User login
Palonosetron and netupitant for prevention of chemotherapy-induced nausea and vomiting
The US Food and Drug Administration (FDA) recently approved NEPA, an oral fixed-dose combination of netupitant and palonosetron for treatment of chemotherapy-induced nausea and vomiting (CINV). Palonosetron is a pharmacologically distinct, best-in-class serotonin (5-hydroxytryptamine) type 3 (5-HT3) receptor antagonist, which prevents CINV during the acute phase (0-24 h) after administration of chemotherapy, and netupitant is a potent and selective neurokinin-1 (NK-1) receptor antagonist, which prevents CINV during both the acute and delayed (25-120 h) phases. The 2 agents have also been shown potentially to act synergistically in inhibiting NK-1 receptor activity.
Click on the PDF icon at the top of this introduction to read the full article.
The US Food and Drug Administration (FDA) recently approved NEPA, an oral fixed-dose combination of netupitant and palonosetron for treatment of chemotherapy-induced nausea and vomiting (CINV). Palonosetron is a pharmacologically distinct, best-in-class serotonin (5-hydroxytryptamine) type 3 (5-HT3) receptor antagonist, which prevents CINV during the acute phase (0-24 h) after administration of chemotherapy, and netupitant is a potent and selective neurokinin-1 (NK-1) receptor antagonist, which prevents CINV during both the acute and delayed (25-120 h) phases. The 2 agents have also been shown potentially to act synergistically in inhibiting NK-1 receptor activity.
Click on the PDF icon at the top of this introduction to read the full article.
The US Food and Drug Administration (FDA) recently approved NEPA, an oral fixed-dose combination of netupitant and palonosetron for treatment of chemotherapy-induced nausea and vomiting (CINV). Palonosetron is a pharmacologically distinct, best-in-class serotonin (5-hydroxytryptamine) type 3 (5-HT3) receptor antagonist, which prevents CINV during the acute phase (0-24 h) after administration of chemotherapy, and netupitant is a potent and selective neurokinin-1 (NK-1) receptor antagonist, which prevents CINV during both the acute and delayed (25-120 h) phases. The 2 agents have also been shown potentially to act synergistically in inhibiting NK-1 receptor activity.
Click on the PDF icon at the top of this introduction to read the full article.
Managing change in oncology
PD-L1 blockade breaks through triple-negative breast cancer
Metastatic triple-negative breast cancer appears to be the latest hard-to-treat cancer to yield to the juggernaut that is now anti-PD-L1 immunotherapy.
MPDL3280L, an investigational monoclonal antibody against programmed death ligand 1 (PD-L1), posted an overall response rate of 19% among 21 evaluable patients in a phase Ia trial (95% confidence interval, 5-42).

This included two complete responses in patients with high PD-L1 expression and two partial responses. Three of the four responses are ongoing, Dr. Leisha Emens reported at the annual meeting of the American Association for Cancer Research.
“I think it very well could be the first targeted therapy that bears out in a larger trial,” she said during a press briefing. “These data are still early, and we need to enroll and treat a lot more patients with this agent, but I think it has great, great promise for this particular breast cancer subtype.”
There is great unmet need for new treatments in triple-negative breast cancer (TNBC) because it has a worse prognosis than other breast cancer subtypes do, and the only approved treatment option in the United States is chemotherapy.
TNBC is a good candidate for immunotherapy, particularly PD-L1 targeted therapies, because it has a higher mutation rate than do other breast cancer subtypes. This produces neoantigens that can be recognized as foreign by the immune system and be more effective targets for an immune response, Dr. Emens of the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore, explained.
TNBC also has higher PD-L1 expression levels, which can inhibit T-cell antitumor responses, and more tumor-infiltrating lymphocytes, which can facilitate a immune response and are associated with improved outcomes when present in high numbers.
MPDL3280A is designed to inhibit the binding of PD-L1 to programmed death receptor 1 (PD-1) and B7.1, which can restore antitumor T-cell activity and enhance T-cell priming, she said.
The checkpoint inhibitor received breakthrough therapy designation for metastatic bladder cancer in 2014 and a second designation in non–small cell lung cancer in February.
The ongoing phase Ia trial enrolled 54 women with metastatic TNBC and an ECOG performance status of 0 or 1. This included 21 patients initially selected for high PD-L1 expression levels (at least 5%) on their immune cells and 33 all-comers. MPDL3280A intravenous infusions were given every 3 weeks at doses of 15 mg/kg, 20 mg/kg, or 1,200 mg. Efficacy was evaluated in the 21 patients and safety in all 54 patients.
At 24 weeks, progression-free survival was 27% (95% CI, 7-47), Dr. Emens said.The median duration of response (range, 18-56+ weeks) has not been reached.
Three patients with progressive disease experienced pseudoprogression, where the target lesion shrank, but new lesions developed. Pseudoprogression, a feature of checkpoint inhibition that also has been seen with ipilimumab (Yervoy), is new for many physicians to manage and requires the patient’s entire clinical picture be taken into account, Dr. Emens said.
“An important component of the phenomenon of pseudoprogression is that if you see evidence of new lesions on a scan and the patient’s doing clinically well, you continue to treat and then reevaluate subsequent to that,” she said. “If there’s progression at that point, then potentially you consider changing the therapy or just following the patient more closely. Another potential option to help sort through that is to try and obtain tissue from one of those lesions to get some idea of what is happening, if it’s a phenomenon of the inflammatory response or a response to the therapy.”
Dr. Emens detailed one such case in which three target lesions decreased in size from baseline on 9- and 20-month follow-up scans, but newly enlarged axillary nodes that appeared inflammatory or necrotic developed near the third target lesion at 9 months. The patient remained on therapy and is doing well today, with further shrinkage of the target lesion and regression of the axillary nodes at 20 months.
MPDL3280A was generally well tolerated, with fatigue, nausea, fever, decreased appetite, and asthenia being the most common adverse events, Dr. Emens said. In all, 11% of patients experienced grade 3 treatment-related events. Two deaths, assessed as drug related by the investigator, are under investigation.
Press briefing moderator Louis M. Winer, director of the Georgetown Lombardi Comprehensive Cancer Center, commented that it wasn’t that long ago that phase I investigators were pleased if they saw even a hint of activity that would justify moving forward to phase II. The activity signals with the checkpoint inhibitors, however, are “unequivocal” and the implications for the future treatment of people with triple negative breast cancer are “very, very exciting,” according to Dr. Winer.
Earlier in the meeting, stellar results with the checkpoint inhibitor pembrolizumab from the KEYNOTE-006 trial upended the treatment paradigm for advanced melanoma. Pembrolizumab has been evaluated in TNBC and the safety profile and responses are similar to those with MPDL3280A, Dr. Emens said.
A global phase III trial evaluating MPDL3280A in combination with paclitaxel (Abraxane) as first-line therapy for metastatic TNBC is preparing to launch.
On Twitter @pwendl
Metastatic triple-negative breast cancer appears to be the latest hard-to-treat cancer to yield to the juggernaut that is now anti-PD-L1 immunotherapy.
MPDL3280L, an investigational monoclonal antibody against programmed death ligand 1 (PD-L1), posted an overall response rate of 19% among 21 evaluable patients in a phase Ia trial (95% confidence interval, 5-42).
