User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Jaw Surgery Limits Severe Sleep Apnea in Soldiers
MINNEAPOLIS – Maxillomandibular advancement may be a reasonable option for patients who have severe sleep apnea and are unable to tolerate continuous positive airway pressure therapy, according to a study by the Department of Veterans Affairs.
In maxillomandibular advancement (MMA), the upper and lower jaws are moved forward to optimize the airway and minimize soft-tissue blockages. Dr. Vincent Mysliwiec and his colleagues in the Critical Care Medicine and Sleep Medicine Service at Madigan Healthcare System, Joint Base Lewis-McChord in Tacoma, Wash., evaluated the outcomes of the surgery in an active-duty population.
"Obstructive sleep apnea is an increasingly common diagnosis in soldiers, and those soldiers with more severe cases are not deployable without going through an extensive waiver process," Dr. Mysliwiec said at the annual meeting of the Associated Professional Sleep Societies. "We wanted to assess whether [MMA] represents a surgical cure that can potentially remove the requirement for CPAP in these individuals and, in so doing, increase the number of soldiers who are fully deployable."
The researchers reviewed all of the MMA procedures performed for obstructive sleep apnea at their institution in 2006-2009 and identified 37 soldiers who had severe disease – defined as an apnea-hypopnea index (AHI) of more than 30 events/hr – and underwent the surgery as well as pre- and postoperative polysomnography. The primary study outcomes were comparisons of the pre- and postoperative AHI and minimum nocturnal oxyhemoglobin saturation. Surgical cure was defined as an AHI reduction of at least 50%, compared with preoperative AHI, and a postoperative AHI of less than 15.
The mean body mass index of the study cohort was 29 kg/m2, and the mean preoperative AHI was 50.5, Dr. Mysliwiec reported. Following the procedure, "the mean postoperative [AHI] dropped significantly to 13.8," he said. "Twenty-two of the soldiers – nearly 60% of the group – reduced their [AHI] by at least half, which met the criteria for surgical cure." Further, he said, 16 of the soldiers had a postoperative AHI of less than 5, "meaning they had no residual disease at all following the procedure." One study patient did not experience a clinically significant reduction in AHI following the surgery. The mean minimum nocturnal oxyhemoglobin saturation increased postoperatively from 85% to 86%, a nonsignificant change (P = .21; standard deviation for both measures, 7%).
"Maxillomandibular advancement significantly reduced the severity of sleep apnea for our patients and improved the quality of their sleep," Dr. Mysliwiec said. "These findings could improve the standard of care for civilians and active-duty service members with severe obstructive sleep apnea who can’t tolerate CPAP or have failed other soft-tissue procedures."
Dr. Mysliwiec reported having no financial conflicts of interest.
MINNEAPOLIS – Maxillomandibular advancement may be a reasonable option for patients who have severe sleep apnea and are unable to tolerate continuous positive airway pressure therapy, according to a study by the Department of Veterans Affairs.
In maxillomandibular advancement (MMA), the upper and lower jaws are moved forward to optimize the airway and minimize soft-tissue blockages. Dr. Vincent Mysliwiec and his colleagues in the Critical Care Medicine and Sleep Medicine Service at Madigan Healthcare System, Joint Base Lewis-McChord in Tacoma, Wash., evaluated the outcomes of the surgery in an active-duty population.
"Obstructive sleep apnea is an increasingly common diagnosis in soldiers, and those soldiers with more severe cases are not deployable without going through an extensive waiver process," Dr. Mysliwiec said at the annual meeting of the Associated Professional Sleep Societies. "We wanted to assess whether [MMA] represents a surgical cure that can potentially remove the requirement for CPAP in these individuals and, in so doing, increase the number of soldiers who are fully deployable."
The researchers reviewed all of the MMA procedures performed for obstructive sleep apnea at their institution in 2006-2009 and identified 37 soldiers who had severe disease – defined as an apnea-hypopnea index (AHI) of more than 30 events/hr – and underwent the surgery as well as pre- and postoperative polysomnography. The primary study outcomes were comparisons of the pre- and postoperative AHI and minimum nocturnal oxyhemoglobin saturation. Surgical cure was defined as an AHI reduction of at least 50%, compared with preoperative AHI, and a postoperative AHI of less than 15.
The mean body mass index of the study cohort was 29 kg/m2, and the mean preoperative AHI was 50.5, Dr. Mysliwiec reported. Following the procedure, "the mean postoperative [AHI] dropped significantly to 13.8," he said. "Twenty-two of the soldiers – nearly 60% of the group – reduced their [AHI] by at least half, which met the criteria for surgical cure." Further, he said, 16 of the soldiers had a postoperative AHI of less than 5, "meaning they had no residual disease at all following the procedure." One study patient did not experience a clinically significant reduction in AHI following the surgery. The mean minimum nocturnal oxyhemoglobin saturation increased postoperatively from 85% to 86%, a nonsignificant change (P = .21; standard deviation for both measures, 7%).
"Maxillomandibular advancement significantly reduced the severity of sleep apnea for our patients and improved the quality of their sleep," Dr. Mysliwiec said. "These findings could improve the standard of care for civilians and active-duty service members with severe obstructive sleep apnea who can’t tolerate CPAP or have failed other soft-tissue procedures."
Dr. Mysliwiec reported having no financial conflicts of interest.
MINNEAPOLIS – Maxillomandibular advancement may be a reasonable option for patients who have severe sleep apnea and are unable to tolerate continuous positive airway pressure therapy, according to a study by the Department of Veterans Affairs.
In maxillomandibular advancement (MMA), the upper and lower jaws are moved forward to optimize the airway and minimize soft-tissue blockages. Dr. Vincent Mysliwiec and his colleagues in the Critical Care Medicine and Sleep Medicine Service at Madigan Healthcare System, Joint Base Lewis-McChord in Tacoma, Wash., evaluated the outcomes of the surgery in an active-duty population.
"Obstructive sleep apnea is an increasingly common diagnosis in soldiers, and those soldiers with more severe cases are not deployable without going through an extensive waiver process," Dr. Mysliwiec said at the annual meeting of the Associated Professional Sleep Societies. "We wanted to assess whether [MMA] represents a surgical cure that can potentially remove the requirement for CPAP in these individuals and, in so doing, increase the number of soldiers who are fully deployable."
