User login
Retrospective Review on the Safety and Efficacy of Direct Oral Anticoagulants Compared With Warfarin in Patients With Cirrhosis
Coagulation in patients with cirrhosis is a complicated area of evolving research. Patients with cirrhosis were originally thought to be naturally anticoagulated due to the decreased production of clotting factors and platelets, combined with an increased international normalized ratio (INR).1 New data have shown that patients with cirrhosis are at a concomitant risk of bleeding and thrombosis due to increased platelet aggregation, decreased fibrinolysis, and decreased production of natural anticoagulants such as protein C and antithrombin.1 Traditionally, patients with cirrhosis needing anticoagulation therapy for comorbid conditions, such as nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) were placed on warfarin therapy. Managing warfarin in patients with cirrhosis poses a challenge to clinicians due to the many food and drug interactions, narrow therapeutic index, and complications with maintaining a therapeutic INR.1
Direct oral anticoagulants (DOACs) have several benefits over warfarin therapy, including convenience, decreased monitoring, decreased drug and dietary restrictions, and faster onset of action.2 Conversely, DOACs undergo extensive hepatic metabolism giving rise to concerns about supratherapeutic drug levels and increased bleeding rates in patients with liver dysfunction.1 Consequently, patients with cirrhosis were excluded from the pivotal trials establishing DOACs for NVAF and VTE treatment. Exclusion of these patients in major clinical trials alongside the challenges of managing warfarin warrant an evaluation of the efficacy and safety of DOACs in patients with cirrhosis.
Recent retrospective studies have examined the use of DOACs in patients with cirrhosis and found favorable results. A retrospective chart review by Intagliata and colleagues consisting of 39 patients with cirrhosis using either a DOAC or warfarin found similar rates of all-cause bleeding and major bleeding between the 2 groups.3 A retrospective cohort study by Hum and colleagues consisting of 45 patients with cirrhosis compared the use of DOACs with warfarin or low-molecular weight heparin (LMWH).4 Hum and colleagues found patients prescribed a DOAC had significantly fewer major bleeding events than did patients using warfarin or LMWH.4 The largest retrospective cohort study consisted of 233 patients with chronic liver disease and found no differences among all-cause bleeding and major bleeding rates between patients using DOACs compared with those of patients using warfarin.5
The purpose of this research is to evaluate the safety and efficacy of DOACs in veteran patients with cirrhosis compared with patients using warfarin.
Methods
A retrospective single-center chart review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center (MEDVAMC) in Houston, Texas, between October 31, 2014 and October 31, 2018. Patients included in the study were adults aged ≥ 18 years with a diagnosis of cirrhosis and prescribed any of the following oral anticoagulants: apixaban, dabigatran, edoxaban, rivaroxaban, or warfarin. Patients prescribed apixaban, dabigatran, edoxaban, or rivaroxaban were collectively grouped into the DOAC group, while patients prescribed warfarin were classified as the standard of care comparator group.
A diagnosis of cirrhosis was confirmed using a combination of the codes from the ninth and tenth editions of the International Classification of Diseases (ICD) for cirrhosis, documentation of diagnostic confirmation by clinicians from the gastroenterology or hepatology services, and positive liver biopsy result. Liver function tests, liver ultrasound results, and FibroSure biomarker assays were used to aid in confirming the diagnosis of cirrhosis but were not considered definitive. Patients were excluded from the trial if they had indications for anticoagulation other than NVAF and VTE and/or were prescribed triple antithrombotic therapy (dual antiplatelet therapy plus an anticoagulant). Patients who switched anticoagulant therapy during the trial period (ie, switched from warfarin to a DOAC) were also excluded from the analysis.
Patient demographic characteristics that were collected included weight; body mass index (BMI); etiology of cirrhosis; Child-Turcotte-Pugh, Model for End-Stage Liver Disease (MELD), and CHA2DS2-VASc score; concomitant antiplatelet, nonsteroidal anti-inflammatory drug (NSAID), proton pump inhibitor (PPI), and histamine-2 receptor antagonist
Two patient lists were used to identify patients for inclusion in the warfarin arm. The first patient list was generated using the US Department of Veterans Affairs (VA) Cirrhosis Tracker, which identified patients with an ICD-9/10 code for cirrhosis and an INR laboratory value. Patients generated from the VA Cirrhosis Tracker with an INR > 1.5 were screened for a warfarin prescription and then evaluated for full study inclusion. The second patient list was generated using the VA Advanced Liver Disease Dashboard which identified patients with ICD-9/10 codes for advanced liver disease and an active warfarin prescription. Patients with an active warfarin prescription were then evaluated for full study inclusion. A single patient list was generated to identify patients for inclusion in the DOAC arm. This patient list was generated using the VA DOAC dashboard, which identified patients with an active DOAC prescription and an ICD-9/10 code for cirrhosis. Patients with an ICD-9/10 code for cirrhosis and prescribed a DOAC were screened for full study inclusion. Patient data were collected from the MEDVAMC Computerized Patient Record System (CPRS) electronic health record (EHR). The research study was approved by the Baylor College of Medicine Institutional Review Board and the VA Office of Research and Development.
Outcomes
The primary endpoint for the study was all-cause bleeding. The secondary endpoints for the study were major bleeding and failed efficacy. Major bleeding was defined using the International Society on Thrombosis and Haemostasis (ISTH) 2005 definition: fatal bleeding, symptomatic bleeding in a critical organ area (ie, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome), or bleeding causing a fall in hemoglobin level of > 2 g/dL or leading to the transfusion of ≥ 2 units of red cells.6 Failed efficacy was a combination endpoint that included development of VTE, stroke, myocardial infarction (MI), and/or death. A prespecified subgroup analysis was conducted at the end of the study period to analyze trends in the DOAC and warfarin groups with respect to all-cause bleeding. All-cause bleeding risk was stratified by weight, BMI, Child-Turcotte-Pugh score, MELD score, presence of gastric and/or esophageal varices, active malignancies, percentage of time within therapeutic INR range in the warfarin group, indications for anticoagulation, and antiplatelet, NSAID, PPI, and H2RA therapy.
Statistical Analysis
Data were analyzed using descriptive and inferential statistics. Continuous data were analyzed using the Student t test, and categorical data were analyzed using the Fisher exact test. Previous studies determined an all-cause bleeding rate of 10 to 17% for warfarin compared with 5% for DOACs.7,8 To detect a 12% difference in the all-cause bleeding rate between DOACs and warfarin, 212 patients would be needed to achieve 80% power at an α level of 0.05.
Results
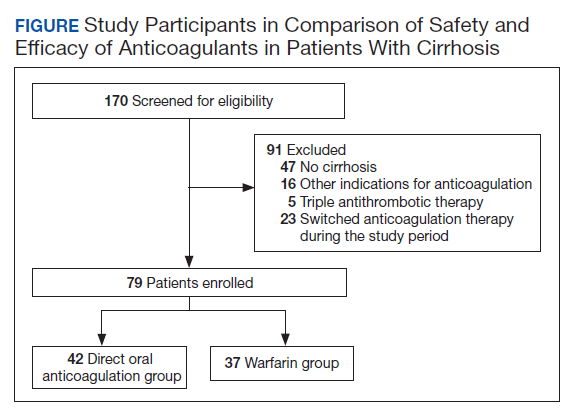
A total of 170 patients were screened, and after applying inclusion and exclusion criteria, 79 patients were enrolled in the study (Figure). The DOAC group included 42 patients, and the warfarin group included 37 patients. In the DOAC group, 69.1% (n = 29) of patients were taking apixaban, 21.4% (n = 9) rivaroxaban, and 9.5% (n = 4) dabigatran. There were no patients prescribed edoxaban during the study period.
Baseline characteristics were similar between the 2 groups except for Child-Turcotte-Pugh score, MELD score, mean INR, and number of days on anticoagulation therapy (Table 1). Most of the patients were male (98.7%), and the mean age was 71 years. The most common causes of cirrhosis were viral (29.1%), nonalcoholic fatty liver disease (NAFLD) (24.1%), multiple causes (22.8%), and alcohol (21.5%). Sixty-two patients (78.5%) had a NVAF indication for anticoagulation. The average CHA2DS2-VASc score was 3.7. Aspirin was prescribed in 51.9% (n = 41) of patients, and PPIs were prescribed in 48.1% (n = 38) of patients. At inclusion, esophageal varices were present in 13 patients and active malignancies were present in 6 patients.
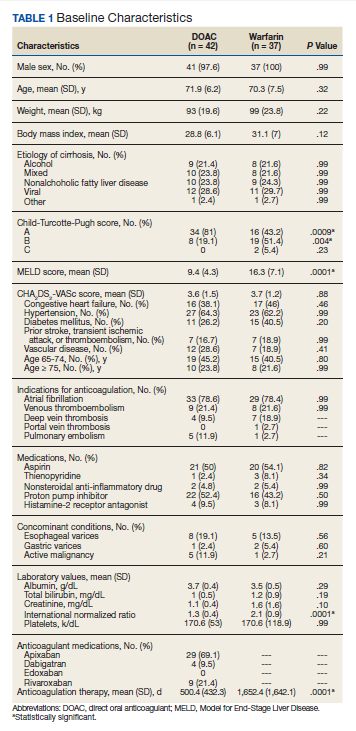
Statistically significant differences in baseline characteristics were found between mean INR, Child-Turcotte-Pugh scores, MELD scores, and number of days on anticoagulant therapy. The mean INR was 1.3 in the DOAC group compared with 2.1 in the warfarin group (P = .0001). Eighty-one percent (n = 34) of patients in the DOAC group had a Child-Turcotte-Pugh score of A compared with 43.2% (n = 16) of patients in the warfarin group (P = .0009). Eight patients in the DOAC group had a Child-Turcotte-Pugh score of B compared with 19 patients in the warfarin group (P = .004). The mean MELD score was 9.4 in the DOAC group compared with 16.3 in the warfarin group (P = .0001). The mean days on anticoagulant therapy was 500.4 days for the DOAC group compared with 1,652.4 days for the warfarin group (P = .0001).
Safety Outcome
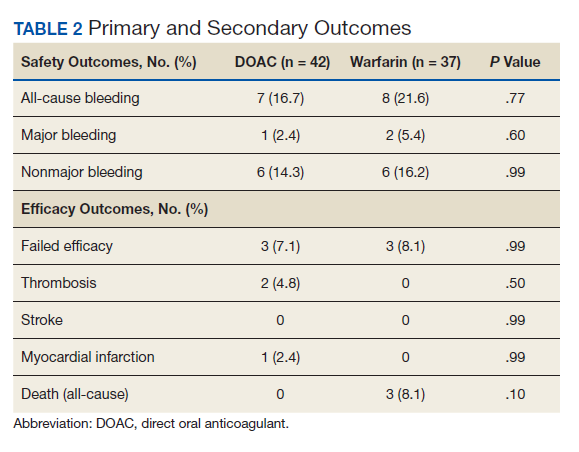
The primary outcome comparing all-cause bleeding rates between patients on DOACs compared with warfarin are listed in Table 2. With respect to the primary outcome, 7 (16.7%) patients on DOACs experienced a bleeding event compared with 8 (21.6%) patients on warfarin (P = .77). No statistically significant differences were detected between the DOAC and warfarin groups with respect to all-cause bleeding. Seven bleeding events occurred in the DOAC group; 1 met the qualification for major bleeding with a suspected gastrointestinal (GI) bleed.6 The other 6 bleeding episodes in the DOAC group consisted of hematoma, epistaxis, hematuria, and hematochezia. Eight bleeding events occurred in the warfarin group; 2 met the qualification for major bleeding with an intracranial hemorrhage and upper GI bleed.6 The other 6 bleeding episodes in the warfarin group consisted of epistaxis, bleeding gums, hematuria, and hematochezia. There were no statistically significant differences between the rates of major bleeding and nonmajor bleeding between the DOAC and warfarin groups.
Efficacy Outcomes
There were 3 events in the DOAC group and 3 events in the warfarin group (P = .99). In the DOAC group, 2 patients experienced a pulmonary embolism, and 1 patient experienced a MI. In the warfarin group, 3 patients died (end-stage heart failure, unknown cause due to death at an outside hospital, and sepsis/organ failure). There were no statistically significant differences between the composite endpoint of failed efficacy or the individual endpoints of VTE, stroke, MI, and death.
Subgroup Analysis
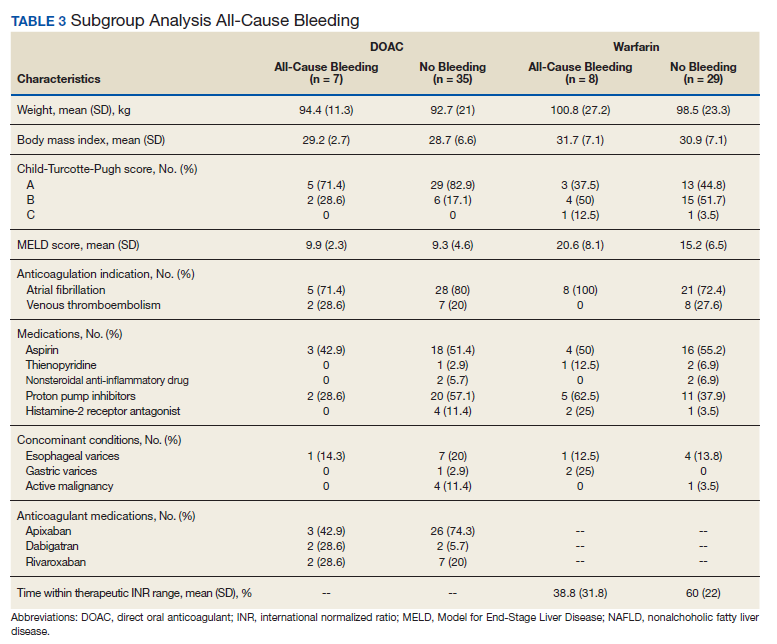
A prespecified subgroup analysis was conducted to determine risk factors for all-cause bleeding within each treatment group (Table 3). No significant trends were observed in the following risk factors: Child-Turcotte-Pugh score, indication for anticoagulation, use of NSAIDs, PPIs or H2RAs, presence of gastric or esophageal varices, active malignancies, and time within therapeutic INR range in the warfarin group. Patients with bleeding events had slightly increased weight and BMI vs patients without bleeding events. Within the warfarin group, patients with bleeding events had slightly elevated MELD scores compared to patients without bleeding events. There was an equal balance of patients prescribed aspirin therapy between the groups with and without bleeding events. Overall, no significant risk factors were identified for all-cause bleeding.
Discussion
Initially, patients with cirrhosis were excluded from DOAC trials due to concerns for increased bleeding risk with hepatically eliminated medications. New retrospective research has concluded that in patients with cirrhosis, DOACs have similar or lower bleeding rates when compared directly to warfarin.9,10
In this study, no statistically significant differences were detected between the primary and secondary outcomes of all-cause bleeding, major bleeding, or failed efficacy. Subgroup analysis did not identify any significant risk factors with respect to all-cause bleeding among patients in the DOAC and warfarin groups. To meet 80% power, 212 patients needed to be enrolled in the study; however, only 79 patients were enrolled, and power was not met. The results of this study should be interpreted cautiously as hypothesis-generating due to the small sample size. Strengths of this study include similar baseline characteristics between the DOAC and warfarin groups, 4-year length of retrospective data review, and availability of both inpatient and outpatient EHR limiting the amount of missing data points.
Baseline characteristics were similar between the groups except for mean INR, Child-Turcotte-Pugh score, MELD score, and number of days on anticoagulation therapy. The difference in mean INR between groups is expected as patients in the warfarin group have a goal INR of 2 to 3 to maintain therapeutic efficacy and safety. INR is not used as a marker of efficacy or safety with DOACs; therefore, a consistent elevation in INR is not expected. Child- Turcotte-Pugh scores are calculated using INR levels.11 When calculating the score, patients with an INR < 1.7 receive 1 point; patients with an INR between 1.7 and 2.3 receive 2 points.11 Therefore, patients in the warfarin group will have artificially inflated Child-Turcotte-Pugh scores as this group has goal INR levels of 2 to 3. This makes Child-Turcotte-Pugh scores unreliable markers of disease severity in patients using warfarin therapy. When the INR scores for patients prescribed warfarin were replaced with values < 1.7, the statistical difference disappeared between the warfarin and DOAC groups. The same effect is seen on MELD scores for patients prescribed warfarin therapy. The MELD score is calculated using INR levels.12 MELD scores also will be artificially elevated in patients prescribed warfarin therapy due to the INR elevation to between 2 and 3. When MELD scores for patients prescribed warfarin were replaced with values similar to those in the DOAC group, the statistical difference disappeared between the warfarin and DOAC groups.
The last statistically significant difference was found in number of days on anticoagulant therapy. This difference was expected as warfarin is the standard of care for anticoagulation treatment in patients with cirrhosis. The first DOAC, dabigatran, was not approved by the US Food and Drug Administration until 2010.13 DOACs have only recently been used in patients with cirrhosis accounting for the statistically significant difference in days on anticoagulation therapy between the warfarin and DOAC groups.
Limitations
The inability to meet power or evaluate adherence and appropriate renal dose adjustments for DOACs limited this study. This study was conducted at a single center in a predominantly male veteran population and therefore may not be generalizable to other populations. A majority of patients in the DOAC group were prescribed apixaban (69.1%), which may have affected the overall rate of major bleeding in the DOAC group. Pivotal trials of apixaban have shown a consistent decreased risk of major bleeding in patients with NVAF or VTE when compared with warfarin.14,15 Therefore, the results of this study may not be generalizable to all DOACs.
An inherent limitation of this study was the inability to collect data verifying adherence in the DOAC group. However, in the warfarin group, percentage of time within the therapeutic INR range of 2 to 3 was collected. While not a direct marker of adherence, this does allow for limited evaluation of therapeutic efficacy and safety within the warfarin group. Last, proper dosing of DOACs in patients with and without adequate renal function was not evaluated in this study.
Conclusions
The results of this study are consistent with other retrospective research and literature reviews. There were no statistically significant differences identified between the rates of all-cause bleeding, major bleeding, and failed efficacy between the DOAC and warfarin groups. DOACs may be a safe alternative to warfarin in patients with cirrhosis requiring anticoagulation for NVAF or VTE, but large randomized trials are required to confirm these results.
1. Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol. 2018;71(19):2162-2175. doi:10.1016/j.jacc.2018.03.023
2. Priyanka P, Kupec JT, Krafft M, Shah NA, Reynolds GJ. Newer oral anticoagulants in the treatment of acute portal vein thrombosis in patients with and without cirrhosis. Int J Hepatol. 2018;2018:8432781. Published 2018 Jun 5. doi:10.1155/2018/8432781
3. Intagliata NM, Henry ZH, Maitland H, et al. Direct oral anticoagulants in cirrhosis patients pose similar risks of bleeding when compared to traditional anticoagulation. Dig Dis Sci. 2016;61(6):1721-1727. doi:10.1007/s10620-015-4012-2
4. Hum J, Shatzel JJ, Jou JH, Deloughery TG. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur J Haematol. 2017;98(4):393-397. doi:10.1111/ejh.12844
5. Goriacko P, Veltri KT. Safety of direct oral anticoagulants vs warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol. 2018;100(5):488-493. doi:10.1111/ejh.13045
6. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
7. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351-358. doi:10.4330/wjc.v3.i11.351
8. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
9. Hoolwerf EW, Kraaijpoel N, Büller HR, van Es N. Direct oral anticoagulants in patients with liver cirrhosis: A systematic review. Thromb Res. 2018;170:102-108. doi:10.1016/j.thromres.2018.08.011
10. Steuber TD, Howard ML, Nisly SA. Direct oral anticoagulants in chronic liver disease. Ann Pharmacother. 2019;53(10):1042-1049. doi:10.1177/1060028019841582
11. Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. doi:10.3889/oamjms.2015.111
12. Singal AK, Kamath PS. Model for End-Stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
13. Joppa SA, Salciccioli J, Adamski J, et al. A practical review of the emerging direct anticoagulants, laboratory monitoring, and reversal agents. J Clin Med. 2018;7(2):29. Published 2018 Feb 11. doi:10.3390/jcm7020029
14. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. doi:10.1056/NEJMoa1107039
15. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799-808. doi:10.1056/NEJMoa1302507
Coagulation in patients with cirrhosis is a complicated area of evolving research. Patients with cirrhosis were originally thought to be naturally anticoagulated due to the decreased production of clotting factors and platelets, combined with an increased international normalized ratio (INR).1 New data have shown that patients with cirrhosis are at a concomitant risk of bleeding and thrombosis due to increased platelet aggregation, decreased fibrinolysis, and decreased production of natural anticoagulants such as protein C and antithrombin.1 Traditionally, patients with cirrhosis needing anticoagulation therapy for comorbid conditions, such as nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) were placed on warfarin therapy. Managing warfarin in patients with cirrhosis poses a challenge to clinicians due to the many food and drug interactions, narrow therapeutic index, and complications with maintaining a therapeutic INR.1
Direct oral anticoagulants (DOACs) have several benefits over warfarin therapy, including convenience, decreased monitoring, decreased drug and dietary restrictions, and faster onset of action.2 Conversely, DOACs undergo extensive hepatic metabolism giving rise to concerns about supratherapeutic drug levels and increased bleeding rates in patients with liver dysfunction.1 Consequently, patients with cirrhosis were excluded from the pivotal trials establishing DOACs for NVAF and VTE treatment. Exclusion of these patients in major clinical trials alongside the challenges of managing warfarin warrant an evaluation of the efficacy and safety of DOACs in patients with cirrhosis.
Recent retrospective studies have examined the use of DOACs in patients with cirrhosis and found favorable results. A retrospective chart review by Intagliata and colleagues consisting of 39 patients with cirrhosis using either a DOAC or warfarin found similar rates of all-cause bleeding and major bleeding between the 2 groups.3 A retrospective cohort study by Hum and colleagues consisting of 45 patients with cirrhosis compared the use of DOACs with warfarin or low-molecular weight heparin (LMWH).4 Hum and colleagues found patients prescribed a DOAC had significantly fewer major bleeding events than did patients using warfarin or LMWH.4 The largest retrospective cohort study consisted of 233 patients with chronic liver disease and found no differences among all-cause bleeding and major bleeding rates between patients using DOACs compared with those of patients using warfarin.5
The purpose of this research is to evaluate the safety and efficacy of DOACs in veteran patients with cirrhosis compared with patients using warfarin.
Methods
A retrospective single-center chart review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center (MEDVAMC) in Houston, Texas, between October 31, 2014 and October 31, 2018. Patients included in the study were adults aged ≥ 18 years with a diagnosis of cirrhosis and prescribed any of the following oral anticoagulants: apixaban, dabigatran, edoxaban, rivaroxaban, or warfarin. Patients prescribed apixaban, dabigatran, edoxaban, or rivaroxaban were collectively grouped into the DOAC group, while patients prescribed warfarin were classified as the standard of care comparator group.
A diagnosis of cirrhosis was confirmed using a combination of the codes from the ninth and tenth editions of the International Classification of Diseases (ICD) for cirrhosis, documentation of diagnostic confirmation by clinicians from the gastroenterology or hepatology services, and positive liver biopsy result. Liver function tests, liver ultrasound results, and FibroSure biomarker assays were used to aid in confirming the diagnosis of cirrhosis but were not considered definitive. Patients were excluded from the trial if they had indications for anticoagulation other than NVAF and VTE and/or were prescribed triple antithrombotic therapy (dual antiplatelet therapy plus an anticoagulant). Patients who switched anticoagulant therapy during the trial period (ie, switched from warfarin to a DOAC) were also excluded from the analysis.
Patient demographic characteristics that were collected included weight; body mass index (BMI); etiology of cirrhosis; Child-Turcotte-Pugh, Model for End-Stage Liver Disease (MELD), and CHA2DS2-VASc score; concomitant antiplatelet, nonsteroidal anti-inflammatory drug (NSAID), proton pump inhibitor (PPI), and histamine-2 receptor antagonist
Two patient lists were used to identify patients for inclusion in the warfarin arm. The first patient list was generated using the US Department of Veterans Affairs (VA) Cirrhosis Tracker, which identified patients with an ICD-9/10 code for cirrhosis and an INR laboratory value. Patients generated from the VA Cirrhosis Tracker with an INR > 1.5 were screened for a warfarin prescription and then evaluated for full study inclusion. The second patient list was generated using the VA Advanced Liver Disease Dashboard which identified patients with ICD-9/10 codes for advanced liver disease and an active warfarin prescription. Patients with an active warfarin prescription were then evaluated for full study inclusion. A single patient list was generated to identify patients for inclusion in the DOAC arm. This patient list was generated using the VA DOAC dashboard, which identified patients with an active DOAC prescription and an ICD-9/10 code for cirrhosis. Patients with an ICD-9/10 code for cirrhosis and prescribed a DOAC were screened for full study inclusion. Patient data were collected from the MEDVAMC Computerized Patient Record System (CPRS) electronic health record (EHR). The research study was approved by the Baylor College of Medicine Institutional Review Board and the VA Office of Research and Development.
Outcomes
The primary endpoint for the study was all-cause bleeding. The secondary endpoints for the study were major bleeding and failed efficacy. Major bleeding was defined using the International Society on Thrombosis and Haemostasis (ISTH) 2005 definition: fatal bleeding, symptomatic bleeding in a critical organ area (ie, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome), or bleeding causing a fall in hemoglobin level of > 2 g/dL or leading to the transfusion of ≥ 2 units of red cells.6 Failed efficacy was a combination endpoint that included development of VTE, stroke, myocardial infarction (MI), and/or death. A prespecified subgroup analysis was conducted at the end of the study period to analyze trends in the DOAC and warfarin groups with respect to all-cause bleeding. All-cause bleeding risk was stratified by weight, BMI, Child-Turcotte-Pugh score, MELD score, presence of gastric and/or esophageal varices, active malignancies, percentage of time within therapeutic INR range in the warfarin group, indications for anticoagulation, and antiplatelet, NSAID, PPI, and H2RA therapy.
Statistical Analysis
Data were analyzed using descriptive and inferential statistics. Continuous data were analyzed using the Student t test, and categorical data were analyzed using the Fisher exact test. Previous studies determined an all-cause bleeding rate of 10 to 17% for warfarin compared with 5% for DOACs.7,8 To detect a 12% difference in the all-cause bleeding rate between DOACs and warfarin, 212 patients would be needed to achieve 80% power at an α level of 0.05.
Results
A total of 170 patients were screened, and after applying inclusion and exclusion criteria, 79 patients were enrolled in the study (Figure). The DOAC group included 42 patients, and the warfarin group included 37 patients. In the DOAC group, 69.1% (n = 29) of patients were taking apixaban, 21.4% (n = 9) rivaroxaban, and 9.5% (n = 4) dabigatran. There were no patients prescribed edoxaban during the study period.
