User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
FDA Updates Ambrisentan Label; Monthly Liver Enzyme Tests No Longer Required
The Food and Drug Administration on March 4 removed a warning pertaining to liver injury from the boxed warning on the ambrisentan label.
After a review of clinical trial data and postmarketing safety information, the FDA determined that ambrisentan (Letairis) presents only a small risk of liver injury and decided that monthly serum liver enzyme tests will no longer be required. The agency added that health care professionals should order liver enzyme tests if deemed clinically necessary. Ambrisentan is approved for the treatment of pulmonary arterial hypertension (PAH).
The boxed warning will continue to contain cautions about the use of ambrisentan during pregnancy. Preclinical studies showed that the drug can cause serious birth defects in animals. The drug will continue to be available only through a restricted distribution program called the Letairis Education and Access Program (LEAP).
In women of childbearing potential, the LEAP program requires evidence of a monthly pregnancy test before ambrisentan may be shipped.
Ambrisentan is an endothelin receptor antagonist. Endothelin is a naturally occurring substance that causes blood vessels to narrow, preventing normal blood flow in people with PAH. Ambrisentan has been shown to improve patients’ ability to exercise and to slow the progression of the disease.
The Food and Drug Administration on March 4 removed a warning pertaining to liver injury from the boxed warning on the ambrisentan label.
After a review of clinical trial data and postmarketing safety information, the FDA determined that ambrisentan (Letairis) presents only a small risk of liver injury and decided that monthly serum liver enzyme tests will no longer be required. The agency added that health care professionals should order liver enzyme tests if deemed clinically necessary. Ambrisentan is approved for the treatment of pulmonary arterial hypertension (PAH).
The boxed warning will continue to contain cautions about the use of ambrisentan during pregnancy. Preclinical studies showed that the drug can cause serious birth defects in animals. The drug will continue to be available only through a restricted distribution program called the Letairis Education and Access Program (LEAP).
In women of childbearing potential, the LEAP program requires evidence of a monthly pregnancy test before ambrisentan may be shipped.
Ambrisentan is an endothelin receptor antagonist. Endothelin is a naturally occurring substance that causes blood vessels to narrow, preventing normal blood flow in people with PAH. Ambrisentan has been shown to improve patients’ ability to exercise and to slow the progression of the disease.
The Food and Drug Administration on March 4 removed a warning pertaining to liver injury from the boxed warning on the ambrisentan label.
After a review of clinical trial data and postmarketing safety information, the FDA determined that ambrisentan (Letairis) presents only a small risk of liver injury and decided that monthly serum liver enzyme tests will no longer be required. The agency added that health care professionals should order liver enzyme tests if deemed clinically necessary. Ambrisentan is approved for the treatment of pulmonary arterial hypertension (PAH).
The boxed warning will continue to contain cautions about the use of ambrisentan during pregnancy. Preclinical studies showed that the drug can cause serious birth defects in animals. The drug will continue to be available only through a restricted distribution program called the Letairis Education and Access Program (LEAP).
In women of childbearing potential, the LEAP program requires evidence of a monthly pregnancy test before ambrisentan may be shipped.
Ambrisentan is an endothelin receptor antagonist. Endothelin is a naturally occurring substance that causes blood vessels to narrow, preventing normal blood flow in people with PAH. Ambrisentan has been shown to improve patients’ ability to exercise and to slow the progression of the disease.
FOOD AND DRUG ADMINISTRATION
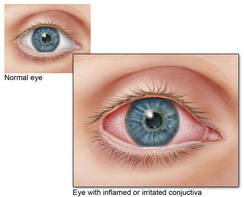
Sublingual Medication Efficacious for Allergic Rhinoconjunctivitis
KEYSTONE, COLO. – Daily sublingual immunotherapy for allergic rhinoconjunctivitis from grass pollens is well tolerated in North American adults, lending support for an alternative treatment modality in a patient population that has conventionally received subcutaneous medication, reported Dr. Harold S. Nelson and his coinvestigators.
Recently published results of a 439-patient randomized, phase III trial showed improved daily symptom and medication scores, compared with placebo, in adult patients using Merck’s Timothy grass (Phleum pratense) allergy immunotherapy tablet (AIT) during the 2009 pollen season, the researchers reported in a poster presentation at a meeting on allergy and respiratory diseases.
Improvements in total combined score (TCS) in patients aged 5-17 years who used the investigational AIT, compared with those who took placebo, were previously reported.
In all, 213 adults were randomized to the AIT (15 mcg of Phl p 5, a formulation of the Timothy grass allergen); the AIT group had a mean TCS score that was a significant 20% higher than the mean score in the placebo group (P = .005). The TCS score was the primary end point of the study and is a sum of the daily symptom score (DSS) and daily medication score (DMS) during the study period, said Dr. Nelson of National Jewish Health, Denver.
Secondary end points were the average DSS and average DMS during the study period, as well as the average weekly score for the Rhinoconjunctivitis Quality of Life Questionnaire. Similar higher scores for the AIT patients were seen in the secondary end points (J. Allergy Clin. Immunol. 2011;127:72-80).
Increases in specific IgE and IgE-blocking factors also were recorded in the AIT group. Levels of specific and blocking IgE were similar in both the AIT and placebo groups at baseline, but they increased in the AIT group over the 16-week treatment period. Levels were significantly increased during the peak and end phases of the season, Dr. Nelson reported at the meeting, which was sponsored by National Jewish Health.
Eleven patients in the AIT group and eight in the placebo group discontinued treatment as a result of adverse events. Adverse reactions were reported as transient in 73% of the AIT group and in 28% of the placebo group. No patients experienced anaphylactic shock.
The multicenter study was designed with a 2008 observational period preceding a dosing period prior to and during the 2009 grass pollen season. The patients had a mean age of 36 years, and most were white. Approximately 85% reported sensitivity to more than one grass pollen. Timothy grass crossreacts with a number of other grasses, including rye, sweet vernal, meadow fescue, bluegrass/june, orchard/cocksfoot, and redtop/bent/velvet.
Oral therapies for grass pollen allergy have been widely studied and used in Europe, but have been used more sporadically in North America. One long-term Danish study of grass AIT therapy in 257 patients supported evidence of a disease-modifying impact (J. Allergy Clin. Immunol. 2010;125:131-8).
In the United States and elsewhere, support for tablet-based medications has risen because of the safety concerns and inconveniences associated with injected immunotherapies.
Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
KEYSTONE, COLO. – Daily sublingual immunotherapy for allergic rhinoconjunctivitis from grass pollens is well tolerated in North American adults, lending support for an alternative treatment modality in a patient population that has conventionally received subcutaneous medication, reported Dr. Harold S. Nelson and his coinvestigators.
Recently published results of a 439-patient randomized, phase III trial showed improved daily symptom and medication scores, compared with placebo, in adult patients using Merck’s Timothy grass (Phleum pratense) allergy immunotherapy tablet (AIT) during the 2009 pollen season, the researchers reported in a poster presentation at a meeting on allergy and respiratory diseases.
Improvements in total combined score (TCS) in patients aged 5-17 years who used the investigational AIT, compared with those who took placebo, were previously reported.
In all, 213 adults were randomized to the AIT (15 mcg of Phl p 5, a formulation of the Timothy grass allergen); the AIT group had a mean TCS score that was a significant 20% higher than the mean score in the placebo group (P = .005). The TCS score was the primary end point of the study and is a sum of the daily symptom score (DSS) and daily medication score (DMS) during the study period, said Dr. Nelson of National Jewish Health, Denver.
Secondary end points were the average DSS and average DMS during the study period, as well as the average weekly score for the Rhinoconjunctivitis Quality of Life Questionnaire. Similar higher scores for the AIT patients were seen in the secondary end points (J. Allergy Clin. Immunol. 2011;127:72-80).
Increases in specific IgE and IgE-blocking factors also were recorded in the AIT group. Levels of specific and blocking IgE were similar in both the AIT and placebo groups at baseline, but they increased in the AIT group over the 16-week treatment period. Levels were significantly increased during the peak and end phases of the season, Dr. Nelson reported at the meeting, which was sponsored by National Jewish Health.
Eleven patients in the AIT group and eight in the placebo group discontinued treatment as a result of adverse events. Adverse reactions were reported as transient in 73% of the AIT group and in 28% of the placebo group. No patients experienced anaphylactic shock.
The multicenter study was designed with a 2008 observational period preceding a dosing period prior to and during the 2009 grass pollen season. The patients had a mean age of 36 years, and most were white. Approximately 85% reported sensitivity to more than one grass pollen. Timothy grass crossreacts with a number of other grasses, including rye, sweet vernal, meadow fescue, bluegrass/june, orchard/cocksfoot, and redtop/bent/velvet.
Oral therapies for grass pollen allergy have been widely studied and used in Europe, but have been used more sporadically in North America. One long-term Danish study of grass AIT therapy in 257 patients supported evidence of a disease-modifying impact (J. Allergy Clin. Immunol. 2010;125:131-8).
In the United States and elsewhere, support for tablet-based medications has risen because of the safety concerns and inconveniences associated with injected immunotherapies.
Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
KEYSTONE, COLO. – Daily sublingual immunotherapy for allergic rhinoconjunctivitis from grass pollens is well tolerated in North American adults, lending support for an alternative treatment modality in a patient population that has conventionally received subcutaneous medication, reported Dr. Harold S. Nelson and his coinvestigators.
Recently published results of a 439-patient randomized, phase III trial showed improved daily symptom and medication scores, compared with placebo, in adult patients using Merck’s Timothy grass (Phleum pratense) allergy immunotherapy tablet (AIT) during the 2009 pollen season, the researchers reported in a poster presentation at a meeting on allergy and respiratory diseases.
Improvements in total combined score (TCS) in patients aged 5-17 years who used the investigational AIT, compared with those who took placebo, were previously reported.
In all, 213 adults were randomized to the AIT (15 mcg of Phl p 5, a formulation of the Timothy grass allergen); the AIT group had a mean TCS score that was a significant 20% higher than the mean score in the placebo group (P = .005). The TCS score was the primary end point of the study and is a sum of the daily symptom score (DSS) and daily medication score (DMS) during the study period, said Dr. Nelson of National Jewish Health, Denver.
Secondary end points were the average DSS and average DMS during the study period, as well as the average weekly score for the Rhinoconjunctivitis Quality of Life Questionnaire. Similar higher scores for the AIT patients were seen in the secondary end points (J. Allergy Clin. Immunol. 2011;127:72-80).
Increases in specific IgE and IgE-blocking factors also were recorded in the AIT group. Levels of specific and blocking IgE were similar in both the AIT and placebo groups at baseline, but they increased in the AIT group over the 16-week treatment period. Levels were significantly increased during the peak and end phases of the season, Dr. Nelson reported at the meeting, which was sponsored by National Jewish Health.
Eleven patients in the AIT group and eight in the placebo group discontinued treatment as a result of adverse events. Adverse reactions were reported as transient in 73% of the AIT group and in 28% of the placebo group. No patients experienced anaphylactic shock.
The multicenter study was designed with a 2008 observational period preceding a dosing period prior to and during the 2009 grass pollen season. The patients had a mean age of 36 years, and most were white. Approximately 85% reported sensitivity to more than one grass pollen. Timothy grass crossreacts with a number of other grasses, including rye, sweet vernal, meadow fescue, bluegrass/june, orchard/cocksfoot, and redtop/bent/velvet.
Oral therapies for grass pollen allergy have been widely studied and used in Europe, but have been used more sporadically in North America. One long-term Danish study of grass AIT therapy in 257 patients supported evidence of a disease-modifying impact (J. Allergy Clin. Immunol. 2010;125:131-8).
In the United States and elsewhere, support for tablet-based medications has risen because of the safety concerns and inconveniences associated with injected immunotherapies.
Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
Major Finding: The total combined daily symptom and medication score was a significant 20% higher with oral immunotherapy, compared with placebo.
Data Source: Phase III, randomized, double-blind study of 439 patients.
Disclosures: Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
Sublingual Medication Efficacious for Allergic Rhinoconjunctivitis
KEYSTONE, COLO. – Daily sublingual immunotherapy for allergic rhinoconjunctivitis from grass pollens is well tolerated in North American adults, lending support for an alternative treatment modality in a patient population that has conventionally received subcutaneous medication, reported Dr. Harold S. Nelson and his coinvestigators.
Recently published results of a 439-patient randomized, phase III trial showed improved daily symptom and medication scores, compared with placebo, in adult patients using Merck’s Timothy grass (Phleum pratense) allergy immunotherapy tablet (AIT) during the 2009 pollen season, the researchers reported in a poster presentation at a meeting on allergy and respiratory diseases.
