User login
Dual HER2 targeting benefits OS of patients with advanced breast cancer
Adding pertuzumab to trastuzumab and docetaxel for treatment of HER2-positive metastatic breast cancer was more effective than adding a placebo to trastuzumab plus chemotherapy, according to Dr. Sandra M. Swain and her associates.

The median overall survival rate for the pertuzumab combination group was 56.5 months, while median survival time in the placebo group was 40.8 months. Median progression-free survival increased by 6.3 months, and the median duration of response was increased by 7.7 months. No significant difference in adverse events was found between the two groups.
While the results were promising, most of the deaths in the study were from breast cancer, indicating that better treatments are still needed. It is also “not clear whether hormonal therapy plus pertuzumab and trastuzumab is more effective than hormonal therapy plus trastuzumab alone in patients,” the investigators said.
Find the full study in the New England Journal of Medicine 2015;372:724-34 (doi:10.1056/NEJMoa1413513).
Adding pertuzumab to trastuzumab and docetaxel for treatment of HER2-positive metastatic breast cancer was more effective than adding a placebo to trastuzumab plus chemotherapy, according to Dr. Sandra M. Swain and her associates.
The median overall survival rate for the pertuzumab combination group was 56.5 months, while median survival time in the placebo group was 40.8 months. Median progression-free survival increased by 6.3 months, and the median duration of response was increased by 7.7 months. No significant difference in adverse events was found between the two groups.
While the results were promising, most of the deaths in the study were from breast cancer, indicating that better treatments are still needed. It is also “not clear whether hormonal therapy plus pertuzumab and trastuzumab is more effective than hormonal therapy plus trastuzumab alone in patients,” the investigators said.
Find the full study in the New England Journal of Medicine 2015;372:724-34 (doi:10.1056/NEJMoa1413513).
Adding pertuzumab to trastuzumab and docetaxel for treatment of HER2-positive metastatic breast cancer was more effective than adding a placebo to trastuzumab plus chemotherapy, according to Dr. Sandra M. Swain and her associates.
The median overall survival rate for the pertuzumab combination group was 56.5 months, while median survival time in the placebo group was 40.8 months. Median progression-free survival increased by 6.3 months, and the median duration of response was increased by 7.7 months. No significant difference in adverse events was found between the two groups.
While the results were promising, most of the deaths in the study were from breast cancer, indicating that better treatments are still needed. It is also “not clear whether hormonal therapy plus pertuzumab and trastuzumab is more effective than hormonal therapy plus trastuzumab alone in patients,” the investigators said.
Find the full study in the New England Journal of Medicine 2015;372:724-34 (doi:10.1056/NEJMoa1413513).

Perceptions about participation in cancer clinical trials in New York state
Background Clinical trials are valuable in advancing cancer care through the investigation of ways in which to better prevent, detect and diagnose, and/or treat cancer. Recruitment of adults into clinical trials has historically been low.
Objective To survey adult cancer patients who reside in New York state to better understand their participation in and attitudes about clinical trials.
Methods From January 2012-April 2013, we conducted a one-time survey about clinical trials in 8 cancer-treatment or cancer-patient support organizations in the state. Surveys were offered in person and online to adults with a past or current cancer diagnosis. Analysis was limited to adults who resided in the state and provided a self-reported status of previous participation in clinical trials.
Results Of the 1,832 participants who completed the survey, 1,475 were included in the analysis. Our sample represented all regions of the state. Most of the respondents (68.1%) had never participated in a clinical trial. Almost 32% said they had never received information about research studies. Most (84%) felt that patients should be asked to participate in clinical trials, but fewer (70%) were willing to be approached about participation.
Limitations The sample is predominantly white and female and overrepresents breast and hematologic cancers.
Conclusions Increased outreach coupled with a team approach to educate and enroll patients in clinical trials may be the necessary first steps to increase participation in trials and ensure a diverse sample of participants.
Click on the PDF icon at the top of this introduction to read the full article.
Background Clinical trials are valuable in advancing cancer care through the investigation of ways in which to better prevent, detect and diagnose, and/or treat cancer. Recruitment of adults into clinical trials has historically been low.
Objective To survey adult cancer patients who reside in New York state to better understand their participation in and attitudes about clinical trials.
Methods From January 2012-April 2013, we conducted a one-time survey about clinical trials in 8 cancer-treatment or cancer-patient support organizations in the state. Surveys were offered in person and online to adults with a past or current cancer diagnosis. Analysis was limited to adults who resided in the state and provided a self-reported status of previous participation in clinical trials.
Results Of the 1,832 participants who completed the survey, 1,475 were included in the analysis. Our sample represented all regions of the state. Most of the respondents (68.1%) had never participated in a clinical trial. Almost 32% said they had never received information about research studies. Most (84%) felt that patients should be asked to participate in clinical trials, but fewer (70%) were willing to be approached about participation.
Limitations The sample is predominantly white and female and overrepresents breast and hematologic cancers.
Conclusions Increased outreach coupled with a team approach to educate and enroll patients in clinical trials may be the necessary first steps to increase participation in trials and ensure a diverse sample of participants.
Click on the PDF icon at the top of this introduction to read the full article.
Background Clinical trials are valuable in advancing cancer care through the investigation of ways in which to better prevent, detect and diagnose, and/or treat cancer. Recruitment of adults into clinical trials has historically been low.
Objective To survey adult cancer patients who reside in New York state to better understand their participation in and attitudes about clinical trials.
Methods From January 2012-April 2013, we conducted a one-time survey about clinical trials in 8 cancer-treatment or cancer-patient support organizations in the state. Surveys were offered in person and online to adults with a past or current cancer diagnosis. Analysis was limited to adults who resided in the state and provided a self-reported status of previous participation in clinical trials.
Results Of the 1,832 participants who completed the survey, 1,475 were included in the analysis. Our sample represented all regions of the state. Most of the respondents (68.1%) had never participated in a clinical trial. Almost 32% said they had never received information about research studies. Most (84%) felt that patients should be asked to participate in clinical trials, but fewer (70%) were willing to be approached about participation.
Limitations The sample is predominantly white and female and overrepresents breast and hematologic cancers.
Conclusions Increased outreach coupled with a team approach to educate and enroll patients in clinical trials may be the necessary first steps to increase participation in trials and ensure a diverse sample of participants.
Click on the PDF icon at the top of this introduction to read the full article.
Joint breast and colorectal cancer screenings in medically underserved women
Background Breast and colon cancer screening in rural community clinics is underused.
Objective To evaluate the effectiveness and cost-effectiveness of alternative interventions designed to promote simultaneous screening for breast and colon cancer in community clinics.
Methods A 3-arm, quasi-experimental evaluation was conducted during May 2008-August 2011 in 8 federally qualified health clinics in predominately rural Louisiana. Baseline screening rates reported by the clinics was <10% for breast cancer (using mammography) and 1%- 2% for colon cancer (using the fecal occult blood test [FOBT]). 744 women aged 50 years or older who were eligible for routine mammography and an FOBT were recruited. The combined screening efforts included: enhanced care; health literacy-informed education (education alone), or health literacy-informed education with nurse support (nurse support).
Results Postintervention screening rates for completing both tests were 28.1% with enhanced care, 23.7% with education alone, and 38.7% with nurse support. After adjusting for age, race, and literacy, patients who received nurse support were 2.21 times more likely to complete both screenings than were those who received the education alone (95% confidence interval [CI], 1.12-4.38; P = .023). The incremental cost per additional woman completing both screenings was $3,987 for education with nurse support over education alone, and $5,987 over enhanced care.
Limitations There were differences between the 3 arms in sociodemographic characteristics, literacy, and previous screening history. Not all variables that were significantly different between arms were adjusted for, therefore adjustments for key variables (age, race, literacy) were made in statistical analyses. Other limitations related generalizability of results.
Conclusions Although joint breast and colon cancer screening rates were increased substantially over existing baseline rates in all 3 arms, the completion rate for both tests was modest. Nurse support and telephone follow-up were most effective. However, it is not likely to be cost effective or affordable in clinics with limited resources.
Funding National Cancer Institute (R01-CA115869-05), supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health.
Click on the PDF icon at the top of this introduction to read the full article.
Background Breast and colon cancer screening in rural community clinics is underused.
Objective To evaluate the effectiveness and cost-effectiveness of alternative interventions designed to promote simultaneous screening for breast and colon cancer in community clinics.
Methods A 3-arm, quasi-experimental evaluation was conducted during May 2008-August 2011 in 8 federally qualified health clinics in predominately rural Louisiana. Baseline screening rates reported by the clinics was <10% for breast cancer (using mammography) and 1%- 2% for colon cancer (using the fecal occult blood test [FOBT]). 744 women aged 50 years or older who were eligible for routine mammography and an FOBT were recruited. The combined screening efforts included: enhanced care; health literacy-informed education (education alone), or health literacy-informed education with nurse support (nurse support).
Results Postintervention screening rates for completing both tests were 28.1% with enhanced care, 23.7% with education alone, and 38.7% with nurse support. After adjusting for age, race, and literacy, patients who received nurse support were 2.21 times more likely to complete both screenings than were those who received the education alone (95% confidence interval [CI], 1.12-4.38; P = .023). The incremental cost per additional woman completing both screenings was $3,987 for education with nurse support over education alone, and $5,987 over enhanced care.
Limitations There were differences between the 3 arms in sociodemographic characteristics, literacy, and previous screening history. Not all variables that were significantly different between arms were adjusted for, therefore adjustments for key variables (age, race, literacy) were made in statistical analyses. Other limitations related generalizability of results.
Conclusions Although joint breast and colon cancer screening rates were increased substantially over existing baseline rates in all 3 arms, the completion rate for both tests was modest. Nurse support and telephone follow-up were most effective. However, it is not likely to be cost effective or affordable in clinics with limited resources.
Funding National Cancer Institute (R01-CA115869-05), supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health.
Click on the PDF icon at the top of this introduction to read the full article.
Background Breast and colon cancer screening in rural community clinics is underused.