Baseline characteristics were similar between the 2 groups except for Child-Turcotte-Pugh score, MELD score, mean INR, and number of days on anticoagulation therapy (Table 1). Most of the patients were male (98.7%), and the mean age was 71 years. The most common causes of cirrhosis were viral (29.1%), nonalcoholic fatty liver disease (NAFLD) (24.1%), multiple causes (22.8%), and alcohol (21.5%). Sixty-two patients (78.5%) had a NVAF indication for anticoagulation. The average CHA2DS2-VASc score was 3.7. Aspirin was prescribed in 51.9% (n = 41) of patients, and PPIs were prescribed in 48.1% (n = 38) of patients. At inclusion, esophageal varices were present in 13 patients and active malignancies were present in 6 patients.
Statistically significant differences in baseline characteristics were found between mean INR, Child-Turcotte-Pugh scores, MELD scores, and number of days on anticoagulant therapy. The mean INR was 1.3 in the DOAC group compared with 2.1 in the warfarin group (P = .0001). Eighty-one percent (n = 34) of patients in the DOAC group had a Child-Turcotte-Pugh score of A compared with 43.2% (n = 16) of patients in the warfarin group (P = .0009). Eight patients in the DOAC group had a Child-Turcotte-Pugh score of B compared with 19 patients in the warfarin group (P = .004). The mean MELD score was 9.4 in the DOAC group compared with 16.3 in the warfarin group (P = .0001). The mean days on anticoagulant therapy was 500.4 days for the DOAC group compared with 1,652.4 days for the warfarin group (P = .0001).
Safety Outcome
The primary outcome comparing all-cause bleeding rates between patients on DOACs compared with warfarin are listed in Table 2. With respect to the primary outcome, 7 (16.7%) patients on DOACs experienced a bleeding event compared with 8 (21.6%) patients on warfarin (P = .77). No statistically significant differences were detected between the DOAC and warfarin groups with respect to all-cause bleeding. Seven bleeding events occurred in the DOAC group; 1 met the qualification for major bleeding with a suspected gastrointestinal (GI) bleed.6 The other 6 bleeding episodes in the DOAC group consisted of hematoma, epistaxis, hematuria, and hematochezia. Eight bleeding events occurred in the warfarin group; 2 met the qualification for major bleeding with an intracranial hemorrhage and upper GI bleed.6 The other 6 bleeding episodes in the warfarin group consisted of epistaxis, bleeding gums, hematuria, and hematochezia. There were no statistically significant differences between the rates of major bleeding and nonmajor bleeding between the DOAC and warfarin groups.
Efficacy Outcomes
There were 3 events in the DOAC group and 3 events in the warfarin group (P = .99). In the DOAC group, 2 patients experienced a pulmonary embolism, and 1 patient experienced a MI. In the warfarin group, 3 patients died (end-stage heart failure, unknown cause due to death at an outside hospital, and sepsis/organ failure). There were no statistically significant differences between the composite endpoint of failed efficacy or the individual endpoints of VTE, stroke, MI, and death.
Subgroup Analysis
A prespecified subgroup analysis was conducted to determine risk factors for all-cause bleeding within each treatment group (Table 3). No significant trends were observed in the following risk factors: Child-Turcotte-Pugh score, indication for anticoagulation, use of NSAIDs, PPIs or H2RAs, presence of gastric or esophageal varices, active malignancies, and time within therapeutic INR range in the warfarin group. Patients with bleeding events had slightly increased weight and BMI vs patients without bleeding events. Within the warfarin group, patients with bleeding events had slightly elevated MELD scores compared to patients without bleeding events. There was an equal balance of patients prescribed aspirin therapy between the groups with and without bleeding events. Overall, no significant risk factors were identified for all-cause bleeding.
Discussion
Initially, patients with cirrhosis were excluded from DOAC trials due to concerns for increased bleeding risk with hepatically eliminated medications. New retrospective research has concluded that in patients with cirrhosis, DOACs have similar or lower bleeding rates when compared directly to warfarin.9,10
In this study, no statistically significant differences were detected between the primary and secondary outcomes of all-cause bleeding, major bleeding, or failed efficacy. Subgroup analysis did not identify any significant risk factors with respect to all-cause bleeding among patients in the DOAC and warfarin groups. To meet 80% power, 212 patients needed to be enrolled in the study; however, only 79 patients were enrolled, and power was not met. The results of this study should be interpreted cautiously as hypothesis-generating due to the small sample size. Strengths of this study include similar baseline characteristics between the DOAC and warfarin groups, 4-year length of retrospective data review, and availability of both inpatient and outpatient EHR limiting the amount of missing data points.
Baseline characteristics were similar between the groups except for mean INR, Child-Turcotte-Pugh score, MELD score, and number of days on anticoagulation therapy. The difference in mean INR between groups is expected as patients in the warfarin group have a goal INR of 2 to 3 to maintain therapeutic efficacy and safety. INR is not used as a marker of efficacy or safety with DOACs; therefore, a consistent elevation in INR is not expected. Child- Turcotte-Pugh scores are calculated using INR levels.11 When calculating the score, patients with an INR < 1.7 receive 1 point; patients with an INR between 1.7 and 2.3 receive 2 points.11 Therefore, patients in the warfarin group will have artificially inflated Child-Turcotte-Pugh scores as this group has goal INR levels of 2 to 3. This makes Child-Turcotte-Pugh scores unreliable markers of disease severity in patients using warfarin therapy. When the INR scores for patients prescribed warfarin were replaced with values < 1.7, the statistical difference disappeared between the warfarin and DOAC groups. The same effect is seen on MELD scores for patients prescribed warfarin therapy. The MELD score is calculated using INR levels.12 MELD scores also will be artificially elevated in patients prescribed warfarin therapy due to the INR elevation to between 2 and 3. When MELD scores for patients prescribed warfarin were replaced with values similar to those in the DOAC group, the statistical difference disappeared between the warfarin and DOAC groups.
The last statistically significant difference was found in number of days on anticoagulant therapy. This difference was expected as warfarin is the standard of care for anticoagulation treatment in patients with cirrhosis. The first DOAC, dabigatran, was not approved by the US Food and Drug Administration until 2010.13 DOACs have only recently been used in patients with cirrhosis accounting for the statistically significant difference in days on anticoagulation therapy between the warfarin and DOAC groups.
Limitations
The inability to meet power or evaluate adherence and appropriate renal dose adjustments for DOACs limited this study. This study was conducted at a single center in a predominantly male veteran population and therefore may not be generalizable to other populations. A majority of patients in the DOAC group were prescribed apixaban (69.1%), which may have affected the overall rate of major bleeding in the DOAC group. Pivotal trials of apixaban have shown a consistent decreased risk of major bleeding in patients with NVAF or VTE when compared with warfarin.14,15 Therefore, the results of this study may not be generalizable to all DOACs.
An inherent limitation of this study was the inability to collect data verifying adherence in the DOAC group. However, in the warfarin group, percentage of time within the therapeutic INR range of 2 to 3 was collected. While not a direct marker of adherence, this does allow for limited evaluation of therapeutic efficacy and safety within the warfarin group. Last, proper dosing of DOACs in patients with and without adequate renal function was not evaluated in this study.
Conclusions
The results of this study are consistent with other retrospective research and literature reviews. There were no statistically significant differences identified between the rates of all-cause bleeding, major bleeding, and failed efficacy between the DOAC and warfarin groups. DOACs may be a safe alternative to warfarin in patients with cirrhosis requiring anticoagulation for NVAF or VTE, but large randomized trials are required to confirm these results.
Coagulation in patients with cirrhosis is a complicated area of evolving research. Patients with cirrhosis were originally thought to be naturally anticoagulated due to the decreased production of clotting factors and platelets, combined with an increased international normalized ratio (INR).1 New data have shown that patients with cirrhosis are at a concomitant risk of bleeding and thrombosis due to increased platelet aggregation, decreased fibrinolysis, and decreased production of natural anticoagulants such as protein C and antithrombin.1 Traditionally, patients with cirrhosis needing anticoagulation therapy for comorbid conditions, such as nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) were placed on warfarin therapy. Managing warfarin in patients with cirrhosis poses a challenge to clinicians due to the many food and drug interactions, narrow therapeutic index, and complications with maintaining a therapeutic INR.1
Direct oral anticoagulants (DOACs) have several benefits over warfarin therapy, including convenience, decreased monitoring, decreased drug and dietary restrictions, and faster onset of action.2 Conversely, DOACs undergo extensive hepatic metabolism giving rise to concerns about supratherapeutic drug levels and increased bleeding rates in patients with liver dysfunction.1 Consequently, patients with cirrhosis were excluded from the pivotal trials establishing DOACs for NVAF and VTE treatment. Exclusion of these patients in major clinical trials alongside the challenges of managing warfarin warrant an evaluation of the efficacy and safety of DOACs in patients with cirrhosis.
Recent retrospective studies have examined the use of DOACs in patients with cirrhosis and found favorable results. A retrospective chart review by Intagliata and colleagues consisting of 39 patients with cirrhosis using either a DOAC or warfarin found similar rates of all-cause bleeding and major bleeding between the 2 groups.3 A retrospective cohort study by Hum and colleagues consisting of 45 patients with cirrhosis compared the use of DOACs with warfarin or low-molecular weight heparin (LMWH).4 Hum and colleagues found patients prescribed a DOAC had significantly fewer major bleeding events than did patients using warfarin or LMWH.4 The largest retrospective cohort study consisted of 233 patients with chronic liver disease and found no differences among all-cause bleeding and major bleeding rates between patients using DOACs compared with those of patients using warfarin.5
The purpose of this research is to evaluate the safety and efficacy of DOACs in veteran patients with cirrhosis compared with patients using warfarin.
Methods
A retrospective single-center chart review was conducted at the Michael E. DeBakey Veterans Affairs Medical Center (MEDVAMC) in Houston, Texas, between October 31, 2014 and October 31, 2018. Patients included in the study were adults aged ≥ 18 years with a diagnosis of cirrhosis and prescribed any of the following oral anticoagulants: apixaban, dabigatran, edoxaban, rivaroxaban, or warfarin. Patients prescribed apixaban, dabigatran, edoxaban, or rivaroxaban were collectively grouped into the DOAC group, while patients prescribed warfarin were classified as the standard of care comparator group.
A diagnosis of cirrhosis was confirmed using a combination of the codes from the ninth and tenth editions of the International Classification of Diseases (ICD) for cirrhosis, documentation of diagnostic confirmation by clinicians from the gastroenterology or hepatology services, and positive liver biopsy result. Liver function tests, liver ultrasound results, and FibroSure biomarker assays were used to aid in confirming the diagnosis of cirrhosis but were not considered definitive. Patients were excluded from the trial if they had indications for anticoagulation other than NVAF and VTE and/or were prescribed triple antithrombotic therapy (dual antiplatelet therapy plus an anticoagulant). Patients who switched anticoagulant therapy during the trial period (ie, switched from warfarin to a DOAC) were also excluded from the analysis.
Patient demographic characteristics that were collected included weight; body mass index (BMI); etiology of cirrhosis; Child-Turcotte-Pugh, Model for End-Stage Liver Disease (MELD), and CHA2DS2-VASc score; concomitant antiplatelet, nonsteroidal anti-inflammatory drug (NSAID), proton pump inhibitor (PPI), and histamine-2 receptor antagonist
Two patient lists were used to identify patients for inclusion in the warfarin arm. The first patient list was generated using the US Department of Veterans Affairs (VA) Cirrhosis Tracker, which identified patients with an ICD-9/10 code for cirrhosis and an INR laboratory value. Patients generated from the VA Cirrhosis Tracker with an INR > 1.5 were screened for a warfarin prescription and then evaluated for full study inclusion. The second patient list was generated using the VA Advanced Liver Disease Dashboard which identified patients with ICD-9/10 codes for advanced liver disease and an active warfarin prescription. Patients with an active warfarin prescription were then evaluated for full study inclusion. A single patient list was generated to identify patients for inclusion in the DOAC arm. This patient list was generated using the VA DOAC dashboard, which identified patients with an active DOAC prescription and an ICD-9/10 code for cirrhosis. Patients with an ICD-9/10 code for cirrhosis and prescribed a DOAC were screened for full study inclusion. Patient data were collected from the MEDVAMC Computerized Patient Record System (CPRS) electronic health record (EHR). The research study was approved by the Baylor College of Medicine Institutional Review Board and the VA Office of Research and Development.
Outcomes
The primary endpoint for the study was all-cause bleeding. The secondary endpoints for the study were major bleeding and failed efficacy. Major bleeding was defined using the International Society on Thrombosis and Haemostasis (ISTH) 2005 definition: fatal bleeding, symptomatic bleeding in a critical organ area (ie, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial, or intramuscular with compartment syndrome), or bleeding causing a fall in hemoglobin level of > 2 g/dL or leading to the transfusion of ≥ 2 units of red cells.6 Failed efficacy was a combination endpoint that included development of VTE, stroke, myocardial infarction (MI), and/or death. A prespecified subgroup analysis was conducted at the end of the study period to analyze trends in the DOAC and warfarin groups with respect to all-cause bleeding. All-cause bleeding risk was stratified by weight, BMI, Child-Turcotte-Pugh score, MELD score, presence of gastric and/or esophageal varices, active malignancies, percentage of time within therapeutic INR range in the warfarin group, indications for anticoagulation, and antiplatelet, NSAID, PPI, and H2RA therapy.
Statistical Analysis
Data were analyzed using descriptive and inferential statistics. Continuous data were analyzed using the Student t test, and categorical data were analyzed using the Fisher exact test. Previous studies determined an all-cause bleeding rate of 10 to 17% for warfarin compared with 5% for DOACs.7,8 To detect a 12% difference in the all-cause bleeding rate between DOACs and warfarin, 212 patients would be needed to achieve 80% power at an α level of 0.05.
Results
A total of 170 patients were screened, and after applying inclusion and exclusion criteria, 79 patients were enrolled in the study (Figure). The DOAC group included 42 patients, and the warfarin group included 37 patients. In the DOAC group, 69.1% (n = 29) of patients were taking apixaban, 21.4% (n = 9) rivaroxaban, and 9.5% (n = 4) dabigatran. There were no patients prescribed edoxaban during the study period.
Baseline characteristics were similar between the 2 groups except for Child-Turcotte-Pugh score, MELD score, mean INR, and number of days on anticoagulation therapy (Table 1). Most of the patients were male (98.7%), and the mean age was 71 years. The most common causes of cirrhosis were viral (29.1%), nonalcoholic fatty liver disease (NAFLD) (24.1%), multiple causes (22.8%), and alcohol (21.5%). Sixty-two patients (78.5%) had a NVAF indication for anticoagulation. The average CHA2DS2-VASc score was 3.7. Aspirin was prescribed in 51.9% (n = 41) of patients, and PPIs were prescribed in 48.1% (n = 38) of patients. At inclusion, esophageal varices were present in 13 patients and active malignancies were present in 6 patients.
Statistically significant differences in baseline characteristics were found between mean INR, Child-Turcotte-Pugh scores, MELD scores, and number of days on anticoagulant therapy. The mean INR was 1.3 in the DOAC group compared with 2.1 in the warfarin group (P = .0001). Eighty-one percent (n = 34) of patients in the DOAC group had a Child-Turcotte-Pugh score of A compared with 43.2% (n = 16) of patients in the warfarin group (P = .0009). Eight patients in the DOAC group had a Child-Turcotte-Pugh score of B compared with 19 patients in the warfarin group (P = .004). The mean MELD score was 9.4 in the DOAC group compared with 16.3 in the warfarin group (P = .0001). The mean days on anticoagulant therapy was 500.4 days for the DOAC group compared with 1,652.4 days for the warfarin group (P = .0001).
Safety Outcome
The primary outcome comparing all-cause bleeding rates between patients on DOACs compared with warfarin are listed in Table 2. With respect to the primary outcome, 7 (16.7%) patients on DOACs experienced a bleeding event compared with 8 (21.6%) patients on warfarin (P = .77). No statistically significant differences were detected between the DOAC and warfarin groups with respect to all-cause bleeding. Seven bleeding events occurred in the DOAC group; 1 met the qualification for major bleeding with a suspected gastrointestinal (GI) bleed.6 The other 6 bleeding episodes in the DOAC group consisted of hematoma, epistaxis, hematuria, and hematochezia. Eight bleeding events occurred in the warfarin group; 2 met the qualification for major bleeding with an intracranial hemorrhage and upper GI bleed.6 The other 6 bleeding episodes in the warfarin group consisted of epistaxis, bleeding gums, hematuria, and hematochezia. There were no statistically significant differences between the rates of major bleeding and nonmajor bleeding between the DOAC and warfarin groups.
Efficacy Outcomes
There were 3 events in the DOAC group and 3 events in the warfarin group (P = .99). In the DOAC group, 2 patients experienced a pulmonary embolism, and 1 patient experienced a MI. In the warfarin group, 3 patients died (end-stage heart failure, unknown cause due to death at an outside hospital, and sepsis/organ failure). There were no statistically significant differences between the composite endpoint of failed efficacy or the individual endpoints of VTE, stroke, MI, and death.
Subgroup Analysis
A prespecified subgroup analysis was conducted to determine risk factors for all-cause bleeding within each treatment group (Table 3). No significant trends were observed in the following risk factors: Child-Turcotte-Pugh score, indication for anticoagulation, use of NSAIDs, PPIs or H2RAs, presence of gastric or esophageal varices, active malignancies, and time within therapeutic INR range in the warfarin group. Patients with bleeding events had slightly increased weight and BMI vs patients without bleeding events. Within the warfarin group, patients with bleeding events had slightly elevated MELD scores compared to patients without bleeding events. There was an equal balance of patients prescribed aspirin therapy between the groups with and without bleeding events. Overall, no significant risk factors were identified for all-cause bleeding.
Discussion
Initially, patients with cirrhosis were excluded from DOAC trials due to concerns for increased bleeding risk with hepatically eliminated medications. New retrospective research has concluded that in patients with cirrhosis, DOACs have similar or lower bleeding rates when compared directly to warfarin.9,10
In this study, no statistically significant differences were detected between the primary and secondary outcomes of all-cause bleeding, major bleeding, or failed efficacy. Subgroup analysis did not identify any significant risk factors with respect to all-cause bleeding among patients in the DOAC and warfarin groups. To meet 80% power, 212 patients needed to be enrolled in the study; however, only 79 patients were enrolled, and power was not met. The results of this study should be interpreted cautiously as hypothesis-generating due to the small sample size. Strengths of this study include similar baseline characteristics between the DOAC and warfarin groups, 4-year length of retrospective data review, and availability of both inpatient and outpatient EHR limiting the amount of missing data points.
Baseline characteristics were similar between the groups except for mean INR, Child-Turcotte-Pugh score, MELD score, and number of days on anticoagulation therapy. The difference in mean INR between groups is expected as patients in the warfarin group have a goal INR of 2 to 3 to maintain therapeutic efficacy and safety. INR is not used as a marker of efficacy or safety with DOACs; therefore, a consistent elevation in INR is not expected. Child- Turcotte-Pugh scores are calculated using INR levels.11 When calculating the score, patients with an INR < 1.7 receive 1 point; patients with an INR between 1.7 and 2.3 receive 2 points.11 Therefore, patients in the warfarin group will have artificially inflated Child-Turcotte-Pugh scores as this group has goal INR levels of 2 to 3. This makes Child-Turcotte-Pugh scores unreliable markers of disease severity in patients using warfarin therapy. When the INR scores for patients prescribed warfarin were replaced with values < 1.7, the statistical difference disappeared between the warfarin and DOAC groups. The same effect is seen on MELD scores for patients prescribed warfarin therapy. The MELD score is calculated using INR levels.12 MELD scores also will be artificially elevated in patients prescribed warfarin therapy due to the INR elevation to between 2 and 3. When MELD scores for patients prescribed warfarin were replaced with values similar to those in the DOAC group, the statistical difference disappeared between the warfarin and DOAC groups.
The last statistically significant difference was found in number of days on anticoagulant therapy. This difference was expected as warfarin is the standard of care for anticoagulation treatment in patients with cirrhosis. The first DOAC, dabigatran, was not approved by the US Food and Drug Administration until 2010.13 DOACs have only recently been used in patients with cirrhosis accounting for the statistically significant difference in days on anticoagulation therapy between the warfarin and DOAC groups.
Limitations
The inability to meet power or evaluate adherence and appropriate renal dose adjustments for DOACs limited this study. This study was conducted at a single center in a predominantly male veteran population and therefore may not be generalizable to other populations. A majority of patients in the DOAC group were prescribed apixaban (69.1%), which may have affected the overall rate of major bleeding in the DOAC group. Pivotal trials of apixaban have shown a consistent decreased risk of major bleeding in patients with NVAF or VTE when compared with warfarin.14,15 Therefore, the results of this study may not be generalizable to all DOACs.
An inherent limitation of this study was the inability to collect data verifying adherence in the DOAC group. However, in the warfarin group, percentage of time within the therapeutic INR range of 2 to 3 was collected. While not a direct marker of adherence, this does allow for limited evaluation of therapeutic efficacy and safety within the warfarin group. Last, proper dosing of DOACs in patients with and without adequate renal function was not evaluated in this study.
Conclusions
The results of this study are consistent with other retrospective research and literature reviews. There were no statistically significant differences identified between the rates of all-cause bleeding, major bleeding, and failed efficacy between the DOAC and warfarin groups. DOACs may be a safe alternative to warfarin in patients with cirrhosis requiring anticoagulation for NVAF or VTE, but large randomized trials are required to confirm these results.
1. Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol. 2018;71(19):2162-2175. doi:10.1016/j.jacc.2018.03.023
2. Priyanka P, Kupec JT, Krafft M, Shah NA, Reynolds GJ. Newer oral anticoagulants in the treatment of acute portal vein thrombosis in patients with and without cirrhosis. Int J Hepatol. 2018;2018:8432781. Published 2018 Jun 5. doi:10.1155/2018/8432781
3. Intagliata NM, Henry ZH, Maitland H, et al. Direct oral anticoagulants in cirrhosis patients pose similar risks of bleeding when compared to traditional anticoagulation. Dig Dis Sci. 2016;61(6):1721-1727. doi:10.1007/s10620-015-4012-2
4. Hum J, Shatzel JJ, Jou JH, Deloughery TG. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur J Haematol. 2017;98(4):393-397. doi:10.1111/ejh.12844
5. Goriacko P, Veltri KT. Safety of direct oral anticoagulants vs warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol. 2018;100(5):488-493. doi:10.1111/ejh.13045
6. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
7. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351-358. doi:10.4330/wjc.v3.i11.351
8. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
9. Hoolwerf EW, Kraaijpoel N, Büller HR, van Es N. Direct oral anticoagulants in patients with liver cirrhosis: A systematic review. Thromb Res. 2018;170:102-108. doi:10.1016/j.thromres.2018.08.011
10. Steuber TD, Howard ML, Nisly SA. Direct oral anticoagulants in chronic liver disease. Ann Pharmacother. 2019;53(10):1042-1049. doi:10.1177/1060028019841582
11. Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. doi:10.3889/oamjms.2015.111
12. Singal AK, Kamath PS. Model for End-Stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
13. Joppa SA, Salciccioli J, Adamski J, et al. A practical review of the emerging direct anticoagulants, laboratory monitoring, and reversal agents. J Clin Med. 2018;7(2):29. Published 2018 Feb 11. doi:10.3390/jcm7020029
14. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. doi:10.1056/NEJMoa1107039
15. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799-808. doi:10.1056/NEJMoa1302507
1. Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol. 2018;71(19):2162-2175. doi:10.1016/j.jacc.2018.03.023
2. Priyanka P, Kupec JT, Krafft M, Shah NA, Reynolds GJ. Newer oral anticoagulants in the treatment of acute portal vein thrombosis in patients with and without cirrhosis. Int J Hepatol. 2018;2018:8432781. Published 2018 Jun 5. doi:10.1155/2018/8432781
3. Intagliata NM, Henry ZH, Maitland H, et al. Direct oral anticoagulants in cirrhosis patients pose similar risks of bleeding when compared to traditional anticoagulation. Dig Dis Sci. 2016;61(6):1721-1727. doi:10.1007/s10620-015-4012-2
4. Hum J, Shatzel JJ, Jou JH, Deloughery TG. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur J Haematol. 2017;98(4):393-397. doi:10.1111/ejh.12844
5. Goriacko P, Veltri KT. Safety of direct oral anticoagulants vs warfarin in patients with chronic liver disease and atrial fibrillation. Eur J Haematol. 2018;100(5):488-493. doi:10.1111/ejh.13045
6. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
7. Rubboli A, Becattini C, Verheugt FW. Incidence, clinical impact and risk of bleeding during oral anticoagulation therapy. World J Cardiol. 2011;3(11):351-358. doi:10.4330/wjc.v3.i11.351
8. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
9. Hoolwerf EW, Kraaijpoel N, Büller HR, van Es N. Direct oral anticoagulants in patients with liver cirrhosis: A systematic review. Thromb Res. 2018;170:102-108. doi:10.1016/j.thromres.2018.08.011
10. Steuber TD, Howard ML, Nisly SA. Direct oral anticoagulants in chronic liver disease. Ann Pharmacother. 2019;53(10):1042-1049. doi:10.1177/1060028019841582
11. Janevska D, Chaloska-Ivanova V, Janevski V. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;3(4):732-736. doi:10.3889/oamjms.2015.111
12. Singal AK, Kamath PS. Model for End-Stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
13. Joppa SA, Salciccioli J, Adamski J, et al. A practical review of the emerging direct anticoagulants, laboratory monitoring, and reversal agents. J Clin Med. 2018;7(2):29. Published 2018 Feb 11. doi:10.3390/jcm7020029
14. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. doi:10.1056/NEJMoa1107039
15. Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369(9):799-808. doi:10.1056/NEJMoa1302507
MI recurrences drop, but women underestimate disease risk
The number of heart attack survivors in the United States who experienced repeat attacks within a year decreased between 2008 and 2017, especially among women, yet women’s awareness of their risk of death from heart disease also decreased, according to data from a pair of studies published in Circulation.
Recurrent MI rates drop, but not enough
Although the overall morbidity and mortality from coronary heart disease (CHD) in the United States has been on the decline for decades, CHD remains the leading cause of death and disability in both sexes, wrote Sanne A.E. Peters, PhD, of Imperial College London, and colleagues.
To better assess the rates of recurrent CHD by sex, the researchers reviewed data from 770,408 women and 700,477 men younger than 65 years with commercial health insurance or aged 66 years and older with Medicare who were hospitalized for myocardial infarction between 2008 and 2017. The patients were followed for 1 year for recurrent MIs, recurrent CHD events, heart failure hospitalization, and all-cause mortality.
In the study of recurrent heart disease, the rate of recurrent heart attacks per 1,000 person-years declined from 89.2 to 72.3 in women and from 94.2 to 81.3 in men. In addition, the rate of recurrent heart disease events (defined as either an MI or an artery-opening procedure), dropped per 1,000 person-years from 166.3 to 133.3 in women and from 198.1 to 176.8 in men. The reduction was significantly greater among women compared with men (P < .001 for both recurrent MIs and recurrent CHD events) and the differences by sex were consistent throughout the study period.
However, no significant difference occurred in recurrent MI rates among younger women (aged 21-54 years), or men aged 55-79 years, the researchers noted.
