 2019.
Overall, 9,723 individuals (12%) were diagnosed with an autoimmune disease between 2016 and 2020.
Exposure to PM10 was associated with a 7% higher risk of diagnosis with any autoimmune disease for every 10 mcg/m3 increase in concentration, but no association appeared between PM2.5 exposure and increased risk of autoimmune diseases.
However, in an adjusted model, chronic exposure to PM10 above 30 mcg/m3 and to PM2.5 above 20 mcg/m3 were associated with a 12% and 13% higher risk, respectively, of any autoimmune disease.
Chronic exposure to high levels of PM10 was specifically associated with a higher risk of rheumatoid arthritis, but no other autoimmune diseases. Chronic exposure to high levels of PM2.5 was associated with a higher risk of rheumatoid arthritis, connective tissue diseases, and inflammatory bowel diseases.
In their discussion, the researchers noted that the smaller diameter of PM2.5 molecules fluctuate less in response to rain and other weather, compared with PM10 molecules, which might make them a more accurate predictor of exposure to chronic air pollution.
The study findings were limited by several factors including the observational design, which prohibits the establishment of cause, and a lack of data on the start of symptoms and dates of diagnoses for autoimmune diseases, the researchers noted. Other limitations include the high percentage of older women in the study, which may limit generalizability, and the inability to account for additional personal exposure to pollutants outside of the environmental exposure, they said.
However, the results were strengthened by the large sample size and wide geographic distribution with variable pollution exposure, they said.
“Unfortunately, we were not surprised at all,” by the findings, Dr. Adami said in an interview.
“The biological rationale underpinning our findings is strong. Nevertheless, the magnitude of the effect was overwhelming. In addition, we saw an effect even at threshold of exposure that is widely considered as safe,” Dr. Adami noted.
Clinicians have been taught to consider cigarette smoking or other lifestyle behaviors as major risk factors for the development of several autoimmune diseases, said Dr. Adami. “In the future, we probably should include air pollution exposure as a risk factor as well. Interestingly, there is also accumulating evidence linking acute exposure to environmental air pollution with flares of chronic arthritis,” he said.
“Our study could have direct societal and political consequences,” and might help direct policy makers’ decisions on addressing strategies aimed to reduce fossil emissions, he said. As for additional research, “we certainly need multination studies to confirm our results on a larger scale,” Dr. Adami emphasized. “In addition, it is time to take action and start designing interventions aimed to reduce acute and chronic exposure to air pollution in patients suffering from RMDs.”
Consider the big picture of air quality
The Italian study is especially timely “given our evolving and emerging understanding of environmental risk factors for acute and chronic diseases, which we must first understand before we can address,” said Eileen Barrett, MD, of the University of New Mexico, Albuquerque, in an interview.
“I am largely surprised about the findings, as most physicians aren’t studying ambient air quality and risk for autoimmune disease,” said Dr. Barrett. “More often we think of air quality when we think of risk for respiratory diseases than autoimmune diseases, per se,” she said.
“There are several take-home messages from this study,” said Dr. Barrett. “The first is that we need more research to understand the consequences of air pollutants on health. Second, this study reminds us to think broadly about how air quality and our environment can affect health. And third, all clinicians should be committed to promoting science that can improve public health and reduce death and disability,” she emphasized.
The findings do not specifically reflect associations between pollution and other conditions such as chronic obstructive pulmonary disease and asthma although previous studies have shown an association between asthma and COPD exacerbations and air pollution, Dr. Barrett said.
“Further research will be needed to confirm the associations reported in this study,” Dr. Barrett said.
More research in other countries, including research related to other autoimmune diseases, and with other datasets on population and community level risks from poor air quality, would be helpful, and that information could be used to advise smart public policy, Dr. Barrett added.
Air pollution’s mental health impact
Air pollution’s effects extend beyond physical to the psychological, a new study of depression in teenagers showed. This study was published in Developmental Psychology.
Previous research on the environmental factors associated with depressive symptoms in teens has focused mainly on individual and family level contributors; the impact of the physical environment has not been well studied, the investigators, Erika M. Manczak, PhD, of the University of Denver and colleagues, wrote.
In their paper, the authors found a significant impact of neighborhood ozone exposure on the trajectory of depressive symptoms in teens over a 4-year period.
“Given that inhaling pollution activates biological pathways implicated in the development of depression, including immune, cardiovascular, and neurodevelopmental processes, exposure to ambient air pollution may influence the development and/or trajectory of depressive symptoms in youth,” they said.
The researchers recruited 213 adolescents in the San Francisco Bay area through local advertisements. The participants were aged 9-13 years at baseline, with an average age of 11 years. A total of 121 were female, 47% were white, 8.5% were African American, 12.3% were Asian, 10.4% were nonwhite Latin, and 21.7% were biracial or another ethnicity. The participants self-reported depressive symptoms and other psychopathology symptoms up to three times during the study period. Ozone exposure was calculated based on home addresses.
After controlling for other personal, family, and neighborhood variables, the researchers found that higher levels of ozone exposure were significantly associated with increased depressive symptoms over time, and the slope of trajectory of depressive symptoms became steeper as the ozone levels increased (P less than .001). Ozone did not significantly predict the trajectory of any other psychopathology symptoms.
“The results of this study provide preliminary support for the possibility that ozone is an overlooked contributor to the development or course of youth depressive symptoms,” the researchers wrote in their discussion.
“Interestingly, the association between ozone and symptom trajectories as measured by Anxious/Depressed subscale of the [Youth Self-Report] was not as strong as it was for the [Children’s Depression Inventory-Short Version] or Withdrawn/Depressed scales, suggesting that associations are more robust for behavioral withdrawal symptoms of depression than for other types of symptoms,” they noted.
The study findings were limited by the use of self-reports and by the inability of the study design to show causality, the researchers said. Other limitations include the use of average assessments of ozone that are less precise, lack of assessment of biological pathways for risk, lack of formal psychiatric diagnoses, and the small geographic region included in the study, they said.
However, the results provide preliminary evidence that ozone exposure is a potential contributing factor to depressive symptoms in youth, and serve as a jumping-off point for future research, they noted. Future studies should address changes in systemic inflammation, neurodevelopment, or stress reactivity, as well as concurrent psychosocial or biological factors, and temporal associations between air pollution and mental health symptoms, they concluded.
Environmental factors drive inflammatory responses
Peter L. Loper Jr., MD, considers the findings of the Developmental Psychology study to be unsurprising but important – because air pollution is simply getting worse.
“As the study authors cite, there is sufficient data correlating ozone to negative physical health outcomes in youth, but a paucity of data exploring the impact of poor air quality on mental health outcomes in this demographic,” noted Dr. Loper, of the University of South Carolina, Columbia, in an interview.
“As discussed by the study researchers, any environmental exposure that increases immune-mediated inflammation can result in negative health outcomes. In fact, there is already data to suggest that similar cytokines, or immune cell signalers, that get released by our immune system due to environmental exposures and that contribute to asthma, may also be implicated in depression and other mental health problems,” he noted.
“Just like downstream symptom indicators of physical illnesses such as asthma are secondary to immune-mediated pulmonary inflammation, downstream symptom indicators of mental illness, such as depression, are secondary to immune-mediated neuroinflammation,” Dr. Loper emphasized. “The most well-characterized upstream phenomenon perpetuating the downstream symptom indicators of depression involve neuroinflammatory states due to psychosocial and relational factors such as chronic stress, poor relationships, or substance use. However, any environmental factor that triggers an immune response and inflammation can promote neuroinflammation that manifests as symptoms of mental illness.”
The message for teens with depression and their families is that “we are a product of our environment,” Dr. Loper said. “When our environments are proinflammatory, or cause our immune system to become overactive, then we will develop illness; however, the most potent mediator of inflammation in the brain, and the downstream symptoms of depression, is our relationships with those we love most,” he said.
Dr. Loper suggested research aimed at identifying other sources of immune-mediated inflammation caused by physical environments and better understanding how environmental phenomenon like ozone may compound previously established risk factors for mental illness could be useful.
The RMD Open study received no outside funding, and its authors had no financial conflicts.
The Developmental Psychology study was supported by the National Institute of Mental Health and the Stanford University Precision Health and Integrated Diagnostics Center. The researchers for that report, and Dr. Loper and Dr. Barrett had no conflicts to disclose.
FROM RMD OPEN

Relax. The dog-tor will see you now
Patients in the emergency room who spent just 10 minutes with a trained therapy dog reported less pain, anxiety, and depression and improved well-being, researchers from the University of Saskatchewan in Canada found.
“The ER is an important community resource but also a scary place for most people,” James Stempien, MD, provincial department head of emergency medicine with the Saskatchewan Health Authority, who worked on the study, said in an interview.
“People tend to visit the ER on the worst day of their life, either for them or a loved one. Interacting with a therapy dog can make the ER visit a little calmer. We have also seen benefit for the staff that get to interact with the dogs as well,” he says.
“Thanks to our wonderful therapy dog volunteer teams, the cost is minimal and the result is priceless,” Dr. Stempien says.
The study, published in the journal PLOS One, builds on earlier “uncontrolled” studies by the Saskatchewan team.
Those studies showed that most ER patients wanted to visit with the therapy dog, if given a chance. After the encounter, patients reported feeling more comfortable, happier, and less distressed while waiting in the ER.
“A controlled trial was the natural next step,” says study investigator Colleen Dell, PhD, of One Health and Wellness at the University of Saskatchewan.
The study was done at the Royal University Hospital (RUH) in Saskatoon, Saskatchewan -- the first emergency department in Canada to introduce therapy dogs to improve the experience of waiting patients.
Nearly 200 adults visiting the ER received either a 10-minute visit with a therapy dog and its handler in addition to usual care or just usual care.
“This did not occur in patients in the ER who did not visit with a therapy dog.
“This gives us confidence in the intervention,” Dr. Dell says.
Pain is a major reason that patients come to the ER, and interactions with a therapy dog may distract from that pain, the researchers believe.
