User login
Potential new neuromodulation treatment for migraines
Most people avoid smartphones when they have a migraine headache, but a noninvasive treatment for episodic migraines may change that.
that can help ease migraine pain.
Tina Montgomery, 58, has suffered from migraines since childhood and spent years looking for something to help manage them. Doctors consider her a “chronic” sufferer in that she has more than 14 migraines a month (fewer than 14 is considered “episodic”). Prescription antidepressants, anticonvulsants, and botulinum toxin shots as preventive treatments helped a little but not enough.
A few years ago, she found some relief using a new preventive injectable medication that targets a peptide known as CGRP, combined with an oral CGRP rescue medication, ubrogepant (Ubrelvy). However, by early 2021, Ms. Montgomery’s chronic migraines were back as she faced stress from the pandemic and her role as a caregiver for her aging parents.
“I was going through so much medication. I just didn’t feel good taking so much,” she said.
Looking for relief, she read about Nerivio, a wearable migraine treatment device that uses remote electrical neuromodulation (REN). She mentioned the device to her neurologist, and he agreed she might benefit from trying it out. Today, she uses the device whenever she feels a migraine may be imminent, she said.
“It really helps me stave off migraines I feel coming on and the milder ones where I would normally hesitate to use prescription medication because [insurance] limits the number of pills they give you in a month,” she said. “I follow through with the Nerivio treatment and usually find that my migraine doesn’t fully develop or is completely gone, and I don’t get a migraine at all.”
Taking it on the arm
The device works by stimulating nerves at the back of the arm right around the triceps. “Those nerve fibers relay information to the brain stem [so it can] work its magic and use the brain’s own natural mechanisms for reducing pain,” said Brian M. Grosberg, MD, director of the Hartford Healthcare Ayer Neuroscience Institute Headache Center, West Hartford, Conn.
These mechanisms are like a bait-and-switch for the brain, said Britany Klenofsky, MD, assistant professor of neurology, Icahn School of Medicine at Mount Sinai, New York. “You’re trying to stimulate pain somewhere else [on the body] to tell the brain to protect itself and release [the neurotransmitter] serotonin,” she said. “You do this by putting the device on your arm, an area that’s away from the head where the pain is actively occurring, turning the device on, and increasing the stimulation to a nearly painful stimulus.”
This pseudo pain prompts the brain to release serotonin, the feel-good hormone along with norepinephrine and noradrenaline. The device works best when it’s used as soon as a migraine starts, so patients should hook up Nerivio within the first 20-30 minutes of onset of pain, said Dr. Grosberg, who was an investigator on the double-blind treatment study that led to FDA clearance. If patients wait too long, the device may not work.
This is why as soon as Ms. Montgomery feels a migraine aura (there are six types of migraine auras, including visual changes and muscle weakness) that occurs right before a migraine strikes, she puts the device armband on her upper arm and launches its smartphone app. Then she turns on the device for a 45-minute treatment, which begins with what she characterizes as tingling and vibration sensations on her arm. She turns up the intensity of the sensations, which are mild electric currents, until they are well-felt but not painful.
Ms. Montgomery said she can use the device and multitask since there’s no need for her to lie down or sit in a darkened room. And since it is worn on the arm, she can wear it under a shirtsleeve while working or out in public without anyone noticing. She also uses the app’s migraine diary and guided meditation to help reduce the anxiety that often accompanies her migraines.
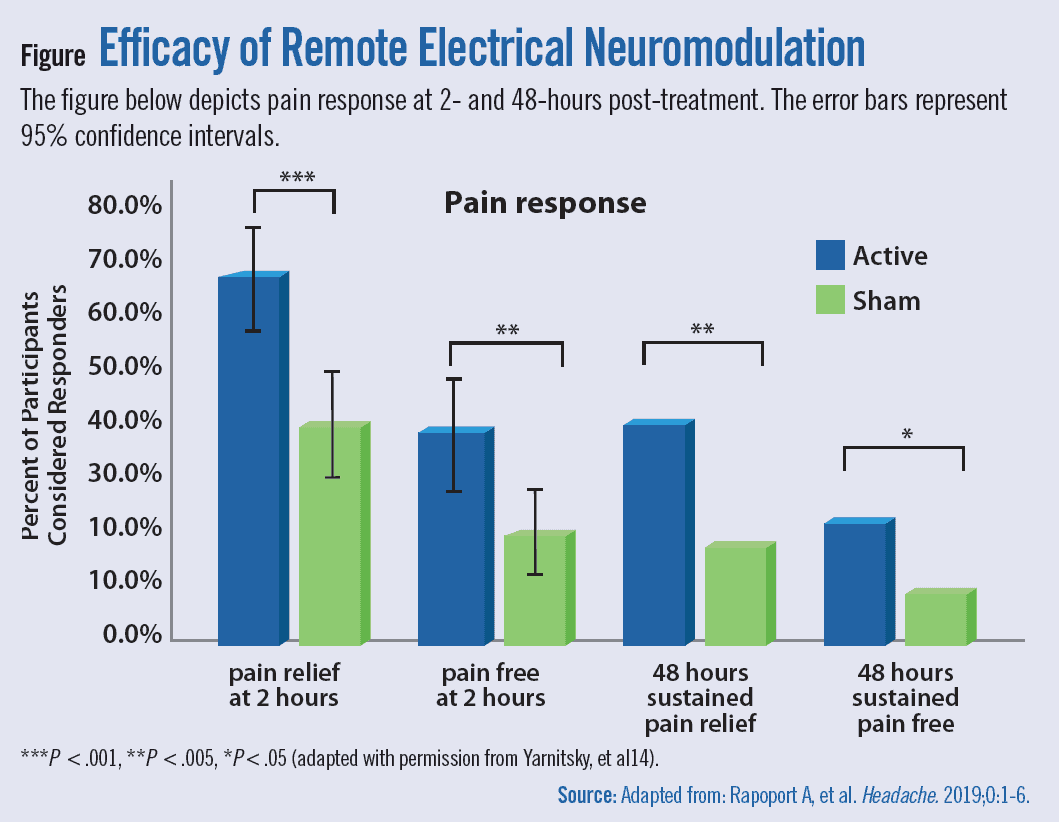
The device is approved for adolescents and adults and can be used for both episodic and chronic migraines. From an efficacy standpoint, the device provides relief about as well as a commonly used pharmaceutical class of drugs, triptans. About 37% of people with episodic migraine achieved complete freedom from pain 2 hours after their treatment. In addition, about two-thirds of people reported pain relief after 2 hours, which is better success than people find with many prescription and nonprescription drugs.
A separate study looked at acute treatment for chronic migraine sufferers and found nearly 60% of people using the device found relief and 21% said they were pain-free after 2 hours. Almost two-thirds of those who experienced pain relief were pain-free 24 hours after the treatment.
{kind=link}
Finding the perfect patient
There are other FDA-cleared noninvasive devices to treat migraines. One device, CEFALY, is an external trigeminal nerve stimulation device that sits on the forehead. Another device, SpringTMS, uses transcranial magnetic stimulation on the back of the head. A third option, the gammaCore Sapphire, is placed on the neck to stimulate the vagus nerve. All three have been cleared by the FDA to work as preventive and acute treatments for migraine.
Theranica, the company that developed Nerivio, is trying to boost use of the device by allowing patients to get a prescription via telehealth visits with a physician.
The company, as well as the companies behind the other neuromodulation devices, are marketing their treatments to children ages 12 and up since nonpharmacologic options are often preferable for parents, said Thomas Berk, MD, a clinical associate professor in the division of headache at NYU Langone Health in New York.
Dr. Berk said the devices could be appealing for those people who don’t want or can’t take medication, such as pregnant women or those who don’t respond well to drugs. “[They] could also be used by somebody who needs something in addition to a medication,” he said.
For now, people like Ms. Montgomery say they are happy to have another tool in their migraine arsenal. “Overall, I’m taking less medication because I haven’t had to have my Ubrelvy refilled as often as I used to,” she said. “It’s really helped me manage changes and stresses in my life.”
A version of this article first appeared on Medscape.com.
Most people avoid smartphones when they have a migraine headache, but a noninvasive treatment for episodic migraines may change that.
that can help ease migraine pain.
Tina Montgomery, 58, has suffered from migraines since childhood and spent years looking for something to help manage them. Doctors consider her a “chronic” sufferer in that she has more than 14 migraines a month (fewer than 14 is considered “episodic”). Prescription antidepressants, anticonvulsants, and botulinum toxin shots as preventive treatments helped a little but not enough.
A few years ago, she found some relief using a new preventive injectable medication that targets a peptide known as CGRP, combined with an oral CGRP rescue medication, ubrogepant (Ubrelvy). However, by early 2021, Ms. Montgomery’s chronic migraines were back as she faced stress from the pandemic and her role as a caregiver for her aging parents.
“I was going through so much medication. I just didn’t feel good taking so much,” she said.
Looking for relief, she read about Nerivio, a wearable migraine treatment device that uses remote electrical neuromodulation (REN). She mentioned the device to her neurologist, and he agreed she might benefit from trying it out. Today, she uses the device whenever she feels a migraine may be imminent, she said.
“It really helps me stave off migraines I feel coming on and the milder ones where I would normally hesitate to use prescription medication because [insurance] limits the number of pills they give you in a month,” she said. “I follow through with the Nerivio treatment and usually find that my migraine doesn’t fully develop or is completely gone, and I don’t get a migraine at all.”
Taking it on the arm
The device works by stimulating nerves at the back of the arm right around the triceps. “Those nerve fibers relay information to the brain stem [so it can] work its magic and use the brain’s own natural mechanisms for reducing pain,” said Brian M. Grosberg, MD, director of the Hartford Healthcare Ayer Neuroscience Institute Headache Center, West Hartford, Conn.
These mechanisms are like a bait-and-switch for the brain, said Britany Klenofsky, MD, assistant professor of neurology, Icahn School of Medicine at Mount Sinai, New York. “You’re trying to stimulate pain somewhere else [on the body] to tell the brain to protect itself and release [the neurotransmitter] serotonin,” she said. “You do this by putting the device on your arm, an area that’s away from the head where the pain is actively occurring, turning the device on, and increasing the stimulation to a nearly painful stimulus.”
