User login
The Hospitalist only
Pediatric Special Section
Meningococcal Disease in Peds
By J. Christopher Day, MD
Thompson, MJ, Ninis N, Perera R, et al. Clinical recognition of meningococcal disease in children and adolescents. Lancet. 2006 Feb 6;367(9508)397-403.
Data from medical records and parental questionnaires were examined to determine the time course and prevalence of signs and symptoms in meningococcal disease (sepsis and meningitis) in 448 children in Wales, England, and Northern Ireland.
The authors note that classic clinical features of the disease appear late in the illness. The symptoms that appear earliest (fever, poor feeding, nausea, vomiting, coryza, sore throat) are very non-specific, but somewhat later symptoms of sepsis including leg pains, cold hands and feet, and abnormal skin color appear before the classical clinical features in 72% of the children studied. The authors hope that recognition of these features can lead to earlier diagnosis and treatment of this severe disease.
Treatment of Infant Botulism
Arnon SS, Schechter R, Maslanka SE, et al. Human botulism immune globulin for the treatment of infant botulism. N Engl J Med. 2006 Feb 2;354((5):462-471.
This is is a report of a randomized, double-blind, placebo controlled trial of the use of human botulism immune globulin intravenous (BIG-IV) used for the treatment of infant botulism. The study was performed on 122 infants with (initially) suspected and (later) laboratory confirmed infant botulism. BIG-IV was given within three days of hospital admission. The authors also performed an open-label study of 382 laboratory confirmed cases. Some of these began treatment as late as 18 days after hospital admission.
In the randomized trial, outcomes compared with placebo included a reduction in hospital stay from 5.7 weeks to 2.6 weeks (P<0.001); a reduction in the mean duration of intensive care by 3.2 weeks (P<0.001); the mean duration of mechanical ventilation by 2.6 weeks (P= 0.01); the mean duration of tube or intravenous feeding by 6.4 weeks; and the mean hospital charges per patient by $88,600 (P<0.001).
The only notable adverse event perhaps related to treatment was a transient blush-like erythematous rash. In the open-label study, treatment given within three days of hospital admission shortened the mean length of stay by approximately one week more than did treatment given four to seven days after admission. BIG-IV is now licensed as BabyBIG. The authors recommend treatment as soon as possible after hospital admission.—JCD
Eczema: Wet Wraps Versus Conventional Treatment
Hindley D, Galloway G, Murray J, et al. A randomised study of “wet wraps” versus conventional treatment for atopic eczema. Arch Dis Child. 2006 Feb;91(2):164-168.
The authors were interested in comparing the efficacy and parent perception of ease of application of conventional treatment (emulsifying ointments and topical steroids) with wet wraps (tubular retention bandages applied wet as occlusive dressings over emulsifying ointments) and topical steroids for exacerbations of eczema.
Fifty children were enrolled and randomized to either treatment group. Treatment was continued and patients were followed for one month. The change in eczema severity was scored using a previously published scale (SCORAD) for assessing severity. No differences were noted between the two groups, though the study had a number of limitations including use of only one potency of steroid (1% hydrocortisone) limiting generalizability, the length of treatment (regimens vary in length), and patient drop-outs (five dropped out—all in the wet wrap group).
Parents felt wet wraps were harder to use. The authors do note that there may be clinical situations (they mention short term treatment of acute erythrodermic eczema) where wet wraps are a useful option. There appear to be no advantages in the group studied over a four-week period and the disadvantages likely include parental perception of difficulty of use and a possibility of increased skin infections.—JCD
A Study of Dehydrated Peds
Mallory MD, Kadish H, Zebrack M, Nelson D. Use of a pediatric observation unit for treatment of children with dehydration caused by gastroenteritis. Pediatr Emerg Care. 2006 Jan;22(1):1-6.
A case-control study was performed to examine 467 admissions to an observation unit in patients with dehydration from vomiting or diarrhea from presumed gastroenteritis. Patients were presumably admitted to the observation unit (staffed by emergency department personnel) if they were believed to require more rehydration than could be reasonably offered in the emergency department itself.
Controls were defined as those patients able to be discharged home from the observation unit within 24 hours and cases as those patients that required subsequent inpatient admission. Nineteen percent of the patients studied required inpatient admission.
One of the goals of the study was to determine variables useful in distinguishing patients who would require subsequent inpatient admission from those who would be discharged home from the observation unit. No such variables were found.
Variables studied included oral intake prior to presentation, urine output at presentation, symptoms at presentation (vomiting versus diarrhea versus both), predominant symptoms (vomiting versus diarrhea versus no predominance), duration of symptoms, abdomen tender to palpation (yes/no), previous visit within five days (yes/no), age, vital signs, bicarbonate levels, and mean sodium levels.—JCD
Routine Neuroimaging: Little Value When Evaluating Febrile Seizures
By Stevie Wilson, RN, CPNP
Teng D, Dayan P, Tyler S, et al. Risk of intracranial pathologic conditions requiring emergency intervention after a first complex febrile seizure episode among children. Pediatrics. 2006;117(2):304-308.
Febrile seizures occur in up to 5% of all children. One-third of febrile seizures are classified as complex (i.e., having multiple seizures, prolonged duration, or focal seizures). Complex febrile seizures have been associated with an increased risk of recurrent febrile seizures and epilepsy. However, they have not been associated with pathologic intracranial lesions that require emergency surgical intervention.
Previous studies suggest that intracranial abnormalities are rare among simple febrile seizures. The American Academy of Pediatrics (AAP) recommends against the use of neuroimaging with simple seizures, however, practice guidelines for emergency neuroimaging for complex seizures do not exist. The objective of this study was to determine the likelihood of a significant intracranial condition requiring emergency intervention in children with the first complex febrile seizure.
A retrospective review of prospectively collected data was performed for 71 children who presented to the pediatric emergency department after a first complex febrile seizure. None of the 71 patients had a pathologic intracranial lesion that required emergency intervention. The authors therefore concluded that the risk of pathologic intracranial conditions requiring emergency intervention is low, suggesting that routine emergency neuroimaging for this population is unnecessary.
Managing Bronchiolitis above Sea Level
Choudhuri JA, Ogden LG, Ruttenber JA, et al. Effect of altitude on hospitalizations for respiratory syncytial virus infection. Pediatrics. 2006;117(2):349-356.
This interesting study sought to evaluate the effect altitude has on hospitalizations for RSV infection. A multivariate analysis was obtained and suggests that the rate of hospitalization for RSV increased by 25% among infants who were younger than one year of age for every 1,000 meters of altitude. The risk of RSV-associated hospitalization was highest at elevations above 2,500 meters.—SW
Dilemmas for Wheezing Peds
By Chris Miller, MD
Oymar K, Halvorsen T, Aksnes L. Mast cell activation and leukotriene secretion in wheezing infants. Relation to respiratory syncytial virus and outcome. Pediatr Allergy Immunol. 2006 Feb;17(1):37-42.
The wheezing infant is a common problem in pediatric medicine; however, the long-term outcome and risk for recurrent wheezing remains unclear. The authors of this study assert that the risk for recurrent wheezing may be related to the type of inflammation and specific underlying virus during the initial wheezing episode.
Several studies have evaluated the specific contribution of eosinophils to respiratory inflammation in the wheezing child. These studies have found that eosinophilic inflammation may play a role in the airway hyper-reactivity in a child with persistent wheezing. Conversely, little information is available regarding mast cell involvement. This prospective study was designed to assess mast cell activation, in relation to respiratory syncytial virus (RSV) infection and persistent wheezing in wheezing infants.
Researchers enrolled 106 wheezing infants who were subsequently admitted to the hospital. None of these infants had a prior history of wheezing. Infants with prior history of atopic disease, lung disease, or signs of bacterial infection were excluded. RSV testing of nasopharyngeal mucous was performed. Sixty-seven (63%) of the wheezing infants had RSV. An additional 23 healthy infants were selected as controls.
To assess the extent of mast cell activation, urinary prostaglandin F2 (U-PGF2) was measured. To assess for leukotriene secretion urinary leukotriene 4 (U-LTE4) was measured. To evaluate for persistence or reoccurrence of wheezing, a 20-month post-hospitalization follow-up was done. One hundred and three (97%) of the previously hospitalized wheezing infants were available for the follow-up.
The authors used the term “persistent wheezing” to describe those children who experienced at least three wheezing episodes including the first hospitalization. These recurrences were identified either by parental report utilizing a standardized questionnaire or physician/hospitalization records. The remaining children were considered “transient wheezers.”
Review of the data regarding U-PGF2, a specific marker for mast cell activation, showed U-PGF2 to be greatest in the RSV positive patients, followed by the RSV negative patients and finally by the control group. U-LTE4, and thus leukotriene involvement, was also found to be significantly elevated in both the RSV positive and negative wheezing infants compared with the controls. No significant difference was found in U-LTE4 between RSV-positive infants and RSV-negative infants. The transient wheezing infant had a higher U-PGF2 than the persistent wheezing infant. Transient wheezers also had a higher U-LTE4 compared with persistent wheezers, although this was not statistically significant.
With univariate regression analysis positive predictive factors for persistent wheezing included increasing age, RSV negative disease, parental atopy, and male gender. Negative predictive factors for persistent wheezing included an elevated U-PGF2 level.
In discussion the authors conclude that mast cell activation and leukotriene secretion is present in a wheezing infant as noted by increased U-PGF2 and U-LTE4 levels, respectively. Higher U-PGF2 levels in RSV-positive patients indicates that mast cell activation may play a bigger part in the inflammatory process of RSV-induced wheezing compared with non-RSV induced wheezing. Leukotrienes appear to be involved in both RSV and non-RSV wheezing infants. Despite these results, mast cell activation and leukotriene secretion do not appear to be associated with persistent wheezing.
Limitations of this interesting study include the small sample size, apparent lack of follow-up with the control patients, and the diagnosis of recurrent wheezing episodes being characterized by the parents.
Influenza Pneumonia in Pediatric Patients
Lahti E, Peltola V, Virkki R, et al. Influenza pneumonia. Pediatr Infect Dis J. 2006 Feb;25(2):160-164.
Influenza and pneumonia are common in children. The objective of this study was to describe the frequency and characteristics of laboratory-documented and radiographically proven influenza-associated pneumonia in children.
This retrospective, single site study was conducted at Turku University Hospital (Finland). Chart reviews of both inpatient and outpatient visits of children younger than 16 were performed for a 24-year period between 1980 through 2003. Children with influenza A or B antigen detected nasopharyngeal aspirates were identified. Also children with chest radiographs obtained during their influenza infection were identified. Clinical findings upon initial presentation were summarized, in addition to laboratory values for white blood cell count (WBC) and C-reactive protein (CRP).
A total of 936 patients with virologically confirmed influenza were identified. Of this total, 79% had influenza A and the remaining had influenza B. Chest radiographs were reported on 400 (43%) of these patients. Of the 400 films, 228 were initially read as having infiltrates. However, during over-reading of the films 70 chest radiographs did not have an infiltrate and an additional 24 films could not be found. In summary, 134 children had both confirmed influenza and radiographically proven pneumonia. Thus 14% of the children with influenza who also had a chest radiograph had pneumonia.
Clinical findings of the 134 patients with influenza and pneumonia were similar among those with influenza A or B. The most common symptoms were fever (98%), cough (84%), and rhinorrhea (65%). The classical findings of headaches and myalgias were difficult to uncover due to the young age of the patients (median age 2.2 years). Of the 134 identified patients with influenza and pneumonia only 27% presented with dyspnea and 22% with tachypnea. Crackles were heard in 22%, rhonchi in 43%, and decreased breath sounds in 10%. No abnormal auscultation findings were found in 32% of the children. Sixty-eight percent of the study population was admitted to the hospital. The rate of hospitalization was greater for the younger patients. One-third of the patients had received antibiotics prior to enrollment, and 80% of the children received antibiotics during the hospitalization or at time of discharge. Four children required ventilator therapy. One patient with muscular dystrophy died of severe pneumonia.
Laboratory assessment found that 89% of the children had WBC less than 15 x 109/liter. CRP values were normal or only slightly increased in 55% of the children. Three children (2%) had laboratory-documented concomitant bacterial infections. Of these three cases two were due to bacteremia and one to a positive tracheal aspirate. Five children (7%) had double viral infections.
In this hospital-based study 14% of the patients with influenza had radiographically proven pneumonia. The authors found that in contrast with what we know about adults with influenza pneumonia, data shows influenza pneumonia in children is generally a benign disease. The greater burden of disease tends to be in the children younger than three years of age. Respiratory clinical findings may be absent in light of radiographically proven pneumonia. Laboratory findings show that most children with influenza pneumonia have normal WBC counts and normal to only slightly elevated CRP levels.
Shortcomings of this informative study include the lack of direct evidence in proving that the presence of influenza in the upper respiratory tract is directly associated with the infiltrate of the lower respiratory tract. The data may also be skewed because fewer than one-half of the patients with influenza had chest radiographs. The authors’ conclusions demonstrated that clinical findings did not correlate well with radiographically proven infiltrates.—CM
Bradycardia During Methadone Therapy in an Infant
By Lisa Carney, MD
Wheeler AD, Tobias JD. Bradycardia during methadone therapy in an infant. Pediatr Crit Care Med. 2006;7(1):83-85.
This retrospective case report demonstrates the occurrence of bradycardia associated with the use of methadone administered to prevent withdrawal in an infant with physical tolerance following long-term opioid therapy in the PICU setting.
The authors describe the onset of sinus bradycardia in an infant following the initiation of methadone therapy as a transition for intravenous fentanyl administration. The onset of bradycardia was temporally related to standard doses of methadone. These episodes resolved with tactile stimulation. No other pathologic conditions were noted that could have been responsible for the bradycardia. Additionally, the episodes resolved with cessation of methadone therapy. It is unlikely that the bradycardia was merely a manifestation of deep sedation with methadone because the infant’s sedation scores were the same as when he had been receiving fentanyl, a time during which no bradycardia was noted.
When administering opioids, the clinician generally focuses on adverse effects such as respiratory depression, slowing of gastrointestinal motility, and physical dependence. But because methadone’s three-dimensional structure shares similarities with calcium channel antagonists, bradycardia may occur—especially at higher doses. This effect has been reported in the adult literature; however, this is the first report in an infant.
As pediatric hospitalists, we may receive a patient in transfer from the PICU who was recently started on methadone therapy. Given the relatively high frequency of this scenario, it is unclear why bradycardia has not been previously reported in the pediatric population. It may be that the effect was not attributed to methadone and in the majority of cases the slowing of the heart rate was likely to have been innocuous from a physiologic standpoint. What may be more significant is the unnecessary investigation into the etiology of the bradycardia if its relationship to methadone is not appreciated. However, there may be a subset of patients who will not tolerate the bradycardia. Thus, close monitoring is suggested during methadone therapy.
Innoculation Conundrums
Halperin SA, Sweet L, Baxendale D, et al. How soon after a prior tetanus-diphtheria vaccination can one give adult formulation tetanus-diphtheria-acellular pertussis vaccine? Pediatr Infect Dis J. 2006 Mar;25(3):195-200.
Adult tetanus/diphtheria toxoids and acellular pertussis vaccines (Tdap) have been developed to prevent pertussis in adolescents and adults. There are concerns that unacceptable rates of severe injection site reactions, including Arthus-type reactions might occur if Tdap is administered too soon after a previous tetanus/diphtheria toxoid vaccine, such as TD or Td.
This study was conducted via a school-based program where more than 7,000 children/adolescents in grades three-12 were enrolled. These students received Tdap vaccine at intervals from previous vaccination with TD or Td of either 18 months-nine years or greater than/equal to 10 years. The 18 month-nine year interval was further divided into eight cohorts. One cohort per year two to nine (+/- 0.5 years) since receipt of the last TD/Td. Approximately 85% of the students provided accurate documentation of adverse events. There were no serious/major adverse events. There were no differences in reports of fever. Injection site erythema and swelling were slightly and statistically significantly increased with those participants with the most recent prior TD/Td. The increase in these localized injection site events ranged from 3.75%-10.3%.
In summary, although there is a slight increase in injection site events with decreasing interval since a previous immunization, Tdap can be safely administered at intervals of greater than or equal to 18 months since a previous TD/Td vaccine.—LC
Viral Occurrences in Young Children
Wolf DG, Greenberg D, Kalkstein D, et al. Comparison of human metapneumovirus, respiratory syncytial virus and influenza A virus lower respiratory tract infections in hospitalized young children. Pediatr Infect Dis J. 2006;25(4):320-324.
The authors compared the clinical and demographic features of children with lower respiratory tract infection (LRI) caused by human metapneumovirus (HMPV), respiratory syncytial virus (RSV), and influenza A virus and sought to determine whether coinfection by HMPV and other respiratory viruses leads to increased disease severity.
This prospective study enrolled 516 children <5 years old who were admitted with LRI at the Soroka University Medical Center in Israel during a one-year period from November 2001 through October 2002. At least one virus was detected in 57% of the enrolled patients.
Of those 293 patients, the viral breakdown was as follows: HMPV (13%), RSV (20%), influenza A (15%), parainfluenza (7%), and adenovirus (2%). The seasonal distribution of HMPV infections resembled those of RSV and influenza with peak incidence between November and March. Twenty-four percent of the HMPV children had co-infections with other respiratory viruses, most commonly RSV.
HMPV patients were older than RSV patients (17.6 +/- 16.8 months versus 10.5 +/- 11.8 months). HMPV was associated with wheezing and hypoxemia at a rate similar to that of RSV and higher than that of influenza A. Atelectasis was more common among HMPV (40%) than among RSV and influenza patients (13%). HMPV was more often associated with a diagnosis of pneumonia than RSV and influenza. HMPV was also more often associated with a diagnosis of asthma and less often with a diagnosis of bronchiolitis than RSV, even when corrected for age. Children who had a co-infection with HMPV had a higher rate of gastrointestinal symptoms but did not show a more severe respiratory picture.
In conclusion, the clinical pattern of HMPV (wheezing, hypoxemia) more closely resembles that of RSV than that of influenza A LRI. Additionally, there was no difference in disease severity between children with HMPV and RSV infection. However, the differences in age, radiographic findings, and clinical diagnosis suggest that HMPV pathogenesis may differ from that of RSV.—LC
Kawasaki Disease in Infants Younger Than Six Months
By Judith Waldman, DO
Chang FY, Hwang B, Chen SJ, et al. Characteristics of Kawasaki disease in infants younger than six months of age. Pediatr Infect Dis J. 2006 Mar;25(3):241-244.
Pi-Chang Lee, MD, and colleagues compared the clinical manifestations, laboratory results, echocardiographic findings, treatment, and outcome between two groups of patients hospitalized with Kawasaki disease. Group one consisted of 20 patients younger than six months. Group two consisted of 100 patients older than six months. The data was collected by chart review.
Researchers found that the time from onset of disease to diagnosis was longer in infants younger than six months. Patients less than six months of age had a higher incidence of incomplete Kawasaki disease. A presentation of full diagnostic criteria within 10 days occurred more frequently in patients greater than six months of age. There was no significant difference in major clinical manifestations between the two groups. However, the frequency of gallbladder hydrops was higher in patients older than six months of age.
Group one had higher white blood cell counts, platelet counts, and triglyceride concentrations and lower hemoglobin values. Group one had higher incidence of coronary involvement, including irregular surface and/or perivascular brightness of coronary artery wall, coronary dilatation, and aneurysm formation. There was no significant difference in giant aneurysm formation between the two groups. Group one had a higher incidence of pericardial effusion and tricuspid regurgitation/mitral regurgitation. Fewer patients received IVIG within 10 days in the younger age group. Diagnostic delay and incomplete presentation postponed IVIG in the patients less than six months of age.
New recommendations pertaining to the diagnosis and treatment of Kawasaki disease in the American Academy of Pediatric’s Red Book in 2006 should be beneficial in making a more rapid diagnosis and thus more timely treatment. In the past, diagnosis of Kawasaki required five full days of fever. Now, IVIG can be started after four days of fever if the patient meets four out of the five total criteria for disease. In cases of incomplete Kawasaki disease, physicians should base diagnosis and treatment on laboratory test results instead of visible symptoms. Obtain a baseline echo as usual. The laboratory criteria are albumin 3 g/dL or less, anemia, high alanine amino transferase, platelets after 7 days to 450,000/mm3 or greater, WBC count is 15,000 mm3 or greater, and urine 10 WBC/high powered field or greater. For patients who do not respond to 2g/kg of IVIG, the new recommendation is to retreat these patients with another 2g/kg of IVIG or use pulse steroid therapy. Look for these recommendations in the new 2006 Red Book. TH
Meningococcal Disease in Peds
By J. Christopher Day, MD
Thompson, MJ, Ninis N, Perera R, et al. Clinical recognition of meningococcal disease in children and adolescents. Lancet. 2006 Feb 6;367(9508)397-403.
Data from medical records and parental questionnaires were examined to determine the time course and prevalence of signs and symptoms in meningococcal disease (sepsis and meningitis) in 448 children in Wales, England, and Northern Ireland.
The authors note that classic clinical features of the disease appear late in the illness. The symptoms that appear earliest (fever, poor feeding, nausea, vomiting, coryza, sore throat) are very non-specific, but somewhat later symptoms of sepsis including leg pains, cold hands and feet, and abnormal skin color appear before the classical clinical features in 72% of the children studied. The authors hope that recognition of these features can lead to earlier diagnosis and treatment of this severe disease.
Treatment of Infant Botulism
Arnon SS, Schechter R, Maslanka SE, et al. Human botulism immune globulin for the treatment of infant botulism. N Engl J Med. 2006 Feb 2;354((5):462-471.
This is is a report of a randomized, double-blind, placebo controlled trial of the use of human botulism immune globulin intravenous (BIG-IV) used for the treatment of infant botulism. The study was performed on 122 infants with (initially) suspected and (later) laboratory confirmed infant botulism. BIG-IV was given within three days of hospital admission. The authors also performed an open-label study of 382 laboratory confirmed cases. Some of these began treatment as late as 18 days after hospital admission.
In the randomized trial, outcomes compared with placebo included a reduction in hospital stay from 5.7 weeks to 2.6 weeks (P<0.001); a reduction in the mean duration of intensive care by 3.2 weeks (P<0.001); the mean duration of mechanical ventilation by 2.6 weeks (P= 0.01); the mean duration of tube or intravenous feeding by 6.4 weeks; and the mean hospital charges per patient by $88,600 (P<0.001).
The only notable adverse event perhaps related to treatment was a transient blush-like erythematous rash. In the open-label study, treatment given within three days of hospital admission shortened the mean length of stay by approximately one week more than did treatment given four to seven days after admission. BIG-IV is now licensed as BabyBIG. The authors recommend treatment as soon as possible after hospital admission.—JCD
Eczema: Wet Wraps Versus Conventional Treatment
Hindley D, Galloway G, Murray J, et al. A randomised study of “wet wraps” versus conventional treatment for atopic eczema. Arch Dis Child. 2006 Feb;91(2):164-168.
The authors were interested in comparing the efficacy and parent perception of ease of application of conventional treatment (emulsifying ointments and topical steroids) with wet wraps (tubular retention bandages applied wet as occlusive dressings over emulsifying ointments) and topical steroids for exacerbations of eczema.
Fifty children were enrolled and randomized to either treatment group. Treatment was continued and patients were followed for one month. The change in eczema severity was scored using a previously published scale (SCORAD) for assessing severity. No differences were noted between the two groups, though the study had a number of limitations including use of only one potency of steroid (1% hydrocortisone) limiting generalizability, the length of treatment (regimens vary in length), and patient drop-outs (five dropped out—all in the wet wrap group).
Parents felt wet wraps were harder to use. The authors do note that there may be clinical situations (they mention short term treatment of acute erythrodermic eczema) where wet wraps are a useful option. There appear to be no advantages in the group studied over a four-week period and the disadvantages likely include parental perception of difficulty of use and a possibility of increased skin infections.—JCD
A Study of Dehydrated Peds
Mallory MD, Kadish H, Zebrack M, Nelson D. Use of a pediatric observation unit for treatment of children with dehydration caused by gastroenteritis. Pediatr Emerg Care. 2006 Jan;22(1):1-6.
A case-control study was performed to examine 467 admissions to an observation unit in patients with dehydration from vomiting or diarrhea from presumed gastroenteritis. Patients were presumably admitted to the observation unit (staffed by emergency department personnel) if they were believed to require more rehydration than could be reasonably offered in the emergency department itself.
Controls were defined as those patients able to be discharged home from the observation unit within 24 hours and cases as those patients that required subsequent inpatient admission. Nineteen percent of the patients studied required inpatient admission.
One of the goals of the study was to determine variables useful in distinguishing patients who would require subsequent inpatient admission from those who would be discharged home from the observation unit. No such variables were found.
Variables studied included oral intake prior to presentation, urine output at presentation, symptoms at presentation (vomiting versus diarrhea versus both), predominant symptoms (vomiting versus diarrhea versus no predominance), duration of symptoms, abdomen tender to palpation (yes/no), previous visit within five days (yes/no), age, vital signs, bicarbonate levels, and mean sodium levels.—JCD
Routine Neuroimaging: Little Value When Evaluating Febrile Seizures
By Stevie Wilson, RN, CPNP
Teng D, Dayan P, Tyler S, et al. Risk of intracranial pathologic conditions requiring emergency intervention after a first complex febrile seizure episode among children. Pediatrics. 2006;117(2):304-308.
Febrile seizures occur in up to 5% of all children. One-third of febrile seizures are classified as complex (i.e., having multiple seizures, prolonged duration, or focal seizures). Complex febrile seizures have been associated with an increased risk of recurrent febrile seizures and epilepsy. However, they have not been associated with pathologic intracranial lesions that require emergency surgical intervention.
Previous studies suggest that intracranial abnormalities are rare among simple febrile seizures. The American Academy of Pediatrics (AAP) recommends against the use of neuroimaging with simple seizures, however, practice guidelines for emergency neuroimaging for complex seizures do not exist. The objective of this study was to determine the likelihood of a significant intracranial condition requiring emergency intervention in children with the first complex febrile seizure.
A retrospective review of prospectively collected data was performed for 71 children who presented to the pediatric emergency department after a first complex febrile seizure. None of the 71 patients had a pathologic intracranial lesion that required emergency intervention. The authors therefore concluded that the risk of pathologic intracranial conditions requiring emergency intervention is low, suggesting that routine emergency neuroimaging for this population is unnecessary.
Managing Bronchiolitis above Sea Level
Choudhuri JA, Ogden LG, Ruttenber JA, et al. Effect of altitude on hospitalizations for respiratory syncytial virus infection. Pediatrics. 2006;117(2):349-356.
This interesting study sought to evaluate the effect altitude has on hospitalizations for RSV infection. A multivariate analysis was obtained and suggests that the rate of hospitalization for RSV increased by 25% among infants who were younger than one year of age for every 1,000 meters of altitude. The risk of RSV-associated hospitalization was highest at elevations above 2,500 meters.—SW
Dilemmas for Wheezing Peds
By Chris Miller, MD
Oymar K, Halvorsen T, Aksnes L. Mast cell activation and leukotriene secretion in wheezing infants. Relation to respiratory syncytial virus and outcome. Pediatr Allergy Immunol. 2006 Feb;17(1):37-42.
The wheezing infant is a common problem in pediatric medicine; however, the long-term outcome and risk for recurrent wheezing remains unclear. The authors of this study assert that the risk for recurrent wheezing may be related to the type of inflammation and specific underlying virus during the initial wheezing episode.
Several studies have evaluated the specific contribution of eosinophils to respiratory inflammation in the wheezing child. These studies have found that eosinophilic inflammation may play a role in the airway hyper-reactivity in a child with persistent wheezing. Conversely, little information is available regarding mast cell involvement. This prospective study was designed to assess mast cell activation, in relation to respiratory syncytial virus (RSV) infection and persistent wheezing in wheezing infants.
Researchers enrolled 106 wheezing infants who were subsequently admitted to the hospital. None of these infants had a prior history of wheezing. Infants with prior history of atopic disease, lung disease, or signs of bacterial infection were excluded. RSV testing of nasopharyngeal mucous was performed. Sixty-seven (63%) of the wheezing infants had RSV. An additional 23 healthy infants were selected as controls.
To assess the extent of mast cell activation, urinary prostaglandin F2 (U-PGF2) was measured. To assess for leukotriene secretion urinary leukotriene 4 (U-LTE4) was measured. To evaluate for persistence or reoccurrence of wheezing, a 20-month post-hospitalization follow-up was done. One hundred and three (97%) of the previously hospitalized wheezing infants were available for the follow-up.
The authors used the term “persistent wheezing” to describe those children who experienced at least three wheezing episodes including the first hospitalization. These recurrences were identified either by parental report utilizing a standardized questionnaire or physician/hospitalization records. The remaining children were considered “transient wheezers.”
Review of the data regarding U-PGF2, a specific marker for mast cell activation, showed U-PGF2 to be greatest in the RSV positive patients, followed by the RSV negative patients and finally by the control group. U-LTE4, and thus leukotriene involvement, was also found to be significantly elevated in both the RSV positive and negative wheezing infants compared with the controls. No significant difference was found in U-LTE4 between RSV-positive infants and RSV-negative infants. The transient wheezing infant had a higher U-PGF2 than the persistent wheezing infant. Transient wheezers also had a higher U-LTE4 compared with persistent wheezers, although this was not statistically significant.
With univariate regression analysis positive predictive factors for persistent wheezing included increasing age, RSV negative disease, parental atopy, and male gender. Negative predictive factors for persistent wheezing included an elevated U-PGF2 level.
In discussion the authors conclude that mast cell activation and leukotriene secretion is present in a wheezing infant as noted by increased U-PGF2 and U-LTE4 levels, respectively. Higher U-PGF2 levels in RSV-positive patients indicates that mast cell activation may play a bigger part in the inflammatory process of RSV-induced wheezing compared with non-RSV induced wheezing. Leukotrienes appear to be involved in both RSV and non-RSV wheezing infants. Despite these results, mast cell activation and leukotriene secretion do not appear to be associated with persistent wheezing.
Limitations of this interesting study include the small sample size, apparent lack of follow-up with the control patients, and the diagnosis of recurrent wheezing episodes being characterized by the parents.
Influenza Pneumonia in Pediatric Patients
Lahti E, Peltola V, Virkki R, et al. Influenza pneumonia. Pediatr Infect Dis J. 2006 Feb;25(2):160-164.
Influenza and pneumonia are common in children. The objective of this study was to describe the frequency and characteristics of laboratory-documented and radiographically proven influenza-associated pneumonia in children.
This retrospective, single site study was conducted at Turku University Hospital (Finland). Chart reviews of both inpatient and outpatient visits of children younger than 16 were performed for a 24-year period between 1980 through 2003. Children with influenza A or B antigen detected nasopharyngeal aspirates were identified. Also children with chest radiographs obtained during their influenza infection were identified. Clinical findings upon initial presentation were summarized, in addition to laboratory values for white blood cell count (WBC) and C-reactive protein (CRP).
A total of 936 patients with virologically confirmed influenza were identified. Of this total, 79% had influenza A and the remaining had influenza B. Chest radiographs were reported on 400 (43%) of these patients. Of the 400 films, 228 were initially read as having infiltrates. However, during over-reading of the films 70 chest radiographs did not have an infiltrate and an additional 24 films could not be found. In summary, 134 children had both confirmed influenza and radiographically proven pneumonia. Thus 14% of the children with influenza who also had a chest radiograph had pneumonia.
Clinical findings of the 134 patients with influenza and pneumonia were similar among those with influenza A or B. The most common symptoms were fever (98%), cough (84%), and rhinorrhea (65%). The classical findings of headaches and myalgias were difficult to uncover due to the young age of the patients (median age 2.2 years). Of the 134 identified patients with influenza and pneumonia only 27% presented with dyspnea and 22% with tachypnea. Crackles were heard in 22%, rhonchi in 43%, and decreased breath sounds in 10%. No abnormal auscultation findings were found in 32% of the children. Sixty-eight percent of the study population was admitted to the hospital. The rate of hospitalization was greater for the younger patients. One-third of the patients had received antibiotics prior to enrollment, and 80% of the children received antibiotics during the hospitalization or at time of discharge. Four children required ventilator therapy. One patient with muscular dystrophy died of severe pneumonia.
Laboratory assessment found that 89% of the children had WBC less than 15 x 109/liter. CRP values were normal or only slightly increased in 55% of the children. Three children (2%) had laboratory-documented concomitant bacterial infections. Of these three cases two were due to bacteremia and one to a positive tracheal aspirate. Five children (7%) had double viral infections.
In this hospital-based study 14% of the patients with influenza had radiographically proven pneumonia. The authors found that in contrast with what we know about adults with influenza pneumonia, data shows influenza pneumonia in children is generally a benign disease. The greater burden of disease tends to be in the children younger than three years of age. Respiratory clinical findings may be absent in light of radiographically proven pneumonia. Laboratory findings show that most children with influenza pneumonia have normal WBC counts and normal to only slightly elevated CRP levels.
Shortcomings of this informative study include the lack of direct evidence in proving that the presence of influenza in the upper respiratory tract is directly associated with the infiltrate of the lower respiratory tract. The data may also be skewed because fewer than one-half of the patients with influenza had chest radiographs. The authors’ conclusions demonstrated that clinical findings did not correlate well with radiographically proven infiltrates.—CM
Bradycardia During Methadone Therapy in an Infant
By Lisa Carney, MD
Wheeler AD, Tobias JD. Bradycardia during methadone therapy in an infant. Pediatr Crit Care Med. 2006;7(1):83-85.
This retrospective case report demonstrates the occurrence of bradycardia associated with the use of methadone administered to prevent withdrawal in an infant with physical tolerance following long-term opioid therapy in the PICU setting.
The authors describe the onset of sinus bradycardia in an infant following the initiation of methadone therapy as a transition for intravenous fentanyl administration. The onset of bradycardia was temporally related to standard doses of methadone. These episodes resolved with tactile stimulation. No other pathologic conditions were noted that could have been responsible for the bradycardia. Additionally, the episodes resolved with cessation of methadone therapy. It is unlikely that the bradycardia was merely a manifestation of deep sedation with methadone because the infant’s sedation scores were the same as when he had been receiving fentanyl, a time during which no bradycardia was noted.
When administering opioids, the clinician generally focuses on adverse effects such as respiratory depression, slowing of gastrointestinal motility, and physical dependence. But because methadone’s three-dimensional structure shares similarities with calcium channel antagonists, bradycardia may occur—especially at higher doses. This effect has been reported in the adult literature; however, this is the first report in an infant.
As pediatric hospitalists, we may receive a patient in transfer from the PICU who was recently started on methadone therapy. Given the relatively high frequency of this scenario, it is unclear why bradycardia has not been previously reported in the pediatric population. It may be that the effect was not attributed to methadone and in the majority of cases the slowing of the heart rate was likely to have been innocuous from a physiologic standpoint. What may be more significant is the unnecessary investigation into the etiology of the bradycardia if its relationship to methadone is not appreciated. However, there may be a subset of patients who will not tolerate the bradycardia. Thus, close monitoring is suggested during methadone therapy.
Innoculation Conundrums
Halperin SA, Sweet L, Baxendale D, et al. How soon after a prior tetanus-diphtheria vaccination can one give adult formulation tetanus-diphtheria-acellular pertussis vaccine? Pediatr Infect Dis J. 2006 Mar;25(3):195-200.
Adult tetanus/diphtheria toxoids and acellular pertussis vaccines (Tdap) have been developed to prevent pertussis in adolescents and adults. There are concerns that unacceptable rates of severe injection site reactions, including Arthus-type reactions might occur if Tdap is administered too soon after a previous tetanus/diphtheria toxoid vaccine, such as TD or Td.
This study was conducted via a school-based program where more than 7,000 children/adolescents in grades three-12 were enrolled. These students received Tdap vaccine at intervals from previous vaccination with TD or Td of either 18 months-nine years or greater than/equal to 10 years. The 18 month-nine year interval was further divided into eight cohorts. One cohort per year two to nine (+/- 0.5 years) since receipt of the last TD/Td. Approximately 85% of the students provided accurate documentation of adverse events. There were no serious/major adverse events. There were no differences in reports of fever. Injection site erythema and swelling were slightly and statistically significantly increased with those participants with the most recent prior TD/Td. The increase in these localized injection site events ranged from 3.75%-10.3%.
In summary, although there is a slight increase in injection site events with decreasing interval since a previous immunization, Tdap can be safely administered at intervals of greater than or equal to 18 months since a previous TD/Td vaccine.—LC
Viral Occurrences in Young Children
Wolf DG, Greenberg D, Kalkstein D, et al. Comparison of human metapneumovirus, respiratory syncytial virus and influenza A virus lower respiratory tract infections in hospitalized young children. Pediatr Infect Dis J. 2006;25(4):320-324.
The authors compared the clinical and demographic features of children with lower respiratory tract infection (LRI) caused by human metapneumovirus (HMPV), respiratory syncytial virus (RSV), and influenza A virus and sought to determine whether coinfection by HMPV and other respiratory viruses leads to increased disease severity.
This prospective study enrolled 516 children <5 years old who were admitted with LRI at the Soroka University Medical Center in Israel during a one-year period from November 2001 through October 2002. At least one virus was detected in 57% of the enrolled patients.
Of those 293 patients, the viral breakdown was as follows: HMPV (13%), RSV (20%), influenza A (15%), parainfluenza (7%), and adenovirus (2%). The seasonal distribution of HMPV infections resembled those of RSV and influenza with peak incidence between November and March. Twenty-four percent of the HMPV children had co-infections with other respiratory viruses, most commonly RSV.
HMPV patients were older than RSV patients (17.6 +/- 16.8 months versus 10.5 +/- 11.8 months). HMPV was associated with wheezing and hypoxemia at a rate similar to that of RSV and higher than that of influenza A. Atelectasis was more common among HMPV (40%) than among RSV and influenza patients (13%). HMPV was more often associated with a diagnosis of pneumonia than RSV and influenza. HMPV was also more often associated with a diagnosis of asthma and less often with a diagnosis of bronchiolitis than RSV, even when corrected for age. Children who had a co-infection with HMPV had a higher rate of gastrointestinal symptoms but did not show a more severe respiratory picture.
In conclusion, the clinical pattern of HMPV (wheezing, hypoxemia) more closely resembles that of RSV than that of influenza A LRI. Additionally, there was no difference in disease severity between children with HMPV and RSV infection. However, the differences in age, radiographic findings, and clinical diagnosis suggest that HMPV pathogenesis may differ from that of RSV.—LC
Kawasaki Disease in Infants Younger Than Six Months
By Judith Waldman, DO
Chang FY, Hwang B, Chen SJ, et al. Characteristics of Kawasaki disease in infants younger than six months of age. Pediatr Infect Dis J. 2006 Mar;25(3):241-244.
Pi-Chang Lee, MD, and colleagues compared the clinical manifestations, laboratory results, echocardiographic findings, treatment, and outcome between two groups of patients hospitalized with Kawasaki disease. Group one consisted of 20 patients younger than six months. Group two consisted of 100 patients older than six months. The data was collected by chart review.
Researchers found that the time from onset of disease to diagnosis was longer in infants younger than six months. Patients less than six months of age had a higher incidence of incomplete Kawasaki disease. A presentation of full diagnostic criteria within 10 days occurred more frequently in patients greater than six months of age. There was no significant difference in major clinical manifestations between the two groups. However, the frequency of gallbladder hydrops was higher in patients older than six months of age.
Group one had higher white blood cell counts, platelet counts, and triglyceride concentrations and lower hemoglobin values. Group one had higher incidence of coronary involvement, including irregular surface and/or perivascular brightness of coronary artery wall, coronary dilatation, and aneurysm formation. There was no significant difference in giant aneurysm formation between the two groups. Group one had a higher incidence of pericardial effusion and tricuspid regurgitation/mitral regurgitation. Fewer patients received IVIG within 10 days in the younger age group. Diagnostic delay and incomplete presentation postponed IVIG in the patients less than six months of age.
New recommendations pertaining to the diagnosis and treatment of Kawasaki disease in the American Academy of Pediatric’s Red Book in 2006 should be beneficial in making a more rapid diagnosis and thus more timely treatment. In the past, diagnosis of Kawasaki required five full days of fever. Now, IVIG can be started after four days of fever if the patient meets four out of the five total criteria for disease. In cases of incomplete Kawasaki disease, physicians should base diagnosis and treatment on laboratory test results instead of visible symptoms. Obtain a baseline echo as usual. The laboratory criteria are albumin 3 g/dL or less, anemia, high alanine amino transferase, platelets after 7 days to 450,000/mm3 or greater, WBC count is 15,000 mm3 or greater, and urine 10 WBC/high powered field or greater. For patients who do not respond to 2g/kg of IVIG, the new recommendation is to retreat these patients with another 2g/kg of IVIG or use pulse steroid therapy. Look for these recommendations in the new 2006 Red Book. TH
Meningococcal Disease in Peds
By J. Christopher Day, MD
Thompson, MJ, Ninis N, Perera R, et al. Clinical recognition of meningococcal disease in children and adolescents. Lancet. 2006 Feb 6;367(9508)397-403.
Data from medical records and parental questionnaires were examined to determine the time course and prevalence of signs and symptoms in meningococcal disease (sepsis and meningitis) in 448 children in Wales, England, and Northern Ireland.
The authors note that classic clinical features of the disease appear late in the illness. The symptoms that appear earliest (fever, poor feeding, nausea, vomiting, coryza, sore throat) are very non-specific, but somewhat later symptoms of sepsis including leg pains, cold hands and feet, and abnormal skin color appear before the classical clinical features in 72% of the children studied. The authors hope that recognition of these features can lead to earlier diagnosis and treatment of this severe disease.