Improvements in total combined score (TCS) in patients aged 5-17 years who used the investigational AIT, compared with those who took placebo, were previously reported.
In all, 213 adults were randomized to the AIT (15 mcg of Phl p 5, a formulation of the Timothy grass allergen); the AIT group had a mean TCS score that was a significant 20% higher than the mean score in the placebo group (P = .005). The TCS score was the primary end point of the study and is a sum of the daily symptom score (DSS) and daily medication score (DMS) during the study period, said Dr. Nelson of National Jewish Health, Denver.
Secondary end points were the average DSS and average DMS during the study period, as well as the average weekly score for the Rhinoconjunctivitis Quality of Life Questionnaire. Similar higher scores for the AIT patients were seen in the secondary end points (J. Allergy Clin. Immunol. 2011;127:72-80).
Increases in specific IgE and IgE-blocking factors also were recorded in the AIT group. Levels of specific and blocking IgE were similar in both the AIT and placebo groups at baseline, but they increased in the AIT group over the 16-week treatment period. Levels were significantly increased during the peak and end phases of the season, Dr. Nelson reported at the meeting, which was sponsored by National Jewish Health.
Eleven patients in the AIT group and eight in the placebo group discontinued treatment as a result of adverse events. Adverse reactions were reported as transient in 73% of the AIT group and in 28% of the placebo group. No patients experienced anaphylactic shock.
The multicenter study was designed with a 2008 observational period preceding a dosing period prior to and during the 2009 grass pollen season. The patients had a mean age of 36 years, and most were white. Approximately 85% reported sensitivity to more than one grass pollen. Timothy grass crossreacts with a number of other grasses, including rye, sweet vernal, meadow fescue, bluegrass/june, orchard/cocksfoot, and redtop/bent/velvet.
Oral therapies for grass pollen allergy have been widely studied and used in Europe, but have been used more sporadically in North America. One long-term Danish study of grass AIT therapy in 257 patients supported evidence of a disease-modifying impact (J. Allergy Clin. Immunol. 2010;125:131-8).
In the United States and elsewhere, support for tablet-based medications has risen because of the safety concerns and inconveniences associated with injected immunotherapies.
Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
KEYSTONE, COLO. – Daily sublingual immunotherapy for allergic rhinoconjunctivitis from grass pollens is well tolerated in North American adults, lending support for an alternative treatment modality in a patient population that has conventionally received subcutaneous medication, reported Dr. Harold S. Nelson and his coinvestigators.
Recently published results of a 439-patient randomized, phase III trial showed improved daily symptom and medication scores, compared with placebo, in adult patients using Merck’s Timothy grass (Phleum pratense) allergy immunotherapy tablet (AIT) during the 2009 pollen season, the researchers reported in a poster presentation at a meeting on allergy and respiratory diseases.
Improvements in total combined score (TCS) in patients aged 5-17 years who used the investigational AIT, compared with those who took placebo, were previously reported.
In all, 213 adults were randomized to the AIT (15 mcg of Phl p 5, a formulation of the Timothy grass allergen); the AIT group had a mean TCS score that was a significant 20% higher than the mean score in the placebo group (P = .005). The TCS score was the primary end point of the study and is a sum of the daily symptom score (DSS) and daily medication score (DMS) during the study period, said Dr. Nelson of National Jewish Health, Denver.
Secondary end points were the average DSS and average DMS during the study period, as well as the average weekly score for the Rhinoconjunctivitis Quality of Life Questionnaire. Similar higher scores for the AIT patients were seen in the secondary end points (J. Allergy Clin. Immunol. 2011;127:72-80).
Increases in specific IgE and IgE-blocking factors also were recorded in the AIT group. Levels of specific and blocking IgE were similar in both the AIT and placebo groups at baseline, but they increased in the AIT group over the 16-week treatment period. Levels were significantly increased during the peak and end phases of the season, Dr. Nelson reported at the meeting, which was sponsored by National Jewish Health.
Eleven patients in the AIT group and eight in the placebo group discontinued treatment as a result of adverse events. Adverse reactions were reported as transient in 73% of the AIT group and in 28% of the placebo group. No patients experienced anaphylactic shock.
The multicenter study was designed with a 2008 observational period preceding a dosing period prior to and during the 2009 grass pollen season. The patients had a mean age of 36 years, and most were white. Approximately 85% reported sensitivity to more than one grass pollen. Timothy grass crossreacts with a number of other grasses, including rye, sweet vernal, meadow fescue, bluegrass/june, orchard/cocksfoot, and redtop/bent/velvet.
Oral therapies for grass pollen allergy have been widely studied and used in Europe, but have been used more sporadically in North America. One long-term Danish study of grass AIT therapy in 257 patients supported evidence of a disease-modifying impact (J. Allergy Clin. Immunol. 2010;125:131-8).
In the United States and elsewhere, support for tablet-based medications has risen because of the safety concerns and inconveniences associated with injected immunotherapies.
Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
KEYSTONE, COLO. – Daily sublingual immunotherapy for allergic rhinoconjunctivitis from grass pollens is well tolerated in North American adults, lending support for an alternative treatment modality in a patient population that has conventionally received subcutaneous medication, reported Dr. Harold S. Nelson and his coinvestigators.
Recently published results of a 439-patient randomized, phase III trial showed improved daily symptom and medication scores, compared with placebo, in adult patients using Merck’s Timothy grass (Phleum pratense) allergy immunotherapy tablet (AIT) during the 2009 pollen season, the researchers reported in a poster presentation at a meeting on allergy and respiratory diseases.
Improvements in total combined score (TCS) in patients aged 5-17 years who used the investigational AIT, compared with those who took placebo, were previously reported.
In all, 213 adults were randomized to the AIT (15 mcg of Phl p 5, a formulation of the Timothy grass allergen); the AIT group had a mean TCS score that was a significant 20% higher than the mean score in the placebo group (P = .005). The TCS score was the primary end point of the study and is a sum of the daily symptom score (DSS) and daily medication score (DMS) during the study period, said Dr. Nelson of National Jewish Health, Denver.
Secondary end points were the average DSS and average DMS during the study period, as well as the average weekly score for the Rhinoconjunctivitis Quality of Life Questionnaire. Similar higher scores for the AIT patients were seen in the secondary end points (J. Allergy Clin. Immunol. 2011;127:72-80).
Increases in specific IgE and IgE-blocking factors also were recorded in the AIT group. Levels of specific and blocking IgE were similar in both the AIT and placebo groups at baseline, but they increased in the AIT group over the 16-week treatment period. Levels were significantly increased during the peak and end phases of the season, Dr. Nelson reported at the meeting, which was sponsored by National Jewish Health.
Eleven patients in the AIT group and eight in the placebo group discontinued treatment as a result of adverse events. Adverse reactions were reported as transient in 73% of the AIT group and in 28% of the placebo group. No patients experienced anaphylactic shock.
The multicenter study was designed with a 2008 observational period preceding a dosing period prior to and during the 2009 grass pollen season. The patients had a mean age of 36 years, and most were white. Approximately 85% reported sensitivity to more than one grass pollen. Timothy grass crossreacts with a number of other grasses, including rye, sweet vernal, meadow fescue, bluegrass/june, orchard/cocksfoot, and redtop/bent/velvet.
Oral therapies for grass pollen allergy have been widely studied and used in Europe, but have been used more sporadically in North America. One long-term Danish study of grass AIT therapy in 257 patients supported evidence of a disease-modifying impact (J. Allergy Clin. Immunol. 2010;125:131-8).
In the United States and elsewhere, support for tablet-based medications has risen because of the safety concerns and inconveniences associated with injected immunotherapies.
Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
Major Finding: The total combined daily symptom and medication score was a significant 20% higher with oral immunotherapy, compared with placebo.
Data Source: Phase III, randomized, double-blind study of 439 patients.
Disclosures: Dr. Nelson and his coauthors reported current consultation and employment relationships, as well as prior advisory board or research support relationships, with study sponsor Merck.
Optimal Lung Resection Therapy Varies by Surgeon Specialty
SAN DIEGO – General surgeons perform the majority of lung resections for cancer in the United States, yet lung cancer resections performed by thoracic surgeons had significantly lower in-hospital mortality rates than did those performed by general surgeons and cardiac surgeons, according to results of a large analysis of national hospital data.
When performing a lung cancer resection, thoracic surgeons performed lymphadenectomy significantly more often than did general surgeons and cardiac surgeons.

"Lymph node status in lung cancer is the main determinant of stage, prognosis, and need for further therapy," Dr. Michelle Ellis said at the annual meeting of the Society of Thoracic Surgeons. "The performance of lymphadenectomy at the time of lung cancer resection can be considered a process measure of quality."
Previously published studies have demonstrated that general surgeons perform the majority of thoracic cases in the United States, while surgeons who specialize in thoracic surgery have lower perioperative morbidity and mortality. "Furthermore, patients who have their lung resection performed by a board-certified cardiothoracic surgeon specializing in general thoracic surgery have longer overall and cancer-specific survival," said Dr. Ellis of Oregon Health and Science University, Portland. "We hypothesized that the completeness of intraoperative oncologic staging at the time of primary lung cancer resection varies by surgeon specialty, and may explain the observed differences in outcome."
To test the hypothesis, Dr. Ellis, with the assistance of Dr. Paul H. Schipper and Dr. John T. Vetto, reviewed 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 who were treated surgically with limited lung resection, lobectomy, or pneumonectomy. The main outcome measure was the presence of lymphadenectomy or mediastinoscopy performed during the same admission.
The researchers divided the surgeons into three main groups based on their case mix of thoracic, cardiac, or other types of surgery. A thoracic surgeon was defined as someone who performed greater than 75% general thoracic surgery operations and less than 10% cardiac operations; a general surgeon was defined as someone who performed fewer than 75% thoracic operations and fewer than 10% cardiac operations, and a cardiac surgeon was defined as someone who performed greater than 10% cardiac operations.
Dr. Ellis reported that lung cancer resections were performed by general surgeons in 62% of cases, by cardiac surgeons in 35% of cases, and by thoracic surgeons in 3% of cases. The median annual case volume was 21 for thoracic surgeons, 23 for cardiac surgeons, and 8 for general surgeons.
In-hospital mortality rates for thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. This translated into an odds ratio for in-hospital mortality of 1.33 for cases performed by cardiac surgeons and 1.55 for those performed by general surgeons.
Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons). Thoracic surgeons also performed mediastinoscopy significantly more often (16% vs. 10% by cardiac surgeons and 11% by general surgeons).
Multivariate analysis revealed that patients were significantly less likely to undergo lymphadenectomy if they were in the lowest two quartiles of household income (odds ratio, 0.74); insured by Medicare (OR, 0.93); received their care at a rural hospital (OR, 0.60) or at an urban nonteaching hospital (OR, 0.74); or had their resection performed by a general surgeon (OR, 0.47) or by a cardiac surgeon (OR, 0.47).
"A patient was more than twice as likely to have a lymphadenectomy performed if the lung cancer resection was performed by a thoracic surgeon," Dr. Ellis said.
Next, the researchers assessed the impact of case volume on their multivariate model. They determined that for every doubling of thoracic surgery case volume, there was a significant increase in the likelihood that a lymphadenectomy would be performed (OR, 1.28). On the other hand, for every doubling of general surgery case volume, there was a significant decrease in lymphadenectomy rates (OR, 0.95). Doubling of cardiac surgery case volume did not affect lymphadenectomy rates.
"Lymphadenectomy rates for all surgeon groups did improve over the study period," Dr. Ellis said. "However, despite these improvements, cardiac and general surgeons still have lymphadenectomy rates significantly lower than [those of] cardiac surgeons. The next step is to ensure that all patients receive adequate staging of the mediastinum, possibly through disseminating knowledge, creating centers of excellence, or providing opportunities to learn the skills necessary to perform adequate lung cancer surgery."
She acknowledged certain limitations of the study, including the fact that it contains only single-admission information. "It also has limited cancer-specific data such as stage, and has no mechanism for long-term follow-up," she said. In addition, surgeons are anonymous in the database, so board certification could not be determined.
Dr. Ellis said that she had no relevant financial disclosures to make.
SAN DIEGO – General surgeons perform the majority of lung resections for cancer in the United States, yet lung cancer resections performed by thoracic surgeons had significantly lower in-hospital mortality rates than did those performed by general surgeons and cardiac surgeons, according to results of a large analysis of national hospital data.
