User login
Old drug verapamil may have new use in type 1 diabetes
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.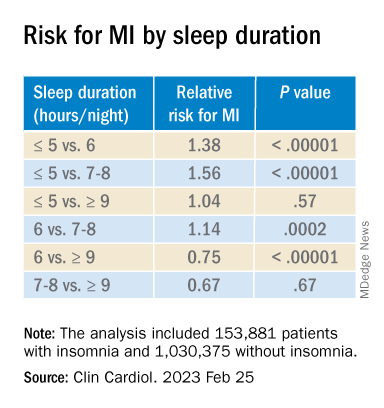
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Fewer than 10% of eligible type 2 diabetes patients get new, pricey drugs
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Artificial sweetener in ‘keto foods’ tied to cardiovascular risk
Erythritol is one of the most widely used artificial sweeteners with rapidly increasing prevalence in processed and “keto-related” foods. Artificial sweeteners are “generally recognized as safe” (GRAS) by the U.S. Food and Drug Administration, so there is no requirement for long-term safety studies, and little is known about the long-term health effects.
The current research, published online in Nature Medicine by Marco Witkowski, MD, of the Lerner Research Institute at Cleveland Clinic and colleagues, had multiple parts.
First, in a group of patients undergoing cardiac risk assessment, the researchers found that high levels of polyols, especially erythritol, were associated with increased 3-year risk of MACE, defined as cardiovascular death or nonfatal myocardial infarction or stroke.
Next, the association of erythritol with this outcome was reproduced in two large U.S. and European groups of stable patients undergoing elective cardiac evaluation.
Next, adding erythritol to whole blood or platelets led to clot activation. And lastly, in eight healthy volunteers, ingesting 30 g of an erythritol-sweetened drink – comparable to a single can of commercially available beverage or a pint of keto ice cream – induced marked and sustained (> 2 day) increases in levels of plasma erythritol.
“Our study shows that when participants consumed an artificially sweetened beverage with an amount of erythritol found in many processed foods, markedly elevated levels in the blood are observed for days – levels well above those observed to enhance clotting risks,” said senior author Stanley L. Hazen, MD, PhD.
“It is important that further safety studies are conducted to examine the long-term effects of artificial sweeteners in general, and erythritol specifically, on risks for heart attack and stroke, particularly in people at higher risk for cardiovascular disease,” Dr. Hazen, co–section head of preventive cardiology at Cleveland Clinic, said in a press release from his institution.
“Sweeteners like erythritol have rapidly increased in popularity in recent years, but there needs to be more in-depth research into their long-term effects. Cardiovascular disease builds over time, and heart disease is the leading cause of death globally. We need to make sure the foods we eat aren’t hidden contributors,” Dr. Hazen urged.
The topic remains controversial.
Duane Mellor, PhD, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England, told the U.K. Science Media Centre: “This paper effectively shows multiple pieces of a jigsaw exploring the effects of erythritol – although it claims to show an associated risk with the use of erythritol as an artificial sweetener and cardiovascular disease, I believe it fails to do so, as ultimately, erythritol can be made inside our bodies and the intake in most people’s diet is much lower than the amount given in this study.”
Dr. Hazen countered that data from the 2013-2014 National Health and Nutrition Examination Survey (NHANES) in the United States show that, in some individuals, daily intake of erythritol is estimated to reach 30 g/day.
“Many try and reduce sugar intake by taking many teaspoons of erythritol in their tea, coffee, etc., instead of sugar,” Dr. Hazen added. “Or they eat keto processed foods that have significant quantities of erythritol within it.”
“These studies are a warning for how our processed food (keto and zero sugar, especially) may inadvertently be causing risk/harm. … in the very subset of subjects who are most vulnerable,” according to Dr. Hazen.
Erythritol marketed as ‘zero calorie’, ‘non-nutritive’, or ‘natural’
Patients with type 2 diabetes and obesity are often advised to replace sugar with artificial sweeteners for better glucose control and weight loss, but growing epidemiologic evidence links artificial sweetener consumption with weight gain, insulin resistance, type 2 diabetes, and cardiovascular disease, the researchers write.
Erythritol is naturally present in low amounts in fruits and vegetables; the artificial sweetener erythritol that is produced from corn is only 70% as sweet as sugar.
Upon ingestion it is poorly metabolized, and most is excreted in the urine, so it is characterized as a “zero-calorie,” “non-nutritive,” or “natural sweetener.” It is predicted to double in marketshare in the sweetener sector in the next 5 years.
Multipart study
In the first part of their study, in a discovery cohort in 1,157 patients undergoing cardiovascular assessment with 3-year outcomes, the researchers identified polyols that were associated with MACE, and erythritol was among the top MACE-associated molecules.
Next, in a U.S. validation cohort of 2,149 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 1.8-fold higher risk of MACE than patients in the lowest quartile (P = .007), after adjusting for cardiovascular risk factors.
In a European validation cohort of 833 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 2.21-fold higher risk of MACE than patients in the lowest quartile (P = .010, after adjustment).
At physiologic levels, erythritol enhanced platelet reactivity in vitro and thrombosis formation in vivo.
Finally, in a prospective pilot intervention study, erythritol ingestion in healthy volunteers induced marked and sustained increases in plasma erythritol levels well above thresholds associated with heightened platelet reactivity and thrombosis potential in in vitro and in vivo studies.
Others weigh in
“While I think the finding certainly warrants further investigation, don’t throw out your sweeteners just yet,” commented Oliver Jones, PhD, professor of chemistry at the Royal Melbourne Institute of Technology.
“This study only looks at erythritol, and artificial sweeteners are generally considered safe. Any possible (and, as yet unproven) risks of excess erythritol would also need to be balanced against the very real health risks of excess glucose consumption,” he said.
Dr. Hazen responded: “True enough. Erythritol is but one of many artificial sweeteners. That is why it is important to read labels. This study can make patients be informed about how to potentially avoid something that might cause them inadvertent harm.”
“The key findings of this study are that high blood levels of erythritol are strongly associated with cardiovascular outcomes in high-risk patients, which has been replicated in separate validation studies,” said Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics, King’s College London.
“Diabetes UK currently advises diabetes patients not to use polyols,” he added.
Dr. Hazen noted that “About three-quarters of the participants had coronary disease, high blood pressure, and about a fifth had diabetes.”
The researchers acknowledge, however, that the observational studies cannot show cause and effect.
The study was supported by the Office of Dietary Supplements at the National Institutes of Health, the Leducq Foundation, and the German Research Foundation (Deutsche Forschungsgemeinschaft). Dr. Mellor, Dr. Jones, and Dr. Sanders have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Erythritol is one of the most widely used artificial sweeteners with rapidly increasing prevalence in processed and “keto-related” foods. Artificial sweeteners are “generally recognized as safe” (GRAS) by the U.S. Food and Drug Administration, so there is no requirement for long-term safety studies, and little is known about the long-term health effects.
The current research, published online in Nature Medicine by Marco Witkowski, MD, of the Lerner Research Institute at Cleveland Clinic and colleagues, had multiple parts.
First, in a group of patients undergoing cardiac risk assessment, the researchers found that high levels of polyols, especially erythritol, were associated with increased 3-year risk of MACE, defined as cardiovascular death or nonfatal myocardial infarction or stroke.
Next, the association of erythritol with this outcome was reproduced in two large U.S. and European groups of stable patients undergoing elective cardiac evaluation.
Next, adding erythritol to whole blood or platelets led to clot activation. And lastly, in eight healthy volunteers, ingesting 30 g of an erythritol-sweetened drink – comparable to a single can of commercially available beverage or a pint of keto ice cream – induced marked and sustained (> 2 day) increases in levels of plasma erythritol.
“Our study shows that when participants consumed an artificially sweetened beverage with an amount of erythritol found in many processed foods, markedly elevated levels in the blood are observed for days – levels well above those observed to enhance clotting risks,” said senior author Stanley L. Hazen, MD, PhD.
“It is important that further safety studies are conducted to examine the long-term effects of artificial sweeteners in general, and erythritol specifically, on risks for heart attack and stroke, particularly in people at higher risk for cardiovascular disease,” Dr. Hazen, co–section head of preventive cardiology at Cleveland Clinic, said in a press release from his institution.
“Sweeteners like erythritol have rapidly increased in popularity in recent years, but there needs to be more in-depth research into their long-term effects. Cardiovascular disease builds over time, and heart disease is the leading cause of death globally. We need to make sure the foods we eat aren’t hidden contributors,” Dr. Hazen urged.
The topic remains controversial.
Duane Mellor, PhD, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England, told the U.K. Science Media Centre: “This paper effectively shows multiple pieces of a jigsaw exploring the effects of erythritol – although it claims to show an associated risk with the use of erythritol as an artificial sweetener and cardiovascular disease, I believe it fails to do so, as ultimately, erythritol can be made inside our bodies and the intake in most people’s diet is much lower than the amount given in this study.”
Dr. Hazen countered that data from the 2013-2014 National Health and Nutrition Examination Survey (NHANES) in the United States show that, in some individuals, daily intake of erythritol is estimated to reach 30 g/day.
“Many try and reduce sugar intake by taking many teaspoons of erythritol in their tea, coffee, etc., instead of sugar,” Dr. Hazen added. “Or they eat keto processed foods that have significant quantities of erythritol within it.”
“These studies are a warning for how our processed food (keto and zero sugar, especially) may inadvertently be causing risk/harm. … in the very subset of subjects who are most vulnerable,” according to Dr. Hazen.
