User login
Wildfire smoke impact, part 2: Resources, advice for patients
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.

What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
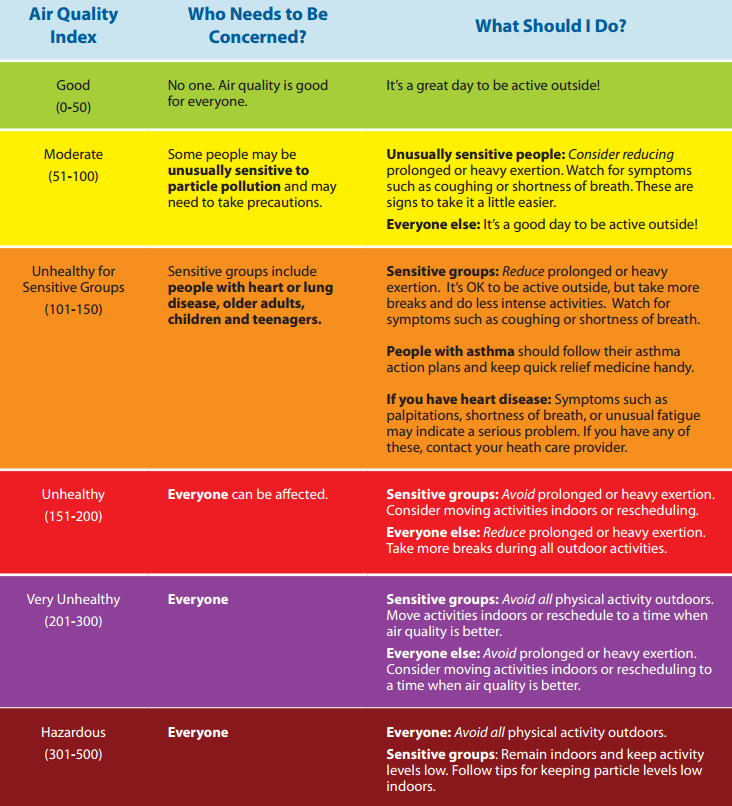
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?

Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality

Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”

The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.
What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?
Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality
Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”
The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Wildfires are on the move in California and communities from the Bay Area to Los Angeles County are once again coping with evacuation, possible destruction of homes, and health concerns related to poor air quality and smoke.
What can doctors tell their patients with cardiovascular and pulmonary conditions about the risks of smoke from wildfires?
EPA resources online
AirNow, a website managed by the Environmental Protection Agency, provides a variety of resources for the public and for health providers, including links to online tutorials, printable health fact sheets, and the newly updated document “Wildfire Smoke: Guide for Public Health Officials 2019.” When wildfire smoke generates an Air Quality Index (AQI) from 101-150, at-risk subgroups like people with asthma, chronic obstructive pulmonary disease (COPD), or heart disease should take precautions.
“An AQI of 151-200 is unhealthy for everyone, and an AQI above 200 is very unhealthy,” John R. Balmes, MD, a pulmonologist at the University of California, San Francisco, and an expert on the respiratory and cardiovascular effects of air pollutants, said in an interview. “That does not mean that everybody is going to die, though. You’re going to have some symptoms of scratchy throat, and you may cough once or twice an hour [from exposure to wildfire smoke], but people who don’t have any preexisting health problems are probably going to be fine and don’t necessarily have to wear an N95 mask. People should wear one if they need to feel comfortable.”
Masks – How much protection?
Wayne Cascio, MD, who directs the EPA’s National Health and Environmental Effects Research Laboratory, notes that some public health officials don’t recommend wearing N95 masks during wildfire smoke events. “There’s a lot of concern that people won’t use them correctly and will therefore feel like they’re protected and will spend more time outdoors than they should and still not get the benefit,” he said. “The masks also pose a challenge for children and for people with severe asthma and COPD.”
Masks also have to fit properly, which can be problematic for kids, added Dr. Balmes, one of the authors of “Wildfires Disaster Guidance: Tips for Staying Healthy During Wildfires” (Am J Respir Crit Care Med. 2019;199[2]:3-4).
“Even the small versions don’t necessarily fit kids well, so they’re not recommended for kids,” he said. “It doesn’t mean a kid couldn’t wear them, but it’s not officially recommended. The actual physiologic work of breathing isn’t much increased by using the N95 mask, but if you’re already struggling to get your breath, or experience dyspnea, then it might be hard to wear one. People with milder COPD can wear an N95 mask just like people with mild asthma if they have to go out.”
The EPA published a tip sheet about where and when to use an N95 or P100 mask, with warnings about the limited protection these devices offer, especially if not used correctly. Most masks do not protect the wearer from harmful gases that can be in wildfire smoke.
Ventilation systems
The EPA also recommends that people with more severe disease should stay indoors and avoid using air conditioning units that only draw in air from the outside or do not have a recirculating option. “If you have to bring in outside air because that’s how your system works, you should have a MERV 13 or better filter to filter out the fine particles,” Dr. Balmes said. “Not every ventilation system can handle it, but most can. That will help the house.”
Dr. Cascio pointed out that the instruction to close all windows and doors is a difficult proposition for people who live in states with moderate weather climates such as Montana and Colorado, where few homes have central air conditioning. “The treatment may be worse than the disease in this case, because it may exacerbate heat stress,” he said. “Try to find a place that has cleaner air. That might be a public building, a school, a fitness center, or a library. Yet we don’t know a lot about whether those areas are cleaner or not. That is currently the subject of some research on our part.”
Traveling away from an area affected by wildfire smoke to ride out the conditions is one option, but that can backfire. One weekend when smoke from the 2008 North Carolina peat fire was particularly troublesome, Dr. Cascio and his family drove about 60 miles west of Greenville to the town of Zebulon, where a minor league baseball game was being played and the air quality was good.
“My thought was to get the family to a better environment for at least a few hours,” Dr. Cascio recalled. “When we arrived in Zebulon the air quality was good as advertised. However, the direction of the wind shifted and the smoke started to move due west and within a short time you could barely see the players on the field. This experience also pointed out one of the lessons of wildfire smoke. That is, in the short term, it is sometimes difficult to predict where it will be present because of the nature of changes in weather and wind.”
Consumer tools to monitor air quality
Colleen E. Reid, PhD, of the department of geography at the University of Colorado, Boulder, an expert on the impact of wildfire smoke on human health, has observed in increase in consumer action to counter smoke inhalation during wildfire events. She said that consumers are buying personal laser particle counters, like the ones made by PurpleAir, to provide a real-time assessment of air quality.
“There is a lot of error with these smaller, cheaper monitors, but I think they give you a sense of trends over time,” Dr. Reid said. “People are trying to figure out how we can work with this sort of real-time data along with the high-quality EPA monitors. If everybody has their own monitor, or ways to better calibrate them to the high-quality data, that would be amazing. Researchers are trying to see how they can use that data to inform our understanding of the spatial and temporal patterning of air pollution.”
The EPA’s Smoke Sense app also holds promise. Characterized on its website as “a citizen science project,” the study uses a free mobile app to engage people living in affected communities to monitor their air quality and their cardiorespiratory symptoms. “Through engagement over time, you learn what the effects on your body are and what the expected effects are, so you can recognize the hazards and change the behavior when you’re experiencing it,” said Ana G. Rappold, PhD, who is the app’s principal investigator at the National Health and Environmental Effects Research Laboratory. One component of the app is time of last measurement of fine particulate matter and ozone based on the user’s location. Another is a module called Be Smoke Smart, which tests the user’s knowledge of wildfire smoke exposure. For example, one question is: “How likely are you to reduce your exposure on an Orange AQI alert day?” (which indicates that sensitive populations may experience health effects).
“Through gamification, they’re engaging with the issue,” Dr. Rappold said. “Then they learn about what others are reporting. In that part we also study how different messages change individuals’ perspective on how likely they are to make a change the next time they’re impacted by smoke.”
Azithromycin prevents airway complications of antibody deficiency
MADRID – Low-dose azithromycin prophylaxis significantly reduced exacerbations and hospitalizations in patients with primary antibody deficiency relative to placebo, according to a randomized multicenter phase 2 trial.

The study results support routine use of low-dose azithromycin in patients with primary antibody deficiency, according to Cinzia Milito, MD, PhD, department of molecular medicine, Sapienza University, Rome. Perhaps more importantly, the long-term benefits might be even greater.
“In patients with primary antibody deficiency, the respiratory tract is the major target of acute infections, leading to inflammation, increased airway reactivity, and over time to tissue remodeling and chronic lung disease,” Dr. Milito said at the annual congress of the European Respiratory Society. “Chronic lung disease is a major cause of death in this population.”
In this study 89 patients with primary antibody deficiency were randomized at seven centers in Italy to 250 mg per day of azithromycin or placebo administered on three consecutive days of each week for three years. Patients were maintained on other treatments, such as IgG replacement.
At the end of study, 33 of the 44 patients randomized to azithromycin and 34 of the 45 patients randomized to placebo remained on therapy. When compared for the primary endpoint of exacerbations, the median incidence rates were 3.6 episodes in the azithromycin group and 5.2 episodes in the placebo group, providing a 1.6 episode or 31% relative reduction (P=0.02).
The median number of hospitalizations for any cause, which was a secondary endpoint, was also significantly lower in the azithromycin arm (0.1 vs. 0.3 episodes).
In addition, the number of additional courses of antibiotics was significantly lower (2.3 vs. 3.6), and the time to the first course of antibiotic course was significantly longer (181.5 vs. 122.4 days) in the azithromycin group, reported Dr. Milito, whose study is now published (Milito C et al. J Allergy Clin Immunol 2019;144: 584-593).
“In a six-month washout at the end of the study, the relative advantages seen for azithromycin were lost,” Dr. Milito said.
Quality of life measured with the St. George’s Respiratory Questionnaire showed an association between low-dose azithromycin prophylaxis and significant improvement in the symptom domain when evaluated during and at the end of the study. Improvement on the Short-Form 36, which was observed one year into the study, was no longer significant at the end of the study.