When performing a lung cancer resection, thoracic surgeons performed lymphadenectomy significantly more often than did general surgeons and cardiac surgeons.
"Lymph node status in lung cancer is the main determinant of stage, prognosis, and need for further therapy," Dr. Michelle Ellis said at the annual meeting of the Society of Thoracic Surgeons. "The performance of lymphadenectomy at the time of lung cancer resection can be considered a process measure of quality."
Previously published studies have demonstrated that general surgeons perform the majority of thoracic cases in the United States, while surgeons who specialize in thoracic surgery have lower perioperative morbidity and mortality. "Furthermore, patients who have their lung resection performed by a board-certified cardiothoracic surgeon specializing in general thoracic surgery have longer overall and cancer-specific survival," said Dr. Ellis of Oregon Health and Science University, Portland. "We hypothesized that the completeness of intraoperative oncologic staging at the time of primary lung cancer resection varies by surgeon specialty, and may explain the observed differences in outcome."
To test the hypothesis, Dr. Ellis, with the assistance of Dr. Paul H. Schipper and Dr. John T. Vetto, reviewed 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 who were treated surgically with limited lung resection, lobectomy, or pneumonectomy. The main outcome measure was the presence of lymphadenectomy or mediastinoscopy performed during the same admission.
The researchers divided the surgeons into three main groups based on their case mix of thoracic, cardiac, or other types of surgery. A thoracic surgeon was defined as someone who performed greater than 75% general thoracic surgery operations and less than 10% cardiac operations; a general surgeon was defined as someone who performed fewer than 75% thoracic operations and fewer than 10% cardiac operations, and a cardiac surgeon was defined as someone who performed greater than 10% cardiac operations.
Dr. Ellis reported that lung cancer resections were performed by general surgeons in 62% of cases, by cardiac surgeons in 35% of cases, and by thoracic surgeons in 3% of cases. The median annual case volume was 21 for thoracic surgeons, 23 for cardiac surgeons, and 8 for general surgeons.
In-hospital mortality rates for thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. This translated into an odds ratio for in-hospital mortality of 1.33 for cases performed by cardiac surgeons and 1.55 for those performed by general surgeons.
Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons). Thoracic surgeons also performed mediastinoscopy significantly more often (16% vs. 10% by cardiac surgeons and 11% by general surgeons).
Multivariate analysis revealed that patients were significantly less likely to undergo lymphadenectomy if they were in the lowest two quartiles of household income (odds ratio, 0.74); insured by Medicare (OR, 0.93); received their care at a rural hospital (OR, 0.60) or at an urban nonteaching hospital (OR, 0.74); or had their resection performed by a general surgeon (OR, 0.47) or by a cardiac surgeon (OR, 0.47).
"A patient was more than twice as likely to have a lymphadenectomy performed if the lung cancer resection was performed by a thoracic surgeon," Dr. Ellis said.
Next, the researchers assessed the impact of case volume on their multivariate model. They determined that for every doubling of thoracic surgery case volume, there was a significant increase in the likelihood that a lymphadenectomy would be performed (OR, 1.28). On the other hand, for every doubling of general surgery case volume, there was a significant decrease in lymphadenectomy rates (OR, 0.95). Doubling of cardiac surgery case volume did not affect lymphadenectomy rates.
"Lymphadenectomy rates for all surgeon groups did improve over the study period," Dr. Ellis said. "However, despite these improvements, cardiac and general surgeons still have lymphadenectomy rates significantly lower than [those of] cardiac surgeons. The next step is to ensure that all patients receive adequate staging of the mediastinum, possibly through disseminating knowledge, creating centers of excellence, or providing opportunities to learn the skills necessary to perform adequate lung cancer surgery."
She acknowledged certain limitations of the study, including the fact that it contains only single-admission information. "It also has limited cancer-specific data such as stage, and has no mechanism for long-term follow-up," she said. In addition, surgeons are anonymous in the database, so board certification could not be determined.
Dr. Ellis said that she had no relevant financial disclosures to make.
SAN DIEGO – General surgeons perform the majority of lung resections for cancer in the United States, yet lung cancer resections performed by thoracic surgeons had significantly lower in-hospital mortality rates than did those performed by general surgeons and cardiac surgeons, according to results of a large analysis of national hospital data.
When performing a lung cancer resection, thoracic surgeons performed lymphadenectomy significantly more often than did general surgeons and cardiac surgeons.
"Lymph node status in lung cancer is the main determinant of stage, prognosis, and need for further therapy," Dr. Michelle Ellis said at the annual meeting of the Society of Thoracic Surgeons. "The performance of lymphadenectomy at the time of lung cancer resection can be considered a process measure of quality."
Previously published studies have demonstrated that general surgeons perform the majority of thoracic cases in the United States, while surgeons who specialize in thoracic surgery have lower perioperative morbidity and mortality. "Furthermore, patients who have their lung resection performed by a board-certified cardiothoracic surgeon specializing in general thoracic surgery have longer overall and cancer-specific survival," said Dr. Ellis of Oregon Health and Science University, Portland. "We hypothesized that the completeness of intraoperative oncologic staging at the time of primary lung cancer resection varies by surgeon specialty, and may explain the observed differences in outcome."
To test the hypothesis, Dr. Ellis, with the assistance of Dr. Paul H. Schipper and Dr. John T. Vetto, reviewed 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 who were treated surgically with limited lung resection, lobectomy, or pneumonectomy. The main outcome measure was the presence of lymphadenectomy or mediastinoscopy performed during the same admission.
The researchers divided the surgeons into three main groups based on their case mix of thoracic, cardiac, or other types of surgery. A thoracic surgeon was defined as someone who performed greater than 75% general thoracic surgery operations and less than 10% cardiac operations; a general surgeon was defined as someone who performed fewer than 75% thoracic operations and fewer than 10% cardiac operations, and a cardiac surgeon was defined as someone who performed greater than 10% cardiac operations.
Dr. Ellis reported that lung cancer resections were performed by general surgeons in 62% of cases, by cardiac surgeons in 35% of cases, and by thoracic surgeons in 3% of cases. The median annual case volume was 21 for thoracic surgeons, 23 for cardiac surgeons, and 8 for general surgeons.
In-hospital mortality rates for thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. This translated into an odds ratio for in-hospital mortality of 1.33 for cases performed by cardiac surgeons and 1.55 for those performed by general surgeons.
Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons). Thoracic surgeons also performed mediastinoscopy significantly more often (16% vs. 10% by cardiac surgeons and 11% by general surgeons).
Multivariate analysis revealed that patients were significantly less likely to undergo lymphadenectomy if they were in the lowest two quartiles of household income (odds ratio, 0.74); insured by Medicare (OR, 0.93); received their care at a rural hospital (OR, 0.60) or at an urban nonteaching hospital (OR, 0.74); or had their resection performed by a general surgeon (OR, 0.47) or by a cardiac surgeon (OR, 0.47).
"A patient was more than twice as likely to have a lymphadenectomy performed if the lung cancer resection was performed by a thoracic surgeon," Dr. Ellis said.
Next, the researchers assessed the impact of case volume on their multivariate model. They determined that for every doubling of thoracic surgery case volume, there was a significant increase in the likelihood that a lymphadenectomy would be performed (OR, 1.28). On the other hand, for every doubling of general surgery case volume, there was a significant decrease in lymphadenectomy rates (OR, 0.95). Doubling of cardiac surgery case volume did not affect lymphadenectomy rates.
"Lymphadenectomy rates for all surgeon groups did improve over the study period," Dr. Ellis said. "However, despite these improvements, cardiac and general surgeons still have lymphadenectomy rates significantly lower than [those of] cardiac surgeons. The next step is to ensure that all patients receive adequate staging of the mediastinum, possibly through disseminating knowledge, creating centers of excellence, or providing opportunities to learn the skills necessary to perform adequate lung cancer surgery."
She acknowledged certain limitations of the study, including the fact that it contains only single-admission information. "It also has limited cancer-specific data such as stage, and has no mechanism for long-term follow-up," she said. In addition, surgeons are anonymous in the database, so board certification could not be determined.
Dr. Ellis said that she had no relevant financial disclosures to make.
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: The in-hospital mortality rates for lung cancer resections performed by thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons).
Data Source: A review of 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 that were treated surgically.
Disclosures: Dr. Ellis said that she had no relevant financial conflicts to disclose.
Optimal Lung Resection Therapy Varies by Surgeon Specialty
SAN DIEGO – General surgeons perform the majority of lung resections for cancer in the United States, yet lung cancer resections performed by thoracic surgeons had significantly lower in-hospital mortality rates than did those performed by general surgeons and cardiac surgeons, according to results of a large analysis of national hospital data.
When performing a lung cancer resection, thoracic surgeons performed lymphadenectomy significantly more often than did general surgeons and cardiac surgeons.
"Lymph node status in lung cancer is the main determinant of stage, prognosis, and need for further therapy," Dr. Michelle Ellis said at the annual meeting of the Society of Thoracic Surgeons. "The performance of lymphadenectomy at the time of lung cancer resection can be considered a process measure of quality."
Previously published studies have demonstrated that general surgeons perform the majority of thoracic cases in the United States, while surgeons who specialize in thoracic surgery have lower perioperative morbidity and mortality. "Furthermore, patients who have their lung resection performed by a board-certified cardiothoracic surgeon specializing in general thoracic surgery have longer overall and cancer-specific survival," said Dr. Ellis of Oregon Health and Science University, Portland. "We hypothesized that the completeness of intraoperative oncologic staging at the time of primary lung cancer resection varies by surgeon specialty, and may explain the observed differences in outcome."
To test the hypothesis, Dr. Ellis, with the assistance of Dr. Paul H. Schipper and Dr. John T. Vetto, reviewed 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 who were treated surgically with limited lung resection, lobectomy, or pneumonectomy. The main outcome measure was the presence of lymphadenectomy or mediastinoscopy performed during the same admission.
The researchers divided the surgeons into three main groups based on their case mix of thoracic, cardiac, or other types of surgery. A thoracic surgeon was defined as someone who performed greater than 75% general thoracic surgery operations and less than 10% cardiac operations; a general surgeon was defined as someone who performed fewer than 75% thoracic operations and fewer than 10% cardiac operations, and a cardiac surgeon was defined as someone who performed greater than 10% cardiac operations.
Dr. Ellis reported that lung cancer resections were performed by general surgeons in 62% of cases, by cardiac surgeons in 35% of cases, and by thoracic surgeons in 3% of cases. The median annual case volume was 21 for thoracic surgeons, 23 for cardiac surgeons, and 8 for general surgeons.
In-hospital mortality rates for thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. This translated into an odds ratio for in-hospital mortality of 1.33 for cases performed by cardiac surgeons and 1.55 for those performed by general surgeons.
Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons). Thoracic surgeons also performed mediastinoscopy significantly more often (16% vs. 10% by cardiac surgeons and 11% by general surgeons).
Multivariate analysis revealed that patients were significantly less likely to undergo lymphadenectomy if they were in the lowest two quartiles of household income (odds ratio, 0.74); insured by Medicare (OR, 0.93); received their care at a rural hospital (OR, 0.60) or at an urban nonteaching hospital (OR, 0.74); or had their resection performed by a general surgeon (OR, 0.47) or by a cardiac surgeon (OR, 0.47).
"A patient was more than twice as likely to have a lymphadenectomy performed if the lung cancer resection was performed by a thoracic surgeon," Dr. Ellis said.
Next, the researchers assessed the impact of case volume on their multivariate model. They determined that for every doubling of thoracic surgery case volume, there was a significant increase in the likelihood that a lymphadenectomy would be performed (OR, 1.28). On the other hand, for every doubling of general surgery case volume, there was a significant decrease in lymphadenectomy rates (OR, 0.95). Doubling of cardiac surgery case volume did not affect lymphadenectomy rates.
"Lymphadenectomy rates for all surgeon groups did improve over the study period," Dr. Ellis said. "However, despite these improvements, cardiac and general surgeons still have lymphadenectomy rates significantly lower than [those of] cardiac surgeons. The next step is to ensure that all patients receive adequate staging of the mediastinum, possibly through disseminating knowledge, creating centers of excellence, or providing opportunities to learn the skills necessary to perform adequate lung cancer surgery."
She acknowledged certain limitations of the study, including the fact that it contains only single-admission information. "It also has limited cancer-specific data such as stage, and has no mechanism for long-term follow-up," she said. In addition, surgeons are anonymous in the database, so board certification could not be determined.