Erythritol marketed as ‘zero calorie’, ‘non-nutritive’, or ‘natural’
Patients with type 2 diabetes and obesity are often advised to replace sugar with artificial sweeteners for better glucose control and weight loss, but growing epidemiologic evidence links artificial sweetener consumption with weight gain, insulin resistance, type 2 diabetes, and cardiovascular disease, the researchers write.
Erythritol is naturally present in low amounts in fruits and vegetables; the artificial sweetener erythritol that is produced from corn is only 70% as sweet as sugar.
Upon ingestion it is poorly metabolized, and most is excreted in the urine, so it is characterized as a “zero-calorie,” “non-nutritive,” or “natural sweetener.” It is predicted to double in marketshare in the sweetener sector in the next 5 years.
Multipart study
In the first part of their study, in a discovery cohort in 1,157 patients undergoing cardiovascular assessment with 3-year outcomes, the researchers identified polyols that were associated with MACE, and erythritol was among the top MACE-associated molecules.
Next, in a U.S. validation cohort of 2,149 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 1.8-fold higher risk of MACE than patients in the lowest quartile (P = .007), after adjusting for cardiovascular risk factors.
In a European validation cohort of 833 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 2.21-fold higher risk of MACE than patients in the lowest quartile (P = .010, after adjustment).
At physiologic levels, erythritol enhanced platelet reactivity in vitro and thrombosis formation in vivo.
Finally, in a prospective pilot intervention study, erythritol ingestion in healthy volunteers induced marked and sustained increases in plasma erythritol levels well above thresholds associated with heightened platelet reactivity and thrombosis potential in in vitro and in vivo studies.
Others weigh in
“While I think the finding certainly warrants further investigation, don’t throw out your sweeteners just yet,” commented Oliver Jones, PhD, professor of chemistry at the Royal Melbourne Institute of Technology.
“This study only looks at erythritol, and artificial sweeteners are generally considered safe. Any possible (and, as yet unproven) risks of excess erythritol would also need to be balanced against the very real health risks of excess glucose consumption,” he said.
Dr. Hazen responded: “True enough. Erythritol is but one of many artificial sweeteners. That is why it is important to read labels. This study can make patients be informed about how to potentially avoid something that might cause them inadvertent harm.”
“The key findings of this study are that high blood levels of erythritol are strongly associated with cardiovascular outcomes in high-risk patients, which has been replicated in separate validation studies,” said Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics, King’s College London.
“Diabetes UK currently advises diabetes patients not to use polyols,” he added.
Dr. Hazen noted that “About three-quarters of the participants had coronary disease, high blood pressure, and about a fifth had diabetes.”
The researchers acknowledge, however, that the observational studies cannot show cause and effect.
The study was supported by the Office of Dietary Supplements at the National Institutes of Health, the Leducq Foundation, and the German Research Foundation (Deutsche Forschungsgemeinschaft). Dr. Mellor, Dr. Jones, and Dr. Sanders have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Erythritol is one of the most widely used artificial sweeteners with rapidly increasing prevalence in processed and “keto-related” foods. Artificial sweeteners are “generally recognized as safe” (GRAS) by the U.S. Food and Drug Administration, so there is no requirement for long-term safety studies, and little is known about the long-term health effects.
The current research, published online in Nature Medicine by Marco Witkowski, MD, of the Lerner Research Institute at Cleveland Clinic and colleagues, had multiple parts.
First, in a group of patients undergoing cardiac risk assessment, the researchers found that high levels of polyols, especially erythritol, were associated with increased 3-year risk of MACE, defined as cardiovascular death or nonfatal myocardial infarction or stroke.
Next, the association of erythritol with this outcome was reproduced in two large U.S. and European groups of stable patients undergoing elective cardiac evaluation.
Next, adding erythritol to whole blood or platelets led to clot activation. And lastly, in eight healthy volunteers, ingesting 30 g of an erythritol-sweetened drink – comparable to a single can of commercially available beverage or a pint of keto ice cream – induced marked and sustained (> 2 day) increases in levels of plasma erythritol.
“Our study shows that when participants consumed an artificially sweetened beverage with an amount of erythritol found in many processed foods, markedly elevated levels in the blood are observed for days – levels well above those observed to enhance clotting risks,” said senior author Stanley L. Hazen, MD, PhD.
“It is important that further safety studies are conducted to examine the long-term effects of artificial sweeteners in general, and erythritol specifically, on risks for heart attack and stroke, particularly in people at higher risk for cardiovascular disease,” Dr. Hazen, co–section head of preventive cardiology at Cleveland Clinic, said in a press release from his institution.
“Sweeteners like erythritol have rapidly increased in popularity in recent years, but there needs to be more in-depth research into their long-term effects. Cardiovascular disease builds over time, and heart disease is the leading cause of death globally. We need to make sure the foods we eat aren’t hidden contributors,” Dr. Hazen urged.
The topic remains controversial.
Duane Mellor, PhD, a registered dietitian and senior teaching fellow at Aston University, Birmingham, England, told the U.K. Science Media Centre: “This paper effectively shows multiple pieces of a jigsaw exploring the effects of erythritol – although it claims to show an associated risk with the use of erythritol as an artificial sweetener and cardiovascular disease, I believe it fails to do so, as ultimately, erythritol can be made inside our bodies and the intake in most people’s diet is much lower than the amount given in this study.”
Dr. Hazen countered that data from the 2013-2014 National Health and Nutrition Examination Survey (NHANES) in the United States show that, in some individuals, daily intake of erythritol is estimated to reach 30 g/day.
“Many try and reduce sugar intake by taking many teaspoons of erythritol in their tea, coffee, etc., instead of sugar,” Dr. Hazen added. “Or they eat keto processed foods that have significant quantities of erythritol within it.”
“These studies are a warning for how our processed food (keto and zero sugar, especially) may inadvertently be causing risk/harm. … in the very subset of subjects who are most vulnerable,” according to Dr. Hazen.
Erythritol marketed as ‘zero calorie’, ‘non-nutritive’, or ‘natural’
Patients with type 2 diabetes and obesity are often advised to replace sugar with artificial sweeteners for better glucose control and weight loss, but growing epidemiologic evidence links artificial sweetener consumption with weight gain, insulin resistance, type 2 diabetes, and cardiovascular disease, the researchers write.
Erythritol is naturally present in low amounts in fruits and vegetables; the artificial sweetener erythritol that is produced from corn is only 70% as sweet as sugar.
Upon ingestion it is poorly metabolized, and most is excreted in the urine, so it is characterized as a “zero-calorie,” “non-nutritive,” or “natural sweetener.” It is predicted to double in marketshare in the sweetener sector in the next 5 years.
Multipart study
In the first part of their study, in a discovery cohort in 1,157 patients undergoing cardiovascular assessment with 3-year outcomes, the researchers identified polyols that were associated with MACE, and erythritol was among the top MACE-associated molecules.
Next, in a U.S. validation cohort of 2,149 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 1.8-fold higher risk of MACE than patients in the lowest quartile (P = .007), after adjusting for cardiovascular risk factors.
In a European validation cohort of 833 patients, over a 3-year follow-up, patients with plasma levels of erythritol in the highest quartile had a 2.21-fold higher risk of MACE than patients in the lowest quartile (P = .010, after adjustment).
At physiologic levels, erythritol enhanced platelet reactivity in vitro and thrombosis formation in vivo.
Finally, in a prospective pilot intervention study, erythritol ingestion in healthy volunteers induced marked and sustained increases in plasma erythritol levels well above thresholds associated with heightened platelet reactivity and thrombosis potential in in vitro and in vivo studies.
Others weigh in
“While I think the finding certainly warrants further investigation, don’t throw out your sweeteners just yet,” commented Oliver Jones, PhD, professor of chemistry at the Royal Melbourne Institute of Technology.
“This study only looks at erythritol, and artificial sweeteners are generally considered safe. Any possible (and, as yet unproven) risks of excess erythritol would also need to be balanced against the very real health risks of excess glucose consumption,” he said.
Dr. Hazen responded: “True enough. Erythritol is but one of many artificial sweeteners. That is why it is important to read labels. This study can make patients be informed about how to potentially avoid something that might cause them inadvertent harm.”
“The key findings of this study are that high blood levels of erythritol are strongly associated with cardiovascular outcomes in high-risk patients, which has been replicated in separate validation studies,” said Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics, King’s College London.
“Diabetes UK currently advises diabetes patients not to use polyols,” he added.
Dr. Hazen noted that “About three-quarters of the participants had coronary disease, high blood pressure, and about a fifth had diabetes.”
The researchers acknowledge, however, that the observational studies cannot show cause and effect.
The study was supported by the Office of Dietary Supplements at the National Institutes of Health, the Leducq Foundation, and the German Research Foundation (Deutsche Forschungsgemeinschaft). Dr. Mellor, Dr. Jones, and Dr. Sanders have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE MEDICINE
New AHA statement urges focus on CV risk before pregnancy
Increased public health and research efforts to optimize prepregnancy cardiovascular health are needed, particularly among those in under-represented racial and ethnic groups, according to a new scientific statement from the American Heart Association.
“We have released this statement at this time because there is a maternal health crisis in the U.S. with rising maternal morbidity and mortality rates, which are the highest among high-income countries,” chair of the scientific statement writing group, Sadiya S. Khan, MD, told this news organization.
Cardiovascular disease (CVD) is the leading cause of death during pregnancy and the postpartum period and represents 26.5% of pregnancy-related deaths, the statement reports.