Treatment of Infant Botulism
Arnon SS, Schechter R, Maslanka SE, et al. Human botulism immune globulin for the treatment of infant botulism. N Engl J Med. 2006 Feb 2;354((5):462-471.
This is is a report of a randomized, double-blind, placebo controlled trial of the use of human botulism immune globulin intravenous (BIG-IV) used for the treatment of infant botulism. The study was performed on 122 infants with (initially) suspected and (later) laboratory confirmed infant botulism. BIG-IV was given within three days of hospital admission. The authors also performed an open-label study of 382 laboratory confirmed cases. Some of these began treatment as late as 18 days after hospital admission.
In the randomized trial, outcomes compared with placebo included a reduction in hospital stay from 5.7 weeks to 2.6 weeks (P<0.001); a reduction in the mean duration of intensive care by 3.2 weeks (P<0.001); the mean duration of mechanical ventilation by 2.6 weeks (P= 0.01); the mean duration of tube or intravenous feeding by 6.4 weeks; and the mean hospital charges per patient by $88,600 (P<0.001).
The only notable adverse event perhaps related to treatment was a transient blush-like erythematous rash. In the open-label study, treatment given within three days of hospital admission shortened the mean length of stay by approximately one week more than did treatment given four to seven days after admission. BIG-IV is now licensed as BabyBIG. The authors recommend treatment as soon as possible after hospital admission.—JCD
Eczema: Wet Wraps Versus Conventional Treatment
Hindley D, Galloway G, Murray J, et al. A randomised study of “wet wraps” versus conventional treatment for atopic eczema. Arch Dis Child. 2006 Feb;91(2):164-168.
The authors were interested in comparing the efficacy and parent perception of ease of application of conventional treatment (emulsifying ointments and topical steroids) with wet wraps (tubular retention bandages applied wet as occlusive dressings over emulsifying ointments) and topical steroids for exacerbations of eczema.
Fifty children were enrolled and randomized to either treatment group. Treatment was continued and patients were followed for one month. The change in eczema severity was scored using a previously published scale (SCORAD) for assessing severity. No differences were noted between the two groups, though the study had a number of limitations including use of only one potency of steroid (1% hydrocortisone) limiting generalizability, the length of treatment (regimens vary in length), and patient drop-outs (five dropped out—all in the wet wrap group).
Parents felt wet wraps were harder to use. The authors do note that there may be clinical situations (they mention short term treatment of acute erythrodermic eczema) where wet wraps are a useful option. There appear to be no advantages in the group studied over a four-week period and the disadvantages likely include parental perception of difficulty of use and a possibility of increased skin infections.—JCD
A Study of Dehydrated Peds
Mallory MD, Kadish H, Zebrack M, Nelson D. Use of a pediatric observation unit for treatment of children with dehydration caused by gastroenteritis. Pediatr Emerg Care. 2006 Jan;22(1):1-6.
A case-control study was performed to examine 467 admissions to an observation unit in patients with dehydration from vomiting or diarrhea from presumed gastroenteritis. Patients were presumably admitted to the observation unit (staffed by emergency department personnel) if they were believed to require more rehydration than could be reasonably offered in the emergency department itself.
Controls were defined as those patients able to be discharged home from the observation unit within 24 hours and cases as those patients that required subsequent inpatient admission. Nineteen percent of the patients studied required inpatient admission.
One of the goals of the study was to determine variables useful in distinguishing patients who would require subsequent inpatient admission from those who would be discharged home from the observation unit. No such variables were found.
Variables studied included oral intake prior to presentation, urine output at presentation, symptoms at presentation (vomiting versus diarrhea versus both), predominant symptoms (vomiting versus diarrhea versus no predominance), duration of symptoms, abdomen tender to palpation (yes/no), previous visit within five days (yes/no), age, vital signs, bicarbonate levels, and mean sodium levels.—JCD
Routine Neuroimaging: Little Value When Evaluating Febrile Seizures
By Stevie Wilson, RN, CPNP
Teng D, Dayan P, Tyler S, et al. Risk of intracranial pathologic conditions requiring emergency intervention after a first complex febrile seizure episode among children. Pediatrics. 2006;117(2):304-308.
Febrile seizures occur in up to 5% of all children. One-third of febrile seizures are classified as complex (i.e., having multiple seizures, prolonged duration, or focal seizures). Complex febrile seizures have been associated with an increased risk of recurrent febrile seizures and epilepsy. However, they have not been associated with pathologic intracranial lesions that require emergency surgical intervention.
Previous studies suggest that intracranial abnormalities are rare among simple febrile seizures. The American Academy of Pediatrics (AAP) recommends against the use of neuroimaging with simple seizures, however, practice guidelines for emergency neuroimaging for complex seizures do not exist. The objective of this study was to determine the likelihood of a significant intracranial condition requiring emergency intervention in children with the first complex febrile seizure.
A retrospective review of prospectively collected data was performed for 71 children who presented to the pediatric emergency department after a first complex febrile seizure. None of the 71 patients had a pathologic intracranial lesion that required emergency intervention. The authors therefore concluded that the risk of pathologic intracranial conditions requiring emergency intervention is low, suggesting that routine emergency neuroimaging for this population is unnecessary.
Managing Bronchiolitis above Sea Level
Choudhuri JA, Ogden LG, Ruttenber JA, et al. Effect of altitude on hospitalizations for respiratory syncytial virus infection. Pediatrics. 2006;117(2):349-356.
This interesting study sought to evaluate the effect altitude has on hospitalizations for RSV infection. A multivariate analysis was obtained and suggests that the rate of hospitalization for RSV increased by 25% among infants who were younger than one year of age for every 1,000 meters of altitude. The risk of RSV-associated hospitalization was highest at elevations above 2,500 meters.—SW
Dilemmas for Wheezing Peds
By Chris Miller, MD
Oymar K, Halvorsen T, Aksnes L. Mast cell activation and leukotriene secretion in wheezing infants. Relation to respiratory syncytial virus and outcome. Pediatr Allergy Immunol. 2006 Feb;17(1):37-42.
The wheezing infant is a common problem in pediatric medicine; however, the long-term outcome and risk for recurrent wheezing remains unclear. The authors of this study assert that the risk for recurrent wheezing may be related to the type of inflammation and specific underlying virus during the initial wheezing episode.
Several studies have evaluated the specific contribution of eosinophils to respiratory inflammation in the wheezing child. These studies have found that eosinophilic inflammation may play a role in the airway hyper-reactivity in a child with persistent wheezing. Conversely, little information is available regarding mast cell involvement. This prospective study was designed to assess mast cell activation, in relation to respiratory syncytial virus (RSV) infection and persistent wheezing in wheezing infants.
Researchers enrolled 106 wheezing infants who were subsequently admitted to the hospital. None of these infants had a prior history of wheezing. Infants with prior history of atopic disease, lung disease, or signs of bacterial infection were excluded. RSV testing of nasopharyngeal mucous was performed. Sixty-seven (63%) of the wheezing infants had RSV. An additional 23 healthy infants were selected as controls.
To assess the extent of mast cell activation, urinary prostaglandin F2 (U-PGF2) was measured. To assess for leukotriene secretion urinary leukotriene 4 (U-LTE4) was measured. To evaluate for persistence or reoccurrence of wheezing, a 20-month post-hospitalization follow-up was done. One hundred and three (97%) of the previously hospitalized wheezing infants were available for the follow-up.
The authors used the term “persistent wheezing” to describe those children who experienced at least three wheezing episodes including the first hospitalization. These recurrences were identified either by parental report utilizing a standardized questionnaire or physician/hospitalization records. The remaining children were considered “transient wheezers.”
Review of the data regarding U-PGF2, a specific marker for mast cell activation, showed U-PGF2 to be greatest in the RSV positive patients, followed by the RSV negative patients and finally by the control group. U-LTE4, and thus leukotriene involvement, was also found to be significantly elevated in both the RSV positive and negative wheezing infants compared with the controls. No significant difference was found in U-LTE4 between RSV-positive infants and RSV-negative infants. The transient wheezing infant had a higher U-PGF2 than the persistent wheezing infant. Transient wheezers also had a higher U-LTE4 compared with persistent wheezers, although this was not statistically significant.
With univariate regression analysis positive predictive factors for persistent wheezing included increasing age, RSV negative disease, parental atopy, and male gender. Negative predictive factors for persistent wheezing included an elevated U-PGF2 level.
In discussion the authors conclude that mast cell activation and leukotriene secretion is present in a wheezing infant as noted by increased U-PGF2 and U-LTE4 levels, respectively. Higher U-PGF2 levels in RSV-positive patients indicates that mast cell activation may play a bigger part in the inflammatory process of RSV-induced wheezing compared with non-RSV induced wheezing. Leukotrienes appear to be involved in both RSV and non-RSV wheezing infants. Despite these results, mast cell activation and leukotriene secretion do not appear to be associated with persistent wheezing.
Limitations of this interesting study include the small sample size, apparent lack of follow-up with the control patients, and the diagnosis of recurrent wheezing episodes being characterized by the parents.
Influenza Pneumonia in Pediatric Patients
Lahti E, Peltola V, Virkki R, et al. Influenza pneumonia. Pediatr Infect Dis J. 2006 Feb;25(2):160-164.
Influenza and pneumonia are common in children. The objective of this study was to describe the frequency and characteristics of laboratory-documented and radiographically proven influenza-associated pneumonia in children.
This retrospective, single site study was conducted at Turku University Hospital (Finland). Chart reviews of both inpatient and outpatient visits of children younger than 16 were performed for a 24-year period between 1980 through 2003. Children with influenza A or B antigen detected nasopharyngeal aspirates were identified. Also children with chest radiographs obtained during their influenza infection were identified. Clinical findings upon initial presentation were summarized, in addition to laboratory values for white blood cell count (WBC) and C-reactive protein (CRP).
A total of 936 patients with virologically confirmed influenza were identified. Of this total, 79% had influenza A and the remaining had influenza B. Chest radiographs were reported on 400 (43%) of these patients. Of the 400 films, 228 were initially read as having infiltrates. However, during over-reading of the films 70 chest radiographs did not have an infiltrate and an additional 24 films could not be found. In summary, 134 children had both confirmed influenza and radiographically proven pneumonia. Thus 14% of the children with influenza who also had a chest radiograph had pneumonia.
Clinical findings of the 134 patients with influenza and pneumonia were similar among those with influenza A or B. The most common symptoms were fever (98%), cough (84%), and rhinorrhea (65%). The classical findings of headaches and myalgias were difficult to uncover due to the young age of the patients (median age 2.2 years). Of the 134 identified patients with influenza and pneumonia only 27% presented with dyspnea and 22% with tachypnea. Crackles were heard in 22%, rhonchi in 43%, and decreased breath sounds in 10%. No abnormal auscultation findings were found in 32% of the children. Sixty-eight percent of the study population was admitted to the hospital. The rate of hospitalization was greater for the younger patients. One-third of the patients had received antibiotics prior to enrollment, and 80% of the children received antibiotics during the hospitalization or at time of discharge. Four children required ventilator therapy. One patient with muscular dystrophy died of severe pneumonia.
Laboratory assessment found that 89% of the children had WBC less than 15 x 109/liter. CRP values were normal or only slightly increased in 55% of the children. Three children (2%) had laboratory-documented concomitant bacterial infections. Of these three cases two were due to bacteremia and one to a positive tracheal aspirate. Five children (7%) had double viral infections.
In this hospital-based study 14% of the patients with influenza had radiographically proven pneumonia. The authors found that in contrast with what we know about adults with influenza pneumonia, data shows influenza pneumonia in children is generally a benign disease. The greater burden of disease tends to be in the children younger than three years of age. Respiratory clinical findings may be absent in light of radiographically proven pneumonia. Laboratory findings show that most children with influenza pneumonia have normal WBC counts and normal to only slightly elevated CRP levels.
Shortcomings of this informative study include the lack of direct evidence in proving that the presence of influenza in the upper respiratory tract is directly associated with the infiltrate of the lower respiratory tract. The data may also be skewed because fewer than one-half of the patients with influenza had chest radiographs. The authors’ conclusions demonstrated that clinical findings did not correlate well with radiographically proven infiltrates.—CM
Bradycardia During Methadone Therapy in an Infant
By Lisa Carney, MD
Wheeler AD, Tobias JD. Bradycardia during methadone therapy in an infant. Pediatr Crit Care Med. 2006;7(1):83-85.
This retrospective case report demonstrates the occurrence of bradycardia associated with the use of methadone administered to prevent withdrawal in an infant with physical tolerance following long-term opioid therapy in the PICU setting.
The authors describe the onset of sinus bradycardia in an infant following the initiation of methadone therapy as a transition for intravenous fentanyl administration. The onset of bradycardia was temporally related to standard doses of methadone. These episodes resolved with tactile stimulation. No other pathologic conditions were noted that could have been responsible for the bradycardia. Additionally, the episodes resolved with cessation of methadone therapy. It is unlikely that the bradycardia was merely a manifestation of deep sedation with methadone because the infant’s sedation scores were the same as when he had been receiving fentanyl, a time during which no bradycardia was noted.
When administering opioids, the clinician generally focuses on adverse effects such as respiratory depression, slowing of gastrointestinal motility, and physical dependence. But because methadone’s three-dimensional structure shares similarities with calcium channel antagonists, bradycardia may occur—especially at higher doses. This effect has been reported in the adult literature; however, this is the first report in an infant.
As pediatric hospitalists, we may receive a patient in transfer from the PICU who was recently started on methadone therapy. Given the relatively high frequency of this scenario, it is unclear why bradycardia has not been previously reported in the pediatric population. It may be that the effect was not attributed to methadone and in the majority of cases the slowing of the heart rate was likely to have been innocuous from a physiologic standpoint. What may be more significant is the unnecessary investigation into the etiology of the bradycardia if its relationship to methadone is not appreciated. However, there may be a subset of patients who will not tolerate the bradycardia. Thus, close monitoring is suggested during methadone therapy.
Innoculation Conundrums
Halperin SA, Sweet L, Baxendale D, et al. How soon after a prior tetanus-diphtheria vaccination can one give adult formulation tetanus-diphtheria-acellular pertussis vaccine? Pediatr Infect Dis J. 2006 Mar;25(3):195-200.
Adult tetanus/diphtheria toxoids and acellular pertussis vaccines (Tdap) have been developed to prevent pertussis in adolescents and adults. There are concerns that unacceptable rates of severe injection site reactions, including Arthus-type reactions might occur if Tdap is administered too soon after a previous tetanus/diphtheria toxoid vaccine, such as TD or Td.
This study was conducted via a school-based program where more than 7,000 children/adolescents in grades three-12 were enrolled. These students received Tdap vaccine at intervals from previous vaccination with TD or Td of either 18 months-nine years or greater than/equal to 10 years. The 18 month-nine year interval was further divided into eight cohorts. One cohort per year two to nine (+/- 0.5 years) since receipt of the last TD/Td. Approximately 85% of the students provided accurate documentation of adverse events. There were no serious/major adverse events. There were no differences in reports of fever. Injection site erythema and swelling were slightly and statistically significantly increased with those participants with the most recent prior TD/Td. The increase in these localized injection site events ranged from 3.75%-10.3%.
In summary, although there is a slight increase in injection site events with decreasing interval since a previous immunization, Tdap can be safely administered at intervals of greater than or equal to 18 months since a previous TD/Td vaccine.—LC
Viral Occurrences in Young Children
Wolf DG, Greenberg D, Kalkstein D, et al. Comparison of human metapneumovirus, respiratory syncytial virus and influenza A virus lower respiratory tract infections in hospitalized young children. Pediatr Infect Dis J. 2006;25(4):320-324.
The authors compared the clinical and demographic features of children with lower respiratory tract infection (LRI) caused by human metapneumovirus (HMPV), respiratory syncytial virus (RSV), and influenza A virus and sought to determine whether coinfection by HMPV and other respiratory viruses leads to increased disease severity.
This prospective study enrolled 516 children <5 years old who were admitted with LRI at the Soroka University Medical Center in Israel during a one-year period from November 2001 through October 2002. At least one virus was detected in 57% of the enrolled patients.
Of those 293 patients, the viral breakdown was as follows: HMPV (13%), RSV (20%), influenza A (15%), parainfluenza (7%), and adenovirus (2%). The seasonal distribution of HMPV infections resembled those of RSV and influenza with peak incidence between November and March. Twenty-four percent of the HMPV children had co-infections with other respiratory viruses, most commonly RSV.
HMPV patients were older than RSV patients (17.6 +/- 16.8 months versus 10.5 +/- 11.8 months). HMPV was associated with wheezing and hypoxemia at a rate similar to that of RSV and higher than that of influenza A. Atelectasis was more common among HMPV (40%) than among RSV and influenza patients (13%). HMPV was more often associated with a diagnosis of pneumonia than RSV and influenza. HMPV was also more often associated with a diagnosis of asthma and less often with a diagnosis of bronchiolitis than RSV, even when corrected for age. Children who had a co-infection with HMPV had a higher rate of gastrointestinal symptoms but did not show a more severe respiratory picture.
In conclusion, the clinical pattern of HMPV (wheezing, hypoxemia) more closely resembles that of RSV than that of influenza A LRI. Additionally, there was no difference in disease severity between children with HMPV and RSV infection. However, the differences in age, radiographic findings, and clinical diagnosis suggest that HMPV pathogenesis may differ from that of RSV.—LC
Kawasaki Disease in Infants Younger Than Six Months
By Judith Waldman, DO
Chang FY, Hwang B, Chen SJ, et al. Characteristics of Kawasaki disease in infants younger than six months of age. Pediatr Infect Dis J. 2006 Mar;25(3):241-244.
Pi-Chang Lee, MD, and colleagues compared the clinical manifestations, laboratory results, echocardiographic findings, treatment, and outcome between two groups of patients hospitalized with Kawasaki disease. Group one consisted of 20 patients younger than six months. Group two consisted of 100 patients older than six months. The data was collected by chart review.
Researchers found that the time from onset of disease to diagnosis was longer in infants younger than six months. Patients less than six months of age had a higher incidence of incomplete Kawasaki disease. A presentation of full diagnostic criteria within 10 days occurred more frequently in patients greater than six months of age. There was no significant difference in major clinical manifestations between the two groups. However, the frequency of gallbladder hydrops was higher in patients older than six months of age.
Group one had higher white blood cell counts, platelet counts, and triglyceride concentrations and lower hemoglobin values. Group one had higher incidence of coronary involvement, including irregular surface and/or perivascular brightness of coronary artery wall, coronary dilatation, and aneurysm formation. There was no significant difference in giant aneurysm formation between the two groups. Group one had a higher incidence of pericardial effusion and tricuspid regurgitation/mitral regurgitation. Fewer patients received IVIG within 10 days in the younger age group. Diagnostic delay and incomplete presentation postponed IVIG in the patients less than six months of age.
New recommendations pertaining to the diagnosis and treatment of Kawasaki disease in the American Academy of Pediatric’s Red Book in 2006 should be beneficial in making a more rapid diagnosis and thus more timely treatment. In the past, diagnosis of Kawasaki required five full days of fever. Now, IVIG can be started after four days of fever if the patient meets four out of the five total criteria for disease. In cases of incomplete Kawasaki disease, physicians should base diagnosis and treatment on laboratory test results instead of visible symptoms. Obtain a baseline echo as usual. The laboratory criteria are albumin 3 g/dL or less, anemia, high alanine amino transferase, platelets after 7 days to 450,000/mm3 or greater, WBC count is 15,000 mm3 or greater, and urine 10 WBC/high powered field or greater. For patients who do not respond to 2g/kg of IVIG, the new recommendation is to retreat these patients with another 2g/kg of IVIG or use pulse steroid therapy. Look for these recommendations in the new 2006 Red Book. TH
In the Literature
Repeat Testing for C. Diff?
By Jeff Glasheen, MD
Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006 Apr;119(4):356.e7-356.e8
Clostridium difficile is a common complication of antibiotic and chemotherapeutic use, especially in hospitalized patients. Yet most nosocomial diarrhea is not caused by C. difficile. Most antibiotics can cause loose stools through changes in the gastrointestinal flora that result in inadequate digestion and absorption of carbohydrates and a resultant osmotic diarrhea. Further, antibiotics such as erythromycin and amoxicillin/clavulanate may result in diarrhea via increases in GI tract motility. While osmotic and motility causes of diarrhea tend to improve with antibiotic discontinuation, C. difficile-associated diarrhea is associated with significant morbidity that often continues until adequately treated.
Thus having a test that differentiates between C. difficile and non-clostridial diarrhea is essential. The most commonly used test is the enzyme immunoassay (EIA) that detects toxins A and B. The sensitivity and specificity of this test has been reported to range between 50%-90% and 70%-95%, respectively. The authors of this paper evaluated the utility of repeat EIA testing in patients with a one negative test in the setting of nosocomial diarrhea associated with antibiotic use.
The authors reviewed 474 sequential EIA tests for C. difficile in 396 patients over a 10-month period at a large university-affiliated community hospital with an EIA sensitivity and specificity of 80%-90% and 80%-95%, respectively. Tests were considered to be “repeat” if they occurred within seven days of the original negative test. Of the 78 repeat tests (16.5% of all tests), only one was positive, resulting in a 0.8% conversion rate. At an institutional cost of $128 per test the total cost of EIA testing over the 10-month period was $60,672. The cost of repeat testing alone was $9,984. The authors conclude that there is limited value—and high cost—in repeat EIA testing and that alternative sources of diarrhea should be sought or we should repeat EIA testing in patients with continued nosocomial diarrhea and a negative EIA test.
While prior studies have shown incremental benefit of retesting for C. difficile with the EIA assay, this study’s authors conclude that repeat “C. difficile testing is not clinically justified and is economically wasteful.” Unfortunately, the authors did not utilize a strong enough research design to defend this statement. From the data presented, all we can conclude is that repeat testing with an EIA assay did not add significant value to the diagnostic workup. The lack of a negative gold standard test, such as the cytotoxin assay or follow up outcomes, such as resolution of diarrhea, leaves the reader pondering if the repeat EIA assays were negative because the patients did not have C. difficile or because the test was not sensitive enough to detect the toxin. The reported sensitivity for the EIA assay used was 80-90%, meaning that 10%-20% of patients with C. difficile disease would have had a false negative test. While a second negative test would lower the likelihood of true disease, it would not lower it enough in a patient with a high pre-test probability of disease to sufficiently rule out the disease such that further testing is indicated.
Additionally, while we can extrapolate that the EIA test was of little utility to the patients studied here, no patient-specific data is presented. Thus it is difficult to determine if our patient population is represented in the study. More knowledge about the patients would allow the reader to use published prediction rules to better delineate how likely it was that this cohort was at high risk for having toxin-mediated diarrhea. Perhaps a more reasonable approach to this clinical conundrum would be to send the repeat stool test for a cytotoxin assay or to treat the patient empirically in situations where either the likelihood of disease or the disease burden is high.
Stroke after MI
By Ethan Cumbler, MD
Witt BJ, Ballman KV, Brown RD Jr, et al. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006 Apr;119(4):354.e1-9.
Stroke and myocardial infarction (MI) share many of the risk factors leading to atherosclerosis, including hypertension, hyperlipidemia, diabetes, tobacco abuse, and age. Logically, patients at risk for one event would also be at risk for the other, yet this interaction appears to be more complex. The study by Witt, et al., aims to elucidate the rate of in-hospital stroke in patients initially admitted with an MI.
The authors analyzed 22 observational studies of myocardial infarction that recorded the incidence of cerebrovascular accidents after acute MI. Clinical trials were excluded from the analysis in order to provide representation of an unselected population. Of the trials reviewed, 11 were included in the analysis of in-hospital strokes, three for the 30-day time point, and two for the one-year time point. The other trials used different time points and were not included in the analysis. The patients had a mean age ranging between 59 and 72.7 years, and all had a predominance of males. The rate of in-hospital stroke was 11.1 events per 1,000 hospitalizations. This incidence rose to 12.2/1,000 at 30 days and 21.4/1,000 at one year.
Plausible hypotheses for why the rate of cerebrovascular accident would be particularly high in the post-MI period include the potential for localized wall motion dysmotility or low flow leading to intracardiac thrombosis, event-related arrhythmia, or procedure-related embolic events. The studies from which this meta-analysis was derived were not designed in such a way for a causal relationship to be identified. However, age, diabetes, hypertension, prior stroke, anterior location of MI, atrial fibrillation, heart failure, and nonwhite race were all found to have an association with increased risk for stroke. Interestingly, angina on presentation was associated with an apparent decreased risk, theorized to potentially be due to ischemic preconditioning.
While this study shares the usual limitations of meta-analyses of observational studies, the authors have done an excellent summation of the data available including both English and non-English language articles in the analysis. Notably, the review included studies spanning more than 25 years and, thus, included data from studies done in the era prior to modern therapy for cardiac ischemia including potent antiplatelet and statin therapy. The three studies with in-hospital time points started in the 1990s had a lower average rate of stroke, which may reflect the effect of more potent anti-platelet agents used in today’s therapy for acute coronary syndromes.
The implication for the hospitalist is to recognize that patients admitted for MI are at high risk for stroke during the index hospitalization. A low threshold for suspicion of a cerebrovascular event needs to be maintained for post-MI patients with new neurologic symptoms. Future studies will be needed to address the risk/benefit of anticoagulation in high-risk patients for stroke following a myocardial infarction.
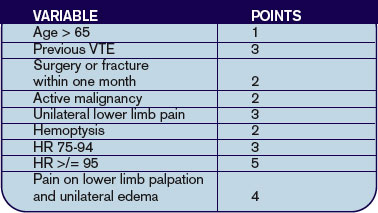
Predicting PE in the ED Using Revised Geneva Score
By Jeffrey Carter, MD
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-171.
Introduction: Pulmonary embolism remains a common life-threatening disorder with imperfect diagnostic modalities and strategies. Much of the current literature focuses on the development and validation of clinical probability assessments that identify low-risk patients who can be safely managed without invasive testing or lung scanning.
Two common scoring systems include the Geneva and Wells criteria, which employ a combination of historical information, clinical and laboratory data to stratify patients into three risk groups.1,2 It has recently been shown that a single negative D-dimer test safely excludes patients with suspected VTE in a large cohort, with a three-month follow-up rate of VTE of 0%.3 Criticism of current clinical probability assessment strategies include the inclusion of subjective criteria or the need for blood gas values.1,2 In this paper, the authors sought to derive and validate a scoring system based on readily available objective clinical data.
Methods: The cohort evaluated in this study consists of the same 965 patients used to prospectively evaluate an emergency department diagnostic strategy of VTE.3 Patients presenting to the emergency ward with complaints of chest pain or shortness of breath were evaluated with a standard diagnostic workup that included a checklist of demographic and historical information, signs and symptoms possibly consistent with VTE, ABG, chest X-ray, and EKG results, as well as the likelihood of another diagnosis. However, the goal was to create a scoring system based on readily available objective data, so ABG, chest X-ray and electrocardiogram results were not evaluated as possible components of the score. Clinical variables associated with pulmonary embolism were evaluated for statistical significance in both a univariate and multivariate model. These variables were then validated both internally and with an external cohort.
Results: The incidence of VTE was 23% (222/965). Ten clinical variables were found to be statistically significantly associated with VTE; these comprise the Revised Geneva Score.
Clinical probability is based on points: 0-3 is low probability; 4-10 is intermediate probability, and >10 is high probability. Low, intermediate, and high clinical probabilities had respective rates of VTE of 8%, 28%, and 74%. These percentages were found in the validation cohort and were similar to those in the derivation cohort.
Discussion: This study focuses on the derivation and validation of a clinical scoring system that can provide a numerical estimate of likelihood of VTE. The diagnostic strategy by which VTE is confirmed or excluded is from derivation cohort and is published elsewhere.3 In that study patients classified as no VTE and not treated had a 90-day risk of VTE of 1%. The nine-point revised Geneva score does indeed provide an accurate assessment of risk of VTE, and can thus help guide clinical decision-making. However it is not clear that the revised Geneva score will help decrease invasive diagnostic tests. In the low-risk group, 8% is too great a risk of a life-threatening illness to forego further diagnostic evaluation. Coupled with a negative ELISA D-dimer, exclusion of these patients is safe, but these patients cannot be safely excluded without risk stratification.3
References
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83:416-420.
- Wicki J, Perneger TV, Junof AF, et al. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 2001 Jan 8;161(1):92-97.
- Perrier A, Roy PM, Aujesky D, et al. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-299.
LMWH for Inpatient Palliative Care
By Jeanie Youngwerth, MD
Noble SI, Nelson A, Turner C, et al. Acceptability of low molecular weight heparin thromboprophylaxis for patients receiving palliative care: qualitative study. BMJ. 2006 Mar 11:332(7541);577-580.ePub 2006 Feb 3.
Venous thromboembolism is a major risk factor for patients with malignancy. VTE may reduce survival time in patients receiving palliative care, with one in seven inpatients with cancer dying from pulmonary embolism. The American College of Chest Physicians recommend low molecular weight heparin (LMWH) in hospitalized patients with cancer as level 1A evidence in their 2004 consensus statement on VTE. There are no thromboprophylaxis guidelines in the United Kingdom. Many physicians view daily injections of LMWH as unnecessary distress for palliative care patients. This study focused on what inpatients with advanced cancer receiving palliative care thought about the effect of thromboprophylaxis on overall quality of life.
This was a qualitative study of 28 inpatients receiving palliative care who had advanced metastatic cancer and who were in a regional cancer center in Wales. The patients had received LMWH for at least five consecutive days. The patients were audiotaped and then had semi-structured interviews transcribed regarding cancer treatments they had received. These interviews covered the patients’ insight into prognosis, their understanding of thromboprophylaxis, their beliefs concerning the effects of thromboprophylaxis on overall quality of life, and the negative aspects of heparin treatment.
The main outcome measures were recurring themes of the effect of thromboprophylaxis on overall quality of life. Major themes identified were insight into prognosis, knowledge and understanding of thromboprophylaxis, acceptability of heparin thromboprophylaxis, reassurance, and optimism. Minor themes identified were bruising, negative impact of antiembolic stockings, and anger at paternalistic views toward terminally ill patients.
Most patients showed clear insight into the nature of their condition and understood heparin prophylaxis for VTE. Many patients identified immobility and surgery as VTE risk factors, with little understanding of cancer as a risk factor. All knew that VTE could cause death, but none were aware of the common symptoms. All patients found LMWH thromboprophylaxis acceptable. Patients believed taking measures to prevent symptoms might improve their quality of life and felt that the medical team had not given up on them.
The only negative experiences of LMWH thromboprophylaxis was bruising. All of the patients who wore antiembolic stockings during previous admissions found them uncomfortable. Patients expressed their need to be involved in decision-making, particularly with respect to withdrawal or non-administration of treatment.
This small, qualitative study showed that, contrary to many physicians’ beliefs, patients in palliative care units believe that LMWH injections are acceptable as thromboprophylaxis, but antiembolic stockings are not. The effect of daily injections had little or no effect on the quality of life, with many patients having positive feelings that things were being done to prevent new problems from occurring.
This study was limited by the small sample size, the qualitative nature that could introduce interpretation bias, and the fact that only patients using LMWH were included. Additionally, the United Kingdom has aggressively educated the public on the risks of VTE associated with long flights such that baseline knowledge may differ in other parts of the world. Resource utilization, including drug costs and length of stay, as well as effect on mortality were not studied.
The implications for hospitalists are that many inpatients with advanced cancer receiving palliative care may find LMWH thromboprophylaxis acceptable therapy, and that discussions with the patient regarding this option should be explored together.
Cost Analysis: Intensive Glycemic Control in Critically Ill Adults
By Whitney Woodmansee, MD
Krinsley JS, Jones, RL. Cost analysis of intensive glycemic control in critically ill adult patients. Chest. 2006;129:644-650.
Several studies have demonstrated improved outcomes and decreased mortality in ICU patients treated with intensive control of blood glucose levels. This study sought to identify the costs associated with intensive glycemic control in the ICU.
An ICU patient database was analyzed for cost data related to intensive glycemic control. A baseline group of 800 consecutive ICU patients admitted prior to initiation (baseline) of an intensive glucose management (blood glucose levels between 80-140 mg/dl protocol were compared with a treatment group of 800 consecutive patients admitted after initiation of the protocol). Previously reported outcomes of these patients demonstrated significant improvement in mortality with tight glycemic control. Costs related to ICU and non-ICU length of stay; duration of mechanical ventilation; and all laboratory, pharmacy, and radiology services were analyzed between groups. Resource utilization was determined by assessing charges from the database and adjusting for inflation and applying Medicare cost, charge ratios for each category, and fiscal year. Costs associated with the intensive glycemic control protocol were determined. Unfortunately, only cost estimates for insulin and associated disposable supplies for each group were available for analysis.
Baseline and treatment populations did not differ significantly regarding demographics such as age, gender, race, admitting diagnosis, diabetes prevalence, or APACHE II scores. There were fewer patients in the treatment group that required mechanical ventilation during their ICU stay (40.6% versus 33.6%). Intensive glucose management was associated with a 13.9% reduction in total ICU days and duration of mechanical ventilation (median of two days decreased to 1.7 days p=0.045). There was a $1,580 adjusted cost savings per patient in the intensive treatment group compared with the baseline group (p<0.001). This reduction in cost was primarily driven by a decrease in laboratory and radiology costs in the ventilated patients. There were nonsignificant cost reductions in the unventilated patients.
Intensive control of hyperglycemia in the hospitalized ICU patient appears to be associated with reduction of morbidity and mortality. This suggests that tight glycemic control also leads to reductions in overall patient care costs—particularly in the ventilated ICU patient. Although not a randomized control trial, database analysis of costs and resource utilization demonstrated an overall cost savings in the treatment group (after initiation of an intensive glycemic control protocol) compared with the baseline group (before protocol initiation). One caveat is that the authors used estimates when determining the costs associated with the implementation of the intensive glucose management protocol. Nevertheless, intensive glycemic control was associated with an overall reduction in patient costs related to decreased ICU days and mechanical ventilation as well as resource utilization in a patient population already shown to have improved mortality. These results, if confirmed, suggest that tight glycemic control in the ICU is cost effective and should become standard medical practice. TH
Repeat Testing for C. Diff?
By Jeff Glasheen, MD
Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006 Apr;119(4):356.e7-356.e8
Clostridium difficile is a common complication of antibiotic and chemotherapeutic use, especially in hospitalized patients. Yet most nosocomial diarrhea is not caused by C. difficile. Most antibiotics can cause loose stools through changes in the gastrointestinal flora that result in inadequate digestion and absorption of carbohydrates and a resultant osmotic diarrhea. Further, antibiotics such as erythromycin and amoxicillin/clavulanate may result in diarrhea via increases in GI tract motility. While osmotic and motility causes of diarrhea tend to improve with antibiotic discontinuation, C. difficile-associated diarrhea is associated with significant morbidity that often continues until adequately treated.
Thus having a test that differentiates between C. difficile and non-clostridial diarrhea is essential. The most commonly used test is the enzyme immunoassay (EIA) that detects toxins A and B. The sensitivity and specificity of this test has been reported to range between 50%-90% and 70%-95%, respectively. The authors of this paper evaluated the utility of repeat EIA testing in patients with a one negative test in the setting of nosocomial diarrhea associated with antibiotic use.
The authors reviewed 474 sequential EIA tests for C. difficile in 396 patients over a 10-month period at a large university-affiliated community hospital with an EIA sensitivity and specificity of 80%-90% and 80%-95%, respectively. Tests were considered to be “repeat” if they occurred within seven days of the original negative test. Of the 78 repeat tests (16.5% of all tests), only one was positive, resulting in a 0.8% conversion rate. At an institutional cost of $128 per test the total cost of EIA testing over the 10-month period was $60,672. The cost of repeat testing alone was $9,984. The authors conclude that there is limited value—and high cost—in repeat EIA testing and that alternative sources of diarrhea should be sought or we should repeat EIA testing in patients with continued nosocomial diarrhea and a negative EIA test.
While prior studies have shown incremental benefit of retesting for C. difficile with the EIA assay, this study’s authors conclude that repeat “C. difficile testing is not clinically justified and is economically wasteful.” Unfortunately, the authors did not utilize a strong enough research design to defend this statement. From the data presented, all we can conclude is that repeat testing with an EIA assay did not add significant value to the diagnostic workup. The lack of a negative gold standard test, such as the cytotoxin assay or follow up outcomes, such as resolution of diarrhea, leaves the reader pondering if the repeat EIA assays were negative because the patients did not have C. difficile or because the test was not sensitive enough to detect the toxin. The reported sensitivity for the EIA assay used was 80-90%, meaning that 10%-20% of patients with C. difficile disease would have had a false negative test. While a second negative test would lower the likelihood of true disease, it would not lower it enough in a patient with a high pre-test probability of disease to sufficiently rule out the disease such that further testing is indicated.
Additionally, while we can extrapolate that the EIA test was of little utility to the patients studied here, no patient-specific data is presented. Thus it is difficult to determine if our patient population is represented in the study. More knowledge about the patients would allow the reader to use published prediction rules to better delineate how likely it was that this cohort was at high risk for having toxin-mediated diarrhea. Perhaps a more reasonable approach to this clinical conundrum would be to send the repeat stool test for a cytotoxin assay or to treat the patient empirically in situations where either the likelihood of disease or the disease burden is high.
Stroke after MI
By Ethan Cumbler, MD
Witt BJ, Ballman KV, Brown RD Jr, et al. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006 Apr;119(4):354.e1-9.
Stroke and myocardial infarction (MI) share many of the risk factors leading to atherosclerosis, including hypertension, hyperlipidemia, diabetes, tobacco abuse, and age. Logically, patients at risk for one event would also be at risk for the other, yet this interaction appears to be more complex. The study by Witt, et al., aims to elucidate the rate of in-hospital stroke in patients initially admitted with an MI.
The authors analyzed 22 observational studies of myocardial infarction that recorded the incidence of cerebrovascular accidents after acute MI. Clinical trials were excluded from the analysis in order to provide representation of an unselected population. Of the trials reviewed, 11 were included in the analysis of in-hospital strokes, three for the 30-day time point, and two for the one-year time point. The other trials used different time points and were not included in the analysis. The patients had a mean age ranging between 59 and 72.7 years, and all had a predominance of males. The rate of in-hospital stroke was 11.1 events per 1,000 hospitalizations. This incidence rose to 12.2/1,000 at 30 days and 21.4/1,000 at one year.
Plausible hypotheses for why the rate of cerebrovascular accident would be particularly high in the post-MI period include the potential for localized wall motion dysmotility or low flow leading to intracardiac thrombosis, event-related arrhythmia, or procedure-related embolic events. The studies from which this meta-analysis was derived were not designed in such a way for a causal relationship to be identified. However, age, diabetes, hypertension, prior stroke, anterior location of MI, atrial fibrillation, heart failure, and nonwhite race were all found to have an association with increased risk for stroke. Interestingly, angina on presentation was associated with an apparent decreased risk, theorized to potentially be due to ischemic preconditioning.
While this study shares the usual limitations of meta-analyses of observational studies, the authors have done an excellent summation of the data available including both English and non-English language articles in the analysis. Notably, the review included studies spanning more than 25 years and, thus, included data from studies done in the era prior to modern therapy for cardiac ischemia including potent antiplatelet and statin therapy. The three studies with in-hospital time points started in the 1990s had a lower average rate of stroke, which may reflect the effect of more potent anti-platelet agents used in today’s therapy for acute coronary syndromes.
The implication for the hospitalist is to recognize that patients admitted for MI are at high risk for stroke during the index hospitalization. A low threshold for suspicion of a cerebrovascular event needs to be maintained for post-MI patients with new neurologic symptoms. Future studies will be needed to address the risk/benefit of anticoagulation in high-risk patients for stroke following a myocardial infarction.
Predicting PE in the ED Using Revised Geneva Score
By Jeffrey Carter, MD
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-171.
Introduction: Pulmonary embolism remains a common life-threatening disorder with imperfect diagnostic modalities and strategies. Much of the current literature focuses on the development and validation of clinical probability assessments that identify low-risk patients who can be safely managed without invasive testing or lung scanning.
Two common scoring systems include the Geneva and Wells criteria, which employ a combination of historical information, clinical and laboratory data to stratify patients into three risk groups.1,2 It has recently been shown that a single negative D-dimer test safely excludes patients with suspected VTE in a large cohort, with a three-month follow-up rate of VTE of 0%.3 Criticism of current clinical probability assessment strategies include the inclusion of subjective criteria or the need for blood gas values.1,2 In this paper, the authors sought to derive and validate a scoring system based on readily available objective clinical data.
Methods: The cohort evaluated in this study consists of the same 965 patients used to prospectively evaluate an emergency department diagnostic strategy of VTE.3 Patients presenting to the emergency ward with complaints of chest pain or shortness of breath were evaluated with a standard diagnostic workup that included a checklist of demographic and historical information, signs and symptoms possibly consistent with VTE, ABG, chest X-ray, and EKG results, as well as the likelihood of another diagnosis. However, the goal was to create a scoring system based on readily available objective data, so ABG, chest X-ray and electrocardiogram results were not evaluated as possible components of the score. Clinical variables associated with pulmonary embolism were evaluated for statistical significance in both a univariate and multivariate model. These variables were then validated both internally and with an external cohort.
Results: The incidence of VTE was 23% (222/965). Ten clinical variables were found to be statistically significantly associated with VTE; these comprise the Revised Geneva Score.