The researchers reviewed all of the MMA procedures performed for obstructive sleep apnea at their institution in 2006-2009 and identified 37 soldiers who had severe disease – defined as an apnea-hypopnea index (AHI) of more than 30 events/hr – and underwent the surgery as well as pre- and postoperative polysomnography. The primary study outcomes were comparisons of the pre- and postoperative AHI and minimum nocturnal oxyhemoglobin saturation. Surgical cure was defined as an AHI reduction of at least 50%, compared with preoperative AHI, and a postoperative AHI of less than 15.
The mean body mass index of the study cohort was 29 kg/m2, and the mean preoperative AHI was 50.5, Dr. Mysliwiec reported. Following the procedure, "the mean postoperative [AHI] dropped significantly to 13.8," he said. "Twenty-two of the soldiers – nearly 60% of the group – reduced their [AHI] by at least half, which met the criteria for surgical cure." Further, he said, 16 of the soldiers had a postoperative AHI of less than 5, "meaning they had no residual disease at all following the procedure." One study patient did not experience a clinically significant reduction in AHI following the surgery. The mean minimum nocturnal oxyhemoglobin saturation increased postoperatively from 85% to 86%, a nonsignificant change (P = .21; standard deviation for both measures, 7%).
"Maxillomandibular advancement significantly reduced the severity of sleep apnea for our patients and improved the quality of their sleep," Dr. Mysliwiec said. "These findings could improve the standard of care for civilians and active-duty service members with severe obstructive sleep apnea who can’t tolerate CPAP or have failed other soft-tissue procedures."
Dr. Mysliwiec reported having no financial conflicts of interest.
FROM THE ANNUAL MEETING OF THE ASSOCIATED PROFESSIONAL SLEEP SOCIETIES
Major Finding: After maxillomandibular advancement surgery, the severity of obstructive sleep apnea was reduced by at least 50% in 22 patients, of whom 16 had no residual disease.
Data Source: A VA retrospective review of 37 active-duty service personnel.
Disclosures: Dr. Mysliwiec reported having no financial conflicts of interest.
Apnea: Wakeful Analysis Eyed as Polysomnography Alternative
MINNEAPOLIS – An automated analysis of tracheal breath sounds while awake was predictive of obstructive sleep apnea in a small study.
If validated in larger studies, the findings may streamline the obstructive sleep apnea (OSA) screening process, resulting in earlier diagnosis and treatment of severe cases, Zahra Moussavi, Ph.D., said at the annual meeting of the Associated Professional Sleep Societies. "The ability to predict the likelihood and severity of obstructive sleep apnea without performing overnight polysomnography is very appealing and would lead to significant reductions in health care costs, compared with full-night sleep assessments."
Obstructive sleep apnea (OSA) is highly prevalent in the general population, but only 30% of patients referred to a sleep lab for evaluation have severe OSA requiring treatment, said Dr. Moussavi, a professor in the department of electrical and computer engineering at the University of Manitoba, Winnipeg. With no fast, accurate, clinical or laboratory tools for predicting the severity of suspected OSA, full-night polysomnography is required to confirm the diagnosis and determine its severity. "Unfortunately, the demand [for full-night sleep studies] outweighs the available resources, resulting in appointment backlogs and long wait times, which can delay the initiation of potentially lifesaving care," she said.
Acoustic analysis has been used during sleep to evaluate the breathing and snoring patterns of suspected apnea patients. To examine wakeful breathing patterns associated with OSA, Dr. Moussavi and colleagues, recorded the tracheal breath sounds of 35 patients with varying severity of OSA and 17 age-matched controls.
"We recorded the tracheal breath sound in supine and upright positions during nose and mouth breathing," said Dr. Moussavi.
Spectral analysis of the respiratory signals indicated that variation in the average power of the tracheal breath sounds at different positions was a characteristic feature that discriminated the OSA and control groups.
Using the maximum relevancy/minimum redundancy method, the investigators reduced the number of sound features that were significantly different between the groups to two, "and unsupervised clustering of these showed an overall accuracy of 84%, with a sensitivity of 88% and a specificity of 80%," Dr. Moussavi reported.
"It is known that [OSA] patients have a smaller and more collapsible pharynx, which is compensated by increased dilator muscle activity during wakefulness. They tend to have more negative pharyngeal pressure, which can be detected via breathing sounds through the nose because of higher resistance," she said. Because breath sounds are directly related to pharyngeal pressure, "this method is sensitive to the severity of [OSA] even during wakefulness."
The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
MINNEAPOLIS – An automated analysis of tracheal breath sounds while awake was predictive of obstructive sleep apnea in a small study.
If validated in larger studies, the findings may streamline the obstructive sleep apnea (OSA) screening process, resulting in earlier diagnosis and treatment of severe cases, Zahra Moussavi, Ph.D., said at the annual meeting of the Associated Professional Sleep Societies. "The ability to predict the likelihood and severity of obstructive sleep apnea without performing overnight polysomnography is very appealing and would lead to significant reductions in health care costs, compared with full-night sleep assessments."
Obstructive sleep apnea (OSA) is highly prevalent in the general population, but only 30% of patients referred to a sleep lab for evaluation have severe OSA requiring treatment, said Dr. Moussavi, a professor in the department of electrical and computer engineering at the University of Manitoba, Winnipeg. With no fast, accurate, clinical or laboratory tools for predicting the severity of suspected OSA, full-night polysomnography is required to confirm the diagnosis and determine its severity. "Unfortunately, the demand [for full-night sleep studies] outweighs the available resources, resulting in appointment backlogs and long wait times, which can delay the initiation of potentially lifesaving care," she said.
Acoustic analysis has been used during sleep to evaluate the breathing and snoring patterns of suspected apnea patients. To examine wakeful breathing patterns associated with OSA, Dr. Moussavi and colleagues, recorded the tracheal breath sounds of 35 patients with varying severity of OSA and 17 age-matched controls.
"We recorded the tracheal breath sound in supine and upright positions during nose and mouth breathing," said Dr. Moussavi.
Spectral analysis of the respiratory signals indicated that variation in the average power of the tracheal breath sounds at different positions was a characteristic feature that discriminated the OSA and control groups.
Using the maximum relevancy/minimum redundancy method, the investigators reduced the number of sound features that were significantly different between the groups to two, "and unsupervised clustering of these showed an overall accuracy of 84%, with a sensitivity of 88% and a specificity of 80%," Dr. Moussavi reported.