Dr. Ellis said that she had no relevant financial disclosures to make.
SAN DIEGO – General surgeons perform the majority of lung resections for cancer in the United States, yet lung cancer resections performed by thoracic surgeons had significantly lower in-hospital mortality rates than did those performed by general surgeons and cardiac surgeons, according to results of a large analysis of national hospital data.
When performing a lung cancer resection, thoracic surgeons performed lymphadenectomy significantly more often than did general surgeons and cardiac surgeons.
"Lymph node status in lung cancer is the main determinant of stage, prognosis, and need for further therapy," Dr. Michelle Ellis said at the annual meeting of the Society of Thoracic Surgeons. "The performance of lymphadenectomy at the time of lung cancer resection can be considered a process measure of quality."
Previously published studies have demonstrated that general surgeons perform the majority of thoracic cases in the United States, while surgeons who specialize in thoracic surgery have lower perioperative morbidity and mortality. "Furthermore, patients who have their lung resection performed by a board-certified cardiothoracic surgeon specializing in general thoracic surgery have longer overall and cancer-specific survival," said Dr. Ellis of Oregon Health and Science University, Portland. "We hypothesized that the completeness of intraoperative oncologic staging at the time of primary lung cancer resection varies by surgeon specialty, and may explain the observed differences in outcome."
To test the hypothesis, Dr. Ellis, with the assistance of Dr. Paul H. Schipper and Dr. John T. Vetto, reviewed 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 who were treated surgically with limited lung resection, lobectomy, or pneumonectomy. The main outcome measure was the presence of lymphadenectomy or mediastinoscopy performed during the same admission.
The researchers divided the surgeons into three main groups based on their case mix of thoracic, cardiac, or other types of surgery. A thoracic surgeon was defined as someone who performed greater than 75% general thoracic surgery operations and less than 10% cardiac operations; a general surgeon was defined as someone who performed fewer than 75% thoracic operations and fewer than 10% cardiac operations, and a cardiac surgeon was defined as someone who performed greater than 10% cardiac operations.
Dr. Ellis reported that lung cancer resections were performed by general surgeons in 62% of cases, by cardiac surgeons in 35% of cases, and by thoracic surgeons in 3% of cases. The median annual case volume was 21 for thoracic surgeons, 23 for cardiac surgeons, and 8 for general surgeons.
In-hospital mortality rates for thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. This translated into an odds ratio for in-hospital mortality of 1.33 for cases performed by cardiac surgeons and 1.55 for those performed by general surgeons.
Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons). Thoracic surgeons also performed mediastinoscopy significantly more often (16% vs. 10% by cardiac surgeons and 11% by general surgeons).
Multivariate analysis revealed that patients were significantly less likely to undergo lymphadenectomy if they were in the lowest two quartiles of household income (odds ratio, 0.74); insured by Medicare (OR, 0.93); received their care at a rural hospital (OR, 0.60) or at an urban nonteaching hospital (OR, 0.74); or had their resection performed by a general surgeon (OR, 0.47) or by a cardiac surgeon (OR, 0.47).
"A patient was more than twice as likely to have a lymphadenectomy performed if the lung cancer resection was performed by a thoracic surgeon," Dr. Ellis said.
Next, the researchers assessed the impact of case volume on their multivariate model. They determined that for every doubling of thoracic surgery case volume, there was a significant increase in the likelihood that a lymphadenectomy would be performed (OR, 1.28). On the other hand, for every doubling of general surgery case volume, there was a significant decrease in lymphadenectomy rates (OR, 0.95). Doubling of cardiac surgery case volume did not affect lymphadenectomy rates.
"Lymphadenectomy rates for all surgeon groups did improve over the study period," Dr. Ellis said. "However, despite these improvements, cardiac and general surgeons still have lymphadenectomy rates significantly lower than [those of] cardiac surgeons. The next step is to ensure that all patients receive adequate staging of the mediastinum, possibly through disseminating knowledge, creating centers of excellence, or providing opportunities to learn the skills necessary to perform adequate lung cancer surgery."
She acknowledged certain limitations of the study, including the fact that it contains only single-admission information. "It also has limited cancer-specific data such as stage, and has no mechanism for long-term follow-up," she said. In addition, surgeons are anonymous in the database, so board certification could not be determined.
Dr. Ellis said that she had no relevant financial disclosures to make.
SAN DIEGO – General surgeons perform the majority of lung resections for cancer in the United States, yet lung cancer resections performed by thoracic surgeons had significantly lower in-hospital mortality rates than did those performed by general surgeons and cardiac surgeons, according to results of a large analysis of national hospital data.
When performing a lung cancer resection, thoracic surgeons performed lymphadenectomy significantly more often than did general surgeons and cardiac surgeons.
"Lymph node status in lung cancer is the main determinant of stage, prognosis, and need for further therapy," Dr. Michelle Ellis said at the annual meeting of the Society of Thoracic Surgeons. "The performance of lymphadenectomy at the time of lung cancer resection can be considered a process measure of quality."
Previously published studies have demonstrated that general surgeons perform the majority of thoracic cases in the United States, while surgeons who specialize in thoracic surgery have lower perioperative morbidity and mortality. "Furthermore, patients who have their lung resection performed by a board-certified cardiothoracic surgeon specializing in general thoracic surgery have longer overall and cancer-specific survival," said Dr. Ellis of Oregon Health and Science University, Portland. "We hypothesized that the completeness of intraoperative oncologic staging at the time of primary lung cancer resection varies by surgeon specialty, and may explain the observed differences in outcome."
To test the hypothesis, Dr. Ellis, with the assistance of Dr. Paul H. Schipper and Dr. John T. Vetto, reviewed 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 who were treated surgically with limited lung resection, lobectomy, or pneumonectomy. The main outcome measure was the presence of lymphadenectomy or mediastinoscopy performed during the same admission.
The researchers divided the surgeons into three main groups based on their case mix of thoracic, cardiac, or other types of surgery. A thoracic surgeon was defined as someone who performed greater than 75% general thoracic surgery operations and less than 10% cardiac operations; a general surgeon was defined as someone who performed fewer than 75% thoracic operations and fewer than 10% cardiac operations, and a cardiac surgeon was defined as someone who performed greater than 10% cardiac operations.
Dr. Ellis reported that lung cancer resections were performed by general surgeons in 62% of cases, by cardiac surgeons in 35% of cases, and by thoracic surgeons in 3% of cases. The median annual case volume was 21 for thoracic surgeons, 23 for cardiac surgeons, and 8 for general surgeons.
In-hospital mortality rates for thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. This translated into an odds ratio for in-hospital mortality of 1.33 for cases performed by cardiac surgeons and 1.55 for those performed by general surgeons.
Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons). Thoracic surgeons also performed mediastinoscopy significantly more often (16% vs. 10% by cardiac surgeons and 11% by general surgeons).
Multivariate analysis revealed that patients were significantly less likely to undergo lymphadenectomy if they were in the lowest two quartiles of household income (odds ratio, 0.74); insured by Medicare (OR, 0.93); received their care at a rural hospital (OR, 0.60) or at an urban nonteaching hospital (OR, 0.74); or had their resection performed by a general surgeon (OR, 0.47) or by a cardiac surgeon (OR, 0.47).
"A patient was more than twice as likely to have a lymphadenectomy performed if the lung cancer resection was performed by a thoracic surgeon," Dr. Ellis said.
Next, the researchers assessed the impact of case volume on their multivariate model. They determined that for every doubling of thoracic surgery case volume, there was a significant increase in the likelihood that a lymphadenectomy would be performed (OR, 1.28). On the other hand, for every doubling of general surgery case volume, there was a significant decrease in lymphadenectomy rates (OR, 0.95). Doubling of cardiac surgery case volume did not affect lymphadenectomy rates.
"Lymphadenectomy rates for all surgeon groups did improve over the study period," Dr. Ellis said. "However, despite these improvements, cardiac and general surgeons still have lymphadenectomy rates significantly lower than [those of] cardiac surgeons. The next step is to ensure that all patients receive adequate staging of the mediastinum, possibly through disseminating knowledge, creating centers of excellence, or providing opportunities to learn the skills necessary to perform adequate lung cancer surgery."
She acknowledged certain limitations of the study, including the fact that it contains only single-admission information. "It also has limited cancer-specific data such as stage, and has no mechanism for long-term follow-up," she said. In addition, surgeons are anonymous in the database, so board certification could not be determined.
Dr. Ellis said that she had no relevant financial disclosures to make.
FROM THE ANNUAL MEETING OF THE SOCIETY OF THORACIC SURGEONS
Major Finding: The in-hospital mortality rates for lung cancer resections performed by thoracic, cardiac, and general surgeons were 2.3%, 3.4%, and 4.0%, respectively. Thoracic surgeons performed lymphadenectomy significantly more often than did their counterparts (73% vs. 55% for both cardiac and general surgeons).
Data Source: A review of 222,233 primary lung cancer cases from the Nationwide Inpatient Sample from 1998 to 2007 that were treated surgically.
Disclosures: Dr. Ellis said that she had no relevant financial conflicts to disclose.
FDA Cracks Down on Unapproved Prescription Cold, Cough, Allergy Drugs
Drug manufacturers have 90 days to stop making unapproved prescription medications to treat cold, cough, and allergy symptoms, officials at the Food and Drug Administration announced on March 2.
The FDA issued a list of about 500 unapproved prescription products that should be pulled from the market. These products were never evaluated by the FDA but continue to be prescribed. In many cases, they have been on the market for years, are listed in the Physicians’ Desk Reference, and are advertised in medical journals. Physicians may not be aware that the drugs were not approved, Deborah M. Autor, director of the Office of Compliance at the FDA’s Center for Drug Evaluation and Research, said during a press conference.
"This action is necessary to protect consumers from the potential risks posed by unapproved drugs because we don’t know what’s in them, whether they work properly, or how they are made," Ms. Autor said.
The FDA announcement is part of a broader crackdown on unapproved drugs that began in 2006. But Ms. Autor said that agency officials have particular concerns about these cold, cough, and allergy medications. For example, some of the drugs are labeled as time-release formulations, but without evaluation by the FDA, it’s unclear whether the drugs are delivering their active ingredients as labeled, Ms. Autor said. The active ingredient may be released too slowly, too quickly, or not at all, she said.
Ms. Autor said that the FDA is also concerned because some of the unapproved drugs are labeled for use in children younger than age 2 years. Some of the unapproved drugs also have names that are similar to the names of other drugs, which could lead to confusion when prescriptions are filled. And some of the drugs on the FDA’s list contain combinations of the same types of ingredients, such as two or more antihistamines, which can lead to oversedation.
If a company has registered its unapproved products with the FDA, it will have 90 days to stop manufacturing and 180 days to stop shipping all products. However, FDA officials said there are likely more unapproved prescription drugs that have never been registered with the agency. Those products must be pulled from the market immediately.
"We do not anticipate today’s action will have a major negative impact on consumers or health professionals because there are multiple other products available to treat cough, cold, and allergy symptoms, either as an FDA-approved prescription drug or an over-the-counter drug that follows appropriate FDA standards," Ms. Autor said. "We do anticipate that today’s action will have a significant positive impact by improving the safety of the American drug supply."
Drug manufacturers have 90 days to stop making unapproved prescription medications to treat cold, cough, and allergy symptoms, officials at the Food and Drug Administration announced on March 2.
The FDA issued a list of about 500 unapproved prescription products that should be pulled from the market. These products were never evaluated by the FDA but continue to be prescribed. In many cases, they have been on the market for years, are listed in the Physicians’ Desk Reference, and are advertised in medical journals. Physicians may not be aware that the drugs were not approved, Deborah M. Autor, director of the Office of Compliance at the FDA’s Center for Drug Evaluation and Research, said during a press conference.
"This action is necessary to protect consumers from the potential risks posed by unapproved drugs because we don’t know what’s in them, whether they work properly, or how they are made," Ms. Autor said.
The FDA announcement is part of a broader crackdown on unapproved drugs that began in 2006. But Ms. Autor said that agency officials have particular concerns about these cold, cough, and allergy medications. For example, some of the drugs are labeled as time-release formulations, but without evaluation by the FDA, it’s unclear whether the drugs are delivering their active ingredients as labeled, Ms. Autor said. The active ingredient may be released too slowly, too quickly, or not at all, she said.
