User login
Drug Combo Effective in Resistant Hepatitis C
A combined regimen of daclatasvir and sofosbuvir achieved sustained virologic response rates greater than 90% in an industry-sponsored trial involving patients with chronic HCV, according to study published online Jan. 16 in the New England Journal of Medicine.
The once-daily oral treatment was effective against HCV type 1 among patients with any viral subtype, as well as among patients who had failed to respond to or had developed resistance to protease inhibitors. The latter group currently has no other treatment options. It also was effective against HCV types 2 and 3, said Dr. Mark S. Sulkowski of Johns Hopkins University, Baltimore, and his associates ((N. Engl. J. Med. 2014 Jan. 16;370:211-21).
In particular, the daclatasvir-sofosbuvir combination was very effective in patients "with characteristics that were previously associated with a poor response to treatment – HCV genotypes 1a and 3, the non-CC IL28B genotype, and black race," the investigators noted.
Dr. Sulkowski and his colleagues assessed the combination therapy in an open-label study involving 211 adults treated during a 17-month period at 18 medical centers across the United States.
Initially, 44 previously untreated patients with HCV 1 infection and 44 patients with HCV 2 or 3 were randomly assigned to receive daclatasvir plus sofosbuvir, with or without concurrent ribavirin, for 24 weeks. Then the study was expanded to include another 123 patients with HCV 1 infection: 82 who were previously untreated were randomly assigned to receive the combination therapy, with or without ribavirin, for 12 weeks; and the remaining 41 who had failed on telaprevir or boceprevir plus peginterferon alfa-ribavirin were assigned to receive the combination therapy, with or without ribavirin, for 24 weeks.
The primary efficacy endpoint was a sustained virologic response (defined as an HCV RNA level of less than 25 IU/mL) at week 12 after the end of treatment.
That rate was 98% (164 of 167 patients) among those who had HCV 1 infection. Of the three patients in that group classified as not having a sustained virologic response at week 12, two missed their assessment visit at 12 weeks but showed a sustained virologic response at 24 weeks, and the third was lost to follow-up.
The rate of sustained virologic response was 91% (40 of 44 patients) among those who had HCV 2 or 3 infection. Individually, the rate was 92% in patients with HCV 2 and 89% among those with HCV 3, the investigators said.

The high rates of sustained virologic response were consistent across all subgroups of patients, including 129 of the 132 (98%) who had genotype 1a; 57 of the 61 (93%) who had genotype IL28B; 25 of the 26 (96%) who were black; 9 of the 10 (90%) who were of "other" race/ethnicity; 85 of the 90 (94%) who received concurrent ribavirin; 119 of the 121 (98%) who did not receive ribavirin; and 40 of the 41 (98%) who had failed on or developed resistance to protease inhibitors.
"This represents proof of concept that a sustained virologic response can be achieved in patients in whom previous treatment with telaprevir or boceprevir had failed, including patients who have persistent HCV variants with resistance to protease inhibitors," Dr. Sulkowski and his associates said.
Two patients discontinued treatment because of adverse events. One patient developed fibromyalgia, and another had a stroke. Both had shown a sustained virologic response to the combination therapy. The most common adverse events were fatigue, headache, and nausea. The most common grade 3 or 4 laboratory abnormalities were low phosphorous levels and elevated glucose levels.
The study was supported by Bristol-Myers Squibb and Pharmasset (now Gilead). Dr. Sulkowski reported financial ties to Bristol-Myers Squibb and Gilead, in addition to other pharmaceutical companies. His associates reported ties to numerous industry sources.
A combined regimen of daclatasvir and sofosbuvir achieved sustained virologic response rates greater than 90% in an industry-sponsored trial involving patients with chronic HCV, according to study published online Jan. 16 in the New England Journal of Medicine.
The once-daily oral treatment was effective against HCV type 1 among patients with any viral subtype, as well as among patients who had failed to respond to or had developed resistance to protease inhibitors. The latter group currently has no other treatment options. It also was effective against HCV types 2 and 3, said Dr. Mark S. Sulkowski of Johns Hopkins University, Baltimore, and his associates ((N. Engl. J. Med. 2014 Jan. 16;370:211-21).
In particular, the daclatasvir-sofosbuvir combination was very effective in patients "with characteristics that were previously associated with a poor response to treatment – HCV genotypes 1a and 3, the non-CC IL28B genotype, and black race," the investigators noted.
Dr. Sulkowski and his colleagues assessed the combination therapy in an open-label study involving 211 adults treated during a 17-month period at 18 medical centers across the United States.
Initially, 44 previously untreated patients with HCV 1 infection and 44 patients with HCV 2 or 3 were randomly assigned to receive daclatasvir plus sofosbuvir, with or without concurrent ribavirin, for 24 weeks. Then the study was expanded to include another 123 patients with HCV 1 infection: 82 who were previously untreated were randomly assigned to receive the combination therapy, with or without ribavirin, for 12 weeks; and the remaining 41 who had failed on telaprevir or boceprevir plus peginterferon alfa-ribavirin were assigned to receive the combination therapy, with or without ribavirin, for 24 weeks.
The primary efficacy endpoint was a sustained virologic response (defined as an HCV RNA level of less than 25 IU/mL) at week 12 after the end of treatment.
That rate was 98% (164 of 167 patients) among those who had HCV 1 infection. Of the three patients in that group classified as not having a sustained virologic response at week 12, two missed their assessment visit at 12 weeks but showed a sustained virologic response at 24 weeks, and the third was lost to follow-up.
The rate of sustained virologic response was 91% (40 of 44 patients) among those who had HCV 2 or 3 infection. Individually, the rate was 92% in patients with HCV 2 and 89% among those with HCV 3, the investigators said.
The high rates of sustained virologic response were consistent across all subgroups of patients, including 129 of the 132 (98%) who had genotype 1a; 57 of the 61 (93%) who had genotype IL28B; 25 of the 26 (96%) who were black; 9 of the 10 (90%) who were of "other" race/ethnicity; 85 of the 90 (94%) who received concurrent ribavirin; 119 of the 121 (98%) who did not receive ribavirin; and 40 of the 41 (98%) who had failed on or developed resistance to protease inhibitors.
"This represents proof of concept that a sustained virologic response can be achieved in patients in whom previous treatment with telaprevir or boceprevir had failed, including patients who have persistent HCV variants with resistance to protease inhibitors," Dr. Sulkowski and his associates said.
Two patients discontinued treatment because of adverse events. One patient developed fibromyalgia, and another had a stroke. Both had shown a sustained virologic response to the combination therapy. The most common adverse events were fatigue, headache, and nausea. The most common grade 3 or 4 laboratory abnormalities were low phosphorous levels and elevated glucose levels.
The study was supported by Bristol-Myers Squibb and Pharmasset (now Gilead). Dr. Sulkowski reported financial ties to Bristol-Myers Squibb and Gilead, in addition to other pharmaceutical companies. His associates reported ties to numerous industry sources.
A combined regimen of daclatasvir and sofosbuvir achieved sustained virologic response rates greater than 90% in an industry-sponsored trial involving patients with chronic HCV, according to study published online Jan. 16 in the New England Journal of Medicine.
The once-daily oral treatment was effective against HCV type 1 among patients with any viral subtype, as well as among patients who had failed to respond to or had developed resistance to protease inhibitors. The latter group currently has no other treatment options. It also was effective against HCV types 2 and 3, said Dr. Mark S. Sulkowski of Johns Hopkins University, Baltimore, and his associates ((N. Engl. J. Med. 2014 Jan. 16;370:211-21).
In particular, the daclatasvir-sofosbuvir combination was very effective in patients "with characteristics that were previously associated with a poor response to treatment – HCV genotypes 1a and 3, the non-CC IL28B genotype, and black race," the investigators noted.
Dr. Sulkowski and his colleagues assessed the combination therapy in an open-label study involving 211 adults treated during a 17-month period at 18 medical centers across the United States.
Initially, 44 previously untreated patients with HCV 1 infection and 44 patients with HCV 2 or 3 were randomly assigned to receive daclatasvir plus sofosbuvir, with or without concurrent ribavirin, for 24 weeks. Then the study was expanded to include another 123 patients with HCV 1 infection: 82 who were previously untreated were randomly assigned to receive the combination therapy, with or without ribavirin, for 12 weeks; and the remaining 41 who had failed on telaprevir or boceprevir plus peginterferon alfa-ribavirin were assigned to receive the combination therapy, with or without ribavirin, for 24 weeks.
The primary efficacy endpoint was a sustained virologic response (defined as an HCV RNA level of less than 25 IU/mL) at week 12 after the end of treatment.
That rate was 98% (164 of 167 patients) among those who had HCV 1 infection. Of the three patients in that group classified as not having a sustained virologic response at week 12, two missed their assessment visit at 12 weeks but showed a sustained virologic response at 24 weeks, and the third was lost to follow-up.
The rate of sustained virologic response was 91% (40 of 44 patients) among those who had HCV 2 or 3 infection. Individually, the rate was 92% in patients with HCV 2 and 89% among those with HCV 3, the investigators said.
The high rates of sustained virologic response were consistent across all subgroups of patients, including 129 of the 132 (98%) who had genotype 1a; 57 of the 61 (93%) who had genotype IL28B; 25 of the 26 (96%) who were black; 9 of the 10 (90%) who were of "other" race/ethnicity; 85 of the 90 (94%) who received concurrent ribavirin; 119 of the 121 (98%) who did not receive ribavirin; and 40 of the 41 (98%) who had failed on or developed resistance to protease inhibitors.
"This represents proof of concept that a sustained virologic response can be achieved in patients in whom previous treatment with telaprevir or boceprevir had failed, including patients who have persistent HCV variants with resistance to protease inhibitors," Dr. Sulkowski and his associates said.
Two patients discontinued treatment because of adverse events. One patient developed fibromyalgia, and another had a stroke. Both had shown a sustained virologic response to the combination therapy. The most common adverse events were fatigue, headache, and nausea. The most common grade 3 or 4 laboratory abnormalities were low phosphorous levels and elevated glucose levels.
The study was supported by Bristol-Myers Squibb and Pharmasset (now Gilead). Dr. Sulkowski reported financial ties to Bristol-Myers Squibb and Gilead, in addition to other pharmaceutical companies. His associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
The Art and Science of Detecting Allergic Contact Dermatitis
WOODINVILLE, WASH. – Identifying the culprit in allergic contact dermatitis often requires careful sleuthing and tailored patch testing, according to Dr. James G. Marks Jr.
Dr. Marks reviewed the current options for patch testing trays, described several cases of allergic contact dermatitis, and shared pointers for diagnosis and management at the annual Coastal Dermatology Symposium.
Allergen-screening series
Dermatologists can now choose from a variety of standard screening trays for patch testing, said Dr. Marks, professor and chair of the department of dermatology, Pennsylvania State University, Hershey. The TRUE test (the only one approved by the Food and Drug Administration) contains 35 antigens.
However, dermatologists can supplement and customize these screening trays to create a system specific to their practice and geographic area. Dr. Marks said he uses a customized tray with 100 antigens.
"The important point is there is no universal standard screening tray, so pick what works for you," he said.
"Those of you who use the TRUE test, great; as you know in the last year you have had another panel [added], so you get more screening antigens," he said. "It makes sense intuitively, and it’s proven by publications of the North American [Contact Dermatitis] Group and others that the more antigens you test with, the more positives you get and the more relevant reactions you can get," he explained.
"Then create your own," Dr. Marks advised. "So if you use the TRUE test, maybe supplement ... with a few more allergens."
Alpha-methylene-gamma-butyrolactone
Florists may come in contact with alpha-methylene-gamma-butyrolactone through handling Alstroemeria (also known as Peruvian lily), a flower popular because of its long-lasting blooms.
The compound is found in the sap that leaks out from cut stems; thus, the presentation is typically finger dermatitis, Dr. Marks said at the meeting, which was presented by the Caribbean Dermatology Symposium.
"It is the most common cause of allergic contact dermatitis in florists. So if you see florists, this is the allergen until proven otherwise," he said.
The compound is also found in the white epidermis of tulips, in which case it is known as tuliposide A. About half of tulip bulb sorters are allergic to it.
"You either patch test with parts of the Alstroemeria plant or get the allergen alpha-methylene-gamma-butyrolactone" commercially, Dr. Marks said. "I test everyone to alpha-methylene-gamma-butyrolactone, even though it’s a small subset. That’s one of my 100 [antigens]."
Methylisothiazolinone
"Methylisothiazolinone has become a very important and hot allergen," Dr. Marks commented. This allergen is increasingly used in personal care products and requires a special approach to patch testing. It is found in many wet wipes, use of which can produce, for example, perioral dermatitis.
The standard combination test antigen, applied at 100 parts per million, contains 3 parts methylchloroisothiazolinone (MCI) and 1 part methylisothiazolinone (MI), he noted. Thus, "you are really only patch testing to 25 parts per million of MI."
"The recommended concentration of patch test to MI is a bit in flux," said Dr. Marks; the North American group currently uses 2,000 parts per million but is considering halving that number, he noted.
"You can see how you can miss patients who are allergic to MI if you only patch test to MCI/MI," he commented. "So those of you who are using the TRUE test, you are going to miss patients who are allergic to MI."
"The important point is you’ve got to test both – MCI/MI and MI alone. ... You should supplement what you are patch testing with MI, certainly at least at 1,000 parts per million, if not at 2,000," Dr. Marks advised.
"The Cosmetic Ingredient Review, which sets limits for [MI] in the U.S., is going to be reevaluating, and I’m sure will be having lower limits in leave-on and rinse-off products," he noted.
Rubber accelerators
Surgeons may develop particularly problematic allergic contact dermatitis as a reaction to the rubber accelerators used in the manufacturing of many surgical gloves, Dr. Marks noted.
He described the case of a surgeon who developed severe hand dermatitis and eventually a generalized dermatitis. "In this case, if you used the TRUE test, you would make the diagnosis; he was positive to thiuram and carba mix."
Allergen avoidance entailed finding an alternative, rubber-free surgical glove, the Derma Prene Ultra glove (manufactured by Ansell), which is made of neoprene. Also, the surgeon switched to vinyl exam gloves for outpatient care.
"There may be other surgical gloves ...," Dr. Marks acknowledged. "But be sure and keep this some place because some time in the future when you have your surgeon friend with hand dermatitis, you can recommend that glove after you patch test them and prove that they are rubber-accelerator positive."
Cocamidopropyl betaine contaminants
Patients may develop allergic contact dermatitis after using shampoos and bath gels containing cocamidopropyl betaine, a surfactant.
In fact, they are actually reacting to a contaminant or impurity generated in the manufacturing process, either 3-dimethylaminopropylamine or amidoamine, according to Dr. Marks.
"So if you have pure cocamidopropyl betaine, there will be no allergy," he noted. But if you test for "cocamidopropyl betaine, and what you are patch testing with is from, say, Chemotechnique or Allergeaze, it’s going to have presumably the contaminants or the impurities in it, 3-dimethylaminopropylamine and amidoamine."
Treatment entails careful reading of labels on personal care products and avoidance of those containing cocamidopropyl betaine.
Acrylates
Don’t rule out acrylates – either acrylic or methacrylic acid – monomers that are polymerized with heat or light to form solid plastics that can cause reactions.
"The monomers are both irritants and allergens, so you need the right concentration to patch test to," Dr. Marks noted. "They are found in all sorts of things – adhesives, inks, artificial nails, dental resins, bone cement, and plastics."
Presentations may vary widely, including, for example, finger dermatitis in patients who have sculptured nails, and gum stomatitis in patients who have undergone procedures involving dental resin, said Dr. Marks.
"If you have workers or patients who have exposure to acrylates, you need more extensive screening," Dr. Marks advised, noting that his acrylate patch test series contains six compounds.
"No one is a screen for all of them," he commented. "Some [experts] feel that ethyl acrylate is the best screen; certainly, for sculptured nails it’s good." Others in his series include methyl methacrylate (found in bone cement) and ethyl cyanoacrylate (found in Super Glue adhesive).
Glyceryl thioglycolate
Allergy to glyceryl thioglycolate, found in acid permanent waves, can manifest as hand dermatitis in hairdressers and as dermatitis of the face, neck, and ears in their clients.
"If you see hairdressers [in your practice], you should consider strongly having this antigen as part of your [patch test] armamentarium," Dr. Marks recommended.
Alkaline perms, by contrast, do not contain glyceryl thioglycolate and thus provide a simple solution. "You can cure that hairdresser, and she or he can continue to do perms just by switching from an acid to an alkaline perm," he explained.
Dr. Marks said he had no relevant financial disclosures.
WOODINVILLE, WASH. – Identifying the culprit in allergic contact dermatitis often requires careful sleuthing and tailored patch testing, according to Dr. James G. Marks Jr.
Dr. Marks reviewed the current options for patch testing trays, described several cases of allergic contact dermatitis, and shared pointers for diagnosis and management at the annual Coastal Dermatology Symposium.
Allergen-screening series
Dermatologists can now choose from a variety of standard screening trays for patch testing, said Dr. Marks, professor and chair of the department of dermatology, Pennsylvania State University, Hershey. The TRUE test (the only one approved by the Food and Drug Administration) contains 35 antigens.
However, dermatologists can supplement and customize these screening trays to create a system specific to their practice and geographic area. Dr. Marks said he uses a customized tray with 100 antigens.
"The important point is there is no universal standard screening tray, so pick what works for you," he said.
"Those of you who use the TRUE test, great; as you know in the last year you have had another panel [added], so you get more screening antigens," he said. "It makes sense intuitively, and it’s proven by publications of the North American [Contact Dermatitis] Group and others that the more antigens you test with, the more positives you get and the more relevant reactions you can get," he explained.
"Then create your own," Dr. Marks advised. "So if you use the TRUE test, maybe supplement ... with a few more allergens."
Alpha-methylene-gamma-butyrolactone
Florists may come in contact with alpha-methylene-gamma-butyrolactone through handling Alstroemeria (also known as Peruvian lily), a flower popular because of its long-lasting blooms.
The compound is found in the sap that leaks out from cut stems; thus, the presentation is typically finger dermatitis, Dr. Marks said at the meeting, which was presented by the Caribbean Dermatology Symposium.
"It is the most common cause of allergic contact dermatitis in florists. So if you see florists, this is the allergen until proven otherwise," he said.
The compound is also found in the white epidermis of tulips, in which case it is known as tuliposide A. About half of tulip bulb sorters are allergic to it.
"You either patch test with parts of the Alstroemeria plant or get the allergen alpha-methylene-gamma-butyrolactone" commercially, Dr. Marks said. "I test everyone to alpha-methylene-gamma-butyrolactone, even though it’s a small subset. That’s one of my 100 [antigens]."
Methylisothiazolinone
"Methylisothiazolinone has become a very important and hot allergen," Dr. Marks commented. This allergen is increasingly used in personal care products and requires a special approach to patch testing. It is found in many wet wipes, use of which can produce, for example, perioral dermatitis.
The standard combination test antigen, applied at 100 parts per million, contains 3 parts methylchloroisothiazolinone (MCI) and 1 part methylisothiazolinone (MI), he noted. Thus, "you are really only patch testing to 25 parts per million of MI."
"The recommended concentration of patch test to MI is a bit in flux," said Dr. Marks; the North American group currently uses 2,000 parts per million but is considering halving that number, he noted.
"You can see how you can miss patients who are allergic to MI if you only patch test to MCI/MI," he commented. "So those of you who are using the TRUE test, you are going to miss patients who are allergic to MI."
"The important point is you’ve got to test both – MCI/MI and MI alone. ... You should supplement what you are patch testing with MI, certainly at least at 1,000 parts per million, if not at 2,000," Dr. Marks advised.
"The Cosmetic Ingredient Review, which sets limits for [MI] in the U.S., is going to be reevaluating, and I’m sure will be having lower limits in leave-on and rinse-off products," he noted.
Rubber accelerators
Surgeons may develop particularly problematic allergic contact dermatitis as a reaction to the rubber accelerators used in the manufacturing of many surgical gloves, Dr. Marks noted.
He described the case of a surgeon who developed severe hand dermatitis and eventually a generalized dermatitis. "In this case, if you used the TRUE test, you would make the diagnosis; he was positive to thiuram and carba mix."
Allergen avoidance entailed finding an alternative, rubber-free surgical glove, the Derma Prene Ultra glove (manufactured by Ansell), which is made of neoprene. Also, the surgeon switched to vinyl exam gloves for outpatient care.
"There may be other surgical gloves ...," Dr. Marks acknowledged. "But be sure and keep this some place because some time in the future when you have your surgeon friend with hand dermatitis, you can recommend that glove after you patch test them and prove that they are rubber-accelerator positive."
Cocamidopropyl betaine contaminants
Patients may develop allergic contact dermatitis after using shampoos and bath gels containing cocamidopropyl betaine, a surfactant.
In fact, they are actually reacting to a contaminant or impurity generated in the manufacturing process, either 3-dimethylaminopropylamine or amidoamine, according to Dr. Marks.
"So if you have pure cocamidopropyl betaine, there will be no allergy," he noted. But if you test for "cocamidopropyl betaine, and what you are patch testing with is from, say, Chemotechnique or Allergeaze, it’s going to have presumably the contaminants or the impurities in it, 3-dimethylaminopropylamine and amidoamine."
Treatment entails careful reading of labels on personal care products and avoidance of those containing cocamidopropyl betaine.
Acrylates
Don’t rule out acrylates – either acrylic or methacrylic acid – monomers that are polymerized with heat or light to form solid plastics that can cause reactions.
"The monomers are both irritants and allergens, so you need the right concentration to patch test to," Dr. Marks noted. "They are found in all sorts of things – adhesives, inks, artificial nails, dental resins, bone cement, and plastics."
Presentations may vary widely, including, for example, finger dermatitis in patients who have sculptured nails, and gum stomatitis in patients who have undergone procedures involving dental resin, said Dr. Marks.
"If you have workers or patients who have exposure to acrylates, you need more extensive screening," Dr. Marks advised, noting that his acrylate patch test series contains six compounds.
"No one is a screen for all of them," he commented. "Some [experts] feel that ethyl acrylate is the best screen; certainly, for sculptured nails it’s good." Others in his series include methyl methacrylate (found in bone cement) and ethyl cyanoacrylate (found in Super Glue adhesive).
Glyceryl thioglycolate
Allergy to glyceryl thioglycolate, found in acid permanent waves, can manifest as hand dermatitis in hairdressers and as dermatitis of the face, neck, and ears in their clients.
"If you see hairdressers [in your practice], you should consider strongly having this antigen as part of your [patch test] armamentarium," Dr. Marks recommended.
Alkaline perms, by contrast, do not contain glyceryl thioglycolate and thus provide a simple solution. "You can cure that hairdresser, and she or he can continue to do perms just by switching from an acid to an alkaline perm," he explained.
Dr. Marks said he had no relevant financial disclosures.
WOODINVILLE, WASH. – Identifying the culprit in allergic contact dermatitis often requires careful sleuthing and tailored patch testing, according to Dr. James G. Marks Jr.
Dr. Marks reviewed the current options for patch testing trays, described several cases of allergic contact dermatitis, and shared pointers for diagnosis and management at the annual Coastal Dermatology Symposium.
Allergen-screening series
Dermatologists can now choose from a variety of standard screening trays for patch testing, said Dr. Marks, professor and chair of the department of dermatology, Pennsylvania State University, Hershey. The TRUE test (the only one approved by the Food and Drug Administration) contains 35 antigens.
However, dermatologists can supplement and customize these screening trays to create a system specific to their practice and geographic area. Dr. Marks said he uses a customized tray with 100 antigens.
"The important point is there is no universal standard screening tray, so pick what works for you," he said.
"Those of you who use the TRUE test, great; as you know in the last year you have had another panel [added], so you get more screening antigens," he said. "It makes sense intuitively, and it’s proven by publications of the North American [Contact Dermatitis] Group and others that the more antigens you test with, the more positives you get and the more relevant reactions you can get," he explained.
"Then create your own," Dr. Marks advised. "So if you use the TRUE test, maybe supplement ... with a few more allergens."
Alpha-methylene-gamma-butyrolactone
Florists may come in contact with alpha-methylene-gamma-butyrolactone through handling Alstroemeria (also known as Peruvian lily), a flower popular because of its long-lasting blooms.
The compound is found in the sap that leaks out from cut stems; thus, the presentation is typically finger dermatitis, Dr. Marks said at the meeting, which was presented by the Caribbean Dermatology Symposium.
"It is the most common cause of allergic contact dermatitis in florists. So if you see florists, this is the allergen until proven otherwise," he said.
The compound is also found in the white epidermis of tulips, in which case it is known as tuliposide A. About half of tulip bulb sorters are allergic to it.
"You either patch test with parts of the Alstroemeria plant or get the allergen alpha-methylene-gamma-butyrolactone" commercially, Dr. Marks said. "I test everyone to alpha-methylene-gamma-butyrolactone, even though it’s a small subset. That’s one of my 100 [antigens]."
Methylisothiazolinone
"Methylisothiazolinone has become a very important and hot allergen," Dr. Marks commented. This allergen is increasingly used in personal care products and requires a special approach to patch testing. It is found in many wet wipes, use of which can produce, for example, perioral dermatitis.
The standard combination test antigen, applied at 100 parts per million, contains 3 parts methylchloroisothiazolinone (MCI) and 1 part methylisothiazolinone (MI), he noted. Thus, "you are really only patch testing to 25 parts per million of MI."
"The recommended concentration of patch test to MI is a bit in flux," said Dr. Marks; the North American group currently uses 2,000 parts per million but is considering halving that number, he noted.
"You can see how you can miss patients who are allergic to MI if you only patch test to MCI/MI," he commented. "So those of you who are using the TRUE test, you are going to miss patients who are allergic to MI."
"The important point is you’ve got to test both – MCI/MI and MI alone. ... You should supplement what you are patch testing with MI, certainly at least at 1,000 parts per million, if not at 2,000," Dr. Marks advised.
"The Cosmetic Ingredient Review, which sets limits for [MI] in the U.S., is going to be reevaluating, and I’m sure will be having lower limits in leave-on and rinse-off products," he noted.
