User login
Surviving Colorectal Cancer, Now at Risk for Hypertension
Colorectal cancer (CRC) survivor rates are improving, which means people are living long enough after the cancer to have other chronic conditions. CRC is the third most commonly diagnosed cancer among users of the US Department of Veterans Affairs (VA) health care system, according to VA researchers, and there is a high prevalence of cardiovascular disease (CVD). The researchers also say emerging evidence suggests that survivors of CRC may be more likely to develop diabetes mellitus (DM) in the 5 years following their cancer diagnosis. But they add that there is a paucity of research about control of CVD-related chronic conditions among survivors of CRC.
In a retrospective study, the researchers compared 9,758 nonmetastatic patients with CRC with 29,066 people who had not had cancer. At baseline, 69% of the survivors of CRC and the matched controls were diagnosed with hypertension, 52% with hyperlipidemia, and 37% with DM.
But somewhat contrary to expectations, the researchers found no significant differences between the 2 groups for DM in the year following the baseline assessment. The researchers point to the VA’s “strong history” of DM risk reduction research and 2 national programs targeting DM, although they do not know whether the people in their study participated in those.
The survivors of CRC also had half the odds of being diagnosed with hyperlipidemia. However, they did have 57% higher odds of being diagnosed with hypertension.
Although the researchers acknowledge that hypertension is a transient adverse effect of certain chemotherapy regimens, they found only 7 survivors of CRC and 11 controls were treated with bevacizumab during their first year postanchor date.
The relationship between nonmetastatic CRC and CVD risk-related chronic conditions is complex, the researchers say. But they share risk factors, including obesity, physical inactivity, and diet.
The researchers call behavioral change interventions that improve survivors of CRC physical activity, dietary habits, and body mass index a “promising beginning” but call for other similar interventions, particularly those targeting blood pressure management and adherence to antihypertensive medications (which was significantly lower among the survivors).
While the magnitude of the effect regarding hypertension seems relatively small, the researchers say, they believe it is still an important difference when considered from a population health perspective—and one that should be addressed. The researchers also note that nonmetastatic survivors of CRC and controls had very similar rates of primary care visits in the 3 years postanchor date and as a result similar opportunities to receive a hypertension diagnosis.
Colorectal cancer (CRC) survivor rates are improving, which means people are living long enough after the cancer to have other chronic conditions. CRC is the third most commonly diagnosed cancer among users of the US Department of Veterans Affairs (VA) health care system, according to VA researchers, and there is a high prevalence of cardiovascular disease (CVD). The researchers also say emerging evidence suggests that survivors of CRC may be more likely to develop diabetes mellitus (DM) in the 5 years following their cancer diagnosis. But they add that there is a paucity of research about control of CVD-related chronic conditions among survivors of CRC.
In a retrospective study, the researchers compared 9,758 nonmetastatic patients with CRC with 29,066 people who had not had cancer. At baseline, 69% of the survivors of CRC and the matched controls were diagnosed with hypertension, 52% with hyperlipidemia, and 37% with DM.
But somewhat contrary to expectations, the researchers found no significant differences between the 2 groups for DM in the year following the baseline assessment. The researchers point to the VA’s “strong history” of DM risk reduction research and 2 national programs targeting DM, although they do not know whether the people in their study participated in those.
The survivors of CRC also had half the odds of being diagnosed with hyperlipidemia. However, they did have 57% higher odds of being diagnosed with hypertension.
Although the researchers acknowledge that hypertension is a transient adverse effect of certain chemotherapy regimens, they found only 7 survivors of CRC and 11 controls were treated with bevacizumab during their first year postanchor date.
The relationship between nonmetastatic CRC and CVD risk-related chronic conditions is complex, the researchers say. But they share risk factors, including obesity, physical inactivity, and diet.
The researchers call behavioral change interventions that improve survivors of CRC physical activity, dietary habits, and body mass index a “promising beginning” but call for other similar interventions, particularly those targeting blood pressure management and adherence to antihypertensive medications (which was significantly lower among the survivors).
While the magnitude of the effect regarding hypertension seems relatively small, the researchers say, they believe it is still an important difference when considered from a population health perspective—and one that should be addressed. The researchers also note that nonmetastatic survivors of CRC and controls had very similar rates of primary care visits in the 3 years postanchor date and as a result similar opportunities to receive a hypertension diagnosis.
Colorectal cancer (CRC) survivor rates are improving, which means people are living long enough after the cancer to have other chronic conditions. CRC is the third most commonly diagnosed cancer among users of the US Department of Veterans Affairs (VA) health care system, according to VA researchers, and there is a high prevalence of cardiovascular disease (CVD). The researchers also say emerging evidence suggests that survivors of CRC may be more likely to develop diabetes mellitus (DM) in the 5 years following their cancer diagnosis. But they add that there is a paucity of research about control of CVD-related chronic conditions among survivors of CRC.
In a retrospective study, the researchers compared 9,758 nonmetastatic patients with CRC with 29,066 people who had not had cancer. At baseline, 69% of the survivors of CRC and the matched controls were diagnosed with hypertension, 52% with hyperlipidemia, and 37% with DM.
But somewhat contrary to expectations, the researchers found no significant differences between the 2 groups for DM in the year following the baseline assessment. The researchers point to the VA’s “strong history” of DM risk reduction research and 2 national programs targeting DM, although they do not know whether the people in their study participated in those.
The survivors of CRC also had half the odds of being diagnosed with hyperlipidemia. However, they did have 57% higher odds of being diagnosed with hypertension.
Although the researchers acknowledge that hypertension is a transient adverse effect of certain chemotherapy regimens, they found only 7 survivors of CRC and 11 controls were treated with bevacizumab during their first year postanchor date.
The relationship between nonmetastatic CRC and CVD risk-related chronic conditions is complex, the researchers say. But they share risk factors, including obesity, physical inactivity, and diet.
The researchers call behavioral change interventions that improve survivors of CRC physical activity, dietary habits, and body mass index a “promising beginning” but call for other similar interventions, particularly those targeting blood pressure management and adherence to antihypertensive medications (which was significantly lower among the survivors).
While the magnitude of the effect regarding hypertension seems relatively small, the researchers say, they believe it is still an important difference when considered from a population health perspective—and one that should be addressed. The researchers also note that nonmetastatic survivors of CRC and controls had very similar rates of primary care visits in the 3 years postanchor date and as a result similar opportunities to receive a hypertension diagnosis.
Open Clinical Trials for Patients With Lung Cancers (FULL)
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors or cosponsors nearly 1,000 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of August 1, 201 8 ; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Lung-MAP (multiple trials)
Lung-MAP (SWOG S1400) is a multidrug, multi-substudy, biomarker-driven squamous cell lung cancer clinical trial that uses state-of-the-art genomic profiling to match patients to substudies testing investigational treatments that may target the genomic alterations, or mutations, found to be driving the growth of their cancer.
ID: NCT02154490, NCT02595944, NCT02766335, NCT02785913, NCT02785939, NCT02926638, NCT02965378, NCT03373760, NCT03377556
Sponsor: Southwest Oncology Group
Locations: VA Connecticut Healthcare System-West Haven Campus; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Ann Arbor VAMC, Michigan; Kansas City VAMC, Missouri; VA New Jersey Health Care System, East Orange; Michael E. DeBakey VAMC Houston, Texas
ALCHEMIST: Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials (multiple trials)
A group of randomized clinical trials for patients with early-stage non-small cell lung cancer whose tumors have been completely removed by surgery.
ID: NCT02193282, NCT02194738, NCT02201992, NCT02595944
Sponsor: National Cancer Institute
Locations: Little Rock VAMC, Arkansas; VA Connecticut Healthcare System West Haven Campus; Atlanta VAMC, Decatur, Georgia; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Minneapolis VAMC, Minnesota; Saint Louis VAMC, Missouri; Veterans Affairs New York Harbor Healthcare System-Brooklyn Campus; Dayton VAMC, Ohio; William S. Middleton VAMC, Madison, Wisconsin
Veterans Affairs Lung Cancer Or Stereotactic Radiotherapy (VALOR)
The standard of care for stage I non-small cell lung cancer has historically been surgical resection in patients who are medically fit to tolerate an operation. Recent data now suggests that stereotactic radiotherapy may be a suitable alternative. This includes the results from a pooled analysis of two incomplete phase III studies that reported a 15% overall survival advantage with stereotactic radiotherapy at 3 years. While these data are promising, the median follow-up period was short, the results underpowered, and the findings were in contradiction to multiple retrospective studies that demonstrate the outcomes with surgery are likely equal or superior. Therefore, the herein trial aims to evaluate these two treatments in a prospective randomized fashion with a goal to compare the overall survival beyond 5 years. It has been designed to enroll patients who have a long life-expectancy, and are fit enough to tolerate an anatomic pulmonary resection with intraoperative lymph node sampling.
ID: NCT02984761
Sponsor: VA Office of Research and Development
Locations: Edward Hines Jr. VA Hospital, Hines, Illinois; Richard L. Roudebush VA Medical Center, Indianapolis, Indiana; Minneapolis VA Health Care System, Minnesota; Durham VAMC, North Carolina; Michael E. DeBakey VAMC, Houston, Texas; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Naloxegol in Treating Patients With Stage IIIB-IV Non-Small Cell Lung Cancer
This randomized pilot clinical trial studies the side effects and best dose of naloxegol and to see how well it works in treating patients with stage IIIB-IV non-small cell lung cancer. Naloxegol may relieve some of the side effects of opioid pain medication and fight off future growth in the cancer.
ID: NCT03087708
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Minneapolis VAMC, Minnesota; Kansas City VAMC, Missouri; VA Western New York Health Care System-Buffalo; Salisbury VAMC, North Carolina
Palliative Care Interventions for Outpatients Newly Diagnosed With Lung Cancer: Phase II (PCI2)
The focus of the study is to test a nurse-led telephone-based palliative care intervention on improving the delivery of care for patients with newly diagnosed lung cancer. The study is a three site randomized control trial to determine the efficacy of the intervention on improving patients’ quality of life, symptom burden, and satisfaction of care. Additionally, the study will test an innovative care delivery model to improve patients’ access to palliative care. The investigators will also determine the effect of the intervention on patient activation to discuss treatment preferences with their clinician and on clinician knowledge of patients’ goals of care.