"It is known that [OSA] patients have a smaller and more collapsible pharynx, which is compensated by increased dilator muscle activity during wakefulness. They tend to have more negative pharyngeal pressure, which can be detected via breathing sounds through the nose because of higher resistance," she said. Because breath sounds are directly related to pharyngeal pressure, "this method is sensitive to the severity of [OSA] even during wakefulness."
The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
MINNEAPOLIS – An automated analysis of tracheal breath sounds while awake was predictive of obstructive sleep apnea in a small study.
If validated in larger studies, the findings may streamline the obstructive sleep apnea (OSA) screening process, resulting in earlier diagnosis and treatment of severe cases, Zahra Moussavi, Ph.D., said at the annual meeting of the Associated Professional Sleep Societies. "The ability to predict the likelihood and severity of obstructive sleep apnea without performing overnight polysomnography is very appealing and would lead to significant reductions in health care costs, compared with full-night sleep assessments."
Obstructive sleep apnea (OSA) is highly prevalent in the general population, but only 30% of patients referred to a sleep lab for evaluation have severe OSA requiring treatment, said Dr. Moussavi, a professor in the department of electrical and computer engineering at the University of Manitoba, Winnipeg. With no fast, accurate, clinical or laboratory tools for predicting the severity of suspected OSA, full-night polysomnography is required to confirm the diagnosis and determine its severity. "Unfortunately, the demand [for full-night sleep studies] outweighs the available resources, resulting in appointment backlogs and long wait times, which can delay the initiation of potentially lifesaving care," she said.
Acoustic analysis has been used during sleep to evaluate the breathing and snoring patterns of suspected apnea patients. To examine wakeful breathing patterns associated with OSA, Dr. Moussavi and colleagues, recorded the tracheal breath sounds of 35 patients with varying severity of OSA and 17 age-matched controls.
"We recorded the tracheal breath sound in supine and upright positions during nose and mouth breathing," said Dr. Moussavi.
Spectral analysis of the respiratory signals indicated that variation in the average power of the tracheal breath sounds at different positions was a characteristic feature that discriminated the OSA and control groups.
Using the maximum relevancy/minimum redundancy method, the investigators reduced the number of sound features that were significantly different between the groups to two, "and unsupervised clustering of these showed an overall accuracy of 84%, with a sensitivity of 88% and a specificity of 80%," Dr. Moussavi reported.
"It is known that [OSA] patients have a smaller and more collapsible pharynx, which is compensated by increased dilator muscle activity during wakefulness. They tend to have more negative pharyngeal pressure, which can be detected via breathing sounds through the nose because of higher resistance," she said. Because breath sounds are directly related to pharyngeal pressure, "this method is sensitive to the severity of [OSA] even during wakefulness."
The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
FROM THE ANNUAL MEETING OF THE ASSOCIATED PROFESSIONAL SLEEP SOCIETIES
Major Finding: Variation in the average power of tracheal breath sounds at different positions was able to predict the severity of obstructive sleep apnea with an approximate accuracy of 84%, with a sensitivity of 88% and a specificity of 80%.
Data Source: A comparison of acoustic analyses of breath sound data acquired from 35 patients with varying degrees of obstructive sleep apnea and 17 age-matched controls while awake to identify characteristic respiratory features associated with the severity of sleep apnea.
Disclosures: The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
Apnea: Wakeful Analysis Eyed as Polysomnography Alternative
MINNEAPOLIS – An automated analysis of tracheal breath sounds while awake was predictive of obstructive sleep apnea in a small study.
If validated in larger studies, the findings may streamline the obstructive sleep apnea (OSA) screening process, resulting in earlier diagnosis and treatment of severe cases, Zahra Moussavi, Ph.D., said at the annual meeting of the Associated Professional Sleep Societies. "The ability to predict the likelihood and severity of obstructive sleep apnea without performing overnight polysomnography is very appealing and would lead to significant reductions in health care costs, compared with full-night sleep assessments."
Obstructive sleep apnea (OSA) is highly prevalent in the general population, but only 30% of patients referred to a sleep lab for evaluation have severe OSA requiring treatment, said Dr. Moussavi, a professor in the department of electrical and computer engineering at the University of Manitoba, Winnipeg. With no fast, accurate, clinical or laboratory tools for predicting the severity of suspected OSA, full-night polysomnography is required to confirm the diagnosis and determine its severity. "Unfortunately, the demand [for full-night sleep studies] outweighs the available resources, resulting in appointment backlogs and long wait times, which can delay the initiation of potentially lifesaving care," she said.
Acoustic analysis has been used during sleep to evaluate the breathing and snoring patterns of suspected apnea patients. To examine wakeful breathing patterns associated with OSA, Dr. Moussavi and colleagues, recorded the tracheal breath sounds of 35 patients with varying severity of OSA and 17 age-matched controls.
"We recorded the tracheal breath sound in supine and upright positions during nose and mouth breathing," said Dr. Moussavi.
Spectral analysis of the respiratory signals indicated that variation in the average power of the tracheal breath sounds at different positions was a characteristic feature that discriminated the OSA and control groups.
Using the maximum relevancy/minimum redundancy method, the investigators reduced the number of sound features that were significantly different between the groups to two, "and unsupervised clustering of these showed an overall accuracy of 84%, with a sensitivity of 88% and a specificity of 80%," Dr. Moussavi reported.
"It is known that [OSA] patients have a smaller and more collapsible pharynx, which is compensated by increased dilator muscle activity during wakefulness. They tend to have more negative pharyngeal pressure, which can be detected via breathing sounds through the nose because of higher resistance," she said. Because breath sounds are directly related to pharyngeal pressure, "this method is sensitive to the severity of [OSA] even during wakefulness."
The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
MINNEAPOLIS – An automated analysis of tracheal breath sounds while awake was predictive of obstructive sleep apnea in a small study.
If validated in larger studies, the findings may streamline the obstructive sleep apnea (OSA) screening process, resulting in earlier diagnosis and treatment of severe cases, Zahra Moussavi, Ph.D., said at the annual meeting of the Associated Professional Sleep Societies. "The ability to predict the likelihood and severity of obstructive sleep apnea without performing overnight polysomnography is very appealing and would lead to significant reductions in health care costs, compared with full-night sleep assessments."