The study results lend more evidence to research that shows animals can help in medical settings, says Kara Rauscher, a licensed social worker and interim director of behavioral health for Nashville CARES in Tennessee, who wasn’t involved in the study.
“There are clearly opportunities to replicate this study in other emergency departments to strengthen our understanding of the potential benefits of these programs,” she says.
Part of her work at Nashville CARES, an AIDS service organization, has been supporting care that moves away from questions like, “What’s wrong with you?” to patient-focused questions like, “What happened to you?” It is a practice known as trauma-informed care.
“This includes bringing in therapy dogs for staff to spend time with during the workday; anecdotally, our staff reported a reduction in stress and improvements in mood,” Ms. Rauscher says.
A version of this article first appeared on WebMD.com.
Patients in the emergency room who spent just 10 minutes with a trained therapy dog reported less pain, anxiety, and depression and improved well-being, researchers from the University of Saskatchewan in Canada found.
“The ER is an important community resource but also a scary place for most people,” James Stempien, MD, provincial department head of emergency medicine with the Saskatchewan Health Authority, who worked on the study, said in an interview.
“People tend to visit the ER on the worst day of their life, either for them or a loved one. Interacting with a therapy dog can make the ER visit a little calmer. We have also seen benefit for the staff that get to interact with the dogs as well,” he says.
“Thanks to our wonderful therapy dog volunteer teams, the cost is minimal and the result is priceless,” Dr. Stempien says.
The study, published in the journal PLOS One, builds on earlier “uncontrolled” studies by the Saskatchewan team.
Those studies showed that most ER patients wanted to visit with the therapy dog, if given a chance. After the encounter, patients reported feeling more comfortable, happier, and less distressed while waiting in the ER.
“A controlled trial was the natural next step,” says study investigator Colleen Dell, PhD, of One Health and Wellness at the University of Saskatchewan.
The study was done at the Royal University Hospital (RUH) in Saskatoon, Saskatchewan -- the first emergency department in Canada to introduce therapy dogs to improve the experience of waiting patients.
Nearly 200 adults visiting the ER received either a 10-minute visit with a therapy dog and its handler in addition to usual care or just usual care.
“This did not occur in patients in the ER who did not visit with a therapy dog.
“This gives us confidence in the intervention,” Dr. Dell says.
Pain is a major reason that patients come to the ER, and interactions with a therapy dog may distract from that pain, the researchers believe.
The study results lend more evidence to research that shows animals can help in medical settings, says Kara Rauscher, a licensed social worker and interim director of behavioral health for Nashville CARES in Tennessee, who wasn’t involved in the study.
“There are clearly opportunities to replicate this study in other emergency departments to strengthen our understanding of the potential benefits of these programs,” she says.
Part of her work at Nashville CARES, an AIDS service organization, has been supporting care that moves away from questions like, “What’s wrong with you?” to patient-focused questions like, “What happened to you?” It is a practice known as trauma-informed care.
“This includes bringing in therapy dogs for staff to spend time with during the workday; anecdotally, our staff reported a reduction in stress and improvements in mood,” Ms. Rauscher says.
A version of this article first appeared on WebMD.com.
Patients in the emergency room who spent just 10 minutes with a trained therapy dog reported less pain, anxiety, and depression and improved well-being, researchers from the University of Saskatchewan in Canada found.
“The ER is an important community resource but also a scary place for most people,” James Stempien, MD, provincial department head of emergency medicine with the Saskatchewan Health Authority, who worked on the study, said in an interview.
“People tend to visit the ER on the worst day of their life, either for them or a loved one. Interacting with a therapy dog can make the ER visit a little calmer. We have also seen benefit for the staff that get to interact with the dogs as well,” he says.
“Thanks to our wonderful therapy dog volunteer teams, the cost is minimal and the result is priceless,” Dr. Stempien says.
The study, published in the journal PLOS One, builds on earlier “uncontrolled” studies by the Saskatchewan team.
Those studies showed that most ER patients wanted to visit with the therapy dog, if given a chance. After the encounter, patients reported feeling more comfortable, happier, and less distressed while waiting in the ER.
“A controlled trial was the natural next step,” says study investigator Colleen Dell, PhD, of One Health and Wellness at the University of Saskatchewan.
The study was done at the Royal University Hospital (RUH) in Saskatoon, Saskatchewan -- the first emergency department in Canada to introduce therapy dogs to improve the experience of waiting patients.
Nearly 200 adults visiting the ER received either a 10-minute visit with a therapy dog and its handler in addition to usual care or just usual care.
“This did not occur in patients in the ER who did not visit with a therapy dog.
“This gives us confidence in the intervention,” Dr. Dell says.
Pain is a major reason that patients come to the ER, and interactions with a therapy dog may distract from that pain, the researchers believe.
The study results lend more evidence to research that shows animals can help in medical settings, says Kara Rauscher, a licensed social worker and interim director of behavioral health for Nashville CARES in Tennessee, who wasn’t involved in the study.
“There are clearly opportunities to replicate this study in other emergency departments to strengthen our understanding of the potential benefits of these programs,” she says.
Part of her work at Nashville CARES, an AIDS service organization, has been supporting care that moves away from questions like, “What’s wrong with you?” to patient-focused questions like, “What happened to you?” It is a practice known as trauma-informed care.
“This includes bringing in therapy dogs for staff to spend time with during the workday; anecdotally, our staff reported a reduction in stress and improvements in mood,” Ms. Rauscher says.
A version of this article first appeared on WebMD.com.
FROM PLOS ONE
FDA clears once-weekly transdermal patch for Alzheimer’s
Adlarity is the first and only once-weekly patch to continuously deliver consistent doses of the acetylcholinesterase inhibitor through the skin, bypassing the digestive system and resulting in low likelihood of gastrointestinal side effects associated with oral donepezil, the company said in a press release.
Each patch delivers either 5 mg or 10 mg of donepezil daily for 7 days. After that, it is removed and a new patch is applied.
“The availability of a once-weekly patch formulation of donepezil has the potential to substantially benefit patients, caregivers, and health care providers,” Pierre Tariot, MD, director of the Banner Alzheimer’s Institute, Phoenix, said in the release.
“It offers effective, well-tolerated, and stable dosing for 7 days for patients who cannot take daily oral donepezil reliably because of impaired memory. It can also offer benefits for those patients who have diminished ability to swallow or have GI side effects associated with ingestion of oral donepezil,” Dr. Tariot added.
The FDA approved Adlarity through the 505(b)(2) regulatory pathway, which allows the agency to refer to previous findings of safety and efficacy for an already-approved product, as well as to review findings from further studies of the product.
The company expects the donepezil transdermal patch to be available in early Fall 2022.
A version of this article first appeared on Medscape.com.
Adlarity is the first and only once-weekly patch to continuously deliver consistent doses of the acetylcholinesterase inhibitor through the skin, bypassing the digestive system and resulting in low likelihood of gastrointestinal side effects associated with oral donepezil, the company said in a press release.
Each patch delivers either 5 mg or 10 mg of donepezil daily for 7 days. After that, it is removed and a new patch is applied.
“The availability of a once-weekly patch formulation of donepezil has the potential to substantially benefit patients, caregivers, and health care providers,” Pierre Tariot, MD, director of the Banner Alzheimer’s Institute, Phoenix, said in the release.
“It offers effective, well-tolerated, and stable dosing for 7 days for patients who cannot take daily oral donepezil reliably because of impaired memory. It can also offer benefits for those patients who have diminished ability to swallow or have GI side effects associated with ingestion of oral donepezil,” Dr. Tariot added.
The FDA approved Adlarity through the 505(b)(2) regulatory pathway, which allows the agency to refer to previous findings of safety and efficacy for an already-approved product, as well as to review findings from further studies of the product.
The company expects the donepezil transdermal patch to be available in early Fall 2022.
A version of this article first appeared on Medscape.com.
Adlarity is the first and only once-weekly patch to continuously deliver consistent doses of the acetylcholinesterase inhibitor through the skin, bypassing the digestive system and resulting in low likelihood of gastrointestinal side effects associated with oral donepezil, the company said in a press release.
Each patch delivers either 5 mg or 10 mg of donepezil daily for 7 days. After that, it is removed and a new patch is applied.
“The availability of a once-weekly patch formulation of donepezil has the potential to substantially benefit patients, caregivers, and health care providers,” Pierre Tariot, MD, director of the Banner Alzheimer’s Institute, Phoenix, said in the release.
“It offers effective, well-tolerated, and stable dosing for 7 days for patients who cannot take daily oral donepezil reliably because of impaired memory. It can also offer benefits for those patients who have diminished ability to swallow or have GI side effects associated with ingestion of oral donepezil,” Dr. Tariot added.
The FDA approved Adlarity through the 505(b)(2) regulatory pathway, which allows the agency to refer to previous findings of safety and efficacy for an already-approved product, as well as to review findings from further studies of the product.
The company expects the donepezil transdermal patch to be available in early Fall 2022.
A version of this article first appeared on Medscape.com.
‘Bigorexia’: Why teenage boys are obsessed with bulking up
Why are teenage boys obsessed with bulking up?
While the effects of Instagram on girls’ body image has long been documented – an article in The Wall Street Journal that was published this fall reported that Facebook knew Instagram was toxic for teen girls – teenage boys are under just as much pressure.
For adolescent boys, the goal is often to get superhero-size buff – and this is leading to anxiety, stress, excessive selfies, and, often, obsessive staring in the mirror to assess their “pec” progress.
So-called “bigorexia” – or extreme gym time, excessive focus on protein diets, and intense muscle-building goals – has hit new and concerning levels, according to a recent New York Times report.
Whether it’s the pandemic or TikTok that’s to blame, teen boys are pushing hard to achieve six-pack abs, with one-third of them in the U.S. trying to bulk up, according to a study published in the Journal of Adolescent Health. What’s more, 22% reported they’re engaging in muscle-enhancing behavior, including excess exercise, taking supplements or steroids, or eating more to bulk up, according to a study published in the International Journal of Eating Disorders.