This pseudo pain prompts the brain to release serotonin, the feel-good hormone along with norepinephrine and noradrenaline. The device works best when it’s used as soon as a migraine starts, so patients should hook up Nerivio within the first 20-30 minutes of onset of pain, said Dr. Grosberg, who was an investigator on the double-blind treatment study that led to FDA clearance. If patients wait too long, the device may not work.
This is why as soon as Ms. Montgomery feels a migraine aura (there are six types of migraine auras, including visual changes and muscle weakness) that occurs right before a migraine strikes, she puts the device armband on her upper arm and launches its smartphone app. Then she turns on the device for a 45-minute treatment, which begins with what she characterizes as tingling and vibration sensations on her arm. She turns up the intensity of the sensations, which are mild electric currents, until they are well-felt but not painful.
Ms. Montgomery said she can use the device and multitask since there’s no need for her to lie down or sit in a darkened room. And since it is worn on the arm, she can wear it under a shirtsleeve while working or out in public without anyone noticing. She also uses the app’s migraine diary and guided meditation to help reduce the anxiety that often accompanies her migraines.
The device is approved for adolescents and adults and can be used for both episodic and chronic migraines. From an efficacy standpoint, the device provides relief about as well as a commonly used pharmaceutical class of drugs, triptans. About 37% of people with episodic migraine achieved complete freedom from pain 2 hours after their treatment. In addition, about two-thirds of people reported pain relief after 2 hours, which is better success than people find with many prescription and nonprescription drugs.
A separate study looked at acute treatment for chronic migraine sufferers and found nearly 60% of people using the device found relief and 21% said they were pain-free after 2 hours. Almost two-thirds of those who experienced pain relief were pain-free 24 hours after the treatment.
Finding the perfect patient
There are other FDA-cleared noninvasive devices to treat migraines. One device, CEFALY, is an external trigeminal nerve stimulation device that sits on the forehead. Another device, SpringTMS, uses transcranial magnetic stimulation on the back of the head. A third option, the gammaCore Sapphire, is placed on the neck to stimulate the vagus nerve. All three have been cleared by the FDA to work as preventive and acute treatments for migraine.
Theranica, the company that developed Nerivio, is trying to boost use of the device by allowing patients to get a prescription via telehealth visits with a physician.
The company, as well as the companies behind the other neuromodulation devices, are marketing their treatments to children ages 12 and up since nonpharmacologic options are often preferable for parents, said Thomas Berk, MD, a clinical associate professor in the division of headache at NYU Langone Health in New York.
Dr. Berk said the devices could be appealing for those people who don’t want or can’t take medication, such as pregnant women or those who don’t respond well to drugs. “[They] could also be used by somebody who needs something in addition to a medication,” he said.
For now, people like Ms. Montgomery say they are happy to have another tool in their migraine arsenal. “Overall, I’m taking less medication because I haven’t had to have my Ubrelvy refilled as often as I used to,” she said. “It’s really helped me manage changes and stresses in my life.”
A version of this article first appeared on Medscape.com.
Most people avoid smartphones when they have a migraine headache, but a noninvasive treatment for episodic migraines may change that.
that can help ease migraine pain.
Tina Montgomery, 58, has suffered from migraines since childhood and spent years looking for something to help manage them. Doctors consider her a “chronic” sufferer in that she has more than 14 migraines a month (fewer than 14 is considered “episodic”). Prescription antidepressants, anticonvulsants, and botulinum toxin shots as preventive treatments helped a little but not enough.
A few years ago, she found some relief using a new preventive injectable medication that targets a peptide known as CGRP, combined with an oral CGRP rescue medication, ubrogepant (Ubrelvy). However, by early 2021, Ms. Montgomery’s chronic migraines were back as she faced stress from the pandemic and her role as a caregiver for her aging parents.
“I was going through so much medication. I just didn’t feel good taking so much,” she said.
Looking for relief, she read about Nerivio, a wearable migraine treatment device that uses remote electrical neuromodulation (REN). She mentioned the device to her neurologist, and he agreed she might benefit from trying it out. Today, she uses the device whenever she feels a migraine may be imminent, she said.
“It really helps me stave off migraines I feel coming on and the milder ones where I would normally hesitate to use prescription medication because [insurance] limits the number of pills they give you in a month,” she said. “I follow through with the Nerivio treatment and usually find that my migraine doesn’t fully develop or is completely gone, and I don’t get a migraine at all.”
Taking it on the arm
The device works by stimulating nerves at the back of the arm right around the triceps. “Those nerve fibers relay information to the brain stem [so it can] work its magic and use the brain’s own natural mechanisms for reducing pain,” said Brian M. Grosberg, MD, director of the Hartford Healthcare Ayer Neuroscience Institute Headache Center, West Hartford, Conn.
These mechanisms are like a bait-and-switch for the brain, said Britany Klenofsky, MD, assistant professor of neurology, Icahn School of Medicine at Mount Sinai, New York. “You’re trying to stimulate pain somewhere else [on the body] to tell the brain to protect itself and release [the neurotransmitter] serotonin,” she said. “You do this by putting the device on your arm, an area that’s away from the head where the pain is actively occurring, turning the device on, and increasing the stimulation to a nearly painful stimulus.”
This pseudo pain prompts the brain to release serotonin, the feel-good hormone along with norepinephrine and noradrenaline. The device works best when it’s used as soon as a migraine starts, so patients should hook up Nerivio within the first 20-30 minutes of onset of pain, said Dr. Grosberg, who was an investigator on the double-blind treatment study that led to FDA clearance. If patients wait too long, the device may not work.
This is why as soon as Ms. Montgomery feels a migraine aura (there are six types of migraine auras, including visual changes and muscle weakness) that occurs right before a migraine strikes, she puts the device armband on her upper arm and launches its smartphone app. Then she turns on the device for a 45-minute treatment, which begins with what she characterizes as tingling and vibration sensations on her arm. She turns up the intensity of the sensations, which are mild electric currents, until they are well-felt but not painful.
Ms. Montgomery said she can use the device and multitask since there’s no need for her to lie down or sit in a darkened room. And since it is worn on the arm, she can wear it under a shirtsleeve while working or out in public without anyone noticing. She also uses the app’s migraine diary and guided meditation to help reduce the anxiety that often accompanies her migraines.
The device is approved for adolescents and adults and can be used for both episodic and chronic migraines. From an efficacy standpoint, the device provides relief about as well as a commonly used pharmaceutical class of drugs, triptans. About 37% of people with episodic migraine achieved complete freedom from pain 2 hours after their treatment. In addition, about two-thirds of people reported pain relief after 2 hours, which is better success than people find with many prescription and nonprescription drugs.
A separate study looked at acute treatment for chronic migraine sufferers and found nearly 60% of people using the device found relief and 21% said they were pain-free after 2 hours. Almost two-thirds of those who experienced pain relief were pain-free 24 hours after the treatment.
Finding the perfect patient
There are other FDA-cleared noninvasive devices to treat migraines. One device, CEFALY, is an external trigeminal nerve stimulation device that sits on the forehead. Another device, SpringTMS, uses transcranial magnetic stimulation on the back of the head. A third option, the gammaCore Sapphire, is placed on the neck to stimulate the vagus nerve. All three have been cleared by the FDA to work as preventive and acute treatments for migraine.
Theranica, the company that developed Nerivio, is trying to boost use of the device by allowing patients to get a prescription via telehealth visits with a physician.
The company, as well as the companies behind the other neuromodulation devices, are marketing their treatments to children ages 12 and up since nonpharmacologic options are often preferable for parents, said Thomas Berk, MD, a clinical associate professor in the division of headache at NYU Langone Health in New York.
Dr. Berk said the devices could be appealing for those people who don’t want or can’t take medication, such as pregnant women or those who don’t respond well to drugs. “[They] could also be used by somebody who needs something in addition to a medication,” he said.
For now, people like Ms. Montgomery say they are happy to have another tool in their migraine arsenal. “Overall, I’m taking less medication because I haven’t had to have my Ubrelvy refilled as often as I used to,” she said. “It’s really helped me manage changes and stresses in my life.”
A version of this article first appeared on Medscape.com.
Clinical Edge Journal Scan Commentary: Migraine February 2022
Most practitioners recommend a host of non-medical therapeutic options to their patients with migraine. The best studied and safest, most effective supplements remain magnesium, riboflavin/B2, and CoQ10. Alpha-lipoic acid (ALA) is a supplement with both antioxidant and anti-inflammatory effects that has showed positive protective effects in a number of medical conditions, including diabetes and episodes of oxidative stress. One migraine study1 evaluated serum ALA levels and found over 90% of people with migraine to deficient. This study sought to observe the potential benefit of supplementation with ALA in patients with episodic migraine.
This was a randomized, double-blind placebo-controlled trial over the course of 3 months. In this study, 92 female subjects with episodic migraine (defined as experiencing >2 but <15 days of headache per month) were recruited and randomized to receiving 300 mg ALA twice daily or placebo. Patients with chronic migraine, in menopause, pregnant, or lactating were excluded, as were patients with the presence of other chronic medical issues, or patients who had taken antioxidant supplements in the previous 4 months.
The primary outcomes of migraine severity, frequency, and Headache Impact Test (HIT-6) score were found to be significantly improved in the intervention group; duration of headache was not significantly different. Biochemical analysis of the two groups did show a difference in the lactate level of the intervention group, and this was considered a secondary outcome. Relevant side effects were primarily gastrointestinal, including stomach pain (higher in the placebo group), increased appetite, and constipation.
There is a great interest in finding effective non-medical treatments for migraine. These are frequently used as an adjunct to other preventive medications, or potentially as a stand-alone treatment for low frequency migraine. Many patients prefer non-medical options as well, and unfortunately many of the treatments they read about online or in less scientific spaces are unproven or unsafe. Supplementation remains an important part of migraine treatment for many practitioners and patients.
This study argues that ALA can be considered a safe and effective treatment for episodic migraine. When patients ask about non-medical options, ALA can be an additional treatment worth considering. Many patients are already taking multiple supplements before seeing their specialist, and this article informs us that there may be some treatment benefit for this supplement as well. We may not be recommending this supplement alone as a preventive treatment for migraine, but we can add a new non-medical option to consider to our mix.
