User login
Prolonged zoledronic acid-induced hypocalcemia in hypercalcemia of malignancy
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Click on the PDF icon at the top of this introduction to read the full article.
Delayed diagnosis tops breast cancer malpractice claims
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.

“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
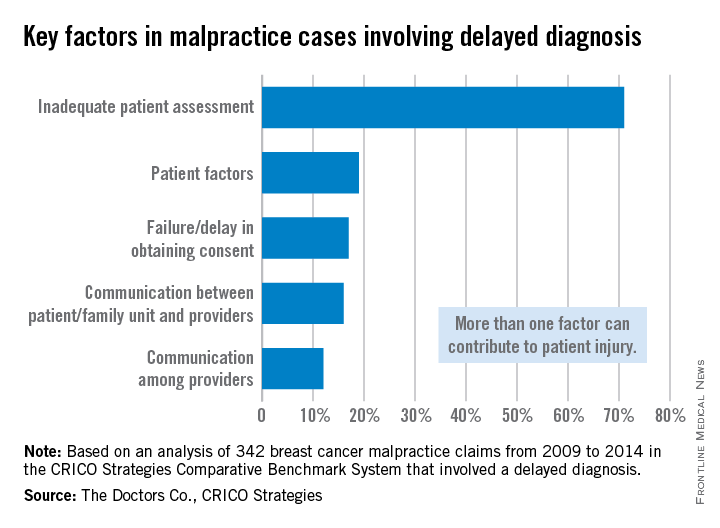
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.
“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.
“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med

Endocrine therapy in metastatic breast cancer: a closer look at the current clinical practice
How to fix clinical trial accrual
Editor Jame Abraham argues that once there is appropriate clinical trial infrastructure, there is only one person who can increase the clinical trial accrual: the treating oncologist.
Click on the PDF icon at the top of this introduction to read the full article.
Editor Jame Abraham argues that once there is appropriate clinical trial infrastructure, there is only one person who can increase the clinical trial accrual: the treating oncologist.
Click on the PDF icon at the top of this introduction to read the full article.
Editor Jame Abraham argues that once there is appropriate clinical trial infrastructure, there is only one person who can increase the clinical trial accrual: the treating oncologist.
Click on the PDF icon at the top of this introduction to read the full article.
VIDEO: Tomosynthesis soon to be standard of care for breast cancer screening
CHICAGO – The uptake of tomosynthesis has been fairly brisk among the nation’s breast cancer screening centers.
There are good reasons for that. In an interview at the annual clinical congress of the American College of Surgeons, Dr. Sarah Friedewald, division chief of breast and women’s imaging at Northwestern University, Chicago, explained the procedure; its pluses and minuses; and why it’s likely to be the standard of care for breast cancer screening within 5 years.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – The uptake of tomosynthesis has been fairly brisk among the nation’s breast cancer screening centers.
There are good reasons for that. In an interview at the annual clinical congress of the American College of Surgeons, Dr. Sarah Friedewald, division chief of breast and women’s imaging at Northwestern University, Chicago, explained the procedure; its pluses and minuses; and why it’s likely to be the standard of care for breast cancer screening within 5 years.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – The uptake of tomosynthesis has been fairly brisk among the nation’s breast cancer screening centers.
There are good reasons for that. In an interview at the annual clinical congress of the American College of Surgeons, Dr. Sarah Friedewald, division chief of breast and women’s imaging at Northwestern University, Chicago, explained the procedure; its pluses and minuses; and why it’s likely to be the standard of care for breast cancer screening within 5 years.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE ACS CLINICAL CONGRESS

VIDEO: Immediate breast reconstruction results reassuring in select patients
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
AT THE ACS ANNUAL CONGRESS

NIH expands cancer research program to include breast density
Officials at the National Institutes of Health are taking a closer look at the role that breast density plays in the development of breast cancer.
As part of the agency’s Breast Cancer and the Environment Research Program (BCERP), grant-funded researchers are being tasked with expanding the study of risk factors that precede breast cancer such as breast density. They will also include more racially and ethnically diverse populations in their studies.
The research will be conducted at six centers: Brigham and Women’s Hospital, Boston; City of Hope/Beckman Research Institute, Duarte, Calif.; Columbia University, New York; Georgetown Lombardi Comprehensive Cancer Center, Washington; Michigan State University, Lansing; University of Massachusetts, Amherst. The research will be coordinated by another center at the University of Wisconsin, Madison.
Breast density is a new area of focus for the NIH. The researchers will consider dense breast tissue as a possible intermediate risk factor for breast cancer with the goal of identifying links between environmental exposures and high breast density, which could provide future prevention strategies.
“These priorities reflect our continued commitment to breast cancer prevention,” Caroline H. Dilworth, Ph.D., BCERP program lead at the National Institute of Environmental Health Sciences, said in a statement. “Our goal is to build on the high-quality science we’ve been funding for more than a decade, while also being responsive to the expert recommendations of the Interagency Breast Cancer and Environmental Research Coordinating Committee] report.”
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Officials at the National Institutes of Health are taking a closer look at the role that breast density plays in the development of breast cancer.
As part of the agency’s Breast Cancer and the Environment Research Program (BCERP), grant-funded researchers are being tasked with expanding the study of risk factors that precede breast cancer such as breast density. They will also include more racially and ethnically diverse populations in their studies.
The research will be conducted at six centers: Brigham and Women’s Hospital, Boston; City of Hope/Beckman Research Institute, Duarte, Calif.; Columbia University, New York; Georgetown Lombardi Comprehensive Cancer Center, Washington; Michigan State University, Lansing; University of Massachusetts, Amherst. The research will be coordinated by another center at the University of Wisconsin, Madison.
Breast density is a new area of focus for the NIH. The researchers will consider dense breast tissue as a possible intermediate risk factor for breast cancer with the goal of identifying links between environmental exposures and high breast density, which could provide future prevention strategies.
“These priorities reflect our continued commitment to breast cancer prevention,” Caroline H. Dilworth, Ph.D., BCERP program lead at the National Institute of Environmental Health Sciences, said in a statement. “Our goal is to build on the high-quality science we’ve been funding for more than a decade, while also being responsive to the expert recommendations of the Interagency Breast Cancer and Environmental Research Coordinating Committee] report.”
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Officials at the National Institutes of Health are taking a closer look at the role that breast density plays in the development of breast cancer.
As part of the agency’s Breast Cancer and the Environment Research Program (BCERP), grant-funded researchers are being tasked with expanding the study of risk factors that precede breast cancer such as breast density. They will also include more racially and ethnically diverse populations in their studies.
The research will be conducted at six centers: Brigham and Women’s Hospital, Boston; City of Hope/Beckman Research Institute, Duarte, Calif.; Columbia University, New York; Georgetown Lombardi Comprehensive Cancer Center, Washington; Michigan State University, Lansing; University of Massachusetts, Amherst. The research will be coordinated by another center at the University of Wisconsin, Madison.
Breast density is a new area of focus for the NIH. The researchers will consider dense breast tissue as a possible intermediate risk factor for breast cancer with the goal of identifying links between environmental exposures and high breast density, which could provide future prevention strategies.
“These priorities reflect our continued commitment to breast cancer prevention,” Caroline H. Dilworth, Ph.D., BCERP program lead at the National Institute of Environmental Health Sciences, said in a statement. “Our goal is to build on the high-quality science we’ve been funding for more than a decade, while also being responsive to the expert recommendations of the Interagency Breast Cancer and Environmental Research Coordinating Committee] report.”
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Race, age, BMI had no impact on pCR rates
SAN FRANCISCO – Age, race, and body mass index (BMI) do not appear to be related to achieving pathologic complete response (pCR) in breast cancer patients, according to data presented at the ASCO Breast Cancer Symposium.
“We did see some suggestions that maybe age and race were associated, but in our modeling, once we accounted for tumor characteristics such as tumor size and lymph node involvement, that association was attenuated to nonsignificance,” said Dr. Erica T. Warner of the Harvard T.H. Chan School of Public Health, Boston.
She noted that some previous research has found a higher pCR among young women and a lower pCR among overweight and obese women.

“Overall we had pretty high pCR rates, much higher than observed in these other studies,” said Dr. Warner. “It is likely due to our definition of pCR, the tumor subtypes that were included in our study, and the studies we included had combination therapy in addition to neoadjuvant therapy.”
Pathologic complete response is an important prognostic indicator and surrogate endpoint, and this is particularly true for patients with hormone receptor–negative breast cancer. Prior research has suggested there may be a differential response to preoperative therapy by age and BMI, although no association has been observed by race.
“Our motivation for this trial was that we know that young age, black race, and obesity are associated with poorer survival, and we wanted to try to better understand the mechanisms behind that,” explained Dr. Warner.
In this study, Dr. Warner and her colleagues conducted an analysis of 1,146 women with breast cancer, who were enrolled in four clinical trials of neoadjuvant chemotherapy (CALGB 40601 and 40603; ACOSOG Z1031 and Z1041). They used logistic regression models to determine the association of race/ethnicity and age at diagnosis with pCR.
Within the cohort, 156 patients (13.6%) were black; 590 tumors (51.5%) were HER2+, 169 (14.7%) were ER+/HER2-, and 387 (33.8%) were triple negative.
In multivariate analyses that controlled for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00), and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR. The researchers found similar associations when they stratified the data by subtype, and found no interaction between age and black race (P = .06), black race and BMI (P = .54), or age and BMI (P = .73).
For the ER+ HER2- subtype, there was a suggestion of an inverse association; per 5-year increase the probability of pCR decreased 17%, but again it was not statistically significant.
There were higher rates of pCR among HER2+ and triple-negative tumors, but there was no difference in pCR according to race (white women, 43.5%; black women, 44.2%; and other/unknown, 46.1%), Dr. Warner pointed out.
There was a lower median age for achieving pCR, as the median age for women who did not achieve pCR was 53, compared with 49 for those who did (P <less than .0001). And for BMI, women who didn’t achieve pCR had an average BMI of 28.6, compared with 28 for those who did (P = .03).
“But there was no association of black race with pCR for any subtype, no association between BMI and pCR for any subtype, and no association for age,” she said.
SAN FRANCISCO – Age, race, and body mass index (BMI) do not appear to be related to achieving pathologic complete response (pCR) in breast cancer patients, according to data presented at the ASCO Breast Cancer Symposium.
“We did see some suggestions that maybe age and race were associated, but in our modeling, once we accounted for tumor characteristics such as tumor size and lymph node involvement, that association was attenuated to nonsignificance,” said Dr. Erica T. Warner of the Harvard T.H. Chan School of Public Health, Boston.
She noted that some previous research has found a higher pCR among young women and a lower pCR among overweight and obese women.
“Overall we had pretty high pCR rates, much higher than observed in these other studies,” said Dr. Warner. “It is likely due to our definition of pCR, the tumor subtypes that were included in our study, and the studies we included had combination therapy in addition to neoadjuvant therapy.”
Pathologic complete response is an important prognostic indicator and surrogate endpoint, and this is particularly true for patients with hormone receptor–negative breast cancer. Prior research has suggested there may be a differential response to preoperative therapy by age and BMI, although no association has been observed by race.
“Our motivation for this trial was that we know that young age, black race, and obesity are associated with poorer survival, and we wanted to try to better understand the mechanisms behind that,” explained Dr. Warner.
In this study, Dr. Warner and her colleagues conducted an analysis of 1,146 women with breast cancer, who were enrolled in four clinical trials of neoadjuvant chemotherapy (CALGB 40601 and 40603; ACOSOG Z1031 and Z1041). They used logistic regression models to determine the association of race/ethnicity and age at diagnosis with pCR.
Within the cohort, 156 patients (13.6%) were black; 590 tumors (51.5%) were HER2+, 169 (14.7%) were ER+/HER2-, and 387 (33.8%) were triple negative.
In multivariate analyses that controlled for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00), and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR. The researchers found similar associations when they stratified the data by subtype, and found no interaction between age and black race (P = .06), black race and BMI (P = .54), or age and BMI (P = .73).
For the ER+ HER2- subtype, there was a suggestion of an inverse association; per 5-year increase the probability of pCR decreased 17%, but again it was not statistically significant.
There were higher rates of pCR among HER2+ and triple-negative tumors, but there was no difference in pCR according to race (white women, 43.5%; black women, 44.2%; and other/unknown, 46.1%), Dr. Warner pointed out.
There was a lower median age for achieving pCR, as the median age for women who did not achieve pCR was 53, compared with 49 for those who did (P <less than .0001). And for BMI, women who didn’t achieve pCR had an average BMI of 28.6, compared with 28 for those who did (P = .03).
“But there was no association of black race with pCR for any subtype, no association between BMI and pCR for any subtype, and no association for age,” she said.
SAN FRANCISCO – Age, race, and body mass index (BMI) do not appear to be related to achieving pathologic complete response (pCR) in breast cancer patients, according to data presented at the ASCO Breast Cancer Symposium.
“We did see some suggestions that maybe age and race were associated, but in our modeling, once we accounted for tumor characteristics such as tumor size and lymph node involvement, that association was attenuated to nonsignificance,” said Dr. Erica T. Warner of the Harvard T.H. Chan School of Public Health, Boston.
She noted that some previous research has found a higher pCR among young women and a lower pCR among overweight and obese women.
“Overall we had pretty high pCR rates, much higher than observed in these other studies,” said Dr. Warner. “It is likely due to our definition of pCR, the tumor subtypes that were included in our study, and the studies we included had combination therapy in addition to neoadjuvant therapy.”
Pathologic complete response is an important prognostic indicator and surrogate endpoint, and this is particularly true for patients with hormone receptor–negative breast cancer. Prior research has suggested there may be a differential response to preoperative therapy by age and BMI, although no association has been observed by race.
“Our motivation for this trial was that we know that young age, black race, and obesity are associated with poorer survival, and we wanted to try to better understand the mechanisms behind that,” explained Dr. Warner.
In this study, Dr. Warner and her colleagues conducted an analysis of 1,146 women with breast cancer, who were enrolled in four clinical trials of neoadjuvant chemotherapy (CALGB 40601 and 40603; ACOSOG Z1031 and Z1041). They used logistic regression models to determine the association of race/ethnicity and age at diagnosis with pCR.
Within the cohort, 156 patients (13.6%) were black; 590 tumors (51.5%) were HER2+, 169 (14.7%) were ER+/HER2-, and 387 (33.8%) were triple negative.
In multivariate analyses that controlled for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00), and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR. The researchers found similar associations when they stratified the data by subtype, and found no interaction between age and black race (P = .06), black race and BMI (P = .54), or age and BMI (P = .73).
For the ER+ HER2- subtype, there was a suggestion of an inverse association; per 5-year increase the probability of pCR decreased 17%, but again it was not statistically significant.
There were higher rates of pCR among HER2+ and triple-negative tumors, but there was no difference in pCR according to race (white women, 43.5%; black women, 44.2%; and other/unknown, 46.1%), Dr. Warner pointed out.
There was a lower median age for achieving pCR, as the median age for women who did not achieve pCR was 53, compared with 49 for those who did (P <less than .0001). And for BMI, women who didn’t achieve pCR had an average BMI of 28.6, compared with 28 for those who did (P = .03).
“But there was no association of black race with pCR for any subtype, no association between BMI and pCR for any subtype, and no association for age,” she said.
FROM THE 2015 ASCO BREAST CANCER SYMPOSIUM
Key clinical point: Race, age, and body mass index do not appear to affect pathologic complete response in breast cancer.
Major finding: In multivariate analyses controlling for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00) and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR.
Data source: An analysis of four clinical trials of neoadjuvant chemotherapy that included 1,146 women with breast cancer.
Disclosures: Dr. Warner had no relevant financial disclosures, and there was no information on outside sponsorship of the study.

Managing menopausal symptoms in women with a BRCA mutation
This audiocast was recorded at the North American Menopause Society Annual Meeting held September 30 to October 3, 2015, in Las Vegas, Nevada
For more on this topic, read Dr. Kaunitz's August 2015 Cases in Menopause article, Is menopausal hormone therapy safe when your patient carries a BRCA mutation?
This audiocast was recorded at the North American Menopause Society Annual Meeting held September 30 to October 3, 2015, in Las Vegas, Nevada
For more on this topic, read Dr. Kaunitz's August 2015 Cases in Menopause article, Is menopausal hormone therapy safe when your patient carries a BRCA mutation?
This audiocast was recorded at the North American Menopause Society Annual Meeting held September 30 to October 3, 2015, in Las Vegas, Nevada
For more on this topic, read Dr. Kaunitz's August 2015 Cases in Menopause article, Is menopausal hormone therapy safe when your patient carries a BRCA mutation?
VIDEO: When to use MRI in breast cancer
CHICAGO – For most women, there’s little role for MRI in screening for and treating breast cancer
However, there are important exceptions. In an interview at the American College of Surgeons Clinical Congress, Dr. Monica Morrow, chief of breast surgery at Memorial Sloan-Kettering Cancer Center in Manhattan, explained what those exceptions are, and how she uses MRI in her practice.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – For most women, there’s little role for MRI in screening for and treating breast cancer
However, there are important exceptions. In an interview at the American College of Surgeons Clinical Congress, Dr. Monica Morrow, chief of breast surgery at Memorial Sloan-Kettering Cancer Center in Manhattan, explained what those exceptions are, and how she uses MRI in her practice.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – For most women, there’s little role for MRI in screening for and treating breast cancer
However, there are important exceptions. In an interview at the American College of Surgeons Clinical Congress, Dr. Monica Morrow, chief of breast surgery at Memorial Sloan-Kettering Cancer Center in Manhattan, explained what those exceptions are, and how she uses MRI in her practice.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE AMERICAN COLLEGE OF SURGEONS CLINICAL CONGRESS