This included two complete responses in patients with high PD-L1 expression and two partial responses. Three of the four responses are ongoing, Dr. Leisha Emens reported at the annual meeting of the American Association for Cancer Research.
“I think it very well could be the first targeted therapy that bears out in a larger trial,” she said during a press briefing. “These data are still early, and we need to enroll and treat a lot more patients with this agent, but I think it has great, great promise for this particular breast cancer subtype.”
There is great unmet need for new treatments in triple-negative breast cancer (TNBC) because it has a worse prognosis than other breast cancer subtypes do, and the only approved treatment option in the United States is chemotherapy.
TNBC is a good candidate for immunotherapy, particularly PD-L1 targeted therapies, because it has a higher mutation rate than do other breast cancer subtypes. This produces neoantigens that can be recognized as foreign by the immune system and be more effective targets for an immune response, Dr. Emens of the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore, explained.
TNBC also has higher PD-L1 expression levels, which can inhibit T-cell antitumor responses, and more tumor-infiltrating lymphocytes, which can facilitate a immune response and are associated with improved outcomes when present in high numbers.
MPDL3280A is designed to inhibit the binding of PD-L1 to programmed death receptor 1 (PD-1) and B7.1, which can restore antitumor T-cell activity and enhance T-cell priming, she said.
The checkpoint inhibitor received breakthrough therapy designation for metastatic bladder cancer in 2014 and a second designation in non–small cell lung cancer in February.
The ongoing phase Ia trial enrolled 54 women with metastatic TNBC and an ECOG performance status of 0 or 1. This included 21 patients initially selected for high PD-L1 expression levels (at least 5%) on their immune cells and 33 all-comers. MPDL3280A intravenous infusions were given every 3 weeks at doses of 15 mg/kg, 20 mg/kg, or 1,200 mg. Efficacy was evaluated in the 21 patients and safety in all 54 patients.
At 24 weeks, progression-free survival was 27% (95% CI, 7-47), Dr. Emens said.The median duration of response (range, 18-56+ weeks) has not been reached.
Three patients with progressive disease experienced pseudoprogression, where the target lesion shrank, but new lesions developed. Pseudoprogression, a feature of checkpoint inhibition that also has been seen with ipilimumab (Yervoy), is new for many physicians to manage and requires the patient’s entire clinical picture be taken into account, Dr. Emens said.
“An important component of the phenomenon of pseudoprogression is that if you see evidence of new lesions on a scan and the patient’s doing clinically well, you continue to treat and then reevaluate subsequent to that,” she said. “If there’s progression at that point, then potentially you consider changing the therapy or just following the patient more closely. Another potential option to help sort through that is to try and obtain tissue from one of those lesions to get some idea of what is happening, if it’s a phenomenon of the inflammatory response or a response to the therapy.”
Dr. Emens detailed one such case in which three target lesions decreased in size from baseline on 9- and 20-month follow-up scans, but newly enlarged axillary nodes that appeared inflammatory or necrotic developed near the third target lesion at 9 months. The patient remained on therapy and is doing well today, with further shrinkage of the target lesion and regression of the axillary nodes at 20 months.
MPDL3280A was generally well tolerated, with fatigue, nausea, fever, decreased appetite, and asthenia being the most common adverse events, Dr. Emens said. In all, 11% of patients experienced grade 3 treatment-related events. Two deaths, assessed as drug related by the investigator, are under investigation.
Press briefing moderator Louis M. Winer, director of the Georgetown Lombardi Comprehensive Cancer Center, commented that it wasn’t that long ago that phase I investigators were pleased if they saw even a hint of activity that would justify moving forward to phase II. The activity signals with the checkpoint inhibitors, however, are “unequivocal” and the implications for the future treatment of people with triple negative breast cancer are “very, very exciting,” according to Dr. Winer.
Earlier in the meeting, stellar results with the checkpoint inhibitor pembrolizumab from the KEYNOTE-006 trial upended the treatment paradigm for advanced melanoma. Pembrolizumab has been evaluated in TNBC and the safety profile and responses are similar to those with MPDL3280A, Dr. Emens said.
A global phase III trial evaluating MPDL3280A in combination with paclitaxel (Abraxane) as first-line therapy for metastatic TNBC is preparing to launch.
On Twitter @pwendl
Metastatic triple-negative breast cancer appears to be the latest hard-to-treat cancer to yield to the juggernaut that is now anti-PD-L1 immunotherapy.
MPDL3280L, an investigational monoclonal antibody against programmed death ligand 1 (PD-L1), posted an overall response rate of 19% among 21 evaluable patients in a phase Ia trial (95% confidence interval, 5-42).
This included two complete responses in patients with high PD-L1 expression and two partial responses. Three of the four responses are ongoing, Dr. Leisha Emens reported at the annual meeting of the American Association for Cancer Research.
“I think it very well could be the first targeted therapy that bears out in a larger trial,” she said during a press briefing. “These data are still early, and we need to enroll and treat a lot more patients with this agent, but I think it has great, great promise for this particular breast cancer subtype.”
There is great unmet need for new treatments in triple-negative breast cancer (TNBC) because it has a worse prognosis than other breast cancer subtypes do, and the only approved treatment option in the United States is chemotherapy.
TNBC is a good candidate for immunotherapy, particularly PD-L1 targeted therapies, because it has a higher mutation rate than do other breast cancer subtypes. This produces neoantigens that can be recognized as foreign by the immune system and be more effective targets for an immune response, Dr. Emens of the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore, explained.
TNBC also has higher PD-L1 expression levels, which can inhibit T-cell antitumor responses, and more tumor-infiltrating lymphocytes, which can facilitate a immune response and are associated with improved outcomes when present in high numbers.
MPDL3280A is designed to inhibit the binding of PD-L1 to programmed death receptor 1 (PD-1) and B7.1, which can restore antitumor T-cell activity and enhance T-cell priming, she said.
The checkpoint inhibitor received breakthrough therapy designation for metastatic bladder cancer in 2014 and a second designation in non–small cell lung cancer in February.
The ongoing phase Ia trial enrolled 54 women with metastatic TNBC and an ECOG performance status of 0 or 1. This included 21 patients initially selected for high PD-L1 expression levels (at least 5%) on their immune cells and 33 all-comers. MPDL3280A intravenous infusions were given every 3 weeks at doses of 15 mg/kg, 20 mg/kg, or 1,200 mg. Efficacy was evaluated in the 21 patients and safety in all 54 patients.
At 24 weeks, progression-free survival was 27% (95% CI, 7-47), Dr. Emens said.The median duration of response (range, 18-56+ weeks) has not been reached.
Three patients with progressive disease experienced pseudoprogression, where the target lesion shrank, but new lesions developed. Pseudoprogression, a feature of checkpoint inhibition that also has been seen with ipilimumab (Yervoy), is new for many physicians to manage and requires the patient’s entire clinical picture be taken into account, Dr. Emens said.
“An important component of the phenomenon of pseudoprogression is that if you see evidence of new lesions on a scan and the patient’s doing clinically well, you continue to treat and then reevaluate subsequent to that,” she said. “If there’s progression at that point, then potentially you consider changing the therapy or just following the patient more closely. Another potential option to help sort through that is to try and obtain tissue from one of those lesions to get some idea of what is happening, if it’s a phenomenon of the inflammatory response or a response to the therapy.”