“While there is a lot of emphasis in trying to reduce cardiovascular risk during the period of actual pregnancy, much of that risk has often already developed and the women have been living with it for some time, so interventions during pregnancy may be too late,” Dr. Khan, assistant professor of medicine and preventive medicine at Northwestern University, Chicago, said.
“We wanted to try and emphasize the importance of starting to reduce cardiovascular risk earlier before pregnancy. In terms of improving cardiovascular health, this should have benefits both for the mother and the child,” she added.
The statement, “Optimizing Prepregnancy Cardiovascular Health to Improve Outcomes in Pregnant and Postpartum Individuals and Offspring” was published online in a “Go Red For Women” spotlight issue of the AHA publication Circulation.
Currently, nearly one in five births are complicated by such an adverse pregnancy outcome, and there is a strong association between these complications and risk for subsequent cardiovascular disease.
Prepregnancy window
Over the past decade, rates of adverse pregnancy outcomes have increased significantly in the United States, with a near doubling in rates of hypertensive disorders of pregnancy, and there are persistent disparities, with Black individuals significantly more likely to experience adverse pregnancy outcomes, the statement notes.
Emerging data suggest that these complications have, at least in part, prepregnancy origins. Thus, the prepregnancy period may be a critical window during which interventions have a great potential for benefit in both women and their offspring, it says.
The authors suggest a life-course approach to measure, modify, and monitor prepregnancy cardiovascular health, with all clinicians who interact with pregnancy-capable individuals emphasizing optimization of cardiovascular health beginning early in childhood.
“Leveraging these opportunities to target cardiovascular health has the potential to improve health across the life course and for subsequent generations,” they add.
Critical research gap
Despite the evidence linking an individual’s prepregnancy health to their offspring’s health, there are no large trials to test whether improving overall cardiovascular health before pregnancy will reduce pregnancy complications, pregnancy-related cardiovascular death, or cardiovascular risk for offspring. The statement authors suggest that such a trial should be considered.
“This would be a big undertaking, but it could be feasible and could be really impactful,” Dr. Khan said. “Of course it would be challenging to recruit women who are planning a pregnancy and to follow them to see if they do get pregnant and consider interventions and outcomes, but given the importance of the need, we think this is something that should be invested in.”
She pointed out that the main way to improve the cardiovascular health of this cohort would be through behavioral counseling on physical activity and diet. “We need to develop strategies tailored to this age group – young women and those who may already have young children – and often the last thing they are thinking about is themselves and their own health.”
She explained that while it is presumed that controlling cardiovascular risk factors will be beneficial, the bigger question is how that can be achieved. “Behavioral interventions are difficult to achieve and often have low adherence, so the focus of the trials should be on strategies on how to deliver behavioral counseling to achieve better cardiovascular health in this population.”
Dr. Khan stressed that any approaches to improving prepregnancy cardiovascular health must address the current racial disparities that are present. “We must make sure that our policies are successful not just in improving cardiovascular health but to ensure it is done equitably. We must find ways to ensure all individuals can access care.”
A version of this article first appeared on Medscape.com.
Increased public health and research efforts to optimize prepregnancy cardiovascular health are needed, particularly among those in under-represented racial and ethnic groups, according to a new scientific statement from the American Heart Association.
“We have released this statement at this time because there is a maternal health crisis in the U.S. with rising maternal morbidity and mortality rates, which are the highest among high-income countries,” chair of the scientific statement writing group, Sadiya S. Khan, MD, told this news organization.
Cardiovascular disease (CVD) is the leading cause of death during pregnancy and the postpartum period and represents 26.5% of pregnancy-related deaths, the statement reports.
“While there is a lot of emphasis in trying to reduce cardiovascular risk during the period of actual pregnancy, much of that risk has often already developed and the women have been living with it for some time, so interventions during pregnancy may be too late,” Dr. Khan, assistant professor of medicine and preventive medicine at Northwestern University, Chicago, said.
“We wanted to try and emphasize the importance of starting to reduce cardiovascular risk earlier before pregnancy. In terms of improving cardiovascular health, this should have benefits both for the mother and the child,” she added.
The statement, “Optimizing Prepregnancy Cardiovascular Health to Improve Outcomes in Pregnant and Postpartum Individuals and Offspring” was published online in a “Go Red For Women” spotlight issue of the AHA publication Circulation.
Currently, nearly one in five births are complicated by such an adverse pregnancy outcome, and there is a strong association between these complications and risk for subsequent cardiovascular disease.
Prepregnancy window
Over the past decade, rates of adverse pregnancy outcomes have increased significantly in the United States, with a near doubling in rates of hypertensive disorders of pregnancy, and there are persistent disparities, with Black individuals significantly more likely to experience adverse pregnancy outcomes, the statement notes.
Emerging data suggest that these complications have, at least in part, prepregnancy origins. Thus, the prepregnancy period may be a critical window during which interventions have a great potential for benefit in both women and their offspring, it says.
The authors suggest a life-course approach to measure, modify, and monitor prepregnancy cardiovascular health, with all clinicians who interact with pregnancy-capable individuals emphasizing optimization of cardiovascular health beginning early in childhood.
“Leveraging these opportunities to target cardiovascular health has the potential to improve health across the life course and for subsequent generations,” they add.
Critical research gap
Despite the evidence linking an individual’s prepregnancy health to their offspring’s health, there are no large trials to test whether improving overall cardiovascular health before pregnancy will reduce pregnancy complications, pregnancy-related cardiovascular death, or cardiovascular risk for offspring. The statement authors suggest that such a trial should be considered.
“This would be a big undertaking, but it could be feasible and could be really impactful,” Dr. Khan said. “Of course it would be challenging to recruit women who are planning a pregnancy and to follow them to see if they do get pregnant and consider interventions and outcomes, but given the importance of the need, we think this is something that should be invested in.”
She pointed out that the main way to improve the cardiovascular health of this cohort would be through behavioral counseling on physical activity and diet. “We need to develop strategies tailored to this age group – young women and those who may already have young children – and often the last thing they are thinking about is themselves and their own health.”
She explained that while it is presumed that controlling cardiovascular risk factors will be beneficial, the bigger question is how that can be achieved. “Behavioral interventions are difficult to achieve and often have low adherence, so the focus of the trials should be on strategies on how to deliver behavioral counseling to achieve better cardiovascular health in this population.”
Dr. Khan stressed that any approaches to improving prepregnancy cardiovascular health must address the current racial disparities that are present. “We must make sure that our policies are successful not just in improving cardiovascular health but to ensure it is done equitably. We must find ways to ensure all individuals can access care.”
A version of this article first appeared on Medscape.com.
Increased public health and research efforts to optimize prepregnancy cardiovascular health are needed, particularly among those in under-represented racial and ethnic groups, according to a new scientific statement from the American Heart Association.
“We have released this statement at this time because there is a maternal health crisis in the U.S. with rising maternal morbidity and mortality rates, which are the highest among high-income countries,” chair of the scientific statement writing group, Sadiya S. Khan, MD, told this news organization.
Cardiovascular disease (CVD) is the leading cause of death during pregnancy and the postpartum period and represents 26.5% of pregnancy-related deaths, the statement reports.
“While there is a lot of emphasis in trying to reduce cardiovascular risk during the period of actual pregnancy, much of that risk has often already developed and the women have been living with it for some time, so interventions during pregnancy may be too late,” Dr. Khan, assistant professor of medicine and preventive medicine at Northwestern University, Chicago, said.
“We wanted to try and emphasize the importance of starting to reduce cardiovascular risk earlier before pregnancy. In terms of improving cardiovascular health, this should have benefits both for the mother and the child,” she added.
The statement, “Optimizing Prepregnancy Cardiovascular Health to Improve Outcomes in Pregnant and Postpartum Individuals and Offspring” was published online in a “Go Red For Women” spotlight issue of the AHA publication Circulation.
Currently, nearly one in five births are complicated by such an adverse pregnancy outcome, and there is a strong association between these complications and risk for subsequent cardiovascular disease.
Prepregnancy window
Over the past decade, rates of adverse pregnancy outcomes have increased significantly in the United States, with a near doubling in rates of hypertensive disorders of pregnancy, and there are persistent disparities, with Black individuals significantly more likely to experience adverse pregnancy outcomes, the statement notes.
Emerging data suggest that these complications have, at least in part, prepregnancy origins. Thus, the prepregnancy period may be a critical window during which interventions have a great potential for benefit in both women and their offspring, it says.
The authors suggest a life-course approach to measure, modify, and monitor prepregnancy cardiovascular health, with all clinicians who interact with pregnancy-capable individuals emphasizing optimization of cardiovascular health beginning early in childhood.
“Leveraging these opportunities to target cardiovascular health has the potential to improve health across the life course and for subsequent generations,” they add.
Critical research gap
Despite the evidence linking an individual’s prepregnancy health to their offspring’s health, there are no large trials to test whether improving overall cardiovascular health before pregnancy will reduce pregnancy complications, pregnancy-related cardiovascular death, or cardiovascular risk for offspring. The statement authors suggest that such a trial should be considered.
“This would be a big undertaking, but it could be feasible and could be really impactful,” Dr. Khan said. “Of course it would be challenging to recruit women who are planning a pregnancy and to follow them to see if they do get pregnant and consider interventions and outcomes, but given the importance of the need, we think this is something that should be invested in.”
She pointed out that the main way to improve the cardiovascular health of this cohort would be through behavioral counseling on physical activity and diet. “We need to develop strategies tailored to this age group – young women and those who may already have young children – and often the last thing they are thinking about is themselves and their own health.”