Azithromycin was well tolerated with no significant differences in the rate of serious adverse events observed between the experimental and control arms of the study. Over the course of the study, however, azithromycin was associated with a significant protective effect against diarrhea (13% vs. 53%) and acute rhinosinusitus (4% vs. 27%).
There was no observed increase in macrolide resistance associated with azithromycin prophylaxis.
Macrolides have been evaluated for preventing progression of several chronic lung diseases, including chronic obstructive pulmonary disease, bronchiectasis, and cystic fibrosis. Like other drugs in its class, “azithromycin, in addition to its antimicrobial effect, has anti-inflammatory properties,” Dr. Milito said. This increases its potential to slow the time to airway damage in patients with primary antibiotic deficiency.
“Chronic lung disease is the result of a vicious cycle that begins with the inflammatory response to infection,” Dr. Milito explained. On the basis of these data, she believes azithromycin “should be considered a valuable addition to usual treatment” for primary antibody deficiencies.
SOURCE: EUROPEAN RESPIRATORY SOCIETY 2019 INTERNATIONAL CONGRESS
MADRID – Low-dose azithromycin prophylaxis significantly reduced exacerbations and hospitalizations in patients with primary antibody deficiency relative to placebo, according to a randomized multicenter phase 2 trial.
The study results support routine use of low-dose azithromycin in patients with primary antibody deficiency, according to Cinzia Milito, MD, PhD, department of molecular medicine, Sapienza University, Rome. Perhaps more importantly, the long-term benefits might be even greater.
“In patients with primary antibody deficiency, the respiratory tract is the major target of acute infections, leading to inflammation, increased airway reactivity, and over time to tissue remodeling and chronic lung disease,” Dr. Milito said at the annual congress of the European Respiratory Society. “Chronic lung disease is a major cause of death in this population.”
In this study 89 patients with primary antibody deficiency were randomized at seven centers in Italy to 250 mg per day of azithromycin or placebo administered on three consecutive days of each week for three years. Patients were maintained on other treatments, such as IgG replacement.
At the end of study, 33 of the 44 patients randomized to azithromycin and 34 of the 45 patients randomized to placebo remained on therapy. When compared for the primary endpoint of exacerbations, the median incidence rates were 3.6 episodes in the azithromycin group and 5.2 episodes in the placebo group, providing a 1.6 episode or 31% relative reduction (P=0.02).
The median number of hospitalizations for any cause, which was a secondary endpoint, was also significantly lower in the azithromycin arm (0.1 vs. 0.3 episodes).
In addition, the number of additional courses of antibiotics was significantly lower (2.3 vs. 3.6), and the time to the first course of antibiotic course was significantly longer (181.5 vs. 122.4 days) in the azithromycin group, reported Dr. Milito, whose study is now published (Milito C et al. J Allergy Clin Immunol 2019;144: 584-593).
“In a six-month washout at the end of the study, the relative advantages seen for azithromycin were lost,” Dr. Milito said.
Quality of life measured with the St. George’s Respiratory Questionnaire showed an association between low-dose azithromycin prophylaxis and significant improvement in the symptom domain when evaluated during and at the end of the study. Improvement on the Short-Form 36, which was observed one year into the study, was no longer significant at the end of the study.
Azithromycin was well tolerated with no significant differences in the rate of serious adverse events observed between the experimental and control arms of the study. Over the course of the study, however, azithromycin was associated with a significant protective effect against diarrhea (13% vs. 53%) and acute rhinosinusitus (4% vs. 27%).
There was no observed increase in macrolide resistance associated with azithromycin prophylaxis.
Macrolides have been evaluated for preventing progression of several chronic lung diseases, including chronic obstructive pulmonary disease, bronchiectasis, and cystic fibrosis. Like other drugs in its class, “azithromycin, in addition to its antimicrobial effect, has anti-inflammatory properties,” Dr. Milito said. This increases its potential to slow the time to airway damage in patients with primary antibiotic deficiency.
“Chronic lung disease is the result of a vicious cycle that begins with the inflammatory response to infection,” Dr. Milito explained. On the basis of these data, she believes azithromycin “should be considered a valuable addition to usual treatment” for primary antibody deficiencies.
SOURCE: EUROPEAN RESPIRATORY SOCIETY 2019 INTERNATIONAL CONGRESS
MADRID – Low-dose azithromycin prophylaxis significantly reduced exacerbations and hospitalizations in patients with primary antibody deficiency relative to placebo, according to a randomized multicenter phase 2 trial.
The study results support routine use of low-dose azithromycin in patients with primary antibody deficiency, according to Cinzia Milito, MD, PhD, department of molecular medicine, Sapienza University, Rome. Perhaps more importantly, the long-term benefits might be even greater.
“In patients with primary antibody deficiency, the respiratory tract is the major target of acute infections, leading to inflammation, increased airway reactivity, and over time to tissue remodeling and chronic lung disease,” Dr. Milito said at the annual congress of the European Respiratory Society. “Chronic lung disease is a major cause of death in this population.”
In this study 89 patients with primary antibody deficiency were randomized at seven centers in Italy to 250 mg per day of azithromycin or placebo administered on three consecutive days of each week for three years. Patients were maintained on other treatments, such as IgG replacement.
At the end of study, 33 of the 44 patients randomized to azithromycin and 34 of the 45 patients randomized to placebo remained on therapy. When compared for the primary endpoint of exacerbations, the median incidence rates were 3.6 episodes in the azithromycin group and 5.2 episodes in the placebo group, providing a 1.6 episode or 31% relative reduction (P=0.02).
The median number of hospitalizations for any cause, which was a secondary endpoint, was also significantly lower in the azithromycin arm (0.1 vs. 0.3 episodes).
In addition, the number of additional courses of antibiotics was significantly lower (2.3 vs. 3.6), and the time to the first course of antibiotic course was significantly longer (181.5 vs. 122.4 days) in the azithromycin group, reported Dr. Milito, whose study is now published (Milito C et al. J Allergy Clin Immunol 2019;144: 584-593).
“In a six-month washout at the end of the study, the relative advantages seen for azithromycin were lost,” Dr. Milito said.
Quality of life measured with the St. George’s Respiratory Questionnaire showed an association between low-dose azithromycin prophylaxis and significant improvement in the symptom domain when evaluated during and at the end of the study. Improvement on the Short-Form 36, which was observed one year into the study, was no longer significant at the end of the study.
Azithromycin was well tolerated with no significant differences in the rate of serious adverse events observed between the experimental and control arms of the study. Over the course of the study, however, azithromycin was associated with a significant protective effect against diarrhea (13% vs. 53%) and acute rhinosinusitus (4% vs. 27%).
There was no observed increase in macrolide resistance associated with azithromycin prophylaxis.
Macrolides have been evaluated for preventing progression of several chronic lung diseases, including chronic obstructive pulmonary disease, bronchiectasis, and cystic fibrosis. Like other drugs in its class, “azithromycin, in addition to its antimicrobial effect, has anti-inflammatory properties,” Dr. Milito said. This increases its potential to slow the time to airway damage in patients with primary antibiotic deficiency.
“Chronic lung disease is the result of a vicious cycle that begins with the inflammatory response to infection,” Dr. Milito explained. On the basis of these data, she believes azithromycin “should be considered a valuable addition to usual treatment” for primary antibody deficiencies.
SOURCE: EUROPEAN RESPIRATORY SOCIETY 2019 INTERNATIONAL CONGRESS
REPORTING FROM ERS 2019
Forgetting the Stuff That Dreams Are Made On
Why do we forget some dreams and remember others? Researchers in a study funded by the National Institute of Neurological Disorders and Stroke say our dream memory may be controlled by a group of neurons commonly associated with appetite. Their findings could shed light on a wide range of memory-related conditions, including posttraumatic stress disorder (PTSD) and Alzheimer disease.
Studies have already shown that sleep helps the brain store new memories and eliminate excess information. Recent mouse studies have found that during sleep the brain prunes synaptic connections made between neurons involved in some types of learning.
But this study shows how that might happen.
The researchers have previously demonstrated that narcolepsy might be linked to the loss of hypocretin/orexin-making neurons in the hypothalamus. In this study, they looked at neighboring cells that produce melanin-concentrating hormone (MCH), which is involved in the control of both sleep and appetite. A majority (53%) of hypothalamic MCH cells fired in mice during REM sleep; 35% fired when they were awake, and 12% fired at both times.
Those cells also may play a role in learning and memory, the researchers suggest. To test their theory that MCH cells might help the brain store memories, they used “genetic tools” to turn MCH neurons on and off during memory tests.
Surprisingly, the researchers say, pharmacogenetic activation—turning on the MCH cells—worsened memory; genetic ablation—turning them off—improved memory. Further experiments suggested MCH neurons exclusively played this role during REM sleep.
The results suggest that MCH neurons help the brain actively forget new, possibly unimportant information. “Since dreams are thought to primarily occur during REM sleep,” says Thomas Kilduff, PhD, senior author of the study, “the sleep stage when the MCH cells turn on, activation of these cells may prevent the content of a dream from being stored in the hippocampus—consequently, the dream is quickly forgotten.”
Why do we forget some dreams and remember others? Researchers in a study funded by the National Institute of Neurological Disorders and Stroke say our dream memory may be controlled by a group of neurons commonly associated with appetite. Their findings could shed light on a wide range of memory-related conditions, including posttraumatic stress disorder (PTSD) and Alzheimer disease.
Studies have already shown that sleep helps the brain store new memories and eliminate excess information. Recent mouse studies have found that during sleep the brain prunes synaptic connections made between neurons involved in some types of learning.
But this study shows how that might happen.
The researchers have previously demonstrated that narcolepsy might be linked to the loss of hypocretin/orexin-making neurons in the hypothalamus. In this study, they looked at neighboring cells that produce melanin-concentrating hormone (MCH), which is involved in the control of both sleep and appetite. A majority (53%) of hypothalamic MCH cells fired in mice during REM sleep; 35% fired when they were awake, and 12% fired at both times.