Clinical probability is based on points: 0-3 is low probability; 4-10 is intermediate probability, and >10 is high probability. Low, intermediate, and high clinical probabilities had respective rates of VTE of 8%, 28%, and 74%. These percentages were found in the validation cohort and were similar to those in the derivation cohort.
Discussion: This study focuses on the derivation and validation of a clinical scoring system that can provide a numerical estimate of likelihood of VTE. The diagnostic strategy by which VTE is confirmed or excluded is from derivation cohort and is published elsewhere.3 In that study patients classified as no VTE and not treated had a 90-day risk of VTE of 1%. The nine-point revised Geneva score does indeed provide an accurate assessment of risk of VTE, and can thus help guide clinical decision-making. However it is not clear that the revised Geneva score will help decrease invasive diagnostic tests. In the low-risk group, 8% is too great a risk of a life-threatening illness to forego further diagnostic evaluation. Coupled with a negative ELISA D-dimer, exclusion of these patients is safe, but these patients cannot be safely excluded without risk stratification.3
References
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83:416-420.
- Wicki J, Perneger TV, Junof AF, et al. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 2001 Jan 8;161(1):92-97.
- Perrier A, Roy PM, Aujesky D, et al. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-299.
LMWH for Inpatient Palliative Care
By Jeanie Youngwerth, MD
Noble SI, Nelson A, Turner C, et al. Acceptability of low molecular weight heparin thromboprophylaxis for patients receiving palliative care: qualitative study. BMJ. 2006 Mar 11:332(7541);577-580.ePub 2006 Feb 3.
Venous thromboembolism is a major risk factor for patients with malignancy. VTE may reduce survival time in patients receiving palliative care, with one in seven inpatients with cancer dying from pulmonary embolism. The American College of Chest Physicians recommend low molecular weight heparin (LMWH) in hospitalized patients with cancer as level 1A evidence in their 2004 consensus statement on VTE. There are no thromboprophylaxis guidelines in the United Kingdom. Many physicians view daily injections of LMWH as unnecessary distress for palliative care patients. This study focused on what inpatients with advanced cancer receiving palliative care thought about the effect of thromboprophylaxis on overall quality of life.
This was a qualitative study of 28 inpatients receiving palliative care who had advanced metastatic cancer and who were in a regional cancer center in Wales. The patients had received LMWH for at least five consecutive days. The patients were audiotaped and then had semi-structured interviews transcribed regarding cancer treatments they had received. These interviews covered the patients’ insight into prognosis, their understanding of thromboprophylaxis, their beliefs concerning the effects of thromboprophylaxis on overall quality of life, and the negative aspects of heparin treatment.
The main outcome measures were recurring themes of the effect of thromboprophylaxis on overall quality of life. Major themes identified were insight into prognosis, knowledge and understanding of thromboprophylaxis, acceptability of heparin thromboprophylaxis, reassurance, and optimism. Minor themes identified were bruising, negative impact of antiembolic stockings, and anger at paternalistic views toward terminally ill patients.
Most patients showed clear insight into the nature of their condition and understood heparin prophylaxis for VTE. Many patients identified immobility and surgery as VTE risk factors, with little understanding of cancer as a risk factor. All knew that VTE could cause death, but none were aware of the common symptoms. All patients found LMWH thromboprophylaxis acceptable. Patients believed taking measures to prevent symptoms might improve their quality of life and felt that the medical team had not given up on them.
The only negative experiences of LMWH thromboprophylaxis was bruising. All of the patients who wore antiembolic stockings during previous admissions found them uncomfortable. Patients expressed their need to be involved in decision-making, particularly with respect to withdrawal or non-administration of treatment.
This small, qualitative study showed that, contrary to many physicians’ beliefs, patients in palliative care units believe that LMWH injections are acceptable as thromboprophylaxis, but antiembolic stockings are not. The effect of daily injections had little or no effect on the quality of life, with many patients having positive feelings that things were being done to prevent new problems from occurring.
This study was limited by the small sample size, the qualitative nature that could introduce interpretation bias, and the fact that only patients using LMWH were included. Additionally, the United Kingdom has aggressively educated the public on the risks of VTE associated with long flights such that baseline knowledge may differ in other parts of the world. Resource utilization, including drug costs and length of stay, as well as effect on mortality were not studied.
The implications for hospitalists are that many inpatients with advanced cancer receiving palliative care may find LMWH thromboprophylaxis acceptable therapy, and that discussions with the patient regarding this option should be explored together.
Cost Analysis: Intensive Glycemic Control in Critically Ill Adults
By Whitney Woodmansee, MD
Krinsley JS, Jones, RL. Cost analysis of intensive glycemic control in critically ill adult patients. Chest. 2006;129:644-650.
Several studies have demonstrated improved outcomes and decreased mortality in ICU patients treated with intensive control of blood glucose levels. This study sought to identify the costs associated with intensive glycemic control in the ICU.
An ICU patient database was analyzed for cost data related to intensive glycemic control. A baseline group of 800 consecutive ICU patients admitted prior to initiation (baseline) of an intensive glucose management (blood glucose levels between 80-140 mg/dl protocol were compared with a treatment group of 800 consecutive patients admitted after initiation of the protocol). Previously reported outcomes of these patients demonstrated significant improvement in mortality with tight glycemic control. Costs related to ICU and non-ICU length of stay; duration of mechanical ventilation; and all laboratory, pharmacy, and radiology services were analyzed between groups. Resource utilization was determined by assessing charges from the database and adjusting for inflation and applying Medicare cost, charge ratios for each category, and fiscal year. Costs associated with the intensive glycemic control protocol were determined. Unfortunately, only cost estimates for insulin and associated disposable supplies for each group were available for analysis.
Baseline and treatment populations did not differ significantly regarding demographics such as age, gender, race, admitting diagnosis, diabetes prevalence, or APACHE II scores. There were fewer patients in the treatment group that required mechanical ventilation during their ICU stay (40.6% versus 33.6%). Intensive glucose management was associated with a 13.9% reduction in total ICU days and duration of mechanical ventilation (median of two days decreased to 1.7 days p=0.045). There was a $1,580 adjusted cost savings per patient in the intensive treatment group compared with the baseline group (p<0.001). This reduction in cost was primarily driven by a decrease in laboratory and radiology costs in the ventilated patients. There were nonsignificant cost reductions in the unventilated patients.
Intensive control of hyperglycemia in the hospitalized ICU patient appears to be associated with reduction of morbidity and mortality. This suggests that tight glycemic control also leads to reductions in overall patient care costs—particularly in the ventilated ICU patient. Although not a randomized control trial, database analysis of costs and resource utilization demonstrated an overall cost savings in the treatment group (after initiation of an intensive glycemic control protocol) compared with the baseline group (before protocol initiation). One caveat is that the authors used estimates when determining the costs associated with the implementation of the intensive glucose management protocol. Nevertheless, intensive glycemic control was associated with an overall reduction in patient costs related to decreased ICU days and mechanical ventilation as well as resource utilization in a patient population already shown to have improved mortality. These results, if confirmed, suggest that tight glycemic control in the ICU is cost effective and should become standard medical practice. TH
Repeat Testing for C. Diff?
By Jeff Glasheen, MD
Mohan SS, McDermott BP, Parchuri S, et al. Lack of value of repeat stool testing for Clostridium difficile toxin. Am J Med. 2006 Apr;119(4):356.e7-356.e8
Clostridium difficile is a common complication of antibiotic and chemotherapeutic use, especially in hospitalized patients. Yet most nosocomial diarrhea is not caused by C. difficile. Most antibiotics can cause loose stools through changes in the gastrointestinal flora that result in inadequate digestion and absorption of carbohydrates and a resultant osmotic diarrhea. Further, antibiotics such as erythromycin and amoxicillin/clavulanate may result in diarrhea via increases in GI tract motility. While osmotic and motility causes of diarrhea tend to improve with antibiotic discontinuation, C. difficile-associated diarrhea is associated with significant morbidity that often continues until adequately treated.
Thus having a test that differentiates between C. difficile and non-clostridial diarrhea is essential. The most commonly used test is the enzyme immunoassay (EIA) that detects toxins A and B. The sensitivity and specificity of this test has been reported to range between 50%-90% and 70%-95%, respectively. The authors of this paper evaluated the utility of repeat EIA testing in patients with a one negative test in the setting of nosocomial diarrhea associated with antibiotic use.
The authors reviewed 474 sequential EIA tests for C. difficile in 396 patients over a 10-month period at a large university-affiliated community hospital with an EIA sensitivity and specificity of 80%-90% and 80%-95%, respectively. Tests were considered to be “repeat” if they occurred within seven days of the original negative test. Of the 78 repeat tests (16.5% of all tests), only one was positive, resulting in a 0.8% conversion rate. At an institutional cost of $128 per test the total cost of EIA testing over the 10-month period was $60,672. The cost of repeat testing alone was $9,984. The authors conclude that there is limited value—and high cost—in repeat EIA testing and that alternative sources of diarrhea should be sought or we should repeat EIA testing in patients with continued nosocomial diarrhea and a negative EIA test.
While prior studies have shown incremental benefit of retesting for C. difficile with the EIA assay, this study’s authors conclude that repeat “C. difficile testing is not clinically justified and is economically wasteful.” Unfortunately, the authors did not utilize a strong enough research design to defend this statement. From the data presented, all we can conclude is that repeat testing with an EIA assay did not add significant value to the diagnostic workup. The lack of a negative gold standard test, such as the cytotoxin assay or follow up outcomes, such as resolution of diarrhea, leaves the reader pondering if the repeat EIA assays were negative because the patients did not have C. difficile or because the test was not sensitive enough to detect the toxin. The reported sensitivity for the EIA assay used was 80-90%, meaning that 10%-20% of patients with C. difficile disease would have had a false negative test. While a second negative test would lower the likelihood of true disease, it would not lower it enough in a patient with a high pre-test probability of disease to sufficiently rule out the disease such that further testing is indicated.
Additionally, while we can extrapolate that the EIA test was of little utility to the patients studied here, no patient-specific data is presented. Thus it is difficult to determine if our patient population is represented in the study. More knowledge about the patients would allow the reader to use published prediction rules to better delineate how likely it was that this cohort was at high risk for having toxin-mediated diarrhea. Perhaps a more reasonable approach to this clinical conundrum would be to send the repeat stool test for a cytotoxin assay or to treat the patient empirically in situations where either the likelihood of disease or the disease burden is high.
Stroke after MI
By Ethan Cumbler, MD
Witt BJ, Ballman KV, Brown RD Jr, et al. The incidence of stroke after myocardial infarction: a meta-analysis. Am J Med. 2006 Apr;119(4):354.e1-9.
Stroke and myocardial infarction (MI) share many of the risk factors leading to atherosclerosis, including hypertension, hyperlipidemia, diabetes, tobacco abuse, and age. Logically, patients at risk for one event would also be at risk for the other, yet this interaction appears to be more complex. The study by Witt, et al., aims to elucidate the rate of in-hospital stroke in patients initially admitted with an MI.
The authors analyzed 22 observational studies of myocardial infarction that recorded the incidence of cerebrovascular accidents after acute MI. Clinical trials were excluded from the analysis in order to provide representation of an unselected population. Of the trials reviewed, 11 were included in the analysis of in-hospital strokes, three for the 30-day time point, and two for the one-year time point. The other trials used different time points and were not included in the analysis. The patients had a mean age ranging between 59 and 72.7 years, and all had a predominance of males. The rate of in-hospital stroke was 11.1 events per 1,000 hospitalizations. This incidence rose to 12.2/1,000 at 30 days and 21.4/1,000 at one year.
Plausible hypotheses for why the rate of cerebrovascular accident would be particularly high in the post-MI period include the potential for localized wall motion dysmotility or low flow leading to intracardiac thrombosis, event-related arrhythmia, or procedure-related embolic events. The studies from which this meta-analysis was derived were not designed in such a way for a causal relationship to be identified. However, age, diabetes, hypertension, prior stroke, anterior location of MI, atrial fibrillation, heart failure, and nonwhite race were all found to have an association with increased risk for stroke. Interestingly, angina on presentation was associated with an apparent decreased risk, theorized to potentially be due to ischemic preconditioning.
While this study shares the usual limitations of meta-analyses of observational studies, the authors have done an excellent summation of the data available including both English and non-English language articles in the analysis. Notably, the review included studies spanning more than 25 years and, thus, included data from studies done in the era prior to modern therapy for cardiac ischemia including potent antiplatelet and statin therapy. The three studies with in-hospital time points started in the 1990s had a lower average rate of stroke, which may reflect the effect of more potent anti-platelet agents used in today’s therapy for acute coronary syndromes.
The implication for the hospitalist is to recognize that patients admitted for MI are at high risk for stroke during the index hospitalization. A low threshold for suspicion of a cerebrovascular event needs to be maintained for post-MI patients with new neurologic symptoms. Future studies will be needed to address the risk/benefit of anticoagulation in high-risk patients for stroke following a myocardial infarction.
Predicting PE in the ED Using Revised Geneva Score
By Jeffrey Carter, MD
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-171.
Introduction: Pulmonary embolism remains a common life-threatening disorder with imperfect diagnostic modalities and strategies. Much of the current literature focuses on the development and validation of clinical probability assessments that identify low-risk patients who can be safely managed without invasive testing or lung scanning.
Two common scoring systems include the Geneva and Wells criteria, which employ a combination of historical information, clinical and laboratory data to stratify patients into three risk groups.1,2 It has recently been shown that a single negative D-dimer test safely excludes patients with suspected VTE in a large cohort, with a three-month follow-up rate of VTE of 0%.3 Criticism of current clinical probability assessment strategies include the inclusion of subjective criteria or the need for blood gas values.1,2 In this paper, the authors sought to derive and validate a scoring system based on readily available objective clinical data.
Methods: The cohort evaluated in this study consists of the same 965 patients used to prospectively evaluate an emergency department diagnostic strategy of VTE.3 Patients presenting to the emergency ward with complaints of chest pain or shortness of breath were evaluated with a standard diagnostic workup that included a checklist of demographic and historical information, signs and symptoms possibly consistent with VTE, ABG, chest X-ray, and EKG results, as well as the likelihood of another diagnosis. However, the goal was to create a scoring system based on readily available objective data, so ABG, chest X-ray and electrocardiogram results were not evaluated as possible components of the score. Clinical variables associated with pulmonary embolism were evaluated for statistical significance in both a univariate and multivariate model. These variables were then validated both internally and with an external cohort.
Results: The incidence of VTE was 23% (222/965). Ten clinical variables were found to be statistically significantly associated with VTE; these comprise the Revised Geneva Score.
Clinical probability is based on points: 0-3 is low probability; 4-10 is intermediate probability, and >10 is high probability. Low, intermediate, and high clinical probabilities had respective rates of VTE of 8%, 28%, and 74%. These percentages were found in the validation cohort and were similar to those in the derivation cohort.
Discussion: This study focuses on the derivation and validation of a clinical scoring system that can provide a numerical estimate of likelihood of VTE. The diagnostic strategy by which VTE is confirmed or excluded is from derivation cohort and is published elsewhere.3 In that study patients classified as no VTE and not treated had a 90-day risk of VTE of 1%. The nine-point revised Geneva score does indeed provide an accurate assessment of risk of VTE, and can thus help guide clinical decision-making. However it is not clear that the revised Geneva score will help decrease invasive diagnostic tests. In the low-risk group, 8% is too great a risk of a life-threatening illness to forego further diagnostic evaluation. Coupled with a negative ELISA D-dimer, exclusion of these patients is safe, but these patients cannot be safely excluded without risk stratification.3
References
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83:416-420.
- Wicki J, Perneger TV, Junof AF, et al. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Arch Intern Med. 2001 Jan 8;161(1):92-97.
- Perrier A, Roy PM, Aujesky D, et al. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-299.
LMWH for Inpatient Palliative Care
By Jeanie Youngwerth, MD
Noble SI, Nelson A, Turner C, et al. Acceptability of low molecular weight heparin thromboprophylaxis for patients receiving palliative care: qualitative study. BMJ. 2006 Mar 11:332(7541);577-580.ePub 2006 Feb 3.
Venous thromboembolism is a major risk factor for patients with malignancy. VTE may reduce survival time in patients receiving palliative care, with one in seven inpatients with cancer dying from pulmonary embolism. The American College of Chest Physicians recommend low molecular weight heparin (LMWH) in hospitalized patients with cancer as level 1A evidence in their 2004 consensus statement on VTE. There are no thromboprophylaxis guidelines in the United Kingdom. Many physicians view daily injections of LMWH as unnecessary distress for palliative care patients. This study focused on what inpatients with advanced cancer receiving palliative care thought about the effect of thromboprophylaxis on overall quality of life.
This was a qualitative study of 28 inpatients receiving palliative care who had advanced metastatic cancer and who were in a regional cancer center in Wales. The patients had received LMWH for at least five consecutive days. The patients were audiotaped and then had semi-structured interviews transcribed regarding cancer treatments they had received. These interviews covered the patients’ insight into prognosis, their understanding of thromboprophylaxis, their beliefs concerning the effects of thromboprophylaxis on overall quality of life, and the negative aspects of heparin treatment.
The main outcome measures were recurring themes of the effect of thromboprophylaxis on overall quality of life. Major themes identified were insight into prognosis, knowledge and understanding of thromboprophylaxis, acceptability of heparin thromboprophylaxis, reassurance, and optimism. Minor themes identified were bruising, negative impact of antiembolic stockings, and anger at paternalistic views toward terminally ill patients.
Most patients showed clear insight into the nature of their condition and understood heparin prophylaxis for VTE. Many patients identified immobility and surgery as VTE risk factors, with little understanding of cancer as a risk factor. All knew that VTE could cause death, but none were aware of the common symptoms. All patients found LMWH thromboprophylaxis acceptable. Patients believed taking measures to prevent symptoms might improve their quality of life and felt that the medical team had not given up on them.
The only negative experiences of LMWH thromboprophylaxis was bruising. All of the patients who wore antiembolic stockings during previous admissions found them uncomfortable. Patients expressed their need to be involved in decision-making, particularly with respect to withdrawal or non-administration of treatment.
This small, qualitative study showed that, contrary to many physicians’ beliefs, patients in palliative care units believe that LMWH injections are acceptable as thromboprophylaxis, but antiembolic stockings are not. The effect of daily injections had little or no effect on the quality of life, with many patients having positive feelings that things were being done to prevent new problems from occurring.
This study was limited by the small sample size, the qualitative nature that could introduce interpretation bias, and the fact that only patients using LMWH were included. Additionally, the United Kingdom has aggressively educated the public on the risks of VTE associated with long flights such that baseline knowledge may differ in other parts of the world. Resource utilization, including drug costs and length of stay, as well as effect on mortality were not studied.
The implications for hospitalists are that many inpatients with advanced cancer receiving palliative care may find LMWH thromboprophylaxis acceptable therapy, and that discussions with the patient regarding this option should be explored together.
Cost Analysis: Intensive Glycemic Control in Critically Ill Adults
By Whitney Woodmansee, MD
Krinsley JS, Jones, RL. Cost analysis of intensive glycemic control in critically ill adult patients. Chest. 2006;129:644-650.
Several studies have demonstrated improved outcomes and decreased mortality in ICU patients treated with intensive control of blood glucose levels. This study sought to identify the costs associated with intensive glycemic control in the ICU.
An ICU patient database was analyzed for cost data related to intensive glycemic control. A baseline group of 800 consecutive ICU patients admitted prior to initiation (baseline) of an intensive glucose management (blood glucose levels between 80-140 mg/dl protocol were compared with a treatment group of 800 consecutive patients admitted after initiation of the protocol). Previously reported outcomes of these patients demonstrated significant improvement in mortality with tight glycemic control. Costs related to ICU and non-ICU length of stay; duration of mechanical ventilation; and all laboratory, pharmacy, and radiology services were analyzed between groups. Resource utilization was determined by assessing charges from the database and adjusting for inflation and applying Medicare cost, charge ratios for each category, and fiscal year. Costs associated with the intensive glycemic control protocol were determined. Unfortunately, only cost estimates for insulin and associated disposable supplies for each group were available for analysis.
Baseline and treatment populations did not differ significantly regarding demographics such as age, gender, race, admitting diagnosis, diabetes prevalence, or APACHE II scores. There were fewer patients in the treatment group that required mechanical ventilation during their ICU stay (40.6% versus 33.6%). Intensive glucose management was associated with a 13.9% reduction in total ICU days and duration of mechanical ventilation (median of two days decreased to 1.7 days p=0.045). There was a $1,580 adjusted cost savings per patient in the intensive treatment group compared with the baseline group (p<0.001). This reduction in cost was primarily driven by a decrease in laboratory and radiology costs in the ventilated patients. There were nonsignificant cost reductions in the unventilated patients.
Intensive control of hyperglycemia in the hospitalized ICU patient appears to be associated with reduction of morbidity and mortality. This suggests that tight glycemic control also leads to reductions in overall patient care costs—particularly in the ventilated ICU patient. Although not a randomized control trial, database analysis of costs and resource utilization demonstrated an overall cost savings in the treatment group (after initiation of an intensive glycemic control protocol) compared with the baseline group (before protocol initiation). One caveat is that the authors used estimates when determining the costs associated with the implementation of the intensive glucose management protocol. Nevertheless, intensive glycemic control was associated with an overall reduction in patient costs related to decreased ICU days and mechanical ventilation as well as resource utilization in a patient population already shown to have improved mortality. These results, if confirmed, suggest that tight glycemic control in the ICU is cost effective and should become standard medical practice. TH
Case Managers Offer Options
Jonathan P. Weisul, MD, FACEP, has direct responsibility over both case management and contracted hospitalist services at CHRISTUS St. Frances Cabrini Hospital in Alexandria, La., where he is regional chief medical officer and vice president of medical affairs. To him, the two most important aspects of the relationship between hospitalists and case managers involve communication and respect.
“In our system it’s a very collaborative approach where the case manager presents options to the physician as discharge planning progresses and the physician explains the progression of the patient’s treatment to the case manager,” he says.
In the early days of managed care, Dr. Weisul says, case management received some bad press in that “it was perceived that their interest was [just] getting patients out of the hospital. And I would say that one area where the communication fails is the oftentimes misheld belief on the physician’s part that case managers are trying to practice medicine,” he explains. “Communication usually involves the case manager presenting options to a physician in a way that would be in the best interest of the patient—not trying to usurp any authority from the physician-patient relationship.”
The greatest partnership between hospitalists and case managers occurs when they both share options and needs, and perhaps the best venue for sharing occurs at interdisciplinary meetings. All case managers interviewed for this article stress the importance of daily meetings as a clear advantage for an effective discharge plan.
L. Greg Cunningham, MHA, CEO of the American Case Management Association (ACMA), headquartered in Little Rock, Ark., says the best thing hospitalists and case managers can do to improve their working relationship is “communicate about their patient caseload first thing in the morning.” Both are sharing information. “One is sharing more expectations of what needs to be done for the patient,” he says. “The other is sharing more expectations about what the physician needs to do in terms of decision-making such as getting signatures on forms and communicating with the patient and family.”

Be Proactive
Theresa Brocato, RN, BSN, CPUR, manager of case management and social work at CHRISTUS St. Frances Cabrini Hospital, has been in that position for almost four years. For seven years before that she worked in managed care for Ochsner Health Plan of Louisiana. In her opinion hospitalists can be most helpful to case managers by thinking proactively.
“We have a very proactive discharge planning department,” she says of her department of nine case managers (all nurses) and five social workers who work directly with patients and families, “because as soon as the patient gets to the hospital we start the discharge planning.”
The case managers interview patients and their family and let them know what their estimated time to wellness will be. “We base the estimate on a working DRG [drug-related group],” she says. “We talk to the hospitalist up front, and [we] say, for instance, ‘For this patient, the average time to wellness is about six days, and we need to start preparing for that ultimate discharge. Is there anything you foresee that you might need on discharge, such as equipment or home health?’ And then we start coordinating with the physicians to get the orders in place and get everything set up so that they have a smooth transition at the time of discharge.”
But Dr. Weisul says this kind of communication can be misinterpreted. “Communication seems to fail in the most difficult cases where the physician seems to perceive that the progress of the medical care might not be going on [in] as timely [a manner] as he or she might expect and feels that the case manager, in … looking at when the appropriate discharge time might be, is pressuring the physician,” he says. “But the reverse is true: What they’re doing is just asking for input from the hospitalist [or other] physician as to progress on the path of returning the patient to health and just looking to the future.”
Brocato says the three hospitalists at Cabrini have been easy to work with, sometimes seeking out the case managers and social workers to ask for their help on difficult cases, working with their fellow interdisciplinary-team members to design discharge plans from innovative ideas that solve patient’s challenges, and including the patient in their planning.
Appropriate Levels of Care
At Cabrini Hospital, the case managers and social workers hold daily interdisciplinary discharge planning meetings. Each case is reviewed according to nationally accepted criteria to ensure that the care provided meets standards appropriate for the acute inpatient level of care. Other treatment levels identified during discharge planning include rehabilitation, long-term acute care, and outpatient levels of care.
One recommendation that Brocato would make to hospitalists to better help the work of the case managers, the hospital, and the patients is to recognize earlier which patients will require a longer length of stay (more than three weeks) so that those individuals can be transitioned into a more appropriate level of care.
Some examples of diagnoses in which long-term acute care might be called for, she says, include “osteomyelitis, where a patient will be on a course of antibiotics for six weeks and may require extensive wound therapy. In that case, as soon as we get the results of the bone scan and we see that, we immediately ask the physician to think about moving the patient.”
Other examples include those patients who will need a long time to recover, such as those in the ICU. “Maybe they’ve have been on a ventilator for a long time and they get debilitated,” says Brocato. “Or if they need to be weaned from the ventilator and need some intensive respiratory toilet. The long-term acute care setting is the more appropriate setting to work on trying to rehabilitate the patient.”
Follow-up
Another important element to a good discharge plan is follow-up. Cabrini Hospital has initiated a program whereby a nurse has been hired to call on patients within two days of discharge to check on how things are going. That is, Brocato says, “whether they understood the discharge instructions, to make sure that they got their prescriptions, and [to ensure] they have some kind of follow-up appointment made and are planning to go to that.”
A 2001 study conducted by the section of general internal medicine in the department of medicine at West Virginia University (Morgantown) showed that the effect of employing a nurse discharge planner to work with the hospitalist service had a positive effect on outcomes in an academic teaching hospital.1 When a general medicine service, specialist-staffed service, and a hospitalist service with nurse discharge planner were compared, the hospitalist-discharge planner group was associated with a lower average cost and shorter average length of hospital stay. There was no apparent compromise in clinical outcomes and patient satisfaction with care.
Competent Colleagues
The American Case Management Association (ACMA), begun in 1999, is the first and only nonprofit hospital-based case management organization in the United States. It represents nurses, social workers, physicians, and other professionals who practice hospital case management. The physicians whom ACMA represents are primarily medical directors hired as the catalyst for attendings who are less than cooperative and are impeding discharge (typically not the hospitalists). “The organization is growing at an average annual growth rate of 25%,” says Cunningham. “We’ve just started a new certification process for hospital-based case managers—one for nurses and one for social workers.”
There is a core portion to the exam that tests for knowledge, and a specialty portion of the exam in which “they have to validate those skill sets. The specialty portion of includes a clinical simulation, which is the application of their skills and knowledge,” explains Cunningham. “They have to [show that they can] make not only a decision, but sequential decisions. So we’re testing their ability to take a case and work through it.”
The hospitalist should expect that high level of competency from a case manager, just as the case manager should be able to expect the highest competency of the hospitalist. “The hospitalist should not lessen their expectation of the clinical competency of the case managers,” says Cunningham. “We are advocating that the physicians … increase their expectations of the clinical competency of those individuals.”
Cunningham recommends that hospitalists discuss their case manager’s background if they suspect there is a diminished competency. “Competent case managers “not only make it better for patients,” he says, “but practitioners’ lives are made much easier when competent case managers are hired.”
All the case managers at Cabrini Hospital have a strong clinical background. “It is really important that the case managers are competent in the field they are working in,” says Brocato, “so that the physicians can trust that they understand the clinical side as well as what might be needed at discharge planning. [At Cabrini Hospital] they are placed in the units where they work based on their careers as nurses. The case manager that works in ICU, for instance, was an ICU nurse for many years.”
Brocato believes “hospitalists need to feel confident that the case managers—or discharge planners as they’re called at some hospitals—have a strong clinical background. In that way, when the hospitalists “are discussing their cases, they feel that we know what they’re talking about. For us, it means that we feel we are all on the same page when we’re dealing with the physicians so that we know what the course of treatment will be. Then the case managers are able to make a better discharge plan based on what the expectations of the hospital stay are going to be, so we can plan ahead.”
Dr. Weisul, who oversees three healthcare facilities in the central Louisiana region, knows that the relationship between hospitalists and case managers can be a fruitful one for all concerned. Cabrini has achieved the lowest case mix-adjusted length of stay in its healthcare system. In addition, when physicians were surveyed regarding the discharge planning process provided to their patients, the hospital achieved a combined rate of 97% “satisfied” or “very satisfied.”
“The idea that case management can achieve, with the physician, a low length of stay does not necessarily have to be in an environment of contention,” says Dr. Weisul.
Conclusion
Realize that case managers are there to assist hospitalists meet patients’ care goals. Watch for patients who a need longer length of stay and alert case managers in those cases to ensure moving them to appropriate levels of care, such as long-term acute care setting as soon as possible. Let case managers know how patients and families can reach you post-discharge. Expect the highest standard of competency from case managers and work with hospital administrators and case management to consistently make this a reality. TH
Andrea Sattinger writes regularly for The Hospitalist.
Reference
- Palmer HC Jr, Armistead NS, Elnicki DM, et al. The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital. Am J Med. 2001;111:627-632.
Resources
- Case Management Society of America (CMSA): www.cmsa.org/
- American Case Management Association (ACMA): www.acmaweb.org/
Jonathan P. Weisul, MD, FACEP, has direct responsibility over both case management and contracted hospitalist services at CHRISTUS St. Frances Cabrini Hospital in Alexandria, La., where he is regional chief medical officer and vice president of medical affairs. To him, the two most important aspects of the relationship between hospitalists and case managers involve communication and respect.
“In our system it’s a very collaborative approach where the case manager presents options to the physician as discharge planning progresses and the physician explains the progression of the patient’s treatment to the case manager,” he says.
In the early days of managed care, Dr. Weisul says, case management received some bad press in that “it was perceived that their interest was [just] getting patients out of the hospital. And I would say that one area where the communication fails is the oftentimes misheld belief on the physician’s part that case managers are trying to practice medicine,” he explains. “Communication usually involves the case manager presenting options to a physician in a way that would be in the best interest of the patient—not trying to usurp any authority from the physician-patient relationship.”
The greatest partnership between hospitalists and case managers occurs when they both share options and needs, and perhaps the best venue for sharing occurs at interdisciplinary meetings. All case managers interviewed for this article stress the importance of daily meetings as a clear advantage for an effective discharge plan.
L. Greg Cunningham, MHA, CEO of the American Case Management Association (ACMA), headquartered in Little Rock, Ark., says the best thing hospitalists and case managers can do to improve their working relationship is “communicate about their patient caseload first thing in the morning.” Both are sharing information. “One is sharing more expectations of what needs to be done for the patient,” he says. “The other is sharing more expectations about what the physician needs to do in terms of decision-making such as getting signatures on forms and communicating with the patient and family.”
Be Proactive
Theresa Brocato, RN, BSN, CPUR, manager of case management and social work at CHRISTUS St. Frances Cabrini Hospital, has been in that position for almost four years. For seven years before that she worked in managed care for Ochsner Health Plan of Louisiana. In her opinion hospitalists can be most helpful to case managers by thinking proactively.
“We have a very proactive discharge planning department,” she says of her department of nine case managers (all nurses) and five social workers who work directly with patients and families, “because as soon as the patient gets to the hospital we start the discharge planning.”
The case managers interview patients and their family and let them know what their estimated time to wellness will be. “We base the estimate on a working DRG [drug-related group],” she says. “We talk to the hospitalist up front, and [we] say, for instance, ‘For this patient, the average time to wellness is about six days, and we need to start preparing for that ultimate discharge. Is there anything you foresee that you might need on discharge, such as equipment or home health?’ And then we start coordinating with the physicians to get the orders in place and get everything set up so that they have a smooth transition at the time of discharge.”
But Dr. Weisul says this kind of communication can be misinterpreted. “Communication seems to fail in the most difficult cases where the physician seems to perceive that the progress of the medical care might not be going on [in] as timely [a manner] as he or she might expect and feels that the case manager, in … looking at when the appropriate discharge time might be, is pressuring the physician,” he says. “But the reverse is true: What they’re doing is just asking for input from the hospitalist [or other] physician as to progress on the path of returning the patient to health and just looking to the future.”
Brocato says the three hospitalists at Cabrini have been easy to work with, sometimes seeking out the case managers and social workers to ask for their help on difficult cases, working with their fellow interdisciplinary-team members to design discharge plans from innovative ideas that solve patient’s challenges, and including the patient in their planning.
Appropriate Levels of Care
At Cabrini Hospital, the case managers and social workers hold daily interdisciplinary discharge planning meetings. Each case is reviewed according to nationally accepted criteria to ensure that the care provided meets standards appropriate for the acute inpatient level of care. Other treatment levels identified during discharge planning include rehabilitation, long-term acute care, and outpatient levels of care.
One recommendation that Brocato would make to hospitalists to better help the work of the case managers, the hospital, and the patients is to recognize earlier which patients will require a longer length of stay (more than three weeks) so that those individuals can be transitioned into a more appropriate level of care.
Some examples of diagnoses in which long-term acute care might be called for, she says, include “osteomyelitis, where a patient will be on a course of antibiotics for six weeks and may require extensive wound therapy. In that case, as soon as we get the results of the bone scan and we see that, we immediately ask the physician to think about moving the patient.”
Other examples include those patients who will need a long time to recover, such as those in the ICU. “Maybe they’ve have been on a ventilator for a long time and they get debilitated,” says Brocato. “Or if they need to be weaned from the ventilator and need some intensive respiratory toilet. The long-term acute care setting is the more appropriate setting to work on trying to rehabilitate the patient.”
Follow-up
Another important element to a good discharge plan is follow-up. Cabrini Hospital has initiated a program whereby a nurse has been hired to call on patients within two days of discharge to check on how things are going. That is, Brocato says, “whether they understood the discharge instructions, to make sure that they got their prescriptions, and [to ensure] they have some kind of follow-up appointment made and are planning to go to that.”
A 2001 study conducted by the section of general internal medicine in the department of medicine at West Virginia University (Morgantown) showed that the effect of employing a nurse discharge planner to work with the hospitalist service had a positive effect on outcomes in an academic teaching hospital.1 When a general medicine service, specialist-staffed service, and a hospitalist service with nurse discharge planner were compared, the hospitalist-discharge planner group was associated with a lower average cost and shorter average length of hospital stay. There was no apparent compromise in clinical outcomes and patient satisfaction with care.
Competent Colleagues
The American Case Management Association (ACMA), begun in 1999, is the first and only nonprofit hospital-based case management organization in the United States. It represents nurses, social workers, physicians, and other professionals who practice hospital case management. The physicians whom ACMA represents are primarily medical directors hired as the catalyst for attendings who are less than cooperative and are impeding discharge (typically not the hospitalists). “The organization is growing at an average annual growth rate of 25%,” says Cunningham. “We’ve just started a new certification process for hospital-based case managers—one for nurses and one for social workers.”
There is a core portion to the exam that tests for knowledge, and a specialty portion of the exam in which “they have to validate those skill sets. The specialty portion of includes a clinical simulation, which is the application of their skills and knowledge,” explains Cunningham. “They have to [show that they can] make not only a decision, but sequential decisions. So we’re testing their ability to take a case and work through it.”
The hospitalist should expect that high level of competency from a case manager, just as the case manager should be able to expect the highest competency of the hospitalist. “The hospitalist should not lessen their expectation of the clinical competency of the case managers,” says Cunningham. “We are advocating that the physicians … increase their expectations of the clinical competency of those individuals.”
Cunningham recommends that hospitalists discuss their case manager’s background if they suspect there is a diminished competency. “Competent case managers “not only make it better for patients,” he says, “but practitioners’ lives are made much easier when competent case managers are hired.”
All the case managers at Cabrini Hospital have a strong clinical background. “It is really important that the case managers are competent in the field they are working in,” says Brocato, “so that the physicians can trust that they understand the clinical side as well as what might be needed at discharge planning. [At Cabrini Hospital] they are placed in the units where they work based on their careers as nurses. The case manager that works in ICU, for instance, was an ICU nurse for many years.”
Brocato believes “hospitalists need to feel confident that the case managers—or discharge planners as they’re called at some hospitals—have a strong clinical background. In that way, when the hospitalists “are discussing their cases, they feel that we know what they’re talking about. For us, it means that we feel we are all on the same page when we’re dealing with the physicians so that we know what the course of treatment will be. Then the case managers are able to make a better discharge plan based on what the expectations of the hospital stay are going to be, so we can plan ahead.”
Dr. Weisul, who oversees three healthcare facilities in the central Louisiana region, knows that the relationship between hospitalists and case managers can be a fruitful one for all concerned. Cabrini has achieved the lowest case mix-adjusted length of stay in its healthcare system. In addition, when physicians were surveyed regarding the discharge planning process provided to their patients, the hospital achieved a combined rate of 97% “satisfied” or “very satisfied.”
“The idea that case management can achieve, with the physician, a low length of stay does not necessarily have to be in an environment of contention,” says Dr. Weisul.
Conclusion
Realize that case managers are there to assist hospitalists meet patients’ care goals. Watch for patients who a need longer length of stay and alert case managers in those cases to ensure moving them to appropriate levels of care, such as long-term acute care setting as soon as possible. Let case managers know how patients and families can reach you post-discharge. Expect the highest standard of competency from case managers and work with hospital administrators and case management to consistently make this a reality. TH
Andrea Sattinger writes regularly for The Hospitalist.
Reference
- Palmer HC Jr, Armistead NS, Elnicki DM, et al. The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital. Am J Med. 2001;111:627-632.
Resources
- Case Management Society of America (CMSA): www.cmsa.org/
- American Case Management Association (ACMA): www.acmaweb.org/
Jonathan P. Weisul, MD, FACEP, has direct responsibility over both case management and contracted hospitalist services at CHRISTUS St. Frances Cabrini Hospital in Alexandria, La., where he is regional chief medical officer and vice president of medical affairs. To him, the two most important aspects of the relationship between hospitalists and case managers involve communication and respect.
“In our system it’s a very collaborative approach where the case manager presents options to the physician as discharge planning progresses and the physician explains the progression of the patient’s treatment to the case manager,” he says.
In the early days of managed care, Dr. Weisul says, case management received some bad press in that “it was perceived that their interest was [just] getting patients out of the hospital. And I would say that one area where the communication fails is the oftentimes misheld belief on the physician’s part that case managers are trying to practice medicine,” he explains. “Communication usually involves the case manager presenting options to a physician in a way that would be in the best interest of the patient—not trying to usurp any authority from the physician-patient relationship.”
The greatest partnership between hospitalists and case managers occurs when they both share options and needs, and perhaps the best venue for sharing occurs at interdisciplinary meetings. All case managers interviewed for this article stress the importance of daily meetings as a clear advantage for an effective discharge plan.
L. Greg Cunningham, MHA, CEO of the American Case Management Association (ACMA), headquartered in Little Rock, Ark., says the best thing hospitalists and case managers can do to improve their working relationship is “communicate about their patient caseload first thing in the morning.” Both are sharing information. “One is sharing more expectations of what needs to be done for the patient,” he says. “The other is sharing more expectations about what the physician needs to do in terms of decision-making such as getting signatures on forms and communicating with the patient and family.”
Be Proactive
Theresa Brocato, RN, BSN, CPUR, manager of case management and social work at CHRISTUS St. Frances Cabrini Hospital, has been in that position for almost four years. For seven years before that she worked in managed care for Ochsner Health Plan of Louisiana. In her opinion hospitalists can be most helpful to case managers by thinking proactively.
“We have a very proactive discharge planning department,” she says of her department of nine case managers (all nurses) and five social workers who work directly with patients and families, “because as soon as the patient gets to the hospital we start the discharge planning.”
The case managers interview patients and their family and let them know what their estimated time to wellness will be. “We base the estimate on a working DRG [drug-related group],” she says. “We talk to the hospitalist up front, and [we] say, for instance, ‘For this patient, the average time to wellness is about six days, and we need to start preparing for that ultimate discharge. Is there anything you foresee that you might need on discharge, such as equipment or home health?’ And then we start coordinating with the physicians to get the orders in place and get everything set up so that they have a smooth transition at the time of discharge.”
But Dr. Weisul says this kind of communication can be misinterpreted. “Communication seems to fail in the most difficult cases where the physician seems to perceive that the progress of the medical care might not be going on [in] as timely [a manner] as he or she might expect and feels that the case manager, in … looking at when the appropriate discharge time might be, is pressuring the physician,” he says. “But the reverse is true: What they’re doing is just asking for input from the hospitalist [or other] physician as to progress on the path of returning the patient to health and just looking to the future.”
Brocato says the three hospitalists at Cabrini have been easy to work with, sometimes seeking out the case managers and social workers to ask for their help on difficult cases, working with their fellow interdisciplinary-team members to design discharge plans from innovative ideas that solve patient’s challenges, and including the patient in their planning.
Appropriate Levels of Care
At Cabrini Hospital, the case managers and social workers hold daily interdisciplinary discharge planning meetings. Each case is reviewed according to nationally accepted criteria to ensure that the care provided meets standards appropriate for the acute inpatient level of care. Other treatment levels identified during discharge planning include rehabilitation, long-term acute care, and outpatient levels of care.
