User login
Hospitals Reap Potential of Data Mining
In one recently publicized demonstration of data mining’s potential, Austin, Texas-based Seton Healthcare Family used software developed by IBM to pore over doctors’ notes and predict the risk of readmission among patients with congestive heart failure. Among the shortlist of biggest predictors, the analysis pointed to a lack of emotional support and a bulging jugular vein—factors that could be easily identified through inpatient screening but might otherwise be overlooked by staff.
Similarly, New York-Presbyterian Hospital used a system by Microsoft to help reduce the rates of blood clotting in patients through an objective analysis of such risk factors as cancer, smoking, and bed confinement.
In June, Deloitte and Utah-based Intermountain Healthcare announced the launch of OutcomesMiner, an analytics tool that uses electronic health records to ferret out important variations and associations among patient populations. Brett Davis, general manager of Deloitte Health Informatics, says understanding asthma patients who are in different age brackets, have different comorbidities, and are on different drugs, for example, can allow providers to better manage the population. Merely using ICD-9 codes often results in inaccurate patient classifications, he warns. Instead, capturing and analyzing data from medications and clinical encounters can be vital for properly defining an asthma patient and separating the signal from the noise.
In one recently publicized demonstration of data mining’s potential, Austin, Texas-based Seton Healthcare Family used software developed by IBM to pore over doctors’ notes and predict the risk of readmission among patients with congestive heart failure. Among the shortlist of biggest predictors, the analysis pointed to a lack of emotional support and a bulging jugular vein—factors that could be easily identified through inpatient screening but might otherwise be overlooked by staff.
Similarly, New York-Presbyterian Hospital used a system by Microsoft to help reduce the rates of blood clotting in patients through an objective analysis of such risk factors as cancer, smoking, and bed confinement.
In June, Deloitte and Utah-based Intermountain Healthcare announced the launch of OutcomesMiner, an analytics tool that uses electronic health records to ferret out important variations and associations among patient populations. Brett Davis, general manager of Deloitte Health Informatics, says understanding asthma patients who are in different age brackets, have different comorbidities, and are on different drugs, for example, can allow providers to better manage the population. Merely using ICD-9 codes often results in inaccurate patient classifications, he warns. Instead, capturing and analyzing data from medications and clinical encounters can be vital for properly defining an asthma patient and separating the signal from the noise.
In one recently publicized demonstration of data mining’s potential, Austin, Texas-based Seton Healthcare Family used software developed by IBM to pore over doctors’ notes and predict the risk of readmission among patients with congestive heart failure. Among the shortlist of biggest predictors, the analysis pointed to a lack of emotional support and a bulging jugular vein—factors that could be easily identified through inpatient screening but might otherwise be overlooked by staff.
Similarly, New York-Presbyterian Hospital used a system by Microsoft to help reduce the rates of blood clotting in patients through an objective analysis of such risk factors as cancer, smoking, and bed confinement.
In June, Deloitte and Utah-based Intermountain Healthcare announced the launch of OutcomesMiner, an analytics tool that uses electronic health records to ferret out important variations and associations among patient populations. Brett Davis, general manager of Deloitte Health Informatics, says understanding asthma patients who are in different age brackets, have different comorbidities, and are on different drugs, for example, can allow providers to better manage the population. Merely using ICD-9 codes often results in inaccurate patient classifications, he warns. Instead, capturing and analyzing data from medications and clinical encounters can be vital for properly defining an asthma patient and separating the signal from the noise.
Hospitalist Groups Extract New Solutions Via Data Mining
One hospital wanted to reduce readmissions among patients with congestive heart failure. Another hoped to improve upon its sepsis mortality rates. A third sought to determine whether its doctors were providing cost-effective care for pneumonia patients. All of them adopted the same type of technology to help identify a solution.
As the healthcare industry tilts toward accountable care, pay for performance and an increasingly

cost-conscious mindset, hospitalists and other providers are tapping into a fast-growing analytical tool collectively known as data mining to help make sense of the growing mounds of information. Although no single technology can be considered a cure-all, HM leaders are so optimistic about data mining’s potential to address cost, outcome, and performance issues that some have labeled it a “game changer” for hospitalists.
Karim Godamunne, MD, MBA, SFHM, chief medical officer at North Fulton Hospital in Roswell, Ga., and a member of SHM’s Practice Management Committee, says he can’t overstate the importance of hospitalists’ involvement in physician data mining. “From my perspective, we’re looking to hospitalists to help drive this quality-utilization bandwagon, to be the real leaders in it,” he says. With the tremendous value that can be generated through understanding and using the information, “it’s good for your group and can be good to your hospital as a whole.”
So what is data mining? The technology fully emerged in the mid-1990s as a way to help scientists analyze large and often disparate bodies of data, present relevant information in new ways, and illuminate previously unknown relationships.1 In the healthcare industry, early adopters realized that the insights gleaned from data mining could help inform their clinical decision-making; organizations used the new tools to help predict health insurance fraud and identify at-risk patients, for example.
Cynthia Burghard, research director of Accountable Care IT Strategies at IDC Health Insights in Framingham, Mass., says researchers in academic medical centers initially conducted most of the clinical analytical work. Within the past few years, however, the increasing availability of data has allowed more hospitals to begin analyzing chronic disease, readmissions, and other areas of concern. In addition, Burghard says, new tools based on natural language processing are giving hospitals better access to unstructured clinical data, such as notes written by doctors and nurses.
“What I’m seeing both in my surveys as well as in conversations with hospitals is that analytics is the top of the investment priority for both hospitals and health plans,” Burghard says. According to IDC estimates, total spending for clinical analytics in the U.S. reached $3.7 billion in 2012 and is expected to grow to $5.14 billion by 2016. Much of the growth, she notes, is being driven by healthcare reform. “If your mandate is to manage populations of patients, it behooves you to know who those patients are and what their illnesses are, and to monitor what you’re doing for them,” she says.
Practice Improvement
Accordingly, a major goal of all this data-mining technology is to change practice behavior in a way that achieves the triple aim of improving quality of care, controlling costs, and bettering patient outcomes.
A growing number of companies are releasing tools that can compile and analyze the separate bits of information captured from claims and billing systems, Medicare reporting requirements, internal benchmarks, and other sources. Unlike passive data sources, such as Medicare’s Hospital Compare website, more active analytics can help their users zoom down to the level of an individual doctor or patient, pan out to the level of a hospitalist group, or expand out even more for a broader comparison among peer institutions.
Some newer data-mining tools with names like CRIMSON, Truven, Iodine, and Imagine are billing themselves as hospitalist-friendly performance-improvement aids and giving individual providers the ability to access and analyze the data themselves. A few of these applications can even provide real-time data via mobile devices (see “Physician Performance Aids,”).
Thomas Frederickson, MD, MBA, SFHM, medical director of the HM service at Alegent Creighton Health in Omaha, Neb., and a member of SHM’s Practice Management Committee, sees the biggest potential of this data-mining technology in its ability to help drive practice consistency. “You can use the database to analyze practice patterns of large groups, or even individuals, and see where variability exists,” he says. “And then, based on that, you can analyze why the variability exists and begin to address whether it’s variability that’s clinically indicated or not.”
When Alegent Creighton Health was scrutinizing the care of its pneumonia patients, for example, officials could compare the number of chest X-rays per pneumonia patient by hospital or across the entire CRIMSON database. At a deeper level, the officials could see how often individual providers ordered the tests compared to their peers. For outliers, they could follow up to determine whether the variability was warranted.
As champions of process improvement, Dr. Frederickson says, hospitalists can make particularly good use of database analytics. “It’s part of the process of making hospitalists invaluable to their hospitals and their systems,” he says. “Part of that is building up expertise on process improvement and safety, and familiarity with these kinds of tools is one thing that will help us do that.”
North Fulton Hospital used CRIMSON to analyze how its doctors care for patients with sepsis and to establish new benchmarks. Dr. Godamunne says the tools allowed the hospital to track its doctors’ progress over time and identify potential problems. “If a patient with sepsis is staying too long, you can see who admitted the patient and see if, a few months ago, the same physician was having similar problems,” he says. Similarly, the hospital was able to track the top DRGs resulting in excess length of stay among patients, to identify potential bottlenecks in the care and discharge processes.
Some tools require only two-day training sessions for basic proficiency, though more advanced manipulations often require a bigger commitment, like the 12-week training session that Dr. Godamunne completed. That training included one hour of online learning and one hour of homework every week, and most of the cases highlighted during his coursework, he says, focused on hospitalists—another sign of the major role he believes HM will play in harnessing data to improve performance quality.

—Thomas Frederickson, MD, MBA, SFHM, medical director, hospital medicine service, Alegent Creighton Health, Omaha, Neb., SHM Practice Management Committee member
Slow—Construction Ahead
The best information is meaningful, individualized, and timely, says Steven Deitelzweig, MD, SFHM, system chairman for hospital medicine and medical director of regional business development at Ochsner Health System in New Orleans. “If you get something back six months after you’ve delivered the care, you’ll have a limited opportunity to improve, versus if you get it back in a week or two, or ideally, in real time,” says Dr. Deitelzweig, chair of SHM’s Practice Management Committee.
In examining length of stay, Dr. Deitelzweig says doctors could use data mining to look at time-stamped elements of patient flow and the timeliness of provider response: how patients go through the ED, and when they receive written orders or lab results. “It could be really powerful, and right now it’s a little bit of a black hole,” he says.
Based on her conversations with hospital executives and leaders, however, Burghard cautions that some real-time mobile applications, although technologically impressive, may be less useful or necessary in practice. “If it’s performance measurement, why do you need that in real time? It’s not going to change your behavior in the moment,” she says. “What you may want to get is an alert that your patient, who is in the hospital, has had some sort of negative event.”
Data mining has other potential limitations. “There’s always going to be questions of attribution, and you need to have clinical knowledge of your location,” Dr. Godamunne says. And data mining is only as good as the data that have been documented, underscoring the importance of securing provider cooperation.
Dr. Frederickson says physician acceptance, in fact, might be one of the biggest obstacles—a major reason why he recommends introducing the technology slowly and explaining why and how it will be used. If introduced too quickly and without adequate explanation about what a hospital or health system hopes to accomplish, he says, “there certainly is the potential for suspicion.” The key, he says, is to emphasize that the tools provide a valuable mechanism for gleaning new insights into doctors’ practice patterns, “not something that’s going to be used against them.”
Paul Roscoe, CEO of the Washington, D.C.-based Advisory Board Company's Crimson division, agrees that personally engaging physicians is essential for a good return on investment in analytical tools like his company’s suite of CRIMSON products. “If you can’t work with the physicians to get them to understand the data and actively use the data in their practice patterns, it becomes a bit meaningless,” he says.

—Karim Godamunne, MD, MBA, SFHM, chief medical officer, North Fulton Hospital, Roswell, Ga., SHM Practice Management Committee member
Roscoe sees big opportunities in prospectively examining information while a patient is still in the hospital and when a change of course by providers could avert a bad outcome. “Suggesting a set of interventions that they could do differently is really the value-add,” he says. But he cautions that those suggestions must be worded carefully to avoid alienating physicians.
“If doctors don’t feel like they’re being judged, they’ll engage with you,” Roscoe says.
Similar nuances can affect how users perceive the tools themselves. After hearing feedback from members that the words “data mining” didn’t conjure trust and confidence, the Advisory Board Company dropped the phrase altogether in favor of “data analytics,” “physician engagement,” and similar descriptors. “It’s simple things like that that can very quickly either turn a physician on or off,” Roscoe says.
Once users take the time to understand data-mining tools and how they can be properly harnessed, advocates say, the technology can lead to a host of unanticipated benefits. When a hospital bills the federal government for a Medicare patient, for example, it must submit an HCC code that describes the patient’s condition. By doing a better job of mining the data, Burghard says, a hospital can more accurately reflect that patient’s contdition. For example, if a hospital is treating a diabetic who comes in with a broken leg, the hospital could receive a lower payment rate if it does not properly identify and record both conditions.
And by using the tools prospectively, Burghard says, “I think there’s the opportunity to make a quantum leap from what we’re doing today. We usually just report on facts, and usually retrospectively. With some of the new technology that’s available, the healthcare industry can begin to do discovery analytics—you’re identifying insights, patterns, and relationships.”
Better integration of computerized physician order entry with data-mining ports, Dr. Godamunne predicts, will allow for much better attribution and finer parsing of the data. As the transparency increases, though, hospitalists will have to adapt to a new reality in which stronger analytical tools may point out individual outliers. And that level of detail, in turn, will require some hospitalists to justify why they’re different than their peers.
Even so, Roscoe says, he’s found that hospitalists are very open to using data to improve performance and that they make up a high percentage of CRIMSON users. “There isn’t a physician group that is in a better position to help drive this quality- and data-driven culture,” he says.
Bryn Nelson is a freelance medical writer in Seattle.
Physician Performance Aids

Company: The Advisory Board Company
Sample product: CRIMSON Continuum of Care
Claim: “Places credible, severity-adjusted performance profiles directly in the hands of physicians, enabling the hospital-physician collaboration needed to advance quality goals and secure cost savings.”
Number of users: More than 850 hospitals
Real-time data? No, but available as add-on service
To learn more: www.advisory.com/Technology/Crimson-Continuum-of-Care
Company: Panacea Developments
Sample product: Iodine
Claim: “An easy-to-use mobile system that analyzes a hospital’s sea of data for knowledge that physicians, case managers, and documentation specialists can act upon to improve length-of-stay, readmissions, and documentation.”
Number of users: More than 50 hospitals
Real-time data? Yes
To learn more: www.panaceadevelopments.com/iodine
Company: Truven Health
Sample product: CareDiscovery
Claim: “Provides powerful insights into a hospital’s or health system’s quality measures and resource utilization to support improvement with objective, fact-based information.”
Real-time data? No
Number of users: More than 3,000 users in 400 hospitals
To learn more: http://truvenhealth.com/products/carediscovery
Company: Ingenious Med
Sample product: Imagine
Claim: “A comprehensive analytics dashboard platform that provides actionable decision making data to optimize physician performance and revenue.”
Real-time data? Yes
Number of users: 25,000 total users (not separated by individual products)
To learn more: http://ingeniousmed.com/what-we-do/imagine
Reference
One hospital wanted to reduce readmissions among patients with congestive heart failure. Another hoped to improve upon its sepsis mortality rates. A third sought to determine whether its doctors were providing cost-effective care for pneumonia patients. All of them adopted the same type of technology to help identify a solution.
As the healthcare industry tilts toward accountable care, pay for performance and an increasingly
cost-conscious mindset, hospitalists and other providers are tapping into a fast-growing analytical tool collectively known as data mining to help make sense of the growing mounds of information. Although no single technology can be considered a cure-all, HM leaders are so optimistic about data mining’s potential to address cost, outcome, and performance issues that some have labeled it a “game changer” for hospitalists.
Karim Godamunne, MD, MBA, SFHM, chief medical officer at North Fulton Hospital in Roswell, Ga., and a member of SHM’s Practice Management Committee, says he can’t overstate the importance of hospitalists’ involvement in physician data mining. “From my perspective, we’re looking to hospitalists to help drive this quality-utilization bandwagon, to be the real leaders in it,” he says. With the tremendous value that can be generated through understanding and using the information, “it’s good for your group and can be good to your hospital as a whole.”