“The pandemic and social media have been a perfect storm for eating disorders and body image issues for all teens, but this has been under-recognized in boys,” says Jason Nagata, MD, a pediatrician who specializes in adolescent medicine at the University of California, San Francisco. “Both are directly connected to an increase in muscle dysmorphia.”
While “bigorexia” is a newer term coined by mental health professionals, the concept of muscular dysmorphia isn’t, says Jennifer Bahrman, PhD, a licensed psychologist with McGovern Medical School at UTHealth Houston. This may be why about a third of boys ages 11-18 reported that they aren’t enamored with their bodies, according to a small survey published in 2019 in the Californian Journal of Health Promotion.
“When we think of dysmorphia, we think of girls having it, since we see it more in females,” says Dr. Bahrman, who works extensively with adolescents and athletes. “The interesting thing about muscular dysmorphia is that it’s the only body dysmorphic disorder that’s almost exclusively present in males.”
Social media’s role
Unlike other things in boys’ lives, like movies, TV, or even the uber-buff GI Joe doll, social media has created opportunities for young men to put their bodies on display – and become an influencer or get followers because of it.
“An everyday teen can become a celebrity,” Dr. Nagata says. “Then, thanks to social media algorithms, if a teenage boy likes or interacts with a post that features a muscular guy or is all about fitness, they’ll start getting all sorts of related content. They’ll get bombarded with tons of ads for protein shakes, for example, as well as bodybuilding equipment, and that will further distort reality.”
Before-and-after photos are also known to be quite misleading.
“Some of the most popular Instagram posts among teens feature people who have experienced a massive body transformation,” Dr. Nagata says. “It’s usually someone who lost a lot of weight or someone who was scrawny and then got muscular. The most drastic changes tend to get the most likes and are perpetuated the most and shared the most often with friends.”
But as many are aware, photos posted to social media are selected to tell the best story – with the best filters, lighting, and angles possible, however exaggerated.
“A guy will post his worst picture out of a thousand for his before shot and then post the best photo out of a thousand,” Dr. Nagata says. “This, in itself, can really confuse a teenager, because the story of this person’s changed body looks so realistic.”
Worse, these images tend to be damaging to your teenager’s self-esteem.
“When you see images of people you’re aspiring to look like, it can be very upsetting,” Dr. Bahrman says. “After all, it’s easy to think, ‘I’m doing all of these pushups, and I don’t look like this.’ From there, it’s easy to begin internalizing that something is wrong with you.”
Red flags to watch out for
If you’ve noticed that your son is obsessed with his appearance, weight, food, or exercise, take note. Also, notice if he’s asking you to buy protein powder or is spending more time at the gym than with his friends.
“Pay attention if he is withdrawing from friends and family because of his concerns about his appearance,” Dr. Nagata says. “For example, we often hear that a teenager will no longer eat family meals or at a restaurant because the protein content isn’t high enough or the food is too fatty.”
If you’re concerned, always make sure to discuss this with your son’s pediatrician.
“Ultimately, you want to make sure you share your concerns before your teen son becomes even more body-image obsessed,” Dr. Nagata says.
A version of this article first appeared on WebMD.com.
Why are teenage boys obsessed with bulking up?
While the effects of Instagram on girls’ body image has long been documented – an article in The Wall Street Journal that was published this fall reported that Facebook knew Instagram was toxic for teen girls – teenage boys are under just as much pressure.
For adolescent boys, the goal is often to get superhero-size buff – and this is leading to anxiety, stress, excessive selfies, and, often, obsessive staring in the mirror to assess their “pec” progress.
So-called “bigorexia” – or extreme gym time, excessive focus on protein diets, and intense muscle-building goals – has hit new and concerning levels, according to a recent New York Times report.
Whether it’s the pandemic or TikTok that’s to blame, teen boys are pushing hard to achieve six-pack abs, with one-third of them in the U.S. trying to bulk up, according to a study published in the Journal of Adolescent Health. What’s more, 22% reported they’re engaging in muscle-enhancing behavior, including excess exercise, taking supplements or steroids, or eating more to bulk up, according to a study published in the International Journal of Eating Disorders.
“The pandemic and social media have been a perfect storm for eating disorders and body image issues for all teens, but this has been under-recognized in boys,” says Jason Nagata, MD, a pediatrician who specializes in adolescent medicine at the University of California, San Francisco. “Both are directly connected to an increase in muscle dysmorphia.”
While “bigorexia” is a newer term coined by mental health professionals, the concept of muscular dysmorphia isn’t, says Jennifer Bahrman, PhD, a licensed psychologist with McGovern Medical School at UTHealth Houston. This may be why about a third of boys ages 11-18 reported that they aren’t enamored with their bodies, according to a small survey published in 2019 in the Californian Journal of Health Promotion.
“When we think of dysmorphia, we think of girls having it, since we see it more in females,” says Dr. Bahrman, who works extensively with adolescents and athletes. “The interesting thing about muscular dysmorphia is that it’s the only body dysmorphic disorder that’s almost exclusively present in males.”
Social media’s role
Unlike other things in boys’ lives, like movies, TV, or even the uber-buff GI Joe doll, social media has created opportunities for young men to put their bodies on display – and become an influencer or get followers because of it.
“An everyday teen can become a celebrity,” Dr. Nagata says. “Then, thanks to social media algorithms, if a teenage boy likes or interacts with a post that features a muscular guy or is all about fitness, they’ll start getting all sorts of related content. They’ll get bombarded with tons of ads for protein shakes, for example, as well as bodybuilding equipment, and that will further distort reality.”
Before-and-after photos are also known to be quite misleading.
“Some of the most popular Instagram posts among teens feature people who have experienced a massive body transformation,” Dr. Nagata says. “It’s usually someone who lost a lot of weight or someone who was scrawny and then got muscular. The most drastic changes tend to get the most likes and are perpetuated the most and shared the most often with friends.”
But as many are aware, photos posted to social media are selected to tell the best story – with the best filters, lighting, and angles possible, however exaggerated.
“A guy will post his worst picture out of a thousand for his before shot and then post the best photo out of a thousand,” Dr. Nagata says. “This, in itself, can really confuse a teenager, because the story of this person’s changed body looks so realistic.”
Worse, these images tend to be damaging to your teenager’s self-esteem.
“When you see images of people you’re aspiring to look like, it can be very upsetting,” Dr. Bahrman says. “After all, it’s easy to think, ‘I’m doing all of these pushups, and I don’t look like this.’ From there, it’s easy to begin internalizing that something is wrong with you.”
Red flags to watch out for
If you’ve noticed that your son is obsessed with his appearance, weight, food, or exercise, take note. Also, notice if he’s asking you to buy protein powder or is spending more time at the gym than with his friends.
“Pay attention if he is withdrawing from friends and family because of his concerns about his appearance,” Dr. Nagata says. “For example, we often hear that a teenager will no longer eat family meals or at a restaurant because the protein content isn’t high enough or the food is too fatty.”
If you’re concerned, always make sure to discuss this with your son’s pediatrician.
“Ultimately, you want to make sure you share your concerns before your teen son becomes even more body-image obsessed,” Dr. Nagata says.
A version of this article first appeared on WebMD.com.
Why are teenage boys obsessed with bulking up?
While the effects of Instagram on girls’ body image has long been documented – an article in The Wall Street Journal that was published this fall reported that Facebook knew Instagram was toxic for teen girls – teenage boys are under just as much pressure.
For adolescent boys, the goal is often to get superhero-size buff – and this is leading to anxiety, stress, excessive selfies, and, often, obsessive staring in the mirror to assess their “pec” progress.
So-called “bigorexia” – or extreme gym time, excessive focus on protein diets, and intense muscle-building goals – has hit new and concerning levels, according to a recent New York Times report.
Whether it’s the pandemic or TikTok that’s to blame, teen boys are pushing hard to achieve six-pack abs, with one-third of them in the U.S. trying to bulk up, according to a study published in the Journal of Adolescent Health. What’s more, 22% reported they’re engaging in muscle-enhancing behavior, including excess exercise, taking supplements or steroids, or eating more to bulk up, according to a study published in the International Journal of Eating Disorders.
“The pandemic and social media have been a perfect storm for eating disorders and body image issues for all teens, but this has been under-recognized in boys,” says Jason Nagata, MD, a pediatrician who specializes in adolescent medicine at the University of California, San Francisco. “Both are directly connected to an increase in muscle dysmorphia.”
While “bigorexia” is a newer term coined by mental health professionals, the concept of muscular dysmorphia isn’t, says Jennifer Bahrman, PhD, a licensed psychologist with McGovern Medical School at UTHealth Houston. This may be why about a third of boys ages 11-18 reported that they aren’t enamored with their bodies, according to a small survey published in 2019 in the Californian Journal of Health Promotion.
“When we think of dysmorphia, we think of girls having it, since we see it more in females,” says Dr. Bahrman, who works extensively with adolescents and athletes. “The interesting thing about muscular dysmorphia is that it’s the only body dysmorphic disorder that’s almost exclusively present in males.”
Social media’s role
Unlike other things in boys’ lives, like movies, TV, or even the uber-buff GI Joe doll, social media has created opportunities for young men to put their bodies on display – and become an influencer or get followers because of it.
“An everyday teen can become a celebrity,” Dr. Nagata says. “Then, thanks to social media algorithms, if a teenage boy likes or interacts with a post that features a muscular guy or is all about fitness, they’ll start getting all sorts of related content. They’ll get bombarded with tons of ads for protein shakes, for example, as well as bodybuilding equipment, and that will further distort reality.”
Before-and-after photos are also known to be quite misleading.
“Some of the most popular Instagram posts among teens feature people who have experienced a massive body transformation,” Dr. Nagata says. “It’s usually someone who lost a lot of weight or someone who was scrawny and then got muscular. The most drastic changes tend to get the most likes and are perpetuated the most and shared the most often with friends.”