Ms. Autor said that the FDA is also concerned because some of the unapproved drugs are labeled for use in children younger than age 2 years. Some of the unapproved drugs also have names that are similar to the names of other drugs, which could lead to confusion when prescriptions are filled. And some of the drugs on the FDA’s list contain combinations of the same types of ingredients, such as two or more antihistamines, which can lead to oversedation.
If a company has registered its unapproved products with the FDA, it will have 90 days to stop manufacturing and 180 days to stop shipping all products. However, FDA officials said there are likely more unapproved prescription drugs that have never been registered with the agency. Those products must be pulled from the market immediately.
"We do not anticipate today’s action will have a major negative impact on consumers or health professionals because there are multiple other products available to treat cough, cold, and allergy symptoms, either as an FDA-approved prescription drug or an over-the-counter drug that follows appropriate FDA standards," Ms. Autor said. "We do anticipate that today’s action will have a significant positive impact by improving the safety of the American drug supply."
Drug manufacturers have 90 days to stop making unapproved prescription medications to treat cold, cough, and allergy symptoms, officials at the Food and Drug Administration announced on March 2.
The FDA issued a list of about 500 unapproved prescription products that should be pulled from the market. These products were never evaluated by the FDA but continue to be prescribed. In many cases, they have been on the market for years, are listed in the Physicians’ Desk Reference, and are advertised in medical journals. Physicians may not be aware that the drugs were not approved, Deborah M. Autor, director of the Office of Compliance at the FDA’s Center for Drug Evaluation and Research, said during a press conference.
"This action is necessary to protect consumers from the potential risks posed by unapproved drugs because we don’t know what’s in them, whether they work properly, or how they are made," Ms. Autor said.
The FDA announcement is part of a broader crackdown on unapproved drugs that began in 2006. But Ms. Autor said that agency officials have particular concerns about these cold, cough, and allergy medications. For example, some of the drugs are labeled as time-release formulations, but without evaluation by the FDA, it’s unclear whether the drugs are delivering their active ingredients as labeled, Ms. Autor said. The active ingredient may be released too slowly, too quickly, or not at all, she said.
Ms. Autor said that the FDA is also concerned because some of the unapproved drugs are labeled for use in children younger than age 2 years. Some of the unapproved drugs also have names that are similar to the names of other drugs, which could lead to confusion when prescriptions are filled. And some of the drugs on the FDA’s list contain combinations of the same types of ingredients, such as two or more antihistamines, which can lead to oversedation.
If a company has registered its unapproved products with the FDA, it will have 90 days to stop manufacturing and 180 days to stop shipping all products. However, FDA officials said there are likely more unapproved prescription drugs that have never been registered with the agency. Those products must be pulled from the market immediately.
"We do not anticipate today’s action will have a major negative impact on consumers or health professionals because there are multiple other products available to treat cough, cold, and allergy symptoms, either as an FDA-approved prescription drug or an over-the-counter drug that follows appropriate FDA standards," Ms. Autor said. "We do anticipate that today’s action will have a significant positive impact by improving the safety of the American drug supply."
FROM THE FDA
FDA Cracks Down on Unapproved Prescription Cold, Cough, Allergy Drugs
Drug manufacturers have 90 days to stop making unapproved prescription medications to treat cold, cough, and allergy symptoms, officials at the Food and Drug Administration announced on March 2.
The FDA issued a list of about 500 unapproved prescription products that should be pulled from the market. These products were never evaluated by the FDA but continue to be prescribed. In many cases, they have been on the market for years, are listed in the Physicians’ Desk Reference, and are advertised in medical journals. Physicians may not be aware that the drugs were not approved, Deborah M. Autor, director of the Office of Compliance at the FDA’s Center for Drug Evaluation and Research, said during a press conference.
"This action is necessary to protect consumers from the potential risks posed by unapproved drugs because we don’t know what’s in them, whether they work properly, or how they are made," Ms. Autor said.
The FDA announcement is part of a broader crackdown on unapproved drugs that began in 2006. But Ms. Autor said that agency officials have particular concerns about these cold, cough, and allergy medications. For example, some of the drugs are labeled as time-release formulations, but without evaluation by the FDA, it’s unclear whether the drugs are delivering their active ingredients as labeled, Ms. Autor said. The active ingredient may be released too slowly, too quickly, or not at all, she said.
Ms. Autor said that the FDA is also concerned because some of the unapproved drugs are labeled for use in children younger than age 2 years. Some of the unapproved drugs also have names that are similar to the names of other drugs, which could lead to confusion when prescriptions are filled. And some of the drugs on the FDA’s list contain combinations of the same types of ingredients, such as two or more antihistamines, which can lead to oversedation.
If a company has registered its unapproved products with the FDA, it will have 90 days to stop manufacturing and 180 days to stop shipping all products. However, FDA officials said there are likely more unapproved prescription drugs that have never been registered with the agency. Those products must be pulled from the market immediately.
"We do not anticipate today’s action will have a major negative impact on consumers or health professionals because there are multiple other products available to treat cough, cold, and allergy symptoms, either as an FDA-approved prescription drug or an over-the-counter drug that follows appropriate FDA standards," Ms. Autor said. "We do anticipate that today’s action will have a significant positive impact by improving the safety of the American drug supply."
Drug manufacturers have 90 days to stop making unapproved prescription medications to treat cold, cough, and allergy symptoms, officials at the Food and Drug Administration announced on March 2.
The FDA issued a list of about 500 unapproved prescription products that should be pulled from the market. These products were never evaluated by the FDA but continue to be prescribed. In many cases, they have been on the market for years, are listed in the Physicians’ Desk Reference, and are advertised in medical journals. Physicians may not be aware that the drugs were not approved, Deborah M. Autor, director of the Office of Compliance at the FDA’s Center for Drug Evaluation and Research, said during a press conference.
"This action is necessary to protect consumers from the potential risks posed by unapproved drugs because we don’t know what’s in them, whether they work properly, or how they are made," Ms. Autor said.
The FDA announcement is part of a broader crackdown on unapproved drugs that began in 2006. But Ms. Autor said that agency officials have particular concerns about these cold, cough, and allergy medications. For example, some of the drugs are labeled as time-release formulations, but without evaluation by the FDA, it’s unclear whether the drugs are delivering their active ingredients as labeled, Ms. Autor said. The active ingredient may be released too slowly, too quickly, or not at all, she said.
Ms. Autor said that the FDA is also concerned because some of the unapproved drugs are labeled for use in children younger than age 2 years. Some of the unapproved drugs also have names that are similar to the names of other drugs, which could lead to confusion when prescriptions are filled. And some of the drugs on the FDA’s list contain combinations of the same types of ingredients, such as two or more antihistamines, which can lead to oversedation.
If a company has registered its unapproved products with the FDA, it will have 90 days to stop manufacturing and 180 days to stop shipping all products. However, FDA officials said there are likely more unapproved prescription drugs that have never been registered with the agency. Those products must be pulled from the market immediately.
"We do not anticipate today’s action will have a major negative impact on consumers or health professionals because there are multiple other products available to treat cough, cold, and allergy symptoms, either as an FDA-approved prescription drug or an over-the-counter drug that follows appropriate FDA standards," Ms. Autor said. "We do anticipate that today’s action will have a significant positive impact by improving the safety of the American drug supply."
Drug manufacturers have 90 days to stop making unapproved prescription medications to treat cold, cough, and allergy symptoms, officials at the Food and Drug Administration announced on March 2.
The FDA issued a list of about 500 unapproved prescription products that should be pulled from the market. These products were never evaluated by the FDA but continue to be prescribed. In many cases, they have been on the market for years, are listed in the Physicians’ Desk Reference, and are advertised in medical journals. Physicians may not be aware that the drugs were not approved, Deborah M. Autor, director of the Office of Compliance at the FDA’s Center for Drug Evaluation and Research, said during a press conference.
"This action is necessary to protect consumers from the potential risks posed by unapproved drugs because we don’t know what’s in them, whether they work properly, or how they are made," Ms. Autor said.
The FDA announcement is part of a broader crackdown on unapproved drugs that began in 2006. But Ms. Autor said that agency officials have particular concerns about these cold, cough, and allergy medications. For example, some of the drugs are labeled as time-release formulations, but without evaluation by the FDA, it’s unclear whether the drugs are delivering their active ingredients as labeled, Ms. Autor said. The active ingredient may be released too slowly, too quickly, or not at all, she said.
Ms. Autor said that the FDA is also concerned because some of the unapproved drugs are labeled for use in children younger than age 2 years. Some of the unapproved drugs also have names that are similar to the names of other drugs, which could lead to confusion when prescriptions are filled. And some of the drugs on the FDA’s list contain combinations of the same types of ingredients, such as two or more antihistamines, which can lead to oversedation.
If a company has registered its unapproved products with the FDA, it will have 90 days to stop manufacturing and 180 days to stop shipping all products. However, FDA officials said there are likely more unapproved prescription drugs that have never been registered with the agency. Those products must be pulled from the market immediately.
"We do not anticipate today’s action will have a major negative impact on consumers or health professionals because there are multiple other products available to treat cough, cold, and allergy symptoms, either as an FDA-approved prescription drug or an over-the-counter drug that follows appropriate FDA standards," Ms. Autor said. "We do anticipate that today’s action will have a significant positive impact by improving the safety of the American drug supply."
FROM THE FDA
Sleep Apnea Implicated in Deaths After Bariatric Surgery
HUNTINGTON BEACH, CALIF. - Underrecognized and undertreated obstructive sleep apnea is the most likely cause of unexplained deaths following bariatric surgery, according to results of a small pilot study.
Because of that, continuous positive airway pressure (CPAP) and continuous pulse oximetry monitoring – with alarms to alert nursing staff to hypoxic episodes and rouse oxygen-desaturated patients from sleep – should be included in postoperative care, said Dr. Scott Gallagher, a bariatric surgeon at the University of South Florida, Tampa, where the study was conducted.

In previous work, the researchers found that severe, prolonged, and frequent arterial hypoxemia is common in sleeping bariatric surgery patients. They sought to determine why such patients – who seemed to be doing well after surgery – died suddenly in their sleep, without pulmonary embolism or any other obvious cause. In 15 gastric bypass patients monitored for 24 hours after surgery, they found that the average episode of hypoxemia lasted 21 minutes, and the longest for hours. Blood oxygen saturation fell as low as 60% (J. Surg. Res. 2010;159:622-6).
Right-to-left shunt, diminished inspired oxygen partial pressure, and other textbook explanations did not provide a rationale for the hypoxemia. Such causes "didn’t exist in these patients," Dr. Gallagher said.
That left either postoperative, narcotic-induced hypoventilation or obstructive sleep apnea as the most likely explanation. Narcotic pain control is common after bariatric surgery, as is sleep apnea.
Dr. Gallagher and his team measured carbon dioxide partial pressures transcutaneously (PtcCO2) to gauge hypoventilation in 20 patients (14 female) during the first 24 hours after Roux-en-Y gastric bypass. Patients also wore blood oxygen saturation (SpO2) ear-clip sensors.
Their mean body mass index was 54 kg/m2, and 15 were diagnosed with obstructive sleep apnea. All were on postoperative narcotics.
As in the previous study, all the patients had multiple episodes of prolonged hypoxemia, with a mean of 191 episodes per patient lasting a mean of 1 minute.
Mean SpO2 was 94%, and mean minimum SpO2 was 60%. Patients spent about 5% of their time (75 minutes) with SpO2 below 88%; hypoxemia lasted longer than 5 minutes in three patients.
All patients also had mild hypercarbia, suggesting mild, chronic hypoventilation.
They had a mean PtcCO2 of 44 mmHg and a mean maximum of 56 mm Hg. The maximum PtcCO2 value recorded in any patient was 75 mm Hg. Heart rates temporarily dropped below 50 bpm in 14 patients.
However, "in no patient could hypoxemia be explained entirely by hypoventilation, and there was no obvious relationship between hypoxemic episodes and [hypoventilation]," said Dr. Krista Haines, a recent University of South Florida graduate now with the University of Nevada, Las Vegas, who presented the findings at the annual Academic Surgical Congress.
The mild hypoventilation by itself was "not clinically significant," leaving obstructive sleep apnea as the most likely cause of hypoxemia following bariatric surgery, Dr. Gallagher stated.
As far as the unexplained deaths go, Dr. Gallagher and his team believe that once patients desaturate, the mild narcotic-induced hypoventilation pushes a few of them over the edge, though no one died in the study.
Because sleep apnea is the likely root cause of such deaths, Dr. Gallagher recommends routine postoperative monitoring of bariatric surgery patients. "[Apneics] need to have their CPAP on" after surgery, especially when receiving narcotics, he said.