Using preventive medication in pediatrics is now more controversial than it had been previously. The well known The Childhood and Adolescent Migraine Prevention (CHAMP) trial2 surprised many in the field by revealing that were no significant differences in headache frequency or disability when comparing children with migraine who received preventive medications or placebo. The CHAMP trial spotlighted the effect of non-medical therapies (cognitive behavioral therapy, biofeedback) and education. Many pediatric specialists have altered their practice paradigm in response to these results and have been more reticent to prescribe preventive medications for children with migraine. This is due to concern for potential side effects in light of the absence of direct benefit.
In an observational study of pediatric migraine,3 the investigators followed 186 children with migraine over a 3-year period to determine if the use of a number of preventive medications addresses disability (measured by Pediatric Migraine Disability Assessment [PedMIDAS]) as well as frequency, severity and duration of migraine. Other bothersome features of migraine were followed including the presence of nausea, vomiting, photophobia, analgesic use, and the side effects of the preventive medication.
The preventive medications used were cyproheptadine, flunarazine, propranolol, and topiramate—all at weight based doses. It is important to note that amitriptyline was not used in the study and there was no placebo group. This was a Turkish population, the median age was 14, and 63% were female, all of which are appropriate for a pediatric migraine study. Treatment efficacy was defined as a 50% reduction of symptoms. This was achieved in 90% of subjects in the topiramate group, 75% in the propranolol group, and 52-53% in the flunarazine and cyproheptadine groups.
Medication side effects were divided into minor or significant side effects. The only significant side effect noted was 3% of patient with palpitations; minor side effects were changes in appetite and drowsiness. More than half (57%) of patients taking topiramate experienced some side effect, 51% of the cyproheptadine group did as well, and the propranolol and flunarazine groups were noted to have side effects in 22% and 13%, respectively. Overall, 31.7% of patients had some side effect.
PedMIDAS scores improved significantly with the use of preventive medications; migraine frequency improved significantly as well, especially in the topiramate group. This study argues for the use of preventive medications in pediatric migraine. One of the most commonly used medications for migraine prevention was not investigated unfortunately. Amitriptyline is widely considered a safe and effective migraine prophylactic medication, especially at low doses. One important takeaway is the frequency of side effects at all, and especially with topiramate. It is unclear how many patients stopped their preventive medications due to a side effect. In light of this study, propranolol, which is often overlooked, might be considered a better choice for children with migraine.
Most of the patients with migraine we see are in their most productive years. Migraine disability can be a major difficulty for our patients, especially as it relates to work. The American Migraine Foundation and American Headache Society have both recently taken on initiatives that relate to migraine in the workplace. Migraine epidemiologic studies have shown that people with migraine are more likely to experience a negative impact on their careers, and migraine disability scores weigh time absent from work as well as lower function at work. Many people with migraine are concerned that having migraine may hold them back from being hired or achieving promotion.
Autio et al performed a retrospective analysis of occupationally active patients treated at a single provider (the Finnish health clinic Terveystalo).4 The authors first looked for erenumab responders, who they defined as patients who received two prescriptions for erenumab and no other calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) medication. These patients were followed for 12 months, and their data was compared to the 12-month period prior to initiating erenumab. The authors evaluated headache-related sick days, all-cause sick days, healthcare visits, and prescriptions for all medications based on a registry. This registry also provided an age- and sex-matched control group of patients with migraine not taking any CGRP mAb medication.
A total of 162 patients were included, 82 in the erenumab responder group. Headache-related sick days decreased by 74%, and headache-related healthcare visits decreased by 44%. Triptan prescription use decreased by 31.5%; all-cause sick days and healthcare visits differences were not statistically significant.
Prevention remains key in improving our patients’ quality of life and a large factor in this is their work life. This study shows that intervention with erenumab significantly decreases migraine-related absenteeism. It could be argued that the other CGRP mAb medications may have the same effect, as can many other preventive therapies. It can also be argued that even with this data we can only assume that patients function better at work with preventive therapies. Further studies will also look at the degree that “presenteeism” plays in the workplace—people who show up to work but are functioning at a lesser extent due to migraine. That said, this is an important step towards recognizing the burden migraine disability has on our patients’ work life, and the extent that prevention can improve their quality of life.
References
- Kelishadi MR et al. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci Rep. 2022;12:271 (Jan 7).
- Powers SW et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. Doi: 10.1056/NEJMoa1610384.
- Tekin H, Edem P. Effects and side effects of migraine prophylaxis in children. Pediatr Int. 2021 (Dec 14).
- Autio H et al. Erenumab decreases headache-related sick leave days and health care visits: a retrospective real-world study in working patients with migraine. Neurol Ther. 2021 (Dec 10).
Most practitioners recommend a host of non-medical therapeutic options to their patients with migraine. The best studied and safest, most effective supplements remain magnesium, riboflavin/B2, and CoQ10. Alpha-lipoic acid (ALA) is a supplement with both antioxidant and anti-inflammatory effects that has showed positive protective effects in a number of medical conditions, including diabetes and episodes of oxidative stress. One migraine study1 evaluated serum ALA levels and found over 90% of people with migraine to deficient. This study sought to observe the potential benefit of supplementation with ALA in patients with episodic migraine.
This was a randomized, double-blind placebo-controlled trial over the course of 3 months. In this study, 92 female subjects with episodic migraine (defined as experiencing >2 but <15 days of headache per month) were recruited and randomized to receiving 300 mg ALA twice daily or placebo. Patients with chronic migraine, in menopause, pregnant, or lactating were excluded, as were patients with the presence of other chronic medical issues, or patients who had taken antioxidant supplements in the previous 4 months.
The primary outcomes of migraine severity, frequency, and Headache Impact Test (HIT-6) score were found to be significantly improved in the intervention group; duration of headache was not significantly different. Biochemical analysis of the two groups did show a difference in the lactate level of the intervention group, and this was considered a secondary outcome. Relevant side effects were primarily gastrointestinal, including stomach pain (higher in the placebo group), increased appetite, and constipation.
There is a great interest in finding effective non-medical treatments for migraine. These are frequently used as an adjunct to other preventive medications, or potentially as a stand-alone treatment for low frequency migraine. Many patients prefer non-medical options as well, and unfortunately many of the treatments they read about online or in less scientific spaces are unproven or unsafe. Supplementation remains an important part of migraine treatment for many practitioners and patients.
This study argues that ALA can be considered a safe and effective treatment for episodic migraine. When patients ask about non-medical options, ALA can be an additional treatment worth considering. Many patients are already taking multiple supplements before seeing their specialist, and this article informs us that there may be some treatment benefit for this supplement as well. We may not be recommending this supplement alone as a preventive treatment for migraine, but we can add a new non-medical option to consider to our mix.
Using preventive medication in pediatrics is now more controversial than it had been previously. The well known The Childhood and Adolescent Migraine Prevention (CHAMP) trial2 surprised many in the field by revealing that were no significant differences in headache frequency or disability when comparing children with migraine who received preventive medications or placebo. The CHAMP trial spotlighted the effect of non-medical therapies (cognitive behavioral therapy, biofeedback) and education. Many pediatric specialists have altered their practice paradigm in response to these results and have been more reticent to prescribe preventive medications for children with migraine. This is due to concern for potential side effects in light of the absence of direct benefit.
In an observational study of pediatric migraine,3 the investigators followed 186 children with migraine over a 3-year period to determine if the use of a number of preventive medications addresses disability (measured by Pediatric Migraine Disability Assessment [PedMIDAS]) as well as frequency, severity and duration of migraine. Other bothersome features of migraine were followed including the presence of nausea, vomiting, photophobia, analgesic use, and the side effects of the preventive medication.
The preventive medications used were cyproheptadine, flunarazine, propranolol, and topiramate—all at weight based doses. It is important to note that amitriptyline was not used in the study and there was no placebo group. This was a Turkish population, the median age was 14, and 63% were female, all of which are appropriate for a pediatric migraine study. Treatment efficacy was defined as a 50% reduction of symptoms. This was achieved in 90% of subjects in the topiramate group, 75% in the propranolol group, and 52-53% in the flunarazine and cyproheptadine groups.
Medication side effects were divided into minor or significant side effects. The only significant side effect noted was 3% of patient with palpitations; minor side effects were changes in appetite and drowsiness. More than half (57%) of patients taking topiramate experienced some side effect, 51% of the cyproheptadine group did as well, and the propranolol and flunarazine groups were noted to have side effects in 22% and 13%, respectively. Overall, 31.7% of patients had some side effect.
PedMIDAS scores improved significantly with the use of preventive medications; migraine frequency improved significantly as well, especially in the topiramate group. This study argues for the use of preventive medications in pediatric migraine. One of the most commonly used medications for migraine prevention was not investigated unfortunately. Amitriptyline is widely considered a safe and effective migraine prophylactic medication, especially at low doses. One important takeaway is the frequency of side effects at all, and especially with topiramate. It is unclear how many patients stopped their preventive medications due to a side effect. In light of this study, propranolol, which is often overlooked, might be considered a better choice for children with migraine.
Most of the patients with migraine we see are in their most productive years. Migraine disability can be a major difficulty for our patients, especially as it relates to work. The American Migraine Foundation and American Headache Society have both recently taken on initiatives that relate to migraine in the workplace. Migraine epidemiologic studies have shown that people with migraine are more likely to experience a negative impact on their careers, and migraine disability scores weigh time absent from work as well as lower function at work. Many people with migraine are concerned that having migraine may hold them back from being hired or achieving promotion.
Autio et al performed a retrospective analysis of occupationally active patients treated at a single provider (the Finnish health clinic Terveystalo).4 The authors first looked for erenumab responders, who they defined as patients who received two prescriptions for erenumab and no other calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) medication. These patients were followed for 12 months, and their data was compared to the 12-month period prior to initiating erenumab. The authors evaluated headache-related sick days, all-cause sick days, healthcare visits, and prescriptions for all medications based on a registry. This registry also provided an age- and sex-matched control group of patients with migraine not taking any CGRP mAb medication.