She explained that while it is presumed that controlling cardiovascular risk factors will be beneficial, the bigger question is how that can be achieved. “Behavioral interventions are difficult to achieve and often have low adherence, so the focus of the trials should be on strategies on how to deliver behavioral counseling to achieve better cardiovascular health in this population.”
Dr. Khan stressed that any approaches to improving prepregnancy cardiovascular health must address the current racial disparities that are present. “We must make sure that our policies are successful not just in improving cardiovascular health but to ensure it is done equitably. We must find ways to ensure all individuals can access care.”
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Drinking beet juice tied to reduced post-PCI restenosis
WASHINGTON – Late lumen loss (LLL) after percutaneous interventions (PCI) can be reduced significantly by a daily glass of beet juice, according to a phase 2 randomized trial.
The protection against LLL, attributed to the nitrate contained in beet juice, was accompanied by a trend for a reduced risk of major adverse cardiovascular events (MACE), according to Krishnaraj Rathod, MBBS, BMedSci, PhD, who presented results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
The study grew out of relatively recent evidence that ingestion of nitrate-rich foods, such as beets, can trigger noncanonical pathways for nitric oxide generation, sometimes referred to as the nitrate-nitrite-nitric oxide sequence. Dr. Rathod cited experimental evidence associating this pathway with the traditional benefits of NO generation, such as anti-inflammatory and antithrombotic effects.
In this study, 300 patients scheduled for PCI to treat stable angina were randomized to the experimental arm of nitrate-rich beetroot juice or the control arm of nitrate-depleted beetroot juice. Each had a 70-mL glass of juice once daily. Dr. Rathod, a senior interventional cardiology registrar, Barts Heart Centre, London, described this as the equivalent of about four beets.
The primary endpoint of the study was in-stent LLL assessed by quantitative coronary angiography (QCA) at 6 months.
MACE, defined as death, MI, need for revascularization, and in-stent thrombosis, was assessed at 3, 9, 12, and 24 months. In addition, markers of NO activation, platelet reactivity, and inflammation were monitored.
Lumen loss reduced less than 50%
On OCA, the median stent LLL at 6 months was 0.244 mm in the nitrate-depleted beet juice group and 0.117 mm (P = .0165) in the group that received natural beet juice. The mean segment LLL similarly favored the natural beet juice (0.269 vs. 0.050 mm; P = .0011).
The same effect was reflected in the measurement of mean change in minimum lumen diameter at 6 months. From baseline, this in-stent measure was reduced at 6 months by 0.244 mm in the control group, but by only 0.117 mm in the group receiving the dietary nitrate (P = .0154 for two-way analysis of variance).
Over 24 months of follow-up, there were 18 MACE events in the control arm versus 9 in the arm randomized to dietary nitrate (P = .0718). There were no in-stent thromboses observed in either group, but death (two vs. five), MI (one vs. six), and target-vessel revascularization (six vs. seven) were all numerically lower in the group receiving dietary nitrate.
“Once-a-day oral dietary nitrate for 6 months was well tolerated and safe,” Dr. Rathod reported at the meeting.
Asked specifically about the taste of the daily glass of beet juice, Dr. Rathod acknowledged that some patients were not enamored, but many had no objections or even liked the taste.
The patients were reasonably representative of a PCI population. The mean age in both groups was 61 years. There were no significant differences in body mass index (approximately 29 kg/m2) or proportion with diabetes (22%), hypertension, or hypercholesterolemia (about 70% in both groups) and other comorbidities.
More PCI was performed in the left anterior descending artery (36.7% vs. 44.0%) in the control group, while less PCI was performed in the right coronary (27.3% vs. 30.7%). Neither difference was significant. The vast majority (~90%) of patients received drug-eluting stents with a mean of 1.4 implanted. Procedural success was 100% in both groups.
Discharge medications, including antiplatelet and antithrombotic therapies, were similar in the two groups.
Results characterized as highly positive
Based on the 53% reduction in LLL at 6 months and the trend for a MACE reduction, Dr. Rathod concluded that the results were highly positive.
“These results suggest that dietary nitrate may have a therapeutic role in reducing restenosis following PCI for stable angina,” he said.
In the discussion, several panelists pointed out that nearly one-third of patients were not available for evaluation at 6 months (41 of 150 in the experimental group and 51 of 150 in the control group) with further attrition at 1 and 2 years of follow-up. Of these about half were lost to follow-up and the other half withdrew.
The lack of follow-up on such a high proportion of participants is one weakness of this study,” acknowledged Hector M. Garcia-Garcia, MD, PhD, a cardiovascular researcher at MedStar Washington Hospital Center. However, he remains enthusiastic about the premise.
“It was encouraging to see every signal moving in the right direction,” said Dr. Garcia, who consulted with Dr. Rathod’s group on the design of the study. He called these data “promising,” and said they provide support for larger trial for a treatment with potential benefits at low cost.
George Dangas, MD, PhD, professor of medicine at the Icahn School of Medicine at Mount Sinai, New York, was among panelists who seemed surprised by such positive findings from a simple but novel concept. However, he remains open to further evaluations.
“As with any surprising result, further confirmation in a large and multicenter trial should be anticipated,” he said in an interview. If, as this study suggests, dietary changes are capable of providing therapeutic NO at the vascular level, he suggested studies to demonstrate anti-inflammatory effects or other mechanistic benefits would be helpful.
“Other sources of oral nitrate would also be a worthwhile investigation,” he said.
Dr. Rathod reports no potential conflicts of interest. Dr. Garcia-Garcia reports ties to Abbott, Biotronik, Boston Scientific, CorFlow, Medtronic, Neovasc, Phillips, and Shockwave. Dr. Dangas reports financial relationships with Abbott Vascular, AstraZeneca, Boston Scientific, Daiichi-Sankyo, and Medtronic.
WASHINGTON – Late lumen loss (LLL) after percutaneous interventions (PCI) can be reduced significantly by a daily glass of beet juice, according to a phase 2 randomized trial.
The protection against LLL, attributed to the nitrate contained in beet juice, was accompanied by a trend for a reduced risk of major adverse cardiovascular events (MACE), according to Krishnaraj Rathod, MBBS, BMedSci, PhD, who presented results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
The study grew out of relatively recent evidence that ingestion of nitrate-rich foods, such as beets, can trigger noncanonical pathways for nitric oxide generation, sometimes referred to as the nitrate-nitrite-nitric oxide sequence. Dr. Rathod cited experimental evidence associating this pathway with the traditional benefits of NO generation, such as anti-inflammatory and antithrombotic effects.
In this study, 300 patients scheduled for PCI to treat stable angina were randomized to the experimental arm of nitrate-rich beetroot juice or the control arm of nitrate-depleted beetroot juice. Each had a 70-mL glass of juice once daily. Dr. Rathod, a senior interventional cardiology registrar, Barts Heart Centre, London, described this as the equivalent of about four beets.
The primary endpoint of the study was in-stent LLL assessed by quantitative coronary angiography (QCA) at 6 months.
MACE, defined as death, MI, need for revascularization, and in-stent thrombosis, was assessed at 3, 9, 12, and 24 months. In addition, markers of NO activation, platelet reactivity, and inflammation were monitored.
Lumen loss reduced less than 50%
On OCA, the median stent LLL at 6 months was 0.244 mm in the nitrate-depleted beet juice group and 0.117 mm (P = .0165) in the group that received natural beet juice. The mean segment LLL similarly favored the natural beet juice (0.269 vs. 0.050 mm; P = .0011).
The same effect was reflected in the measurement of mean change in minimum lumen diameter at 6 months. From baseline, this in-stent measure was reduced at 6 months by 0.244 mm in the control group, but by only 0.117 mm in the group receiving the dietary nitrate (P = .0154 for two-way analysis of variance).
Over 24 months of follow-up, there were 18 MACE events in the control arm versus 9 in the arm randomized to dietary nitrate (P = .0718). There were no in-stent thromboses observed in either group, but death (two vs. five), MI (one vs. six), and target-vessel revascularization (six vs. seven) were all numerically lower in the group receiving dietary nitrate.
“Once-a-day oral dietary nitrate for 6 months was well tolerated and safe,” Dr. Rathod reported at the meeting.
Asked specifically about the taste of the daily glass of beet juice, Dr. Rathod acknowledged that some patients were not enamored, but many had no objections or even liked the taste.
The patients were reasonably representative of a PCI population. The mean age in both groups was 61 years. There were no significant differences in body mass index (approximately 29 kg/m2) or proportion with diabetes (22%), hypertension, or hypercholesterolemia (about 70% in both groups) and other comorbidities.
More PCI was performed in the left anterior descending artery (36.7% vs. 44.0%) in the control group, while less PCI was performed in the right coronary (27.3% vs. 30.7%). Neither difference was significant. The vast majority (~90%) of patients received drug-eluting stents with a mean of 1.4 implanted. Procedural success was 100% in both groups.
Discharge medications, including antiplatelet and antithrombotic therapies, were similar in the two groups.
Results characterized as highly positive
Based on the 53% reduction in LLL at 6 months and the trend for a MACE reduction, Dr. Rathod concluded that the results were highly positive.
“These results suggest that dietary nitrate may have a therapeutic role in reducing restenosis following PCI for stable angina,” he said.
In the discussion, several panelists pointed out that nearly one-third of patients were not available for evaluation at 6 months (41 of 150 in the experimental group and 51 of 150 in the control group) with further attrition at 1 and 2 years of follow-up. Of these about half were lost to follow-up and the other half withdrew.