ID: NCT03007953
Sponsor: VA Office of Research and Development
Locations: Birmingham VAMC, Alabama; VA Portland Health Care System, Oregon; VA Puget Sound Health Care System Seattle Division, Washington
Radiation Therapy Regimens in Treating Patients With Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide
Radiation therapy uses high-energy x-rays to kill tumor cells. Drugs used in chemotherapy, such as etoposide, carboplatin and cisplatin, work in different ways to stop the growth of tumor cells, either by killing the cells or by stopping them from dividing. It is not yet known which radiation therapy regimen is more effective when given together with chemotherapy in treating patients with limited-stage small cell lung cancer. This randomized phase III trial is comparing different chest radiation therapy regimens to see how well they work in treating patients with limited-stage small cell lung cancer.
ID: NCT00632853
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Baltimore VAMC, Maryland; Kansas City VAMC, Missouri; VA Western New York Health Care System, Buffalo, New York; Dayton VAMC, Ohio; Zablocki VAMC, Milwaukee, Wisconsin
Comparison of Different Types of Surgery in Treating Patients With Stage IA Non-Small Cell Lung Cancer
Wedge resection or segmentectomy may be less invasive types of surgery than lobectomy for non-small cell lung cancer and may have fewer side effects and improve recovery. It is not yet known whether wedge resection or segmentectomy are more effective than lobectomy in treating stage IA non-small cell lung cancer.
ID: NCT00499330
Sponsor: Alliance for Clinical Trials in Oncology
Locations: VA Loma Linda Healthcare System, California; VA Long Beach Medical Center, California; Richard L. Roudebush VAMC, Indianapolis, Indiana; Portland VAMC, Oregon
Lung Cancer Screening Decisions (VA-LCSDecTool)
Veterans have a high risk of developing lung in comparison to general populations due to their older age and smoking history. Recent evidence indicates that lung cancer screening with low dose CT scan reduces lung cancer mortality among older heavy smokers. However, the rates of false positive findings are high, requiring further testing and evaluation. Preliminary studies report that while some Veterans are enthusiastic about screening, others are highly reluctant. Patient preferences should be considered as part of an informed decision making process for this emerging paradigm of lung cancer control. Effective methods for preference assessment among Veterans have not yet been developed, evaluated, and integrated into clinical practice. The specific aims of this study are to 1) elicit patient and provider stakeholder input to inform the development of a lung cancer screening decision tool, 2) develop a web based Lung Cancer Screening Decision Tool (LCSDecTool) that incorporates patient and provider input, and 3) evaluate the impact of the LCSDecTool compared to usual care on the decision process, clinical outcomes, and quality of life.
ID
Sponsor: VA Office of Research and Development
Locations: VA Connecticut Healthcare System West Haven Campus; Corporal Michael J. Crescenz VAMC Philadelphia, Pennsylvania
Molecular Predictors of Cancer in Patients at High Risk of Lung Cancer
Using samples of blood, urine, sputum, and lung tissue from patients at high risk of cancer for laboratory studies may help doctors learn more about changes that may occur in DNA and identify biomarkers related to cancer.
ID: NCT00898313
Sponsor: Vanderbilt-Ingram Cancer Center
Location: VAMC Nashville, Tennessee
Improving Supportive Care for Patients With Thoracic Malignancies
The purpose of this study is to use a proactive approach to improve symptom management of patients with thoracic malignancies. In this pilot study, the investigators propose to evaluate the feasibility of using outbound, proactive telephone symptom assessment strategies and measure the efficacy of this approach on patient satisfaction with their care, patient activation, quality of life and use of healthcare resources.
ID: NCT03216109
Sponsor: Palo Alto Veterans Institute for Research
Location: VA Palo Alto Health Care System, California
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors or cosponsors nearly 1,000 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of August 1, 201 8 ; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Lung-MAP (multiple trials)
Lung-MAP (SWOG S1400) is a multidrug, multi-substudy, biomarker-driven squamous cell lung cancer clinical trial that uses state-of-the-art genomic profiling to match patients to substudies testing investigational treatments that may target the genomic alterations, or mutations, found to be driving the growth of their cancer.
ID: NCT02154490, NCT02595944, NCT02766335, NCT02785913, NCT02785939, NCT02926638, NCT02965378, NCT03373760, NCT03377556
Sponsor: Southwest Oncology Group
Locations: VA Connecticut Healthcare System-West Haven Campus; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Ann Arbor VAMC, Michigan; Kansas City VAMC, Missouri; VA New Jersey Health Care System, East Orange; Michael E. DeBakey VAMC Houston, Texas
ALCHEMIST: Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials (multiple trials)
A group of randomized clinical trials for patients with early-stage non-small cell lung cancer whose tumors have been completely removed by surgery.
ID: NCT02193282, NCT02194738, NCT02201992, NCT02595944
Sponsor: National Cancer Institute
Locations: Little Rock VAMC, Arkansas; VA Connecticut Healthcare System West Haven Campus; Atlanta VAMC, Decatur, Georgia; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Minneapolis VAMC, Minnesota; Saint Louis VAMC, Missouri; Veterans Affairs New York Harbor Healthcare System-Brooklyn Campus; Dayton VAMC, Ohio; William S. Middleton VAMC, Madison, Wisconsin
Veterans Affairs Lung Cancer Or Stereotactic Radiotherapy (VALOR)
The standard of care for stage I non-small cell lung cancer has historically been surgical resection in patients who are medically fit to tolerate an operation. Recent data now suggests that stereotactic radiotherapy may be a suitable alternative. This includes the results from a pooled analysis of two incomplete phase III studies that reported a 15% overall survival advantage with stereotactic radiotherapy at 3 years. While these data are promising, the median follow-up period was short, the results underpowered, and the findings were in contradiction to multiple retrospective studies that demonstrate the outcomes with surgery are likely equal or superior. Therefore, the herein trial aims to evaluate these two treatments in a prospective randomized fashion with a goal to compare the overall survival beyond 5 years. It has been designed to enroll patients who have a long life-expectancy, and are fit enough to tolerate an anatomic pulmonary resection with intraoperative lymph node sampling.
ID: NCT02984761
Sponsor: VA Office of Research and Development
Locations: Edward Hines Jr. VA Hospital, Hines, Illinois; Richard L. Roudebush VA Medical Center, Indianapolis, Indiana; Minneapolis VA Health Care System, Minnesota; Durham VAMC, North Carolina; Michael E. DeBakey VAMC, Houston, Texas; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Naloxegol in Treating Patients With Stage IIIB-IV Non-Small Cell Lung Cancer
This randomized pilot clinical trial studies the side effects and best dose of naloxegol and to see how well it works in treating patients with stage IIIB-IV non-small cell lung cancer. Naloxegol may relieve some of the side effects of opioid pain medication and fight off future growth in the cancer.
ID: NCT03087708
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Minneapolis VAMC, Minnesota; Kansas City VAMC, Missouri; VA Western New York Health Care System-Buffalo; Salisbury VAMC, North Carolina
Palliative Care Interventions for Outpatients Newly Diagnosed With Lung Cancer: Phase II (PCI2)
The focus of the study is to test a nurse-led telephone-based palliative care intervention on improving the delivery of care for patients with newly diagnosed lung cancer. The study is a three site randomized control trial to determine the efficacy of the intervention on improving patients’ quality of life, symptom burden, and satisfaction of care. Additionally, the study will test an innovative care delivery model to improve patients’ access to palliative care. The investigators will also determine the effect of the intervention on patient activation to discuss treatment preferences with their clinician and on clinician knowledge of patients’ goals of care.
ID: NCT03007953
Sponsor: VA Office of Research and Development
Locations: Birmingham VAMC, Alabama; VA Portland Health Care System, Oregon; VA Puget Sound Health Care System Seattle Division, Washington
Radiation Therapy Regimens in Treating Patients With Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide
Radiation therapy uses high-energy x-rays to kill tumor cells. Drugs used in chemotherapy, such as etoposide, carboplatin and cisplatin, work in different ways to stop the growth of tumor cells, either by killing the cells or by stopping them from dividing. It is not yet known which radiation therapy regimen is more effective when given together with chemotherapy in treating patients with limited-stage small cell lung cancer. This randomized phase III trial is comparing different chest radiation therapy regimens to see how well they work in treating patients with limited-stage small cell lung cancer.
ID: NCT00632853
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Baltimore VAMC, Maryland; Kansas City VAMC, Missouri; VA Western New York Health Care System, Buffalo, New York; Dayton VAMC, Ohio; Zablocki VAMC, Milwaukee, Wisconsin
Comparison of Different Types of Surgery in Treating Patients With Stage IA Non-Small Cell Lung Cancer
Wedge resection or segmentectomy may be less invasive types of surgery than lobectomy for non-small cell lung cancer and may have fewer side effects and improve recovery. It is not yet known whether wedge resection or segmentectomy are more effective than lobectomy in treating stage IA non-small cell lung cancer.
ID: NCT00499330
Sponsor: Alliance for Clinical Trials in Oncology
Locations: VA Loma Linda Healthcare System, California; VA Long Beach Medical Center, California; Richard L. Roudebush VAMC, Indianapolis, Indiana; Portland VAMC, Oregon
Lung Cancer Screening Decisions (VA-LCSDecTool)
Veterans have a high risk of developing lung in comparison to general populations due to their older age and smoking history. Recent evidence indicates that lung cancer screening with low dose CT scan reduces lung cancer mortality among older heavy smokers. However, the rates of false positive findings are high, requiring further testing and evaluation. Preliminary studies report that while some Veterans are enthusiastic about screening, others are highly reluctant. Patient preferences should be considered as part of an informed decision making process for this emerging paradigm of lung cancer control. Effective methods for preference assessment among Veterans have not yet been developed, evaluated, and integrated into clinical practice. The specific aims of this study are to 1) elicit patient and provider stakeholder input to inform the development of a lung cancer screening decision tool, 2) develop a web based Lung Cancer Screening Decision Tool (LCSDecTool) that incorporates patient and provider input, and 3) evaluate the impact of the LCSDecTool compared to usual care on the decision process, clinical outcomes, and quality of life.
ID
Sponsor: VA Office of Research and Development
Locations: VA Connecticut Healthcare System West Haven Campus; Corporal Michael J. Crescenz VAMC Philadelphia, Pennsylvania
Molecular Predictors of Cancer in Patients at High Risk of Lung Cancer
Using samples of blood, urine, sputum, and lung tissue from patients at high risk of cancer for laboratory studies may help doctors learn more about changes that may occur in DNA and identify biomarkers related to cancer.