A total of 162 patients were included, 82 in the erenumab responder group. Headache-related sick days decreased by 74%, and headache-related healthcare visits decreased by 44%. Triptan prescription use decreased by 31.5%; all-cause sick days and healthcare visits differences were not statistically significant.
Prevention remains key in improving our patients’ quality of life and a large factor in this is their work life. This study shows that intervention with erenumab significantly decreases migraine-related absenteeism. It could be argued that the other CGRP mAb medications may have the same effect, as can many other preventive therapies. It can also be argued that even with this data we can only assume that patients function better at work with preventive therapies. Further studies will also look at the degree that “presenteeism” plays in the workplace—people who show up to work but are functioning at a lesser extent due to migraine. That said, this is an important step towards recognizing the burden migraine disability has on our patients’ work life, and the extent that prevention can improve their quality of life.
References
- Kelishadi MR et al. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci Rep. 2022;12:271 (Jan 7).
- Powers SW et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. Doi: 10.1056/NEJMoa1610384.
- Tekin H, Edem P. Effects and side effects of migraine prophylaxis in children. Pediatr Int. 2021 (Dec 14).
- Autio H et al. Erenumab decreases headache-related sick leave days and health care visits: a retrospective real-world study in working patients with migraine. Neurol Ther. 2021 (Dec 10).
Most practitioners recommend a host of non-medical therapeutic options to their patients with migraine. The best studied and safest, most effective supplements remain magnesium, riboflavin/B2, and CoQ10. Alpha-lipoic acid (ALA) is a supplement with both antioxidant and anti-inflammatory effects that has showed positive protective effects in a number of medical conditions, including diabetes and episodes of oxidative stress. One migraine study1 evaluated serum ALA levels and found over 90% of people with migraine to deficient. This study sought to observe the potential benefit of supplementation with ALA in patients with episodic migraine.
This was a randomized, double-blind placebo-controlled trial over the course of 3 months. In this study, 92 female subjects with episodic migraine (defined as experiencing >2 but <15 days of headache per month) were recruited and randomized to receiving 300 mg ALA twice daily or placebo. Patients with chronic migraine, in menopause, pregnant, or lactating were excluded, as were patients with the presence of other chronic medical issues, or patients who had taken antioxidant supplements in the previous 4 months.
The primary outcomes of migraine severity, frequency, and Headache Impact Test (HIT-6) score were found to be significantly improved in the intervention group; duration of headache was not significantly different. Biochemical analysis of the two groups did show a difference in the lactate level of the intervention group, and this was considered a secondary outcome. Relevant side effects were primarily gastrointestinal, including stomach pain (higher in the placebo group), increased appetite, and constipation.
There is a great interest in finding effective non-medical treatments for migraine. These are frequently used as an adjunct to other preventive medications, or potentially as a stand-alone treatment for low frequency migraine. Many patients prefer non-medical options as well, and unfortunately many of the treatments they read about online or in less scientific spaces are unproven or unsafe. Supplementation remains an important part of migraine treatment for many practitioners and patients.
This study argues that ALA can be considered a safe and effective treatment for episodic migraine. When patients ask about non-medical options, ALA can be an additional treatment worth considering. Many patients are already taking multiple supplements before seeing their specialist, and this article informs us that there may be some treatment benefit for this supplement as well. We may not be recommending this supplement alone as a preventive treatment for migraine, but we can add a new non-medical option to consider to our mix.
Using preventive medication in pediatrics is now more controversial than it had been previously. The well known The Childhood and Adolescent Migraine Prevention (CHAMP) trial2 surprised many in the field by revealing that were no significant differences in headache frequency or disability when comparing children with migraine who received preventive medications or placebo. The CHAMP trial spotlighted the effect of non-medical therapies (cognitive behavioral therapy, biofeedback) and education. Many pediatric specialists have altered their practice paradigm in response to these results and have been more reticent to prescribe preventive medications for children with migraine. This is due to concern for potential side effects in light of the absence of direct benefit.
In an observational study of pediatric migraine,3 the investigators followed 186 children with migraine over a 3-year period to determine if the use of a number of preventive medications addresses disability (measured by Pediatric Migraine Disability Assessment [PedMIDAS]) as well as frequency, severity and duration of migraine. Other bothersome features of migraine were followed including the presence of nausea, vomiting, photophobia, analgesic use, and the side effects of the preventive medication.
The preventive medications used were cyproheptadine, flunarazine, propranolol, and topiramate—all at weight based doses. It is important to note that amitriptyline was not used in the study and there was no placebo group. This was a Turkish population, the median age was 14, and 63% were female, all of which are appropriate for a pediatric migraine study. Treatment efficacy was defined as a 50% reduction of symptoms. This was achieved in 90% of subjects in the topiramate group, 75% in the propranolol group, and 52-53% in the flunarazine and cyproheptadine groups.
Medication side effects were divided into minor or significant side effects. The only significant side effect noted was 3% of patient with palpitations; minor side effects were changes in appetite and drowsiness. More than half (57%) of patients taking topiramate experienced some side effect, 51% of the cyproheptadine group did as well, and the propranolol and flunarazine groups were noted to have side effects in 22% and 13%, respectively. Overall, 31.7% of patients had some side effect.
PedMIDAS scores improved significantly with the use of preventive medications; migraine frequency improved significantly as well, especially in the topiramate group. This study argues for the use of preventive medications in pediatric migraine. One of the most commonly used medications for migraine prevention was not investigated unfortunately. Amitriptyline is widely considered a safe and effective migraine prophylactic medication, especially at low doses. One important takeaway is the frequency of side effects at all, and especially with topiramate. It is unclear how many patients stopped their preventive medications due to a side effect. In light of this study, propranolol, which is often overlooked, might be considered a better choice for children with migraine.
Most of the patients with migraine we see are in their most productive years. Migraine disability can be a major difficulty for our patients, especially as it relates to work. The American Migraine Foundation and American Headache Society have both recently taken on initiatives that relate to migraine in the workplace. Migraine epidemiologic studies have shown that people with migraine are more likely to experience a negative impact on their careers, and migraine disability scores weigh time absent from work as well as lower function at work. Many people with migraine are concerned that having migraine may hold them back from being hired or achieving promotion.
Autio et al performed a retrospective analysis of occupationally active patients treated at a single provider (the Finnish health clinic Terveystalo).4 The authors first looked for erenumab responders, who they defined as patients who received two prescriptions for erenumab and no other calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) medication. These patients were followed for 12 months, and their data was compared to the 12-month period prior to initiating erenumab. The authors evaluated headache-related sick days, all-cause sick days, healthcare visits, and prescriptions for all medications based on a registry. This registry also provided an age- and sex-matched control group of patients with migraine not taking any CGRP mAb medication.
A total of 162 patients were included, 82 in the erenumab responder group. Headache-related sick days decreased by 74%, and headache-related healthcare visits decreased by 44%. Triptan prescription use decreased by 31.5%; all-cause sick days and healthcare visits differences were not statistically significant.
Prevention remains key in improving our patients’ quality of life and a large factor in this is their work life. This study shows that intervention with erenumab significantly decreases migraine-related absenteeism. It could be argued that the other CGRP mAb medications may have the same effect, as can many other preventive therapies. It can also be argued that even with this data we can only assume that patients function better at work with preventive therapies. Further studies will also look at the degree that “presenteeism” plays in the workplace—people who show up to work but are functioning at a lesser extent due to migraine. That said, this is an important step towards recognizing the burden migraine disability has on our patients’ work life, and the extent that prevention can improve their quality of life.
References
- Kelishadi MR et al. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci Rep. 2022;12:271 (Jan 7).
- Powers SW et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. Doi: 10.1056/NEJMoa1610384.
- Tekin H, Edem P. Effects and side effects of migraine prophylaxis in children. Pediatr Int. 2021 (Dec 14).
- Autio H et al. Erenumab decreases headache-related sick leave days and health care visits: a retrospective real-world study in working patients with migraine. Neurol Ther. 2021 (Dec 10).
Clinical Edge Journal Scan Commentary: Migraine February 2022
Most practitioners recommend a host of non-medical therapeutic options to their patients with migraine. The best studied and safest, most effective supplements remain magnesium, riboflavin/B2, and CoQ10. Alpha-lipoic acid (ALA) is a supplement with both antioxidant and anti-inflammatory effects that has showed positive protective effects in a number of medical conditions, including diabetes and episodes of oxidative stress. One migraine study1 evaluated serum ALA levels and found over 90% of people with migraine to deficient. This study sought to observe the potential benefit of supplementation with ALA in patients with episodic migraine.
This was a randomized, double-blind placebo-controlled trial over the course of 3 months. In this study, 92 female subjects with episodic migraine (defined as experiencing >2 but <15 days of headache per month) were recruited and randomized to receiving 300 mg ALA twice daily or placebo. Patients with chronic migraine, in menopause, pregnant, or lactating were excluded, as were patients with the presence of other chronic medical issues, or patients who had taken antioxidant supplements in the previous 4 months.
The primary outcomes of migraine severity, frequency, and Headache Impact Test (HIT-6) score were found to be significantly improved in the intervention group; duration of headache was not significantly different. Biochemical analysis of the two groups did show a difference in the lactate level of the intervention group, and this was considered a secondary outcome. Relevant side effects were primarily gastrointestinal, including stomach pain (higher in the placebo group), increased appetite, and constipation.
There is a great interest in finding effective non-medical treatments for migraine. These are frequently used as an adjunct to other preventive medications, or potentially as a stand-alone treatment for low frequency migraine. Many patients prefer non-medical options as well, and unfortunately many of the treatments they read about online or in less scientific spaces are unproven or unsafe. Supplementation remains an important part of migraine treatment for many practitioners and patients.
This study argues that ALA can be considered a safe and effective treatment for episodic migraine. When patients ask about non-medical options, ALA can be an additional treatment worth considering. Many patients are already taking multiple supplements before seeing their specialist, and this article informs us that there may be some treatment benefit for this supplement as well. We may not be recommending this supplement alone as a preventive treatment for migraine, but we can add a new non-medical option to consider to our mix.