One recommendation that Brocato would make to hospitalists to better help the work of the case managers, the hospital, and the patients is to recognize earlier which patients will require a longer length of stay (more than three weeks) so that those individuals can be transitioned into a more appropriate level of care.
Some examples of diagnoses in which long-term acute care might be called for, she says, include “osteomyelitis, where a patient will be on a course of antibiotics for six weeks and may require extensive wound therapy. In that case, as soon as we get the results of the bone scan and we see that, we immediately ask the physician to think about moving the patient.”
Other examples include those patients who will need a long time to recover, such as those in the ICU. “Maybe they’ve have been on a ventilator for a long time and they get debilitated,” says Brocato. “Or if they need to be weaned from the ventilator and need some intensive respiratory toilet. The long-term acute care setting is the more appropriate setting to work on trying to rehabilitate the patient.”
Follow-up
Another important element to a good discharge plan is follow-up. Cabrini Hospital has initiated a program whereby a nurse has been hired to call on patients within two days of discharge to check on how things are going. That is, Brocato says, “whether they understood the discharge instructions, to make sure that they got their prescriptions, and [to ensure] they have some kind of follow-up appointment made and are planning to go to that.”
A 2001 study conducted by the section of general internal medicine in the department of medicine at West Virginia University (Morgantown) showed that the effect of employing a nurse discharge planner to work with the hospitalist service had a positive effect on outcomes in an academic teaching hospital.1 When a general medicine service, specialist-staffed service, and a hospitalist service with nurse discharge planner were compared, the hospitalist-discharge planner group was associated with a lower average cost and shorter average length of hospital stay. There was no apparent compromise in clinical outcomes and patient satisfaction with care.
Competent Colleagues
The American Case Management Association (ACMA), begun in 1999, is the first and only nonprofit hospital-based case management organization in the United States. It represents nurses, social workers, physicians, and other professionals who practice hospital case management. The physicians whom ACMA represents are primarily medical directors hired as the catalyst for attendings who are less than cooperative and are impeding discharge (typically not the hospitalists). “The organization is growing at an average annual growth rate of 25%,” says Cunningham. “We’ve just started a new certification process for hospital-based case managers—one for nurses and one for social workers.”
There is a core portion to the exam that tests for knowledge, and a specialty portion of the exam in which “they have to validate those skill sets. The specialty portion of includes a clinical simulation, which is the application of their skills and knowledge,” explains Cunningham. “They have to [show that they can] make not only a decision, but sequential decisions. So we’re testing their ability to take a case and work through it.”
The hospitalist should expect that high level of competency from a case manager, just as the case manager should be able to expect the highest competency of the hospitalist. “The hospitalist should not lessen their expectation of the clinical competency of the case managers,” says Cunningham. “We are advocating that the physicians … increase their expectations of the clinical competency of those individuals.”
Cunningham recommends that hospitalists discuss their case manager’s background if they suspect there is a diminished competency. “Competent case managers “not only make it better for patients,” he says, “but practitioners’ lives are made much easier when competent case managers are hired.”
All the case managers at Cabrini Hospital have a strong clinical background. “It is really important that the case managers are competent in the field they are working in,” says Brocato, “so that the physicians can trust that they understand the clinical side as well as what might be needed at discharge planning. [At Cabrini Hospital] they are placed in the units where they work based on their careers as nurses. The case manager that works in ICU, for instance, was an ICU nurse for many years.”
Brocato believes “hospitalists need to feel confident that the case managers—or discharge planners as they’re called at some hospitals—have a strong clinical background. In that way, when the hospitalists “are discussing their cases, they feel that we know what they’re talking about. For us, it means that we feel we are all on the same page when we’re dealing with the physicians so that we know what the course of treatment will be. Then the case managers are able to make a better discharge plan based on what the expectations of the hospital stay are going to be, so we can plan ahead.”
Dr. Weisul, who oversees three healthcare facilities in the central Louisiana region, knows that the relationship between hospitalists and case managers can be a fruitful one for all concerned. Cabrini has achieved the lowest case mix-adjusted length of stay in its healthcare system. In addition, when physicians were surveyed regarding the discharge planning process provided to their patients, the hospital achieved a combined rate of 97% “satisfied” or “very satisfied.”
“The idea that case management can achieve, with the physician, a low length of stay does not necessarily have to be in an environment of contention,” says Dr. Weisul.
Conclusion
Realize that case managers are there to assist hospitalists meet patients’ care goals. Watch for patients who a need longer length of stay and alert case managers in those cases to ensure moving them to appropriate levels of care, such as long-term acute care setting as soon as possible. Let case managers know how patients and families can reach you post-discharge. Expect the highest standard of competency from case managers and work with hospital administrators and case management to consistently make this a reality. TH
Andrea Sattinger writes regularly for The Hospitalist.
Reference
- Palmer HC Jr, Armistead NS, Elnicki DM, et al. The effect of a hospitalist service with nurse discharge planner on patient care in an academic teaching hospital. Am J Med. 2001;111:627-632.
Resources
- Case Management Society of America (CMSA): www.cmsa.org/
- American Case Management Association (ACMA): www.acmaweb.org/
Liability, Medical Error Legislation
Liability. To a physician, the word conjures the threat of a malpractice lawsuit and the reality of escalating insurance costs. But some protection may be at hand in the form of several laws recently passed by Congress that aim to relieve both threat and reality.
Hospitalists and Liability
For the time being, the majority of hospitalists are covered by their employer’s liability insurance, according to the cover article in the December 2005 issue of The Hospitalist (“A Malpractice Primer” p. 1). However, that doesn’t mean they’re unaffected by risk of malpractice suits.
—Mary A. Germann, RN, MN, CHE
Mary A. Germann, RN, MN, CHE, certified healthcare compliance officer and founder of Operations Solutions for Healthcare, Inc., a consulting firm based in Atlanta, has answered many liability questions from hospitalists and believes they are at least as worried about the issue as other physicians.
“Hospitalists tend to be concerned about their risk,” she says. “They want to know how to protect themselves. Even though they may not be ‘personally’ at risk, their medical license is still on the line."
Germann explains that hospitalists may in fact be more vulnerable to liability suits than other physicians. “In some ways [hospitalists] are more at risk because they are usually new to their patients,” she says. “They have not had the opportunity to build a relationship with a patient, and must create trust and open communications in a very short time. This weak link can increase a hospitalist’s vulnerability. Lack of information and communication is one of the biggest reasons reported that patients choose to sue.”
With this in mind, let’s take a look at current and pending legislation that will shape liability risk and claims for years to come.
The HEALTH Act of 2005
Passed into law in July of last year, the HEALTH Act (or Help Efficient, Accessible, Low-cost, Timely Healthcare Act), places multiple limits on liability claims. The law caps noneconomic damages in medical malpractice suits at $250,000 for compensating patient injury, limits attorneys’ contingency fees, and requires a finding of malicious intent to support an award of punitive damages. The law also exempts manufacturers and distributors of medical products from punitive damage awards if the U.S. Food and Drug Administration approved the product.
The Patient Safety and Quality Improvement Act of 2005
Also signed into law last July, this act establishes a voluntary, confidential reporting structure for use by physicians, hospitals, and other healthcare professional and entities. This law renders reported medical errors into confidential, privileged data and allows healthcare providers to report their medical errors under a “patient safety activity” umbrella that prohibits the information from being used in a civil action (i.e. liability case). All medical errors reported are covered by the law and not subject to subpoena, Freedom of Information Act request, or use in a disciplinary proceeding.
On reporting medical errors within a hospital system, Germann says, “This is really a joint effort; I don’t think any one entity or organization can do it by themselves. Hospitals have to have a system in place for reporting errors and near misses. Studies have shown that organizations that aggressively support error disclosure have a decreased incidence in the number of suits and a decrease in the compensation payouts.”
The National Medical Error Disclosure and Compensation Act of 2005
Also known as the MEDiC Act, this bill was introduced in the Senate in September 2005 by Senator Hillary Rodham Clinton (D-N.Y.) and Senator Barack Obama (D-Ill.).
Designed to extend the Patient Safety and Quality Improvement Act of 2005 and “promote a culture of safety within hospitals, health systems, clinics, and other sites of healthcare,” this act would establish a federal Office of Patient Safety and Health Care Quality to implement and oversee a new national patient safety database, as well as the MEDiC Program. This program would provide funding to those healthcare providers with systems to disclose medical errors to patients and offer fair compensation to patients if the provider is at fault.
In reducing administrative and legal costs for medical malpractice claims, the MEDiC Act would require participating medical liability insurance companies and healthcare providers to apply a percentage of their savings toward reducing medical errors. The bill also requires that, to the extent possible, some of these cost savings be passed along to providers as lower malpractice insurance premiums.
Although not specifically stated in the bill, a goal of the MEDiC Act is to provide an interim solution to the escalating costs of liability lawsuits.
“I think [medical error reporting] is a very good direction to take,” says Germann. “One of the major barriers to disclosing errors is fear of malpractice suits. To improve quality and decrease medical errors, it’s important for physicians to be able to disclose errors.”
In addition, she stresses that hospitalists and other physicians have little to fear in disclosure. “The majority of errors are not caused by incompetent physicians,” notes Germann. “They are secondary to system failures. Physicians must be able to expose these. And hospitalists see more system errors because they live within the system; they can be a great asset in helping hospital administrators improve quality and systems.”
The MEDiC Act has been under review by the Senate Committee on Health, Education, Labor, and Pensions since September.
So far, 2005 and 2006 have seen big changes in liability reform and in medical error reporting. Together, this legislation—perhaps in conjunction with future laws—will change the risks of liability faced by hospitalists. "No one law is going to solve the entire problem,” says Germann. “All of these together will make the improvements." TH
Jane Jerrard writes “Public Policy” every month for The Hospitalist.
Liability. To a physician, the word conjures the threat of a malpractice lawsuit and the reality of escalating insurance costs. But some protection may be at hand in the form of several laws recently passed by Congress that aim to relieve both threat and reality.
Hospitalists and Liability
For the time being, the majority of hospitalists are covered by their employer’s liability insurance, according to the cover article in the December 2005 issue of The Hospitalist (“A Malpractice Primer” p. 1). However, that doesn’t mean they’re unaffected by risk of malpractice suits.
—Mary A. Germann, RN, MN, CHE
Mary A. Germann, RN, MN, CHE, certified healthcare compliance officer and founder of Operations Solutions for Healthcare, Inc., a consulting firm based in Atlanta, has answered many liability questions from hospitalists and believes they are at least as worried about the issue as other physicians.
“Hospitalists tend to be concerned about their risk,” she says. “They want to know how to protect themselves. Even though they may not be ‘personally’ at risk, their medical license is still on the line."
Germann explains that hospitalists may in fact be more vulnerable to liability suits than other physicians. “In some ways [hospitalists] are more at risk because they are usually new to their patients,” she says. “They have not had the opportunity to build a relationship with a patient, and must create trust and open communications in a very short time. This weak link can increase a hospitalist’s vulnerability. Lack of information and communication is one of the biggest reasons reported that patients choose to sue.”
With this in mind, let’s take a look at current and pending legislation that will shape liability risk and claims for years to come.
The HEALTH Act of 2005
Passed into law in July of last year, the HEALTH Act (or Help Efficient, Accessible, Low-cost, Timely Healthcare Act), places multiple limits on liability claims. The law caps noneconomic damages in medical malpractice suits at $250,000 for compensating patient injury, limits attorneys’ contingency fees, and requires a finding of malicious intent to support an award of punitive damages. The law also exempts manufacturers and distributors of medical products from punitive damage awards if the U.S. Food and Drug Administration approved the product.
The Patient Safety and Quality Improvement Act of 2005
Also signed into law last July, this act establishes a voluntary, confidential reporting structure for use by physicians, hospitals, and other healthcare professional and entities. This law renders reported medical errors into confidential, privileged data and allows healthcare providers to report their medical errors under a “patient safety activity” umbrella that prohibits the information from being used in a civil action (i.e. liability case). All medical errors reported are covered by the law and not subject to subpoena, Freedom of Information Act request, or use in a disciplinary proceeding.
On reporting medical errors within a hospital system, Germann says, “This is really a joint effort; I don’t think any one entity or organization can do it by themselves. Hospitals have to have a system in place for reporting errors and near misses. Studies have shown that organizations that aggressively support error disclosure have a decreased incidence in the number of suits and a decrease in the compensation payouts.”
The National Medical Error Disclosure and Compensation Act of 2005
Also known as the MEDiC Act, this bill was introduced in the Senate in September 2005 by Senator Hillary Rodham Clinton (D-N.Y.) and Senator Barack Obama (D-Ill.).
Designed to extend the Patient Safety and Quality Improvement Act of 2005 and “promote a culture of safety within hospitals, health systems, clinics, and other sites of healthcare,” this act would establish a federal Office of Patient Safety and Health Care Quality to implement and oversee a new national patient safety database, as well as the MEDiC Program. This program would provide funding to those healthcare providers with systems to disclose medical errors to patients and offer fair compensation to patients if the provider is at fault.
In reducing administrative and legal costs for medical malpractice claims, the MEDiC Act would require participating medical liability insurance companies and healthcare providers to apply a percentage of their savings toward reducing medical errors. The bill also requires that, to the extent possible, some of these cost savings be passed along to providers as lower malpractice insurance premiums.
Although not specifically stated in the bill, a goal of the MEDiC Act is to provide an interim solution to the escalating costs of liability lawsuits.
“I think [medical error reporting] is a very good direction to take,” says Germann. “One of the major barriers to disclosing errors is fear of malpractice suits. To improve quality and decrease medical errors, it’s important for physicians to be able to disclose errors.”
In addition, she stresses that hospitalists and other physicians have little to fear in disclosure. “The majority of errors are not caused by incompetent physicians,” notes Germann. “They are secondary to system failures. Physicians must be able to expose these. And hospitalists see more system errors because they live within the system; they can be a great asset in helping hospital administrators improve quality and systems.”
The MEDiC Act has been under review by the Senate Committee on Health, Education, Labor, and Pensions since September.
So far, 2005 and 2006 have seen big changes in liability reform and in medical error reporting. Together, this legislation—perhaps in conjunction with future laws—will change the risks of liability faced by hospitalists. "No one law is going to solve the entire problem,” says Germann. “All of these together will make the improvements." TH
Jane Jerrard writes “Public Policy” every month for The Hospitalist.
Liability. To a physician, the word conjures the threat of a malpractice lawsuit and the reality of escalating insurance costs. But some protection may be at hand in the form of several laws recently passed by Congress that aim to relieve both threat and reality.
Hospitalists and Liability
For the time being, the majority of hospitalists are covered by their employer’s liability insurance, according to the cover article in the December 2005 issue of The Hospitalist (“A Malpractice Primer” p. 1). However, that doesn’t mean they’re unaffected by risk of malpractice suits.
—Mary A. Germann, RN, MN, CHE
Mary A. Germann, RN, MN, CHE, certified healthcare compliance officer and founder of Operations Solutions for Healthcare, Inc., a consulting firm based in Atlanta, has answered many liability questions from hospitalists and believes they are at least as worried about the issue as other physicians.
“Hospitalists tend to be concerned about their risk,” she says. “They want to know how to protect themselves. Even though they may not be ‘personally’ at risk, their medical license is still on the line."
Germann explains that hospitalists may in fact be more vulnerable to liability suits than other physicians. “In some ways [hospitalists] are more at risk because they are usually new to their patients,” she says. “They have not had the opportunity to build a relationship with a patient, and must create trust and open communications in a very short time. This weak link can increase a hospitalist’s vulnerability. Lack of information and communication is one of the biggest reasons reported that patients choose to sue.”
With this in mind, let’s take a look at current and pending legislation that will shape liability risk and claims for years to come.
The HEALTH Act of 2005
Passed into law in July of last year, the HEALTH Act (or Help Efficient, Accessible, Low-cost, Timely Healthcare Act), places multiple limits on liability claims. The law caps noneconomic damages in medical malpractice suits at $250,000 for compensating patient injury, limits attorneys’ contingency fees, and requires a finding of malicious intent to support an award of punitive damages. The law also exempts manufacturers and distributors of medical products from punitive damage awards if the U.S. Food and Drug Administration approved the product.
The Patient Safety and Quality Improvement Act of 2005
Also signed into law last July, this act establishes a voluntary, confidential reporting structure for use by physicians, hospitals, and other healthcare professional and entities. This law renders reported medical errors into confidential, privileged data and allows healthcare providers to report their medical errors under a “patient safety activity” umbrella that prohibits the information from being used in a civil action (i.e. liability case). All medical errors reported are covered by the law and not subject to subpoena, Freedom of Information Act request, or use in a disciplinary proceeding.
On reporting medical errors within a hospital system, Germann says, “This is really a joint effort; I don’t think any one entity or organization can do it by themselves. Hospitals have to have a system in place for reporting errors and near misses. Studies have shown that organizations that aggressively support error disclosure have a decreased incidence in the number of suits and a decrease in the compensation payouts.”
The National Medical Error Disclosure and Compensation Act of 2005
Also known as the MEDiC Act, this bill was introduced in the Senate in September 2005 by Senator Hillary Rodham Clinton (D-N.Y.) and Senator Barack Obama (D-Ill.).
Designed to extend the Patient Safety and Quality Improvement Act of 2005 and “promote a culture of safety within hospitals, health systems, clinics, and other sites of healthcare,” this act would establish a federal Office of Patient Safety and Health Care Quality to implement and oversee a new national patient safety database, as well as the MEDiC Program. This program would provide funding to those healthcare providers with systems to disclose medical errors to patients and offer fair compensation to patients if the provider is at fault.
In reducing administrative and legal costs for medical malpractice claims, the MEDiC Act would require participating medical liability insurance companies and healthcare providers to apply a percentage of their savings toward reducing medical errors. The bill also requires that, to the extent possible, some of these cost savings be passed along to providers as lower malpractice insurance premiums.
Although not specifically stated in the bill, a goal of the MEDiC Act is to provide an interim solution to the escalating costs of liability lawsuits.
“I think [medical error reporting] is a very good direction to take,” says Germann. “One of the major barriers to disclosing errors is fear of malpractice suits. To improve quality and decrease medical errors, it’s important for physicians to be able to disclose errors.”
In addition, she stresses that hospitalists and other physicians have little to fear in disclosure. “The majority of errors are not caused by incompetent physicians,” notes Germann. “They are secondary to system failures. Physicians must be able to expose these. And hospitalists see more system errors because they live within the system; they can be a great asset in helping hospital administrators improve quality and systems.”
The MEDiC Act has been under review by the Senate Committee on Health, Education, Labor, and Pensions since September.
So far, 2005 and 2006 have seen big changes in liability reform and in medical error reporting. Together, this legislation—perhaps in conjunction with future laws—will change the risks of liability faced by hospitalists. "No one law is going to solve the entire problem,” says Germann. “All of these together will make the improvements." TH
Jane Jerrard writes “Public Policy” every month for The Hospitalist.
Urine for a Surprise
A58-year-old white female presented with a two-week history of severe fatigue. She was admitted for acute renal failure (creatinine of 3.0 mg/dL with baseline 0.9 mg/dL two months prior) and anemia (hematocrit of 27.9 with baseline 37.5 two month prior). She had no prior history of renal failure. Her review of systems was otherwise negative. Her urine was orange and dipstick was positive for bilirubin but serum bilirubin was normal. (See photo at right.) Blood smear showed schistocytes and haptoglobin was undetectable. Physical exam showed yellow sclera, but was otherwise normal.

What is the most appropriate treatment for this patient?
- Draw serum complement levels and spin urine for sediment analysis;
- Order a STAT renal ultrasound;
- Ask the patient about over-the-counter medication use;
- Check urine porphyrin levels; or
- Order immediate referral for plasmapheresis.
Discussion
The answer is C: Ask the patient about over-the-counter (OTC) medication use. This patient’s presentation was consistent with overuse of phenazopyridine. Phenazopyridine is an azo dye, which appears to exert a local anesthetic action on urinary tract mucosa. It’s reported adverse reactions include acute renal failure, hemolytic anemia, hepatitis, and methemoglobinemia, which have been reported after acute ingestions, chronic overdoses, and in chronically appropriate doses.1-7 The mechanism of these adverse reactions is not well understood. Although the differential diagnosis for renal failure and hemolytic anemia is extensive, yellow sclera and orange urine in the setting of a normal bilirubin level raised the suspicion of phenazopyridine use in this patient.
This case highlights the common overuse of over the counter medications, as well as global lack of knowledge of their potential adverse reactions. Although phenazopyridine is widely used, 50% of product consumers do not know that it is a urinary tract analgesic, and 80% do not know either the cause of their symptoms or the action of the drug.8
Additionally, although OTC medication use is reported by two-thirds of all hospitalized patients, documentation of them is present in only 10% of admission paperwork.9-10 Given that drug related hospitalizations account for 5%-8% of all hospital stays, it is essential that a complete OTC medication list be included as a routine part of the history obtained from all patients at the time of hospital admission.11-12 With history taking vigilance and patient education, adverse events from OTC medications can be minimized. TH
References
- Gabor EP, Lowenstein L, De Leeuw NK. Hemolytic anemia induced by Phenylazo-Diamino-Pyridine (Pyridium). Can Med Assoc J. 1964 Oct;91:756-759.
- Nathan DM, Siegel AJ, Bunn HF. Acute methemoglobinemia and hemolytic anemia with phenazopyridine: possible relation to acute renal failure. Arch Int Med. 1977 Nov;137(11):1636-1638.
- Gavish D, Knobler H, Gottehrer N, et al. Methemoglobinemia, muscle damage and renal failure complicating phenazopyridine overdose. Isr J Med Sci. 1986 Jan;22(1):45-47.
- Vega J. Acute Renal Failure caused by phenazopyridine. Rev Med Chil. 2003 May;131(5):541-544.
- Kornowski R, Averbuch M, Jaffe A, et al. Sedural toxicity. Harefuah. 1991 Mar 15;120(6):324-325.
- Thomas RJ, Doddabele S, Karnad AB. Chronic severe hemolytic anemia related to surreptitious phenazopyridine abuse. Ann Int Med. 1994;121:308.
- Landman J, Kavaler E, Waterhouse R. Acquired methemoglobinemia possibly related to phenazopyridine in a woman with normal renal function. J Urol. 1997 Oct;158(4):1520-1521.
- Chih-Wen S, Asch SM, Fielder E, et al. Consumer knowledge of over-the-counter phenazopyridine. Ann Fam Med. 2004 May-Jun;2(3):240-244.
- Chrischilles EA, Foley DJ, Wallace RB, et al. Use of medications by persons 65 and over; data from the established populations for epidemiologic studies of the elderly. J Geront. 1992 Sep;47(5):M137-144.
- Simons LA, Tett S, Simons J, et al. Multiple medication use in the elderly. Use of prescription and non-prescription drugs in an Australian community setting. Med J Aust. 1992 Aug 17;157(4):242-246.
- Hallas J, Jensen KB, Grodum E, et al. Drug-related admissions to a department of medical gastroenterology. The role of self-medicated and prescribed drugs. Scand J Gastroenterol. 1991 Feb;26(2):174-180.
- Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ. 2004 Jul;329(7456):15-19.
A58-year-old white female presented with a two-week history of severe fatigue. She was admitted for acute renal failure (creatinine of 3.0 mg/dL with baseline 0.9 mg/dL two months prior) and anemia (hematocrit of 27.9 with baseline 37.5 two month prior). She had no prior history of renal failure. Her review of systems was otherwise negative. Her urine was orange and dipstick was positive for bilirubin but serum bilirubin was normal. (See photo at right.) Blood smear showed schistocytes and haptoglobin was undetectable. Physical exam showed yellow sclera, but was otherwise normal.
What is the most appropriate treatment for this patient?
- Draw serum complement levels and spin urine for sediment analysis;
- Order a STAT renal ultrasound;
- Ask the patient about over-the-counter medication use;
- Check urine porphyrin levels; or
- Order immediate referral for plasmapheresis.
Discussion
The answer is C: Ask the patient about over-the-counter (OTC) medication use. This patient’s presentation was consistent with overuse of phenazopyridine. Phenazopyridine is an azo dye, which appears to exert a local anesthetic action on urinary tract mucosa. It’s reported adverse reactions include acute renal failure, hemolytic anemia, hepatitis, and methemoglobinemia, which have been reported after acute ingestions, chronic overdoses, and in chronically appropriate doses.1-7 The mechanism of these adverse reactions is not well understood. Although the differential diagnosis for renal failure and hemolytic anemia is extensive, yellow sclera and orange urine in the setting of a normal bilirubin level raised the suspicion of phenazopyridine use in this patient.
This case highlights the common overuse of over the counter medications, as well as global lack of knowledge of their potential adverse reactions. Although phenazopyridine is widely used, 50% of product consumers do not know that it is a urinary tract analgesic, and 80% do not know either the cause of their symptoms or the action of the drug.8
Additionally, although OTC medication use is reported by two-thirds of all hospitalized patients, documentation of them is present in only 10% of admission paperwork.9-10 Given that drug related hospitalizations account for 5%-8% of all hospital stays, it is essential that a complete OTC medication list be included as a routine part of the history obtained from all patients at the time of hospital admission.11-12 With history taking vigilance and patient education, adverse events from OTC medications can be minimized. TH
References
- Gabor EP, Lowenstein L, De Leeuw NK. Hemolytic anemia induced by Phenylazo-Diamino-Pyridine (Pyridium). Can Med Assoc J. 1964 Oct;91:756-759.
- Nathan DM, Siegel AJ, Bunn HF. Acute methemoglobinemia and hemolytic anemia with phenazopyridine: possible relation to acute renal failure. Arch Int Med. 1977 Nov;137(11):1636-1638.
- Gavish D, Knobler H, Gottehrer N, et al. Methemoglobinemia, muscle damage and renal failure complicating phenazopyridine overdose. Isr J Med Sci. 1986 Jan;22(1):45-47.
- Vega J. Acute Renal Failure caused by phenazopyridine. Rev Med Chil. 2003 May;131(5):541-544.
- Kornowski R, Averbuch M, Jaffe A, et al. Sedural toxicity. Harefuah. 1991 Mar 15;120(6):324-325.
- Thomas RJ, Doddabele S, Karnad AB. Chronic severe hemolytic anemia related to surreptitious phenazopyridine abuse. Ann Int Med. 1994;121:308.
- Landman J, Kavaler E, Waterhouse R. Acquired methemoglobinemia possibly related to phenazopyridine in a woman with normal renal function. J Urol. 1997 Oct;158(4):1520-1521.
- Chih-Wen S, Asch SM, Fielder E, et al. Consumer knowledge of over-the-counter phenazopyridine. Ann Fam Med. 2004 May-Jun;2(3):240-244.
- Chrischilles EA, Foley DJ, Wallace RB, et al. Use of medications by persons 65 and over; data from the established populations for epidemiologic studies of the elderly. J Geront. 1992 Sep;47(5):M137-144.
- Simons LA, Tett S, Simons J, et al. Multiple medication use in the elderly. Use of prescription and non-prescription drugs in an Australian community setting. Med J Aust. 1992 Aug 17;157(4):242-246.
- Hallas J, Jensen KB, Grodum E, et al. Drug-related admissions to a department of medical gastroenterology. The role of self-medicated and prescribed drugs. Scand J Gastroenterol. 1991 Feb;26(2):174-180.
- Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ. 2004 Jul;329(7456):15-19.
A58-year-old white female presented with a two-week history of severe fatigue. She was admitted for acute renal failure (creatinine of 3.0 mg/dL with baseline 0.9 mg/dL two months prior) and anemia (hematocrit of 27.9 with baseline 37.5 two month prior). She had no prior history of renal failure. Her review of systems was otherwise negative. Her urine was orange and dipstick was positive for bilirubin but serum bilirubin was normal. (See photo at right.) Blood smear showed schistocytes and haptoglobin was undetectable. Physical exam showed yellow sclera, but was otherwise normal.
What is the most appropriate treatment for this patient?
- Draw serum complement levels and spin urine for sediment analysis;
- Order a STAT renal ultrasound;
- Ask the patient about over-the-counter medication use;
- Check urine porphyrin levels; or
- Order immediate referral for plasmapheresis.
Discussion
The answer is C: Ask the patient about over-the-counter (OTC) medication use. This patient’s presentation was consistent with overuse of phenazopyridine. Phenazopyridine is an azo dye, which appears to exert a local anesthetic action on urinary tract mucosa. It’s reported adverse reactions include acute renal failure, hemolytic anemia, hepatitis, and methemoglobinemia, which have been reported after acute ingestions, chronic overdoses, and in chronically appropriate doses.1-7 The mechanism of these adverse reactions is not well understood. Although the differential diagnosis for renal failure and hemolytic anemia is extensive, yellow sclera and orange urine in the setting of a normal bilirubin level raised the suspicion of phenazopyridine use in this patient.
This case highlights the common overuse of over the counter medications, as well as global lack of knowledge of their potential adverse reactions. Although phenazopyridine is widely used, 50% of product consumers do not know that it is a urinary tract analgesic, and 80% do not know either the cause of their symptoms or the action of the drug.8
Additionally, although OTC medication use is reported by two-thirds of all hospitalized patients, documentation of them is present in only 10% of admission paperwork.9-10 Given that drug related hospitalizations account for 5%-8% of all hospital stays, it is essential that a complete OTC medication list be included as a routine part of the history obtained from all patients at the time of hospital admission.11-12 With history taking vigilance and patient education, adverse events from OTC medications can be minimized. TH
References
- Gabor EP, Lowenstein L, De Leeuw NK. Hemolytic anemia induced by Phenylazo-Diamino-Pyridine (Pyridium). Can Med Assoc J. 1964 Oct;91:756-759.
- Nathan DM, Siegel AJ, Bunn HF. Acute methemoglobinemia and hemolytic anemia with phenazopyridine: possible relation to acute renal failure. Arch Int Med. 1977 Nov;137(11):1636-1638.
- Gavish D, Knobler H, Gottehrer N, et al. Methemoglobinemia, muscle damage and renal failure complicating phenazopyridine overdose. Isr J Med Sci. 1986 Jan;22(1):45-47.
- Vega J. Acute Renal Failure caused by phenazopyridine. Rev Med Chil. 2003 May;131(5):541-544.
- Kornowski R, Averbuch M, Jaffe A, et al. Sedural toxicity. Harefuah. 1991 Mar 15;120(6):324-325.
- Thomas RJ, Doddabele S, Karnad AB. Chronic severe hemolytic anemia related to surreptitious phenazopyridine abuse. Ann Int Med. 1994;121:308.
- Landman J, Kavaler E, Waterhouse R. Acquired methemoglobinemia possibly related to phenazopyridine in a woman with normal renal function. J Urol. 1997 Oct;158(4):1520-1521.
- Chih-Wen S, Asch SM, Fielder E, et al. Consumer knowledge of over-the-counter phenazopyridine. Ann Fam Med. 2004 May-Jun;2(3):240-244.
- Chrischilles EA, Foley DJ, Wallace RB, et al. Use of medications by persons 65 and over; data from the established populations for epidemiologic studies of the elderly. J Geront. 1992 Sep;47(5):M137-144.
- Simons LA, Tett S, Simons J, et al. Multiple medication use in the elderly. Use of prescription and non-prescription drugs in an Australian community setting. Med J Aust. 1992 Aug 17;157(4):242-246.
- Hallas J, Jensen KB, Grodum E, et al. Drug-related admissions to a department of medical gastroenterology. The role of self-medicated and prescribed drugs. Scand J Gastroenterol. 1991 Feb;26(2):174-180.
- Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ. 2004 Jul;329(7456):15-19.
Expert Testimony and the Hospitalist
An attorney approaches you about testifying as an expert witness on behalf of a patient against a physician in your area. How do you decide whether to testify?
The decision of whether to testify in a malpractice case is one of the most difficult, yet one of the most important non-patient care decisions a physician can make. Expert testimony is essential to medical malpractice litigation.
The physician expert, however, is often caught in the middle of conflicting tensions. The obligation to promote fairness, justice, and self-regulation of the profession are balanced against the professional and social pressure not to testify against colleagues and not to participate in a legal system that many physicians feel victimizes members of the profession. Nonetheless, the legal system relies on competent medical expertise to be just and fair, and relies on medical professionals to provide that expertise. An individual physician’s decision to participate in a medical malpractice case should be guided by careful consideration of their duties as applied to the specific situation.
What Is Expert Testimony, and Who Is an Expert?
A medical malpractice claim requires that the plaintiff show that the defendant(s) breached a duty to the plaintiff by failing to perform to the standard of care. The central issue in many malpractice cases involves defining the standard of care and determining whether the defendant(s) deviated from it. The only way for a jury to determine what is the standard of care is to listen to the opinions of experts and make a decision based on the persuasiveness and credibility of the experts.
Expert witnesses differ from other witnesses because expert witnesses can offer opinions while other witnesses can only testify to facts or their own personal experience.1 Expert witnesses must have specialized knowledge or experience to be allowed to offer opinion testimony. The U.S. Supreme Court has required that scientific testimony be relevant and reliable, and requires the judge presiding over a case to determine the validity of scientific testimony.2 If the judge decides that scientific testimony to be offered by an expert is not valid or reliable, the judge may refuse to allow it. Thus, the judge determines who may serve as an expert in front of the jury.
Licensed physicians are usually considered experts on the standard of care, regardless of the specialty or area of practice of the testifying expert. Tort reform in many states is focusing on expert testimony, including limiting judicial discretion in qualifying experts. For example, in Pennsylvania, only an expert in the field of the defendant may give expert testimony against him or her.
Given that most physicians are allowed by most judges to testify as to the standard of care, an expert may be testifying outside their scope of practice or the area in which they have actual specialized knowledge and experience. Further, once an expert is allowed to testify, there are no consequences for offering opinions that are unsupported by evidence or patently inaccurate. These are the areas where professional integrity is crucial, and professional societies can play a role in regulation and oversight of physicians serving as experts.3
Self-Regulation of Expert Witnesses
What do individuals and professional societies need to contribute to oversight of expert testimony? A physician’s obligation to participate in malpractice cases arises from the privilege of self-regulation enjoyed by the medical profession. As a result of the degree of specialized knowledge and skill needed to practice medicine, physicians have a duty to take action against other physicians who are impaired or incompetent.3 Professional societies promote the highest ethical and professional standards for members and therefore have a responsibility to discipline members who are irresponsible or unqualified in their expert legal involvement.
Physicians also have a duty to patients to provide expert testimony. In the event of harm caused by negligence, patients are denied any compensation at all if responsible physicians are unwilling to become involved as plaintiff’s experts. Physicians must uphold the duty to act in the best interest of patients and society and to promote justice in the system by rendering fair and honest opinions—even if that results in liability for a fellow physicians and despite the current atmosphere of negativity toward physicians testifying against other physicians.3
Based on these ethical principles, physicians have a duty to provide accurate and responsible expert testimony. Inaccurate expert testimony is damaging to the system in many ways: It increases malpractice costs, injures the reputation of individual practitioners, and adversely affects the standard of care by promoting false standards. Distinguishing irresponsible testimony from reasonable differences of opinion may be challenging. Any valid lawsuit will involve conflicting opinions as to whether the standard of care was met—otherwise there would be no need for expert testimony. To protect against overreaching, physicians should limit themselves to areas of their own academic and experiential expertise, and should limit their testimony to their scope of training or practice. Their opinions should be consistent with prevailing literature and good clinical practice. Offering an unusual opinion that contradicts the literature may be appropriate if the expert has good reason to believe the atypical opinion is correct and can provide evidence to support the claim.
Applying these principles to the practice of hospitalists requires special considerations. Hospital medicine is not a discrete specialty in the sense of having a certifying board or mandatory focused training requirements; however, hospitalists practice in a particular environment and should limit their expert testimony to that environment. Hospitalists have diverse practices and some practice outpatient medicine or primary care as well. Thus, it is particularly important for hospitalists to demonstrate responsibility and integrity in limiting their testimony to areas where they have genuine specialized knowledge and experience. Other physicians, attorneys, and judges must rely on hospitalists to enforce standards themselves because no single standard can be applied to all hospitalists.
As a further consideration in the interests of justice and professionalism, physicians should recuse themselves from any case with an actual or perceived conflict of interest. Prominent physicians, including public figures and society leaders, have the same duty regarding self-regulation in the profession and promotion of justice in the system as any other physician. Any reason to be personally predisposed to one side of the case or the other as a result of personal involvement or professional interests may make the physician an inappropriate expert. Unless testifying on behalf of the position of a society, a physician should not use society membership as direct evidence of expertise. Society leaders should be cautious about the appearance of conflict of interest, specifically that their status in the society confers special expert qualifications.
Professional societies have a special role in ensuring quality healthcare and a special role in the trust of society. Many societies, including the American Medical Association and the American Academy of Pediatrics have created guidelines for expert witnesses, and the AMA has further discussed the need for a more active role in expert oversight by professional societies.3 Societies need to establish standards for members who act as experts and create enforcement mechanisms for those standards. Further, societies should decide whether they intend to undertake formal disciplinary actions against physicians acting improperly by making the state disciplinary boards aware of their findings of improper conduct. Such standards and policies must be explicit, documented, and published. This is an expanded role for professional societies in the arena of explicit regulation and discipline of members, but there has been increasing recognition that professional societies are an ideal forum for increasing regulation and standards for expert testimony.4-5
The Verdict
The decision to participate in a medical malpractice case as an expert witness requires competence, accurate self-assessment, and integrity. A physician should testify only to what he or she genuinely believes to be the standard of care, regardless of which side approaches him or her. The physician should consider his or her current practice and expertise to decide if he or she can provide honest and accurate expert testimony.
He or she should keep in mind the interests of patients in having access to the courts and to fair compensation from injuries, and therefore physicians should have the courage and integrity to testify against colleagues when he or she genuinely believes that the colleague injured the plaintiff through a deviation from the standard of care. Society relies upon physicians to risk disfavor with colleagues in the interest of promoting justice and protecting patients when the physician believes that is the right thing to do. Physicians interested in policy issues around expert testimony should become involved in their professional societies to create and enforce quality standards for expert witnesses.
References
- Federal Rules of Evidence 701, 702, 703.
- Daubert v. Merrell Dow, 509 U.S. 579; 113 S. Ct. 2786; 125 L. Ed. 2d 469 (1993).
- American Medical Association Code of Medical Ethics, Discipline in Medicine, E-9.04 Available at www.ama-assn.org. Last accessed May 25, 2006.
- Feld AD, Carey WD. Expert witness malfeasance: how should specialty societies respond? Am J Gastroenterol. 2005 May;100(5):991-995.
- Gomez JCB. Silencing the hired guns: ensuring honesty in medical testimony. J Leg Med. 2005 Sep;26(3):385-399.
SHM: BEHIND THE SCENES
SHM Online
By Scott Johnson

Last month, my next door neighbor at the office and SHM’s director of membership, Todd Von Deak, wrote a new column meant to share with you a “behind the scenes” look at SHM. I am pleased to carry the torch in this issue of The Hospitalist and give you a sneak peek at what’s next for SHM’s Web and IT initiatives.
First, let’s step back and look at some changes we’ve recently implemented and how each should benefit your membership.
Our database is key in our efforts to keep you up to date on not only the latest news from SHM, but also from the hospital medicine community at large. Over the past couple of months, we have completed a major review of our data-gathering processes and made changes to how we store your information. These changes will not only better protect your privacy, which is a major concern of ours, but also better enable us to reach you at your preferred address—whether at home or work.
Part of great customer service is listening. Many members have shared that they find it cumbersome to have to remember their member number in order to log onto SHM’s Web site. We’re pleased to announce that you can now access the SHM Web site with your own personalized username and password.
To create your own login and password, just visit www.hospitalmedicine.org/activate. Once online, you will be asked to enter your member number and last name, and then asked to choose a new username and password.
In addition to allowing you to create your own username and password, we’ve also streamlined the process to renew your membership or join online. Check it out when you get a chance. I’d love to hear your feedback.
Now that we have had our flashback, let’s discuss what we’ve got planned for the future. Since launching the new Career Center (www.hospitalmedicine.org/careercenter) we have begun working on projects to create a more personal experience for you as you visit the SHM Web site and receive our monthly e-mail newsletter.
The SHM Store, which launched in June, features a variety of SHM products and resources. Key educational products such as the results from our “Survey on the State of the Hospital Medicine Movement” will be available, as will favorites like SHM hats and golf shirts (both men’s and women’s).
The next evolution of SHM’s eNewsletter, our monthly e-mail newsletter, will occur this fall. In addition to a new look and feel, the eNewsletter will contain information unique for members and non-members and will be personalized to your areas of interest.
We are also creating a personally tailored Web site where you can create your own “My SHM” page. Once live, this new benefit will enable you to select topics of interest and have related articles, stories, and links automatically appear on your own “My SHM” page.
Having worked with healthcare associations for almost seven years I recognize how important your time is and the value of having the best and most current information at your fingertips. Our goal is to not only create a place where you can find the information you need to excel in your field, but to find ways in which you can “pull” the information relevant to you to your inbox, PDA, or iPod.
For the moment, we are focused on improving and enhancing the current tools in SHM’s tool belt. But on the not-too-distant horizon you’ll be hearing more about our plans to use new tools, such as PDAs and iPods, to provide you with even more information and resources. We’re confident that these resources will help you enhance the quality of care you provide to your patients and their families.
Steve Jobs, CEO of Apple Computer, once said, “The journey is the reward.” In the time I have spent with SHM it has already been quite a rewarding journey and I am excited about the landscape that lies before us.
Next month, you’ll hear from Geri Barnes, our director of education and quality initiatives. Geri is leading the charge to keep our education program in its current position as the most informative and innovative set of offerings within our specialty.