Obstructive sleep apnea (OSA) is highly prevalent in the general population, but only 30% of patients referred to a sleep lab for evaluation have severe OSA requiring treatment, said Dr. Moussavi, a professor in the department of electrical and computer engineering at the University of Manitoba, Winnipeg. With no fast, accurate, clinical or laboratory tools for predicting the severity of suspected OSA, full-night polysomnography is required to confirm the diagnosis and determine its severity. "Unfortunately, the demand [for full-night sleep studies] outweighs the available resources, resulting in appointment backlogs and long wait times, which can delay the initiation of potentially lifesaving care," she said.
Acoustic analysis has been used during sleep to evaluate the breathing and snoring patterns of suspected apnea patients. To examine wakeful breathing patterns associated with OSA, Dr. Moussavi and colleagues, recorded the tracheal breath sounds of 35 patients with varying severity of OSA and 17 age-matched controls.
"We recorded the tracheal breath sound in supine and upright positions during nose and mouth breathing," said Dr. Moussavi.
Spectral analysis of the respiratory signals indicated that variation in the average power of the tracheal breath sounds at different positions was a characteristic feature that discriminated the OSA and control groups.
Using the maximum relevancy/minimum redundancy method, the investigators reduced the number of sound features that were significantly different between the groups to two, "and unsupervised clustering of these showed an overall accuracy of 84%, with a sensitivity of 88% and a specificity of 80%," Dr. Moussavi reported.
"It is known that [OSA] patients have a smaller and more collapsible pharynx, which is compensated by increased dilator muscle activity during wakefulness. They tend to have more negative pharyngeal pressure, which can be detected via breathing sounds through the nose because of higher resistance," she said. Because breath sounds are directly related to pharyngeal pressure, "this method is sensitive to the severity of [OSA] even during wakefulness."
The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
MINNEAPOLIS – An automated analysis of tracheal breath sounds while awake was predictive of obstructive sleep apnea in a small study.
If validated in larger studies, the findings may streamline the obstructive sleep apnea (OSA) screening process, resulting in earlier diagnosis and treatment of severe cases, Zahra Moussavi, Ph.D., said at the annual meeting of the Associated Professional Sleep Societies. "The ability to predict the likelihood and severity of obstructive sleep apnea without performing overnight polysomnography is very appealing and would lead to significant reductions in health care costs, compared with full-night sleep assessments."
Obstructive sleep apnea (OSA) is highly prevalent in the general population, but only 30% of patients referred to a sleep lab for evaluation have severe OSA requiring treatment, said Dr. Moussavi, a professor in the department of electrical and computer engineering at the University of Manitoba, Winnipeg. With no fast, accurate, clinical or laboratory tools for predicting the severity of suspected OSA, full-night polysomnography is required to confirm the diagnosis and determine its severity. "Unfortunately, the demand [for full-night sleep studies] outweighs the available resources, resulting in appointment backlogs and long wait times, which can delay the initiation of potentially lifesaving care," she said.
Acoustic analysis has been used during sleep to evaluate the breathing and snoring patterns of suspected apnea patients. To examine wakeful breathing patterns associated with OSA, Dr. Moussavi and colleagues, recorded the tracheal breath sounds of 35 patients with varying severity of OSA and 17 age-matched controls.
"We recorded the tracheal breath sound in supine and upright positions during nose and mouth breathing," said Dr. Moussavi.
Spectral analysis of the respiratory signals indicated that variation in the average power of the tracheal breath sounds at different positions was a characteristic feature that discriminated the OSA and control groups.
Using the maximum relevancy/minimum redundancy method, the investigators reduced the number of sound features that were significantly different between the groups to two, "and unsupervised clustering of these showed an overall accuracy of 84%, with a sensitivity of 88% and a specificity of 80%," Dr. Moussavi reported.
"It is known that [OSA] patients have a smaller and more collapsible pharynx, which is compensated by increased dilator muscle activity during wakefulness. They tend to have more negative pharyngeal pressure, which can be detected via breathing sounds through the nose because of higher resistance," she said. Because breath sounds are directly related to pharyngeal pressure, "this method is sensitive to the severity of [OSA] even during wakefulness."
The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
FROM THE ANNUAL MEETING OF THE ASSOCIATED PROFESSIONAL SLEEP SOCIETIES
Major Finding: Variation in the average power of tracheal breath sounds at different positions was able to predict the severity of obstructive sleep apnea with an approximate accuracy of 84%, with a sensitivity of 88% and a specificity of 80%.
Data Source: A comparison of acoustic analyses of breath sound data acquired from 35 patients with varying degrees of obstructive sleep apnea and 17 age-matched controls while awake to identify characteristic respiratory features associated with the severity of sleep apnea.
Disclosures: The study was supported by the National Sciences and Engineering Research Council of Canada and TRI Labs Winnipeg where Dr. Moussavi is an adjunct scientist.
Trends in Use of Nitric Oxide for Congenital Diaphragmatic Hernia Studied
PALM DESERT, CALIF. – Nitric oxide use in neonates with diaphragmatic hernia remains widespread even though its efficacy remains to be proven, results from a large national analysis demonstrated.
"Nitric oxide has been studied extensively in newborns with hypoxemic respiratory failure," Dr. Brendan T. Campbell said at the annual meeting of the American Pediatric Surgical Association. "There have been 14 randomized, controlled trials done in term newborns with respiratory failure, and two of these studies enrolled significant numbers of patients with congenital diaphragmatic hernia. Both studies demonstrated conclusively that treatment with nitric oxide does not improve outcomes in newborns with congenital diaphragmatic hernia."
The first of these studies, he said, found that patients treated with nitric oxide were actually 30% more likely to require extracorporeal membrane oxygenation than were those who did not receive nitric oxide (Pediatrics 1997;99:838-45).
In an effort to describe national trends, interhospital variability in use, and costs associated with nitric oxide use in neonates with congenital diaphragmatic hernia (CDH), a health services research team led by Dr. Campbell analyzed records in the Pediatric Health Information System (PHIS) database. For the years 2003-2010, they identified all patients with a diagnostic code of CDH and a procedural code for CDH repair at 40 children’s hospitals that contribute data to the PHIS. Patients with congenital cardiac anomalies and inaccurate nitric oxide discharge data were excluded from analysis, said Dr. Campbell, a pediatric surgeon at Connecticut Children’s Medical Center, Hartford, who is also with the departments of surgery and pediatrics at the University of Connecticut, Storrs.