Objective To evaluate the effectiveness and cost-effectiveness of alternative interventions designed to promote simultaneous screening for breast and colon cancer in community clinics.
Methods A 3-arm, quasi-experimental evaluation was conducted during May 2008-August 2011 in 8 federally qualified health clinics in predominately rural Louisiana. Baseline screening rates reported by the clinics was <10% for breast cancer (using mammography) and 1%- 2% for colon cancer (using the fecal occult blood test [FOBT]). 744 women aged 50 years or older who were eligible for routine mammography and an FOBT were recruited. The combined screening efforts included: enhanced care; health literacy-informed education (education alone), or health literacy-informed education with nurse support (nurse support).
Results Postintervention screening rates for completing both tests were 28.1% with enhanced care, 23.7% with education alone, and 38.7% with nurse support. After adjusting for age, race, and literacy, patients who received nurse support were 2.21 times more likely to complete both screenings than were those who received the education alone (95% confidence interval [CI], 1.12-4.38; P = .023). The incremental cost per additional woman completing both screenings was $3,987 for education with nurse support over education alone, and $5,987 over enhanced care.
Limitations There were differences between the 3 arms in sociodemographic characteristics, literacy, and previous screening history. Not all variables that were significantly different between arms were adjusted for, therefore adjustments for key variables (age, race, literacy) were made in statistical analyses. Other limitations related generalizability of results.
Conclusions Although joint breast and colon cancer screening rates were increased substantially over existing baseline rates in all 3 arms, the completion rate for both tests was modest. Nurse support and telephone follow-up were most effective. However, it is not likely to be cost effective or affordable in clinics with limited resources.
Funding National Cancer Institute (R01-CA115869-05), supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health.
Click on the PDF icon at the top of this introduction to read the full article.
Bevacizumab plus ET failed to improve PFS in HER2-negative, HR-positive BC
First-line treatment with endocrine therapy plus bevacizumab did not significantly improve PFS compared with endocrine therapy alone for postmenopausal women with hormone receptor–positive, HER2-negative advanced breast cancer, according to results from a multicenter phase III trial published online Feb. 17 in Journal of Clinical Oncology.
Furthermore, patients taking endocrine therapy plus bevacizumab (ET-B) had significantly more adverse events.
“On the basis of this particular trial and in light of the higher toxicity, ET-B should not be recommended in the treatment of advanced hormone receptor-positive/HER2-negative breast cancer,” wrote Dr. Miguel Martín of Universidad Complutense de Madrid and his associates (J. Clin. Oncol. 2015 Feb. 17 [doi:10.1200/JCO.2014.57.2388]).
Previous studies have shown overexpression of VEGF in breast cancer and that high VEGF levels are associated with early recurrence and resistance to hormone therapy. The Letrozole/Fulvestrant and Avastin (LEA) Study evaluated whether anti-VEGF bevacizumab in combination with ET would improve outcomes. After a median follow up of 23.7 months, patients in the ET-B arm had a median PFS of 19.3 months (95% CI, 16.5-22.1) vs. 14.4 months (11.4-17.5) for patients taking ET alone (P = .125). Compared with the ET alone arm, patients in the ET-B arm had improved ORR (40.8% vs 21.9%, P < .001) and CBR (76.8% vs 67.4%, P = .041). Grade 3-4 adverse events were significantly more frequent in the ET-B arm, including hypertension (15.0% vs 3.0%, P < .001), aminotransferase elevation (3.7% vs 1.0%, P = .068), and proteinuria (7.0% vs 0.0%, P < .001). In the ET-B arm, 39 patients (20.5%) discontinued treatment, including 8 patients who died. There were no toxicity-related deaths in the ET arm.
“Although the potential impact of age and comorbidities should not be discounted in the mortality outcomes of the LEA study, we observed an unexpectedly high rate of toxicity-related deaths among patients receiving ET-B. In addition, adverse events were significantly higher in the ET-B arm. Therefore, a toxicity interaction between these agents cannot be ruled out and should be carefully monitored in ongoing studies with this combination,” wrote Dr. Martin and colleagues.
First-line treatment with endocrine therapy plus bevacizumab did not significantly improve PFS compared with endocrine therapy alone for postmenopausal women with hormone receptor–positive, HER2-negative advanced breast cancer, according to results from a multicenter phase III trial published online Feb. 17 in Journal of Clinical Oncology.
Furthermore, patients taking endocrine therapy plus bevacizumab (ET-B) had significantly more adverse events.
“On the basis of this particular trial and in light of the higher toxicity, ET-B should not be recommended in the treatment of advanced hormone receptor-positive/HER2-negative breast cancer,” wrote Dr. Miguel Martín of Universidad Complutense de Madrid and his associates (J. Clin. Oncol. 2015 Feb. 17 [doi:10.1200/JCO.2014.57.2388]).
Previous studies have shown overexpression of VEGF in breast cancer and that high VEGF levels are associated with early recurrence and resistance to hormone therapy. The Letrozole/Fulvestrant and Avastin (LEA) Study evaluated whether anti-VEGF bevacizumab in combination with ET would improve outcomes. After a median follow up of 23.7 months, patients in the ET-B arm had a median PFS of 19.3 months (95% CI, 16.5-22.1) vs. 14.4 months (11.4-17.5) for patients taking ET alone (P = .125). Compared with the ET alone arm, patients in the ET-B arm had improved ORR (40.8% vs 21.9%, P < .001) and CBR (76.8% vs 67.4%, P = .041). Grade 3-4 adverse events were significantly more frequent in the ET-B arm, including hypertension (15.0% vs 3.0%, P < .001), aminotransferase elevation (3.7% vs 1.0%, P = .068), and proteinuria (7.0% vs 0.0%, P < .001). In the ET-B arm, 39 patients (20.5%) discontinued treatment, including 8 patients who died. There were no toxicity-related deaths in the ET arm.
“Although the potential impact of age and comorbidities should not be discounted in the mortality outcomes of the LEA study, we observed an unexpectedly high rate of toxicity-related deaths among patients receiving ET-B. In addition, adverse events were significantly higher in the ET-B arm. Therefore, a toxicity interaction between these agents cannot be ruled out and should be carefully monitored in ongoing studies with this combination,” wrote Dr. Martin and colleagues.
First-line treatment with endocrine therapy plus bevacizumab did not significantly improve PFS compared with endocrine therapy alone for postmenopausal women with hormone receptor–positive, HER2-negative advanced breast cancer, according to results from a multicenter phase III trial published online Feb. 17 in Journal of Clinical Oncology.
Furthermore, patients taking endocrine therapy plus bevacizumab (ET-B) had significantly more adverse events.
“On the basis of this particular trial and in light of the higher toxicity, ET-B should not be recommended in the treatment of advanced hormone receptor-positive/HER2-negative breast cancer,” wrote Dr. Miguel Martín of Universidad Complutense de Madrid and his associates (J. Clin. Oncol. 2015 Feb. 17 [doi:10.1200/JCO.2014.57.2388]).
Previous studies have shown overexpression of VEGF in breast cancer and that high VEGF levels are associated with early recurrence and resistance to hormone therapy. The Letrozole/Fulvestrant and Avastin (LEA) Study evaluated whether anti-VEGF bevacizumab in combination with ET would improve outcomes. After a median follow up of 23.7 months, patients in the ET-B arm had a median PFS of 19.3 months (95% CI, 16.5-22.1) vs. 14.4 months (11.4-17.5) for patients taking ET alone (P = .125). Compared with the ET alone arm, patients in the ET-B arm had improved ORR (40.8% vs 21.9%, P < .001) and CBR (76.8% vs 67.4%, P = .041). Grade 3-4 adverse events were significantly more frequent in the ET-B arm, including hypertension (15.0% vs 3.0%, P < .001), aminotransferase elevation (3.7% vs 1.0%, P = .068), and proteinuria (7.0% vs 0.0%, P < .001). In the ET-B arm, 39 patients (20.5%) discontinued treatment, including 8 patients who died. There were no toxicity-related deaths in the ET arm.
“Although the potential impact of age and comorbidities should not be discounted in the mortality outcomes of the LEA study, we observed an unexpectedly high rate of toxicity-related deaths among patients receiving ET-B. In addition, adverse events were significantly higher in the ET-B arm. Therefore, a toxicity interaction between these agents cannot be ruled out and should be carefully monitored in ongoing studies with this combination,” wrote Dr. Martin and colleagues.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: In women with HER2-negative, hormone receptor–positive breast cancer, the addition of bevacizumab to endocrine therapy did not significantly improve PFS or OS.
Major finding: Median PFS for ET alone vs ET-B was 14.4 months vs 19.3 months; patients taking ET-B had significantly more adverse events.
Data source: The open-label phase III Letrozole/Fulvestrant and Avastin Study that randomized 374 patients to receive fulvestrant or letrozole alone (n = 184) or ET plus bevacizumab (n = 190).
Disclosures: Dr. Martín disclosed that he is a consultant for Roche/Genentech.
Cancer mortality lowest in western United States
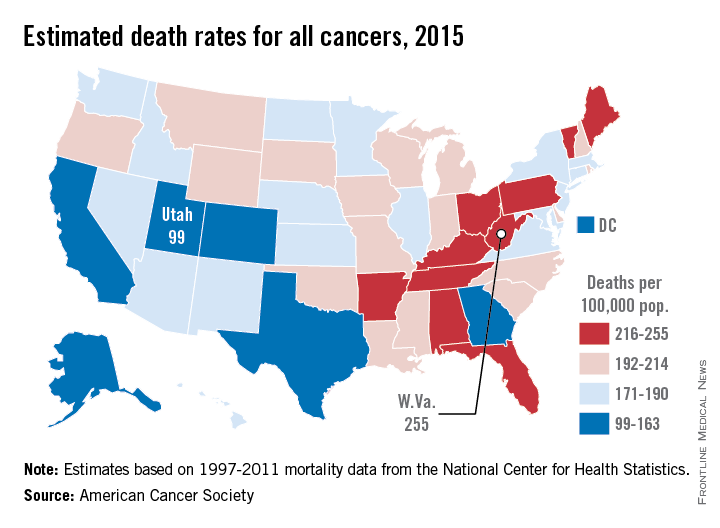
Utah will have the lowest cancer mortality rate in the United States in 2015, according to a report from the American Cancer Society.