The lack of follow-up on such a high proportion of participants is one weakness of this study,” acknowledged Hector M. Garcia-Garcia, MD, PhD, a cardiovascular researcher at MedStar Washington Hospital Center. However, he remains enthusiastic about the premise.
“It was encouraging to see every signal moving in the right direction,” said Dr. Garcia, who consulted with Dr. Rathod’s group on the design of the study. He called these data “promising,” and said they provide support for larger trial for a treatment with potential benefits at low cost.
George Dangas, MD, PhD, professor of medicine at the Icahn School of Medicine at Mount Sinai, New York, was among panelists who seemed surprised by such positive findings from a simple but novel concept. However, he remains open to further evaluations.
“As with any surprising result, further confirmation in a large and multicenter trial should be anticipated,” he said in an interview. If, as this study suggests, dietary changes are capable of providing therapeutic NO at the vascular level, he suggested studies to demonstrate anti-inflammatory effects or other mechanistic benefits would be helpful.
“Other sources of oral nitrate would also be a worthwhile investigation,” he said.
Dr. Rathod reports no potential conflicts of interest. Dr. Garcia-Garcia reports ties to Abbott, Biotronik, Boston Scientific, CorFlow, Medtronic, Neovasc, Phillips, and Shockwave. Dr. Dangas reports financial relationships with Abbott Vascular, AstraZeneca, Boston Scientific, Daiichi-Sankyo, and Medtronic.
WASHINGTON – Late lumen loss (LLL) after percutaneous interventions (PCI) can be reduced significantly by a daily glass of beet juice, according to a phase 2 randomized trial.
The protection against LLL, attributed to the nitrate contained in beet juice, was accompanied by a trend for a reduced risk of major adverse cardiovascular events (MACE), according to Krishnaraj Rathod, MBBS, BMedSci, PhD, who presented results at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
The study grew out of relatively recent evidence that ingestion of nitrate-rich foods, such as beets, can trigger noncanonical pathways for nitric oxide generation, sometimes referred to as the nitrate-nitrite-nitric oxide sequence. Dr. Rathod cited experimental evidence associating this pathway with the traditional benefits of NO generation, such as anti-inflammatory and antithrombotic effects.
In this study, 300 patients scheduled for PCI to treat stable angina were randomized to the experimental arm of nitrate-rich beetroot juice or the control arm of nitrate-depleted beetroot juice. Each had a 70-mL glass of juice once daily. Dr. Rathod, a senior interventional cardiology registrar, Barts Heart Centre, London, described this as the equivalent of about four beets.
The primary endpoint of the study was in-stent LLL assessed by quantitative coronary angiography (QCA) at 6 months.
MACE, defined as death, MI, need for revascularization, and in-stent thrombosis, was assessed at 3, 9, 12, and 24 months. In addition, markers of NO activation, platelet reactivity, and inflammation were monitored.
Lumen loss reduced less than 50%
On OCA, the median stent LLL at 6 months was 0.244 mm in the nitrate-depleted beet juice group and 0.117 mm (P = .0165) in the group that received natural beet juice. The mean segment LLL similarly favored the natural beet juice (0.269 vs. 0.050 mm; P = .0011).
The same effect was reflected in the measurement of mean change in minimum lumen diameter at 6 months. From baseline, this in-stent measure was reduced at 6 months by 0.244 mm in the control group, but by only 0.117 mm in the group receiving the dietary nitrate (P = .0154 for two-way analysis of variance).
Over 24 months of follow-up, there were 18 MACE events in the control arm versus 9 in the arm randomized to dietary nitrate (P = .0718). There were no in-stent thromboses observed in either group, but death (two vs. five), MI (one vs. six), and target-vessel revascularization (six vs. seven) were all numerically lower in the group receiving dietary nitrate.
“Once-a-day oral dietary nitrate for 6 months was well tolerated and safe,” Dr. Rathod reported at the meeting.
Asked specifically about the taste of the daily glass of beet juice, Dr. Rathod acknowledged that some patients were not enamored, but many had no objections or even liked the taste.
The patients were reasonably representative of a PCI population. The mean age in both groups was 61 years. There were no significant differences in body mass index (approximately 29 kg/m2) or proportion with diabetes (22%), hypertension, or hypercholesterolemia (about 70% in both groups) and other comorbidities.
More PCI was performed in the left anterior descending artery (36.7% vs. 44.0%) in the control group, while less PCI was performed in the right coronary (27.3% vs. 30.7%). Neither difference was significant. The vast majority (~90%) of patients received drug-eluting stents with a mean of 1.4 implanted. Procedural success was 100% in both groups.
Discharge medications, including antiplatelet and antithrombotic therapies, were similar in the two groups.
Results characterized as highly positive
Based on the 53% reduction in LLL at 6 months and the trend for a MACE reduction, Dr. Rathod concluded that the results were highly positive.
“These results suggest that dietary nitrate may have a therapeutic role in reducing restenosis following PCI for stable angina,” he said.
In the discussion, several panelists pointed out that nearly one-third of patients were not available for evaluation at 6 months (41 of 150 in the experimental group and 51 of 150 in the control group) with further attrition at 1 and 2 years of follow-up. Of these about half were lost to follow-up and the other half withdrew.
The lack of follow-up on such a high proportion of participants is one weakness of this study,” acknowledged Hector M. Garcia-Garcia, MD, PhD, a cardiovascular researcher at MedStar Washington Hospital Center. However, he remains enthusiastic about the premise.
“It was encouraging to see every signal moving in the right direction,” said Dr. Garcia, who consulted with Dr. Rathod’s group on the design of the study. He called these data “promising,” and said they provide support for larger trial for a treatment with potential benefits at low cost.
George Dangas, MD, PhD, professor of medicine at the Icahn School of Medicine at Mount Sinai, New York, was among panelists who seemed surprised by such positive findings from a simple but novel concept. However, he remains open to further evaluations.
“As with any surprising result, further confirmation in a large and multicenter trial should be anticipated,” he said in an interview. If, as this study suggests, dietary changes are capable of providing therapeutic NO at the vascular level, he suggested studies to demonstrate anti-inflammatory effects or other mechanistic benefits would be helpful.
“Other sources of oral nitrate would also be a worthwhile investigation,” he said.
Dr. Rathod reports no potential conflicts of interest. Dr. Garcia-Garcia reports ties to Abbott, Biotronik, Boston Scientific, CorFlow, Medtronic, Neovasc, Phillips, and Shockwave. Dr. Dangas reports financial relationships with Abbott Vascular, AstraZeneca, Boston Scientific, Daiichi-Sankyo, and Medtronic.
AT CRT 2023
Irregular sleep tied to markers of atherosclerosis
a new report suggests.
In particular, variation in sleep duration of more than 2 hours per night in the same week was tied to higher rates of atherosclerosis.
“Poor sleep is linked with several cardiovascular conditions, including heart disease, hypertension, and type 2 diabetes,” lead author Kelsie M. Full, PhD, MPH, assistant professor of medicine at Vanderbilt University Medical Center, Nashville, Tenn., said in an interview.
“Overall, we found that participants who slept varying amounts of hours throughout the week (meaning that one night they slept less, one night they slept more) were more likely to have atherosclerosis than participants who slept about the same amount of time each night,” she said.
The study was published online in the Journal of the American Heart Association.
Analyzing associations
Dr. Full and colleagues examined data from 2032 participants in the Multi-Ethnic Study of Atherosclerosis Sleep Ancillary Study, which included adults aged between 45 and 84 years in six U.S. communities who completed 7-day wrist actigraphy assessment and kept a sleep diary between 2010 and 2013.
For subclinical markers of cardiovascular disease, participants underwent assessments of coronary artery calcium, carotid plaque presence, carotid intima-media thickness, and ankle-brachial index.
The research team assessed sleep duration, or the total number of minutes of sleep in a night, and sleep timing regularity, which was determined on the basis of the time someone initially fell asleep each night. They adjusted for cardiovascular disease risk factors and sleep characteristics, such as obstructive sleep apnea, sleep duration, and sleep fragmentation.
The average age of the participants was 68.6 years, and 53.6% were women. About 37.9% identified as White, 27.6% as Black or African American, 23.4% as Hispanic American, and 11.1% as Chinese American.
During the 7-day period, about 38% of participants experienced a change in sleep duration of more than 90 minutes, and 18% experienced a sleep duration change of more than 120 minutes. Those who had irregular sleep were more likely to be non-White, current smokers, have lower average annual incomes, have work shift schedules or did not work, and have a higher average body mass index.
For the study, sleep duration irregularity was defined as a standard deviation of more than 120 minutes. Those participants who had a greater degree of sleep irregularity were more likely to have high coronary artery calcium burden than those whose sleep duration was more more regular, defined as an SD of 60 minutes or less (> 300; prevalence ratio, 1.33; 95% confidence interval, 1.03-1.71), as well as abnormal ankle-brachial index (< 0.9, prevalence ratio, 1.75;95% CI, 1.03-2.95).
Further, those with irregular sleep timing (SD > 90 minutes) were more likely to have a high coronary artery calcium burden (prevalence ratio, 1.39; 95% CI, 1.07-1.82) in comparison with those with more regular sleep timing (SD < 30 minutes).
“The biggest surprise to me was that 30% of the participants in the study had total sleep times that varied by more than 90 minutes over the course of the week,” Dr. Full said. “This is consistent with prior studies that suggest that a large proportion of the general public have irregular sleep patterns, not just shift workers.”