But as many are aware, photos posted to social media are selected to tell the best story – with the best filters, lighting, and angles possible, however exaggerated.
“A guy will post his worst picture out of a thousand for his before shot and then post the best photo out of a thousand,” Dr. Nagata says. “This, in itself, can really confuse a teenager, because the story of this person’s changed body looks so realistic.”
Worse, these images tend to be damaging to your teenager’s self-esteem.
“When you see images of people you’re aspiring to look like, it can be very upsetting,” Dr. Bahrman says. “After all, it’s easy to think, ‘I’m doing all of these pushups, and I don’t look like this.’ From there, it’s easy to begin internalizing that something is wrong with you.”
Red flags to watch out for
If you’ve noticed that your son is obsessed with his appearance, weight, food, or exercise, take note. Also, notice if he’s asking you to buy protein powder or is spending more time at the gym than with his friends.
“Pay attention if he is withdrawing from friends and family because of his concerns about his appearance,” Dr. Nagata says. “For example, we often hear that a teenager will no longer eat family meals or at a restaurant because the protein content isn’t high enough or the food is too fatty.”
If you’re concerned, always make sure to discuss this with your son’s pediatrician.
“Ultimately, you want to make sure you share your concerns before your teen son becomes even more body-image obsessed,” Dr. Nagata says.
A version of this article first appeared on WebMD.com.
Schizophrenia and HIV: missed opportunities for care
“People don’t think about schizophrenia when they think about HIV,” Christina Mangurian, MD, professor of clinical psychiatry and vice chair for diversity and health equity at the University of California, San Francisco (UCSF), told this news organization.

The problem is complicated. According to the Centers for Disease Control and Prevention and National Institutes of Health, roughly 6% of people with serious mental illness are living with HIV, a rate that is about 10 times higher than the general U.S. population (0.4%). However, findings from a study by Dr. Mangurian and her team, published online in the journal AIDS, demonstrated that half of Medicaid patients with schizophrenia and HIV admitted to inpatient units in New York State were not coded as such upon discharge.
These data raise the question: , lack of social support, and under-recognition by practitioners that a problem even exists?
Lost in the care continuum
Dr. Mangurian and her research team examined documentation of pre-existing HIV/AIDS diagnoses and absence of ICD-9-CM HIV/AIDS coding at psychiatric discharge among 14,602 adults (aged 18-64 years) admitted to hospital inpatient units in New York State between Jan. 1, 2012, and Dec. 31, 2013. HIV diagnoses were defined as recent (within 30 days of admission) or distant (within 30-366 days of admission), and first admission was used as the index in people with multiple hospitalizations.
People living with HIV comprised 5.1% (741) of the overall dataset; 34% were diagnosed with schizophrenia and 27.9% with bipolar disorders. Overall, 54.5% were male and 50.7% were non-Hispanic Black. Furthermore, 58.3% were discharged without HIV/AIDS ICD-9 coding, reinforcing the likelihood that they were lost in the care continuum.
Dr. Mangurian explained that this break in the chain of care upon discharge can have an important impact on efforts to break the cycle of HIV transmission.
“There’s data that people with serious mental illnesses like schizophrenia are less likely to have sex, but when they do they’re more likely to engage in risky sexual behaviors, including sex for money [and] unprotected sex with partners who use injection drugs or who have HIV,” she said.
Although the majority of patients – both with and without prior HIV diagnoses – were older, adjusted models demonstrated that people aged 18-24 years had more than twice the odds of having their HIV/AIDS undocumented at discharge, compared with older adults aged 55-64 years (adjusted odds ratio, 2.37; P = .038), as were those aged 25-34 years (aOR, 2.17; P = .003). Individuals with more distant HIV diagnoses had three times the odds for an undocumented HIV/AIDS discharge, compared with more recent diagnoses (aOR, 3.25; P < .001).
Additional factors contributing to the lack of ICD-9 discharge coding included shorter lengths of stay (0-3 days vs. 15-30 days; aOR, 0.03; P = .01) and fewer HIV claims for HIV/AIDS services before hospitalization (1-2 vs. 3-9; aOR, 0.34; P < .01). Hospitals serving medium or high levels of Medicaid patients were also less likely to document HIV/AIDS before discharge (medium aOR, 1.69, P = .01; high aOR, 1.71, P = .03).
The study is not without limitations. For example, the 10-year-old dataset might not entirely reflect more recent structural or systemic changes for improving HIV detection on inpatient psychiatric units. Moreover, there was no comparator group without psychiatric inpatient admission.
Still, “[if these patients] didn’t have a discharge diagnosis, then it’s possible that they were not managed for their HIV, or their HIV was not addressed while they were in the hospital,” Sarah Andrews, MD, assistant professor of psychiatry and behavioral sciences and AIDS psychiatrist at Johns Hopkins School of Medicine, Baltimore, explained.
Dr. Andrews, who was not involved in the study, noted that this omission is significant. “A psychiatric admission or medical admission in general is a great opportunity to further manage and treat comorbidities. When we have a patient who comes in with HIV and they haven’t been on an antiviral prior to admission, we try to get infectious disease to give us recommendations of what to start, what labs to draw, to help them re-establish care,” she said.
Severe mental health an HIV disparity
Despite the burden of HIV among patient populations with serious mental health issues and data suggesting that these populations are over-represented among new HIV infections, the study findings point to an important missed opportunity for meeting several key outcomes on the HIV/AIDS care continuum, especially linkage to and retention in care.
The challenge is multifactorial.
In an earlier publication appearing in April 2021 in The Lancet HIV, Dr. Mangurian and colleagues explore a concept known as the “purview paradox,” which refers to a practitioner’s belief about who should be responsible for offering patients a particular intervention.
Structural and systemic issues also abound, as psychiatry records are often kept separate from the rest of the medical system due to insurer billing issues. “The true integration of all psychiatric and medical care has to happen to make sure that all of our patients receive the care that they deserve,” explained Dr. Mangurian.
Dr. Andrews agrees. “HIV care, as well as psychiatry, case management, pharmacy ... putting them together really helps decrease the risk of falling through the cracks and being able to refer appropriately for mental health,” she said.
Aside from changing practitioner attitudes and awareness and changing systems to include the wrap-around care model, current guidelines also need to reflect the role that patients with HIV and psychiatric comorbidities play in HIV transmission. Dr. Andrews and Dr. Mangurian agree: Routine screening in psychiatric inpatient units might be a good start.
The study was independently supported. Dr. Mangurian has reported grant funding from Genentech Charitable Foundation. Dr. Andrews has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“People don’t think about schizophrenia when they think about HIV,” Christina Mangurian, MD, professor of clinical psychiatry and vice chair for diversity and health equity at the University of California, San Francisco (UCSF), told this news organization.
The problem is complicated. According to the Centers for Disease Control and Prevention and National Institutes of Health, roughly 6% of people with serious mental illness are living with HIV, a rate that is about 10 times higher than the general U.S. population (0.4%). However, findings from a study by Dr. Mangurian and her team, published online in the journal AIDS, demonstrated that half of Medicaid patients with schizophrenia and HIV admitted to inpatient units in New York State were not coded as such upon discharge.
These data raise the question: , lack of social support, and under-recognition by practitioners that a problem even exists?
Lost in the care continuum
Dr. Mangurian and her research team examined documentation of pre-existing HIV/AIDS diagnoses and absence of ICD-9-CM HIV/AIDS coding at psychiatric discharge among 14,602 adults (aged 18-64 years) admitted to hospital inpatient units in New York State between Jan. 1, 2012, and Dec. 31, 2013. HIV diagnoses were defined as recent (within 30 days of admission) or distant (within 30-366 days of admission), and first admission was used as the index in people with multiple hospitalizations.
People living with HIV comprised 5.1% (741) of the overall dataset; 34% were diagnosed with schizophrenia and 27.9% with bipolar disorders. Overall, 54.5% were male and 50.7% were non-Hispanic Black. Furthermore, 58.3% were discharged without HIV/AIDS ICD-9 coding, reinforcing the likelihood that they were lost in the care continuum.
Dr. Mangurian explained that this break in the chain of care upon discharge can have an important impact on efforts to break the cycle of HIV transmission.
“There’s data that people with serious mental illnesses like schizophrenia are less likely to have sex, but when they do they’re more likely to engage in risky sexual behaviors, including sex for money [and] unprotected sex with partners who use injection drugs or who have HIV,” she said.
Although the majority of patients – both with and without prior HIV diagnoses – were older, adjusted models demonstrated that people aged 18-24 years had more than twice the odds of having their HIV/AIDS undocumented at discharge, compared with older adults aged 55-64 years (adjusted odds ratio, 2.37; P = .038), as were those aged 25-34 years (aOR, 2.17; P = .003). Individuals with more distant HIV diagnoses had three times the odds for an undocumented HIV/AIDS discharge, compared with more recent diagnoses (aOR, 3.25; P < .001).
Additional factors contributing to the lack of ICD-9 discharge coding included shorter lengths of stay (0-3 days vs. 15-30 days; aOR, 0.03; P = .01) and fewer HIV claims for HIV/AIDS services before hospitalization (1-2 vs. 3-9; aOR, 0.34; P < .01). Hospitals serving medium or high levels of Medicaid patients were also less likely to document HIV/AIDS before discharge (medium aOR, 1.69, P = .01; high aOR, 1.71, P = .03).
The study is not without limitations. For example, the 10-year-old dataset might not entirely reflect more recent structural or systemic changes for improving HIV detection on inpatient psychiatric units. Moreover, there was no comparator group without psychiatric inpatient admission.
Still, “[if these patients] didn’t have a discharge diagnosis, then it’s possible that they were not managed for their HIV, or their HIV was not addressed while they were in the hospital,” Sarah Andrews, MD, assistant professor of psychiatry and behavioral sciences and AIDS psychiatrist at Johns Hopkins School of Medicine, Baltimore, explained.