Dr. Emens detailed one such case in which three target lesions decreased in size from baseline on 9- and 20-month follow-up scans, but newly enlarged axillary nodes that appeared inflammatory or necrotic developed near the third target lesion at 9 months. The patient remained on therapy and is doing well today, with further shrinkage of the target lesion and regression of the axillary nodes at 20 months.
MPDL3280A was generally well tolerated, with fatigue, nausea, fever, decreased appetite, and asthenia being the most common adverse events, Dr. Emens said. In all, 11% of patients experienced grade 3 treatment-related events. Two deaths, assessed as drug related by the investigator, are under investigation.
Press briefing moderator Louis M. Winer, director of the Georgetown Lombardi Comprehensive Cancer Center, commented that it wasn’t that long ago that phase I investigators were pleased if they saw even a hint of activity that would justify moving forward to phase II. The activity signals with the checkpoint inhibitors, however, are “unequivocal” and the implications for the future treatment of people with triple negative breast cancer are “very, very exciting,” according to Dr. Winer.
Earlier in the meeting, stellar results with the checkpoint inhibitor pembrolizumab from the KEYNOTE-006 trial upended the treatment paradigm for advanced melanoma. Pembrolizumab has been evaluated in TNBC and the safety profile and responses are similar to those with MPDL3280A, Dr. Emens said.
A global phase III trial evaluating MPDL3280A in combination with paclitaxel (Abraxane) as first-line therapy for metastatic TNBC is preparing to launch.
On Twitter @pwendl
FROM THE AACR ANNUAL MEETING
Key clinical point: The investigative anti-PD-L1 immunotherapy MPDL3280A was clinically active and generally well tolerated in metastatic triple-negative breast cancer.
Major finding: The objective response rate was 19% and 24-week progression-free survival 27%.
Data source: Phase Ia trial in 54 women with metastatic triple-negative breast cancer.
Disclosures: Genentech/Roche sponsored the study. Dr. Emens reported consulting for Vaccinex, Celgene, Aveo, Bristol-Myers Squibb, and research/grant support from Genentech, Roche, EMD Serono, MaxCyte, Amplimmune, and Merck. Dr. Emens and her institution also receive payments and royalty on a breast cancer vaccine.

Task Force: Start biennial mammograms at age 50
The U.S. Preventive Services Task Force is continuing to recommend routine mammograms every 2 years for women starting at age 50, according to newly released draft screening recommendations for breast cancer.
The draft recommendations, issued on April 20, largely reaffirm the group’s advice from 2009. Recent research findings have not altered the USPSTF’s key recommendation: routine mammograms every 2 years for women 50-74 years old. The USPSTF gave this recommendation a grade B, meaning that the evidence is strong enough for clinicians to adopt this practice. For women 75 years or older, the evidence remains inadequate to recommend for or against routine mammography.
For women 40-49 years old, the task force continued to state that the decision to start screening should be an individual one. The USPSTF gave mammography screening in this age group a grade C, concluding that the benefit of screening mammography outweighs the harms, but only by a small amount.

“Women who place a higher value on the potential benefit than the potential harms may choose to begin biennial screening between the ages of 40 and 49 years,” the task force members wrote.
In contrast, the American College of Obstetricians and Gynecologists, the American Cancer Society, the American College of Radiology, and the Society for Breast Imaging all recommend annual mammography starting at age 40.
The USPSTF is not advising against screening at age 40, but the task force members wrote that younger women with average breast cancer risk “must weigh a very important but infrequent benefit (small reduction in breast cancer deaths) against a group of meaningful and much more common harms (overdiagnosis and overtreatment; unnecessary and sometimes invasive follow-up testing; psychological harms associated with false-positive tests; and false reassurance from false-negative tests).”
The USPSTF’s recommendations apply to asymptomatic women without preexisting breast cancer, a previously diagnosed high-risk breast lesion, underlying genetic mutations, or a family history that puts them at high risk.
New for 2015, the group also weighed in on tomosynthesis (3-D mammography) for primary screening, and additional screening – ultrasound, MRI, tomosynthesis, or other methods – in women with dense breasts but otherwise negative mammogram results.
“In both cases, while there is some information about the accuracy of these modalities, there is no information on the effects of their use on health outcomes, such as breast cancer incidence, mortality, or overdiagnosis rates,” the USPSTF wrote.
The task force did not recommend for or against their use, stating only that more research is needed.
“From the limited data available, tomosynthesis appears to reduce recall rates for false-positive tests, compared with 2-D digital mammography alone. Available data also suggest that tomosynthesis increases the cancer detection rate, compared with 2-D digital mammography alone. However, current study designs do not answer the question of whether all of the additional cancers detected would have become clinically significant or whether there is an incremental clinical benefit to detecting these cancers earlier,” the task force members wrote.
Also, as currently practiced in most settings, tomosynthesis exposes women to about twice the amount of radiation of 2-D digital mammography. Tomosynthesis may also increase the rate of breast biopsy in women with abnormal findings, compared with 2-D digital mammography, according to the draft recommendations.
Meanwhile, “many important questions remain about the potential role of breast density in individualizing screening approaches; the current evidence is insufficient to recommend a specific screening strategy for women with increased breast density,” the group said.
The draft recommendations are available at www.screeningforbreastcancer.org. The group will accept public comments on the recommendations through May 18.
The U.S. Preventive Services Task Force is continuing to recommend routine mammograms every 2 years for women starting at age 50, according to newly released draft screening recommendations for breast cancer.
The draft recommendations, issued on April 20, largely reaffirm the group’s advice from 2009. Recent research findings have not altered the USPSTF’s key recommendation: routine mammograms every 2 years for women 50-74 years old. The USPSTF gave this recommendation a grade B, meaning that the evidence is strong enough for clinicians to adopt this practice. For women 75 years or older, the evidence remains inadequate to recommend for or against routine mammography.
For women 40-49 years old, the task force continued to state that the decision to start screening should be an individual one. The USPSTF gave mammography screening in this age group a grade C, concluding that the benefit of screening mammography outweighs the harms, but only by a small amount.
“Women who place a higher value on the potential benefit than the potential harms may choose to begin biennial screening between the ages of 40 and 49 years,” the task force members wrote.
In contrast, the American College of Obstetricians and Gynecologists, the American Cancer Society, the American College of Radiology, and the Society for Breast Imaging all recommend annual mammography starting at age 40.
The USPSTF is not advising against screening at age 40, but the task force members wrote that younger women with average breast cancer risk “must weigh a very important but infrequent benefit (small reduction in breast cancer deaths) against a group of meaningful and much more common harms (overdiagnosis and overtreatment; unnecessary and sometimes invasive follow-up testing; psychological harms associated with false-positive tests; and false reassurance from false-negative tests).”
The USPSTF’s recommendations apply to asymptomatic women without preexisting breast cancer, a previously diagnosed high-risk breast lesion, underlying genetic mutations, or a family history that puts them at high risk.
New for 2015, the group also weighed in on tomosynthesis (3-D mammography) for primary screening, and additional screening – ultrasound, MRI, tomosynthesis, or other methods – in women with dense breasts but otherwise negative mammogram results.
“In both cases, while there is some information about the accuracy of these modalities, there is no information on the effects of their use on health outcomes, such as breast cancer incidence, mortality, or overdiagnosis rates,” the USPSTF wrote.