Using preventive medication in pediatrics is now more controversial than it had been previously. The well known The Childhood and Adolescent Migraine Prevention (CHAMP) trial2 surprised many in the field by revealing that were no significant differences in headache frequency or disability when comparing children with migraine who received preventive medications or placebo. The CHAMP trial spotlighted the effect of non-medical therapies (cognitive behavioral therapy, biofeedback) and education. Many pediatric specialists have altered their practice paradigm in response to these results and have been more reticent to prescribe preventive medications for children with migraine. This is due to concern for potential side effects in light of the absence of direct benefit.
In an observational study of pediatric migraine,3 the investigators followed 186 children with migraine over a 3-year period to determine if the use of a number of preventive medications addresses disability (measured by Pediatric Migraine Disability Assessment [PedMIDAS]) as well as frequency, severity and duration of migraine. Other bothersome features of migraine were followed including the presence of nausea, vomiting, photophobia, analgesic use, and the side effects of the preventive medication.
The preventive medications used were cyproheptadine, flunarazine, propranolol, and topiramate—all at weight based doses. It is important to note that amitriptyline was not used in the study and there was no placebo group. This was a Turkish population, the median age was 14, and 63% were female, all of which are appropriate for a pediatric migraine study. Treatment efficacy was defined as a 50% reduction of symptoms. This was achieved in 90% of subjects in the topiramate group, 75% in the propranolol group, and 52-53% in the flunarazine and cyproheptadine groups.
Medication side effects were divided into minor or significant side effects. The only significant side effect noted was 3% of patient with palpitations; minor side effects were changes in appetite and drowsiness. More than half (57%) of patients taking topiramate experienced some side effect, 51% of the cyproheptadine group did as well, and the propranolol and flunarazine groups were noted to have side effects in 22% and 13%, respectively. Overall, 31.7% of patients had some side effect.
PedMIDAS scores improved significantly with the use of preventive medications; migraine frequency improved significantly as well, especially in the topiramate group. This study argues for the use of preventive medications in pediatric migraine. One of the most commonly used medications for migraine prevention was not investigated unfortunately. Amitriptyline is widely considered a safe and effective migraine prophylactic medication, especially at low doses. One important takeaway is the frequency of side effects at all, and especially with topiramate. It is unclear how many patients stopped their preventive medications due to a side effect. In light of this study, propranolol, which is often overlooked, might be considered a better choice for children with migraine.
Most of the patients with migraine we see are in their most productive years. Migraine disability can be a major difficulty for our patients, especially as it relates to work. The American Migraine Foundation and American Headache Society have both recently taken on initiatives that relate to migraine in the workplace. Migraine epidemiologic studies have shown that people with migraine are more likely to experience a negative impact on their careers, and migraine disability scores weigh time absent from work as well as lower function at work. Many people with migraine are concerned that having migraine may hold them back from being hired or achieving promotion.
Autio et al performed a retrospective analysis of occupationally active patients treated at a single provider (the Finnish health clinic Terveystalo).4 The authors first looked for erenumab responders, who they defined as patients who received two prescriptions for erenumab and no other calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) medication. These patients were followed for 12 months, and their data was compared to the 12-month period prior to initiating erenumab. The authors evaluated headache-related sick days, all-cause sick days, healthcare visits, and prescriptions for all medications based on a registry. This registry also provided an age- and sex-matched control group of patients with migraine not taking any CGRP mAb medication.
A total of 162 patients were included, 82 in the erenumab responder group. Headache-related sick days decreased by 74%, and headache-related healthcare visits decreased by 44%. Triptan prescription use decreased by 31.5%; all-cause sick days and healthcare visits differences were not statistically significant.
Prevention remains key in improving our patients’ quality of life and a large factor in this is their work life. This study shows that intervention with erenumab significantly decreases migraine-related absenteeism. It could be argued that the other CGRP mAb medications may have the same effect, as can many other preventive therapies. It can also be argued that even with this data we can only assume that patients function better at work with preventive therapies. Further studies will also look at the degree that “presenteeism” plays in the workplace—people who show up to work but are functioning at a lesser extent due to migraine. That said, this is an important step towards recognizing the burden migraine disability has on our patients’ work life, and the extent that prevention can improve their quality of life.
References
- Kelishadi MR et al. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci Rep. 2022;12:271 (Jan 7).
- Powers SW et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. Doi: 10.1056/NEJMoa1610384.
- Tekin H, Edem P. Effects and side effects of migraine prophylaxis in children. Pediatr Int. 2021 (Dec 14).
- Autio H et al. Erenumab decreases headache-related sick leave days and health care visits: a retrospective real-world study in working patients with migraine. Neurol Ther. 2021 (Dec 10).
Most practitioners recommend a host of non-medical therapeutic options to their patients with migraine. The best studied and safest, most effective supplements remain magnesium, riboflavin/B2, and CoQ10. Alpha-lipoic acid (ALA) is a supplement with both antioxidant and anti-inflammatory effects that has showed positive protective effects in a number of medical conditions, including diabetes and episodes of oxidative stress. One migraine study1 evaluated serum ALA levels and found over 90% of people with migraine to deficient. This study sought to observe the potential benefit of supplementation with ALA in patients with episodic migraine.
This was a randomized, double-blind placebo-controlled trial over the course of 3 months. In this study, 92 female subjects with episodic migraine (defined as experiencing >2 but <15 days of headache per month) were recruited and randomized to receiving 300 mg ALA twice daily or placebo. Patients with chronic migraine, in menopause, pregnant, or lactating were excluded, as were patients with the presence of other chronic medical issues, or patients who had taken antioxidant supplements in the previous 4 months.
The primary outcomes of migraine severity, frequency, and Headache Impact Test (HIT-6) score were found to be significantly improved in the intervention group; duration of headache was not significantly different. Biochemical analysis of the two groups did show a difference in the lactate level of the intervention group, and this was considered a secondary outcome. Relevant side effects were primarily gastrointestinal, including stomach pain (higher in the placebo group), increased appetite, and constipation.
There is a great interest in finding effective non-medical treatments for migraine. These are frequently used as an adjunct to other preventive medications, or potentially as a stand-alone treatment for low frequency migraine. Many patients prefer non-medical options as well, and unfortunately many of the treatments they read about online or in less scientific spaces are unproven or unsafe. Supplementation remains an important part of migraine treatment for many practitioners and patients.
This study argues that ALA can be considered a safe and effective treatment for episodic migraine. When patients ask about non-medical options, ALA can be an additional treatment worth considering. Many patients are already taking multiple supplements before seeing their specialist, and this article informs us that there may be some treatment benefit for this supplement as well. We may not be recommending this supplement alone as a preventive treatment for migraine, but we can add a new non-medical option to consider to our mix.
Using preventive medication in pediatrics is now more controversial than it had been previously. The well known The Childhood and Adolescent Migraine Prevention (CHAMP) trial2 surprised many in the field by revealing that were no significant differences in headache frequency or disability when comparing children with migraine who received preventive medications or placebo. The CHAMP trial spotlighted the effect of non-medical therapies (cognitive behavioral therapy, biofeedback) and education. Many pediatric specialists have altered their practice paradigm in response to these results and have been more reticent to prescribe preventive medications for children with migraine. This is due to concern for potential side effects in light of the absence of direct benefit.
In an observational study of pediatric migraine,3 the investigators followed 186 children with migraine over a 3-year period to determine if the use of a number of preventive medications addresses disability (measured by Pediatric Migraine Disability Assessment [PedMIDAS]) as well as frequency, severity and duration of migraine. Other bothersome features of migraine were followed including the presence of nausea, vomiting, photophobia, analgesic use, and the side effects of the preventive medication.
The preventive medications used were cyproheptadine, flunarazine, propranolol, and topiramate—all at weight based doses. It is important to note that amitriptyline was not used in the study and there was no placebo group. This was a Turkish population, the median age was 14, and 63% were female, all of which are appropriate for a pediatric migraine study. Treatment efficacy was defined as a 50% reduction of symptoms. This was achieved in 90% of subjects in the topiramate group, 75% in the propranolol group, and 52-53% in the flunarazine and cyproheptadine groups.
Medication side effects were divided into minor or significant side effects. The only significant side effect noted was 3% of patient with palpitations; minor side effects were changes in appetite and drowsiness. More than half (57%) of patients taking topiramate experienced some side effect, 51% of the cyproheptadine group did as well, and the propranolol and flunarazine groups were noted to have side effects in 22% and 13%, respectively. Overall, 31.7% of patients had some side effect.
PedMIDAS scores improved significantly with the use of preventive medications; migraine frequency improved significantly as well, especially in the topiramate group. This study argues for the use of preventive medications in pediatric migraine. One of the most commonly used medications for migraine prevention was not investigated unfortunately. Amitriptyline is widely considered a safe and effective migraine prophylactic medication, especially at low doses. One important takeaway is the frequency of side effects at all, and especially with topiramate. It is unclear how many patients stopped their preventive medications due to a side effect. In light of this study, propranolol, which is often overlooked, might be considered a better choice for children with migraine.
Most of the patients with migraine we see are in their most productive years. Migraine disability can be a major difficulty for our patients, especially as it relates to work. The American Migraine Foundation and American Headache Society have both recently taken on initiatives that relate to migraine in the workplace. Migraine epidemiologic studies have shown that people with migraine are more likely to experience a negative impact on their careers, and migraine disability scores weigh time absent from work as well as lower function at work. Many people with migraine are concerned that having migraine may hold them back from being hired or achieving promotion.
Autio et al performed a retrospective analysis of occupationally active patients treated at a single provider (the Finnish health clinic Terveystalo).4 The authors first looked for erenumab responders, who they defined as patients who received two prescriptions for erenumab and no other calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) medication. These patients were followed for 12 months, and their data was compared to the 12-month period prior to initiating erenumab. The authors evaluated headache-related sick days, all-cause sick days, healthcare visits, and prescriptions for all medications based on a registry. This registry also provided an age- and sex-matched control group of patients with migraine not taking any CGRP mAb medication.
A total of 162 patients were included, 82 in the erenumab responder group. Headache-related sick days decreased by 74%, and headache-related healthcare visits decreased by 44%. Triptan prescription use decreased by 31.5%; all-cause sick days and healthcare visits differences were not statistically significant.