Dr. Andrews, who was not involved in the study, noted that this omission is significant. “A psychiatric admission or medical admission in general is a great opportunity to further manage and treat comorbidities. When we have a patient who comes in with HIV and they haven’t been on an antiviral prior to admission, we try to get infectious disease to give us recommendations of what to start, what labs to draw, to help them re-establish care,” she said.
Severe mental health an HIV disparity
Despite the burden of HIV among patient populations with serious mental health issues and data suggesting that these populations are over-represented among new HIV infections, the study findings point to an important missed opportunity for meeting several key outcomes on the HIV/AIDS care continuum, especially linkage to and retention in care.
The challenge is multifactorial.
In an earlier publication appearing in April 2021 in The Lancet HIV, Dr. Mangurian and colleagues explore a concept known as the “purview paradox,” which refers to a practitioner’s belief about who should be responsible for offering patients a particular intervention.
Structural and systemic issues also abound, as psychiatry records are often kept separate from the rest of the medical system due to insurer billing issues. “The true integration of all psychiatric and medical care has to happen to make sure that all of our patients receive the care that they deserve,” explained Dr. Mangurian.
Dr. Andrews agrees. “HIV care, as well as psychiatry, case management, pharmacy ... putting them together really helps decrease the risk of falling through the cracks and being able to refer appropriately for mental health,” she said.
Aside from changing practitioner attitudes and awareness and changing systems to include the wrap-around care model, current guidelines also need to reflect the role that patients with HIV and psychiatric comorbidities play in HIV transmission. Dr. Andrews and Dr. Mangurian agree: Routine screening in psychiatric inpatient units might be a good start.
The study was independently supported. Dr. Mangurian has reported grant funding from Genentech Charitable Foundation. Dr. Andrews has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“People don’t think about schizophrenia when they think about HIV,” Christina Mangurian, MD, professor of clinical psychiatry and vice chair for diversity and health equity at the University of California, San Francisco (UCSF), told this news organization.
The problem is complicated. According to the Centers for Disease Control and Prevention and National Institutes of Health, roughly 6% of people with serious mental illness are living with HIV, a rate that is about 10 times higher than the general U.S. population (0.4%). However, findings from a study by Dr. Mangurian and her team, published online in the journal AIDS, demonstrated that half of Medicaid patients with schizophrenia and HIV admitted to inpatient units in New York State were not coded as such upon discharge.
These data raise the question: , lack of social support, and under-recognition by practitioners that a problem even exists?
Lost in the care continuum
Dr. Mangurian and her research team examined documentation of pre-existing HIV/AIDS diagnoses and absence of ICD-9-CM HIV/AIDS coding at psychiatric discharge among 14,602 adults (aged 18-64 years) admitted to hospital inpatient units in New York State between Jan. 1, 2012, and Dec. 31, 2013. HIV diagnoses were defined as recent (within 30 days of admission) or distant (within 30-366 days of admission), and first admission was used as the index in people with multiple hospitalizations.
People living with HIV comprised 5.1% (741) of the overall dataset; 34% were diagnosed with schizophrenia and 27.9% with bipolar disorders. Overall, 54.5% were male and 50.7% were non-Hispanic Black. Furthermore, 58.3% were discharged without HIV/AIDS ICD-9 coding, reinforcing the likelihood that they were lost in the care continuum.
Dr. Mangurian explained that this break in the chain of care upon discharge can have an important impact on efforts to break the cycle of HIV transmission.
“There’s data that people with serious mental illnesses like schizophrenia are less likely to have sex, but when they do they’re more likely to engage in risky sexual behaviors, including sex for money [and] unprotected sex with partners who use injection drugs or who have HIV,” she said.
Although the majority of patients – both with and without prior HIV diagnoses – were older, adjusted models demonstrated that people aged 18-24 years had more than twice the odds of having their HIV/AIDS undocumented at discharge, compared with older adults aged 55-64 years (adjusted odds ratio, 2.37; P = .038), as were those aged 25-34 years (aOR, 2.17; P = .003). Individuals with more distant HIV diagnoses had three times the odds for an undocumented HIV/AIDS discharge, compared with more recent diagnoses (aOR, 3.25; P < .001).
Additional factors contributing to the lack of ICD-9 discharge coding included shorter lengths of stay (0-3 days vs. 15-30 days; aOR, 0.03; P = .01) and fewer HIV claims for HIV/AIDS services before hospitalization (1-2 vs. 3-9; aOR, 0.34; P < .01). Hospitals serving medium or high levels of Medicaid patients were also less likely to document HIV/AIDS before discharge (medium aOR, 1.69, P = .01; high aOR, 1.71, P = .03).
The study is not without limitations. For example, the 10-year-old dataset might not entirely reflect more recent structural or systemic changes for improving HIV detection on inpatient psychiatric units. Moreover, there was no comparator group without psychiatric inpatient admission.
Still, “[if these patients] didn’t have a discharge diagnosis, then it’s possible that they were not managed for their HIV, or their HIV was not addressed while they were in the hospital,” Sarah Andrews, MD, assistant professor of psychiatry and behavioral sciences and AIDS psychiatrist at Johns Hopkins School of Medicine, Baltimore, explained.
Dr. Andrews, who was not involved in the study, noted that this omission is significant. “A psychiatric admission or medical admission in general is a great opportunity to further manage and treat comorbidities. When we have a patient who comes in with HIV and they haven’t been on an antiviral prior to admission, we try to get infectious disease to give us recommendations of what to start, what labs to draw, to help them re-establish care,” she said.
Severe mental health an HIV disparity
Despite the burden of HIV among patient populations with serious mental health issues and data suggesting that these populations are over-represented among new HIV infections, the study findings point to an important missed opportunity for meeting several key outcomes on the HIV/AIDS care continuum, especially linkage to and retention in care.
The challenge is multifactorial.
In an earlier publication appearing in April 2021 in The Lancet HIV, Dr. Mangurian and colleagues explore a concept known as the “purview paradox,” which refers to a practitioner’s belief about who should be responsible for offering patients a particular intervention.
Structural and systemic issues also abound, as psychiatry records are often kept separate from the rest of the medical system due to insurer billing issues. “The true integration of all psychiatric and medical care has to happen to make sure that all of our patients receive the care that they deserve,” explained Dr. Mangurian.
Dr. Andrews agrees. “HIV care, as well as psychiatry, case management, pharmacy ... putting them together really helps decrease the risk of falling through the cracks and being able to refer appropriately for mental health,” she said.
Aside from changing practitioner attitudes and awareness and changing systems to include the wrap-around care model, current guidelines also need to reflect the role that patients with HIV and psychiatric comorbidities play in HIV transmission. Dr. Andrews and Dr. Mangurian agree: Routine screening in psychiatric inpatient units might be a good start.
The study was independently supported. Dr. Mangurian has reported grant funding from Genentech Charitable Foundation. Dr. Andrews has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Why is there an increased risk of cancer in depressed patients?
LAS VEGAS – Is the relationship between major depressive disorder and the development of cancer, cardiovascular disease, and other medical conditions a coincidence, or is there more at play?
According to Charles B. Nemeroff, MD, PhD, a host of circumstances potentially underlies this association, including treatment of the medical disorder itself.

“The best example of that is probably the use of interferon-alpha for the treatment of malignant melanoma,” Dr. Nemeroff, professor and chair of the department of psychiatry and behavioral sciences at the University of Texas at Austin, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “Many patients treated with interferon-alpha ended up with very severe depression, including several documented suicides. Another possibility of the relationship between depression and medical disorders is that treating a patient for depression could result in a medical disorder. The best example of this is the use of 20 mg of olanzapine to augment the effects of an antidepressant, resulting in a 50-pound weight gain and the development of type 2 diabetes and metabolic syndrome. Both of those scenarios are well understood.”
Then there’s the behavioral aspects of the relationship, he continued, in which patients adopt the mindset that “I’m depressed. I don’t want to exercise. I’m a couch potato. I have been gaining a lot of weight. It’s bad for my heart.”
Converging biology is another possibility. “Is it possible that the biology of depression is linked to the biology of other disorders?” asked Dr. Nemeroff, who directs the university’s Institute for Early Life Adversity Research. “We can talk about this in relation to thyroid disease, a well known cause of depression, but we can also talk about the relationship to other disorders. There’s amazing epidemiologic evidence that patients with PTSD are much more likely to develop Alzheimer’s disease than patients without PTSD.”
Psychosocial issues also play a role. He recalled seeing patient in a clinic for the underserved who had underlying severe ulcerative colitis and anemia and couldn’t afford medical treatment. “The patient had a low hemoglobin, so it was impossible to distinguish between that and whether they had a primary depressive disorder or not,” he said.
In a study that explored the relationship between major depression and cancer, Dr. Nemeroff and colleagues found that the prevalence was highest in those with pancreatic cancer (50%), followed by oropharyngeal (40%), colon (13-25%), breast (18-25%), and gynecologic (23%), and Hodgkin’s lymphoma (17%) (Arch Gen Psychiatry 1995;52[2]:89-99). “Not all cancers have the same rate of depression,” he said. “One of the central questions is, not so much is the cancer patient depressed, but is depression a risk factor for developing cancer? The answer is a resounding yes. But what we don’t know is if you treat the depression aggressively, can you reduce that risk of either developing cancer or the progression of cancer?”
Dr. Nemeroff spotlighted several studies largely from the oncology literature, including a prospective survival analysis of 578 women with early-stage breast cancer (Lancet 1999;354:1331-6). After 5 years, 395 were alive and without relapse, 50 were alive with relapse, and 133 had died. The researchers found a significantly increased risk of death from all causes by 5 years in women with a high depression score (HR 3.59). There was a significantly increased risk of relapse or death at 5 years in women with high scores on helplessness and hopelessness measures.