So what is data mining? The technology fully emerged in the mid-1990s as a way to help scientists analyze large and often disparate bodies of data, present relevant information in new ways, and illuminate previously unknown relationships.1 In the healthcare industry, early adopters realized that the insights gleaned from data mining could help inform their clinical decision-making; organizations used the new tools to help predict health insurance fraud and identify at-risk patients, for example.
Cynthia Burghard, research director of Accountable Care IT Strategies at IDC Health Insights in Framingham, Mass., says researchers in academic medical centers initially conducted most of the clinical analytical work. Within the past few years, however, the increasing availability of data has allowed more hospitals to begin analyzing chronic disease, readmissions, and other areas of concern. In addition, Burghard says, new tools based on natural language processing are giving hospitals better access to unstructured clinical data, such as notes written by doctors and nurses.
“What I’m seeing both in my surveys as well as in conversations with hospitals is that analytics is the top of the investment priority for both hospitals and health plans,” Burghard says. According to IDC estimates, total spending for clinical analytics in the U.S. reached $3.7 billion in 2012 and is expected to grow to $5.14 billion by 2016. Much of the growth, she notes, is being driven by healthcare reform. “If your mandate is to manage populations of patients, it behooves you to know who those patients are and what their illnesses are, and to monitor what you’re doing for them,” she says.
Practice Improvement
Accordingly, a major goal of all this data-mining technology is to change practice behavior in a way that achieves the triple aim of improving quality of care, controlling costs, and bettering patient outcomes.
A growing number of companies are releasing tools that can compile and analyze the separate bits of information captured from claims and billing systems, Medicare reporting requirements, internal benchmarks, and other sources. Unlike passive data sources, such as Medicare’s Hospital Compare website, more active analytics can help their users zoom down to the level of an individual doctor or patient, pan out to the level of a hospitalist group, or expand out even more for a broader comparison among peer institutions.
Some newer data-mining tools with names like CRIMSON, Truven, Iodine, and Imagine are billing themselves as hospitalist-friendly performance-improvement aids and giving individual providers the ability to access and analyze the data themselves. A few of these applications can even provide real-time data via mobile devices (see “Physician Performance Aids,”).
Thomas Frederickson, MD, MBA, SFHM, medical director of the HM service at Alegent Creighton Health in Omaha, Neb., and a member of SHM’s Practice Management Committee, sees the biggest potential of this data-mining technology in its ability to help drive practice consistency. “You can use the database to analyze practice patterns of large groups, or even individuals, and see where variability exists,” he says. “And then, based on that, you can analyze why the variability exists and begin to address whether it’s variability that’s clinically indicated or not.”
When Alegent Creighton Health was scrutinizing the care of its pneumonia patients, for example, officials could compare the number of chest X-rays per pneumonia patient by hospital or across the entire CRIMSON database. At a deeper level, the officials could see how often individual providers ordered the tests compared to their peers. For outliers, they could follow up to determine whether the variability was warranted.
As champions of process improvement, Dr. Frederickson says, hospitalists can make particularly good use of database analytics. “It’s part of the process of making hospitalists invaluable to their hospitals and their systems,” he says. “Part of that is building up expertise on process improvement and safety, and familiarity with these kinds of tools is one thing that will help us do that.”
North Fulton Hospital used CRIMSON to analyze how its doctors care for patients with sepsis and to establish new benchmarks. Dr. Godamunne says the tools allowed the hospital to track its doctors’ progress over time and identify potential problems. “If a patient with sepsis is staying too long, you can see who admitted the patient and see if, a few months ago, the same physician was having similar problems,” he says. Similarly, the hospital was able to track the top DRGs resulting in excess length of stay among patients, to identify potential bottlenecks in the care and discharge processes.
Some tools require only two-day training sessions for basic proficiency, though more advanced manipulations often require a bigger commitment, like the 12-week training session that Dr. Godamunne completed. That training included one hour of online learning and one hour of homework every week, and most of the cases highlighted during his coursework, he says, focused on hospitalists—another sign of the major role he believes HM will play in harnessing data to improve performance quality.
—Thomas Frederickson, MD, MBA, SFHM, medical director, hospital medicine service, Alegent Creighton Health, Omaha, Neb., SHM Practice Management Committee member
Slow—Construction Ahead
The best information is meaningful, individualized, and timely, says Steven Deitelzweig, MD, SFHM, system chairman for hospital medicine and medical director of regional business development at Ochsner Health System in New Orleans. “If you get something back six months after you’ve delivered the care, you’ll have a limited opportunity to improve, versus if you get it back in a week or two, or ideally, in real time,” says Dr. Deitelzweig, chair of SHM’s Practice Management Committee.
In examining length of stay, Dr. Deitelzweig says doctors could use data mining to look at time-stamped elements of patient flow and the timeliness of provider response: how patients go through the ED, and when they receive written orders or lab results. “It could be really powerful, and right now it’s a little bit of a black hole,” he says.
Based on her conversations with hospital executives and leaders, however, Burghard cautions that some real-time mobile applications, although technologically impressive, may be less useful or necessary in practice. “If it’s performance measurement, why do you need that in real time? It’s not going to change your behavior in the moment,” she says. “What you may want to get is an alert that your patient, who is in the hospital, has had some sort of negative event.”
Data mining has other potential limitations. “There’s always going to be questions of attribution, and you need to have clinical knowledge of your location,” Dr. Godamunne says. And data mining is only as good as the data that have been documented, underscoring the importance of securing provider cooperation.
Dr. Frederickson says physician acceptance, in fact, might be one of the biggest obstacles—a major reason why he recommends introducing the technology slowly and explaining why and how it will be used. If introduced too quickly and without adequate explanation about what a hospital or health system hopes to accomplish, he says, “there certainly is the potential for suspicion.” The key, he says, is to emphasize that the tools provide a valuable mechanism for gleaning new insights into doctors’ practice patterns, “not something that’s going to be used against them.”
Paul Roscoe, CEO of the Washington, D.C.-based Advisory Board Company's Crimson division, agrees that personally engaging physicians is essential for a good return on investment in analytical tools like his company’s suite of CRIMSON products. “If you can’t work with the physicians to get them to understand the data and actively use the data in their practice patterns, it becomes a bit meaningless,” he says.
—Karim Godamunne, MD, MBA, SFHM, chief medical officer, North Fulton Hospital, Roswell, Ga., SHM Practice Management Committee member
Roscoe sees big opportunities in prospectively examining information while a patient is still in the hospital and when a change of course by providers could avert a bad outcome. “Suggesting a set of interventions that they could do differently is really the value-add,” he says. But he cautions that those suggestions must be worded carefully to avoid alienating physicians.
“If doctors don’t feel like they’re being judged, they’ll engage with you,” Roscoe says.
Similar nuances can affect how users perceive the tools themselves. After hearing feedback from members that the words “data mining” didn’t conjure trust and confidence, the Advisory Board Company dropped the phrase altogether in favor of “data analytics,” “physician engagement,” and similar descriptors. “It’s simple things like that that can very quickly either turn a physician on or off,” Roscoe says.
Once users take the time to understand data-mining tools and how they can be properly harnessed, advocates say, the technology can lead to a host of unanticipated benefits. When a hospital bills the federal government for a Medicare patient, for example, it must submit an HCC code that describes the patient’s condition. By doing a better job of mining the data, Burghard says, a hospital can more accurately reflect that patient’s contdition. For example, if a hospital is treating a diabetic who comes in with a broken leg, the hospital could receive a lower payment rate if it does not properly identify and record both conditions.
And by using the tools prospectively, Burghard says, “I think there’s the opportunity to make a quantum leap from what we’re doing today. We usually just report on facts, and usually retrospectively. With some of the new technology that’s available, the healthcare industry can begin to do discovery analytics—you’re identifying insights, patterns, and relationships.”
Better integration of computerized physician order entry with data-mining ports, Dr. Godamunne predicts, will allow for much better attribution and finer parsing of the data. As the transparency increases, though, hospitalists will have to adapt to a new reality in which stronger analytical tools may point out individual outliers. And that level of detail, in turn, will require some hospitalists to justify why they’re different than their peers.
Even so, Roscoe says, he’s found that hospitalists are very open to using data to improve performance and that they make up a high percentage of CRIMSON users. “There isn’t a physician group that is in a better position to help drive this quality- and data-driven culture,” he says.
Bryn Nelson is a freelance medical writer in Seattle.
Physician Performance Aids
Company: The Advisory Board Company
Sample product: CRIMSON Continuum of Care
Claim: “Places credible, severity-adjusted performance profiles directly in the hands of physicians, enabling the hospital-physician collaboration needed to advance quality goals and secure cost savings.”
Number of users: More than 850 hospitals
Real-time data? No, but available as add-on service
To learn more: www.advisory.com/Technology/Crimson-Continuum-of-Care
Company: Panacea Developments
Sample product: Iodine
Claim: “An easy-to-use mobile system that analyzes a hospital’s sea of data for knowledge that physicians, case managers, and documentation specialists can act upon to improve length-of-stay, readmissions, and documentation.”
Number of users: More than 50 hospitals
Real-time data? Yes
To learn more: www.panaceadevelopments.com/iodine
Company: Truven Health
Sample product: CareDiscovery
Claim: “Provides powerful insights into a hospital’s or health system’s quality measures and resource utilization to support improvement with objective, fact-based information.”
Real-time data? No
Number of users: More than 3,000 users in 400 hospitals
To learn more: http://truvenhealth.com/products/carediscovery
Company: Ingenious Med
Sample product: Imagine
Claim: “A comprehensive analytics dashboard platform that provides actionable decision making data to optimize physician performance and revenue.”
Real-time data? Yes
Number of users: 25,000 total users (not separated by individual products)
To learn more: http://ingeniousmed.com/what-we-do/imagine
Reference
One hospital wanted to reduce readmissions among patients with congestive heart failure. Another hoped to improve upon its sepsis mortality rates. A third sought to determine whether its doctors were providing cost-effective care for pneumonia patients. All of them adopted the same type of technology to help identify a solution.
As the healthcare industry tilts toward accountable care, pay for performance and an increasingly
cost-conscious mindset, hospitalists and other providers are tapping into a fast-growing analytical tool collectively known as data mining to help make sense of the growing mounds of information. Although no single technology can be considered a cure-all, HM leaders are so optimistic about data mining’s potential to address cost, outcome, and performance issues that some have labeled it a “game changer” for hospitalists.
Karim Godamunne, MD, MBA, SFHM, chief medical officer at North Fulton Hospital in Roswell, Ga., and a member of SHM’s Practice Management Committee, says he can’t overstate the importance of hospitalists’ involvement in physician data mining. “From my perspective, we’re looking to hospitalists to help drive this quality-utilization bandwagon, to be the real leaders in it,” he says. With the tremendous value that can be generated through understanding and using the information, “it’s good for your group and can be good to your hospital as a whole.”
So what is data mining? The technology fully emerged in the mid-1990s as a way to help scientists analyze large and often disparate bodies of data, present relevant information in new ways, and illuminate previously unknown relationships.1 In the healthcare industry, early adopters realized that the insights gleaned from data mining could help inform their clinical decision-making; organizations used the new tools to help predict health insurance fraud and identify at-risk patients, for example.
Cynthia Burghard, research director of Accountable Care IT Strategies at IDC Health Insights in Framingham, Mass., says researchers in academic medical centers initially conducted most of the clinical analytical work. Within the past few years, however, the increasing availability of data has allowed more hospitals to begin analyzing chronic disease, readmissions, and other areas of concern. In addition, Burghard says, new tools based on natural language processing are giving hospitals better access to unstructured clinical data, such as notes written by doctors and nurses.
“What I’m seeing both in my surveys as well as in conversations with hospitals is that analytics is the top of the investment priority for both hospitals and health plans,” Burghard says. According to IDC estimates, total spending for clinical analytics in the U.S. reached $3.7 billion in 2012 and is expected to grow to $5.14 billion by 2016. Much of the growth, she notes, is being driven by healthcare reform. “If your mandate is to manage populations of patients, it behooves you to know who those patients are and what their illnesses are, and to monitor what you’re doing for them,” she says.
Practice Improvement
Accordingly, a major goal of all this data-mining technology is to change practice behavior in a way that achieves the triple aim of improving quality of care, controlling costs, and bettering patient outcomes.
A growing number of companies are releasing tools that can compile and analyze the separate bits of information captured from claims and billing systems, Medicare reporting requirements, internal benchmarks, and other sources. Unlike passive data sources, such as Medicare’s Hospital Compare website, more active analytics can help their users zoom down to the level of an individual doctor or patient, pan out to the level of a hospitalist group, or expand out even more for a broader comparison among peer institutions.
Some newer data-mining tools with names like CRIMSON, Truven, Iodine, and Imagine are billing themselves as hospitalist-friendly performance-improvement aids and giving individual providers the ability to access and analyze the data themselves. A few of these applications can even provide real-time data via mobile devices (see “Physician Performance Aids,”).
Thomas Frederickson, MD, MBA, SFHM, medical director of the HM service at Alegent Creighton Health in Omaha, Neb., and a member of SHM’s Practice Management Committee, sees the biggest potential of this data-mining technology in its ability to help drive practice consistency. “You can use the database to analyze practice patterns of large groups, or even individuals, and see where variability exists,” he says. “And then, based on that, you can analyze why the variability exists and begin to address whether it’s variability that’s clinically indicated or not.”
When Alegent Creighton Health was scrutinizing the care of its pneumonia patients, for example, officials could compare the number of chest X-rays per pneumonia patient by hospital or across the entire CRIMSON database. At a deeper level, the officials could see how often individual providers ordered the tests compared to their peers. For outliers, they could follow up to determine whether the variability was warranted.
As champions of process improvement, Dr. Frederickson says, hospitalists can make particularly good use of database analytics. “It’s part of the process of making hospitalists invaluable to their hospitals and their systems,” he says. “Part of that is building up expertise on process improvement and safety, and familiarity with these kinds of tools is one thing that will help us do that.”
North Fulton Hospital used CRIMSON to analyze how its doctors care for patients with sepsis and to establish new benchmarks. Dr. Godamunne says the tools allowed the hospital to track its doctors’ progress over time and identify potential problems. “If a patient with sepsis is staying too long, you can see who admitted the patient and see if, a few months ago, the same physician was having similar problems,” he says. Similarly, the hospital was able to track the top DRGs resulting in excess length of stay among patients, to identify potential bottlenecks in the care and discharge processes.
Some tools require only two-day training sessions for basic proficiency, though more advanced manipulations often require a bigger commitment, like the 12-week training session that Dr. Godamunne completed. That training included one hour of online learning and one hour of homework every week, and most of the cases highlighted during his coursework, he says, focused on hospitalists—another sign of the major role he believes HM will play in harnessing data to improve performance quality.