ID: NCT00898313
Sponsor: Vanderbilt-Ingram Cancer Center
Location: VAMC Nashville, Tennessee
Improving Supportive Care for Patients With Thoracic Malignancies
The purpose of this study is to use a proactive approach to improve symptom management of patients with thoracic malignancies. In this pilot study, the investigators propose to evaluate the feasibility of using outbound, proactive telephone symptom assessment strategies and measure the efficacy of this approach on patient satisfaction with their care, patient activation, quality of life and use of healthcare resources.
ID: NCT03216109
Sponsor: Palo Alto Veterans Institute for Research
Location: VA Palo Alto Health Care System, California
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors or cosponsors nearly 1,000 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of August 1, 201 8 ; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Lung-MAP (multiple trials)
Lung-MAP (SWOG S1400) is a multidrug, multi-substudy, biomarker-driven squamous cell lung cancer clinical trial that uses state-of-the-art genomic profiling to match patients to substudies testing investigational treatments that may target the genomic alterations, or mutations, found to be driving the growth of their cancer.
ID: NCT02154490, NCT02595944, NCT02766335, NCT02785913, NCT02785939, NCT02926638, NCT02965378, NCT03373760, NCT03377556
Sponsor: Southwest Oncology Group
Locations: VA Connecticut Healthcare System-West Haven Campus; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Ann Arbor VAMC, Michigan; Kansas City VAMC, Missouri; VA New Jersey Health Care System, East Orange; Michael E. DeBakey VAMC Houston, Texas
ALCHEMIST: Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trials (multiple trials)
A group of randomized clinical trials for patients with early-stage non-small cell lung cancer whose tumors have been completely removed by surgery.
ID: NCT02193282, NCT02194738, NCT02201992, NCT02595944
Sponsor: National Cancer Institute
Locations: Little Rock VAMC, Arkansas; VA Connecticut Healthcare System West Haven Campus; Atlanta VAMC, Decatur, Georgia; Hines VA Hospital, Illinois; Richard L. Roudebush VAMC, Indianapolis, Indiana; Minneapolis VAMC, Minnesota; Saint Louis VAMC, Missouri; Veterans Affairs New York Harbor Healthcare System-Brooklyn Campus; Dayton VAMC, Ohio; William S. Middleton VAMC, Madison, Wisconsin
Veterans Affairs Lung Cancer Or Stereotactic Radiotherapy (VALOR)
The standard of care for stage I non-small cell lung cancer has historically been surgical resection in patients who are medically fit to tolerate an operation. Recent data now suggests that stereotactic radiotherapy may be a suitable alternative. This includes the results from a pooled analysis of two incomplete phase III studies that reported a 15% overall survival advantage with stereotactic radiotherapy at 3 years. While these data are promising, the median follow-up period was short, the results underpowered, and the findings were in contradiction to multiple retrospective studies that demonstrate the outcomes with surgery are likely equal or superior. Therefore, the herein trial aims to evaluate these two treatments in a prospective randomized fashion with a goal to compare the overall survival beyond 5 years. It has been designed to enroll patients who have a long life-expectancy, and are fit enough to tolerate an anatomic pulmonary resection with intraoperative lymph node sampling.
ID: NCT02984761
Sponsor: VA Office of Research and Development
Locations: Edward Hines Jr. VA Hospital, Hines, Illinois; Richard L. Roudebush VA Medical Center, Indianapolis, Indiana; Minneapolis VA Health Care System, Minnesota; Durham VAMC, North Carolina; Michael E. DeBakey VAMC, Houston, Texas; Hunter Holmes McGuire VA Medical Center, Richmond, Virginia
Naloxegol in Treating Patients With Stage IIIB-IV Non-Small Cell Lung Cancer
This randomized pilot clinical trial studies the side effects and best dose of naloxegol and to see how well it works in treating patients with stage IIIB-IV non-small cell lung cancer. Naloxegol may relieve some of the side effects of opioid pain medication and fight off future growth in the cancer.
ID: NCT03087708
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Minneapolis VAMC, Minnesota; Kansas City VAMC, Missouri; VA Western New York Health Care System-Buffalo; Salisbury VAMC, North Carolina
Palliative Care Interventions for Outpatients Newly Diagnosed With Lung Cancer: Phase II (PCI2)
The focus of the study is to test a nurse-led telephone-based palliative care intervention on improving the delivery of care for patients with newly diagnosed lung cancer. The study is a three site randomized control trial to determine the efficacy of the intervention on improving patients’ quality of life, symptom burden, and satisfaction of care. Additionally, the study will test an innovative care delivery model to improve patients’ access to palliative care. The investigators will also determine the effect of the intervention on patient activation to discuss treatment preferences with their clinician and on clinician knowledge of patients’ goals of care.
ID: NCT03007953
Sponsor: VA Office of Research and Development
Locations: Birmingham VAMC, Alabama; VA Portland Health Care System, Oregon; VA Puget Sound Health Care System Seattle Division, Washington
Radiation Therapy Regimens in Treating Patients With Limited-Stage Small Cell Lung Cancer Receiving Cisplatin and Etoposide
Radiation therapy uses high-energy x-rays to kill tumor cells. Drugs used in chemotherapy, such as etoposide, carboplatin and cisplatin, work in different ways to stop the growth of tumor cells, either by killing the cells or by stopping them from dividing. It is not yet known which radiation therapy regimen is more effective when given together with chemotherapy in treating patients with limited-stage small cell lung cancer. This randomized phase III trial is comparing different chest radiation therapy regimens to see how well they work in treating patients with limited-stage small cell lung cancer.
ID: NCT00632853
Sponsor: Alliance for Clinical Trials in Oncology
Locations: Baltimore VAMC, Maryland; Kansas City VAMC, Missouri; VA Western New York Health Care System, Buffalo, New York; Dayton VAMC, Ohio; Zablocki VAMC, Milwaukee, Wisconsin
Comparison of Different Types of Surgery in Treating Patients With Stage IA Non-Small Cell Lung Cancer
Wedge resection or segmentectomy may be less invasive types of surgery than lobectomy for non-small cell lung cancer and may have fewer side effects and improve recovery. It is not yet known whether wedge resection or segmentectomy are more effective than lobectomy in treating stage IA non-small cell lung cancer.
ID: NCT00499330
Sponsor: Alliance for Clinical Trials in Oncology
Locations: VA Loma Linda Healthcare System, California; VA Long Beach Medical Center, California; Richard L. Roudebush VAMC, Indianapolis, Indiana; Portland VAMC, Oregon
Lung Cancer Screening Decisions (VA-LCSDecTool)
Veterans have a high risk of developing lung in comparison to general populations due to their older age and smoking history. Recent evidence indicates that lung cancer screening with low dose CT scan reduces lung cancer mortality among older heavy smokers. However, the rates of false positive findings are high, requiring further testing and evaluation. Preliminary studies report that while some Veterans are enthusiastic about screening, others are highly reluctant. Patient preferences should be considered as part of an informed decision making process for this emerging paradigm of lung cancer control. Effective methods for preference assessment among Veterans have not yet been developed, evaluated, and integrated into clinical practice. The specific aims of this study are to 1) elicit patient and provider stakeholder input to inform the development of a lung cancer screening decision tool, 2) develop a web based Lung Cancer Screening Decision Tool (LCSDecTool) that incorporates patient and provider input, and 3) evaluate the impact of the LCSDecTool compared to usual care on the decision process, clinical outcomes, and quality of life.
ID
Sponsor: VA Office of Research and Development
Locations: VA Connecticut Healthcare System West Haven Campus; Corporal Michael J. Crescenz VAMC Philadelphia, Pennsylvania
Molecular Predictors of Cancer in Patients at High Risk of Lung Cancer
Using samples of blood, urine, sputum, and lung tissue from patients at high risk of cancer for laboratory studies may help doctors learn more about changes that may occur in DNA and identify biomarkers related to cancer.
ID: NCT00898313
Sponsor: Vanderbilt-Ingram Cancer Center
Location: VAMC Nashville, Tennessee
Improving Supportive Care for Patients With Thoracic Malignancies
The purpose of this study is to use a proactive approach to improve symptom management of patients with thoracic malignancies. In this pilot study, the investigators propose to evaluate the feasibility of using outbound, proactive telephone symptom assessment strategies and measure the efficacy of this approach on patient satisfaction with their care, patient activation, quality of life and use of healthcare resources.
ID: NCT03216109
Sponsor: Palo Alto Veterans Institute for Research
Location: VA Palo Alto Health Care System, California
IHS Launches Pilot to Redress Racial Misclassification in Records
American Indians and Alaska Natives (AI/AN) are often misidentified as other races in public health administrative records. In the Northwest, for instance, the Northwest Tribal Epidemiology Center (NTEC) has found that about 10% of AI/AN birth and death records and up to 60% of hospitalization records are misclassified.
Racial misclassification makes it difficult to accurately assess the health of Native people: The numbers affected by a disease may appear lower or higher than they actually are. It can muddle and misrepresent information in birth certificates, cancer registries, death certificates, emergency department records, hospitalization records, injury reports. Without accurate health data, says Lisa Neel, director of the Indian Health Service (IHS) Tribal Epidemiology Center Program, tribes cannot make informed decisions about how best to serve their people.
That is why the IHS and the Center recently signed an agreement supporting a new information-sharing project. The agreement will allow the IHS to provide the NTEC with a list of people who have received health services at IHS, tribal, and urban Indian health programs in the Portland Area. The list will include no information about patients’ medical histories and will not be shared outside the NTEC. The center will then compare the list with outside information sources, such as state cancer registries, to check for racial misclassification.
The NTEC is 1 of 13 national “EpiCenters” charged with collecting tribal health status data, evaluating data monitoring and delivery systems, and helping tribes identify local priorities for health care delivery and health education. NTEC serves the 43 federally recognized tribes in Idaho, Oregon, and Washington. The center is housed in the Northwest Portland Area Indian Health Board (NPAIHB), whose delegates, representing the member tribes, direct and oversee activities, including health promotion, disease prevention, training and technical assistance.
The IHS plans for this to be a pilot project, possibly pointing the way for other tribal EpiCenters to launch similar projects.
American Indians and Alaska Natives (AI/AN) are often misidentified as other races in public health administrative records. In the Northwest, for instance, the Northwest Tribal Epidemiology Center (NTEC) has found that about 10% of AI/AN birth and death records and up to 60% of hospitalization records are misclassified.
Racial misclassification makes it difficult to accurately assess the health of Native people: The numbers affected by a disease may appear lower or higher than they actually are. It can muddle and misrepresent information in birth certificates, cancer registries, death certificates, emergency department records, hospitalization records, injury reports. Without accurate health data, says Lisa Neel, director of the Indian Health Service (IHS) Tribal Epidemiology Center Program, tribes cannot make informed decisions about how best to serve their people.