Heart failure rates per 1,000 person-years decreased from 177.4 to 158.1 in women and from 162.9 to 156.1 in men during the study period, and all-cause mortality decreased per 1,000 person-years from 403.2 to 389.5 for women and from 436.1 to 417.9 in men.
Potential contributing factors to the reductions in rates of recurrent events after a heart attack may include improved acute cardiac procedures, in-hospital therapy, and secondary prevention, the researchers noted. In addition, “changes in the type and definition of MI may also have contributed to the decline in recurrent events,” they said. “Also, the introduction and increasing sensitivity of cardiac biomarkers assays, especially cardiac troponin, may have contributed to an increased detection of less severe MIs over time, which, in turn, could have resulted in artifactual reductions in the consequences of MI,” they said.
The study findings were limited by several factors including the use of claims data, lack of information on the severity of heart attacks, and inability to analyze population subgroups, but the results were strengthened by the use of a large, multicultural database.
Despite the decline seen in this study, overall rates of recurrent MI, recurrent CHD events, heart failure hospitalization, and mortality remain high, the researchers said, and the results “highlight the need for interventions to ensure men and women receive guideline recommended treatment to lower the risk for recurrent MI, recurrent CHD, heart failure, and mortality after hospital discharge for MI,” they concluded.
Many women don’t recognize heart disease risk
Although women showed a greater reduction in recurrent MI and recurrent CHD events compared with men, the awareness of heart disease as the No. 1 killer of women has declined, according to a special report from the American Heart Association.
Based on survey data from 2009, 65% of women were aware that heart disease was their leading cause of death (LCOD); by 2019 the number dropped to 44%. The 10-year decline occurred across all races and ethnicities, as well as ages, with the exception of women aged 65 years and older.
The American Heart Association has conducted national surveys since 1997 to monitor awareness of cardiovascular disease among U.S. women. Data from earlier surveys showed increased awareness of heart disease as LCOD and increased awareness of heart attack symptoms between 1997 and 2012, wrote Mary Cushman, MD, of the University of Vermont, Burlington, chair of the writing group for the statement, and colleagues.

However, overall awareness and knowledge of heart disease among women remains poor, they wrote.
“Awareness programs designed to educate the public about CVD among women in the United States include Go Red for Women by the American Heart Association; The Heart Truth by the National Heart, Lung, and Blood Institute; and Make the Call, Don’t Miss a Beat by the U.S. Department of Health and Human Services,” the researchers noted. To determine the change in awareness of heart disease as the LCOD among women, the researchers conducted a multivariate analysis of 1,158 women who completed the 2009 survey and 1,345 who completed the 2019 survey. The average age was 50 years; roughly 70% of the participants in the 2009 survey and 62% in the 2019 survey were non-Hispanic White.
The greatest declines in awareness of heart disease as LCOD occurred among Hispanics and non-Hispanic Blacks and among all respondents aged 25-34 years.
Awareness of heart disease as LCOD was 30% lower among women with high blood pressure compared with women overall, the researchers noted.
“In both surveys, higher educational attainment was strongly related to awareness that heart disease is the LCOD,” the researchers said. However, the results highlight the need for renewed efforts to educate younger women, Hispanic women, and non-Hispanic Black women, they emphasized. Unpublished data from the AHA survey showed that “younger women were less likely to report leading a heart-healthy lifestyle and were more likely to identify multiple barriers to leading a heart-healthy lifestyle, including lack of time, stress, and lack of confidence,” they wrote.
In addition, awareness of heart attack warning signs declined overall and within each ethnic group between 2009 and 2019.
The survey results were limited by several factors including the use of an online-only model that might limit generalizability to populations without online access, and was conducted only in English, the researchers wrote.
Heart disease needs new PR plan
The study of heart disease risk awareness among women was an important update to understand how well the message about women’s risk is getting out, said Martha Gulati, MD, president-elect of the American Society of Preventive Cardiology, in an interview.
The issue remains that heart disease is the No. 1 killer of women, and the decrease in awareness “means we need to amplify our message,” she said.
“I also question whether the symbol of the red dress [for women’s heart disease] is working, and it seems that now is the time to change this symbol,” she emphasized. “I wear a red dress pin on my lab coat and every day someone asks what it means, and no one recognizes it,” she said. “I think ‘Go Red for Women’ is great and part of our outward campaign, but our symbol needs to change to increase the connection and awareness in women,” she said.
What might be a better symbol? Simply, a heart, said Dr. Gulati. But “we need to study whatever is next to really connect with women and make them understand their risk for heart disease,” she added.
“Additionally, we really need to get to minority women,” she said. “We are lagging there, and the survey was conducted in English so it missed many people,” she noted.
Dr. Gulati said she was shocked at how much awareness of heart disease risk has fallen among women, even in those with risk factors such as hypertension, who were 30% less likely to be aware that heart disease remains their leading cause of death. “Younger women as well as very unaware; what this means to me is that our public education efforts need to be amplified,” Dr. Gulati said.
Barriers to educating women about heart disease risk include language and access to affordable screening, Dr. Gulati emphasized. “We need to ensure screening for heart disease is always included as a covered cost for a preventive service,” she said.
“Research needs to be done to identify what works toward educating women about cardiac risk. We need to identify a marketing tool to increase awareness in women. It might be something different for one race versus another,” Dr. Gulati said. “Our messaging needs to improve, but how we improve it needs more than just health care professionals,” she said.
Focus on prevention to reduce MI recurrence
“The study regarding recurrent events after MI is important because we really don’t know much about recurrent coronary heart disease after a MI over time,” said Dr. Gulati. These data can be helpful in managing surviving patients and understanding future risk, she said. “But I was surprised to see fewer recurrent events in women, as women still have more heart failure than men even if it has declined with time,” she noted.
Dr. Gulati questioned several aspects of the study and highlighted some of the limitations. “These are claims data, so do they accurately reflect the U.S. population?” she asked. “Remember, this is a study of people who survived a heart attack; those who didn’t survive aren’t included, and that group is more likely to be women, especially women younger than 55 years,” she said.
In addition, Dr. Gulati noted the lack of data on type of heart attack and on treatment adherence or referral to cardiac rehab, as well as lack of data on long-term medication adherence or follow-up care.
Prevention is the key take-home message from both studies, “whether we are talking primary prevention for the heart disease awareness study or secondary prevention for the recurrent heart attack study,” Dr. Gulati said.
The recurrent heart disease study was supported in part by Amgen and the University of Alabama at Birmingham. Lead author Dr. Peters disclosed support from a UK Medical Research Council Skills Development Fellowship with no financial conflicts. Dr. Cushman had no financial conflicts to disclose; several coauthors on the writing committee disclosed relationships with companies including Amarin and Boehringer Ingelheim. Dr. Gulati had no financial conflicts to disclose.
SOURCE: Peters SAE et al. Circulation. 2020 Sep 21. doi: 10.1161/CIRCULATIONAHA.120.047065; Cushman M et al. Circulation. 2020 Sep 21. doi: 10.1161/CIR.0000000000000907.
The number of heart attack survivors in the United States who experienced repeat attacks within a year decreased between 2008 and 2017, especially among women, yet women’s awareness of their risk of death from heart disease also decreased, according to data from a pair of studies published in Circulation.
Recurrent MI rates drop, but not enough
Although the overall morbidity and mortality from coronary heart disease (CHD) in the United States has been on the decline for decades, CHD remains the leading cause of death and disability in both sexes, wrote Sanne A.E. Peters, PhD, of Imperial College London, and colleagues.
To better assess the rates of recurrent CHD by sex, the researchers reviewed data from 770,408 women and 700,477 men younger than 65 years with commercial health insurance or aged 66 years and older with Medicare who were hospitalized for myocardial infarction between 2008 and 2017. The patients were followed for 1 year for recurrent MIs, recurrent CHD events, heart failure hospitalization, and all-cause mortality.
In the study of recurrent heart disease, the rate of recurrent heart attacks per 1,000 person-years declined from 89.2 to 72.3 in women and from 94.2 to 81.3 in men. In addition, the rate of recurrent heart disease events (defined as either an MI or an artery-opening procedure), dropped per 1,000 person-years from 166.3 to 133.3 in women and from 198.1 to 176.8 in men. The reduction was significantly greater among women compared with men (P < .001 for both recurrent MIs and recurrent CHD events) and the differences by sex were consistent throughout the study period.
However, no significant difference occurred in recurrent MI rates among younger women (aged 21-54 years), or men aged 55-79 years, the researchers noted.
Heart failure rates per 1,000 person-years decreased from 177.4 to 158.1 in women and from 162.9 to 156.1 in men during the study period, and all-cause mortality decreased per 1,000 person-years from 403.2 to 389.5 for women and from 436.1 to 417.9 in men.
Potential contributing factors to the reductions in rates of recurrent events after a heart attack may include improved acute cardiac procedures, in-hospital therapy, and secondary prevention, the researchers noted. In addition, “changes in the type and definition of MI may also have contributed to the decline in recurrent events,” they said. “Also, the introduction and increasing sensitivity of cardiac biomarkers assays, especially cardiac troponin, may have contributed to an increased detection of less severe MIs over time, which, in turn, could have resulted in artifactual reductions in the consequences of MI,” they said.
The study findings were limited by several factors including the use of claims data, lack of information on the severity of heart attacks, and inability to analyze population subgroups, but the results were strengthened by the use of a large, multicultural database.
Despite the decline seen in this study, overall rates of recurrent MI, recurrent CHD events, heart failure hospitalization, and mortality remain high, the researchers said, and the results “highlight the need for interventions to ensure men and women receive guideline recommended treatment to lower the risk for recurrent MI, recurrent CHD, heart failure, and mortality after hospital discharge for MI,” they concluded.
Many women don’t recognize heart disease risk
Although women showed a greater reduction in recurrent MI and recurrent CHD events compared with men, the awareness of heart disease as the No. 1 killer of women has declined, according to a special report from the American Heart Association.
Based on survey data from 2009, 65% of women were aware that heart disease was their leading cause of death (LCOD); by 2019 the number dropped to 44%. The 10-year decline occurred across all races and ethnicities, as well as ages, with the exception of women aged 65 years and older.
The American Heart Association has conducted national surveys since 1997 to monitor awareness of cardiovascular disease among U.S. women. Data from earlier surveys showed increased awareness of heart disease as LCOD and increased awareness of heart attack symptoms between 1997 and 2012, wrote Mary Cushman, MD, of the University of Vermont, Burlington, chair of the writing group for the statement, and colleagues.
However, overall awareness and knowledge of heart disease among women remains poor, they wrote.
“Awareness programs designed to educate the public about CVD among women in the United States include Go Red for Women by the American Heart Association; The Heart Truth by the National Heart, Lung, and Blood Institute; and Make the Call, Don’t Miss a Beat by the U.S. Department of Health and Human Services,” the researchers noted. To determine the change in awareness of heart disease as the LCOD among women, the researchers conducted a multivariate analysis of 1,158 women who completed the 2009 survey and 1,345 who completed the 2019 survey. The average age was 50 years; roughly 70% of the participants in the 2009 survey and 62% in the 2019 survey were non-Hispanic White.
The greatest declines in awareness of heart disease as LCOD occurred among Hispanics and non-Hispanic Blacks and among all respondents aged 25-34 years.
Awareness of heart disease as LCOD was 30% lower among women with high blood pressure compared with women overall, the researchers noted.
“In both surveys, higher educational attainment was strongly related to awareness that heart disease is the LCOD,” the researchers said. However, the results highlight the need for renewed efforts to educate younger women, Hispanic women, and non-Hispanic Black women, they emphasized. Unpublished data from the AHA survey showed that “younger women were less likely to report leading a heart-healthy lifestyle and were more likely to identify multiple barriers to leading a heart-healthy lifestyle, including lack of time, stress, and lack of confidence,” they wrote.
In addition, awareness of heart attack warning signs declined overall and within each ethnic group between 2009 and 2019.
The survey results were limited by several factors including the use of an online-only model that might limit generalizability to populations without online access, and was conducted only in English, the researchers wrote.
Heart disease needs new PR plan
The study of heart disease risk awareness among women was an important update to understand how well the message about women’s risk is getting out, said Martha Gulati, MD, president-elect of the American Society of Preventive Cardiology, in an interview.
The issue remains that heart disease is the No. 1 killer of women, and the decrease in awareness “means we need to amplify our message,” she said.
“I also question whether the symbol of the red dress [for women’s heart disease] is working, and it seems that now is the time to change this symbol,” she emphasized. “I wear a red dress pin on my lab coat and every day someone asks what it means, and no one recognizes it,” she said. “I think ‘Go Red for Women’ is great and part of our outward campaign, but our symbol needs to change to increase the connection and awareness in women,” she said.
What might be a better symbol? Simply, a heart, said Dr. Gulati. But “we need to study whatever is next to really connect with women and make them understand their risk for heart disease,” she added.
“Additionally, we really need to get to minority women,” she said. “We are lagging there, and the survey was conducted in English so it missed many people,” she noted.
Dr. Gulati said she was shocked at how much awareness of heart disease risk has fallen among women, even in those with risk factors such as hypertension, who were 30% less likely to be aware that heart disease remains their leading cause of death. “Younger women as well as very unaware; what this means to me is that our public education efforts need to be amplified,” Dr. Gulati said.
Barriers to educating women about heart disease risk include language and access to affordable screening, Dr. Gulati emphasized. “We need to ensure screening for heart disease is always included as a covered cost for a preventive service,” she said.
“Research needs to be done to identify what works toward educating women about cardiac risk. We need to identify a marketing tool to increase awareness in women. It might be something different for one race versus another,” Dr. Gulati said. “Our messaging needs to improve, but how we improve it needs more than just health care professionals,” she said.
Focus on prevention to reduce MI recurrence
“The study regarding recurrent events after MI is important because we really don’t know much about recurrent coronary heart disease after a MI over time,” said Dr. Gulati. These data can be helpful in managing surviving patients and understanding future risk, she said. “But I was surprised to see fewer recurrent events in women, as women still have more heart failure than men even if it has declined with time,” she noted.
Dr. Gulati questioned several aspects of the study and highlighted some of the limitations. “These are claims data, so do they accurately reflect the U.S. population?” she asked. “Remember, this is a study of people who survived a heart attack; those who didn’t survive aren’t included, and that group is more likely to be women, especially women younger than 55 years,” she said.
In addition, Dr. Gulati noted the lack of data on type of heart attack and on treatment adherence or referral to cardiac rehab, as well as lack of data on long-term medication adherence or follow-up care.
Prevention is the key take-home message from both studies, “whether we are talking primary prevention for the heart disease awareness study or secondary prevention for the recurrent heart attack study,” Dr. Gulati said.
The recurrent heart disease study was supported in part by Amgen and the University of Alabama at Birmingham. Lead author Dr. Peters disclosed support from a UK Medical Research Council Skills Development Fellowship with no financial conflicts. Dr. Cushman had no financial conflicts to disclose; several coauthors on the writing committee disclosed relationships with companies including Amarin and Boehringer Ingelheim. Dr. Gulati had no financial conflicts to disclose.
SOURCE: Peters SAE et al. Circulation. 2020 Sep 21. doi: 10.1161/CIRCULATIONAHA.120.047065; Cushman M et al. Circulation. 2020 Sep 21. doi: 10.1161/CIR.0000000000000907.
The number of heart attack survivors in the United States who experienced repeat attacks within a year decreased between 2008 and 2017, especially among women, yet women’s awareness of their risk of death from heart disease also decreased, according to data from a pair of studies published in Circulation.
Recurrent MI rates drop, but not enough
Although the overall morbidity and mortality from coronary heart disease (CHD) in the United States has been on the decline for decades, CHD remains the leading cause of death and disability in both sexes, wrote Sanne A.E. Peters, PhD, of Imperial College London, and colleagues.
To better assess the rates of recurrent CHD by sex, the researchers reviewed data from 770,408 women and 700,477 men younger than 65 years with commercial health insurance or aged 66 years and older with Medicare who were hospitalized for myocardial infarction between 2008 and 2017. The patients were followed for 1 year for recurrent MIs, recurrent CHD events, heart failure hospitalization, and all-cause mortality.
In the study of recurrent heart disease, the rate of recurrent heart attacks per 1,000 person-years declined from 89.2 to 72.3 in women and from 94.2 to 81.3 in men. In addition, the rate of recurrent heart disease events (defined as either an MI or an artery-opening procedure), dropped per 1,000 person-years from 166.3 to 133.3 in women and from 198.1 to 176.8 in men. The reduction was significantly greater among women compared with men (P < .001 for both recurrent MIs and recurrent CHD events) and the differences by sex were consistent throughout the study period.
However, no significant difference occurred in recurrent MI rates among younger women (aged 21-54 years), or men aged 55-79 years, the researchers noted.
Heart failure rates per 1,000 person-years decreased from 177.4 to 158.1 in women and from 162.9 to 156.1 in men during the study period, and all-cause mortality decreased per 1,000 person-years from 403.2 to 389.5 for women and from 436.1 to 417.9 in men.
Potential contributing factors to the reductions in rates of recurrent events after a heart attack may include improved acute cardiac procedures, in-hospital therapy, and secondary prevention, the researchers noted. In addition, “changes in the type and definition of MI may also have contributed to the decline in recurrent events,” they said. “Also, the introduction and increasing sensitivity of cardiac biomarkers assays, especially cardiac troponin, may have contributed to an increased detection of less severe MIs over time, which, in turn, could have resulted in artifactual reductions in the consequences of MI,” they said.
The study findings were limited by several factors including the use of claims data, lack of information on the severity of heart attacks, and inability to analyze population subgroups, but the results were strengthened by the use of a large, multicultural database.
Despite the decline seen in this study, overall rates of recurrent MI, recurrent CHD events, heart failure hospitalization, and mortality remain high, the researchers said, and the results “highlight the need for interventions to ensure men and women receive guideline recommended treatment to lower the risk for recurrent MI, recurrent CHD, heart failure, and mortality after hospital discharge for MI,” they concluded.
Many women don’t recognize heart disease risk
Although women showed a greater reduction in recurrent MI and recurrent CHD events compared with men, the awareness of heart disease as the No. 1 killer of women has declined, according to a special report from the American Heart Association.
Based on survey data from 2009, 65% of women were aware that heart disease was their leading cause of death (LCOD); by 2019 the number dropped to 44%. The 10-year decline occurred across all races and ethnicities, as well as ages, with the exception of women aged 65 years and older.
The American Heart Association has conducted national surveys since 1997 to monitor awareness of cardiovascular disease among U.S. women. Data from earlier surveys showed increased awareness of heart disease as LCOD and increased awareness of heart attack symptoms between 1997 and 2012, wrote Mary Cushman, MD, of the University of Vermont, Burlington, chair of the writing group for the statement, and colleagues.
However, overall awareness and knowledge of heart disease among women remains poor, they wrote.
“Awareness programs designed to educate the public about CVD among women in the United States include Go Red for Women by the American Heart Association; The Heart Truth by the National Heart, Lung, and Blood Institute; and Make the Call, Don’t Miss a Beat by the U.S. Department of Health and Human Services,” the researchers noted. To determine the change in awareness of heart disease as the LCOD among women, the researchers conducted a multivariate analysis of 1,158 women who completed the 2009 survey and 1,345 who completed the 2019 survey. The average age was 50 years; roughly 70% of the participants in the 2009 survey and 62% in the 2019 survey were non-Hispanic White.
The greatest declines in awareness of heart disease as LCOD occurred among Hispanics and non-Hispanic Blacks and among all respondents aged 25-34 years.
Awareness of heart disease as LCOD was 30% lower among women with high blood pressure compared with women overall, the researchers noted.
“In both surveys, higher educational attainment was strongly related to awareness that heart disease is the LCOD,” the researchers said. However, the results highlight the need for renewed efforts to educate younger women, Hispanic women, and non-Hispanic Black women, they emphasized. Unpublished data from the AHA survey showed that “younger women were less likely to report leading a heart-healthy lifestyle and were more likely to identify multiple barriers to leading a heart-healthy lifestyle, including lack of time, stress, and lack of confidence,” they wrote.
In addition, awareness of heart attack warning signs declined overall and within each ethnic group between 2009 and 2019.
The survey results were limited by several factors including the use of an online-only model that might limit generalizability to populations without online access, and was conducted only in English, the researchers wrote.
Heart disease needs new PR plan
The study of heart disease risk awareness among women was an important update to understand how well the message about women’s risk is getting out, said Martha Gulati, MD, president-elect of the American Society of Preventive Cardiology, in an interview.
The issue remains that heart disease is the No. 1 killer of women, and the decrease in awareness “means we need to amplify our message,” she said.
“I also question whether the symbol of the red dress [for women’s heart disease] is working, and it seems that now is the time to change this symbol,” she emphasized. “I wear a red dress pin on my lab coat and every day someone asks what it means, and no one recognizes it,” she said. “I think ‘Go Red for Women’ is great and part of our outward campaign, but our symbol needs to change to increase the connection and awareness in women,” she said.
What might be a better symbol? Simply, a heart, said Dr. Gulati. But “we need to study whatever is next to really connect with women and make them understand their risk for heart disease,” she added.
“Additionally, we really need to get to minority women,” she said. “We are lagging there, and the survey was conducted in English so it missed many people,” she noted.
Dr. Gulati said she was shocked at how much awareness of heart disease risk has fallen among women, even in those with risk factors such as hypertension, who were 30% less likely to be aware that heart disease remains their leading cause of death. “Younger women as well as very unaware; what this means to me is that our public education efforts need to be amplified,” Dr. Gulati said.
Barriers to educating women about heart disease risk include language and access to affordable screening, Dr. Gulati emphasized. “We need to ensure screening for heart disease is always included as a covered cost for a preventive service,” she said.
“Research needs to be done to identify what works toward educating women about cardiac risk. We need to identify a marketing tool to increase awareness in women. It might be something different for one race versus another,” Dr. Gulati said. “Our messaging needs to improve, but how we improve it needs more than just health care professionals,” she said.
Focus on prevention to reduce MI recurrence
“The study regarding recurrent events after MI is important because we really don’t know much about recurrent coronary heart disease after a MI over time,” said Dr. Gulati. These data can be helpful in managing surviving patients and understanding future risk, she said. “But I was surprised to see fewer recurrent events in women, as women still have more heart failure than men even if it has declined with time,” she noted.
Dr. Gulati questioned several aspects of the study and highlighted some of the limitations. “These are claims data, so do they accurately reflect the U.S. population?” she asked. “Remember, this is a study of people who survived a heart attack; those who didn’t survive aren’t included, and that group is more likely to be women, especially women younger than 55 years,” she said.
In addition, Dr. Gulati noted the lack of data on type of heart attack and on treatment adherence or referral to cardiac rehab, as well as lack of data on long-term medication adherence or follow-up care.
Prevention is the key take-home message from both studies, “whether we are talking primary prevention for the heart disease awareness study or secondary prevention for the recurrent heart attack study,” Dr. Gulati said.
The recurrent heart disease study was supported in part by Amgen and the University of Alabama at Birmingham. Lead author Dr. Peters disclosed support from a UK Medical Research Council Skills Development Fellowship with no financial conflicts. Dr. Cushman had no financial conflicts to disclose; several coauthors on the writing committee disclosed relationships with companies including Amarin and Boehringer Ingelheim. Dr. Gulati had no financial conflicts to disclose.
SOURCE: Peters SAE et al. Circulation. 2020 Sep 21. doi: 10.1161/CIRCULATIONAHA.120.047065; Cushman M et al. Circulation. 2020 Sep 21. doi: 10.1161/CIR.0000000000000907.
FROM CIRCULATION
Time-restricted eating shows no weight-loss benefit in RCT
The popular new weight-loss approach of eating within a restricted window of time during the day, allowing for an extended period of fasting – also known as intermittent fasting – does not result in greater weight loss, compared with nonrestricted meal timing, results from a randomized clinical trial show.
“I was very surprised by all of [the results],” senior author Ethan J. Weiss, MD, said in an interview.
“Part of the reason we did the study was because I had been doing time-restricted eating myself for years and even recommending it to friends and patients as an effective weight-loss tool,” said Dr. Weiss, of the Cardiovascular Research Institute, University of California, San Francisco.
“But no matter how you slice it, prescription of time-restricted eating – at least this version –is not a very effective weight-loss strategy,” Dr. Weiss said.
The study, published online in JAMA Internal Medicine by Dylan A. Lowe, PhD, also of the University of California, San Francisco, involved 116 participants who were randomized to a 12-week regimen of either three structured meals per day or time-restricted eating, with instructions to eat only between 12:00 p.m. and 8:00 p.m. and to completely abstain from eating at other times.
The participants were not given any specific instructions regarding caloric or macronutrient intake “so as to offer a simple, real-world recommendation to free-living individuals,” the authors wrote.
Although some prior research has shown improvements in measures such as glucose tolerance with time-restricted eating, studies showing weight loss with the approach, including one recently reported by Medscape Medical News, have been small and lacked control groups.
“To my knowledge this is the first randomized, controlled trial and definitely the biggest,” Dr. Weiss. “I think it is the most comprehensive dataset available in people, at least for this intervention.”
Participants used app to log details
At baseline, participants had a mean weight of 99.2 kg (approximately 219 lb). Their mean age was 46.5 years and 60.3% were men. They were drawn from anywhere in the United States and received study surveys through a custom mobile study application on the Eureka Research Platform. They were given a Bluetooth weight scale to use daily, which was connected with the app, and randomized to one of the two interventions. A subset of 50 participants living near San Francisco underwent in-person testing.
At the end of the 12 weeks, those in the time-restricted eating group (n = 59) did have a significant decrease in weight, compared with baseline (−0.94 kg; P = .01), while weight loss in the consistent-meal group (n = 57) was not significant (−0.68 kg; P = .07).
But importantly, the difference in weight loss between the groups was not significant (−0.26 kg; P = .63).
There were no significant differences in secondary outcomes of fasting insulin, glucose, hemoglobin A1c, or blood lipids within or between the time-restricted eating and consistent-meal group either. Nor were there any significant differences in resting metabolic rate.
Although participants did not self-report their caloric intake, the authors estimated that the differences were not significant using mathematical modeling developed at the National Institutes of Health.
Rates of adherence to the diets were 92.1% in the consistent-meal group versus 83.5% in the time-restricted group.
Not all diets are equal: Time-restricted eating group lost more lean mass
In a subset analysis, loss of lean mass was significantly greater in the time-restricted eating group, compared with the consistent-meals group, in terms of both appendicular lean mass (P = .009) and the appendicular lean mass index (P = .005).
In fact, as much as 65% of the weight lost (1.10 kg of the average 1.70 kg) in the time-restricted eating group consisted of lean mass, while much less was fat mass (0.51 kg).
“The proportion of lean mass loss in this study (approximately 65%) far exceeds the normal range of 20%-30%,” the authors wrote. “In addition, there was a highly significant between-group difference in appendicular lean mass.”
Appendicular lean mass correlates with nutritional and physical status, and its reduction can lead to weakness, disability, and impaired quality of life.
“This serves as a caution for patient populations at risk for sarcopenia because time-restricted eating could exacerbate muscle loss,” the authors asserted.
Furthermore, previous studies suggest that the loss of lean mass in such studies is positively linked with weight regain.