Investigating next steps
In additional analyses, Dr. Full and colleagues found that sleep duration regularity continued to be associated with high coronary artery calcium burden and abnormal ankle-brachial index when accounting for severe obstructive sleep apnea, average nightly sleep duration, and average sleep fragmentation.
Notably, when sleep duration was added, all participants with more irregular sleep durations (SD > 60 minutes) were more likely to have a high coronary artery calcium burden, compared with those with regular sleep durations (SD < 60 minutes). The results remained when participants who reported shift work, including night shift work, were excluded.
Additional studies are needed to understand the mechanisms, the study authors wrote. Night-to-night variability in sleep duration and sleep timing can cause desynchronization in the sleep-wake timing and circadian disruption.
“A key issue highlighted in this study is that sleep irregularity itself, independent of how much sleep people were getting, was related to heart health. Sleep is a naturally recurring phenomenon, and maintaining regularity helps provide stability and predictability to the body,” Michael Grandner, PhD, associate professor of psychiatry and director of the sleep and health research program at the University of Arizona, Tucson, said in an interview.
Dr. Grandner, who wasn’t involved with this study, has researched sleep irregularity and associations with cardiovascular disease, diabetes, obesity, and many other adverse outcomes.
“When people have very irregular sleep schedules, it may make it harder for the body to optimally make good use of the sleep it is getting, since it such a moving target,” he said. “The unique angle here is the ability to focus on regularity of sleep.”
The study was supported by the National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences of the National Institutes of Health. One author received grants and consulting fees from pharmaceutical companies unrelated to the research. The other authors and Dr. Grandner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a new report suggests.
In particular, variation in sleep duration of more than 2 hours per night in the same week was tied to higher rates of atherosclerosis.
“Poor sleep is linked with several cardiovascular conditions, including heart disease, hypertension, and type 2 diabetes,” lead author Kelsie M. Full, PhD, MPH, assistant professor of medicine at Vanderbilt University Medical Center, Nashville, Tenn., said in an interview.
“Overall, we found that participants who slept varying amounts of hours throughout the week (meaning that one night they slept less, one night they slept more) were more likely to have atherosclerosis than participants who slept about the same amount of time each night,” she said.
The study was published online in the Journal of the American Heart Association.
Analyzing associations
Dr. Full and colleagues examined data from 2032 participants in the Multi-Ethnic Study of Atherosclerosis Sleep Ancillary Study, which included adults aged between 45 and 84 years in six U.S. communities who completed 7-day wrist actigraphy assessment and kept a sleep diary between 2010 and 2013.
For subclinical markers of cardiovascular disease, participants underwent assessments of coronary artery calcium, carotid plaque presence, carotid intima-media thickness, and ankle-brachial index.
The research team assessed sleep duration, or the total number of minutes of sleep in a night, and sleep timing regularity, which was determined on the basis of the time someone initially fell asleep each night. They adjusted for cardiovascular disease risk factors and sleep characteristics, such as obstructive sleep apnea, sleep duration, and sleep fragmentation.
The average age of the participants was 68.6 years, and 53.6% were women. About 37.9% identified as White, 27.6% as Black or African American, 23.4% as Hispanic American, and 11.1% as Chinese American.
During the 7-day period, about 38% of participants experienced a change in sleep duration of more than 90 minutes, and 18% experienced a sleep duration change of more than 120 minutes. Those who had irregular sleep were more likely to be non-White, current smokers, have lower average annual incomes, have work shift schedules or did not work, and have a higher average body mass index.
For the study, sleep duration irregularity was defined as a standard deviation of more than 120 minutes. Those participants who had a greater degree of sleep irregularity were more likely to have high coronary artery calcium burden than those whose sleep duration was more more regular, defined as an SD of 60 minutes or less (> 300; prevalence ratio, 1.33; 95% confidence interval, 1.03-1.71), as well as abnormal ankle-brachial index (< 0.9, prevalence ratio, 1.75;95% CI, 1.03-2.95).
Further, those with irregular sleep timing (SD > 90 minutes) were more likely to have a high coronary artery calcium burden (prevalence ratio, 1.39; 95% CI, 1.07-1.82) in comparison with those with more regular sleep timing (SD < 30 minutes).
“The biggest surprise to me was that 30% of the participants in the study had total sleep times that varied by more than 90 minutes over the course of the week,” Dr. Full said. “This is consistent with prior studies that suggest that a large proportion of the general public have irregular sleep patterns, not just shift workers.”
Investigating next steps
In additional analyses, Dr. Full and colleagues found that sleep duration regularity continued to be associated with high coronary artery calcium burden and abnormal ankle-brachial index when accounting for severe obstructive sleep apnea, average nightly sleep duration, and average sleep fragmentation.
Notably, when sleep duration was added, all participants with more irregular sleep durations (SD > 60 minutes) were more likely to have a high coronary artery calcium burden, compared with those with regular sleep durations (SD < 60 minutes). The results remained when participants who reported shift work, including night shift work, were excluded.
Additional studies are needed to understand the mechanisms, the study authors wrote. Night-to-night variability in sleep duration and sleep timing can cause desynchronization in the sleep-wake timing and circadian disruption.
“A key issue highlighted in this study is that sleep irregularity itself, independent of how much sleep people were getting, was related to heart health. Sleep is a naturally recurring phenomenon, and maintaining regularity helps provide stability and predictability to the body,” Michael Grandner, PhD, associate professor of psychiatry and director of the sleep and health research program at the University of Arizona, Tucson, said in an interview.
Dr. Grandner, who wasn’t involved with this study, has researched sleep irregularity and associations with cardiovascular disease, diabetes, obesity, and many other adverse outcomes.
“When people have very irregular sleep schedules, it may make it harder for the body to optimally make good use of the sleep it is getting, since it such a moving target,” he said. “The unique angle here is the ability to focus on regularity of sleep.”
The study was supported by the National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences of the National Institutes of Health. One author received grants and consulting fees from pharmaceutical companies unrelated to the research. The other authors and Dr. Grandner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
a new report suggests.
In particular, variation in sleep duration of more than 2 hours per night in the same week was tied to higher rates of atherosclerosis.
“Poor sleep is linked with several cardiovascular conditions, including heart disease, hypertension, and type 2 diabetes,” lead author Kelsie M. Full, PhD, MPH, assistant professor of medicine at Vanderbilt University Medical Center, Nashville, Tenn., said in an interview.
“Overall, we found that participants who slept varying amounts of hours throughout the week (meaning that one night they slept less, one night they slept more) were more likely to have atherosclerosis than participants who slept about the same amount of time each night,” she said.
The study was published online in the Journal of the American Heart Association.
Analyzing associations
Dr. Full and colleagues examined data from 2032 participants in the Multi-Ethnic Study of Atherosclerosis Sleep Ancillary Study, which included adults aged between 45 and 84 years in six U.S. communities who completed 7-day wrist actigraphy assessment and kept a sleep diary between 2010 and 2013.
For subclinical markers of cardiovascular disease, participants underwent assessments of coronary artery calcium, carotid plaque presence, carotid intima-media thickness, and ankle-brachial index.
The research team assessed sleep duration, or the total number of minutes of sleep in a night, and sleep timing regularity, which was determined on the basis of the time someone initially fell asleep each night. They adjusted for cardiovascular disease risk factors and sleep characteristics, such as obstructive sleep apnea, sleep duration, and sleep fragmentation.
The average age of the participants was 68.6 years, and 53.6% were women. About 37.9% identified as White, 27.6% as Black or African American, 23.4% as Hispanic American, and 11.1% as Chinese American.
During the 7-day period, about 38% of participants experienced a change in sleep duration of more than 90 minutes, and 18% experienced a sleep duration change of more than 120 minutes. Those who had irregular sleep were more likely to be non-White, current smokers, have lower average annual incomes, have work shift schedules or did not work, and have a higher average body mass index.
For the study, sleep duration irregularity was defined as a standard deviation of more than 120 minutes. Those participants who had a greater degree of sleep irregularity were more likely to have high coronary artery calcium burden than those whose sleep duration was more more regular, defined as an SD of 60 minutes or less (> 300; prevalence ratio, 1.33; 95% confidence interval, 1.03-1.71), as well as abnormal ankle-brachial index (< 0.9, prevalence ratio, 1.75;95% CI, 1.03-2.95).
Further, those with irregular sleep timing (SD > 90 minutes) were more likely to have a high coronary artery calcium burden (prevalence ratio, 1.39; 95% CI, 1.07-1.82) in comparison with those with more regular sleep timing (SD < 30 minutes).
“The biggest surprise to me was that 30% of the participants in the study had total sleep times that varied by more than 90 minutes over the course of the week,” Dr. Full said. “This is consistent with prior studies that suggest that a large proportion of the general public have irregular sleep patterns, not just shift workers.”
Investigating next steps
In additional analyses, Dr. Full and colleagues found that sleep duration regularity continued to be associated with high coronary artery calcium burden and abnormal ankle-brachial index when accounting for severe obstructive sleep apnea, average nightly sleep duration, and average sleep fragmentation.
Notably, when sleep duration was added, all participants with more irregular sleep durations (SD > 60 minutes) were more likely to have a high coronary artery calcium burden, compared with those with regular sleep durations (SD < 60 minutes). The results remained when participants who reported shift work, including night shift work, were excluded.
Additional studies are needed to understand the mechanisms, the study authors wrote. Night-to-night variability in sleep duration and sleep timing can cause desynchronization in the sleep-wake timing and circadian disruption.