Those cells also may play a role in learning and memory, the researchers suggest. To test their theory that MCH cells might help the brain store memories, they used “genetic tools” to turn MCH neurons on and off during memory tests.
Surprisingly, the researchers say, pharmacogenetic activation—turning on the MCH cells—worsened memory; genetic ablation—turning them off—improved memory. Further experiments suggested MCH neurons exclusively played this role during REM sleep.
The results suggest that MCH neurons help the brain actively forget new, possibly unimportant information. “Since dreams are thought to primarily occur during REM sleep,” says Thomas Kilduff, PhD, senior author of the study, “the sleep stage when the MCH cells turn on, activation of these cells may prevent the content of a dream from being stored in the hippocampus—consequently, the dream is quickly forgotten.”
Why do we forget some dreams and remember others? Researchers in a study funded by the National Institute of Neurological Disorders and Stroke say our dream memory may be controlled by a group of neurons commonly associated with appetite. Their findings could shed light on a wide range of memory-related conditions, including posttraumatic stress disorder (PTSD) and Alzheimer disease.
Studies have already shown that sleep helps the brain store new memories and eliminate excess information. Recent mouse studies have found that during sleep the brain prunes synaptic connections made between neurons involved in some types of learning.
But this study shows how that might happen.
The researchers have previously demonstrated that narcolepsy might be linked to the loss of hypocretin/orexin-making neurons in the hypothalamus. In this study, they looked at neighboring cells that produce melanin-concentrating hormone (MCH), which is involved in the control of both sleep and appetite. A majority (53%) of hypothalamic MCH cells fired in mice during REM sleep; 35% fired when they were awake, and 12% fired at both times.
Those cells also may play a role in learning and memory, the researchers suggest. To test their theory that MCH cells might help the brain store memories, they used “genetic tools” to turn MCH neurons on and off during memory tests.
Surprisingly, the researchers say, pharmacogenetic activation—turning on the MCH cells—worsened memory; genetic ablation—turning them off—improved memory. Further experiments suggested MCH neurons exclusively played this role during REM sleep.
The results suggest that MCH neurons help the brain actively forget new, possibly unimportant information. “Since dreams are thought to primarily occur during REM sleep,” says Thomas Kilduff, PhD, senior author of the study, “the sleep stage when the MCH cells turn on, activation of these cells may prevent the content of a dream from being stored in the hippocampus—consequently, the dream is quickly forgotten.”
CDC updates guidance on vaping-associated lung injury
The Centers for Disease Control and Prevention has released an updated interim clinical guidance for health providers for evaluating and treating patients with lung injury associated with e-cigarette use or vaping.
In a telebriefing, Anne Schuchat, MD, CDC principal deputy director, and her colleagues answered questions about the current investigation into the source of this lung injury outbreak and the updated clinical guidance. Dr. Schuchat said, “I can’t stress enough the seriousness of these injuries.” She added, “We are not seeing a drop in cases” but a continuation of the trend of hospitalization and deaths that started in August 2019.
Investigation update
The investigation to date has yielded some information about current cases of lung injury related to vaping:
• The acronym EVALI has been developed to refer to e-cigarette, or vaping products use associated lung injury;
• 1,299 EVALI cases have been reported as of Oct. 8;
• No single compound or ingredient has emerged as the cause of these injuries, and more than one substance may be involved;
• Among the 573 patients for whom data are available on vaping products used in the previous 90 days, 76% reported using THC-containing products; 58% reported using nicotine-containing products; 32% reported exclusive use of THC-containing products, and 13% reported exclusive use of nicotine-containing products;
• Of the 700+ samples sent to the CDC for analysis, most had little or no liquid remaining in the device, limiting content analysis. In 28 THC-containing samples, THC concentrations were found to be 13% - 77% (mean 41%).
• A “handful” of cases of readmission have been reported and the CDC is currently investigating whether these cases included patients who took up vaping again or had some other possible contributing factor.
• The CDC is currently developing an ICD-10 code relevant to EVALI.
Clinical guidance update
The CDC provided detailed guidance on evaluating and caring for patients with EVALI. The recommendations focus on patient history, lab testing, criteria for hospitalization, and follow-up of these patients.
Detailed history of patients presenting with suspected EVALI is especially important for this patient population, given the many unknowns surrounding this condition. The updated guidance states, “All health care providers evaluating patients for EVALI should ask about the use of e-cigarette, or vaping, products and ideally should ask about types of substances used (e.g.,THC, cannabis [oil, dabs], nicotine, modified products or the addition of substances not intended by the manufacturer); product source, specific product brand and name; duration and frequency of use, time of last use; product delivery system, and method of use (aerosolization, dabbing, or dripping).” The approach recommended for soliciting accurate information is “empathetic, nonjudgmental” and, the guidelines say, patients should be questioned in private regarding sensitive information to assure confidentiality.
A respiratory virus panel is recommended for all suspected EVALI patients, although at this time, these tests cannot be used to distinguish EVALI from infectious etiologies. All patients should be considered for urine toxicology testing, including testing for THC.
Imaging guidance for suspected EVALI patients includes chest x-ray, with additional CT scan when the x-ray result does not correlate with clinical findings or to evaluate severe or worsening disease.
Recommended criteria for hospitalization of patients with suspected EVALI are those patients with decreased O2 saturation (less than 95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. As of Oct. 8, 96% of patients with suspected EVALI reported to CDC have been hospitalized.
As for medical treatment of these patients, corticosteroids have been found helpful. The statement noted, “Among 140 cases reported nationally to CDC that received corticosteroids, 82% of patients improved
The natural progression of this injury is not known, however, and it is possible that patients might recover without corticosteroids. Given the unknown etiology of the disease and “because the diagnosis remains one of exclusion, aggressive empiric therapy with corticosteroids, antimicrobial, and antiviral therapy might be warranted for patients with severe illness. A range of corticosteroid doses, durations, and taper plans might be considered on a case-by-case basis.”
The report concludes with a strong recommendation that patients hospitalized with EVALI are followed closely with a visit 1-2 weeks after discharge and again with additional testing 1-2 months later. Health care providers are also advised to consult medical specialists, in particular pulmonologists, who can offer further evaluation, recommend empiric treatment, and review indications for bronchoscopy.
Mitch Zeller, JD, director, Center for Tobacco Products with the Food and Drug Administration emphasized the extraordinary complexity of the EVALI problem but noted that the FDA and CDC “will leave no stone unturned until we get to the bottom of it.”
The Centers for Disease Control and Prevention has released an updated interim clinical guidance for health providers for evaluating and treating patients with lung injury associated with e-cigarette use or vaping.
In a telebriefing, Anne Schuchat, MD, CDC principal deputy director, and her colleagues answered questions about the current investigation into the source of this lung injury outbreak and the updated clinical guidance. Dr. Schuchat said, “I can’t stress enough the seriousness of these injuries.” She added, “We are not seeing a drop in cases” but a continuation of the trend of hospitalization and deaths that started in August 2019.
Investigation update
The investigation to date has yielded some information about current cases of lung injury related to vaping:
• The acronym EVALI has been developed to refer to e-cigarette, or vaping products use associated lung injury;
• 1,299 EVALI cases have been reported as of Oct. 8;
• No single compound or ingredient has emerged as the cause of these injuries, and more than one substance may be involved;
• Among the 573 patients for whom data are available on vaping products used in the previous 90 days, 76% reported using THC-containing products; 58% reported using nicotine-containing products; 32% reported exclusive use of THC-containing products, and 13% reported exclusive use of nicotine-containing products;
• Of the 700+ samples sent to the CDC for analysis, most had little or no liquid remaining in the device, limiting content analysis. In 28 THC-containing samples, THC concentrations were found to be 13% - 77% (mean 41%).
• A “handful” of cases of readmission have been reported and the CDC is currently investigating whether these cases included patients who took up vaping again or had some other possible contributing factor.
• The CDC is currently developing an ICD-10 code relevant to EVALI.
Clinical guidance update
The CDC provided detailed guidance on evaluating and caring for patients with EVALI. The recommendations focus on patient history, lab testing, criteria for hospitalization, and follow-up of these patients.
Detailed history of patients presenting with suspected EVALI is especially important for this patient population, given the many unknowns surrounding this condition. The updated guidance states, “All health care providers evaluating patients for EVALI should ask about the use of e-cigarette, or vaping, products and ideally should ask about types of substances used (e.g.,THC, cannabis [oil, dabs], nicotine, modified products or the addition of substances not intended by the manufacturer); product source, specific product brand and name; duration and frequency of use, time of last use; product delivery system, and method of use (aerosolization, dabbing, or dripping).” The approach recommended for soliciting accurate information is “empathetic, nonjudgmental” and, the guidelines say, patients should be questioned in private regarding sensitive information to assure confidentiality.
A respiratory virus panel is recommended for all suspected EVALI patients, although at this time, these tests cannot be used to distinguish EVALI from infectious etiologies. All patients should be considered for urine toxicology testing, including testing for THC.
Imaging guidance for suspected EVALI patients includes chest x-ray, with additional CT scan when the x-ray result does not correlate with clinical findings or to evaluate severe or worsening disease.
Recommended criteria for hospitalization of patients with suspected EVALI are those patients with decreased O2 saturation (less than 95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. As of Oct. 8, 96% of patients with suspected EVALI reported to CDC have been hospitalized.
As for medical treatment of these patients, corticosteroids have been found helpful. The statement noted, “Among 140 cases reported nationally to CDC that received corticosteroids, 82% of patients improved
The natural progression of this injury is not known, however, and it is possible that patients might recover without corticosteroids. Given the unknown etiology of the disease and “because the diagnosis remains one of exclusion, aggressive empiric therapy with corticosteroids, antimicrobial, and antiviral therapy might be warranted for patients with severe illness. A range of corticosteroid doses, durations, and taper plans might be considered on a case-by-case basis.”