Rubber accelerators
Surgeons may develop particularly problematic allergic contact dermatitis as a reaction to the rubber accelerators used in the manufacturing of many surgical gloves, Dr. Marks noted.
He described the case of a surgeon who developed severe hand dermatitis and eventually a generalized dermatitis. "In this case, if you used the TRUE test, you would make the diagnosis; he was positive to thiuram and carba mix."
Allergen avoidance entailed finding an alternative, rubber-free surgical glove, the Derma Prene Ultra glove (manufactured by Ansell), which is made of neoprene. Also, the surgeon switched to vinyl exam gloves for outpatient care.
"There may be other surgical gloves ...," Dr. Marks acknowledged. "But be sure and keep this some place because some time in the future when you have your surgeon friend with hand dermatitis, you can recommend that glove after you patch test them and prove that they are rubber-accelerator positive."
Cocamidopropyl betaine contaminants
Patients may develop allergic contact dermatitis after using shampoos and bath gels containing cocamidopropyl betaine, a surfactant.
In fact, they are actually reacting to a contaminant or impurity generated in the manufacturing process, either 3-dimethylaminopropylamine or amidoamine, according to Dr. Marks.
"So if you have pure cocamidopropyl betaine, there will be no allergy," he noted. But if you test for "cocamidopropyl betaine, and what you are patch testing with is from, say, Chemotechnique or Allergeaze, it’s going to have presumably the contaminants or the impurities in it, 3-dimethylaminopropylamine and amidoamine."
Treatment entails careful reading of labels on personal care products and avoidance of those containing cocamidopropyl betaine.
Acrylates
Don’t rule out acrylates – either acrylic or methacrylic acid – monomers that are polymerized with heat or light to form solid plastics that can cause reactions.
"The monomers are both irritants and allergens, so you need the right concentration to patch test to," Dr. Marks noted. "They are found in all sorts of things – adhesives, inks, artificial nails, dental resins, bone cement, and plastics."
Presentations may vary widely, including, for example, finger dermatitis in patients who have sculptured nails, and gum stomatitis in patients who have undergone procedures involving dental resin, said Dr. Marks.
"If you have workers or patients who have exposure to acrylates, you need more extensive screening," Dr. Marks advised, noting that his acrylate patch test series contains six compounds.
"No one is a screen for all of them," he commented. "Some [experts] feel that ethyl acrylate is the best screen; certainly, for sculptured nails it’s good." Others in his series include methyl methacrylate (found in bone cement) and ethyl cyanoacrylate (found in Super Glue adhesive).
Glyceryl thioglycolate
Allergy to glyceryl thioglycolate, found in acid permanent waves, can manifest as hand dermatitis in hairdressers and as dermatitis of the face, neck, and ears in their clients.
"If you see hairdressers [in your practice], you should consider strongly having this antigen as part of your [patch test] armamentarium," Dr. Marks recommended.
Alkaline perms, by contrast, do not contain glyceryl thioglycolate and thus provide a simple solution. "You can cure that hairdresser, and she or he can continue to do perms just by switching from an acid to an alkaline perm," he explained.
Dr. Marks said he had no relevant financial disclosures.
AT THE COASTAL DERMATOLOGY SYMPOSIUM

Clinician Recommendation Key to HPV Vaccine Coverage
Better vaccine coverage of adolescents against HPV infection hinges on clinicians and other health care professionals both recommending the vaccine and educating patients and parents about its importance, according to a report published online Nov. 25 in JAMA Pediatrics.
In a review of the extensive literature concerning barriers to HPV vaccination among patients aged 11-17 years, health care professionals’ failure to recommend the vaccine was found to be a leading obstacle to more widespread coverage, said Dawn M. Holman of the division of cancer prevention and control, Centers for Disease Control and Prevention, Atlanta, and her associates.

The most recent data from the National Immunization Survey indicates that only 53% of adolescent girls in the United States have received at least one dose of the HPV vaccine series, only 35% have completed all three doses in the series, and only 8% of adolescent boys in the United States have initiated the HPV vaccine series. By comparison, coverage for the meningococcal conjugate vaccine is approximately 70% and coverage for the tetanus, diphtheria, and acellular pertussis vaccine is 78% in the same age group.
Ms. Holman and her associates performed a systematic review of the literature and found 55 studies published in 2009-2012 that addressed obstacles to HPV vaccination in this age group.
In ten articles that addressed barriers to HPV vaccination among health care professionals, researchers found that while most physicians support HPV vaccination and offer it to their patients, many tend not to offer it to the youngest adolescents or to boys. Many also offer HPV vaccination only according to their own perception of the patient’s risk of contracting the virus. And many do not appear to understand the importance of giving the HPV vaccine well before adolescents become sexually active.
Health care professionals also tend not to provide detailed information to either patients or their parents regarding the risks and benefits of HPV vaccination, or they emphasize the fact that it is optional – both of which come across to patients and parents as a less-than-ringing endorsement. Some health care professionals reported that HPV vaccination is under the parents’ control rather than theirs, and many cited the cost of the HPV vaccine, and the lack or lateness of insurance reimbursement, as a significant obstacle.
In contrast, concerns about the safety and efficacy of the HPV vaccine were rarely cited as contributing to poor coverage (JAMA Pediatrics 2013 Nov. 25 [doi:10.1001/jamapediatrics.2013.2752]).
A total of 64% of the reviewed articles involved barriers to vaccination among parents. Not having a physician recommendation and not getting enough information about the HPV vaccine from health care providers were the chief obstacles to greater coverage in this group. Certain religious affiliations also were associated with opposition to the HPV vaccine.
In contrast, costs and lack of access were cited infrequently. Few parents reported concerns about vaccine safety or efficacy, and few reported concern that the vaccination might affect their child’s sexual behavior.
"Providing adequate, clear, and accessible information to parents about HPV infection, vaccine safety, adverse effects, and the appropriate age for vaccination may be one way health care professionals can reduce concerns and misconceptions about the vaccine," Ms. Holman and her colleagues noted.
Other strategies to improve HPV vaccination coverage include educating health care professionals and the public in general about the importance of vaccinating adolescent males, and ensuring that underserved populations are informed about and given access to the vaccine, they added.
Better vaccine coverage of adolescents against HPV infection hinges on clinicians and other health care professionals both recommending the vaccine and educating patients and parents about its importance, according to a report published online Nov. 25 in JAMA Pediatrics.
In a review of the extensive literature concerning barriers to HPV vaccination among patients aged 11-17 years, health care professionals’ failure to recommend the vaccine was found to be a leading obstacle to more widespread coverage, said Dawn M. Holman of the division of cancer prevention and control, Centers for Disease Control and Prevention, Atlanta, and her associates.
The most recent data from the National Immunization Survey indicates that only 53% of adolescent girls in the United States have received at least one dose of the HPV vaccine series, only 35% have completed all three doses in the series, and only 8% of adolescent boys in the United States have initiated the HPV vaccine series. By comparison, coverage for the meningococcal conjugate vaccine is approximately 70% and coverage for the tetanus, diphtheria, and acellular pertussis vaccine is 78% in the same age group.
Ms. Holman and her associates performed a systematic review of the literature and found 55 studies published in 2009-2012 that addressed obstacles to HPV vaccination in this age group.
In ten articles that addressed barriers to HPV vaccination among health care professionals, researchers found that while most physicians support HPV vaccination and offer it to their patients, many tend not to offer it to the youngest adolescents or to boys. Many also offer HPV vaccination only according to their own perception of the patient’s risk of contracting the virus. And many do not appear to understand the importance of giving the HPV vaccine well before adolescents become sexually active.
Health care professionals also tend not to provide detailed information to either patients or their parents regarding the risks and benefits of HPV vaccination, or they emphasize the fact that it is optional – both of which come across to patients and parents as a less-than-ringing endorsement. Some health care professionals reported that HPV vaccination is under the parents’ control rather than theirs, and many cited the cost of the HPV vaccine, and the lack or lateness of insurance reimbursement, as a significant obstacle.
In contrast, concerns about the safety and efficacy of the HPV vaccine were rarely cited as contributing to poor coverage (JAMA Pediatrics 2013 Nov. 25 [doi:10.1001/jamapediatrics.2013.2752]).
A total of 64% of the reviewed articles involved barriers to vaccination among parents. Not having a physician recommendation and not getting enough information about the HPV vaccine from health care providers were the chief obstacles to greater coverage in this group. Certain religious affiliations also were associated with opposition to the HPV vaccine.
In contrast, costs and lack of access were cited infrequently. Few parents reported concerns about vaccine safety or efficacy, and few reported concern that the vaccination might affect their child’s sexual behavior.
"Providing adequate, clear, and accessible information to parents about HPV infection, vaccine safety, adverse effects, and the appropriate age for vaccination may be one way health care professionals can reduce concerns and misconceptions about the vaccine," Ms. Holman and her colleagues noted.
Other strategies to improve HPV vaccination coverage include educating health care professionals and the public in general about the importance of vaccinating adolescent males, and ensuring that underserved populations are informed about and given access to the vaccine, they added.
Better vaccine coverage of adolescents against HPV infection hinges on clinicians and other health care professionals both recommending the vaccine and educating patients and parents about its importance, according to a report published online Nov. 25 in JAMA Pediatrics.
In a review of the extensive literature concerning barriers to HPV vaccination among patients aged 11-17 years, health care professionals’ failure to recommend the vaccine was found to be a leading obstacle to more widespread coverage, said Dawn M. Holman of the division of cancer prevention and control, Centers for Disease Control and Prevention, Atlanta, and her associates.
The most recent data from the National Immunization Survey indicates that only 53% of adolescent girls in the United States have received at least one dose of the HPV vaccine series, only 35% have completed all three doses in the series, and only 8% of adolescent boys in the United States have initiated the HPV vaccine series. By comparison, coverage for the meningococcal conjugate vaccine is approximately 70% and coverage for the tetanus, diphtheria, and acellular pertussis vaccine is 78% in the same age group.
Ms. Holman and her associates performed a systematic review of the literature and found 55 studies published in 2009-2012 that addressed obstacles to HPV vaccination in this age group.
In ten articles that addressed barriers to HPV vaccination among health care professionals, researchers found that while most physicians support HPV vaccination and offer it to their patients, many tend not to offer it to the youngest adolescents or to boys. Many also offer HPV vaccination only according to their own perception of the patient’s risk of contracting the virus. And many do not appear to understand the importance of giving the HPV vaccine well before adolescents become sexually active.
Health care professionals also tend not to provide detailed information to either patients or their parents regarding the risks and benefits of HPV vaccination, or they emphasize the fact that it is optional – both of which come across to patients and parents as a less-than-ringing endorsement. Some health care professionals reported that HPV vaccination is under the parents’ control rather than theirs, and many cited the cost of the HPV vaccine, and the lack or lateness of insurance reimbursement, as a significant obstacle.
In contrast, concerns about the safety and efficacy of the HPV vaccine were rarely cited as contributing to poor coverage (JAMA Pediatrics 2013 Nov. 25 [doi:10.1001/jamapediatrics.2013.2752]).
A total of 64% of the reviewed articles involved barriers to vaccination among parents. Not having a physician recommendation and not getting enough information about the HPV vaccine from health care providers were the chief obstacles to greater coverage in this group. Certain religious affiliations also were associated with opposition to the HPV vaccine.
In contrast, costs and lack of access were cited infrequently. Few parents reported concerns about vaccine safety or efficacy, and few reported concern that the vaccination might affect their child’s sexual behavior.
"Providing adequate, clear, and accessible information to parents about HPV infection, vaccine safety, adverse effects, and the appropriate age for vaccination may be one way health care professionals can reduce concerns and misconceptions about the vaccine," Ms. Holman and her colleagues noted.
Other strategies to improve HPV vaccination coverage include educating health care professionals and the public in general about the importance of vaccinating adolescent males, and ensuring that underserved populations are informed about and given access to the vaccine, they added.
FROM JAMA PEDIATRICS

Shingles Vaccine Most Effective When Given to Patients in Their 60s
Because efficacy of the shingles vaccine appears to wane over time, it should not routinely be given to people in their 50s, according to information presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
"At this time, there is insufficient evidence supporting long-term protection of the vaccine, so if people younger than 60 [years] are vaccinated, they might not be protected when chance of disease is highest," said Dr. Jeff Duchin, chair of the ACIP’s herpes zoster working group. "We will continue to monitor data as they becomes available, but at this point we are reaffirming that vaccination be done in those age 60 [years] and older."

The committee made its recommendation after reviewing newly released data from Merck’s Long-Term Persistence Study for shingles. It found that, 10 years after vaccination, the overall incidence rate of shingles had increased from about 4/1,000 person-years to 11/1,000 person-years. The observed incidence rate of shingles in historical controls is about 13 cases/1,000 person-years.
Dr. Janie Parrino, director of vaccine clinical research at Merck Research Laboratories, presented results of the company’s latest study of the vaccine’s extended efficacy. The shingles Long-Term Persistence Study is an 8-year follow-up of the Shingles Prevention Study, in which subjects were randomized to Merck’s Zostavax vaccine or placebo. It showed that the vaccine significantly reduced the incidence of herpes zoster and postherpetic neuralgia (PHN) as well as the shingles burden of illness, in adults older than 60 years.
A short-term follow-up study appeared last year; it added 4 more years of follow-up data on more than 14,000 of the original cohort.
It found a gradual decrease in vaccine efficacy by 6-7 years after vaccination. "Analysis of vaccine efficacy in each year after vaccination for all outcomes showed a decrease after year 1, with a further decline thereafter," the investigators said. "Vaccine efficacy was statistically significant for the incidence of herpes zoster and herpes zoster burden of illness through year 5 after vaccination, but vaccine efficacy is uncertain beyond that point."
The long-term study presented at the Atlanta meeting involved up to 12 years of data on almost 7,000 people in the original cohort. It demonstrated a continuous time-bound waning of efficacy.
In addition to the increasing annual incidence of shingles, the study found an increasing incidence of PHN, from less than 1/1,000 person-years during the year of vaccination to about 1/1,000 person years by year 10. However, the incidence among placebo subjects and historical controls was more than 2/1,000 person years by that time. The shingles burden of illness (a measure of acute pain) also increased as time passed, Dr. Parrino noted.
Taking into account both clinical efficacy and cost, Ismael Ortega-Sanchez, Ph.D., a health economist with the CDC, concluded that the shingles vaccine is most effective when given to people in their 60s and 70s.
Vaccinating from age 50-59 years would prevent about 20,000 shingles cases annually. But vaccinating in the 60s would prevent 26,000 and, in the 70s, 21,000. The trend was similar for cases of PHN: prevention of 1,000 cases for vaccinating in the 50s, 4,000 for vaccinating in the 60s, and 8,000 for vaccinating in the 70s.
Other outcomes – emergency visits, ambulatory visits, hospitalizations, length of hospital stay, and prescriptions – also increased significantly over the 3 decades.
Savings tracked clinical outcomes in a value assessment model of 6 million people: 1 million vaccinated and unvaccinated in each of the three age cohorts.
Compared with not vaccinating, vaccinating those in their 50s would save $16.8 million annually. Vaccinating during the 60s would save about $24.3 million, and during the 70s, $31.9 million.
And, because younger people are likely to have more systemic reactions, they cost more to vaccinate. A model that accounted for the cost of the vaccine, administration, and treating local and systemic reactions, put the total price tag at $193 million for those in their 50s, and $190 million for each of the two older groups.
Finally, the number needed to treat to prevent one case of shingles, PHN, or non-PHN complication case was higher in those in their 50s than in those in their 60s or 70s (one shingles case – 51, 38, and 47 respectively; one PHN case – 988, 247, and 124).
"This isn’t intended to tell people not to get the vaccine early, but to make them aware of the risks and benefits, given that the greatest risk of the disease is later in life," Dr. Duchin said. Since there are no data on booster shingles vaccines, he said "we only have one shot at this and we need to focus our efforts on those at the greatest risk."
Because efficacy of the shingles vaccine appears to wane over time, it should not routinely be given to people in their 50s, according to information presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
"At this time, there is insufficient evidence supporting long-term protection of the vaccine, so if people younger than 60 [years] are vaccinated, they might not be protected when chance of disease is highest," said Dr. Jeff Duchin, chair of the ACIP’s herpes zoster working group. "We will continue to monitor data as they becomes available, but at this point we are reaffirming that vaccination be done in those age 60 [years] and older."
The committee made its recommendation after reviewing newly released data from Merck’s Long-Term Persistence Study for shingles. It found that, 10 years after vaccination, the overall incidence rate of shingles had increased from about 4/1,000 person-years to 11/1,000 person-years. The observed incidence rate of shingles in historical controls is about 13 cases/1,000 person-years.
Dr. Janie Parrino, director of vaccine clinical research at Merck Research Laboratories, presented results of the company’s latest study of the vaccine’s extended efficacy. The shingles Long-Term Persistence Study is an 8-year follow-up of the Shingles Prevention Study, in which subjects were randomized to Merck’s Zostavax vaccine or placebo. It showed that the vaccine significantly reduced the incidence of herpes zoster and postherpetic neuralgia (PHN) as well as the shingles burden of illness, in adults older than 60 years.
A short-term follow-up study appeared last year; it added 4 more years of follow-up data on more than 14,000 of the original cohort.
It found a gradual decrease in vaccine efficacy by 6-7 years after vaccination. "Analysis of vaccine efficacy in each year after vaccination for all outcomes showed a decrease after year 1, with a further decline thereafter," the investigators said. "Vaccine efficacy was statistically significant for the incidence of herpes zoster and herpes zoster burden of illness through year 5 after vaccination, but vaccine efficacy is uncertain beyond that point."
The long-term study presented at the Atlanta meeting involved up to 12 years of data on almost 7,000 people in the original cohort. It demonstrated a continuous time-bound waning of efficacy.
In addition to the increasing annual incidence of shingles, the study found an increasing incidence of PHN, from less than 1/1,000 person-years during the year of vaccination to about 1/1,000 person years by year 10. However, the incidence among placebo subjects and historical controls was more than 2/1,000 person years by that time. The shingles burden of illness (a measure of acute pain) also increased as time passed, Dr. Parrino noted.
Taking into account both clinical efficacy and cost, Ismael Ortega-Sanchez, Ph.D., a health economist with the CDC, concluded that the shingles vaccine is most effective when given to people in their 60s and 70s.
Vaccinating from age 50-59 years would prevent about 20,000 shingles cases annually. But vaccinating in the 60s would prevent 26,000 and, in the 70s, 21,000. The trend was similar for cases of PHN: prevention of 1,000 cases for vaccinating in the 50s, 4,000 for vaccinating in the 60s, and 8,000 for vaccinating in the 70s.
Other outcomes – emergency visits, ambulatory visits, hospitalizations, length of hospital stay, and prescriptions – also increased significantly over the 3 decades.
Savings tracked clinical outcomes in a value assessment model of 6 million people: 1 million vaccinated and unvaccinated in each of the three age cohorts.
Compared with not vaccinating, vaccinating those in their 50s would save $16.8 million annually. Vaccinating during the 60s would save about $24.3 million, and during the 70s, $31.9 million.
And, because younger people are likely to have more systemic reactions, they cost more to vaccinate. A model that accounted for the cost of the vaccine, administration, and treating local and systemic reactions, put the total price tag at $193 million for those in their 50s, and $190 million for each of the two older groups.
Finally, the number needed to treat to prevent one case of shingles, PHN, or non-PHN complication case was higher in those in their 50s than in those in their 60s or 70s (one shingles case – 51, 38, and 47 respectively; one PHN case – 988, 247, and 124).
"This isn’t intended to tell people not to get the vaccine early, but to make them aware of the risks and benefits, given that the greatest risk of the disease is later in life," Dr. Duchin said. Since there are no data on booster shingles vaccines, he said "we only have one shot at this and we need to focus our efforts on those at the greatest risk."
Because efficacy of the shingles vaccine appears to wane over time, it should not routinely be given to people in their 50s, according to information presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
"At this time, there is insufficient evidence supporting long-term protection of the vaccine, so if people younger than 60 [years] are vaccinated, they might not be protected when chance of disease is highest," said Dr. Jeff Duchin, chair of the ACIP’s herpes zoster working group. "We will continue to monitor data as they becomes available, but at this point we are reaffirming that vaccination be done in those age 60 [years] and older."
The committee made its recommendation after reviewing newly released data from Merck’s Long-Term Persistence Study for shingles. It found that, 10 years after vaccination, the overall incidence rate of shingles had increased from about 4/1,000 person-years to 11/1,000 person-years. The observed incidence rate of shingles in historical controls is about 13 cases/1,000 person-years.
Dr. Janie Parrino, director of vaccine clinical research at Merck Research Laboratories, presented results of the company’s latest study of the vaccine’s extended efficacy. The shingles Long-Term Persistence Study is an 8-year follow-up of the Shingles Prevention Study, in which subjects were randomized to Merck’s Zostavax vaccine or placebo. It showed that the vaccine significantly reduced the incidence of herpes zoster and postherpetic neuralgia (PHN) as well as the shingles burden of illness, in adults older than 60 years.
A short-term follow-up study appeared last year; it added 4 more years of follow-up data on more than 14,000 of the original cohort.
It found a gradual decrease in vaccine efficacy by 6-7 years after vaccination. "Analysis of vaccine efficacy in each year after vaccination for all outcomes showed a decrease after year 1, with a further decline thereafter," the investigators said. "Vaccine efficacy was statistically significant for the incidence of herpes zoster and herpes zoster burden of illness through year 5 after vaccination, but vaccine efficacy is uncertain beyond that point."
The long-term study presented at the Atlanta meeting involved up to 12 years of data on almost 7,000 people in the original cohort. It demonstrated a continuous time-bound waning of efficacy.
In addition to the increasing annual incidence of shingles, the study found an increasing incidence of PHN, from less than 1/1,000 person-years during the year of vaccination to about 1/1,000 person years by year 10. However, the incidence among placebo subjects and historical controls was more than 2/1,000 person years by that time. The shingles burden of illness (a measure of acute pain) also increased as time passed, Dr. Parrino noted.
Taking into account both clinical efficacy and cost, Ismael Ortega-Sanchez, Ph.D., a health economist with the CDC, concluded that the shingles vaccine is most effective when given to people in their 60s and 70s.
Vaccinating from age 50-59 years would prevent about 20,000 shingles cases annually. But vaccinating in the 60s would prevent 26,000 and, in the 70s, 21,000. The trend was similar for cases of PHN: prevention of 1,000 cases for vaccinating in the 50s, 4,000 for vaccinating in the 60s, and 8,000 for vaccinating in the 70s.
Other outcomes – emergency visits, ambulatory visits, hospitalizations, length of hospital stay, and prescriptions – also increased significantly over the 3 decades.
Savings tracked clinical outcomes in a value assessment model of 6 million people: 1 million vaccinated and unvaccinated in each of the three age cohorts.
Compared with not vaccinating, vaccinating those in their 50s would save $16.8 million annually. Vaccinating during the 60s would save about $24.3 million, and during the 70s, $31.9 million.
And, because younger people are likely to have more systemic reactions, they cost more to vaccinate. A model that accounted for the cost of the vaccine, administration, and treating local and systemic reactions, put the total price tag at $193 million for those in their 50s, and $190 million for each of the two older groups.
Finally, the number needed to treat to prevent one case of shingles, PHN, or non-PHN complication case was higher in those in their 50s than in those in their 60s or 70s (one shingles case – 51, 38, and 47 respectively; one PHN case – 988, 247, and 124).
"This isn’t intended to tell people not to get the vaccine early, but to make them aware of the risks and benefits, given that the greatest risk of the disease is later in life," Dr. Duchin said. Since there are no data on booster shingles vaccines, he said "we only have one shot at this and we need to focus our efforts on those at the greatest risk."
FROM ACIP

Single Dose of HPV16/18 Vaccine Appears Immunogenic
Even a single dose of the human papillomavirus 16/18 virus-like particle vaccine appears to be immunogenic for at least 4 years, inducing an antibody response only slightly lower than that from two or the recommended three doses, according to a report in the November issue of Cancer Prevention Research.
Geometric mean titers (GMTs) of HPV antibodies persisted at a plateau level from 6 months after vaccination until the conclusion of this 4-year study, regardless of whether the female participants received one, two, or three doses of the vaccine. In all cases, the GMTs were higher than those induced from natural HPV infection, said Dr. Mahboobeh Safaeian of the division of cancer epidemiology and genetics, National Cancer Institute, Bethesda, Md., and her associates.
These findings that long-term protection may not require the fivefold higher antibody titers induced by three doses of the vaccine may have important implications for HPV virus-like particle (VLP) vaccine programs. Fewer doses would be less expensive and much easier to deliver, particularly in the developing world where more than 85% of cervical cancers occur and where they are the primary cause of cancer-related death in women, the investigators said.
Dr. Safaeian and her colleagues evaluated the immunogenicity of the HPV16/18 VLP vaccine by studying women who participated in the Costa Rica Vaccine Trial. In this publicly funded, community-based phase III study, 7,466 women were randomly assigned to receive either the HPV or the hepatitis A vaccine (control group). Approximately 20% of the study population received fewer than the recommended three doses of each vaccine.
For their study, Dr. Safaeian and her associates assessed serum samples from 78 women who received one HPV vaccine dose, 140 who received one dose at baseline and a second dose 1 month later, 52 who received one dose at baseline and a second dose 6 months later, and 120 who received all three doses. For comparison, they also assessed serum samples from 113 women who were seropositive for HPV 16 or 18 at baseline from naturally occurring infection.
Almost all of the study subjects in all the dose groups were seropositive for HPV antibodies at 1 month after the first dose, "indicating that all groups had similar intrinsic ability to respond to the vaccine," the investigators wrote (Cancer Prev. Res. 2013 November [doi:10.1158/1940-6207.CAPR-13-0203]).
Antibody GMTs were stable in all dose groups from 6 months post vaccination throughout the remainder of the 4-year follow-up. HPV antibody levels at 1 year were strongly predictive of what those levels would be at 3 and 4 years across all dose groups.