While a limitation of the work is that self-reported measures of energy or macronutrient or protein intake were not obtained, the authors speculated that the role of protein intake could be linked to the greater loss of lean mass.
“Given the loss of appendicular lean mass in participants in the time-restricted eating arm and previous reports of decreased protein consumption from time-restricted eating, it is possible that protein intake was altered by time-restricted eating in this cohort, and this clearly warrants future study,” they wrote.
Dr. Weiss said the findings underscore that not all weight loss in dieting is beneficial.
“Losing 1 kg of lean mass (is not equal) to a kilogram of fat,” he said. “Indeed, if one loses 0.65 kg of lean mass and only 0.35 kg of fat mass, that is an intervention I’d probably pass on.”
Time-restricted eating is popular, perhaps because it’s easy?
Time-restricted eating has gained popularity in recent years.
The approach “is attractive as a weight-loss option in that it does not require tedious and time-consuming methods such as calorie counting or adherence to complicated diets,” the authors noted. “Indeed, we found that self-reported adherence to the time-restricted eating schedule was high; however, in contrast to our hypothesis, there was no greater weight loss with time-restricted eating compared with the consistent meal timing.”
They explain that the 12 p.m. to 8 p.m. window for eating was chosen because they thought people might find it easier culturally to skip breakfast than dinner, the more social meal.
However, an 8 p.m. cutoff is somewhat late given there is some suggestion that fasting several hours before bedtime is most beneficial, Dr. Weiss noted. So it may be worth examining different time windows.
“I am very intrigued about looking at early time-restricted eating – 6 a.m. to 2 p.m.,” for example, he said. “It is on our list.”
Meanwhile, the study results support previous research showing no effect on weight outcomes in relation to skipping breakfast.
The study received funding from the UCSF cardiology division’s Cardiology Innovations Award Program and the National Institute of Diabetes and Digestive and Kidney Diseases, with additional support from the James Peter Read Foundation. Dr. Weiss has reported nonfinancial support from Mocacare and nonfinancial support from iHealth Labs during the conduct of the study. He also is a cofounder and equity stakeholder of Keyto, and owns stock and was formerly on the board of Virta.
A version of this article originally appeared on Medscape.com.
The popular new weight-loss approach of eating within a restricted window of time during the day, allowing for an extended period of fasting – also known as intermittent fasting – does not result in greater weight loss, compared with nonrestricted meal timing, results from a randomized clinical trial show.
“I was very surprised by all of [the results],” senior author Ethan J. Weiss, MD, said in an interview.
“Part of the reason we did the study was because I had been doing time-restricted eating myself for years and even recommending it to friends and patients as an effective weight-loss tool,” said Dr. Weiss, of the Cardiovascular Research Institute, University of California, San Francisco.
“But no matter how you slice it, prescription of time-restricted eating – at least this version –is not a very effective weight-loss strategy,” Dr. Weiss said.
The study, published online in JAMA Internal Medicine by Dylan A. Lowe, PhD, also of the University of California, San Francisco, involved 116 participants who were randomized to a 12-week regimen of either three structured meals per day or time-restricted eating, with instructions to eat only between 12:00 p.m. and 8:00 p.m. and to completely abstain from eating at other times.
The participants were not given any specific instructions regarding caloric or macronutrient intake “so as to offer a simple, real-world recommendation to free-living individuals,” the authors wrote.
Although some prior research has shown improvements in measures such as glucose tolerance with time-restricted eating, studies showing weight loss with the approach, including one recently reported by Medscape Medical News, have been small and lacked control groups.
“To my knowledge this is the first randomized, controlled trial and definitely the biggest,” Dr. Weiss. “I think it is the most comprehensive dataset available in people, at least for this intervention.”
Participants used app to log details
At baseline, participants had a mean weight of 99.2 kg (approximately 219 lb). Their mean age was 46.5 years and 60.3% were men. They were drawn from anywhere in the United States and received study surveys through a custom mobile study application on the Eureka Research Platform. They were given a Bluetooth weight scale to use daily, which was connected with the app, and randomized to one of the two interventions. A subset of 50 participants living near San Francisco underwent in-person testing.
At the end of the 12 weeks, those in the time-restricted eating group (n = 59) did have a significant decrease in weight, compared with baseline (−0.94 kg; P = .01), while weight loss in the consistent-meal group (n = 57) was not significant (−0.68 kg; P = .07).
But importantly, the difference in weight loss between the groups was not significant (−0.26 kg; P = .63).
There were no significant differences in secondary outcomes of fasting insulin, glucose, hemoglobin A1c, or blood lipids within or between the time-restricted eating and consistent-meal group either. Nor were there any significant differences in resting metabolic rate.
Although participants did not self-report their caloric intake, the authors estimated that the differences were not significant using mathematical modeling developed at the National Institutes of Health.
Rates of adherence to the diets were 92.1% in the consistent-meal group versus 83.5% in the time-restricted group.
Not all diets are equal: Time-restricted eating group lost more lean mass
In a subset analysis, loss of lean mass was significantly greater in the time-restricted eating group, compared with the consistent-meals group, in terms of both appendicular lean mass (P = .009) and the appendicular lean mass index (P = .005).
In fact, as much as 65% of the weight lost (1.10 kg of the average 1.70 kg) in the time-restricted eating group consisted of lean mass, while much less was fat mass (0.51 kg).
“The proportion of lean mass loss in this study (approximately 65%) far exceeds the normal range of 20%-30%,” the authors wrote. “In addition, there was a highly significant between-group difference in appendicular lean mass.”
Appendicular lean mass correlates with nutritional and physical status, and its reduction can lead to weakness, disability, and impaired quality of life.
“This serves as a caution for patient populations at risk for sarcopenia because time-restricted eating could exacerbate muscle loss,” the authors asserted.
Furthermore, previous studies suggest that the loss of lean mass in such studies is positively linked with weight regain.
While a limitation of the work is that self-reported measures of energy or macronutrient or protein intake were not obtained, the authors speculated that the role of protein intake could be linked to the greater loss of lean mass.
“Given the loss of appendicular lean mass in participants in the time-restricted eating arm and previous reports of decreased protein consumption from time-restricted eating, it is possible that protein intake was altered by time-restricted eating in this cohort, and this clearly warrants future study,” they wrote.
Dr. Weiss said the findings underscore that not all weight loss in dieting is beneficial.
“Losing 1 kg of lean mass (is not equal) to a kilogram of fat,” he said. “Indeed, if one loses 0.65 kg of lean mass and only 0.35 kg of fat mass, that is an intervention I’d probably pass on.”
Time-restricted eating is popular, perhaps because it’s easy?
Time-restricted eating has gained popularity in recent years.
The approach “is attractive as a weight-loss option in that it does not require tedious and time-consuming methods such as calorie counting or adherence to complicated diets,” the authors noted. “Indeed, we found that self-reported adherence to the time-restricted eating schedule was high; however, in contrast to our hypothesis, there was no greater weight loss with time-restricted eating compared with the consistent meal timing.”
They explain that the 12 p.m. to 8 p.m. window for eating was chosen because they thought people might find it easier culturally to skip breakfast than dinner, the more social meal.
However, an 8 p.m. cutoff is somewhat late given there is some suggestion that fasting several hours before bedtime is most beneficial, Dr. Weiss noted. So it may be worth examining different time windows.
“I am very intrigued about looking at early time-restricted eating – 6 a.m. to 2 p.m.,” for example, he said. “It is on our list.”
Meanwhile, the study results support previous research showing no effect on weight outcomes in relation to skipping breakfast.
The study received funding from the UCSF cardiology division’s Cardiology Innovations Award Program and the National Institute of Diabetes and Digestive and Kidney Diseases, with additional support from the James Peter Read Foundation. Dr. Weiss has reported nonfinancial support from Mocacare and nonfinancial support from iHealth Labs during the conduct of the study. He also is a cofounder and equity stakeholder of Keyto, and owns stock and was formerly on the board of Virta.
A version of this article originally appeared on Medscape.com.
The popular new weight-loss approach of eating within a restricted window of time during the day, allowing for an extended period of fasting – also known as intermittent fasting – does not result in greater weight loss, compared with nonrestricted meal timing, results from a randomized clinical trial show.
“I was very surprised by all of [the results],” senior author Ethan J. Weiss, MD, said in an interview.
“Part of the reason we did the study was because I had been doing time-restricted eating myself for years and even recommending it to friends and patients as an effective weight-loss tool,” said Dr. Weiss, of the Cardiovascular Research Institute, University of California, San Francisco.
“But no matter how you slice it, prescription of time-restricted eating – at least this version –is not a very effective weight-loss strategy,” Dr. Weiss said.
The study, published online in JAMA Internal Medicine by Dylan A. Lowe, PhD, also of the University of California, San Francisco, involved 116 participants who were randomized to a 12-week regimen of either three structured meals per day or time-restricted eating, with instructions to eat only between 12:00 p.m. and 8:00 p.m. and to completely abstain from eating at other times.
The participants were not given any specific instructions regarding caloric or macronutrient intake “so as to offer a simple, real-world recommendation to free-living individuals,” the authors wrote.
Although some prior research has shown improvements in measures such as glucose tolerance with time-restricted eating, studies showing weight loss with the approach, including one recently reported by Medscape Medical News, have been small and lacked control groups.
“To my knowledge this is the first randomized, controlled trial and definitely the biggest,” Dr. Weiss. “I think it is the most comprehensive dataset available in people, at least for this intervention.”
Participants used app to log details
At baseline, participants had a mean weight of 99.2 kg (approximately 219 lb). Their mean age was 46.5 years and 60.3% were men. They were drawn from anywhere in the United States and received study surveys through a custom mobile study application on the Eureka Research Platform. They were given a Bluetooth weight scale to use daily, which was connected with the app, and randomized to one of the two interventions. A subset of 50 participants living near San Francisco underwent in-person testing.
At the end of the 12 weeks, those in the time-restricted eating group (n = 59) did have a significant decrease in weight, compared with baseline (−0.94 kg; P = .01), while weight loss in the consistent-meal group (n = 57) was not significant (−0.68 kg; P = .07).
But importantly, the difference in weight loss between the groups was not significant (−0.26 kg; P = .63).
There were no significant differences in secondary outcomes of fasting insulin, glucose, hemoglobin A1c, or blood lipids within or between the time-restricted eating and consistent-meal group either. Nor were there any significant differences in resting metabolic rate.
Although participants did not self-report their caloric intake, the authors estimated that the differences were not significant using mathematical modeling developed at the National Institutes of Health.
Rates of adherence to the diets were 92.1% in the consistent-meal group versus 83.5% in the time-restricted group.
Not all diets are equal: Time-restricted eating group lost more lean mass
In a subset analysis, loss of lean mass was significantly greater in the time-restricted eating group, compared with the consistent-meals group, in terms of both appendicular lean mass (P = .009) and the appendicular lean mass index (P = .005).
In fact, as much as 65% of the weight lost (1.10 kg of the average 1.70 kg) in the time-restricted eating group consisted of lean mass, while much less was fat mass (0.51 kg).
“The proportion of lean mass loss in this study (approximately 65%) far exceeds the normal range of 20%-30%,” the authors wrote. “In addition, there was a highly significant between-group difference in appendicular lean mass.”
Appendicular lean mass correlates with nutritional and physical status, and its reduction can lead to weakness, disability, and impaired quality of life.
“This serves as a caution for patient populations at risk for sarcopenia because time-restricted eating could exacerbate muscle loss,” the authors asserted.
Furthermore, previous studies suggest that the loss of lean mass in such studies is positively linked with weight regain.
While a limitation of the work is that self-reported measures of energy or macronutrient or protein intake were not obtained, the authors speculated that the role of protein intake could be linked to the greater loss of lean mass.
“Given the loss of appendicular lean mass in participants in the time-restricted eating arm and previous reports of decreased protein consumption from time-restricted eating, it is possible that protein intake was altered by time-restricted eating in this cohort, and this clearly warrants future study,” they wrote.
Dr. Weiss said the findings underscore that not all weight loss in dieting is beneficial.
“Losing 1 kg of lean mass (is not equal) to a kilogram of fat,” he said. “Indeed, if one loses 0.65 kg of lean mass and only 0.35 kg of fat mass, that is an intervention I’d probably pass on.”
Time-restricted eating is popular, perhaps because it’s easy?
Time-restricted eating has gained popularity in recent years.
The approach “is attractive as a weight-loss option in that it does not require tedious and time-consuming methods such as calorie counting or adherence to complicated diets,” the authors noted. “Indeed, we found that self-reported adherence to the time-restricted eating schedule was high; however, in contrast to our hypothesis, there was no greater weight loss with time-restricted eating compared with the consistent meal timing.”
They explain that the 12 p.m. to 8 p.m. window for eating was chosen because they thought people might find it easier culturally to skip breakfast than dinner, the more social meal.
However, an 8 p.m. cutoff is somewhat late given there is some suggestion that fasting several hours before bedtime is most beneficial, Dr. Weiss noted. So it may be worth examining different time windows.
“I am very intrigued about looking at early time-restricted eating – 6 a.m. to 2 p.m.,” for example, he said. “It is on our list.”
Meanwhile, the study results support previous research showing no effect on weight outcomes in relation to skipping breakfast.
The study received funding from the UCSF cardiology division’s Cardiology Innovations Award Program and the National Institute of Diabetes and Digestive and Kidney Diseases, with additional support from the James Peter Read Foundation. Dr. Weiss has reported nonfinancial support from Mocacare and nonfinancial support from iHealth Labs during the conduct of the study. He also is a cofounder and equity stakeholder of Keyto, and owns stock and was formerly on the board of Virta.
A version of this article originally appeared on Medscape.com.
Psychosocial resilience associated with better cardiovascular health in Blacks
Resilience might deserve targeting
Increased psychosocial resilience, which captures a sense of purpose, optimism, and life-coping strategies, correlates with improved cardiovascular (CV) health in Black Americans, according to a study that might hold a key for identifying new strategies for CV disease prevention.

“Our findings highlight the importance of individual psychosocial factors that promote cardiovascular health among Black adults, traditionally considered to be a high-risk population,” according to a team of authors collaborating on a study produced by the Morehouse-Emory Cardiovascular Center for Health Equity in Atlanta.
Studies associating psychosocial resilience with improved health outcomes have been published before. In a 12-study review of this concept, it was emphasized that resilience is a dynamic process, not a personality trait, and has shown promise as a target of efforts to relieve the burden of disease (Johnston MC et al. Psychosomatics 2015;56:168-80).
In this study, which received partial support from the American Heart Association, psychosocial resilience was evaluated at both the individual level and at the community level among 389 Black adults living in Atlanta. The senior author was Tené T. Lewis, PhD, of the department of epidemiology at Emory’s Rollins School of Public Health (Circ Cardiovasc Qual Outcomes 2020 Oct 7;13:3006638).
Psychosocial resilience was calculated across the domains of environmental mastery, purpose of life, optimism, coping, and lack of depression with standardized tests, such as the Life Orientation Test-Revised questionnaire for optimism and the Ryff Scales of Psychological Well-Being for the domains of environmental mastery and purpose of life. A composite score for psychosocial resilience was reached by calculating the median score across the measured domains.
Patients with high psychosocial resilience, defined as a composite score above the median, or low resilience, defined as a lower score, were then compared for CV health based on the AHA’s Life’s Simple 7 (LS7) score.
LS7 scores incorporate measures for exercise, diet, smoking history, blood pressure, glucose, cholesterol, and body mass index. Composite LS7 scores range from 0 to 14. Prior work cited by the authors have associated each 1-unit increase in LS7 score with a 13% lower risk of CVD.
As a continuous variable for CV risk at the individual level, each higher standard-deviation increment in the composite psychosocial resilience score was associated with a highly significant 0.42-point increase in LS7 score (P < .001) for study participants. In other words, increasing resilience predicted lower CV risk scores.
Resilience was also calculated at the community level by looking at census tract-level rates of CV mortality and morbidity relative to socioeconomic status. Again, high CV resilience, defined as scores above the median, were compared with lower scores across neighborhoods with similar median household income. As a continuous variable in this analysis, each higher standard-deviation increment in the resilience score was associated with a 0.27-point increase in LS7 score (P = .01).
After adjustment for sociodemographic factors, the association between psychosocial resilience and CV health remained significant for both the individual and community calculations, according to the authors. When examined jointly, high individual psychosocial resilience remained independently associated with improved CV health, but living in a high-resilience neighborhood was not an independent predictor.
When evaluated individually, each of the domains in the psychosocial resistance score were positively correlated with higher LS7 scores, meaning lower CV risk. The strongest associations on a statistical level were low depressive symptoms (P = .001), environmental mastery (P = .006), and purpose in life (P = .009).
The impact of high psychosocial resistance scores was greatest in Black adults living in low-resilience neighborhoods. Among these subjects, high resilience was associated with a nearly 1-point increase in LS7 score relative to low resilience (8.38 vs. 7.42). This was unexpected, but it “is consistent with some broader conceptual literature that posits that individual psychosocial resilience matters more under conditions of adversity,” the authors reported.
Understanding disparities is key
Black race has repeatedly been associated with an increased risk of CV events, but this study is valuable for providing a fresh perspective on the potential reasons, according to the authors of an accompanying editorial, Amber E. Johnson, MD, and Jared Magnani, MD, who are both affiliated with the division of cardiology at the University of Pittsburgh (Circ Cardiovasc Qual Outcomes 2020 Oct 7. doi: 10.1161/CIRCOUTCOMES.120.007357.
“Clinicians increasingly recognize that race-based disparities do not stem inherently from race; instead, the disparities stem from the underlying social determinations of health,” they wrote, citing such variables as unequal access to pay and acceptable living conditions “and the structural racism that perpetuates them.”
They agreed with the authors that promotion of psychosocial resilience among Black people living in communities with poor CV health has the potential to improve CV outcomes, but they warned that this is complex. Although they contend that resilience techniques can be taught, they cautioned there might be limitations if the underlying factors associated with poor psychosocial resilience remain unchanged.
“Thus, the superficial application of positive psychology strategies is likely insufficient to bring parity to CV health outcomes,” they wrote, concluding that strategies to promote health equity would negate the need for interventions to bolster resilience.
Studies that focus on Black adults and cardiovascular health, including this investigation into the role of psychosocial factors “are much needed and very welcome,” said Harlan M. Krumholz, MD, a cardiologist and professor in the Institute for Social and Policy Studies at Yale University, New Haven, Conn.
He sees a broad array of potential directions of research.
“The study opens many questions about whether the resilience can be strengthened by interventions; whether addressing structural racism could reduce the need for such resilience, and whether this association is specific to Black adults in an urban center or is generally present in other settings and in other populations,” Dr. Krumholz said.
An effort is now needed to determine “whether this is a marker or a mediator of cardiovascular health,” he added.
In either case, resilience is a potentially important factor for understanding racial disparities in CV-disease prevalence and outcomes, according to the authors of the accompanying editorial and Dr. Krumholz.
SOURCE: Kim JH et al. Circ Cardiovasc Qual Outcomes. 2020 Oct 7;13:e006638.
Resilience might deserve targeting
Resilience might deserve targeting
Increased psychosocial resilience, which captures a sense of purpose, optimism, and life-coping strategies, correlates with improved cardiovascular (CV) health in Black Americans, according to a study that might hold a key for identifying new strategies for CV disease prevention.
“Our findings highlight the importance of individual psychosocial factors that promote cardiovascular health among Black adults, traditionally considered to be a high-risk population,” according to a team of authors collaborating on a study produced by the Morehouse-Emory Cardiovascular Center for Health Equity in Atlanta.
Studies associating psychosocial resilience with improved health outcomes have been published before. In a 12-study review of this concept, it was emphasized that resilience is a dynamic process, not a personality trait, and has shown promise as a target of efforts to relieve the burden of disease (Johnston MC et al. Psychosomatics 2015;56:168-80).
In this study, which received partial support from the American Heart Association, psychosocial resilience was evaluated at both the individual level and at the community level among 389 Black adults living in Atlanta. The senior author was Tené T. Lewis, PhD, of the department of epidemiology at Emory’s Rollins School of Public Health (Circ Cardiovasc Qual Outcomes 2020 Oct 7;13:3006638).
Psychosocial resilience was calculated across the domains of environmental mastery, purpose of life, optimism, coping, and lack of depression with standardized tests, such as the Life Orientation Test-Revised questionnaire for optimism and the Ryff Scales of Psychological Well-Being for the domains of environmental mastery and purpose of life. A composite score for psychosocial resilience was reached by calculating the median score across the measured domains.
Patients with high psychosocial resilience, defined as a composite score above the median, or low resilience, defined as a lower score, were then compared for CV health based on the AHA’s Life’s Simple 7 (LS7) score.
LS7 scores incorporate measures for exercise, diet, smoking history, blood pressure, glucose, cholesterol, and body mass index. Composite LS7 scores range from 0 to 14. Prior work cited by the authors have associated each 1-unit increase in LS7 score with a 13% lower risk of CVD.
As a continuous variable for CV risk at the individual level, each higher standard-deviation increment in the composite psychosocial resilience score was associated with a highly significant 0.42-point increase in LS7 score (P < .001) for study participants. In other words, increasing resilience predicted lower CV risk scores.
Resilience was also calculated at the community level by looking at census tract-level rates of CV mortality and morbidity relative to socioeconomic status. Again, high CV resilience, defined as scores above the median, were compared with lower scores across neighborhoods with similar median household income. As a continuous variable in this analysis, each higher standard-deviation increment in the resilience score was associated with a 0.27-point increase in LS7 score (P = .01).
After adjustment for sociodemographic factors, the association between psychosocial resilience and CV health remained significant for both the individual and community calculations, according to the authors. When examined jointly, high individual psychosocial resilience remained independently associated with improved CV health, but living in a high-resilience neighborhood was not an independent predictor.
When evaluated individually, each of the domains in the psychosocial resistance score were positively correlated with higher LS7 scores, meaning lower CV risk. The strongest associations on a statistical level were low depressive symptoms (P = .001), environmental mastery (P = .006), and purpose in life (P = .009).
The impact of high psychosocial resistance scores was greatest in Black adults living in low-resilience neighborhoods. Among these subjects, high resilience was associated with a nearly 1-point increase in LS7 score relative to low resilience (8.38 vs. 7.42). This was unexpected, but it “is consistent with some broader conceptual literature that posits that individual psychosocial resilience matters more under conditions of adversity,” the authors reported.
Understanding disparities is key
Black race has repeatedly been associated with an increased risk of CV events, but this study is valuable for providing a fresh perspective on the potential reasons, according to the authors of an accompanying editorial, Amber E. Johnson, MD, and Jared Magnani, MD, who are both affiliated with the division of cardiology at the University of Pittsburgh (Circ Cardiovasc Qual Outcomes 2020 Oct 7. doi: 10.1161/CIRCOUTCOMES.120.007357.
“Clinicians increasingly recognize that race-based disparities do not stem inherently from race; instead, the disparities stem from the underlying social determinations of health,” they wrote, citing such variables as unequal access to pay and acceptable living conditions “and the structural racism that perpetuates them.”
They agreed with the authors that promotion of psychosocial resilience among Black people living in communities with poor CV health has the potential to improve CV outcomes, but they warned that this is complex. Although they contend that resilience techniques can be taught, they cautioned there might be limitations if the underlying factors associated with poor psychosocial resilience remain unchanged.
“Thus, the superficial application of positive psychology strategies is likely insufficient to bring parity to CV health outcomes,” they wrote, concluding that strategies to promote health equity would negate the need for interventions to bolster resilience.
Studies that focus on Black adults and cardiovascular health, including this investigation into the role of psychosocial factors “are much needed and very welcome,” said Harlan M. Krumholz, MD, a cardiologist and professor in the Institute for Social and Policy Studies at Yale University, New Haven, Conn.
He sees a broad array of potential directions of research.
“The study opens many questions about whether the resilience can be strengthened by interventions; whether addressing structural racism could reduce the need for such resilience, and whether this association is specific to Black adults in an urban center or is generally present in other settings and in other populations,” Dr. Krumholz said.
An effort is now needed to determine “whether this is a marker or a mediator of cardiovascular health,” he added.
In either case, resilience is a potentially important factor for understanding racial disparities in CV-disease prevalence and outcomes, according to the authors of the accompanying editorial and Dr. Krumholz.
SOURCE: Kim JH et al. Circ Cardiovasc Qual Outcomes. 2020 Oct 7;13:e006638.
Increased psychosocial resilience, which captures a sense of purpose, optimism, and life-coping strategies, correlates with improved cardiovascular (CV) health in Black Americans, according to a study that might hold a key for identifying new strategies for CV disease prevention.
“Our findings highlight the importance of individual psychosocial factors that promote cardiovascular health among Black adults, traditionally considered to be a high-risk population,” according to a team of authors collaborating on a study produced by the Morehouse-Emory Cardiovascular Center for Health Equity in Atlanta.
Studies associating psychosocial resilience with improved health outcomes have been published before. In a 12-study review of this concept, it was emphasized that resilience is a dynamic process, not a personality trait, and has shown promise as a target of efforts to relieve the burden of disease (Johnston MC et al. Psychosomatics 2015;56:168-80).
In this study, which received partial support from the American Heart Association, psychosocial resilience was evaluated at both the individual level and at the community level among 389 Black adults living in Atlanta. The senior author was Tené T. Lewis, PhD, of the department of epidemiology at Emory’s Rollins School of Public Health (Circ Cardiovasc Qual Outcomes 2020 Oct 7;13:3006638).
Psychosocial resilience was calculated across the domains of environmental mastery, purpose of life, optimism, coping, and lack of depression with standardized tests, such as the Life Orientation Test-Revised questionnaire for optimism and the Ryff Scales of Psychological Well-Being for the domains of environmental mastery and purpose of life. A composite score for psychosocial resilience was reached by calculating the median score across the measured domains.
Patients with high psychosocial resilience, defined as a composite score above the median, or low resilience, defined as a lower score, were then compared for CV health based on the AHA’s Life’s Simple 7 (LS7) score.
LS7 scores incorporate measures for exercise, diet, smoking history, blood pressure, glucose, cholesterol, and body mass index. Composite LS7 scores range from 0 to 14. Prior work cited by the authors have associated each 1-unit increase in LS7 score with a 13% lower risk of CVD.
As a continuous variable for CV risk at the individual level, each higher standard-deviation increment in the composite psychosocial resilience score was associated with a highly significant 0.42-point increase in LS7 score (P < .001) for study participants. In other words, increasing resilience predicted lower CV risk scores.
Resilience was also calculated at the community level by looking at census tract-level rates of CV mortality and morbidity relative to socioeconomic status. Again, high CV resilience, defined as scores above the median, were compared with lower scores across neighborhoods with similar median household income. As a continuous variable in this analysis, each higher standard-deviation increment in the resilience score was associated with a 0.27-point increase in LS7 score (P = .01).
After adjustment for sociodemographic factors, the association between psychosocial resilience and CV health remained significant for both the individual and community calculations, according to the authors. When examined jointly, high individual psychosocial resilience remained independently associated with improved CV health, but living in a high-resilience neighborhood was not an independent predictor.
When evaluated individually, each of the domains in the psychosocial resistance score were positively correlated with higher LS7 scores, meaning lower CV risk. The strongest associations on a statistical level were low depressive symptoms (P = .001), environmental mastery (P = .006), and purpose in life (P = .009).