“A key issue highlighted in this study is that sleep irregularity itself, independent of how much sleep people were getting, was related to heart health. Sleep is a naturally recurring phenomenon, and maintaining regularity helps provide stability and predictability to the body,” Michael Grandner, PhD, associate professor of psychiatry and director of the sleep and health research program at the University of Arizona, Tucson, said in an interview.
Dr. Grandner, who wasn’t involved with this study, has researched sleep irregularity and associations with cardiovascular disease, diabetes, obesity, and many other adverse outcomes.
“When people have very irregular sleep schedules, it may make it harder for the body to optimally make good use of the sleep it is getting, since it such a moving target,” he said. “The unique angle here is the ability to focus on regularity of sleep.”
The study was supported by the National Heart, Lung, and Blood Institute and the National Center for Advancing Translational Sciences of the National Institutes of Health. One author received grants and consulting fees from pharmaceutical companies unrelated to the research. The other authors and Dr. Grandner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Concussion burden tied to later hypertension in football players
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
FROM CIRCULATION
No advantage for full-term aspirin in preventing preterm preeclampsia
Stopping aspirin at 24-28 weeks of gestation has no disadvantage, compared with continuing aspirin full term, for preventing preterm preeclampsia in women at high risk of preeclampsia who have a normal fms-like tyrosine kinase 1 to placental growth factor (sFlt-1:PlGF) ratio, a randomized controlled trial has found.
The findings were published online in JAMA.
Editorialists advise careful consideration
However, in an accompanying editorial, Ukachi N. Emeruwa, MD, MPH, with the division of maternal fetal medicine, department of obstetrics, gynecology, and reproductive sciences at the University of California, San Diego, and colleagues noted that the questions surrounding continuing or discontinuing aspirin in this high-risk population need further consideration.
They added that the results from this study – conducted in nine maternity hospitals across Spain – are hard to translate for the U.S. population.
In this study, Manel Mendoza, PhD, with the maternal fetal medicine unit, department of obstetrics, at the Universitat Autònoma de Barcelona, and colleagues compared the two approaches because of the potential to mitigate peripartum bleeding by discontinuing aspirin before full term (37 weeks’ gestation) and by an accurate selection of women in the first trimester at higher risk of preeclampsia.
Aspirin cuts preterm preeclampsia by 62% in women at high risk
While aspirin might be associated with an increased risk of peripartum bleeding, aspirin has been proven to reduce the incidence of preterm preeclampsia by 62% in pregnant women at high risk of preeclampsia.
In the multicenter, open-label, randomized, phase 3, noninferiority trial, pregnant women who had a high risk of preeclampsia during the first-trimester screening and an sFlt-1:PlGF ratio of 38 or less at 24-28 weeks’ gestation were recruited between Aug. 20, 2019, and Sept. 15, 2021. Of those, 936 were analyzed (473 in the intervention group [stopping aspirin] and 473 in the control group [continuing]).
Screening for risk of preterm preeclampsia included analyzing maternal factors, uterine artery pulsatility index, mean arterial pressure, serum pregnancy-associated plasma protein A, and placental growth factor. Follow-up was until delivery for all participants.
Incidence of preterm preeclampsia was 1.48% in the intervention group (discontinuing aspirin) and 1.73% in the control group (continuing aspirin until 36 weeks of gestation; absolute difference, –0.25%; 95% confidence interval, –1.86% to 1.36%), which indicates noninferiority for stopping aspirin. The bar for noninferiority was less than a 1.9% difference in preterm preeclampsia incidences between groups.
Researchers did find a higher incidence of minor antepartum bleeding in the group that continued aspirin (7.61% in the low-dose aspirin discontinuation group vs. 12.31% in the low-dose aspirin continuation group; absolute difference, –4.70; 95% CI, –8.53 to –0.87).
Differences in U.S. guidelines
Dr. Emeruwa and colleagues noted the study challenges a growing body of evidence favoring increasingly widespread use of low-dose aspirin in pregnancy.
They called the study “well designed and provocative,” but wrote that the findings are hard to interpret for a U.S. population. Some key differences in the U.S. preeclampsia prevention guidelines, compared with the practices of the study’s authors, included the reliance on clinical maternal factors in the United States for screening for low-dose aspirin prophylaxis as opposed to molecular biomarkers; a different aspirin dose prescribed in the United States (81 mg daily), compared with international societies (150 mg daily); and a lack of a recommendation in the United States to stop prophylactic low-dose aspirin at 36 weeks.
Dr. Emeruwa and colleagues also questioned the scope of the outcome measure used.
They wrote that limiting outcomes to preterm preeclampsia dims the effects of all types of preeclampsia on perinatal and maternal outcomes and that early-onset preeclampsia at less than 34 weeks “occurs in just 0.38% of pregnancies, while 3%-5% are affected by late-onset preeclampsia.”
‘Late-onset preeclampsia has a higher overall impact’
Dr. Emeruwa and colleagues wrote: “Though the odds of adverse perinatal and maternal outcomes are higher with preterm preeclampsia, due to its overall higher incidence, late-onset preeclampsia has a higher overall impact on perinatal and maternal morbidity and mortality.”
The study can inform future U.S. approaches, the editorialists wrote, and build on work already being done in the United States.
The study investigators used biophysical and molecular markers to more accurately assess risk for starting low-dose aspirin prophylaxis in the first trimester and applied a growing body of data showing the high negative predictive value of second-trimester biomarkers.
The editorialists noted that the U.S. Preventive Services Task Force recommendations would have captured “less than 50% of the at-risk population” that Dr. Mendoza’s team found eligible for low-dose aspirin.
Those factors, the editorialists wrote, point to the potential to improve guidelines for personalized preeclampsia management in pregnancy.
They concluded: “U.S. practitioners and professional societies should reconsider current risk assessment strategies, which are largely based on maternal factors, and evaluate whether incorporation of molecular biomarkers would improve maternal and fetal/neonatal outcomes.”
The study authors acknowledged that 92% of participants in the study were White, thus limiting generalizability.
The authors and editorialists reported no relevant financial relationships.
Stopping aspirin at 24-28 weeks of gestation has no disadvantage, compared with continuing aspirin full term, for preventing preterm preeclampsia in women at high risk of preeclampsia who have a normal fms-like tyrosine kinase 1 to placental growth factor (sFlt-1:PlGF) ratio, a randomized controlled trial has found.
The findings were published online in JAMA.
Editorialists advise careful consideration
However, in an accompanying editorial, Ukachi N. Emeruwa, MD, MPH, with the division of maternal fetal medicine, department of obstetrics, gynecology, and reproductive sciences at the University of California, San Diego, and colleagues noted that the questions surrounding continuing or discontinuing aspirin in this high-risk population need further consideration.
They added that the results from this study – conducted in nine maternity hospitals across Spain – are hard to translate for the U.S. population.
In this study, Manel Mendoza, PhD, with the maternal fetal medicine unit, department of obstetrics, at the Universitat Autònoma de Barcelona, and colleagues compared the two approaches because of the potential to mitigate peripartum bleeding by discontinuing aspirin before full term (37 weeks’ gestation) and by an accurate selection of women in the first trimester at higher risk of preeclampsia.
Aspirin cuts preterm preeclampsia by 62% in women at high risk
While aspirin might be associated with an increased risk of peripartum bleeding, aspirin has been proven to reduce the incidence of preterm preeclampsia by 62% in pregnant women at high risk of preeclampsia.
In the multicenter, open-label, randomized, phase 3, noninferiority trial, pregnant women who had a high risk of preeclampsia during the first-trimester screening and an sFlt-1:PlGF ratio of 38 or less at 24-28 weeks’ gestation were recruited between Aug. 20, 2019, and Sept. 15, 2021. Of those, 936 were analyzed (473 in the intervention group [stopping aspirin] and 473 in the control group [continuing]).
Screening for risk of preterm preeclampsia included analyzing maternal factors, uterine artery pulsatility index, mean arterial pressure, serum pregnancy-associated plasma protein A, and placental growth factor. Follow-up was until delivery for all participants.
Incidence of preterm preeclampsia was 1.48% in the intervention group (discontinuing aspirin) and 1.73% in the control group (continuing aspirin until 36 weeks of gestation; absolute difference, –0.25%; 95% confidence interval, –1.86% to 1.36%), which indicates noninferiority for stopping aspirin. The bar for noninferiority was less than a 1.9% difference in preterm preeclampsia incidences between groups.
Researchers did find a higher incidence of minor antepartum bleeding in the group that continued aspirin (7.61% in the low-dose aspirin discontinuation group vs. 12.31% in the low-dose aspirin continuation group; absolute difference, –4.70; 95% CI, –8.53 to –0.87).
Differences in U.S. guidelines
Dr. Emeruwa and colleagues noted the study challenges a growing body of evidence favoring increasingly widespread use of low-dose aspirin in pregnancy.
They called the study “well designed and provocative,” but wrote that the findings are hard to interpret for a U.S. population. Some key differences in the U.S. preeclampsia prevention guidelines, compared with the practices of the study’s authors, included the reliance on clinical maternal factors in the United States for screening for low-dose aspirin prophylaxis as opposed to molecular biomarkers; a different aspirin dose prescribed in the United States (81 mg daily), compared with international societies (150 mg daily); and a lack of a recommendation in the United States to stop prophylactic low-dose aspirin at 36 weeks.
Dr. Emeruwa and colleagues also questioned the scope of the outcome measure used.