—Thomas Frederickson, MD, MBA, SFHM, medical director, hospital medicine service, Alegent Creighton Health, Omaha, Neb., SHM Practice Management Committee member
Slow—Construction Ahead
The best information is meaningful, individualized, and timely, says Steven Deitelzweig, MD, SFHM, system chairman for hospital medicine and medical director of regional business development at Ochsner Health System in New Orleans. “If you get something back six months after you’ve delivered the care, you’ll have a limited opportunity to improve, versus if you get it back in a week or two, or ideally, in real time,” says Dr. Deitelzweig, chair of SHM’s Practice Management Committee.
In examining length of stay, Dr. Deitelzweig says doctors could use data mining to look at time-stamped elements of patient flow and the timeliness of provider response: how patients go through the ED, and when they receive written orders or lab results. “It could be really powerful, and right now it’s a little bit of a black hole,” he says.
Based on her conversations with hospital executives and leaders, however, Burghard cautions that some real-time mobile applications, although technologically impressive, may be less useful or necessary in practice. “If it’s performance measurement, why do you need that in real time? It’s not going to change your behavior in the moment,” she says. “What you may want to get is an alert that your patient, who is in the hospital, has had some sort of negative event.”
Data mining has other potential limitations. “There’s always going to be questions of attribution, and you need to have clinical knowledge of your location,” Dr. Godamunne says. And data mining is only as good as the data that have been documented, underscoring the importance of securing provider cooperation.
Dr. Frederickson says physician acceptance, in fact, might be one of the biggest obstacles—a major reason why he recommends introducing the technology slowly and explaining why and how it will be used. If introduced too quickly and without adequate explanation about what a hospital or health system hopes to accomplish, he says, “there certainly is the potential for suspicion.” The key, he says, is to emphasize that the tools provide a valuable mechanism for gleaning new insights into doctors’ practice patterns, “not something that’s going to be used against them.”
Paul Roscoe, CEO of the Washington, D.C.-based Advisory Board Company's Crimson division, agrees that personally engaging physicians is essential for a good return on investment in analytical tools like his company’s suite of CRIMSON products. “If you can’t work with the physicians to get them to understand the data and actively use the data in their practice patterns, it becomes a bit meaningless,” he says.
—Karim Godamunne, MD, MBA, SFHM, chief medical officer, North Fulton Hospital, Roswell, Ga., SHM Practice Management Committee member
Roscoe sees big opportunities in prospectively examining information while a patient is still in the hospital and when a change of course by providers could avert a bad outcome. “Suggesting a set of interventions that they could do differently is really the value-add,” he says. But he cautions that those suggestions must be worded carefully to avoid alienating physicians.
“If doctors don’t feel like they’re being judged, they’ll engage with you,” Roscoe says.
Similar nuances can affect how users perceive the tools themselves. After hearing feedback from members that the words “data mining” didn’t conjure trust and confidence, the Advisory Board Company dropped the phrase altogether in favor of “data analytics,” “physician engagement,” and similar descriptors. “It’s simple things like that that can very quickly either turn a physician on or off,” Roscoe says.
Once users take the time to understand data-mining tools and how they can be properly harnessed, advocates say, the technology can lead to a host of unanticipated benefits. When a hospital bills the federal government for a Medicare patient, for example, it must submit an HCC code that describes the patient’s condition. By doing a better job of mining the data, Burghard says, a hospital can more accurately reflect that patient’s contdition. For example, if a hospital is treating a diabetic who comes in with a broken leg, the hospital could receive a lower payment rate if it does not properly identify and record both conditions.
And by using the tools prospectively, Burghard says, “I think there’s the opportunity to make a quantum leap from what we’re doing today. We usually just report on facts, and usually retrospectively. With some of the new technology that’s available, the healthcare industry can begin to do discovery analytics—you’re identifying insights, patterns, and relationships.”
Better integration of computerized physician order entry with data-mining ports, Dr. Godamunne predicts, will allow for much better attribution and finer parsing of the data. As the transparency increases, though, hospitalists will have to adapt to a new reality in which stronger analytical tools may point out individual outliers. And that level of detail, in turn, will require some hospitalists to justify why they’re different than their peers.
Even so, Roscoe says, he’s found that hospitalists are very open to using data to improve performance and that they make up a high percentage of CRIMSON users. “There isn’t a physician group that is in a better position to help drive this quality- and data-driven culture,” he says.
Bryn Nelson is a freelance medical writer in Seattle.
Physician Performance Aids
Company: The Advisory Board Company
Sample product: CRIMSON Continuum of Care
Claim: “Places credible, severity-adjusted performance profiles directly in the hands of physicians, enabling the hospital-physician collaboration needed to advance quality goals and secure cost savings.”
Number of users: More than 850 hospitals
Real-time data? No, but available as add-on service
To learn more: www.advisory.com/Technology/Crimson-Continuum-of-Care
Company: Panacea Developments
Sample product: Iodine
Claim: “An easy-to-use mobile system that analyzes a hospital’s sea of data for knowledge that physicians, case managers, and documentation specialists can act upon to improve length-of-stay, readmissions, and documentation.”
Number of users: More than 50 hospitals
Real-time data? Yes
To learn more: www.panaceadevelopments.com/iodine
Company: Truven Health
Sample product: CareDiscovery
Claim: “Provides powerful insights into a hospital’s or health system’s quality measures and resource utilization to support improvement with objective, fact-based information.”
Real-time data? No
Number of users: More than 3,000 users in 400 hospitals
To learn more: http://truvenhealth.com/products/carediscovery
Company: Ingenious Med
Sample product: Imagine
Claim: “A comprehensive analytics dashboard platform that provides actionable decision making data to optimize physician performance and revenue.”
Real-time data? Yes
Number of users: 25,000 total users (not separated by individual products)
To learn more: http://ingeniousmed.com/what-we-do/imagine
Reference
Actors Help Health-Care Providers Develop Better Patient Communication Skills

Hospitalists and ED physicians at Newton Medical Center in New Jersey recently participated in an improvised, interactive learning experience with actors who portrayed problematic patients. “Developing Doctor-Patient Relations through Better Communication” is a curriculum to test and teach communication skills for doctors that was created by Anthony Orsini, MD, a neonatologist at Morristown Medical Center, Newton’s sister facility in the Atlantic Health System. Dr. Orsini founded the Breaking Bad News Foundation (www.bbnfoundation.org) more than a decade ago to help health professionals impart bad medical news to patients and families.
Physicians role-play with actors in such difficult scenarios as imparting a troubling diagnosis to a patient who does not want to hear it. This interaction is viewed remotely by instructors from the foundation and by peers, who then meet with the doctor to go over the videotaped encounter regarding its effectiveness, spoken messages, body language, and other communications.
The project to improve staff communication skills is enhancing teamwork between Newton’s hospitalists and emergency doctors, according to David Stuhlmiller, MD, the hospital’s director of emergency medicine.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Hospitalists and ED physicians at Newton Medical Center in New Jersey recently participated in an improvised, interactive learning experience with actors who portrayed problematic patients. “Developing Doctor-Patient Relations through Better Communication” is a curriculum to test and teach communication skills for doctors that was created by Anthony Orsini, MD, a neonatologist at Morristown Medical Center, Newton’s sister facility in the Atlantic Health System. Dr. Orsini founded the Breaking Bad News Foundation (www.bbnfoundation.org) more than a decade ago to help health professionals impart bad medical news to patients and families.
Physicians role-play with actors in such difficult scenarios as imparting a troubling diagnosis to a patient who does not want to hear it. This interaction is viewed remotely by instructors from the foundation and by peers, who then meet with the doctor to go over the videotaped encounter regarding its effectiveness, spoken messages, body language, and other communications.
The project to improve staff communication skills is enhancing teamwork between Newton’s hospitalists and emergency doctors, according to David Stuhlmiller, MD, the hospital’s director of emergency medicine.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Hospitalists and ED physicians at Newton Medical Center in New Jersey recently participated in an improvised, interactive learning experience with actors who portrayed problematic patients. “Developing Doctor-Patient Relations through Better Communication” is a curriculum to test and teach communication skills for doctors that was created by Anthony Orsini, MD, a neonatologist at Morristown Medical Center, Newton’s sister facility in the Atlantic Health System. Dr. Orsini founded the Breaking Bad News Foundation (www.bbnfoundation.org) more than a decade ago to help health professionals impart bad medical news to patients and families.
Physicians role-play with actors in such difficult scenarios as imparting a troubling diagnosis to a patient who does not want to hear it. This interaction is viewed remotely by instructors from the foundation and by peers, who then meet with the doctor to go over the videotaped encounter regarding its effectiveness, spoken messages, body language, and other communications.
The project to improve staff communication skills is enhancing teamwork between Newton’s hospitalists and emergency doctors, according to David Stuhlmiller, MD, the hospital’s director of emergency medicine.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Multiple Approaches to Combat High Hospital Patient Census

In this age of cost containment and fiscal frugality, how do you handle high-census periods without jeopardizing patient care?
–Michael P. Mason, Tulsa, Okla.
Dr. Hospitalist responds:
Your group must first define the term “high census,” because workload is based on many factors. Seeing 20 patients a day in a large inner-city hospital is much different from seeing 20 patients in a suburban hospital in an affluent part of town. Also, seeing 20 patients geographically located on the same floor is much easier than 20 patients spread all over the hospital. Mid-level or nurse case-management support also makes a difference.
Once defined, there are many different ways to handle the high census; each hospitalist group must decide what works for them.
Many groups rely on their compensation structure to entice their physicians to see higher numbers of patients. The pay structure may be production-based and entice many of the group members to see more patients. Typically, for the member that does not want to see the large volumes, there are usually colleagues who are more than happy to cover the excess patients.
Some groups employ a hybrid system, with their compensation based on production and salary. Generally, bonuses or incentives are applied after meeting a specific relative value unit (RVU) threshold. These thresholds vary and usually are raised periodically based on the percentage of staff able to collect. Again, some group members may volunteer to see the excess patients for higher compensation. It is up to the group to develop mechanisms to measure the quality of care of these high producers and monitor for burnout.
Then there are groups that have no volume incentives and everyone is paid a salary. Many groups that utilize any of these compensation models have group members “on call” to come in when needed and see the excess patients. Many pay the on-call person some nominal amount just for being on call, or a per-patient or hourly rate if they have to come in. Others make it a mandatory part of the schedule without any additional compensation.
Many groups have integrated advanced-practice providers (nurse practitioners and physician assistants) into their systems. They can help hospitalists improve efficiency by seeing patients that are less ill or awaiting placement, or by performing such labor-intensive tasks as admissions and discharges.
HM groups should collaborate with the hospital’s chief financial officer. Like clinicians, most administrators recognize it is very difficult to deliver high-quality and efficient care when the numbers get high. It is in their best interest to help devise strategies and models that deliver quality care and the metrics needed to sustain support.
HM has become such a large specialty that there is no-one-size-fits-all solution to high censuses. In the end, you have to be comfortable with the system created by your group, work to help improve it, or seek a better fit.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
In this age of cost containment and fiscal frugality, how do you handle high-census periods without jeopardizing patient care?
–Michael P. Mason, Tulsa, Okla.
Dr. Hospitalist responds:
Your group must first define the term “high census,” because workload is based on many factors. Seeing 20 patients a day in a large inner-city hospital is much different from seeing 20 patients in a suburban hospital in an affluent part of town. Also, seeing 20 patients geographically located on the same floor is much easier than 20 patients spread all over the hospital. Mid-level or nurse case-management support also makes a difference.
Once defined, there are many different ways to handle the high census; each hospitalist group must decide what works for them.
Many groups rely on their compensation structure to entice their physicians to see higher numbers of patients. The pay structure may be production-based and entice many of the group members to see more patients. Typically, for the member that does not want to see the large volumes, there are usually colleagues who are more than happy to cover the excess patients.
Some groups employ a hybrid system, with their compensation based on production and salary. Generally, bonuses or incentives are applied after meeting a specific relative value unit (RVU) threshold. These thresholds vary and usually are raised periodically based on the percentage of staff able to collect. Again, some group members may volunteer to see the excess patients for higher compensation. It is up to the group to develop mechanisms to measure the quality of care of these high producers and monitor for burnout.
Then there are groups that have no volume incentives and everyone is paid a salary. Many groups that utilize any of these compensation models have group members “on call” to come in when needed and see the excess patients. Many pay the on-call person some nominal amount just for being on call, or a per-patient or hourly rate if they have to come in. Others make it a mandatory part of the schedule without any additional compensation.
Many groups have integrated advanced-practice providers (nurse practitioners and physician assistants) into their systems. They can help hospitalists improve efficiency by seeing patients that are less ill or awaiting placement, or by performing such labor-intensive tasks as admissions and discharges.
HM groups should collaborate with the hospital’s chief financial officer. Like clinicians, most administrators recognize it is very difficult to deliver high-quality and efficient care when the numbers get high. It is in their best interest to help devise strategies and models that deliver quality care and the metrics needed to sustain support.
HM has become such a large specialty that there is no-one-size-fits-all solution to high censuses. In the end, you have to be comfortable with the system created by your group, work to help improve it, or seek a better fit.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
In this age of cost containment and fiscal frugality, how do you handle high-census periods without jeopardizing patient care?
–Michael P. Mason, Tulsa, Okla.
Dr. Hospitalist responds:
Your group must first define the term “high census,” because workload is based on many factors. Seeing 20 patients a day in a large inner-city hospital is much different from seeing 20 patients in a suburban hospital in an affluent part of town. Also, seeing 20 patients geographically located on the same floor is much easier than 20 patients spread all over the hospital. Mid-level or nurse case-management support also makes a difference.
Once defined, there are many different ways to handle the high census; each hospitalist group must decide what works for them.
Many groups rely on their compensation structure to entice their physicians to see higher numbers of patients. The pay structure may be production-based and entice many of the group members to see more patients. Typically, for the member that does not want to see the large volumes, there are usually colleagues who are more than happy to cover the excess patients.
Some groups employ a hybrid system, with their compensation based on production and salary. Generally, bonuses or incentives are applied after meeting a specific relative value unit (RVU) threshold. These thresholds vary and usually are raised periodically based on the percentage of staff able to collect. Again, some group members may volunteer to see the excess patients for higher compensation. It is up to the group to develop mechanisms to measure the quality of care of these high producers and monitor for burnout.
Then there are groups that have no volume incentives and everyone is paid a salary. Many groups that utilize any of these compensation models have group members “on call” to come in when needed and see the excess patients. Many pay the on-call person some nominal amount just for being on call, or a per-patient or hourly rate if they have to come in. Others make it a mandatory part of the schedule without any additional compensation.
Many groups have integrated advanced-practice providers (nurse practitioners and physician assistants) into their systems. They can help hospitalists improve efficiency by seeing patients that are less ill or awaiting placement, or by performing such labor-intensive tasks as admissions and discharges.
HM groups should collaborate with the hospital’s chief financial officer. Like clinicians, most administrators recognize it is very difficult to deliver high-quality and efficient care when the numbers get high. It is in their best interest to help devise strategies and models that deliver quality care and the metrics needed to sustain support.
HM has become such a large specialty that there is no-one-size-fits-all solution to high censuses. In the end, you have to be comfortable with the system created by your group, work to help improve it, or seek a better fit.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to drhospit@wiley.com.