The impact of high psychosocial resistance scores was greatest in Black adults living in low-resilience neighborhoods. Among these subjects, high resilience was associated with a nearly 1-point increase in LS7 score relative to low resilience (8.38 vs. 7.42). This was unexpected, but it “is consistent with some broader conceptual literature that posits that individual psychosocial resilience matters more under conditions of adversity,” the authors reported.
Understanding disparities is key
Black race has repeatedly been associated with an increased risk of CV events, but this study is valuable for providing a fresh perspective on the potential reasons, according to the authors of an accompanying editorial, Amber E. Johnson, MD, and Jared Magnani, MD, who are both affiliated with the division of cardiology at the University of Pittsburgh (Circ Cardiovasc Qual Outcomes 2020 Oct 7. doi: 10.1161/CIRCOUTCOMES.120.007357.
“Clinicians increasingly recognize that race-based disparities do not stem inherently from race; instead, the disparities stem from the underlying social determinations of health,” they wrote, citing such variables as unequal access to pay and acceptable living conditions “and the structural racism that perpetuates them.”
They agreed with the authors that promotion of psychosocial resilience among Black people living in communities with poor CV health has the potential to improve CV outcomes, but they warned that this is complex. Although they contend that resilience techniques can be taught, they cautioned there might be limitations if the underlying factors associated with poor psychosocial resilience remain unchanged.
“Thus, the superficial application of positive psychology strategies is likely insufficient to bring parity to CV health outcomes,” they wrote, concluding that strategies to promote health equity would negate the need for interventions to bolster resilience.
Studies that focus on Black adults and cardiovascular health, including this investigation into the role of psychosocial factors “are much needed and very welcome,” said Harlan M. Krumholz, MD, a cardiologist and professor in the Institute for Social and Policy Studies at Yale University, New Haven, Conn.
He sees a broad array of potential directions of research.
“The study opens many questions about whether the resilience can be strengthened by interventions; whether addressing structural racism could reduce the need for such resilience, and whether this association is specific to Black adults in an urban center or is generally present in other settings and in other populations,” Dr. Krumholz said.
An effort is now needed to determine “whether this is a marker or a mediator of cardiovascular health,” he added.
In either case, resilience is a potentially important factor for understanding racial disparities in CV-disease prevalence and outcomes, according to the authors of the accompanying editorial and Dr. Krumholz.
SOURCE: Kim JH et al. Circ Cardiovasc Qual Outcomes. 2020 Oct 7;13:e006638.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
EMPEROR-Reduced: Empagliflozin’s HFrEF benefit holds steady on top of sacubitril/valsartan
The latest drug shown to benefit patients with heart failure with reduced ejection fraction, the SGLT2 inhibitor empagliflozin, works just as well when added on top of a second major agent used to treat these patients, the renin-angiotensin system–inhibiting combination of sacubitril/valsartan, based on a post-hoc analysis of data from the EMPEROR-Reduced trial.

“When there are two very effective treatments, it’s common for people to ask: Which should I use?’ The goal of my presentation was to emphasize that the answer is both. We shouldn’t choose between neprilysin inhibition [sacubitril inhibits the enzyme neprilysin] and SGLT2 [sodium-glucose transporter 2] inhibition; we should use both,” said Milton Packer, MD at the virtual annual meeting of the Heart Failure Society of America.
EMPEROR-Reduced had the primary goal of testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in patients with heart failure with reduced ejection fraction (HFrEF). The results showed that adding this drug on top of standard treatments led to a 25% relative cut in the study’s primary efficacy endpoint, compared with placebo, and had this effect regardless of whether or not patients also had type 2 diabetes (N Engl J Med. 2020 Aug 29. doi: 10.1056/NEJMoa2022190).
Among the 3,730 patients enrolled in the trial, 727 (19%) were on sacubitril/valsartan (Entresto) at entry, which gave Dr. Packer the data to perform the analysis he reported. He presented the study’s three major endpoints as well as a quality of life analysis that compared the performance of empagliflozin in patients who were on sacubitril/valsartan at baseline with the other study patients, who were either on a different type of renin-angiotensin system (RAS) blocker (roughly 70% of study patients) or on no RAS inhibition (about 10% of patients).
The results showed no statistically significant indication of an interaction, suggesting that patients with sacubitril/valsartan on board had just as good response to empagliflozin as patients who were not on this combination. The landmark PARADIGM-HF trial proved several years ago that treatment of HFrEF patients with sacubitril/valsartan led to significantly better outcomes than did treatment with another form of RAS inhibition (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
For example, EMPEROR-Reduced’s primary endpoint, the combined rate of cardiovascular death or hospitalization for heart failure, fell by 36% relative to placebo in patients who received empagliflozin on top of sacubitril/valsartan, and by 23% relative to placebo among the remaining patients who received empagliflozin on top of a different type of RAS inhibitor drug or no RAS inhibition.
“Background treatment with sacubitril/valsartan did not diminish, and may have enhanced the efficacy of empagliflozin,” concluded Dr. Packer. Further analyses also showed that concurrent sacubitril/valsartan had no statistically significant impact on empagliflozin’s ability to reduce the rate of total heart failure hospitalizations, or to slow progressive loss of renal function, compared with placebo. The fourth efficacy analysis Dr. Packer presented showed that empagliflozin was also as effective for improving a quality-of-life measure in patients compared with placebo regardless of the type of RAS inhibition used. For all four outcomes, the point-estimate of empagliflozin’s benefit was higher when used along with sacubitril/valsartan.
Brian L. Claggett, PhD, a biostatistician at Brigham and Women’s Hospital and Harvard Medical School in Boston, designated discussant for the report, disagreed with Dr. Packer’s suggestion that the efficacy of empagliflozin may have been greater when administered against a background of sacubitril/valsartan. From a statistical perspective, there is no basis to suggest that patients did better when they were on both drugs, he cautioned. But Dr. Claggett acknowledged that the new analyses suggested that empagliflozin’s benefit wasn’t compromised by concurrent sacubitril/valsartan use. He also highlighted the value of more fully documenting the safety and efficacy of a new drug when used as part of “comprehensive therapy” with the established drugs that a patient may concurrently receive.
Dr. Packer also presented several measures of treatment safety that all showed similar rates of adverse effects between the empagliflozin and placebo recipients regardless of background RAS inhibition. A notable finding was that the incidence of hypokalemia was 5.9% in patients on empagliflozin and sacubitril/valsartan and 7.5% among patients on empagliflozin and a different type of RAS inhibition.
EMPEROR-Reduced was funded by Boehringer Ingelheim and Eli Lilly, the companies that market empagliflozin. Dr. Packer has received personal fees from Boehringer Ingelheim and Eli Lilly and from several other companies. Dr. Claggett has been a consultant to Amgen, AO Biome, Biogen, Corvia, Myokardia, and Novartis.
The latest drug shown to benefit patients with heart failure with reduced ejection fraction, the SGLT2 inhibitor empagliflozin, works just as well when added on top of a second major agent used to treat these patients, the renin-angiotensin system–inhibiting combination of sacubitril/valsartan, based on a post-hoc analysis of data from the EMPEROR-Reduced trial.
“When there are two very effective treatments, it’s common for people to ask: Which should I use?’ The goal of my presentation was to emphasize that the answer is both. We shouldn’t choose between neprilysin inhibition [sacubitril inhibits the enzyme neprilysin] and SGLT2 [sodium-glucose transporter 2] inhibition; we should use both,” said Milton Packer, MD at the virtual annual meeting of the Heart Failure Society of America.
EMPEROR-Reduced had the primary goal of testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in patients with heart failure with reduced ejection fraction (HFrEF). The results showed that adding this drug on top of standard treatments led to a 25% relative cut in the study’s primary efficacy endpoint, compared with placebo, and had this effect regardless of whether or not patients also had type 2 diabetes (N Engl J Med. 2020 Aug 29. doi: 10.1056/NEJMoa2022190).
Among the 3,730 patients enrolled in the trial, 727 (19%) were on sacubitril/valsartan (Entresto) at entry, which gave Dr. Packer the data to perform the analysis he reported. He presented the study’s three major endpoints as well as a quality of life analysis that compared the performance of empagliflozin in patients who were on sacubitril/valsartan at baseline with the other study patients, who were either on a different type of renin-angiotensin system (RAS) blocker (roughly 70% of study patients) or on no RAS inhibition (about 10% of patients).
The results showed no statistically significant indication of an interaction, suggesting that patients with sacubitril/valsartan on board had just as good response to empagliflozin as patients who were not on this combination. The landmark PARADIGM-HF trial proved several years ago that treatment of HFrEF patients with sacubitril/valsartan led to significantly better outcomes than did treatment with another form of RAS inhibition (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
For example, EMPEROR-Reduced’s primary endpoint, the combined rate of cardiovascular death or hospitalization for heart failure, fell by 36% relative to placebo in patients who received empagliflozin on top of sacubitril/valsartan, and by 23% relative to placebo among the remaining patients who received empagliflozin on top of a different type of RAS inhibitor drug or no RAS inhibition.
“Background treatment with sacubitril/valsartan did not diminish, and may have enhanced the efficacy of empagliflozin,” concluded Dr. Packer. Further analyses also showed that concurrent sacubitril/valsartan had no statistically significant impact on empagliflozin’s ability to reduce the rate of total heart failure hospitalizations, or to slow progressive loss of renal function, compared with placebo. The fourth efficacy analysis Dr. Packer presented showed that empagliflozin was also as effective for improving a quality-of-life measure in patients compared with placebo regardless of the type of RAS inhibition used. For all four outcomes, the point-estimate of empagliflozin’s benefit was higher when used along with sacubitril/valsartan.
Brian L. Claggett, PhD, a biostatistician at Brigham and Women’s Hospital and Harvard Medical School in Boston, designated discussant for the report, disagreed with Dr. Packer’s suggestion that the efficacy of empagliflozin may have been greater when administered against a background of sacubitril/valsartan. From a statistical perspective, there is no basis to suggest that patients did better when they were on both drugs, he cautioned. But Dr. Claggett acknowledged that the new analyses suggested that empagliflozin’s benefit wasn’t compromised by concurrent sacubitril/valsartan use. He also highlighted the value of more fully documenting the safety and efficacy of a new drug when used as part of “comprehensive therapy” with the established drugs that a patient may concurrently receive.
Dr. Packer also presented several measures of treatment safety that all showed similar rates of adverse effects between the empagliflozin and placebo recipients regardless of background RAS inhibition. A notable finding was that the incidence of hypokalemia was 5.9% in patients on empagliflozin and sacubitril/valsartan and 7.5% among patients on empagliflozin and a different type of RAS inhibition.
EMPEROR-Reduced was funded by Boehringer Ingelheim and Eli Lilly, the companies that market empagliflozin. Dr. Packer has received personal fees from Boehringer Ingelheim and Eli Lilly and from several other companies. Dr. Claggett has been a consultant to Amgen, AO Biome, Biogen, Corvia, Myokardia, and Novartis.
The latest drug shown to benefit patients with heart failure with reduced ejection fraction, the SGLT2 inhibitor empagliflozin, works just as well when added on top of a second major agent used to treat these patients, the renin-angiotensin system–inhibiting combination of sacubitril/valsartan, based on a post-hoc analysis of data from the EMPEROR-Reduced trial.
“When there are two very effective treatments, it’s common for people to ask: Which should I use?’ The goal of my presentation was to emphasize that the answer is both. We shouldn’t choose between neprilysin inhibition [sacubitril inhibits the enzyme neprilysin] and SGLT2 [sodium-glucose transporter 2] inhibition; we should use both,” said Milton Packer, MD at the virtual annual meeting of the Heart Failure Society of America.
EMPEROR-Reduced had the primary goal of testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in patients with heart failure with reduced ejection fraction (HFrEF). The results showed that adding this drug on top of standard treatments led to a 25% relative cut in the study’s primary efficacy endpoint, compared with placebo, and had this effect regardless of whether or not patients also had type 2 diabetes (N Engl J Med. 2020 Aug 29. doi: 10.1056/NEJMoa2022190).
Among the 3,730 patients enrolled in the trial, 727 (19%) were on sacubitril/valsartan (Entresto) at entry, which gave Dr. Packer the data to perform the analysis he reported. He presented the study’s three major endpoints as well as a quality of life analysis that compared the performance of empagliflozin in patients who were on sacubitril/valsartan at baseline with the other study patients, who were either on a different type of renin-angiotensin system (RAS) blocker (roughly 70% of study patients) or on no RAS inhibition (about 10% of patients).
The results showed no statistically significant indication of an interaction, suggesting that patients with sacubitril/valsartan on board had just as good response to empagliflozin as patients who were not on this combination. The landmark PARADIGM-HF trial proved several years ago that treatment of HFrEF patients with sacubitril/valsartan led to significantly better outcomes than did treatment with another form of RAS inhibition (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
For example, EMPEROR-Reduced’s primary endpoint, the combined rate of cardiovascular death or hospitalization for heart failure, fell by 36% relative to placebo in patients who received empagliflozin on top of sacubitril/valsartan, and by 23% relative to placebo among the remaining patients who received empagliflozin on top of a different type of RAS inhibitor drug or no RAS inhibition.
“Background treatment with sacubitril/valsartan did not diminish, and may have enhanced the efficacy of empagliflozin,” concluded Dr. Packer. Further analyses also showed that concurrent sacubitril/valsartan had no statistically significant impact on empagliflozin’s ability to reduce the rate of total heart failure hospitalizations, or to slow progressive loss of renal function, compared with placebo. The fourth efficacy analysis Dr. Packer presented showed that empagliflozin was also as effective for improving a quality-of-life measure in patients compared with placebo regardless of the type of RAS inhibition used. For all four outcomes, the point-estimate of empagliflozin’s benefit was higher when used along with sacubitril/valsartan.
Brian L. Claggett, PhD, a biostatistician at Brigham and Women’s Hospital and Harvard Medical School in Boston, designated discussant for the report, disagreed with Dr. Packer’s suggestion that the efficacy of empagliflozin may have been greater when administered against a background of sacubitril/valsartan. From a statistical perspective, there is no basis to suggest that patients did better when they were on both drugs, he cautioned. But Dr. Claggett acknowledged that the new analyses suggested that empagliflozin’s benefit wasn’t compromised by concurrent sacubitril/valsartan use. He also highlighted the value of more fully documenting the safety and efficacy of a new drug when used as part of “comprehensive therapy” with the established drugs that a patient may concurrently receive.
Dr. Packer also presented several measures of treatment safety that all showed similar rates of adverse effects between the empagliflozin and placebo recipients regardless of background RAS inhibition. A notable finding was that the incidence of hypokalemia was 5.9% in patients on empagliflozin and sacubitril/valsartan and 7.5% among patients on empagliflozin and a different type of RAS inhibition.
EMPEROR-Reduced was funded by Boehringer Ingelheim and Eli Lilly, the companies that market empagliflozin. Dr. Packer has received personal fees from Boehringer Ingelheim and Eli Lilly and from several other companies. Dr. Claggett has been a consultant to Amgen, AO Biome, Biogen, Corvia, Myokardia, and Novartis.
FROM HFSA 2020
Music’s charms may soothe heart failure’s effects
Music listening and singing each showed early, promising evidence for producing cardiovascular benefits, part of a burgeoning area of research that is exploring and documenting ways to effectively use music to improve health.

A study run at four centers in Italy randomized 159 patients with heart failure, primarily New York Heart Association class I or II disease, to either a daily regimen of at least 30 minutes spent listening to music daily or to a control group that received usual care with no music prescription. After 3 months, the 82 patients in the daily music-listening group had a statistically significant improvement in their Minnesota Living with Heart Failure Questionnaire scores, compared with 77 controls for the study’s primary outcome measure. The results also showed significant benefits, compared with placebo, for other, secondary efficacy measures including improvements in anxiety, depression, sleep quality, and cognition.
Although the results are considered preliminary, they drew significant attention when published in July 2020 (J Card Fail. 2020 Jul 1;26[7]:541-9), where it was accompanied by two editorials in the same issue as well as an editor’s statement. All these commentators as well as other experts interested in music as medicine gathered to further discuss the topic during a panel session at the virtual annual meeting of the Heart Failure Society of America.
Music as a calming influence
The source of the primary benefits seen in this Italian study likely involved “emotional, psychological, and relaxation,” suggested Jerome L. Fleg, MD, program officer for clinical cardiovascular disease at the National Heart, Lung, and Blood Institute in Bethesda, Md. Researchers had used calming potential as a major criterion when selecting the 80 classical pieces that the heart failure patients in the intervention arm of the study could shuffle on their play lists.
“The tempo/rhythm was set up in a range between 60 and 80 beats per minute, because this range mirrors the human heart rate and facilitates relaxation,” the investigators said in their published report. Unfortunately, noted Dr. Fleg, the study lacked physiologic and biomarker measurements that could have provided objective evidence of effects from music. And the study failed to include a control arm of patients instructed to spend 30 minutes a day resting and relaxing without instruction to listen to music, he noted.
Dr. Fleg had authored one of the July editorials, where he said “It is hoped that findings from these studies and others can expand the scientific evidence for music-based interventions and bring these therapies into clinical practice. The current study from Burrai et al. is a positive step in this direction for patients with heart failure.” (J Card Fail. 2020 Jul 1;26[7]: 550-1). What’s needed now, he added during the virtual session, are “more objective data” to better and more comprehensively document the benefits from a music-based intervention in patients with heart failure.
An add-on to standard care
The findings in heart failure patients follows a growing literature that’s shown music can generate a restful state by doing things like activating autonomic parasympathetic outflow while dampening sympathetic outflow. This produces moderation in mood and emotion as well as depressed heart rate, lowered blood pressure, and slowed respiration, commented Emmeline Edwards, PhD director of the division of extramural research of the National Center for Complementary and Integrative Health in Bethesda, Md. Music also seems able to stimulate higher-order brain regions that can result in reduced psychological stress, anxiety, and depression.
“It’s a promising protective intervention to add to standard care for cardiac patients,” Dr. Edwards said during the virtual session. “Music is part of the toolbox for managing symptoms and improving health and well-being.”
“Music is not a substitute for standard therapy, but could add to it,” declared Dr. Fleg.
The already-established intervention known as music therapy has identified music’s ability to modulate breathing as an important mediator of music’s effect.
“Breathing is one of the few physiological processes that can be voluntarily controlled making it a viable target for intervention,” noted opera soprano Renée Fleming and Sheri L. Robb, PhD, in the second editorial that accompanied the Italian heart failure report (J Card Fail. 2020 Jul 1;26[7]:552-4). The music-listening intervention “may have had more effect if they had used compositional features [of the music] to teach patients how to structure their breathing,” said Dr. Robb, a music therapist at Indiana University–Purdue University Indianapolis, during the virtual session.
Another variable to consider is the type of music. “What is the emotional response to the music, and how does that affect heart rate,” wondered Dr. Robb, a professor at the Indiana University School of Nursing in Indianapolis.
Music as exercise
The division that Dr. Edwards directs recently funded a pilot study that assessed the feasibility of using music to stimulate activity and improve breathing another way, by repurposing singing as a novel form of rehabilitative exercise.
The pilot study enrolled patients with coronary disease into a randomized study that tested whether a 14-minute session of supervised singing could produce acute improvement in vascular function, “a biomarker for the risk of future cardiovascular disease events,” explained Jacqueline P. Kulinski, MD, a preventive cardiologist at the Medical College of Wisconsin in Milwaukee. Dr. Kulinski did not report details of her yet-unpublished study, but said that her initial findings held promise for developing musical activities such as singing as a novel way to stimulate therapeutic physical activity in patients with heart disease.
“It’s exciting to see this signal” of benefit. “I envision music therapy as a part of cardiac rehabilitation, or an alternative for patients who can’t participate in traditional rehab,” Dr. Kulinski said during the virtual session. “I think of singing as a physical activity, as exercise, and using this exercise as medicine.”
Harmonizing with the NIH
“Singing is like swimming: You need to hold your breath,” agreed Ms. Fleming, who participated on the virtual panel and has spearheaded a collaboration between the National Institutes of Health and the Kennedy Center for the Performing Arts, the Sound Health Initiative, that’s coordinating research into the connections between music and health. Ms. Fleming helped launch the Sound Health Initiative in 2017 by coauthoring a JAMA article with the NIH director that spelled out the rationale and goals of the project (JAMA. 2017 Jun 27;317[24]:2470-1), and by launching a lecture tour on the topic in a presentation she calls Music and the Mind.

Ms. Fleming has given her talk in more than 30 locations worldwide, and she’s found that “audiences love” the combination of neuroscience and music that her talks cover, she said. Her lectures highlight that, in addition to cardiovascular disease, the potential for music therapy and related interventions has been shown in patients with disorders that include autism, psychosis, pain, Parkinson’s disease, Alzheimer’s disease, and epilepsy.
The research highlighted in the session “opens new doors to prevention and treatment strategies using music for patients with heart failure and cardiovascular disease,” summed up Biykem Bozkurt, MD, professor of medicine at the Baylor College of Medicine in Houston and president of the Heart Failure Society of America, who helped organize the virtual session.
Dr. Fleg, Dr. Edwards, Dr. Robb, Dr Kulinski, Ms. Fleming, and Dr. Bozkurt had no relevant financial disclosures.
Music listening and singing each showed early, promising evidence for producing cardiovascular benefits, part of a burgeoning area of research that is exploring and documenting ways to effectively use music to improve health.
A study run at four centers in Italy randomized 159 patients with heart failure, primarily New York Heart Association class I or II disease, to either a daily regimen of at least 30 minutes spent listening to music daily or to a control group that received usual care with no music prescription. After 3 months, the 82 patients in the daily music-listening group had a statistically significant improvement in their Minnesota Living with Heart Failure Questionnaire scores, compared with 77 controls for the study’s primary outcome measure. The results also showed significant benefits, compared with placebo, for other, secondary efficacy measures including improvements in anxiety, depression, sleep quality, and cognition.
Although the results are considered preliminary, they drew significant attention when published in July 2020 (J Card Fail. 2020 Jul 1;26[7]:541-9), where it was accompanied by two editorials in the same issue as well as an editor’s statement. All these commentators as well as other experts interested in music as medicine gathered to further discuss the topic during a panel session at the virtual annual meeting of the Heart Failure Society of America.
Music as a calming influence
The source of the primary benefits seen in this Italian study likely involved “emotional, psychological, and relaxation,” suggested Jerome L. Fleg, MD, program officer for clinical cardiovascular disease at the National Heart, Lung, and Blood Institute in Bethesda, Md. Researchers had used calming potential as a major criterion when selecting the 80 classical pieces that the heart failure patients in the intervention arm of the study could shuffle on their play lists.
“The tempo/rhythm was set up in a range between 60 and 80 beats per minute, because this range mirrors the human heart rate and facilitates relaxation,” the investigators said in their published report. Unfortunately, noted Dr. Fleg, the study lacked physiologic and biomarker measurements that could have provided objective evidence of effects from music. And the study failed to include a control arm of patients instructed to spend 30 minutes a day resting and relaxing without instruction to listen to music, he noted.
Dr. Fleg had authored one of the July editorials, where he said “It is hoped that findings from these studies and others can expand the scientific evidence for music-based interventions and bring these therapies into clinical practice. The current study from Burrai et al. is a positive step in this direction for patients with heart failure.” (J Card Fail. 2020 Jul 1;26[7]: 550-1). What’s needed now, he added during the virtual session, are “more objective data” to better and more comprehensively document the benefits from a music-based intervention in patients with heart failure.
An add-on to standard care
The findings in heart failure patients follows a growing literature that’s shown music can generate a restful state by doing things like activating autonomic parasympathetic outflow while dampening sympathetic outflow. This produces moderation in mood and emotion as well as depressed heart rate, lowered blood pressure, and slowed respiration, commented Emmeline Edwards, PhD director of the division of extramural research of the National Center for Complementary and Integrative Health in Bethesda, Md. Music also seems able to stimulate higher-order brain regions that can result in reduced psychological stress, anxiety, and depression.
“It’s a promising protective intervention to add to standard care for cardiac patients,” Dr. Edwards said during the virtual session. “Music is part of the toolbox for managing symptoms and improving health and well-being.”
“Music is not a substitute for standard therapy, but could add to it,” declared Dr. Fleg.
The already-established intervention known as music therapy has identified music’s ability to modulate breathing as an important mediator of music’s effect.
“Breathing is one of the few physiological processes that can be voluntarily controlled making it a viable target for intervention,” noted opera soprano Renée Fleming and Sheri L. Robb, PhD, in the second editorial that accompanied the Italian heart failure report (J Card Fail. 2020 Jul 1;26[7]:552-4). The music-listening intervention “may have had more effect if they had used compositional features [of the music] to teach patients how to structure their breathing,” said Dr. Robb, a music therapist at Indiana University–Purdue University Indianapolis, during the virtual session.
Another variable to consider is the type of music. “What is the emotional response to the music, and how does that affect heart rate,” wondered Dr. Robb, a professor at the Indiana University School of Nursing in Indianapolis.
Music as exercise
The division that Dr. Edwards directs recently funded a pilot study that assessed the feasibility of using music to stimulate activity and improve breathing another way, by repurposing singing as a novel form of rehabilitative exercise.
The pilot study enrolled patients with coronary disease into a randomized study that tested whether a 14-minute session of supervised singing could produce acute improvement in vascular function, “a biomarker for the risk of future cardiovascular disease events,” explained Jacqueline P. Kulinski, MD, a preventive cardiologist at the Medical College of Wisconsin in Milwaukee. Dr. Kulinski did not report details of her yet-unpublished study, but said that her initial findings held promise for developing musical activities such as singing as a novel way to stimulate therapeutic physical activity in patients with heart disease.
“It’s exciting to see this signal” of benefit. “I envision music therapy as a part of cardiac rehabilitation, or an alternative for patients who can’t participate in traditional rehab,” Dr. Kulinski said during the virtual session. “I think of singing as a physical activity, as exercise, and using this exercise as medicine.”
Harmonizing with the NIH
“Singing is like swimming: You need to hold your breath,” agreed Ms. Fleming, who participated on the virtual panel and has spearheaded a collaboration between the National Institutes of Health and the Kennedy Center for the Performing Arts, the Sound Health Initiative, that’s coordinating research into the connections between music and health. Ms. Fleming helped launch the Sound Health Initiative in 2017 by coauthoring a JAMA article with the NIH director that spelled out the rationale and goals of the project (JAMA. 2017 Jun 27;317[24]:2470-1), and by launching a lecture tour on the topic in a presentation she calls Music and the Mind.
Ms. Fleming has given her talk in more than 30 locations worldwide, and she’s found that “audiences love” the combination of neuroscience and music that her talks cover, she said. Her lectures highlight that, in addition to cardiovascular disease, the potential for music therapy and related interventions has been shown in patients with disorders that include autism, psychosis, pain, Parkinson’s disease, Alzheimer’s disease, and epilepsy.
The research highlighted in the session “opens new doors to prevention and treatment strategies using music for patients with heart failure and cardiovascular disease,” summed up Biykem Bozkurt, MD, professor of medicine at the Baylor College of Medicine in Houston and president of the Heart Failure Society of America, who helped organize the virtual session.