In an analysis of the association between breast cancer and traumatic events, women who had severe stress or a traumatic event had lower rates of disease-free intervals (J Psychosomatic Res 2007;63:233-9). Another study by the same investigators found that a decrease in depression symptoms is associated with longer survival in patients with metastatic breast cancer (J Clin Oncol 2010;29:413-20). The median survival was 53.6 months for women with decreasing depression scores over 1 year and 25.1 months for women with increasing depression scores.
A more recent study of cervical cancer patients found that those exposed to psychological stress had an increased risk of cancer-specific mortality (HR 1.33) (Cancer Res 2019;79:3965-72). The association was mainly driven by distress experienced within 1 year before or after diagnosis (HR 1.30) but not afterward (HR 1.12). In addition, data from the large longitudinal Nurses’ Health Study II found that women with high PTSD symptoms had a twofold greater risk of ovarian cancer compared with women who had no trauma exposure (Cancer Res 2019;79:5113-20).
Authors of a separate study analyzed data from the Women’s Health Initiative to examine if depression precedes the development of a cancer diagnosis. They found that depression 3 years before a diagnosis of breast cancer was associated with all-cause mortality (HR 1.35) (Cancer 2017;123[16]:3107-15). Meanwhile, among women with late-stage breast cancer, newly developed depression at year 3 was significantly associated with all-cause mortality (HR 2.0) and breast cancer-specific mortality (HR 2.42). “That’s a pretty amazing finding,” Dr. Nemeroff said. “We have to think about depression as a systemic illness. What is depression doing that’s creating a fertile environment for cancer or worsening of cancer?”
He then discussed the risk of suicide in patients who are newly diagnosed with cancer. “No one ever talks about this, and I can’t get anybody to support research in this area,” he said. In one of the first studies on the topic, researchers conducted a case-control study of Medicare patients and determined risk of suicide among those with cancer was 2.3-fold higher compared with controls, even after adjustment for psychiatric illness and the risk of dying within a year (J Clin Oncol 2008;26[29]:4720-4). More recently, authors of a large population-based study in England found that the overall standardized mortality ratio for suicide was 1.20 (JAMA Psychiatry 2019;76[1]51-60). The risk was highest among patients with mesothelioma, with a 4.51-fold risk, followed by pancreatic (3.89-fold), esophageal (2.65-fold), lung (2.57-fold), and stomach cancer (2.20-fold). “They reported that the first 6 months after the diagnosis is associated with an increased risk of suicide – unrelated to prognosis,” Dr. Nemeroff said.
A separate analysis of SEER data from 1973-2014 and comprising more than 8.6 million cancer patients found that newly diagnosed cancer patients are 4.4 times more likely to die from suicide than patients in the same age group without cancer (Nat Commun 2019;10[1]:207). The highest risk was in lung cancer, followed by head and neck, testes, bladder, and Hodgkin’s lymphoma.
According to Dr. Nemeroff, For example, he said, if the depressed environment is associated with a marked increase in tumor necrosis factor, interleukin 6, and other inflammatory markers, “that probably contributes to the body’s ability to fight disease. Ironically, depression is associated with an increase in inflammation but a decreased in T cell function. Remember, there are two fundamental types of immunity: the antibody response and the cellular response. What’s odd about depression is that there’s an increase in inflammatory markers but a decrease in the ability of T cells to function in terms of cellular immunity.”
Dr. Nemeroff disclosed that he has served as a consultant and/or scientific adviser for numerous pharmaceutical companies. He has received research and grant support from the National Institutes of Health.
LAS VEGAS – Is the relationship between major depressive disorder and the development of cancer, cardiovascular disease, and other medical conditions a coincidence, or is there more at play?
According to Charles B. Nemeroff, MD, PhD, a host of circumstances potentially underlies this association, including treatment of the medical disorder itself.
“The best example of that is probably the use of interferon-alpha for the treatment of malignant melanoma,” Dr. Nemeroff, professor and chair of the department of psychiatry and behavioral sciences at the University of Texas at Austin, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “Many patients treated with interferon-alpha ended up with very severe depression, including several documented suicides. Another possibility of the relationship between depression and medical disorders is that treating a patient for depression could result in a medical disorder. The best example of this is the use of 20 mg of olanzapine to augment the effects of an antidepressant, resulting in a 50-pound weight gain and the development of type 2 diabetes and metabolic syndrome. Both of those scenarios are well understood.”
Then there’s the behavioral aspects of the relationship, he continued, in which patients adopt the mindset that “I’m depressed. I don’t want to exercise. I’m a couch potato. I have been gaining a lot of weight. It’s bad for my heart.”
Converging biology is another possibility. “Is it possible that the biology of depression is linked to the biology of other disorders?” asked Dr. Nemeroff, who directs the university’s Institute for Early Life Adversity Research. “We can talk about this in relation to thyroid disease, a well known cause of depression, but we can also talk about the relationship to other disorders. There’s amazing epidemiologic evidence that patients with PTSD are much more likely to develop Alzheimer’s disease than patients without PTSD.”
Psychosocial issues also play a role. He recalled seeing patient in a clinic for the underserved who had underlying severe ulcerative colitis and anemia and couldn’t afford medical treatment. “The patient had a low hemoglobin, so it was impossible to distinguish between that and whether they had a primary depressive disorder or not,” he said.
In a study that explored the relationship between major depression and cancer, Dr. Nemeroff and colleagues found that the prevalence was highest in those with pancreatic cancer (50%), followed by oropharyngeal (40%), colon (13-25%), breast (18-25%), and gynecologic (23%), and Hodgkin’s lymphoma (17%) (Arch Gen Psychiatry 1995;52[2]:89-99). “Not all cancers have the same rate of depression,” he said. “One of the central questions is, not so much is the cancer patient depressed, but is depression a risk factor for developing cancer? The answer is a resounding yes. But what we don’t know is if you treat the depression aggressively, can you reduce that risk of either developing cancer or the progression of cancer?”
Dr. Nemeroff spotlighted several studies largely from the oncology literature, including a prospective survival analysis of 578 women with early-stage breast cancer (Lancet 1999;354:1331-6). After 5 years, 395 were alive and without relapse, 50 were alive with relapse, and 133 had died. The researchers found a significantly increased risk of death from all causes by 5 years in women with a high depression score (HR 3.59). There was a significantly increased risk of relapse or death at 5 years in women with high scores on helplessness and hopelessness measures.
In an analysis of the association between breast cancer and traumatic events, women who had severe stress or a traumatic event had lower rates of disease-free intervals (J Psychosomatic Res 2007;63:233-9). Another study by the same investigators found that a decrease in depression symptoms is associated with longer survival in patients with metastatic breast cancer (J Clin Oncol 2010;29:413-20). The median survival was 53.6 months for women with decreasing depression scores over 1 year and 25.1 months for women with increasing depression scores.
A more recent study of cervical cancer patients found that those exposed to psychological stress had an increased risk of cancer-specific mortality (HR 1.33) (Cancer Res 2019;79:3965-72). The association was mainly driven by distress experienced within 1 year before or after diagnosis (HR 1.30) but not afterward (HR 1.12). In addition, data from the large longitudinal Nurses’ Health Study II found that women with high PTSD symptoms had a twofold greater risk of ovarian cancer compared with women who had no trauma exposure (Cancer Res 2019;79:5113-20).
Authors of a separate study analyzed data from the Women’s Health Initiative to examine if depression precedes the development of a cancer diagnosis. They found that depression 3 years before a diagnosis of breast cancer was associated with all-cause mortality (HR 1.35) (Cancer 2017;123[16]:3107-15). Meanwhile, among women with late-stage breast cancer, newly developed depression at year 3 was significantly associated with all-cause mortality (HR 2.0) and breast cancer-specific mortality (HR 2.42). “That’s a pretty amazing finding,” Dr. Nemeroff said. “We have to think about depression as a systemic illness. What is depression doing that’s creating a fertile environment for cancer or worsening of cancer?”
He then discussed the risk of suicide in patients who are newly diagnosed with cancer. “No one ever talks about this, and I can’t get anybody to support research in this area,” he said. In one of the first studies on the topic, researchers conducted a case-control study of Medicare patients and determined risk of suicide among those with cancer was 2.3-fold higher compared with controls, even after adjustment for psychiatric illness and the risk of dying within a year (J Clin Oncol 2008;26[29]:4720-4). More recently, authors of a large population-based study in England found that the overall standardized mortality ratio for suicide was 1.20 (JAMA Psychiatry 2019;76[1]51-60). The risk was highest among patients with mesothelioma, with a 4.51-fold risk, followed by pancreatic (3.89-fold), esophageal (2.65-fold), lung (2.57-fold), and stomach cancer (2.20-fold). “They reported that the first 6 months after the diagnosis is associated with an increased risk of suicide – unrelated to prognosis,” Dr. Nemeroff said.
A separate analysis of SEER data from 1973-2014 and comprising more than 8.6 million cancer patients found that newly diagnosed cancer patients are 4.4 times more likely to die from suicide than patients in the same age group without cancer (Nat Commun 2019;10[1]:207). The highest risk was in lung cancer, followed by head and neck, testes, bladder, and Hodgkin’s lymphoma.
According to Dr. Nemeroff, For example, he said, if the depressed environment is associated with a marked increase in tumor necrosis factor, interleukin 6, and other inflammatory markers, “that probably contributes to the body’s ability to fight disease. Ironically, depression is associated with an increase in inflammation but a decreased in T cell function. Remember, there are two fundamental types of immunity: the antibody response and the cellular response. What’s odd about depression is that there’s an increase in inflammatory markers but a decrease in the ability of T cells to function in terms of cellular immunity.”
Dr. Nemeroff disclosed that he has served as a consultant and/or scientific adviser for numerous pharmaceutical companies. He has received research and grant support from the National Institutes of Health.
LAS VEGAS – Is the relationship between major depressive disorder and the development of cancer, cardiovascular disease, and other medical conditions a coincidence, or is there more at play?
According to Charles B. Nemeroff, MD, PhD, a host of circumstances potentially underlies this association, including treatment of the medical disorder itself.