Reviews of Research on Health-Care Acquired Infections, Glucocorticoid Therapy in COPD, and Blood-Pressure Lowering in Intracerebral Hemorrhages
In This Edition
Literature At A Glance
A guide to this month’s studies
- Perioperative SSRI use associated with adverse surgical outcomes
- Copper-surfaced rooms reduce health-care-acquired infections
- Glucocorticoid therapy for five days not inferior to 14 days for COPD exacerbation
- Patient preference for participation in medical decision-making may be associated with increased resource utilization
- Early parenteral nutrition in critically ill adults does not significantly affect mortality or infection rates
- Aggressive fluid and sodium restriction in acute decompensated heart failure did not improve outcomes
- Lower rate of pacemaker, defibrillator device-pocket hematoma without anticoagulation interruption
- Prophylactic penicillin decreased risk of recurrent leg cellulitis
- Universal ICU decolonization reduced rates of mrsa clinical isolates and bloodstream infection
- Intensive blood-pressure lowering in intracerebral hemorrhage did not reduce death or severe disability
Perioperative SSRI Use Associated with Adverse Surgical Outcomes
Clinical question: Does selective serotonin reuptake inhibitor (SSRI) use during hospitalization for surgery increase the risk of adverse perioperative outcomes?
Background: SSRIs commonly are prescribed but are associated with a small but higher risk for hemorrhage, arrhythmia, and sudden death. Single-site studies have described an association between SSRIs and adverse perioperative outcomes, but larger studies utilizing a broad range of surgical cases are lacking.
Study design: Retrospective cohort study.
Setting: Three hundred hospitals concentrated in the Southern U.S.
Synopsis: Using the “Perspective” database, this study examined 530,416 patients age >18 years undergoing major elective surgery, 72,540 (13.7%) of whom received an SSRI. Regression analysis showed patients receiving an SSRI had higher odds of mortality (OR 1.2, 95% CI [1.07-1.36]), higher odds of 30-day readmission (OR 1.22 [1.18-1.26]), and higher odds for bleeding (1.09 [1.04-1.15]). When the analysis was restricted to only patients with a diagnosis of depression, a higher risk of bleeding and readmission persisted.
This study reaffirms an association but does not establish a causal relationship between SSRI use and adverse perioperative outcomes. SSRI use may be a surrogate for other factors, including more severe mood disorders, poorer functional status, or chronic pain. Additionally, no information has been provided as to optimal duration of withholding SSRIs preoperatively. As such, it may be premature for hospitalists involved in perioperative care to modify recommendations based on this study.
Bottom line: Perioperative SSRI use is associated with an increased risk of bleeding and 30-day readmission.
Citation: Auerbach AD, Vittinghoff E, Maselli J, et al. Perioperative use of selective serotonin reuptake inhibitors and risks for adverse outcomes of surgery. JAMA Intern Med. 2013;173(12):1075-1081.
Copper-Surfaced Rooms Reduce Health-Care-Acquired Infections
Clinical question: Can copper alloy surfaces in ICU rooms lower rates of health-care-acquired infections (HAIs)?
Background: Environmental contamination is a potential source of HAIs. Copper has intrinsic broad-spectrum antimicrobial properties. This study tests the efficacy copper-surfaced items in hospital rooms have in preventing HAIs.
Study design: Randomized controlled trial.
Setting: Medical ICUs at Medical University of South Carolina and Ralph H. Johnson Veterans Affairs Medical Center in Charleston, and the Memorial Sloan Kettering Cancer Center in New York City.
Synopsis: Six hundred fifty ICU patients were randomized to receive care either in rooms with copper surfacing on commonly handled patient care objects or in traditional rooms. Patients were screened for methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) on admission. The proportion of patients that developed either an HAI and/or MRSA or VRE colonization was significantly lower among patients in rooms with the copper-surfaced items (0.071 vs. 0.128; P=0.02). The rate of HAIs alone was also lower in the rooms with the copper (0.034 vs. 0.081; P=0.013).
A potential limitation to this study is that the rooms with copper items appeared different than traditional rooms, and therefore might have changed the behavior of health-care workers. Further, it is unclear how much copper surfacing would be necessary on general wards, where patients are more mobile. Still, HAIs are associated with longer lengths of stay and higher 30-day readmission rates, so these encouraging results warrant additional investigation into antimicrobial copper-alloy surfaces.
Bottom line: Copper-surfaced objects reduce HAI rates in ICU patients.
Citation: Salgado CD, Sepkowitz, KA, John JF, et al. Copper surfaces reduce the rate of healthcare-acquired infections in the intensive care unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
Glucocorticoid Therapy for Five Days Not Inferior to 14 Days for COPD Exacerbation
Clinical question: Do short-course glucocorticoids work as well as conventional long courses for COPD exacerbation?
Background: International guidelines advocate a seven- to 14-day treatment course with glucocorticoids for COPD exacerbation, but the optimal duration of treatment is not known, and there are potential risks associated with glucocorticoid exposure.
Study design: Randomized, noninferiority, multicenter trial.
Setting: Five Swiss teaching hospitals.
Synopsis: Three hundred fourteen patients presenting to the ED with acute COPD exacerbation and without a history of asthma were randomized to receive treatment with 40 mg prednisone daily for either five or 14 days in a placebo-controlled, double-blinded fashion. There was no significant difference in the primary endpoint of re-exacerbation within six months. Patients in the five-day glucocorticoid group compared with the 14-day group were exposed to significantly less glucocorticoid.
Bottom line: Treatment for five days with glucocorticoids was not inferior to 14 days for acute COPD exacerbations with regard to re-exacerbations within six months and resulted in less glucocorticoid exposure overall.
Citation: Leuppi JF, Schuetz P, Bingisser R, et al. Short-term vs. conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE Randomized Clinical Trial. JAMA. 2013;390(21):2223-2231.
Patient Preference for Participation in Medical Decision-Making May Be Associated with Increased Resource Utilization
Clinical question: Do patient preferences for participation in medical decision-making affect health-care utilization?
Background: Patient participation in medical decision-making has been associated with improved patient satisfaction and health outcomes. There is little evidence to support theories that patient preferences might decrease or increase health-care utilization.
Study design: Survey study in academic research setting.
Setting: University of Chicago Medical Center.
Synopsis: More than 21,700 patients admitted to a general internal-medicine service completed a survey that included questions regarding preferences about receiving medical information and participation in medical decision-making. Survey data were linked with administrative data, including length of stay and total hospitalization costs.
Most patients (96.3%) expressed interest in receiving information about their illness and treatment options, but the majority of patients (71.1%) also expressed a preference to leave medical decision-making to their physician. Patients who preferred to participate in medical decision-making had significantly longer hospital LOS and higher total hospitalization cost.
Bottom line: Participation in medical decision-making significantly increased LOS and total costs.
Citation: Tak HJ, Ruhnke GW, Meltzer DO. Association of patient preferences for participation in decision making with length of stay and costs among hospitalized patients. JAMA Intern Med. 2013;173(13):1195-1205. doi: 10.1001/jamainternmed.2013.6048.
Early Parenteral Nutrition in Critically Ill Adults Does Not Significantly Affect Mortality or Infection Rates
Clinical question: Does providing early parenteral nutrition to critically ill adults with short-term relative contraindications to early enteral nutrition affect outcomes?
Background: The appropriate use of parenteral nutrition in critically ill adults is controversial. A systematic review found that critically ill patients randomized to receive early parenteral nutrition had significantly lower mortality but increased infection rates compared with standard care. A large-scale randomized trial was necessary to confirm the results.
Study design: Multicenter, randomized, single-blinded, controlled trial.
Setting: ICUs in 31 tertiary-care and community hospitals in Australia and New Zealand.
Synopsis: Researchers randomized 1,372 critically ill adults with relative contraindications to early enteral nutrition upon admission to the ICU to receive early parenteral nutrition or standard care. Early parenteral nutrition was started an average of 44 minutes after randomization. Clinicians defined standard care, with most patients remaining unfed for 2.8 days after randomization. Results were analyzed by intention-to-treat analysis, and loss to follow-up was 1%.
There was no significant difference in the primary outcome of 60-day mortality. Early parenteral nutrition patients received significantly fewer days of invasive ventilation, but did not have shorter ICU or hospital stays. Early parenteral nutrition patients experienced significantly less muscle-wasting and fat loss. There was no significant difference in new infection rates.
Bottom line: Early parenteral nutrition in critically ill adults resulted in significantly fewer days of invasive mechanical ventilation but did not cause a significant difference in length of stay, infection rates, or 60-day mortality.
Citation: Doig GS, Simpson F, Sweetman EA, et al. Early parenteral nutrition in critically ill patients with short-term relative contraindications to early enteral nutrition. JAMA. 2013;309(20): 2130-2138.
Aggressive Fluid and Sodium Restriction in Acute Decompensated Heart Failure Did Not Improve Outcomes
Clinical question: Does aggressive fluid and sodium restriction in acute decompensated heart failure (ADHF) result in increased weight loss, improved clinical stability, or decreased 30-day readmission rate?
Background: Fluid and sodium restriction are standard nonpharmacologic measures used in the management of ADHF in hospitalized patients, despite an absence of data to support their efficacy.
Study design: Randomized, controlled clinical trial with blinded outcome assessments.
Setting: A public teaching hospital in Brazil.
Synopsis: Seventy-five patients hospitalized with ADHF were randomized to receive aggressive fluid (800 mL/day) and sodium restriction (800 mg/day) or liberal intake (at least 2.5 L/day fluid, 3 to 5 g/day sodium). There were no significant between-group differences in diuretic administration. The primary outcomes of weight loss and clinical stability at three days were not significantly different between the groups. The heart-failure-specific readmission rate at 30 days was not significantly different between the groups. The aggressive restriction group had significantly worse thirst.
The study is limited by the small fraction of patients enrolled (9.2% of 813 screened) and homogenous population. Additional confirmatory trials likely are needed to change the standard of care, but this study demonstrated that aggressive fluid and sodium restriction does not benefit hospitalized patients with ADHF.
Bottom line: Aggressive fluid and sodium restriction in hospitalized patients with ADHF does not result in improved short-term weight loss, clinical stability, or decreased 30-day readmission rate, but it does cause significantly worse thirst.
Citation: Aliti GB, Rabelo ER, Clausell N, et al. Aggressive fluid and sodium restriction in acute decompensated heart failure. JAMA Intern Med. 2013;173(12):1058-1064.
Lower Rate of Pacemaker, Defibrillator Device-Pocket Hematoma without Anticoagulation Interruption
Clinical question: Is it safer to place a pacemaker or implantable cardioverter-defibrillator (ICD) while on therapeutic warfarin versus bridging with heparin/low-molecular-weight heparin (LMWH)?
Background: Current guidelines recommend bridging with heparin or LMWH for patients at high risk for thromboembolic events around the time of pacemaker or ICD placement, but it is associated with significant risk of device-pocket hematoma. Some centers place pacemakers and ICDs without interruption of warfarin. However, there are limited data to support the safety of this approach.
Study design: Multicenter, single-blinded, randomized, controlled trial.
Setting: Seventeen centers in Canada and one center in Brazil.
Synopsis: Patients with a predicted annual risk of 5% of thromboembolism were randomized to continue anticoagulation with warfarin (median INR 2.3) or to bridge therapy with heparin or LMWH; they then evaluated the incidence of clinically significant hematoma requiring prolonged hospitalization, interruption of anticoagulation therapy, or further surgical intervention. After reviewing the data on 668 patients, the Data and Safety Monitoring Board recommended termination of the study given a significantly lower rate of device-pocket hematoma in the warfarin group (3.5%) compared with the bridge group (16%) with RR 0.19 (95% CI 0.10-0.36, P<0.001). Otherwise, major surgical and thromboembolic complications were rare and not significantly different in both groups.
Bottom line: Continued warfarin therapy was associated with significantly reduced incidence of device-pocket hematoma compared with bridge with heparin or LMWH.
Citation: Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. N Engl J Med. 2013;368(22):2084-2093.
Prophylactic Penicillin Decreased Risk of Recurrent Leg Cellulitis
Clinical question: Does prophylactic, low-dose penicillin prevent recurrent cellulitis in patients with a history of two or more episodes of cellulitis?
Background: Some guidelines recommend prophylactic antibiotics for recurrent leg cellulitis, but there is no large randomized trial to support this practice, and clinical opinion is mixed.
Study design: Double-blinded, randomized, controlled trial.
Setting: Twenty-eight hospitals in the United Kingdom and Ireland.
Synopsis: Researchers randomized 274 patients with recurrent episodes of leg cellulitis (at least two episodes within the previous three years) to low-dose penicillin (250 mg) or placebo for 12 months and followed them for more than three years. During the prophylactic period, the penicillin group had a 45% reduction in the risk of a repeat cellulitis as compared to placebo (22% vs. 37%), equivalent to a number needed to treat to prevent a first recurrent cellulitis of five. The number of repeat episodes of cellulitis was lower overall in penicillin compared with the placebo group (119 vs. 164, P=0.02), although no significant difference was noted during the three-year follow-up period.
Factors associated with prophylaxis failure included three or more previous episodes of cellulitis, body mass index of 33 kg/m² or higher, and the presence of edema. No significant difference in adverse events was noted between the groups. Complete follow-up data was not available for participants during the follow-up period. Further study is needed to assess the long-term adverse effects and the duration of prophylaxis needed.
Bottom line: Prophylactic penicillin was effective in preventing recurrent leg cellulitis without increasing adverse effects, but its protective effect gradually declined once discontinued.
Citation: Thomas KS, Crook AM, Nunn AJ, et al. Penicillin to prevent recurrent leg cellulitis. N Engl J Med. 2013;368(18):1695-1703.
Universal ICU Decolonization Reduced Rates of MRSA Clinical Isolates and Bloodstream Infection
Clinical question: What is the most effective decolonization strategy for reducing methicillin-resistant Staphylococcus aureus (MRSA) and other pathogens in ICUs?
Background: Studies have shown that daily chlorhexidine bathing of all patients in ICUs reduced MRSA acquisition and bloodstream infection from all pathogens. However, this universal strategy has not been compared to MRSA screening and contact precautions alone, or to targeted decolonization of MRSA carriers.
Study design: Cluster-randomized comparative-effectiveness trial.
Setting: Adult ICUs in 43 Hospital Corporation of America (HCA) hospitals in 16 states.
Synopsis: All adult ICUs in a given hospital were randomized to one of three infection prevention strategies: Group 1 continued MRSA screening and isolation; Group 2 performed screening, isolation, and decolonization of MRSA carriers; and Group 3 implemented universal decolonization with intranasal mupirocin and daily bathing with chlorhexidine-impregnated cloths but no screening.
Forty-three hospitals, including 74 ICUs and 74,256 patients, underwent randomization. Significant reductions in the primary outcome of ICU-attributable MRSA clinical isolates (excluding MRSA screening tests) and the secondary outcome of bloodstream infection due to any pathogen were demonstrated across the three groups. One bloodstream infection was prevented for every 54 patients who underwent decolonization. Formal cost-effectiveness analysis was not performed.
Bottom line: In the ICU, universal decolonization was more effective than screening and isolation or targeted decolonization in the reduction of clinical MRSA isolates and bloodstream infection due to any pathogen, although monitoring for emerging resistance is necessary.