The task force did not recommend for or against their use, stating only that more research is needed.
“From the limited data available, tomosynthesis appears to reduce recall rates for false-positive tests, compared with 2-D digital mammography alone. Available data also suggest that tomosynthesis increases the cancer detection rate, compared with 2-D digital mammography alone. However, current study designs do not answer the question of whether all of the additional cancers detected would have become clinically significant or whether there is an incremental clinical benefit to detecting these cancers earlier,” the task force members wrote.
Also, as currently practiced in most settings, tomosynthesis exposes women to about twice the amount of radiation of 2-D digital mammography. Tomosynthesis may also increase the rate of breast biopsy in women with abnormal findings, compared with 2-D digital mammography, according to the draft recommendations.
Meanwhile, “many important questions remain about the potential role of breast density in individualizing screening approaches; the current evidence is insufficient to recommend a specific screening strategy for women with increased breast density,” the group said.
The draft recommendations are available at www.screeningforbreastcancer.org. The group will accept public comments on the recommendations through May 18.
The U.S. Preventive Services Task Force is continuing to recommend routine mammograms every 2 years for women starting at age 50, according to newly released draft screening recommendations for breast cancer.
The draft recommendations, issued on April 20, largely reaffirm the group’s advice from 2009. Recent research findings have not altered the USPSTF’s key recommendation: routine mammograms every 2 years for women 50-74 years old. The USPSTF gave this recommendation a grade B, meaning that the evidence is strong enough for clinicians to adopt this practice. For women 75 years or older, the evidence remains inadequate to recommend for or against routine mammography.
For women 40-49 years old, the task force continued to state that the decision to start screening should be an individual one. The USPSTF gave mammography screening in this age group a grade C, concluding that the benefit of screening mammography outweighs the harms, but only by a small amount.
“Women who place a higher value on the potential benefit than the potential harms may choose to begin biennial screening between the ages of 40 and 49 years,” the task force members wrote.
In contrast, the American College of Obstetricians and Gynecologists, the American Cancer Society, the American College of Radiology, and the Society for Breast Imaging all recommend annual mammography starting at age 40.
The USPSTF is not advising against screening at age 40, but the task force members wrote that younger women with average breast cancer risk “must weigh a very important but infrequent benefit (small reduction in breast cancer deaths) against a group of meaningful and much more common harms (overdiagnosis and overtreatment; unnecessary and sometimes invasive follow-up testing; psychological harms associated with false-positive tests; and false reassurance from false-negative tests).”
The USPSTF’s recommendations apply to asymptomatic women without preexisting breast cancer, a previously diagnosed high-risk breast lesion, underlying genetic mutations, or a family history that puts them at high risk.
New for 2015, the group also weighed in on tomosynthesis (3-D mammography) for primary screening, and additional screening – ultrasound, MRI, tomosynthesis, or other methods – in women with dense breasts but otherwise negative mammogram results.
“In both cases, while there is some information about the accuracy of these modalities, there is no information on the effects of their use on health outcomes, such as breast cancer incidence, mortality, or overdiagnosis rates,” the USPSTF wrote.
The task force did not recommend for or against their use, stating only that more research is needed.
“From the limited data available, tomosynthesis appears to reduce recall rates for false-positive tests, compared with 2-D digital mammography alone. Available data also suggest that tomosynthesis increases the cancer detection rate, compared with 2-D digital mammography alone. However, current study designs do not answer the question of whether all of the additional cancers detected would have become clinically significant or whether there is an incremental clinical benefit to detecting these cancers earlier,” the task force members wrote.
Also, as currently practiced in most settings, tomosynthesis exposes women to about twice the amount of radiation of 2-D digital mammography. Tomosynthesis may also increase the rate of breast biopsy in women with abnormal findings, compared with 2-D digital mammography, according to the draft recommendations.
Meanwhile, “many important questions remain about the potential role of breast density in individualizing screening approaches; the current evidence is insufficient to recommend a specific screening strategy for women with increased breast density,” the group said.
The draft recommendations are available at www.screeningforbreastcancer.org. The group will accept public comments on the recommendations through May 18.
FROM THE U.S. PREVENTIVE SERVICES TASK FORCE

Class of 2015: New drugs projected to earn billions and billions
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
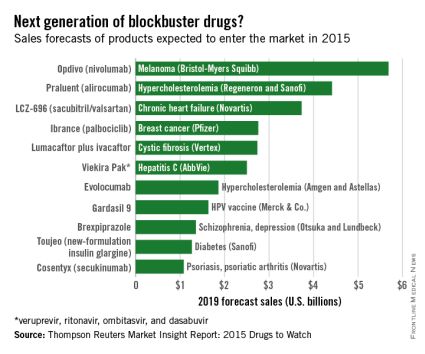
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Sleep disorders in patients with cancer
Sleep disturbances are common among patients with cancer for many reasons. Sleep problems can be present at any stage during treatment for cancer and in some patients, sleep disturbance may be the presenting symptoms that lead to the diagnosis of some types of cancer. Poor sleep impairs quality of life In people with cancer, but most do not specifically complain of sleep problems unless they are explicitly asked. Insomnia and fatigue are most common sleep disorders in this cohort, although primary sleep disorders, including obstructive sleep apnea and restless legs syndrome, which are common in the general population, have not been carefully studied in the oncology setting despite significant their impairment of quality of life.
Click on the PDF icon at the top of this introduction to read the full article.
disorder
Sleep disturbances are common among patients with cancer for many reasons. Sleep problems can be present at any stage during treatment for cancer and in some patients, sleep disturbance may be the presenting symptoms that lead to the diagnosis of some types of cancer. Poor sleep impairs quality of life In people with cancer, but most do not specifically complain of sleep problems unless they are explicitly asked. Insomnia and fatigue are most common sleep disorders in this cohort, although primary sleep disorders, including obstructive sleep apnea and restless legs syndrome, which are common in the general population, have not been carefully studied in the oncology setting despite significant their impairment of quality of life.
Click on the PDF icon at the top of this introduction to read the full article.
Sleep disturbances are common among patients with cancer for many reasons. Sleep problems can be present at any stage during treatment for cancer and in some patients, sleep disturbance may be the presenting symptoms that lead to the diagnosis of some types of cancer. Poor sleep impairs quality of life In people with cancer, but most do not specifically complain of sleep problems unless they are explicitly asked. Insomnia and fatigue are most common sleep disorders in this cohort, although primary sleep disorders, including obstructive sleep apnea and restless legs syndrome, which are common in the general population, have not been carefully studied in the oncology setting despite significant their impairment of quality of life.
Click on the PDF icon at the top of this introduction to read the full article.
disorder
disorder
Neoadjuvant therapy facilitates breast conservation
HOUSTON – For some women with breast cancer, neoadjuvant therapy can increase the likelihood of breast-conserving treatment and may limit the extent of axillary dissection, a breast cancer researcher says.
“Neoadjuvant chemotherapy has long been used in the management of inflammatory breast cancer, in patients with locally advanced, or inoperable disease, and it’s increasingly being used in patients who have operable breast cancer,” said Dr. Elizabeth A. Mittendorf of the University of Texas MD Anderson Cancer Center, Houston.