While 11 states are predicted to have fewer cancer-related deaths in 2015 than 2014, the mortality rate will be lowest in Utah, with just 99 deaths per 100,000 people. Alaska and Colorado will have the next lowest mortality rates at 141 and 142 per 100,000 people, respectively. West Virginia is estimated to have the highest cancer mortality rate at 255 per 100,000 people, followed by Kentucky and Arkansas at 231 and 228, respectively. The national cancer mortality rate will be 185 per 100,000.
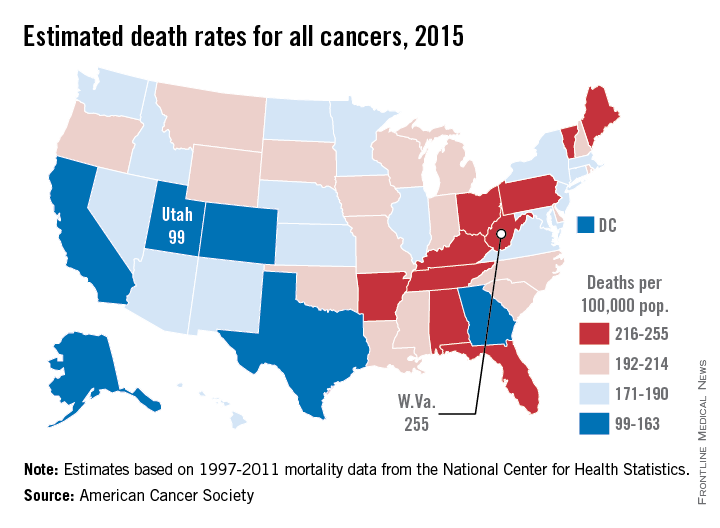
There will be about 1.66 million new cases of cancer in 2015 and about 590,000 deaths. Female breast cancer will probably be the most common with 231,000 new cases, but with an estimated 221,000 new cases each, lung/bronchus and prostate cancer also will rank high. Lung and bronchus cancer will be the most common cause of death, with 158,000 deaths predicted in 2015, more than a quarter of overall cancer deaths, according to the ACS.
Socioeconomic status makes a big difference in both cancer incidence and mortality. Cancer can stem from a higher likelihood to engage in risky behavior such as smoking, an unhealthy diet, or a sedentary lifestyle. Demographics matter more than ethnicity for cancer mortality, as “cancer mortality rates among both black and non-Hispanic white men with 12 or fewer years of education are almost 3 times higher than those of college graduates for all cancers combined and 4-5 times higher for lung cancer,” the ACS said.
Estimated data were based on 1995-2011 cancer incidence rates collected by the National Center for Health Statistics and the ACS.
Utah will have the lowest cancer mortality rate in the United States in 2015, according to a report from the American Cancer Society.
While 11 states are predicted to have fewer cancer-related deaths in 2015 than 2014, the mortality rate will be lowest in Utah, with just 99 deaths per 100,000 people. Alaska and Colorado will have the next lowest mortality rates at 141 and 142 per 100,000 people, respectively. West Virginia is estimated to have the highest cancer mortality rate at 255 per 100,000 people, followed by Kentucky and Arkansas at 231 and 228, respectively. The national cancer mortality rate will be 185 per 100,000.
There will be about 1.66 million new cases of cancer in 2015 and about 590,000 deaths. Female breast cancer will probably be the most common with 231,000 new cases, but with an estimated 221,000 new cases each, lung/bronchus and prostate cancer also will rank high. Lung and bronchus cancer will be the most common cause of death, with 158,000 deaths predicted in 2015, more than a quarter of overall cancer deaths, according to the ACS.
Socioeconomic status makes a big difference in both cancer incidence and mortality. Cancer can stem from a higher likelihood to engage in risky behavior such as smoking, an unhealthy diet, or a sedentary lifestyle. Demographics matter more than ethnicity for cancer mortality, as “cancer mortality rates among both black and non-Hispanic white men with 12 or fewer years of education are almost 3 times higher than those of college graduates for all cancers combined and 4-5 times higher for lung cancer,” the ACS said.
Estimated data were based on 1995-2011 cancer incidence rates collected by the National Center for Health Statistics and the ACS.
Utah will have the lowest cancer mortality rate in the United States in 2015, according to a report from the American Cancer Society.
While 11 states are predicted to have fewer cancer-related deaths in 2015 than 2014, the mortality rate will be lowest in Utah, with just 99 deaths per 100,000 people. Alaska and Colorado will have the next lowest mortality rates at 141 and 142 per 100,000 people, respectively. West Virginia is estimated to have the highest cancer mortality rate at 255 per 100,000 people, followed by Kentucky and Arkansas at 231 and 228, respectively. The national cancer mortality rate will be 185 per 100,000.
There will be about 1.66 million new cases of cancer in 2015 and about 590,000 deaths. Female breast cancer will probably be the most common with 231,000 new cases, but with an estimated 221,000 new cases each, lung/bronchus and prostate cancer also will rank high. Lung and bronchus cancer will be the most common cause of death, with 158,000 deaths predicted in 2015, more than a quarter of overall cancer deaths, according to the ACS.
Socioeconomic status makes a big difference in both cancer incidence and mortality. Cancer can stem from a higher likelihood to engage in risky behavior such as smoking, an unhealthy diet, or a sedentary lifestyle. Demographics matter more than ethnicity for cancer mortality, as “cancer mortality rates among both black and non-Hispanic white men with 12 or fewer years of education are almost 3 times higher than those of college graduates for all cancers combined and 4-5 times higher for lung cancer,” the ACS said.
Estimated data were based on 1995-2011 cancer incidence rates collected by the National Center for Health Statistics and the ACS.
Treatments for metastatic breast cancer expanding but decisions personalized
PARIS – With an expanding array of treatment choices and no fixed algorithm to decide which to use and when, treatment choice for metastatic breast cancer remains based on a conglomeration of tumor biology, prior therapies, toxicities, patients’ performance status and their choice or preference for treatment, Dr. Sandra M. Swain said during a state-of-the-art lecture on metastatic breast cancer at an international congress on anti-cancer treatment.
Compared to 30 years ago when there were only a few drugs available” to treat metastatic disease, “it’s really gratifying to be able to say to a patient, and really mean it, that ‘this is not your last option: we have a lot of other opportunities after this if this treatment doesn’t work or if you don’t like the toxicities from it’,” said Dr. Swain, director of the Washington Cancer Institute at MedStar Washington Hospital Center and professor of medicine at Georgetown University, Washington.

The past decade has seen several drugs approved by the Food and Drug Administration for use in metastatic breast cancer: eribulin in 2010, pertuzumab and everolimus in 2012, trastuzumab-DM1 in 2013, and most recently palbociclib in 2015, she said.
Although treatment goals largely remain the same – to extend survival and minimize toxicity, as well as maximizing patients’ quality of life – there has been a shift to looking at the value of metastatic cancer treatment, taking all these factors and the cost of treatment into consideration.
Looking at available chemotherapies listed in the National Comprehensive Cancer Network guidelines, Dr. Swain noted that no one regimen was preferred over others and highlighted the multiple choices that were recommended.
“My preference is to use sequential single agents, unless we have a patient who is very sick and we need an immediate response, “Dr. Swain said. Response rates are often higher with combination regimens but quality of life may be worse or there are added toxicities that need to be factored into the equation.
Dr. Swain highlighted that newer is not necessarily better. Results of the federal-sponsored CALGB 40502 study, for example, showed that neither weekly nab-paclitaxel (Abraxane) or ixabepilone (Ixempra) was better than weekly treatment with paclitaxel (J. Clin. Oncol. 2012;30:Abstr. CRA1002).
“I think in the U.S. this was very important because paclitaxel is generic and much easier for many patients to afford,” Dr. Swain said.
Expanding Treatment Choices
Studies in metastatic breast cancer highlighted by Dr. Swain include the Triple Negative Trial (TNT), the Breast Cancer Trial of Oral Everolimus 2 (BOLERO-2), and the Tamoxifen Plus Everolimus (TAMRAD) study.
Results of TNT were presented at the 2014 San Antonio Breast Cancer Symposium and showed that carboplatin might be a better choice than docetaxel for women with triple-negative breast cancer and the BRCA1/2 mutation.
BOLERO-2 showed that combining everolimus with exemestane increased progression-free survival by 64% in women with ER-positive, HER2-negative postmenopausal metastatic breast cancer who were refractory to treatment with other AIs (N. Engl. J. Med. 2012;366:520-9). The clinical implications of these data were that the use of everolimus could overcome resistance to endocrine therapy although stomatitis can occur within the first 3 months of treatment. Studies are looking at preventing this side effect with a steroid mouthwash, Dr. Swain said.
TAMRAD was a phase II study looking at the combination of everolimus and tamoxifen, showing improved response rates and overall survival over tamoxifen alone in postmenopausal women with AI-resistant metastatic breast cancer (J. Clin. Oncol. 2012;30:2718-24).
Dr. Swain also discussed the recent fast-tracked FDA approval of palbociclib, a cyclin-dependent kinase 4/6 inhibitor approved for use in combination with letrozole (Femara) for estrogen receptor–positive, HER2-negative, postmenopausal, metastatic breast cancer.
Approval was based on the results of the PALOMA-1 study (Lancet Oncol. 2015;16:25-35), which showed “a striking benefit, with a 50% reduction in progression-free survival” with the combination versus letrozole alone, she said.
“The biggest side effect is neutropenia,” Dr. Swain cautioned, with around 50% of patients treated with the combination experiencing grade 3 or 4 neutropenia.
“So that’s what we need to be careful of now that this drug is going to be on the market,” she said. While there were no reports of febrile neutropenia in the trial, she felt that this would be seen in the “real world” and needs to be considered.
Whether using granulocyte colony–stimulating factor to prevent neutropenia would be possible or even safe is a topic for future research.