That is why the IHS and the Center recently signed an agreement supporting a new information-sharing project. The agreement will allow the IHS to provide the NTEC with a list of people who have received health services at IHS, tribal, and urban Indian health programs in the Portland Area. The list will include no information about patients’ medical histories and will not be shared outside the NTEC. The center will then compare the list with outside information sources, such as state cancer registries, to check for racial misclassification.
The NTEC is 1 of 13 national “EpiCenters” charged with collecting tribal health status data, evaluating data monitoring and delivery systems, and helping tribes identify local priorities for health care delivery and health education. NTEC serves the 43 federally recognized tribes in Idaho, Oregon, and Washington. The center is housed in the Northwest Portland Area Indian Health Board (NPAIHB), whose delegates, representing the member tribes, direct and oversee activities, including health promotion, disease prevention, training and technical assistance.
The IHS plans for this to be a pilot project, possibly pointing the way for other tribal EpiCenters to launch similar projects.
American Indians and Alaska Natives (AI/AN) are often misidentified as other races in public health administrative records. In the Northwest, for instance, the Northwest Tribal Epidemiology Center (NTEC) has found that about 10% of AI/AN birth and death records and up to 60% of hospitalization records are misclassified.
Racial misclassification makes it difficult to accurately assess the health of Native people: The numbers affected by a disease may appear lower or higher than they actually are. It can muddle and misrepresent information in birth certificates, cancer registries, death certificates, emergency department records, hospitalization records, injury reports. Without accurate health data, says Lisa Neel, director of the Indian Health Service (IHS) Tribal Epidemiology Center Program, tribes cannot make informed decisions about how best to serve their people.
That is why the IHS and the Center recently signed an agreement supporting a new information-sharing project. The agreement will allow the IHS to provide the NTEC with a list of people who have received health services at IHS, tribal, and urban Indian health programs in the Portland Area. The list will include no information about patients’ medical histories and will not be shared outside the NTEC. The center will then compare the list with outside information sources, such as state cancer registries, to check for racial misclassification.
The NTEC is 1 of 13 national “EpiCenters” charged with collecting tribal health status data, evaluating data monitoring and delivery systems, and helping tribes identify local priorities for health care delivery and health education. NTEC serves the 43 federally recognized tribes in Idaho, Oregon, and Washington. The center is housed in the Northwest Portland Area Indian Health Board (NPAIHB), whose delegates, representing the member tribes, direct and oversee activities, including health promotion, disease prevention, training and technical assistance.
The IHS plans for this to be a pilot project, possibly pointing the way for other tribal EpiCenters to launch similar projects.
FGF21 could be tied to psychopathology of bipolar mania
Patients’ fibroblast growth factor–21 levels dropped after 4 weeks of taking antipsychotics
Fibroblast growth factor–21 (FGF21), a protein that regulates carbohydrate and lipid metabolism, could be a biomarker in patients with bipolar mania, a new study suggests.
“In addition, our data indicates that FGF21 may monitor and/or prevent metabolic abnormalities induced by psychotropic drugs,” wrote Qing Hu of Xiamen City Xianyue Hospital, in Fujian, China, and associates. The study was published in Psychiatry Research.
To investigate how the expression of FGF21 changes in response to psychotropics taken by patients with bipolar mania, the researchers recruited 99 inpatients with bipolar mania with or without psychosis and 99 healthy controls. Eighty-two of the patients received psychotropics only, and 17 received psychotropics and lipid-lowering or hypotensive agents. Those in the smaller group were later excluded from follow-up.
At baseline, no significant differences were found between the patients and controls on several metabolic measures, such as cholesterol and apolipoprotein. The patients with bipolar mania had higher uric acid and triglyceride levels, although the latter was not statistically significant. However, compared with the FGF21 serum levels of the controls.
After 4 weeks of taking the antipsychotics, the patients experienced increases in several metabolic measures, such as BMI (23.68 kg/m2 vs. 24.02 kg/m2), LDL cholesterol (2.61 mg/dL vs. 2.98 mg/dL), and glucose (4.74 mg/dL vs. 4.88 mg/dL). However, their FGF21 levels declined, from 279.45 pg/mL to 215.12 pg/mL.
“In light of these findings, our future research will focus on investigating whether ... the change in FGF21 expression is a causal factor or a consequence of bipolar disorder,” the investigators wrote.
They cited several limitations. One is that psychotropic dosages were not discussed, and another is that evaluation data from the Young Mania Rating Scale were missing.
The researchers reported no conflicts of interest.
SOURCE: Hu Q et al. Psychiatry Res. 2019;272:643-8.
Patients’ fibroblast growth factor–21 levels dropped after 4 weeks of taking antipsychotics
Patients’ fibroblast growth factor–21 levels dropped after 4 weeks of taking antipsychotics
Fibroblast growth factor–21 (FGF21), a protein that regulates carbohydrate and lipid metabolism, could be a biomarker in patients with bipolar mania, a new study suggests.
“In addition, our data indicates that FGF21 may monitor and/or prevent metabolic abnormalities induced by psychotropic drugs,” wrote Qing Hu of Xiamen City Xianyue Hospital, in Fujian, China, and associates. The study was published in Psychiatry Research.
To investigate how the expression of FGF21 changes in response to psychotropics taken by patients with bipolar mania, the researchers recruited 99 inpatients with bipolar mania with or without psychosis and 99 healthy controls. Eighty-two of the patients received psychotropics only, and 17 received psychotropics and lipid-lowering or hypotensive agents. Those in the smaller group were later excluded from follow-up.
At baseline, no significant differences were found between the patients and controls on several metabolic measures, such as cholesterol and apolipoprotein. The patients with bipolar mania had higher uric acid and triglyceride levels, although the latter was not statistically significant. However, compared with the FGF21 serum levels of the controls.
After 4 weeks of taking the antipsychotics, the patients experienced increases in several metabolic measures, such as BMI (23.68 kg/m2 vs. 24.02 kg/m2), LDL cholesterol (2.61 mg/dL vs. 2.98 mg/dL), and glucose (4.74 mg/dL vs. 4.88 mg/dL). However, their FGF21 levels declined, from 279.45 pg/mL to 215.12 pg/mL.
“In light of these findings, our future research will focus on investigating whether ... the change in FGF21 expression is a causal factor or a consequence of bipolar disorder,” the investigators wrote.
They cited several limitations. One is that psychotropic dosages were not discussed, and another is that evaluation data from the Young Mania Rating Scale were missing.
The researchers reported no conflicts of interest.
SOURCE: Hu Q et al. Psychiatry Res. 2019;272:643-8.
Fibroblast growth factor–21 (FGF21), a protein that regulates carbohydrate and lipid metabolism, could be a biomarker in patients with bipolar mania, a new study suggests.
“In addition, our data indicates that FGF21 may monitor and/or prevent metabolic abnormalities induced by psychotropic drugs,” wrote Qing Hu of Xiamen City Xianyue Hospital, in Fujian, China, and associates. The study was published in Psychiatry Research.
To investigate how the expression of FGF21 changes in response to psychotropics taken by patients with bipolar mania, the researchers recruited 99 inpatients with bipolar mania with or without psychosis and 99 healthy controls. Eighty-two of the patients received psychotropics only, and 17 received psychotropics and lipid-lowering or hypotensive agents. Those in the smaller group were later excluded from follow-up.
At baseline, no significant differences were found between the patients and controls on several metabolic measures, such as cholesterol and apolipoprotein. The patients with bipolar mania had higher uric acid and triglyceride levels, although the latter was not statistically significant. However, compared with the FGF21 serum levels of the controls.
After 4 weeks of taking the antipsychotics, the patients experienced increases in several metabolic measures, such as BMI (23.68 kg/m2 vs. 24.02 kg/m2), LDL cholesterol (2.61 mg/dL vs. 2.98 mg/dL), and glucose (4.74 mg/dL vs. 4.88 mg/dL). However, their FGF21 levels declined, from 279.45 pg/mL to 215.12 pg/mL.
“In light of these findings, our future research will focus on investigating whether ... the change in FGF21 expression is a causal factor or a consequence of bipolar disorder,” the investigators wrote.
They cited several limitations. One is that psychotropic dosages were not discussed, and another is that evaluation data from the Young Mania Rating Scale were missing.
The researchers reported no conflicts of interest.
SOURCE: Hu Q et al. Psychiatry Res. 2019;272:643-8.
FROM PSYCHIATRY RESEARCH
Does PTSD Get Passed Down?
Do parents pass along posttraumatic stress disorder (PTSD) to their children? Researchers from Universidade do Porto in Portugal, say although it seems a reasonable possibility, the “degree of controversy is high,” and studies have had conflicting results. For instance, some research has found that children of war veterans with PTSD have higher depression scores and higher rates of aggression and anxiety. While other research has shown no differences between veterans’ and nonveterans’ children.
The Universidade do Porto study involved 46 veterans of Portugal’s war with Angola, Mozambique, and Guinea from 1961 to 1974. The researchers studied the association of war veterans’ PTSD lifetime diagnosis and war exposure intensity with the self-reported psychopathology of their adult offspring, assessed 40 years after the end of the war. They also studied childhood adversities and attachment patterns, which have been implicated in intergenerational transmission of trauma and PTSD.
Both veterans and offspring were assessed via questionnaires, clinical interviews, and symptom scales, including the Brief Symptom Inventory (BSI). The veterans also answered the War Experiences Questionnaire. Offspring of fathers with PTSD were not different from offspring of fathers without PTSD, with respect to age, gender, socioeconomic status, and marital status.
The researchers found no association between the veterans’ lifetime PTSD and their children’s psychopathology, attachment dimensions, and self-reported overall childhood maltreatment. The fathers’ war experience carried more weight. It seemed, the researchers say, that the children were able to overcome living with a parent’s PTSD symptoms, but they were less resilient when it came to their fathers’ war experience.
Veterans’ war exposure was associated with BSI in the offspring with regard to somatization, phobic anxiety, Global Severity Index, and Positive Symptom Distress Index. It was also associated with offspring’s physical neglect as a childhood adversity.
These findings could have considerable social importance, the researchers say. They suggest that mental health support could benefit the children especially if provided early after highly traumatized veterans return from war, “not just later on—if and when they develop PTSD.”