Among women who only received a single dose of the HPV16/18 vaccine, 54% had HPV16 antibody levels and 81% had HPV18 antibody levels comparable with those in women who received all three doses. "Our study is the first to show that even a single HPV16/18 vaccine dose induces an antibody response that was readily detected in all vaccinated women at the end of 4-year follow-up, although the titers were lower than after 2 or 3 doses," Dr. Safaeian and her associates said.
"Coupled with our previous demonstration that a single vaccine dose of [HPV vaccine] induced strong protection in the Costa Rica Vaccine Trial, these findings suggest that antibody titers induced by two or three vaccine doses may be substantially higher than needed for long-term protection," they added.
HPV16 antibody levels were 24 times higher and HPV18 antibody levels were 14 times higher among women who received two doses of the vaccine than among women who had been infected naturally. HPV16 antibody levels were nine times higher and HPV18 antibody levels were five times higher among women who only received one dose of the vaccine than among those who had already been infected naturally.
This study was supported by the National Cancer Institute, the National Institutes of Health Office of Research on Women’s Health, and the Ministry of Health of Costa Rica. GlaxoSmithKline provided the vaccine and support for other aspects of the trial. Dr. Safaeian’s associates reported ties to GlaxoSmithKline, Merck, and DDl Diagnostic Laboratory.
Even a single dose of the human papillomavirus 16/18 virus-like particle vaccine appears to be immunogenic for at least 4 years, inducing an antibody response only slightly lower than that from two or the recommended three doses, according to a report in the November issue of Cancer Prevention Research.
Geometric mean titers (GMTs) of HPV antibodies persisted at a plateau level from 6 months after vaccination until the conclusion of this 4-year study, regardless of whether the female participants received one, two, or three doses of the vaccine. In all cases, the GMTs were higher than those induced from natural HPV infection, said Dr. Mahboobeh Safaeian of the division of cancer epidemiology and genetics, National Cancer Institute, Bethesda, Md., and her associates.
These findings that long-term protection may not require the fivefold higher antibody titers induced by three doses of the vaccine may have important implications for HPV virus-like particle (VLP) vaccine programs. Fewer doses would be less expensive and much easier to deliver, particularly in the developing world where more than 85% of cervical cancers occur and where they are the primary cause of cancer-related death in women, the investigators said.
Dr. Safaeian and her colleagues evaluated the immunogenicity of the HPV16/18 VLP vaccine by studying women who participated in the Costa Rica Vaccine Trial. In this publicly funded, community-based phase III study, 7,466 women were randomly assigned to receive either the HPV or the hepatitis A vaccine (control group). Approximately 20% of the study population received fewer than the recommended three doses of each vaccine.
For their study, Dr. Safaeian and her associates assessed serum samples from 78 women who received one HPV vaccine dose, 140 who received one dose at baseline and a second dose 1 month later, 52 who received one dose at baseline and a second dose 6 months later, and 120 who received all three doses. For comparison, they also assessed serum samples from 113 women who were seropositive for HPV 16 or 18 at baseline from naturally occurring infection.
Almost all of the study subjects in all the dose groups were seropositive for HPV antibodies at 1 month after the first dose, "indicating that all groups had similar intrinsic ability to respond to the vaccine," the investigators wrote (Cancer Prev. Res. 2013 November [doi:10.1158/1940-6207.CAPR-13-0203]).
Antibody GMTs were stable in all dose groups from 6 months post vaccination throughout the remainder of the 4-year follow-up. HPV antibody levels at 1 year were strongly predictive of what those levels would be at 3 and 4 years across all dose groups.
Among women who only received a single dose of the HPV16/18 vaccine, 54% had HPV16 antibody levels and 81% had HPV18 antibody levels comparable with those in women who received all three doses. "Our study is the first to show that even a single HPV16/18 vaccine dose induces an antibody response that was readily detected in all vaccinated women at the end of 4-year follow-up, although the titers were lower than after 2 or 3 doses," Dr. Safaeian and her associates said.
"Coupled with our previous demonstration that a single vaccine dose of [HPV vaccine] induced strong protection in the Costa Rica Vaccine Trial, these findings suggest that antibody titers induced by two or three vaccine doses may be substantially higher than needed for long-term protection," they added.
HPV16 antibody levels were 24 times higher and HPV18 antibody levels were 14 times higher among women who received two doses of the vaccine than among women who had been infected naturally. HPV16 antibody levels were nine times higher and HPV18 antibody levels were five times higher among women who only received one dose of the vaccine than among those who had already been infected naturally.
This study was supported by the National Cancer Institute, the National Institutes of Health Office of Research on Women’s Health, and the Ministry of Health of Costa Rica. GlaxoSmithKline provided the vaccine and support for other aspects of the trial. Dr. Safaeian’s associates reported ties to GlaxoSmithKline, Merck, and DDl Diagnostic Laboratory.
Even a single dose of the human papillomavirus 16/18 virus-like particle vaccine appears to be immunogenic for at least 4 years, inducing an antibody response only slightly lower than that from two or the recommended three doses, according to a report in the November issue of Cancer Prevention Research.
Geometric mean titers (GMTs) of HPV antibodies persisted at a plateau level from 6 months after vaccination until the conclusion of this 4-year study, regardless of whether the female participants received one, two, or three doses of the vaccine. In all cases, the GMTs were higher than those induced from natural HPV infection, said Dr. Mahboobeh Safaeian of the division of cancer epidemiology and genetics, National Cancer Institute, Bethesda, Md., and her associates.
These findings that long-term protection may not require the fivefold higher antibody titers induced by three doses of the vaccine may have important implications for HPV virus-like particle (VLP) vaccine programs. Fewer doses would be less expensive and much easier to deliver, particularly in the developing world where more than 85% of cervical cancers occur and where they are the primary cause of cancer-related death in women, the investigators said.
Dr. Safaeian and her colleagues evaluated the immunogenicity of the HPV16/18 VLP vaccine by studying women who participated in the Costa Rica Vaccine Trial. In this publicly funded, community-based phase III study, 7,466 women were randomly assigned to receive either the HPV or the hepatitis A vaccine (control group). Approximately 20% of the study population received fewer than the recommended three doses of each vaccine.
For their study, Dr. Safaeian and her associates assessed serum samples from 78 women who received one HPV vaccine dose, 140 who received one dose at baseline and a second dose 1 month later, 52 who received one dose at baseline and a second dose 6 months later, and 120 who received all three doses. For comparison, they also assessed serum samples from 113 women who were seropositive for HPV 16 or 18 at baseline from naturally occurring infection.
Almost all of the study subjects in all the dose groups were seropositive for HPV antibodies at 1 month after the first dose, "indicating that all groups had similar intrinsic ability to respond to the vaccine," the investigators wrote (Cancer Prev. Res. 2013 November [doi:10.1158/1940-6207.CAPR-13-0203]).
Antibody GMTs were stable in all dose groups from 6 months post vaccination throughout the remainder of the 4-year follow-up. HPV antibody levels at 1 year were strongly predictive of what those levels would be at 3 and 4 years across all dose groups.
Among women who only received a single dose of the HPV16/18 vaccine, 54% had HPV16 antibody levels and 81% had HPV18 antibody levels comparable with those in women who received all three doses. "Our study is the first to show that even a single HPV16/18 vaccine dose induces an antibody response that was readily detected in all vaccinated women at the end of 4-year follow-up, although the titers were lower than after 2 or 3 doses," Dr. Safaeian and her associates said.
"Coupled with our previous demonstration that a single vaccine dose of [HPV vaccine] induced strong protection in the Costa Rica Vaccine Trial, these findings suggest that antibody titers induced by two or three vaccine doses may be substantially higher than needed for long-term protection," they added.
HPV16 antibody levels were 24 times higher and HPV18 antibody levels were 14 times higher among women who received two doses of the vaccine than among women who had been infected naturally. HPV16 antibody levels were nine times higher and HPV18 antibody levels were five times higher among women who only received one dose of the vaccine than among those who had already been infected naturally.
This study was supported by the National Cancer Institute, the National Institutes of Health Office of Research on Women’s Health, and the Ministry of Health of Costa Rica. GlaxoSmithKline provided the vaccine and support for other aspects of the trial. Dr. Safaeian’s associates reported ties to GlaxoSmithKline, Merck, and DDl Diagnostic Laboratory.
FROM CANCER PREVENTION RESEARCH

How to Manage Anemia From HCV Treatment
The results of a randomized, open-label study suggest that reducing the ribavirin dose should be the "primary approach" for managing anemia associated with peginterferon, ribavirin, and boceprevir therapy in patients with chronic hepatitis C, the authors of the study concluded.
In the study, the effects of two anemia-management strategies, ribavirin (RBV) dose reduction and erythropoietin (EPO) treatment, on the sustained virologic response (SVR) were similar – there was less than 1% difference between the two groups, according to the investigators, Dr. Fred F. Poordad of the Texas Liver Institute, at the University of Texas Health Science Center, San Antonio, and his associates. They also found that SVR rates were significantly lower among those who received less than half of the total ribavirin dose during the entire treatment period, compared with those who received a greater proportion of the total dosage.
"There appears to be no apparent benefit of using EPO as a first-line anemia-management strategy to enhance SVR rate or minimize relapse," the authors concluded. "EPO can be used as a secondary management strategy to prevent treatment interruption if RBV dosage reduction alone is inadequate, but the safety of EPO use in this setting has not been clearly established," they added. The study was published in the November issue of Gastroenterology (2013 [doi:10.1053/j.gastro.2013.07.051]).
The study includes an algorithm for managing boceprevir-related anemia, based on the results of this and other clinical studies, and the authors’ expertise.
See the full algorithm here.
The study, conducted between December 2009 and October 2011, compared the two regimens in 500 of 687 previously untreated patients with chronic HCV genotype-1 infections, who became anemic (hemoglobin levels dropping to 10 g/dL or lower) during treatment with the three drugs: peginterferon alfa-2b (PegIntron) at a dose of 1.5 mcg/kg per week; ribavirin at a dose of 600-1400 mg per day depending on weight; and boceprevir (Victrelis) at a dose of 800 mg three times a day. (After 4 weeks of treatment with peginterferon and RBV, boceprevir was added for 24 or 44 weeks). Their mean age was about 50 years, 33% were men, 77% were white, and 18% were black; 91% had a baseline viral load of more than 400,000 IU/mL. Almost 90% were in the United States, the rest were in Canada and Europe.
The 500 patients were randomized to treatment with EPO (a subcutaneous infusion of 40,000 IU a week) or a reduction in the ribavirin dose (200 mg/day or, for those on the 1,400 mg daily dose, a 400-mg reduction). If hemoglobin levels dropped to 7.5 g/dL or lower, the patients were dropped from the study.
The SVR rate (undetectable HCV RNA 24 weeks after the end of treatment) was 71.5% among those whose ribavirin dosage was reduced and 70.9% among those treated with EPO. Among the 187 patients who did not develop anemia, the SVR rate was 40.1%; this group included a large number of patients who discontinued treatment because of adverse events. But of the 64 who completed treatment, the SVR rate was 89%. The overall SVR rate – among all 687 patients, those randomized and not randomized – was 63%.
Common adverse events were similar in the two randomized treatment groups, with anemia, fatigue, nausea, and headache being the most commonly reported. The rates of serious adverse events were 16% among those in the RBV dose-reduction arm and 13% of those on EPO. There were more thromboembolic events among the patients treated with EPO. There was one death in a patient in the RBV arm, a sudden cardiac death 3 weeks after stopping treatment.
The algorithm proposed by the authors, which has different hemoglobin monitoring recommendations for those with and without advanced fibrosis and cirrhosis, recommends that the primary intervention for managing anemia should be to reduce the RBV dosage. But if hemoglobin levels remain below 10 g/dL, "secondary interventions, such as administration of EPO, red cell transfusions, and reducing the dosage of peginterferon can be considered," the authors wrote. In addition, "it is important that the patient receives at least 50% of the total milligrams of RBV calculated from the initial RBV dosage (mg/d) and the assigned duration" defined by the response-guided therapy algorithm, they added.
The open-label design was one of the study’s limitations, and whether these results apply to other HCV treatment regimens is unclear, the authors noted. However, the results "would most likely be applicable to all RBV- and peginterferon/RBV-based regimens" for hepatitis C, they added.
The study was funded by Schering-Plough, the manufacturer of PegIntron and combination packs of PegIntron with ribavirin, which is now part of Merck. The investigator disclosures included having served as consultants and speakers, and/or having received grants from multiple pharmaceutical companies; the investigators include several current and former employees of Merck Sharp & Dohme Corp. (a subsidiary of Merck & Co.), the manufacturer of Victrelis.
The results of a randomized, open-label study suggest that reducing the ribavirin dose should be the "primary approach" for managing anemia associated with peginterferon, ribavirin, and boceprevir therapy in patients with chronic hepatitis C, the authors of the study concluded.
In the study, the effects of two anemia-management strategies, ribavirin (RBV) dose reduction and erythropoietin (EPO) treatment, on the sustained virologic response (SVR) were similar – there was less than 1% difference between the two groups, according to the investigators, Dr. Fred F. Poordad of the Texas Liver Institute, at the University of Texas Health Science Center, San Antonio, and his associates. They also found that SVR rates were significantly lower among those who received less than half of the total ribavirin dose during the entire treatment period, compared with those who received a greater proportion of the total dosage.
"There appears to be no apparent benefit of using EPO as a first-line anemia-management strategy to enhance SVR rate or minimize relapse," the authors concluded. "EPO can be used as a secondary management strategy to prevent treatment interruption if RBV dosage reduction alone is inadequate, but the safety of EPO use in this setting has not been clearly established," they added. The study was published in the November issue of Gastroenterology (2013 [doi:10.1053/j.gastro.2013.07.051]).
The study includes an algorithm for managing boceprevir-related anemia, based on the results of this and other clinical studies, and the authors’ expertise.
See the full algorithm here.
The study, conducted between December 2009 and October 2011, compared the two regimens in 500 of 687 previously untreated patients with chronic HCV genotype-1 infections, who became anemic (hemoglobin levels dropping to 10 g/dL or lower) during treatment with the three drugs: peginterferon alfa-2b (PegIntron) at a dose of 1.5 mcg/kg per week; ribavirin at a dose of 600-1400 mg per day depending on weight; and boceprevir (Victrelis) at a dose of 800 mg three times a day. (After 4 weeks of treatment with peginterferon and RBV, boceprevir was added for 24 or 44 weeks). Their mean age was about 50 years, 33% were men, 77% were white, and 18% were black; 91% had a baseline viral load of more than 400,000 IU/mL. Almost 90% were in the United States, the rest were in Canada and Europe.
The 500 patients were randomized to treatment with EPO (a subcutaneous infusion of 40,000 IU a week) or a reduction in the ribavirin dose (200 mg/day or, for those on the 1,400 mg daily dose, a 400-mg reduction). If hemoglobin levels dropped to 7.5 g/dL or lower, the patients were dropped from the study.
The SVR rate (undetectable HCV RNA 24 weeks after the end of treatment) was 71.5% among those whose ribavirin dosage was reduced and 70.9% among those treated with EPO. Among the 187 patients who did not develop anemia, the SVR rate was 40.1%; this group included a large number of patients who discontinued treatment because of adverse events. But of the 64 who completed treatment, the SVR rate was 89%. The overall SVR rate – among all 687 patients, those randomized and not randomized – was 63%.
Common adverse events were similar in the two randomized treatment groups, with anemia, fatigue, nausea, and headache being the most commonly reported. The rates of serious adverse events were 16% among those in the RBV dose-reduction arm and 13% of those on EPO. There were more thromboembolic events among the patients treated with EPO. There was one death in a patient in the RBV arm, a sudden cardiac death 3 weeks after stopping treatment.
The algorithm proposed by the authors, which has different hemoglobin monitoring recommendations for those with and without advanced fibrosis and cirrhosis, recommends that the primary intervention for managing anemia should be to reduce the RBV dosage. But if hemoglobin levels remain below 10 g/dL, "secondary interventions, such as administration of EPO, red cell transfusions, and reducing the dosage of peginterferon can be considered," the authors wrote. In addition, "it is important that the patient receives at least 50% of the total milligrams of RBV calculated from the initial RBV dosage (mg/d) and the assigned duration" defined by the response-guided therapy algorithm, they added.
The open-label design was one of the study’s limitations, and whether these results apply to other HCV treatment regimens is unclear, the authors noted. However, the results "would most likely be applicable to all RBV- and peginterferon/RBV-based regimens" for hepatitis C, they added.
The study was funded by Schering-Plough, the manufacturer of PegIntron and combination packs of PegIntron with ribavirin, which is now part of Merck. The investigator disclosures included having served as consultants and speakers, and/or having received grants from multiple pharmaceutical companies; the investigators include several current and former employees of Merck Sharp & Dohme Corp. (a subsidiary of Merck & Co.), the manufacturer of Victrelis.
The results of a randomized, open-label study suggest that reducing the ribavirin dose should be the "primary approach" for managing anemia associated with peginterferon, ribavirin, and boceprevir therapy in patients with chronic hepatitis C, the authors of the study concluded.
In the study, the effects of two anemia-management strategies, ribavirin (RBV) dose reduction and erythropoietin (EPO) treatment, on the sustained virologic response (SVR) were similar – there was less than 1% difference between the two groups, according to the investigators, Dr. Fred F. Poordad of the Texas Liver Institute, at the University of Texas Health Science Center, San Antonio, and his associates. They also found that SVR rates were significantly lower among those who received less than half of the total ribavirin dose during the entire treatment period, compared with those who received a greater proportion of the total dosage.
"There appears to be no apparent benefit of using EPO as a first-line anemia-management strategy to enhance SVR rate or minimize relapse," the authors concluded. "EPO can be used as a secondary management strategy to prevent treatment interruption if RBV dosage reduction alone is inadequate, but the safety of EPO use in this setting has not been clearly established," they added. The study was published in the November issue of Gastroenterology (2013 [doi:10.1053/j.gastro.2013.07.051]).
The study includes an algorithm for managing boceprevir-related anemia, based on the results of this and other clinical studies, and the authors’ expertise.
See the full algorithm here.
The study, conducted between December 2009 and October 2011, compared the two regimens in 500 of 687 previously untreated patients with chronic HCV genotype-1 infections, who became anemic (hemoglobin levels dropping to 10 g/dL or lower) during treatment with the three drugs: peginterferon alfa-2b (PegIntron) at a dose of 1.5 mcg/kg per week; ribavirin at a dose of 600-1400 mg per day depending on weight; and boceprevir (Victrelis) at a dose of 800 mg three times a day. (After 4 weeks of treatment with peginterferon and RBV, boceprevir was added for 24 or 44 weeks). Their mean age was about 50 years, 33% were men, 77% were white, and 18% were black; 91% had a baseline viral load of more than 400,000 IU/mL. Almost 90% were in the United States, the rest were in Canada and Europe.
The 500 patients were randomized to treatment with EPO (a subcutaneous infusion of 40,000 IU a week) or a reduction in the ribavirin dose (200 mg/day or, for those on the 1,400 mg daily dose, a 400-mg reduction). If hemoglobin levels dropped to 7.5 g/dL or lower, the patients were dropped from the study.
The SVR rate (undetectable HCV RNA 24 weeks after the end of treatment) was 71.5% among those whose ribavirin dosage was reduced and 70.9% among those treated with EPO. Among the 187 patients who did not develop anemia, the SVR rate was 40.1%; this group included a large number of patients who discontinued treatment because of adverse events. But of the 64 who completed treatment, the SVR rate was 89%. The overall SVR rate – among all 687 patients, those randomized and not randomized – was 63%.
Common adverse events were similar in the two randomized treatment groups, with anemia, fatigue, nausea, and headache being the most commonly reported. The rates of serious adverse events were 16% among those in the RBV dose-reduction arm and 13% of those on EPO. There were more thromboembolic events among the patients treated with EPO. There was one death in a patient in the RBV arm, a sudden cardiac death 3 weeks after stopping treatment.
The algorithm proposed by the authors, which has different hemoglobin monitoring recommendations for those with and without advanced fibrosis and cirrhosis, recommends that the primary intervention for managing anemia should be to reduce the RBV dosage. But if hemoglobin levels remain below 10 g/dL, "secondary interventions, such as administration of EPO, red cell transfusions, and reducing the dosage of peginterferon can be considered," the authors wrote. In addition, "it is important that the patient receives at least 50% of the total milligrams of RBV calculated from the initial RBV dosage (mg/d) and the assigned duration" defined by the response-guided therapy algorithm, they added.
The open-label design was one of the study’s limitations, and whether these results apply to other HCV treatment regimens is unclear, the authors noted. However, the results "would most likely be applicable to all RBV- and peginterferon/RBV-based regimens" for hepatitis C, they added.
The study was funded by Schering-Plough, the manufacturer of PegIntron and combination packs of PegIntron with ribavirin, which is now part of Merck. The investigator disclosures included having served as consultants and speakers, and/or having received grants from multiple pharmaceutical companies; the investigators include several current and former employees of Merck Sharp & Dohme Corp. (a subsidiary of Merck & Co.), the manufacturer of Victrelis.
FROM GASTROENTEROLOGY

Myasthenia gravis: Newer therapies offer sustained improvement
Current therapies for myasthenia gravis can help most patients achieve sustained improvement. The overall prognosis has dramatically improved over the last 4 decades: the mortality rate used to be 75%; now it is 4.5%.1
Myasthenia gravis is the most common disorder of neuromuscular junction transmission and is also one of the best characterized autoimmune diseases. However, its symptoms—primarily weakness—vary from patient to patient, and in the same patient, by time of day and over longer time periods. The variation in symptoms can be very confusing to undiagnosed patients and puzzling to unsuspecting physicians. Such diagnostic uncertainty can give the patient additional frustration and emotional stress, which in turn exacerbate his or her condition.
In this review, we will give an overview of the pathogenesis, clinical manifestations, diagnosis, and treatment of myasthenia gravis.
TWO PEAKS IN INCIDENCE BY AGE
The annual incidence of myasthenia gravis is approximately 10 to 20 new cases per million, with a prevalence of about 150 to 200 per million.2
The age of onset has a bimodal distribution, with an early incidence peak in the second to third decade with a female predominance and a late peak in the 6th to the 8th decade with a male predominance.2
Myasthenia gravis is commonly associated with several other autoimmune disorders, including hypothyroidism, hyperthyroidism, systemic lupus erythematosus, rheumatoid arthritis, vitiligo, diabetes, and, more recently recognized, neuromyelitis optica.3
ANTIBODIES AGAINST AChR AND MuSK
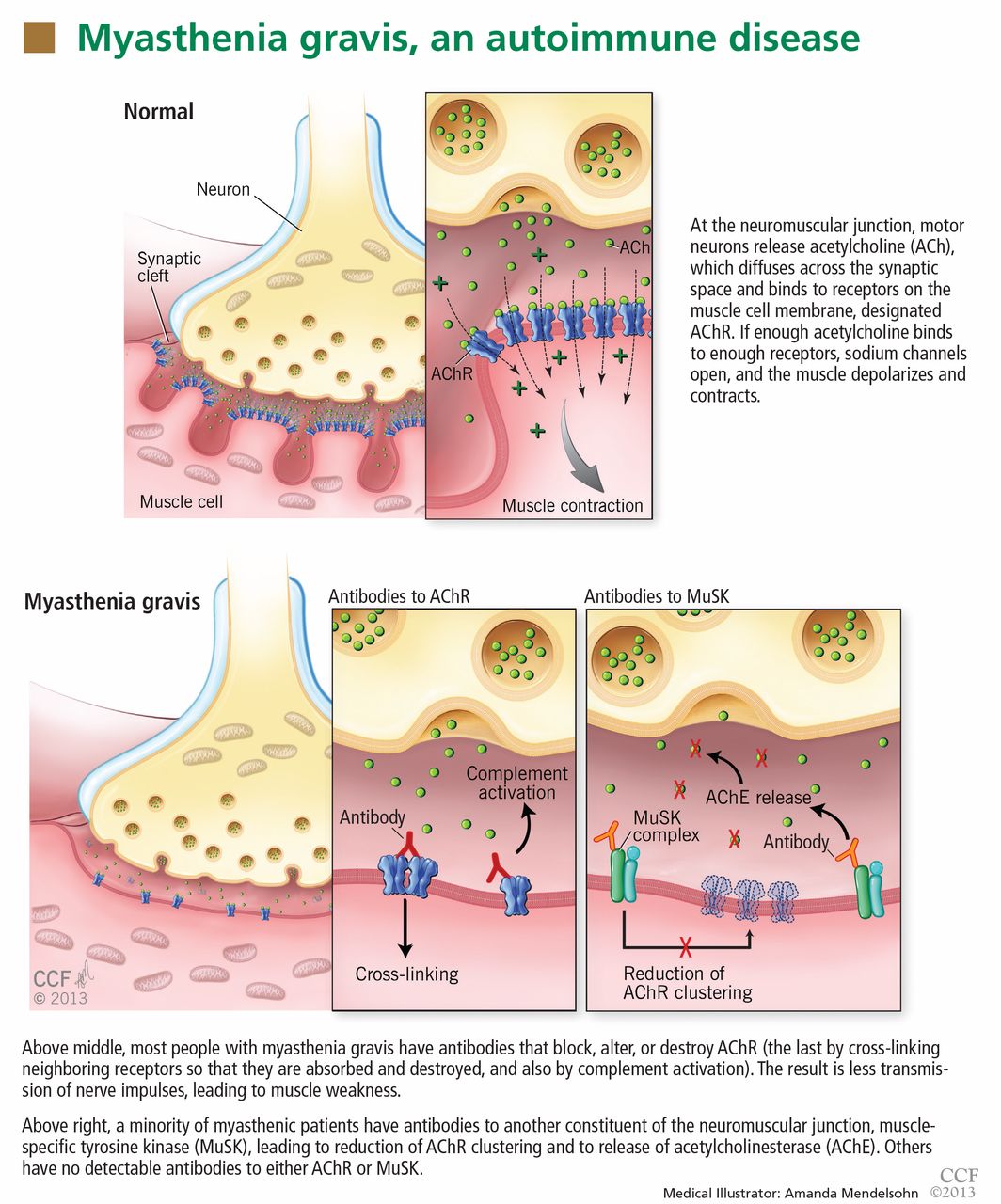
In most cases of myasthenia gravis the patient has autoimmune antibodies against constituents of the neuromuscular junction, specifically acetylcholine receptor (AChR) and muscle-specific tyrosine kinase (MuSK) (Figure 1).