Dr. Fleg, Dr. Edwards, Dr. Robb, Dr Kulinski, Ms. Fleming, and Dr. Bozkurt had no relevant financial disclosures.
Music listening and singing each showed early, promising evidence for producing cardiovascular benefits, part of a burgeoning area of research that is exploring and documenting ways to effectively use music to improve health.
A study run at four centers in Italy randomized 159 patients with heart failure, primarily New York Heart Association class I or II disease, to either a daily regimen of at least 30 minutes spent listening to music daily or to a control group that received usual care with no music prescription. After 3 months, the 82 patients in the daily music-listening group had a statistically significant improvement in their Minnesota Living with Heart Failure Questionnaire scores, compared with 77 controls for the study’s primary outcome measure. The results also showed significant benefits, compared with placebo, for other, secondary efficacy measures including improvements in anxiety, depression, sleep quality, and cognition.
Although the results are considered preliminary, they drew significant attention when published in July 2020 (J Card Fail. 2020 Jul 1;26[7]:541-9), where it was accompanied by two editorials in the same issue as well as an editor’s statement. All these commentators as well as other experts interested in music as medicine gathered to further discuss the topic during a panel session at the virtual annual meeting of the Heart Failure Society of America.
Music as a calming influence
The source of the primary benefits seen in this Italian study likely involved “emotional, psychological, and relaxation,” suggested Jerome L. Fleg, MD, program officer for clinical cardiovascular disease at the National Heart, Lung, and Blood Institute in Bethesda, Md. Researchers had used calming potential as a major criterion when selecting the 80 classical pieces that the heart failure patients in the intervention arm of the study could shuffle on their play lists.
“The tempo/rhythm was set up in a range between 60 and 80 beats per minute, because this range mirrors the human heart rate and facilitates relaxation,” the investigators said in their published report. Unfortunately, noted Dr. Fleg, the study lacked physiologic and biomarker measurements that could have provided objective evidence of effects from music. And the study failed to include a control arm of patients instructed to spend 30 minutes a day resting and relaxing without instruction to listen to music, he noted.
Dr. Fleg had authored one of the July editorials, where he said “It is hoped that findings from these studies and others can expand the scientific evidence for music-based interventions and bring these therapies into clinical practice. The current study from Burrai et al. is a positive step in this direction for patients with heart failure.” (J Card Fail. 2020 Jul 1;26[7]: 550-1). What’s needed now, he added during the virtual session, are “more objective data” to better and more comprehensively document the benefits from a music-based intervention in patients with heart failure.
An add-on to standard care
The findings in heart failure patients follows a growing literature that’s shown music can generate a restful state by doing things like activating autonomic parasympathetic outflow while dampening sympathetic outflow. This produces moderation in mood and emotion as well as depressed heart rate, lowered blood pressure, and slowed respiration, commented Emmeline Edwards, PhD director of the division of extramural research of the National Center for Complementary and Integrative Health in Bethesda, Md. Music also seems able to stimulate higher-order brain regions that can result in reduced psychological stress, anxiety, and depression.
“It’s a promising protective intervention to add to standard care for cardiac patients,” Dr. Edwards said during the virtual session. “Music is part of the toolbox for managing symptoms and improving health and well-being.”
“Music is not a substitute for standard therapy, but could add to it,” declared Dr. Fleg.
The already-established intervention known as music therapy has identified music’s ability to modulate breathing as an important mediator of music’s effect.
“Breathing is one of the few physiological processes that can be voluntarily controlled making it a viable target for intervention,” noted opera soprano Renée Fleming and Sheri L. Robb, PhD, in the second editorial that accompanied the Italian heart failure report (J Card Fail. 2020 Jul 1;26[7]:552-4). The music-listening intervention “may have had more effect if they had used compositional features [of the music] to teach patients how to structure their breathing,” said Dr. Robb, a music therapist at Indiana University–Purdue University Indianapolis, during the virtual session.
Another variable to consider is the type of music. “What is the emotional response to the music, and how does that affect heart rate,” wondered Dr. Robb, a professor at the Indiana University School of Nursing in Indianapolis.
Music as exercise
The division that Dr. Edwards directs recently funded a pilot study that assessed the feasibility of using music to stimulate activity and improve breathing another way, by repurposing singing as a novel form of rehabilitative exercise.
The pilot study enrolled patients with coronary disease into a randomized study that tested whether a 14-minute session of supervised singing could produce acute improvement in vascular function, “a biomarker for the risk of future cardiovascular disease events,” explained Jacqueline P. Kulinski, MD, a preventive cardiologist at the Medical College of Wisconsin in Milwaukee. Dr. Kulinski did not report details of her yet-unpublished study, but said that her initial findings held promise for developing musical activities such as singing as a novel way to stimulate therapeutic physical activity in patients with heart disease.
“It’s exciting to see this signal” of benefit. “I envision music therapy as a part of cardiac rehabilitation, or an alternative for patients who can’t participate in traditional rehab,” Dr. Kulinski said during the virtual session. “I think of singing as a physical activity, as exercise, and using this exercise as medicine.”
Harmonizing with the NIH
“Singing is like swimming: You need to hold your breath,” agreed Ms. Fleming, who participated on the virtual panel and has spearheaded a collaboration between the National Institutes of Health and the Kennedy Center for the Performing Arts, the Sound Health Initiative, that’s coordinating research into the connections between music and health. Ms. Fleming helped launch the Sound Health Initiative in 2017 by coauthoring a JAMA article with the NIH director that spelled out the rationale and goals of the project (JAMA. 2017 Jun 27;317[24]:2470-1), and by launching a lecture tour on the topic in a presentation she calls Music and the Mind.
Ms. Fleming has given her talk in more than 30 locations worldwide, and she’s found that “audiences love” the combination of neuroscience and music that her talks cover, she said. Her lectures highlight that, in addition to cardiovascular disease, the potential for music therapy and related interventions has been shown in patients with disorders that include autism, psychosis, pain, Parkinson’s disease, Alzheimer’s disease, and epilepsy.
The research highlighted in the session “opens new doors to prevention and treatment strategies using music for patients with heart failure and cardiovascular disease,” summed up Biykem Bozkurt, MD, professor of medicine at the Baylor College of Medicine in Houston and president of the Heart Failure Society of America, who helped organize the virtual session.
Dr. Fleg, Dr. Edwards, Dr. Robb, Dr Kulinski, Ms. Fleming, and Dr. Bozkurt had no relevant financial disclosures.
Dapagliflozin’s CKD performance sends heart failure messages
The DAPA-CKD trial results, which proved dapagliflozin’s efficacy for slowing chronic kidney disease progression in patients selected for signs of worsening renal function, also have important messages for cardiologists, especially heart failure physicians.

Those messages include findings that were “consistent” with the results of the earlier DAPA-HF trial, which tested the same sodium-glucose transporter 2 (SGLT2) inhibitor in patients selected for having heart failure with reduced ejection fraction (HFrEF). In addition, a specific action of dapagliflozin (Farxiga) on the patients in DAPA-CKD, which enrolled patients based on markers of chronic kidney disease (CKD), was prevention of first and recurrent heart failure hospitalizations, John J.V. McMurray, MD, said at the virtual annual scientific meeting of the Heart Failure Society of America, further highlighting the role that dapagliflozin has in reducing both heart failure and renal events.
What DAPA-CKD means for heart failure
The main findings from the DAPA-CKD trial, published in September in the New England Journal of Medicine, included as a secondary outcome the combined rate of death from cardiovascular causes or hospitalization for heart failure (HHF). Treatment with dapagliflozin linked with a significant 29% relative reduction in this endpoint, compared with placebo-treated patients. At the HFSA meeting, Dr. McMurray reported for the first time the specific HHF numbers, a prespecified secondary endpoint for the study.
Patients on dapagliflozin had 37 total HHF events (1.7%), including both first-time and subsequent hospitalizations, while patients in the placebo arm had a total of 71 HHF events (3.3%) during the study’s median 2.4 years of follow-up, an absolute reduction of 1.6% that translated into a relative risk reduction of 49%.
The HHF findings from DAPA-CKD importantly showed that SGLT2 inhibition in patients with signs of renal dysfunction “will not only slow progression of kidney disease but will also reduce the risk of developing heart failure, crucially in patients with or without type 2 diabetes,” explained Dr. McMurray in an interview. “Cardiologists often consult in the kidney wards and advise on management of patients with chronic kidney disease, even those without heart failure.”
The DAPA-CKD findings carry another important message for heart failure management regarding the minimum level of renal function a patient can have and still safely receive dapagliflozin or possibly another agent from the same SGLT2 inhibitor class. In DAPA-CKD, patients safely received dapagliflozin with an estimated glomerular filtration rate (eGFR) as low as 25 mL/min per 1.73 m2; 14% of enrolled patients had an eGFR of 25-29 mL/min per 1.73 m2.
“Typically, about 40%-50% of patients with heart failure have chronic kidney disease,” which makes this safety finding important to clinicians who care for heart failure patients, but it’s also important for any patient who might be a candidate for dapagliflozin or another drug from its class. “We had no strong evidence before this trial that SGLT2 inhibition could reduce hard renal endpoints,” specifically need for chronic dialysis, renal transplant, or renal death, “in patients with or without diabetes,” Dr. McMurray said.
DAPA-CKD grows the pool of eligible heart failure patients
A further consequence of the DAPA-CKD findings is that when, as expected, regulatory bodies give dapagliflozin an indication for treating the types of CKD patients enrolled in the trial, it will functionally expand this treatment to an even larger swath of heart failure patients who currently don’t qualify for this treatment, specifically patients with CKD who also have heart failure with preserved ejection fraction (HFpEF). On Oct. 2, 2020, the Food and Drug Administration fast-tracked dapagliflozin for the CKD indication by granting it Breakthrough Therapy Designation based on the DAPA-CKD results.
Results first reported in 2019 from the DAPA-HF trial led to dapagliflozin receiving a labeled indication for treating HFrEF, the types of heart failure patients enrolled in the trial. Direct evidence on the efficacy of SGLT2 inhibitors for patients with HFpEF will not be available until results from a few trials now in progress become available during the next 12 months.
In the meantime, nearly half of patients with HFpEF also have CKD, noted Dr. McMurray, and another large portion of HFpEF patients have type 2 diabetes and hence qualify for SGLT2 inhibitor treatment that way. “Obviously, we would like to know specifically about heart failure outcomes in patients with HFpEF” on SGLT2 inhibitor treatment, he acknowledged. But the recent approval of dapagliflozin for patients with HFrEF and the likely indication coming soon for treating CKD means that the number of patients with heart failure who are not eligible for SGLT2 inhibitor treatment is dwindling down to some extent.
New DAPA-HF results show no drug, device interactions
In a separate session at the HFSA virtual meeting, Dr. McMurray and several collaborators on the DAPA-HF trial presented results from some new analyses. Dr. McMurray looked at the impact of dapagliflozin treatment on the primary endpoint when patients were stratified by the diuretic dosage they received at study entry. The results showed that “the benefits from dapagliflozin were irrespective of the use of background diuretic therapy or the diuretic dose,” he reported. Study findings also showed that roughly three-quarters of patients in the study had no change in their diuretic dosage during the course of the trial, that the fraction of patients who had an increase in their dosage was about the same as those whose diuretic dosage decreased, and that this pattern was similar in both the patients on dapagliflozin and in those randomized to placebo.
Another set of new analyses from DAPA-HF looked at the impact on dapagliflozin efficacy of background medical and device therapies for heart failure, as well as background diabetes therapies. The findings showed no signal of an interaction with background therapies. “The effects of dapagliflozin are incremental and complimentary to conventional therapies for HFrEF,” concluded Lars Kober, MD, a professor and heart failure physician at Copenhagen University Hospital.
DAPA-CKD was funded by AstraZeneca, the company that markets dapagliflozin (Farxiga). Dr. McMurray’s employer, Glasgow University, has received payments from AstraZeneca and several other companies to compensate for his time overseeing various clinical trials. Dr. Kober has received honoraria for speaking on behalf of several companies including AstraZeneca.
The DAPA-CKD trial results, which proved dapagliflozin’s efficacy for slowing chronic kidney disease progression in patients selected for signs of worsening renal function, also have important messages for cardiologists, especially heart failure physicians.
Those messages include findings that were “consistent” with the results of the earlier DAPA-HF trial, which tested the same sodium-glucose transporter 2 (SGLT2) inhibitor in patients selected for having heart failure with reduced ejection fraction (HFrEF). In addition, a specific action of dapagliflozin (Farxiga) on the patients in DAPA-CKD, which enrolled patients based on markers of chronic kidney disease (CKD), was prevention of first and recurrent heart failure hospitalizations, John J.V. McMurray, MD, said at the virtual annual scientific meeting of the Heart Failure Society of America, further highlighting the role that dapagliflozin has in reducing both heart failure and renal events.
What DAPA-CKD means for heart failure
The main findings from the DAPA-CKD trial, published in September in the New England Journal of Medicine, included as a secondary outcome the combined rate of death from cardiovascular causes or hospitalization for heart failure (HHF). Treatment with dapagliflozin linked with a significant 29% relative reduction in this endpoint, compared with placebo-treated patients. At the HFSA meeting, Dr. McMurray reported for the first time the specific HHF numbers, a prespecified secondary endpoint for the study.
Patients on dapagliflozin had 37 total HHF events (1.7%), including both first-time and subsequent hospitalizations, while patients in the placebo arm had a total of 71 HHF events (3.3%) during the study’s median 2.4 years of follow-up, an absolute reduction of 1.6% that translated into a relative risk reduction of 49%.
The HHF findings from DAPA-CKD importantly showed that SGLT2 inhibition in patients with signs of renal dysfunction “will not only slow progression of kidney disease but will also reduce the risk of developing heart failure, crucially in patients with or without type 2 diabetes,” explained Dr. McMurray in an interview. “Cardiologists often consult in the kidney wards and advise on management of patients with chronic kidney disease, even those without heart failure.”
The DAPA-CKD findings carry another important message for heart failure management regarding the minimum level of renal function a patient can have and still safely receive dapagliflozin or possibly another agent from the same SGLT2 inhibitor class. In DAPA-CKD, patients safely received dapagliflozin with an estimated glomerular filtration rate (eGFR) as low as 25 mL/min per 1.73 m2; 14% of enrolled patients had an eGFR of 25-29 mL/min per 1.73 m2.
“Typically, about 40%-50% of patients with heart failure have chronic kidney disease,” which makes this safety finding important to clinicians who care for heart failure patients, but it’s also important for any patient who might be a candidate for dapagliflozin or another drug from its class. “We had no strong evidence before this trial that SGLT2 inhibition could reduce hard renal endpoints,” specifically need for chronic dialysis, renal transplant, or renal death, “in patients with or without diabetes,” Dr. McMurray said.
DAPA-CKD grows the pool of eligible heart failure patients
A further consequence of the DAPA-CKD findings is that when, as expected, regulatory bodies give dapagliflozin an indication for treating the types of CKD patients enrolled in the trial, it will functionally expand this treatment to an even larger swath of heart failure patients who currently don’t qualify for this treatment, specifically patients with CKD who also have heart failure with preserved ejection fraction (HFpEF). On Oct. 2, 2020, the Food and Drug Administration fast-tracked dapagliflozin for the CKD indication by granting it Breakthrough Therapy Designation based on the DAPA-CKD results.
Results first reported in 2019 from the DAPA-HF trial led to dapagliflozin receiving a labeled indication for treating HFrEF, the types of heart failure patients enrolled in the trial. Direct evidence on the efficacy of SGLT2 inhibitors for patients with HFpEF will not be available until results from a few trials now in progress become available during the next 12 months.
In the meantime, nearly half of patients with HFpEF also have CKD, noted Dr. McMurray, and another large portion of HFpEF patients have type 2 diabetes and hence qualify for SGLT2 inhibitor treatment that way. “Obviously, we would like to know specifically about heart failure outcomes in patients with HFpEF” on SGLT2 inhibitor treatment, he acknowledged. But the recent approval of dapagliflozin for patients with HFrEF and the likely indication coming soon for treating CKD means that the number of patients with heart failure who are not eligible for SGLT2 inhibitor treatment is dwindling down to some extent.
New DAPA-HF results show no drug, device interactions
In a separate session at the HFSA virtual meeting, Dr. McMurray and several collaborators on the DAPA-HF trial presented results from some new analyses. Dr. McMurray looked at the impact of dapagliflozin treatment on the primary endpoint when patients were stratified by the diuretic dosage they received at study entry. The results showed that “the benefits from dapagliflozin were irrespective of the use of background diuretic therapy or the diuretic dose,” he reported. Study findings also showed that roughly three-quarters of patients in the study had no change in their diuretic dosage during the course of the trial, that the fraction of patients who had an increase in their dosage was about the same as those whose diuretic dosage decreased, and that this pattern was similar in both the patients on dapagliflozin and in those randomized to placebo.
Another set of new analyses from DAPA-HF looked at the impact on dapagliflozin efficacy of background medical and device therapies for heart failure, as well as background diabetes therapies. The findings showed no signal of an interaction with background therapies. “The effects of dapagliflozin are incremental and complimentary to conventional therapies for HFrEF,” concluded Lars Kober, MD, a professor and heart failure physician at Copenhagen University Hospital.
DAPA-CKD was funded by AstraZeneca, the company that markets dapagliflozin (Farxiga). Dr. McMurray’s employer, Glasgow University, has received payments from AstraZeneca and several other companies to compensate for his time overseeing various clinical trials. Dr. Kober has received honoraria for speaking on behalf of several companies including AstraZeneca.
The DAPA-CKD trial results, which proved dapagliflozin’s efficacy for slowing chronic kidney disease progression in patients selected for signs of worsening renal function, also have important messages for cardiologists, especially heart failure physicians.
Those messages include findings that were “consistent” with the results of the earlier DAPA-HF trial, which tested the same sodium-glucose transporter 2 (SGLT2) inhibitor in patients selected for having heart failure with reduced ejection fraction (HFrEF). In addition, a specific action of dapagliflozin (Farxiga) on the patients in DAPA-CKD, which enrolled patients based on markers of chronic kidney disease (CKD), was prevention of first and recurrent heart failure hospitalizations, John J.V. McMurray, MD, said at the virtual annual scientific meeting of the Heart Failure Society of America, further highlighting the role that dapagliflozin has in reducing both heart failure and renal events.
What DAPA-CKD means for heart failure
The main findings from the DAPA-CKD trial, published in September in the New England Journal of Medicine, included as a secondary outcome the combined rate of death from cardiovascular causes or hospitalization for heart failure (HHF). Treatment with dapagliflozin linked with a significant 29% relative reduction in this endpoint, compared with placebo-treated patients. At the HFSA meeting, Dr. McMurray reported for the first time the specific HHF numbers, a prespecified secondary endpoint for the study.
Patients on dapagliflozin had 37 total HHF events (1.7%), including both first-time and subsequent hospitalizations, while patients in the placebo arm had a total of 71 HHF events (3.3%) during the study’s median 2.4 years of follow-up, an absolute reduction of 1.6% that translated into a relative risk reduction of 49%.
The HHF findings from DAPA-CKD importantly showed that SGLT2 inhibition in patients with signs of renal dysfunction “will not only slow progression of kidney disease but will also reduce the risk of developing heart failure, crucially in patients with or without type 2 diabetes,” explained Dr. McMurray in an interview. “Cardiologists often consult in the kidney wards and advise on management of patients with chronic kidney disease, even those without heart failure.”
The DAPA-CKD findings carry another important message for heart failure management regarding the minimum level of renal function a patient can have and still safely receive dapagliflozin or possibly another agent from the same SGLT2 inhibitor class. In DAPA-CKD, patients safely received dapagliflozin with an estimated glomerular filtration rate (eGFR) as low as 25 mL/min per 1.73 m2; 14% of enrolled patients had an eGFR of 25-29 mL/min per 1.73 m2.
“Typically, about 40%-50% of patients with heart failure have chronic kidney disease,” which makes this safety finding important to clinicians who care for heart failure patients, but it’s also important for any patient who might be a candidate for dapagliflozin or another drug from its class. “We had no strong evidence before this trial that SGLT2 inhibition could reduce hard renal endpoints,” specifically need for chronic dialysis, renal transplant, or renal death, “in patients with or without diabetes,” Dr. McMurray said.
DAPA-CKD grows the pool of eligible heart failure patients
A further consequence of the DAPA-CKD findings is that when, as expected, regulatory bodies give dapagliflozin an indication for treating the types of CKD patients enrolled in the trial, it will functionally expand this treatment to an even larger swath of heart failure patients who currently don’t qualify for this treatment, specifically patients with CKD who also have heart failure with preserved ejection fraction (HFpEF). On Oct. 2, 2020, the Food and Drug Administration fast-tracked dapagliflozin for the CKD indication by granting it Breakthrough Therapy Designation based on the DAPA-CKD results.
Results first reported in 2019 from the DAPA-HF trial led to dapagliflozin receiving a labeled indication for treating HFrEF, the types of heart failure patients enrolled in the trial. Direct evidence on the efficacy of SGLT2 inhibitors for patients with HFpEF will not be available until results from a few trials now in progress become available during the next 12 months.
In the meantime, nearly half of patients with HFpEF also have CKD, noted Dr. McMurray, and another large portion of HFpEF patients have type 2 diabetes and hence qualify for SGLT2 inhibitor treatment that way. “Obviously, we would like to know specifically about heart failure outcomes in patients with HFpEF” on SGLT2 inhibitor treatment, he acknowledged. But the recent approval of dapagliflozin for patients with HFrEF and the likely indication coming soon for treating CKD means that the number of patients with heart failure who are not eligible for SGLT2 inhibitor treatment is dwindling down to some extent.
New DAPA-HF results show no drug, device interactions
In a separate session at the HFSA virtual meeting, Dr. McMurray and several collaborators on the DAPA-HF trial presented results from some new analyses. Dr. McMurray looked at the impact of dapagliflozin treatment on the primary endpoint when patients were stratified by the diuretic dosage they received at study entry. The results showed that “the benefits from dapagliflozin were irrespective of the use of background diuretic therapy or the diuretic dose,” he reported. Study findings also showed that roughly three-quarters of patients in the study had no change in their diuretic dosage during the course of the trial, that the fraction of patients who had an increase in their dosage was about the same as those whose diuretic dosage decreased, and that this pattern was similar in both the patients on dapagliflozin and in those randomized to placebo.
Another set of new analyses from DAPA-HF looked at the impact on dapagliflozin efficacy of background medical and device therapies for heart failure, as well as background diabetes therapies. The findings showed no signal of an interaction with background therapies. “The effects of dapagliflozin are incremental and complimentary to conventional therapies for HFrEF,” concluded Lars Kober, MD, a professor and heart failure physician at Copenhagen University Hospital.
DAPA-CKD was funded by AstraZeneca, the company that markets dapagliflozin (Farxiga). Dr. McMurray’s employer, Glasgow University, has received payments from AstraZeneca and several other companies to compensate for his time overseeing various clinical trials. Dr. Kober has received honoraria for speaking on behalf of several companies including AstraZeneca.
FROM HFSA 2020
AHA scientific statement highlights cardiorenal benefit of new diabetes drugs
To protect the heart and kidneys, sodium-glucose transporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) receptor agonists should be considered for people with type 2 diabetes and chronic kidney disease (CKD), the American Heart Association advised in a new scientific statement.
Taken together, the results of relevant clinical trials indicate that SGLT2 inhibitors and GLP-1 receptor agonists safely and significantly reduce the risk for cardiovascular (CV) events, death, and the slow progression of CKD to end-stage kidney disease, including the risks for dialysis, transplantation, and death, the writing group says.
The scientific statement was published online Sept. 28 in Circulation.
“There has been rapid reporting of high-quality data in the cardio-renal-metabolic space with significant heart and kidney benefits, particularly with these two newer classes of antihyperglycemic agents,” Janani Rangaswami, MD, who chaired the writing group, said in an interview.
“More recent data show benefits in chronic kidney disease and heart failure even in patients without diabetes,” said Dr. Rangaswami, Einstein Medical Center and Sidney Kimmel Medical College, both in Philadelphia.
“These data are practice-changing in both cardiology and nephrology, and usher in a new era of disease-modifying therapies in heart and kidney disease,” Dr. Rangaswami added.
Recommendations at a glance
- Provide early and ongoing assessment of risks for CVD and CKD to patients who may benefit from SGLT2 inhibitors of GLP-1 receptor agonists.
- Tailor medication choices that meet the needs of individual patients. Realize that, given “consistent class-wide effects,” the choice of a specific SGLT2 inhibitor or GLP-1 receptor agonist may be dictated by affordability, coverage, and formulary considerations.
- Adjust all medications in tandem with these medicines and consider the burden of polypharmacy, which is common among people with type 2 diabetes. Adjust concomitant therapies and deprescribe where possible.
- Identify risks for hypoglycemia and educate patients on the signs so they can seek treatment quickly.
- Monitor and control high blood pressure.
- Counsel patients about the risks for and symptoms of euglycemic diabetic ketoacidosis when taking SGLT2 inhibitors, as well as classic DKA, which can be fatal.
- Regularly screen and counsel patients about foot care to prevent foot ulcers or blisters that can quickly become infected and lead to amputation.
The writing group identified two additional patient subgroups that may benefit from SGLT2 inhibitors and GLP-1 receptor agonists: those with heart failure with reduced ejection fraction with or without diabetes; and those with CKD who do not have diabetes. They say more data are anticipated to validate the use of SGLT2 inhibitors and GLP-1 receptor agonists in these “at-risk” patients.
Collaborative care model
The writing group proposed a collaborative care model, bridging cardiologists, nephrologists, endocrinologists, and primary care physicians, to help facilitate the “prompt and appropriate” integration of these new classes of medications in the management of patients with type 2 diabetes and CKD.
There is “an unmet need for a cardio-renal-metabolic care model that incorporates best practices in the real world to help align these therapies, especially with vulnerable high-risk patients with cardiorenal disease, and to overcome barriers toward uptake of these agents. Hopefully this statement provides some guidance to the cardiology and nephrology communities in that area,” Dr. Rangaswami said in an interview.
But old habits die hard, as research continues to show the slow adoption of these newer medications in the real world.
For example, a large observational study published last year showed a “striking” discordance between evidence-based, guideline-recommended use of SGLT2 inhibitors for the treatment of type 2 diabetes and their actual uptake in clinical practice.
Paradoxically, patients with CVD, heart failure, hypertension, CKD, and those at risk for hypoglycemia were less apt to receive an SGLT2 inhibitor than other patients.
“The relatively slow uptake of these agents is multifactorial,” Dr. Rangaswami said. “Cardiologists and nephrologists may suffer from some level of ‘therapeutic inertia’ when using new agents they are unfamiliar with and originally branded as ‘antidiabetic’ agents, with the perception of these agents being outside the scope of their practice.”
Two other factors are also at play. “The current health care system is based on ‘specialty silos,’ where specialists tend to stick to the traditional scope of their specialty and are reluctant to view these agents as part of their therapeutic armamentarium. Finally, insurance coverage barriers and affordability also limit the use on a widespread basis,” Dr. Rangaswami said.