Citation: Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255-2265.
Intensive Blood-Pressure Lowering in Intracerebral Hemorrhage Did Not Reduce Death or Severe Disability
Clinical question: What is the efficacy and safety of early intensive blood-pressure lowering in patients with acute intracerebral hemorrhage?
Background: After intracerebral hemorrhage, blood pressure often becomes elevated and is a predictor of outcome. It is not known whether rapid lowering of blood pressure would improve outcome.
Study design: International, multicenter, prospective, randomized, open-treatment, blinded end-point trial.
Setting: One hundred forty-four hospitals in 21 countries.
Synopsis: Researchers randomly assigned 2,839 patients with intracerebral hemorrhage in the previous six hours to intensive blood-pressure lowering with target systolic blood pressure of <140 mmHg within one hour, or guideline-recommended treatment with target systolic blood pressure of <180 mmHg. The mean systolic blood pressure achieved was 150 mmHg in the intensive-treatment group and 164 mmHg in the standard-treatment group.
There was no significant difference between the two groups in the primary outcome of death or major disability. A pre-specified ordinal analysis of modified Rankin score (score of 0 indicates no symptoms; a score of 5 indicates severe disability) did show significantly lower modified Rankin scores with intensive treatment. There was no difference between the two groups in the rate of serious adverse events.
Bottom line: Early intensive blood-pressure lowering in patients with acute intracerebral hemorrhage did not reduce death or major disability, although there may be improved functional outcomes with intensive blood-pressure lowering.
Citation: Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368(25):2355-2365.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Perioperative SSRI use associated with adverse surgical outcomes
- Copper-surfaced rooms reduce health-care-acquired infections
- Glucocorticoid therapy for five days not inferior to 14 days for COPD exacerbation
- Patient preference for participation in medical decision-making may be associated with increased resource utilization
- Early parenteral nutrition in critically ill adults does not significantly affect mortality or infection rates
- Aggressive fluid and sodium restriction in acute decompensated heart failure did not improve outcomes
- Lower rate of pacemaker, defibrillator device-pocket hematoma without anticoagulation interruption
- Prophylactic penicillin decreased risk of recurrent leg cellulitis
- Universal ICU decolonization reduced rates of mrsa clinical isolates and bloodstream infection
- Intensive blood-pressure lowering in intracerebral hemorrhage did not reduce death or severe disability
Perioperative SSRI Use Associated with Adverse Surgical Outcomes
Clinical question: Does selective serotonin reuptake inhibitor (SSRI) use during hospitalization for surgery increase the risk of adverse perioperative outcomes?
Background: SSRIs commonly are prescribed but are associated with a small but higher risk for hemorrhage, arrhythmia, and sudden death. Single-site studies have described an association between SSRIs and adverse perioperative outcomes, but larger studies utilizing a broad range of surgical cases are lacking.
Study design: Retrospective cohort study.
Setting: Three hundred hospitals concentrated in the Southern U.S.
Synopsis: Using the “Perspective” database, this study examined 530,416 patients age >18 years undergoing major elective surgery, 72,540 (13.7%) of whom received an SSRI. Regression analysis showed patients receiving an SSRI had higher odds of mortality (OR 1.2, 95% CI [1.07-1.36]), higher odds of 30-day readmission (OR 1.22 [1.18-1.26]), and higher odds for bleeding (1.09 [1.04-1.15]). When the analysis was restricted to only patients with a diagnosis of depression, a higher risk of bleeding and readmission persisted.
This study reaffirms an association but does not establish a causal relationship between SSRI use and adverse perioperative outcomes. SSRI use may be a surrogate for other factors, including more severe mood disorders, poorer functional status, or chronic pain. Additionally, no information has been provided as to optimal duration of withholding SSRIs preoperatively. As such, it may be premature for hospitalists involved in perioperative care to modify recommendations based on this study.
Bottom line: Perioperative SSRI use is associated with an increased risk of bleeding and 30-day readmission.
Citation: Auerbach AD, Vittinghoff E, Maselli J, et al. Perioperative use of selective serotonin reuptake inhibitors and risks for adverse outcomes of surgery. JAMA Intern Med. 2013;173(12):1075-1081.
Copper-Surfaced Rooms Reduce Health-Care-Acquired Infections
Clinical question: Can copper alloy surfaces in ICU rooms lower rates of health-care-acquired infections (HAIs)?
Background: Environmental contamination is a potential source of HAIs. Copper has intrinsic broad-spectrum antimicrobial properties. This study tests the efficacy copper-surfaced items in hospital rooms have in preventing HAIs.
Study design: Randomized controlled trial.
Setting: Medical ICUs at Medical University of South Carolina and Ralph H. Johnson Veterans Affairs Medical Center in Charleston, and the Memorial Sloan Kettering Cancer Center in New York City.
Synopsis: Six hundred fifty ICU patients were randomized to receive care either in rooms with copper surfacing on commonly handled patient care objects or in traditional rooms. Patients were screened for methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) on admission. The proportion of patients that developed either an HAI and/or MRSA or VRE colonization was significantly lower among patients in rooms with the copper-surfaced items (0.071 vs. 0.128; P=0.02). The rate of HAIs alone was also lower in the rooms with the copper (0.034 vs. 0.081; P=0.013).
A potential limitation to this study is that the rooms with copper items appeared different than traditional rooms, and therefore might have changed the behavior of health-care workers. Further, it is unclear how much copper surfacing would be necessary on general wards, where patients are more mobile. Still, HAIs are associated with longer lengths of stay and higher 30-day readmission rates, so these encouraging results warrant additional investigation into antimicrobial copper-alloy surfaces.
Bottom line: Copper-surfaced objects reduce HAI rates in ICU patients.
Citation: Salgado CD, Sepkowitz, KA, John JF, et al. Copper surfaces reduce the rate of healthcare-acquired infections in the intensive care unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
Glucocorticoid Therapy for Five Days Not Inferior to 14 Days for COPD Exacerbation
Clinical question: Do short-course glucocorticoids work as well as conventional long courses for COPD exacerbation?
Background: International guidelines advocate a seven- to 14-day treatment course with glucocorticoids for COPD exacerbation, but the optimal duration of treatment is not known, and there are potential risks associated with glucocorticoid exposure.
Study design: Randomized, noninferiority, multicenter trial.
Setting: Five Swiss teaching hospitals.
Synopsis: Three hundred fourteen patients presenting to the ED with acute COPD exacerbation and without a history of asthma were randomized to receive treatment with 40 mg prednisone daily for either five or 14 days in a placebo-controlled, double-blinded fashion. There was no significant difference in the primary endpoint of re-exacerbation within six months. Patients in the five-day glucocorticoid group compared with the 14-day group were exposed to significantly less glucocorticoid.
Bottom line: Treatment for five days with glucocorticoids was not inferior to 14 days for acute COPD exacerbations with regard to re-exacerbations within six months and resulted in less glucocorticoid exposure overall.
Citation: Leuppi JF, Schuetz P, Bingisser R, et al. Short-term vs. conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE Randomized Clinical Trial. JAMA. 2013;390(21):2223-2231.
Patient Preference for Participation in Medical Decision-Making May Be Associated with Increased Resource Utilization
Clinical question: Do patient preferences for participation in medical decision-making affect health-care utilization?
Background: Patient participation in medical decision-making has been associated with improved patient satisfaction and health outcomes. There is little evidence to support theories that patient preferences might decrease or increase health-care utilization.
Study design: Survey study in academic research setting.
Setting: University of Chicago Medical Center.
Synopsis: More than 21,700 patients admitted to a general internal-medicine service completed a survey that included questions regarding preferences about receiving medical information and participation in medical decision-making. Survey data were linked with administrative data, including length of stay and total hospitalization costs.
Most patients (96.3%) expressed interest in receiving information about their illness and treatment options, but the majority of patients (71.1%) also expressed a preference to leave medical decision-making to their physician. Patients who preferred to participate in medical decision-making had significantly longer hospital LOS and higher total hospitalization cost.
Bottom line: Participation in medical decision-making significantly increased LOS and total costs.
Citation: Tak HJ, Ruhnke GW, Meltzer DO. Association of patient preferences for participation in decision making with length of stay and costs among hospitalized patients. JAMA Intern Med. 2013;173(13):1195-1205. doi: 10.1001/jamainternmed.2013.6048.
Early Parenteral Nutrition in Critically Ill Adults Does Not Significantly Affect Mortality or Infection Rates
Clinical question: Does providing early parenteral nutrition to critically ill adults with short-term relative contraindications to early enteral nutrition affect outcomes?
Background: The appropriate use of parenteral nutrition in critically ill adults is controversial. A systematic review found that critically ill patients randomized to receive early parenteral nutrition had significantly lower mortality but increased infection rates compared with standard care. A large-scale randomized trial was necessary to confirm the results.
Study design: Multicenter, randomized, single-blinded, controlled trial.
Setting: ICUs in 31 tertiary-care and community hospitals in Australia and New Zealand.
Synopsis: Researchers randomized 1,372 critically ill adults with relative contraindications to early enteral nutrition upon admission to the ICU to receive early parenteral nutrition or standard care. Early parenteral nutrition was started an average of 44 minutes after randomization. Clinicians defined standard care, with most patients remaining unfed for 2.8 days after randomization. Results were analyzed by intention-to-treat analysis, and loss to follow-up was 1%.
There was no significant difference in the primary outcome of 60-day mortality. Early parenteral nutrition patients received significantly fewer days of invasive ventilation, but did not have shorter ICU or hospital stays. Early parenteral nutrition patients experienced significantly less muscle-wasting and fat loss. There was no significant difference in new infection rates.
Bottom line: Early parenteral nutrition in critically ill adults resulted in significantly fewer days of invasive mechanical ventilation but did not cause a significant difference in length of stay, infection rates, or 60-day mortality.
Citation: Doig GS, Simpson F, Sweetman EA, et al. Early parenteral nutrition in critically ill patients with short-term relative contraindications to early enteral nutrition. JAMA. 2013;309(20): 2130-2138.
Aggressive Fluid and Sodium Restriction in Acute Decompensated Heart Failure Did Not Improve Outcomes
Clinical question: Does aggressive fluid and sodium restriction in acute decompensated heart failure (ADHF) result in increased weight loss, improved clinical stability, or decreased 30-day readmission rate?
Background: Fluid and sodium restriction are standard nonpharmacologic measures used in the management of ADHF in hospitalized patients, despite an absence of data to support their efficacy.
Study design: Randomized, controlled clinical trial with blinded outcome assessments.
Setting: A public teaching hospital in Brazil.
Synopsis: Seventy-five patients hospitalized with ADHF were randomized to receive aggressive fluid (800 mL/day) and sodium restriction (800 mg/day) or liberal intake (at least 2.5 L/day fluid, 3 to 5 g/day sodium). There were no significant between-group differences in diuretic administration. The primary outcomes of weight loss and clinical stability at three days were not significantly different between the groups. The heart-failure-specific readmission rate at 30 days was not significantly different between the groups. The aggressive restriction group had significantly worse thirst.
The study is limited by the small fraction of patients enrolled (9.2% of 813 screened) and homogenous population. Additional confirmatory trials likely are needed to change the standard of care, but this study demonstrated that aggressive fluid and sodium restriction does not benefit hospitalized patients with ADHF.
Bottom line: Aggressive fluid and sodium restriction in hospitalized patients with ADHF does not result in improved short-term weight loss, clinical stability, or decreased 30-day readmission rate, but it does cause significantly worse thirst.
Citation: Aliti GB, Rabelo ER, Clausell N, et al. Aggressive fluid and sodium restriction in acute decompensated heart failure. JAMA Intern Med. 2013;173(12):1058-1064.
Lower Rate of Pacemaker, Defibrillator Device-Pocket Hematoma without Anticoagulation Interruption
Clinical question: Is it safer to place a pacemaker or implantable cardioverter-defibrillator (ICD) while on therapeutic warfarin versus bridging with heparin/low-molecular-weight heparin (LMWH)?
Background: Current guidelines recommend bridging with heparin or LMWH for patients at high risk for thromboembolic events around the time of pacemaker or ICD placement, but it is associated with significant risk of device-pocket hematoma. Some centers place pacemakers and ICDs without interruption of warfarin. However, there are limited data to support the safety of this approach.
Study design: Multicenter, single-blinded, randomized, controlled trial.
Setting: Seventeen centers in Canada and one center in Brazil.
Synopsis: Patients with a predicted annual risk of 5% of thromboembolism were randomized to continue anticoagulation with warfarin (median INR 2.3) or to bridge therapy with heparin or LMWH; they then evaluated the incidence of clinically significant hematoma requiring prolonged hospitalization, interruption of anticoagulation therapy, or further surgical intervention. After reviewing the data on 668 patients, the Data and Safety Monitoring Board recommended termination of the study given a significantly lower rate of device-pocket hematoma in the warfarin group (3.5%) compared with the bridge group (16%) with RR 0.19 (95% CI 0.10-0.36, P<0.001). Otherwise, major surgical and thromboembolic complications were rare and not significantly different in both groups.
Bottom line: Continued warfarin therapy was associated with significantly reduced incidence of device-pocket hematoma compared with bridge with heparin or LMWH.
Citation: Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. N Engl J Med. 2013;368(22):2084-2093.
Prophylactic Penicillin Decreased Risk of Recurrent Leg Cellulitis
Clinical question: Does prophylactic, low-dose penicillin prevent recurrent cellulitis in patients with a history of two or more episodes of cellulitis?
Background: Some guidelines recommend prophylactic antibiotics for recurrent leg cellulitis, but there is no large randomized trial to support this practice, and clinical opinion is mixed.
Study design: Double-blinded, randomized, controlled trial.
Setting: Twenty-eight hospitals in the United Kingdom and Ireland.
Synopsis: Researchers randomized 274 patients with recurrent episodes of leg cellulitis (at least two episodes within the previous three years) to low-dose penicillin (250 mg) or placebo for 12 months and followed them for more than three years. During the prophylactic period, the penicillin group had a 45% reduction in the risk of a repeat cellulitis as compared to placebo (22% vs. 37%), equivalent to a number needed to treat to prevent a first recurrent cellulitis of five. The number of repeat episodes of cellulitis was lower overall in penicillin compared with the placebo group (119 vs. 164, P=0.02), although no significant difference was noted during the three-year follow-up period.
Factors associated with prophylaxis failure included three or more previous episodes of cellulitis, body mass index of 33 kg/m² or higher, and the presence of edema. No significant difference in adverse events was noted between the groups. Complete follow-up data was not available for participants during the follow-up period. Further study is needed to assess the long-term adverse effects and the duration of prophylaxis needed.
Bottom line: Prophylactic penicillin was effective in preventing recurrent leg cellulitis without increasing adverse effects, but its protective effect gradually declined once discontinued.
Citation: Thomas KS, Crook AM, Nunn AJ, et al. Penicillin to prevent recurrent leg cellulitis. N Engl J Med. 2013;368(18):1695-1703.
Universal ICU Decolonization Reduced Rates of MRSA Clinical Isolates and Bloodstream Infection
Clinical question: What is the most effective decolonization strategy for reducing methicillin-resistant Staphylococcus aureus (MRSA) and other pathogens in ICUs?