Prevention remains key in improving our patients’ quality of life and a large factor in this is their work life. This study shows that intervention with erenumab significantly decreases migraine-related absenteeism. It could be argued that the other CGRP mAb medications may have the same effect, as can many other preventive therapies. It can also be argued that even with this data we can only assume that patients function better at work with preventive therapies. Further studies will also look at the degree that “presenteeism” plays in the workplace—people who show up to work but are functioning at a lesser extent due to migraine. That said, this is an important step towards recognizing the burden migraine disability has on our patients’ work life, and the extent that prevention can improve their quality of life.
References
- Kelishadi MR et al. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci Rep. 2022;12:271 (Jan 7).
- Powers SW et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. Doi: 10.1056/NEJMoa1610384.
- Tekin H, Edem P. Effects and side effects of migraine prophylaxis in children. Pediatr Int. 2021 (Dec 14).
- Autio H et al. Erenumab decreases headache-related sick leave days and health care visits: a retrospective real-world study in working patients with migraine. Neurol Ther. 2021 (Dec 10).
Most practitioners recommend a host of non-medical therapeutic options to their patients with migraine. The best studied and safest, most effective supplements remain magnesium, riboflavin/B2, and CoQ10. Alpha-lipoic acid (ALA) is a supplement with both antioxidant and anti-inflammatory effects that has showed positive protective effects in a number of medical conditions, including diabetes and episodes of oxidative stress. One migraine study1 evaluated serum ALA levels and found over 90% of people with migraine to deficient. This study sought to observe the potential benefit of supplementation with ALA in patients with episodic migraine.
This was a randomized, double-blind placebo-controlled trial over the course of 3 months. In this study, 92 female subjects with episodic migraine (defined as experiencing >2 but <15 days of headache per month) were recruited and randomized to receiving 300 mg ALA twice daily or placebo. Patients with chronic migraine, in menopause, pregnant, or lactating were excluded, as were patients with the presence of other chronic medical issues, or patients who had taken antioxidant supplements in the previous 4 months.
The primary outcomes of migraine severity, frequency, and Headache Impact Test (HIT-6) score were found to be significantly improved in the intervention group; duration of headache was not significantly different. Biochemical analysis of the two groups did show a difference in the lactate level of the intervention group, and this was considered a secondary outcome. Relevant side effects were primarily gastrointestinal, including stomach pain (higher in the placebo group), increased appetite, and constipation.
There is a great interest in finding effective non-medical treatments for migraine. These are frequently used as an adjunct to other preventive medications, or potentially as a stand-alone treatment for low frequency migraine. Many patients prefer non-medical options as well, and unfortunately many of the treatments they read about online or in less scientific spaces are unproven or unsafe. Supplementation remains an important part of migraine treatment for many practitioners and patients.
This study argues that ALA can be considered a safe and effective treatment for episodic migraine. When patients ask about non-medical options, ALA can be an additional treatment worth considering. Many patients are already taking multiple supplements before seeing their specialist, and this article informs us that there may be some treatment benefit for this supplement as well. We may not be recommending this supplement alone as a preventive treatment for migraine, but we can add a new non-medical option to consider to our mix.
Using preventive medication in pediatrics is now more controversial than it had been previously. The well known The Childhood and Adolescent Migraine Prevention (CHAMP) trial2 surprised many in the field by revealing that were no significant differences in headache frequency or disability when comparing children with migraine who received preventive medications or placebo. The CHAMP trial spotlighted the effect of non-medical therapies (cognitive behavioral therapy, biofeedback) and education. Many pediatric specialists have altered their practice paradigm in response to these results and have been more reticent to prescribe preventive medications for children with migraine. This is due to concern for potential side effects in light of the absence of direct benefit.
In an observational study of pediatric migraine,3 the investigators followed 186 children with migraine over a 3-year period to determine if the use of a number of preventive medications addresses disability (measured by Pediatric Migraine Disability Assessment [PedMIDAS]) as well as frequency, severity and duration of migraine. Other bothersome features of migraine were followed including the presence of nausea, vomiting, photophobia, analgesic use, and the side effects of the preventive medication.
The preventive medications used were cyproheptadine, flunarazine, propranolol, and topiramate—all at weight based doses. It is important to note that amitriptyline was not used in the study and there was no placebo group. This was a Turkish population, the median age was 14, and 63% were female, all of which are appropriate for a pediatric migraine study. Treatment efficacy was defined as a 50% reduction of symptoms. This was achieved in 90% of subjects in the topiramate group, 75% in the propranolol group, and 52-53% in the flunarazine and cyproheptadine groups.
Medication side effects were divided into minor or significant side effects. The only significant side effect noted was 3% of patient with palpitations; minor side effects were changes in appetite and drowsiness. More than half (57%) of patients taking topiramate experienced some side effect, 51% of the cyproheptadine group did as well, and the propranolol and flunarazine groups were noted to have side effects in 22% and 13%, respectively. Overall, 31.7% of patients had some side effect.
PedMIDAS scores improved significantly with the use of preventive medications; migraine frequency improved significantly as well, especially in the topiramate group. This study argues for the use of preventive medications in pediatric migraine. One of the most commonly used medications for migraine prevention was not investigated unfortunately. Amitriptyline is widely considered a safe and effective migraine prophylactic medication, especially at low doses. One important takeaway is the frequency of side effects at all, and especially with topiramate. It is unclear how many patients stopped their preventive medications due to a side effect. In light of this study, propranolol, which is often overlooked, might be considered a better choice for children with migraine.
Most of the patients with migraine we see are in their most productive years. Migraine disability can be a major difficulty for our patients, especially as it relates to work. The American Migraine Foundation and American Headache Society have both recently taken on initiatives that relate to migraine in the workplace. Migraine epidemiologic studies have shown that people with migraine are more likely to experience a negative impact on their careers, and migraine disability scores weigh time absent from work as well as lower function at work. Many people with migraine are concerned that having migraine may hold them back from being hired or achieving promotion.
Autio et al performed a retrospective analysis of occupationally active patients treated at a single provider (the Finnish health clinic Terveystalo).4 The authors first looked for erenumab responders, who they defined as patients who received two prescriptions for erenumab and no other calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) medication. These patients were followed for 12 months, and their data was compared to the 12-month period prior to initiating erenumab. The authors evaluated headache-related sick days, all-cause sick days, healthcare visits, and prescriptions for all medications based on a registry. This registry also provided an age- and sex-matched control group of patients with migraine not taking any CGRP mAb medication.
A total of 162 patients were included, 82 in the erenumab responder group. Headache-related sick days decreased by 74%, and headache-related healthcare visits decreased by 44%. Triptan prescription use decreased by 31.5%; all-cause sick days and healthcare visits differences were not statistically significant.
Prevention remains key in improving our patients’ quality of life and a large factor in this is their work life. This study shows that intervention with erenumab significantly decreases migraine-related absenteeism. It could be argued that the other CGRP mAb medications may have the same effect, as can many other preventive therapies. It can also be argued that even with this data we can only assume that patients function better at work with preventive therapies. Further studies will also look at the degree that “presenteeism” plays in the workplace—people who show up to work but are functioning at a lesser extent due to migraine. That said, this is an important step towards recognizing the burden migraine disability has on our patients’ work life, and the extent that prevention can improve their quality of life.
References
- Kelishadi MR et al. The beneficial effect of Alpha-lipoic acid supplementation as a potential adjunct treatment in episodic migraines. Sci Rep. 2022;12:271 (Jan 7).
- Powers SW et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. Doi: 10.1056/NEJMoa1610384.
- Tekin H, Edem P. Effects and side effects of migraine prophylaxis in children. Pediatr Int. 2021 (Dec 14).
- Autio H et al. Erenumab decreases headache-related sick leave days and health care visits: a retrospective real-world study in working patients with migraine. Neurol Ther. 2021 (Dec 10).
Postoperative migraine: General and neuraxial anesthesia may be equally potent risk factors
Key clinical point: General anesthesia administered during major surgery poses a similar risk of postoperative migraine as neuraxial anesthesia.
Main finding: General anesthesia was not associated with a significantly higher risk of postoperative migraine compared with neuraxial anesthesia (adjusted odds ratio [aOR] 0.93; P = .357), even across patient subgroups varying in age (≥65 years: aOR 0.94; P = .698; <65 years: aOR 0.93; P = .397) or migraine subtype (with aura: aOR 1.02; P = .929; without aura: aOR 0.73; P = .069).
Study details: The data come from a nationwide population-based cohort study that matched 68,131 patients with no prior history of migraine undergoing major surgery with general anesthesia with an equal number of those undergoing neuraxial anesthesia-supported surgery.
Disclosures: The study was sponsored by Taipei Medical University, Taiwan. The authors declared having no conflicts of interest.
Source: Liao C-Y et al. Int J Environ Res Public Health. 2021;19(1):362 (Dec 30). Doi: 10.3390/ijerph19010362.
Key clinical point: General anesthesia administered during major surgery poses a similar risk of postoperative migraine as neuraxial anesthesia.
Main finding: General anesthesia was not associated with a significantly higher risk of postoperative migraine compared with neuraxial anesthesia (adjusted odds ratio [aOR] 0.93; P = .357), even across patient subgroups varying in age (≥65 years: aOR 0.94; P = .698; <65 years: aOR 0.93; P = .397) or migraine subtype (with aura: aOR 1.02; P = .929; without aura: aOR 0.73; P = .069).
Study details: The data come from a nationwide population-based cohort study that matched 68,131 patients with no prior history of migraine undergoing major surgery with general anesthesia with an equal number of those undergoing neuraxial anesthesia-supported surgery.
Disclosures: The study was sponsored by Taipei Medical University, Taiwan. The authors declared having no conflicts of interest.
Source: Liao C-Y et al. Int J Environ Res Public Health. 2021;19(1):362 (Dec 30). Doi: 10.3390/ijerph19010362.
Key clinical point: General anesthesia administered during major surgery poses a similar risk of postoperative migraine as neuraxial anesthesia.