If you ever have any questions about our Web-based offerings, or feedback on how we can improve existing products and programs, please e-mail me at sjohnson@hospitalmedicine.org.
Johnson is SHM’s director of information services.
New Leadership AcademyOffering to Debut in Nashville
Level II track created in response to demand

SHM is pleased to announce the expansion of its cutting edge leadership program, with the debut of a Level II track as part of the Leadership Academy Sept. 11-14 in Nashville, Tenn.
Over the course of four days, the Leadership Academy will provide hospitalist leaders with the skills and resources required to successfully lead and manage a hospital medicine program now and in the future.
Topics that will be addressed include:
- Leadership challenges in hospital medicine;
- Finance and the hospitalist;
- Leading recruitment, retention, and staff development; and
- Leading and managing change.
This course was created in response to feedback from previous Leadership Academy attendees and is designed to give them the opportunity to build on the time they’ve spent back at the hospital since attending a Leadership Academy. Level II offers an in-depth look at how to finance a hospital, insight on how to lead recruitment, retention, and staff development. It also presents advanced skills in negotiation.
Because Level II is considered an advanced course, attendees must have participated in a previous leadership academy or have completed an MBA program to be accepted.
As with any SHM educational event, ample time will be set aside for interaction with faculty and participants so you can get answers to your pressing questions and make connections for the future.
“The fact that learning takes place both inside and outside of the classroom is one of the things that makes SHM’s Leadership Academies so powerful,” says Larry Wellikson, CEO of SHM.
According to Scott Enderby, a Leadership Academy graduate, “This is the only medical conference I’ve ever gone to where I went to every meeting and still wanted more.”
The September venue—the Gaylord Nashville Resort & Convention Center in Nashville—offers ample opportunity to relax in the midst of your intense learning experience. From tours aboard the hotel’s Delta Flatboats to the chance to play 18 holes at the Grand Ole Opry Course, there is something for everyone, including your family.
To register for the September Leadership Academy, visit www.hospitalmedicine.org or call (800) 843-3360.
Can’t join us in Nashville? Mark your calendars for our winter Leadership Academy, Feb. 26-March 1, 2007, in Orlando, Fla. TH
An attorney approaches you about testifying as an expert witness on behalf of a patient against a physician in your area. How do you decide whether to testify?
The decision of whether to testify in a malpractice case is one of the most difficult, yet one of the most important non-patient care decisions a physician can make. Expert testimony is essential to medical malpractice litigation.
The physician expert, however, is often caught in the middle of conflicting tensions. The obligation to promote fairness, justice, and self-regulation of the profession are balanced against the professional and social pressure not to testify against colleagues and not to participate in a legal system that many physicians feel victimizes members of the profession. Nonetheless, the legal system relies on competent medical expertise to be just and fair, and relies on medical professionals to provide that expertise. An individual physician’s decision to participate in a medical malpractice case should be guided by careful consideration of their duties as applied to the specific situation.
What Is Expert Testimony, and Who Is an Expert?
A medical malpractice claim requires that the plaintiff show that the defendant(s) breached a duty to the plaintiff by failing to perform to the standard of care. The central issue in many malpractice cases involves defining the standard of care and determining whether the defendant(s) deviated from it. The only way for a jury to determine what is the standard of care is to listen to the opinions of experts and make a decision based on the persuasiveness and credibility of the experts.
Expert witnesses differ from other witnesses because expert witnesses can offer opinions while other witnesses can only testify to facts or their own personal experience.1 Expert witnesses must have specialized knowledge or experience to be allowed to offer opinion testimony. The U.S. Supreme Court has required that scientific testimony be relevant and reliable, and requires the judge presiding over a case to determine the validity of scientific testimony.2 If the judge decides that scientific testimony to be offered by an expert is not valid or reliable, the judge may refuse to allow it. Thus, the judge determines who may serve as an expert in front of the jury.
Licensed physicians are usually considered experts on the standard of care, regardless of the specialty or area of practice of the testifying expert. Tort reform in many states is focusing on expert testimony, including limiting judicial discretion in qualifying experts. For example, in Pennsylvania, only an expert in the field of the defendant may give expert testimony against him or her.
Given that most physicians are allowed by most judges to testify as to the standard of care, an expert may be testifying outside their scope of practice or the area in which they have actual specialized knowledge and experience. Further, once an expert is allowed to testify, there are no consequences for offering opinions that are unsupported by evidence or patently inaccurate. These are the areas where professional integrity is crucial, and professional societies can play a role in regulation and oversight of physicians serving as experts.3
Self-Regulation of Expert Witnesses
What do individuals and professional societies need to contribute to oversight of expert testimony? A physician’s obligation to participate in malpractice cases arises from the privilege of self-regulation enjoyed by the medical profession. As a result of the degree of specialized knowledge and skill needed to practice medicine, physicians have a duty to take action against other physicians who are impaired or incompetent.3 Professional societies promote the highest ethical and professional standards for members and therefore have a responsibility to discipline members who are irresponsible or unqualified in their expert legal involvement.
Physicians also have a duty to patients to provide expert testimony. In the event of harm caused by negligence, patients are denied any compensation at all if responsible physicians are unwilling to become involved as plaintiff’s experts. Physicians must uphold the duty to act in the best interest of patients and society and to promote justice in the system by rendering fair and honest opinions—even if that results in liability for a fellow physicians and despite the current atmosphere of negativity toward physicians testifying against other physicians.3
Based on these ethical principles, physicians have a duty to provide accurate and responsible expert testimony. Inaccurate expert testimony is damaging to the system in many ways: It increases malpractice costs, injures the reputation of individual practitioners, and adversely affects the standard of care by promoting false standards. Distinguishing irresponsible testimony from reasonable differences of opinion may be challenging. Any valid lawsuit will involve conflicting opinions as to whether the standard of care was met—otherwise there would be no need for expert testimony. To protect against overreaching, physicians should limit themselves to areas of their own academic and experiential expertise, and should limit their testimony to their scope of training or practice. Their opinions should be consistent with prevailing literature and good clinical practice. Offering an unusual opinion that contradicts the literature may be appropriate if the expert has good reason to believe the atypical opinion is correct and can provide evidence to support the claim.
Applying these principles to the practice of hospitalists requires special considerations. Hospital medicine is not a discrete specialty in the sense of having a certifying board or mandatory focused training requirements; however, hospitalists practice in a particular environment and should limit their expert testimony to that environment. Hospitalists have diverse practices and some practice outpatient medicine or primary care as well. Thus, it is particularly important for hospitalists to demonstrate responsibility and integrity in limiting their testimony to areas where they have genuine specialized knowledge and experience. Other physicians, attorneys, and judges must rely on hospitalists to enforce standards themselves because no single standard can be applied to all hospitalists.
As a further consideration in the interests of justice and professionalism, physicians should recuse themselves from any case with an actual or perceived conflict of interest. Prominent physicians, including public figures and society leaders, have the same duty regarding self-regulation in the profession and promotion of justice in the system as any other physician. Any reason to be personally predisposed to one side of the case or the other as a result of personal involvement or professional interests may make the physician an inappropriate expert. Unless testifying on behalf of the position of a society, a physician should not use society membership as direct evidence of expertise. Society leaders should be cautious about the appearance of conflict of interest, specifically that their status in the society confers special expert qualifications.
Professional societies have a special role in ensuring quality healthcare and a special role in the trust of society. Many societies, including the American Medical Association and the American Academy of Pediatrics have created guidelines for expert witnesses, and the AMA has further discussed the need for a more active role in expert oversight by professional societies.3 Societies need to establish standards for members who act as experts and create enforcement mechanisms for those standards. Further, societies should decide whether they intend to undertake formal disciplinary actions against physicians acting improperly by making the state disciplinary boards aware of their findings of improper conduct. Such standards and policies must be explicit, documented, and published. This is an expanded role for professional societies in the arena of explicit regulation and discipline of members, but there has been increasing recognition that professional societies are an ideal forum for increasing regulation and standards for expert testimony.4-5
The Verdict
The decision to participate in a medical malpractice case as an expert witness requires competence, accurate self-assessment, and integrity. A physician should testify only to what he or she genuinely believes to be the standard of care, regardless of which side approaches him or her. The physician should consider his or her current practice and expertise to decide if he or she can provide honest and accurate expert testimony.
He or she should keep in mind the interests of patients in having access to the courts and to fair compensation from injuries, and therefore physicians should have the courage and integrity to testify against colleagues when he or she genuinely believes that the colleague injured the plaintiff through a deviation from the standard of care. Society relies upon physicians to risk disfavor with colleagues in the interest of promoting justice and protecting patients when the physician believes that is the right thing to do. Physicians interested in policy issues around expert testimony should become involved in their professional societies to create and enforce quality standards for expert witnesses.
References
- Federal Rules of Evidence 701, 702, 703.
- Daubert v. Merrell Dow, 509 U.S. 579; 113 S. Ct. 2786; 125 L. Ed. 2d 469 (1993).
- American Medical Association Code of Medical Ethics, Discipline in Medicine, E-9.04 Available at www.ama-assn.org. Last accessed May 25, 2006.
- Feld AD, Carey WD. Expert witness malfeasance: how should specialty societies respond? Am J Gastroenterol. 2005 May;100(5):991-995.
- Gomez JCB. Silencing the hired guns: ensuring honesty in medical testimony. J Leg Med. 2005 Sep;26(3):385-399.
SHM: BEHIND THE SCENES
SHM Online
By Scott Johnson
Last month, my next door neighbor at the office and SHM’s director of membership, Todd Von Deak, wrote a new column meant to share with you a “behind the scenes” look at SHM. I am pleased to carry the torch in this issue of The Hospitalist and give you a sneak peek at what’s next for SHM’s Web and IT initiatives.
First, let’s step back and look at some changes we’ve recently implemented and how each should benefit your membership.
Our database is key in our efforts to keep you up to date on not only the latest news from SHM, but also from the hospital medicine community at large. Over the past couple of months, we have completed a major review of our data-gathering processes and made changes to how we store your information. These changes will not only better protect your privacy, which is a major concern of ours, but also better enable us to reach you at your preferred address—whether at home or work.
Part of great customer service is listening. Many members have shared that they find it cumbersome to have to remember their member number in order to log onto SHM’s Web site. We’re pleased to announce that you can now access the SHM Web site with your own personalized username and password.
To create your own login and password, just visit www.hospitalmedicine.org/activate. Once online, you will be asked to enter your member number and last name, and then asked to choose a new username and password.
In addition to allowing you to create your own username and password, we’ve also streamlined the process to renew your membership or join online. Check it out when you get a chance. I’d love to hear your feedback.
Now that we have had our flashback, let’s discuss what we’ve got planned for the future. Since launching the new Career Center (www.hospitalmedicine.org/careercenter) we have begun working on projects to create a more personal experience for you as you visit the SHM Web site and receive our monthly e-mail newsletter.
The SHM Store, which launched in June, features a variety of SHM products and resources. Key educational products such as the results from our “Survey on the State of the Hospital Medicine Movement” will be available, as will favorites like SHM hats and golf shirts (both men’s and women’s).
The next evolution of SHM’s eNewsletter, our monthly e-mail newsletter, will occur this fall. In addition to a new look and feel, the eNewsletter will contain information unique for members and non-members and will be personalized to your areas of interest.
We are also creating a personally tailored Web site where you can create your own “My SHM” page. Once live, this new benefit will enable you to select topics of interest and have related articles, stories, and links automatically appear on your own “My SHM” page.
Having worked with healthcare associations for almost seven years I recognize how important your time is and the value of having the best and most current information at your fingertips. Our goal is to not only create a place where you can find the information you need to excel in your field, but to find ways in which you can “pull” the information relevant to you to your inbox, PDA, or iPod.
For the moment, we are focused on improving and enhancing the current tools in SHM’s tool belt. But on the not-too-distant horizon you’ll be hearing more about our plans to use new tools, such as PDAs and iPods, to provide you with even more information and resources. We’re confident that these resources will help you enhance the quality of care you provide to your patients and their families.
Steve Jobs, CEO of Apple Computer, once said, “The journey is the reward.” In the time I have spent with SHM it has already been quite a rewarding journey and I am excited about the landscape that lies before us.
Next month, you’ll hear from Geri Barnes, our director of education and quality initiatives. Geri is leading the charge to keep our education program in its current position as the most informative and innovative set of offerings within our specialty.
If you ever have any questions about our Web-based offerings, or feedback on how we can improve existing products and programs, please e-mail me at sjohnson@hospitalmedicine.org.
Johnson is SHM’s director of information services.
New Leadership AcademyOffering to Debut in Nashville
Level II track created in response to demand
SHM is pleased to announce the expansion of its cutting edge leadership program, with the debut of a Level II track as part of the Leadership Academy Sept. 11-14 in Nashville, Tenn.
Over the course of four days, the Leadership Academy will provide hospitalist leaders with the skills and resources required to successfully lead and manage a hospital medicine program now and in the future.
Topics that will be addressed include:
- Leadership challenges in hospital medicine;
- Finance and the hospitalist;
- Leading recruitment, retention, and staff development; and
- Leading and managing change.
This course was created in response to feedback from previous Leadership Academy attendees and is designed to give them the opportunity to build on the time they’ve spent back at the hospital since attending a Leadership Academy. Level II offers an in-depth look at how to finance a hospital, insight on how to lead recruitment, retention, and staff development. It also presents advanced skills in negotiation.
Because Level II is considered an advanced course, attendees must have participated in a previous leadership academy or have completed an MBA program to be accepted.
As with any SHM educational event, ample time will be set aside for interaction with faculty and participants so you can get answers to your pressing questions and make connections for the future.
“The fact that learning takes place both inside and outside of the classroom is one of the things that makes SHM’s Leadership Academies so powerful,” says Larry Wellikson, CEO of SHM.
According to Scott Enderby, a Leadership Academy graduate, “This is the only medical conference I’ve ever gone to where I went to every meeting and still wanted more.”
The September venue—the Gaylord Nashville Resort & Convention Center in Nashville—offers ample opportunity to relax in the midst of your intense learning experience. From tours aboard the hotel’s Delta Flatboats to the chance to play 18 holes at the Grand Ole Opry Course, there is something for everyone, including your family.
To register for the September Leadership Academy, visit www.hospitalmedicine.org or call (800) 843-3360.
Can’t join us in Nashville? Mark your calendars for our winter Leadership Academy, Feb. 26-March 1, 2007, in Orlando, Fla. TH
An attorney approaches you about testifying as an expert witness on behalf of a patient against a physician in your area. How do you decide whether to testify?
The decision of whether to testify in a malpractice case is one of the most difficult, yet one of the most important non-patient care decisions a physician can make. Expert testimony is essential to medical malpractice litigation.
The physician expert, however, is often caught in the middle of conflicting tensions. The obligation to promote fairness, justice, and self-regulation of the profession are balanced against the professional and social pressure not to testify against colleagues and not to participate in a legal system that many physicians feel victimizes members of the profession. Nonetheless, the legal system relies on competent medical expertise to be just and fair, and relies on medical professionals to provide that expertise. An individual physician’s decision to participate in a medical malpractice case should be guided by careful consideration of their duties as applied to the specific situation.
What Is Expert Testimony, and Who Is an Expert?
A medical malpractice claim requires that the plaintiff show that the defendant(s) breached a duty to the plaintiff by failing to perform to the standard of care. The central issue in many malpractice cases involves defining the standard of care and determining whether the defendant(s) deviated from it. The only way for a jury to determine what is the standard of care is to listen to the opinions of experts and make a decision based on the persuasiveness and credibility of the experts.
Expert witnesses differ from other witnesses because expert witnesses can offer opinions while other witnesses can only testify to facts or their own personal experience.1 Expert witnesses must have specialized knowledge or experience to be allowed to offer opinion testimony. The U.S. Supreme Court has required that scientific testimony be relevant and reliable, and requires the judge presiding over a case to determine the validity of scientific testimony.2 If the judge decides that scientific testimony to be offered by an expert is not valid or reliable, the judge may refuse to allow it. Thus, the judge determines who may serve as an expert in front of the jury.
Licensed physicians are usually considered experts on the standard of care, regardless of the specialty or area of practice of the testifying expert. Tort reform in many states is focusing on expert testimony, including limiting judicial discretion in qualifying experts. For example, in Pennsylvania, only an expert in the field of the defendant may give expert testimony against him or her.
Given that most physicians are allowed by most judges to testify as to the standard of care, an expert may be testifying outside their scope of practice or the area in which they have actual specialized knowledge and experience. Further, once an expert is allowed to testify, there are no consequences for offering opinions that are unsupported by evidence or patently inaccurate. These are the areas where professional integrity is crucial, and professional societies can play a role in regulation and oversight of physicians serving as experts.3
Self-Regulation of Expert Witnesses
What do individuals and professional societies need to contribute to oversight of expert testimony? A physician’s obligation to participate in malpractice cases arises from the privilege of self-regulation enjoyed by the medical profession. As a result of the degree of specialized knowledge and skill needed to practice medicine, physicians have a duty to take action against other physicians who are impaired or incompetent.3 Professional societies promote the highest ethical and professional standards for members and therefore have a responsibility to discipline members who are irresponsible or unqualified in their expert legal involvement.
Physicians also have a duty to patients to provide expert testimony. In the event of harm caused by negligence, patients are denied any compensation at all if responsible physicians are unwilling to become involved as plaintiff’s experts. Physicians must uphold the duty to act in the best interest of patients and society and to promote justice in the system by rendering fair and honest opinions—even if that results in liability for a fellow physicians and despite the current atmosphere of negativity toward physicians testifying against other physicians.3
Based on these ethical principles, physicians have a duty to provide accurate and responsible expert testimony. Inaccurate expert testimony is damaging to the system in many ways: It increases malpractice costs, injures the reputation of individual practitioners, and adversely affects the standard of care by promoting false standards. Distinguishing irresponsible testimony from reasonable differences of opinion may be challenging. Any valid lawsuit will involve conflicting opinions as to whether the standard of care was met—otherwise there would be no need for expert testimony. To protect against overreaching, physicians should limit themselves to areas of their own academic and experiential expertise, and should limit their testimony to their scope of training or practice. Their opinions should be consistent with prevailing literature and good clinical practice. Offering an unusual opinion that contradicts the literature may be appropriate if the expert has good reason to believe the atypical opinion is correct and can provide evidence to support the claim.
Applying these principles to the practice of hospitalists requires special considerations. Hospital medicine is not a discrete specialty in the sense of having a certifying board or mandatory focused training requirements; however, hospitalists practice in a particular environment and should limit their expert testimony to that environment. Hospitalists have diverse practices and some practice outpatient medicine or primary care as well. Thus, it is particularly important for hospitalists to demonstrate responsibility and integrity in limiting their testimony to areas where they have genuine specialized knowledge and experience. Other physicians, attorneys, and judges must rely on hospitalists to enforce standards themselves because no single standard can be applied to all hospitalists.
As a further consideration in the interests of justice and professionalism, physicians should recuse themselves from any case with an actual or perceived conflict of interest. Prominent physicians, including public figures and society leaders, have the same duty regarding self-regulation in the profession and promotion of justice in the system as any other physician. Any reason to be personally predisposed to one side of the case or the other as a result of personal involvement or professional interests may make the physician an inappropriate expert. Unless testifying on behalf of the position of a society, a physician should not use society membership as direct evidence of expertise. Society leaders should be cautious about the appearance of conflict of interest, specifically that their status in the society confers special expert qualifications.
Professional societies have a special role in ensuring quality healthcare and a special role in the trust of society. Many societies, including the American Medical Association and the American Academy of Pediatrics have created guidelines for expert witnesses, and the AMA has further discussed the need for a more active role in expert oversight by professional societies.3 Societies need to establish standards for members who act as experts and create enforcement mechanisms for those standards. Further, societies should decide whether they intend to undertake formal disciplinary actions against physicians acting improperly by making the state disciplinary boards aware of their findings of improper conduct. Such standards and policies must be explicit, documented, and published. This is an expanded role for professional societies in the arena of explicit regulation and discipline of members, but there has been increasing recognition that professional societies are an ideal forum for increasing regulation and standards for expert testimony.4-5
The Verdict
The decision to participate in a medical malpractice case as an expert witness requires competence, accurate self-assessment, and integrity. A physician should testify only to what he or she genuinely believes to be the standard of care, regardless of which side approaches him or her. The physician should consider his or her current practice and expertise to decide if he or she can provide honest and accurate expert testimony.
He or she should keep in mind the interests of patients in having access to the courts and to fair compensation from injuries, and therefore physicians should have the courage and integrity to testify against colleagues when he or she genuinely believes that the colleague injured the plaintiff through a deviation from the standard of care. Society relies upon physicians to risk disfavor with colleagues in the interest of promoting justice and protecting patients when the physician believes that is the right thing to do. Physicians interested in policy issues around expert testimony should become involved in their professional societies to create and enforce quality standards for expert witnesses.
References
- Federal Rules of Evidence 701, 702, 703.
- Daubert v. Merrell Dow, 509 U.S. 579; 113 S. Ct. 2786; 125 L. Ed. 2d 469 (1993).
- American Medical Association Code of Medical Ethics, Discipline in Medicine, E-9.04 Available at www.ama-assn.org. Last accessed May 25, 2006.
- Feld AD, Carey WD. Expert witness malfeasance: how should specialty societies respond? Am J Gastroenterol. 2005 May;100(5):991-995.
- Gomez JCB. Silencing the hired guns: ensuring honesty in medical testimony. J Leg Med. 2005 Sep;26(3):385-399.
SHM: BEHIND THE SCENES
SHM Online
By Scott Johnson
Last month, my next door neighbor at the office and SHM’s director of membership, Todd Von Deak, wrote a new column meant to share with you a “behind the scenes” look at SHM. I am pleased to carry the torch in this issue of The Hospitalist and give you a sneak peek at what’s next for SHM’s Web and IT initiatives.
First, let’s step back and look at some changes we’ve recently implemented and how each should benefit your membership.
Our database is key in our efforts to keep you up to date on not only the latest news from SHM, but also from the hospital medicine community at large. Over the past couple of months, we have completed a major review of our data-gathering processes and made changes to how we store your information. These changes will not only better protect your privacy, which is a major concern of ours, but also better enable us to reach you at your preferred address—whether at home or work.
Part of great customer service is listening. Many members have shared that they find it cumbersome to have to remember their member number in order to log onto SHM’s Web site. We’re pleased to announce that you can now access the SHM Web site with your own personalized username and password.
To create your own login and password, just visit www.hospitalmedicine.org/activate. Once online, you will be asked to enter your member number and last name, and then asked to choose a new username and password.
In addition to allowing you to create your own username and password, we’ve also streamlined the process to renew your membership or join online. Check it out when you get a chance. I’d love to hear your feedback.
Now that we have had our flashback, let’s discuss what we’ve got planned for the future. Since launching the new Career Center (www.hospitalmedicine.org/careercenter) we have begun working on projects to create a more personal experience for you as you visit the SHM Web site and receive our monthly e-mail newsletter.
The SHM Store, which launched in June, features a variety of SHM products and resources. Key educational products such as the results from our “Survey on the State of the Hospital Medicine Movement” will be available, as will favorites like SHM hats and golf shirts (both men’s and women’s).
The next evolution of SHM’s eNewsletter, our monthly e-mail newsletter, will occur this fall. In addition to a new look and feel, the eNewsletter will contain information unique for members and non-members and will be personalized to your areas of interest.
We are also creating a personally tailored Web site where you can create your own “My SHM” page. Once live, this new benefit will enable you to select topics of interest and have related articles, stories, and links automatically appear on your own “My SHM” page.
Having worked with healthcare associations for almost seven years I recognize how important your time is and the value of having the best and most current information at your fingertips. Our goal is to not only create a place where you can find the information you need to excel in your field, but to find ways in which you can “pull” the information relevant to you to your inbox, PDA, or iPod.
For the moment, we are focused on improving and enhancing the current tools in SHM’s tool belt. But on the not-too-distant horizon you’ll be hearing more about our plans to use new tools, such as PDAs and iPods, to provide you with even more information and resources. We’re confident that these resources will help you enhance the quality of care you provide to your patients and their families.
Steve Jobs, CEO of Apple Computer, once said, “The journey is the reward.” In the time I have spent with SHM it has already been quite a rewarding journey and I am excited about the landscape that lies before us.
Next month, you’ll hear from Geri Barnes, our director of education and quality initiatives. Geri is leading the charge to keep our education program in its current position as the most informative and innovative set of offerings within our specialty.
If you ever have any questions about our Web-based offerings, or feedback on how we can improve existing products and programs, please e-mail me at sjohnson@hospitalmedicine.org.
Johnson is SHM’s director of information services.
New Leadership AcademyOffering to Debut in Nashville
Level II track created in response to demand
SHM is pleased to announce the expansion of its cutting edge leadership program, with the debut of a Level II track as part of the Leadership Academy Sept. 11-14 in Nashville, Tenn.
Over the course of four days, the Leadership Academy will provide hospitalist leaders with the skills and resources required to successfully lead and manage a hospital medicine program now and in the future.
Topics that will be addressed include:
- Leadership challenges in hospital medicine;
- Finance and the hospitalist;
- Leading recruitment, retention, and staff development; and
- Leading and managing change.
This course was created in response to feedback from previous Leadership Academy attendees and is designed to give them the opportunity to build on the time they’ve spent back at the hospital since attending a Leadership Academy. Level II offers an in-depth look at how to finance a hospital, insight on how to lead recruitment, retention, and staff development. It also presents advanced skills in negotiation.
Because Level II is considered an advanced course, attendees must have participated in a previous leadership academy or have completed an MBA program to be accepted.
As with any SHM educational event, ample time will be set aside for interaction with faculty and participants so you can get answers to your pressing questions and make connections for the future.
“The fact that learning takes place both inside and outside of the classroom is one of the things that makes SHM’s Leadership Academies so powerful,” says Larry Wellikson, CEO of SHM.
According to Scott Enderby, a Leadership Academy graduate, “This is the only medical conference I’ve ever gone to where I went to every meeting and still wanted more.”
The September venue—the Gaylord Nashville Resort & Convention Center in Nashville—offers ample opportunity to relax in the midst of your intense learning experience. From tours aboard the hotel’s Delta Flatboats to the chance to play 18 holes at the Grand Ole Opry Course, there is something for everyone, including your family.
To register for the September Leadership Academy, visit www.hospitalmedicine.org or call (800) 843-3360.
Can’t join us in Nashville? Mark your calendars for our winter Leadership Academy, Feb. 26-March 1, 2007, in Orlando, Fla. TH
Hospital Med in the Land of Rocky Top
If a busy doctor is a happy doctor, then the hospitalists in the Methodist Medical Group at Methodist Hospital in Oak Ridge, Tenn., are ecstatic. Chris Frost, MD, the hospital medicine group’s chief hospitalist and medical director, has seen the group’s average daily census climb to 70, then 90, and now 100 patients. Fortunately, the group is growing, too, from nine full-time employees in late October 2005 to 12 before year-end, a projection for 15 by first quarter 2006, and several intensivists to help by March.
The hospital itself has grown as well: It’s in the midst of a $40 million renovation and expansion started in 2004. By August 2006, Methodist Medical will have 230 new private rooms, 12 beds in a new acute care unit, and an emergency department twice the size of its predecessor.

—Chris Frost, MD
How It Started
Methodist Medical Group has been shaped by Oak Ridge’s traditions and demographics. Nestled between the Great Smokey and Cumberland Mountains, Oak Ridge was one of three research and production sites for the Manhattan Project (an effort by the United States, in conjunction with Canada and the United Kingdom to develop nuclear weapons). At its height, Oak Ridge had 75,000 inhabitants. Now its population is 28,000, with a Medicare age group that comprises 42% more of its population than the average Tennessee city. It continues as a magnet for scientists, and its physicians—both office-based and hospitalists—form a close-knit community.

Given its dynamics and demographics, when Oak Ridge’s primary care physicians asked Methodist Hospital in 1993 for help in admitting their patients, the hospital responded affirmatively. Hospital President Jan McNally, BSN, MHA, recalls how things unfolded. “Dr. Richard Dew, a highly respected primary practice physician with a busy office, wanted to change his life. His son had died and he decided to close his office, but he wanted to stay in medicine in Oak Ridge. He agreed to practice inpatient medicine at Methodist,” she explains. “The beauty of it was that he was universally respected. Barriers to the program fell because the admitting doctors and the patients all knew him.”
When Dr. Dew retired in 2002, Anthony Garton, MD, who closed his solo practice to join Dr. Dew as Methodist’s second hospitalist, stayed on. Dr. Garton became a hospitalist because “office procedures just brought me to break even financially. Only the things I did that didn’t have office overhead, such as being medical director at a nursing home and doing physicals for Boeing, made sense financially.” Dr. Garton, who worked with a nephrology group for 13 years, made a smooth transition to a hospitalist career.
From the hospitalist program’s inception, Methodist turned to Team Health, Inc., of Knoxville, an outsourcer of medical personnel, for staffing. Team Health Vice President Kenneth Burns saw a natural fit; his firm already supplied Methodist’s emergency department physicians.
“We understood the problems faced by Methodist’s ED docs,” says Burns. “Patients got stuck there and couldn’t be admitted rapidly to inpatient floors.”
He identified the hospitalist’s necessary skills as an ability to cooperate with community physicians, and an interest in improving processes to boost care quality and decrease costs. Methodist’s hospitalists have been independent contractors since the program’s inception. They receive hourly wages plus incentives based on productivity and metrics negotiated with hospital administrators.
Team Health recently rethought the model as potential recruits balked. In 2006 Methodist’s hospitalists became employees, with health benefits and defined contribution plans. Hospitalist Helen Bidawid, MD, says being employees improves recruiting because many doctors—particularly those just out of residency—find getting loans, buying health insurance, and other business associated with independent contractor status troublesome.
Symbiosis

The relationship of Methodist’s hospitalist program to Oak Ridge’s community physicians has changed over the years. Early on the group hired a hospitalist Dr. Garton describes as “very bright, knew his medicine, and would wow them in academia, but he antagonized the local docs. He left after one year and that was good because our census got low.”
Tact wasn’t that hospitalist’s long suit, and the community doctors who were uncomfortable with him didn’t refer many patients to the hospitalists. With the odd man out, hiring new hospitalists such as Joel Perkerson, MD, put the program back on track.

Dr. Perkerson left an office practice he had been in for 12 years. “I was drowning in paperwork, and it was so frustrating,” he says. “I couldn’t get my homework done or help my son, who was struggling academically.”
Having been both an office- and a hospital-based physician in Oak Ridge, he says it’s too hectic to do both. Being a hospitalist is challenging enough.
“It’s like the movie ‘Field of Dreams.’ Build it, and they will come. Demand keeps growing for our services and we all work a lot of hours,” he says, crediting the increasing load both to Dr. Frost’s leadership, which has made the subspecialists comfortable with the hospitalists’ management of medically complex patients, and to ex-TennCare patients flooding the emergency department. (See “When Politics Collide with Healthcare,” p. 38.)
Under Dr. Frost’s direction (he took over as medical director in 2003 after being recruited as assistant medical director), the hospitalist program has thrived. Dr. Frost has built relationships with Oak Ridge’s subspecialists, particularly pulmonologists, hematologists, oncologists, gastroenterologists, and orthopedists. Typical of Dr. Frost’s leadership is his response to Oak Ridge’s only pulmonary group imploding from six physicians to two. The hospitalists now admit all the group’s patients and Dr. Frost worked with Team Health to recruit intensivists for those very ill patients.
“I’m very pleased with the growth of the hospitalist program,” says Dr. Frost. “We feel empowered that more and more primary care doctors and subspecialists are allowing us to admit and take an active role in managing their patients.”
Tackling one problem that has bedeviled other hospitalist programs, Jan McNally has added a mechanism to ensure cooperation from referring doctors. She expects referring subspecialists to come for consults ASAP when a hospitalist calls.
“We must have that commitment from specialists,” she says. “We have about 15 percent who are laggards, but we will impose disciplinary action if they don’t come when called.”
Dr. Frost favors specialists willing to turn their patients over to the hospitalists in order to improve care quality. He diligently writes care guidelines, focuses on core measures, has deepened discussion of end-of-life care issues, and built such strong esprit de corps that the hospitalists willingly work long and irregular schedules until more physicians arrive. Helen Bidawid, MD, who has been a Methodist hospitalist for about a year, enjoys the hospitalist group, doesn’t mind pitching in to support her colleagues, and says “we function very well together. We watch out for all of our patients, share our responsibilities, and ask each other for help.”
Dr. Bidawid, who was in a non-supportive hospitalist group before her current position, asked herself before she arrived at Methodist: “’Will I be nurtured here or thrown to the wolves?’ Fortunately, I found a very supportive environment.”
With the course set, Dr. Frost still has challenges ahead. There’s growing patient volume, more complex cases to co-manage, carve-outs such as cardiology, neurology, and stroke care, and TennCare disenrollees to contend with.
“Our goal is to add value to Methodist Medical Center,” he says. “As a 24/7 hospitalist program, we help the medical community to be more profitable by enabling them to see more patients in the office and doing more procedures in the hospital. Better communication between physicians, patients, and their families benefits everyone and, we hope, will grow Methodist’s market share.” TH
Marlene Piturro is based in New York.
Quality Counts

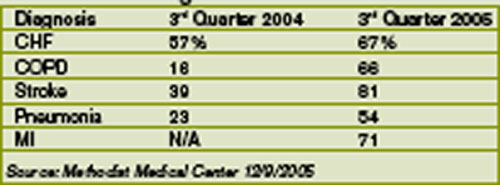
Methodist Medical ranks #1 in Tennessee on its compliance with Medicare core measures. Coletta Manning, RN, MHA, Methodist’s director of outcomes management, provided these data to show how they did it: (Table 1)
Manning cites this caveat in interpreting the data: When a patient is admitted and a diagnosis associated with a core measure is not made until the second day of hospitalization, the case isn’t considered in compliance. An example is abdominal pain that on further examination turns out to be caused by a myocardial infarction. If that were the case, the core measure of giving aspirin immediately would not be met because the diagnosis was not made within the first 24 hours of admission. “We get dinged sometimes,” says Manning.
Internally, the hospitalists measure their performance on compliance with the group’s own care design (critical pathway) utilization. Dr. Frost is pleased with the hospitalists’ growing acceptance of care designs and is working with Team Health on a sophisticated computer system to help the hospitalists use
If a busy doctor is a happy doctor, then the hospitalists in the Methodist Medical Group at Methodist Hospital in Oak Ridge, Tenn., are ecstatic. Chris Frost, MD, the hospital medicine group’s chief hospitalist and medical director, has seen the group’s average daily census climb to 70, then 90, and now 100 patients. Fortunately, the group is growing, too, from nine full-time employees in late October 2005 to 12 before year-end, a projection for 15 by first quarter 2006, and several intensivists to help by March.
The hospital itself has grown as well: It’s in the midst of a $40 million renovation and expansion started in 2004. By August 2006, Methodist Medical will have 230 new private rooms, 12 beds in a new acute care unit, and an emergency department twice the size of its predecessor.
—Chris Frost, MD
How It Started
Methodist Medical Group has been shaped by Oak Ridge’s traditions and demographics. Nestled between the Great Smokey and Cumberland Mountains, Oak Ridge was one of three research and production sites for the Manhattan Project (an effort by the United States, in conjunction with Canada and the United Kingdom to develop nuclear weapons). At its height, Oak Ridge had 75,000 inhabitants. Now its population is 28,000, with a Medicare age group that comprises 42% more of its population than the average Tennessee city. It continues as a magnet for scientists, and its physicians—both office-based and hospitalists—form a close-knit community.
Given its dynamics and demographics, when Oak Ridge’s primary care physicians asked Methodist Hospital in 1993 for help in admitting their patients, the hospital responded affirmatively. Hospital President Jan McNally, BSN, MHA, recalls how things unfolded. “Dr. Richard Dew, a highly respected primary practice physician with a busy office, wanted to change his life. His son had died and he decided to close his office, but he wanted to stay in medicine in Oak Ridge. He agreed to practice inpatient medicine at Methodist,” she explains. “The beauty of it was that he was universally respected. Barriers to the program fell because the admitting doctors and the patients all knew him.”
When Dr. Dew retired in 2002, Anthony Garton, MD, who closed his solo practice to join Dr. Dew as Methodist’s second hospitalist, stayed on. Dr. Garton became a hospitalist because “office procedures just brought me to break even financially. Only the things I did that didn’t have office overhead, such as being medical director at a nursing home and doing physicals for Boeing, made sense financially.” Dr. Garton, who worked with a nephrology group for 13 years, made a smooth transition to a hospitalist career.
From the hospitalist program’s inception, Methodist turned to Team Health, Inc., of Knoxville, an outsourcer of medical personnel, for staffing. Team Health Vice President Kenneth Burns saw a natural fit; his firm already supplied Methodist’s emergency department physicians.
“We understood the problems faced by Methodist’s ED docs,” says Burns. “Patients got stuck there and couldn’t be admitted rapidly to inpatient floors.”
He identified the hospitalist’s necessary skills as an ability to cooperate with community physicians, and an interest in improving processes to boost care quality and decrease costs. Methodist’s hospitalists have been independent contractors since the program’s inception. They receive hourly wages plus incentives based on productivity and metrics negotiated with hospital administrators.
Team Health recently rethought the model as potential recruits balked. In 2006 Methodist’s hospitalists became employees, with health benefits and defined contribution plans. Hospitalist Helen Bidawid, MD, says being employees improves recruiting because many doctors—particularly those just out of residency—find getting loans, buying health insurance, and other business associated with independent contractor status troublesome.
Symbiosis
The relationship of Methodist’s hospitalist program to Oak Ridge’s community physicians has changed over the years. Early on the group hired a hospitalist Dr. Garton describes as “very bright, knew his medicine, and would wow them in academia, but he antagonized the local docs. He left after one year and that was good because our census got low.”
Tact wasn’t that hospitalist’s long suit, and the community doctors who were uncomfortable with him didn’t refer many patients to the hospitalists. With the odd man out, hiring new hospitalists such as Joel Perkerson, MD, put the program back on track.
Dr. Perkerson left an office practice he had been in for 12 years. “I was drowning in paperwork, and it was so frustrating,” he says. “I couldn’t get my homework done or help my son, who was struggling academically.”
Having been both an office- and a hospital-based physician in Oak Ridge, he says it’s too hectic to do both. Being a hospitalist is challenging enough.
“It’s like the movie ‘Field of Dreams.’ Build it, and they will come. Demand keeps growing for our services and we all work a lot of hours,” he says, crediting the increasing load both to Dr. Frost’s leadership, which has made the subspecialists comfortable with the hospitalists’ management of medically complex patients, and to ex-TennCare patients flooding the emergency department. (See “When Politics Collide with Healthcare,” p. 38.)
Under Dr. Frost’s direction (he took over as medical director in 2003 after being recruited as assistant medical director), the hospitalist program has thrived. Dr. Frost has built relationships with Oak Ridge’s subspecialists, particularly pulmonologists, hematologists, oncologists, gastroenterologists, and orthopedists. Typical of Dr. Frost’s leadership is his response to Oak Ridge’s only pulmonary group imploding from six physicians to two. The hospitalists now admit all the group’s patients and Dr. Frost worked with Team Health to recruit intensivists for those very ill patients.
“I’m very pleased with the growth of the hospitalist program,” says Dr. Frost. “We feel empowered that more and more primary care doctors and subspecialists are allowing us to admit and take an active role in managing their patients.”
Tackling one problem that has bedeviled other hospitalist programs, Jan McNally has added a mechanism to ensure cooperation from referring doctors. She expects referring subspecialists to come for consults ASAP when a hospitalist calls.
“We must have that commitment from specialists,” she says. “We have about 15 percent who are laggards, but we will impose disciplinary action if they don’t come when called.”
Dr. Frost favors specialists willing to turn their patients over to the hospitalists in order to improve care quality. He diligently writes care guidelines, focuses on core measures, has deepened discussion of end-of-life care issues, and built such strong esprit de corps that the hospitalists willingly work long and irregular schedules until more physicians arrive. Helen Bidawid, MD, who has been a Methodist hospitalist for about a year, enjoys the hospitalist group, doesn’t mind pitching in to support her colleagues, and says “we function very well together. We watch out for all of our patients, share our responsibilities, and ask each other for help.”
Dr. Bidawid, who was in a non-supportive hospitalist group before her current position, asked herself before she arrived at Methodist: “’Will I be nurtured here or thrown to the wolves?’ Fortunately, I found a very supportive environment.”
With the course set, Dr. Frost still has challenges ahead. There’s growing patient volume, more complex cases to co-manage, carve-outs such as cardiology, neurology, and stroke care, and TennCare disenrollees to contend with.
“Our goal is to add value to Methodist Medical Center,” he says. “As a 24/7 hospitalist program, we help the medical community to be more profitable by enabling them to see more patients in the office and doing more procedures in the hospital. Better communication between physicians, patients, and their families benefits everyone and, we hope, will grow Methodist’s market share.” TH
Marlene Piturro is based in New York.
Quality Counts
Methodist Medical ranks #1 in Tennessee on its compliance with Medicare core measures. Coletta Manning, RN, MHA, Methodist’s director of outcomes management, provided these data to show how they did it: (Table 1)
Manning cites this caveat in interpreting the data: When a patient is admitted and a diagnosis associated with a core measure is not made until the second day of hospitalization, the case isn’t considered in compliance. An example is abdominal pain that on further examination turns out to be caused by a myocardial infarction. If that were the case, the core measure of giving aspirin immediately would not be met because the diagnosis was not made within the first 24 hours of admission. “We get dinged sometimes,” says Manning.