CPAP and postoperative monitoring are necessary until sleep apnea resolves, usually after a weight loss of 50-75 pounds. In his study, he noted that 14 patients had machines but still desaturated. Barring faulty gear or incorrect settings, that means the machines weren’t being used throughout the night.
He also pointed out the supplemental oxygen used in the study didn’t prevent hypercarbia or hypoxemia and seems to have no therapeutic role at this point.
In many places, sleep apnea screens, CPAP, and nighttime pulse oximetry are not the standard of care following bariatric surgery, Dr. Gallagher said.
Dr. Stefan Holubar, a colorectal surgeon and comoderator of the session, thinks that needs to change.
"The standard of care should include formal obstructive sleep apnea [screening] for all patients undergoing bariatric surgery, or they should all be empirically treated [with CPAP] regardless of whether or not they have the diagnosis," said Dr. Holubar of Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
"Although it’s a small pilot study, there are profound implications," he added.
The study "is a great start," said comoderator Dr. George Chang, a colorectal surgeon at that University of Texas at Houston. But the team needs to "demonstrate an association between unexplained deaths and these measures. You’d have to do a very large long-term study to see if those unexplained deaths go down."
Dr. Gallagher and his team are considering a randomized study to further investigate the issue, and they plan to include obese people having other kinds of operations.
Dr. Gallagher believes what the team has found thus far is "the tip of the iceberg."
Dr. Gallagher and Dr. Haines said they have no conflicts of interest. The study received no outside funding.
HUNTINGTON BEACH, CALIF. - Underrecognized and undertreated obstructive sleep apnea is the most likely cause of unexplained deaths following bariatric surgery, according to results of a small pilot study.
Because of that, continuous positive airway pressure (CPAP) and continuous pulse oximetry monitoring – with alarms to alert nursing staff to hypoxic episodes and rouse oxygen-desaturated patients from sleep – should be included in postoperative care, said Dr. Scott Gallagher, a bariatric surgeon at the University of South Florida, Tampa, where the study was conducted.
In previous work, the researchers found that severe, prolonged, and frequent arterial hypoxemia is common in sleeping bariatric surgery patients. They sought to determine why such patients – who seemed to be doing well after surgery – died suddenly in their sleep, without pulmonary embolism or any other obvious cause. In 15 gastric bypass patients monitored for 24 hours after surgery, they found that the average episode of hypoxemia lasted 21 minutes, and the longest for hours. Blood oxygen saturation fell as low as 60% (J. Surg. Res. 2010;159:622-6).
Right-to-left shunt, diminished inspired oxygen partial pressure, and other textbook explanations did not provide a rationale for the hypoxemia. Such causes "didn’t exist in these patients," Dr. Gallagher said.
That left either postoperative, narcotic-induced hypoventilation or obstructive sleep apnea as the most likely explanation. Narcotic pain control is common after bariatric surgery, as is sleep apnea.
Dr. Gallagher and his team measured carbon dioxide partial pressures transcutaneously (PtcCO2) to gauge hypoventilation in 20 patients (14 female) during the first 24 hours after Roux-en-Y gastric bypass. Patients also wore blood oxygen saturation (SpO2) ear-clip sensors.
Their mean body mass index was 54 kg/m2, and 15 were diagnosed with obstructive sleep apnea. All were on postoperative narcotics.
As in the previous study, all the patients had multiple episodes of prolonged hypoxemia, with a mean of 191 episodes per patient lasting a mean of 1 minute.
Mean SpO2 was 94%, and mean minimum SpO2 was 60%. Patients spent about 5% of their time (75 minutes) with SpO2 below 88%; hypoxemia lasted longer than 5 minutes in three patients.
All patients also had mild hypercarbia, suggesting mild, chronic hypoventilation.
They had a mean PtcCO2 of 44 mmHg and a mean maximum of 56 mm Hg. The maximum PtcCO2 value recorded in any patient was 75 mm Hg. Heart rates temporarily dropped below 50 bpm in 14 patients.
However, "in no patient could hypoxemia be explained entirely by hypoventilation, and there was no obvious relationship between hypoxemic episodes and [hypoventilation]," said Dr. Krista Haines, a recent University of South Florida graduate now with the University of Nevada, Las Vegas, who presented the findings at the annual Academic Surgical Congress.
The mild hypoventilation by itself was "not clinically significant," leaving obstructive sleep apnea as the most likely cause of hypoxemia following bariatric surgery, Dr. Gallagher stated.
As far as the unexplained deaths go, Dr. Gallagher and his team believe that once patients desaturate, the mild narcotic-induced hypoventilation pushes a few of them over the edge, though no one died in the study.
Because sleep apnea is the likely root cause of such deaths, Dr. Gallagher recommends routine postoperative monitoring of bariatric surgery patients. "[Apneics] need to have their CPAP on" after surgery, especially when receiving narcotics, he said.
CPAP and postoperative monitoring are necessary until sleep apnea resolves, usually after a weight loss of 50-75 pounds. In his study, he noted that 14 patients had machines but still desaturated. Barring faulty gear or incorrect settings, that means the machines weren’t being used throughout the night.
He also pointed out the supplemental oxygen used in the study didn’t prevent hypercarbia or hypoxemia and seems to have no therapeutic role at this point.
In many places, sleep apnea screens, CPAP, and nighttime pulse oximetry are not the standard of care following bariatric surgery, Dr. Gallagher said.
Dr. Stefan Holubar, a colorectal surgeon and comoderator of the session, thinks that needs to change.
"The standard of care should include formal obstructive sleep apnea [screening] for all patients undergoing bariatric surgery, or they should all be empirically treated [with CPAP] regardless of whether or not they have the diagnosis," said Dr. Holubar of Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
"Although it’s a small pilot study, there are profound implications," he added.
The study "is a great start," said comoderator Dr. George Chang, a colorectal surgeon at that University of Texas at Houston. But the team needs to "demonstrate an association between unexplained deaths and these measures. You’d have to do a very large long-term study to see if those unexplained deaths go down."
Dr. Gallagher and his team are considering a randomized study to further investigate the issue, and they plan to include obese people having other kinds of operations.
Dr. Gallagher believes what the team has found thus far is "the tip of the iceberg."
Dr. Gallagher and Dr. Haines said they have no conflicts of interest. The study received no outside funding.
HUNTINGTON BEACH, CALIF. - Underrecognized and undertreated obstructive sleep apnea is the most likely cause of unexplained deaths following bariatric surgery, according to results of a small pilot study.
Because of that, continuous positive airway pressure (CPAP) and continuous pulse oximetry monitoring – with alarms to alert nursing staff to hypoxic episodes and rouse oxygen-desaturated patients from sleep – should be included in postoperative care, said Dr. Scott Gallagher, a bariatric surgeon at the University of South Florida, Tampa, where the study was conducted.
In previous work, the researchers found that severe, prolonged, and frequent arterial hypoxemia is common in sleeping bariatric surgery patients. They sought to determine why such patients – who seemed to be doing well after surgery – died suddenly in their sleep, without pulmonary embolism or any other obvious cause. In 15 gastric bypass patients monitored for 24 hours after surgery, they found that the average episode of hypoxemia lasted 21 minutes, and the longest for hours. Blood oxygen saturation fell as low as 60% (J. Surg. Res. 2010;159:622-6).
Right-to-left shunt, diminished inspired oxygen partial pressure, and other textbook explanations did not provide a rationale for the hypoxemia. Such causes "didn’t exist in these patients," Dr. Gallagher said.
That left either postoperative, narcotic-induced hypoventilation or obstructive sleep apnea as the most likely explanation. Narcotic pain control is common after bariatric surgery, as is sleep apnea.
Dr. Gallagher and his team measured carbon dioxide partial pressures transcutaneously (PtcCO2) to gauge hypoventilation in 20 patients (14 female) during the first 24 hours after Roux-en-Y gastric bypass. Patients also wore blood oxygen saturation (SpO2) ear-clip sensors.
Their mean body mass index was 54 kg/m2, and 15 were diagnosed with obstructive sleep apnea. All were on postoperative narcotics.
As in the previous study, all the patients had multiple episodes of prolonged hypoxemia, with a mean of 191 episodes per patient lasting a mean of 1 minute.
Mean SpO2 was 94%, and mean minimum SpO2 was 60%. Patients spent about 5% of their time (75 minutes) with SpO2 below 88%; hypoxemia lasted longer than 5 minutes in three patients.
All patients also had mild hypercarbia, suggesting mild, chronic hypoventilation.
They had a mean PtcCO2 of 44 mmHg and a mean maximum of 56 mm Hg. The maximum PtcCO2 value recorded in any patient was 75 mm Hg. Heart rates temporarily dropped below 50 bpm in 14 patients.
However, "in no patient could hypoxemia be explained entirely by hypoventilation, and there was no obvious relationship between hypoxemic episodes and [hypoventilation]," said Dr. Krista Haines, a recent University of South Florida graduate now with the University of Nevada, Las Vegas, who presented the findings at the annual Academic Surgical Congress.
The mild hypoventilation by itself was "not clinically significant," leaving obstructive sleep apnea as the most likely cause of hypoxemia following bariatric surgery, Dr. Gallagher stated.
As far as the unexplained deaths go, Dr. Gallagher and his team believe that once patients desaturate, the mild narcotic-induced hypoventilation pushes a few of them over the edge, though no one died in the study.
Because sleep apnea is the likely root cause of such deaths, Dr. Gallagher recommends routine postoperative monitoring of bariatric surgery patients. "[Apneics] need to have their CPAP on" after surgery, especially when receiving narcotics, he said.
CPAP and postoperative monitoring are necessary until sleep apnea resolves, usually after a weight loss of 50-75 pounds. In his study, he noted that 14 patients had machines but still desaturated. Barring faulty gear or incorrect settings, that means the machines weren’t being used throughout the night.
He also pointed out the supplemental oxygen used in the study didn’t prevent hypercarbia or hypoxemia and seems to have no therapeutic role at this point.
In many places, sleep apnea screens, CPAP, and nighttime pulse oximetry are not the standard of care following bariatric surgery, Dr. Gallagher said.
Dr. Stefan Holubar, a colorectal surgeon and comoderator of the session, thinks that needs to change.
"The standard of care should include formal obstructive sleep apnea [screening] for all patients undergoing bariatric surgery, or they should all be empirically treated [with CPAP] regardless of whether or not they have the diagnosis," said Dr. Holubar of Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
"Although it’s a small pilot study, there are profound implications," he added.
The study "is a great start," said comoderator Dr. George Chang, a colorectal surgeon at that University of Texas at Houston. But the team needs to "demonstrate an association between unexplained deaths and these measures. You’d have to do a very large long-term study to see if those unexplained deaths go down."
Dr. Gallagher and his team are considering a randomized study to further investigate the issue, and they plan to include obese people having other kinds of operations.
Dr. Gallagher believes what the team has found thus far is "the tip of the iceberg."
Dr. Gallagher and Dr. Haines said they have no conflicts of interest. The study received no outside funding.
FROM THE ANNUAL ACADEMIC SURGICAL CONGRESS
Major Finding: Obstructive sleep apnea causes profound, prolonged, and, in some cases, life-threatening hypoxemia in bariatric patients.
Data Source: Prospective case series of 20 patients.
Disclosures: Dr. Gallagher and Dr. Haines said they have no conflicts of interest.
Sleep Apnea Implicated in Deaths After Bariatric Surgery
HUNTINGTON BEACH, CALIF. - Underrecognized and undertreated obstructive sleep apnea is the most likely cause of unexplained deaths following bariatric surgery, according to results of a small pilot study.
Because of that, continuous positive airway pressure (CPAP) and continuous pulse oximetry monitoring – with alarms to alert nursing staff to hypoxic episodes and rouse oxygen-desaturated patients from sleep – should be included in postoperative care, said Dr. Scott Gallagher, a bariatric surgeon at the University of South Florida, Tampa, where the study was conducted.
In previous work, the researchers found that severe, prolonged, and frequent arterial hypoxemia is common in sleeping bariatric surgery patients. They sought to determine why such patients – who seemed to be doing well after surgery – died suddenly in their sleep, without pulmonary embolism or any other obvious cause. In 15 gastric bypass patients monitored for 24 hours after surgery, they found that the average episode of hypoxemia lasted 21 minutes, and the longest for hours. Blood oxygen saturation fell as low as 60% (J. Surg. Res. 2010;159:622-6).