The report concludes with a strong recommendation that patients hospitalized with EVALI are followed closely with a visit 1-2 weeks after discharge and again with additional testing 1-2 months later. Health care providers are also advised to consult medical specialists, in particular pulmonologists, who can offer further evaluation, recommend empiric treatment, and review indications for bronchoscopy.
Mitch Zeller, JD, director, Center for Tobacco Products with the Food and Drug Administration emphasized the extraordinary complexity of the EVALI problem but noted that the FDA and CDC “will leave no stone unturned until we get to the bottom of it.”
The Centers for Disease Control and Prevention has released an updated interim clinical guidance for health providers for evaluating and treating patients with lung injury associated with e-cigarette use or vaping.
In a telebriefing, Anne Schuchat, MD, CDC principal deputy director, and her colleagues answered questions about the current investigation into the source of this lung injury outbreak and the updated clinical guidance. Dr. Schuchat said, “I can’t stress enough the seriousness of these injuries.” She added, “We are not seeing a drop in cases” but a continuation of the trend of hospitalization and deaths that started in August 2019.
Investigation update
The investigation to date has yielded some information about current cases of lung injury related to vaping:
• The acronym EVALI has been developed to refer to e-cigarette, or vaping products use associated lung injury;
• 1,299 EVALI cases have been reported as of Oct. 8;
• No single compound or ingredient has emerged as the cause of these injuries, and more than one substance may be involved;
• Among the 573 patients for whom data are available on vaping products used in the previous 90 days, 76% reported using THC-containing products; 58% reported using nicotine-containing products; 32% reported exclusive use of THC-containing products, and 13% reported exclusive use of nicotine-containing products;
• Of the 700+ samples sent to the CDC for analysis, most had little or no liquid remaining in the device, limiting content analysis. In 28 THC-containing samples, THC concentrations were found to be 13% - 77% (mean 41%).
• A “handful” of cases of readmission have been reported and the CDC is currently investigating whether these cases included patients who took up vaping again or had some other possible contributing factor.
• The CDC is currently developing an ICD-10 code relevant to EVALI.
Clinical guidance update
The CDC provided detailed guidance on evaluating and caring for patients with EVALI. The recommendations focus on patient history, lab testing, criteria for hospitalization, and follow-up of these patients.
Detailed history of patients presenting with suspected EVALI is especially important for this patient population, given the many unknowns surrounding this condition. The updated guidance states, “All health care providers evaluating patients for EVALI should ask about the use of e-cigarette, or vaping, products and ideally should ask about types of substances used (e.g.,THC, cannabis [oil, dabs], nicotine, modified products or the addition of substances not intended by the manufacturer); product source, specific product brand and name; duration and frequency of use, time of last use; product delivery system, and method of use (aerosolization, dabbing, or dripping).” The approach recommended for soliciting accurate information is “empathetic, nonjudgmental” and, the guidelines say, patients should be questioned in private regarding sensitive information to assure confidentiality.
A respiratory virus panel is recommended for all suspected EVALI patients, although at this time, these tests cannot be used to distinguish EVALI from infectious etiologies. All patients should be considered for urine toxicology testing, including testing for THC.
Imaging guidance for suspected EVALI patients includes chest x-ray, with additional CT scan when the x-ray result does not correlate with clinical findings or to evaluate severe or worsening disease.
Recommended criteria for hospitalization of patients with suspected EVALI are those patients with decreased O2 saturation (less than 95%) on room air, are in respiratory distress, or have comorbidities that compromise pulmonary reserve. As of Oct. 8, 96% of patients with suspected EVALI reported to CDC have been hospitalized.
As for medical treatment of these patients, corticosteroids have been found helpful. The statement noted, “Among 140 cases reported nationally to CDC that received corticosteroids, 82% of patients improved
The natural progression of this injury is not known, however, and it is possible that patients might recover without corticosteroids. Given the unknown etiology of the disease and “because the diagnosis remains one of exclusion, aggressive empiric therapy with corticosteroids, antimicrobial, and antiviral therapy might be warranted for patients with severe illness. A range of corticosteroid doses, durations, and taper plans might be considered on a case-by-case basis.”
The report concludes with a strong recommendation that patients hospitalized with EVALI are followed closely with a visit 1-2 weeks after discharge and again with additional testing 1-2 months later. Health care providers are also advised to consult medical specialists, in particular pulmonologists, who can offer further evaluation, recommend empiric treatment, and review indications for bronchoscopy.
Mitch Zeller, JD, director, Center for Tobacco Products with the Food and Drug Administration emphasized the extraordinary complexity of the EVALI problem but noted that the FDA and CDC “will leave no stone unturned until we get to the bottom of it.”
REPORTING FROM A CDC TELEBRIEFING

Mesh nebulizer worked faster to control acute asthma
MADRID – Consistent with previous evidence of higher relative rates of drug delivery, mesh nebulizers offer several advantages over jet nebulizers for treatment of acute asthma in children presenting to an emergency department, according to results of a randomized trial presented at the annual congress of the European Respiratory Society.
For the primary outcome of hospital admission, the advantage of the mesh over the jet nebulizer only reached significance when used with a mask, rather than a valve, but trial results overall support the conclusion that the mesh device delivers drug more efficiently, according to Gerald Moody, RRT-NPS, clinical research coordinator at Children’s Medical Center, Dallas.
In this multicenter, single-blinded trial, 217 children presenting to an ED with acute asthma of moderate or greater severity were randomized to receive bronchodilator treatment delivered with a mesh device or a jet device. For drug delivery, aerosol masks or mouthpiece valves were permitted and selected at the discretion of the clinician administrating treatment. Masks were used in 80% of cases.
Patients remained in the study until either symptom control was achieved or a decision was reached to advise hospital admission. Patients with complex comorbidities or who had received oral corticosteroids within the previous 24 hours were excluded.
For the primary outcome of hospital discharge, the 31% reduction (P = .22) in hospitalization in favor of the mesh nebulizer failed to reach statistical significance. Although the study is likely to have been underpowered, Mr. Moody also pointed out an uneven distribution in severity of disease at baseline. In addition to a significantly higher median asthma score (9.0 vs. 8.0; P = .042) in the mesh nebulizer group, there was also a significantly higher percentage with severe disease (57% vs. 42%; P = .025).
“There were no significant differences in any of the other variables we evaluated, such as age, gender, race, or body mass index,” Mr. Moody reported.
Despite the higher disease burden in the mesh nebulizer group, there was a 48% reduction (P = .03) in hospital admissions among those randomized to the mesh nebulizer when both groups received treatment through a mask.
In addition, those treated with the mask required on average only two treatments before achieving symptom control whether they met criteria for moderate or severe asthma at baseline. The median numbers of treatments in the jet nebulizer group for moderate and severe asthma were 3 and 3.5, respectively.
In previous experimental studies, which ultimately provided the rationale for this trial, the estimated amount of drug reaching the airways with a mesh nebulizer was approximately twice as great as that estimated in the model when delivery was performed with a jet device, according to Mr. Moody.
This study appeared to corroborate that advantage. Both the median doses of albuterol (10 mg vs. 15 mg) and ipratropium (1,000 mcg vs. 1,500 mcg) were significantly lower (P less than .001 for both) among the patients randomized to the mesh nebulizer.
Although the jet nebulizers are widely employed “for their ease of use and low cost,” Mr. Moody characterized mesh nebulizers as an advance in technology. In this study, which Mr. Moody said is the first to evaluate whether the experimental evidence of greater drug delivery efficiency translates into a clinical advantage, the primary endpoint was missed, but Mr. Moody indicated that the overall findings support the potential for a difference.
The ERS-invited discussant on this study, Celeste Michala Porsbjerg, MD, Bispebjerg Hospital, Copenhagen University, expressed a concern that might deserve attention in a larger trial. Based on the premise that more efficient delivery increases drug exposure, she questioned whether it might not also increase risks.
There were no significant treatment-related adverse events reported in either arm of this study, Mr. Moody responded, but he conceded that this is an appropriate focus of attention for future studies.
Mr. Moody reported a financial relationship with Aerogen, which produces the mesh device tested in this trial.
MADRID – Consistent with previous evidence of higher relative rates of drug delivery, mesh nebulizers offer several advantages over jet nebulizers for treatment of acute asthma in children presenting to an emergency department, according to results of a randomized trial presented at the annual congress of the European Respiratory Society.
For the primary outcome of hospital admission, the advantage of the mesh over the jet nebulizer only reached significance when used with a mask, rather than a valve, but trial results overall support the conclusion that the mesh device delivers drug more efficiently, according to Gerald Moody, RRT-NPS, clinical research coordinator at Children’s Medical Center, Dallas.
In this multicenter, single-blinded trial, 217 children presenting to an ED with acute asthma of moderate or greater severity were randomized to receive bronchodilator treatment delivered with a mesh device or a jet device. For drug delivery, aerosol masks or mouthpiece valves were permitted and selected at the discretion of the clinician administrating treatment. Masks were used in 80% of cases.
Patients remained in the study until either symptom control was achieved or a decision was reached to advise hospital admission. Patients with complex comorbidities or who had received oral corticosteroids within the previous 24 hours were excluded.
For the primary outcome of hospital discharge, the 31% reduction (P = .22) in hospitalization in favor of the mesh nebulizer failed to reach statistical significance. Although the study is likely to have been underpowered, Mr. Moody also pointed out an uneven distribution in severity of disease at baseline. In addition to a significantly higher median asthma score (9.0 vs. 8.0; P = .042) in the mesh nebulizer group, there was also a significantly higher percentage with severe disease (57% vs. 42%; P = .025).
“There were no significant differences in any of the other variables we evaluated, such as age, gender, race, or body mass index,” Mr. Moody reported.
Despite the higher disease burden in the mesh nebulizer group, there was a 48% reduction (P = .03) in hospital admissions among those randomized to the mesh nebulizer when both groups received treatment through a mask.