They wrote that limiting outcomes to preterm preeclampsia dims the effects of all types of preeclampsia on perinatal and maternal outcomes and that early-onset preeclampsia at less than 34 weeks “occurs in just 0.38% of pregnancies, while 3%-5% are affected by late-onset preeclampsia.”
‘Late-onset preeclampsia has a higher overall impact’
Dr. Emeruwa and colleagues wrote: “Though the odds of adverse perinatal and maternal outcomes are higher with preterm preeclampsia, due to its overall higher incidence, late-onset preeclampsia has a higher overall impact on perinatal and maternal morbidity and mortality.”
The study can inform future U.S. approaches, the editorialists wrote, and build on work already being done in the United States.
The study investigators used biophysical and molecular markers to more accurately assess risk for starting low-dose aspirin prophylaxis in the first trimester and applied a growing body of data showing the high negative predictive value of second-trimester biomarkers.
The editorialists noted that the U.S. Preventive Services Task Force recommendations would have captured “less than 50% of the at-risk population” that Dr. Mendoza’s team found eligible for low-dose aspirin.
Those factors, the editorialists wrote, point to the potential to improve guidelines for personalized preeclampsia management in pregnancy.
They concluded: “U.S. practitioners and professional societies should reconsider current risk assessment strategies, which are largely based on maternal factors, and evaluate whether incorporation of molecular biomarkers would improve maternal and fetal/neonatal outcomes.”
The study authors acknowledged that 92% of participants in the study were White, thus limiting generalizability.
The authors and editorialists reported no relevant financial relationships.
Stopping aspirin at 24-28 weeks of gestation has no disadvantage, compared with continuing aspirin full term, for preventing preterm preeclampsia in women at high risk of preeclampsia who have a normal fms-like tyrosine kinase 1 to placental growth factor (sFlt-1:PlGF) ratio, a randomized controlled trial has found.
The findings were published online in JAMA.
Editorialists advise careful consideration
However, in an accompanying editorial, Ukachi N. Emeruwa, MD, MPH, with the division of maternal fetal medicine, department of obstetrics, gynecology, and reproductive sciences at the University of California, San Diego, and colleagues noted that the questions surrounding continuing or discontinuing aspirin in this high-risk population need further consideration.
They added that the results from this study – conducted in nine maternity hospitals across Spain – are hard to translate for the U.S. population.
In this study, Manel Mendoza, PhD, with the maternal fetal medicine unit, department of obstetrics, at the Universitat Autònoma de Barcelona, and colleagues compared the two approaches because of the potential to mitigate peripartum bleeding by discontinuing aspirin before full term (37 weeks’ gestation) and by an accurate selection of women in the first trimester at higher risk of preeclampsia.
Aspirin cuts preterm preeclampsia by 62% in women at high risk
While aspirin might be associated with an increased risk of peripartum bleeding, aspirin has been proven to reduce the incidence of preterm preeclampsia by 62% in pregnant women at high risk of preeclampsia.
In the multicenter, open-label, randomized, phase 3, noninferiority trial, pregnant women who had a high risk of preeclampsia during the first-trimester screening and an sFlt-1:PlGF ratio of 38 or less at 24-28 weeks’ gestation were recruited between Aug. 20, 2019, and Sept. 15, 2021. Of those, 936 were analyzed (473 in the intervention group [stopping aspirin] and 473 in the control group [continuing]).
Screening for risk of preterm preeclampsia included analyzing maternal factors, uterine artery pulsatility index, mean arterial pressure, serum pregnancy-associated plasma protein A, and placental growth factor. Follow-up was until delivery for all participants.
Incidence of preterm preeclampsia was 1.48% in the intervention group (discontinuing aspirin) and 1.73% in the control group (continuing aspirin until 36 weeks of gestation; absolute difference, –0.25%; 95% confidence interval, –1.86% to 1.36%), which indicates noninferiority for stopping aspirin. The bar for noninferiority was less than a 1.9% difference in preterm preeclampsia incidences between groups.
Researchers did find a higher incidence of minor antepartum bleeding in the group that continued aspirin (7.61% in the low-dose aspirin discontinuation group vs. 12.31% in the low-dose aspirin continuation group; absolute difference, –4.70; 95% CI, –8.53 to –0.87).
Differences in U.S. guidelines
Dr. Emeruwa and colleagues noted the study challenges a growing body of evidence favoring increasingly widespread use of low-dose aspirin in pregnancy.
They called the study “well designed and provocative,” but wrote that the findings are hard to interpret for a U.S. population. Some key differences in the U.S. preeclampsia prevention guidelines, compared with the practices of the study’s authors, included the reliance on clinical maternal factors in the United States for screening for low-dose aspirin prophylaxis as opposed to molecular biomarkers; a different aspirin dose prescribed in the United States (81 mg daily), compared with international societies (150 mg daily); and a lack of a recommendation in the United States to stop prophylactic low-dose aspirin at 36 weeks.
Dr. Emeruwa and colleagues also questioned the scope of the outcome measure used.
They wrote that limiting outcomes to preterm preeclampsia dims the effects of all types of preeclampsia on perinatal and maternal outcomes and that early-onset preeclampsia at less than 34 weeks “occurs in just 0.38% of pregnancies, while 3%-5% are affected by late-onset preeclampsia.”
‘Late-onset preeclampsia has a higher overall impact’
Dr. Emeruwa and colleagues wrote: “Though the odds of adverse perinatal and maternal outcomes are higher with preterm preeclampsia, due to its overall higher incidence, late-onset preeclampsia has a higher overall impact on perinatal and maternal morbidity and mortality.”
The study can inform future U.S. approaches, the editorialists wrote, and build on work already being done in the United States.
The study investigators used biophysical and molecular markers to more accurately assess risk for starting low-dose aspirin prophylaxis in the first trimester and applied a growing body of data showing the high negative predictive value of second-trimester biomarkers.
The editorialists noted that the U.S. Preventive Services Task Force recommendations would have captured “less than 50% of the at-risk population” that Dr. Mendoza’s team found eligible for low-dose aspirin.
Those factors, the editorialists wrote, point to the potential to improve guidelines for personalized preeclampsia management in pregnancy.
They concluded: “U.S. practitioners and professional societies should reconsider current risk assessment strategies, which are largely based on maternal factors, and evaluate whether incorporation of molecular biomarkers would improve maternal and fetal/neonatal outcomes.”
The study authors acknowledged that 92% of participants in the study were White, thus limiting generalizability.
The authors and editorialists reported no relevant financial relationships.
FROM JAMA
Two cups of coffee increase heart dangers with hypertension
according to researchers at Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine, Tokyo.
What to know
People with severely high blood pressure who drink two or more cups of caffeinated coffee each day could double their risk of dying from a heart attack, stroke, or any type of cardiovascular disease.
Too much coffee may raise blood pressure and lead to anxiety, heart palpitations, and difficulty sleeping.
An 8-ounce cup of coffee has 80-100 mg of caffeine, while an 8-ounce cup of green or black tea has 30-50 mg.
Drinking one cup of coffee a day or any amount of green tea was not associated with risk of death across any blood pressure categories, and drinking green tea was not associated with increased risk of death related to cardiovascular disease at any blood pressure level.
Frequent consumers of coffee were more likely to be younger, current smokers, current drinkers, to eat fewer vegetables, and to have higher total cholesterol levels and lower systolic blood pressure regardless of their blood pressure category.
This is a summary of the article “Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension,” published in the Journal of the American Heart Association.
A version of this article first appeared on Medscape.com.
according to researchers at Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine, Tokyo.
What to know
People with severely high blood pressure who drink two or more cups of caffeinated coffee each day could double their risk of dying from a heart attack, stroke, or any type of cardiovascular disease.
Too much coffee may raise blood pressure and lead to anxiety, heart palpitations, and difficulty sleeping.
An 8-ounce cup of coffee has 80-100 mg of caffeine, while an 8-ounce cup of green or black tea has 30-50 mg.
Drinking one cup of coffee a day or any amount of green tea was not associated with risk of death across any blood pressure categories, and drinking green tea was not associated with increased risk of death related to cardiovascular disease at any blood pressure level.
Frequent consumers of coffee were more likely to be younger, current smokers, current drinkers, to eat fewer vegetables, and to have higher total cholesterol levels and lower systolic blood pressure regardless of their blood pressure category.
This is a summary of the article “Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension,” published in the Journal of the American Heart Association.
A version of this article first appeared on Medscape.com.
according to researchers at Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine, Tokyo.
What to know
People with severely high blood pressure who drink two or more cups of caffeinated coffee each day could double their risk of dying from a heart attack, stroke, or any type of cardiovascular disease.
Too much coffee may raise blood pressure and lead to anxiety, heart palpitations, and difficulty sleeping.
An 8-ounce cup of coffee has 80-100 mg of caffeine, while an 8-ounce cup of green or black tea has 30-50 mg.
Drinking one cup of coffee a day or any amount of green tea was not associated with risk of death across any blood pressure categories, and drinking green tea was not associated with increased risk of death related to cardiovascular disease at any blood pressure level.
Frequent consumers of coffee were more likely to be younger, current smokers, current drinkers, to eat fewer vegetables, and to have higher total cholesterol levels and lower systolic blood pressure regardless of their blood pressure category.
This is a summary of the article “Coffee and Green Tea Consumption and Cardiovascular Disease Mortality Among People With and Without Hypertension,” published in the Journal of the American Heart Association.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF AMERICAN HEART ASSOCIATION