Right-to-left shunt, diminished inspired oxygen partial pressure, and other textbook explanations did not provide a rationale for the hypoxemia. Such causes "didn’t exist in these patients," Dr. Gallagher said.
That left either postoperative, narcotic-induced hypoventilation or obstructive sleep apnea as the most likely explanation. Narcotic pain control is common after bariatric surgery, as is sleep apnea.
Dr. Gallagher and his team measured carbon dioxide partial pressures transcutaneously (PtcCO2) to gauge hypoventilation in 20 patients (14 female) during the first 24 hours after Roux-en-Y gastric bypass. Patients also wore blood oxygen saturation (SpO2) ear-clip sensors.
Their mean body mass index was 54 kg/m2, and 15 were diagnosed with obstructive sleep apnea. All were on postoperative narcotics.
As in the previous study, all the patients had multiple episodes of prolonged hypoxemia, with a mean of 191 episodes per patient lasting a mean of 1 minute.
Mean SpO2 was 94%, and mean minimum SpO2 was 60%. Patients spent about 5% of their time (75 minutes) with SpO2 below 88%; hypoxemia lasted longer than 5 minutes in three patients.
All patients also had mild hypercarbia, suggesting mild, chronic hypoventilation.
They had a mean PtcCO2 of 44 mmHg and a mean maximum of 56 mm Hg. The maximum PtcCO2 value recorded in any patient was 75 mm Hg. Heart rates temporarily dropped below 50 bpm in 14 patients.
However, "in no patient could hypoxemia be explained entirely by hypoventilation, and there was no obvious relationship between hypoxemic episodes and [hypoventilation]," said Dr. Krista Haines, a recent University of South Florida graduate now with the University of Nevada, Las Vegas, who presented the findings at the annual Academic Surgical Congress.
The mild hypoventilation by itself was "not clinically significant," leaving obstructive sleep apnea as the most likely cause of hypoxemia following bariatric surgery, Dr. Gallagher stated.
As far as the unexplained deaths go, Dr. Gallagher and his team believe that once patients desaturate, the mild narcotic-induced hypoventilation pushes a few of them over the edge, though no one died in the study.
Because sleep apnea is the likely root cause of such deaths, Dr. Gallagher recommends routine postoperative monitoring of bariatric surgery patients. "[Apneics] need to have their CPAP on" after surgery, especially when receiving narcotics, he said.
CPAP and postoperative monitoring are necessary until sleep apnea resolves, usually after a weight loss of 50-75 pounds. In his study, he noted that 14 patients had machines but still desaturated. Barring faulty gear or incorrect settings, that means the machines weren’t being used throughout the night.
He also pointed out the supplemental oxygen used in the study didn’t prevent hypercarbia or hypoxemia and seems to have no therapeutic role at this point.
In many places, sleep apnea screens, CPAP, and nighttime pulse oximetry are not the standard of care following bariatric surgery, Dr. Gallagher said.
Dr. Stefan Holubar, a colorectal surgeon and comoderator of the session, thinks that needs to change.
"The standard of care should include formal obstructive sleep apnea [screening] for all patients undergoing bariatric surgery, or they should all be empirically treated [with CPAP] regardless of whether or not they have the diagnosis," said Dr. Holubar of Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
"Although it’s a small pilot study, there are profound implications," he added.
The study "is a great start," said comoderator Dr. George Chang, a colorectal surgeon at that University of Texas at Houston. But the team needs to "demonstrate an association between unexplained deaths and these measures. You’d have to do a very large long-term study to see if those unexplained deaths go down."
Dr. Gallagher and his team are considering a randomized study to further investigate the issue, and they plan to include obese people having other kinds of operations.
Dr. Gallagher believes what the team has found thus far is "the tip of the iceberg."
Dr. Gallagher and Dr. Haines said they have no conflicts of interest. The study received no outside funding.
HUNTINGTON BEACH, CALIF. - Underrecognized and undertreated obstructive sleep apnea is the most likely cause of unexplained deaths following bariatric surgery, according to results of a small pilot study.
Because of that, continuous positive airway pressure (CPAP) and continuous pulse oximetry monitoring – with alarms to alert nursing staff to hypoxic episodes and rouse oxygen-desaturated patients from sleep – should be included in postoperative care, said Dr. Scott Gallagher, a bariatric surgeon at the University of South Florida, Tampa, where the study was conducted.
In previous work, the researchers found that severe, prolonged, and frequent arterial hypoxemia is common in sleeping bariatric surgery patients. They sought to determine why such patients – who seemed to be doing well after surgery – died suddenly in their sleep, without pulmonary embolism or any other obvious cause. In 15 gastric bypass patients monitored for 24 hours after surgery, they found that the average episode of hypoxemia lasted 21 minutes, and the longest for hours. Blood oxygen saturation fell as low as 60% (J. Surg. Res. 2010;159:622-6).
Right-to-left shunt, diminished inspired oxygen partial pressure, and other textbook explanations did not provide a rationale for the hypoxemia. Such causes "didn’t exist in these patients," Dr. Gallagher said.
That left either postoperative, narcotic-induced hypoventilation or obstructive sleep apnea as the most likely explanation. Narcotic pain control is common after bariatric surgery, as is sleep apnea.
Dr. Gallagher and his team measured carbon dioxide partial pressures transcutaneously (PtcCO2) to gauge hypoventilation in 20 patients (14 female) during the first 24 hours after Roux-en-Y gastric bypass. Patients also wore blood oxygen saturation (SpO2) ear-clip sensors.
Their mean body mass index was 54 kg/m2, and 15 were diagnosed with obstructive sleep apnea. All were on postoperative narcotics.
As in the previous study, all the patients had multiple episodes of prolonged hypoxemia, with a mean of 191 episodes per patient lasting a mean of 1 minute.
Mean SpO2 was 94%, and mean minimum SpO2 was 60%. Patients spent about 5% of their time (75 minutes) with SpO2 below 88%; hypoxemia lasted longer than 5 minutes in three patients.
All patients also had mild hypercarbia, suggesting mild, chronic hypoventilation.
They had a mean PtcCO2 of 44 mmHg and a mean maximum of 56 mm Hg. The maximum PtcCO2 value recorded in any patient was 75 mm Hg. Heart rates temporarily dropped below 50 bpm in 14 patients.
However, "in no patient could hypoxemia be explained entirely by hypoventilation, and there was no obvious relationship between hypoxemic episodes and [hypoventilation]," said Dr. Krista Haines, a recent University of South Florida graduate now with the University of Nevada, Las Vegas, who presented the findings at the annual Academic Surgical Congress.
The mild hypoventilation by itself was "not clinically significant," leaving obstructive sleep apnea as the most likely cause of hypoxemia following bariatric surgery, Dr. Gallagher stated.
As far as the unexplained deaths go, Dr. Gallagher and his team believe that once patients desaturate, the mild narcotic-induced hypoventilation pushes a few of them over the edge, though no one died in the study.
Because sleep apnea is the likely root cause of such deaths, Dr. Gallagher recommends routine postoperative monitoring of bariatric surgery patients. "[Apneics] need to have their CPAP on" after surgery, especially when receiving narcotics, he said.
CPAP and postoperative monitoring are necessary until sleep apnea resolves, usually after a weight loss of 50-75 pounds. In his study, he noted that 14 patients had machines but still desaturated. Barring faulty gear or incorrect settings, that means the machines weren’t being used throughout the night.
He also pointed out the supplemental oxygen used in the study didn’t prevent hypercarbia or hypoxemia and seems to have no therapeutic role at this point.
In many places, sleep apnea screens, CPAP, and nighttime pulse oximetry are not the standard of care following bariatric surgery, Dr. Gallagher said.
Dr. Stefan Holubar, a colorectal surgeon and comoderator of the session, thinks that needs to change.
"The standard of care should include formal obstructive sleep apnea [screening] for all patients undergoing bariatric surgery, or they should all be empirically treated [with CPAP] regardless of whether or not they have the diagnosis," said Dr. Holubar of Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
"Although it’s a small pilot study, there are profound implications," he added.
The study "is a great start," said comoderator Dr. George Chang, a colorectal surgeon at that University of Texas at Houston. But the team needs to "demonstrate an association between unexplained deaths and these measures. You’d have to do a very large long-term study to see if those unexplained deaths go down."
Dr. Gallagher and his team are considering a randomized study to further investigate the issue, and they plan to include obese people having other kinds of operations.
Dr. Gallagher believes what the team has found thus far is "the tip of the iceberg."
Dr. Gallagher and Dr. Haines said they have no conflicts of interest. The study received no outside funding.
HUNTINGTON BEACH, CALIF. - Underrecognized and undertreated obstructive sleep apnea is the most likely cause of unexplained deaths following bariatric surgery, according to results of a small pilot study.
Because of that, continuous positive airway pressure (CPAP) and continuous pulse oximetry monitoring – with alarms to alert nursing staff to hypoxic episodes and rouse oxygen-desaturated patients from sleep – should be included in postoperative care, said Dr. Scott Gallagher, a bariatric surgeon at the University of South Florida, Tampa, where the study was conducted.
In previous work, the researchers found that severe, prolonged, and frequent arterial hypoxemia is common in sleeping bariatric surgery patients. They sought to determine why such patients – who seemed to be doing well after surgery – died suddenly in their sleep, without pulmonary embolism or any other obvious cause. In 15 gastric bypass patients monitored for 24 hours after surgery, they found that the average episode of hypoxemia lasted 21 minutes, and the longest for hours. Blood oxygen saturation fell as low as 60% (J. Surg. Res. 2010;159:622-6).
Right-to-left shunt, diminished inspired oxygen partial pressure, and other textbook explanations did not provide a rationale for the hypoxemia. Such causes "didn’t exist in these patients," Dr. Gallagher said.
That left either postoperative, narcotic-induced hypoventilation or obstructive sleep apnea as the most likely explanation. Narcotic pain control is common after bariatric surgery, as is sleep apnea.
Dr. Gallagher and his team measured carbon dioxide partial pressures transcutaneously (PtcCO2) to gauge hypoventilation in 20 patients (14 female) during the first 24 hours after Roux-en-Y gastric bypass. Patients also wore blood oxygen saturation (SpO2) ear-clip sensors.
Their mean body mass index was 54 kg/m2, and 15 were diagnosed with obstructive sleep apnea. All were on postoperative narcotics.
As in the previous study, all the patients had multiple episodes of prolonged hypoxemia, with a mean of 191 episodes per patient lasting a mean of 1 minute.
Mean SpO2 was 94%, and mean minimum SpO2 was 60%. Patients spent about 5% of their time (75 minutes) with SpO2 below 88%; hypoxemia lasted longer than 5 minutes in three patients.
All patients also had mild hypercarbia, suggesting mild, chronic hypoventilation.
They had a mean PtcCO2 of 44 mmHg and a mean maximum of 56 mm Hg. The maximum PtcCO2 value recorded in any patient was 75 mm Hg. Heart rates temporarily dropped below 50 bpm in 14 patients.
However, "in no patient could hypoxemia be explained entirely by hypoventilation, and there was no obvious relationship between hypoxemic episodes and [hypoventilation]," said Dr. Krista Haines, a recent University of South Florida graduate now with the University of Nevada, Las Vegas, who presented the findings at the annual Academic Surgical Congress.
The mild hypoventilation by itself was "not clinically significant," leaving obstructive sleep apnea as the most likely cause of hypoxemia following bariatric surgery, Dr. Gallagher stated.
As far as the unexplained deaths go, Dr. Gallagher and his team believe that once patients desaturate, the mild narcotic-induced hypoventilation pushes a few of them over the edge, though no one died in the study.
Because sleep apnea is the likely root cause of such deaths, Dr. Gallagher recommends routine postoperative monitoring of bariatric surgery patients. "[Apneics] need to have their CPAP on" after surgery, especially when receiving narcotics, he said.
CPAP and postoperative monitoring are necessary until sleep apnea resolves, usually after a weight loss of 50-75 pounds. In his study, he noted that 14 patients had machines but still desaturated. Barring faulty gear or incorrect settings, that means the machines weren’t being used throughout the night.
He also pointed out the supplemental oxygen used in the study didn’t prevent hypercarbia or hypoxemia and seems to have no therapeutic role at this point.
In many places, sleep apnea screens, CPAP, and nighttime pulse oximetry are not the standard of care following bariatric surgery, Dr. Gallagher said.
Dr. Stefan Holubar, a colorectal surgeon and comoderator of the session, thinks that needs to change.