AChR antibody-positive myasthenia gravis
When antibodies bind to AChR on the postsynaptic membrane, they cross-link neighboring AChR units, which are absorbed into the muscle fiber and are broken up.4 In addition, the complement system is activated to mediate further damage on the postsynaptic membrane.
AChR antibodies may come from germinal centers of the thymus, where clustered myoid cells express AChR on the plasma membrane surface.5 About 60% of AChR antibody-positive myasthenia gravis patients have an enlarged thymus, and 10% have a thymoma—a tumor of the epithelial cells of this organ. Conversely, about 15% of patients with a thymoma have clinical myasthenia gravis, and an additional 20% possess antibodies against AChR in the serum without myasthenic symptoms.5
MuSK antibody-positive myasthenia gravis
Like AChR, MuSK is a transmembrane component of the postsynaptic neuromuscular junction. During formation of the neuromuscular junction, MuSK is activated through the binding of agrin (a nerve-derived proteoglycan) to lipoprotein-related protein 4 (LRP4), after which complicated intracellular signaling promotes the assembly and stabilization of AChR.6
Unlike AChR antibodies, antibodies against MuSK do not activate the complement system, and complement fixation is not essential for clinical myasthenic symptoms to appear.7 Also, myasthenia gravis with MuSK antibodies is rarely associated with thymoma.8
The precise mechanism by which MuSK antibody impairs transmission at the neuromuscular junction has been a mystery until recently. Animal models, including MuSK-mutant mice and mice injected with MuSK protein or with purified immunoglobulin G from patients with this disease, have revealed a significant reduction of AChR clusters and destruction of neuromuscular junction structures.7,9–12
In addition, MuSK antibodies produce pre-synaptic dysfunction, manifesting as a reduction of acetylcholine content. This information is based on studies in mice and on in vitro electrophysiologic analyses of neuromuscular junctions from a patient with this disease.7,9–13
Finally, MuSK antibodies may indirectly affect the recycling of acetylcholine. After post-synaptic activation, acetylcholine is normally hydrolized by acetylcholinesterase, which is located in the synaptic cleft but anchored to MuSK on the postsynaptic membrane. MuSK antibodies block the binding of MuSK to acetylcholinesterase, possibly leading to less accumulation of acetylcholinesterase.14 This process may explain why patients with MuSK antibody-positive myasthenia gravis tend to respond poorly to acetylcholinesterase inhibitors (more about this below).
Seronegative myasthenia gravis
In a series of 562 consecutive patients with generalized weakness due to myasthenia gravis, 92% were positive for AChR antibody, 3% were positive for MuSK antibody, and 5% were seronegative (possessing neither antibody).15 In contrast, about 50% of patients with purely ocular myasthenia gravis (ie, with isolated weakness of the levator palpebrae superioris, orbicularis oculi, or oculomotor muscles) are seropositive for AChR antibody. Only a few ocular MuSK antibody-positive cases have been described, leaving the rest seronegative. Rarely, both antibodies can be detected in the same patient.16
In patients who are negative for AChR antibodies at the time of disease onset, sero-conversion may occur later during the course. Repeating serologic testing 6 to 12 months later may detect AChR antibodies in approximately 15% of patients who were initially seronegative.15,17
The clinical presentation, electrophysiologic findings, thymic pathologic findings, and treatment responses are similar in AChR antibody-positive and seronegative myasthenia gravis.17 Muscle biopsy study in seronegative cases demonstrates a loss of AChR as well.18
Based on these observations, it has been proposed that seronegative patients may have low-affinity antibodies that can bind to tightly clustered AChRs on the postsynaptic membrane but escape detection by routine radioimmunoassays in a solution phase. With a sensitive cell-based immunofluorescence assay, low-affinity antibodies to clustered AChRs were detected in 66% of patients with generalized myasthenia gravis and in 50% of those with ocular myasthenia gravis who were seronegative on standard assays.19,20 These low-affinity AChR antibodies can also activate complement in vitro, increasing the likelihood that they are pathogenic. However, assays to detect low-affinity AChR antibodies are not yet commercially available.
Within the past year, three research groups independently reported detecting antibodies to LRP4 in 2% to 50% of seronegative myasthenia gravis patients. This wide variation in the prevalence of LRP4 antibodies could be related to patient ethnicity and methods of detection.21–23 LRP4 is a receptor for agrin and is required for agrin-induced MuSK activation and AChR clustering. LRP antibodies can activate complement; therefore, it is plausible that LRP4 antibody binding leads to AChR loss on the postsynaptic membrane. However, additional study is needed to determine if LRP4 antibodies are truly pathogenic in myasthenia gravis.
A DISORDER OF FATIGABLE WEAKNESS
Myasthenia gravis is a disorder of fatigable weakness producing fluctuating symptoms. Symptoms related to the involvement of specific muscle groups are listed in Table 1. Muscle weakness is often worse later in the day or after exercise.
Ocular myasthenia gravis accounts for about 15% of all cases. Of patients initially presenting with ocular symptoms only, twothirds will ultimately develop generalized symptoms, most within the first 2 years.24 No factor has been identified that predicts conversion from an ocular to a generalized form.
Several clinical phenotypes of MuSK antibody-positive myasthenia gravis have been described. An oculobulbar form presents with diplopia, ptosis, dysarthria, and profound atrophy of the muscles of the tongue and face. A restricted myopathic form presents with prominent neck, shoulder, and respiratory weakness without ocular involvement. A third form is a combination of ocular and proximal limb weakness, indistinguishable from AChR antibody-positive disease.25
MuSK antibody-positive patients do not respond as well to acetylcholinesterase inhibitors as AChR antibody-positive patients do. In one study, nearly 70% of MuSK antibody-positive patients demonstrated no response, poor tolerance, or cholinergic hypersensitivity to these agents.25 Fortunately, most MuSK antibody-positive patients have a favorable response to immunosuppressive therapy—sometimes a dramatic improvement after plasmapheresis.8
DIAGNOSIS OF MYASTHENIA GRAVIS
The common differential diagnoses for myasthenia gravis are listed in Table 2.
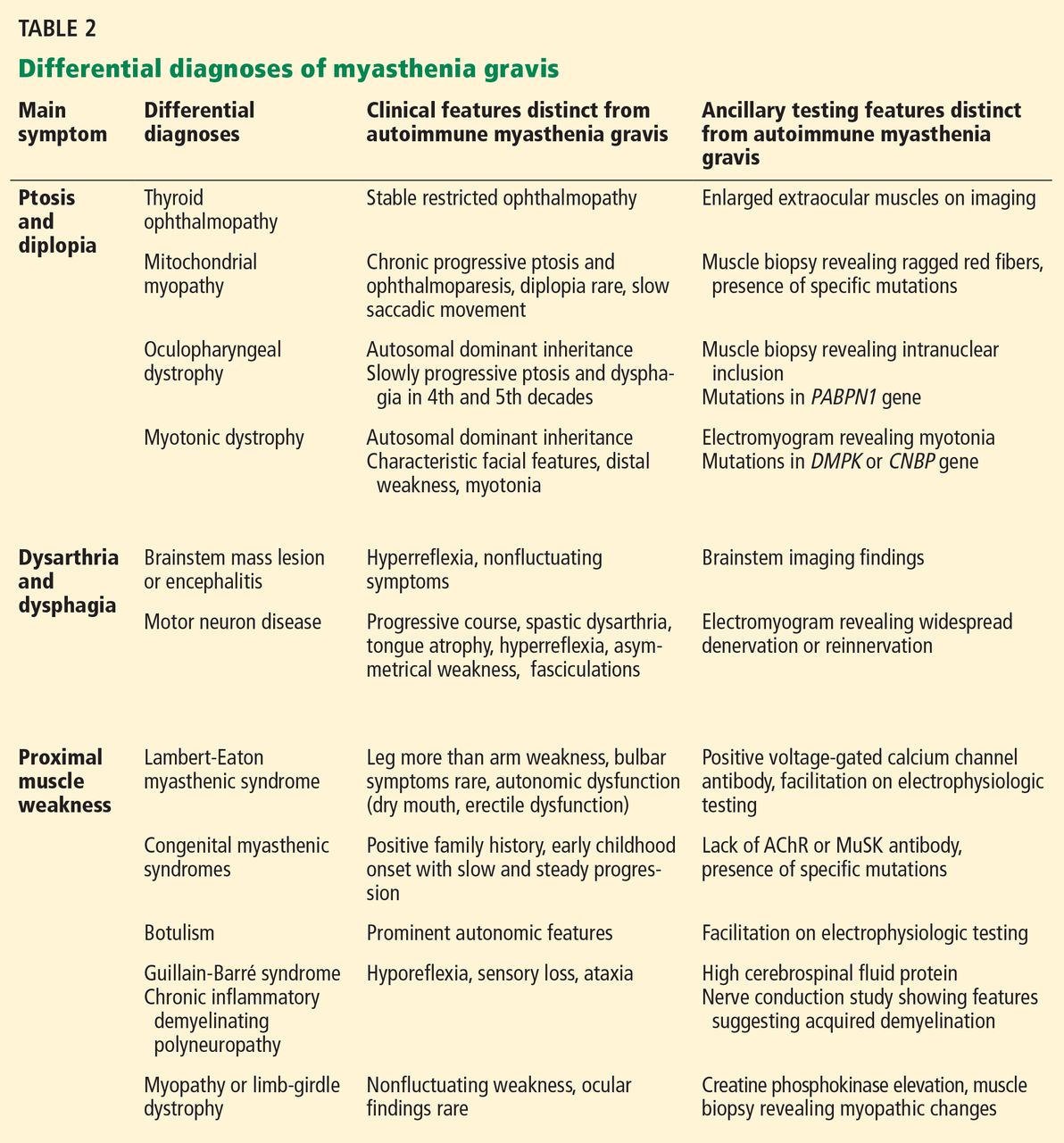
The essential feature of myasthenia gravis is fluctuating muscle weakness, often with fatigue. Many patients complain of weakness of specific muscle groups after their repeated usage. Pain is generally a less conspicuous symptom, and generalized fatigue without objective weakness is inconsistent with myasthenia gravis.
Signs of muscle weakness may include droopy eyelids, diplopia, inability to hold the head straight, difficulty swallowing or chewing, speech disturbances, difficulty breathing, and difficulty raising the arms or rising from the sitting position. A historical pattern of ptosis alternating from one eye to the other is fairly characteristic of myasthenia gravis.
The weakness of orbicularis oculi is easily identified on examination by prying open the eyes during forced eye closure. Limb weakness is usually more significant in the arms than in the legs. An often-neglected feature of myasthenia gravis is finger extensor weakness with a relative sparing of other distal hand muscles.2
The ice-pack test is performed by placing a small bag of ice over the ptotic eye for 2 to 5 minutes and assessing the degree of ptosis for any noticeable improvement. This test is not very helpful for assessing ocular motor weakness.
The edrophonium (Tensilon) test can be used for patients with ptosis or ophthalmoparesis. Edrophonium, a short-acting acetylcholinesterase inhibitor, is given intravenously while the patient is observed for objective improvement. The patient’s cardiovascular status should be monitored for arrhythmias and hypotension. Atropine should be immediately available in case severe bradycardia develops.
The ice-pack test and the edrophonium test can give false-negative and false-positive results, and the diagnosis of myasthenia gravis must be verified by other diagnostic tests.
Testing for antibodies
Testing for circulating AChR antibodies, MuSK antibodies, or both is the first step in the laboratory confirmation of myasthenia gravis.
There are three AChR antibody subtypes: binding, blocking, and modulating. Binding antibodies are present in 80% to 90% of patients with generalized myasthenia gravis and 50% of those with ocular myasthenia gravis. Testing for blocking and modulating AChR antibodies increases the sensitivity by less than 5% when added to testing for binding antibodies.
AChR antibody titers correlate poorly with disease severity between patients. However, in individual patients, antibody titers tend to go down in parallel with clinical improvement.
MuSK antibody is detected in nearly half of myasthenia gravis patients with generalized weakness who are negative for AChR antibody.
Electrophysiologic tests
Electrophysiologic tests can usually confirm the diagnosis of seronegative myasthenia gravis. They are also helpful in seropositive patients who have unusual clinical features or a poor response to treatment.
Repetitive nerve stimulation studies use a slow rate (2–5 Hz) of repetitive electrical stimulation. The study is positive if the motor response declines by more than 10%. However, a decremental response is not specific for myasthenia gravis, as it may be seen in other neuromuscular disorders such as motor neuron disease or Lambert-Eaton myasthenic syndrome.
This test is technically easier to do in distal muscles than in proximal muscles, but less sensitive. Therefore, proximal muscles such as the trapezius or facial muscles are usually also sampled to maximize the yield. To further maximize the sensitivity, muscles being tested should be warm, and acetylcholinesterase inhibitors should be withheld for 12 hours before.
Repetitive nerve stimulation studies in distal muscles are positive in approximately 75% of patients with generalized myasthenia gravis and in 30% with ocular myasthenia gravis.26
Single-fiber electromyography is more technically demanding than repetitive nerve stimulation and is less widely available. It is usually performed with a special needle electrode that can simultaneously identify action potentials arising from individual muscle fibers innervated by the same axon.
Variability in time of the second action potential relative to the first is called “jitter.” Abnormal jitter is seen in more than 95% of patients with generalized myasthenia gravis and in 85% to 90% of those with ocular myasthenia gravis.26,27 However, abnormal jitter can also be seen in other neuromuscular diseases such as motor neuron disease or in neuromuscular junctional disorders such as Lambert-Eaton myasthenic syndrome.
Imaging studies
Chest computed tomography or magnetic resonance imaging with contrast should be performed in all myasthenia gravis patients to look for a thymoma.
TREATMENT OF MYASTHENIA GRAVIS
Acetylcholinesterase inhibitors
As a reasonable first therapy in mild cases of myasthenia gravis, acetylcholinesterase inhibitors slow down the degradation of acetylcholine and prolong its effect in the neuromuscular junction, but they are not disease-modifying and their benefits are mild.
Pyridostigmine is the usual choice of acetylcholinesterase inhibitor. Its onset of action is rapid (15 to 30 minutes) and its action lasts for 3 to 4 hours. For most patients, the effective dosage range is 60 mg to 90 mg every 4 to 6 hours. A long-acting form is also available and can be given as a single nighttime dose.
Immunomodulating therapy
Patients who have moderate to severe symptoms require some form of immunomodulating therapy.
Plasmapheresis or intravenous immune globulin is reserved for patients with severe or rapidly worsening disease because their beneficial effects can be seen within the first week of treatment.
Longer-acting immunotherapies (corticosteroids, azathioprine, mycophenolate mofetil and others) have a slower onset of responses but provide sustained benefits. Which drug to use depends on factors such as comorbidity, side effects, and cost.
Drugs to avoid
A number of medications can exacerbate weakness in myasthenia gravis and should be avoided or used with caution. The list is long, but ones that deserve the most attention are penicillamine, interferons, procainamide, quinidine, and antibiotics, including quinolones and aminoglycosides. A more comprehensive list of medications that may exacerbate myasthenia gravis symptoms can be found in a review by Keesey.2
RAPID INDUCTION IMMUNOTHERAPIES : PLASMAPHERESIS, IMMUNE GLOBULIN
Both plasmapheresis and intravenous immune globulin act quickly over days, but in most patients their effects last only a few weeks. Both are used as rescue therapies for myasthenic crises, bridging therapy to slow-acting immunotherapeutic agents, or maintenance treatment for poorly controlled cases.
Several retrospective studies have confirmed the efficacy of plasmapheresis in more than 80% of patients with generalized symptoms.28,29
In a randomized trial in patients with generalized therapies, intravenous immune globulin improved muscle strength in the group of patients with severe symptoms.30 The effective dosage of intravenous immune globulin varies from 1 to 2 g/kg without observed difference between doses.31 Trials comparing the efficacy of intravenous immune globulin and plasmapheresis in acute and severe myasthenia gravis did not reveal a difference in efficacy.32,33 Intravenous immune globulin at a minimal dose of 0.4 g/kg every 3 months has been successfully used as a long-term maintenance monotherapy, and such a role could be expanded to more patients with further studies.34
The choice between plasmapheresis and intravenous immune globulin is often based on the ability of a patient to tolerate each treatment and on the availability of the plasmapheresis procedure. Intravenous immune globulin is easier to administer, is associated with fewer adverse events related to vascular access, and is therefore more appropriate than plasmapheresis in some centers.
CHRONIC MAINTENANCE IMMUNOMODULATING TREATMENT
Corticosteroids
Prednisone, the most commonly used agent, leads to remission or marked improvement in 70% to 80% of patients with ocular or generalized myasthenia gravis.35 It may also reduce the progression of ocular myasthenia gravis to the generalized form.36
The effective dose of prednisone depends on the severity and distribution of symptoms. Some patients may need up to 1.0 mg/kg/day (usually 50 to 80 mg per day). In patients with mild to moderate symptoms, a lower maximal dosage such as 20 to 40 mg per day can be sufficient.
Within 1 to 2 weeks after starting high-dose prednisone, up to 50% of patients may develop a transient deterioration, including possible precipitation of a myasthenic crisis.37 For this reason, high-dose prednisone is commonly started only in hospitalized patients who are also receiving plasmapheresis or intravenous immune globulin. Otherwise, an outpatient dose-escalation protocol can be used to achieve a target dose over several weeks.
Prednisone tapering can begin after the patient has been on the maximal dose for 1 to 2 months and significant improvement is evident. A monthly tapering of 5 to 10 mg is preferred, then more slowly after the daily dose reaches 30 mg. The usual maintenance dose averages about 5 mg daily.
Common side effects of prednisone include weight gain, cushingoid features, easy bruising, cataracts, glaucoma, hypertension, diabetes, dyslipidemia, and osteoporosis. Patients are advised to take supplemental calcium (1,500 mg per day) and vitamin D (400 to 800 IU per day). For those most at risk of osteoporosis, treatment with a bisphosphonate should be considered.
Other immunotherapeutic agents are often needed, either to replace the corticosteroid or to permit use of lower doses of it. Because of their delayed onset of action, starting such corticosteroid-sparing agents early in the course is often necessary. These agents are often initially combined with high-dose prednisone, with an eventual goal of weaning off prednisone entirely. This strategy offers the advantage of relatively rapid induction while avoiding the long-term adverse effects of corticosteroid treatment.
Azathioprine
Azathioprine doesn’t begin to show a beneficial effect in myasthenia gravis for 6 to 12 months, and it often reaches its maximal efficacy only after 1 to 2 years of treatment.38
In a study of 78 myasthenia gravis patients, 91% improved when treated with azathioprine alone or together with prednisone.39 In another study using azathioprine and prednisolone for generalized myasthenia gravis, nearly two-thirds of patients came off prednisolone while maintaining remission for 3 years.38
A typical maintenance dose is 2 to 3 mg/kg/day. Common side effects are nausea, vomiting, and malaise. Less frequent side effects include hematologic abnormalities, abnormal liver function, and pancreatitis. Monthly monitoring of complete blood cell counts and liver function tests is warranted for the first 6 months, then less often.
One in 300 people in the general population is homozygous for a mutant allele in the thiopurine methyltransferase (TPMT) gene. Patients with this genotype should not receive azathioprine because of the risk of life-threatening bone marrow suppression.40 A slightly increased risk of various forms of lymphoma has been documented.41
Mycophenolate mofetil
A well-tolerated medication with few side effects, mycophenolate mofetil is being used more in myasthenia gravis. The results of two recent randomized trials suggested that it is not effective in improving myasthenia gravis symptoms or sparing prednisone dosage when used for 90 days or 36 weeks.42,43 However, extensive clinical experience supports its longterm efficacy in myasthenia gravis.
In a retrospective study of 85 patients with generalized myasthenia gravis, mycophenolate at doses of 1 to 3 g daily improved symptoms in 73% and produced remission in 50%. Steroid dosage was reduced in 71% of patients.44
Another retrospective study, with 102 patients, verified a slow development of clinical benefit after months of mycophenolate therapy alone or in combination with prednisone. Approximately 50% of patients achieved a minimal manifestation status after 6 to 12 months of mycophenolate treatment. Eventually, at 24 months of treatment, 80% of patients had a desirable outcome of minimal clinical manifestation or better, 55% of patients were able to come off prednisone entirely, and 75% were taking less than 7.5 mg of prednisone per day.45
Common side effects of mycophenolate include nausea, diarrhea, and infections such as urinary tract infections and herpes reactivation. The complete blood cell count needs to be monitored frequently during the first 6 months of therapy. Leukopenia can occur but rarely necessitates stopping mycophenolate. Long-term safety data are lacking, but so far there has been no clearly increased risk of malignancy.
Mycophenolate exposure in pregnancy results in a high incidence of major fetal malformations. Therefore, its use in pregnant patients is discouraged, and women of child-bearing age should use effective contraception.46
Cyclosporine
A randomized trial in a small number of patients suggested that cyclosporine is fairly effective as monotherapy.47 Its onset of action in myasthenia gravis is faster than that of other corticosteroid-sparing agents, and clinical benefit can often be observed as early as 1 to 2 months. A dose of 5 mg/kg/day and a maintenance serum level of 100 to 150 ng/mL are generally recommended. However, renal, hepatic, and hematologic toxicities and interactions with other medications make cyclosporine a less attractive choice.
Methotrexate
A randomized trial evaluated the utility of methotrexate as a steroid-sparing agent compared with azathioprine.48 At 24 months, its steroid-sparing effect was similar to that of azathioprine, and the prednisone dosage had been reduced in more than 50% of patients.
Another phase II trial studying the efficacy of methotrexate in myasthenia gravis is under way.49
Rituximab
Rituximab is a monoclonal antibody against B-cell membrane marker CD20. A growing number of case series support its efficacy in patients with severe generalized myasthenia gravis refractory to multiple immunosuppressants.16,50 It seems particularly effective for MuSK antibody-positive disease, reducing MuSK antibody titers and having a treatment effect that lasts for years.
The standard dosage is 375 mg/m2 per week for 4 consecutive weeks. Peripheral B cells tend to be depleted within 2 weeks after the first infusion, while T-cell populations remain unchanged.50
A minimal infusion reaction such as flushing and chills can be seen with the first infusion. Patients may be more susceptible to certain infections such as reactivation of herpes zoster, but overall rituximab is well tolerated. Rare cases of progressive multifocal leukoencephalopathy have been reported in patients taking it, but none have occurred so far in myasthenia gravis treatment.
Cyclophosphamide
Cyclophosphamide is an alkylating agent that reduces proliferation of both B and T cells. It can be effective in myasthenia gravis, but potentially serious side effects limit its use. It should be reserved for the small percentage of cases that are refractory to other immunotherapies.
Thymectomy
Surgical treatment should be considered for patients with thymoma. If the tumor cannot be surgically resected, chemoradiotherapy can be considered for relief of myasthenic symptoms and for prevention of local invasion.
Thymomas recur in a minority of patients many years after the initial resection, sometimes without myasthenia gravis symptoms. A recurrence of symptoms does not necessarily indicate a recurrence of thymoma. The lack of correlation between myasthenia gravis symptoms and thymoma recurrence highlights the importance of radiologic follow-up in these patients.
For patients without thymoma, many experts believe that thymectomy is beneficial in patients under age 60 who have generalized myasthenia gravis. The likelihood of medication-free remission is about twice as high, and the likelihood of becoming asymptomatic is about one and a half times higher after thymectomy.51 However, it takes up to several years for the benefits of thymectomy to manifest, and thymectomy does not guarantee protection from developing AChR antibody-positive myasthenia gravis in the future.
The optimal timing of thymectomy is not well established; however, the procedure is usually recommended within the first 3 years of diagnosis.52 The response rates from thymectomy are similar for AChR antibody-positive and seronegative patients. In general, thymectomy for MuSK antibody-positive patients has not been effective, and its role in ocular myasthenia gravis is unclear.2,53
- Alshekhlee A, Miles JD, Katirji B, Preston DC, Kaminski HJ. Incidence and mortality rates of myasthenia gravis and myasthenic crisis in US hospitals. Neurology 2009; 72:1548–1554.
- Keesey JC. Clinical evaluation and management of myasthenia gravis. Muscle Nerve 2004; 29:484–505.
- Leite MI, Coutinho E, Lana-Peixoto M, et al. Myasthenia gravis and neuromyelitis optica spectrum disorder: a multicenter study of 16 patients. Neurology 2012; 78:1601–1607.
- Drachman DB, Angus CW, Adams RN, Michelson JD, Hoffman GJ. Myasthenic antibodies cross-link acetylcholine receptors to accelerate degradation. N Engl J Med 1978; 298:1116–1122.
- Fujii Y. The thymus, thymoma and myasthenia gravis. Surg Today 2013; 43:461–466.
- Evoli A, Lindstrom J. Myasthenia gravis with antibodies to MuSK: another step toward solving mystery? Neurology 2011; 77:1783–1784.
- Mori S, Kubo S, Akiyoshi T, et al. Antibodies against muscle-specific kinase impair both presynaptic and postsynaptic functions in a murine model of myasthenia gravis. Am J Pathol 2012; 180:798–810.
- Guptill JT, Sanders DB, Evoli A. Anti-MuSK antibody myasthenia gravis: clinical findings and response to treatment in two large cohorts. Muscle Nerve 2011; 44:36–40.
- Chevessier F, Girard E, Molgó J, et al. A mouse model for congenital myasthenic syndrome due to MuSK mutations reveals defects in structure and function of neuromuscular junctions. Hum Mol Genet 2008; 17:3577–3595.