In addition, those treated with the mask required on average only two treatments before achieving symptom control whether they met criteria for moderate or severe asthma at baseline. The median numbers of treatments in the jet nebulizer group for moderate and severe asthma were 3 and 3.5, respectively.
In previous experimental studies, which ultimately provided the rationale for this trial, the estimated amount of drug reaching the airways with a mesh nebulizer was approximately twice as great as that estimated in the model when delivery was performed with a jet device, according to Mr. Moody.
This study appeared to corroborate that advantage. Both the median doses of albuterol (10 mg vs. 15 mg) and ipratropium (1,000 mcg vs. 1,500 mcg) were significantly lower (P less than .001 for both) among the patients randomized to the mesh nebulizer.
Although the jet nebulizers are widely employed “for their ease of use and low cost,” Mr. Moody characterized mesh nebulizers as an advance in technology. In this study, which Mr. Moody said is the first to evaluate whether the experimental evidence of greater drug delivery efficiency translates into a clinical advantage, the primary endpoint was missed, but Mr. Moody indicated that the overall findings support the potential for a difference.
The ERS-invited discussant on this study, Celeste Michala Porsbjerg, MD, Bispebjerg Hospital, Copenhagen University, expressed a concern that might deserve attention in a larger trial. Based on the premise that more efficient delivery increases drug exposure, she questioned whether it might not also increase risks.
There were no significant treatment-related adverse events reported in either arm of this study, Mr. Moody responded, but he conceded that this is an appropriate focus of attention for future studies.
Mr. Moody reported a financial relationship with Aerogen, which produces the mesh device tested in this trial.
MADRID – Consistent with previous evidence of higher relative rates of drug delivery, mesh nebulizers offer several advantages over jet nebulizers for treatment of acute asthma in children presenting to an emergency department, according to results of a randomized trial presented at the annual congress of the European Respiratory Society.
For the primary outcome of hospital admission, the advantage of the mesh over the jet nebulizer only reached significance when used with a mask, rather than a valve, but trial results overall support the conclusion that the mesh device delivers drug more efficiently, according to Gerald Moody, RRT-NPS, clinical research coordinator at Children’s Medical Center, Dallas.
In this multicenter, single-blinded trial, 217 children presenting to an ED with acute asthma of moderate or greater severity were randomized to receive bronchodilator treatment delivered with a mesh device or a jet device. For drug delivery, aerosol masks or mouthpiece valves were permitted and selected at the discretion of the clinician administrating treatment. Masks were used in 80% of cases.
Patients remained in the study until either symptom control was achieved or a decision was reached to advise hospital admission. Patients with complex comorbidities or who had received oral corticosteroids within the previous 24 hours were excluded.
For the primary outcome of hospital discharge, the 31% reduction (P = .22) in hospitalization in favor of the mesh nebulizer failed to reach statistical significance. Although the study is likely to have been underpowered, Mr. Moody also pointed out an uneven distribution in severity of disease at baseline. In addition to a significantly higher median asthma score (9.0 vs. 8.0; P = .042) in the mesh nebulizer group, there was also a significantly higher percentage with severe disease (57% vs. 42%; P = .025).
“There were no significant differences in any of the other variables we evaluated, such as age, gender, race, or body mass index,” Mr. Moody reported.
Despite the higher disease burden in the mesh nebulizer group, there was a 48% reduction (P = .03) in hospital admissions among those randomized to the mesh nebulizer when both groups received treatment through a mask.
In addition, those treated with the mask required on average only two treatments before achieving symptom control whether they met criteria for moderate or severe asthma at baseline. The median numbers of treatments in the jet nebulizer group for moderate and severe asthma were 3 and 3.5, respectively.
In previous experimental studies, which ultimately provided the rationale for this trial, the estimated amount of drug reaching the airways with a mesh nebulizer was approximately twice as great as that estimated in the model when delivery was performed with a jet device, according to Mr. Moody.
This study appeared to corroborate that advantage. Both the median doses of albuterol (10 mg vs. 15 mg) and ipratropium (1,000 mcg vs. 1,500 mcg) were significantly lower (P less than .001 for both) among the patients randomized to the mesh nebulizer.
Although the jet nebulizers are widely employed “for their ease of use and low cost,” Mr. Moody characterized mesh nebulizers as an advance in technology. In this study, which Mr. Moody said is the first to evaluate whether the experimental evidence of greater drug delivery efficiency translates into a clinical advantage, the primary endpoint was missed, but Mr. Moody indicated that the overall findings support the potential for a difference.
The ERS-invited discussant on this study, Celeste Michala Porsbjerg, MD, Bispebjerg Hospital, Copenhagen University, expressed a concern that might deserve attention in a larger trial. Based on the premise that more efficient delivery increases drug exposure, she questioned whether it might not also increase risks.
There were no significant treatment-related adverse events reported in either arm of this study, Mr. Moody responded, but he conceded that this is an appropriate focus of attention for future studies.
Mr. Moody reported a financial relationship with Aerogen, which produces the mesh device tested in this trial.
REPORTING FROM ERS 2019
Urine Reveals Biomarker for Potential TBI
Even a mild blast to the brain can cause long-term, life-changing health problems, says Riyi Shi, professor of neuroscience and biomedical engineering at Purdue University in Lafayette, Indiana. However, the effects can be subtle: “The individual appears to be fine, and it’s difficult to tell if you just look at a person. But the fact is that these types of hits are multiplied over years and often ignored until someone reaches an age when other factors come into play.”
Treating the incidents sooner can help mitigate later-life issues, such as Parkinson disease (PD). Shi led a study that found checking the urine within 7 days following a blast incident—even a mild one—provides faster diagnosis when brain injury is suspected.
A simple urine analysis reveals elevations in the neurotoxin acrolein, Shi says, which is a biomarker for brain injury. In the study, the researchers evaluated the changes of α-synuclein and tyrosine hydroxylase, hallmarks of PD, and acrolein, a marker of oxidative stress. The researchers say in animal models of PD and traumatic brain injury (TBI), acrolein is “likely a point of pathogenic convergence.”
They found that after a single mild blast TBI, acrolein was elevated for up to a week, systemically in urine, and in whole brain tissue, specifically the substantia nigra and striatum. The elevation was accompanied by heightened α-synuclein oligomerization, dopaminergic dysregulation, and acrolein/α-synuclein interaction in the same brain regions. Taken together, the researchers say, the data suggest that acrolein likely plays a key role in inducing PD following blast TBI.
The presence of the biomarker “alerts us to the injury, creating an opportunity for intervention,” Shi says. “This early detection and subsequent treatment window could offer tremendous benefits for long-term patient neurologic health.”
Even a mild blast to the brain can cause long-term, life-changing health problems, says Riyi Shi, professor of neuroscience and biomedical engineering at Purdue University in Lafayette, Indiana. However, the effects can be subtle: “The individual appears to be fine, and it’s difficult to tell if you just look at a person. But the fact is that these types of hits are multiplied over years and often ignored until someone reaches an age when other factors come into play.”
Treating the incidents sooner can help mitigate later-life issues, such as Parkinson disease (PD). Shi led a study that found checking the urine within 7 days following a blast incident—even a mild one—provides faster diagnosis when brain injury is suspected.
A simple urine analysis reveals elevations in the neurotoxin acrolein, Shi says, which is a biomarker for brain injury. In the study, the researchers evaluated the changes of α-synuclein and tyrosine hydroxylase, hallmarks of PD, and acrolein, a marker of oxidative stress. The researchers say in animal models of PD and traumatic brain injury (TBI), acrolein is “likely a point of pathogenic convergence.”
They found that after a single mild blast TBI, acrolein was elevated for up to a week, systemically in urine, and in whole brain tissue, specifically the substantia nigra and striatum. The elevation was accompanied by heightened α-synuclein oligomerization, dopaminergic dysregulation, and acrolein/α-synuclein interaction in the same brain regions. Taken together, the researchers say, the data suggest that acrolein likely plays a key role in inducing PD following blast TBI.
The presence of the biomarker “alerts us to the injury, creating an opportunity for intervention,” Shi says. “This early detection and subsequent treatment window could offer tremendous benefits for long-term patient neurologic health.”
Even a mild blast to the brain can cause long-term, life-changing health problems, says Riyi Shi, professor of neuroscience and biomedical engineering at Purdue University in Lafayette, Indiana. However, the effects can be subtle: “The individual appears to be fine, and it’s difficult to tell if you just look at a person. But the fact is that these types of hits are multiplied over years and often ignored until someone reaches an age when other factors come into play.”
Treating the incidents sooner can help mitigate later-life issues, such as Parkinson disease (PD). Shi led a study that found checking the urine within 7 days following a blast incident—even a mild one—provides faster diagnosis when brain injury is suspected.
A simple urine analysis reveals elevations in the neurotoxin acrolein, Shi says, which is a biomarker for brain injury. In the study, the researchers evaluated the changes of α-synuclein and tyrosine hydroxylase, hallmarks of PD, and acrolein, a marker of oxidative stress. The researchers say in animal models of PD and traumatic brain injury (TBI), acrolein is “likely a point of pathogenic convergence.”
They found that after a single mild blast TBI, acrolein was elevated for up to a week, systemically in urine, and in whole brain tissue, specifically the substantia nigra and striatum. The elevation was accompanied by heightened α-synuclein oligomerization, dopaminergic dysregulation, and acrolein/α-synuclein interaction in the same brain regions. Taken together, the researchers say, the data suggest that acrolein likely plays a key role in inducing PD following blast TBI.
The presence of the biomarker “alerts us to the injury, creating an opportunity for intervention,” Shi says. “This early detection and subsequent treatment window could offer tremendous benefits for long-term patient neurologic health.”
Trial confirms as-needed inhalers suffice for mild to moderate asthma
MADRID – In the context of three previous trials, a new phase 3 trial demonstrates that the efficacy of as-needed inhaled corticosteroids (ICS) plus a long-acting beta agonist (LABA) is at least comparable to maintenance ICS for preventing severe exacerbations in the routine care of patients with mild to moderate asthma, according to a presentation at the 2019 ERS International Congress.