Internally, the hospitalists measure their performance on compliance with the group’s own care design (critical pathway) utilization. Dr. Frost is pleased with the hospitalists’ growing acceptance of care designs and is working with Team Health on a sophisticated computer system to help the hospitalists use
If a busy doctor is a happy doctor, then the hospitalists in the Methodist Medical Group at Methodist Hospital in Oak Ridge, Tenn., are ecstatic. Chris Frost, MD, the hospital medicine group’s chief hospitalist and medical director, has seen the group’s average daily census climb to 70, then 90, and now 100 patients. Fortunately, the group is growing, too, from nine full-time employees in late October 2005 to 12 before year-end, a projection for 15 by first quarter 2006, and several intensivists to help by March.
The hospital itself has grown as well: It’s in the midst of a $40 million renovation and expansion started in 2004. By August 2006, Methodist Medical will have 230 new private rooms, 12 beds in a new acute care unit, and an emergency department twice the size of its predecessor.
—Chris Frost, MD
How It Started
Methodist Medical Group has been shaped by Oak Ridge’s traditions and demographics. Nestled between the Great Smokey and Cumberland Mountains, Oak Ridge was one of three research and production sites for the Manhattan Project (an effort by the United States, in conjunction with Canada and the United Kingdom to develop nuclear weapons). At its height, Oak Ridge had 75,000 inhabitants. Now its population is 28,000, with a Medicare age group that comprises 42% more of its population than the average Tennessee city. It continues as a magnet for scientists, and its physicians—both office-based and hospitalists—form a close-knit community.
Given its dynamics and demographics, when Oak Ridge’s primary care physicians asked Methodist Hospital in 1993 for help in admitting their patients, the hospital responded affirmatively. Hospital President Jan McNally, BSN, MHA, recalls how things unfolded. “Dr. Richard Dew, a highly respected primary practice physician with a busy office, wanted to change his life. His son had died and he decided to close his office, but he wanted to stay in medicine in Oak Ridge. He agreed to practice inpatient medicine at Methodist,” she explains. “The beauty of it was that he was universally respected. Barriers to the program fell because the admitting doctors and the patients all knew him.”
When Dr. Dew retired in 2002, Anthony Garton, MD, who closed his solo practice to join Dr. Dew as Methodist’s second hospitalist, stayed on. Dr. Garton became a hospitalist because “office procedures just brought me to break even financially. Only the things I did that didn’t have office overhead, such as being medical director at a nursing home and doing physicals for Boeing, made sense financially.” Dr. Garton, who worked with a nephrology group for 13 years, made a smooth transition to a hospitalist career.
From the hospitalist program’s inception, Methodist turned to Team Health, Inc., of Knoxville, an outsourcer of medical personnel, for staffing. Team Health Vice President Kenneth Burns saw a natural fit; his firm already supplied Methodist’s emergency department physicians.
“We understood the problems faced by Methodist’s ED docs,” says Burns. “Patients got stuck there and couldn’t be admitted rapidly to inpatient floors.”
He identified the hospitalist’s necessary skills as an ability to cooperate with community physicians, and an interest in improving processes to boost care quality and decrease costs. Methodist’s hospitalists have been independent contractors since the program’s inception. They receive hourly wages plus incentives based on productivity and metrics negotiated with hospital administrators.
Team Health recently rethought the model as potential recruits balked. In 2006 Methodist’s hospitalists became employees, with health benefits and defined contribution plans. Hospitalist Helen Bidawid, MD, says being employees improves recruiting because many doctors—particularly those just out of residency—find getting loans, buying health insurance, and other business associated with independent contractor status troublesome.
Symbiosis
The relationship of Methodist’s hospitalist program to Oak Ridge’s community physicians has changed over the years. Early on the group hired a hospitalist Dr. Garton describes as “very bright, knew his medicine, and would wow them in academia, but he antagonized the local docs. He left after one year and that was good because our census got low.”
Tact wasn’t that hospitalist’s long suit, and the community doctors who were uncomfortable with him didn’t refer many patients to the hospitalists. With the odd man out, hiring new hospitalists such as Joel Perkerson, MD, put the program back on track.
Dr. Perkerson left an office practice he had been in for 12 years. “I was drowning in paperwork, and it was so frustrating,” he says. “I couldn’t get my homework done or help my son, who was struggling academically.”
Having been both an office- and a hospital-based physician in Oak Ridge, he says it’s too hectic to do both. Being a hospitalist is challenging enough.
“It’s like the movie ‘Field of Dreams.’ Build it, and they will come. Demand keeps growing for our services and we all work a lot of hours,” he says, crediting the increasing load both to Dr. Frost’s leadership, which has made the subspecialists comfortable with the hospitalists’ management of medically complex patients, and to ex-TennCare patients flooding the emergency department. (See “When Politics Collide with Healthcare,” p. 38.)
Under Dr. Frost’s direction (he took over as medical director in 2003 after being recruited as assistant medical director), the hospitalist program has thrived. Dr. Frost has built relationships with Oak Ridge’s subspecialists, particularly pulmonologists, hematologists, oncologists, gastroenterologists, and orthopedists. Typical of Dr. Frost’s leadership is his response to Oak Ridge’s only pulmonary group imploding from six physicians to two. The hospitalists now admit all the group’s patients and Dr. Frost worked with Team Health to recruit intensivists for those very ill patients.
“I’m very pleased with the growth of the hospitalist program,” says Dr. Frost. “We feel empowered that more and more primary care doctors and subspecialists are allowing us to admit and take an active role in managing their patients.”
Tackling one problem that has bedeviled other hospitalist programs, Jan McNally has added a mechanism to ensure cooperation from referring doctors. She expects referring subspecialists to come for consults ASAP when a hospitalist calls.
“We must have that commitment from specialists,” she says. “We have about 15 percent who are laggards, but we will impose disciplinary action if they don’t come when called.”
Dr. Frost favors specialists willing to turn their patients over to the hospitalists in order to improve care quality. He diligently writes care guidelines, focuses on core measures, has deepened discussion of end-of-life care issues, and built such strong esprit de corps that the hospitalists willingly work long and irregular schedules until more physicians arrive. Helen Bidawid, MD, who has been a Methodist hospitalist for about a year, enjoys the hospitalist group, doesn’t mind pitching in to support her colleagues, and says “we function very well together. We watch out for all of our patients, share our responsibilities, and ask each other for help.”
Dr. Bidawid, who was in a non-supportive hospitalist group before her current position, asked herself before she arrived at Methodist: “’Will I be nurtured here or thrown to the wolves?’ Fortunately, I found a very supportive environment.”
With the course set, Dr. Frost still has challenges ahead. There’s growing patient volume, more complex cases to co-manage, carve-outs such as cardiology, neurology, and stroke care, and TennCare disenrollees to contend with.
“Our goal is to add value to Methodist Medical Center,” he says. “As a 24/7 hospitalist program, we help the medical community to be more profitable by enabling them to see more patients in the office and doing more procedures in the hospital. Better communication between physicians, patients, and their families benefits everyone and, we hope, will grow Methodist’s market share.” TH
Marlene Piturro is based in New York.
Quality Counts
Methodist Medical ranks #1 in Tennessee on its compliance with Medicare core measures. Coletta Manning, RN, MHA, Methodist’s director of outcomes management, provided these data to show how they did it: (Table 1)
Manning cites this caveat in interpreting the data: When a patient is admitted and a diagnosis associated with a core measure is not made until the second day of hospitalization, the case isn’t considered in compliance. An example is abdominal pain that on further examination turns out to be caused by a myocardial infarction. If that were the case, the core measure of giving aspirin immediately would not be met because the diagnosis was not made within the first 24 hours of admission. “We get dinged sometimes,” says Manning.
Internally, the hospitalists measure their performance on compliance with the group’s own care design (critical pathway) utilization. Dr. Frost is pleased with the hospitalists’ growing acceptance of care designs and is working with Team Health on a sophisticated computer system to help the hospitalists use
Changing of the Guard
Each year a new team of SHM officers is elected to lend their wisdom, time, experience, and skills in a collaborative effort to help manage the business of our organization, drive new initiatives, and support the society’s mission. At this year’s annual meeting in Washington, D.C., we again witnessed that familiar changing of the guard with the following inductions:
- President Mary Jo Gorman, MD, MBA;
- President-Elect Russell Holman, MD;
- Treasurer Patrick Cawley, MD; and
- Secretary Jack Percelay, MD, MPH.
“Hospitalists are squarely in the spotlight today on key issues affecting patient care, quality of hospital care, hospital leadership, and other concerns. So it is important that we have a strong, hands-on leadership team that is committed to continuing the positive momentum SHM has generated for hospitalists,” says Larry Wellikson, MD, FACP, CEO of SHM. “I couldn’t be more thrilled with our slate of newly appointed officers. Time and again through the years Mary Jo, Rusty, Pat, and Jack have proven that they are active participants, and that they are leaders who will rise to the occasion to help us meet our objectives.”

Dr. Gorman, a charter member of SHM, has been a practicing hospitalist since 1997, when she founded the first hospitalist practice in St. Louis. In early 1999, her group merged into IPC—The Hospitalist Company and grew to become the dominant hospitalist group in the city. In 2001, Dr. Gorman was promoted to vice-president of medical affairs for IPC, responsible for the design and implementation of company-wide programs involving business development, recruitment, physician training, and operations in all of IPC’s markets. In 2003, she was named chief medical officer and today works with more than 300 physicians nationwide to develop programs and strategies that enhance clinical performance and drive the delivery system towards more efficient care and greater patient satisfaction. She also oversees IPC’s physician training, mentoring and retention programs, as well as IPC’s call center nurses, healthcare services and clinical studies.
A cum laude graduate of St. Louis University, Dr. Gorman earned a BA in Chemistry/Biology in 1981, then went on to earn her MD in 1984 from Southern Illinois University School of Medicine in Springfield. In 1996, she earned a MBA from Washington University, Olin School of Business, in St. Louis.

SHM’s new President-Elect Dr. Holman is senior vice president and national medical director for Cogent Healthcare, an organization that manages hospital medicine programs throughout the country. He is responsible for program implementation and management, quality systems reporting and auditing, physician leadership development, and data systems integration. Formerly, Dr. Holman was the medical director of Hospital Services for HealthPartners Medical Group & Clinics, part of HealthPartners, Inc. in Minnesota. There he also was the founder and director of the HPMG Fellowship Program in Hospital Medicine.
A long-time member of SHM, Dr. Holman served on the Board of Directors as treasurer from 2004-2005. He was previously chair of the Leadership Development Committee, chair of the Midwest Council, course director of the SHM Leadership Academy, and a member of the Public Policy Committee. In February 2006 he co-authored the “Update in Hospital Medicine,” which appeared in Annals of Internal Medicine. In 2002, he received the SHM Award for Outstanding Service in Hospital Medicine.
Through the years, Dr. Holman’s commitment to hospital medicine has helped produce nationally recognized standards in the areas of quality improvement activities, models of medical education, observation units, communication systems, compensation plans, case management, surgical co-management collaborations, and patient flow initiatives. Dr. Holman serves on two national editorial boards for medical publications and is currently co-authoring a comprehensive textbook and electronic decision support tool in hospital medicine.
Dr. Holman earned his MD from Washington University School of Medicine in St. Louis and trained as a resident and chief medical resident at the University of Minnesota in Minneapolis.

New Treasurer Dr. Cawley is a hospitalist at the Medical University of South Carolina in Charleston, where he currently serves as interim executive medical director of MUSC Medical Center. He previously served as the chief of the Section of Hospital Medicine, vice chairman of clinical affairs in the Department of Medicine, and associate executive medical director at MUSC Medical Center.
A charter member of SHM, Dr. Cawley has served on numerous committees and was previously secretary of the Board for the 2004-2005 term. He has worked in both academic and nonacademic hospitals and has served as a consultant to numerous hospitals in the development of hospital medicine programs.
Dr. Cawley received his Bachelor of Science in 1988 from the University of Scranton (Pa.) and his MD from Georgetown University School of Medicine in Washington, D.C. He completed an internal medicine residency at Duke University in Durham, N.C. Later this year, he will complete his MBA from the University of Massachusetts-Amherst.

SHM’s new secretary is Dr. Percelay. He is director of Virtua Inpatient Pediatrics, a large pediatric hospital medicine group in Southern New Jersey with 14 full-time hospitalists covering two hospitals. Since 1991, Dr. Percelay has worked in a variety of community-based settings including the general pediatric ward, pediatric sub-specialty units, pediatric intensive care unit (PICU), neonatal intensive care unit (NICU), and the emergency department.
A charter member of SHM and one of the nation’s first pediatric hospitalists, Dr. Percelay currently holds the Pediatric Seat on the SHM Board, in addition to serving on the Public Policy Committee and co-chairing the Pediatric Committee. He has been intimately involved in collaborative Pediatric hospital medicine projects such as the PRIS research network and the Denver 2005 and 2007 Pediatric Hospital Medicine conferences.
Dr. Percelay is also the founding chairperson and immediate past chair of the American Academy of Pediatrics Section on Hospital Medicine and co-authored the AAP policy statement on pediatric hospitalists. He completed his medical school and pediatric training at the University of California at San Francisco, along with an MPH at the University of California at Berkeley.
SHM congratulates these new officers and thanks our 2005 officers (Steve Pantilat, MD, president, William Atchley, MD, FACP, treasurer, and Lisa Kettering, MD, FACP, secretary) for their exemplary work.
Annual Meeting e-Community a Success
If the feedback from attendees at this year’s Annual Meeting was any indication, the inaugural launch of SHM’s Annual Meeting e-Community was a success.
Each year, SHM’s Annual Meeting provides an opportunity for hospital medicine professionals to network with colleagues and take advantage of more than 40 educational sessions during the course of three days.
While the location for the meeting changes regularly, there is a constant desire within the Annual Meeting planning committee (a group of volunteer members) to improve the attendee experience. The Annual Meeting e-Community (AMeC) was designed with that in mind.
The AMeC effectively extended the reach of the annual meeting both before and after the event. Since early April, attendees have been able to access the handouts for the presentations that were given at the event and network with colleagues thanks to dedicated discussion communities. There are also listings of exhibitors scheduled to be in attendance and general information about Washington, D.C., on the AMeC.
Because of the positive feedback received, the e-Community will stay online through early July, giving attendees the chance to download presentations from sessions that they didn’t attend and make contact with colleagues they met while in Washington, D.C.
Attendees appreciated the ability to access meeting materials prior to the event. “The Annual Meeting e-Community gave me a great opportunity to really plan out the sessions that I wanted to attend prior to the meeting,” says William Rifkin, MD, a hospitalist from the Yale School of Medicine.
According to Joy Wittnebert, AMeC project manager, the site was launched in response to feedback from past annual meetings. “Attendees have been consistently telling us that they want to be able to customize their experience and have more opportunities to network with colleagues before and after the event,” she says.
In the coming months, SHM staff will work with the Annual Meeting Committee to analyze additional feedback and begin making plans for the 2007 version of the site.
SHM Education Committee Launches 18-Month Strategic Plan
Helping our members and the hospital medicine community advance in professional growth and development has been on center stage as seen in the SHM Education Committee’s recent completion of an 18-month strategic plan. The plan is a framework designed to guide staff and volunteer leadership as they work to expand the society’s current slate of educational offerings. Inherent in the framework’s design is a focus on taking advantage of the myriad new channels that have come online for delivering educational content.
The plan is rooted primarily in the recently released Core Competencies in Hospital Medicine. The Core Competencies are a benchmark for the development of curricula within the hospital medicine specialty.
“One of the most exciting parts of this plan is its connection to the Core Competencies,” says Geri Barnes, SHM’s director of education and quality initiatives. “The connection means that this is one of the strongest educational plans that the society has put forward.”
A driving force in the creation of this plan was the committee’s desire to expand SHM’s educational offerings through a variety of technologic venues. “In the coming year, our educational offerings will truly become multi-dimensional,” says Scott Johnson, SHM’s director of information services. “As we expand into audio CDs, podcasts, and Web-based offerings, more hospitalists will be able to take advantage of these learning opportunities, which will have profound effects on the hospital medicine movement.”
With the education plan approved by SHM’s Board of Directors at its recent meeting, the Education Committee, chaired by Preetha Basaviah, MD, from Stanford University, will turn its attention to the first stage of implementation—a complete needs analysis. Some research has already taken place as part of SHM’s ongoing internal quality improvement processes.
“The key to the success of our plan is that we will be integrating feedback from hospitalists throughout North America as we move forward,” says Dr. Basaviah. “Ultimately, this kind of communication will ensure that we reach our primary goal: to provide tools and resources that help hospital medicine professionals improve the quality of care that they provide.”
Stay tuned to The Hospitalist for updates on the committee’s progress and an advanced look at new educational products.
Palliative Care: a Core Competency for Hospitalists
By Theresa Kristopaitis, MD, with input from Howard Epstein, MD, and the SHM Palliative Care Task Force
Palliative care is focused on the relief of suffering and support for the best quality of life for patients facing serious, life-threatening, or advanced illness, as well as their families. Palliative care is a general approach to healthcare that should be routinely integrated with disease modifying therapies. It is also a growing practice specialty for appropriately trained healthcare professionals dedicating their practice to the delivery of palliative care services.1
Optimally palliative care is delivered through an interdisciplinary team consisting of physicians, nurses, chaplains, social workers, pharmacists, as well as other disciplines as patient/family needs warrant. Models of palliative care delivery include hospital-based inpatient consultation services, inpatient palliative care units, outpatient and home-based consultation services, and ambulatory clinics. Hospitalists are ideally positioned to start inpatient palliative care services and reap the professional and institutional benefits that palliative care offers. Tools to develop a program can be obtained through the Center to Advance Palliative Care (www.capc.org).
A Core Competency
The skills gained from developing expertise in palliative care are indispensable to hospitalists—even if they don’t formally work with a palliative care team. Palliative care itself is identified as a healthcare systems core competency of hospital medicine.2 In addition, other hospital medicine competencies overlap with those key to palliative care: pain management, care of the elderly patient and vulnerable populations, communication, hospitalist as consultant, team approach and multidisciplinary care, transitions of care, and medical ethics.3 For some of the most challenging, yet common, inpatient clinical scenarios, palliative care and hospital practice can become indistinguishable.
Inpatient Scenarios: How Can Palliative Care Help?
Scenario 1: A patient on chronic long-acting opiate therapy is admitted to the hospital with complaints of pain, nausea, and vomiting.
The appropriate assessment and management of pain is a patient’s right and an institution’s responsibility, yet it is often inadequate.4 Many barriers to effective pain management have been identified, including limited physician undergraduate and graduate training.4,5 A fundamental goal of palliative care is pain relief. In turn, expertise in the pathophysiology of pain and safe prescribing of opioid, non-opioid, and adjuvant analgesics is critical for palliative care physicians. Palliative care training and resources focus on principles of analgesic pharmacology, equianalgesia, changing routes of administration, control of continuous and breakthrough pain, opioid rotation, and adverse effects of analgesics. A comprehensive introduction to the fundamentals of pain management can be obtained via Education on Palliative and End of Life Care (www.epec.net.) Pain Management Module.
Non-pain symptoms can be as troubling for patients with advanced illness as pain. The formal assessment, reassessment, and management of common symptoms, including nausea, vomiting, dyspnea, constipation, fatigue, and delirium, are a primary domain of palliative medicine. Nausea and vomiting, for example, can become a demoralizing symptom complex. Stimuli to the vomiting center can arise from the cerebral cortex, vestibular apparatus, chemoreceptor zone, and gastrointestinal tract resulting in a broad etiologic differential diagnosis.
With a solid understanding of its pathogenesis and pharmacologic and non-pharmacologic therapeutic principles, nausea and vomiting can be treated in the vast majority of patients. Multiple agents addressing multiple mechanisms may be required. Even the nausea associated with complete bowel obstruction often can be successfully palliated, without the use of nasogastric tubes or surgery.6 The End of Life/Palliative Education Resource Center (www.eperc.mcw.edu) is one of many resources with tools to improve a hospitalist’s evaluation and treatment of non-pain physical symptoms.
Scenario 2: A patient with advanced heart failure and his family are overwhelmed by differing consultant opinions on the appropriateness of implantable cardioverter defibrillator (ICD) insertion.
Effective communication with patients is a core responsibility of both hospitalists and palliative care physicians. A complementary—and at times challenging—skill is the ability to promote communication and consensus about care among multiple specialist consultants. Ripamonti and colleagues write, “Almost invariably, the act of communication is an important part of therapy: Occasionally it is the only constituent. It usually requires greater thought and planning than a drug prescription, and unfortunately it is commonly administered in subtherapeutic doses.”6
The American Academy of Hospice and Palliative Medicine UNIPAC series is a resource for physicians to hone their general communication skills, as well as those more specific to palliative care, such as sharing news (often bad) with patients and families and engaging in therapeutic dialogue.8
Palliative care begins with establishing the goals of care with a patient.9 All physicians bring great value to patient care when they are skilled at negotiating goals of care. There are numerous possible goals of care, from prevention, to cure, to prolongation of life, to achieving a good death. Ideally, goals of care should be discussed with patients and families as early as possible in the course of a serious, life-threatening illness. Establishing realistic and attainable goals of care assumes increased importance in the setting of advanced disease, where treatments intended to prolong life may become more burdensome than beneficial.9
As the reader may have experienced, too often these discussions have not taken place or are held late in the trajectory of illness, such as when patients are hospitalized for severe progressive disease or are facing imminent death.10 In the scenario of potential ICD insertion, conversations with patients to clarify device-specific goals are best accomplished before they are placed and in the context of a broader discussion of the patient’s general medical condition and overall goals for care.11 This type of discussion ultimately improves the informed consent process for ICDs and other technologies. ICD recipients should be guided to periodically revisit their goals, particularly when their health status significantly changes.11 Unlike for initial ICD placement, there are no guidelines for disabling already implanted ICDs. The opportunity to discuss this issue with a patient before a crisis or before they lose decision-making capacity is frequently lost and occurs all too often at life’s end.12
Scenario 3: An elderly debilitated woman with advanced cervical cancer has been hospitalized six times in the past two months. She is cared for at home. Her family is tired but they are doing “the best they can.” She is brought to the emergency department again with weakness.
Effective implementation of care management strategies for patients with life-threatening and advanced disease requires assessment of their physical, social, emotional, and spiritual concerns.1 Similarly, family caregivers have their own—often unvoiced—biopsychosocial stressors.13 Physicians directing patient care must appreciate the significance of these multiple issues, even if they are not comfortable or are ill-equipped to handle them on their own. The power of the interdisciplinary palliative care model is that team members evaluate the patient from different perspectives and pool their expertise in addressing the complex needs of their patients and families.8
In some multidisciplinary models, the onus may lie on the physician to recognize the patient and family needs and mobilize the appropriate resources. Coordination of care at home for patients in the later stages of chronic illness may seem daunting during hospital stays. However, by employing measures utilized by palliative care teams, such as reviewing the goals of care, introducing community resources to help patients and families manage at home, providing anticipatory grief and bereavement support, and considering hospice referral, discharge planning and transitions in care can be much more sustainable.14 With these interventions, patients, families, physicians, and hospitals all benefit.
Conclusion
Hospital-based palliative care programs are growing exponentially.15 Hospitalists are in a unique position to continue their development. Even if the time or circumstances are not yet right for you to become a part of a formal palliative care program, there are daily opportunities to reap rewards from the knowledge, attitudes, and skills that palliative care training offers.
References
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available at www.nationalconsensusproject.org. Last accessed April 28, 2006.
- Pistoria MJ, Amin AN, Dressler DD, et al. The core competencies in hospital medicine. J Hosp Med. 2006;1:2(S1).
- American Board of Hospice and Palliative Medicine. Available at www.abhpm.org. Last accessed April 28, 2006.
- Phillips DM. JCAHO pain management standards unveiled. JAMA. 2000;284:428-429.
- Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-of-life care: a national report. J Gen Intern Med. 2003;18:685-695.
- Ripamonti C, De Conno F, Ventafridda V, et al. Management of bowel obstruction in advanced and terminal cancer patients. Ann Oncol. 1993 Jan;4(1):15-21.
- Buckman R. Communication in palliative care: a practical guide. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine. New York: Oxford Community Press; 1993:47-61.
- Storey P, Knight CF. UNIPAC five—caring for the terminally ill—communication and the physician’s role in the interdisciplinary team. In: Hospice/Palliative Care Training for Physicians—A Self Study Program. New York: Mary Ann Liebert; 2003:1-147.
- Morrison RS, Meier DE. Palliative care. NEJM. 2004;350:2582-2590.
- Quill TE. Initiating end of life discussion with seriously ill patients: addressing the “elephant in the room.” JAMA. 2000;284:2502-2507.
- Berger, JT. The ethics of deactivating implanted cardioverter defibrillators. Ann Intern Med. 2005;142:631-634.
- Goldstein NE, Lampert R, Bradely E, et al. Management of implantable cardioverter defibrillators in end-of-life care. Ann Intern Med. 2004;141:835-838.
- Levine C. The loneliness of the long-term caregiver. NEJM. 1999;340:1587-1590.
- Meier D. Palliative care in hospitals. J Hosp Med. 2006;1:21-28.
- Morrison RS, et al. The growth of palliative care programs in United States hospitals. J Pall Med. 2006; 8 (6):1127-1133.
Get a Job!
SHM Launches the first-ever career Web site exclusively for hospitalists
By Jeannette Wick
Job boards—Internet sites designed to allow employers and prospective employees to find each other electronically—are among the most active Internet sites. For many job seekers Monster.com, CareerBuilder.com, and Indeed.com (among others) have become essential job search tools. Until now, however, no site has catered to healthcare professionals in general—much less to hospitalists in particular.
Thanks to the new SHM Career Center (http://hospitalmedicine.org/careercenter), though, things are about to change. The Career Center is part of a comprehensive, “cradle-to-grave” approach SHM is taking to assist hospital medicine professionals in their career development pursuits. The site offers numerous advantages over traditional job-hunting tools, such as classified advertisements, personal contacts, and randomly mailing resumes to interesting employers—advantages such as the ability to post your resume in a searchable database, a database of open positions across North America that you can search using a variety of variables and the opportunity to receive a notification when a job that matches your criteria is posted online.
The Career Center also represents an improvement over general job boards because the pool of positions offered and solicited on the site is restricted to those only for hospital medicine professionals. The site is free for all, although SHM members are able to take advantage of certain “members-only” functionality (resume posting, e-mail notification of new job postings). “Career opportunists,” or hospitalists who are gainfully employed but constantly curious about what else is available, will enjoy this site, too.
The Way it Works
SHM’s Career Center matches applicants and jobs using search features that allow applicants to tailor their search. As an applicant, you enter your job preferences as you would when searching for an article in PubMed or when looking online for a board-certified specialist in a specific geographic region when referring a patient. The boxes prompt you to provide the minimum information necessary for an acceptable search. For example, you need to provide geographical preferences, the type of position you’re looking for, and the specialty area you’re interested in to best tailor your search.
Visitors can browse all jobs by specialty or state—or view the complete list of jobs. The advanced search option augments the specialty and state fields with the ability to specify keywords (see “Hospitalists and Keywords,” p. 10), specialty, employment type (full time, moonlighting, and so on), and the announcement opening date. (The latter is important to applicants who believe older announcements raise a red flag indicating conditions that make it unattractive to candidates.)
The advanced search option also allows you to look at job summaries with the results. So instead of receiving a simple list of the job title, the location, and the announcement date, the summary includes a short description of the position. But visitor beware: You have to click a box to make this happen. Otherwise, your search will create a simple list of jobs, and clicking on any individual job will bring up the job summary. The information is accessible either way.
Get Started
Most job seekers will find the site quite easy to navigate, although a few may be impeded by cookies. (For more information, see “Got Cookies,” p. 10.) The FAQ area is a site strength and will help you eliminate hurdles, from inability to navigate the site, to figuring out how to be notified electronically when new jobs are added.
Once you enter your search criteria, a list of jobs displays. Then click on a specific job to open another page describing the position in great detail. After seeing the array of positions available, SHM non-members are likely to join the society just to have access to the full functionality of the Career Center.
Your next step is to create an account; doing so allows you to apply for positions with just a click. Once you establish an account (a process that takes just a few minutes), click on “Edit My Profile.” In this area, you’ll establish your profile.
Meat and Potatoes: Post Your Resume
The Career Center’s features are state-of-the-art. You can create a resume and a cover letter. To post your resume in “My Account,” for example, select “Post My Resume,” then “Document Management,” and then “Resume.” You’ll need to open a plain text version (no bold, underlining, italics, or bullets) of your current resume on your computer, and then copy your resume to the clipboard.
Never done this before? Here again, you can open a guidance window or a printable FAQ to walk you through the process. Two minor system limitations appear here: You must click a box to make the text wrap automatically, and the site has no spell-check function. You have to spell check your cover letter and resume before you copy and paste. If you edit your text at any time while in the Career Center boxes, then be sure to proofread to ensure you haven’t introduced any errors. After you create your resume, you can open a text version (a file that ends in the suffix .txt) to see how employers will view it.
In the past, hospital medicine applicants could stand out with a well-formatted resume on quality paper. Online documents force every applicant’s information into the same mold, and this often concerns applicants. Will a skilled, tri-lingual, well-published hospitalist look like every other applicant when an employer is looking at a simple text version of your resume?
The Career Center allows you to upload up to three formatted documents that can be attached to applications. If you are unable to upload your documents, you may e-mail them to the site, which will then attach them to your account. Some applicants find it useful to have two specific types of resumes on hand: a traditional reverse chronological resume that emphasizes experience, and a less structured functional resume that describes transferable skills.
Depending on your computer savvy, the time it takes to set up your account and load your resume will vary. Hospitalists with robust skills may be able to load a resume in fewer than 30 minutes, but it may take longer for others. Regardless, the return on investment is large because the information you enter will form the foundation of your materials that a perspective employer will review. Once your resume is loaded, applying for a position only requires a few clicks.
Benefits That Make Your Search Sizzle
If you are an SHM member, the “Job Agent” functionality allows you to receive weekly updates of new jobs added that match your search criteria. (Note: You can join SHM online through the Career Center or by visiting www.joinshm.org) This function is located in your account. It allows you to specify the date you would like to stop receiving notification e-mails. Your account also tracks applications submitted.
After you log in, click “Job Applications” to display any jobs you have applied for and the date that the application was submitted. When a job posting expires (according to a pre-established date set by the employer) a strikethrough line will appear through the job application. Applications remain in your account for 90 days from the submission date. Clicking on the “Apply for this Job” icon opens a new screen, and it allows applicants to edit applications even after you’ve sent it and until the job posting closes. Once the job posting is closed, no application changes can be made.
Employers post their vacancies for 30 days at a time, and they can select packages that include print advertisements in The Hospitalist and/or the Journal of Hospital Medicine. Approximately 85% of employers who advertise in print media also advertise on the Career Center, although a few advertise only on the Career Center. To cover your bases, look in all three places.
Just as some applicants prefer anonymity, some companies choose to list their ads confidentially. In these cases, you will submit your online application, and the employer will contact you via the system with more information if you are a good match.
Employer responses will be forwarded to your e-mail account through the Career Center. Once you begin talking with a prospective employer, it is up to you to use good research and interview skills to ensure that this is indeed a good match. When you find a position, you can remove your resume from circulation. Or, you can store it in the Career Center database for future opportunities by clicking “No, do not post my resume.”
Alternatively, you can remove your information from the database permanently: Go to “My Account” and select “Delete Account.”
What the Future Holds
SHM’s information services team will keep tabs on the recently launched SHM Career Center Web site and invites user feedback—specifically any demographic information that will help them build the most practical, useful career site for hospitalists.
With the average age of a hospitalist about 37, SHM expects that visitors and users to comprise a youthful, computer savvy group. Eventually, SHM wants to expand the site so it tells you more than just what jobs are available (e.g., how to create a resume, interview techniques, and how to build desirable hospital medicine skill sets). They will also track how many employer-employee matches are made using the Career Center.
Conclusion
When unemployment is low, as it most certainly is for hospitalists, leverage rests with job seekers, not employers. While employers are looking for talent and availability, career opportunists crave convenience. The SHM Career Center represents the most comprehensive collection of hospitalist opportunities available on the Internet.
Users will find site navigation easy, and prompts and cues offered by the site designers clear and accurate. Traffic on the site is expected to grow quickly as it becomes what SHM hopes is the most indispensable tool for hospitalists conducting job searches.TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
SHM: BEHIND THE SCENES
Membership: Listen, Then Act
By Todd Von Deak

As I write this column, there are only seven days left before the start of this year’s annual meeting. At last check, more 1,100 hospital medicine professionals were registered to join us in Washington, D.C., for the most important meeting in hospital medicine. Our office is abuzz with activity and last minute preparations. I’m sure there’s something else that I’m supposed to be doing right now, but I need the break.
While I take my break and write, I can’t help but think, “what’s next,” once the Annual Meeting is over? SHM is fast approaching the start of a new fiscal year, and, like any membership director, I am eager to hit the ground running.
The more I reflect on what’s next, the more I realize that part of my answer lies within the pages of The Hospitalist. Our research continues to show that you consider The Hospitalist to be one of the most valuable benefits of membership.
What strikes me as I read through past issues is that we have another story to tell. So this month we’re launching “SHM: Behind the Scenes.”
There are many reasons why we need to share this story. Key to those reasons is the fact that our sole purpose is to serve the hospital medicine community. You entrust us with your dues and meeting registrations to provide resources that will enable you to better serve your patients and grow your careers in the process. So it’s important that we, the staff, tell you firsthand what we are doing with your investment, and how we plan on continuing to earn your trust in the years to come.
Each month a different member of our senior staff will take turns writing this column. During the coming year you’ll hear from the heads of education and quality initiatives, business operations, membership, information services, marketing, legislative affairs, and research. In each column you’ll find a mix of current news, future plans, and tips for maximizing the value of your membership. If we do our jobs correctly, each month you will have a clearer picture on the true return of your membership investment.
We want you to clearly understand why—if you only belong to one organization—it has to be SHM.
This month I’ll focus on membership and our plans for the coming year. (See below.) Next month you’ll hear from Scott Johnson, SHM’s director of information services. Scott is our chief technologist in many ways and is leading the charge to use today’s latest technology to expand the reach of our educational products and enhance your membership investment as well.
Each year, membership departments at non-profit organizations write their strategic plans for the coming year. SHM is no exception.
For most, these strategic plans are based on a set of assumptions. In more offices than you’d like to believe, the staff just sits around and makes their best guesses in order to answer critical questions, including “what do members want to get out of their membership?”
Based on these guesses, the staff then plots their course expansion and enhances the benefits and services that the organization offers. These organizations are doomed to mediocrity.
Successful organizations, including SHM, actively seek to better understand their membership and use a variety of media to get to the heart of the questions that matter. I am proud to say that SHM is among the second group.
Building on previous efforts, the SHM Membership Department has been actively engaged in a “listening tour.” Our goal is to not rely on assumptions but rather to use your feedback in formulating our plans for the coming year.
Here’s some of what we’ve identified.
Top reasons for being a member:
- Education and quality improvement resources;
- The ability to affect the hospital medicine movement; and
- Subscriptions to The Hospitalist and Journal of Hospital Medicine.
Your main goals as a member:
- To learn from educational and quality improvement resources;
- Take advantage of networking opportunities; and
- Gain exposure for career advancement.
The benefits of membership that matter most:
- Information on www.hospitalmedicine.org;
- Access to results from SHM’s “Authoritative Source on the State of the Hospital Medicine Movement;” and
- The Hospitalist.
We’re already using this data, along with other information that we’ve gathered, to enhance the SHM experience and increase the return on your investment. Just look at the new SHM Career Center (www.hospitalmedicine.org/careercenter).
Like any good membership department, we realize that our data collection has just begun. So I’d like to pose a couple of questions:
- Do you agree with our findings?
- Should we offer a new benefit of membership?
- What can we do to enhance your SHM experience?
I’d love to hear your thoughts. Send them to me via e-mail at tvondeak@hospitalmedicine.org. Anyone who e-mails will be entered in a prize drawing.
In my next column, I will share a selection of the responses I receive and tell you the concrete steps we’re taking to improve communication with you and other members.
Von Deak is SHM’s director of membership and marketing.
Each year a new team of SHM officers is elected to lend their wisdom, time, experience, and skills in a collaborative effort to help manage the business of our organization, drive new initiatives, and support the society’s mission. At this year’s annual meeting in Washington, D.C., we again witnessed that familiar changing of the guard with the following inductions:
- President Mary Jo Gorman, MD, MBA;
- President-Elect Russell Holman, MD;
- Treasurer Patrick Cawley, MD; and
- Secretary Jack Percelay, MD, MPH.
“Hospitalists are squarely in the spotlight today on key issues affecting patient care, quality of hospital care, hospital leadership, and other concerns. So it is important that we have a strong, hands-on leadership team that is committed to continuing the positive momentum SHM has generated for hospitalists,” says Larry Wellikson, MD, FACP, CEO of SHM. “I couldn’t be more thrilled with our slate of newly appointed officers. Time and again through the years Mary Jo, Rusty, Pat, and Jack have proven that they are active participants, and that they are leaders who will rise to the occasion to help us meet our objectives.”
Dr. Gorman, a charter member of SHM, has been a practicing hospitalist since 1997, when she founded the first hospitalist practice in St. Louis. In early 1999, her group merged into IPC—The Hospitalist Company and grew to become the dominant hospitalist group in the city. In 2001, Dr. Gorman was promoted to vice-president of medical affairs for IPC, responsible for the design and implementation of company-wide programs involving business development, recruitment, physician training, and operations in all of IPC’s markets. In 2003, she was named chief medical officer and today works with more than 300 physicians nationwide to develop programs and strategies that enhance clinical performance and drive the delivery system towards more efficient care and greater patient satisfaction. She also oversees IPC’s physician training, mentoring and retention programs, as well as IPC’s call center nurses, healthcare services and clinical studies.
A cum laude graduate of St. Louis University, Dr. Gorman earned a BA in Chemistry/Biology in 1981, then went on to earn her MD in 1984 from Southern Illinois University School of Medicine in Springfield. In 1996, she earned a MBA from Washington University, Olin School of Business, in St. Louis.
SHM’s new President-Elect Dr. Holman is senior vice president and national medical director for Cogent Healthcare, an organization that manages hospital medicine programs throughout the country. He is responsible for program implementation and management, quality systems reporting and auditing, physician leadership development, and data systems integration. Formerly, Dr. Holman was the medical director of Hospital Services for HealthPartners Medical Group & Clinics, part of HealthPartners, Inc. in Minnesota. There he also was the founder and director of the HPMG Fellowship Program in Hospital Medicine.
A long-time member of SHM, Dr. Holman served on the Board of Directors as treasurer from 2004-2005. He was previously chair of the Leadership Development Committee, chair of the Midwest Council, course director of the SHM Leadership Academy, and a member of the Public Policy Committee. In February 2006 he co-authored the “Update in Hospital Medicine,” which appeared in Annals of Internal Medicine. In 2002, he received the SHM Award for Outstanding Service in Hospital Medicine.
Through the years, Dr. Holman’s commitment to hospital medicine has helped produce nationally recognized standards in the areas of quality improvement activities, models of medical education, observation units, communication systems, compensation plans, case management, surgical co-management collaborations, and patient flow initiatives. Dr. Holman serves on two national editorial boards for medical publications and is currently co-authoring a comprehensive textbook and electronic decision support tool in hospital medicine.
Dr. Holman earned his MD from Washington University School of Medicine in St. Louis and trained as a resident and chief medical resident at the University of Minnesota in Minneapolis.
New Treasurer Dr. Cawley is a hospitalist at the Medical University of South Carolina in Charleston, where he currently serves as interim executive medical director of MUSC Medical Center. He previously served as the chief of the Section of Hospital Medicine, vice chairman of clinical affairs in the Department of Medicine, and associate executive medical director at MUSC Medical Center.
A charter member of SHM, Dr. Cawley has served on numerous committees and was previously secretary of the Board for the 2004-2005 term. He has worked in both academic and nonacademic hospitals and has served as a consultant to numerous hospitals in the development of hospital medicine programs.
Dr. Cawley received his Bachelor of Science in 1988 from the University of Scranton (Pa.) and his MD from Georgetown University School of Medicine in Washington, D.C. He completed an internal medicine residency at Duke University in Durham, N.C. Later this year, he will complete his MBA from the University of Massachusetts-Amherst.
SHM’s new secretary is Dr. Percelay. He is director of Virtua Inpatient Pediatrics, a large pediatric hospital medicine group in Southern New Jersey with 14 full-time hospitalists covering two hospitals. Since 1991, Dr. Percelay has worked in a variety of community-based settings including the general pediatric ward, pediatric sub-specialty units, pediatric intensive care unit (PICU), neonatal intensive care unit (NICU), and the emergency department.
A charter member of SHM and one of the nation’s first pediatric hospitalists, Dr. Percelay currently holds the Pediatric Seat on the SHM Board, in addition to serving on the Public Policy Committee and co-chairing the Pediatric Committee. He has been intimately involved in collaborative Pediatric hospital medicine projects such as the PRIS research network and the Denver 2005 and 2007 Pediatric Hospital Medicine conferences.
Dr. Percelay is also the founding chairperson and immediate past chair of the American Academy of Pediatrics Section on Hospital Medicine and co-authored the AAP policy statement on pediatric hospitalists. He completed his medical school and pediatric training at the University of California at San Francisco, along with an MPH at the University of California at Berkeley.