Several phase III studies with palbociclib have been completed or are ongoing. These include PALOMA-2 in combination with letrozole as first-line treatment for ER-positive, HER2-negative metastatic breast cancer; PALOMA-3 in combination with fulvestrant (Faslodex) in patients who have progressed on hormonal therapy; PENELOPE-B in the postneoadjuvant setting; and PEARL in women with ER-positive metastatic breast cancer that is not responsive to treatment with an aromatase inhibitor.
There are also two other CDK 4/6 inhibitors currently under investigation: abemaciclib and LEE011, both in phase III trials.
Dr. Swain has received research funding from Genentech, Pfizer, Puma Biotechnology, and Roche. She has also acted as an advisor or consultant and served as a steering committee member for Genentech and Roche, uncompensated. She has received honoraria from Genentech/Roche and Clinigen. She has received travel funding from Genentech.
PARIS – With an expanding array of treatment choices and no fixed algorithm to decide which to use and when, treatment choice for metastatic breast cancer remains based on a conglomeration of tumor biology, prior therapies, toxicities, patients’ performance status and their choice or preference for treatment, Dr. Sandra M. Swain said during a state-of-the-art lecture on metastatic breast cancer at an international congress on anti-cancer treatment.
Compared to 30 years ago when there were only a few drugs available” to treat metastatic disease, “it’s really gratifying to be able to say to a patient, and really mean it, that ‘this is not your last option: we have a lot of other opportunities after this if this treatment doesn’t work or if you don’t like the toxicities from it’,” said Dr. Swain, director of the Washington Cancer Institute at MedStar Washington Hospital Center and professor of medicine at Georgetown University, Washington.
The past decade has seen several drugs approved by the Food and Drug Administration for use in metastatic breast cancer: eribulin in 2010, pertuzumab and everolimus in 2012, trastuzumab-DM1 in 2013, and most recently palbociclib in 2015, she said.
Although treatment goals largely remain the same – to extend survival and minimize toxicity, as well as maximizing patients’ quality of life – there has been a shift to looking at the value of metastatic cancer treatment, taking all these factors and the cost of treatment into consideration.
Looking at available chemotherapies listed in the National Comprehensive Cancer Network guidelines, Dr. Swain noted that no one regimen was preferred over others and highlighted the multiple choices that were recommended.
“My preference is to use sequential single agents, unless we have a patient who is very sick and we need an immediate response, “Dr. Swain said. Response rates are often higher with combination regimens but quality of life may be worse or there are added toxicities that need to be factored into the equation.
Dr. Swain highlighted that newer is not necessarily better. Results of the federal-sponsored CALGB 40502 study, for example, showed that neither weekly nab-paclitaxel (Abraxane) or ixabepilone (Ixempra) was better than weekly treatment with paclitaxel (J. Clin. Oncol. 2012;30:Abstr. CRA1002).
“I think in the U.S. this was very important because paclitaxel is generic and much easier for many patients to afford,” Dr. Swain said.
Expanding Treatment Choices
Studies in metastatic breast cancer highlighted by Dr. Swain include the Triple Negative Trial (TNT), the Breast Cancer Trial of Oral Everolimus 2 (BOLERO-2), and the Tamoxifen Plus Everolimus (TAMRAD) study.
Results of TNT were presented at the 2014 San Antonio Breast Cancer Symposium and showed that carboplatin might be a better choice than docetaxel for women with triple-negative breast cancer and the BRCA1/2 mutation.
BOLERO-2 showed that combining everolimus with exemestane increased progression-free survival by 64% in women with ER-positive, HER2-negative postmenopausal metastatic breast cancer who were refractory to treatment with other AIs (N. Engl. J. Med. 2012;366:520-9). The clinical implications of these data were that the use of everolimus could overcome resistance to endocrine therapy although stomatitis can occur within the first 3 months of treatment. Studies are looking at preventing this side effect with a steroid mouthwash, Dr. Swain said.
TAMRAD was a phase II study looking at the combination of everolimus and tamoxifen, showing improved response rates and overall survival over tamoxifen alone in postmenopausal women with AI-resistant metastatic breast cancer (J. Clin. Oncol. 2012;30:2718-24).
Dr. Swain also discussed the recent fast-tracked FDA approval of palbociclib, a cyclin-dependent kinase 4/6 inhibitor approved for use in combination with letrozole (Femara) for estrogen receptor–positive, HER2-negative, postmenopausal, metastatic breast cancer.
Approval was based on the results of the PALOMA-1 study (Lancet Oncol. 2015;16:25-35), which showed “a striking benefit, with a 50% reduction in progression-free survival” with the combination versus letrozole alone, she said.
“The biggest side effect is neutropenia,” Dr. Swain cautioned, with around 50% of patients treated with the combination experiencing grade 3 or 4 neutropenia.
“So that’s what we need to be careful of now that this drug is going to be on the market,” she said. While there were no reports of febrile neutropenia in the trial, she felt that this would be seen in the “real world” and needs to be considered.
Whether using granulocyte colony–stimulating factor to prevent neutropenia would be possible or even safe is a topic for future research.
Several phase III studies with palbociclib have been completed or are ongoing. These include PALOMA-2 in combination with letrozole as first-line treatment for ER-positive, HER2-negative metastatic breast cancer; PALOMA-3 in combination with fulvestrant (Faslodex) in patients who have progressed on hormonal therapy; PENELOPE-B in the postneoadjuvant setting; and PEARL in women with ER-positive metastatic breast cancer that is not responsive to treatment with an aromatase inhibitor.
There are also two other CDK 4/6 inhibitors currently under investigation: abemaciclib and LEE011, both in phase III trials.
Dr. Swain has received research funding from Genentech, Pfizer, Puma Biotechnology, and Roche. She has also acted as an advisor or consultant and served as a steering committee member for Genentech and Roche, uncompensated. She has received honoraria from Genentech/Roche and Clinigen. She has received travel funding from Genentech.
PARIS – With an expanding array of treatment choices and no fixed algorithm to decide which to use and when, treatment choice for metastatic breast cancer remains based on a conglomeration of tumor biology, prior therapies, toxicities, patients’ performance status and their choice or preference for treatment, Dr. Sandra M. Swain said during a state-of-the-art lecture on metastatic breast cancer at an international congress on anti-cancer treatment.
Compared to 30 years ago when there were only a few drugs available” to treat metastatic disease, “it’s really gratifying to be able to say to a patient, and really mean it, that ‘this is not your last option: we have a lot of other opportunities after this if this treatment doesn’t work or if you don’t like the toxicities from it’,” said Dr. Swain, director of the Washington Cancer Institute at MedStar Washington Hospital Center and professor of medicine at Georgetown University, Washington.
The past decade has seen several drugs approved by the Food and Drug Administration for use in metastatic breast cancer: eribulin in 2010, pertuzumab and everolimus in 2012, trastuzumab-DM1 in 2013, and most recently palbociclib in 2015, she said.
Although treatment goals largely remain the same – to extend survival and minimize toxicity, as well as maximizing patients’ quality of life – there has been a shift to looking at the value of metastatic cancer treatment, taking all these factors and the cost of treatment into consideration.
Looking at available chemotherapies listed in the National Comprehensive Cancer Network guidelines, Dr. Swain noted that no one regimen was preferred over others and highlighted the multiple choices that were recommended.
“My preference is to use sequential single agents, unless we have a patient who is very sick and we need an immediate response, “Dr. Swain said. Response rates are often higher with combination regimens but quality of life may be worse or there are added toxicities that need to be factored into the equation.
Dr. Swain highlighted that newer is not necessarily better. Results of the federal-sponsored CALGB 40502 study, for example, showed that neither weekly nab-paclitaxel (Abraxane) or ixabepilone (Ixempra) was better than weekly treatment with paclitaxel (J. Clin. Oncol. 2012;30:Abstr. CRA1002).
“I think in the U.S. this was very important because paclitaxel is generic and much easier for many patients to afford,” Dr. Swain said.
Expanding Treatment Choices
Studies in metastatic breast cancer highlighted by Dr. Swain include the Triple Negative Trial (TNT), the Breast Cancer Trial of Oral Everolimus 2 (BOLERO-2), and the Tamoxifen Plus Everolimus (TAMRAD) study.
Results of TNT were presented at the 2014 San Antonio Breast Cancer Symposium and showed that carboplatin might be a better choice than docetaxel for women with triple-negative breast cancer and the BRCA1/2 mutation.
BOLERO-2 showed that combining everolimus with exemestane increased progression-free survival by 64% in women with ER-positive, HER2-negative postmenopausal metastatic breast cancer who were refractory to treatment with other AIs (N. Engl. J. Med. 2012;366:520-9). The clinical implications of these data were that the use of everolimus could overcome resistance to endocrine therapy although stomatitis can occur within the first 3 months of treatment. Studies are looking at preventing this side effect with a steroid mouthwash, Dr. Swain said.
TAMRAD was a phase II study looking at the combination of everolimus and tamoxifen, showing improved response rates and overall survival over tamoxifen alone in postmenopausal women with AI-resistant metastatic breast cancer (J. Clin. Oncol. 2012;30:2718-24).
Dr. Swain also discussed the recent fast-tracked FDA approval of palbociclib, a cyclin-dependent kinase 4/6 inhibitor approved for use in combination with letrozole (Femara) for estrogen receptor–positive, HER2-negative, postmenopausal, metastatic breast cancer.
Approval was based on the results of the PALOMA-1 study (Lancet Oncol. 2015;16:25-35), which showed “a striking benefit, with a 50% reduction in progression-free survival” with the combination versus letrozole alone, she said.
“The biggest side effect is neutropenia,” Dr. Swain cautioned, with around 50% of patients treated with the combination experiencing grade 3 or 4 neutropenia.
“So that’s what we need to be careful of now that this drug is going to be on the market,” she said. While there were no reports of febrile neutropenia in the trial, she felt that this would be seen in the “real world” and needs to be considered.
Whether using granulocyte colony–stimulating factor to prevent neutropenia would be possible or even safe is a topic for future research.