Background: Studies have shown that daily chlorhexidine bathing of all patients in ICUs reduced MRSA acquisition and bloodstream infection from all pathogens. However, this universal strategy has not been compared to MRSA screening and contact precautions alone, or to targeted decolonization of MRSA carriers.
Study design: Cluster-randomized comparative-effectiveness trial.
Setting: Adult ICUs in 43 Hospital Corporation of America (HCA) hospitals in 16 states.
Synopsis: All adult ICUs in a given hospital were randomized to one of three infection prevention strategies: Group 1 continued MRSA screening and isolation; Group 2 performed screening, isolation, and decolonization of MRSA carriers; and Group 3 implemented universal decolonization with intranasal mupirocin and daily bathing with chlorhexidine-impregnated cloths but no screening.
Forty-three hospitals, including 74 ICUs and 74,256 patients, underwent randomization. Significant reductions in the primary outcome of ICU-attributable MRSA clinical isolates (excluding MRSA screening tests) and the secondary outcome of bloodstream infection due to any pathogen were demonstrated across the three groups. One bloodstream infection was prevented for every 54 patients who underwent decolonization. Formal cost-effectiveness analysis was not performed.
Bottom line: In the ICU, universal decolonization was more effective than screening and isolation or targeted decolonization in the reduction of clinical MRSA isolates and bloodstream infection due to any pathogen, although monitoring for emerging resistance is necessary.
Citation: Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255-2265.
Intensive Blood-Pressure Lowering in Intracerebral Hemorrhage Did Not Reduce Death or Severe Disability
Clinical question: What is the efficacy and safety of early intensive blood-pressure lowering in patients with acute intracerebral hemorrhage?
Background: After intracerebral hemorrhage, blood pressure often becomes elevated and is a predictor of outcome. It is not known whether rapid lowering of blood pressure would improve outcome.
Study design: International, multicenter, prospective, randomized, open-treatment, blinded end-point trial.
Setting: One hundred forty-four hospitals in 21 countries.
Synopsis: Researchers randomly assigned 2,839 patients with intracerebral hemorrhage in the previous six hours to intensive blood-pressure lowering with target systolic blood pressure of <140 mmHg within one hour, or guideline-recommended treatment with target systolic blood pressure of <180 mmHg. The mean systolic blood pressure achieved was 150 mmHg in the intensive-treatment group and 164 mmHg in the standard-treatment group.
There was no significant difference between the two groups in the primary outcome of death or major disability. A pre-specified ordinal analysis of modified Rankin score (score of 0 indicates no symptoms; a score of 5 indicates severe disability) did show significantly lower modified Rankin scores with intensive treatment. There was no difference between the two groups in the rate of serious adverse events.
Bottom line: Early intensive blood-pressure lowering in patients with acute intracerebral hemorrhage did not reduce death or major disability, although there may be improved functional outcomes with intensive blood-pressure lowering.
Citation: Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368(25):2355-2365.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Perioperative SSRI use associated with adverse surgical outcomes
- Copper-surfaced rooms reduce health-care-acquired infections
- Glucocorticoid therapy for five days not inferior to 14 days for COPD exacerbation
- Patient preference for participation in medical decision-making may be associated with increased resource utilization
- Early parenteral nutrition in critically ill adults does not significantly affect mortality or infection rates
- Aggressive fluid and sodium restriction in acute decompensated heart failure did not improve outcomes
- Lower rate of pacemaker, defibrillator device-pocket hematoma without anticoagulation interruption
- Prophylactic penicillin decreased risk of recurrent leg cellulitis
- Universal ICU decolonization reduced rates of mrsa clinical isolates and bloodstream infection
- Intensive blood-pressure lowering in intracerebral hemorrhage did not reduce death or severe disability
Perioperative SSRI Use Associated with Adverse Surgical Outcomes
Clinical question: Does selective serotonin reuptake inhibitor (SSRI) use during hospitalization for surgery increase the risk of adverse perioperative outcomes?
Background: SSRIs commonly are prescribed but are associated with a small but higher risk for hemorrhage, arrhythmia, and sudden death. Single-site studies have described an association between SSRIs and adverse perioperative outcomes, but larger studies utilizing a broad range of surgical cases are lacking.
Study design: Retrospective cohort study.
Setting: Three hundred hospitals concentrated in the Southern U.S.
Synopsis: Using the “Perspective” database, this study examined 530,416 patients age >18 years undergoing major elective surgery, 72,540 (13.7%) of whom received an SSRI. Regression analysis showed patients receiving an SSRI had higher odds of mortality (OR 1.2, 95% CI [1.07-1.36]), higher odds of 30-day readmission (OR 1.22 [1.18-1.26]), and higher odds for bleeding (1.09 [1.04-1.15]). When the analysis was restricted to only patients with a diagnosis of depression, a higher risk of bleeding and readmission persisted.
This study reaffirms an association but does not establish a causal relationship between SSRI use and adverse perioperative outcomes. SSRI use may be a surrogate for other factors, including more severe mood disorders, poorer functional status, or chronic pain. Additionally, no information has been provided as to optimal duration of withholding SSRIs preoperatively. As such, it may be premature for hospitalists involved in perioperative care to modify recommendations based on this study.
Bottom line: Perioperative SSRI use is associated with an increased risk of bleeding and 30-day readmission.
Citation: Auerbach AD, Vittinghoff E, Maselli J, et al. Perioperative use of selective serotonin reuptake inhibitors and risks for adverse outcomes of surgery. JAMA Intern Med. 2013;173(12):1075-1081.
Copper-Surfaced Rooms Reduce Health-Care-Acquired Infections
Clinical question: Can copper alloy surfaces in ICU rooms lower rates of health-care-acquired infections (HAIs)?
Background: Environmental contamination is a potential source of HAIs. Copper has intrinsic broad-spectrum antimicrobial properties. This study tests the efficacy copper-surfaced items in hospital rooms have in preventing HAIs.
Study design: Randomized controlled trial.
Setting: Medical ICUs at Medical University of South Carolina and Ralph H. Johnson Veterans Affairs Medical Center in Charleston, and the Memorial Sloan Kettering Cancer Center in New York City.
Synopsis: Six hundred fifty ICU patients were randomized to receive care either in rooms with copper surfacing on commonly handled patient care objects or in traditional rooms. Patients were screened for methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) on admission. The proportion of patients that developed either an HAI and/or MRSA or VRE colonization was significantly lower among patients in rooms with the copper-surfaced items (0.071 vs. 0.128; P=0.02). The rate of HAIs alone was also lower in the rooms with the copper (0.034 vs. 0.081; P=0.013).
A potential limitation to this study is that the rooms with copper items appeared different than traditional rooms, and therefore might have changed the behavior of health-care workers. Further, it is unclear how much copper surfacing would be necessary on general wards, where patients are more mobile. Still, HAIs are associated with longer lengths of stay and higher 30-day readmission rates, so these encouraging results warrant additional investigation into antimicrobial copper-alloy surfaces.
Bottom line: Copper-surfaced objects reduce HAI rates in ICU patients.
Citation: Salgado CD, Sepkowitz, KA, John JF, et al. Copper surfaces reduce the rate of healthcare-acquired infections in the intensive care unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
Glucocorticoid Therapy for Five Days Not Inferior to 14 Days for COPD Exacerbation
Clinical question: Do short-course glucocorticoids work as well as conventional long courses for COPD exacerbation?
Background: International guidelines advocate a seven- to 14-day treatment course with glucocorticoids for COPD exacerbation, but the optimal duration of treatment is not known, and there are potential risks associated with glucocorticoid exposure.
Study design: Randomized, noninferiority, multicenter trial.
Setting: Five Swiss teaching hospitals.
Synopsis: Three hundred fourteen patients presenting to the ED with acute COPD exacerbation and without a history of asthma were randomized to receive treatment with 40 mg prednisone daily for either five or 14 days in a placebo-controlled, double-blinded fashion. There was no significant difference in the primary endpoint of re-exacerbation within six months. Patients in the five-day glucocorticoid group compared with the 14-day group were exposed to significantly less glucocorticoid.
Bottom line: Treatment for five days with glucocorticoids was not inferior to 14 days for acute COPD exacerbations with regard to re-exacerbations within six months and resulted in less glucocorticoid exposure overall.
Citation: Leuppi JF, Schuetz P, Bingisser R, et al. Short-term vs. conventional glucocorticoid therapy in acute exacerbations of chronic obstructive pulmonary disease: the REDUCE Randomized Clinical Trial. JAMA. 2013;390(21):2223-2231.
Patient Preference for Participation in Medical Decision-Making May Be Associated with Increased Resource Utilization
Clinical question: Do patient preferences for participation in medical decision-making affect health-care utilization?
Background: Patient participation in medical decision-making has been associated with improved patient satisfaction and health outcomes. There is little evidence to support theories that patient preferences might decrease or increase health-care utilization.
Study design: Survey study in academic research setting.
Setting: University of Chicago Medical Center.
Synopsis: More than 21,700 patients admitted to a general internal-medicine service completed a survey that included questions regarding preferences about receiving medical information and participation in medical decision-making. Survey data were linked with administrative data, including length of stay and total hospitalization costs.
Most patients (96.3%) expressed interest in receiving information about their illness and treatment options, but the majority of patients (71.1%) also expressed a preference to leave medical decision-making to their physician. Patients who preferred to participate in medical decision-making had significantly longer hospital LOS and higher total hospitalization cost.
Bottom line: Participation in medical decision-making significantly increased LOS and total costs.
Citation: Tak HJ, Ruhnke GW, Meltzer DO. Association of patient preferences for participation in decision making with length of stay and costs among hospitalized patients. JAMA Intern Med. 2013;173(13):1195-1205. doi: 10.1001/jamainternmed.2013.6048.
Early Parenteral Nutrition in Critically Ill Adults Does Not Significantly Affect Mortality or Infection Rates
Clinical question: Does providing early parenteral nutrition to critically ill adults with short-term relative contraindications to early enteral nutrition affect outcomes?
Background: The appropriate use of parenteral nutrition in critically ill adults is controversial. A systematic review found that critically ill patients randomized to receive early parenteral nutrition had significantly lower mortality but increased infection rates compared with standard care. A large-scale randomized trial was necessary to confirm the results.
Study design: Multicenter, randomized, single-blinded, controlled trial.
Setting: ICUs in 31 tertiary-care and community hospitals in Australia and New Zealand.
Synopsis: Researchers randomized 1,372 critically ill adults with relative contraindications to early enteral nutrition upon admission to the ICU to receive early parenteral nutrition or standard care. Early parenteral nutrition was started an average of 44 minutes after randomization. Clinicians defined standard care, with most patients remaining unfed for 2.8 days after randomization. Results were analyzed by intention-to-treat analysis, and loss to follow-up was 1%.
There was no significant difference in the primary outcome of 60-day mortality. Early parenteral nutrition patients received significantly fewer days of invasive ventilation, but did not have shorter ICU or hospital stays. Early parenteral nutrition patients experienced significantly less muscle-wasting and fat loss. There was no significant difference in new infection rates.
Bottom line: Early parenteral nutrition in critically ill adults resulted in significantly fewer days of invasive mechanical ventilation but did not cause a significant difference in length of stay, infection rates, or 60-day mortality.
Citation: Doig GS, Simpson F, Sweetman EA, et al. Early parenteral nutrition in critically ill patients with short-term relative contraindications to early enteral nutrition. JAMA. 2013;309(20): 2130-2138.
Aggressive Fluid and Sodium Restriction in Acute Decompensated Heart Failure Did Not Improve Outcomes
Clinical question: Does aggressive fluid and sodium restriction in acute decompensated heart failure (ADHF) result in increased weight loss, improved clinical stability, or decreased 30-day readmission rate?
Background: Fluid and sodium restriction are standard nonpharmacologic measures used in the management of ADHF in hospitalized patients, despite an absence of data to support their efficacy.
Study design: Randomized, controlled clinical trial with blinded outcome assessments.
Setting: A public teaching hospital in Brazil.
Synopsis: Seventy-five patients hospitalized with ADHF were randomized to receive aggressive fluid (800 mL/day) and sodium restriction (800 mg/day) or liberal intake (at least 2.5 L/day fluid, 3 to 5 g/day sodium). There were no significant between-group differences in diuretic administration. The primary outcomes of weight loss and clinical stability at three days were not significantly different between the groups. The heart-failure-specific readmission rate at 30 days was not significantly different between the groups. The aggressive restriction group had significantly worse thirst.
The study is limited by the small fraction of patients enrolled (9.2% of 813 screened) and homogenous population. Additional confirmatory trials likely are needed to change the standard of care, but this study demonstrated that aggressive fluid and sodium restriction does not benefit hospitalized patients with ADHF.
Bottom line: Aggressive fluid and sodium restriction in hospitalized patients with ADHF does not result in improved short-term weight loss, clinical stability, or decreased 30-day readmission rate, but it does cause significantly worse thirst.
Citation: Aliti GB, Rabelo ER, Clausell N, et al. Aggressive fluid and sodium restriction in acute decompensated heart failure. JAMA Intern Med. 2013;173(12):1058-1064.
Lower Rate of Pacemaker, Defibrillator Device-Pocket Hematoma without Anticoagulation Interruption
Clinical question: Is it safer to place a pacemaker or implantable cardioverter-defibrillator (ICD) while on therapeutic warfarin versus bridging with heparin/low-molecular-weight heparin (LMWH)?
Background: Current guidelines recommend bridging with heparin or LMWH for patients at high risk for thromboembolic events around the time of pacemaker or ICD placement, but it is associated with significant risk of device-pocket hematoma. Some centers place pacemakers and ICDs without interruption of warfarin. However, there are limited data to support the safety of this approach.
Study design: Multicenter, single-blinded, randomized, controlled trial.
Setting: Seventeen centers in Canada and one center in Brazil.
Synopsis: Patients with a predicted annual risk of 5% of thromboembolism were randomized to continue anticoagulation with warfarin (median INR 2.3) or to bridge therapy with heparin or LMWH; they then evaluated the incidence of clinically significant hematoma requiring prolonged hospitalization, interruption of anticoagulation therapy, or further surgical intervention. After reviewing the data on 668 patients, the Data and Safety Monitoring Board recommended termination of the study given a significantly lower rate of device-pocket hematoma in the warfarin group (3.5%) compared with the bridge group (16%) with RR 0.19 (95% CI 0.10-0.36, P<0.001). Otherwise, major surgical and thromboembolic complications were rare and not significantly different in both groups.
Bottom line: Continued warfarin therapy was associated with significantly reduced incidence of device-pocket hematoma compared with bridge with heparin or LMWH.
Citation: Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. N Engl J Med. 2013;368(22):2084-2093.
Prophylactic Penicillin Decreased Risk of Recurrent Leg Cellulitis
Clinical question: Does prophylactic, low-dose penicillin prevent recurrent cellulitis in patients with a history of two or more episodes of cellulitis?
Background: Some guidelines recommend prophylactic antibiotics for recurrent leg cellulitis, but there is no large randomized trial to support this practice, and clinical opinion is mixed.
Study design: Double-blinded, randomized, controlled trial.