A total of 3,651 infants with CDH were identified in the analysis, and 514 with cardiac anomalies and missing or inaccurate data were excluded. The overall mortality rate was 15%, but the mortality rate for the 761 patients treated with nitric oxide was 47%, compared with roughly 5% for the 2,376 patients who were not treated with nitric oxide.
Patients treated with nitric oxide had a significantly longer median length of stay, compared with their counterparts (a median of 31 days vs. 6 days, respectively), and significantly higher median total charges billed (a median of $456,473 vs. $36,270).
Dr. Campbell estimated that the 761 patients treated with nitric oxide generated nearly $34 million in unnecessary hospital charges. "Reducing nitric oxide use in these patients would significantly lower costs without adversely affecting outcomes," he said.
Wide variation in the use of nitric oxide in neonates with CDH existed among the 40 PHIS hospitals. At one hospital, for example, more than 50% were treated with nitric oxide, while the rate was 10% or less at two other PHIS hospitals.
Limitations of the study included its retrospective design and the potential for coding errors and missing data.
Dr. Campbell said that he had no relevant financial conflicts to disclose.
The meeting was supported by a grant from Elsevier, which owns this news organization.
PALM DESERT, CALIF. – Nitric oxide use in neonates with diaphragmatic hernia remains widespread even though its efficacy remains to be proven, results from a large national analysis demonstrated.
"Nitric oxide has been studied extensively in newborns with hypoxemic respiratory failure," Dr. Brendan T. Campbell said at the annual meeting of the American Pediatric Surgical Association. "There have been 14 randomized, controlled trials done in term newborns with respiratory failure, and two of these studies enrolled significant numbers of patients with congenital diaphragmatic hernia. Both studies demonstrated conclusively that treatment with nitric oxide does not improve outcomes in newborns with congenital diaphragmatic hernia."
The first of these studies, he said, found that patients treated with nitric oxide were actually 30% more likely to require extracorporeal membrane oxygenation than were those who did not receive nitric oxide (Pediatrics 1997;99:838-45).
In an effort to describe national trends, interhospital variability in use, and costs associated with nitric oxide use in neonates with congenital diaphragmatic hernia (CDH), a health services research team led by Dr. Campbell analyzed records in the Pediatric Health Information System (PHIS) database. For the years 2003-2010, they identified all patients with a diagnostic code of CDH and a procedural code for CDH repair at 40 children’s hospitals that contribute data to the PHIS. Patients with congenital cardiac anomalies and inaccurate nitric oxide discharge data were excluded from analysis, said Dr. Campbell, a pediatric surgeon at Connecticut Children’s Medical Center, Hartford, who is also with the departments of surgery and pediatrics at the University of Connecticut, Storrs.
A total of 3,651 infants with CDH were identified in the analysis, and 514 with cardiac anomalies and missing or inaccurate data were excluded. The overall mortality rate was 15%, but the mortality rate for the 761 patients treated with nitric oxide was 47%, compared with roughly 5% for the 2,376 patients who were not treated with nitric oxide.
Patients treated with nitric oxide had a significantly longer median length of stay, compared with their counterparts (a median of 31 days vs. 6 days, respectively), and significantly higher median total charges billed (a median of $456,473 vs. $36,270).
Dr. Campbell estimated that the 761 patients treated with nitric oxide generated nearly $34 million in unnecessary hospital charges. "Reducing nitric oxide use in these patients would significantly lower costs without adversely affecting outcomes," he said.
Wide variation in the use of nitric oxide in neonates with CDH existed among the 40 PHIS hospitals. At one hospital, for example, more than 50% were treated with nitric oxide, while the rate was 10% or less at two other PHIS hospitals.
Limitations of the study included its retrospective design and the potential for coding errors and missing data.
Dr. Campbell said that he had no relevant financial conflicts to disclose.
The meeting was supported by a grant from Elsevier, which owns this news organization.
PALM DESERT, CALIF. – Nitric oxide use in neonates with diaphragmatic hernia remains widespread even though its efficacy remains to be proven, results from a large national analysis demonstrated.
"Nitric oxide has been studied extensively in newborns with hypoxemic respiratory failure," Dr. Brendan T. Campbell said at the annual meeting of the American Pediatric Surgical Association. "There have been 14 randomized, controlled trials done in term newborns with respiratory failure, and two of these studies enrolled significant numbers of patients with congenital diaphragmatic hernia. Both studies demonstrated conclusively that treatment with nitric oxide does not improve outcomes in newborns with congenital diaphragmatic hernia."
The first of these studies, he said, found that patients treated with nitric oxide were actually 30% more likely to require extracorporeal membrane oxygenation than were those who did not receive nitric oxide (Pediatrics 1997;99:838-45).
In an effort to describe national trends, interhospital variability in use, and costs associated with nitric oxide use in neonates with congenital diaphragmatic hernia (CDH), a health services research team led by Dr. Campbell analyzed records in the Pediatric Health Information System (PHIS) database. For the years 2003-2010, they identified all patients with a diagnostic code of CDH and a procedural code for CDH repair at 40 children’s hospitals that contribute data to the PHIS. Patients with congenital cardiac anomalies and inaccurate nitric oxide discharge data were excluded from analysis, said Dr. Campbell, a pediatric surgeon at Connecticut Children’s Medical Center, Hartford, who is also with the departments of surgery and pediatrics at the University of Connecticut, Storrs.
A total of 3,651 infants with CDH were identified in the analysis, and 514 with cardiac anomalies and missing or inaccurate data were excluded. The overall mortality rate was 15%, but the mortality rate for the 761 patients treated with nitric oxide was 47%, compared with roughly 5% for the 2,376 patients who were not treated with nitric oxide.
Patients treated with nitric oxide had a significantly longer median length of stay, compared with their counterparts (a median of 31 days vs. 6 days, respectively), and significantly higher median total charges billed (a median of $456,473 vs. $36,270).
Dr. Campbell estimated that the 761 patients treated with nitric oxide generated nearly $34 million in unnecessary hospital charges. "Reducing nitric oxide use in these patients would significantly lower costs without adversely affecting outcomes," he said.
Wide variation in the use of nitric oxide in neonates with CDH existed among the 40 PHIS hospitals. At one hospital, for example, more than 50% were treated with nitric oxide, while the rate was 10% or less at two other PHIS hospitals.
Limitations of the study included its retrospective design and the potential for coding errors and missing data.
Dr. Campbell said that he had no relevant financial conflicts to disclose.
The meeting was supported by a grant from Elsevier, which owns this news organization.