Several phase III studies with palbociclib have been completed or are ongoing. These include PALOMA-2 in combination with letrozole as first-line treatment for ER-positive, HER2-negative metastatic breast cancer; PALOMA-3 in combination with fulvestrant (Faslodex) in patients who have progressed on hormonal therapy; PENELOPE-B in the postneoadjuvant setting; and PEARL in women with ER-positive metastatic breast cancer that is not responsive to treatment with an aromatase inhibitor.
There are also two other CDK 4/6 inhibitors currently under investigation: abemaciclib and LEE011, both in phase III trials.
Dr. Swain has received research funding from Genentech, Pfizer, Puma Biotechnology, and Roche. She has also acted as an advisor or consultant and served as a steering committee member for Genentech and Roche, uncompensated. She has received honoraria from Genentech/Roche and Clinigen. She has received travel funding from Genentech.
EXPERT ANALYSIS FROM ICACT 2015

Smoking linked to many ‘new’ causes of death
Smoking causes death from many diseases that until now have not been linked officially to tobacco use, including digestive disorders, liver cirrhosis, infections, renal failure, and breast and prostate cancers, according to a report published online Feb. 11 in the New England Journal of Medicine.
“Our results suggest that the number of persons in the United States who die each year as a result of smoking cigarettes may be substantially greater than currently estimated,” said Brian D. Carter of the epidemiology research program, American Cancer Society, Atlanta, and his associates.

The 2014 Surgeon General’s report estimated that smoking causes more than 480,000 deaths every year in the United States, based on mortality figures from 21 diseases that have been formally established as caused by smoking: 12 types of cancer, 6 types of cardiovascular disease, diabetes, chronic obstructive pulmonary disease, and pneumonia. Mr. Carter and his associates pooled data from five large cohort studies to examine possible associations between smoking and an additional 31 cause-of-death categories. They now estimate that an additional 60,000-120,000 deaths each year can be attributed to smoking.
For their study, the investigators assessed 421,378 men and 532,651 women aged 55 years and older at baseline whose smoking status was carefully recorded and who were followed from 2000 to 2011 in the Cancer Prevention Study II Nutrition Cohort, the Nurses’ Health Study I, the Health Professionals Follow-up Study, the Women’s Health Initiative, and the National Institutes of Health-AARP Diet and Health Study.
As expected, smokers had a twofold to threefold higher mortality from any cause, compared with nonsmokers. Smokers also had a markedly higher risk of death than nonsmokers from all 21 causes already established as attributable to tobacco use, such as lung cancer, oral cancer, ischemic heart disease, atherosclerosis, and stroke. But approximately 17% of smokers’ excess mortality was accounted for by several diseases that previously have not been attributable to tobacco use.
For example, the risk of death due to intestinal ischemia was approximately six times higher among smokers than among nonsmokers, a remarkably strong association that was also reported in the Million Women Study. “Smoking acutely reduces blood flow to the intestines, and evidence suggests that smoking causes risk factors that can often lead to intestinal ischemia, including atherosclerosis, platelet aggregation, and congestive heart failure,” Mr. Carter and his associates said (N. Engl. J. Med. 2015 Feb. 12 [doi:10.1056/NEJMsa140721]). In this study, smoking also more than doubled the risk of dying from other digestive diseases. Previous studies have suggested a link between smoking and digestive disorders such as Crohn’s disease, peptic ulcers, acute pancreatitis, paralytic ileus, bowel obstruction, choletlithiasis, diverticulitis, and gastrointestinal hemorrhage. “Although these diseases are not common causes of death, they account for millions of hospitalizations each year,” the investigators noted.
The mortality risk from liver cirrhosis, after the data were adjusted to account for alcohol consumption, was more than three times higher in smokers than in nonsmokers. Even smokers who did not drink alcohol were at significantly increased risk of cirrhosis, compared with nonsmokers.
The risk of death due to infection was 2.3 times higher in smokers than in nonsmokers. This strong association was dose-dependent, as infection-related mortality rose with increasing smoking intensity. And among study participants who had quit smoking, infection-related mortality declined as the number of years since cessation increased.
The rate of death due to renal failure was twice as high among smokers as among nonsmokers. And the rate of death due to hypertensive heart disease, the only category of heart disease not already established as smoking related, was 2.4 times higher in smokers. The latter association “is relevant for assessing the public health burden of smoking, since a considerable number of deaths in the United States are attributable to hypertensive heart disease,” according to Mr. Carter and his associates.
Smoking also was strongly associated with “multiple diseases too uncommon to examine individually.” This included all rare cancers combined, rare digestive diseases, and respiratory diseases other than those already known to stem from smoking.
In women, smoking raised breast cancer mortality, with a relative risk of 1.3. This association was strongly dose dependent. In men, smoking raised prostate cancer mortality, with a relative risk of 1.4.
This study was limited in that most of the participants were white and better educated than the general population, which may affect the applicability of the results to other populations.
The findings reported by Carter et al. substantiate that until now, estimates of premature deaths due to smoking have markedly underestimated the burden of tobacco use on U.S. society. Attributing 60,000-120,000 additional deaths each year to smoking would have an important public health impact, since it is comparable to the number of annual deaths attributed to excess alcohol intake.
Many people see the war against smoking as one that we have already won, given that rates have declined so much since the 1960s. But these findings show that although we have had some major victories, the war on smoking is far from over.
Dr. Graham A. Colditz is at Washington University, St. Louis. He reported having no financial disclosures. Dr. Colditz made these remarks in an editorial accompanying Mr. Carter’s report (N. Engl. J. Med. 2015 Feb. 12 [doi:10.1056/NEJMe1414318]).
The findings reported by Carter et al. substantiate that until now, estimates of premature deaths due to smoking have markedly underestimated the burden of tobacco use on U.S. society. Attributing 60,000-120,000 additional deaths each year to smoking would have an important public health impact, since it is comparable to the number of annual deaths attributed to excess alcohol intake.
Many people see the war against smoking as one that we have already won, given that rates have declined so much since the 1960s. But these findings show that although we have had some major victories, the war on smoking is far from over.
Dr. Graham A. Colditz is at Washington University, St. Louis. He reported having no financial disclosures. Dr. Colditz made these remarks in an editorial accompanying Mr. Carter’s report (N. Engl. J. Med. 2015 Feb. 12 [doi:10.1056/NEJMe1414318]).
The findings reported by Carter et al. substantiate that until now, estimates of premature deaths due to smoking have markedly underestimated the burden of tobacco use on U.S. society. Attributing 60,000-120,000 additional deaths each year to smoking would have an important public health impact, since it is comparable to the number of annual deaths attributed to excess alcohol intake.
Many people see the war against smoking as one that we have already won, given that rates have declined so much since the 1960s. But these findings show that although we have had some major victories, the war on smoking is far from over.
Dr. Graham A. Colditz is at Washington University, St. Louis. He reported having no financial disclosures. Dr. Colditz made these remarks in an editorial accompanying Mr. Carter’s report (N. Engl. J. Med. 2015 Feb. 12 [doi:10.1056/NEJMe1414318]).
Smoking causes death from many diseases that until now have not been linked officially to tobacco use, including digestive disorders, liver cirrhosis, infections, renal failure, and breast and prostate cancers, according to a report published online Feb. 11 in the New England Journal of Medicine.
“Our results suggest that the number of persons in the United States who die each year as a result of smoking cigarettes may be substantially greater than currently estimated,” said Brian D. Carter of the epidemiology research program, American Cancer Society, Atlanta, and his associates.
The 2014 Surgeon General’s report estimated that smoking causes more than 480,000 deaths every year in the United States, based on mortality figures from 21 diseases that have been formally established as caused by smoking: 12 types of cancer, 6 types of cardiovascular disease, diabetes, chronic obstructive pulmonary disease, and pneumonia. Mr. Carter and his associates pooled data from five large cohort studies to examine possible associations between smoking and an additional 31 cause-of-death categories. They now estimate that an additional 60,000-120,000 deaths each year can be attributed to smoking.
For their study, the investigators assessed 421,378 men and 532,651 women aged 55 years and older at baseline whose smoking status was carefully recorded and who were followed from 2000 to 2011 in the Cancer Prevention Study II Nutrition Cohort, the Nurses’ Health Study I, the Health Professionals Follow-up Study, the Women’s Health Initiative, and the National Institutes of Health-AARP Diet and Health Study.
As expected, smokers had a twofold to threefold higher mortality from any cause, compared with nonsmokers. Smokers also had a markedly higher risk of death than nonsmokers from all 21 causes already established as attributable to tobacco use, such as lung cancer, oral cancer, ischemic heart disease, atherosclerosis, and stroke. But approximately 17% of smokers’ excess mortality was accounted for by several diseases that previously have not been attributable to tobacco use.
For example, the risk of death due to intestinal ischemia was approximately six times higher among smokers than among nonsmokers, a remarkably strong association that was also reported in the Million Women Study. “Smoking acutely reduces blood flow to the intestines, and evidence suggests that smoking causes risk factors that can often lead to intestinal ischemia, including atherosclerosis, platelet aggregation, and congestive heart failure,” Mr. Carter and his associates said (N. Engl. J. Med. 2015 Feb. 12 [doi:10.1056/NEJMsa140721]). In this study, smoking also more than doubled the risk of dying from other digestive diseases. Previous studies have suggested a link between smoking and digestive disorders such as Crohn’s disease, peptic ulcers, acute pancreatitis, paralytic ileus, bowel obstruction, choletlithiasis, diverticulitis, and gastrointestinal hemorrhage. “Although these diseases are not common causes of death, they account for millions of hospitalizations each year,” the investigators noted.
The mortality risk from liver cirrhosis, after the data were adjusted to account for alcohol consumption, was more than three times higher in smokers than in nonsmokers. Even smokers who did not drink alcohol were at significantly increased risk of cirrhosis, compared with nonsmokers.
The risk of death due to infection was 2.3 times higher in smokers than in nonsmokers. This strong association was dose-dependent, as infection-related mortality rose with increasing smoking intensity. And among study participants who had quit smoking, infection-related mortality declined as the number of years since cessation increased.
The rate of death due to renal failure was twice as high among smokers as among nonsmokers. And the rate of death due to hypertensive heart disease, the only category of heart disease not already established as smoking related, was 2.4 times higher in smokers. The latter association “is relevant for assessing the public health burden of smoking, since a considerable number of deaths in the United States are attributable to hypertensive heart disease,” according to Mr. Carter and his associates.
Smoking also was strongly associated with “multiple diseases too uncommon to examine individually.” This included all rare cancers combined, rare digestive diseases, and respiratory diseases other than those already known to stem from smoking.
In women, smoking raised breast cancer mortality, with a relative risk of 1.3. This association was strongly dose dependent. In men, smoking raised prostate cancer mortality, with a relative risk of 1.4.
This study was limited in that most of the participants were white and better educated than the general population, which may affect the applicability of the results to other populations.
Smoking causes death from many diseases that until now have not been linked officially to tobacco use, including digestive disorders, liver cirrhosis, infections, renal failure, and breast and prostate cancers, according to a report published online Feb. 11 in the New England Journal of Medicine.
“Our results suggest that the number of persons in the United States who die each year as a result of smoking cigarettes may be substantially greater than currently estimated,” said Brian D. Carter of the epidemiology research program, American Cancer Society, Atlanta, and his associates.
The 2014 Surgeon General’s report estimated that smoking causes more than 480,000 deaths every year in the United States, based on mortality figures from 21 diseases that have been formally established as caused by smoking: 12 types of cancer, 6 types of cardiovascular disease, diabetes, chronic obstructive pulmonary disease, and pneumonia. Mr. Carter and his associates pooled data from five large cohort studies to examine possible associations between smoking and an additional 31 cause-of-death categories. They now estimate that an additional 60,000-120,000 deaths each year can be attributed to smoking.
For their study, the investigators assessed 421,378 men and 532,651 women aged 55 years and older at baseline whose smoking status was carefully recorded and who were followed from 2000 to 2011 in the Cancer Prevention Study II Nutrition Cohort, the Nurses’ Health Study I, the Health Professionals Follow-up Study, the Women’s Health Initiative, and the National Institutes of Health-AARP Diet and Health Study.
As expected, smokers had a twofold to threefold higher mortality from any cause, compared with nonsmokers. Smokers also had a markedly higher risk of death than nonsmokers from all 21 causes already established as attributable to tobacco use, such as lung cancer, oral cancer, ischemic heart disease, atherosclerosis, and stroke. But approximately 17% of smokers’ excess mortality was accounted for by several diseases that previously have not been attributable to tobacco use.
For example, the risk of death due to intestinal ischemia was approximately six times higher among smokers than among nonsmokers, a remarkably strong association that was also reported in the Million Women Study. “Smoking acutely reduces blood flow to the intestines, and evidence suggests that smoking causes risk factors that can often lead to intestinal ischemia, including atherosclerosis, platelet aggregation, and congestive heart failure,” Mr. Carter and his associates said (N. Engl. J. Med. 2015 Feb. 12 [doi:10.1056/NEJMsa140721]). In this study, smoking also more than doubled the risk of dying from other digestive diseases. Previous studies have suggested a link between smoking and digestive disorders such as Crohn’s disease, peptic ulcers, acute pancreatitis, paralytic ileus, bowel obstruction, choletlithiasis, diverticulitis, and gastrointestinal hemorrhage. “Although these diseases are not common causes of death, they account for millions of hospitalizations each year,” the investigators noted.
The mortality risk from liver cirrhosis, after the data were adjusted to account for alcohol consumption, was more than three times higher in smokers than in nonsmokers. Even smokers who did not drink alcohol were at significantly increased risk of cirrhosis, compared with nonsmokers.
The risk of death due to infection was 2.3 times higher in smokers than in nonsmokers. This strong association was dose-dependent, as infection-related mortality rose with increasing smoking intensity. And among study participants who had quit smoking, infection-related mortality declined as the number of years since cessation increased.
The rate of death due to renal failure was twice as high among smokers as among nonsmokers. And the rate of death due to hypertensive heart disease, the only category of heart disease not already established as smoking related, was 2.4 times higher in smokers. The latter association “is relevant for assessing the public health burden of smoking, since a considerable number of deaths in the United States are attributable to hypertensive heart disease,” according to Mr. Carter and his associates.
Smoking also was strongly associated with “multiple diseases too uncommon to examine individually.” This included all rare cancers combined, rare digestive diseases, and respiratory diseases other than those already known to stem from smoking.
In women, smoking raised breast cancer mortality, with a relative risk of 1.3. This association was strongly dose dependent. In men, smoking raised prostate cancer mortality, with a relative risk of 1.4.
This study was limited in that most of the participants were white and better educated than the general population, which may affect the applicability of the results to other populations.
Key clinical point: Smoking is now thought to cause many deaths from infections; renal failure; liver cirrhosis; digestive diseases; and breast, prostate, and other cancers.
Major finding: Several diseases that previously have not been attributable to tobacco use accounted for 17% of smokers’ excess mortality.
Data source: An analysis of pooled data from five large cohort studies involving 954,029 people aged 55 years and older followed for 12 years to examine associations between smoking and 52 possible causes of death.
Disclosures: This study was supported by the American Cancer Society. Mr. Carter reported having no financial disclosures; one of his associates reported receiving grant support from Novo Nordisk.

Stage trumps biology for most small triple-negative breast cancers
SAN ANTONIO – Patients with stage T1a or T1b triple-negative breast cancer have an excellent prognosis even without chemotherapy, according to Dr. Eric P. Winer.
“There’s a perception on the part of many patients and physicians that all triple-negative breast cancer is bad, and that it’s destined to threaten and ultimately take a woman’s life. But even in an era where biology is king, stage still matters,” he observed at the San Antonio Breast Cancer Symposium.

He was a coinvestigator in a recent prospective cohort study which included 4,113 women with stage T1a or 1b breast cancer – that is, a tumor size no greater than 10 mm in its greatest dimension – without regional lymph node metastases or evidence of distant metastases. The patients, drawn from the National Comprehensive Cancer Network database, were treated in accord with institutional practice and followed for a median of 5.5 years.
Slightly over half of those in the subset with triple-negative breast cancer (TNBC) got chemotherapy. Those who received chemotherapy for T1a TNBC as defined by a tumor size not greater than 5 mm had a 5-year distant relapse-free survival (DRFS) of 100%, but the rate was still close to 95% in those not treated with chemotherapy. Outcomes were also quite favorable for patients with T1b TNBC who didn’t receive chemotherapy (J. Clin. Oncol. 2014;32:2142-50), said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
He noted that the findings in this study echo those of an earlier study by investigators at University of Texas M.D. Anderson Cancer Center, Houston, who reported a 5-year DRFS rate of 96% in 125 patients with T1a or 1b, lymph node-negative TNBC untreated with chemotherapy (J. Clin. Oncol. 2009;27:5700-6).
Dr. Winer said that while the consensus among most experts is that standard adjuvant chemotherapy regimens for patients with stage 2 or 3 TNBC include both anthracyclines and taxanes, his own view is that for patients with stage 1 TNBC “if you’re going to pursue chemotherapy, then treatment with a somewhat less toxic, shorter regimen would seem to be more appropriate.”
SAN ANTONIO – Patients with stage T1a or T1b triple-negative breast cancer have an excellent prognosis even without chemotherapy, according to Dr. Eric P. Winer.
“There’s a perception on the part of many patients and physicians that all triple-negative breast cancer is bad, and that it’s destined to threaten and ultimately take a woman’s life. But even in an era where biology is king, stage still matters,” he observed at the San Antonio Breast Cancer Symposium.
He was a coinvestigator in a recent prospective cohort study which included 4,113 women with stage T1a or 1b breast cancer – that is, a tumor size no greater than 10 mm in its greatest dimension – without regional lymph node metastases or evidence of distant metastases. The patients, drawn from the National Comprehensive Cancer Network database, were treated in accord with institutional practice and followed for a median of 5.5 years.
Slightly over half of those in the subset with triple-negative breast cancer (TNBC) got chemotherapy. Those who received chemotherapy for T1a TNBC as defined by a tumor size not greater than 5 mm had a 5-year distant relapse-free survival (DRFS) of 100%, but the rate was still close to 95% in those not treated with chemotherapy. Outcomes were also quite favorable for patients with T1b TNBC who didn’t receive chemotherapy (J. Clin. Oncol. 2014;32:2142-50), said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
He noted that the findings in this study echo those of an earlier study by investigators at University of Texas M.D. Anderson Cancer Center, Houston, who reported a 5-year DRFS rate of 96% in 125 patients with T1a or 1b, lymph node-negative TNBC untreated with chemotherapy (J. Clin. Oncol. 2009;27:5700-6).
Dr. Winer said that while the consensus among most experts is that standard adjuvant chemotherapy regimens for patients with stage 2 or 3 TNBC include both anthracyclines and taxanes, his own view is that for patients with stage 1 TNBC “if you’re going to pursue chemotherapy, then treatment with a somewhat less toxic, shorter regimen would seem to be more appropriate.”
SAN ANTONIO – Patients with stage T1a or T1b triple-negative breast cancer have an excellent prognosis even without chemotherapy, according to Dr. Eric P. Winer.
“There’s a perception on the part of many patients and physicians that all triple-negative breast cancer is bad, and that it’s destined to threaten and ultimately take a woman’s life. But even in an era where biology is king, stage still matters,” he observed at the San Antonio Breast Cancer Symposium.
He was a coinvestigator in a recent prospective cohort study which included 4,113 women with stage T1a or 1b breast cancer – that is, a tumor size no greater than 10 mm in its greatest dimension – without regional lymph node metastases or evidence of distant metastases. The patients, drawn from the National Comprehensive Cancer Network database, were treated in accord with institutional practice and followed for a median of 5.5 years.
Slightly over half of those in the subset with triple-negative breast cancer (TNBC) got chemotherapy. Those who received chemotherapy for T1a TNBC as defined by a tumor size not greater than 5 mm had a 5-year distant relapse-free survival (DRFS) of 100%, but the rate was still close to 95% in those not treated with chemotherapy. Outcomes were also quite favorable for patients with T1b TNBC who didn’t receive chemotherapy (J. Clin. Oncol. 2014;32:2142-50), said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
He noted that the findings in this study echo those of an earlier study by investigators at University of Texas M.D. Anderson Cancer Center, Houston, who reported a 5-year DRFS rate of 96% in 125 patients with T1a or 1b, lymph node-negative TNBC untreated with chemotherapy (J. Clin. Oncol. 2009;27:5700-6).
Dr. Winer said that while the consensus among most experts is that standard adjuvant chemotherapy regimens for patients with stage 2 or 3 TNBC include both anthracyclines and taxanes, his own view is that for patients with stage 1 TNBC “if you’re going to pursue chemotherapy, then treatment with a somewhat less toxic, shorter regimen would seem to be more appropriate.”
EXPERT ANALYSIS FROM SABCS 2014

Controversy continues over platinum for TNBC patients
SAN ANTONIO – Oncologists are split over the use of platinum compounds as adjuvant or neoadjuvant therapy for triple-negative breast cancer patients, a rift likely to continue until definitive outcome data become available several years from now.
“In the U.S., I would say that about half of all medical oncologists are now in a fairly routine manner giving carboplatin in this setting,” Dr. Eric P. Winer estimated at the San Antonio Breast Cancer Symposium.
He’s not among them.

“Is carboplatin ready for prime time use in the adjuvant or neoadjuvant setting in triple-negative breast cancer? I personally feel we first need a definitive study showing improvement in disease-free survival and/or overall survival, or something close to that,” said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
Proponents of platinum salts cite two positive phase II randomized trials – GeparSixto and CALGB 40603 – which demonstrated significantly higher pathologic complete response (pCR) rates in patients with stage II or III triple-negative breast cancer (TNBC) with the addition of carboplatin to neoadjuvant chemotherapy.
The pro-platinum camp points to evidence suggesting a pCR in women with TNBC appears to be a good surrogate endpoint for event-free survival and overall survival, as shown in a recent meta-analysis by Dr. Patricia Cortazar of the Food and Drug Administration and her coworkers. The investigators concluded that pCR in response to neoadjuvant therapy with various regimens was associated with a 76% improvement in event-free survival and an 84% improvement in overall survival in 557 women with TNBC (Lancet 2014;384:164-72).
“The two phase II studies are going in the same direction,” observed Dr. Gunter von Minckwitz of the German Breast Group and principal investigator in the GeparSixto trial. “We have surveyed our group of investigators, and they are all using platinum in triple-negative breast cancer. The German guidelines say you can, but you don’t have to.”
But Dr. Winer, and by his estimate roughly half of all American medical oncologists, remain unconvinced.
“I think we should all keep in mind that pCR is a marker of better outcome, it’s not necessarily a required step in the process,” he said.
He’s leery of relying upon pCR as a surrogate endpoint in light of the deeply disappointing BEATRICE experience. The phase III BEATRICE trial included nearly 2,600 women with TNBC who were randomized to adjuvant chemotherapy alone or in combination with bevacizumab. The bevacizumab group had a higher pCR, but no improvement in disease-free survival or overall survival (Lancet Oncol. 2013;14:933-42).
“I would hate to see us all indiscriminately adding platinum to standard regimens, increasing toxicity, particularly if it is not associated with long-term benefit,” Dr. Winer said. “And even if it is associated with long-term benefit, I want to tease out who really benefits and which triple-negative patients are most sensitive to these agents.”
Progress is occurring in this area, he added. In GeparSixto, the addition of neoadjuvant carboplatin to paclitaxel and nonpegylated liposomal doxorubicin was associated with a 66.7% pCR rate in the subgroup of TNBC patients with a BRCA 1 or 2 germline mutation and a 43.5% rate in those without such mutations (Lancet Oncol. 2014;15:747-56).

Moreover, in the phase III Triple Negative Breast Cancer Trial (TNT) presented at this year’s San Antonio symposium, Dr. Andrew N.J. Tutt reported that in a prespecified analysis of the small subgroup comprising 43 BRCA mutation-positive patients, the objective response rate was 68% in those randomized to carboplatin, compared with 33% in those assigned to docetaxel. Moreover, mean progression-free survival was 6.8 months with carboplatin, significantly better than the 4.8 months with docetaxel or the 3.1 months in carboplatin-treated patients without a BRCA 1/2 mutation.
The TNT trial included 376 patients with metastatic or recurrent locally advanced TNBC randomized to single agent therapy. While the study provides no evidence of a superior response to carboplatin, compared with docetaxel in unselected patients with metastatic TNBC, it does support BRCA 1/2 mutation genotyping as part of decision making regarding therapy in metastatic TNBC and familial breast cancer, according to Dr. Tutt, professor of breast oncology at the Institute of Cancer Research, London.
The trial also tested the utility of Myriad Genetics’ novel Homologous Recombination Deficiency (HRD) score as a predictor of platinum-responsiveness of TNBC and concluded it was without benefit.
Dr. Winer noted that TNBC accounts for only about 15% of breast cancers. Still, that’s roughly 35,000 new cases per year in the United States alone – and TNBC is responsible for a disproportionate degree of breast cancer mortality.
“Perhaps in patients with BRCA 1 or 2 mutations, we’re getting close to thinking that platinum may be a standard, but even here I would await the completion of ongoing trials before we embrace that concept,” he said.
Among these studies is the 12-258 INFORM trial, a multicenter study in which 166 newly diagnosed breast cancer patients with BRCA1 or 2 mutations are being randomized to preoperative cisplatin or doxorubicin/cyclophosphamide.
Dr. William M. Sikov, principal investigator for the CALGB 40603 trial (J. Clin. Oncol. 2015;33:13-21), predicted there will be little crossover between the platinum-user and nonuser camps until definitive trials report whether the therapy improves relapse-free or overall survival.
“One group will say, ‘There’s an absolute increase in pathologic complete response with carboplatin in these two studies, and I’m convinced it’s a beneficial drug in these patients.’ It’s inexpensive, it’s available, although not approved for triple negative breast cancer, and it has some hematologic toxicities. But we have no long-term outcomes yet. I don’t think the TNT results will change anyone’s mind,” according to Dr. Sikov of Women and Infants Hospital in Providence, R.I.
Dr. Winer reported receiving research funding from Genentech. Dr. Sikov serves as a consultant to AbbVie and Celgene. Dr. Tutt reported having no financial conflicts.
SAN ANTONIO – Oncologists are split over the use of platinum compounds as adjuvant or neoadjuvant therapy for triple-negative breast cancer patients, a rift likely to continue until definitive outcome data become available several years from now.
“In the U.S., I would say that about half of all medical oncologists are now in a fairly routine manner giving carboplatin in this setting,” Dr. Eric P. Winer estimated at the San Antonio Breast Cancer Symposium.
He’s not among them.
“Is carboplatin ready for prime time use in the adjuvant or neoadjuvant setting in triple-negative breast cancer? I personally feel we first need a definitive study showing improvement in disease-free survival and/or overall survival, or something close to that,” said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
Proponents of platinum salts cite two positive phase II randomized trials – GeparSixto and CALGB 40603 – which demonstrated significantly higher pathologic complete response (pCR) rates in patients with stage II or III triple-negative breast cancer (TNBC) with the addition of carboplatin to neoadjuvant chemotherapy.
The pro-platinum camp points to evidence suggesting a pCR in women with TNBC appears to be a good surrogate endpoint for event-free survival and overall survival, as shown in a recent meta-analysis by Dr. Patricia Cortazar of the Food and Drug Administration and her coworkers. The investigators concluded that pCR in response to neoadjuvant therapy with various regimens was associated with a 76% improvement in event-free survival and an 84% improvement in overall survival in 557 women with TNBC (Lancet 2014;384:164-72).
“The two phase II studies are going in the same direction,” observed Dr. Gunter von Minckwitz of the German Breast Group and principal investigator in the GeparSixto trial. “We have surveyed our group of investigators, and they are all using platinum in triple-negative breast cancer. The German guidelines say you can, but you don’t have to.”
But Dr. Winer, and by his estimate roughly half of all American medical oncologists, remain unconvinced.
“I think we should all keep in mind that pCR is a marker of better outcome, it’s not necessarily a required step in the process,” he said.
He’s leery of relying upon pCR as a surrogate endpoint in light of the deeply disappointing BEATRICE experience. The phase III BEATRICE trial included nearly 2,600 women with TNBC who were randomized to adjuvant chemotherapy alone or in combination with bevacizumab. The bevacizumab group had a higher pCR, but no improvement in disease-free survival or overall survival (Lancet Oncol. 2013;14:933-42).
“I would hate to see us all indiscriminately adding platinum to standard regimens, increasing toxicity, particularly if it is not associated with long-term benefit,” Dr. Winer said. “And even if it is associated with long-term benefit, I want to tease out who really benefits and which triple-negative patients are most sensitive to these agents.”
Progress is occurring in this area, he added. In GeparSixto, the addition of neoadjuvant carboplatin to paclitaxel and nonpegylated liposomal doxorubicin was associated with a 66.7% pCR rate in the subgroup of TNBC patients with a BRCA 1 or 2 germline mutation and a 43.5% rate in those without such mutations (Lancet Oncol. 2014;15:747-56).
Moreover, in the phase III Triple Negative Breast Cancer Trial (TNT) presented at this year’s San Antonio symposium, Dr. Andrew N.J. Tutt reported that in a prespecified analysis of the small subgroup comprising 43 BRCA mutation-positive patients, the objective response rate was 68% in those randomized to carboplatin, compared with 33% in those assigned to docetaxel. Moreover, mean progression-free survival was 6.8 months with carboplatin, significantly better than the 4.8 months with docetaxel or the 3.1 months in carboplatin-treated patients without a BRCA 1/2 mutation.
The TNT trial included 376 patients with metastatic or recurrent locally advanced TNBC randomized to single agent therapy. While the study provides no evidence of a superior response to carboplatin, compared with docetaxel in unselected patients with metastatic TNBC, it does support BRCA 1/2 mutation genotyping as part of decision making regarding therapy in metastatic TNBC and familial breast cancer, according to Dr. Tutt, professor of breast oncology at the Institute of Cancer Research, London.
The trial also tested the utility of Myriad Genetics’ novel Homologous Recombination Deficiency (HRD) score as a predictor of platinum-responsiveness of TNBC and concluded it was without benefit.
Dr. Winer noted that TNBC accounts for only about 15% of breast cancers. Still, that’s roughly 35,000 new cases per year in the United States alone – and TNBC is responsible for a disproportionate degree of breast cancer mortality.
“Perhaps in patients with BRCA 1 or 2 mutations, we’re getting close to thinking that platinum may be a standard, but even here I would await the completion of ongoing trials before we embrace that concept,” he said.
Among these studies is the 12-258 INFORM trial, a multicenter study in which 166 newly diagnosed breast cancer patients with BRCA1 or 2 mutations are being randomized to preoperative cisplatin or doxorubicin/cyclophosphamide.
Dr. William M. Sikov, principal investigator for the CALGB 40603 trial (J. Clin. Oncol. 2015;33:13-21), predicted there will be little crossover between the platinum-user and nonuser camps until definitive trials report whether the therapy improves relapse-free or overall survival.
“One group will say, ‘There’s an absolute increase in pathologic complete response with carboplatin in these two studies, and I’m convinced it’s a beneficial drug in these patients.’ It’s inexpensive, it’s available, although not approved for triple negative breast cancer, and it has some hematologic toxicities. But we have no long-term outcomes yet. I don’t think the TNT results will change anyone’s mind,” according to Dr. Sikov of Women and Infants Hospital in Providence, R.I.
Dr. Winer reported receiving research funding from Genentech. Dr. Sikov serves as a consultant to AbbVie and Celgene. Dr. Tutt reported having no financial conflicts.
SAN ANTONIO – Oncologists are split over the use of platinum compounds as adjuvant or neoadjuvant therapy for triple-negative breast cancer patients, a rift likely to continue until definitive outcome data become available several years from now.
“In the U.S., I would say that about half of all medical oncologists are now in a fairly routine manner giving carboplatin in this setting,” Dr. Eric P. Winer estimated at the San Antonio Breast Cancer Symposium.
He’s not among them.
“Is carboplatin ready for prime time use in the adjuvant or neoadjuvant setting in triple-negative breast cancer? I personally feel we first need a definitive study showing improvement in disease-free survival and/or overall survival, or something close to that,” said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
Proponents of platinum salts cite two positive phase II randomized trials – GeparSixto and CALGB 40603 – which demonstrated significantly higher pathologic complete response (pCR) rates in patients with stage II or III triple-negative breast cancer (TNBC) with the addition of carboplatin to neoadjuvant chemotherapy.
The pro-platinum camp points to evidence suggesting a pCR in women with TNBC appears to be a good surrogate endpoint for event-free survival and overall survival, as shown in a recent meta-analysis by Dr. Patricia Cortazar of the Food and Drug Administration and her coworkers. The investigators concluded that pCR in response to neoadjuvant therapy with various regimens was associated with a 76% improvement in event-free survival and an 84% improvement in overall survival in 557 women with TNBC (Lancet 2014;384:164-72).
“The two phase II studies are going in the same direction,” observed Dr. Gunter von Minckwitz of the German Breast Group and principal investigator in the GeparSixto trial. “We have surveyed our group of investigators, and they are all using platinum in triple-negative breast cancer. The German guidelines say you can, but you don’t have to.”
But Dr. Winer, and by his estimate roughly half of all American medical oncologists, remain unconvinced.
“I think we should all keep in mind that pCR is a marker of better outcome, it’s not necessarily a required step in the process,” he said.
He’s leery of relying upon pCR as a surrogate endpoint in light of the deeply disappointing BEATRICE experience. The phase III BEATRICE trial included nearly 2,600 women with TNBC who were randomized to adjuvant chemotherapy alone or in combination with bevacizumab. The bevacizumab group had a higher pCR, but no improvement in disease-free survival or overall survival (Lancet Oncol. 2013;14:933-42).
“I would hate to see us all indiscriminately adding platinum to standard regimens, increasing toxicity, particularly if it is not associated with long-term benefit,” Dr. Winer said. “And even if it is associated with long-term benefit, I want to tease out who really benefits and which triple-negative patients are most sensitive to these agents.”
Progress is occurring in this area, he added. In GeparSixto, the addition of neoadjuvant carboplatin to paclitaxel and nonpegylated liposomal doxorubicin was associated with a 66.7% pCR rate in the subgroup of TNBC patients with a BRCA 1 or 2 germline mutation and a 43.5% rate in those without such mutations (Lancet Oncol. 2014;15:747-56).
Moreover, in the phase III Triple Negative Breast Cancer Trial (TNT) presented at this year’s San Antonio symposium, Dr. Andrew N.J. Tutt reported that in a prespecified analysis of the small subgroup comprising 43 BRCA mutation-positive patients, the objective response rate was 68% in those randomized to carboplatin, compared with 33% in those assigned to docetaxel. Moreover, mean progression-free survival was 6.8 months with carboplatin, significantly better than the 4.8 months with docetaxel or the 3.1 months in carboplatin-treated patients without a BRCA 1/2 mutation.
The TNT trial included 376 patients with metastatic or recurrent locally advanced TNBC randomized to single agent therapy. While the study provides no evidence of a superior response to carboplatin, compared with docetaxel in unselected patients with metastatic TNBC, it does support BRCA 1/2 mutation genotyping as part of decision making regarding therapy in metastatic TNBC and familial breast cancer, according to Dr. Tutt, professor of breast oncology at the Institute of Cancer Research, London.
The trial also tested the utility of Myriad Genetics’ novel Homologous Recombination Deficiency (HRD) score as a predictor of platinum-responsiveness of TNBC and concluded it was without benefit.
Dr. Winer noted that TNBC accounts for only about 15% of breast cancers. Still, that’s roughly 35,000 new cases per year in the United States alone – and TNBC is responsible for a disproportionate degree of breast cancer mortality.
“Perhaps in patients with BRCA 1 or 2 mutations, we’re getting close to thinking that platinum may be a standard, but even here I would await the completion of ongoing trials before we embrace that concept,” he said.
Among these studies is the 12-258 INFORM trial, a multicenter study in which 166 newly diagnosed breast cancer patients with BRCA1 or 2 mutations are being randomized to preoperative cisplatin or doxorubicin/cyclophosphamide.
Dr. William M. Sikov, principal investigator for the CALGB 40603 trial (J. Clin. Oncol. 2015;33:13-21), predicted there will be little crossover between the platinum-user and nonuser camps until definitive trials report whether the therapy improves relapse-free or overall survival.
“One group will say, ‘There’s an absolute increase in pathologic complete response with carboplatin in these two studies, and I’m convinced it’s a beneficial drug in these patients.’ It’s inexpensive, it’s available, although not approved for triple negative breast cancer, and it has some hematologic toxicities. But we have no long-term outcomes yet. I don’t think the TNT results will change anyone’s mind,” according to Dr. Sikov of Women and Infants Hospital in Providence, R.I.
Dr. Winer reported receiving research funding from Genentech. Dr. Sikov serves as a consultant to AbbVie and Celgene. Dr. Tutt reported having no financial conflicts.
EXPERT ANALYSIS FROM SABCS 2014

Lung cancer bypasses breast cancer as leading cause of cancer death for women in developed countries
An estimated 14.1 million new cancer cases and 8.2 million cancer deaths occurred in 2012, although incidences of certain cancers, such as lung cancer, are increasing rapidly in less developed countries, according to GLOBOCAN 2012, a research project produced by the International Agency for Research on Cancer (IARC) to determine worldwide estimates of cancer incidence and mortality.
Interestingly, less developed countries account for only 57% of cases and 65% of cancer deaths worldwide, despite their share of the population surveyed being significantly larger than that of more developed countries.
Lung cancer is the leading cause of cancer death among males in both more and less developed countries, and among females in more developed countries. Breast cancer remains the leading cause of cancer death among females in less developed countries, although this may change as breast cancer testing becomes more commonplace and more countries adapt Western lifestyle habits, the researchers noted.
Read the full article here: CA Cancer J. Clin. 2015;000:000-000 (doi:10.3322/caac.21262).
An estimated 14.1 million new cancer cases and 8.2 million cancer deaths occurred in 2012, although incidences of certain cancers, such as lung cancer, are increasing rapidly in less developed countries, according to GLOBOCAN 2012, a research project produced by the International Agency for Research on Cancer (IARC) to determine worldwide estimates of cancer incidence and mortality.
Interestingly, less developed countries account for only 57% of cases and 65% of cancer deaths worldwide, despite their share of the population surveyed being significantly larger than that of more developed countries.
Lung cancer is the leading cause of cancer death among males in both more and less developed countries, and among females in more developed countries. Breast cancer remains the leading cause of cancer death among females in less developed countries, although this may change as breast cancer testing becomes more commonplace and more countries adapt Western lifestyle habits, the researchers noted.
Read the full article here: CA Cancer J. Clin. 2015;000:000-000 (doi:10.3322/caac.21262).
An estimated 14.1 million new cancer cases and 8.2 million cancer deaths occurred in 2012, although incidences of certain cancers, such as lung cancer, are increasing rapidly in less developed countries, according to GLOBOCAN 2012, a research project produced by the International Agency for Research on Cancer (IARC) to determine worldwide estimates of cancer incidence and mortality.
Interestingly, less developed countries account for only 57% of cases and 65% of cancer deaths worldwide, despite their share of the population surveyed being significantly larger than that of more developed countries.
Lung cancer is the leading cause of cancer death among males in both more and less developed countries, and among females in more developed countries. Breast cancer remains the leading cause of cancer death among females in less developed countries, although this may change as breast cancer testing becomes more commonplace and more countries adapt Western lifestyle habits, the researchers noted.
Read the full article here: CA Cancer J. Clin. 2015;000:000-000 (doi:10.3322/caac.21262).