SHM congratulates these new officers and thanks our 2005 officers (Steve Pantilat, MD, president, William Atchley, MD, FACP, treasurer, and Lisa Kettering, MD, FACP, secretary) for their exemplary work.
Annual Meeting e-Community a Success
If the feedback from attendees at this year’s Annual Meeting was any indication, the inaugural launch of SHM’s Annual Meeting e-Community was a success.
Each year, SHM’s Annual Meeting provides an opportunity for hospital medicine professionals to network with colleagues and take advantage of more than 40 educational sessions during the course of three days.
While the location for the meeting changes regularly, there is a constant desire within the Annual Meeting planning committee (a group of volunteer members) to improve the attendee experience. The Annual Meeting e-Community (AMeC) was designed with that in mind.
The AMeC effectively extended the reach of the annual meeting both before and after the event. Since early April, attendees have been able to access the handouts for the presentations that were given at the event and network with colleagues thanks to dedicated discussion communities. There are also listings of exhibitors scheduled to be in attendance and general information about Washington, D.C., on the AMeC.
Because of the positive feedback received, the e-Community will stay online through early July, giving attendees the chance to download presentations from sessions that they didn’t attend and make contact with colleagues they met while in Washington, D.C.
Attendees appreciated the ability to access meeting materials prior to the event. “The Annual Meeting e-Community gave me a great opportunity to really plan out the sessions that I wanted to attend prior to the meeting,” says William Rifkin, MD, a hospitalist from the Yale School of Medicine.
According to Joy Wittnebert, AMeC project manager, the site was launched in response to feedback from past annual meetings. “Attendees have been consistently telling us that they want to be able to customize their experience and have more opportunities to network with colleagues before and after the event,” she says.
In the coming months, SHM staff will work with the Annual Meeting Committee to analyze additional feedback and begin making plans for the 2007 version of the site.
SHM Education Committee Launches 18-Month Strategic Plan
Helping our members and the hospital medicine community advance in professional growth and development has been on center stage as seen in the SHM Education Committee’s recent completion of an 18-month strategic plan. The plan is a framework designed to guide staff and volunteer leadership as they work to expand the society’s current slate of educational offerings. Inherent in the framework’s design is a focus on taking advantage of the myriad new channels that have come online for delivering educational content.
The plan is rooted primarily in the recently released Core Competencies in Hospital Medicine. The Core Competencies are a benchmark for the development of curricula within the hospital medicine specialty.
“One of the most exciting parts of this plan is its connection to the Core Competencies,” says Geri Barnes, SHM’s director of education and quality initiatives. “The connection means that this is one of the strongest educational plans that the society has put forward.”
A driving force in the creation of this plan was the committee’s desire to expand SHM’s educational offerings through a variety of technologic venues. “In the coming year, our educational offerings will truly become multi-dimensional,” says Scott Johnson, SHM’s director of information services. “As we expand into audio CDs, podcasts, and Web-based offerings, more hospitalists will be able to take advantage of these learning opportunities, which will have profound effects on the hospital medicine movement.”
With the education plan approved by SHM’s Board of Directors at its recent meeting, the Education Committee, chaired by Preetha Basaviah, MD, from Stanford University, will turn its attention to the first stage of implementation—a complete needs analysis. Some research has already taken place as part of SHM’s ongoing internal quality improvement processes.
“The key to the success of our plan is that we will be integrating feedback from hospitalists throughout North America as we move forward,” says Dr. Basaviah. “Ultimately, this kind of communication will ensure that we reach our primary goal: to provide tools and resources that help hospital medicine professionals improve the quality of care that they provide.”
Stay tuned to The Hospitalist for updates on the committee’s progress and an advanced look at new educational products.
Palliative Care: a Core Competency for Hospitalists
By Theresa Kristopaitis, MD, with input from Howard Epstein, MD, and the SHM Palliative Care Task Force
Palliative care is focused on the relief of suffering and support for the best quality of life for patients facing serious, life-threatening, or advanced illness, as well as their families. Palliative care is a general approach to healthcare that should be routinely integrated with disease modifying therapies. It is also a growing practice specialty for appropriately trained healthcare professionals dedicating their practice to the delivery of palliative care services.1
Optimally palliative care is delivered through an interdisciplinary team consisting of physicians, nurses, chaplains, social workers, pharmacists, as well as other disciplines as patient/family needs warrant. Models of palliative care delivery include hospital-based inpatient consultation services, inpatient palliative care units, outpatient and home-based consultation services, and ambulatory clinics. Hospitalists are ideally positioned to start inpatient palliative care services and reap the professional and institutional benefits that palliative care offers. Tools to develop a program can be obtained through the Center to Advance Palliative Care (www.capc.org).
A Core Competency
The skills gained from developing expertise in palliative care are indispensable to hospitalists—even if they don’t formally work with a palliative care team. Palliative care itself is identified as a healthcare systems core competency of hospital medicine.2 In addition, other hospital medicine competencies overlap with those key to palliative care: pain management, care of the elderly patient and vulnerable populations, communication, hospitalist as consultant, team approach and multidisciplinary care, transitions of care, and medical ethics.3 For some of the most challenging, yet common, inpatient clinical scenarios, palliative care and hospital practice can become indistinguishable.
Inpatient Scenarios: How Can Palliative Care Help?
Scenario 1: A patient on chronic long-acting opiate therapy is admitted to the hospital with complaints of pain, nausea, and vomiting.
The appropriate assessment and management of pain is a patient’s right and an institution’s responsibility, yet it is often inadequate.4 Many barriers to effective pain management have been identified, including limited physician undergraduate and graduate training.4,5 A fundamental goal of palliative care is pain relief. In turn, expertise in the pathophysiology of pain and safe prescribing of opioid, non-opioid, and adjuvant analgesics is critical for palliative care physicians. Palliative care training and resources focus on principles of analgesic pharmacology, equianalgesia, changing routes of administration, control of continuous and breakthrough pain, opioid rotation, and adverse effects of analgesics. A comprehensive introduction to the fundamentals of pain management can be obtained via Education on Palliative and End of Life Care (www.epec.net.) Pain Management Module.
Non-pain symptoms can be as troubling for patients with advanced illness as pain. The formal assessment, reassessment, and management of common symptoms, including nausea, vomiting, dyspnea, constipation, fatigue, and delirium, are a primary domain of palliative medicine. Nausea and vomiting, for example, can become a demoralizing symptom complex. Stimuli to the vomiting center can arise from the cerebral cortex, vestibular apparatus, chemoreceptor zone, and gastrointestinal tract resulting in a broad etiologic differential diagnosis.
With a solid understanding of its pathogenesis and pharmacologic and non-pharmacologic therapeutic principles, nausea and vomiting can be treated in the vast majority of patients. Multiple agents addressing multiple mechanisms may be required. Even the nausea associated with complete bowel obstruction often can be successfully palliated, without the use of nasogastric tubes or surgery.6 The End of Life/Palliative Education Resource Center (www.eperc.mcw.edu) is one of many resources with tools to improve a hospitalist’s evaluation and treatment of non-pain physical symptoms.
Scenario 2: A patient with advanced heart failure and his family are overwhelmed by differing consultant opinions on the appropriateness of implantable cardioverter defibrillator (ICD) insertion.
Effective communication with patients is a core responsibility of both hospitalists and palliative care physicians. A complementary—and at times challenging—skill is the ability to promote communication and consensus about care among multiple specialist consultants. Ripamonti and colleagues write, “Almost invariably, the act of communication is an important part of therapy: Occasionally it is the only constituent. It usually requires greater thought and planning than a drug prescription, and unfortunately it is commonly administered in subtherapeutic doses.”6
The American Academy of Hospice and Palliative Medicine UNIPAC series is a resource for physicians to hone their general communication skills, as well as those more specific to palliative care, such as sharing news (often bad) with patients and families and engaging in therapeutic dialogue.8
Palliative care begins with establishing the goals of care with a patient.9 All physicians bring great value to patient care when they are skilled at negotiating goals of care. There are numerous possible goals of care, from prevention, to cure, to prolongation of life, to achieving a good death. Ideally, goals of care should be discussed with patients and families as early as possible in the course of a serious, life-threatening illness. Establishing realistic and attainable goals of care assumes increased importance in the setting of advanced disease, where treatments intended to prolong life may become more burdensome than beneficial.9
As the reader may have experienced, too often these discussions have not taken place or are held late in the trajectory of illness, such as when patients are hospitalized for severe progressive disease or are facing imminent death.10 In the scenario of potential ICD insertion, conversations with patients to clarify device-specific goals are best accomplished before they are placed and in the context of a broader discussion of the patient’s general medical condition and overall goals for care.11 This type of discussion ultimately improves the informed consent process for ICDs and other technologies. ICD recipients should be guided to periodically revisit their goals, particularly when their health status significantly changes.11 Unlike for initial ICD placement, there are no guidelines for disabling already implanted ICDs. The opportunity to discuss this issue with a patient before a crisis or before they lose decision-making capacity is frequently lost and occurs all too often at life’s end.12
Scenario 3: An elderly debilitated woman with advanced cervical cancer has been hospitalized six times in the past two months. She is cared for at home. Her family is tired but they are doing “the best they can.” She is brought to the emergency department again with weakness.
Effective implementation of care management strategies for patients with life-threatening and advanced disease requires assessment of their physical, social, emotional, and spiritual concerns.1 Similarly, family caregivers have their own—often unvoiced—biopsychosocial stressors.13 Physicians directing patient care must appreciate the significance of these multiple issues, even if they are not comfortable or are ill-equipped to handle them on their own. The power of the interdisciplinary palliative care model is that team members evaluate the patient from different perspectives and pool their expertise in addressing the complex needs of their patients and families.8
In some multidisciplinary models, the onus may lie on the physician to recognize the patient and family needs and mobilize the appropriate resources. Coordination of care at home for patients in the later stages of chronic illness may seem daunting during hospital stays. However, by employing measures utilized by palliative care teams, such as reviewing the goals of care, introducing community resources to help patients and families manage at home, providing anticipatory grief and bereavement support, and considering hospice referral, discharge planning and transitions in care can be much more sustainable.14 With these interventions, patients, families, physicians, and hospitals all benefit.
Conclusion
Hospital-based palliative care programs are growing exponentially.15 Hospitalists are in a unique position to continue their development. Even if the time or circumstances are not yet right for you to become a part of a formal palliative care program, there are daily opportunities to reap rewards from the knowledge, attitudes, and skills that palliative care training offers.
References
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available at www.nationalconsensusproject.org. Last accessed April 28, 2006.
- Pistoria MJ, Amin AN, Dressler DD, et al. The core competencies in hospital medicine. J Hosp Med. 2006;1:2(S1).
- American Board of Hospice and Palliative Medicine. Available at www.abhpm.org. Last accessed April 28, 2006.
- Phillips DM. JCAHO pain management standards unveiled. JAMA. 2000;284:428-429.
- Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-of-life care: a national report. J Gen Intern Med. 2003;18:685-695.
- Ripamonti C, De Conno F, Ventafridda V, et al. Management of bowel obstruction in advanced and terminal cancer patients. Ann Oncol. 1993 Jan;4(1):15-21.
- Buckman R. Communication in palliative care: a practical guide. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine. New York: Oxford Community Press; 1993:47-61.
- Storey P, Knight CF. UNIPAC five—caring for the terminally ill—communication and the physician’s role in the interdisciplinary team. In: Hospice/Palliative Care Training for Physicians—A Self Study Program. New York: Mary Ann Liebert; 2003:1-147.
- Morrison RS, Meier DE. Palliative care. NEJM. 2004;350:2582-2590.
- Quill TE. Initiating end of life discussion with seriously ill patients: addressing the “elephant in the room.” JAMA. 2000;284:2502-2507.
- Berger, JT. The ethics of deactivating implanted cardioverter defibrillators. Ann Intern Med. 2005;142:631-634.
- Goldstein NE, Lampert R, Bradely E, et al. Management of implantable cardioverter defibrillators in end-of-life care. Ann Intern Med. 2004;141:835-838.
- Levine C. The loneliness of the long-term caregiver. NEJM. 1999;340:1587-1590.
- Meier D. Palliative care in hospitals. J Hosp Med. 2006;1:21-28.
- Morrison RS, et al. The growth of palliative care programs in United States hospitals. J Pall Med. 2006; 8 (6):1127-1133.
Get a Job!
SHM Launches the first-ever career Web site exclusively for hospitalists
By Jeannette Wick
Job boards—Internet sites designed to allow employers and prospective employees to find each other electronically—are among the most active Internet sites. For many job seekers Monster.com, CareerBuilder.com, and Indeed.com (among others) have become essential job search tools. Until now, however, no site has catered to healthcare professionals in general—much less to hospitalists in particular.
Thanks to the new SHM Career Center (http://hospitalmedicine.org/careercenter), though, things are about to change. The Career Center is part of a comprehensive, “cradle-to-grave” approach SHM is taking to assist hospital medicine professionals in their career development pursuits. The site offers numerous advantages over traditional job-hunting tools, such as classified advertisements, personal contacts, and randomly mailing resumes to interesting employers—advantages such as the ability to post your resume in a searchable database, a database of open positions across North America that you can search using a variety of variables and the opportunity to receive a notification when a job that matches your criteria is posted online.
The Career Center also represents an improvement over general job boards because the pool of positions offered and solicited on the site is restricted to those only for hospital medicine professionals. The site is free for all, although SHM members are able to take advantage of certain “members-only” functionality (resume posting, e-mail notification of new job postings). “Career opportunists,” or hospitalists who are gainfully employed but constantly curious about what else is available, will enjoy this site, too.
The Way it Works
SHM’s Career Center matches applicants and jobs using search features that allow applicants to tailor their search. As an applicant, you enter your job preferences as you would when searching for an article in PubMed or when looking online for a board-certified specialist in a specific geographic region when referring a patient. The boxes prompt you to provide the minimum information necessary for an acceptable search. For example, you need to provide geographical preferences, the type of position you’re looking for, and the specialty area you’re interested in to best tailor your search.
Visitors can browse all jobs by specialty or state—or view the complete list of jobs. The advanced search option augments the specialty and state fields with the ability to specify keywords (see “Hospitalists and Keywords,” p. 10), specialty, employment type (full time, moonlighting, and so on), and the announcement opening date. (The latter is important to applicants who believe older announcements raise a red flag indicating conditions that make it unattractive to candidates.)
The advanced search option also allows you to look at job summaries with the results. So instead of receiving a simple list of the job title, the location, and the announcement date, the summary includes a short description of the position. But visitor beware: You have to click a box to make this happen. Otherwise, your search will create a simple list of jobs, and clicking on any individual job will bring up the job summary. The information is accessible either way.
Get Started
Most job seekers will find the site quite easy to navigate, although a few may be impeded by cookies. (For more information, see “Got Cookies,” p. 10.) The FAQ area is a site strength and will help you eliminate hurdles, from inability to navigate the site, to figuring out how to be notified electronically when new jobs are added.
Once you enter your search criteria, a list of jobs displays. Then click on a specific job to open another page describing the position in great detail. After seeing the array of positions available, SHM non-members are likely to join the society just to have access to the full functionality of the Career Center.
Your next step is to create an account; doing so allows you to apply for positions with just a click. Once you establish an account (a process that takes just a few minutes), click on “Edit My Profile.” In this area, you’ll establish your profile.
Meat and Potatoes: Post Your Resume
The Career Center’s features are state-of-the-art. You can create a resume and a cover letter. To post your resume in “My Account,” for example, select “Post My Resume,” then “Document Management,” and then “Resume.” You’ll need to open a plain text version (no bold, underlining, italics, or bullets) of your current resume on your computer, and then copy your resume to the clipboard.
Never done this before? Here again, you can open a guidance window or a printable FAQ to walk you through the process. Two minor system limitations appear here: You must click a box to make the text wrap automatically, and the site has no spell-check function. You have to spell check your cover letter and resume before you copy and paste. If you edit your text at any time while in the Career Center boxes, then be sure to proofread to ensure you haven’t introduced any errors. After you create your resume, you can open a text version (a file that ends in the suffix .txt) to see how employers will view it.
In the past, hospital medicine applicants could stand out with a well-formatted resume on quality paper. Online documents force every applicant’s information into the same mold, and this often concerns applicants. Will a skilled, tri-lingual, well-published hospitalist look like every other applicant when an employer is looking at a simple text version of your resume?
The Career Center allows you to upload up to three formatted documents that can be attached to applications. If you are unable to upload your documents, you may e-mail them to the site, which will then attach them to your account. Some applicants find it useful to have two specific types of resumes on hand: a traditional reverse chronological resume that emphasizes experience, and a less structured functional resume that describes transferable skills.
Depending on your computer savvy, the time it takes to set up your account and load your resume will vary. Hospitalists with robust skills may be able to load a resume in fewer than 30 minutes, but it may take longer for others. Regardless, the return on investment is large because the information you enter will form the foundation of your materials that a perspective employer will review. Once your resume is loaded, applying for a position only requires a few clicks.
Benefits That Make Your Search Sizzle
If you are an SHM member, the “Job Agent” functionality allows you to receive weekly updates of new jobs added that match your search criteria. (Note: You can join SHM online through the Career Center or by visiting www.joinshm.org) This function is located in your account. It allows you to specify the date you would like to stop receiving notification e-mails. Your account also tracks applications submitted.
After you log in, click “Job Applications” to display any jobs you have applied for and the date that the application was submitted. When a job posting expires (according to a pre-established date set by the employer) a strikethrough line will appear through the job application. Applications remain in your account for 90 days from the submission date. Clicking on the “Apply for this Job” icon opens a new screen, and it allows applicants to edit applications even after you’ve sent it and until the job posting closes. Once the job posting is closed, no application changes can be made.
Employers post their vacancies for 30 days at a time, and they can select packages that include print advertisements in The Hospitalist and/or the Journal of Hospital Medicine. Approximately 85% of employers who advertise in print media also advertise on the Career Center, although a few advertise only on the Career Center. To cover your bases, look in all three places.
Just as some applicants prefer anonymity, some companies choose to list their ads confidentially. In these cases, you will submit your online application, and the employer will contact you via the system with more information if you are a good match.
Employer responses will be forwarded to your e-mail account through the Career Center. Once you begin talking with a prospective employer, it is up to you to use good research and interview skills to ensure that this is indeed a good match. When you find a position, you can remove your resume from circulation. Or, you can store it in the Career Center database for future opportunities by clicking “No, do not post my resume.”
Alternatively, you can remove your information from the database permanently: Go to “My Account” and select “Delete Account.”
What the Future Holds
SHM’s information services team will keep tabs on the recently launched SHM Career Center Web site and invites user feedback—specifically any demographic information that will help them build the most practical, useful career site for hospitalists.
With the average age of a hospitalist about 37, SHM expects that visitors and users to comprise a youthful, computer savvy group. Eventually, SHM wants to expand the site so it tells you more than just what jobs are available (e.g., how to create a resume, interview techniques, and how to build desirable hospital medicine skill sets). They will also track how many employer-employee matches are made using the Career Center.
Conclusion
When unemployment is low, as it most certainly is for hospitalists, leverage rests with job seekers, not employers. While employers are looking for talent and availability, career opportunists crave convenience. The SHM Career Center represents the most comprehensive collection of hospitalist opportunities available on the Internet.
Users will find site navigation easy, and prompts and cues offered by the site designers clear and accurate. Traffic on the site is expected to grow quickly as it becomes what SHM hopes is the most indispensable tool for hospitalists conducting job searches.TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
SHM: BEHIND THE SCENES
Membership: Listen, Then Act
By Todd Von Deak
As I write this column, there are only seven days left before the start of this year’s annual meeting. At last check, more 1,100 hospital medicine professionals were registered to join us in Washington, D.C., for the most important meeting in hospital medicine. Our office is abuzz with activity and last minute preparations. I’m sure there’s something else that I’m supposed to be doing right now, but I need the break.
While I take my break and write, I can’t help but think, “what’s next,” once the Annual Meeting is over? SHM is fast approaching the start of a new fiscal year, and, like any membership director, I am eager to hit the ground running.
The more I reflect on what’s next, the more I realize that part of my answer lies within the pages of The Hospitalist. Our research continues to show that you consider The Hospitalist to be one of the most valuable benefits of membership.
What strikes me as I read through past issues is that we have another story to tell. So this month we’re launching “SHM: Behind the Scenes.”
There are many reasons why we need to share this story. Key to those reasons is the fact that our sole purpose is to serve the hospital medicine community. You entrust us with your dues and meeting registrations to provide resources that will enable you to better serve your patients and grow your careers in the process. So it’s important that we, the staff, tell you firsthand what we are doing with your investment, and how we plan on continuing to earn your trust in the years to come.
Each month a different member of our senior staff will take turns writing this column. During the coming year you’ll hear from the heads of education and quality initiatives, business operations, membership, information services, marketing, legislative affairs, and research. In each column you’ll find a mix of current news, future plans, and tips for maximizing the value of your membership. If we do our jobs correctly, each month you will have a clearer picture on the true return of your membership investment.
We want you to clearly understand why—if you only belong to one organization—it has to be SHM.
This month I’ll focus on membership and our plans for the coming year. (See below.) Next month you’ll hear from Scott Johnson, SHM’s director of information services. Scott is our chief technologist in many ways and is leading the charge to use today’s latest technology to expand the reach of our educational products and enhance your membership investment as well.
Each year, membership departments at non-profit organizations write their strategic plans for the coming year. SHM is no exception.
For most, these strategic plans are based on a set of assumptions. In more offices than you’d like to believe, the staff just sits around and makes their best guesses in order to answer critical questions, including “what do members want to get out of their membership?”
Based on these guesses, the staff then plots their course expansion and enhances the benefits and services that the organization offers. These organizations are doomed to mediocrity.
Successful organizations, including SHM, actively seek to better understand their membership and use a variety of media to get to the heart of the questions that matter. I am proud to say that SHM is among the second group.
Building on previous efforts, the SHM Membership Department has been actively engaged in a “listening tour.” Our goal is to not rely on assumptions but rather to use your feedback in formulating our plans for the coming year.
Here’s some of what we’ve identified.
Top reasons for being a member:
- Education and quality improvement resources;
- The ability to affect the hospital medicine movement; and
- Subscriptions to The Hospitalist and Journal of Hospital Medicine.
Your main goals as a member:
- To learn from educational and quality improvement resources;
- Take advantage of networking opportunities; and
- Gain exposure for career advancement.
The benefits of membership that matter most:
- Information on www.hospitalmedicine.org;
- Access to results from SHM’s “Authoritative Source on the State of the Hospital Medicine Movement;” and
- The Hospitalist.
We’re already using this data, along with other information that we’ve gathered, to enhance the SHM experience and increase the return on your investment. Just look at the new SHM Career Center (www.hospitalmedicine.org/careercenter).
Like any good membership department, we realize that our data collection has just begun. So I’d like to pose a couple of questions:
- Do you agree with our findings?
- Should we offer a new benefit of membership?
- What can we do to enhance your SHM experience?
I’d love to hear your thoughts. Send them to me via e-mail at tvondeak@hospitalmedicine.org. Anyone who e-mails will be entered in a prize drawing.
In my next column, I will share a selection of the responses I receive and tell you the concrete steps we’re taking to improve communication with you and other members.
Von Deak is SHM’s director of membership and marketing.
Each year a new team of SHM officers is elected to lend their wisdom, time, experience, and skills in a collaborative effort to help manage the business of our organization, drive new initiatives, and support the society’s mission. At this year’s annual meeting in Washington, D.C., we again witnessed that familiar changing of the guard with the following inductions:
- President Mary Jo Gorman, MD, MBA;
- President-Elect Russell Holman, MD;
- Treasurer Patrick Cawley, MD; and
- Secretary Jack Percelay, MD, MPH.
“Hospitalists are squarely in the spotlight today on key issues affecting patient care, quality of hospital care, hospital leadership, and other concerns. So it is important that we have a strong, hands-on leadership team that is committed to continuing the positive momentum SHM has generated for hospitalists,” says Larry Wellikson, MD, FACP, CEO of SHM. “I couldn’t be more thrilled with our slate of newly appointed officers. Time and again through the years Mary Jo, Rusty, Pat, and Jack have proven that they are active participants, and that they are leaders who will rise to the occasion to help us meet our objectives.”
Dr. Gorman, a charter member of SHM, has been a practicing hospitalist since 1997, when she founded the first hospitalist practice in St. Louis. In early 1999, her group merged into IPC—The Hospitalist Company and grew to become the dominant hospitalist group in the city. In 2001, Dr. Gorman was promoted to vice-president of medical affairs for IPC, responsible for the design and implementation of company-wide programs involving business development, recruitment, physician training, and operations in all of IPC’s markets. In 2003, she was named chief medical officer and today works with more than 300 physicians nationwide to develop programs and strategies that enhance clinical performance and drive the delivery system towards more efficient care and greater patient satisfaction. She also oversees IPC’s physician training, mentoring and retention programs, as well as IPC’s call center nurses, healthcare services and clinical studies.
A cum laude graduate of St. Louis University, Dr. Gorman earned a BA in Chemistry/Biology in 1981, then went on to earn her MD in 1984 from Southern Illinois University School of Medicine in Springfield. In 1996, she earned a MBA from Washington University, Olin School of Business, in St. Louis.
SHM’s new President-Elect Dr. Holman is senior vice president and national medical director for Cogent Healthcare, an organization that manages hospital medicine programs throughout the country. He is responsible for program implementation and management, quality systems reporting and auditing, physician leadership development, and data systems integration. Formerly, Dr. Holman was the medical director of Hospital Services for HealthPartners Medical Group & Clinics, part of HealthPartners, Inc. in Minnesota. There he also was the founder and director of the HPMG Fellowship Program in Hospital Medicine.
A long-time member of SHM, Dr. Holman served on the Board of Directors as treasurer from 2004-2005. He was previously chair of the Leadership Development Committee, chair of the Midwest Council, course director of the SHM Leadership Academy, and a member of the Public Policy Committee. In February 2006 he co-authored the “Update in Hospital Medicine,” which appeared in Annals of Internal Medicine. In 2002, he received the SHM Award for Outstanding Service in Hospital Medicine.
Through the years, Dr. Holman’s commitment to hospital medicine has helped produce nationally recognized standards in the areas of quality improvement activities, models of medical education, observation units, communication systems, compensation plans, case management, surgical co-management collaborations, and patient flow initiatives. Dr. Holman serves on two national editorial boards for medical publications and is currently co-authoring a comprehensive textbook and electronic decision support tool in hospital medicine.
Dr. Holman earned his MD from Washington University School of Medicine in St. Louis and trained as a resident and chief medical resident at the University of Minnesota in Minneapolis.
New Treasurer Dr. Cawley is a hospitalist at the Medical University of South Carolina in Charleston, where he currently serves as interim executive medical director of MUSC Medical Center. He previously served as the chief of the Section of Hospital Medicine, vice chairman of clinical affairs in the Department of Medicine, and associate executive medical director at MUSC Medical Center.
A charter member of SHM, Dr. Cawley has served on numerous committees and was previously secretary of the Board for the 2004-2005 term. He has worked in both academic and nonacademic hospitals and has served as a consultant to numerous hospitals in the development of hospital medicine programs.
Dr. Cawley received his Bachelor of Science in 1988 from the University of Scranton (Pa.) and his MD from Georgetown University School of Medicine in Washington, D.C. He completed an internal medicine residency at Duke University in Durham, N.C. Later this year, he will complete his MBA from the University of Massachusetts-Amherst.
SHM’s new secretary is Dr. Percelay. He is director of Virtua Inpatient Pediatrics, a large pediatric hospital medicine group in Southern New Jersey with 14 full-time hospitalists covering two hospitals. Since 1991, Dr. Percelay has worked in a variety of community-based settings including the general pediatric ward, pediatric sub-specialty units, pediatric intensive care unit (PICU), neonatal intensive care unit (NICU), and the emergency department.
A charter member of SHM and one of the nation’s first pediatric hospitalists, Dr. Percelay currently holds the Pediatric Seat on the SHM Board, in addition to serving on the Public Policy Committee and co-chairing the Pediatric Committee. He has been intimately involved in collaborative Pediatric hospital medicine projects such as the PRIS research network and the Denver 2005 and 2007 Pediatric Hospital Medicine conferences.
Dr. Percelay is also the founding chairperson and immediate past chair of the American Academy of Pediatrics Section on Hospital Medicine and co-authored the AAP policy statement on pediatric hospitalists. He completed his medical school and pediatric training at the University of California at San Francisco, along with an MPH at the University of California at Berkeley.
SHM congratulates these new officers and thanks our 2005 officers (Steve Pantilat, MD, president, William Atchley, MD, FACP, treasurer, and Lisa Kettering, MD, FACP, secretary) for their exemplary work.
Annual Meeting e-Community a Success
If the feedback from attendees at this year’s Annual Meeting was any indication, the inaugural launch of SHM’s Annual Meeting e-Community was a success.
Each year, SHM’s Annual Meeting provides an opportunity for hospital medicine professionals to network with colleagues and take advantage of more than 40 educational sessions during the course of three days.
While the location for the meeting changes regularly, there is a constant desire within the Annual Meeting planning committee (a group of volunteer members) to improve the attendee experience. The Annual Meeting e-Community (AMeC) was designed with that in mind.
The AMeC effectively extended the reach of the annual meeting both before and after the event. Since early April, attendees have been able to access the handouts for the presentations that were given at the event and network with colleagues thanks to dedicated discussion communities. There are also listings of exhibitors scheduled to be in attendance and general information about Washington, D.C., on the AMeC.
Because of the positive feedback received, the e-Community will stay online through early July, giving attendees the chance to download presentations from sessions that they didn’t attend and make contact with colleagues they met while in Washington, D.C.
Attendees appreciated the ability to access meeting materials prior to the event. “The Annual Meeting e-Community gave me a great opportunity to really plan out the sessions that I wanted to attend prior to the meeting,” says William Rifkin, MD, a hospitalist from the Yale School of Medicine.
According to Joy Wittnebert, AMeC project manager, the site was launched in response to feedback from past annual meetings. “Attendees have been consistently telling us that they want to be able to customize their experience and have more opportunities to network with colleagues before and after the event,” she says.
In the coming months, SHM staff will work with the Annual Meeting Committee to analyze additional feedback and begin making plans for the 2007 version of the site.
SHM Education Committee Launches 18-Month Strategic Plan
Helping our members and the hospital medicine community advance in professional growth and development has been on center stage as seen in the SHM Education Committee’s recent completion of an 18-month strategic plan. The plan is a framework designed to guide staff and volunteer leadership as they work to expand the society’s current slate of educational offerings. Inherent in the framework’s design is a focus on taking advantage of the myriad new channels that have come online for delivering educational content.
The plan is rooted primarily in the recently released Core Competencies in Hospital Medicine. The Core Competencies are a benchmark for the development of curricula within the hospital medicine specialty.
“One of the most exciting parts of this plan is its connection to the Core Competencies,” says Geri Barnes, SHM’s director of education and quality initiatives. “The connection means that this is one of the strongest educational plans that the society has put forward.”
A driving force in the creation of this plan was the committee’s desire to expand SHM’s educational offerings through a variety of technologic venues. “In the coming year, our educational offerings will truly become multi-dimensional,” says Scott Johnson, SHM’s director of information services. “As we expand into audio CDs, podcasts, and Web-based offerings, more hospitalists will be able to take advantage of these learning opportunities, which will have profound effects on the hospital medicine movement.”
With the education plan approved by SHM’s Board of Directors at its recent meeting, the Education Committee, chaired by Preetha Basaviah, MD, from Stanford University, will turn its attention to the first stage of implementation—a complete needs analysis. Some research has already taken place as part of SHM’s ongoing internal quality improvement processes.
“The key to the success of our plan is that we will be integrating feedback from hospitalists throughout North America as we move forward,” says Dr. Basaviah. “Ultimately, this kind of communication will ensure that we reach our primary goal: to provide tools and resources that help hospital medicine professionals improve the quality of care that they provide.”
Stay tuned to The Hospitalist for updates on the committee’s progress and an advanced look at new educational products.
Palliative Care: a Core Competency for Hospitalists
By Theresa Kristopaitis, MD, with input from Howard Epstein, MD, and the SHM Palliative Care Task Force
Palliative care is focused on the relief of suffering and support for the best quality of life for patients facing serious, life-threatening, or advanced illness, as well as their families. Palliative care is a general approach to healthcare that should be routinely integrated with disease modifying therapies. It is also a growing practice specialty for appropriately trained healthcare professionals dedicating their practice to the delivery of palliative care services.1
Optimally palliative care is delivered through an interdisciplinary team consisting of physicians, nurses, chaplains, social workers, pharmacists, as well as other disciplines as patient/family needs warrant. Models of palliative care delivery include hospital-based inpatient consultation services, inpatient palliative care units, outpatient and home-based consultation services, and ambulatory clinics. Hospitalists are ideally positioned to start inpatient palliative care services and reap the professional and institutional benefits that palliative care offers. Tools to develop a program can be obtained through the Center to Advance Palliative Care (www.capc.org).
A Core Competency
The skills gained from developing expertise in palliative care are indispensable to hospitalists—even if they don’t formally work with a palliative care team. Palliative care itself is identified as a healthcare systems core competency of hospital medicine.2 In addition, other hospital medicine competencies overlap with those key to palliative care: pain management, care of the elderly patient and vulnerable populations, communication, hospitalist as consultant, team approach and multidisciplinary care, transitions of care, and medical ethics.3 For some of the most challenging, yet common, inpatient clinical scenarios, palliative care and hospital practice can become indistinguishable.
Inpatient Scenarios: How Can Palliative Care Help?
Scenario 1: A patient on chronic long-acting opiate therapy is admitted to the hospital with complaints of pain, nausea, and vomiting.
The appropriate assessment and management of pain is a patient’s right and an institution’s responsibility, yet it is often inadequate.4 Many barriers to effective pain management have been identified, including limited physician undergraduate and graduate training.4,5 A fundamental goal of palliative care is pain relief. In turn, expertise in the pathophysiology of pain and safe prescribing of opioid, non-opioid, and adjuvant analgesics is critical for palliative care physicians. Palliative care training and resources focus on principles of analgesic pharmacology, equianalgesia, changing routes of administration, control of continuous and breakthrough pain, opioid rotation, and adverse effects of analgesics. A comprehensive introduction to the fundamentals of pain management can be obtained via Education on Palliative and End of Life Care (www.epec.net.) Pain Management Module.
Non-pain symptoms can be as troubling for patients with advanced illness as pain. The formal assessment, reassessment, and management of common symptoms, including nausea, vomiting, dyspnea, constipation, fatigue, and delirium, are a primary domain of palliative medicine. Nausea and vomiting, for example, can become a demoralizing symptom complex. Stimuli to the vomiting center can arise from the cerebral cortex, vestibular apparatus, chemoreceptor zone, and gastrointestinal tract resulting in a broad etiologic differential diagnosis.
With a solid understanding of its pathogenesis and pharmacologic and non-pharmacologic therapeutic principles, nausea and vomiting can be treated in the vast majority of patients. Multiple agents addressing multiple mechanisms may be required. Even the nausea associated with complete bowel obstruction often can be successfully palliated, without the use of nasogastric tubes or surgery.6 The End of Life/Palliative Education Resource Center (www.eperc.mcw.edu) is one of many resources with tools to improve a hospitalist’s evaluation and treatment of non-pain physical symptoms.
Scenario 2: A patient with advanced heart failure and his family are overwhelmed by differing consultant opinions on the appropriateness of implantable cardioverter defibrillator (ICD) insertion.
Effective communication with patients is a core responsibility of both hospitalists and palliative care physicians. A complementary—and at times challenging—skill is the ability to promote communication and consensus about care among multiple specialist consultants. Ripamonti and colleagues write, “Almost invariably, the act of communication is an important part of therapy: Occasionally it is the only constituent. It usually requires greater thought and planning than a drug prescription, and unfortunately it is commonly administered in subtherapeutic doses.”6
The American Academy of Hospice and Palliative Medicine UNIPAC series is a resource for physicians to hone their general communication skills, as well as those more specific to palliative care, such as sharing news (often bad) with patients and families and engaging in therapeutic dialogue.8
Palliative care begins with establishing the goals of care with a patient.9 All physicians bring great value to patient care when they are skilled at negotiating goals of care. There are numerous possible goals of care, from prevention, to cure, to prolongation of life, to achieving a good death. Ideally, goals of care should be discussed with patients and families as early as possible in the course of a serious, life-threatening illness. Establishing realistic and attainable goals of care assumes increased importance in the setting of advanced disease, where treatments intended to prolong life may become more burdensome than beneficial.9
As the reader may have experienced, too often these discussions have not taken place or are held late in the trajectory of illness, such as when patients are hospitalized for severe progressive disease or are facing imminent death.10 In the scenario of potential ICD insertion, conversations with patients to clarify device-specific goals are best accomplished before they are placed and in the context of a broader discussion of the patient’s general medical condition and overall goals for care.11 This type of discussion ultimately improves the informed consent process for ICDs and other technologies. ICD recipients should be guided to periodically revisit their goals, particularly when their health status significantly changes.11 Unlike for initial ICD placement, there are no guidelines for disabling already implanted ICDs. The opportunity to discuss this issue with a patient before a crisis or before they lose decision-making capacity is frequently lost and occurs all too often at life’s end.12
Scenario 3: An elderly debilitated woman with advanced cervical cancer has been hospitalized six times in the past two months. She is cared for at home. Her family is tired but they are doing “the best they can.” She is brought to the emergency department again with weakness.
Effective implementation of care management strategies for patients with life-threatening and advanced disease requires assessment of their physical, social, emotional, and spiritual concerns.1 Similarly, family caregivers have their own—often unvoiced—biopsychosocial stressors.13 Physicians directing patient care must appreciate the significance of these multiple issues, even if they are not comfortable or are ill-equipped to handle them on their own. The power of the interdisciplinary palliative care model is that team members evaluate the patient from different perspectives and pool their expertise in addressing the complex needs of their patients and families.8
In some multidisciplinary models, the onus may lie on the physician to recognize the patient and family needs and mobilize the appropriate resources. Coordination of care at home for patients in the later stages of chronic illness may seem daunting during hospital stays. However, by employing measures utilized by palliative care teams, such as reviewing the goals of care, introducing community resources to help patients and families manage at home, providing anticipatory grief and bereavement support, and considering hospice referral, discharge planning and transitions in care can be much more sustainable.14 With these interventions, patients, families, physicians, and hospitals all benefit.
Conclusion
Hospital-based palliative care programs are growing exponentially.15 Hospitalists are in a unique position to continue their development. Even if the time or circumstances are not yet right for you to become a part of a formal palliative care program, there are daily opportunities to reap rewards from the knowledge, attitudes, and skills that palliative care training offers.
References
- National Consensus Project for Quality Palliative Care: The development of practice guidelines 2004. Available at www.nationalconsensusproject.org. Last accessed April 28, 2006.
- Pistoria MJ, Amin AN, Dressler DD, et al. The core competencies in hospital medicine. J Hosp Med. 2006;1:2(S1).
- American Board of Hospice and Palliative Medicine. Available at www.abhpm.org. Last accessed April 28, 2006.
- Phillips DM. JCAHO pain management standards unveiled. JAMA. 2000;284:428-429.
- Sullivan AM, Lakoma MD, Block SD. The status of medical education in end-of-life care: a national report. J Gen Intern Med. 2003;18:685-695.
- Ripamonti C, De Conno F, Ventafridda V, et al. Management of bowel obstruction in advanced and terminal cancer patients. Ann Oncol. 1993 Jan;4(1):15-21.
- Buckman R. Communication in palliative care: a practical guide. In: Doyle D, Hanks GWC, MacDonald N, eds. Oxford Textbook of Palliative Medicine. New York: Oxford Community Press; 1993:47-61.
- Storey P, Knight CF. UNIPAC five—caring for the terminally ill—communication and the physician’s role in the interdisciplinary team. In: Hospice/Palliative Care Training for Physicians—A Self Study Program. New York: Mary Ann Liebert; 2003:1-147.
- Morrison RS, Meier DE. Palliative care. NEJM. 2004;350:2582-2590.
- Quill TE. Initiating end of life discussion with seriously ill patients: addressing the “elephant in the room.” JAMA. 2000;284:2502-2507.
- Berger, JT. The ethics of deactivating implanted cardioverter defibrillators. Ann Intern Med. 2005;142:631-634.
- Goldstein NE, Lampert R, Bradely E, et al. Management of implantable cardioverter defibrillators in end-of-life care. Ann Intern Med. 2004;141:835-838.
- Levine C. The loneliness of the long-term caregiver. NEJM. 1999;340:1587-1590.
- Meier D. Palliative care in hospitals. J Hosp Med. 2006;1:21-28.
- Morrison RS, et al. The growth of palliative care programs in United States hospitals. J Pall Med. 2006; 8 (6):1127-1133.
Get a Job!
SHM Launches the first-ever career Web site exclusively for hospitalists
By Jeannette Wick
Job boards—Internet sites designed to allow employers and prospective employees to find each other electronically—are among the most active Internet sites. For many job seekers Monster.com, CareerBuilder.com, and Indeed.com (among others) have become essential job search tools. Until now, however, no site has catered to healthcare professionals in general—much less to hospitalists in particular.
Thanks to the new SHM Career Center (http://hospitalmedicine.org/careercenter), though, things are about to change. The Career Center is part of a comprehensive, “cradle-to-grave” approach SHM is taking to assist hospital medicine professionals in their career development pursuits. The site offers numerous advantages over traditional job-hunting tools, such as classified advertisements, personal contacts, and randomly mailing resumes to interesting employers—advantages such as the ability to post your resume in a searchable database, a database of open positions across North America that you can search using a variety of variables and the opportunity to receive a notification when a job that matches your criteria is posted online.