This “real-world” study, called PRACTICAL, produced results similar to those of the previous three studies. It showed similar or modestly improved efficacy for the as-needed approach in patients enrolled with mild to moderate asthma, according to Joanna Hardy, MD, a research fellow at the Medical Research Institute of New Zealand, Wellington.
Currently, the Global Initiative for Asthma (GINA) guidelines identify either of the two strategies tested in this trial as acceptable for patients eligible for step 2 asthma control. This study, as in the three trials published previously, provided reassurance that an as-needed approach is adequate for patients insufficiently adherent to daily maintenance therapy.
In PRACTICAL, the results of which were published just prior to the 2019 ERS Congress (Lancet 2019;394:919-28), 890 patients were randomized to use of a single inhaler containing 200 mcg budesonide plus 6 mcg formoterol as needed for symptoms or to a maintenance regimen with the same dose of budesonide taken twice daily. The protocol allowed 250 mcg terbutaline as needed for symptom control in the maintenance arm. The patients were followed for 52 weeks.
For the primary endpoint of the per-patient number of severe exacerbations, defined as need for 3 consecutive days of oral corticosteroids or an emergency department visit to receive oral corticosteroids, the as-needed approach reduced the relative risk by 31% (hazard ratio, 0.69; P = .049). The per-patient rates of exacerbations for the as-needed and maintenance arms were 0.0119 and 0.172, respectively.
The time to first exacerbation, a secondary endpoint, approached significance in favor of as-needed treatment (HR 0.6; P = .05). There was no difference in asthma control as measured with the Asthma Control Questionnaire or in lung function as measured with forced expiratory volume in 1 second (FEV1) at any visit or at the end of the study.
Two SYGMA trials (SYGMA 1 and SYGMA 2), both published in the New England Journal of Medicine in 2018, addressed the same question. Most like PRACTICAL, SYGMA 2 randomized 4,215 patients with mild asthma and found as-needed budesonide/formoterol noninferior to budesonide maintenance for preventing severe exacerbations.
In SYGMA 1, which included an as-needed terbutaline arm, 3,849 patients were randomized. Although as-needed budesonide-formoterol was inferior to budesonide maintenance in that study (but superior to as-needed to terbutaline), the adherence to budesonide maintenance was 78.9%, which Dr. Hardy said does not reflect real-world patient behavior.
“The problem is that we have a lot of data to show that adherence to maintenance asthma therapy in mild asthma is poor,” Dr. Hardy said. In PRACTICAL, all patients were provided with an asthma action plan but no strategies were offered to improve compliance over those employed in usual practice.
In the open-label Novel START trial, published in 2019 in the New England Journal of Medicine, the question posed was different. In that study, which randomized 675 patients, as-needed budesonide/formoterol was superior to as-needed albuterol for prevention of asthma exacerbations at 52 weeks, the time point employed in all four studies. The results, while confirming the importance of the ICS component, have been generally interpreted as supporting the as-needed therapy in mild asthma.
At the ERS 2019 Congress, one of the moderators of the session in which Dr. Hardy spoke, Guy Brusselle, MD, Ghent (Belgium) University, agreed that the available evidence supports as-needed therapy as a viable strategy in mild asthma, but expressed concern about applying this conclusion to patients who have asthma requiring therapy beyond GINA step 2.
“These data might put patients who need GINA step 3 or 4 therapy at risk of not receiving the maintenance therapy they need for disease control,” Dr. Brusselle said.
In light of the challenge of separating those with moderate from mild asthma, Dr. Brusselle suggested another arm to add to real-world clinical trials attempting to identify the most effective approach.
“The optimal arm might be maintenance budesonide with as-needed ICS/LABA,” Dr. Brusselle said. He explained that even if compliance is low, at least some patients will be receiving a maintenance therapy, and this approach might ultimately offer more benefit than one in which patients do not even consider maintenance.
Dr. Hardy reports no potential conflicts of interest.
MADRID – In the context of three previous trials, a new phase 3 trial demonstrates that the efficacy of as-needed inhaled corticosteroids (ICS) plus a long-acting beta agonist (LABA) is at least comparable to maintenance ICS for preventing severe exacerbations in the routine care of patients with mild to moderate asthma, according to a presentation at the 2019 ERS International Congress.
This “real-world” study, called PRACTICAL, produced results similar to those of the previous three studies. It showed similar or modestly improved efficacy for the as-needed approach in patients enrolled with mild to moderate asthma, according to Joanna Hardy, MD, a research fellow at the Medical Research Institute of New Zealand, Wellington.
Currently, the Global Initiative for Asthma (GINA) guidelines identify either of the two strategies tested in this trial as acceptable for patients eligible for step 2 asthma control. This study, as in the three trials published previously, provided reassurance that an as-needed approach is adequate for patients insufficiently adherent to daily maintenance therapy.
In PRACTICAL, the results of which were published just prior to the 2019 ERS Congress (Lancet 2019;394:919-28), 890 patients were randomized to use of a single inhaler containing 200 mcg budesonide plus 6 mcg formoterol as needed for symptoms or to a maintenance regimen with the same dose of budesonide taken twice daily. The protocol allowed 250 mcg terbutaline as needed for symptom control in the maintenance arm. The patients were followed for 52 weeks.
For the primary endpoint of the per-patient number of severe exacerbations, defined as need for 3 consecutive days of oral corticosteroids or an emergency department visit to receive oral corticosteroids, the as-needed approach reduced the relative risk by 31% (hazard ratio, 0.69; P = .049). The per-patient rates of exacerbations for the as-needed and maintenance arms were 0.0119 and 0.172, respectively.
The time to first exacerbation, a secondary endpoint, approached significance in favor of as-needed treatment (HR 0.6; P = .05). There was no difference in asthma control as measured with the Asthma Control Questionnaire or in lung function as measured with forced expiratory volume in 1 second (FEV1) at any visit or at the end of the study.
Two SYGMA trials (SYGMA 1 and SYGMA 2), both published in the New England Journal of Medicine in 2018, addressed the same question. Most like PRACTICAL, SYGMA 2 randomized 4,215 patients with mild asthma and found as-needed budesonide/formoterol noninferior to budesonide maintenance for preventing severe exacerbations.
In SYGMA 1, which included an as-needed terbutaline arm, 3,849 patients were randomized. Although as-needed budesonide-formoterol was inferior to budesonide maintenance in that study (but superior to as-needed to terbutaline), the adherence to budesonide maintenance was 78.9%, which Dr. Hardy said does not reflect real-world patient behavior.
“The problem is that we have a lot of data to show that adherence to maintenance asthma therapy in mild asthma is poor,” Dr. Hardy said. In PRACTICAL, all patients were provided with an asthma action plan but no strategies were offered to improve compliance over those employed in usual practice.
In the open-label Novel START trial, published in 2019 in the New England Journal of Medicine, the question posed was different. In that study, which randomized 675 patients, as-needed budesonide/formoterol was superior to as-needed albuterol for prevention of asthma exacerbations at 52 weeks, the time point employed in all four studies. The results, while confirming the importance of the ICS component, have been generally interpreted as supporting the as-needed therapy in mild asthma.
At the ERS 2019 Congress, one of the moderators of the session in which Dr. Hardy spoke, Guy Brusselle, MD, Ghent (Belgium) University, agreed that the available evidence supports as-needed therapy as a viable strategy in mild asthma, but expressed concern about applying this conclusion to patients who have asthma requiring therapy beyond GINA step 2.
“These data might put patients who need GINA step 3 or 4 therapy at risk of not receiving the maintenance therapy they need for disease control,” Dr. Brusselle said.
In light of the challenge of separating those with moderate from mild asthma, Dr. Brusselle suggested another arm to add to real-world clinical trials attempting to identify the most effective approach.
“The optimal arm might be maintenance budesonide with as-needed ICS/LABA,” Dr. Brusselle said. He explained that even if compliance is low, at least some patients will be receiving a maintenance therapy, and this approach might ultimately offer more benefit than one in which patients do not even consider maintenance.
Dr. Hardy reports no potential conflicts of interest.
MADRID – In the context of three previous trials, a new phase 3 trial demonstrates that the efficacy of as-needed inhaled corticosteroids (ICS) plus a long-acting beta agonist (LABA) is at least comparable to maintenance ICS for preventing severe exacerbations in the routine care of patients with mild to moderate asthma, according to a presentation at the 2019 ERS International Congress.
This “real-world” study, called PRACTICAL, produced results similar to those of the previous three studies. It showed similar or modestly improved efficacy for the as-needed approach in patients enrolled with mild to moderate asthma, according to Joanna Hardy, MD, a research fellow at the Medical Research Institute of New Zealand, Wellington.
Currently, the Global Initiative for Asthma (GINA) guidelines identify either of the two strategies tested in this trial as acceptable for patients eligible for step 2 asthma control. This study, as in the three trials published previously, provided reassurance that an as-needed approach is adequate for patients insufficiently adherent to daily maintenance therapy.
In PRACTICAL, the results of which were published just prior to the 2019 ERS Congress (Lancet 2019;394:919-28), 890 patients were randomized to use of a single inhaler containing 200 mcg budesonide plus 6 mcg formoterol as needed for symptoms or to a maintenance regimen with the same dose of budesonide taken twice daily. The protocol allowed 250 mcg terbutaline as needed for symptom control in the maintenance arm. The patients were followed for 52 weeks.
For the primary endpoint of the per-patient number of severe exacerbations, defined as need for 3 consecutive days of oral corticosteroids or an emergency department visit to receive oral corticosteroids, the as-needed approach reduced the relative risk by 31% (hazard ratio, 0.69; P = .049). The per-patient rates of exacerbations for the as-needed and maintenance arms were 0.0119 and 0.172, respectively.