- Richman DP, Nishi K, Morell SW, et al. Acute severe animal model of anti-muscle-specific kinase myasthenia: combined postsynaptic and presynaptic changes. Arch Neurol 2012; 69:453–460.
- Klooster R, Plomp JJ, Huijbers MG, et al. Muscle-specific kinase myasthenia gravis IgG4 autoantibodies cause severe neuromuscular junction dysfunction in mice. Brain 2012; 135:1081–1101.
- Viegas S, Jacobson L, Waters P, et al. Passive and active immunization models of MuSK-Ab positive myasthenia: electrophysiological evidence for pre and postsynaptic defects. Exp Neurol 2012; 234:506–512.
- Niks EH, Kuks JB, Wokke JH, et al. Pre- and postsynaptic neuromuscular junction abnormalities in musk myasthenia. Muscle Nerve 2010; 42:283–288.
- Kawakami Y, Ito M, Hirayama M, et al. Anti-MuSK autoantibodies block binding of collagen Q to MuSK. Neurology 2011; 77:1819–1826.
- Chan KH, Lachance DH, Harper CM, Lennon VA. Frequency of seronegativity in adult-acquired generalized myasthenia gravis. Muscle Nerve 2007; 36:651–658.
- Collongues N, Casez O, Lacour A, et al. Rituximab in refractory and non-refractory myasthenia: a retrospective multicenter study. Muscle Nerve 2012; 46:687–691.
- Sanders DB, Andrews PI, Howard JF, Massey JM. Seronegative myasthenia gravis. Neurology 1997; 48(suppl 5):40S–45S.
- Shiraishi H, Motomura M, Yoshimura T, et al. Acetylcholine receptors loss and postsynaptic damage in MuSK antibody-positive myasthenia gravis. Ann Neurol 2005; 57:289–293.
- Leite MI, Jacob S, Viegas S, et al. IgG1 antibodies to acetylcholine receptors in ‘seronegative’ myasthenia gravis. Brain 2008; 131:1940–1952.
- Jacob S, Viegas S, Leite MI, et al. Presence and pathogenic relevance of antibodies to clustered acetylcholine receptor in ocular and generalized myasthenia gravis. Arch Neurol 2012; 69:994–1001.
- Higuchi O, Hamuro J, Motomura M, Yamanashi Y. Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann Neurol 2011; 69:418–422.
- Pevzner A, Schoser B, Peters K, et al. Anti-LRP4 autoantibodies in AChR- and MuSK-antibody-negative myasthenia gravis. J Neurol 2012; 259:427–435.
- Zhang B, Tzartos JS, Belimezi M, et al. Autoantibodies to lipoprotein-related protein 4 in patients with double-seronegative myasthenia gravis. Arch Neurol 2012; 69:445–451.
- Kupersmith MJ, Latkany R, Homel P. Development of generalized disease at 2 years in patients with ocular myasthenia gravis. Arch Neurol 2003; 60:243–248.
- Pasnoor M, Wolfe GI, Nations S, et al. Clinical findings in MuSK-antibody positive myasthenia gravis: a US experience. Muscle Nerve 2010; 41:370–374.
- Oh SJ, Kim DE, Kuruoglu R, Bradley RJ, Dwyer D. Diagnostic sensitivity of the laboratory tests in myasthenia gravis. Muscle Nerve 1992; 15:720–724.
- Sanders DB, Stålberg EV. AAEM minimonograph #25: single-fiber electromyography. Muscle Nerve 1996; 19:1069–1083.
- Lazo-Langner A, Espinosa-Poblano I, Tirado-Cárdenas N, et al. Therapeutic plasma exchange in Mexico: experience from a single institution. Am J Hematol 2002; 70:16–21.
- Carandina-Maffeis R, Nucci A, Marques JF, et al. Plasmapheresis in the treatment of myasthenia gravis: retrospective study of 26 patients. Arq Neuropsiquiatr 2004; 62:391–395.
- Zinman L, Ng E, Bril V. IV immunoglobulin in patients with myasthenia gravis: a randomized controlled trial. Neurology 2007; 68:837–841.
- Gajdos P, Tranchant C, Clair B, et al; Myasthenia Gravis Clinical Study Group. Treatment of myasthenia gravis exacerbation with intravenous immunoglobulin: a randomized double-blind clinical trial. Arch Neurol 2005; 62:1689–1693.
- Rønager J, Ravnborg M, Hermansen I, Vorstrup S. Immunoglobulin treatment versus plasma exchange in patients with chronic moderate to severe myasthenia gravis. Artif Organs 2001; 25:967–973.
- Barth D, Nabavi Nouri M, Ng E, Nwe P, Bril V. Comparison of IVIg and PLEX in patients with myasthenia gravis. Neurology 2011; 76:2017–2023.
- Wegner B, Ahmed I. Intravenous immunoglobulin monotherapy in long-term treatment of myasthenia gravis. Clin Neurol Neurosurg 2002; 105:3–8.
- Pascuzzi RM, Coslett HB, Johns TR. Long-term corticosteroid treatment of myasthenia gravis: report of 116 patients. Ann Neurol 1984; 15:291–298.
- Monsul NT, Patwa HS, Knorr AM, Lesser RL, Goldstein JM. The effect of prednisone on the progression from ocular to generalized myasthenia gravis. J Neurol Sci 2004; 217:131–133.
- Miller RG, Milner-Brown HS, Mirka A. Prednisone-induced worsening of neuromuscular function in myasthenia gravis. Neurology 1986; 36:729–732.
- Palace J, Newsom-Davis J, Lecky B. A randomized double-blind trial of prednisolone alone or with azathioprine in myasthenia gravis. Myasthenia Gravis Study Group. Neurology 1998; 50:1778–1783.
- Mertens HG, Hertel G, Reuther P, Ricker K. Effect of immunosuppressive drugs (azathioprine). Ann N Y Acad Sci 1981; 377:691–699.
- Relling MV, Gardner EE, Sandborn WJ, et al; Clinical Pharmacogenetics Implementation Consortium. Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clin Pharmacol Ther 2011; 89:387–391.
- Finelli PF. Primary CNS lymphoma in myasthenic on long-term azathioprine. J Neurooncol 2005; 74:91–92.
- Sanders DB, Hart IK, Mantegazza R, et al. An international, phase III, randomized trial of mycophenolate mofetil in myasthenia gravis. Neurology 2008; 71:400–406.
- Muscle Study Group. A trial of mycophenolate mofetil with prednisone as initial immunotherapy in myasthenia gravis. Neurology 2008; 71:394–399.
- Meriggioli MN, Ciafaloni E, Al-Hayk KA, et al. Mycophenolate mofetil for myasthenia gravis: an analysis of efficacy, safety, and tolerability. Neurology 2003; 61:1438–1440.
- Hehir MK, Burns TM, Alpers J, Conaway MR, Sawa M, Sanders DB. Mycophenolate mofetil in AChR-antibody-positive myasthenia gravis: outcomes in 102 patients. Muscle Nerve 2010; 41:593–598.
- Merlob P, Stahl B, Klinger G. Tetrada of the possible mycophenolate mofetil embryopathy: a review. Reprod Toxicol 2009; 28:105–108.
- Tindall RS, Rollins JA, Phillips JT, Greenlee RG, Wells L, Belendiuk G. Preliminary results of a double-blind, randomized, placebo-controlled trial of cyclosporine in myasthenia gravis. N Engl J Med 1987; 316:719–724.
- Heckmann JM, Rawoot A, Bateman K, Renison R, Badri M. A single-blinded trial of methotrexate versus azathioprine as steroid-sparing agents in generalized myasthenia gravis. BMC Neurol 2011; 11:97.
- Pasnoor M, He J, Herbelin L, Dimachkie M, Barohn RJ; Muscle Study Group. Phase II trial of methotrexate in myasthenia gravis. Ann N Y Acad Sci 2012; 1275:23–28.
- Díaz-Manera J, Martínez-Hernández E, Querol L, et al. Long-lasting treatment effect of rituximab in MuSK myasthenia. Neurology 2012; 78:189–193.
- Gronseth GS, Barohn RJ. Practice parameter: thymectomy for autoimmune myasthenia gravis (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55:7–15.
- Kumar V, Kaminski HJ. Treatment of myasthenia gravis. Curr Neurol Neurosci Rep 2011; 11:89–96.
- Pompeo E, Tacconi F, Massa R, Mineo D, Nahmias S, Mineo TC. Long-term outcome of thoracoscopic extended thymectomy for nonthymomatous myasthenia gravis. Eur J Cardiothorac Surg 2009; 36:164–169.
Current therapies for myasthenia gravis can help most patients achieve sustained improvement. The overall prognosis has dramatically improved over the last 4 decades: the mortality rate used to be 75%; now it is 4.5%.1
Myasthenia gravis is the most common disorder of neuromuscular junction transmission and is also one of the best characterized autoimmune diseases. However, its symptoms—primarily weakness—vary from patient to patient, and in the same patient, by time of day and over longer time periods. The variation in symptoms can be very confusing to undiagnosed patients and puzzling to unsuspecting physicians. Such diagnostic uncertainty can give the patient additional frustration and emotional stress, which in turn exacerbate his or her condition.
In this review, we will give an overview of the pathogenesis, clinical manifestations, diagnosis, and treatment of myasthenia gravis.
TWO PEAKS IN INCIDENCE BY AGE
The annual incidence of myasthenia gravis is approximately 10 to 20 new cases per million, with a prevalence of about 150 to 200 per million.2
The age of onset has a bimodal distribution, with an early incidence peak in the second to third decade with a female predominance and a late peak in the 6th to the 8th decade with a male predominance.2
Myasthenia gravis is commonly associated with several other autoimmune disorders, including hypothyroidism, hyperthyroidism, systemic lupus erythematosus, rheumatoid arthritis, vitiligo, diabetes, and, more recently recognized, neuromyelitis optica.3
ANTIBODIES AGAINST AChR AND MuSK
In most cases of myasthenia gravis the patient has autoimmune antibodies against constituents of the neuromuscular junction, specifically acetylcholine receptor (AChR) and muscle-specific tyrosine kinase (MuSK) (Figure 1).
AChR antibody-positive myasthenia gravis
When antibodies bind to AChR on the postsynaptic membrane, they cross-link neighboring AChR units, which are absorbed into the muscle fiber and are broken up.4 In addition, the complement system is activated to mediate further damage on the postsynaptic membrane.
AChR antibodies may come from germinal centers of the thymus, where clustered myoid cells express AChR on the plasma membrane surface.5 About 60% of AChR antibody-positive myasthenia gravis patients have an enlarged thymus, and 10% have a thymoma—a tumor of the epithelial cells of this organ. Conversely, about 15% of patients with a thymoma have clinical myasthenia gravis, and an additional 20% possess antibodies against AChR in the serum without myasthenic symptoms.5
MuSK antibody-positive myasthenia gravis
Like AChR, MuSK is a transmembrane component of the postsynaptic neuromuscular junction. During formation of the neuromuscular junction, MuSK is activated through the binding of agrin (a nerve-derived proteoglycan) to lipoprotein-related protein 4 (LRP4), after which complicated intracellular signaling promotes the assembly and stabilization of AChR.6
Unlike AChR antibodies, antibodies against MuSK do not activate the complement system, and complement fixation is not essential for clinical myasthenic symptoms to appear.7 Also, myasthenia gravis with MuSK antibodies is rarely associated with thymoma.8
The precise mechanism by which MuSK antibody impairs transmission at the neuromuscular junction has been a mystery until recently. Animal models, including MuSK-mutant mice and mice injected with MuSK protein or with purified immunoglobulin G from patients with this disease, have revealed a significant reduction of AChR clusters and destruction of neuromuscular junction structures.7,9–12
In addition, MuSK antibodies produce pre-synaptic dysfunction, manifesting as a reduction of acetylcholine content. This information is based on studies in mice and on in vitro electrophysiologic analyses of neuromuscular junctions from a patient with this disease.7,9–13
Finally, MuSK antibodies may indirectly affect the recycling of acetylcholine. After post-synaptic activation, acetylcholine is normally hydrolized by acetylcholinesterase, which is located in the synaptic cleft but anchored to MuSK on the postsynaptic membrane. MuSK antibodies block the binding of MuSK to acetylcholinesterase, possibly leading to less accumulation of acetylcholinesterase.14 This process may explain why patients with MuSK antibody-positive myasthenia gravis tend to respond poorly to acetylcholinesterase inhibitors (more about this below).
Seronegative myasthenia gravis
In a series of 562 consecutive patients with generalized weakness due to myasthenia gravis, 92% were positive for AChR antibody, 3% were positive for MuSK antibody, and 5% were seronegative (possessing neither antibody).15 In contrast, about 50% of patients with purely ocular myasthenia gravis (ie, with isolated weakness of the levator palpebrae superioris, orbicularis oculi, or oculomotor muscles) are seropositive for AChR antibody. Only a few ocular MuSK antibody-positive cases have been described, leaving the rest seronegative. Rarely, both antibodies can be detected in the same patient.16
In patients who are negative for AChR antibodies at the time of disease onset, sero-conversion may occur later during the course. Repeating serologic testing 6 to 12 months later may detect AChR antibodies in approximately 15% of patients who were initially seronegative.15,17
The clinical presentation, electrophysiologic findings, thymic pathologic findings, and treatment responses are similar in AChR antibody-positive and seronegative myasthenia gravis.17 Muscle biopsy study in seronegative cases demonstrates a loss of AChR as well.18
Based on these observations, it has been proposed that seronegative patients may have low-affinity antibodies that can bind to tightly clustered AChRs on the postsynaptic membrane but escape detection by routine radioimmunoassays in a solution phase. With a sensitive cell-based immunofluorescence assay, low-affinity antibodies to clustered AChRs were detected in 66% of patients with generalized myasthenia gravis and in 50% of those with ocular myasthenia gravis who were seronegative on standard assays.19,20 These low-affinity AChR antibodies can also activate complement in vitro, increasing the likelihood that they are pathogenic. However, assays to detect low-affinity AChR antibodies are not yet commercially available.
Within the past year, three research groups independently reported detecting antibodies to LRP4 in 2% to 50% of seronegative myasthenia gravis patients. This wide variation in the prevalence of LRP4 antibodies could be related to patient ethnicity and methods of detection.21–23 LRP4 is a receptor for agrin and is required for agrin-induced MuSK activation and AChR clustering. LRP antibodies can activate complement; therefore, it is plausible that LRP4 antibody binding leads to AChR loss on the postsynaptic membrane. However, additional study is needed to determine if LRP4 antibodies are truly pathogenic in myasthenia gravis.
A DISORDER OF FATIGABLE WEAKNESS
Myasthenia gravis is a disorder of fatigable weakness producing fluctuating symptoms. Symptoms related to the involvement of specific muscle groups are listed in Table 1. Muscle weakness is often worse later in the day or after exercise.
Ocular myasthenia gravis accounts for about 15% of all cases. Of patients initially presenting with ocular symptoms only, twothirds will ultimately develop generalized symptoms, most within the first 2 years.24 No factor has been identified that predicts conversion from an ocular to a generalized form.
Several clinical phenotypes of MuSK antibody-positive myasthenia gravis have been described. An oculobulbar form presents with diplopia, ptosis, dysarthria, and profound atrophy of the muscles of the tongue and face. A restricted myopathic form presents with prominent neck, shoulder, and respiratory weakness without ocular involvement. A third form is a combination of ocular and proximal limb weakness, indistinguishable from AChR antibody-positive disease.25
MuSK antibody-positive patients do not respond as well to acetylcholinesterase inhibitors as AChR antibody-positive patients do. In one study, nearly 70% of MuSK antibody-positive patients demonstrated no response, poor tolerance, or cholinergic hypersensitivity to these agents.25 Fortunately, most MuSK antibody-positive patients have a favorable response to immunosuppressive therapy—sometimes a dramatic improvement after plasmapheresis.8
DIAGNOSIS OF MYASTHENIA GRAVIS
The common differential diagnoses for myasthenia gravis are listed in Table 2.
The essential feature of myasthenia gravis is fluctuating muscle weakness, often with fatigue. Many patients complain of weakness of specific muscle groups after their repeated usage. Pain is generally a less conspicuous symptom, and generalized fatigue without objective weakness is inconsistent with myasthenia gravis.
Signs of muscle weakness may include droopy eyelids, diplopia, inability to hold the head straight, difficulty swallowing or chewing, speech disturbances, difficulty breathing, and difficulty raising the arms or rising from the sitting position. A historical pattern of ptosis alternating from one eye to the other is fairly characteristic of myasthenia gravis.
The weakness of orbicularis oculi is easily identified on examination by prying open the eyes during forced eye closure. Limb weakness is usually more significant in the arms than in the legs. An often-neglected feature of myasthenia gravis is finger extensor weakness with a relative sparing of other distal hand muscles.2
The ice-pack test is performed by placing a small bag of ice over the ptotic eye for 2 to 5 minutes and assessing the degree of ptosis for any noticeable improvement. This test is not very helpful for assessing ocular motor weakness.
The edrophonium (Tensilon) test can be used for patients with ptosis or ophthalmoparesis. Edrophonium, a short-acting acetylcholinesterase inhibitor, is given intravenously while the patient is observed for objective improvement. The patient’s cardiovascular status should be monitored for arrhythmias and hypotension. Atropine should be immediately available in case severe bradycardia develops.
The ice-pack test and the edrophonium test can give false-negative and false-positive results, and the diagnosis of myasthenia gravis must be verified by other diagnostic tests.
Testing for antibodies
Testing for circulating AChR antibodies, MuSK antibodies, or both is the first step in the laboratory confirmation of myasthenia gravis.
There are three AChR antibody subtypes: binding, blocking, and modulating. Binding antibodies are present in 80% to 90% of patients with generalized myasthenia gravis and 50% of those with ocular myasthenia gravis. Testing for blocking and modulating AChR antibodies increases the sensitivity by less than 5% when added to testing for binding antibodies.
AChR antibody titers correlate poorly with disease severity between patients. However, in individual patients, antibody titers tend to go down in parallel with clinical improvement.
MuSK antibody is detected in nearly half of myasthenia gravis patients with generalized weakness who are negative for AChR antibody.
Electrophysiologic tests
Electrophysiologic tests can usually confirm the diagnosis of seronegative myasthenia gravis. They are also helpful in seropositive patients who have unusual clinical features or a poor response to treatment.
Repetitive nerve stimulation studies use a slow rate (2–5 Hz) of repetitive electrical stimulation. The study is positive if the motor response declines by more than 10%. However, a decremental response is not specific for myasthenia gravis, as it may be seen in other neuromuscular disorders such as motor neuron disease or Lambert-Eaton myasthenic syndrome.
This test is technically easier to do in distal muscles than in proximal muscles, but less sensitive. Therefore, proximal muscles such as the trapezius or facial muscles are usually also sampled to maximize the yield. To further maximize the sensitivity, muscles being tested should be warm, and acetylcholinesterase inhibitors should be withheld for 12 hours before.
Repetitive nerve stimulation studies in distal muscles are positive in approximately 75% of patients with generalized myasthenia gravis and in 30% with ocular myasthenia gravis.26
Single-fiber electromyography is more technically demanding than repetitive nerve stimulation and is less widely available. It is usually performed with a special needle electrode that can simultaneously identify action potentials arising from individual muscle fibers innervated by the same axon.
Variability in time of the second action potential relative to the first is called “jitter.” Abnormal jitter is seen in more than 95% of patients with generalized myasthenia gravis and in 85% to 90% of those with ocular myasthenia gravis.26,27 However, abnormal jitter can also be seen in other neuromuscular diseases such as motor neuron disease or in neuromuscular junctional disorders such as Lambert-Eaton myasthenic syndrome.
Imaging studies
Chest computed tomography or magnetic resonance imaging with contrast should be performed in all myasthenia gravis patients to look for a thymoma.
TREATMENT OF MYASTHENIA GRAVIS
Acetylcholinesterase inhibitors
As a reasonable first therapy in mild cases of myasthenia gravis, acetylcholinesterase inhibitors slow down the degradation of acetylcholine and prolong its effect in the neuromuscular junction, but they are not disease-modifying and their benefits are mild.
Pyridostigmine is the usual choice of acetylcholinesterase inhibitor. Its onset of action is rapid (15 to 30 minutes) and its action lasts for 3 to 4 hours. For most patients, the effective dosage range is 60 mg to 90 mg every 4 to 6 hours. A long-acting form is also available and can be given as a single nighttime dose.
Immunomodulating therapy
Patients who have moderate to severe symptoms require some form of immunomodulating therapy.
Plasmapheresis or intravenous immune globulin is reserved for patients with severe or rapidly worsening disease because their beneficial effects can be seen within the first week of treatment.
Longer-acting immunotherapies (corticosteroids, azathioprine, mycophenolate mofetil and others) have a slower onset of responses but provide sustained benefits. Which drug to use depends on factors such as comorbidity, side effects, and cost.
Drugs to avoid
A number of medications can exacerbate weakness in myasthenia gravis and should be avoided or used with caution. The list is long, but ones that deserve the most attention are penicillamine, interferons, procainamide, quinidine, and antibiotics, including quinolones and aminoglycosides. A more comprehensive list of medications that may exacerbate myasthenia gravis symptoms can be found in a review by Keesey.2
RAPID INDUCTION IMMUNOTHERAPIES : PLASMAPHERESIS, IMMUNE GLOBULIN
Both plasmapheresis and intravenous immune globulin act quickly over days, but in most patients their effects last only a few weeks. Both are used as rescue therapies for myasthenic crises, bridging therapy to slow-acting immunotherapeutic agents, or maintenance treatment for poorly controlled cases.
Several retrospective studies have confirmed the efficacy of plasmapheresis in more than 80% of patients with generalized symptoms.28,29
In a randomized trial in patients with generalized therapies, intravenous immune globulin improved muscle strength in the group of patients with severe symptoms.30 The effective dosage of intravenous immune globulin varies from 1 to 2 g/kg without observed difference between doses.31 Trials comparing the efficacy of intravenous immune globulin and plasmapheresis in acute and severe myasthenia gravis did not reveal a difference in efficacy.32,33 Intravenous immune globulin at a minimal dose of 0.4 g/kg every 3 months has been successfully used as a long-term maintenance monotherapy, and such a role could be expanded to more patients with further studies.34
The choice between plasmapheresis and intravenous immune globulin is often based on the ability of a patient to tolerate each treatment and on the availability of the plasmapheresis procedure. Intravenous immune globulin is easier to administer, is associated with fewer adverse events related to vascular access, and is therefore more appropriate than plasmapheresis in some centers.
CHRONIC MAINTENANCE IMMUNOMODULATING TREATMENT
Corticosteroids
Prednisone, the most commonly used agent, leads to remission or marked improvement in 70% to 80% of patients with ocular or generalized myasthenia gravis.35 It may also reduce the progression of ocular myasthenia gravis to the generalized form.36
The effective dose of prednisone depends on the severity and distribution of symptoms. Some patients may need up to 1.0 mg/kg/day (usually 50 to 80 mg per day). In patients with mild to moderate symptoms, a lower maximal dosage such as 20 to 40 mg per day can be sufficient.
Within 1 to 2 weeks after starting high-dose prednisone, up to 50% of patients may develop a transient deterioration, including possible precipitation of a myasthenic crisis.37 For this reason, high-dose prednisone is commonly started only in hospitalized patients who are also receiving plasmapheresis or intravenous immune globulin. Otherwise, an outpatient dose-escalation protocol can be used to achieve a target dose over several weeks.
Prednisone tapering can begin after the patient has been on the maximal dose for 1 to 2 months and significant improvement is evident. A monthly tapering of 5 to 10 mg is preferred, then more slowly after the daily dose reaches 30 mg. The usual maintenance dose averages about 5 mg daily.
Common side effects of prednisone include weight gain, cushingoid features, easy bruising, cataracts, glaucoma, hypertension, diabetes, dyslipidemia, and osteoporosis. Patients are advised to take supplemental calcium (1,500 mg per day) and vitamin D (400 to 800 IU per day). For those most at risk of osteoporosis, treatment with a bisphosphonate should be considered.
Other immunotherapeutic agents are often needed, either to replace the corticosteroid or to permit use of lower doses of it. Because of their delayed onset of action, starting such corticosteroid-sparing agents early in the course is often necessary. These agents are often initially combined with high-dose prednisone, with an eventual goal of weaning off prednisone entirely. This strategy offers the advantage of relatively rapid induction while avoiding the long-term adverse effects of corticosteroid treatment.
Azathioprine
Azathioprine doesn’t begin to show a beneficial effect in myasthenia gravis for 6 to 12 months, and it often reaches its maximal efficacy only after 1 to 2 years of treatment.38
In a study of 78 myasthenia gravis patients, 91% improved when treated with azathioprine alone or together with prednisone.39 In another study using azathioprine and prednisolone for generalized myasthenia gravis, nearly two-thirds of patients came off prednisolone while maintaining remission for 3 years.38
A typical maintenance dose is 2 to 3 mg/kg/day. Common side effects are nausea, vomiting, and malaise. Less frequent side effects include hematologic abnormalities, abnormal liver function, and pancreatitis. Monthly monitoring of complete blood cell counts and liver function tests is warranted for the first 6 months, then less often.
One in 300 people in the general population is homozygous for a mutant allele in the thiopurine methyltransferase (TPMT) gene. Patients with this genotype should not receive azathioprine because of the risk of life-threatening bone marrow suppression.40 A slightly increased risk of various forms of lymphoma has been documented.41
Mycophenolate mofetil
A well-tolerated medication with few side effects, mycophenolate mofetil is being used more in myasthenia gravis. The results of two recent randomized trials suggested that it is not effective in improving myasthenia gravis symptoms or sparing prednisone dosage when used for 90 days or 36 weeks.42,43 However, extensive clinical experience supports its longterm efficacy in myasthenia gravis.