FROM THE ANNUAL MEETING OF THE AMERICAN PEDIATRIC SURGICAL ASSOCIATION
Major Finding: Newborns with congenital diaphragmatic hernia who were treated with nitric oxide had a 47% mortality rate, compared with roughly 5% for patients not treated with nitric oxide.
Data Source: An analysis of 3,137 patients at 40 children’s hospitals that contribute data to the Pediatric Health Information System database.
Disclosures: Dr. Campbell said that he had no relevant financial disclosures to make.
Missed aortic aneurysm proves fatal ... Too-late cancer Dx blamed on neglected x-ray findings... More
Missed dissecting aortic aneurysm proves fatal
A 43-YEAR-OLD MAN was admitted to the hospital complaining of severe chest pain, shortness of breath, sweating, and dry mouth. After being seen by several physicians, the patient suffered an aortic dissection, which caused bleeding in the wall of the aorta, an aortic rupture, and bleeding into the pericardium. He died 2 days later.
PLAINTIFF’S CLAIM The defendants failed to order tests to rule out a dissecting aortic aneurysm and did not include aortic dissection in the differential diagnosis. They failed to provide appropriate drug therapy to decrease cardiac impulse and lower the systolic blood pressure. They did not obtain an emergency cardiac consultation or admit the patient to a cardiovascular surgical intensive care unit.
THE DEFENSE The defendants denied negligence and claimed that nothing they did or failed to do contributed to the patient’s death.
VERDICT $250,000 Michigan settlement.
COMMENT Just yesterday, a malpractice lawyer presented me with a case very similar to this one: a patient with unexplained chest pain who died of a dissecting aneurysm. Remember, not all chest pain is caused by coronary artery disease.
Too-late cancer Dx blamed on neglected x-ray findings
A LONG-TERM CIGARETTE SMOKER IN HER 50s saw a physician in 2001 for symptoms of pneumonia. The doctor prescribed antibiotics and referred her to another facility for a chest radiograph.
Five days later, she returned to the physician’s office, where she was seen by another internist in the practice. The internist noted that the chest radiograph showed parenchymal densities in the right lung. Parenchymal densities had also showed up on 2 previous chest radiographs, but were more prevalent on the latest film. The internist advised the patient to finish her antibiotic regimen; he did not prescribe further tests or treatment.
Over the following 40 months, doctors in the patient’s medical group examined her 8 times. Each time she complained of impaired respiration. The internist believed that the symptoms were caused by asthma.
In 2004, the patient was diagnosed with stage IV cancer of the right lung, which had spread to her bones and was untreatable. She died several weeks later.
PLAINTIFF’S CLAIM A proper diagnosis in 2001 would have allowed the cancer to be cured. A computed tomography scan should have been performed and a pulmonologist consulted at that time.
THE DEFENSE Findings from the radiograph from 2001 did not necessitate further action. Because the patient’s cancer had metastasized before that radiograph, treatment then (or later) would not have changed the outcome.
VERDICT $850,000 New York verdict.
COMMENT Careful follow-up and diagnosis of chest radiograph abnormalities is paramount.
Yes, it was a stroke
WEAKNESS, NUMBNESS, AND TINGLING IN HIS RIGHT ARM prompted a 56-year-old man to visit his primary care physician. The physician sent the patient to the emergency department (ED) for testing because he believed the man was experiencing stroke-like symptoms. As the patient and his wife drove to the hospital, the physician faxed the patient’s medical records to the ED.
When the patient’s wife tried to give ED employees the physician’s orders for tests and tell them of the doctor’s concern about a stroke, they told her that all the beds were full and she should sit down and wait.
The patient was eventually evaluated as a low-priority patient with numbness in his right hand. The examining doctor ordered radiographs of the right wrist and discharged the patient with a diagnosis of carpal tunnel syndrome.
Twenty minutes later, a nurse left a message telling the patient to return to the hospital for the stroke-related tests that had been ordered by his primary care physician. An ED physician other than the one who first examined the patient performed the tests—except for a test of blood flow to the brain. The physician diagnosed stroke-like symptoms and requested a consultation with another physician, which never happened. The patient was discharged about 6 hours after his first discharge.
About 16 hours later, the patient suffered a stroke. Subsequent testing revealed an obstruction in the left carotid artery. The stroke resulted in permanent neurologic injury.
PLAINTIFF’S CLAIM No information about the plaintiff’s claim is available.
THE DEFENSE The defendants denied negligence and disputed the extent of the patient’s injuries.
VERDICT $1.123 million Maryland verdict.
COMMENT Coordination of care remains critical, particularly between our outpatient offices and the busy ED.
Missed dissecting aortic aneurysm proves fatal
A 43-YEAR-OLD MAN was admitted to the hospital complaining of severe chest pain, shortness of breath, sweating, and dry mouth. After being seen by several physicians, the patient suffered an aortic dissection, which caused bleeding in the wall of the aorta, an aortic rupture, and bleeding into the pericardium. He died 2 days later.
PLAINTIFF’S CLAIM The defendants failed to order tests to rule out a dissecting aortic aneurysm and did not include aortic dissection in the differential diagnosis. They failed to provide appropriate drug therapy to decrease cardiac impulse and lower the systolic blood pressure. They did not obtain an emergency cardiac consultation or admit the patient to a cardiovascular surgical intensive care unit.
THE DEFENSE The defendants denied negligence and claimed that nothing they did or failed to do contributed to the patient’s death.
VERDICT $250,000 Michigan settlement.
COMMENT Just yesterday, a malpractice lawyer presented me with a case very similar to this one: a patient with unexplained chest pain who died of a dissecting aneurysm. Remember, not all chest pain is caused by coronary artery disease.
Too-late cancer Dx blamed on neglected x-ray findings
A LONG-TERM CIGARETTE SMOKER IN HER 50s saw a physician in 2001 for symptoms of pneumonia. The doctor prescribed antibiotics and referred her to another facility for a chest radiograph.
Five days later, she returned to the physician’s office, where she was seen by another internist in the practice. The internist noted that the chest radiograph showed parenchymal densities in the right lung. Parenchymal densities had also showed up on 2 previous chest radiographs, but were more prevalent on the latest film. The internist advised the patient to finish her antibiotic regimen; he did not prescribe further tests or treatment.
Over the following 40 months, doctors in the patient’s medical group examined her 8 times. Each time she complained of impaired respiration. The internist believed that the symptoms were caused by asthma.