"The standard of care should include formal obstructive sleep apnea [screening] for all patients undergoing bariatric surgery, or they should all be empirically treated [with CPAP] regardless of whether or not they have the diagnosis," said Dr. Holubar of Dartmouth-Hitchcock Medical Center in Lebanon, N.H.
"Although it’s a small pilot study, there are profound implications," he added.
The study "is a great start," said comoderator Dr. George Chang, a colorectal surgeon at that University of Texas at Houston. But the team needs to "demonstrate an association between unexplained deaths and these measures. You’d have to do a very large long-term study to see if those unexplained deaths go down."
Dr. Gallagher and his team are considering a randomized study to further investigate the issue, and they plan to include obese people having other kinds of operations.
Dr. Gallagher believes what the team has found thus far is "the tip of the iceberg."
Dr. Gallagher and Dr. Haines said they have no conflicts of interest. The study received no outside funding.
FROM THE ANNUAL ACADEMIC SURGICAL CONGRESS
Major Finding: Obstructive sleep apnea causes profound, prolonged, and, in some cases, life-threatening hypoxemia in bariatric patients.
Data Source: Prospective case series of 20 patients.
Disclosures: Dr. Gallagher and Dr. Haines said they have no conflicts of interest.
FDA Approves PD-4 Inhibitor for COPD Flares
Roflumilast was approved by the Food and Drug Administration March 1 to decrease the frequency of exacerbations in patients with severe chronic obstructive pulmonary disease associated with chronic bronchitis and a history of exacerbations.
The drug is the only PD-4 inhibitor approved for this indication, according to Forest Pharmaceuticals, which developed the agent. It will be marketed as Daliresp and is expected to be commercially available later this year.
Roflumilast will be available in 500-mcg pills to be taken daily for the prevention of COPD flares in patients with severe disease, according to the agency.
The decision stands in contrast to an FDA advisory panel’s recommendation. In April 2010, members of the Pulmonary-Allergy Drugs Advisory Committee voted 10-5 that the efficacy and safety data on the drug did not support approval for the maintenance treatment of COPD associated with chronic bronchitis in patients at risk of exacerbations.
This was the original proposed indication, but in January 2010 – a month after Forest Research Institute Inc., acquired the drug from another company – Forest changed the proposed indication to a more focused one: "Maintenance treatment to reduce exacerbations of COPD." Because this was done 6 months into the FDA review period, however, the panel was asked to vote on the original indication.
The reasons panelists gave for voting against approval of the original, broader indication included what some described as the "meager" or modest beneficial effect of roflumilast in studies, the need to compare it with other COPD treatments like theophylline (a nonspecific PDE inhibitor and the only PDE inhibitor marketed in the United States), and the need to evaluate its efficacy when added to standard COPD treatments like inhaled corticosteroids.
Its efficacy and safety were evaluated in eight clinical studies comprising 9,394 adult patients, of whom 4,425 took the drug, according a statement issued by Forest. Two of these studies were 1-year placebo-controlled trials that together enrolled more than 3,100 patients. Those treated had a history of COPD associated with chronic bronchitis and had experienced an exacerbation of the disease during the 12 months before beginning treatment. All patients were taking concomitant medications, including long- and short-acting beta-2 agonists or short-acting anticholinergics.
Overall, the drug reduced the rate of moderate or severe exacerbations by 15% in one trial and 18% in the other, compared with placebo. The drug also improved prebronchodilator lung function.
Among the eight trials, most common adverse reactions in those taking the drug included diarrhea, weight decrease, nausea, headache, back pain, influenza, insomnia, dizziness, and decreased appetite. Fourteen percent of patients taking roflumilast withdrew from the studies because of adverse events: 5% for gastrointestinal upset and the rest for other problems. Serious adverse events occurred in 14% of those taking placebo and 13% of those taking roflumilast. Death from COPD occurred in 20 patients in the roflumilast group and 22 in the placebo group – not a significant difference.
The company also noted that weight change occurred more often in those taking the drug. It occurred mostly in obese rather than underweight patients and caused no increased morbidity relative to placebo. However, the company warned in a 2010 FDA presentation, "patients and physicians should be informed that weight loss is associated with roflumilast and weight should be regularly monitored."
The drug is contraindicated in patients with moderate to severe liver impairment (Child-Pugh B or C), according to the company’s statement.
Other safety warnings will appear on the packaging:
• Roflumilast is not a bronchodilator and should not be used for the relief of acute bronchospasm.
• Psychiatric events including suicidality are associated with its use, occurring in 5.9% of treated patients compared with 3.3% of those taking placebo. Three patients experienced suicide-related adverse reactions, with one completion and two attempts, compared with one suicidal ideation in one placebo-treated patient.
• The drug should not be used in conjunction with strong P450 enzyme inducers and used with caution in patients taking inhibitors of the CYP3A4 or CYP1A2 enzymes.
• Roflumilast should not be used by pregnant women unless the risks and benefits are carefully weighed, and should not be taken during labor and delivery.
The drug’s mechanism of action is not fully understood, the company noted. "It is thought to be related to the effects of increased intracellular adenosine monophosphate."
Roflumilast was approved by the Food and Drug Administration March 1 to decrease the frequency of exacerbations in patients with severe chronic obstructive pulmonary disease associated with chronic bronchitis and a history of exacerbations.
The drug is the only PD-4 inhibitor approved for this indication, according to Forest Pharmaceuticals, which developed the agent. It will be marketed as Daliresp and is expected to be commercially available later this year.
Roflumilast will be available in 500-mcg pills to be taken daily for the prevention of COPD flares in patients with severe disease, according to the agency.
The decision stands in contrast to an FDA advisory panel’s recommendation. In April 2010, members of the Pulmonary-Allergy Drugs Advisory Committee voted 10-5 that the efficacy and safety data on the drug did not support approval for the maintenance treatment of COPD associated with chronic bronchitis in patients at risk of exacerbations.
This was the original proposed indication, but in January 2010 – a month after Forest Research Institute Inc., acquired the drug from another company – Forest changed the proposed indication to a more focused one: "Maintenance treatment to reduce exacerbations of COPD." Because this was done 6 months into the FDA review period, however, the panel was asked to vote on the original indication.
The reasons panelists gave for voting against approval of the original, broader indication included what some described as the "meager" or modest beneficial effect of roflumilast in studies, the need to compare it with other COPD treatments like theophylline (a nonspecific PDE inhibitor and the only PDE inhibitor marketed in the United States), and the need to evaluate its efficacy when added to standard COPD treatments like inhaled corticosteroids.
Its efficacy and safety were evaluated in eight clinical studies comprising 9,394 adult patients, of whom 4,425 took the drug, according a statement issued by Forest. Two of these studies were 1-year placebo-controlled trials that together enrolled more than 3,100 patients. Those treated had a history of COPD associated with chronic bronchitis and had experienced an exacerbation of the disease during the 12 months before beginning treatment. All patients were taking concomitant medications, including long- and short-acting beta-2 agonists or short-acting anticholinergics.
Overall, the drug reduced the rate of moderate or severe exacerbations by 15% in one trial and 18% in the other, compared with placebo. The drug also improved prebronchodilator lung function.
Among the eight trials, most common adverse reactions in those taking the drug included diarrhea, weight decrease, nausea, headache, back pain, influenza, insomnia, dizziness, and decreased appetite. Fourteen percent of patients taking roflumilast withdrew from the studies because of adverse events: 5% for gastrointestinal upset and the rest for other problems. Serious adverse events occurred in 14% of those taking placebo and 13% of those taking roflumilast. Death from COPD occurred in 20 patients in the roflumilast group and 22 in the placebo group – not a significant difference.
The company also noted that weight change occurred more often in those taking the drug. It occurred mostly in obese rather than underweight patients and caused no increased morbidity relative to placebo. However, the company warned in a 2010 FDA presentation, "patients and physicians should be informed that weight loss is associated with roflumilast and weight should be regularly monitored."
The drug is contraindicated in patients with moderate to severe liver impairment (Child-Pugh B or C), according to the company’s statement.
Other safety warnings will appear on the packaging:
• Roflumilast is not a bronchodilator and should not be used for the relief of acute bronchospasm.
• Psychiatric events including suicidality are associated with its use, occurring in 5.9% of treated patients compared with 3.3% of those taking placebo. Three patients experienced suicide-related adverse reactions, with one completion and two attempts, compared with one suicidal ideation in one placebo-treated patient.
• The drug should not be used in conjunction with strong P450 enzyme inducers and used with caution in patients taking inhibitors of the CYP3A4 or CYP1A2 enzymes.
• Roflumilast should not be used by pregnant women unless the risks and benefits are carefully weighed, and should not be taken during labor and delivery.
The drug’s mechanism of action is not fully understood, the company noted. "It is thought to be related to the effects of increased intracellular adenosine monophosphate."
Roflumilast was approved by the Food and Drug Administration March 1 to decrease the frequency of exacerbations in patients with severe chronic obstructive pulmonary disease associated with chronic bronchitis and a history of exacerbations.
The drug is the only PD-4 inhibitor approved for this indication, according to Forest Pharmaceuticals, which developed the agent. It will be marketed as Daliresp and is expected to be commercially available later this year.
Roflumilast will be available in 500-mcg pills to be taken daily for the prevention of COPD flares in patients with severe disease, according to the agency.
The decision stands in contrast to an FDA advisory panel’s recommendation. In April 2010, members of the Pulmonary-Allergy Drugs Advisory Committee voted 10-5 that the efficacy and safety data on the drug did not support approval for the maintenance treatment of COPD associated with chronic bronchitis in patients at risk of exacerbations.
This was the original proposed indication, but in January 2010 – a month after Forest Research Institute Inc., acquired the drug from another company – Forest changed the proposed indication to a more focused one: "Maintenance treatment to reduce exacerbations of COPD." Because this was done 6 months into the FDA review period, however, the panel was asked to vote on the original indication.
The reasons panelists gave for voting against approval of the original, broader indication included what some described as the "meager" or modest beneficial effect of roflumilast in studies, the need to compare it with other COPD treatments like theophylline (a nonspecific PDE inhibitor and the only PDE inhibitor marketed in the United States), and the need to evaluate its efficacy when added to standard COPD treatments like inhaled corticosteroids.
Its efficacy and safety were evaluated in eight clinical studies comprising 9,394 adult patients, of whom 4,425 took the drug, according a statement issued by Forest. Two of these studies were 1-year placebo-controlled trials that together enrolled more than 3,100 patients. Those treated had a history of COPD associated with chronic bronchitis and had experienced an exacerbation of the disease during the 12 months before beginning treatment. All patients were taking concomitant medications, including long- and short-acting beta-2 agonists or short-acting anticholinergics.
Overall, the drug reduced the rate of moderate or severe exacerbations by 15% in one trial and 18% in the other, compared with placebo. The drug also improved prebronchodilator lung function.
Among the eight trials, most common adverse reactions in those taking the drug included diarrhea, weight decrease, nausea, headache, back pain, influenza, insomnia, dizziness, and decreased appetite. Fourteen percent of patients taking roflumilast withdrew from the studies because of adverse events: 5% for gastrointestinal upset and the rest for other problems. Serious adverse events occurred in 14% of those taking placebo and 13% of those taking roflumilast. Death from COPD occurred in 20 patients in the roflumilast group and 22 in the placebo group – not a significant difference.
The company also noted that weight change occurred more often in those taking the drug. It occurred mostly in obese rather than underweight patients and caused no increased morbidity relative to placebo. However, the company warned in a 2010 FDA presentation, "patients and physicians should be informed that weight loss is associated with roflumilast and weight should be regularly monitored."
The drug is contraindicated in patients with moderate to severe liver impairment (Child-Pugh B or C), according to the company’s statement.
Other safety warnings will appear on the packaging:
• Roflumilast is not a bronchodilator and should not be used for the relief of acute bronchospasm.
• Psychiatric events including suicidality are associated with its use, occurring in 5.9% of treated patients compared with 3.3% of those taking placebo. Three patients experienced suicide-related adverse reactions, with one completion and two attempts, compared with one suicidal ideation in one placebo-treated patient.
• The drug should not be used in conjunction with strong P450 enzyme inducers and used with caution in patients taking inhibitors of the CYP3A4 or CYP1A2 enzymes.
• Roflumilast should not be used by pregnant women unless the risks and benefits are carefully weighed, and should not be taken during labor and delivery.
The drug’s mechanism of action is not fully understood, the company noted. "It is thought to be related to the effects of increased intracellular adenosine monophosphate."
FROM A PRESS STATEMENT ISSUED BY THE FOOD AND DRUG ADMINISTRATION