Do parents pass along posttraumatic stress disorder (PTSD) to their children? Researchers from Universidade do Porto in Portugal, say although it seems a reasonable possibility, the “degree of controversy is high,” and studies have had conflicting results. For instance, some research has found that children of war veterans with PTSD have higher depression scores and higher rates of aggression and anxiety. While other research has shown no differences between veterans’ and nonveterans’ children.
The Universidade do Porto study involved 46 veterans of Portugal’s war with Angola, Mozambique, and Guinea from 1961 to 1974. The researchers studied the association of war veterans’ PTSD lifetime diagnosis and war exposure intensity with the self-reported psychopathology of their adult offspring, assessed 40 years after the end of the war. They also studied childhood adversities and attachment patterns, which have been implicated in intergenerational transmission of trauma and PTSD.
Both veterans and offspring were assessed via questionnaires, clinical interviews, and symptom scales, including the Brief Symptom Inventory (BSI). The veterans also answered the War Experiences Questionnaire. Offspring of fathers with PTSD were not different from offspring of fathers without PTSD, with respect to age, gender, socioeconomic status, and marital status.
The researchers found no association between the veterans’ lifetime PTSD and their children’s psychopathology, attachment dimensions, and self-reported overall childhood maltreatment. The fathers’ war experience carried more weight. It seemed, the researchers say, that the children were able to overcome living with a parent’s PTSD symptoms, but they were less resilient when it came to their fathers’ war experience.
Veterans’ war exposure was associated with BSI in the offspring with regard to somatization, phobic anxiety, Global Severity Index, and Positive Symptom Distress Index. It was also associated with offspring’s physical neglect as a childhood adversity.
These findings could have considerable social importance, the researchers say. They suggest that mental health support could benefit the children especially if provided early after highly traumatized veterans return from war, “not just later on—if and when they develop PTSD.”
Do parents pass along posttraumatic stress disorder (PTSD) to their children? Researchers from Universidade do Porto in Portugal, say although it seems a reasonable possibility, the “degree of controversy is high,” and studies have had conflicting results. For instance, some research has found that children of war veterans with PTSD have higher depression scores and higher rates of aggression and anxiety. While other research has shown no differences between veterans’ and nonveterans’ children.
The Universidade do Porto study involved 46 veterans of Portugal’s war with Angola, Mozambique, and Guinea from 1961 to 1974. The researchers studied the association of war veterans’ PTSD lifetime diagnosis and war exposure intensity with the self-reported psychopathology of their adult offspring, assessed 40 years after the end of the war. They also studied childhood adversities and attachment patterns, which have been implicated in intergenerational transmission of trauma and PTSD.
Both veterans and offspring were assessed via questionnaires, clinical interviews, and symptom scales, including the Brief Symptom Inventory (BSI). The veterans also answered the War Experiences Questionnaire. Offspring of fathers with PTSD were not different from offspring of fathers without PTSD, with respect to age, gender, socioeconomic status, and marital status.
The researchers found no association between the veterans’ lifetime PTSD and their children’s psychopathology, attachment dimensions, and self-reported overall childhood maltreatment. The fathers’ war experience carried more weight. It seemed, the researchers say, that the children were able to overcome living with a parent’s PTSD symptoms, but they were less resilient when it came to their fathers’ war experience.
Veterans’ war exposure was associated with BSI in the offspring with regard to somatization, phobic anxiety, Global Severity Index, and Positive Symptom Distress Index. It was also associated with offspring’s physical neglect as a childhood adversity.
These findings could have considerable social importance, the researchers say. They suggest that mental health support could benefit the children especially if provided early after highly traumatized veterans return from war, “not just later on—if and when they develop PTSD.”
Smoldering Lesions: Red Flags for Severe MS
“Smoldering” lesions—signaling chronic inflammation—may be a hallmark of more aggressive forms of multiple sclerosis (MS), according to researchers from the National Institute of Neurological Disorders and Stroke (NINDS). New technology that allows long-term in vivo monitoring could make it possible for the first time to predict who is at risk for progressive MS and potential treatments.
MS lesions appear as spots on brain scans. Some lesions heal. Others remain and may have characteristic dark rims, which is inflammatory demyelination at the edges. The dark-rimmed lesions appear to expand, or “smolder” for years. But until recently, researchers did not fully understand what role those chronic active lesions played in MS because it was difficult to find the ones that remain inflamed.
The researchers conducted 3 studies at the NIH Clinical Center. In the first, using a high-powered, 7-tesla MRI scanner and a 3D printer, they scanned the brains of 192 MS patients. Of those, 40% had no rimmed lesions; 32% had 1 to 3 rims; and 20% had ≥ 4 rims. Regardless of the treatment they were receiving, 56% of the patients had at < 1 rimmed lesion.
The researchers compared the brain scans to the patients’ baseline neurologic examinations. Patients with ≥ 4 rimmed lesions were nearly twice as likely to be diagnosed with progressive MS than were those without rimmed lesions. Moreover, the patients with rimmed lesions developed motor and cognitive disabilities at a younger age than did patients without rimmed lesions. Patients with ≥ 4 rimmed lesions also had less white matter and smaller basal ganglia.
When they analyzed a subset of patients whose brains had been scanned once a year for ≥ 10 years, the researchers found that although the rimless lesions generally shrank, the rimmed lesions grew or stayed the same size and were “particularly damaged.”
The team also used a 3D printer to compare the spots they had seen on scans with lesions in brain tissue samples from a patient who died during the trial. All 10 expanding rimmed spots on the scans had the “telltale features” of chronic active lesions when examined under a microscope.
“Figuring out how to spot chronic active lesions was a big step,” said research team member Martina Absinta, MD, PhD. “We could not have done it without the high-powered MRI scanner.” Most MRI scanners used clinically have field strengths of 1.5 or 3 Tesla. The research team had previously published instructions for programming lower powered MRI scanners to detect rimmed chronic active lesions.
Chronic active lesions are common and exert ongoing tissue damage, said Daniel S. Reich, MD, PHD, senior investigator at NINDS, and senior author of the paper. The fact that these lesions are present in patients who are receiving anti-inflammatory drugs, he added, suggests that the field of MS research may want to focus on new treatments that target the brain’s unique immune system—especially a type of brain cell called microglia, which are instrumental in the immune response.
Their findings, the researchers say, should prompt MRI-based clinical trials aimed at treating perilesional chronic inflammation in MS. Dr. Reich said, “Our results point the way toward using specialized brain scans to predict who is at risk of developing progressive MS.”
“Smoldering” lesions—signaling chronic inflammation—may be a hallmark of more aggressive forms of multiple sclerosis (MS), according to researchers from the National Institute of Neurological Disorders and Stroke (NINDS). New technology that allows long-term in vivo monitoring could make it possible for the first time to predict who is at risk for progressive MS and potential treatments.
MS lesions appear as spots on brain scans. Some lesions heal. Others remain and may have characteristic dark rims, which is inflammatory demyelination at the edges. The dark-rimmed lesions appear to expand, or “smolder” for years. But until recently, researchers did not fully understand what role those chronic active lesions played in MS because it was difficult to find the ones that remain inflamed.
The researchers conducted 3 studies at the NIH Clinical Center. In the first, using a high-powered, 7-tesla MRI scanner and a 3D printer, they scanned the brains of 192 MS patients. Of those, 40% had no rimmed lesions; 32% had 1 to 3 rims; and 20% had ≥ 4 rims. Regardless of the treatment they were receiving, 56% of the patients had at < 1 rimmed lesion.
The researchers compared the brain scans to the patients’ baseline neurologic examinations. Patients with ≥ 4 rimmed lesions were nearly twice as likely to be diagnosed with progressive MS than were those without rimmed lesions. Moreover, the patients with rimmed lesions developed motor and cognitive disabilities at a younger age than did patients without rimmed lesions. Patients with ≥ 4 rimmed lesions also had less white matter and smaller basal ganglia.
When they analyzed a subset of patients whose brains had been scanned once a year for ≥ 10 years, the researchers found that although the rimless lesions generally shrank, the rimmed lesions grew or stayed the same size and were “particularly damaged.”
The team also used a 3D printer to compare the spots they had seen on scans with lesions in brain tissue samples from a patient who died during the trial. All 10 expanding rimmed spots on the scans had the “telltale features” of chronic active lesions when examined under a microscope.
“Figuring out how to spot chronic active lesions was a big step,” said research team member Martina Absinta, MD, PhD. “We could not have done it without the high-powered MRI scanner.” Most MRI scanners used clinically have field strengths of 1.5 or 3 Tesla. The research team had previously published instructions for programming lower powered MRI scanners to detect rimmed chronic active lesions.
Chronic active lesions are common and exert ongoing tissue damage, said Daniel S. Reich, MD, PHD, senior investigator at NINDS, and senior author of the paper. The fact that these lesions are present in patients who are receiving anti-inflammatory drugs, he added, suggests that the field of MS research may want to focus on new treatments that target the brain’s unique immune system—especially a type of brain cell called microglia, which are instrumental in the immune response.
Their findings, the researchers say, should prompt MRI-based clinical trials aimed at treating perilesional chronic inflammation in MS. Dr. Reich said, “Our results point the way toward using specialized brain scans to predict who is at risk of developing progressive MS.”
“Smoldering” lesions—signaling chronic inflammation—may be a hallmark of more aggressive forms of multiple sclerosis (MS), according to researchers from the National Institute of Neurological Disorders and Stroke (NINDS). New technology that allows long-term in vivo monitoring could make it possible for the first time to predict who is at risk for progressive MS and potential treatments.
MS lesions appear as spots on brain scans. Some lesions heal. Others remain and may have characteristic dark rims, which is inflammatory demyelination at the edges. The dark-rimmed lesions appear to expand, or “smolder” for years. But until recently, researchers did not fully understand what role those chronic active lesions played in MS because it was difficult to find the ones that remain inflamed.
The researchers conducted 3 studies at the NIH Clinical Center. In the first, using a high-powered, 7-tesla MRI scanner and a 3D printer, they scanned the brains of 192 MS patients. Of those, 40% had no rimmed lesions; 32% had 1 to 3 rims; and 20% had ≥ 4 rims. Regardless of the treatment they were receiving, 56% of the patients had at < 1 rimmed lesion.
The researchers compared the brain scans to the patients’ baseline neurologic examinations. Patients with ≥ 4 rimmed lesions were nearly twice as likely to be diagnosed with progressive MS than were those without rimmed lesions. Moreover, the patients with rimmed lesions developed motor and cognitive disabilities at a younger age than did patients without rimmed lesions. Patients with ≥ 4 rimmed lesions also had less white matter and smaller basal ganglia.