In a retrospective study of 85 patients with generalized myasthenia gravis, mycophenolate at doses of 1 to 3 g daily improved symptoms in 73% and produced remission in 50%. Steroid dosage was reduced in 71% of patients.44
Another retrospective study, with 102 patients, verified a slow development of clinical benefit after months of mycophenolate therapy alone or in combination with prednisone. Approximately 50% of patients achieved a minimal manifestation status after 6 to 12 months of mycophenolate treatment. Eventually, at 24 months of treatment, 80% of patients had a desirable outcome of minimal clinical manifestation or better, 55% of patients were able to come off prednisone entirely, and 75% were taking less than 7.5 mg of prednisone per day.45
Common side effects of mycophenolate include nausea, diarrhea, and infections such as urinary tract infections and herpes reactivation. The complete blood cell count needs to be monitored frequently during the first 6 months of therapy. Leukopenia can occur but rarely necessitates stopping mycophenolate. Long-term safety data are lacking, but so far there has been no clearly increased risk of malignancy.
Mycophenolate exposure in pregnancy results in a high incidence of major fetal malformations. Therefore, its use in pregnant patients is discouraged, and women of child-bearing age should use effective contraception.46
Cyclosporine
A randomized trial in a small number of patients suggested that cyclosporine is fairly effective as monotherapy.47 Its onset of action in myasthenia gravis is faster than that of other corticosteroid-sparing agents, and clinical benefit can often be observed as early as 1 to 2 months. A dose of 5 mg/kg/day and a maintenance serum level of 100 to 150 ng/mL are generally recommended. However, renal, hepatic, and hematologic toxicities and interactions with other medications make cyclosporine a less attractive choice.
Methotrexate
A randomized trial evaluated the utility of methotrexate as a steroid-sparing agent compared with azathioprine.48 At 24 months, its steroid-sparing effect was similar to that of azathioprine, and the prednisone dosage had been reduced in more than 50% of patients.
Another phase II trial studying the efficacy of methotrexate in myasthenia gravis is under way.49
Rituximab
Rituximab is a monoclonal antibody against B-cell membrane marker CD20. A growing number of case series support its efficacy in patients with severe generalized myasthenia gravis refractory to multiple immunosuppressants.16,50 It seems particularly effective for MuSK antibody-positive disease, reducing MuSK antibody titers and having a treatment effect that lasts for years.
The standard dosage is 375 mg/m2 per week for 4 consecutive weeks. Peripheral B cells tend to be depleted within 2 weeks after the first infusion, while T-cell populations remain unchanged.50
A minimal infusion reaction such as flushing and chills can be seen with the first infusion. Patients may be more susceptible to certain infections such as reactivation of herpes zoster, but overall rituximab is well tolerated. Rare cases of progressive multifocal leukoencephalopathy have been reported in patients taking it, but none have occurred so far in myasthenia gravis treatment.
Cyclophosphamide
Cyclophosphamide is an alkylating agent that reduces proliferation of both B and T cells. It can be effective in myasthenia gravis, but potentially serious side effects limit its use. It should be reserved for the small percentage of cases that are refractory to other immunotherapies.
Thymectomy
Surgical treatment should be considered for patients with thymoma. If the tumor cannot be surgically resected, chemoradiotherapy can be considered for relief of myasthenic symptoms and for prevention of local invasion.
Thymomas recur in a minority of patients many years after the initial resection, sometimes without myasthenia gravis symptoms. A recurrence of symptoms does not necessarily indicate a recurrence of thymoma. The lack of correlation between myasthenia gravis symptoms and thymoma recurrence highlights the importance of radiologic follow-up in these patients.
For patients without thymoma, many experts believe that thymectomy is beneficial in patients under age 60 who have generalized myasthenia gravis. The likelihood of medication-free remission is about twice as high, and the likelihood of becoming asymptomatic is about one and a half times higher after thymectomy.51 However, it takes up to several years for the benefits of thymectomy to manifest, and thymectomy does not guarantee protection from developing AChR antibody-positive myasthenia gravis in the future.
The optimal timing of thymectomy is not well established; however, the procedure is usually recommended within the first 3 years of diagnosis.52 The response rates from thymectomy are similar for AChR antibody-positive and seronegative patients. In general, thymectomy for MuSK antibody-positive patients has not been effective, and its role in ocular myasthenia gravis is unclear.2,53
Current therapies for myasthenia gravis can help most patients achieve sustained improvement. The overall prognosis has dramatically improved over the last 4 decades: the mortality rate used to be 75%; now it is 4.5%.1
Myasthenia gravis is the most common disorder of neuromuscular junction transmission and is also one of the best characterized autoimmune diseases. However, its symptoms—primarily weakness—vary from patient to patient, and in the same patient, by time of day and over longer time periods. The variation in symptoms can be very confusing to undiagnosed patients and puzzling to unsuspecting physicians. Such diagnostic uncertainty can give the patient additional frustration and emotional stress, which in turn exacerbate his or her condition.
In this review, we will give an overview of the pathogenesis, clinical manifestations, diagnosis, and treatment of myasthenia gravis.
TWO PEAKS IN INCIDENCE BY AGE
The annual incidence of myasthenia gravis is approximately 10 to 20 new cases per million, with a prevalence of about 150 to 200 per million.2
The age of onset has a bimodal distribution, with an early incidence peak in the second to third decade with a female predominance and a late peak in the 6th to the 8th decade with a male predominance.2
Myasthenia gravis is commonly associated with several other autoimmune disorders, including hypothyroidism, hyperthyroidism, systemic lupus erythematosus, rheumatoid arthritis, vitiligo, diabetes, and, more recently recognized, neuromyelitis optica.3
ANTIBODIES AGAINST AChR AND MuSK
In most cases of myasthenia gravis the patient has autoimmune antibodies against constituents of the neuromuscular junction, specifically acetylcholine receptor (AChR) and muscle-specific tyrosine kinase (MuSK) (Figure 1).
AChR antibody-positive myasthenia gravis
When antibodies bind to AChR on the postsynaptic membrane, they cross-link neighboring AChR units, which are absorbed into the muscle fiber and are broken up.4 In addition, the complement system is activated to mediate further damage on the postsynaptic membrane.
AChR antibodies may come from germinal centers of the thymus, where clustered myoid cells express AChR on the plasma membrane surface.5 About 60% of AChR antibody-positive myasthenia gravis patients have an enlarged thymus, and 10% have a thymoma—a tumor of the epithelial cells of this organ. Conversely, about 15% of patients with a thymoma have clinical myasthenia gravis, and an additional 20% possess antibodies against AChR in the serum without myasthenic symptoms.5
MuSK antibody-positive myasthenia gravis
Like AChR, MuSK is a transmembrane component of the postsynaptic neuromuscular junction. During formation of the neuromuscular junction, MuSK is activated through the binding of agrin (a nerve-derived proteoglycan) to lipoprotein-related protein 4 (LRP4), after which complicated intracellular signaling promotes the assembly and stabilization of AChR.6
Unlike AChR antibodies, antibodies against MuSK do not activate the complement system, and complement fixation is not essential for clinical myasthenic symptoms to appear.7 Also, myasthenia gravis with MuSK antibodies is rarely associated with thymoma.8
The precise mechanism by which MuSK antibody impairs transmission at the neuromuscular junction has been a mystery until recently. Animal models, including MuSK-mutant mice and mice injected with MuSK protein or with purified immunoglobulin G from patients with this disease, have revealed a significant reduction of AChR clusters and destruction of neuromuscular junction structures.7,9–12
In addition, MuSK antibodies produce pre-synaptic dysfunction, manifesting as a reduction of acetylcholine content. This information is based on studies in mice and on in vitro electrophysiologic analyses of neuromuscular junctions from a patient with this disease.7,9–13
Finally, MuSK antibodies may indirectly affect the recycling of acetylcholine. After post-synaptic activation, acetylcholine is normally hydrolized by acetylcholinesterase, which is located in the synaptic cleft but anchored to MuSK on the postsynaptic membrane. MuSK antibodies block the binding of MuSK to acetylcholinesterase, possibly leading to less accumulation of acetylcholinesterase.14 This process may explain why patients with MuSK antibody-positive myasthenia gravis tend to respond poorly to acetylcholinesterase inhibitors (more about this below).
Seronegative myasthenia gravis
In a series of 562 consecutive patients with generalized weakness due to myasthenia gravis, 92% were positive for AChR antibody, 3% were positive for MuSK antibody, and 5% were seronegative (possessing neither antibody).15 In contrast, about 50% of patients with purely ocular myasthenia gravis (ie, with isolated weakness of the levator palpebrae superioris, orbicularis oculi, or oculomotor muscles) are seropositive for AChR antibody. Only a few ocular MuSK antibody-positive cases have been described, leaving the rest seronegative. Rarely, both antibodies can be detected in the same patient.16
In patients who are negative for AChR antibodies at the time of disease onset, sero-conversion may occur later during the course. Repeating serologic testing 6 to 12 months later may detect AChR antibodies in approximately 15% of patients who were initially seronegative.15,17
The clinical presentation, electrophysiologic findings, thymic pathologic findings, and treatment responses are similar in AChR antibody-positive and seronegative myasthenia gravis.17 Muscle biopsy study in seronegative cases demonstrates a loss of AChR as well.18
Based on these observations, it has been proposed that seronegative patients may have low-affinity antibodies that can bind to tightly clustered AChRs on the postsynaptic membrane but escape detection by routine radioimmunoassays in a solution phase. With a sensitive cell-based immunofluorescence assay, low-affinity antibodies to clustered AChRs were detected in 66% of patients with generalized myasthenia gravis and in 50% of those with ocular myasthenia gravis who were seronegative on standard assays.19,20 These low-affinity AChR antibodies can also activate complement in vitro, increasing the likelihood that they are pathogenic. However, assays to detect low-affinity AChR antibodies are not yet commercially available.
Within the past year, three research groups independently reported detecting antibodies to LRP4 in 2% to 50% of seronegative myasthenia gravis patients. This wide variation in the prevalence of LRP4 antibodies could be related to patient ethnicity and methods of detection.21–23 LRP4 is a receptor for agrin and is required for agrin-induced MuSK activation and AChR clustering. LRP antibodies can activate complement; therefore, it is plausible that LRP4 antibody binding leads to AChR loss on the postsynaptic membrane. However, additional study is needed to determine if LRP4 antibodies are truly pathogenic in myasthenia gravis.
A DISORDER OF FATIGABLE WEAKNESS
Myasthenia gravis is a disorder of fatigable weakness producing fluctuating symptoms. Symptoms related to the involvement of specific muscle groups are listed in Table 1. Muscle weakness is often worse later in the day or after exercise.
Ocular myasthenia gravis accounts for about 15% of all cases. Of patients initially presenting with ocular symptoms only, twothirds will ultimately develop generalized symptoms, most within the first 2 years.24 No factor has been identified that predicts conversion from an ocular to a generalized form.
Several clinical phenotypes of MuSK antibody-positive myasthenia gravis have been described. An oculobulbar form presents with diplopia, ptosis, dysarthria, and profound atrophy of the muscles of the tongue and face. A restricted myopathic form presents with prominent neck, shoulder, and respiratory weakness without ocular involvement. A third form is a combination of ocular and proximal limb weakness, indistinguishable from AChR antibody-positive disease.25
MuSK antibody-positive patients do not respond as well to acetylcholinesterase inhibitors as AChR antibody-positive patients do. In one study, nearly 70% of MuSK antibody-positive patients demonstrated no response, poor tolerance, or cholinergic hypersensitivity to these agents.25 Fortunately, most MuSK antibody-positive patients have a favorable response to immunosuppressive therapy—sometimes a dramatic improvement after plasmapheresis.8
DIAGNOSIS OF MYASTHENIA GRAVIS
The common differential diagnoses for myasthenia gravis are listed in Table 2.
The essential feature of myasthenia gravis is fluctuating muscle weakness, often with fatigue. Many patients complain of weakness of specific muscle groups after their repeated usage. Pain is generally a less conspicuous symptom, and generalized fatigue without objective weakness is inconsistent with myasthenia gravis.
Signs of muscle weakness may include droopy eyelids, diplopia, inability to hold the head straight, difficulty swallowing or chewing, speech disturbances, difficulty breathing, and difficulty raising the arms or rising from the sitting position. A historical pattern of ptosis alternating from one eye to the other is fairly characteristic of myasthenia gravis.
The weakness of orbicularis oculi is easily identified on examination by prying open the eyes during forced eye closure. Limb weakness is usually more significant in the arms than in the legs. An often-neglected feature of myasthenia gravis is finger extensor weakness with a relative sparing of other distal hand muscles.2
The ice-pack test is performed by placing a small bag of ice over the ptotic eye for 2 to 5 minutes and assessing the degree of ptosis for any noticeable improvement. This test is not very helpful for assessing ocular motor weakness.
The edrophonium (Tensilon) test can be used for patients with ptosis or ophthalmoparesis. Edrophonium, a short-acting acetylcholinesterase inhibitor, is given intravenously while the patient is observed for objective improvement. The patient’s cardiovascular status should be monitored for arrhythmias and hypotension. Atropine should be immediately available in case severe bradycardia develops.
The ice-pack test and the edrophonium test can give false-negative and false-positive results, and the diagnosis of myasthenia gravis must be verified by other diagnostic tests.
Testing for antibodies
Testing for circulating AChR antibodies, MuSK antibodies, or both is the first step in the laboratory confirmation of myasthenia gravis.
There are three AChR antibody subtypes: binding, blocking, and modulating. Binding antibodies are present in 80% to 90% of patients with generalized myasthenia gravis and 50% of those with ocular myasthenia gravis. Testing for blocking and modulating AChR antibodies increases the sensitivity by less than 5% when added to testing for binding antibodies.
AChR antibody titers correlate poorly with disease severity between patients. However, in individual patients, antibody titers tend to go down in parallel with clinical improvement.
MuSK antibody is detected in nearly half of myasthenia gravis patients with generalized weakness who are negative for AChR antibody.
Electrophysiologic tests
Electrophysiologic tests can usually confirm the diagnosis of seronegative myasthenia gravis. They are also helpful in seropositive patients who have unusual clinical features or a poor response to treatment.
Repetitive nerve stimulation studies use a slow rate (2–5 Hz) of repetitive electrical stimulation. The study is positive if the motor response declines by more than 10%. However, a decremental response is not specific for myasthenia gravis, as it may be seen in other neuromuscular disorders such as motor neuron disease or Lambert-Eaton myasthenic syndrome.
This test is technically easier to do in distal muscles than in proximal muscles, but less sensitive. Therefore, proximal muscles such as the trapezius or facial muscles are usually also sampled to maximize the yield. To further maximize the sensitivity, muscles being tested should be warm, and acetylcholinesterase inhibitors should be withheld for 12 hours before.
Repetitive nerve stimulation studies in distal muscles are positive in approximately 75% of patients with generalized myasthenia gravis and in 30% with ocular myasthenia gravis.26
Single-fiber electromyography is more technically demanding than repetitive nerve stimulation and is less widely available. It is usually performed with a special needle electrode that can simultaneously identify action potentials arising from individual muscle fibers innervated by the same axon.
Variability in time of the second action potential relative to the first is called “jitter.” Abnormal jitter is seen in more than 95% of patients with generalized myasthenia gravis and in 85% to 90% of those with ocular myasthenia gravis.26,27 However, abnormal jitter can also be seen in other neuromuscular diseases such as motor neuron disease or in neuromuscular junctional disorders such as Lambert-Eaton myasthenic syndrome.
Imaging studies
Chest computed tomography or magnetic resonance imaging with contrast should be performed in all myasthenia gravis patients to look for a thymoma.
TREATMENT OF MYASTHENIA GRAVIS
Acetylcholinesterase inhibitors
As a reasonable first therapy in mild cases of myasthenia gravis, acetylcholinesterase inhibitors slow down the degradation of acetylcholine and prolong its effect in the neuromuscular junction, but they are not disease-modifying and their benefits are mild.
Pyridostigmine is the usual choice of acetylcholinesterase inhibitor. Its onset of action is rapid (15 to 30 minutes) and its action lasts for 3 to 4 hours. For most patients, the effective dosage range is 60 mg to 90 mg every 4 to 6 hours. A long-acting form is also available and can be given as a single nighttime dose.
Immunomodulating therapy
Patients who have moderate to severe symptoms require some form of immunomodulating therapy.
Plasmapheresis or intravenous immune globulin is reserved for patients with severe or rapidly worsening disease because their beneficial effects can be seen within the first week of treatment.
Longer-acting immunotherapies (corticosteroids, azathioprine, mycophenolate mofetil and others) have a slower onset of responses but provide sustained benefits. Which drug to use depends on factors such as comorbidity, side effects, and cost.
Drugs to avoid
A number of medications can exacerbate weakness in myasthenia gravis and should be avoided or used with caution. The list is long, but ones that deserve the most attention are penicillamine, interferons, procainamide, quinidine, and antibiotics, including quinolones and aminoglycosides. A more comprehensive list of medications that may exacerbate myasthenia gravis symptoms can be found in a review by Keesey.2
RAPID INDUCTION IMMUNOTHERAPIES : PLASMAPHERESIS, IMMUNE GLOBULIN
Both plasmapheresis and intravenous immune globulin act quickly over days, but in most patients their effects last only a few weeks. Both are used as rescue therapies for myasthenic crises, bridging therapy to slow-acting immunotherapeutic agents, or maintenance treatment for poorly controlled cases.
Several retrospective studies have confirmed the efficacy of plasmapheresis in more than 80% of patients with generalized symptoms.28,29
In a randomized trial in patients with generalized therapies, intravenous immune globulin improved muscle strength in the group of patients with severe symptoms.30 The effective dosage of intravenous immune globulin varies from 1 to 2 g/kg without observed difference between doses.31 Trials comparing the efficacy of intravenous immune globulin and plasmapheresis in acute and severe myasthenia gravis did not reveal a difference in efficacy.32,33 Intravenous immune globulin at a minimal dose of 0.4 g/kg every 3 months has been successfully used as a long-term maintenance monotherapy, and such a role could be expanded to more patients with further studies.34
The choice between plasmapheresis and intravenous immune globulin is often based on the ability of a patient to tolerate each treatment and on the availability of the plasmapheresis procedure. Intravenous immune globulin is easier to administer, is associated with fewer adverse events related to vascular access, and is therefore more appropriate than plasmapheresis in some centers.
CHRONIC MAINTENANCE IMMUNOMODULATING TREATMENT
Corticosteroids
Prednisone, the most commonly used agent, leads to remission or marked improvement in 70% to 80% of patients with ocular or generalized myasthenia gravis.35 It may also reduce the progression of ocular myasthenia gravis to the generalized form.36
The effective dose of prednisone depends on the severity and distribution of symptoms. Some patients may need up to 1.0 mg/kg/day (usually 50 to 80 mg per day). In patients with mild to moderate symptoms, a lower maximal dosage such as 20 to 40 mg per day can be sufficient.
Within 1 to 2 weeks after starting high-dose prednisone, up to 50% of patients may develop a transient deterioration, including possible precipitation of a myasthenic crisis.37 For this reason, high-dose prednisone is commonly started only in hospitalized patients who are also receiving plasmapheresis or intravenous immune globulin. Otherwise, an outpatient dose-escalation protocol can be used to achieve a target dose over several weeks.
Prednisone tapering can begin after the patient has been on the maximal dose for 1 to 2 months and significant improvement is evident. A monthly tapering of 5 to 10 mg is preferred, then more slowly after the daily dose reaches 30 mg. The usual maintenance dose averages about 5 mg daily.
Common side effects of prednisone include weight gain, cushingoid features, easy bruising, cataracts, glaucoma, hypertension, diabetes, dyslipidemia, and osteoporosis. Patients are advised to take supplemental calcium (1,500 mg per day) and vitamin D (400 to 800 IU per day). For those most at risk of osteoporosis, treatment with a bisphosphonate should be considered.
Other immunotherapeutic agents are often needed, either to replace the corticosteroid or to permit use of lower doses of it. Because of their delayed onset of action, starting such corticosteroid-sparing agents early in the course is often necessary. These agents are often initially combined with high-dose prednisone, with an eventual goal of weaning off prednisone entirely. This strategy offers the advantage of relatively rapid induction while avoiding the long-term adverse effects of corticosteroid treatment.
Azathioprine
Azathioprine doesn’t begin to show a beneficial effect in myasthenia gravis for 6 to 12 months, and it often reaches its maximal efficacy only after 1 to 2 years of treatment.38
In a study of 78 myasthenia gravis patients, 91% improved when treated with azathioprine alone or together with prednisone.39 In another study using azathioprine and prednisolone for generalized myasthenia gravis, nearly two-thirds of patients came off prednisolone while maintaining remission for 3 years.38
A typical maintenance dose is 2 to 3 mg/kg/day. Common side effects are nausea, vomiting, and malaise. Less frequent side effects include hematologic abnormalities, abnormal liver function, and pancreatitis. Monthly monitoring of complete blood cell counts and liver function tests is warranted for the first 6 months, then less often.
One in 300 people in the general population is homozygous for a mutant allele in the thiopurine methyltransferase (TPMT) gene. Patients with this genotype should not receive azathioprine because of the risk of life-threatening bone marrow suppression.40 A slightly increased risk of various forms of lymphoma has been documented.41
Mycophenolate mofetil
A well-tolerated medication with few side effects, mycophenolate mofetil is being used more in myasthenia gravis. The results of two recent randomized trials suggested that it is not effective in improving myasthenia gravis symptoms or sparing prednisone dosage when used for 90 days or 36 weeks.42,43 However, extensive clinical experience supports its longterm efficacy in myasthenia gravis.
In a retrospective study of 85 patients with generalized myasthenia gravis, mycophenolate at doses of 1 to 3 g daily improved symptoms in 73% and produced remission in 50%. Steroid dosage was reduced in 71% of patients.44
Another retrospective study, with 102 patients, verified a slow development of clinical benefit after months of mycophenolate therapy alone or in combination with prednisone. Approximately 50% of patients achieved a minimal manifestation status after 6 to 12 months of mycophenolate treatment. Eventually, at 24 months of treatment, 80% of patients had a desirable outcome of minimal clinical manifestation or better, 55% of patients were able to come off prednisone entirely, and 75% were taking less than 7.5 mg of prednisone per day.45
Common side effects of mycophenolate include nausea, diarrhea, and infections such as urinary tract infections and herpes reactivation. The complete blood cell count needs to be monitored frequently during the first 6 months of therapy. Leukopenia can occur but rarely necessitates stopping mycophenolate. Long-term safety data are lacking, but so far there has been no clearly increased risk of malignancy.
Mycophenolate exposure in pregnancy results in a high incidence of major fetal malformations. Therefore, its use in pregnant patients is discouraged, and women of child-bearing age should use effective contraception.46
Cyclosporine
A randomized trial in a small number of patients suggested that cyclosporine is fairly effective as monotherapy.47 Its onset of action in myasthenia gravis is faster than that of other corticosteroid-sparing agents, and clinical benefit can often be observed as early as 1 to 2 months. A dose of 5 mg/kg/day and a maintenance serum level of 100 to 150 ng/mL are generally recommended. However, renal, hepatic, and hematologic toxicities and interactions with other medications make cyclosporine a less attractive choice.
Methotrexate
A randomized trial evaluated the utility of methotrexate as a steroid-sparing agent compared with azathioprine.48 At 24 months, its steroid-sparing effect was similar to that of azathioprine, and the prednisone dosage had been reduced in more than 50% of patients.
Another phase II trial studying the efficacy of methotrexate in myasthenia gravis is under way.49
Rituximab
Rituximab is a monoclonal antibody against B-cell membrane marker CD20. A growing number of case series support its efficacy in patients with severe generalized myasthenia gravis refractory to multiple immunosuppressants.16,50 It seems particularly effective for MuSK antibody-positive disease, reducing MuSK antibody titers and having a treatment effect that lasts for years.
The standard dosage is 375 mg/m2 per week for 4 consecutive weeks. Peripheral B cells tend to be depleted within 2 weeks after the first infusion, while T-cell populations remain unchanged.50
A minimal infusion reaction such as flushing and chills can be seen with the first infusion. Patients may be more susceptible to certain infections such as reactivation of herpes zoster, but overall rituximab is well tolerated. Rare cases of progressive multifocal leukoencephalopathy have been reported in patients taking it, but none have occurred so far in myasthenia gravis treatment.
Cyclophosphamide
Cyclophosphamide is an alkylating agent that reduces proliferation of both B and T cells. It can be effective in myasthenia gravis, but potentially serious side effects limit its use. It should be reserved for the small percentage of cases that are refractory to other immunotherapies.
Thymectomy
Surgical treatment should be considered for patients with thymoma. If the tumor cannot be surgically resected, chemoradiotherapy can be considered for relief of myasthenic symptoms and for prevention of local invasion.
Thymomas recur in a minority of patients many years after the initial resection, sometimes without myasthenia gravis symptoms. A recurrence of symptoms does not necessarily indicate a recurrence of thymoma. The lack of correlation between myasthenia gravis symptoms and thymoma recurrence highlights the importance of radiologic follow-up in these patients.
For patients without thymoma, many experts believe that thymectomy is beneficial in patients under age 60 who have generalized myasthenia gravis. The likelihood of medication-free remission is about twice as high, and the likelihood of becoming asymptomatic is about one and a half times higher after thymectomy.51 However, it takes up to several years for the benefits of thymectomy to manifest, and thymectomy does not guarantee protection from developing AChR antibody-positive myasthenia gravis in the future.
The optimal timing of thymectomy is not well established; however, the procedure is usually recommended within the first 3 years of diagnosis.52 The response rates from thymectomy are similar for AChR antibody-positive and seronegative patients. In general, thymectomy for MuSK antibody-positive patients has not been effective, and its role in ocular myasthenia gravis is unclear.2,53
- Alshekhlee A, Miles JD, Katirji B, Preston DC, Kaminski HJ. Incidence and mortality rates of myasthenia gravis and myasthenic crisis in US hospitals. Neurology 2009; 72:1548–1554.
- Keesey JC. Clinical evaluation and management of myasthenia gravis. Muscle Nerve 2004; 29:484–505.
- Leite MI, Coutinho E, Lana-Peixoto M, et al. Myasthenia gravis and neuromyelitis optica spectrum disorder: a multicenter study of 16 patients. Neurology 2012; 78:1601–1607.