In 2004, the patient was diagnosed with stage IV cancer of the right lung, which had spread to her bones and was untreatable. She died several weeks later.
PLAINTIFF’S CLAIM A proper diagnosis in 2001 would have allowed the cancer to be cured. A computed tomography scan should have been performed and a pulmonologist consulted at that time.
THE DEFENSE Findings from the radiograph from 2001 did not necessitate further action. Because the patient’s cancer had metastasized before that radiograph, treatment then (or later) would not have changed the outcome.
VERDICT $850,000 New York verdict.
COMMENT Careful follow-up and diagnosis of chest radiograph abnormalities is paramount.
Yes, it was a stroke
WEAKNESS, NUMBNESS, AND TINGLING IN HIS RIGHT ARM prompted a 56-year-old man to visit his primary care physician. The physician sent the patient to the emergency department (ED) for testing because he believed the man was experiencing stroke-like symptoms. As the patient and his wife drove to the hospital, the physician faxed the patient’s medical records to the ED.
When the patient’s wife tried to give ED employees the physician’s orders for tests and tell them of the doctor’s concern about a stroke, they told her that all the beds were full and she should sit down and wait.
The patient was eventually evaluated as a low-priority patient with numbness in his right hand. The examining doctor ordered radiographs of the right wrist and discharged the patient with a diagnosis of carpal tunnel syndrome.
Twenty minutes later, a nurse left a message telling the patient to return to the hospital for the stroke-related tests that had been ordered by his primary care physician. An ED physician other than the one who first examined the patient performed the tests—except for a test of blood flow to the brain. The physician diagnosed stroke-like symptoms and requested a consultation with another physician, which never happened. The patient was discharged about 6 hours after his first discharge.
About 16 hours later, the patient suffered a stroke. Subsequent testing revealed an obstruction in the left carotid artery. The stroke resulted in permanent neurologic injury.
PLAINTIFF’S CLAIM No information about the plaintiff’s claim is available.
THE DEFENSE The defendants denied negligence and disputed the extent of the patient’s injuries.
VERDICT $1.123 million Maryland verdict.
COMMENT Coordination of care remains critical, particularly between our outpatient offices and the busy ED.
Missed dissecting aortic aneurysm proves fatal
A 43-YEAR-OLD MAN was admitted to the hospital complaining of severe chest pain, shortness of breath, sweating, and dry mouth. After being seen by several physicians, the patient suffered an aortic dissection, which caused bleeding in the wall of the aorta, an aortic rupture, and bleeding into the pericardium. He died 2 days later.
PLAINTIFF’S CLAIM The defendants failed to order tests to rule out a dissecting aortic aneurysm and did not include aortic dissection in the differential diagnosis. They failed to provide appropriate drug therapy to decrease cardiac impulse and lower the systolic blood pressure. They did not obtain an emergency cardiac consultation or admit the patient to a cardiovascular surgical intensive care unit.
THE DEFENSE The defendants denied negligence and claimed that nothing they did or failed to do contributed to the patient’s death.
VERDICT $250,000 Michigan settlement.
COMMENT Just yesterday, a malpractice lawyer presented me with a case very similar to this one: a patient with unexplained chest pain who died of a dissecting aneurysm. Remember, not all chest pain is caused by coronary artery disease.
Too-late cancer Dx blamed on neglected x-ray findings
A LONG-TERM CIGARETTE SMOKER IN HER 50s saw a physician in 2001 for symptoms of pneumonia. The doctor prescribed antibiotics and referred her to another facility for a chest radiograph.
Five days later, she returned to the physician’s office, where she was seen by another internist in the practice. The internist noted that the chest radiograph showed parenchymal densities in the right lung. Parenchymal densities had also showed up on 2 previous chest radiographs, but were more prevalent on the latest film. The internist advised the patient to finish her antibiotic regimen; he did not prescribe further tests or treatment.
Over the following 40 months, doctors in the patient’s medical group examined her 8 times. Each time she complained of impaired respiration. The internist believed that the symptoms were caused by asthma.
In 2004, the patient was diagnosed with stage IV cancer of the right lung, which had spread to her bones and was untreatable. She died several weeks later.
PLAINTIFF’S CLAIM A proper diagnosis in 2001 would have allowed the cancer to be cured. A computed tomography scan should have been performed and a pulmonologist consulted at that time.
THE DEFENSE Findings from the radiograph from 2001 did not necessitate further action. Because the patient’s cancer had metastasized before that radiograph, treatment then (or later) would not have changed the outcome.
VERDICT $850,000 New York verdict.
COMMENT Careful follow-up and diagnosis of chest radiograph abnormalities is paramount.
Yes, it was a stroke
WEAKNESS, NUMBNESS, AND TINGLING IN HIS RIGHT ARM prompted a 56-year-old man to visit his primary care physician. The physician sent the patient to the emergency department (ED) for testing because he believed the man was experiencing stroke-like symptoms. As the patient and his wife drove to the hospital, the physician faxed the patient’s medical records to the ED.
When the patient’s wife tried to give ED employees the physician’s orders for tests and tell them of the doctor’s concern about a stroke, they told her that all the beds were full and she should sit down and wait.
The patient was eventually evaluated as a low-priority patient with numbness in his right hand. The examining doctor ordered radiographs of the right wrist and discharged the patient with a diagnosis of carpal tunnel syndrome.
Twenty minutes later, a nurse left a message telling the patient to return to the hospital for the stroke-related tests that had been ordered by his primary care physician. An ED physician other than the one who first examined the patient performed the tests—except for a test of blood flow to the brain. The physician diagnosed stroke-like symptoms and requested a consultation with another physician, which never happened. The patient was discharged about 6 hours after his first discharge.
About 16 hours later, the patient suffered a stroke. Subsequent testing revealed an obstruction in the left carotid artery. The stroke resulted in permanent neurologic injury.
PLAINTIFF’S CLAIM No information about the plaintiff’s claim is available.
THE DEFENSE The defendants denied negligence and disputed the extent of the patient’s injuries.
VERDICT $1.123 million Maryland verdict.
COMMENT Coordination of care remains critical, particularly between our outpatient offices and the busy ED.