Main finding: General anesthesia was not associated with a significantly higher risk of postoperative migraine compared with neuraxial anesthesia (adjusted odds ratio [aOR] 0.93; P = .357), even across patient subgroups varying in age (≥65 years: aOR 0.94; P = .698; <65 years: aOR 0.93; P = .397) or migraine subtype (with aura: aOR 1.02; P = .929; without aura: aOR 0.73; P = .069).
Study details: The data come from a nationwide population-based cohort study that matched 68,131 patients with no prior history of migraine undergoing major surgery with general anesthesia with an equal number of those undergoing neuraxial anesthesia-supported surgery.
Disclosures: The study was sponsored by Taipei Medical University, Taiwan. The authors declared having no conflicts of interest.
Source: Liao C-Y et al. Int J Environ Res Public Health. 2021;19(1):362 (Dec 30). Doi: 10.3390/ijerph19010362.
Prophylactic treatment lifts the quality of life in pediatric migraine
Key clinical point: When administered prophylactically, propranolol, topiramate, flunarizine, and cyproheptadine are effective at improving the health-related quality of life in pediatric patients with migraine.
Main finding: The before vs. after mean Pediatric Migraine Disability Assessment scores showed significant improvement with prophylactic topiramate (11.33 ± 13.82 vs. 33.50 ± 13.97), propranolol (12.58 ± 15.67 vs. 30.16 ± 22.97), cyproheptadine (17.00 ± 17.43 vs. 27.33 ± 19.22), or flunarizine (17.50 ± 20.14 vs. 29.89 ± 21.53; all P < .001).
Study details: The data are derived from a retrospective review study including 186 pediatric patients (aged 6 to 18 years) with migraine who were being treated prophylactically for at least 6 months with either topiramate (n = 30), cyproheptadine (n = 45), propranolol (n = 55), or flunarizine (n = 56).
Disclosures: The authors did not receive any financial aid for the study. No conflicts of interest were reported.
Source: Tekin H et al. Pediatr Int. 2021 (Dec 14). Doi: 10.1111/ped.15094.
Key clinical point: When administered prophylactically, propranolol, topiramate, flunarizine, and cyproheptadine are effective at improving the health-related quality of life in pediatric patients with migraine.
Main finding: The before vs. after mean Pediatric Migraine Disability Assessment scores showed significant improvement with prophylactic topiramate (11.33 ± 13.82 vs. 33.50 ± 13.97), propranolol (12.58 ± 15.67 vs. 30.16 ± 22.97), cyproheptadine (17.00 ± 17.43 vs. 27.33 ± 19.22), or flunarizine (17.50 ± 20.14 vs. 29.89 ± 21.53; all P < .001).
Study details: The data are derived from a retrospective review study including 186 pediatric patients (aged 6 to 18 years) with migraine who were being treated prophylactically for at least 6 months with either topiramate (n = 30), cyproheptadine (n = 45), propranolol (n = 55), or flunarizine (n = 56).
Disclosures: The authors did not receive any financial aid for the study. No conflicts of interest were reported.
Source: Tekin H et al. Pediatr Int. 2021 (Dec 14). Doi: 10.1111/ped.15094.
Key clinical point: When administered prophylactically, propranolol, topiramate, flunarizine, and cyproheptadine are effective at improving the health-related quality of life in pediatric patients with migraine.
Main finding: The before vs. after mean Pediatric Migraine Disability Assessment scores showed significant improvement with prophylactic topiramate (11.33 ± 13.82 vs. 33.50 ± 13.97), propranolol (12.58 ± 15.67 vs. 30.16 ± 22.97), cyproheptadine (17.00 ± 17.43 vs. 27.33 ± 19.22), or flunarizine (17.50 ± 20.14 vs. 29.89 ± 21.53; all P < .001).
Study details: The data are derived from a retrospective review study including 186 pediatric patients (aged 6 to 18 years) with migraine who were being treated prophylactically for at least 6 months with either topiramate (n = 30), cyproheptadine (n = 45), propranolol (n = 55), or flunarizine (n = 56).
Disclosures: The authors did not receive any financial aid for the study. No conflicts of interest were reported.
Source: Tekin H et al. Pediatr Int. 2021 (Dec 14). Doi: 10.1111/ped.15094.
Therapeutic alpha-lipoic acid supplementation may improve migraine symptoms
Key clinical point: Alpha-lipoic acid (ALA) supplementation may serve as a potential adjunct treatment option for migraine.
Main finding: ALA supplementation vs. placebo over 3 months caused a significant decrease in baseline mean headache severity (−3.59 vs. −0.70; P < .001), frequency of attacks/month (−2.55 vs. −0.40; P = .001), headache diary result (−158.79 vs. −38.63; P = .003), headache impact test-6 (HIT-6) score (−20.09 vs. −2.83; P < .001), and migraine headache index score (MHIS, −65.32 vs. −0.33; P < .001).
Study details: This was a randomized, double-blind trial including 92 female patients aged 20-50 years with episodic migraine who were randomly assigned to receive ALA (n = 47) or placebo (n = 45) for 3 months.
Disclosures: The study received financial support from the Isfahan University of Medical Sciences, Isfahan, Iran. The authors reported no potential conflict of interests.
Source: Kelishadi MR et al. Sci Rep. 2022;12:271 (Jan 7). Doi: 10.1038/s41598-021-04397-z.
Key clinical point: Alpha-lipoic acid (ALA) supplementation may serve as a potential adjunct treatment option for migraine.
Main finding: ALA supplementation vs. placebo over 3 months caused a significant decrease in baseline mean headache severity (−3.59 vs. −0.70; P < .001), frequency of attacks/month (−2.55 vs. −0.40; P = .001), headache diary result (−158.79 vs. −38.63; P = .003), headache impact test-6 (HIT-6) score (−20.09 vs. −2.83; P < .001), and migraine headache index score (MHIS, −65.32 vs. −0.33; P < .001).
Study details: This was a randomized, double-blind trial including 92 female patients aged 20-50 years with episodic migraine who were randomly assigned to receive ALA (n = 47) or placebo (n = 45) for 3 months.
Disclosures: The study received financial support from the Isfahan University of Medical Sciences, Isfahan, Iran. The authors reported no potential conflict of interests.
Source: Kelishadi MR et al. Sci Rep. 2022;12:271 (Jan 7). Doi: 10.1038/s41598-021-04397-z.
Key clinical point: Alpha-lipoic acid (ALA) supplementation may serve as a potential adjunct treatment option for migraine.
Main finding: ALA supplementation vs. placebo over 3 months caused a significant decrease in baseline mean headache severity (−3.59 vs. −0.70; P < .001), frequency of attacks/month (−2.55 vs. −0.40; P = .001), headache diary result (−158.79 vs. −38.63; P = .003), headache impact test-6 (HIT-6) score (−20.09 vs. −2.83; P < .001), and migraine headache index score (MHIS, −65.32 vs. −0.33; P < .001).
Study details: This was a randomized, double-blind trial including 92 female patients aged 20-50 years with episodic migraine who were randomly assigned to receive ALA (n = 47) or placebo (n = 45) for 3 months.
Disclosures: The study received financial support from the Isfahan University of Medical Sciences, Isfahan, Iran. The authors reported no potential conflict of interests.
Source: Kelishadi MR et al. Sci Rep. 2022;12:271 (Jan 7). Doi: 10.1038/s41598-021-04397-z.
How is migraine associated with cardiovascular and cerebrovascular events?
Key clinical point: Patients with migraine are at an increased risk of myocardial infarction (MI) and stroke, and those with migraine with aura are also at an increased risk of overall cardiovascular mortality.
Main finding: Migraine showed a positive association with MI (hazard ratio [HR] 1.36; P < .001), unspecified stroke (HR 1.30; P = .01), ischemic stroke (HR 1.35; P = .03), and hemorrhagic stroke (HR 1.43; P = .02). Migraine with aura was positively associated with cardiovascular mortality (HR 1.27; P < .001).
Study details: Findings are from a meta-analysis of 18 prospective cohort studies including 362,434 patients with migraine and 1,323,714 control participants.
Disclosures: BYQ Tan declared receiving the Ministry of Health Healthcare Research Scholarship, Singapore, and the Chan Heng Leong Research Award. CH Sia received financial support from the National University of Singapore Yong Loo Lin School of Medicine’s Junior Academic Faculty Scheme. The authors declared no competing interests.
Source: Ng CYH et al. J Neurol. 2022 (Jan 8). Doi: 10.1007/s00415-021-10930-x.
Key clinical point: Patients with migraine are at an increased risk of myocardial infarction (MI) and stroke, and those with migraine with aura are also at an increased risk of overall cardiovascular mortality.
Main finding: Migraine showed a positive association with MI (hazard ratio [HR] 1.36; P < .001), unspecified stroke (HR 1.30; P = .01), ischemic stroke (HR 1.35; P = .03), and hemorrhagic stroke (HR 1.43; P = .02). Migraine with aura was positively associated with cardiovascular mortality (HR 1.27; P < .001).
Study details: Findings are from a meta-analysis of 18 prospective cohort studies including 362,434 patients with migraine and 1,323,714 control participants.
Disclosures: BYQ Tan declared receiving the Ministry of Health Healthcare Research Scholarship, Singapore, and the Chan Heng Leong Research Award. CH Sia received financial support from the National University of Singapore Yong Loo Lin School of Medicine’s Junior Academic Faculty Scheme. The authors declared no competing interests.
Source: Ng CYH et al. J Neurol. 2022 (Jan 8). Doi: 10.1007/s00415-021-10930-x.
Key clinical point: Patients with migraine are at an increased risk of myocardial infarction (MI) and stroke, and those with migraine with aura are also at an increased risk of overall cardiovascular mortality.
Main finding: Migraine showed a positive association with MI (hazard ratio [HR] 1.36; P < .001), unspecified stroke (HR 1.30; P = .01), ischemic stroke (HR 1.35; P = .03), and hemorrhagic stroke (HR 1.43; P = .02). Migraine with aura was positively associated with cardiovascular mortality (HR 1.27; P < .001).
Study details: Findings are from a meta-analysis of 18 prospective cohort studies including 362,434 patients with migraine and 1,323,714 control participants.
Disclosures: BYQ Tan declared receiving the Ministry of Health Healthcare Research Scholarship, Singapore, and the Chan Heng Leong Research Award. CH Sia received financial support from the National University of Singapore Yong Loo Lin School of Medicine’s Junior Academic Faculty Scheme. The authors declared no competing interests.