“The best example of that is probably the use of interferon-alpha for the treatment of malignant melanoma,” Dr. Nemeroff, professor and chair of the department of psychiatry and behavioral sciences at the University of Texas at Austin, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “Many patients treated with interferon-alpha ended up with very severe depression, including several documented suicides. Another possibility of the relationship between depression and medical disorders is that treating a patient for depression could result in a medical disorder. The best example of this is the use of 20 mg of olanzapine to augment the effects of an antidepressant, resulting in a 50-pound weight gain and the development of type 2 diabetes and metabolic syndrome. Both of those scenarios are well understood.”
Then there’s the behavioral aspects of the relationship, he continued, in which patients adopt the mindset that “I’m depressed. I don’t want to exercise. I’m a couch potato. I have been gaining a lot of weight. It’s bad for my heart.”
Converging biology is another possibility. “Is it possible that the biology of depression is linked to the biology of other disorders?” asked Dr. Nemeroff, who directs the university’s Institute for Early Life Adversity Research. “We can talk about this in relation to thyroid disease, a well known cause of depression, but we can also talk about the relationship to other disorders. There’s amazing epidemiologic evidence that patients with PTSD are much more likely to develop Alzheimer’s disease than patients without PTSD.”
Psychosocial issues also play a role. He recalled seeing patient in a clinic for the underserved who had underlying severe ulcerative colitis and anemia and couldn’t afford medical treatment. “The patient had a low hemoglobin, so it was impossible to distinguish between that and whether they had a primary depressive disorder or not,” he said.
In a study that explored the relationship between major depression and cancer, Dr. Nemeroff and colleagues found that the prevalence was highest in those with pancreatic cancer (50%), followed by oropharyngeal (40%), colon (13-25%), breast (18-25%), and gynecologic (23%), and Hodgkin’s lymphoma (17%) (Arch Gen Psychiatry 1995;52[2]:89-99). “Not all cancers have the same rate of depression,” he said. “One of the central questions is, not so much is the cancer patient depressed, but is depression a risk factor for developing cancer? The answer is a resounding yes. But what we don’t know is if you treat the depression aggressively, can you reduce that risk of either developing cancer or the progression of cancer?”
Dr. Nemeroff spotlighted several studies largely from the oncology literature, including a prospective survival analysis of 578 women with early-stage breast cancer (Lancet 1999;354:1331-6). After 5 years, 395 were alive and without relapse, 50 were alive with relapse, and 133 had died. The researchers found a significantly increased risk of death from all causes by 5 years in women with a high depression score (HR 3.59). There was a significantly increased risk of relapse or death at 5 years in women with high scores on helplessness and hopelessness measures.
In an analysis of the association between breast cancer and traumatic events, women who had severe stress or a traumatic event had lower rates of disease-free intervals (J Psychosomatic Res 2007;63:233-9). Another study by the same investigators found that a decrease in depression symptoms is associated with longer survival in patients with metastatic breast cancer (J Clin Oncol 2010;29:413-20). The median survival was 53.6 months for women with decreasing depression scores over 1 year and 25.1 months for women with increasing depression scores.
A more recent study of cervical cancer patients found that those exposed to psychological stress had an increased risk of cancer-specific mortality (HR 1.33) (Cancer Res 2019;79:3965-72). The association was mainly driven by distress experienced within 1 year before or after diagnosis (HR 1.30) but not afterward (HR 1.12). In addition, data from the large longitudinal Nurses’ Health Study II found that women with high PTSD symptoms had a twofold greater risk of ovarian cancer compared with women who had no trauma exposure (Cancer Res 2019;79:5113-20).
Authors of a separate study analyzed data from the Women’s Health Initiative to examine if depression precedes the development of a cancer diagnosis. They found that depression 3 years before a diagnosis of breast cancer was associated with all-cause mortality (HR 1.35) (Cancer 2017;123[16]:3107-15). Meanwhile, among women with late-stage breast cancer, newly developed depression at year 3 was significantly associated with all-cause mortality (HR 2.0) and breast cancer-specific mortality (HR 2.42). “That’s a pretty amazing finding,” Dr. Nemeroff said. “We have to think about depression as a systemic illness. What is depression doing that’s creating a fertile environment for cancer or worsening of cancer?”
He then discussed the risk of suicide in patients who are newly diagnosed with cancer. “No one ever talks about this, and I can’t get anybody to support research in this area,” he said. In one of the first studies on the topic, researchers conducted a case-control study of Medicare patients and determined risk of suicide among those with cancer was 2.3-fold higher compared with controls, even after adjustment for psychiatric illness and the risk of dying within a year (J Clin Oncol 2008;26[29]:4720-4). More recently, authors of a large population-based study in England found that the overall standardized mortality ratio for suicide was 1.20 (JAMA Psychiatry 2019;76[1]51-60). The risk was highest among patients with mesothelioma, with a 4.51-fold risk, followed by pancreatic (3.89-fold), esophageal (2.65-fold), lung (2.57-fold), and stomach cancer (2.20-fold). “They reported that the first 6 months after the diagnosis is associated with an increased risk of suicide – unrelated to prognosis,” Dr. Nemeroff said.
A separate analysis of SEER data from 1973-2014 and comprising more than 8.6 million cancer patients found that newly diagnosed cancer patients are 4.4 times more likely to die from suicide than patients in the same age group without cancer (Nat Commun 2019;10[1]:207). The highest risk was in lung cancer, followed by head and neck, testes, bladder, and Hodgkin’s lymphoma.
According to Dr. Nemeroff, For example, he said, if the depressed environment is associated with a marked increase in tumor necrosis factor, interleukin 6, and other inflammatory markers, “that probably contributes to the body’s ability to fight disease. Ironically, depression is associated with an increase in inflammation but a decreased in T cell function. Remember, there are two fundamental types of immunity: the antibody response and the cellular response. What’s odd about depression is that there’s an increase in inflammatory markers but a decrease in the ability of T cells to function in terms of cellular immunity.”
Dr. Nemeroff disclosed that he has served as a consultant and/or scientific adviser for numerous pharmaceutical companies. He has received research and grant support from the National Institutes of Health.
FROM NPA 2022
Cat ownership in childhood linked ‘conditionally’ to psychosis in adult males
Owning an outdoor cat as a child is associated with an increased risk of psychotic experiences in adulthood – but only in males, new research suggests.
Investigators found

The suspected culprit is not the cat itself but rather exposure to Toxoplasma gondii, a common parasite carried by rodents and sometimes found in cat feces. The study adds to a growing evidence showing exposure to T. gondii may be a risk factor for schizophrenia and other psychotic disorders.
“These are small pieces of evidence but it’s interesting to consider that there might be combinations of risk factors at play,” lead author Vincent Paquin, MD, psychiatry resident at McGill University, Montreal, said in an interview.
“And even if the magnitude of the risk is small at the individual level,” he added, “cats and Toxoplasma gondii are so present in our society that if we add up all these small potential effects then it becomes a potential public health question.”
The study was published online Jan. 30, 2022, in the Journal of Psychiatric Research.
Inconsistent evidence
T. gondii infects about 30% of the human population and is usually transmitted by cats. Most infections are asymptomatic, but T. gondii can cause toxoplasmosis in humans, which has been linked to increased risk of schizophrenia, suicide attempts, and more recently, mild cognitive impairment.
Although some studies show an association between cat ownership and increased risk of mental illness, the research findings have been inconsistent.
“The evidence has been mixed about the association between cat ownership and psychosis expression, so our approach was to consider whether specific factors or combinations of factors could explain this mixed evidence,” Dr. Paquin said.
For the study, 2206 individuals aged 18-40 years completed the Community Assessment of Psychic Experiences (CAPE-42) and a questionnaire to gather information about cat ownership at any time between birth and age 13 and if the cats lived exclusively indoors (nonhunting) or if they were allowed outside (rodent hunting).
Participants were also asked about the number of residential moves between birth and age 15, date and place of birth, lifetime history of head trauma, and tobacco smoking history.
Rodent-hunting cat ownership was associated with higher risk of psychosis in male participants, compared with owning no cat or a nonhunting cat. When the investigators added head trauma and residential moves to rodent-hunting cat ownership, psychosis risk was elevated in both men and women.
Independent of cat ownership, younger age, moving more than three times as a child, a history of head trauma, and being a smoker were all associated with higher psychosis risk.

The study wasn’t designed to explore potential biological mechanisms to explain the sex differences in psychosis risk seen among rodent-hunting cat owners, but “one possible explanation based on the animal model literature is that the neurobiological effects of parasitic exposure may be greater with male sex,” senior author Suzanne King, PhD, professor of psychiatry at McGill, said in an interview.
The new study is part of a larger, long-term project called EnviroGen, led by Dr. King, examining the environmental and genetic risk factors for schizophrenia.
Need for replication
Commenting on the findings, E. Fuller Torrey, MD, who was among the first researchers to identify a link between cat ownership, T. gondii infection, and schizophrenia, said the study is “an interesting addition to the studies of cat ownership in childhood as a risk factor for psychosis.”
Of the approximately 10 published studies on the topic, about half suggest a link between cat ownership and psychosis later in life, said Dr. Torrey, associate director for research at the Stanley Medical Research Institute in Rockville, Md.
“The Canadian study is interesting in that it is the first study that separates exposure to permanently indoor cats from cats that are allowed to go outdoors, and the results were positive only for outdoor cats,” Dr. Torrey said.
The study has limitations, Dr. Torrey added, including its retrospective design and the use of a self-report questionnaire to assess psychotic experiences in adulthood.
Also commenting on findings, James Kirkbride, PhD, professor of psychiatric and social epidemiology, University College London, noted the same limitations.
Dr. Kirkbride is the lead author of a 2017 study that showed no link between cat ownership and serious mental illness that included nearly 5,000 people born in 1991 or 1992 and followed until age 18. In this study, there was no link between psychosis and cat ownership during pregnancy or at ages 4 or 10 years.