A meta-analysis published in 2007 suggested that neoadjuvant therapy in patients with operable breast cancer reduced the mastectomy rate by 17%, a figure that Dr. Mittendorf said likely underestimates the benefit, because many of the trials included in the analysis did not require patients to be considered for breast conservation at presentation.
The meta-analysis also showed that local recurrence rates did not differ from those seen with mastectomy when patients treated with neoadjuvant therapy were downstaged to breast-conserving therapy, and that there were no differences in local recurrence rates for neoadjuvant vs. adjuvant chemotherapy stratified by type of surgery, Dr. Mittendorf said at the annual Society of Surgical Oncology Cancer Symposium.
Key clinical trials, including the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and B-27 trials, showed that neoadjuvant chemotherapy did not have an effect on either disease-free or overall survival compared with adjuvant chemotherapy, Dr. Mittendorf noted.
Response to neoadjuvant chemotherapy is also a good predictor of prognosis, she said, pointing to a pooled analysis of 12 studies published in 2014 in The Lancet. The authors of the analysis reported that patients with a pathologic complete response (pCR; no invasive disease in either the breast or axilla) after neoadjuvant chemotherapy had significantly improved survival, with the greatest prognostic values seen in patients with aggressive tumor subtypes.
Factors to consider when selecting neoadjuvant chemotherapy include:
• Tumor size.
• Lymph node status.
• Estrogen, progesterone, and/or HER2 status.
• Treatment sensitivity (as measured by Ki-67 or other markers).
• Pathologic complete response rates.
Chemo for HR-positive?
“With respect to hormone receptor–positive breast cancer, I think the most important question for these patients is do they even need chemotherapy?” Dr. Mittendorf said.
Hormone receptor–positive (HR-positive) breast cancers have been shown to be less responsive to neoadjuvant chemotherapy, and pCR is less prognostic of outcome in this tumor subtype. Older patients with HR-positive cancers who are borderline candidates for breast-conserving therapy might benefit from neoadjuvant therapy with an aromatase inhibitor, she noted.
HER2-positive disease
For patients with HER2-positive breast cancers, it may be possible to tailor neoadjuvant therapy, so that patients who achieve a pCR with neoadjuvant trastuzumab (Herceptin) might be spared an additional 6 months of adjuvant therapy. Dr. Mittendorf’s group published a recent study
Combination anti-HER2 therapies (trastuzumab and pertuzumab [Perjeta] as used in the NeoSphere Trial may help to improve pCR rates and outcomes in patients with HER2-positive tumors, Dr. Mittendorf said.
Triple negative disease
Among patients with triple-negative breast cancer (tumors lacking hormonal receptors and HER2), those who have residual cancer after neoadjuvant chemotherapy have a poor prognosis. At MD Anderson, patients with localized triple-negative breast cancer who are scheduled to receive neoadjuvant chemotherapy first have a biopsy with molecular profiling, and are immediately started on an anthracycline-based regimen.
Patients who have a response to the chemotherapy proceed to receive a taxane, while nonresponders will be triaged onto phase II studies based on the subtype of triple-negative breast cancer. Patients who are positive for BRCA mutations will be started on a carboplatin/paclitaxel regimen, while those with mesenchymal tumor subtypes will be started on a phosphoinositide 3-kinase (PI3K) inhibitor, and those with basal-like tumors will be started on an immunotherapy protocol.Better understanding of the biology of different tumor subtypes may also help to reduce the extent of axillary surgery, by helping clinicians to identify those patients who are likely to have a nodal pCR, Dr. Mittendorf said.
HOUSTON – For some women with breast cancer, neoadjuvant therapy can increase the likelihood of breast-conserving treatment and may limit the extent of axillary dissection, a breast cancer researcher says.
“Neoadjuvant chemotherapy has long been used in the management of inflammatory breast cancer, in patients with locally advanced, or inoperable disease, and it’s increasingly being used in patients who have operable breast cancer,” said Dr. Elizabeth A. Mittendorf of the University of Texas MD Anderson Cancer Center, Houston.
A meta-analysis published in 2007 suggested that neoadjuvant therapy in patients with operable breast cancer reduced the mastectomy rate by 17%, a figure that Dr. Mittendorf said likely underestimates the benefit, because many of the trials included in the analysis did not require patients to be considered for breast conservation at presentation.
The meta-analysis also showed that local recurrence rates did not differ from those seen with mastectomy when patients treated with neoadjuvant therapy were downstaged to breast-conserving therapy, and that there were no differences in local recurrence rates for neoadjuvant vs. adjuvant chemotherapy stratified by type of surgery, Dr. Mittendorf said at the annual Society of Surgical Oncology Cancer Symposium.
Key clinical trials, including the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and B-27 trials, showed that neoadjuvant chemotherapy did not have an effect on either disease-free or overall survival compared with adjuvant chemotherapy, Dr. Mittendorf noted.
Response to neoadjuvant chemotherapy is also a good predictor of prognosis, she said, pointing to a pooled analysis of 12 studies published in 2014 in The Lancet. The authors of the analysis reported that patients with a pathologic complete response (pCR; no invasive disease in either the breast or axilla) after neoadjuvant chemotherapy had significantly improved survival, with the greatest prognostic values seen in patients with aggressive tumor subtypes.
Factors to consider when selecting neoadjuvant chemotherapy include:
• Tumor size.
• Lymph node status.
• Estrogen, progesterone, and/or HER2 status.
• Treatment sensitivity (as measured by Ki-67 or other markers).
• Pathologic complete response rates.
Chemo for HR-positive?
“With respect to hormone receptor–positive breast cancer, I think the most important question for these patients is do they even need chemotherapy?” Dr. Mittendorf said.
Hormone receptor–positive (HR-positive) breast cancers have been shown to be less responsive to neoadjuvant chemotherapy, and pCR is less prognostic of outcome in this tumor subtype. Older patients with HR-positive cancers who are borderline candidates for breast-conserving therapy might benefit from neoadjuvant therapy with an aromatase inhibitor, she noted.
HER2-positive disease
For patients with HER2-positive breast cancers, it may be possible to tailor neoadjuvant therapy, so that patients who achieve a pCR with neoadjuvant trastuzumab (Herceptin) might be spared an additional 6 months of adjuvant therapy. Dr. Mittendorf’s group published a recent study
Combination anti-HER2 therapies (trastuzumab and pertuzumab [Perjeta] as used in the NeoSphere Trial may help to improve pCR rates and outcomes in patients with HER2-positive tumors, Dr. Mittendorf said.
Triple negative disease
Among patients with triple-negative breast cancer (tumors lacking hormonal receptors and HER2), those who have residual cancer after neoadjuvant chemotherapy have a poor prognosis. At MD Anderson, patients with localized triple-negative breast cancer who are scheduled to receive neoadjuvant chemotherapy first have a biopsy with molecular profiling, and are immediately started on an anthracycline-based regimen.
Patients who have a response to the chemotherapy proceed to receive a taxane, while nonresponders will be triaged onto phase II studies based on the subtype of triple-negative breast cancer. Patients who are positive for BRCA mutations will be started on a carboplatin/paclitaxel regimen, while those with mesenchymal tumor subtypes will be started on a phosphoinositide 3-kinase (PI3K) inhibitor, and those with basal-like tumors will be started on an immunotherapy protocol.Better understanding of the biology of different tumor subtypes may also help to reduce the extent of axillary surgery, by helping clinicians to identify those patients who are likely to have a nodal pCR, Dr. Mittendorf said.