Source: Ng CYH et al. J Neurol. 2022 (Jan 8). Doi: 10.1007/s00415-021-10930-x.
Effects of pausing migraine prophylaxis with CGRP-receptor mAb hint at therapy resumption
Key clinical point: Cessation of calcitonin gene‐related peptide-receptor (CGRP-R) monoclonal antibody (mAb) prophylaxis worsens headache impact and health-related quality of life in patients with migraine.
Main finding: After 16 weeks from the last mAb injection, the mean Headache Impact Test-6 sum score increased by 3.69 (P < .001), mean EuroQol-5-Dimension-5-level declined by −0.07 (P = .013) and mean physical and mental component summary of Short Form-12 score deteriorated by −4.04 (P = .013) and −2.73 (P = .003), respectively.
Study details: This was a longitudinal, prospective cohort study involving 61 adult patients with episodic/chronic migraine receiving prophylaxis with a CGRP-R mAb (erenumab, n = 29; galcanezumab/fremanezumab, n = 32) for ≥8 months before a planned treatment cessation attempt.
Disclosures: The authors did not receive any financial support for the study. Some of the authors, including the lead author, reported serving on the advisory board of or receiving personal fees, speaker/consultant honoraria, and research grants from various organizations.
Source: Terhart M et al. J Headache Pain. 2021;22:158 (Dec 31). Doi: 10.1186/s10194-021-01368-7.
Key clinical point: Cessation of calcitonin gene‐related peptide-receptor (CGRP-R) monoclonal antibody (mAb) prophylaxis worsens headache impact and health-related quality of life in patients with migraine.
Main finding: After 16 weeks from the last mAb injection, the mean Headache Impact Test-6 sum score increased by 3.69 (P < .001), mean EuroQol-5-Dimension-5-level declined by −0.07 (P = .013) and mean physical and mental component summary of Short Form-12 score deteriorated by −4.04 (P = .013) and −2.73 (P = .003), respectively.
Study details: This was a longitudinal, prospective cohort study involving 61 adult patients with episodic/chronic migraine receiving prophylaxis with a CGRP-R mAb (erenumab, n = 29; galcanezumab/fremanezumab, n = 32) for ≥8 months before a planned treatment cessation attempt.
Disclosures: The authors did not receive any financial support for the study. Some of the authors, including the lead author, reported serving on the advisory board of or receiving personal fees, speaker/consultant honoraria, and research grants from various organizations.
Source: Terhart M et al. J Headache Pain. 2021;22:158 (Dec 31). Doi: 10.1186/s10194-021-01368-7.
Key clinical point: Cessation of calcitonin gene‐related peptide-receptor (CGRP-R) monoclonal antibody (mAb) prophylaxis worsens headache impact and health-related quality of life in patients with migraine.
Main finding: After 16 weeks from the last mAb injection, the mean Headache Impact Test-6 sum score increased by 3.69 (P < .001), mean EuroQol-5-Dimension-5-level declined by −0.07 (P = .013) and mean physical and mental component summary of Short Form-12 score deteriorated by −4.04 (P = .013) and −2.73 (P = .003), respectively.
Study details: This was a longitudinal, prospective cohort study involving 61 adult patients with episodic/chronic migraine receiving prophylaxis with a CGRP-R mAb (erenumab, n = 29; galcanezumab/fremanezumab, n = 32) for ≥8 months before a planned treatment cessation attempt.
Disclosures: The authors did not receive any financial support for the study. Some of the authors, including the lead author, reported serving on the advisory board of or receiving personal fees, speaker/consultant honoraria, and research grants from various organizations.
Source: Terhart M et al. J Headache Pain. 2021;22:158 (Dec 31). Doi: 10.1186/s10194-021-01368-7.
Real-world value of fremanezumab therapy against migraine
Key clinical point: Fremanezumab therapy led to significant reductions in patient-reported headache frequency and migraine pain intensity in patients with migraine.
Main finding: After fremanezumab initiation, the mean number of headache days/month reduced from 22.24 days preindex to 8.24 days postindex (P < .0001) and the mean visual analog scale pain score from 5.47 preindex to 4.51 postindex (P = .014).
Study details: This was a retrospective, observational cohort study including 172 adult patients with migraine who received fremanezumab (index event), had ≥6 months of enrollment/treatment history preindex and ≥1 month postindex along with no pregnancy event during the study.
Disclosures: The study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc. The lead author received research support from and served as a consultant for various organizations including Teva. Some of the authors are current/former employees of Teva.
Source: McAllister P et al. J Headache Pain. 2021;22:156 (Dec 20). Doi: 10.1186/s10194-021-01358-9.
Key clinical point: Fremanezumab therapy led to significant reductions in patient-reported headache frequency and migraine pain intensity in patients with migraine.
Main finding: After fremanezumab initiation, the mean number of headache days/month reduced from 22.24 days preindex to 8.24 days postindex (P < .0001) and the mean visual analog scale pain score from 5.47 preindex to 4.51 postindex (P = .014).
Study details: This was a retrospective, observational cohort study including 172 adult patients with migraine who received fremanezumab (index event), had ≥6 months of enrollment/treatment history preindex and ≥1 month postindex along with no pregnancy event during the study.
Disclosures: The study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc. The lead author received research support from and served as a consultant for various organizations including Teva. Some of the authors are current/former employees of Teva.
Source: McAllister P et al. J Headache Pain. 2021;22:156 (Dec 20). Doi: 10.1186/s10194-021-01358-9.
Key clinical point: Fremanezumab therapy led to significant reductions in patient-reported headache frequency and migraine pain intensity in patients with migraine.
Main finding: After fremanezumab initiation, the mean number of headache days/month reduced from 22.24 days preindex to 8.24 days postindex (P < .0001) and the mean visual analog scale pain score from 5.47 preindex to 4.51 postindex (P = .014).
Study details: This was a retrospective, observational cohort study including 172 adult patients with migraine who received fremanezumab (index event), had ≥6 months of enrollment/treatment history preindex and ≥1 month postindex along with no pregnancy event during the study.
Disclosures: The study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc. The lead author received research support from and served as a consultant for various organizations including Teva. Some of the authors are current/former employees of Teva.
Source: McAllister P et al. J Headache Pain. 2021;22:156 (Dec 20). Doi: 10.1186/s10194-021-01358-9.
Fremanezumab efficacy against difficult-to-treat migraine is unperturbed by age or sex
Key clinical point: The efficacy of fremanezumab for preventive treatment of difficult-to-treat migraine remains unaffected by age or sex.
Main finding: At week 12, quarterly and monthly fremanezumab reduced the monthly average of migraine days irrespective of age (18-45 years: quarterly, −4.1 days; monthly, −4.7 days; placebo, −0.9 days; >45 years: quarterly, −3.6 days; monthly, −3.7 days; placebo, −0.3 days; both P < .001) and sex (men: quarterly, −4.1 days; monthly, −4.6 days; placebo, −0.3 days; women: quarterly, −3.6 days; monthly, −3.9 days; placebo, −0.6 days; both P < .001).
Study details: This post hoc analysis of the phase 3b FOCUS trial included 837 adult patients with chronic/episodic migraine and an inadequate response to multiple alternative therapies, who were randomly assigned to quarterly fremanezumab, monthly fremanezumab, or placebo over 12 weeks.
Disclosures: The study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc., PA. Some of the authors, including the lead author, received research funds or consultancy/speaker fees from various sources including Teva, which the rest were employees/stock owners of.
Source: MaassenVanDenBrink A et al. J Headache Pain. 2021;22:152 (Dec 18). Doi: 10.1186/s10194-021-01336-1.
Key clinical point: The efficacy of fremanezumab for preventive treatment of difficult-to-treat migraine remains unaffected by age or sex.
Main finding: At week 12, quarterly and monthly fremanezumab reduced the monthly average of migraine days irrespective of age (18-45 years: quarterly, −4.1 days; monthly, −4.7 days; placebo, −0.9 days; >45 years: quarterly, −3.6 days; monthly, −3.7 days; placebo, −0.3 days; both P < .001) and sex (men: quarterly, −4.1 days; monthly, −4.6 days; placebo, −0.3 days; women: quarterly, −3.6 days; monthly, −3.9 days; placebo, −0.6 days; both P < .001).
Study details: This post hoc analysis of the phase 3b FOCUS trial included 837 adult patients with chronic/episodic migraine and an inadequate response to multiple alternative therapies, who were randomly assigned to quarterly fremanezumab, monthly fremanezumab, or placebo over 12 weeks.
Disclosures: The study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc., PA. Some of the authors, including the lead author, received research funds or consultancy/speaker fees from various sources including Teva, which the rest were employees/stock owners of.
Source: MaassenVanDenBrink A et al. J Headache Pain. 2021;22:152 (Dec 18). Doi: 10.1186/s10194-021-01336-1.
Key clinical point: The efficacy of fremanezumab for preventive treatment of difficult-to-treat migraine remains unaffected by age or sex.
Main finding: At week 12, quarterly and monthly fremanezumab reduced the monthly average of migraine days irrespective of age (18-45 years: quarterly, −4.1 days; monthly, −4.7 days; placebo, −0.9 days; >45 years: quarterly, −3.6 days; monthly, −3.7 days; placebo, −0.3 days; both P < .001) and sex (men: quarterly, −4.1 days; monthly, −4.6 days; placebo, −0.3 days; women: quarterly, −3.6 days; monthly, −3.9 days; placebo, −0.6 days; both P < .001).
Study details: This post hoc analysis of the phase 3b FOCUS trial included 837 adult patients with chronic/episodic migraine and an inadequate response to multiple alternative therapies, who were randomly assigned to quarterly fremanezumab, monthly fremanezumab, or placebo over 12 weeks.
Disclosures: The study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc., PA. Some of the authors, including the lead author, received research funds or consultancy/speaker fees from various sources including Teva, which the rest were employees/stock owners of.
Source: MaassenVanDenBrink A et al. J Headache Pain. 2021;22:152 (Dec 18). Doi: 10.1186/s10194-021-01336-1.