Setting: Twenty-eight hospitals in the United Kingdom and Ireland.
Synopsis: Researchers randomized 274 patients with recurrent episodes of leg cellulitis (at least two episodes within the previous three years) to low-dose penicillin (250 mg) or placebo for 12 months and followed them for more than three years. During the prophylactic period, the penicillin group had a 45% reduction in the risk of a repeat cellulitis as compared to placebo (22% vs. 37%), equivalent to a number needed to treat to prevent a first recurrent cellulitis of five. The number of repeat episodes of cellulitis was lower overall in penicillin compared with the placebo group (119 vs. 164, P=0.02), although no significant difference was noted during the three-year follow-up period.
Factors associated with prophylaxis failure included three or more previous episodes of cellulitis, body mass index of 33 kg/m² or higher, and the presence of edema. No significant difference in adverse events was noted between the groups. Complete follow-up data was not available for participants during the follow-up period. Further study is needed to assess the long-term adverse effects and the duration of prophylaxis needed.
Bottom line: Prophylactic penicillin was effective in preventing recurrent leg cellulitis without increasing adverse effects, but its protective effect gradually declined once discontinued.
Citation: Thomas KS, Crook AM, Nunn AJ, et al. Penicillin to prevent recurrent leg cellulitis. N Engl J Med. 2013;368(18):1695-1703.
Universal ICU Decolonization Reduced Rates of MRSA Clinical Isolates and Bloodstream Infection
Clinical question: What is the most effective decolonization strategy for reducing methicillin-resistant Staphylococcus aureus (MRSA) and other pathogens in ICUs?
Background: Studies have shown that daily chlorhexidine bathing of all patients in ICUs reduced MRSA acquisition and bloodstream infection from all pathogens. However, this universal strategy has not been compared to MRSA screening and contact precautions alone, or to targeted decolonization of MRSA carriers.
Study design: Cluster-randomized comparative-effectiveness trial.
Setting: Adult ICUs in 43 Hospital Corporation of America (HCA) hospitals in 16 states.
Synopsis: All adult ICUs in a given hospital were randomized to one of three infection prevention strategies: Group 1 continued MRSA screening and isolation; Group 2 performed screening, isolation, and decolonization of MRSA carriers; and Group 3 implemented universal decolonization with intranasal mupirocin and daily bathing with chlorhexidine-impregnated cloths but no screening.
Forty-three hospitals, including 74 ICUs and 74,256 patients, underwent randomization. Significant reductions in the primary outcome of ICU-attributable MRSA clinical isolates (excluding MRSA screening tests) and the secondary outcome of bloodstream infection due to any pathogen were demonstrated across the three groups. One bloodstream infection was prevented for every 54 patients who underwent decolonization. Formal cost-effectiveness analysis was not performed.
Bottom line: In the ICU, universal decolonization was more effective than screening and isolation or targeted decolonization in the reduction of clinical MRSA isolates and bloodstream infection due to any pathogen, although monitoring for emerging resistance is necessary.
Citation: Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255-2265.
Intensive Blood-Pressure Lowering in Intracerebral Hemorrhage Did Not Reduce Death or Severe Disability
Clinical question: What is the efficacy and safety of early intensive blood-pressure lowering in patients with acute intracerebral hemorrhage?
Background: After intracerebral hemorrhage, blood pressure often becomes elevated and is a predictor of outcome. It is not known whether rapid lowering of blood pressure would improve outcome.
Study design: International, multicenter, prospective, randomized, open-treatment, blinded end-point trial.
Setting: One hundred forty-four hospitals in 21 countries.
Synopsis: Researchers randomly assigned 2,839 patients with intracerebral hemorrhage in the previous six hours to intensive blood-pressure lowering with target systolic blood pressure of <140 mmHg within one hour, or guideline-recommended treatment with target systolic blood pressure of <180 mmHg. The mean systolic blood pressure achieved was 150 mmHg in the intensive-treatment group and 164 mmHg in the standard-treatment group.
There was no significant difference between the two groups in the primary outcome of death or major disability. A pre-specified ordinal analysis of modified Rankin score (score of 0 indicates no symptoms; a score of 5 indicates severe disability) did show significantly lower modified Rankin scores with intensive treatment. There was no difference between the two groups in the rate of serious adverse events.
Bottom line: Early intensive blood-pressure lowering in patients with acute intracerebral hemorrhage did not reduce death or major disability, although there may be improved functional outcomes with intensive blood-pressure lowering.
Citation: Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368(25):2355-2365.
What Are the Indications for a Blood Transfusion?

Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
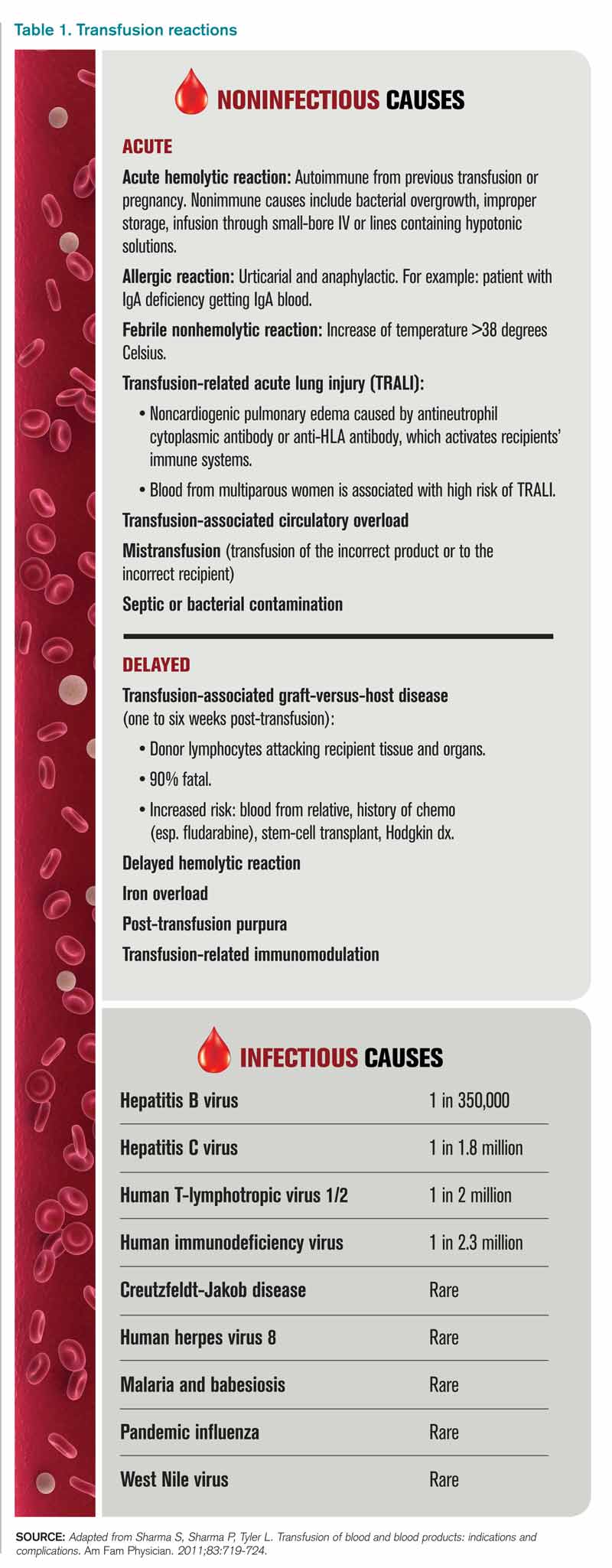
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
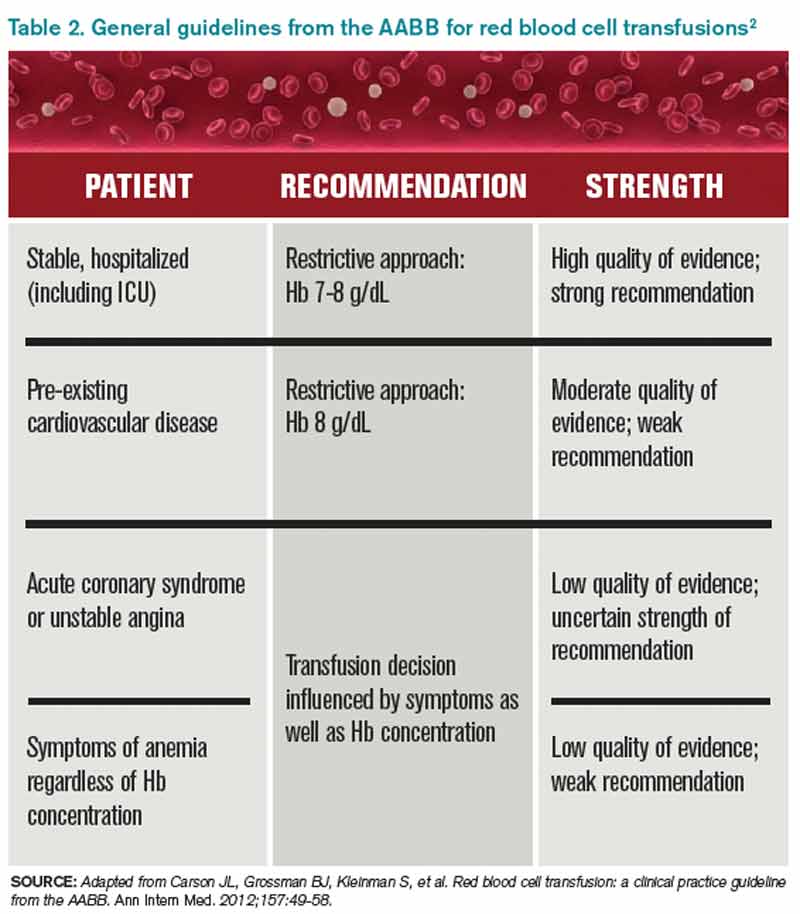
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Wasteful Practices in Hospital Cardiac Services Identified
A recent article in the American Journal of Medical Quality reviewed 366 cardiac-related medical studies and 21 practice guidelines to identify eight measures of potential waste in hospital cardiac services.4 The wasteful measures included excess use of higher-cost implantable cardioverter-defibrillators and similar cardiac devices, the use of dual-chamber defibrillators rather than single-chamber devices, and excess lengths of stay in the hospital. The eight measures were validated with data from 261 hospitals.
The authors emphasize that their set of measures is not designed to determine clinical appropriateness but to highlight areas of potential overutilization that can be benchmarked with other hospitals.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
A recent article in the American Journal of Medical Quality reviewed 366 cardiac-related medical studies and 21 practice guidelines to identify eight measures of potential waste in hospital cardiac services.4 The wasteful measures included excess use of higher-cost implantable cardioverter-defibrillators and similar cardiac devices, the use of dual-chamber defibrillators rather than single-chamber devices, and excess lengths of stay in the hospital. The eight measures were validated with data from 261 hospitals.
The authors emphasize that their set of measures is not designed to determine clinical appropriateness but to highlight areas of potential overutilization that can be benchmarked with other hospitals.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
A recent article in the American Journal of Medical Quality reviewed 366 cardiac-related medical studies and 21 practice guidelines to identify eight measures of potential waste in hospital cardiac services.4 The wasteful measures included excess use of higher-cost implantable cardioverter-defibrillators and similar cardiac devices, the use of dual-chamber defibrillators rather than single-chamber devices, and excess lengths of stay in the hospital. The eight measures were validated with data from 261 hospitals.
The authors emphasize that their set of measures is not designed to determine clinical appropriateness but to highlight areas of potential overutilization that can be benchmarked with other hospitals.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Applied Psychology Improves Hand Hygiene in Hospitals
According to a recent New York Times report, hand-hygiene compliance in hospitals can be as low as 30%, with serious implications regarding hospital-acquired infections.1 While many initiatives have employed secret observers, vibrating badges, or hand-washing coaches, a Research, Innovations, and Clinical Vignettes (RIV) poster at HM13 outlined how a multidisciplinary committee at University of Colorado Hospital in Aurora applied principles of psychology to the challenge of compliance.2
The initiative focused on behavioral changes: surreptitiously auditing staff behaviors, real-time feedback, and immediate public corrections for observed nonadherence on the test unit from an infection-control champion. The study randomly assigned daily auditing responsibilities across all members of the nursing staff, including aides. Taking a page from soccer referees, auditors handed out red tickets to hygiene violators—and individually wrapped Life Savers to reinforce adherence.
When unprofessional behavior is the response to a verbal correction, leadership has to be prepared to act, explains hospitalist and lead author Ethan Cumbler, MD, FACP.
“We need to stop thinking about hospital staff and physicians as rational actors when it comes to hand hygiene, but as social animals who will respond to positive and negative reinforcements and group culture,” he says.
Noncompliant hand hygiene is largely unconscious behavior that needs to be brought to conscious attention but is amenable to change, Dr. Cumbler says, adding that “unit leadership steps in for repeated nonadherence or an unprofessional response to correction. We have never needed to intervene more than once with the same person.”
Hand-hygiene adherence reached 97% on the pilot unit in the second quarter of 2012 and has remained at that level, Dr. Cumbler says. Additionally, iatrogenic infections dropped to zero from 4.8 per 1,000 urinary catheter days, with bloodstream infections falling at a similar rate.
Similar results with hand-hygiene compliance have been reported at St. Mary’s Health Center in St. Louis, which has been testing a system that reminds nurses to wash their hands at various checkpoints in the hospital, tracking their compliance with a badge that turns green when registering the presence of hand sanitizer, thereby informing patients that the nurse’s hands are clean.
The system, developed by Biovigil Hygiene Technologies of Ann Arbor, Mich., started on two pilot units last year, where compliance has grown to 97% and 99%, respectively. System set-up can cost about $2,000 per patient room, plus monthly subscriptions per employee, but more hospitals in the system could sign on next year, reports the St. Louis Post-Dispatch.3
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
According to a recent New York Times report, hand-hygiene compliance in hospitals can be as low as 30%, with serious implications regarding hospital-acquired infections.1 While many initiatives have employed secret observers, vibrating badges, or hand-washing coaches, a Research, Innovations, and Clinical Vignettes (RIV) poster at HM13 outlined how a multidisciplinary committee at University of Colorado Hospital in Aurora applied principles of psychology to the challenge of compliance.2
The initiative focused on behavioral changes: surreptitiously auditing staff behaviors, real-time feedback, and immediate public corrections for observed nonadherence on the test unit from an infection-control champion. The study randomly assigned daily auditing responsibilities across all members of the nursing staff, including aides. Taking a page from soccer referees, auditors handed out red tickets to hygiene violators—and individually wrapped Life Savers to reinforce adherence.
When unprofessional behavior is the response to a verbal correction, leadership has to be prepared to act, explains hospitalist and lead author Ethan Cumbler, MD, FACP.
“We need to stop thinking about hospital staff and physicians as rational actors when it comes to hand hygiene, but as social animals who will respond to positive and negative reinforcements and group culture,” he says.
Noncompliant hand hygiene is largely unconscious behavior that needs to be brought to conscious attention but is amenable to change, Dr. Cumbler says, adding that “unit leadership steps in for repeated nonadherence or an unprofessional response to correction. We have never needed to intervene more than once with the same person.”