HOUSTON – For some women with breast cancer, neoadjuvant therapy can increase the likelihood of breast-conserving treatment and may limit the extent of axillary dissection, a breast cancer researcher says.
“Neoadjuvant chemotherapy has long been used in the management of inflammatory breast cancer, in patients with locally advanced, or inoperable disease, and it’s increasingly being used in patients who have operable breast cancer,” said Dr. Elizabeth A. Mittendorf of the University of Texas MD Anderson Cancer Center, Houston.
A meta-analysis published in 2007 suggested that neoadjuvant therapy in patients with operable breast cancer reduced the mastectomy rate by 17%, a figure that Dr. Mittendorf said likely underestimates the benefit, because many of the trials included in the analysis did not require patients to be considered for breast conservation at presentation.
The meta-analysis also showed that local recurrence rates did not differ from those seen with mastectomy when patients treated with neoadjuvant therapy were downstaged to breast-conserving therapy, and that there were no differences in local recurrence rates for neoadjuvant vs. adjuvant chemotherapy stratified by type of surgery, Dr. Mittendorf said at the annual Society of Surgical Oncology Cancer Symposium.
Key clinical trials, including the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and B-27 trials, showed that neoadjuvant chemotherapy did not have an effect on either disease-free or overall survival compared with adjuvant chemotherapy, Dr. Mittendorf noted.
Response to neoadjuvant chemotherapy is also a good predictor of prognosis, she said, pointing to a pooled analysis of 12 studies published in 2014 in The Lancet. The authors of the analysis reported that patients with a pathologic complete response (pCR; no invasive disease in either the breast or axilla) after neoadjuvant chemotherapy had significantly improved survival, with the greatest prognostic values seen in patients with aggressive tumor subtypes.
Factors to consider when selecting neoadjuvant chemotherapy include:
• Tumor size.
• Lymph node status.
• Estrogen, progesterone, and/or HER2 status.
• Treatment sensitivity (as measured by Ki-67 or other markers).
• Pathologic complete response rates.
Chemo for HR-positive?
“With respect to hormone receptor–positive breast cancer, I think the most important question for these patients is do they even need chemotherapy?” Dr. Mittendorf said.
Hormone receptor–positive (HR-positive) breast cancers have been shown to be less responsive to neoadjuvant chemotherapy, and pCR is less prognostic of outcome in this tumor subtype. Older patients with HR-positive cancers who are borderline candidates for breast-conserving therapy might benefit from neoadjuvant therapy with an aromatase inhibitor, she noted.
HER2-positive disease
For patients with HER2-positive breast cancers, it may be possible to tailor neoadjuvant therapy, so that patients who achieve a pCR with neoadjuvant trastuzumab (Herceptin) might be spared an additional 6 months of adjuvant therapy. Dr. Mittendorf’s group published a recent study
Combination anti-HER2 therapies (trastuzumab and pertuzumab [Perjeta] as used in the NeoSphere Trial may help to improve pCR rates and outcomes in patients with HER2-positive tumors, Dr. Mittendorf said.
Triple negative disease
Among patients with triple-negative breast cancer (tumors lacking hormonal receptors and HER2), those who have residual cancer after neoadjuvant chemotherapy have a poor prognosis. At MD Anderson, patients with localized triple-negative breast cancer who are scheduled to receive neoadjuvant chemotherapy first have a biopsy with molecular profiling, and are immediately started on an anthracycline-based regimen.
Patients who have a response to the chemotherapy proceed to receive a taxane, while nonresponders will be triaged onto phase II studies based on the subtype of triple-negative breast cancer. Patients who are positive for BRCA mutations will be started on a carboplatin/paclitaxel regimen, while those with mesenchymal tumor subtypes will be started on a phosphoinositide 3-kinase (PI3K) inhibitor, and those with basal-like tumors will be started on an immunotherapy protocol.Better understanding of the biology of different tumor subtypes may also help to reduce the extent of axillary surgery, by helping clinicians to identify those patients who are likely to have a nodal pCR, Dr. Mittendorf said.

Type, location of BRCA mutations influence risk
Among women who carry BRCA1 or BRCA2 mutations, the type and exact location of the mutation influences the risk it confers for breast and ovarian cancer, according to a report published online April 7 in JAMA.
Investigators examined differences in cancer risks by analyzing data in the Consortium of Investigators of Modifiers of BRCA (CIMBA), a collection of clinical and genetic information for carriers of disease-associated BRCA mutations in 33 countries.
For this study, data were assessed for 19,581 women with BRCA1 mutations and 11,900 women with BRCA2 mutations for whom there was sufficient information to estimate hazard ratios. The types of mutations included nonsense, frame shift, in-frame, missense, splicing, rearrangement, premature termination codons, and nonsense-mediated decay mutations, said Timothy R. Rebbeck, Ph.D., of Abramson Cancer Center and the Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, and his associates.
Among the study participants with BRCA1 mutations, 9,052 women (46%) developed breast cancer, 2,317 (12%) developed ovarian cancer, and 1,041 (5%) developed both breast and ovarian cancer. Among the women with BRCA2 mutations, 6,180 (52%) developed breast cancer, 682 (6%) developed ovarian cancer, and 272 (2%) developed both breast and ovarian cancer. A woman’s risk for cancer differed significantly according to the type of BRCA1 or BRCA2 mutation she carried and according to the location of the mutation on the nucleotide, the investigators said (JAMA 2015 April 7 [doi:10.1001/jama.2014.5985]).
Further research is needed to determine the absolute risks of cancer associated with each mutation and “to better understand what level of risk difference will change decision-making and standards of care, such as preventive surgery” for BRCA1 and BRCA2 carriers, Dr. Rebbeck and his associates added.
This study was funded primarily by Cancer Research UK and also was supported by the U.S. National Institutes of Health, the Basser Research Center at the University of Pennsylvania, the Breast Cancer Research Foundation, and the Rooney Family Foundation. Dr. Rebbeck reported having no financial disclosures; his associates reported numerous ties to industry sources.
Among women who carry BRCA1 or BRCA2 mutations, the type and exact location of the mutation influences the risk it confers for breast and ovarian cancer, according to a report published online April 7 in JAMA.
Investigators examined differences in cancer risks by analyzing data in the Consortium of Investigators of Modifiers of BRCA (CIMBA), a collection of clinical and genetic information for carriers of disease-associated BRCA mutations in 33 countries.
For this study, data were assessed for 19,581 women with BRCA1 mutations and 11,900 women with BRCA2 mutations for whom there was sufficient information to estimate hazard ratios. The types of mutations included nonsense, frame shift, in-frame, missense, splicing, rearrangement, premature termination codons, and nonsense-mediated decay mutations, said Timothy R. Rebbeck, Ph.D., of Abramson Cancer Center and the Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, and his associates.
Among the study participants with BRCA1 mutations, 9,052 women (46%) developed breast cancer, 2,317 (12%) developed ovarian cancer, and 1,041 (5%) developed both breast and ovarian cancer. Among the women with BRCA2 mutations, 6,180 (52%) developed breast cancer, 682 (6%) developed ovarian cancer, and 272 (2%) developed both breast and ovarian cancer. A woman’s risk for cancer differed significantly according to the type of BRCA1 or BRCA2 mutation she carried and according to the location of the mutation on the nucleotide, the investigators said (JAMA 2015 April 7 [doi:10.1001/jama.2014.5985]).