- Drachman DB, Angus CW, Adams RN, Michelson JD, Hoffman GJ. Myasthenic antibodies cross-link acetylcholine receptors to accelerate degradation. N Engl J Med 1978; 298:1116–1122.
- Fujii Y. The thymus, thymoma and myasthenia gravis. Surg Today 2013; 43:461–466.
- Evoli A, Lindstrom J. Myasthenia gravis with antibodies to MuSK: another step toward solving mystery? Neurology 2011; 77:1783–1784.
- Mori S, Kubo S, Akiyoshi T, et al. Antibodies against muscle-specific kinase impair both presynaptic and postsynaptic functions in a murine model of myasthenia gravis. Am J Pathol 2012; 180:798–810.
- Guptill JT, Sanders DB, Evoli A. Anti-MuSK antibody myasthenia gravis: clinical findings and response to treatment in two large cohorts. Muscle Nerve 2011; 44:36–40.
- Chevessier F, Girard E, Molgó J, et al. A mouse model for congenital myasthenic syndrome due to MuSK mutations reveals defects in structure and function of neuromuscular junctions. Hum Mol Genet 2008; 17:3577–3595.
- Richman DP, Nishi K, Morell SW, et al. Acute severe animal model of anti-muscle-specific kinase myasthenia: combined postsynaptic and presynaptic changes. Arch Neurol 2012; 69:453–460.
- Klooster R, Plomp JJ, Huijbers MG, et al. Muscle-specific kinase myasthenia gravis IgG4 autoantibodies cause severe neuromuscular junction dysfunction in mice. Brain 2012; 135:1081–1101.
- Viegas S, Jacobson L, Waters P, et al. Passive and active immunization models of MuSK-Ab positive myasthenia: electrophysiological evidence for pre and postsynaptic defects. Exp Neurol 2012; 234:506–512.
- Niks EH, Kuks JB, Wokke JH, et al. Pre- and postsynaptic neuromuscular junction abnormalities in musk myasthenia. Muscle Nerve 2010; 42:283–288.
- Kawakami Y, Ito M, Hirayama M, et al. Anti-MuSK autoantibodies block binding of collagen Q to MuSK. Neurology 2011; 77:1819–1826.
- Chan KH, Lachance DH, Harper CM, Lennon VA. Frequency of seronegativity in adult-acquired generalized myasthenia gravis. Muscle Nerve 2007; 36:651–658.
- Collongues N, Casez O, Lacour A, et al. Rituximab in refractory and non-refractory myasthenia: a retrospective multicenter study. Muscle Nerve 2012; 46:687–691.
- Sanders DB, Andrews PI, Howard JF, Massey JM. Seronegative myasthenia gravis. Neurology 1997; 48(suppl 5):40S–45S.
- Shiraishi H, Motomura M, Yoshimura T, et al. Acetylcholine receptors loss and postsynaptic damage in MuSK antibody-positive myasthenia gravis. Ann Neurol 2005; 57:289–293.
- Leite MI, Jacob S, Viegas S, et al. IgG1 antibodies to acetylcholine receptors in ‘seronegative’ myasthenia gravis. Brain 2008; 131:1940–1952.
- Jacob S, Viegas S, Leite MI, et al. Presence and pathogenic relevance of antibodies to clustered acetylcholine receptor in ocular and generalized myasthenia gravis. Arch Neurol 2012; 69:994–1001.
- Higuchi O, Hamuro J, Motomura M, Yamanashi Y. Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann Neurol 2011; 69:418–422.
- Pevzner A, Schoser B, Peters K, et al. Anti-LRP4 autoantibodies in AChR- and MuSK-antibody-negative myasthenia gravis. J Neurol 2012; 259:427–435.
- Zhang B, Tzartos JS, Belimezi M, et al. Autoantibodies to lipoprotein-related protein 4 in patients with double-seronegative myasthenia gravis. Arch Neurol 2012; 69:445–451.
- Kupersmith MJ, Latkany R, Homel P. Development of generalized disease at 2 years in patients with ocular myasthenia gravis. Arch Neurol 2003; 60:243–248.
- Pasnoor M, Wolfe GI, Nations S, et al. Clinical findings in MuSK-antibody positive myasthenia gravis: a US experience. Muscle Nerve 2010; 41:370–374.
- Oh SJ, Kim DE, Kuruoglu R, Bradley RJ, Dwyer D. Diagnostic sensitivity of the laboratory tests in myasthenia gravis. Muscle Nerve 1992; 15:720–724.
- Sanders DB, Stålberg EV. AAEM minimonograph #25: single-fiber electromyography. Muscle Nerve 1996; 19:1069–1083.
- Lazo-Langner A, Espinosa-Poblano I, Tirado-Cárdenas N, et al. Therapeutic plasma exchange in Mexico: experience from a single institution. Am J Hematol 2002; 70:16–21.
- Carandina-Maffeis R, Nucci A, Marques JF, et al. Plasmapheresis in the treatment of myasthenia gravis: retrospective study of 26 patients. Arq Neuropsiquiatr 2004; 62:391–395.
- Zinman L, Ng E, Bril V. IV immunoglobulin in patients with myasthenia gravis: a randomized controlled trial. Neurology 2007; 68:837–841.
- Gajdos P, Tranchant C, Clair B, et al; Myasthenia Gravis Clinical Study Group. Treatment of myasthenia gravis exacerbation with intravenous immunoglobulin: a randomized double-blind clinical trial. Arch Neurol 2005; 62:1689–1693.
- Rønager J, Ravnborg M, Hermansen I, Vorstrup S. Immunoglobulin treatment versus plasma exchange in patients with chronic moderate to severe myasthenia gravis. Artif Organs 2001; 25:967–973.
- Barth D, Nabavi Nouri M, Ng E, Nwe P, Bril V. Comparison of IVIg and PLEX in patients with myasthenia gravis. Neurology 2011; 76:2017–2023.
- Wegner B, Ahmed I. Intravenous immunoglobulin monotherapy in long-term treatment of myasthenia gravis. Clin Neurol Neurosurg 2002; 105:3–8.
- Pascuzzi RM, Coslett HB, Johns TR. Long-term corticosteroid treatment of myasthenia gravis: report of 116 patients. Ann Neurol 1984; 15:291–298.
- Monsul NT, Patwa HS, Knorr AM, Lesser RL, Goldstein JM. The effect of prednisone on the progression from ocular to generalized myasthenia gravis. J Neurol Sci 2004; 217:131–133.
- Miller RG, Milner-Brown HS, Mirka A. Prednisone-induced worsening of neuromuscular function in myasthenia gravis. Neurology 1986; 36:729–732.
- Palace J, Newsom-Davis J, Lecky B. A randomized double-blind trial of prednisolone alone or with azathioprine in myasthenia gravis. Myasthenia Gravis Study Group. Neurology 1998; 50:1778–1783.
- Mertens HG, Hertel G, Reuther P, Ricker K. Effect of immunosuppressive drugs (azathioprine). Ann N Y Acad Sci 1981; 377:691–699.
- Relling MV, Gardner EE, Sandborn WJ, et al; Clinical Pharmacogenetics Implementation Consortium. Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clin Pharmacol Ther 2011; 89:387–391.
- Finelli PF. Primary CNS lymphoma in myasthenic on long-term azathioprine. J Neurooncol 2005; 74:91–92.
- Sanders DB, Hart IK, Mantegazza R, et al. An international, phase III, randomized trial of mycophenolate mofetil in myasthenia gravis. Neurology 2008; 71:400–406.
- Muscle Study Group. A trial of mycophenolate mofetil with prednisone as initial immunotherapy in myasthenia gravis. Neurology 2008; 71:394–399.
- Meriggioli MN, Ciafaloni E, Al-Hayk KA, et al. Mycophenolate mofetil for myasthenia gravis: an analysis of efficacy, safety, and tolerability. Neurology 2003; 61:1438–1440.
- Hehir MK, Burns TM, Alpers J, Conaway MR, Sawa M, Sanders DB. Mycophenolate mofetil in AChR-antibody-positive myasthenia gravis: outcomes in 102 patients. Muscle Nerve 2010; 41:593–598.
- Merlob P, Stahl B, Klinger G. Tetrada of the possible mycophenolate mofetil embryopathy: a review. Reprod Toxicol 2009; 28:105–108.
- Tindall RS, Rollins JA, Phillips JT, Greenlee RG, Wells L, Belendiuk G. Preliminary results of a double-blind, randomized, placebo-controlled trial of cyclosporine in myasthenia gravis. N Engl J Med 1987; 316:719–724.
- Heckmann JM, Rawoot A, Bateman K, Renison R, Badri M. A single-blinded trial of methotrexate versus azathioprine as steroid-sparing agents in generalized myasthenia gravis. BMC Neurol 2011; 11:97.
- Pasnoor M, He J, Herbelin L, Dimachkie M, Barohn RJ; Muscle Study Group. Phase II trial of methotrexate in myasthenia gravis. Ann N Y Acad Sci 2012; 1275:23–28.
- Díaz-Manera J, Martínez-Hernández E, Querol L, et al. Long-lasting treatment effect of rituximab in MuSK myasthenia. Neurology 2012; 78:189–193.
- Gronseth GS, Barohn RJ. Practice parameter: thymectomy for autoimmune myasthenia gravis (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55:7–15.
- Kumar V, Kaminski HJ. Treatment of myasthenia gravis. Curr Neurol Neurosci Rep 2011; 11:89–96.
- Pompeo E, Tacconi F, Massa R, Mineo D, Nahmias S, Mineo TC. Long-term outcome of thoracoscopic extended thymectomy for nonthymomatous myasthenia gravis. Eur J Cardiothorac Surg 2009; 36:164–169.
- Alshekhlee A, Miles JD, Katirji B, Preston DC, Kaminski HJ. Incidence and mortality rates of myasthenia gravis and myasthenic crisis in US hospitals. Neurology 2009; 72:1548–1554.
- Keesey JC. Clinical evaluation and management of myasthenia gravis. Muscle Nerve 2004; 29:484–505.
- Leite MI, Coutinho E, Lana-Peixoto M, et al. Myasthenia gravis and neuromyelitis optica spectrum disorder: a multicenter study of 16 patients. Neurology 2012; 78:1601–1607.
- Drachman DB, Angus CW, Adams RN, Michelson JD, Hoffman GJ. Myasthenic antibodies cross-link acetylcholine receptors to accelerate degradation. N Engl J Med 1978; 298:1116–1122.
- Fujii Y. The thymus, thymoma and myasthenia gravis. Surg Today 2013; 43:461–466.
- Evoli A, Lindstrom J. Myasthenia gravis with antibodies to MuSK: another step toward solving mystery? Neurology 2011; 77:1783–1784.
- Mori S, Kubo S, Akiyoshi T, et al. Antibodies against muscle-specific kinase impair both presynaptic and postsynaptic functions in a murine model of myasthenia gravis. Am J Pathol 2012; 180:798–810.
- Guptill JT, Sanders DB, Evoli A. Anti-MuSK antibody myasthenia gravis: clinical findings and response to treatment in two large cohorts. Muscle Nerve 2011; 44:36–40.
- Chevessier F, Girard E, Molgó J, et al. A mouse model for congenital myasthenic syndrome due to MuSK mutations reveals defects in structure and function of neuromuscular junctions. Hum Mol Genet 2008; 17:3577–3595.
- Richman DP, Nishi K, Morell SW, et al. Acute severe animal model of anti-muscle-specific kinase myasthenia: combined postsynaptic and presynaptic changes. Arch Neurol 2012; 69:453–460.
- Klooster R, Plomp JJ, Huijbers MG, et al. Muscle-specific kinase myasthenia gravis IgG4 autoantibodies cause severe neuromuscular junction dysfunction in mice. Brain 2012; 135:1081–1101.
- Viegas S, Jacobson L, Waters P, et al. Passive and active immunization models of MuSK-Ab positive myasthenia: electrophysiological evidence for pre and postsynaptic defects. Exp Neurol 2012; 234:506–512.
- Niks EH, Kuks JB, Wokke JH, et al. Pre- and postsynaptic neuromuscular junction abnormalities in musk myasthenia. Muscle Nerve 2010; 42:283–288.
- Kawakami Y, Ito M, Hirayama M, et al. Anti-MuSK autoantibodies block binding of collagen Q to MuSK. Neurology 2011; 77:1819–1826.
- Chan KH, Lachance DH, Harper CM, Lennon VA. Frequency of seronegativity in adult-acquired generalized myasthenia gravis. Muscle Nerve 2007; 36:651–658.
- Collongues N, Casez O, Lacour A, et al. Rituximab in refractory and non-refractory myasthenia: a retrospective multicenter study. Muscle Nerve 2012; 46:687–691.
- Sanders DB, Andrews PI, Howard JF, Massey JM. Seronegative myasthenia gravis. Neurology 1997; 48(suppl 5):40S–45S.
- Shiraishi H, Motomura M, Yoshimura T, et al. Acetylcholine receptors loss and postsynaptic damage in MuSK antibody-positive myasthenia gravis. Ann Neurol 2005; 57:289–293.
- Leite MI, Jacob S, Viegas S, et al. IgG1 antibodies to acetylcholine receptors in ‘seronegative’ myasthenia gravis. Brain 2008; 131:1940–1952.
- Jacob S, Viegas S, Leite MI, et al. Presence and pathogenic relevance of antibodies to clustered acetylcholine receptor in ocular and generalized myasthenia gravis. Arch Neurol 2012; 69:994–1001.
- Higuchi O, Hamuro J, Motomura M, Yamanashi Y. Autoantibodies to low-density lipoprotein receptor-related protein 4 in myasthenia gravis. Ann Neurol 2011; 69:418–422.
- Pevzner A, Schoser B, Peters K, et al. Anti-LRP4 autoantibodies in AChR- and MuSK-antibody-negative myasthenia gravis. J Neurol 2012; 259:427–435.
- Zhang B, Tzartos JS, Belimezi M, et al. Autoantibodies to lipoprotein-related protein 4 in patients with double-seronegative myasthenia gravis. Arch Neurol 2012; 69:445–451.
- Kupersmith MJ, Latkany R, Homel P. Development of generalized disease at 2 years in patients with ocular myasthenia gravis. Arch Neurol 2003; 60:243–248.
- Pasnoor M, Wolfe GI, Nations S, et al. Clinical findings in MuSK-antibody positive myasthenia gravis: a US experience. Muscle Nerve 2010; 41:370–374.
- Oh SJ, Kim DE, Kuruoglu R, Bradley RJ, Dwyer D. Diagnostic sensitivity of the laboratory tests in myasthenia gravis. Muscle Nerve 1992; 15:720–724.
- Sanders DB, Stålberg EV. AAEM minimonograph #25: single-fiber electromyography. Muscle Nerve 1996; 19:1069–1083.
- Lazo-Langner A, Espinosa-Poblano I, Tirado-Cárdenas N, et al. Therapeutic plasma exchange in Mexico: experience from a single institution. Am J Hematol 2002; 70:16–21.
- Carandina-Maffeis R, Nucci A, Marques JF, et al. Plasmapheresis in the treatment of myasthenia gravis: retrospective study of 26 patients. Arq Neuropsiquiatr 2004; 62:391–395.
- Zinman L, Ng E, Bril V. IV immunoglobulin in patients with myasthenia gravis: a randomized controlled trial. Neurology 2007; 68:837–841.
- Gajdos P, Tranchant C, Clair B, et al; Myasthenia Gravis Clinical Study Group. Treatment of myasthenia gravis exacerbation with intravenous immunoglobulin: a randomized double-blind clinical trial. Arch Neurol 2005; 62:1689–1693.
- Rønager J, Ravnborg M, Hermansen I, Vorstrup S. Immunoglobulin treatment versus plasma exchange in patients with chronic moderate to severe myasthenia gravis. Artif Organs 2001; 25:967–973.
- Barth D, Nabavi Nouri M, Ng E, Nwe P, Bril V. Comparison of IVIg and PLEX in patients with myasthenia gravis. Neurology 2011; 76:2017–2023.
- Wegner B, Ahmed I. Intravenous immunoglobulin monotherapy in long-term treatment of myasthenia gravis. Clin Neurol Neurosurg 2002; 105:3–8.
- Pascuzzi RM, Coslett HB, Johns TR. Long-term corticosteroid treatment of myasthenia gravis: report of 116 patients. Ann Neurol 1984; 15:291–298.
- Monsul NT, Patwa HS, Knorr AM, Lesser RL, Goldstein JM. The effect of prednisone on the progression from ocular to generalized myasthenia gravis. J Neurol Sci 2004; 217:131–133.
- Miller RG, Milner-Brown HS, Mirka A. Prednisone-induced worsening of neuromuscular function in myasthenia gravis. Neurology 1986; 36:729–732.
- Palace J, Newsom-Davis J, Lecky B. A randomized double-blind trial of prednisolone alone or with azathioprine in myasthenia gravis. Myasthenia Gravis Study Group. Neurology 1998; 50:1778–1783.
- Mertens HG, Hertel G, Reuther P, Ricker K. Effect of immunosuppressive drugs (azathioprine). Ann N Y Acad Sci 1981; 377:691–699.
- Relling MV, Gardner EE, Sandborn WJ, et al; Clinical Pharmacogenetics Implementation Consortium. Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clin Pharmacol Ther 2011; 89:387–391.
- Finelli PF. Primary CNS lymphoma in myasthenic on long-term azathioprine. J Neurooncol 2005; 74:91–92.
- Sanders DB, Hart IK, Mantegazza R, et al. An international, phase III, randomized trial of mycophenolate mofetil in myasthenia gravis. Neurology 2008; 71:400–406.
- Muscle Study Group. A trial of mycophenolate mofetil with prednisone as initial immunotherapy in myasthenia gravis. Neurology 2008; 71:394–399.
- Meriggioli MN, Ciafaloni E, Al-Hayk KA, et al. Mycophenolate mofetil for myasthenia gravis: an analysis of efficacy, safety, and tolerability. Neurology 2003; 61:1438–1440.
- Hehir MK, Burns TM, Alpers J, Conaway MR, Sawa M, Sanders DB. Mycophenolate mofetil in AChR-antibody-positive myasthenia gravis: outcomes in 102 patients. Muscle Nerve 2010; 41:593–598.
- Merlob P, Stahl B, Klinger G. Tetrada of the possible mycophenolate mofetil embryopathy: a review. Reprod Toxicol 2009; 28:105–108.
- Tindall RS, Rollins JA, Phillips JT, Greenlee RG, Wells L, Belendiuk G. Preliminary results of a double-blind, randomized, placebo-controlled trial of cyclosporine in myasthenia gravis. N Engl J Med 1987; 316:719–724.
- Heckmann JM, Rawoot A, Bateman K, Renison R, Badri M. A single-blinded trial of methotrexate versus azathioprine as steroid-sparing agents in generalized myasthenia gravis. BMC Neurol 2011; 11:97.
- Pasnoor M, He J, Herbelin L, Dimachkie M, Barohn RJ; Muscle Study Group. Phase II trial of methotrexate in myasthenia gravis. Ann N Y Acad Sci 2012; 1275:23–28.
- Díaz-Manera J, Martínez-Hernández E, Querol L, et al. Long-lasting treatment effect of rituximab in MuSK myasthenia. Neurology 2012; 78:189–193.
- Gronseth GS, Barohn RJ. Practice parameter: thymectomy for autoimmune myasthenia gravis (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55:7–15.
- Kumar V, Kaminski HJ. Treatment of myasthenia gravis. Curr Neurol Neurosci Rep 2011; 11:89–96.
- Pompeo E, Tacconi F, Massa R, Mineo D, Nahmias S, Mineo TC. Long-term outcome of thoracoscopic extended thymectomy for nonthymomatous myasthenia gravis. Eur J Cardiothorac Surg 2009; 36:164–169.
KEY POINTS
- In most cases of myasthenia gravis, the patient has antibodies against acetylcholine receptor (AChR) or musclespecific tyrosine kinase (MuSK).
- Myasthenia gravis is diagnosed by clinical signs, bedside tests (the ice-pack test or the edrophonium test), serologic tests for AChR antibodies or MuSK antibodies, and electrophysiologic tests.
- Acetylcholinesterase inhibitors are the first-step therapy, but patients who have moderate to severe symptoms require some form of immunomodulating therapy.
- A number of drugs can exacerbate weakness in myasthenia gravis and should be avoided or used with caution. These include penicillamine, interferons, procainamide, quinidine, and antibiotics such as quinolones and aminoglycosides.
HPV Vaccine Uptake Low in Autoimmune Disease Patients
SAN DIEGO – Only 8.5% of children and young adults with autoimmune diseases and 9.1% of those without such diseases received one or more doses of the human papillomavirus vaccine, a large analysis of national claims data showed.
"Despite the high efficacy of HPV vaccine in preventing cervical cancer and clinically acceptable safety profile in the general population, the vast majority of patients aged 9-26 in our study cohort with and without autoimmune diseases did not receive the HPV vaccine," Dr. Seoyoung C. Kim said in an interview prior to the annual meeting of the American College of Rheumatology, where the study was presented.
"Patients at high risk of persistent HPV infection should be encouraged to receive the vaccine, although future study is needed to determine the effectiveness of HPV vaccine in patients with autoimmune diseases, particularly those on immunosuppressive drugs," she added.
In 2006 and 2009, two three-dose series HPV vaccines were approved for use in males and females aged 9-26 years. Prior research has suggested that patients with lupus or inflammatory bowel disease or those who take immunosuppressive agents have a higher risk of persistent HPV infection or cervical dysplasia, said Dr. Kim of the division of pharmacoepidemiology and pharmacoeconomics in the department of medicine at Brigham and Women’s Hospital, Boston.
"HPV vaccine has been available for the past several years in the U.S. and in other countries," she said. "As far as we know, there has not been any study looking at the uptake of HPV vaccine in the autoimmune disease population."
Using United HealthCare national claims data for 2005-2012, Dr. Kim and her associates identified patients aged 9-26 years with at least 1 year of continuous enrollment who had at least two autoimmune disease diagnosis codes 7 or more days apart. Vaccination was defined as one or more vaccine codes after 2006, and the researchers accounted for coexisting diseases, use of health care treatments, and geographic regions when assessing vaccine uptake.
Dr. Kim, the study’s senior investigator, reported data for 29,255 children and young adults with autoimmune diseases and 117,020 without. The mean age was 19 years, and 59% were female. Patients in the autoimmune diseases group had a higher number of physician visits, abnormal pap smears, and sexually transmitted diseases, compared with their counterparts without autoimmune disease (all P values less than .01).
Overall, autoimmune disease patients and their counterparts had similarly low uptake of at least one vaccine dose (8.5% vs. 9.1%, respectively; P = .34). The uptake was higher among females in both groups (13.1% vs. 14.1%, respectively; P less than .01), yet fewer than 5% of female patients in both groups completed a three-dose vaccine series (4.7% vs. 4.6%; P = .57). A higher percentage of patients in the Northeast received one or more HPV vaccine doses (16.3% vs. 11.8%; P = .02); otherwise vaccinations were equally distributed from a geographic standpoint.
In a subgroup of female patients who had at least 2 years of follow-up, 20.6% with autoimmune disease and 23.1% without autoimmune disease received at least one vaccine dose. Of those, 53.1% and 51.4%, respectively, completed the series.
"We were generally surprised to see how low the uptake has been in both autoimmune and nonautoimmune populations," Dr. Kim said. She acknowledged certain limitations of the study, including the fact that it was conducting using the claims data from United HealthCare, "so it only captures patients who used the insurance card to pay for the vaccine," she said. "However, given the high cost of the HPV vaccine, this limitation is probably not substantial. We [also] did not have information on race/ethnicity."
Dr. Kim disclosed that she is supported by a grant from the National Institutes of Health. She received a research grant from Pfizer and tuition support for the pharmacoepidemiology program at the Harvard School of Public Health, which is funded by Pfizer, Millennium Pharma, and Asisa.
persistent HPV infection, immunosuppressive drugs,
SAN DIEGO – Only 8.5% of children and young adults with autoimmune diseases and 9.1% of those without such diseases received one or more doses of the human papillomavirus vaccine, a large analysis of national claims data showed.
"Despite the high efficacy of HPV vaccine in preventing cervical cancer and clinically acceptable safety profile in the general population, the vast majority of patients aged 9-26 in our study cohort with and without autoimmune diseases did not receive the HPV vaccine," Dr. Seoyoung C. Kim said in an interview prior to the annual meeting of the American College of Rheumatology, where the study was presented.
"Patients at high risk of persistent HPV infection should be encouraged to receive the vaccine, although future study is needed to determine the effectiveness of HPV vaccine in patients with autoimmune diseases, particularly those on immunosuppressive drugs," she added.
In 2006 and 2009, two three-dose series HPV vaccines were approved for use in males and females aged 9-26 years. Prior research has suggested that patients with lupus or inflammatory bowel disease or those who take immunosuppressive agents have a higher risk of persistent HPV infection or cervical dysplasia, said Dr. Kim of the division of pharmacoepidemiology and pharmacoeconomics in the department of medicine at Brigham and Women’s Hospital, Boston.
"HPV vaccine has been available for the past several years in the U.S. and in other countries," she said. "As far as we know, there has not been any study looking at the uptake of HPV vaccine in the autoimmune disease population."
Using United HealthCare national claims data for 2005-2012, Dr. Kim and her associates identified patients aged 9-26 years with at least 1 year of continuous enrollment who had at least two autoimmune disease diagnosis codes 7 or more days apart. Vaccination was defined as one or more vaccine codes after 2006, and the researchers accounted for coexisting diseases, use of health care treatments, and geographic regions when assessing vaccine uptake.
Dr. Kim, the study’s senior investigator, reported data for 29,255 children and young adults with autoimmune diseases and 117,020 without. The mean age was 19 years, and 59% were female. Patients in the autoimmune diseases group had a higher number of physician visits, abnormal pap smears, and sexually transmitted diseases, compared with their counterparts without autoimmune disease (all P values less than .01).