A version of this article originally appeared on Medscape.com .
To protect the heart and kidneys, sodium-glucose transporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) receptor agonists should be considered for people with type 2 diabetes and chronic kidney disease (CKD), the American Heart Association advised in a new scientific statement.
Taken together, the results of relevant clinical trials indicate that SGLT2 inhibitors and GLP-1 receptor agonists safely and significantly reduce the risk for cardiovascular (CV) events, death, and the slow progression of CKD to end-stage kidney disease, including the risks for dialysis, transplantation, and death, the writing group says.
The scientific statement was published online Sept. 28 in Circulation.
“There has been rapid reporting of high-quality data in the cardio-renal-metabolic space with significant heart and kidney benefits, particularly with these two newer classes of antihyperglycemic agents,” Janani Rangaswami, MD, who chaired the writing group, said in an interview.
“More recent data show benefits in chronic kidney disease and heart failure even in patients without diabetes,” said Dr. Rangaswami, Einstein Medical Center and Sidney Kimmel Medical College, both in Philadelphia.
“These data are practice-changing in both cardiology and nephrology, and usher in a new era of disease-modifying therapies in heart and kidney disease,” Dr. Rangaswami added.
Recommendations at a glance
- Provide early and ongoing assessment of risks for CVD and CKD to patients who may benefit from SGLT2 inhibitors of GLP-1 receptor agonists.
- Tailor medication choices that meet the needs of individual patients. Realize that, given “consistent class-wide effects,” the choice of a specific SGLT2 inhibitor or GLP-1 receptor agonist may be dictated by affordability, coverage, and formulary considerations.
- Adjust all medications in tandem with these medicines and consider the burden of polypharmacy, which is common among people with type 2 diabetes. Adjust concomitant therapies and deprescribe where possible.
- Identify risks for hypoglycemia and educate patients on the signs so they can seek treatment quickly.
- Monitor and control high blood pressure.
- Counsel patients about the risks for and symptoms of euglycemic diabetic ketoacidosis when taking SGLT2 inhibitors, as well as classic DKA, which can be fatal.
- Regularly screen and counsel patients about foot care to prevent foot ulcers or blisters that can quickly become infected and lead to amputation.
The writing group identified two additional patient subgroups that may benefit from SGLT2 inhibitors and GLP-1 receptor agonists: those with heart failure with reduced ejection fraction with or without diabetes; and those with CKD who do not have diabetes. They say more data are anticipated to validate the use of SGLT2 inhibitors and GLP-1 receptor agonists in these “at-risk” patients.
Collaborative care model
The writing group proposed a collaborative care model, bridging cardiologists, nephrologists, endocrinologists, and primary care physicians, to help facilitate the “prompt and appropriate” integration of these new classes of medications in the management of patients with type 2 diabetes and CKD.
There is “an unmet need for a cardio-renal-metabolic care model that incorporates best practices in the real world to help align these therapies, especially with vulnerable high-risk patients with cardiorenal disease, and to overcome barriers toward uptake of these agents. Hopefully this statement provides some guidance to the cardiology and nephrology communities in that area,” Dr. Rangaswami said in an interview.
But old habits die hard, as research continues to show the slow adoption of these newer medications in the real world.
For example, a large observational study published last year showed a “striking” discordance between evidence-based, guideline-recommended use of SGLT2 inhibitors for the treatment of type 2 diabetes and their actual uptake in clinical practice.
Paradoxically, patients with CVD, heart failure, hypertension, CKD, and those at risk for hypoglycemia were less apt to receive an SGLT2 inhibitor than other patients.
“The relatively slow uptake of these agents is multifactorial,” Dr. Rangaswami said. “Cardiologists and nephrologists may suffer from some level of ‘therapeutic inertia’ when using new agents they are unfamiliar with and originally branded as ‘antidiabetic’ agents, with the perception of these agents being outside the scope of their practice.”
Two other factors are also at play. “The current health care system is based on ‘specialty silos,’ where specialists tend to stick to the traditional scope of their specialty and are reluctant to view these agents as part of their therapeutic armamentarium. Finally, insurance coverage barriers and affordability also limit the use on a widespread basis,” Dr. Rangaswami said.
A version of this article originally appeared on Medscape.com .
To protect the heart and kidneys, sodium-glucose transporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) receptor agonists should be considered for people with type 2 diabetes and chronic kidney disease (CKD), the American Heart Association advised in a new scientific statement.
Taken together, the results of relevant clinical trials indicate that SGLT2 inhibitors and GLP-1 receptor agonists safely and significantly reduce the risk for cardiovascular (CV) events, death, and the slow progression of CKD to end-stage kidney disease, including the risks for dialysis, transplantation, and death, the writing group says.
The scientific statement was published online Sept. 28 in Circulation.
“There has been rapid reporting of high-quality data in the cardio-renal-metabolic space with significant heart and kidney benefits, particularly with these two newer classes of antihyperglycemic agents,” Janani Rangaswami, MD, who chaired the writing group, said in an interview.
“More recent data show benefits in chronic kidney disease and heart failure even in patients without diabetes,” said Dr. Rangaswami, Einstein Medical Center and Sidney Kimmel Medical College, both in Philadelphia.
“These data are practice-changing in both cardiology and nephrology, and usher in a new era of disease-modifying therapies in heart and kidney disease,” Dr. Rangaswami added.
Recommendations at a glance
- Provide early and ongoing assessment of risks for CVD and CKD to patients who may benefit from SGLT2 inhibitors of GLP-1 receptor agonists.
- Tailor medication choices that meet the needs of individual patients. Realize that, given “consistent class-wide effects,” the choice of a specific SGLT2 inhibitor or GLP-1 receptor agonist may be dictated by affordability, coverage, and formulary considerations.
- Adjust all medications in tandem with these medicines and consider the burden of polypharmacy, which is common among people with type 2 diabetes. Adjust concomitant therapies and deprescribe where possible.
- Identify risks for hypoglycemia and educate patients on the signs so they can seek treatment quickly.
- Monitor and control high blood pressure.
- Counsel patients about the risks for and symptoms of euglycemic diabetic ketoacidosis when taking SGLT2 inhibitors, as well as classic DKA, which can be fatal.
- Regularly screen and counsel patients about foot care to prevent foot ulcers or blisters that can quickly become infected and lead to amputation.
The writing group identified two additional patient subgroups that may benefit from SGLT2 inhibitors and GLP-1 receptor agonists: those with heart failure with reduced ejection fraction with or without diabetes; and those with CKD who do not have diabetes. They say more data are anticipated to validate the use of SGLT2 inhibitors and GLP-1 receptor agonists in these “at-risk” patients.
Collaborative care model
The writing group proposed a collaborative care model, bridging cardiologists, nephrologists, endocrinologists, and primary care physicians, to help facilitate the “prompt and appropriate” integration of these new classes of medications in the management of patients with type 2 diabetes and CKD.
There is “an unmet need for a cardio-renal-metabolic care model that incorporates best practices in the real world to help align these therapies, especially with vulnerable high-risk patients with cardiorenal disease, and to overcome barriers toward uptake of these agents. Hopefully this statement provides some guidance to the cardiology and nephrology communities in that area,” Dr. Rangaswami said in an interview.
But old habits die hard, as research continues to show the slow adoption of these newer medications in the real world.
For example, a large observational study published last year showed a “striking” discordance between evidence-based, guideline-recommended use of SGLT2 inhibitors for the treatment of type 2 diabetes and their actual uptake in clinical practice.
Paradoxically, patients with CVD, heart failure, hypertension, CKD, and those at risk for hypoglycemia were less apt to receive an SGLT2 inhibitor than other patients.
“The relatively slow uptake of these agents is multifactorial,” Dr. Rangaswami said. “Cardiologists and nephrologists may suffer from some level of ‘therapeutic inertia’ when using new agents they are unfamiliar with and originally branded as ‘antidiabetic’ agents, with the perception of these agents being outside the scope of their practice.”
Two other factors are also at play. “The current health care system is based on ‘specialty silos,’ where specialists tend to stick to the traditional scope of their specialty and are reluctant to view these agents as part of their therapeutic armamentarium. Finally, insurance coverage barriers and affordability also limit the use on a widespread basis,” Dr. Rangaswami said.
A version of this article originally appeared on Medscape.com .
Geriatric patients: My three rules for them
I have been in practice for 31 years, so many of my patients are now in their 80s and 90s. Practices age with us, and I have been seeing many of these patients for 25-30 years.
Absolutely, positively make sure you move!

Our older patients often have many reasons not to move, including pain from arthritis, deconditioning, muscle weakness, fatigue, and depression. “Keeping moving” is probably the most important thing a patient can do for their health.
Holme and Anderssen studied a large cohort of men for cardiovascular risk in 1972 and again in 2000. The surviving men were followed over an additional 12 years.1 They found that 30 minutes of physical activity 6 days a week was associated with a 40% reduction in mortality. Sedentary men had a reduced life expectancy of about 5 years, compared with men who were moderately to vigorously physically active.
Stewart etal. studied the benefit of physical activity in people with stable coronary disease.2 They concluded that, in patients with stable coronary heart disease, more physical activity was associated with lower mortality, and the largest benefit occurred in the sedentary patient groups and the highest cardiac risk groups.
Saint-Maurice et al. studied the effects of total daily step count and step intensity on mortality risk.3 They found that the risk of all-cause mortality decreases as the total number of daily steps increases, but that the speed of those steps did not make a difference. This is very encouraging data for our elderly patients. Moving is the secret, even if it may not be moving at a fast pace!
Never, ever get on a ladder!
This one should be part of every geriatric’s assessment and every Medicare wellness exam. I first experienced the horror of what can happen when elderly people climb when a 96-year-old healthy patient of mine fell off his roof and died. I never thought to tell him climbing on the roof was an awful idea.
Akland et al. looked at the epidemiology and outcomes of ladder-related falls that required ICU admission.4 Hospital mortality was 26%, and almost all of the mortalities occurred in older males in domestic falls, who died as a result of traumatic brain injury. Fewer than half of the survivors were living independently 1 year after the fall.
Valmuur et al. studied ladder related falls in Australia.5 They found that rates of ladder related falls requiring hospitalization rose from about 20/100,000 for men ages 15-29 years to 78/100,000 for men aged over 60 years. Of those who died from fall-related injury, 82% were over the age of 60, with more than 70% dying from head injuries.
Schaffarczyk et al. looked at the impact of nonoccupational falls from ladders in men aged over 50 years.6 The mean age of the patients in the study was 64 years (range, 50-85), with 27% suffering severe trauma. There was a striking impact on long-term function occurring in over half the study patients. The authors did interviews with patients in follow-up long after the falls and found that most never thought of themselves at risk for a fall, and after the experience of a bad fall, would never consider going on a ladder again. I think it is important for health care professionals to discuss the dangers of ladder use with our older patients, pointing out the higher risk of falling and the potential for the fall to be a life-changing or life-ending event.
Let them eat!
Many patients have a reduced appetite as they age. We work hard with our patients to choose a healthy diet throughout their lives, to help ward off obesity, treat hypertension, prevent or control diabetes, or provide heart health. Many patients just stop being interested in food, reduce intake, and may lose weight and muscle mass. When my patients pass the age of 85, I change my focus to encouraging them to eat for calories, socialization, and joy. I think the marginal benefits of more restrictive diets are small, compared with the benefits of helping your patients enjoy eating again. I ask patients what their very favorite foods are and encourage them to have them.
Pearl
Keep your patients eating and moving, except not onto a ladder!
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Holme I, Anderssen SA. Increases in physical activity is as important as smoking cessation for reduction in total mortality in elderly men: 12 years of follow-up of the Oslo II study. Br J Sports Med. 2015; 49:743-8.
2. Stewart RAH et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. 2017 Oct 3;70(14):1689-1700..
3. Saint-Maurice PF et al. Association of daily step count and step intensity with mortality among U.S. adults. JAMA 2020;323:1151-60.
4. Ackland HM et al. Danger at every rung: Epidemiology and outcomes of ICU-admitted ladder-related trauma. Injury. 2016;47:1109-117.
5. Vallmuur K et al. Falls from ladders in Australia: comparing occupational and nonoccupational injuries across age groups. Aust N Z J Public Health. 2016 Dec;40(6):559-63.
6. Schaffarczyk K et al. Nonoccupational falls from ladders in men 50 years and over: Contributing factors and impact. Injury. 2020 Aug;51(8):1798-1804.
I have been in practice for 31 years, so many of my patients are now in their 80s and 90s. Practices age with us, and I have been seeing many of these patients for 25-30 years.
Absolutely, positively make sure you move!
Our older patients often have many reasons not to move, including pain from arthritis, deconditioning, muscle weakness, fatigue, and depression. “Keeping moving” is probably the most important thing a patient can do for their health.
Holme and Anderssen studied a large cohort of men for cardiovascular risk in 1972 and again in 2000. The surviving men were followed over an additional 12 years.1 They found that 30 minutes of physical activity 6 days a week was associated with a 40% reduction in mortality. Sedentary men had a reduced life expectancy of about 5 years, compared with men who were moderately to vigorously physically active.
Stewart etal. studied the benefit of physical activity in people with stable coronary disease.2 They concluded that, in patients with stable coronary heart disease, more physical activity was associated with lower mortality, and the largest benefit occurred in the sedentary patient groups and the highest cardiac risk groups.
Saint-Maurice et al. studied the effects of total daily step count and step intensity on mortality risk.3 They found that the risk of all-cause mortality decreases as the total number of daily steps increases, but that the speed of those steps did not make a difference. This is very encouraging data for our elderly patients. Moving is the secret, even if it may not be moving at a fast pace!
Never, ever get on a ladder!
This one should be part of every geriatric’s assessment and every Medicare wellness exam. I first experienced the horror of what can happen when elderly people climb when a 96-year-old healthy patient of mine fell off his roof and died. I never thought to tell him climbing on the roof was an awful idea.
Akland et al. looked at the epidemiology and outcomes of ladder-related falls that required ICU admission.4 Hospital mortality was 26%, and almost all of the mortalities occurred in older males in domestic falls, who died as a result of traumatic brain injury. Fewer than half of the survivors were living independently 1 year after the fall.
Valmuur et al. studied ladder related falls in Australia.5 They found that rates of ladder related falls requiring hospitalization rose from about 20/100,000 for men ages 15-29 years to 78/100,000 for men aged over 60 years. Of those who died from fall-related injury, 82% were over the age of 60, with more than 70% dying from head injuries.
Schaffarczyk et al. looked at the impact of nonoccupational falls from ladders in men aged over 50 years.6 The mean age of the patients in the study was 64 years (range, 50-85), with 27% suffering severe trauma. There was a striking impact on long-term function occurring in over half the study patients. The authors did interviews with patients in follow-up long after the falls and found that most never thought of themselves at risk for a fall, and after the experience of a bad fall, would never consider going on a ladder again. I think it is important for health care professionals to discuss the dangers of ladder use with our older patients, pointing out the higher risk of falling and the potential for the fall to be a life-changing or life-ending event.
Let them eat!
Many patients have a reduced appetite as they age. We work hard with our patients to choose a healthy diet throughout their lives, to help ward off obesity, treat hypertension, prevent or control diabetes, or provide heart health. Many patients just stop being interested in food, reduce intake, and may lose weight and muscle mass. When my patients pass the age of 85, I change my focus to encouraging them to eat for calories, socialization, and joy. I think the marginal benefits of more restrictive diets are small, compared with the benefits of helping your patients enjoy eating again. I ask patients what their very favorite foods are and encourage them to have them.
Pearl
Keep your patients eating and moving, except not onto a ladder!
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Holme I, Anderssen SA. Increases in physical activity is as important as smoking cessation for reduction in total mortality in elderly men: 12 years of follow-up of the Oslo II study. Br J Sports Med. 2015; 49:743-8.
2. Stewart RAH et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. 2017 Oct 3;70(14):1689-1700..
3. Saint-Maurice PF et al. Association of daily step count and step intensity with mortality among U.S. adults. JAMA 2020;323:1151-60.
4. Ackland HM et al. Danger at every rung: Epidemiology and outcomes of ICU-admitted ladder-related trauma. Injury. 2016;47:1109-117.
5. Vallmuur K et al. Falls from ladders in Australia: comparing occupational and nonoccupational injuries across age groups. Aust N Z J Public Health. 2016 Dec;40(6):559-63.
6. Schaffarczyk K et al. Nonoccupational falls from ladders in men 50 years and over: Contributing factors and impact. Injury. 2020 Aug;51(8):1798-1804.
I have been in practice for 31 years, so many of my patients are now in their 80s and 90s. Practices age with us, and I have been seeing many of these patients for 25-30 years.
Absolutely, positively make sure you move!
Our older patients often have many reasons not to move, including pain from arthritis, deconditioning, muscle weakness, fatigue, and depression. “Keeping moving” is probably the most important thing a patient can do for their health.
Holme and Anderssen studied a large cohort of men for cardiovascular risk in 1972 and again in 2000. The surviving men were followed over an additional 12 years.1 They found that 30 minutes of physical activity 6 days a week was associated with a 40% reduction in mortality. Sedentary men had a reduced life expectancy of about 5 years, compared with men who were moderately to vigorously physically active.
Stewart etal. studied the benefit of physical activity in people with stable coronary disease.2 They concluded that, in patients with stable coronary heart disease, more physical activity was associated with lower mortality, and the largest benefit occurred in the sedentary patient groups and the highest cardiac risk groups.
Saint-Maurice et al. studied the effects of total daily step count and step intensity on mortality risk.3 They found that the risk of all-cause mortality decreases as the total number of daily steps increases, but that the speed of those steps did not make a difference. This is very encouraging data for our elderly patients. Moving is the secret, even if it may not be moving at a fast pace!
Never, ever get on a ladder!
This one should be part of every geriatric’s assessment and every Medicare wellness exam. I first experienced the horror of what can happen when elderly people climb when a 96-year-old healthy patient of mine fell off his roof and died. I never thought to tell him climbing on the roof was an awful idea.
Akland et al. looked at the epidemiology and outcomes of ladder-related falls that required ICU admission.4 Hospital mortality was 26%, and almost all of the mortalities occurred in older males in domestic falls, who died as a result of traumatic brain injury. Fewer than half of the survivors were living independently 1 year after the fall.
Valmuur et al. studied ladder related falls in Australia.5 They found that rates of ladder related falls requiring hospitalization rose from about 20/100,000 for men ages 15-29 years to 78/100,000 for men aged over 60 years. Of those who died from fall-related injury, 82% were over the age of 60, with more than 70% dying from head injuries.
Schaffarczyk et al. looked at the impact of nonoccupational falls from ladders in men aged over 50 years.6 The mean age of the patients in the study was 64 years (range, 50-85), with 27% suffering severe trauma. There was a striking impact on long-term function occurring in over half the study patients. The authors did interviews with patients in follow-up long after the falls and found that most never thought of themselves at risk for a fall, and after the experience of a bad fall, would never consider going on a ladder again. I think it is important for health care professionals to discuss the dangers of ladder use with our older patients, pointing out the higher risk of falling and the potential for the fall to be a life-changing or life-ending event.
Let them eat!
Many patients have a reduced appetite as they age. We work hard with our patients to choose a healthy diet throughout their lives, to help ward off obesity, treat hypertension, prevent or control diabetes, or provide heart health. Many patients just stop being interested in food, reduce intake, and may lose weight and muscle mass. When my patients pass the age of 85, I change my focus to encouraging them to eat for calories, socialization, and joy. I think the marginal benefits of more restrictive diets are small, compared with the benefits of helping your patients enjoy eating again. I ask patients what their very favorite foods are and encourage them to have them.
Pearl
Keep your patients eating and moving, except not onto a ladder!
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Holme I, Anderssen SA. Increases in physical activity is as important as smoking cessation for reduction in total mortality in elderly men: 12 years of follow-up of the Oslo II study. Br J Sports Med. 2015; 49:743-8.
2. Stewart RAH et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. 2017 Oct 3;70(14):1689-1700..
3. Saint-Maurice PF et al. Association of daily step count and step intensity with mortality among U.S. adults. JAMA 2020;323:1151-60.
4. Ackland HM et al. Danger at every rung: Epidemiology and outcomes of ICU-admitted ladder-related trauma. Injury. 2016;47:1109-117.
5. Vallmuur K et al. Falls from ladders in Australia: comparing occupational and nonoccupational injuries across age groups. Aust N Z J Public Health. 2016 Dec;40(6):559-63.
6. Schaffarczyk K et al. Nonoccupational falls from ladders in men 50 years and over: Contributing factors and impact. Injury. 2020 Aug;51(8):1798-1804.
New data challenge primary care’s inattention to aldosterone in hypertension
Jun Yang, MBBS, had watched as her father, who had battled hypertension for decades, ended up on four medications that still couldn’t bring his blood pressure to a healthy level. The cardiovascular endocrinologist then ran some tests, and soon thereafter her father had his blood pressure optimized on just one targeted medication.

Dr. Yang’s father was found to have a hormonal condition known as primary aldosteronism (PA) as the cause of his hypertension.
It turns out that PA is not as rare as once thought.
An eye-catching report in Annals of Internal Medicine this spring of an unexpectedly high prevalence of primary aldosteronism among a diverse cross section of U.S. patients with hypertension has raised issues that could dramatically change the way doctors in America, and elsewhere, assess and manage high blood pressure.
Foremost is the question of whether primary care physicians – the clinicians at the front line for diagnosing and initially treating most patients with hypertension – will absorb and act on this new evidence. For them, aldosteronism doesn’t automatically come to mind when they see high numbers on a BP monitor, and yet this latest research found that up to a third of all 726 patients in the study who were diagnosed with hypertension and with high urinary salt levels had PA.
That translates to a roughly three- to fivefold increase over standard prevalence estimates, and is a ”game changer” for how clinicians should approach hypertension management and PA diagnosis going forward, said John W. Funder, MD, in an editorial accompanying the Annals study.
Long considered relatively uncommon, hypertension driven by an excess of the hormone aldosterone, often because of an adenoma on the adrenal gland, is not the same as conventional “essential” hypertension. The former benefits from early diagnosis because its treatment is completely different – close to half of all PA patients can be treated definitively and quickly with surgical removal of an adenoma from one side of the adrenal gland.
For other PA patients, who have bilateral adrenal hyperplasia that is impossible to resolve surgically, treatment with drugs called mineralocorticoid receptor antagonists (MRAs), such as spironolactone, is needed because they target the hormonal cause of the high BP.
But what usually happens is that a patient with PA is mistakenly diagnosed with essential hypertension, in which the classic approach to treatment is to start with one regular antihypertensive drug, and add on further ones from different drug classes if blood pressure is not adequately controlled. When patients are taking three drugs, without adequate control, they are labeled as having “resistant hypertension.”
But in the case of PA, none of these conventional antihypertensives work, and the process of continuing to monitor and add different drugs wastes time, during which patients deteriorate.
“We need to change the culture of waiting for hypertension to be resistant and have patients riddled with end-organ damage,” due to years of persistently high BP and excess aldosterone “before we look for a secondary cause” like PA, declared Dr. Yang, of Hudson Institute of Medical Research and Monash University in Melbourne, during an interview.
So early diagnosis and prompt treatment of PA is key.
In addition to boosting the public health importance of early PA detection in hypertensive patients, the new up-sized PA prevalence numbers throw a spotlight on primary care physicians (PCPs) as key players who will need to apply the findings to practice on a public health scale.
These novel results create a need for “new guidelines, and a radically revised game plan with the key role of PCPs” emphasized in future management of patients with hypertension, said Dr. Funder, a professor of medicine at Monash University, in a second recent editorial in Hypertension.

“Buy-in by PCPs is essential,” agrees Robert M. Carey, MD, a cardiovascular endocrinologist and professor of medicine at the University of Virginia in Charlottesville, and a coauthor of the new study.
But he too acknowledges that this presents a major challenge. PCPs and internists, who diagnose a lot of hypertension, are “not used to thinking about aldosterone,” he said in an interview, encapsulating the key problem faced by proponents of earlier and more widespread PA assessment.
This dilemma looms as a “huge public health issue,” Dr. Carey warned.
‘We’re a long way from getting’ PCPs to buy in to PA screening
Will PCPs grow more comfortable with screening patients for PA themselves, or might they become more willing to refer hypertensive individuals for assessment at an expert center?
One skeptic is Ross D. Feldman, MD, a hypertension-management researcher and professor of medicine at the University of Manitoba in Winnipeg. The finding about high PA prevalence in patients with hypertension “is brand new, [and] the message needs to get to PCPs,” he said. But, “We’re a long way from getting it” to them. “I don’t know how to do that. It will be a tough sell.”
In addition, repositioning MRAs as an earlier option for many hypertensive patients won’t be easy either, because “we’ll never have outcome-trial data for MRAs,” given that they are now generic drugs, he noted.
“No clinical trial data show [MRAs] are first-line drugs,” said Dr. Feldman, who explained that, instead, MRAs are considered “go-to drugs” for patients with treatment-resistant hypertension, a niche therapeutic area. Results from the PATHWAY-2 trial published 5 years ago in Lancet showed “spironolactone was clearly the most effective treatment for the condition,” according to the report authors.
But even among patients with resistant hypertension, screening for PA dramatically lags despite being enshrined in guidelines.

“PCPs should start checking aldosterone-to-renin ratios [a widely used PA screen] in all patients with resistant hypertension or hypertension with hypokalemia, and then refer patients to specialists for testing and management,” said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia.
But recent studies of U.S. patient populations with clinical characteristics that meet existing criteria for PA screening showed that just 1%-2% of these individuals underwent an initial PA assessment, she noted, citing reports in the journals Surgery and Hypertension.
“We need to prioritize improving screening in these high-risk patients,” she stressed in an interview.
This illustrates that, in some respects, the new prevalence numbers are beside the point, because PA has been going unscreened and overlooked far too often even in the context of historical, lower prevalence rates, said Dr. Yang.
“The key point is that approximately 1 in 10 people with hypertension, and even more with resistant hypertension, have a form of the disease that is worse than essential hypertension but is routinely missed at present” and is also highly treatable.
“Evidence for the need for increased awareness of PA has been building for 2 decades,” stressed Dr. Yang, who has coauthored several commentaries and reviews that have bemoaned PA’s underappreciated status.
Interest in partnering with PCPs on guidance grows
One potential solution is to have endocrinologists and hypertension specialists’ partner with PCPs to come up with diagnostic and management recommendations. Both Dr. Funder and Dr. Carey are opinion leaders regarding the role of aldosterone in hypertension, and both were coauthors of the 2016 Endocrine Society guideline for PA assessment and management published in the Journal of Clinical Endocrinology & Metabolism , with Dr. Funder chairing the writing panel.
Now approaching its fifth year in effect, this guideline is “due for revision,” and “my hope is that we’ll be able to partner with one or more PCP organizations to come up with a version of the guideline targeted to PCPs,” Dr. Carey said.
He voiced interest in working on this with the American College of Physicians, which represents U.S. internal medicine physicians, and the American Academy of Family Physicians.
“We definitely need a partnership and educational efforts to get the word out from these organizations and not from a specialty society,” said Dr. Carey.