The time to first exacerbation, a secondary endpoint, approached significance in favor of as-needed treatment (HR 0.6; P = .05). There was no difference in asthma control as measured with the Asthma Control Questionnaire or in lung function as measured with forced expiratory volume in 1 second (FEV1) at any visit or at the end of the study.
Two SYGMA trials (SYGMA 1 and SYGMA 2), both published in the New England Journal of Medicine in 2018, addressed the same question. Most like PRACTICAL, SYGMA 2 randomized 4,215 patients with mild asthma and found as-needed budesonide/formoterol noninferior to budesonide maintenance for preventing severe exacerbations.
In SYGMA 1, which included an as-needed terbutaline arm, 3,849 patients were randomized. Although as-needed budesonide-formoterol was inferior to budesonide maintenance in that study (but superior to as-needed to terbutaline), the adherence to budesonide maintenance was 78.9%, which Dr. Hardy said does not reflect real-world patient behavior.
“The problem is that we have a lot of data to show that adherence to maintenance asthma therapy in mild asthma is poor,” Dr. Hardy said. In PRACTICAL, all patients were provided with an asthma action plan but no strategies were offered to improve compliance over those employed in usual practice.
In the open-label Novel START trial, published in 2019 in the New England Journal of Medicine, the question posed was different. In that study, which randomized 675 patients, as-needed budesonide/formoterol was superior to as-needed albuterol for prevention of asthma exacerbations at 52 weeks, the time point employed in all four studies. The results, while confirming the importance of the ICS component, have been generally interpreted as supporting the as-needed therapy in mild asthma.
At the ERS 2019 Congress, one of the moderators of the session in which Dr. Hardy spoke, Guy Brusselle, MD, Ghent (Belgium) University, agreed that the available evidence supports as-needed therapy as a viable strategy in mild asthma, but expressed concern about applying this conclusion to patients who have asthma requiring therapy beyond GINA step 2.
“These data might put patients who need GINA step 3 or 4 therapy at risk of not receiving the maintenance therapy they need for disease control,” Dr. Brusselle said.
In light of the challenge of separating those with moderate from mild asthma, Dr. Brusselle suggested another arm to add to real-world clinical trials attempting to identify the most effective approach.
“The optimal arm might be maintenance budesonide with as-needed ICS/LABA,” Dr. Brusselle said. He explained that even if compliance is low, at least some patients will be receiving a maintenance therapy, and this approach might ultimately offer more benefit than one in which patients do not even consider maintenance.
Dr. Hardy reports no potential conflicts of interest.
REPORTING FROM ERS 2019
Dysregulated sleep is common in children with eosinophilic esophagitis
, Rasintra Siriwat, MD, and colleagues have ascertained.

Children with eosinophilic esophagitis (EoE) also were found to have a high prevalence of atopic diseases, including allergic rhinitis and eczema – findings that could be driving the breathing problems, said Dr. Siriwat, a neurology fellow at the Cleveland Clinic, and coauthors.
The retrospective study comprised 81 children with a diagnosis of EoE who were referred to sleep clinics. In this group, 46 of the children had active EoE (having gastrointestinal symptoms, including feeding difficulties, dysphagia, reflux, nausea/vomiting, or epigastric pain at presentation). The other 35 had an EoE diagnosis but no symptoms on presentation and were categorized as having inactive EoE. Most were male (71.6%) and white (92.5%). The mean age in the cohort was 10 years and the mean body mass index for all subjects was 22 kg/m2. A control group of 192 children without an EoE diagnosis who had overnight polysomnography were included in the analysis.
Allergic-type comorbidities were common among those with active EoE, including allergic rhinitis (55.5%), food allergy (39.5%), and eczema (26%). In addition, a quarter had attention-deficit/hyperactivity disorder, 22% an autism spectrum disorder, 21% a neurological disease, and 29% a psychiatric disorder.
Several sleep complaints were common in the entire EoE cohort, including snoring (76.5 %), restless sleep (66.6%), legs jerking or leg discomfort (43.2%), and daytime sleepiness (58%).
All children underwent an overnight polysomnography. Compared with controls, the children with EoE had significantly higher non-REM2 sleep, significantly lower non-REM3 sleep, lower REM, increased periodic leg movement disorder, and increased arousal index.
“Of note, we found a much higher percentage of [periodic leg movement disorder] in active EoE compared to inactive EoE,” the authors said.
The most common sleep diagnosis for the children with EoE was sleep-disordered breathing. Of 62 children with EoE and sleep disordered breathing, 37% had obstructive sleep apnea (OSA). Two patients had central sleep apnea and five had nocturnal hypoventilation. Children with EoE also reported parasomnia symptoms such as sleep talking (35.8%), sleepwalking (16%), bruxism (23.4%), night terrors (28.4%), and nocturnal enuresis (21.2%).
Of the 59 children with leg movement, 20 had periodic limb movement disorder and 5 were diagnosed with restless leg syndrome. Two were diagnosed with narcolepsy and three with hypersomnia. Four children had a circadian rhythm disorder.
“Notably, the majority of children with EoE had symptoms of sleep-disordered breathing, and more than one-third of total subjects were diagnosed with OSA,” the authors noted. “However, most of them were mild-moderate OSA. It should be noted that the prevalence of OSA in the pediatric population is 1%-5% mostly between the ages of 2-8 years, while the mean age of our subjects was 10 years old. The high prevalence of mild-moderate OSA in the EoE population might be explained by the relationship between EoE and atopic disease.”
Dr. Siriwat had no financial disclosures. The study was supported by Cincinnati Children’s Hospital Research Fund.
SOURCE: Siriwat R et al. Sleep Med. 2019 Sep 11. doi: 10.1016/j.sleep.2019.08.018.
, Rasintra Siriwat, MD, and colleagues have ascertained.
Children with eosinophilic esophagitis (EoE) also were found to have a high prevalence of atopic diseases, including allergic rhinitis and eczema – findings that could be driving the breathing problems, said Dr. Siriwat, a neurology fellow at the Cleveland Clinic, and coauthors.
The retrospective study comprised 81 children with a diagnosis of EoE who were referred to sleep clinics. In this group, 46 of the children had active EoE (having gastrointestinal symptoms, including feeding difficulties, dysphagia, reflux, nausea/vomiting, or epigastric pain at presentation). The other 35 had an EoE diagnosis but no symptoms on presentation and were categorized as having inactive EoE. Most were male (71.6%) and white (92.5%). The mean age in the cohort was 10 years and the mean body mass index for all subjects was 22 kg/m2. A control group of 192 children without an EoE diagnosis who had overnight polysomnography were included in the analysis.
Allergic-type comorbidities were common among those with active EoE, including allergic rhinitis (55.5%), food allergy (39.5%), and eczema (26%). In addition, a quarter had attention-deficit/hyperactivity disorder, 22% an autism spectrum disorder, 21% a neurological disease, and 29% a psychiatric disorder.
Several sleep complaints were common in the entire EoE cohort, including snoring (76.5 %), restless sleep (66.6%), legs jerking or leg discomfort (43.2%), and daytime sleepiness (58%).
All children underwent an overnight polysomnography. Compared with controls, the children with EoE had significantly higher non-REM2 sleep, significantly lower non-REM3 sleep, lower REM, increased periodic leg movement disorder, and increased arousal index.
“Of note, we found a much higher percentage of [periodic leg movement disorder] in active EoE compared to inactive EoE,” the authors said.
The most common sleep diagnosis for the children with EoE was sleep-disordered breathing. Of 62 children with EoE and sleep disordered breathing, 37% had obstructive sleep apnea (OSA). Two patients had central sleep apnea and five had nocturnal hypoventilation. Children with EoE also reported parasomnia symptoms such as sleep talking (35.8%), sleepwalking (16%), bruxism (23.4%), night terrors (28.4%), and nocturnal enuresis (21.2%).
Of the 59 children with leg movement, 20 had periodic limb movement disorder and 5 were diagnosed with restless leg syndrome. Two were diagnosed with narcolepsy and three with hypersomnia. Four children had a circadian rhythm disorder.
“Notably, the majority of children with EoE had symptoms of sleep-disordered breathing, and more than one-third of total subjects were diagnosed with OSA,” the authors noted. “However, most of them were mild-moderate OSA. It should be noted that the prevalence of OSA in the pediatric population is 1%-5% mostly between the ages of 2-8 years, while the mean age of our subjects was 10 years old. The high prevalence of mild-moderate OSA in the EoE population might be explained by the relationship between EoE and atopic disease.”
Dr. Siriwat had no financial disclosures. The study was supported by Cincinnati Children’s Hospital Research Fund.
SOURCE: Siriwat R et al. Sleep Med. 2019 Sep 11. doi: 10.1016/j.sleep.2019.08.018.
, Rasintra Siriwat, MD, and colleagues have ascertained.
Children with eosinophilic esophagitis (EoE) also were found to have a high prevalence of atopic diseases, including allergic rhinitis and eczema – findings that could be driving the breathing problems, said Dr. Siriwat, a neurology fellow at the Cleveland Clinic, and coauthors.
The retrospective study comprised 81 children with a diagnosis of EoE who were referred to sleep clinics. In this group, 46 of the children had active EoE (having gastrointestinal symptoms, including feeding difficulties, dysphagia, reflux, nausea/vomiting, or epigastric pain at presentation). The other 35 had an EoE diagnosis but no symptoms on presentation and were categorized as having inactive EoE. Most were male (71.6%) and white (92.5%). The mean age in the cohort was 10 years and the mean body mass index for all subjects was 22 kg/m2. A control group of 192 children without an EoE diagnosis who had overnight polysomnography were included in the analysis.
Allergic-type comorbidities were common among those with active EoE, including allergic rhinitis (55.5%), food allergy (39.5%), and eczema (26%). In addition, a quarter had attention-deficit/hyperactivity disorder, 22% an autism spectrum disorder, 21% a neurological disease, and 29% a psychiatric disorder.