The Career Center also represents an improvement over general job boards because the pool of positions offered and solicited on the site is restricted to those only for hospital medicine professionals. The site is free for all, although SHM members are able to take advantage of certain “members-only” functionality (resume posting, e-mail notification of new job postings). “Career opportunists,” or hospitalists who are gainfully employed but constantly curious about what else is available, will enjoy this site, too.
The Way it Works
SHM’s Career Center matches applicants and jobs using search features that allow applicants to tailor their search. As an applicant, you enter your job preferences as you would when searching for an article in PubMed or when looking online for a board-certified specialist in a specific geographic region when referring a patient. The boxes prompt you to provide the minimum information necessary for an acceptable search. For example, you need to provide geographical preferences, the type of position you’re looking for, and the specialty area you’re interested in to best tailor your search.
Visitors can browse all jobs by specialty or state—or view the complete list of jobs. The advanced search option augments the specialty and state fields with the ability to specify keywords (see “Hospitalists and Keywords,” p. 10), specialty, employment type (full time, moonlighting, and so on), and the announcement opening date. (The latter is important to applicants who believe older announcements raise a red flag indicating conditions that make it unattractive to candidates.)
The advanced search option also allows you to look at job summaries with the results. So instead of receiving a simple list of the job title, the location, and the announcement date, the summary includes a short description of the position. But visitor beware: You have to click a box to make this happen. Otherwise, your search will create a simple list of jobs, and clicking on any individual job will bring up the job summary. The information is accessible either way.
Get Started
Most job seekers will find the site quite easy to navigate, although a few may be impeded by cookies. (For more information, see “Got Cookies,” p. 10.) The FAQ area is a site strength and will help you eliminate hurdles, from inability to navigate the site, to figuring out how to be notified electronically when new jobs are added.
Once you enter your search criteria, a list of jobs displays. Then click on a specific job to open another page describing the position in great detail. After seeing the array of positions available, SHM non-members are likely to join the society just to have access to the full functionality of the Career Center.
Your next step is to create an account; doing so allows you to apply for positions with just a click. Once you establish an account (a process that takes just a few minutes), click on “Edit My Profile.” In this area, you’ll establish your profile.
Meat and Potatoes: Post Your Resume
The Career Center’s features are state-of-the-art. You can create a resume and a cover letter. To post your resume in “My Account,” for example, select “Post My Resume,” then “Document Management,” and then “Resume.” You’ll need to open a plain text version (no bold, underlining, italics, or bullets) of your current resume on your computer, and then copy your resume to the clipboard.
Never done this before? Here again, you can open a guidance window or a printable FAQ to walk you through the process. Two minor system limitations appear here: You must click a box to make the text wrap automatically, and the site has no spell-check function. You have to spell check your cover letter and resume before you copy and paste. If you edit your text at any time while in the Career Center boxes, then be sure to proofread to ensure you haven’t introduced any errors. After you create your resume, you can open a text version (a file that ends in the suffix .txt) to see how employers will view it.
In the past, hospital medicine applicants could stand out with a well-formatted resume on quality paper. Online documents force every applicant’s information into the same mold, and this often concerns applicants. Will a skilled, tri-lingual, well-published hospitalist look like every other applicant when an employer is looking at a simple text version of your resume?
The Career Center allows you to upload up to three formatted documents that can be attached to applications. If you are unable to upload your documents, you may e-mail them to the site, which will then attach them to your account. Some applicants find it useful to have two specific types of resumes on hand: a traditional reverse chronological resume that emphasizes experience, and a less structured functional resume that describes transferable skills.
Depending on your computer savvy, the time it takes to set up your account and load your resume will vary. Hospitalists with robust skills may be able to load a resume in fewer than 30 minutes, but it may take longer for others. Regardless, the return on investment is large because the information you enter will form the foundation of your materials that a perspective employer will review. Once your resume is loaded, applying for a position only requires a few clicks.
Benefits That Make Your Search Sizzle
If you are an SHM member, the “Job Agent” functionality allows you to receive weekly updates of new jobs added that match your search criteria. (Note: You can join SHM online through the Career Center or by visiting www.joinshm.org) This function is located in your account. It allows you to specify the date you would like to stop receiving notification e-mails. Your account also tracks applications submitted.
After you log in, click “Job Applications” to display any jobs you have applied for and the date that the application was submitted. When a job posting expires (according to a pre-established date set by the employer) a strikethrough line will appear through the job application. Applications remain in your account for 90 days from the submission date. Clicking on the “Apply for this Job” icon opens a new screen, and it allows applicants to edit applications even after you’ve sent it and until the job posting closes. Once the job posting is closed, no application changes can be made.
Employers post their vacancies for 30 days at a time, and they can select packages that include print advertisements in The Hospitalist and/or the Journal of Hospital Medicine. Approximately 85% of employers who advertise in print media also advertise on the Career Center, although a few advertise only on the Career Center. To cover your bases, look in all three places.
Just as some applicants prefer anonymity, some companies choose to list their ads confidentially. In these cases, you will submit your online application, and the employer will contact you via the system with more information if you are a good match.
Employer responses will be forwarded to your e-mail account through the Career Center. Once you begin talking with a prospective employer, it is up to you to use good research and interview skills to ensure that this is indeed a good match. When you find a position, you can remove your resume from circulation. Or, you can store it in the Career Center database for future opportunities by clicking “No, do not post my resume.”
Alternatively, you can remove your information from the database permanently: Go to “My Account” and select “Delete Account.”
What the Future Holds
SHM’s information services team will keep tabs on the recently launched SHM Career Center Web site and invites user feedback—specifically any demographic information that will help them build the most practical, useful career site for hospitalists.
With the average age of a hospitalist about 37, SHM expects that visitors and users to comprise a youthful, computer savvy group. Eventually, SHM wants to expand the site so it tells you more than just what jobs are available (e.g., how to create a resume, interview techniques, and how to build desirable hospital medicine skill sets). They will also track how many employer-employee matches are made using the Career Center.
Conclusion
When unemployment is low, as it most certainly is for hospitalists, leverage rests with job seekers, not employers. While employers are looking for talent and availability, career opportunists crave convenience. The SHM Career Center represents the most comprehensive collection of hospitalist opportunities available on the Internet.
Users will find site navigation easy, and prompts and cues offered by the site designers clear and accurate. Traffic on the site is expected to grow quickly as it becomes what SHM hopes is the most indispensable tool for hospitalists conducting job searches.TH
Jeannette Yeznach Wick, RPh, MBA, FASCP, is a freelance medical writer based in Arlington, Va.
SHM: BEHIND THE SCENES
Membership: Listen, Then Act
By Todd Von Deak
As I write this column, there are only seven days left before the start of this year’s annual meeting. At last check, more 1,100 hospital medicine professionals were registered to join us in Washington, D.C., for the most important meeting in hospital medicine. Our office is abuzz with activity and last minute preparations. I’m sure there’s something else that I’m supposed to be doing right now, but I need the break.
While I take my break and write, I can’t help but think, “what’s next,” once the Annual Meeting is over? SHM is fast approaching the start of a new fiscal year, and, like any membership director, I am eager to hit the ground running.
The more I reflect on what’s next, the more I realize that part of my answer lies within the pages of The Hospitalist. Our research continues to show that you consider The Hospitalist to be one of the most valuable benefits of membership.
What strikes me as I read through past issues is that we have another story to tell. So this month we’re launching “SHM: Behind the Scenes.”
There are many reasons why we need to share this story. Key to those reasons is the fact that our sole purpose is to serve the hospital medicine community. You entrust us with your dues and meeting registrations to provide resources that will enable you to better serve your patients and grow your careers in the process. So it’s important that we, the staff, tell you firsthand what we are doing with your investment, and how we plan on continuing to earn your trust in the years to come.
Each month a different member of our senior staff will take turns writing this column. During the coming year you’ll hear from the heads of education and quality initiatives, business operations, membership, information services, marketing, legislative affairs, and research. In each column you’ll find a mix of current news, future plans, and tips for maximizing the value of your membership. If we do our jobs correctly, each month you will have a clearer picture on the true return of your membership investment.
We want you to clearly understand why—if you only belong to one organization—it has to be SHM.
This month I’ll focus on membership and our plans for the coming year. (See below.) Next month you’ll hear from Scott Johnson, SHM’s director of information services. Scott is our chief technologist in many ways and is leading the charge to use today’s latest technology to expand the reach of our educational products and enhance your membership investment as well.
Each year, membership departments at non-profit organizations write their strategic plans for the coming year. SHM is no exception.
For most, these strategic plans are based on a set of assumptions. In more offices than you’d like to believe, the staff just sits around and makes their best guesses in order to answer critical questions, including “what do members want to get out of their membership?”
Based on these guesses, the staff then plots their course expansion and enhances the benefits and services that the organization offers. These organizations are doomed to mediocrity.
Successful organizations, including SHM, actively seek to better understand their membership and use a variety of media to get to the heart of the questions that matter. I am proud to say that SHM is among the second group.
Building on previous efforts, the SHM Membership Department has been actively engaged in a “listening tour.” Our goal is to not rely on assumptions but rather to use your feedback in formulating our plans for the coming year.
Here’s some of what we’ve identified.
Top reasons for being a member:
- Education and quality improvement resources;
- The ability to affect the hospital medicine movement; and
- Subscriptions to The Hospitalist and Journal of Hospital Medicine.
Your main goals as a member:
- To learn from educational and quality improvement resources;
- Take advantage of networking opportunities; and
- Gain exposure for career advancement.
The benefits of membership that matter most:
- Information on www.hospitalmedicine.org;
- Access to results from SHM’s “Authoritative Source on the State of the Hospital Medicine Movement;” and
- The Hospitalist.
We’re already using this data, along with other information that we’ve gathered, to enhance the SHM experience and increase the return on your investment. Just look at the new SHM Career Center (www.hospitalmedicine.org/careercenter).
Like any good membership department, we realize that our data collection has just begun. So I’d like to pose a couple of questions:
- Do you agree with our findings?
- Should we offer a new benefit of membership?
- What can we do to enhance your SHM experience?
I’d love to hear your thoughts. Send them to me via e-mail at tvondeak@hospitalmedicine.org. Anyone who e-mails will be entered in a prize drawing.
In my next column, I will share a selection of the responses I receive and tell you the concrete steps we’re taking to improve communication with you and other members.
Von Deak is SHM’s director of membership and marketing.
Insulin Therapy, C. Diff Update, LMWH or UFH for Acute Coronary Syndrome
C. Difficile Update
- Loo VG, Poirier L, Miller MA, et al. A Predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005 Dec 8;353(23):2442-2449.
- McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med. 2005 Dec 8;353(23):2433-2441.
- Warny M, Pepin J, Fang A, et al. Toxin production by an emerging strain of Clostridium difficile associated with outbreaks of severe disease in North American and Europe. Lancet. 2005 Sep 24-30;366(9491):1079-1084.
In 1978, Clostridium difficile was linked to antibiotic-associated diarrhea and pseudomembranous colitis. This spore-forming gram-positive rod causes disease through two toxins—A and B—which can be detected with cytotoxin assays. It colonizes a significant proportion of hospitalized patients, but causes disease in less than 1%. The primary risk factor for developing disease is antibiotic exposure, presumably through disruption of normal gut flora. Outcomes range from mild diarrhea to life-threatening pseudomembranous colitis requiring colectomy.
Since 2000 a number of hospitals in the United States and Canada have witnessed outbreaks of C. difficile characterized by increases in both the incidence and severity of disease. Three recent publications have shed light on the changes in microbiology that have contributed to those findings. All of the studies characterized C. difficile isolates from these outbreaks, and one included information about patient outcomes.
When isolates from the outbreaks were collected, all three studies identified a predominant strain of C. difficile known as NAP1/027. It accounted for 50%-82% of isolates from the outbreaks in these studies. In contrast, NAP1/027 was present in only 14 isolates from a database of more than 6,000 strains isolated in the United States prior to 2001.
NAP1/027 has a number of concerning microbiologic characteristics. It contains a deletion in the gene tcdC, which normally suppresses the production of toxins A and B. Warny, et al. found that the NAP1/027 strain produces levels of toxins A and B that are 16 and 23 times higher, respectively, than a historically dominant strain. NAP1/027 also produces a binary toxin previously uncommon in C. difficile isolates. The role of binary toxin is not well understood, but it may mediate increased pathogenicity. Finally, the NAP1/027 strain displays high levels of fluoroquinolone resistance, which is uncommon in previous strains of C. difficile.
Loo, et al. also studied patient outcomes in 1,703 patients with C. difficile disease outbreaks in 12 Canadian hospitals. The 30-day mortality rate attributable to C. difficile infection was 6.9%, compared with 0.5-5.5% in previous studies. Patients older than 80 had a higher risk of developing C. difficile infection. For those who did, the 30-day mortality rate attributable to C. difficile was more than 10%.
The discovery of the NAP1/027 strain should strengthen our resolve to use antibiotics judiciously, to recognize and treat C. difficile infections promptly, and to implement strict isolation when cases are discovered. Special attention should be given to elderly patients, who may be at higher risk. Finally, it stresses the importance of hospital epidemiology and infection control, areas in which hospitalists can take an active role.—SM
The Controversy of Thrombolytic Therapy in Hemodynamically Stable Patients with Acute PE
Söhne M, Ten Wolde M Boomsma F, et al. Brain natriuretic peptide in hemodynamically stable acute pulmonary embolism. J Thromb Haemost. 2006 Mar;4(3):552-526.
The role of thrombolytic therapy in hemodynamically stable patients with acute pulmonary embolism is controversial. Right ventricular dysfunction can be an indication for thrombolytics in some patients, but clinical examination is limited and emergent echocardiography is unavailable in many institutions. Rapid measurement of brain natriuretic peptide (BNP) as a marker of right ventricular strain may assist with decision-making in the management of acute PE. Söhne, et al, hypothesized that BNP at presentation would predict the risk of recurrent venous thromboembolism (VTE), including fatal pulmonary embolism.
A nested-case control study was performed within a large, randomized-controlled study of initial treatment of pulmonary embolism. Patients with recurrent VTE within three months were each matched to three controls. BNP levels were drawn at baseline, and both hypertension and congestive heart failure were evaluated as potential confounders.
Cases had significantly higher baseline BNP values than controls (2.45 pmol/L versus 0.80 pmol/L). The odds ratio for each unit increase in the (log) BNP was 2.4 (95% CI: 1.5-3.7). Hypertension was not a confounding factor, but patients with a history of congestive heart failure had no association between elevated BNP and recurrent VTE. Using receiver-operating characteristic analysis, the optimal BNP cut-off of 1.25 pmol/L resulted in a sensitivity and specificity for recurrent VTE of 60% and 62%, respectively.
Three recent studies have suggested that BNP can be used to predict adverse outcomes in patients with pulmonary embolism, including mortality and eventual need for mechanical ventilation, cardiopulmonary resuscitation or thrombolysis. In this study, which included only hemodynamically stable patients with acute pulmonary embolism, however, BNP did not independently predict adverse outcomes. Nonetheless, BNP may be a useful adjunct to other clinical data in deciding whether or not to initiate thrombolytic therapy in pulmonary embolism patients without a history of congestive heart failure.—CR
Insulin Therapy in the ICU
Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
A landmark 2001 study by Van den Berghe, et al. compared tight versus liberal control of blood sugars in surgical ICU patients. The authors found that patients randomized to intensive insulin therapy had decreased mortality during intensive care compared to those receiving conventional treatment (ARR 3.4%, NNT 29).
In this follow-up study, Van den Berghe, et al., shifted the focus toward medical ICU patients. As their previous results were most dramatic in patients who stayed in the ICU for at least five days, they recruited patients expected to require at least three ICU days.
Twelve hundred patients were randomized to receive either conventional (goal BG 180-200 mg/dl) or intensive (goal BG 80-110 mg/dl) insulin treatment. The primary end point was all-cause mortality in the hospital. Secondary outcomes were also defined, including ICU mortality, 90-day mortality, days to weaning from mechanical ventilation, days in the ICU and in the hospital, renal failure, and incidence of bacteremia.
In the intention-to-treat analysis, there was no statistically significant difference in the primary end point of in-hospital mortality. Predefined subgroup analysis of patients who stayed in the ICU longer than three days showed a significant mortality benefit for the intensive insulin regimen (ARR 6.8%, NNT 15). However, in the subgroup of patients staying less than three days in the ICU, there was increased risk of death from all causes (ARI 8.2%, NNH 12). This finding did or did not meet statistical significance depending on the statistical method employed. Some secondary outcome measures assessing morbidity suggested a benefit of intensive insulin therapy. These included a reduction in kidney failure (ARR 3%, NNT 33), earlier weaning from mechanical ventilation, and earlier discharge from the ICU and from the hospital.
The results of this important study are sure to fuel more debate on ideal goals for blood sugar control in the critically ill. The study confirms previous findings that intensive insulin management improves mortality in patients with longer stays in the ICU. As length of stay in the ICU is difficult to predict in advance, the possibility of tight glycemic control increasing mortality in patients with short ICU stays complicates the decision to implement intensive insulin therapy. These results should especially give us pause in extrapolating the original study results to our sick floor patients.—RH
LMWH or UFH for High-Risk Patients with ACS
Mahaffey KW, Cohen M, Garg J, et al. High-risk patients with acute coronary syndromes treated with low-molecular-weight or unfractionated heparin: outcomes at 6 months and 1 year in the SYNERGY trial. JAMA. 2005 Nov 23;294(20):2594-2600.
In July 2004 the SYNERGY (Superior Yield of the New Strategy of Enoxaparin, Revascularization, and Glycoprotein IIb/IIIa Inhibitors) trial reported 30-day post hospitalization data. This study compared low molecular weight heparin (LMWH) to unfractionated heparin (UFH) during acute coronary syndrome (ACS) and found it “at least as effective” as UFH. Further data extending to six months and 12 months was reported in November.
This prospective, randomized, open-labeled multicentered trial enrolled 9,978 patients and compared LMWH versus UFH in ACS. Enrolled patients had had active ischemic symptoms within 24 hours of enrollment, and met two of the following three criteria:
- Age 60 or older;
- Elevated cardiac enzymes; and
- Ischemic ECG changes other than ST elevations.
All patients were treated with standard medical therapy with 50% in both groups receiving GIIb/IIIa inhibitors. Interventions were pursued equally in both groups of patients; 92% had angiograms within 24 hours, 47% had percutaneous interventions, and 19% underwent coronary artery bypass grafting during the index hospitalization.
Six-month and 12-month data confirmed that LMWH use was noninferior to UFH. At six months there was no significant difference between the groups in frequency of nonfatal MI, further revascularization, CVA, or hospitalization. At 12 months, all cause mortality was found to be equivalent between the two groups. Interestingly, nearly 18% died or experienced nonfatal MI through six months of follow-up and 7.4% died by one-year follow-up, despite aggressive coronary revascularization and high use of evidence-based therapies at the time of hospital discharge.
When compared with other trials, these higher than “normal” rates of death and MI were believed related to the high-risk patient population and a lower threshold of cardiac enzyme abnormality. In this high-risk group of patients, LMWH and UFH appear to be equally safe and efficacious for the treatment of ACS, with equivalent long-term outcomes.—RM TH
C. Difficile Update
- Loo VG, Poirier L, Miller MA, et al. A Predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005 Dec 8;353(23):2442-2449.
- McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med. 2005 Dec 8;353(23):2433-2441.
- Warny M, Pepin J, Fang A, et al. Toxin production by an emerging strain of Clostridium difficile associated with outbreaks of severe disease in North American and Europe. Lancet. 2005 Sep 24-30;366(9491):1079-1084.
In 1978, Clostridium difficile was linked to antibiotic-associated diarrhea and pseudomembranous colitis. This spore-forming gram-positive rod causes disease through two toxins—A and B—which can be detected with cytotoxin assays. It colonizes a significant proportion of hospitalized patients, but causes disease in less than 1%. The primary risk factor for developing disease is antibiotic exposure, presumably through disruption of normal gut flora. Outcomes range from mild diarrhea to life-threatening pseudomembranous colitis requiring colectomy.
Since 2000 a number of hospitals in the United States and Canada have witnessed outbreaks of C. difficile characterized by increases in both the incidence and severity of disease. Three recent publications have shed light on the changes in microbiology that have contributed to those findings. All of the studies characterized C. difficile isolates from these outbreaks, and one included information about patient outcomes.
When isolates from the outbreaks were collected, all three studies identified a predominant strain of C. difficile known as NAP1/027. It accounted for 50%-82% of isolates from the outbreaks in these studies. In contrast, NAP1/027 was present in only 14 isolates from a database of more than 6,000 strains isolated in the United States prior to 2001.
NAP1/027 has a number of concerning microbiologic characteristics. It contains a deletion in the gene tcdC, which normally suppresses the production of toxins A and B. Warny, et al. found that the NAP1/027 strain produces levels of toxins A and B that are 16 and 23 times higher, respectively, than a historically dominant strain. NAP1/027 also produces a binary toxin previously uncommon in C. difficile isolates. The role of binary toxin is not well understood, but it may mediate increased pathogenicity. Finally, the NAP1/027 strain displays high levels of fluoroquinolone resistance, which is uncommon in previous strains of C. difficile.
Loo, et al. also studied patient outcomes in 1,703 patients with C. difficile disease outbreaks in 12 Canadian hospitals. The 30-day mortality rate attributable to C. difficile infection was 6.9%, compared with 0.5-5.5% in previous studies. Patients older than 80 had a higher risk of developing C. difficile infection. For those who did, the 30-day mortality rate attributable to C. difficile was more than 10%.
The discovery of the NAP1/027 strain should strengthen our resolve to use antibiotics judiciously, to recognize and treat C. difficile infections promptly, and to implement strict isolation when cases are discovered. Special attention should be given to elderly patients, who may be at higher risk. Finally, it stresses the importance of hospital epidemiology and infection control, areas in which hospitalists can take an active role.—SM
The Controversy of Thrombolytic Therapy in Hemodynamically Stable Patients with Acute PE
Söhne M, Ten Wolde M Boomsma F, et al. Brain natriuretic peptide in hemodynamically stable acute pulmonary embolism. J Thromb Haemost. 2006 Mar;4(3):552-526.
The role of thrombolytic therapy in hemodynamically stable patients with acute pulmonary embolism is controversial. Right ventricular dysfunction can be an indication for thrombolytics in some patients, but clinical examination is limited and emergent echocardiography is unavailable in many institutions. Rapid measurement of brain natriuretic peptide (BNP) as a marker of right ventricular strain may assist with decision-making in the management of acute PE. Söhne, et al, hypothesized that BNP at presentation would predict the risk of recurrent venous thromboembolism (VTE), including fatal pulmonary embolism.
A nested-case control study was performed within a large, randomized-controlled study of initial treatment of pulmonary embolism. Patients with recurrent VTE within three months were each matched to three controls. BNP levels were drawn at baseline, and both hypertension and congestive heart failure were evaluated as potential confounders.
Cases had significantly higher baseline BNP values than controls (2.45 pmol/L versus 0.80 pmol/L). The odds ratio for each unit increase in the (log) BNP was 2.4 (95% CI: 1.5-3.7). Hypertension was not a confounding factor, but patients with a history of congestive heart failure had no association between elevated BNP and recurrent VTE. Using receiver-operating characteristic analysis, the optimal BNP cut-off of 1.25 pmol/L resulted in a sensitivity and specificity for recurrent VTE of 60% and 62%, respectively.
Three recent studies have suggested that BNP can be used to predict adverse outcomes in patients with pulmonary embolism, including mortality and eventual need for mechanical ventilation, cardiopulmonary resuscitation or thrombolysis. In this study, which included only hemodynamically stable patients with acute pulmonary embolism, however, BNP did not independently predict adverse outcomes. Nonetheless, BNP may be a useful adjunct to other clinical data in deciding whether or not to initiate thrombolytic therapy in pulmonary embolism patients without a history of congestive heart failure.—CR
Insulin Therapy in the ICU
Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
A landmark 2001 study by Van den Berghe, et al. compared tight versus liberal control of blood sugars in surgical ICU patients. The authors found that patients randomized to intensive insulin therapy had decreased mortality during intensive care compared to those receiving conventional treatment (ARR 3.4%, NNT 29).
In this follow-up study, Van den Berghe, et al., shifted the focus toward medical ICU patients. As their previous results were most dramatic in patients who stayed in the ICU for at least five days, they recruited patients expected to require at least three ICU days.
Twelve hundred patients were randomized to receive either conventional (goal BG 180-200 mg/dl) or intensive (goal BG 80-110 mg/dl) insulin treatment. The primary end point was all-cause mortality in the hospital. Secondary outcomes were also defined, including ICU mortality, 90-day mortality, days to weaning from mechanical ventilation, days in the ICU and in the hospital, renal failure, and incidence of bacteremia.
In the intention-to-treat analysis, there was no statistically significant difference in the primary end point of in-hospital mortality. Predefined subgroup analysis of patients who stayed in the ICU longer than three days showed a significant mortality benefit for the intensive insulin regimen (ARR 6.8%, NNT 15). However, in the subgroup of patients staying less than three days in the ICU, there was increased risk of death from all causes (ARI 8.2%, NNH 12). This finding did or did not meet statistical significance depending on the statistical method employed. Some secondary outcome measures assessing morbidity suggested a benefit of intensive insulin therapy. These included a reduction in kidney failure (ARR 3%, NNT 33), earlier weaning from mechanical ventilation, and earlier discharge from the ICU and from the hospital.
The results of this important study are sure to fuel more debate on ideal goals for blood sugar control in the critically ill. The study confirms previous findings that intensive insulin management improves mortality in patients with longer stays in the ICU. As length of stay in the ICU is difficult to predict in advance, the possibility of tight glycemic control increasing mortality in patients with short ICU stays complicates the decision to implement intensive insulin therapy. These results should especially give us pause in extrapolating the original study results to our sick floor patients.—RH
LMWH or UFH for High-Risk Patients with ACS
Mahaffey KW, Cohen M, Garg J, et al. High-risk patients with acute coronary syndromes treated with low-molecular-weight or unfractionated heparin: outcomes at 6 months and 1 year in the SYNERGY trial. JAMA. 2005 Nov 23;294(20):2594-2600.
In July 2004 the SYNERGY (Superior Yield of the New Strategy of Enoxaparin, Revascularization, and Glycoprotein IIb/IIIa Inhibitors) trial reported 30-day post hospitalization data. This study compared low molecular weight heparin (LMWH) to unfractionated heparin (UFH) during acute coronary syndrome (ACS) and found it “at least as effective” as UFH. Further data extending to six months and 12 months was reported in November.
This prospective, randomized, open-labeled multicentered trial enrolled 9,978 patients and compared LMWH versus UFH in ACS. Enrolled patients had had active ischemic symptoms within 24 hours of enrollment, and met two of the following three criteria:
- Age 60 or older;
- Elevated cardiac enzymes; and
- Ischemic ECG changes other than ST elevations.
All patients were treated with standard medical therapy with 50% in both groups receiving GIIb/IIIa inhibitors. Interventions were pursued equally in both groups of patients; 92% had angiograms within 24 hours, 47% had percutaneous interventions, and 19% underwent coronary artery bypass grafting during the index hospitalization.
Six-month and 12-month data confirmed that LMWH use was noninferior to UFH. At six months there was no significant difference between the groups in frequency of nonfatal MI, further revascularization, CVA, or hospitalization. At 12 months, all cause mortality was found to be equivalent between the two groups. Interestingly, nearly 18% died or experienced nonfatal MI through six months of follow-up and 7.4% died by one-year follow-up, despite aggressive coronary revascularization and high use of evidence-based therapies at the time of hospital discharge.
When compared with other trials, these higher than “normal” rates of death and MI were believed related to the high-risk patient population and a lower threshold of cardiac enzyme abnormality. In this high-risk group of patients, LMWH and UFH appear to be equally safe and efficacious for the treatment of ACS, with equivalent long-term outcomes.—RM TH
C. Difficile Update
- Loo VG, Poirier L, Miller MA, et al. A Predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005 Dec 8;353(23):2442-2449.
- McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med. 2005 Dec 8;353(23):2433-2441.
- Warny M, Pepin J, Fang A, et al. Toxin production by an emerging strain of Clostridium difficile associated with outbreaks of severe disease in North American and Europe. Lancet. 2005 Sep 24-30;366(9491):1079-1084.
In 1978, Clostridium difficile was linked to antibiotic-associated diarrhea and pseudomembranous colitis. This spore-forming gram-positive rod causes disease through two toxins—A and B—which can be detected with cytotoxin assays. It colonizes a significant proportion of hospitalized patients, but causes disease in less than 1%. The primary risk factor for developing disease is antibiotic exposure, presumably through disruption of normal gut flora. Outcomes range from mild diarrhea to life-threatening pseudomembranous colitis requiring colectomy.
Since 2000 a number of hospitals in the United States and Canada have witnessed outbreaks of C. difficile characterized by increases in both the incidence and severity of disease. Three recent publications have shed light on the changes in microbiology that have contributed to those findings. All of the studies characterized C. difficile isolates from these outbreaks, and one included information about patient outcomes.
When isolates from the outbreaks were collected, all three studies identified a predominant strain of C. difficile known as NAP1/027. It accounted for 50%-82% of isolates from the outbreaks in these studies. In contrast, NAP1/027 was present in only 14 isolates from a database of more than 6,000 strains isolated in the United States prior to 2001.
NAP1/027 has a number of concerning microbiologic characteristics. It contains a deletion in the gene tcdC, which normally suppresses the production of toxins A and B. Warny, et al. found that the NAP1/027 strain produces levels of toxins A and B that are 16 and 23 times higher, respectively, than a historically dominant strain. NAP1/027 also produces a binary toxin previously uncommon in C. difficile isolates. The role of binary toxin is not well understood, but it may mediate increased pathogenicity. Finally, the NAP1/027 strain displays high levels of fluoroquinolone resistance, which is uncommon in previous strains of C. difficile.
Loo, et al. also studied patient outcomes in 1,703 patients with C. difficile disease outbreaks in 12 Canadian hospitals. The 30-day mortality rate attributable to C. difficile infection was 6.9%, compared with 0.5-5.5% in previous studies. Patients older than 80 had a higher risk of developing C. difficile infection. For those who did, the 30-day mortality rate attributable to C. difficile was more than 10%.
The discovery of the NAP1/027 strain should strengthen our resolve to use antibiotics judiciously, to recognize and treat C. difficile infections promptly, and to implement strict isolation when cases are discovered. Special attention should be given to elderly patients, who may be at higher risk. Finally, it stresses the importance of hospital epidemiology and infection control, areas in which hospitalists can take an active role.—SM
The Controversy of Thrombolytic Therapy in Hemodynamically Stable Patients with Acute PE
Söhne M, Ten Wolde M Boomsma F, et al. Brain natriuretic peptide in hemodynamically stable acute pulmonary embolism. J Thromb Haemost. 2006 Mar;4(3):552-526.
The role of thrombolytic therapy in hemodynamically stable patients with acute pulmonary embolism is controversial. Right ventricular dysfunction can be an indication for thrombolytics in some patients, but clinical examination is limited and emergent echocardiography is unavailable in many institutions. Rapid measurement of brain natriuretic peptide (BNP) as a marker of right ventricular strain may assist with decision-making in the management of acute PE. Söhne, et al, hypothesized that BNP at presentation would predict the risk of recurrent venous thromboembolism (VTE), including fatal pulmonary embolism.
A nested-case control study was performed within a large, randomized-controlled study of initial treatment of pulmonary embolism. Patients with recurrent VTE within three months were each matched to three controls. BNP levels were drawn at baseline, and both hypertension and congestive heart failure were evaluated as potential confounders.
Cases had significantly higher baseline BNP values than controls (2.45 pmol/L versus 0.80 pmol/L). The odds ratio for each unit increase in the (log) BNP was 2.4 (95% CI: 1.5-3.7). Hypertension was not a confounding factor, but patients with a history of congestive heart failure had no association between elevated BNP and recurrent VTE. Using receiver-operating characteristic analysis, the optimal BNP cut-off of 1.25 pmol/L resulted in a sensitivity and specificity for recurrent VTE of 60% and 62%, respectively.
Three recent studies have suggested that BNP can be used to predict adverse outcomes in patients with pulmonary embolism, including mortality and eventual need for mechanical ventilation, cardiopulmonary resuscitation or thrombolysis. In this study, which included only hemodynamically stable patients with acute pulmonary embolism, however, BNP did not independently predict adverse outcomes. Nonetheless, BNP may be a useful adjunct to other clinical data in deciding whether or not to initiate thrombolytic therapy in pulmonary embolism patients without a history of congestive heart failure.—CR
Insulin Therapy in the ICU
Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
A landmark 2001 study by Van den Berghe, et al. compared tight versus liberal control of blood sugars in surgical ICU patients. The authors found that patients randomized to intensive insulin therapy had decreased mortality during intensive care compared to those receiving conventional treatment (ARR 3.4%, NNT 29).
In this follow-up study, Van den Berghe, et al., shifted the focus toward medical ICU patients. As their previous results were most dramatic in patients who stayed in the ICU for at least five days, they recruited patients expected to require at least three ICU days.
Twelve hundred patients were randomized to receive either conventional (goal BG 180-200 mg/dl) or intensive (goal BG 80-110 mg/dl) insulin treatment. The primary end point was all-cause mortality in the hospital. Secondary outcomes were also defined, including ICU mortality, 90-day mortality, days to weaning from mechanical ventilation, days in the ICU and in the hospital, renal failure, and incidence of bacteremia.
In the intention-to-treat analysis, there was no statistically significant difference in the primary end point of in-hospital mortality. Predefined subgroup analysis of patients who stayed in the ICU longer than three days showed a significant mortality benefit for the intensive insulin regimen (ARR 6.8%, NNT 15). However, in the subgroup of patients staying less than three days in the ICU, there was increased risk of death from all causes (ARI 8.2%, NNH 12). This finding did or did not meet statistical significance depending on the statistical method employed. Some secondary outcome measures assessing morbidity suggested a benefit of intensive insulin therapy. These included a reduction in kidney failure (ARR 3%, NNT 33), earlier weaning from mechanical ventilation, and earlier discharge from the ICU and from the hospital.
The results of this important study are sure to fuel more debate on ideal goals for blood sugar control in the critically ill. The study confirms previous findings that intensive insulin management improves mortality in patients with longer stays in the ICU. As length of stay in the ICU is difficult to predict in advance, the possibility of tight glycemic control increasing mortality in patients with short ICU stays complicates the decision to implement intensive insulin therapy. These results should especially give us pause in extrapolating the original study results to our sick floor patients.—RH
LMWH or UFH for High-Risk Patients with ACS
Mahaffey KW, Cohen M, Garg J, et al. High-risk patients with acute coronary syndromes treated with low-molecular-weight or unfractionated heparin: outcomes at 6 months and 1 year in the SYNERGY trial. JAMA. 2005 Nov 23;294(20):2594-2600.
In July 2004 the SYNERGY (Superior Yield of the New Strategy of Enoxaparin, Revascularization, and Glycoprotein IIb/IIIa Inhibitors) trial reported 30-day post hospitalization data. This study compared low molecular weight heparin (LMWH) to unfractionated heparin (UFH) during acute coronary syndrome (ACS) and found it “at least as effective” as UFH. Further data extending to six months and 12 months was reported in November.
This prospective, randomized, open-labeled multicentered trial enrolled 9,978 patients and compared LMWH versus UFH in ACS. Enrolled patients had had active ischemic symptoms within 24 hours of enrollment, and met two of the following three criteria:
- Age 60 or older;
- Elevated cardiac enzymes; and
- Ischemic ECG changes other than ST elevations.
All patients were treated with standard medical therapy with 50% in both groups receiving GIIb/IIIa inhibitors. Interventions were pursued equally in both groups of patients; 92% had angiograms within 24 hours, 47% had percutaneous interventions, and 19% underwent coronary artery bypass grafting during the index hospitalization.
Six-month and 12-month data confirmed that LMWH use was noninferior to UFH. At six months there was no significant difference between the groups in frequency of nonfatal MI, further revascularization, CVA, or hospitalization. At 12 months, all cause mortality was found to be equivalent between the two groups. Interestingly, nearly 18% died or experienced nonfatal MI through six months of follow-up and 7.4% died by one-year follow-up, despite aggressive coronary revascularization and high use of evidence-based therapies at the time of hospital discharge.
When compared with other trials, these higher than “normal” rates of death and MI were believed related to the high-risk patient population and a lower threshold of cardiac enzyme abnormality. In this high-risk group of patients, LMWH and UFH appear to be equally safe and efficacious for the treatment of ACS, with equivalent long-term outcomes.—RM TH
An Analysis of Clinical Reasoning Errors
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. Mar;2003:25(2);177-181.
Many hospitalists are involved in processes to reduce errors in the hospital. Given the dozens of clinical decisions hospitalists make each day, errors in clinical reasoning are worth exploring. However, few physicians are familiar with the terminology and classes of clinical reasoning errors as described in the literature.
This article outlines two models of clinical reasoning and explains common biases that distort clinical reasoning. Although the examples used to illustrate these errors draw from primary care internal medicine, they are easily recognizable.
Biases are defined as inaccurate beliefs that affect decision-making.
When generating a differential diagnosis, the bias of availability (aka recall bias) involves a clinician being influenced by what is easily recalled, creating a false sense of prevalence. This is especially common with less experienced clinicians, residents, and medical students.
The bias of representativeness (aka judging by similarity) involves the physician choosing a diagnosis based solely on signs and symptoms, while neglecting the prevalence of competing diagnoses.
The bias of confirmation involves the clinician using additional testing to confirm a suspected diagnosis, but failing to test competing hypotheses.
The bias of anchoring and adjustment involves the clinician inadequately adjusting the differential in light of new data.
The bias of bounded rationality (aka search satisfying) involves the clinician stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Outcome bias involves judging a clinical decision retrospectively based on the outcome, rather than on logic and evidence supporting the original decision.
Omission bias involves placing undue emphasis on avoiding the adverse effect of a therapy, leading to under-utilization of a beneficial treatment.
Most of the work in clinical reasoning errors is published in the cognitive psychology and education literature, which most hospitalists do not regularly read. By becoming familiar with the concepts and terminology, hospitalists can more readily engage in discussions of clinical reasoning errors and how to avoid them. TH
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. Mar;2003:25(2);177-181.
Many hospitalists are involved in processes to reduce errors in the hospital. Given the dozens of clinical decisions hospitalists make each day, errors in clinical reasoning are worth exploring. However, few physicians are familiar with the terminology and classes of clinical reasoning errors as described in the literature.
This article outlines two models of clinical reasoning and explains common biases that distort clinical reasoning. Although the examples used to illustrate these errors draw from primary care internal medicine, they are easily recognizable.
Biases are defined as inaccurate beliefs that affect decision-making.
When generating a differential diagnosis, the bias of availability (aka recall bias) involves a clinician being influenced by what is easily recalled, creating a false sense of prevalence. This is especially common with less experienced clinicians, residents, and medical students.
The bias of representativeness (aka judging by similarity) involves the physician choosing a diagnosis based solely on signs and symptoms, while neglecting the prevalence of competing diagnoses.
The bias of confirmation involves the clinician using additional testing to confirm a suspected diagnosis, but failing to test competing hypotheses.
The bias of anchoring and adjustment involves the clinician inadequately adjusting the differential in light of new data.
The bias of bounded rationality (aka search satisfying) involves the clinician stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Outcome bias involves judging a clinical decision retrospectively based on the outcome, rather than on logic and evidence supporting the original decision.
Omission bias involves placing undue emphasis on avoiding the adverse effect of a therapy, leading to under-utilization of a beneficial treatment.
Most of the work in clinical reasoning errors is published in the cognitive psychology and education literature, which most hospitalists do not regularly read. By becoming familiar with the concepts and terminology, hospitalists can more readily engage in discussions of clinical reasoning errors and how to avoid them. TH
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Med Teach. Mar;2003:25(2);177-181.
Many hospitalists are involved in processes to reduce errors in the hospital. Given the dozens of clinical decisions hospitalists make each day, errors in clinical reasoning are worth exploring. However, few physicians are familiar with the terminology and classes of clinical reasoning errors as described in the literature.
This article outlines two models of clinical reasoning and explains common biases that distort clinical reasoning. Although the examples used to illustrate these errors draw from primary care internal medicine, they are easily recognizable.
Biases are defined as inaccurate beliefs that affect decision-making.
When generating a differential diagnosis, the bias of availability (aka recall bias) involves a clinician being influenced by what is easily recalled, creating a false sense of prevalence. This is especially common with less experienced clinicians, residents, and medical students.
The bias of representativeness (aka judging by similarity) involves the physician choosing a diagnosis based solely on signs and symptoms, while neglecting the prevalence of competing diagnoses.
The bias of confirmation involves the clinician using additional testing to confirm a suspected diagnosis, but failing to test competing hypotheses.
The bias of anchoring and adjustment involves the clinician inadequately adjusting the differential in light of new data.
The bias of bounded rationality (aka search satisfying) involves the clinician stopping the search for additional diagnoses after the anticipated diagnosis has been made.
Outcome bias involves judging a clinical decision retrospectively based on the outcome, rather than on logic and evidence supporting the original decision.
Omission bias involves placing undue emphasis on avoiding the adverse effect of a therapy, leading to under-utilization of a beneficial treatment.
Most of the work in clinical reasoning errors is published in the cognitive psychology and education literature, which most hospitalists do not regularly read. By becoming familiar with the concepts and terminology, hospitalists can more readily engage in discussions of clinical reasoning errors and how to avoid them. TH