Hand-hygiene adherence reached 97% on the pilot unit in the second quarter of 2012 and has remained at that level, Dr. Cumbler says. Additionally, iatrogenic infections dropped to zero from 4.8 per 1,000 urinary catheter days, with bloodstream infections falling at a similar rate.
Similar results with hand-hygiene compliance have been reported at St. Mary’s Health Center in St. Louis, which has been testing a system that reminds nurses to wash their hands at various checkpoints in the hospital, tracking their compliance with a badge that turns green when registering the presence of hand sanitizer, thereby informing patients that the nurse’s hands are clean.
The system, developed by Biovigil Hygiene Technologies of Ann Arbor, Mich., started on two pilot units last year, where compliance has grown to 97% and 99%, respectively. System set-up can cost about $2,000 per patient room, plus monthly subscriptions per employee, but more hospitals in the system could sign on next year, reports the St. Louis Post-Dispatch.3
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
According to a recent New York Times report, hand-hygiene compliance in hospitals can be as low as 30%, with serious implications regarding hospital-acquired infections.1 While many initiatives have employed secret observers, vibrating badges, or hand-washing coaches, a Research, Innovations, and Clinical Vignettes (RIV) poster at HM13 outlined how a multidisciplinary committee at University of Colorado Hospital in Aurora applied principles of psychology to the challenge of compliance.2
The initiative focused on behavioral changes: surreptitiously auditing staff behaviors, real-time feedback, and immediate public corrections for observed nonadherence on the test unit from an infection-control champion. The study randomly assigned daily auditing responsibilities across all members of the nursing staff, including aides. Taking a page from soccer referees, auditors handed out red tickets to hygiene violators—and individually wrapped Life Savers to reinforce adherence.
When unprofessional behavior is the response to a verbal correction, leadership has to be prepared to act, explains hospitalist and lead author Ethan Cumbler, MD, FACP.
“We need to stop thinking about hospital staff and physicians as rational actors when it comes to hand hygiene, but as social animals who will respond to positive and negative reinforcements and group culture,” he says.
Noncompliant hand hygiene is largely unconscious behavior that needs to be brought to conscious attention but is amenable to change, Dr. Cumbler says, adding that “unit leadership steps in for repeated nonadherence or an unprofessional response to correction. We have never needed to intervene more than once with the same person.”
Hand-hygiene adherence reached 97% on the pilot unit in the second quarter of 2012 and has remained at that level, Dr. Cumbler says. Additionally, iatrogenic infections dropped to zero from 4.8 per 1,000 urinary catheter days, with bloodstream infections falling at a similar rate.
Similar results with hand-hygiene compliance have been reported at St. Mary’s Health Center in St. Louis, which has been testing a system that reminds nurses to wash their hands at various checkpoints in the hospital, tracking their compliance with a badge that turns green when registering the presence of hand sanitizer, thereby informing patients that the nurse’s hands are clean.
The system, developed by Biovigil Hygiene Technologies of Ann Arbor, Mich., started on two pilot units last year, where compliance has grown to 97% and 99%, respectively. System set-up can cost about $2,000 per patient room, plus monthly subscriptions per employee, but more hospitals in the system could sign on next year, reports the St. Louis Post-Dispatch.3
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Intravenous Immunoglobulin Most Common Retreatment Approach for Refractory Kawasaki Disease

Clinical question: How is refractory Kawasaki disease (rKD) treated in the United States?
Background: Kawasaki disease (KD) is an immunologically mediated disease of primarily small to medium-sized arteries. It is the most common cause of acquired heart disease in children in the United States.
The current standard of care for KD treatment is a single 2 g/kg dose of intravenous immunoglobulin (IVIG), infused over 10 to 12 hours, accompanied by aspirin (80 to 100 mg/kg/day by mouth in four divided doses). Fevers persistent more than 36 hours after initial treatment represent refractory Kawasaki disease (rKD). There are no current national guidelines or standards for rKD treatment, although a 2004 joint statement from the American Academy of Pediatrics and the American Heart Association suggested a second dose of IVIG for rKD.
Study design: Multicenter, retrospective, cross-sectional study.
Setting: Forty freestanding children’s hospitals.
Synopsis: Researchers examined data obtained from the Pediatric Health Information System (PHIS), a clinical and financial database of care provided at 43 nonprofit, freestanding children’s hospitals in the United States. Data from 40 of these hospitals were deemed complete enough for analysis and were collected from Jan. 1, 2005, to June 30, 2009. Subjects were included if they received at least one dose of IVIG and had a principal diagnosis of KD. To be considered rKD, the subject must have received additional treatment after the initial diagnosis of rKD.
The most commonly used treatment after initial IVIG treatment was retreatment with IVIG (65%), followed by intravenous methylprednisolone (27%), then infliximab (8%). Significant regional variation was observed, with hospitals in the Northeast using methylprednisolone most frequently for rKD (55%). Infliximab was used at a much higher frequency in the West (29%) compared with other regions.
Bottom line: Retreatment with IVIG is the most common treatment for rKD, but significant regional variation exists, possibly due to the influence of regional experts.
Citation: Ghelani SJ, Pastor W, Parikh K. Demographic and treatment variability of refractory Kawasaki Disease: a multicenter analysis from 2005 to 2009. Hospital Pediatrics. 2012;2:71-76.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FAAP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: How is refractory Kawasaki disease (rKD) treated in the United States?
Background: Kawasaki disease (KD) is an immunologically mediated disease of primarily small to medium-sized arteries. It is the most common cause of acquired heart disease in children in the United States.
The current standard of care for KD treatment is a single 2 g/kg dose of intravenous immunoglobulin (IVIG), infused over 10 to 12 hours, accompanied by aspirin (80 to 100 mg/kg/day by mouth in four divided doses). Fevers persistent more than 36 hours after initial treatment represent refractory Kawasaki disease (rKD). There are no current national guidelines or standards for rKD treatment, although a 2004 joint statement from the American Academy of Pediatrics and the American Heart Association suggested a second dose of IVIG for rKD.
Study design: Multicenter, retrospective, cross-sectional study.
Setting: Forty freestanding children’s hospitals.
Synopsis: Researchers examined data obtained from the Pediatric Health Information System (PHIS), a clinical and financial database of care provided at 43 nonprofit, freestanding children’s hospitals in the United States. Data from 40 of these hospitals were deemed complete enough for analysis and were collected from Jan. 1, 2005, to June 30, 2009. Subjects were included if they received at least one dose of IVIG and had a principal diagnosis of KD. To be considered rKD, the subject must have received additional treatment after the initial diagnosis of rKD.
The most commonly used treatment after initial IVIG treatment was retreatment with IVIG (65%), followed by intravenous methylprednisolone (27%), then infliximab (8%). Significant regional variation was observed, with hospitals in the Northeast using methylprednisolone most frequently for rKD (55%). Infliximab was used at a much higher frequency in the West (29%) compared with other regions.
Bottom line: Retreatment with IVIG is the most common treatment for rKD, but significant regional variation exists, possibly due to the influence of regional experts.
Citation: Ghelani SJ, Pastor W, Parikh K. Demographic and treatment variability of refractory Kawasaki Disease: a multicenter analysis from 2005 to 2009. Hospital Pediatrics. 2012;2:71-76.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FAAP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Clinical question: How is refractory Kawasaki disease (rKD) treated in the United States?
Background: Kawasaki disease (KD) is an immunologically mediated disease of primarily small to medium-sized arteries. It is the most common cause of acquired heart disease in children in the United States.
The current standard of care for KD treatment is a single 2 g/kg dose of intravenous immunoglobulin (IVIG), infused over 10 to 12 hours, accompanied by aspirin (80 to 100 mg/kg/day by mouth in four divided doses). Fevers persistent more than 36 hours after initial treatment represent refractory Kawasaki disease (rKD). There are no current national guidelines or standards for rKD treatment, although a 2004 joint statement from the American Academy of Pediatrics and the American Heart Association suggested a second dose of IVIG for rKD.
Study design: Multicenter, retrospective, cross-sectional study.
Setting: Forty freestanding children’s hospitals.
Synopsis: Researchers examined data obtained from the Pediatric Health Information System (PHIS), a clinical and financial database of care provided at 43 nonprofit, freestanding children’s hospitals in the United States. Data from 40 of these hospitals were deemed complete enough for analysis and were collected from Jan. 1, 2005, to June 30, 2009. Subjects were included if they received at least one dose of IVIG and had a principal diagnosis of KD. To be considered rKD, the subject must have received additional treatment after the initial diagnosis of rKD.
The most commonly used treatment after initial IVIG treatment was retreatment with IVIG (65%), followed by intravenous methylprednisolone (27%), then infliximab (8%). Significant regional variation was observed, with hospitals in the Northeast using methylprednisolone most frequently for rKD (55%). Infliximab was used at a much higher frequency in the West (29%) compared with other regions.
Bottom line: Retreatment with IVIG is the most common treatment for rKD, but significant regional variation exists, possibly due to the influence of regional experts.
Citation: Ghelani SJ, Pastor W, Parikh K. Demographic and treatment variability of refractory Kawasaki Disease: a multicenter analysis from 2005 to 2009. Hospital Pediatrics. 2012;2:71-76.
Reviewed by Pediatric Editor Weijen Chang, MD, SFHM, FAAP, associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine, and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital.
Academic Hospitalist Academy Provides Resources for Success

SHM asked Academic Hospitalist Academy course co-directors Jeffrey Glasheen, MD, SFHM, and Bradley Sharpe, MD, SFHM, why academic hospitalists should attend this year’s academy.
Question: What has you personally excited about this year’s Academic Hospitalist Academy?
Dr. Sharpe: I’ll be honest—it is one of my favorite weeks of the year. It is a tremendous opportunity to engage with academic hospitalists and help them develop the core skills they need to be successful.
Dr. Glasheen: For me, it’s about the energy, the talent, and the excitement that the attendees bring to the course. It ends up being a tremendously energizing week for me personally. To see the talent in the room begin to find outlets for success is truly invigorating.
Q: If you were talking one on one with an academic hospitalist, what would you say to encourage them to attend?
Dr. Sharpe: Based on previous attendees, these four days could truly change your life. We are confident you will leave with newfound energy and enthusiasm and key building blocks to help you be successful when you go back home. Don’t miss it.
Dr. Glasheen: There is a magical transformation that happens every year. Very talented individuals enter the program. Nearly uniformly, they are struggling with the same issues around mentorship, sense of purpose, direction, and resources for success. They all want to be successful but sense there is something that is missing, and within the course of four days, they find it.
Q: What have you heard from previous AHA attendees?
Dr. Sharpe: Here are a couple of emails I received: “I can’t say enough about the AHA. It was possibly the most important 3 days of my young career. Thank you both for the knowledge and guidance.” “I have fond memories of the whole AHA conference. The great Jeff Wiese!!! But most of all, the small group sessions were extremely helpful.”
Dr. Glasheen: To a person, they all say the meeting is “transformational.” They gain skills in teaching, confidence in evaluating learners, methods for scholarly success, and a roadmap for navigating the tricky world on academic medicine. But beyond that, they gain a peer network. They leave tied in with 80 other national colleagues that are struggling with the same issues. This network becomes their home away from home—people they can turn to with a question, catch up with at a national meeting, and look to as exemplars in the field.
SHM asked Academic Hospitalist Academy course co-directors Jeffrey Glasheen, MD, SFHM, and Bradley Sharpe, MD, SFHM, why academic hospitalists should attend this year’s academy.
Question: What has you personally excited about this year’s Academic Hospitalist Academy?
Dr. Sharpe: I’ll be honest—it is one of my favorite weeks of the year. It is a tremendous opportunity to engage with academic hospitalists and help them develop the core skills they need to be successful.
Dr. Glasheen: For me, it’s about the energy, the talent, and the excitement that the attendees bring to the course. It ends up being a tremendously energizing week for me personally. To see the talent in the room begin to find outlets for success is truly invigorating.
Q: If you were talking one on one with an academic hospitalist, what would you say to encourage them to attend?
Dr. Sharpe: Based on previous attendees, these four days could truly change your life. We are confident you will leave with newfound energy and enthusiasm and key building blocks to help you be successful when you go back home. Don’t miss it.
Dr. Glasheen: There is a magical transformation that happens every year. Very talented individuals enter the program. Nearly uniformly, they are struggling with the same issues around mentorship, sense of purpose, direction, and resources for success. They all want to be successful but sense there is something that is missing, and within the course of four days, they find it.
Q: What have you heard from previous AHA attendees?
Dr. Sharpe: Here are a couple of emails I received: “I can’t say enough about the AHA. It was possibly the most important 3 days of my young career. Thank you both for the knowledge and guidance.” “I have fond memories of the whole AHA conference. The great Jeff Wiese!!! But most of all, the small group sessions were extremely helpful.”
Dr. Glasheen: To a person, they all say the meeting is “transformational.” They gain skills in teaching, confidence in evaluating learners, methods for scholarly success, and a roadmap for navigating the tricky world on academic medicine. But beyond that, they gain a peer network. They leave tied in with 80 other national colleagues that are struggling with the same issues. This network becomes their home away from home—people they can turn to with a question, catch up with at a national meeting, and look to as exemplars in the field.
SHM asked Academic Hospitalist Academy course co-directors Jeffrey Glasheen, MD, SFHM, and Bradley Sharpe, MD, SFHM, why academic hospitalists should attend this year’s academy.
Question: What has you personally excited about this year’s Academic Hospitalist Academy?
Dr. Sharpe: I’ll be honest—it is one of my favorite weeks of the year. It is a tremendous opportunity to engage with academic hospitalists and help them develop the core skills they need to be successful.
Dr. Glasheen: For me, it’s about the energy, the talent, and the excitement that the attendees bring to the course. It ends up being a tremendously energizing week for me personally. To see the talent in the room begin to find outlets for success is truly invigorating.
Q: If you were talking one on one with an academic hospitalist, what would you say to encourage them to attend?
Dr. Sharpe: Based on previous attendees, these four days could truly change your life. We are confident you will leave with newfound energy and enthusiasm and key building blocks to help you be successful when you go back home. Don’t miss it.
Dr. Glasheen: There is a magical transformation that happens every year. Very talented individuals enter the program. Nearly uniformly, they are struggling with the same issues around mentorship, sense of purpose, direction, and resources for success. They all want to be successful but sense there is something that is missing, and within the course of four days, they find it.
Q: What have you heard from previous AHA attendees?
Dr. Sharpe: Here are a couple of emails I received: “I can’t say enough about the AHA. It was possibly the most important 3 days of my young career. Thank you both for the knowledge and guidance.” “I have fond memories of the whole AHA conference. The great Jeff Wiese!!! But most of all, the small group sessions were extremely helpful.”
Dr. Glasheen: To a person, they all say the meeting is “transformational.” They gain skills in teaching, confidence in evaluating learners, methods for scholarly success, and a roadmap for navigating the tricky world on academic medicine. But beyond that, they gain a peer network. They leave tied in with 80 other national colleagues that are struggling with the same issues. This network becomes their home away from home—people they can turn to with a question, catch up with at a national meeting, and look to as exemplars in the field.