Several sleep complaints were common in the entire EoE cohort, including snoring (76.5 %), restless sleep (66.6%), legs jerking or leg discomfort (43.2%), and daytime sleepiness (58%).
All children underwent an overnight polysomnography. Compared with controls, the children with EoE had significantly higher non-REM2 sleep, significantly lower non-REM3 sleep, lower REM, increased periodic leg movement disorder, and increased arousal index.
“Of note, we found a much higher percentage of [periodic leg movement disorder] in active EoE compared to inactive EoE,” the authors said.
The most common sleep diagnosis for the children with EoE was sleep-disordered breathing. Of 62 children with EoE and sleep disordered breathing, 37% had obstructive sleep apnea (OSA). Two patients had central sleep apnea and five had nocturnal hypoventilation. Children with EoE also reported parasomnia symptoms such as sleep talking (35.8%), sleepwalking (16%), bruxism (23.4%), night terrors (28.4%), and nocturnal enuresis (21.2%).
Of the 59 children with leg movement, 20 had periodic limb movement disorder and 5 were diagnosed with restless leg syndrome. Two were diagnosed with narcolepsy and three with hypersomnia. Four children had a circadian rhythm disorder.
“Notably, the majority of children with EoE had symptoms of sleep-disordered breathing, and more than one-third of total subjects were diagnosed with OSA,” the authors noted. “However, most of them were mild-moderate OSA. It should be noted that the prevalence of OSA in the pediatric population is 1%-5% mostly between the ages of 2-8 years, while the mean age of our subjects was 10 years old. The high prevalence of mild-moderate OSA in the EoE population might be explained by the relationship between EoE and atopic disease.”
Dr. Siriwat had no financial disclosures. The study was supported by Cincinnati Children’s Hospital Research Fund.
SOURCE: Siriwat R et al. Sleep Med. 2019 Sep 11. doi: 10.1016/j.sleep.2019.08.018.
FROM SLEEP MEDICINE
FDA approves benralizumab autoinjector for eosinophilic asthma
according to a press release from AstraZeneca. Benralizumab is already approved as add-on maintenance for this form of asthma, but not for other eosinophilic conditions or for acute bronchospasm or status asthmaticus.

The autoinjector “pen” was tested for usability and pharmacokinetic exposure in two studies, the phase 3 GRECO trial and the phase 1 AMES trial, respectively. The multicenter, open-label GRECO trial was designed to assess patient- or caregiver-reported functionality, and it found that 97% of at-home administrations were successful at week 12 and week 16. The multicenter, randomized, open-label, parallel-group AMES trial compared pharmacokinetic exposure with the subcutaneous administration using either prefilled syringe or prefilled autoinjector; it found that the eosinophils were rapidly depleted in patients with use of either device.
The safety profiles in both trials were comparable to those seen in previous trials. Hypersensitivity reactions have been sometimes observed in the hours following administration of benralizumab; discontinuation is advised in case of any hypersensitivity reaction. The therapy should not be used to treat acute asthma symptoms, such as exacerbations, or bronchospasm, and any reduction in corticosteroid therapy should be gradual and performed under careful supervision of a health care professional. Although benralizumab’s effects on helminth infections are currently unknown, care should be taken with preexisting or incident infections.
Full prescribing information can be found on the AstraZeneca website.
according to a press release from AstraZeneca. Benralizumab is already approved as add-on maintenance for this form of asthma, but not for other eosinophilic conditions or for acute bronchospasm or status asthmaticus.
The autoinjector “pen” was tested for usability and pharmacokinetic exposure in two studies, the phase 3 GRECO trial and the phase 1 AMES trial, respectively. The multicenter, open-label GRECO trial was designed to assess patient- or caregiver-reported functionality, and it found that 97% of at-home administrations were successful at week 12 and week 16. The multicenter, randomized, open-label, parallel-group AMES trial compared pharmacokinetic exposure with the subcutaneous administration using either prefilled syringe or prefilled autoinjector; it found that the eosinophils were rapidly depleted in patients with use of either device.
The safety profiles in both trials were comparable to those seen in previous trials. Hypersensitivity reactions have been sometimes observed in the hours following administration of benralizumab; discontinuation is advised in case of any hypersensitivity reaction. The therapy should not be used to treat acute asthma symptoms, such as exacerbations, or bronchospasm, and any reduction in corticosteroid therapy should be gradual and performed under careful supervision of a health care professional. Although benralizumab’s effects on helminth infections are currently unknown, care should be taken with preexisting or incident infections.
Full prescribing information can be found on the AstraZeneca website.
according to a press release from AstraZeneca. Benralizumab is already approved as add-on maintenance for this form of asthma, but not for other eosinophilic conditions or for acute bronchospasm or status asthmaticus.
The autoinjector “pen” was tested for usability and pharmacokinetic exposure in two studies, the phase 3 GRECO trial and the phase 1 AMES trial, respectively. The multicenter, open-label GRECO trial was designed to assess patient- or caregiver-reported functionality, and it found that 97% of at-home administrations were successful at week 12 and week 16. The multicenter, randomized, open-label, parallel-group AMES trial compared pharmacokinetic exposure with the subcutaneous administration using either prefilled syringe or prefilled autoinjector; it found that the eosinophils were rapidly depleted in patients with use of either device.
The safety profiles in both trials were comparable to those seen in previous trials. Hypersensitivity reactions have been sometimes observed in the hours following administration of benralizumab; discontinuation is advised in case of any hypersensitivity reaction. The therapy should not be used to treat acute asthma symptoms, such as exacerbations, or bronchospasm, and any reduction in corticosteroid therapy should be gradual and performed under careful supervision of a health care professional. Although benralizumab’s effects on helminth infections are currently unknown, care should be taken with preexisting or incident infections.
Full prescribing information can be found on the AstraZeneca website.
Histologic analysis of vaping-associated lung injury suggests chemical pneumonitis
Vaping-associated lung injury is likely a form of airway-centered chemical pneumonitis, not exogenous lipoid pneumonia, according to Yasmeen M. Butt, MD, of the University of Texas Southwestern Medical Center, Dallas, and associates.

Dr. Butt and associates performed a review of lung biopsies from 17 patients (13 men; median age, 35 years) with a history of vaping and either suspected or confirmed vaping-associated lung injury. All cases showed patterns of acute lung injury, including acute fibrinous pneumonitis, diffuse alveolar damage, or organizing pneumonia, the authors noted in a letter to the editor published in the New England Journal of Medicine.
While no histologic findings were specific, foamy macrophages and pneumocyte vacuolization were seen in all cases, the authors added. Pigmented macrophages were occasionally present but not dominant, neutrophils were often prominent, eosinophils were rare, and granulomas were not seen. Two patients eventually died, despite treatment with glucocorticoids and maximum supportive care.
“None of our cases showed histologic evidence of exogenous lipoid pneumonia and no radiologic evidence thereof has been found; this calls into question the diagnostic utility of identifying lipid-laden macrophages or performing oil red O staining on bronchioloalveolar lavage fluid as a marker of vaping-associated lung injury, as has been proposed,” Dr. Butt and associates wrote.
No conflicts of interest were reported.
SOURCE: Butt YM et al. N Engl J Med. 2019 Oct 2. doi: 10.1056/NEJMc1913069.
Vaping-associated lung injury is likely a form of airway-centered chemical pneumonitis, not exogenous lipoid pneumonia, according to Yasmeen M. Butt, MD, of the University of Texas Southwestern Medical Center, Dallas, and associates.
Dr. Butt and associates performed a review of lung biopsies from 17 patients (13 men; median age, 35 years) with a history of vaping and either suspected or confirmed vaping-associated lung injury. All cases showed patterns of acute lung injury, including acute fibrinous pneumonitis, diffuse alveolar damage, or organizing pneumonia, the authors noted in a letter to the editor published in the New England Journal of Medicine.
While no histologic findings were specific, foamy macrophages and pneumocyte vacuolization were seen in all cases, the authors added. Pigmented macrophages were occasionally present but not dominant, neutrophils were often prominent, eosinophils were rare, and granulomas were not seen. Two patients eventually died, despite treatment with glucocorticoids and maximum supportive care.
“None of our cases showed histologic evidence of exogenous lipoid pneumonia and no radiologic evidence thereof has been found; this calls into question the diagnostic utility of identifying lipid-laden macrophages or performing oil red O staining on bronchioloalveolar lavage fluid as a marker of vaping-associated lung injury, as has been proposed,” Dr. Butt and associates wrote.
No conflicts of interest were reported.
SOURCE: Butt YM et al. N Engl J Med. 2019 Oct 2. doi: 10.1056/NEJMc1913069.
Vaping-associated lung injury is likely a form of airway-centered chemical pneumonitis, not exogenous lipoid pneumonia, according to Yasmeen M. Butt, MD, of the University of Texas Southwestern Medical Center, Dallas, and associates.
Dr. Butt and associates performed a review of lung biopsies from 17 patients (13 men; median age, 35 years) with a history of vaping and either suspected or confirmed vaping-associated lung injury. All cases showed patterns of acute lung injury, including acute fibrinous pneumonitis, diffuse alveolar damage, or organizing pneumonia, the authors noted in a letter to the editor published in the New England Journal of Medicine.
While no histologic findings were specific, foamy macrophages and pneumocyte vacuolization were seen in all cases, the authors added. Pigmented macrophages were occasionally present but not dominant, neutrophils were often prominent, eosinophils were rare, and granulomas were not seen. Two patients eventually died, despite treatment with glucocorticoids and maximum supportive care.
“None of our cases showed histologic evidence of exogenous lipoid pneumonia and no radiologic evidence thereof has been found; this calls into question the diagnostic utility of identifying lipid-laden macrophages or performing oil red O staining on bronchioloalveolar lavage fluid as a marker of vaping-associated lung injury, as has been proposed,” Dr. Butt and associates wrote.
No conflicts of interest were reported.
SOURCE: Butt YM et al. N Engl J Med. 2019 Oct 2. doi: 10.1056/NEJMc1913069.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE