User login
The Hospitalist only
Practice Guidelines for the Management of Bacterial Meningitis
Enter text here
Enter text here
Enter text here
Rates, Predictors, and Outcomes of Major Hemorrhage in Patients with Atrial Fibrillation
Background: Although warfarin is extremely effective in reducing the risk of ischemic stroke from atrial fibrillation (AF), it also increases the risk for significant hemorrhage. We assessed rates, predictors, and short-term mortality after hospitalization for major hemorrhage in a cohort of AF patients on and off warfarin.
Methods: We prospectively studied 13,559 adults with AF. Patients hospitalized for hemorrhage were identified from clinical databases and confirmed using chart review. Major hemorrhage was defined as fatal, transfusion of ≥ 2 units packed blood cells, or into a critical anatomic site; separate analyses were performed for intracranial hemorrhage (ICH) and extracranial hemorrhage. We used multivariable log-linear regression to assess for predictors of hemorrhage, adjusting for demographic and clinical characteristics.
Results: Out of 30,994 person-years of follow-up, we identified 78 ICHs in patients on warfarin and 51 off warfarin. Out of 30,830 person-years, there were 98 major extracranial hemorrhages on warfarin and 116 off warfarin. Although rates of hemorrhage increased with age, absolute rates of hemorrhage in anticoagulated patients were similar to those in non-anticoagulated patients. In patients aged 80 and older, the annual rate of ICH was 0.8% on warfarin and 0.7% off warfarin; for extracranial hemorrhage, the rate was 0.7% on warfarin and 1.0% off warfarin. In patients who developed ICH while taking warfarin, independent risk factors included age ≥ 80 (OR 2.8 [1.1-7.2] compared to age <60) and hypertension (OR 1.7 [1.0-2.8]).
Predictors of ICH off warfarin were age ≥ 80 (OR 6.2 [1.7-23]) and prior stroke (OR 2.4 [1.1-5.0]). Independent predictors of extracranial hemorrhage were age ≥ 80 (OR 3.8 [1.1-13] on warfarin and 3.8 [1.7-8.6] off warfarin) and prior gastrointestinal hemorrhage (OR 5.3 [2.9-9.8] on warfarin and 2.0 [1.1-3.6] off warfarin). INR ≥ 4.0 (compared to INR<4.0) was the strongest predictor of hemorrhage in patients taking warfarin: OR 15 [8.1-29] for ICH and OR 18 [10-30] for extracranial hemorrhage. Of the 48 deaths, 81% were from ICH, with a 30-day mortality rate of 50% after ICH on warfarin and 28% off warfarin. In contrast, 30-day mortality after major extracranial hemorrhage was relatively low (5% for patients on warfarin and 10% off warfarin).
Conclusions: In this largest prospective study to date of individuals with AF, absolute rates of major hemorrhage were low and similar in patients on and off warfarin, even in the most elderly. Hemorrhage contributed to few short-term deaths and the majority of deaths resulted from ICH, not extracranial hemorrhage. The benefits of warfarin in reducing ischemic stroke continue to outweigh the risk of hemorrhage, especially in older patients.
Background: Although warfarin is extremely effective in reducing the risk of ischemic stroke from atrial fibrillation (AF), it also increases the risk for significant hemorrhage. We assessed rates, predictors, and short-term mortality after hospitalization for major hemorrhage in a cohort of AF patients on and off warfarin.
Methods: We prospectively studied 13,559 adults with AF. Patients hospitalized for hemorrhage were identified from clinical databases and confirmed using chart review. Major hemorrhage was defined as fatal, transfusion of ≥ 2 units packed blood cells, or into a critical anatomic site; separate analyses were performed for intracranial hemorrhage (ICH) and extracranial hemorrhage. We used multivariable log-linear regression to assess for predictors of hemorrhage, adjusting for demographic and clinical characteristics.
Results: Out of 30,994 person-years of follow-up, we identified 78 ICHs in patients on warfarin and 51 off warfarin. Out of 30,830 person-years, there were 98 major extracranial hemorrhages on warfarin and 116 off warfarin. Although rates of hemorrhage increased with age, absolute rates of hemorrhage in anticoagulated patients were similar to those in non-anticoagulated patients. In patients aged 80 and older, the annual rate of ICH was 0.8% on warfarin and 0.7% off warfarin; for extracranial hemorrhage, the rate was 0.7% on warfarin and 1.0% off warfarin. In patients who developed ICH while taking warfarin, independent risk factors included age ≥ 80 (OR 2.8 [1.1-7.2] compared to age <60) and hypertension (OR 1.7 [1.0-2.8]).
Predictors of ICH off warfarin were age ≥ 80 (OR 6.2 [1.7-23]) and prior stroke (OR 2.4 [1.1-5.0]). Independent predictors of extracranial hemorrhage were age ≥ 80 (OR 3.8 [1.1-13] on warfarin and 3.8 [1.7-8.6] off warfarin) and prior gastrointestinal hemorrhage (OR 5.3 [2.9-9.8] on warfarin and 2.0 [1.1-3.6] off warfarin). INR ≥ 4.0 (compared to INR<4.0) was the strongest predictor of hemorrhage in patients taking warfarin: OR 15 [8.1-29] for ICH and OR 18 [10-30] for extracranial hemorrhage. Of the 48 deaths, 81% were from ICH, with a 30-day mortality rate of 50% after ICH on warfarin and 28% off warfarin. In contrast, 30-day mortality after major extracranial hemorrhage was relatively low (5% for patients on warfarin and 10% off warfarin).
Conclusions: In this largest prospective study to date of individuals with AF, absolute rates of major hemorrhage were low and similar in patients on and off warfarin, even in the most elderly. Hemorrhage contributed to few short-term deaths and the majority of deaths resulted from ICH, not extracranial hemorrhage. The benefits of warfarin in reducing ischemic stroke continue to outweigh the risk of hemorrhage, especially in older patients.
Background: Although warfarin is extremely effective in reducing the risk of ischemic stroke from atrial fibrillation (AF), it also increases the risk for significant hemorrhage. We assessed rates, predictors, and short-term mortality after hospitalization for major hemorrhage in a cohort of AF patients on and off warfarin.
Methods: We prospectively studied 13,559 adults with AF. Patients hospitalized for hemorrhage were identified from clinical databases and confirmed using chart review. Major hemorrhage was defined as fatal, transfusion of ≥ 2 units packed blood cells, or into a critical anatomic site; separate analyses were performed for intracranial hemorrhage (ICH) and extracranial hemorrhage. We used multivariable log-linear regression to assess for predictors of hemorrhage, adjusting for demographic and clinical characteristics.
Results: Out of 30,994 person-years of follow-up, we identified 78 ICHs in patients on warfarin and 51 off warfarin. Out of 30,830 person-years, there were 98 major extracranial hemorrhages on warfarin and 116 off warfarin. Although rates of hemorrhage increased with age, absolute rates of hemorrhage in anticoagulated patients were similar to those in non-anticoagulated patients. In patients aged 80 and older, the annual rate of ICH was 0.8% on warfarin and 0.7% off warfarin; for extracranial hemorrhage, the rate was 0.7% on warfarin and 1.0% off warfarin. In patients who developed ICH while taking warfarin, independent risk factors included age ≥ 80 (OR 2.8 [1.1-7.2] compared to age <60) and hypertension (OR 1.7 [1.0-2.8]).
Predictors of ICH off warfarin were age ≥ 80 (OR 6.2 [1.7-23]) and prior stroke (OR 2.4 [1.1-5.0]). Independent predictors of extracranial hemorrhage were age ≥ 80 (OR 3.8 [1.1-13] on warfarin and 3.8 [1.7-8.6] off warfarin) and prior gastrointestinal hemorrhage (OR 5.3 [2.9-9.8] on warfarin and 2.0 [1.1-3.6] off warfarin). INR ≥ 4.0 (compared to INR<4.0) was the strongest predictor of hemorrhage in patients taking warfarin: OR 15 [8.1-29] for ICH and OR 18 [10-30] for extracranial hemorrhage. Of the 48 deaths, 81% were from ICH, with a 30-day mortality rate of 50% after ICH on warfarin and 28% off warfarin. In contrast, 30-day mortality after major extracranial hemorrhage was relatively low (5% for patients on warfarin and 10% off warfarin).
Conclusions: In this largest prospective study to date of individuals with AF, absolute rates of major hemorrhage were low and similar in patients on and off warfarin, even in the most elderly. Hemorrhage contributed to few short-term deaths and the majority of deaths resulted from ICH, not extracranial hemorrhage. The benefits of warfarin in reducing ischemic stroke continue to outweigh the risk of hemorrhage, especially in older patients.
The Fountain of Youth
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion


This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
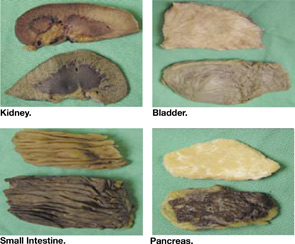
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
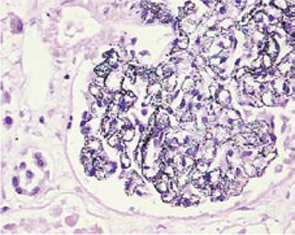
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion
This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion
This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”