“Researchers have long been fascinated with the idea that cat ownership may affect mental health. This paper may have them chasing their own tail,” Dr. Kirkbride said.
“Evidence of any association is limited to certain subgroups without a strong theoretical basis for why this may be the case,” he added. “The retrospective and cross-sectional nature of the survey also raise the possibility that the results are impacted by differential recall bias, as well as the broader issues of chance and unobserved confounding.”
Dr. King noted that recall bias is a limitation the researchers highlighted in their study, but “considering the exposures are relatively objective and factual, we do not believe the potential for recall bias is substantial.”
“Nonetheless, we strongly believe that replication of our results in prospective, population-representative cohorts will be crucial to making firmer conclusions,” he added.
The study was funded by grants from the Quebec Health Research Fund. The study authors and Dr. Kirkbride disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Owning an outdoor cat as a child is associated with an increased risk of psychotic experiences in adulthood – but only in males, new research suggests.
Investigators found
The suspected culprit is not the cat itself but rather exposure to Toxoplasma gondii, a common parasite carried by rodents and sometimes found in cat feces. The study adds to a growing evidence showing exposure to T. gondii may be a risk factor for schizophrenia and other psychotic disorders.
“These are small pieces of evidence but it’s interesting to consider that there might be combinations of risk factors at play,” lead author Vincent Paquin, MD, psychiatry resident at McGill University, Montreal, said in an interview.
“And even if the magnitude of the risk is small at the individual level,” he added, “cats and Toxoplasma gondii are so present in our society that if we add up all these small potential effects then it becomes a potential public health question.”
The study was published online Jan. 30, 2022, in the Journal of Psychiatric Research.
Inconsistent evidence
T. gondii infects about 30% of the human population and is usually transmitted by cats. Most infections are asymptomatic, but T. gondii can cause toxoplasmosis in humans, which has been linked to increased risk of schizophrenia, suicide attempts, and more recently, mild cognitive impairment.
Although some studies show an association between cat ownership and increased risk of mental illness, the research findings have been inconsistent.
“The evidence has been mixed about the association between cat ownership and psychosis expression, so our approach was to consider whether specific factors or combinations of factors could explain this mixed evidence,” Dr. Paquin said.
For the study, 2206 individuals aged 18-40 years completed the Community Assessment of Psychic Experiences (CAPE-42) and a questionnaire to gather information about cat ownership at any time between birth and age 13 and if the cats lived exclusively indoors (nonhunting) or if they were allowed outside (rodent hunting).
Participants were also asked about the number of residential moves between birth and age 15, date and place of birth, lifetime history of head trauma, and tobacco smoking history.
Rodent-hunting cat ownership was associated with higher risk of psychosis in male participants, compared with owning no cat or a nonhunting cat. When the investigators added head trauma and residential moves to rodent-hunting cat ownership, psychosis risk was elevated in both men and women.
Independent of cat ownership, younger age, moving more than three times as a child, a history of head trauma, and being a smoker were all associated with higher psychosis risk.
The study wasn’t designed to explore potential biological mechanisms to explain the sex differences in psychosis risk seen among rodent-hunting cat owners, but “one possible explanation based on the animal model literature is that the neurobiological effects of parasitic exposure may be greater with male sex,” senior author Suzanne King, PhD, professor of psychiatry at McGill, said in an interview.
The new study is part of a larger, long-term project called EnviroGen, led by Dr. King, examining the environmental and genetic risk factors for schizophrenia.
Need for replication
Commenting on the findings, E. Fuller Torrey, MD, who was among the first researchers to identify a link between cat ownership, T. gondii infection, and schizophrenia, said the study is “an interesting addition to the studies of cat ownership in childhood as a risk factor for psychosis.”
Of the approximately 10 published studies on the topic, about half suggest a link between cat ownership and psychosis later in life, said Dr. Torrey, associate director for research at the Stanley Medical Research Institute in Rockville, Md.
“The Canadian study is interesting in that it is the first study that separates exposure to permanently indoor cats from cats that are allowed to go outdoors, and the results were positive only for outdoor cats,” Dr. Torrey said.
The study has limitations, Dr. Torrey added, including its retrospective design and the use of a self-report questionnaire to assess psychotic experiences in adulthood.
Also commenting on findings, James Kirkbride, PhD, professor of psychiatric and social epidemiology, University College London, noted the same limitations.
Dr. Kirkbride is the lead author of a 2017 study that showed no link between cat ownership and serious mental illness that included nearly 5,000 people born in 1991 or 1992 and followed until age 18. In this study, there was no link between psychosis and cat ownership during pregnancy or at ages 4 or 10 years.
“Researchers have long been fascinated with the idea that cat ownership may affect mental health. This paper may have them chasing their own tail,” Dr. Kirkbride said.
“Evidence of any association is limited to certain subgroups without a strong theoretical basis for why this may be the case,” he added. “The retrospective and cross-sectional nature of the survey also raise the possibility that the results are impacted by differential recall bias, as well as the broader issues of chance and unobserved confounding.”
Dr. King noted that recall bias is a limitation the researchers highlighted in their study, but “considering the exposures are relatively objective and factual, we do not believe the potential for recall bias is substantial.”
“Nonetheless, we strongly believe that replication of our results in prospective, population-representative cohorts will be crucial to making firmer conclusions,” he added.
The study was funded by grants from the Quebec Health Research Fund. The study authors and Dr. Kirkbride disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Owning an outdoor cat as a child is associated with an increased risk of psychotic experiences in adulthood – but only in males, new research suggests.
Investigators found
The suspected culprit is not the cat itself but rather exposure to Toxoplasma gondii, a common parasite carried by rodents and sometimes found in cat feces. The study adds to a growing evidence showing exposure to T. gondii may be a risk factor for schizophrenia and other psychotic disorders.
“These are small pieces of evidence but it’s interesting to consider that there might be combinations of risk factors at play,” lead author Vincent Paquin, MD, psychiatry resident at McGill University, Montreal, said in an interview.
“And even if the magnitude of the risk is small at the individual level,” he added, “cats and Toxoplasma gondii are so present in our society that if we add up all these small potential effects then it becomes a potential public health question.”
The study was published online Jan. 30, 2022, in the Journal of Psychiatric Research.
Inconsistent evidence
T. gondii infects about 30% of the human population and is usually transmitted by cats. Most infections are asymptomatic, but T. gondii can cause toxoplasmosis in humans, which has been linked to increased risk of schizophrenia, suicide attempts, and more recently, mild cognitive impairment.
Although some studies show an association between cat ownership and increased risk of mental illness, the research findings have been inconsistent.
“The evidence has been mixed about the association between cat ownership and psychosis expression, so our approach was to consider whether specific factors or combinations of factors could explain this mixed evidence,” Dr. Paquin said.
For the study, 2206 individuals aged 18-40 years completed the Community Assessment of Psychic Experiences (CAPE-42) and a questionnaire to gather information about cat ownership at any time between birth and age 13 and if the cats lived exclusively indoors (nonhunting) or if they were allowed outside (rodent hunting).
Participants were also asked about the number of residential moves between birth and age 15, date and place of birth, lifetime history of head trauma, and tobacco smoking history.
Rodent-hunting cat ownership was associated with higher risk of psychosis in male participants, compared with owning no cat or a nonhunting cat. When the investigators added head trauma and residential moves to rodent-hunting cat ownership, psychosis risk was elevated in both men and women.
Independent of cat ownership, younger age, moving more than three times as a child, a history of head trauma, and being a smoker were all associated with higher psychosis risk.
The study wasn’t designed to explore potential biological mechanisms to explain the sex differences in psychosis risk seen among rodent-hunting cat owners, but “one possible explanation based on the animal model literature is that the neurobiological effects of parasitic exposure may be greater with male sex,” senior author Suzanne King, PhD, professor of psychiatry at McGill, said in an interview.
The new study is part of a larger, long-term project called EnviroGen, led by Dr. King, examining the environmental and genetic risk factors for schizophrenia.
Need for replication
Commenting on the findings, E. Fuller Torrey, MD, who was among the first researchers to identify a link between cat ownership, T. gondii infection, and schizophrenia, said the study is “an interesting addition to the studies of cat ownership in childhood as a risk factor for psychosis.”
Of the approximately 10 published studies on the topic, about half suggest a link between cat ownership and psychosis later in life, said Dr. Torrey, associate director for research at the Stanley Medical Research Institute in Rockville, Md.
“The Canadian study is interesting in that it is the first study that separates exposure to permanently indoor cats from cats that are allowed to go outdoors, and the results were positive only for outdoor cats,” Dr. Torrey said.
The study has limitations, Dr. Torrey added, including its retrospective design and the use of a self-report questionnaire to assess psychotic experiences in adulthood.
Also commenting on findings, James Kirkbride, PhD, professor of psychiatric and social epidemiology, University College London, noted the same limitations.
Dr. Kirkbride is the lead author of a 2017 study that showed no link between cat ownership and serious mental illness that included nearly 5,000 people born in 1991 or 1992 and followed until age 18. In this study, there was no link between psychosis and cat ownership during pregnancy or at ages 4 or 10 years.
“Researchers have long been fascinated with the idea that cat ownership may affect mental health. This paper may have them chasing their own tail,” Dr. Kirkbride said.
“Evidence of any association is limited to certain subgroups without a strong theoretical basis for why this may be the case,” he added. “The retrospective and cross-sectional nature of the survey also raise the possibility that the results are impacted by differential recall bias, as well as the broader issues of chance and unobserved confounding.”
Dr. King noted that recall bias is a limitation the researchers highlighted in their study, but “considering the exposures are relatively objective and factual, we do not believe the potential for recall bias is substantial.”
“Nonetheless, we strongly believe that replication of our results in prospective, population-representative cohorts will be crucial to making firmer conclusions,” he added.
The study was funded by grants from the Quebec Health Research Fund. The study authors and Dr. Kirkbride disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF PSYCHIATRIC RESEARCH