Further research is needed to determine the absolute risks of cancer associated with each mutation and “to better understand what level of risk difference will change decision-making and standards of care, such as preventive surgery” for BRCA1 and BRCA2 carriers, Dr. Rebbeck and his associates added.
This study was funded primarily by Cancer Research UK and also was supported by the U.S. National Institutes of Health, the Basser Research Center at the University of Pennsylvania, the Breast Cancer Research Foundation, and the Rooney Family Foundation. Dr. Rebbeck reported having no financial disclosures; his associates reported numerous ties to industry sources.
Among women who carry BRCA1 or BRCA2 mutations, the type and exact location of the mutation influences the risk it confers for breast and ovarian cancer, according to a report published online April 7 in JAMA.
Investigators examined differences in cancer risks by analyzing data in the Consortium of Investigators of Modifiers of BRCA (CIMBA), a collection of clinical and genetic information for carriers of disease-associated BRCA mutations in 33 countries.
For this study, data were assessed for 19,581 women with BRCA1 mutations and 11,900 women with BRCA2 mutations for whom there was sufficient information to estimate hazard ratios. The types of mutations included nonsense, frame shift, in-frame, missense, splicing, rearrangement, premature termination codons, and nonsense-mediated decay mutations, said Timothy R. Rebbeck, Ph.D., of Abramson Cancer Center and the Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, and his associates.
Among the study participants with BRCA1 mutations, 9,052 women (46%) developed breast cancer, 2,317 (12%) developed ovarian cancer, and 1,041 (5%) developed both breast and ovarian cancer. Among the women with BRCA2 mutations, 6,180 (52%) developed breast cancer, 682 (6%) developed ovarian cancer, and 272 (2%) developed both breast and ovarian cancer. A woman’s risk for cancer differed significantly according to the type of BRCA1 or BRCA2 mutation she carried and according to the location of the mutation on the nucleotide, the investigators said (JAMA 2015 April 7 [doi:10.1001/jama.2014.5985]).
Further research is needed to determine the absolute risks of cancer associated with each mutation and “to better understand what level of risk difference will change decision-making and standards of care, such as preventive surgery” for BRCA1 and BRCA2 carriers, Dr. Rebbeck and his associates added.
This study was funded primarily by Cancer Research UK and also was supported by the U.S. National Institutes of Health, the Basser Research Center at the University of Pennsylvania, the Breast Cancer Research Foundation, and the Rooney Family Foundation. Dr. Rebbeck reported having no financial disclosures; his associates reported numerous ties to industry sources.
FROM JAMA
Key clinical point: The type and exact location of BRCA1 and BRCA2 mutations affect the risk they confer for breast and ovarian cancer.
Major finding: Among the study participants with BRCA1 mutations, 46% developed breast cancer, 12% developed ovarian cancer, and 5% developed both breast and ovarian cancer; among those with BRCA2 mutations, 52% developed breast cancer, 6% developed ovarian cancer, and 2% developed both breast and ovarian cancer.
Data source: An observational analysis of cancer risks among 31,481 women in an international database of carriers of any deleterious BRCA mutations.
Disclosures: This study was funded primarily by Cancer Research UK and also was supported by the U.S. National Institutes of Health, the Basser Research Center at the University of Pennsylvania, the Breast Cancer Research Foundation, and the Rooney Family Foundation. Dr. Rebbeck reported having no financial disclosures; his associates reported numerous ties to industry sources.
False-positive mammograms cost $2.8 billion a year
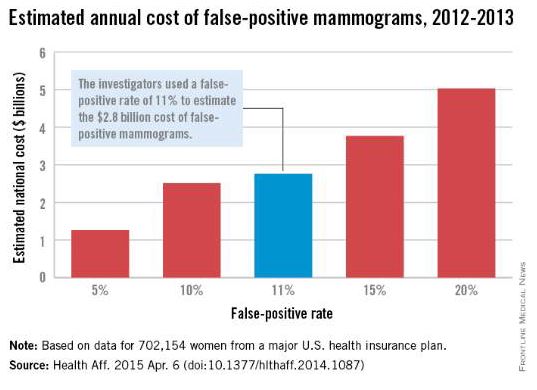
False-positive mammograms in women aged 40-59 years cost an estimated $2.8 billion per year in the United States in 2012-2013, according to a report published April 6 in Health Affairs.
The cost of screen-detected invasive breast cancer overdiagnoses was $1.2 billion a year for that time period and age group. Invasive breast cancers represent about $1 billion of that, with the rest coming from overdiagnoses of ductal carcinoma in situ (DCIS), Mei-Sing Ong, Ph.D., and Dr. Kenneth D. Mandl, both of Boston Children’s Hospital, estimated.
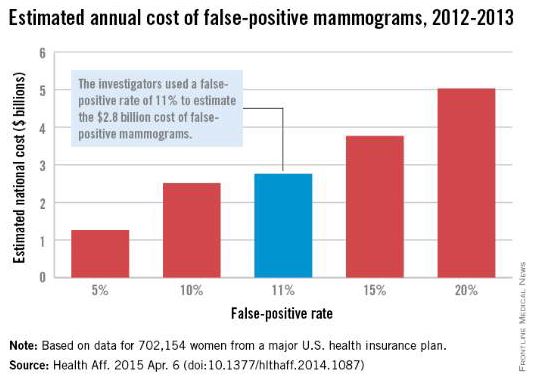
Using expenditure data for 702,154 women from a major U.S. health care insurance plan, the investigators calculated that the average cost of a false-positive mammogram – the mammography plus all related costs over the next 12 months – was $852. The average 12-month costs for invasive breast cancer and DCIS were $51,837 and $12,369, they reported (Health Aff. 2015 Apr. 6 [doi:10.1377/hlthaff.2014.1087]).
Dr. Ong and Dr. Mandl used a false-positive rate of 11% for the mammogram estimate, although they also calculated costs based on a range of rates from 5% to 20%. Based on recent studies in the New England Journal of Medicine and the BMJ, they used an overdiagnosis rate of 22% for the breast cancer estimate; the overdiagnosis rate of 86% for DCIS came from a 2004 study.
“The disutility of overdiagnosis,” together with the high diagnostic and treatment costs of mammography, “may tilt the balance to the point where screening [based on age] appears relatively cost ineffective,” Dr. Ong and Dr. Mandl wrote. It may be time to “shape a more individualized approach to determining who should receive screening, focusing on women who are most likely to benefit.”
Dr. Ong is supported by a fellowship from the National Health and Medical Research Council in Australia, which played no role in the study. Dr. Mandl did not report any conflicts.
False-positive mammograms in women aged 40-59 years cost an estimated $2.8 billion per year in the United States in 2012-2013, according to a report published April 6 in Health Affairs.
The cost of screen-detected invasive breast cancer overdiagnoses was $1.2 billion a year for that time period and age group. Invasive breast cancers represent about $1 billion of that, with the rest coming from overdiagnoses of ductal carcinoma in situ (DCIS), Mei-Sing Ong, Ph.D., and Dr. Kenneth D. Mandl, both of Boston Children’s Hospital, estimated.