When they analyzed a subset of patients whose brains had been scanned once a year for ≥ 10 years, the researchers found that although the rimless lesions generally shrank, the rimmed lesions grew or stayed the same size and were “particularly damaged.”
The team also used a 3D printer to compare the spots they had seen on scans with lesions in brain tissue samples from a patient who died during the trial. All 10 expanding rimmed spots on the scans had the “telltale features” of chronic active lesions when examined under a microscope.
“Figuring out how to spot chronic active lesions was a big step,” said research team member Martina Absinta, MD, PhD. “We could not have done it without the high-powered MRI scanner.” Most MRI scanners used clinically have field strengths of 1.5 or 3 Tesla. The research team had previously published instructions for programming lower powered MRI scanners to detect rimmed chronic active lesions.
Chronic active lesions are common and exert ongoing tissue damage, said Daniel S. Reich, MD, PHD, senior investigator at NINDS, and senior author of the paper. The fact that these lesions are present in patients who are receiving anti-inflammatory drugs, he added, suggests that the field of MS research may want to focus on new treatments that target the brain’s unique immune system—especially a type of brain cell called microglia, which are instrumental in the immune response.
Their findings, the researchers say, should prompt MRI-based clinical trials aimed at treating perilesional chronic inflammation in MS. Dr. Reich said, “Our results point the way toward using specialized brain scans to predict who is at risk of developing progressive MS.”
FUO, pneumonia often distinguishes influenza from RSV in hospitalized young children
LJUBLJANA, SLOVENIA – as the cause of hospitalization in infants and young children, Cihan Papan, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.

Dr. Papan, a pediatrician at University Children’s Hospital Mannheim (Germany) and Heidelberg (Germany) University, presented a retrospective single-center study of all 573 children aged under 2 years hospitalized over the course of several seasons for respiratory syncytial virus (RSV) or influenza as confirmed by rapid antigen testing. Even though these are two of the leading causes of hospitalization among young children, there is surprisingly sparse data comparing the two in terms of disease severity and hospital resource utilization, including antibiotic consumption. That information gap provided the basis for this study.
There were 476 children with confirmed RSV, 96 with influenza, and 1 RSV/influenza coinfection. Notably, even though the RSV group had lower temperatures and C-reactive protein levels, they were nevertheless more likely to be treated with antibiotics, by a margin of 29% to 23%.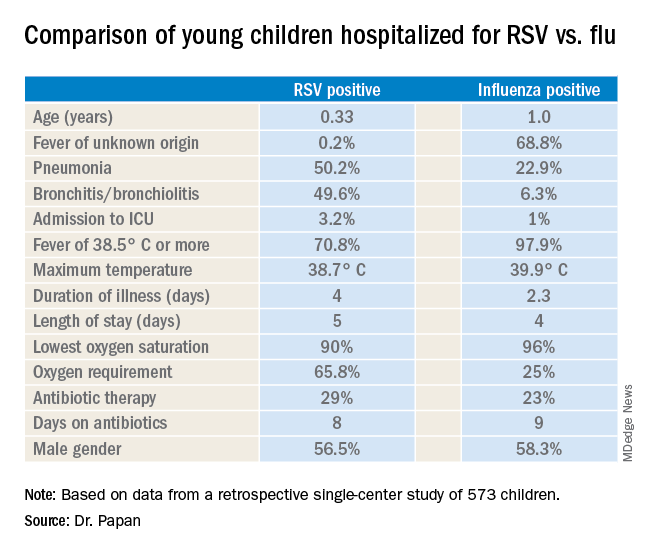
“These findings open new possibilities for antimicrobial stewardship in these groups of virally infected children,” observed Dr. Papan.
Fever of unknown origin was present in 68.8% of the influenza-positive patients, compared with just 0.2% of the RSV-positive children. In contrast, 50.2% of the RSV group had pneumonia and 49.6% had bronchitis or bronchiolitis, versus just 22.9% and 6.3% of the influenza patients, respectively. A larger proportion of the young children with RSV infection presented in a severely ill–looking condition. Children with RSV infection also were significantly younger.
Dr. Papan reported having no financial conflicts regarding his study.
LJUBLJANA, SLOVENIA – as the cause of hospitalization in infants and young children, Cihan Papan, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
Dr. Papan, a pediatrician at University Children’s Hospital Mannheim (Germany) and Heidelberg (Germany) University, presented a retrospective single-center study of all 573 children aged under 2 years hospitalized over the course of several seasons for respiratory syncytial virus (RSV) or influenza as confirmed by rapid antigen testing. Even though these are two of the leading causes of hospitalization among young children, there is surprisingly sparse data comparing the two in terms of disease severity and hospital resource utilization, including antibiotic consumption. That information gap provided the basis for this study.
There were 476 children with confirmed RSV, 96 with influenza, and 1 RSV/influenza coinfection. Notably, even though the RSV group had lower temperatures and C-reactive protein levels, they were nevertheless more likely to be treated with antibiotics, by a margin of 29% to 23%.
“These findings open new possibilities for antimicrobial stewardship in these groups of virally infected children,” observed Dr. Papan.
Fever of unknown origin was present in 68.8% of the influenza-positive patients, compared with just 0.2% of the RSV-positive children. In contrast, 50.2% of the RSV group had pneumonia and 49.6% had bronchitis or bronchiolitis, versus just 22.9% and 6.3% of the influenza patients, respectively. A larger proportion of the young children with RSV infection presented in a severely ill–looking condition. Children with RSV infection also were significantly younger.
Dr. Papan reported having no financial conflicts regarding his study.
LJUBLJANA, SLOVENIA – as the cause of hospitalization in infants and young children, Cihan Papan, MD, reported at the annual meeting of the European Society for Paediatric Infectious Diseases.
Dr. Papan, a pediatrician at University Children’s Hospital Mannheim (Germany) and Heidelberg (Germany) University, presented a retrospective single-center study of all 573 children aged under 2 years hospitalized over the course of several seasons for respiratory syncytial virus (RSV) or influenza as confirmed by rapid antigen testing. Even though these are two of the leading causes of hospitalization among young children, there is surprisingly sparse data comparing the two in terms of disease severity and hospital resource utilization, including antibiotic consumption. That information gap provided the basis for this study.
There were 476 children with confirmed RSV, 96 with influenza, and 1 RSV/influenza coinfection. Notably, even though the RSV group had lower temperatures and C-reactive protein levels, they were nevertheless more likely to be treated with antibiotics, by a margin of 29% to 23%.
“These findings open new possibilities for antimicrobial stewardship in these groups of virally infected children,” observed Dr. Papan.
Fever of unknown origin was present in 68.8% of the influenza-positive patients, compared with just 0.2% of the RSV-positive children. In contrast, 50.2% of the RSV group had pneumonia and 49.6% had bronchitis or bronchiolitis, versus just 22.9% and 6.3% of the influenza patients, respectively. A larger proportion of the young children with RSV infection presented in a severely ill–looking condition. Children with RSV infection also were significantly younger.
Dr. Papan reported having no financial conflicts regarding his study.
REPORTING FROM ESPID 2019
PTSD symptom reduction tied to lower risk of type 2 diabetes
Veterans with a clinically meaningful reduction in symptoms of PTSD are less likely to develop type 2 diabetes, research from a retrospective study shows.
“We cautiously speculate that normalization of hypothalamic-pituitary-adrenal axis and cortisol levels could be one mechanism behind our results,” wrote Jeffrey F. Scherrer, PhD, and colleagues. “PTSD is associated with inflammation, which may in turn be associated with increased risk for [type 2 diabetes].” The study was published in JAMA Psychiatry.
Using medical record data from the Veterans Health Administration, Dr. Scherrer and colleagues identified 5,916 patients with PTSD who visited a VHA medical center between 2008 and 2012, and scored at least 50 points or higher on the PTSD Checklist (PCL) followed by another PCL score at least 8 months after the previous score. The mean age of patients in the study was 42.1 years, the cohort consisted of 84.3% men, and 66.3% patients were white. PCL score reduction was deemed clinically meaningful if there was a decrease of 20 points or more in the score, reported Dr. Scherrer of the department of family and community medicine at Saint Louis University and colleagues.
Patients who were older (mean 43.6 years vs. mean 41.7 years; P = .02) and those who underwent minimally adequate duration of PTSD psychotherapy (P less than .001) were significantly more likely to have a clinically meaningful decrease in PCL scores. Patients who received antidepressants (P = .004) or antipsychotics (P less than .001) were significantly more likely to have less than clinically meaningful decreases in PCL scores. Factors that put patients at significantly higher risk of developing type 2 diabetes included older age (hazard ratio, 1.05; 95% confidence interval, 1.04-1.07; P less than .001), black race/ethnicity (HR, 1.86; 95% CI, 1.23-2.83; P = .004), hypertension (HR, 3.46; 95% CI, 2.33-5.16), hyperlipidemia (HR, 2.82; 95% CI, 1.91-4.16), and obesity (HR, 3.32; 95% CI, 2.12-5.21) (all P less than .001).
Minimally adequate duration of PTSD psychotherapy and high use of primary care health services also were associated with developing type 2 diabetes.
In a Cox proportional hazards regression model, patients with clinically meaningful decreases in PCL scores had significantly lower risk of developing type 2 diabetes, and those results remained consistent after adjusting for age, calculating the results using weighted data, and factoring in hypertension, obesity, and hyperlipidemia.
“This result was independent of numerous demographics and psychiatric and physical comorbidities,” said Dr. Scherrer and colleagues. “The association was also independent of the number of PTSD psychotherapy sessions used, suggesting that a healthy adherer effect, or a general orientation to improve health, is unlikely to explain our observations.”
Dr. Scherrer and colleagues cited several limitations, such as unmeasured confounding and the difficulty of generalizing the results beyond PTSD patients in a VHA setting. In addition, the researchers were unable to calculate the lifetime effect of reduced PTSD symptoms and incidence of type 2 diabetes.
This study was funded in part by a grant from the National Heart, Lung, and Blood Institute. Four authors reported receiving one or more grants from the National Heart, Lung, and Blood Institute during the study period. Some authors reported receiving other support from Noblis Therapeutics and Saint Louis University both during and outside the study period. The other authors reported no relevant conflicts of interest.
SOURCE: Scherrer JF et al. JAMA Psychiatry. 2019 Aug 21. doi: 10.1001/jamapsychiatry.2019.2096.
Veterans with a clinically meaningful reduction in symptoms of PTSD are less likely to develop type 2 diabetes, research from a retrospective study shows.
“We cautiously speculate that normalization of hypothalamic-pituitary-adrenal axis and cortisol levels could be one mechanism behind our results,” wrote Jeffrey F. Scherrer, PhD, and colleagues. “PTSD is associated with inflammation, which may in turn be associated with increased risk for [type 2 diabetes].” The study was published in JAMA Psychiatry.
Using medical record data from the Veterans Health Administration, Dr. Scherrer and colleagues identified 5,916 patients with PTSD who visited a VHA medical center between 2008 and 2012, and scored at least 50 points or higher on the PTSD Checklist (PCL) followed by another PCL score at least 8 months after the previous score. The mean age of patients in the study was 42.1 years, the cohort consisted of 84.3% men, and 66.3% patients were white. PCL score reduction was deemed clinically meaningful if there was a decrease of 20 points or more in the score, reported Dr. Scherrer of the department of family and community medicine at Saint Louis University and colleagues.
Patients who were older (mean 43.6 years vs. mean 41.7 years; P = .02) and those who underwent minimally adequate duration of PTSD psychotherapy (P less than .001) were significantly more likely to have a clinically meaningful decrease in PCL scores. Patients who received antidepressants (P = .004) or antipsychotics (P less than .001) were significantly more likely to have less than clinically meaningful decreases in PCL scores. Factors that put patients at significantly higher risk of developing type 2 diabetes included older age (hazard ratio, 1.05; 95% confidence interval, 1.04-1.07; P less than .001), black race/ethnicity (HR, 1.86; 95% CI, 1.23-2.83; P = .004), hypertension (HR, 3.46; 95% CI, 2.33-5.16), hyperlipidemia (HR, 2.82; 95% CI, 1.91-4.16), and obesity (HR, 3.32; 95% CI, 2.12-5.21) (all P less than .001).
Minimally adequate duration of PTSD psychotherapy and high use of primary care health services also were associated with developing type 2 diabetes.
In a Cox proportional hazards regression model, patients with clinically meaningful decreases in PCL scores had significantly lower risk of developing type 2 diabetes, and those results remained consistent after adjusting for age, calculating the results using weighted data, and factoring in hypertension, obesity, and hyperlipidemia.
“This result was independent of numerous demographics and psychiatric and physical comorbidities,” said Dr. Scherrer and colleagues. “The association was also independent of the number of PTSD psychotherapy sessions used, suggesting that a healthy adherer effect, or a general orientation to improve health, is unlikely to explain our observations.”
Dr. Scherrer and colleagues cited several limitations, such as unmeasured confounding and the difficulty of generalizing the results beyond PTSD patients in a VHA setting. In addition, the researchers were unable to calculate the lifetime effect of reduced PTSD symptoms and incidence of type 2 diabetes.
This study was funded in part by a grant from the National Heart, Lung, and Blood Institute. Four authors reported receiving one or more grants from the National Heart, Lung, and Blood Institute during the study period. Some authors reported receiving other support from Noblis Therapeutics and Saint Louis University both during and outside the study period. The other authors reported no relevant conflicts of interest.
SOURCE: Scherrer JF et al. JAMA Psychiatry. 2019 Aug 21. doi: 10.1001/jamapsychiatry.2019.2096.
Veterans with a clinically meaningful reduction in symptoms of PTSD are less likely to develop type 2 diabetes, research from a retrospective study shows.
“We cautiously speculate that normalization of hypothalamic-pituitary-adrenal axis and cortisol levels could be one mechanism behind our results,” wrote Jeffrey F. Scherrer, PhD, and colleagues. “PTSD is associated with inflammation, which may in turn be associated with increased risk for [type 2 diabetes].” The study was published in JAMA Psychiatry.
Using medical record data from the Veterans Health Administration, Dr. Scherrer and colleagues identified 5,916 patients with PTSD who visited a VHA medical center between 2008 and 2012, and scored at least 50 points or higher on the PTSD Checklist (PCL) followed by another PCL score at least 8 months after the previous score. The mean age of patients in the study was 42.1 years, the cohort consisted of 84.3% men, and 66.3% patients were white. PCL score reduction was deemed clinically meaningful if there was a decrease of 20 points or more in the score, reported Dr. Scherrer of the department of family and community medicine at Saint Louis University and colleagues.
Patients who were older (mean 43.6 years vs. mean 41.7 years; P = .02) and those who underwent minimally adequate duration of PTSD psychotherapy (P less than .001) were significantly more likely to have a clinically meaningful decrease in PCL scores. Patients who received antidepressants (P = .004) or antipsychotics (P less than .001) were significantly more likely to have less than clinically meaningful decreases in PCL scores. Factors that put patients at significantly higher risk of developing type 2 diabetes included older age (hazard ratio, 1.05; 95% confidence interval, 1.04-1.07; P less than .001), black race/ethnicity (HR, 1.86; 95% CI, 1.23-2.83; P = .004), hypertension (HR, 3.46; 95% CI, 2.33-5.16), hyperlipidemia (HR, 2.82; 95% CI, 1.91-4.16), and obesity (HR, 3.32; 95% CI, 2.12-5.21) (all P less than .001).
Minimally adequate duration of PTSD psychotherapy and high use of primary care health services also were associated with developing type 2 diabetes.
In a Cox proportional hazards regression model, patients with clinically meaningful decreases in PCL scores had significantly lower risk of developing type 2 diabetes, and those results remained consistent after adjusting for age, calculating the results using weighted data, and factoring in hypertension, obesity, and hyperlipidemia.
“This result was independent of numerous demographics and psychiatric and physical comorbidities,” said Dr. Scherrer and colleagues. “The association was also independent of the number of PTSD psychotherapy sessions used, suggesting that a healthy adherer effect, or a general orientation to improve health, is unlikely to explain our observations.”
Dr. Scherrer and colleagues cited several limitations, such as unmeasured confounding and the difficulty of generalizing the results beyond PTSD patients in a VHA setting. In addition, the researchers were unable to calculate the lifetime effect of reduced PTSD symptoms and incidence of type 2 diabetes.
This study was funded in part by a grant from the National Heart, Lung, and Blood Institute. Four authors reported receiving one or more grants from the National Heart, Lung, and Blood Institute during the study period. Some authors reported receiving other support from Noblis Therapeutics and Saint Louis University both during and outside the study period. The other authors reported no relevant conflicts of interest.
SOURCE: Scherrer JF et al. JAMA Psychiatry. 2019 Aug 21. doi: 10.1001/jamapsychiatry.2019.2096.
FROM JAMA PSYCHIATRY
New Method Helps Restore Respiratory Muscle Function in Patients with Spinal Cord Injury
Many patients with spinal cord injury (SCI) need mechanical ventilatory support. One type of support is diaphragm pacing, which stimulates the diaphragm, helping the person breathe. A minimally invasive form of diaphragm pacing via laparoscopically placed intramuscular diaphragm electrodes has “liberated thousands of patients from mechanical ventilation,” says Anthony DiMarco, MD. He and VA colleague Krzysztof Kowalski, PhD, have found a way to completely restore respiratory muscle function in patients with SCI safely and effectively.
In mid-thoracic and higher level SCIs, the expiratory muscles are paralyzed, putting patients at risk for respiratory tract infections and atelectasis, a major cause of morbidity and mortality in that population. The research team, led by DiMarco and Kowalski, combined diaphragm pacing with a minimally invasive system that allows the patient—simply with the press of a button—to cough effectively, reducing the risk of aspiration and infections. It is the first method in the world, says Dr. Kowalski, that activates abdominal and lower rib cage muscles to produce an effective cough.
An interventional clinical trial in 3 patients demonstrated that using the 2 systems in tandem was safe. The new system was implanted surgically, with disc electrodes placed on the dorsal surface of the spinal cord via laminectomy. Participants in the study used a stimulator to produce several different cough efforts from light to strong.
Mean peak expiratory airflow and airway pressure generation during spontaneous efforts were 1.7 ± 0.2 L/s and 31 ± 7 cmH2O, respectively. After the spinal cord stimulation was applied, peak expiratory airflow was 9.0 ± 1.9 L/s and airway pressure generation was 90 ± 6 cmH2O. In other words, results “characteristic of a normal cough,” the researchers concluded. Moreover, each patient raised secretions much more easily.
The research is being done at the Cleveland Functional Electrical Stimulation Center, a consortium of MetroHealth Medical Center, Case Western Reserve University, and Louis Stokes Cleveland VA Medical Center.
Army veteran David Powers, one of the study participants, in an interview with the VAntage Point blog, says, “Being a part of this research trial has made me feel great. For not only my own health but helping to improve the lives of others as well.”
Many patients with spinal cord injury (SCI) need mechanical ventilatory support. One type of support is diaphragm pacing, which stimulates the diaphragm, helping the person breathe. A minimally invasive form of diaphragm pacing via laparoscopically placed intramuscular diaphragm electrodes has “liberated thousands of patients from mechanical ventilation,” says Anthony DiMarco, MD. He and VA colleague Krzysztof Kowalski, PhD, have found a way to completely restore respiratory muscle function in patients with SCI safely and effectively.
In mid-thoracic and higher level SCIs, the expiratory muscles are paralyzed, putting patients at risk for respiratory tract infections and atelectasis, a major cause of morbidity and mortality in that population. The research team, led by DiMarco and Kowalski, combined diaphragm pacing with a minimally invasive system that allows the patient—simply with the press of a button—to cough effectively, reducing the risk of aspiration and infections. It is the first method in the world, says Dr. Kowalski, that activates abdominal and lower rib cage muscles to produce an effective cough.
An interventional clinical trial in 3 patients demonstrated that using the 2 systems in tandem was safe. The new system was implanted surgically, with disc electrodes placed on the dorsal surface of the spinal cord via laminectomy. Participants in the study used a stimulator to produce several different cough efforts from light to strong.
Mean peak expiratory airflow and airway pressure generation during spontaneous efforts were 1.7 ± 0.2 L/s and 31 ± 7 cmH2O, respectively. After the spinal cord stimulation was applied, peak expiratory airflow was 9.0 ± 1.9 L/s and airway pressure generation was 90 ± 6 cmH2O. In other words, results “characteristic of a normal cough,” the researchers concluded. Moreover, each patient raised secretions much more easily.
The research is being done at the Cleveland Functional Electrical Stimulation Center, a consortium of MetroHealth Medical Center, Case Western Reserve University, and Louis Stokes Cleveland VA Medical Center.
Army veteran David Powers, one of the study participants, in an interview with the VAntage Point blog, says, “Being a part of this research trial has made me feel great. For not only my own health but helping to improve the lives of others as well.”
Many patients with spinal cord injury (SCI) need mechanical ventilatory support. One type of support is diaphragm pacing, which stimulates the diaphragm, helping the person breathe. A minimally invasive form of diaphragm pacing via laparoscopically placed intramuscular diaphragm electrodes has “liberated thousands of patients from mechanical ventilation,” says Anthony DiMarco, MD. He and VA colleague Krzysztof Kowalski, PhD, have found a way to completely restore respiratory muscle function in patients with SCI safely and effectively.
In mid-thoracic and higher level SCIs, the expiratory muscles are paralyzed, putting patients at risk for respiratory tract infections and atelectasis, a major cause of morbidity and mortality in that population. The research team, led by DiMarco and Kowalski, combined diaphragm pacing with a minimally invasive system that allows the patient—simply with the press of a button—to cough effectively, reducing the risk of aspiration and infections. It is the first method in the world, says Dr. Kowalski, that activates abdominal and lower rib cage muscles to produce an effective cough.
An interventional clinical trial in 3 patients demonstrated that using the 2 systems in tandem was safe. The new system was implanted surgically, with disc electrodes placed on the dorsal surface of the spinal cord via laminectomy. Participants in the study used a stimulator to produce several different cough efforts from light to strong.
Mean peak expiratory airflow and airway pressure generation during spontaneous efforts were 1.7 ± 0.2 L/s and 31 ± 7 cmH2O, respectively. After the spinal cord stimulation was applied, peak expiratory airflow was 9.0 ± 1.9 L/s and airway pressure generation was 90 ± 6 cmH2O. In other words, results “characteristic of a normal cough,” the researchers concluded. Moreover, each patient raised secretions much more easily.
The research is being done at the Cleveland Functional Electrical Stimulation Center, a consortium of MetroHealth Medical Center, Case Western Reserve University, and Louis Stokes Cleveland VA Medical Center.
Army veteran David Powers, one of the study participants, in an interview with the VAntage Point blog, says, “Being a part of this research trial has made me feel great. For not only my own health but helping to improve the lives of others as well.”
Cardiovascular cost of smoking may last up to 25 years
Quitting smoking significantly reduces the risk of cardiovascular disease, but past smokers are still at elevated cardiovascular risk, compared with nonsmokers, for up to 25 years after smoking cessation, research in JAMA suggests.

A retrospective analysis of data from 8,770 individuals in the Framingham Heart Study compared the incidence of myocardial infarction, stroke, heart failure, or cardiovascular death in ever-smokers with that of never smokers.
Only 40% of the total cohort had never smoked. Of the 4,115 current smokers at baseline, 38.6% quit during the course of the study and did not relapse but 51.4% continued to smoke until they developed cardiovascular disease or dropped out of the study.
Current smokers had a significant 4.68-fold higher incidence of cardiovascular disease, compared with those who had never smoked, but those who stopped smoking showed a 39% decline in their risk of cardiovascular disease within 5 years of cessation.
However, individuals who were formerly heavy smokers – defined as at least 20 pack-years of smoking – retained a risk of cardiovascular disease 25% higher than that of never smokers until 10-15 years after quitting smoking. At 16 years, the 95% confidence interval for cardiovascular disease risk among former smokers versus that of never smokers finally and consistently included the null value of 1.
The study pooled two cohorts; the original cohort, who attended their fourth examination during 1954-1958 and an offspring cohort who attended their first examination during 1971-1975. The authors saw a difference between the two cohorts in the time course of cardiovascular disease risk in heavy smokers.
In the original cohort, former heavy smoking ceased to be significantly associated with increased cardiovascular disease risk within 5-10 years of cessation, but in the offspring cohort, it took 25 years after cessation for the incidence to decline to the same level of risk seen in never smokers.
“The upper estimate of this time course is a decade longer than that of the Nurses’ Health Study results for coronary heart disease and cardiovascular death and more than 20 years longer than in some prior reports for coronary heart disease and stroke,” wrote Meredith S. Duncan from the division of cardiovascular medicine at the Vanderbilt University Medical Center, Nashville, Tenn., and coauthors. “Although the exact amount of time after quitting at which former smokers’ CVD risk ceases to differ significantly from that of never smokers is unknown (and may further depend on cumulative exposure), these findings support a longer time course of risk reduction than was previously thought, yielding implications for CVD risk stratification of former smokers.”
However, they did note that the study could not account for environmental tobacco smoke exposure and that the participants were mostly of white European ancestry, which limited the generalizability of the findings to other populations.
The Framingham Health Study was supported by the National Heart, Lung, and Blood Institute. One author declared a consultancy with a pharmaceutical company on a proposed clinical trial. No other conflicts of interest were declared.
SOURCE: Duncan M et al. JAMA 2019. doi: 10.1001/jama.2019.10298.
Quitting smoking significantly reduces the risk of cardiovascular disease, but past smokers are still at elevated cardiovascular risk, compared with nonsmokers, for up to 25 years after smoking cessation, research in JAMA suggests.
A retrospective analysis of data from 8,770 individuals in the Framingham Heart Study compared the incidence of myocardial infarction, stroke, heart failure, or cardiovascular death in ever-smokers with that of never smokers.
Only 40% of the total cohort had never smoked. Of the 4,115 current smokers at baseline, 38.6% quit during the course of the study and did not relapse but 51.4% continued to smoke until they developed cardiovascular disease or dropped out of the study.
Current smokers had a significant 4.68-fold higher incidence of cardiovascular disease, compared with those who had never smoked, but those who stopped smoking showed a 39% decline in their risk of cardiovascular disease within 5 years of cessation.
However, individuals who were formerly heavy smokers – defined as at least 20 pack-years of smoking – retained a risk of cardiovascular disease 25% higher than that of never smokers until 10-15 years after quitting smoking. At 16 years, the 95% confidence interval for cardiovascular disease risk among former smokers versus that of never smokers finally and consistently included the null value of 1.
The study pooled two cohorts; the original cohort, who attended their fourth examination during 1954-1958 and an offspring cohort who attended their first examination during 1971-1975. The authors saw a difference between the two cohorts in the time course of cardiovascular disease risk in heavy smokers.
In the original cohort, former heavy smoking ceased to be significantly associated with increased cardiovascular disease risk within 5-10 years of cessation, but in the offspring cohort, it took 25 years after cessation for the incidence to decline to the same level of risk seen in never smokers.
“The upper estimate of this time course is a decade longer than that of the Nurses’ Health Study results for coronary heart disease and cardiovascular death and more than 20 years longer than in some prior reports for coronary heart disease and stroke,” wrote Meredith S. Duncan from the division of cardiovascular medicine at the Vanderbilt University Medical Center, Nashville, Tenn., and coauthors. “Although the exact amount of time after quitting at which former smokers’ CVD risk ceases to differ significantly from that of never smokers is unknown (and may further depend on cumulative exposure), these findings support a longer time course of risk reduction than was previously thought, yielding implications for CVD risk stratification of former smokers.”
However, they did note that the study could not account for environmental tobacco smoke exposure and that the participants were mostly of white European ancestry, which limited the generalizability of the findings to other populations.
The Framingham Health Study was supported by the National Heart, Lung, and Blood Institute. One author declared a consultancy with a pharmaceutical company on a proposed clinical trial. No other conflicts of interest were declared.
SOURCE: Duncan M et al. JAMA 2019. doi: 10.1001/jama.2019.10298.
Quitting smoking significantly reduces the risk of cardiovascular disease, but past smokers are still at elevated cardiovascular risk, compared with nonsmokers, for up to 25 years after smoking cessation, research in JAMA suggests.
A retrospective analysis of data from 8,770 individuals in the Framingham Heart Study compared the incidence of myocardial infarction, stroke, heart failure, or cardiovascular death in ever-smokers with that of never smokers.
Only 40% of the total cohort had never smoked. Of the 4,115 current smokers at baseline, 38.6% quit during the course of the study and did not relapse but 51.4% continued to smoke until they developed cardiovascular disease or dropped out of the study.
Current smokers had a significant 4.68-fold higher incidence of cardiovascular disease, compared with those who had never smoked, but those who stopped smoking showed a 39% decline in their risk of cardiovascular disease within 5 years of cessation.
However, individuals who were formerly heavy smokers – defined as at least 20 pack-years of smoking – retained a risk of cardiovascular disease 25% higher than that of never smokers until 10-15 years after quitting smoking. At 16 years, the 95% confidence interval for cardiovascular disease risk among former smokers versus that of never smokers finally and consistently included the null value of 1.
The study pooled two cohorts; the original cohort, who attended their fourth examination during 1954-1958 and an offspring cohort who attended their first examination during 1971-1975. The authors saw a difference between the two cohorts in the time course of cardiovascular disease risk in heavy smokers.
In the original cohort, former heavy smoking ceased to be significantly associated with increased cardiovascular disease risk within 5-10 years of cessation, but in the offspring cohort, it took 25 years after cessation for the incidence to decline to the same level of risk seen in never smokers.
“The upper estimate of this time course is a decade longer than that of the Nurses’ Health Study results for coronary heart disease and cardiovascular death and more than 20 years longer than in some prior reports for coronary heart disease and stroke,” wrote Meredith S. Duncan from the division of cardiovascular medicine at the Vanderbilt University Medical Center, Nashville, Tenn., and coauthors. “Although the exact amount of time after quitting at which former smokers’ CVD risk ceases to differ significantly from that of never smokers is unknown (and may further depend on cumulative exposure), these findings support a longer time course of risk reduction than was previously thought, yielding implications for CVD risk stratification of former smokers.”
However, they did note that the study could not account for environmental tobacco smoke exposure and that the participants were mostly of white European ancestry, which limited the generalizability of the findings to other populations.
The Framingham Health Study was supported by the National Heart, Lung, and Blood Institute. One author declared a consultancy with a pharmaceutical company on a proposed clinical trial. No other conflicts of interest were declared.
SOURCE: Duncan M et al. JAMA 2019. doi: 10.1001/jama.2019.10298.
FROM JAMA
Key clinical point:
Major finding: In the offspring cohort, heavy smokers showed elevated incidence of CVD for up to 25 years after quitting smoking.
Study details: A retrospective analysis of data from 8,770 individuals in the Framingham Heart Study.
Disclosures: The Framingham Health Study was supported by the National Heart, Lung, and Blood Institute. One author declared a consultancy with a pharmaceutical company on a proposed clinical trial. No other conflicts of interest were declared.
Source: Duncan M et al. JAMA. 2019. doi: 10.1001/jama.2019.10298.