Dr. Funder said he has submitted a proposal to the Endocrine Society for a guidelines update he would chair with Dr. Carey’s assistance and with a diverse writing group that includes PCPs. Dr. Carey said that ideally this panel would write and release a revised guideline in 2021.
“Several of us are chomping at the bit to get this done,” he noted.
But participation by the ACP and AAFP remain uncertain as of September 2020. When approached about this, an ACP spokesperson said the organization had no comment. A spokesperson for the AAFP said, “It’s too early to tell if we will partner with any other organizations to develop guidelines specific to excess aldosterone, and how such guidelines might be received by our members.”
Recent history shows little cooperation between ACP, AAFP, and what might be termed the U.S. hypertension “establishment.” For example, when the American College of Cardiology and the American Heart Association released their most recent essential hypertension management guidelines in Hypertension in 2018, it was never adopted by ACP or AAFP.
The latter two organizations continue to endorse a higher BP threshold for diagnosing hypertension, and higher treatment targets set by alternative expert panels to those of the AHA/ACC.
Collaboration feasible, although PCPs overworked
Dr. Carey hopes that this episode will not preclude agreement over PA screening.
“I think it is still possible to partner with [the ACP and AAFP],” he observed, adding that he believes high PA prevalence among hypertensive patients and its consequences when unrecognized is “noncontentious.”
But he acknowledges that other, substantial hurdles also exist, notably the “overwhelming workload” that American PCPs already face.
David O’Gurek, MD, a family and community medicine physician at the Lewis Katz School of Medicine of Temple University in Philadelphia, agrees that a revamped approach to PA screening developed cooperatively between PCPs and specialists is an important goal and potentially feasible despite prior disagreements. “There has to be room for collaboration,” he said, but also emphasized the need for developing policies based on a systematic evidence review and a focus on patient-centered outcomes.
“We’re certainly missing patients with PA, but there needs to be greater clarity and standardization about the most appropriate screening approach and cutoff level” for flagging patients who need specialized assessment, Dr. O’Gurek said in an interview.
The current endocrinology literature also shows that experts remain divided on how best to accomplish this.
And some hypertension specialists question whether existing evidence is conclusive enough to warrant revised guidelines.
Dr. Cohen, the nephrologist and hypertension researcher, said that, while the recent prevalence report in Annals of Internal Medicine is “intriguing, hypothesis-generating information that suggests we are missing many cases of hyperaldosteronism in routine care,” she nevertheless believes that “we need additional data to be able to truly understand the breadth and implications of the findings.”
William C. Cushman, MD, a hypertension management specialist at the University of Tennessee Health Science Center in Memphis, agrees.
Changing existing practice guidelines “really needs randomized, controlled trials demonstrating a difference in long-term outcomes, ideally major cardiovascular outcomes,” that result from broader PA screening, he said.
Dr. Carey concurs that more evidence is needed to confirm the Annals report, but is confident this evidence will be in hand by the time a guideline-revision panel meets in 2021.
Australian model of PCPs screening for PA could be implemented in United States
An example of what might be possible when PCPs, endocrinologists, and hypertension specialists work together to make PA screening more accessible can be found in Melbourne, at the Endocrine Hypertension Service of Monash Health, in association with the Hudson Institute of Medical Research.
This began operating in July 2016, cofounded by Dr. Yang, whose experiences with her own father made her sensitive to the issue.
The service’s aim is to “address the underdiagnosis of PA, and to offer a streamlined diagnostic service for patients with hypertension,” with an “extensive outreach program” targeted to regional PCPs that, among other messages, encourages them to screen patients for PA when blood pressures exceed 140/90 mm Hg.
During its first 3 years of operation, the service saw 267 patients, with PA diagnosed in 135 and ruled out in 73 patients.
Notably, the proportion of these patients referred from PCPs jumped from 21% of 70 patients during the first year of operation to 47% of 70 patients during year 2, and 52% of 127 patients during the third year, ending in July 2019, said Dr. Yang, who continues to help run the service.
During the first year, a scant 3% of referred patients had recently diagnosed hypertension, but this rose to 14% during the second year, and to 19% during the most recent year with data available.
The median duration of diagnosed hypertension among referred patients fell from 11 years during year 1, to 7 years during year 3.
Service clinicians diagnosed 37 patients with unilateral adenomas, and removed them from 23 patients with four more awaiting surgery and the remaining 10 opting instead for medical management. Another 95 patients went on therapy with a MRA, and during the most recent year studied all patients who began a MRA regimen had a partial or complete clinical response.
Dr. Carey said the “creative program represents a model for implementation in U.S. practice.
Dr. Funder, Dr. Carey, Dr. Feldman, Dr. Yang, Dr. Cohen, and Dr. O’Gurek had no relevant disclosures. Dr. Cushman has been a consultant to Novartis, received personal fees from Sanofi, and research funding from Eli Lilly.
Jun Yang, MBBS, had watched as her father, who had battled hypertension for decades, ended up on four medications that still couldn’t bring his blood pressure to a healthy level. The cardiovascular endocrinologist then ran some tests, and soon thereafter her father had his blood pressure optimized on just one targeted medication.
Dr. Yang’s father was found to have a hormonal condition known as primary aldosteronism (PA) as the cause of his hypertension.
It turns out that PA is not as rare as once thought.
An eye-catching report in Annals of Internal Medicine this spring of an unexpectedly high prevalence of primary aldosteronism among a diverse cross section of U.S. patients with hypertension has raised issues that could dramatically change the way doctors in America, and elsewhere, assess and manage high blood pressure.
Foremost is the question of whether primary care physicians – the clinicians at the front line for diagnosing and initially treating most patients with hypertension – will absorb and act on this new evidence. For them, aldosteronism doesn’t automatically come to mind when they see high numbers on a BP monitor, and yet this latest research found that up to a third of all 726 patients in the study who were diagnosed with hypertension and with high urinary salt levels had PA.
That translates to a roughly three- to fivefold increase over standard prevalence estimates, and is a ”game changer” for how clinicians should approach hypertension management and PA diagnosis going forward, said John W. Funder, MD, in an editorial accompanying the Annals study.
Long considered relatively uncommon, hypertension driven by an excess of the hormone aldosterone, often because of an adenoma on the adrenal gland, is not the same as conventional “essential” hypertension. The former benefits from early diagnosis because its treatment is completely different – close to half of all PA patients can be treated definitively and quickly with surgical removal of an adenoma from one side of the adrenal gland.
For other PA patients, who have bilateral adrenal hyperplasia that is impossible to resolve surgically, treatment with drugs called mineralocorticoid receptor antagonists (MRAs), such as spironolactone, is needed because they target the hormonal cause of the high BP.
But what usually happens is that a patient with PA is mistakenly diagnosed with essential hypertension, in which the classic approach to treatment is to start with one regular antihypertensive drug, and add on further ones from different drug classes if blood pressure is not adequately controlled. When patients are taking three drugs, without adequate control, they are labeled as having “resistant hypertension.”
But in the case of PA, none of these conventional antihypertensives work, and the process of continuing to monitor and add different drugs wastes time, during which patients deteriorate.
“We need to change the culture of waiting for hypertension to be resistant and have patients riddled with end-organ damage,” due to years of persistently high BP and excess aldosterone “before we look for a secondary cause” like PA, declared Dr. Yang, of Hudson Institute of Medical Research and Monash University in Melbourne, during an interview.
So early diagnosis and prompt treatment of PA is key.
In addition to boosting the public health importance of early PA detection in hypertensive patients, the new up-sized PA prevalence numbers throw a spotlight on primary care physicians (PCPs) as key players who will need to apply the findings to practice on a public health scale.
These novel results create a need for “new guidelines, and a radically revised game plan with the key role of PCPs” emphasized in future management of patients with hypertension, said Dr. Funder, a professor of medicine at Monash University, in a second recent editorial in Hypertension.
“Buy-in by PCPs is essential,” agrees Robert M. Carey, MD, a cardiovascular endocrinologist and professor of medicine at the University of Virginia in Charlottesville, and a coauthor of the new study.
But he too acknowledges that this presents a major challenge. PCPs and internists, who diagnose a lot of hypertension, are “not used to thinking about aldosterone,” he said in an interview, encapsulating the key problem faced by proponents of earlier and more widespread PA assessment.
This dilemma looms as a “huge public health issue,” Dr. Carey warned.
‘We’re a long way from getting’ PCPs to buy in to PA screening
Will PCPs grow more comfortable with screening patients for PA themselves, or might they become more willing to refer hypertensive individuals for assessment at an expert center?
One skeptic is Ross D. Feldman, MD, a hypertension-management researcher and professor of medicine at the University of Manitoba in Winnipeg. The finding about high PA prevalence in patients with hypertension “is brand new, [and] the message needs to get to PCPs,” he said. But, “We’re a long way from getting it” to them. “I don’t know how to do that. It will be a tough sell.”
In addition, repositioning MRAs as an earlier option for many hypertensive patients won’t be easy either, because “we’ll never have outcome-trial data for MRAs,” given that they are now generic drugs, he noted.
“No clinical trial data show [MRAs] are first-line drugs,” said Dr. Feldman, who explained that, instead, MRAs are considered “go-to drugs” for patients with treatment-resistant hypertension, a niche therapeutic area. Results from the PATHWAY-2 trial published 5 years ago in Lancet showed “spironolactone was clearly the most effective treatment for the condition,” according to the report authors.
But even among patients with resistant hypertension, screening for PA dramatically lags despite being enshrined in guidelines.
“PCPs should start checking aldosterone-to-renin ratios [a widely used PA screen] in all patients with resistant hypertension or hypertension with hypokalemia, and then refer patients to specialists for testing and management,” said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia.
But recent studies of U.S. patient populations with clinical characteristics that meet existing criteria for PA screening showed that just 1%-2% of these individuals underwent an initial PA assessment, she noted, citing reports in the journals Surgery and Hypertension.
“We need to prioritize improving screening in these high-risk patients,” she stressed in an interview.
This illustrates that, in some respects, the new prevalence numbers are beside the point, because PA has been going unscreened and overlooked far too often even in the context of historical, lower prevalence rates, said Dr. Yang.
“The key point is that approximately 1 in 10 people with hypertension, and even more with resistant hypertension, have a form of the disease that is worse than essential hypertension but is routinely missed at present” and is also highly treatable.
“Evidence for the need for increased awareness of PA has been building for 2 decades,” stressed Dr. Yang, who has coauthored several commentaries and reviews that have bemoaned PA’s underappreciated status.
Interest in partnering with PCPs on guidance grows
One potential solution is to have endocrinologists and hypertension specialists’ partner with PCPs to come up with diagnostic and management recommendations. Both Dr. Funder and Dr. Carey are opinion leaders regarding the role of aldosterone in hypertension, and both were coauthors of the 2016 Endocrine Society guideline for PA assessment and management published in the Journal of Clinical Endocrinology & Metabolism , with Dr. Funder chairing the writing panel.
Now approaching its fifth year in effect, this guideline is “due for revision,” and “my hope is that we’ll be able to partner with one or more PCP organizations to come up with a version of the guideline targeted to PCPs,” Dr. Carey said.
He voiced interest in working on this with the American College of Physicians, which represents U.S. internal medicine physicians, and the American Academy of Family Physicians.
“We definitely need a partnership and educational efforts to get the word out from these organizations and not from a specialty society,” said Dr. Carey.
Dr. Funder said he has submitted a proposal to the Endocrine Society for a guidelines update he would chair with Dr. Carey’s assistance and with a diverse writing group that includes PCPs. Dr. Carey said that ideally this panel would write and release a revised guideline in 2021.
“Several of us are chomping at the bit to get this done,” he noted.
But participation by the ACP and AAFP remain uncertain as of September 2020. When approached about this, an ACP spokesperson said the organization had no comment. A spokesperson for the AAFP said, “It’s too early to tell if we will partner with any other organizations to develop guidelines specific to excess aldosterone, and how such guidelines might be received by our members.”
Recent history shows little cooperation between ACP, AAFP, and what might be termed the U.S. hypertension “establishment.” For example, when the American College of Cardiology and the American Heart Association released their most recent essential hypertension management guidelines in Hypertension in 2018, it was never adopted by ACP or AAFP.
The latter two organizations continue to endorse a higher BP threshold for diagnosing hypertension, and higher treatment targets set by alternative expert panels to those of the AHA/ACC.
Collaboration feasible, although PCPs overworked
Dr. Carey hopes that this episode will not preclude agreement over PA screening.
“I think it is still possible to partner with [the ACP and AAFP],” he observed, adding that he believes high PA prevalence among hypertensive patients and its consequences when unrecognized is “noncontentious.”
But he acknowledges that other, substantial hurdles also exist, notably the “overwhelming workload” that American PCPs already face.
David O’Gurek, MD, a family and community medicine physician at the Lewis Katz School of Medicine of Temple University in Philadelphia, agrees that a revamped approach to PA screening developed cooperatively between PCPs and specialists is an important goal and potentially feasible despite prior disagreements. “There has to be room for collaboration,” he said, but also emphasized the need for developing policies based on a systematic evidence review and a focus on patient-centered outcomes.
“We’re certainly missing patients with PA, but there needs to be greater clarity and standardization about the most appropriate screening approach and cutoff level” for flagging patients who need specialized assessment, Dr. O’Gurek said in an interview.
The current endocrinology literature also shows that experts remain divided on how best to accomplish this.
And some hypertension specialists question whether existing evidence is conclusive enough to warrant revised guidelines.
Dr. Cohen, the nephrologist and hypertension researcher, said that, while the recent prevalence report in Annals of Internal Medicine is “intriguing, hypothesis-generating information that suggests we are missing many cases of hyperaldosteronism in routine care,” she nevertheless believes that “we need additional data to be able to truly understand the breadth and implications of the findings.”
William C. Cushman, MD, a hypertension management specialist at the University of Tennessee Health Science Center in Memphis, agrees.
Changing existing practice guidelines “really needs randomized, controlled trials demonstrating a difference in long-term outcomes, ideally major cardiovascular outcomes,” that result from broader PA screening, he said.
Dr. Carey concurs that more evidence is needed to confirm the Annals report, but is confident this evidence will be in hand by the time a guideline-revision panel meets in 2021.
Australian model of PCPs screening for PA could be implemented in United States
An example of what might be possible when PCPs, endocrinologists, and hypertension specialists work together to make PA screening more accessible can be found in Melbourne, at the Endocrine Hypertension Service of Monash Health, in association with the Hudson Institute of Medical Research.
This began operating in July 2016, cofounded by Dr. Yang, whose experiences with her own father made her sensitive to the issue.
The service’s aim is to “address the underdiagnosis of PA, and to offer a streamlined diagnostic service for patients with hypertension,” with an “extensive outreach program” targeted to regional PCPs that, among other messages, encourages them to screen patients for PA when blood pressures exceed 140/90 mm Hg.
During its first 3 years of operation, the service saw 267 patients, with PA diagnosed in 135 and ruled out in 73 patients.
Notably, the proportion of these patients referred from PCPs jumped from 21% of 70 patients during the first year of operation to 47% of 70 patients during year 2, and 52% of 127 patients during the third year, ending in July 2019, said Dr. Yang, who continues to help run the service.
During the first year, a scant 3% of referred patients had recently diagnosed hypertension, but this rose to 14% during the second year, and to 19% during the most recent year with data available.
The median duration of diagnosed hypertension among referred patients fell from 11 years during year 1, to 7 years during year 3.
Service clinicians diagnosed 37 patients with unilateral adenomas, and removed them from 23 patients with four more awaiting surgery and the remaining 10 opting instead for medical management. Another 95 patients went on therapy with a MRA, and during the most recent year studied all patients who began a MRA regimen had a partial or complete clinical response.
Dr. Carey said the “creative program represents a model for implementation in U.S. practice.
Dr. Funder, Dr. Carey, Dr. Feldman, Dr. Yang, Dr. Cohen, and Dr. O’Gurek had no relevant disclosures. Dr. Cushman has been a consultant to Novartis, received personal fees from Sanofi, and research funding from Eli Lilly.
Jun Yang, MBBS, had watched as her father, who had battled hypertension for decades, ended up on four medications that still couldn’t bring his blood pressure to a healthy level. The cardiovascular endocrinologist then ran some tests, and soon thereafter her father had his blood pressure optimized on just one targeted medication.
Dr. Yang’s father was found to have a hormonal condition known as primary aldosteronism (PA) as the cause of his hypertension.
It turns out that PA is not as rare as once thought.
An eye-catching report in Annals of Internal Medicine this spring of an unexpectedly high prevalence of primary aldosteronism among a diverse cross section of U.S. patients with hypertension has raised issues that could dramatically change the way doctors in America, and elsewhere, assess and manage high blood pressure.
Foremost is the question of whether primary care physicians – the clinicians at the front line for diagnosing and initially treating most patients with hypertension – will absorb and act on this new evidence. For them, aldosteronism doesn’t automatically come to mind when they see high numbers on a BP monitor, and yet this latest research found that up to a third of all 726 patients in the study who were diagnosed with hypertension and with high urinary salt levels had PA.
That translates to a roughly three- to fivefold increase over standard prevalence estimates, and is a ”game changer” for how clinicians should approach hypertension management and PA diagnosis going forward, said John W. Funder, MD, in an editorial accompanying the Annals study.
Long considered relatively uncommon, hypertension driven by an excess of the hormone aldosterone, often because of an adenoma on the adrenal gland, is not the same as conventional “essential” hypertension. The former benefits from early diagnosis because its treatment is completely different – close to half of all PA patients can be treated definitively and quickly with surgical removal of an adenoma from one side of the adrenal gland.
For other PA patients, who have bilateral adrenal hyperplasia that is impossible to resolve surgically, treatment with drugs called mineralocorticoid receptor antagonists (MRAs), such as spironolactone, is needed because they target the hormonal cause of the high BP.
But what usually happens is that a patient with PA is mistakenly diagnosed with essential hypertension, in which the classic approach to treatment is to start with one regular antihypertensive drug, and add on further ones from different drug classes if blood pressure is not adequately controlled. When patients are taking three drugs, without adequate control, they are labeled as having “resistant hypertension.”
But in the case of PA, none of these conventional antihypertensives work, and the process of continuing to monitor and add different drugs wastes time, during which patients deteriorate.
“We need to change the culture of waiting for hypertension to be resistant and have patients riddled with end-organ damage,” due to years of persistently high BP and excess aldosterone “before we look for a secondary cause” like PA, declared Dr. Yang, of Hudson Institute of Medical Research and Monash University in Melbourne, during an interview.
So early diagnosis and prompt treatment of PA is key.
In addition to boosting the public health importance of early PA detection in hypertensive patients, the new up-sized PA prevalence numbers throw a spotlight on primary care physicians (PCPs) as key players who will need to apply the findings to practice on a public health scale.
These novel results create a need for “new guidelines, and a radically revised game plan with the key role of PCPs” emphasized in future management of patients with hypertension, said Dr. Funder, a professor of medicine at Monash University, in a second recent editorial in Hypertension.
“Buy-in by PCPs is essential,” agrees Robert M. Carey, MD, a cardiovascular endocrinologist and professor of medicine at the University of Virginia in Charlottesville, and a coauthor of the new study.
But he too acknowledges that this presents a major challenge. PCPs and internists, who diagnose a lot of hypertension, are “not used to thinking about aldosterone,” he said in an interview, encapsulating the key problem faced by proponents of earlier and more widespread PA assessment.
This dilemma looms as a “huge public health issue,” Dr. Carey warned.
‘We’re a long way from getting’ PCPs to buy in to PA screening
Will PCPs grow more comfortable with screening patients for PA themselves, or might they become more willing to refer hypertensive individuals for assessment at an expert center?
One skeptic is Ross D. Feldman, MD, a hypertension-management researcher and professor of medicine at the University of Manitoba in Winnipeg. The finding about high PA prevalence in patients with hypertension “is brand new, [and] the message needs to get to PCPs,” he said. But, “We’re a long way from getting it” to them. “I don’t know how to do that. It will be a tough sell.”
In addition, repositioning MRAs as an earlier option for many hypertensive patients won’t be easy either, because “we’ll never have outcome-trial data for MRAs,” given that they are now generic drugs, he noted.
“No clinical trial data show [MRAs] are first-line drugs,” said Dr. Feldman, who explained that, instead, MRAs are considered “go-to drugs” for patients with treatment-resistant hypertension, a niche therapeutic area. Results from the PATHWAY-2 trial published 5 years ago in Lancet showed “spironolactone was clearly the most effective treatment for the condition,” according to the report authors.
But even among patients with resistant hypertension, screening for PA dramatically lags despite being enshrined in guidelines.
“PCPs should start checking aldosterone-to-renin ratios [a widely used PA screen] in all patients with resistant hypertension or hypertension with hypokalemia, and then refer patients to specialists for testing and management,” said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia.
But recent studies of U.S. patient populations with clinical characteristics that meet existing criteria for PA screening showed that just 1%-2% of these individuals underwent an initial PA assessment, she noted, citing reports in the journals Surgery and Hypertension.
“We need to prioritize improving screening in these high-risk patients,” she stressed in an interview.
This illustrates that, in some respects, the new prevalence numbers are beside the point, because PA has been going unscreened and overlooked far too often even in the context of historical, lower prevalence rates, said Dr. Yang.
“The key point is that approximately 1 in 10 people with hypertension, and even more with resistant hypertension, have a form of the disease that is worse than essential hypertension but is routinely missed at present” and is also highly treatable.
“Evidence for the need for increased awareness of PA has been building for 2 decades,” stressed Dr. Yang, who has coauthored several commentaries and reviews that have bemoaned PA’s underappreciated status.
Interest in partnering with PCPs on guidance grows
One potential solution is to have endocrinologists and hypertension specialists’ partner with PCPs to come up with diagnostic and management recommendations. Both Dr. Funder and Dr. Carey are opinion leaders regarding the role of aldosterone in hypertension, and both were coauthors of the 2016 Endocrine Society guideline for PA assessment and management published in the Journal of Clinical Endocrinology & Metabolism , with Dr. Funder chairing the writing panel.
Now approaching its fifth year in effect, this guideline is “due for revision,” and “my hope is that we’ll be able to partner with one or more PCP organizations to come up with a version of the guideline targeted to PCPs,” Dr. Carey said.
He voiced interest in working on this with the American College of Physicians, which represents U.S. internal medicine physicians, and the American Academy of Family Physicians.
“We definitely need a partnership and educational efforts to get the word out from these organizations and not from a specialty society,” said Dr. Carey.
Dr. Funder said he has submitted a proposal to the Endocrine Society for a guidelines update he would chair with Dr. Carey’s assistance and with a diverse writing group that includes PCPs. Dr. Carey said that ideally this panel would write and release a revised guideline in 2021.
“Several of us are chomping at the bit to get this done,” he noted.
But participation by the ACP and AAFP remain uncertain as of September 2020. When approached about this, an ACP spokesperson said the organization had no comment. A spokesperson for the AAFP said, “It’s too early to tell if we will partner with any other organizations to develop guidelines specific to excess aldosterone, and how such guidelines might be received by our members.”
Recent history shows little cooperation between ACP, AAFP, and what might be termed the U.S. hypertension “establishment.” For example, when the American College of Cardiology and the American Heart Association released their most recent essential hypertension management guidelines in Hypertension in 2018, it was never adopted by ACP or AAFP.
The latter two organizations continue to endorse a higher BP threshold for diagnosing hypertension, and higher treatment targets set by alternative expert panels to those of the AHA/ACC.
Collaboration feasible, although PCPs overworked
Dr. Carey hopes that this episode will not preclude agreement over PA screening.
“I think it is still possible to partner with [the ACP and AAFP],” he observed, adding that he believes high PA prevalence among hypertensive patients and its consequences when unrecognized is “noncontentious.”
But he acknowledges that other, substantial hurdles also exist, notably the “overwhelming workload” that American PCPs already face.
David O’Gurek, MD, a family and community medicine physician at the Lewis Katz School of Medicine of Temple University in Philadelphia, agrees that a revamped approach to PA screening developed cooperatively between PCPs and specialists is an important goal and potentially feasible despite prior disagreements. “There has to be room for collaboration,” he said, but also emphasized the need for developing policies based on a systematic evidence review and a focus on patient-centered outcomes.
“We’re certainly missing patients with PA, but there needs to be greater clarity and standardization about the most appropriate screening approach and cutoff level” for flagging patients who need specialized assessment, Dr. O’Gurek said in an interview.
The current endocrinology literature also shows that experts remain divided on how best to accomplish this.
And some hypertension specialists question whether existing evidence is conclusive enough to warrant revised guidelines.
Dr. Cohen, the nephrologist and hypertension researcher, said that, while the recent prevalence report in Annals of Internal Medicine is “intriguing, hypothesis-generating information that suggests we are missing many cases of hyperaldosteronism in routine care,” she nevertheless believes that “we need additional data to be able to truly understand the breadth and implications of the findings.”
William C. Cushman, MD, a hypertension management specialist at the University of Tennessee Health Science Center in Memphis, agrees.
Changing existing practice guidelines “really needs randomized, controlled trials demonstrating a difference in long-term outcomes, ideally major cardiovascular outcomes,” that result from broader PA screening, he said.
Dr. Carey concurs that more evidence is needed to confirm the Annals report, but is confident this evidence will be in hand by the time a guideline-revision panel meets in 2021.
Australian model of PCPs screening for PA could be implemented in United States
An example of what might be possible when PCPs, endocrinologists, and hypertension specialists work together to make PA screening more accessible can be found in Melbourne, at the Endocrine Hypertension Service of Monash Health, in association with the Hudson Institute of Medical Research.
This began operating in July 2016, cofounded by Dr. Yang, whose experiences with her own father made her sensitive to the issue.
The service’s aim is to “address the underdiagnosis of PA, and to offer a streamlined diagnostic service for patients with hypertension,” with an “extensive outreach program” targeted to regional PCPs that, among other messages, encourages them to screen patients for PA when blood pressures exceed 140/90 mm Hg.
During its first 3 years of operation, the service saw 267 patients, with PA diagnosed in 135 and ruled out in 73 patients.
Notably, the proportion of these patients referred from PCPs jumped from 21% of 70 patients during the first year of operation to 47% of 70 patients during year 2, and 52% of 127 patients during the third year, ending in July 2019, said Dr. Yang, who continues to help run the service.
During the first year, a scant 3% of referred patients had recently diagnosed hypertension, but this rose to 14% during the second year, and to 19% during the most recent year with data available.
The median duration of diagnosed hypertension among referred patients fell from 11 years during year 1, to 7 years during year 3.
Service clinicians diagnosed 37 patients with unilateral adenomas, and removed them from 23 patients with four more awaiting surgery and the remaining 10 opting instead for medical management. Another 95 patients went on therapy with a MRA, and during the most recent year studied all patients who began a MRA regimen had a partial or complete clinical response.
Dr. Carey said the “creative program represents a model for implementation in U.S. practice.
Dr. Funder, Dr. Carey, Dr. Feldman, Dr. Yang, Dr. Cohen, and Dr. O’Gurek had no relevant disclosures. Dr. Cushman has been a consultant to Novartis, received personal fees from Sanofi, and research funding from Eli Lilly.