Overall, autoimmune disease patients and their counterparts had similarly low uptake of at least one vaccine dose (8.5% vs. 9.1%, respectively; P = .34). The uptake was higher among females in both groups (13.1% vs. 14.1%, respectively; P less than .01), yet fewer than 5% of female patients in both groups completed a three-dose vaccine series (4.7% vs. 4.6%; P = .57). A higher percentage of patients in the Northeast received one or more HPV vaccine doses (16.3% vs. 11.8%; P = .02); otherwise vaccinations were equally distributed from a geographic standpoint.
In a subgroup of female patients who had at least 2 years of follow-up, 20.6% with autoimmune disease and 23.1% without autoimmune disease received at least one vaccine dose. Of those, 53.1% and 51.4%, respectively, completed the series.
"We were generally surprised to see how low the uptake has been in both autoimmune and nonautoimmune populations," Dr. Kim said. She acknowledged certain limitations of the study, including the fact that it was conducting using the claims data from United HealthCare, "so it only captures patients who used the insurance card to pay for the vaccine," she said. "However, given the high cost of the HPV vaccine, this limitation is probably not substantial. We [also] did not have information on race/ethnicity."
Dr. Kim disclosed that she is supported by a grant from the National Institutes of Health. She received a research grant from Pfizer and tuition support for the pharmacoepidemiology program at the Harvard School of Public Health, which is funded by Pfizer, Millennium Pharma, and Asisa.
SAN DIEGO – Only 8.5% of children and young adults with autoimmune diseases and 9.1% of those without such diseases received one or more doses of the human papillomavirus vaccine, a large analysis of national claims data showed.
"Despite the high efficacy of HPV vaccine in preventing cervical cancer and clinically acceptable safety profile in the general population, the vast majority of patients aged 9-26 in our study cohort with and without autoimmune diseases did not receive the HPV vaccine," Dr. Seoyoung C. Kim said in an interview prior to the annual meeting of the American College of Rheumatology, where the study was presented.
"Patients at high risk of persistent HPV infection should be encouraged to receive the vaccine, although future study is needed to determine the effectiveness of HPV vaccine in patients with autoimmune diseases, particularly those on immunosuppressive drugs," she added.
In 2006 and 2009, two three-dose series HPV vaccines were approved for use in males and females aged 9-26 years. Prior research has suggested that patients with lupus or inflammatory bowel disease or those who take immunosuppressive agents have a higher risk of persistent HPV infection or cervical dysplasia, said Dr. Kim of the division of pharmacoepidemiology and pharmacoeconomics in the department of medicine at Brigham and Women’s Hospital, Boston.
"HPV vaccine has been available for the past several years in the U.S. and in other countries," she said. "As far as we know, there has not been any study looking at the uptake of HPV vaccine in the autoimmune disease population."
Using United HealthCare national claims data for 2005-2012, Dr. Kim and her associates identified patients aged 9-26 years with at least 1 year of continuous enrollment who had at least two autoimmune disease diagnosis codes 7 or more days apart. Vaccination was defined as one or more vaccine codes after 2006, and the researchers accounted for coexisting diseases, use of health care treatments, and geographic regions when assessing vaccine uptake.
Dr. Kim, the study’s senior investigator, reported data for 29,255 children and young adults with autoimmune diseases and 117,020 without. The mean age was 19 years, and 59% were female. Patients in the autoimmune diseases group had a higher number of physician visits, abnormal pap smears, and sexually transmitted diseases, compared with their counterparts without autoimmune disease (all P values less than .01).
Overall, autoimmune disease patients and their counterparts had similarly low uptake of at least one vaccine dose (8.5% vs. 9.1%, respectively; P = .34). The uptake was higher among females in both groups (13.1% vs. 14.1%, respectively; P less than .01), yet fewer than 5% of female patients in both groups completed a three-dose vaccine series (4.7% vs. 4.6%; P = .57). A higher percentage of patients in the Northeast received one or more HPV vaccine doses (16.3% vs. 11.8%; P = .02); otherwise vaccinations were equally distributed from a geographic standpoint.
In a subgroup of female patients who had at least 2 years of follow-up, 20.6% with autoimmune disease and 23.1% without autoimmune disease received at least one vaccine dose. Of those, 53.1% and 51.4%, respectively, completed the series.
"We were generally surprised to see how low the uptake has been in both autoimmune and nonautoimmune populations," Dr. Kim said. She acknowledged certain limitations of the study, including the fact that it was conducting using the claims data from United HealthCare, "so it only captures patients who used the insurance card to pay for the vaccine," she said. "However, given the high cost of the HPV vaccine, this limitation is probably not substantial. We [also] did not have information on race/ethnicity."
Dr. Kim disclosed that she is supported by a grant from the National Institutes of Health. She received a research grant from Pfizer and tuition support for the pharmacoepidemiology program at the Harvard School of Public Health, which is funded by Pfizer, Millennium Pharma, and Asisa.
persistent HPV infection, immunosuppressive drugs,
persistent HPV infection, immunosuppressive drugs,
AT THE ACR ANNUAL MEETING

Meningococcal Vaccine for At-risk Infants
The quadrivalent meningococcal vaccine MenACWY-CRM, or Menveo, may now be given to infants aged 2-23 months who are considered at high risk for meningococcal disease or who travel to areas where it is hyperendemic or epidemic, according to the recommendations of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
High-risk children are those with component complement deficiency, HIV infection, or anatomic or functional asplenia. Children in an outbreak of a vaccine-preventable meningitis serogroup also should receive the series. About 5,000 infants per year fit into these categories.
The Advisory Committee on Immunization Practices (ACIP) approved the decision by a vote of 13-1, with one abstention. The decision aligns ACIP’s recommendation with the recently expanded indication for the vaccine, which protects against serotypes A, C, W-135, and Y. In August, the Food and Drug Administration approved the vaccine for infants and toddlers older than 2 months.
However, because of the extremely low incidence of meningococcal disease in children in the United States, the committee did not recommend it for all healthy children. "Very few children are considered at increased risk, so a routine recommendation would prevent just a very low number of cases," said Jessica MacNeil, an epidemiologist with the CDC.
The FDA licensing of MenACWY-CRM and ACIP’s recommendation give pediatricians a third option for infant meningococcal vaccination. HibMenCY-TT (MenHibrix) and MenACWY-D (Menactra) are also approved for some of these same indications. However, Ms. MacNeil noted, Menactra cannot be used in children with asplenia, and MenHibrix can’t be used for travel or as a booster dose.
The committee based its decision on three phase III safety and efficacy trials. These studies comprised nearly 11,000 infants – 9,000 of whom had the four-dose series and 2,000 of whom had a two-dose series, said Dr. Peter Dull of Novartis Vaccines.
The studies confirmed an average 90% efficacy against all four serotypes after the 12-month dose. By 40 months of age, efficacy had waned somewhat: 10% of infants had a seroresponse to type A; 34%, to type C; 76%, to type W-135; and 67%, to type Y. Of the strains included in the vaccine, types C, Y, and W-135 cause 75% of meningococcal disease in those aged 11 years and older.
Dr. Dull said that Novartis is following a cohort that received the vaccine as infants; next year, 60-month immunogenicity data will be available.
After adjustment for some confounders, the vaccine did not significantly interact with the immunogenic potential of other recommended childhood vaccines. Novartis studies also found it safe. Up to 60% of children had mild to moderate injection site reactions. The incidence of systemic reactions was no different from that for routine vaccines alone.
There were 11 serious adverse events possibly related to the vaccine among the 5,000 children included in the safety analyses. These included acute encephalomyelitis, cellulitis, complex partial seizure, epilepsy, febrile seizure, and Kawasaki disease. Ten deaths occurred, but were not considered vaccine related.
The recommended dosing schedule will be:
• Aged 2-6 months: Four doses at 2, 4, 6, and 12 months.
• Aged 7-23 months: Two doses with the second dose given in the second year of life.
• Aged 2-11 years: One or two doses.
Boosters should be given to those who remain at risk, beginning at 3 years after the primary series and then every 5 years thereafter.
The committee also agreed, by a vote of 14 with one abstention, to include MenACWY-CRM in the Vaccines for Children program.
One member who voted disclosed that her institution receives research funding from drug companies. None of the other voting members had any relevant financial disclosures.
The quadrivalent meningococcal vaccine MenACWY-CRM, or Menveo, may now be given to infants aged 2-23 months who are considered at high risk for meningococcal disease or who travel to areas where it is hyperendemic or epidemic, according to the recommendations of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
High-risk children are those with component complement deficiency, HIV infection, or anatomic or functional asplenia. Children in an outbreak of a vaccine-preventable meningitis serogroup also should receive the series. About 5,000 infants per year fit into these categories.
The Advisory Committee on Immunization Practices (ACIP) approved the decision by a vote of 13-1, with one abstention. The decision aligns ACIP’s recommendation with the recently expanded indication for the vaccine, which protects against serotypes A, C, W-135, and Y. In August, the Food and Drug Administration approved the vaccine for infants and toddlers older than 2 months.
However, because of the extremely low incidence of meningococcal disease in children in the United States, the committee did not recommend it for all healthy children. "Very few children are considered at increased risk, so a routine recommendation would prevent just a very low number of cases," said Jessica MacNeil, an epidemiologist with the CDC.
The FDA licensing of MenACWY-CRM and ACIP’s recommendation give pediatricians a third option for infant meningococcal vaccination. HibMenCY-TT (MenHibrix) and MenACWY-D (Menactra) are also approved for some of these same indications. However, Ms. MacNeil noted, Menactra cannot be used in children with asplenia, and MenHibrix can’t be used for travel or as a booster dose.
The committee based its decision on three phase III safety and efficacy trials. These studies comprised nearly 11,000 infants – 9,000 of whom had the four-dose series and 2,000 of whom had a two-dose series, said Dr. Peter Dull of Novartis Vaccines.
The studies confirmed an average 90% efficacy against all four serotypes after the 12-month dose. By 40 months of age, efficacy had waned somewhat: 10% of infants had a seroresponse to type A; 34%, to type C; 76%, to type W-135; and 67%, to type Y. Of the strains included in the vaccine, types C, Y, and W-135 cause 75% of meningococcal disease in those aged 11 years and older.
Dr. Dull said that Novartis is following a cohort that received the vaccine as infants; next year, 60-month immunogenicity data will be available.
After adjustment for some confounders, the vaccine did not significantly interact with the immunogenic potential of other recommended childhood vaccines. Novartis studies also found it safe. Up to 60% of children had mild to moderate injection site reactions. The incidence of systemic reactions was no different from that for routine vaccines alone.
There were 11 serious adverse events possibly related to the vaccine among the 5,000 children included in the safety analyses. These included acute encephalomyelitis, cellulitis, complex partial seizure, epilepsy, febrile seizure, and Kawasaki disease. Ten deaths occurred, but were not considered vaccine related.
The recommended dosing schedule will be:
• Aged 2-6 months: Four doses at 2, 4, 6, and 12 months.
• Aged 7-23 months: Two doses with the second dose given in the second year of life.
• Aged 2-11 years: One or two doses.
Boosters should be given to those who remain at risk, beginning at 3 years after the primary series and then every 5 years thereafter.
The committee also agreed, by a vote of 14 with one abstention, to include MenACWY-CRM in the Vaccines for Children program.
One member who voted disclosed that her institution receives research funding from drug companies. None of the other voting members had any relevant financial disclosures.
The quadrivalent meningococcal vaccine MenACWY-CRM, or Menveo, may now be given to infants aged 2-23 months who are considered at high risk for meningococcal disease or who travel to areas where it is hyperendemic or epidemic, according to the recommendations of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
High-risk children are those with component complement deficiency, HIV infection, or anatomic or functional asplenia. Children in an outbreak of a vaccine-preventable meningitis serogroup also should receive the series. About 5,000 infants per year fit into these categories.
The Advisory Committee on Immunization Practices (ACIP) approved the decision by a vote of 13-1, with one abstention. The decision aligns ACIP’s recommendation with the recently expanded indication for the vaccine, which protects against serotypes A, C, W-135, and Y. In August, the Food and Drug Administration approved the vaccine for infants and toddlers older than 2 months.
However, because of the extremely low incidence of meningococcal disease in children in the United States, the committee did not recommend it for all healthy children. "Very few children are considered at increased risk, so a routine recommendation would prevent just a very low number of cases," said Jessica MacNeil, an epidemiologist with the CDC.
The FDA licensing of MenACWY-CRM and ACIP’s recommendation give pediatricians a third option for infant meningococcal vaccination. HibMenCY-TT (MenHibrix) and MenACWY-D (Menactra) are also approved for some of these same indications. However, Ms. MacNeil noted, Menactra cannot be used in children with asplenia, and MenHibrix can’t be used for travel or as a booster dose.
The committee based its decision on three phase III safety and efficacy trials. These studies comprised nearly 11,000 infants – 9,000 of whom had the four-dose series and 2,000 of whom had a two-dose series, said Dr. Peter Dull of Novartis Vaccines.
The studies confirmed an average 90% efficacy against all four serotypes after the 12-month dose. By 40 months of age, efficacy had waned somewhat: 10% of infants had a seroresponse to type A; 34%, to type C; 76%, to type W-135; and 67%, to type Y. Of the strains included in the vaccine, types C, Y, and W-135 cause 75% of meningococcal disease in those aged 11 years and older.
Dr. Dull said that Novartis is following a cohort that received the vaccine as infants; next year, 60-month immunogenicity data will be available.
After adjustment for some confounders, the vaccine did not significantly interact with the immunogenic potential of other recommended childhood vaccines. Novartis studies also found it safe. Up to 60% of children had mild to moderate injection site reactions. The incidence of systemic reactions was no different from that for routine vaccines alone.
There were 11 serious adverse events possibly related to the vaccine among the 5,000 children included in the safety analyses. These included acute encephalomyelitis, cellulitis, complex partial seizure, epilepsy, febrile seizure, and Kawasaki disease. Ten deaths occurred, but were not considered vaccine related.
The recommended dosing schedule will be:
• Aged 2-6 months: Four doses at 2, 4, 6, and 12 months.
• Aged 7-23 months: Two doses with the second dose given in the second year of life.
• Aged 2-11 years: One or two doses.
Boosters should be given to those who remain at risk, beginning at 3 years after the primary series and then every 5 years thereafter.
The committee also agreed, by a vote of 14 with one abstention, to include MenACWY-CRM in the Vaccines for Children program.
One member who voted disclosed that her institution receives research funding from drug companies. None of the other voting members had any relevant financial disclosures.
AT ACIP

Consider MRSA in Skin and Soft Tissue Infections
WASHINGTON – Community-acquired methicillin-resistant Staphylococcus aureus should be considered in the differential diagnosis of skin and soft tissue infections, as well as neonatal eye infections, Dr. Morven Edwards said at a practical pediatrics meeting sponsored by the American Academy of Pediatrics.
Dr. Edwards, an infectious disease specialist at Texas Children’s Hospital, Houston, said that unlike a decade ago, she now considers community-acquired MRSA as a possible cause "in almost any manifestation of a problem with the skin or soft tissue, even including those entities that we used to think were caused by other microorganisms."
For example, in the past, perianal dermatitis in a young infant "was essentially a pathognomonic presentation for group A strep infection," which did not even require a culture for an accurate diagnosis and appropriate treatment, said Dr. Edwards, who is a professor of pediatrics at Baylor College of Medicine, Houston.
She referred to a small retrospective study of children between the ages of 5 months and 12 years with perianal erythema, which found that the dominant culture results were MRSA and methicillin-sensitive S. aureus (MSSA), some streptococci, and some mixed infections. In the past, staphylococcal skin and soft tissue infections were considered uncommon among healthy term newborns discharged home, "unless it was just a very mild diaper dermatitis," she noted.
In a 2006 study of healthy term babies who returned to the hospital within a month of discharge to Texas Children’s Hospital’s emergency department, cases of MRSA peaked at 8-12 days after discharge. Almost all were skin and soft tissue infections (SSTIs), and some of the babies had mild, pustular skin disease and were treated as outpatients with topical therapy and/or oral antistaphylococcal medications. But almost 40% required admission for incision and drainage and parenteral antibiotic therapy.
Dr. Edwards referred to a case of an SSTI that started with a stubbed toe and progressed to a disseminated staphylococcal infection and endocarditis – illustrating that "even with an apparently limited minor staph infection, it always should go through our minds that this could be one that’s more serious."
The healthy teenage boy had stubbed his toe during a wrestling match, then developed fever, fatigue, and buttock and back pain, along with swelling and pain in the toe 4 days later. A fracture was diagnosed at an urgent care clinic, and he was sent home, but 9 days after the initial injury, symptoms persisted and he was admitted to the hospital for treatment with broad-spectrum antimicrobials, including clindamycin.
On the fourth day in the hospital, he had a fever of 104° F, "massive" facial swelling, bibasilar crackles, a systolic murmur, left lower quadrant pain, and a large parietal abscess seen on MRI. He had vegetations on the anterior leaflet of the mitral valve and multiple microemboli to the brain. The abscess was drained, and he had a vegetectomy, where vegetation was "peeled" off the leaflet, leaving the valve intact. After 6 weeks of intravenous antimicrobial treatment, he did well and was discharged.
"The lesson is that a seemingly innocuous SSTI always has the potential to disseminate," Dr. Edwards said, adding that while this is very uncommon, especially in a healthy child, "it’s always something to keep in mind."
Transmitted by direct contact, risk factors for community-acquired MRSA include chronic skin conditions, participation in sports teams that involve close contact with other players, and a history of such infections in family members, she noted.
In infants, MRSA infection also should be included in the differential diagnosis of ophthalmia neonatorum, Dr. Edwards said. She described the case of a healthy term 4-day-old baby who presented with eye swelling and purulent discharge, but no other systemic findings. The mother’s pregnancy had been uncomplicated; maternal tests were negative for group B streptococcus, chlamydia, and Neisseria gonorrhoea; and the baby had been discharged home by the second day after a normal vaginal birth.
The cause turned out to be community-acquired MRSA infection. "We need to consider this diagnosis with a higher index of suspicion in young infants now," she said, noting that the peak onset is at age 4-6 days, and it is characterized by a purulent discharge not likely to be a gonococcal infection. The baby was admitted to the hospital and treated with parenteral antimicrobial therapy.
Dr. Edwards disclosed that she is a consultant for and has received research funds from Novartis related to the development of a group B streptococcus vaccine.
WASHINGTON – Community-acquired methicillin-resistant Staphylococcus aureus should be considered in the differential diagnosis of skin and soft tissue infections, as well as neonatal eye infections, Dr. Morven Edwards said at a practical pediatrics meeting sponsored by the American Academy of Pediatrics.
Dr. Edwards, an infectious disease specialist at Texas Children’s Hospital, Houston, said that unlike a decade ago, she now considers community-acquired MRSA as a possible cause "in almost any manifestation of a problem with the skin or soft tissue, even including those entities that we used to think were caused by other microorganisms."
For example, in the past, perianal dermatitis in a young infant "was essentially a pathognomonic presentation for group A strep infection," which did not even require a culture for an accurate diagnosis and appropriate treatment, said Dr. Edwards, who is a professor of pediatrics at Baylor College of Medicine, Houston.
She referred to a small retrospective study of children between the ages of 5 months and 12 years with perianal erythema, which found that the dominant culture results were MRSA and methicillin-sensitive S. aureus (MSSA), some streptococci, and some mixed infections. In the past, staphylococcal skin and soft tissue infections were considered uncommon among healthy term newborns discharged home, "unless it was just a very mild diaper dermatitis," she noted.
In a 2006 study of healthy term babies who returned to the hospital within a month of discharge to Texas Children’s Hospital’s emergency department, cases of MRSA peaked at 8-12 days after discharge. Almost all were skin and soft tissue infections (SSTIs), and some of the babies had mild, pustular skin disease and were treated as outpatients with topical therapy and/or oral antistaphylococcal medications. But almost 40% required admission for incision and drainage and parenteral antibiotic therapy.
Dr. Edwards referred to a case of an SSTI that started with a stubbed toe and progressed to a disseminated staphylococcal infection and endocarditis – illustrating that "even with an apparently limited minor staph infection, it always should go through our minds that this could be one that’s more serious."
The healthy teenage boy had stubbed his toe during a wrestling match, then developed fever, fatigue, and buttock and back pain, along with swelling and pain in the toe 4 days later. A fracture was diagnosed at an urgent care clinic, and he was sent home, but 9 days after the initial injury, symptoms persisted and he was admitted to the hospital for treatment with broad-spectrum antimicrobials, including clindamycin.
On the fourth day in the hospital, he had a fever of 104° F, "massive" facial swelling, bibasilar crackles, a systolic murmur, left lower quadrant pain, and a large parietal abscess seen on MRI. He had vegetations on the anterior leaflet of the mitral valve and multiple microemboli to the brain. The abscess was drained, and he had a vegetectomy, where vegetation was "peeled" off the leaflet, leaving the valve intact. After 6 weeks of intravenous antimicrobial treatment, he did well and was discharged.
"The lesson is that a seemingly innocuous SSTI always has the potential to disseminate," Dr. Edwards said, adding that while this is very uncommon, especially in a healthy child, "it’s always something to keep in mind."
Transmitted by direct contact, risk factors for community-acquired MRSA include chronic skin conditions, participation in sports teams that involve close contact with other players, and a history of such infections in family members, she noted.
In infants, MRSA infection also should be included in the differential diagnosis of ophthalmia neonatorum, Dr. Edwards said. She described the case of a healthy term 4-day-old baby who presented with eye swelling and purulent discharge, but no other systemic findings. The mother’s pregnancy had been uncomplicated; maternal tests were negative for group B streptococcus, chlamydia, and Neisseria gonorrhoea; and the baby had been discharged home by the second day after a normal vaginal birth.
The cause turned out to be community-acquired MRSA infection. "We need to consider this diagnosis with a higher index of suspicion in young infants now," she said, noting that the peak onset is at age 4-6 days, and it is characterized by a purulent discharge not likely to be a gonococcal infection. The baby was admitted to the hospital and treated with parenteral antimicrobial therapy.
Dr. Edwards disclosed that she is a consultant for and has received research funds from Novartis related to the development of a group B streptococcus vaccine.
WASHINGTON – Community-acquired methicillin-resistant Staphylococcus aureus should be considered in the differential diagnosis of skin and soft tissue infections, as well as neonatal eye infections, Dr. Morven Edwards said at a practical pediatrics meeting sponsored by the American Academy of Pediatrics.
Dr. Edwards, an infectious disease specialist at Texas Children’s Hospital, Houston, said that unlike a decade ago, she now considers community-acquired MRSA as a possible cause "in almost any manifestation of a problem with the skin or soft tissue, even including those entities that we used to think were caused by other microorganisms."
For example, in the past, perianal dermatitis in a young infant "was essentially a pathognomonic presentation for group A strep infection," which did not even require a culture for an accurate diagnosis and appropriate treatment, said Dr. Edwards, who is a professor of pediatrics at Baylor College of Medicine, Houston.
She referred to a small retrospective study of children between the ages of 5 months and 12 years with perianal erythema, which found that the dominant culture results were MRSA and methicillin-sensitive S. aureus (MSSA), some streptococci, and some mixed infections. In the past, staphylococcal skin and soft tissue infections were considered uncommon among healthy term newborns discharged home, "unless it was just a very mild diaper dermatitis," she noted.
In a 2006 study of healthy term babies who returned to the hospital within a month of discharge to Texas Children’s Hospital’s emergency department, cases of MRSA peaked at 8-12 days after discharge. Almost all were skin and soft tissue infections (SSTIs), and some of the babies had mild, pustular skin disease and were treated as outpatients with topical therapy and/or oral antistaphylococcal medications. But almost 40% required admission for incision and drainage and parenteral antibiotic therapy.
Dr. Edwards referred to a case of an SSTI that started with a stubbed toe and progressed to a disseminated staphylococcal infection and endocarditis – illustrating that "even with an apparently limited minor staph infection, it always should go through our minds that this could be one that’s more serious."
The healthy teenage boy had stubbed his toe during a wrestling match, then developed fever, fatigue, and buttock and back pain, along with swelling and pain in the toe 4 days later. A fracture was diagnosed at an urgent care clinic, and he was sent home, but 9 days after the initial injury, symptoms persisted and he was admitted to the hospital for treatment with broad-spectrum antimicrobials, including clindamycin.
On the fourth day in the hospital, he had a fever of 104° F, "massive" facial swelling, bibasilar crackles, a systolic murmur, left lower quadrant pain, and a large parietal abscess seen on MRI. He had vegetations on the anterior leaflet of the mitral valve and multiple microemboli to the brain. The abscess was drained, and he had a vegetectomy, where vegetation was "peeled" off the leaflet, leaving the valve intact. After 6 weeks of intravenous antimicrobial treatment, he did well and was discharged.
"The lesson is that a seemingly innocuous SSTI always has the potential to disseminate," Dr. Edwards said, adding that while this is very uncommon, especially in a healthy child, "it’s always something to keep in mind."
Transmitted by direct contact, risk factors for community-acquired MRSA include chronic skin conditions, participation in sports teams that involve close contact with other players, and a history of such infections in family members, she noted.
In infants, MRSA infection also should be included in the differential diagnosis of ophthalmia neonatorum, Dr. Edwards said. She described the case of a healthy term 4-day-old baby who presented with eye swelling and purulent discharge, but no other systemic findings. The mother’s pregnancy had been uncomplicated; maternal tests were negative for group B streptococcus, chlamydia, and Neisseria gonorrhoea; and the baby had been discharged home by the second day after a normal vaginal birth.
The cause turned out to be community-acquired MRSA infection. "We need to consider this diagnosis with a higher index of suspicion in young infants now," she said, noting that the peak onset is at age 4-6 days, and it is characterized by a purulent discharge not likely to be a gonococcal infection. The baby was admitted to the hospital and treated with parenteral antimicrobial therapy.
Dr. Edwards disclosed that she is a consultant for and has received research funds from Novartis related to the development of a group B streptococcus vaccine.
EXPERT ANALYSIS FROM PRACTICAL PEDIATRICS