Using expenditure data for 702,154 women from a major U.S. health care insurance plan, the investigators calculated that the average cost of a false-positive mammogram – the mammography plus all related costs over the next 12 months – was $852. The average 12-month costs for invasive breast cancer and DCIS were $51,837 and $12,369, they reported (Health Aff. 2015 Apr. 6 [doi:10.1377/hlthaff.2014.1087]).
Dr. Ong and Dr. Mandl used a false-positive rate of 11% for the mammogram estimate, although they also calculated costs based on a range of rates from 5% to 20%. Based on recent studies in the New England Journal of Medicine and the BMJ, they used an overdiagnosis rate of 22% for the breast cancer estimate; the overdiagnosis rate of 86% for DCIS came from a 2004 study.
“The disutility of overdiagnosis,” together with the high diagnostic and treatment costs of mammography, “may tilt the balance to the point where screening [based on age] appears relatively cost ineffective,” Dr. Ong and Dr. Mandl wrote. It may be time to “shape a more individualized approach to determining who should receive screening, focusing on women who are most likely to benefit.”
Dr. Ong is supported by a fellowship from the National Health and Medical Research Council in Australia, which played no role in the study. Dr. Mandl did not report any conflicts.
False-positive mammograms in women aged 40-59 years cost an estimated $2.8 billion per year in the United States in 2012-2013, according to a report published April 6 in Health Affairs.
The cost of screen-detected invasive breast cancer overdiagnoses was $1.2 billion a year for that time period and age group. Invasive breast cancers represent about $1 billion of that, with the rest coming from overdiagnoses of ductal carcinoma in situ (DCIS), Mei-Sing Ong, Ph.D., and Dr. Kenneth D. Mandl, both of Boston Children’s Hospital, estimated.
Using expenditure data for 702,154 women from a major U.S. health care insurance plan, the investigators calculated that the average cost of a false-positive mammogram – the mammography plus all related costs over the next 12 months – was $852. The average 12-month costs for invasive breast cancer and DCIS were $51,837 and $12,369, they reported (Health Aff. 2015 Apr. 6 [doi:10.1377/hlthaff.2014.1087]).
Dr. Ong and Dr. Mandl used a false-positive rate of 11% for the mammogram estimate, although they also calculated costs based on a range of rates from 5% to 20%. Based on recent studies in the New England Journal of Medicine and the BMJ, they used an overdiagnosis rate of 22% for the breast cancer estimate; the overdiagnosis rate of 86% for DCIS came from a 2004 study.
“The disutility of overdiagnosis,” together with the high diagnostic and treatment costs of mammography, “may tilt the balance to the point where screening [based on age] appears relatively cost ineffective,” Dr. Ong and Dr. Mandl wrote. It may be time to “shape a more individualized approach to determining who should receive screening, focusing on women who are most likely to benefit.”
Dr. Ong is supported by a fellowship from the National Health and Medical Research Council in Australia, which played no role in the study. Dr. Mandl did not report any conflicts.
FROM HEALTH AFFAIRS
Does a family history of both breast and prostate cancer (vs breast only) put a woman at greater risk for future breast cancer?
The most common invasive cancers diagnosed in US women and men are breast and prostate cancers, respectively. This analysis from the Women’s Health Initiative observational study involved 78,171 women aged 50 to 79 years at enrollment. Invasive breast cancer was diagnosed in 3,506 women (4.5%) during a median of 132 months of follow-up. Having a first-degree relative with breast or prostate cancer was associated with an elevated adjusted hazard ratio of breast cancer of 1.42 and 1.14, respectively. Women who had a history of both cancers among first-degree relatives had an adjusted HR of 1.78. Although the difference did not achieve statistical significance, there was a suggestion that the elevated risk for breast cancer associated with relatives with prostate and breast cancer was higher in African-American women compared with white women. The risk for breast cancer was not elevated in women who had first-degree relatives with cancers other than breast or prostate.
The authors point out that another study also reported that a family history that includes both cancers is associated with a greater elevation in the risk for breast cancer than family history of prostate cancer alone. Although BRCA 1 and 2 mutations are associated with an elevated risk of not only breast but also prostate cancer, the authors indicate that such mutations account for only a small proportion of the observed aggregation of breast and prostate cancer in first-degree relatives of women with breast cancer in their analysis.
What this evidence means for practice
The associations observed by these authors underscore that, when taking family histories, women’s health clinicians should pay attention not only to breast but also to prostate cancer, and counsel patients regarding risk and screening practices accordingly.
—Andrew M. Kaunitz, MD
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The most common invasive cancers diagnosed in US women and men are breast and prostate cancers, respectively. This analysis from the Women’s Health Initiative observational study involved 78,171 women aged 50 to 79 years at enrollment. Invasive breast cancer was diagnosed in 3,506 women (4.5%) during a median of 132 months of follow-up. Having a first-degree relative with breast or prostate cancer was associated with an elevated adjusted hazard ratio of breast cancer of 1.42 and 1.14, respectively. Women who had a history of both cancers among first-degree relatives had an adjusted HR of 1.78. Although the difference did not achieve statistical significance, there was a suggestion that the elevated risk for breast cancer associated with relatives with prostate and breast cancer was higher in African-American women compared with white women. The risk for breast cancer was not elevated in women who had first-degree relatives with cancers other than breast or prostate.
The authors point out that another study also reported that a family history that includes both cancers is associated with a greater elevation in the risk for breast cancer than family history of prostate cancer alone. Although BRCA 1 and 2 mutations are associated with an elevated risk of not only breast but also prostate cancer, the authors indicate that such mutations account for only a small proportion of the observed aggregation of breast and prostate cancer in first-degree relatives of women with breast cancer in their analysis.
What this evidence means for practice
The associations observed by these authors underscore that, when taking family histories, women’s health clinicians should pay attention not only to breast but also to prostate cancer, and counsel patients regarding risk and screening practices accordingly.
—Andrew M. Kaunitz, MD
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The most common invasive cancers diagnosed in US women and men are breast and prostate cancers, respectively. This analysis from the Women’s Health Initiative observational study involved 78,171 women aged 50 to 79 years at enrollment. Invasive breast cancer was diagnosed in 3,506 women (4.5%) during a median of 132 months of follow-up. Having a first-degree relative with breast or prostate cancer was associated with an elevated adjusted hazard ratio of breast cancer of 1.42 and 1.14, respectively. Women who had a history of both cancers among first-degree relatives had an adjusted HR of 1.78. Although the difference did not achieve statistical significance, there was a suggestion that the elevated risk for breast cancer associated with relatives with prostate and breast cancer was higher in African-American women compared with white women. The risk for breast cancer was not elevated in women who had first-degree relatives with cancers other than breast or prostate.
The authors point out that another study also reported that a family history that includes both cancers is associated with a greater elevation in the risk for breast cancer than family history of prostate cancer alone. Although BRCA 1 and 2 mutations are associated with an elevated risk of not only breast but also prostate cancer, the authors indicate that such mutations account for only a small proportion of the observed aggregation of breast and prostate cancer in first-degree relatives of women with breast cancer in their analysis.
What this evidence means for practice
The associations observed by these authors underscore that, when taking family histories, women’s health clinicians should pay attention not only to breast but also to prostate cancer, and counsel patients regarding risk and screening practices accordingly.
—Andrew M. Kaunitz, MD
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.