Looking beyond the D-dimer
A 44-year-old woman sought care at the emergency department (ED) because she was having difficulty breathing and felt faint. She had been fine until that morning. Three days earlier the patient, who had a history of high blood pressure and elevated cholesterol levels, had driven from Connecticut to New York and back, spending a total of 4 hours in her car. The patient indicated that she’d been taking oral contraceptives (OCPs) for several years, but she did not smoke. There was no history of hemoptysis, recent surgery, or trauma. Neither blood clots nor cancer were part of her or her family’s history.
In the ED, the patient did not have any signs or symptoms of a deep venous thrombosis (DVT). She was obese, with a body mass index of 40.3 kg/m2; other vitals were: blood pressure (BP), 134/88 mm Hg; heart rate (HR), 64 beats per minute (bpm); respiratory rate (RR), 12; and O2 saturation, 99% with ambulation.
The ED physician strongly suspected a pulmonary embolism (PE), but the patient’s score on a clinical probability algorithm (using the Wells criteria) was a 3, indicating only “moderate probability“ of a PE (TABLE 1). (She scored a 3 because an “alternative diagnosis [was] less likely than PE.”) In addition, her D-dimer level was 160 ng/mL using the Triage D-Dimer Test by Biosite, Inc (normal <400 ng/mL), which ruled out a PE. (Many ED physicians at our institution are more cautious when using this D-dimer assay and use a lower cutoff value.)
Given these results, the ED physician did not order imaging studies because the expense and radiation exposure outweighed the probability of the patient having a PE. A subsequent coronary work-up was also negative. The patient was discharged to home and advised to follow up with her primary care physician a few days later.
Two days later we saw the patient at our office. Not only had her dyspnea gotten worse while the presyncope remained, but she now had left-sided pleuritic chest pain. She also reported mild pain in her right calf. On examination, the patient’s BP was 126/86 mm Hg, HR was 82 bpm, RR was 12, and O2 saturation was 96% with ambulation. Her Wells score was now 6, still a moderate probability for PE. (She received another 3 points for the new DVT symptoms—“clinically suspected DVT.”)
Although the patient did not also have signs of a DVT, her additional symptoms along with the original symptoms’ persistence and the existence of other risk factors (OCP use and obesity) led us to reconsider a PE diagnosis. These suspicions prompted us to send the patient back to the ED, where a Doppler ultrasound of the right lower extremity was negative, but the D-dimer was positive at 565 ng/mL.
A pulmonary computed tomography angiogram (CTA) showed 2 small pulmonary emboli within the distal left upper lobe pulmonary arteries.
The patient was treated with heparin and warfarin and discharged without complications.
TABLE 1
Calculating and interpreting the Wells score4,5,7,9,10
| Clinical parameter | Points |
|---|---|
| Clinically suspected DVT | 3.0 |
| Alternative diagnosis less likely than PE | 3.0 |
| Tachycardia | 1.5 |
| Immobilization/surgery (within 4 weeks) | 1.5 |
| History of DVT or PE | 1.5 |
| Hemoptysis | 1.0 |
| Malignancy (treatment within 6 months, palliative) | 1.0 |
| TOTAL | |
| Score | Traditional interpretation |
| <2.0 | Low probability of PE |
| 2.0-6.0 | Moderate probability of PE |
| >6.0 | High probability of PE |
| Score | Alternative classification scheme |
| ≤4.0 | PE unlikely |
| >4.0 | PE likely |
| DVT, deep venous thrombosis; PE, pulmonary embolism. | |
Discussion
The incidence of PE in the United States varies significantly: Individuals younger than 40 have a risk of 1 in 10,000 compared with 1 in 100 for those older than 80.1 Mortality associated with undiagnosed PE varies widely, from 9.2% to 51%.2 This percentage is significant given that half of all PEs go undiagnosed.3 In addition, when left untreated, PE will recur in 30% to 50% of patients, with a fatality rate of 10% to 45%.1 Further, up to 4% of patients with acute PE develop chronic PE and subsequent pulmonary hypertension.4,5 Given the consequences of failing to diagnose a PE, clinicians must consider this condition in patients who present with unexplained hypotension, dyspnea, or chest pain.6
Not an easy diagnosis
This case report demonstrates the inherent difficulty in diagnosing a PE. Still, certain clinical symptoms/signs can aid in the decision-making process. Fever, crackles, and wheezes decrease the probability of PE, whereas syncope, hemodynamic shock, leg edema, and hemoptysis increase its likelihood.7 Despite the many commonly reported risk factors for PE, only malignancy, recent surgery, or a history of DVT/PE significantly increase the risk of developing a clot.8
The Wells criteria. This scoring system groups patients according to the probability of having a PE: low (score: <2), moderate (score: 2-6), and high (score: >6).6 An alternative classification scheme divides patients into 2 groups: likely to have a PE (score: >4) or unlikely to have a PE (score: ≤4).8
This case report illustrates a key problem with the Wells criteria—the somewhat subjective nature of the scoring. Some physicians find it questionable to award 3 points for “alternative diagnosis less likely than PE,” for example.4 Similarly, with respect to immobilization, some clinicians might have awarded our patient 1.5 points for her recent car trip to New York. We did not think that riding in a car for 2 uninterrupted hours for each leg of the trip was significant enough. However, awarding this patient 1.5 points could have made an important difference in her clinical management if the alternative classification scheme was used. Instead of having a score of 3, the patient would have had a score of 4.5, placing her in the “likely to have a PE” group and prompting us to perform a CTA sooner (FIGURE).
FIGURE
Diagnostic algorithm for pulmonary embolism6,7,10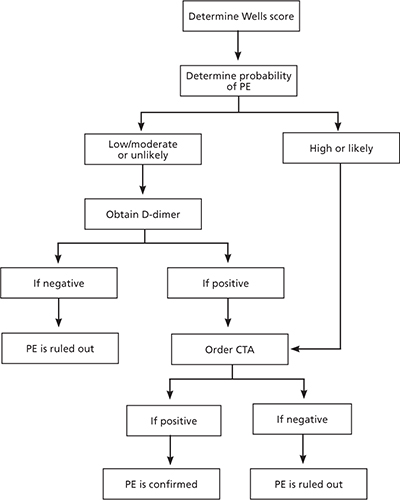
CTA, computed tomography angiogram; PE, pulmonary embolism.
Inappropriate work-ups are common
Some physicians ignore algorithms when working up a PE and simply order a CTA. In fact, a large multicenter trial showed that 43% of patients suspected of having a PE were inappropriately managed diagnostically.9 Similarly, a meta-analysis of 4 studies including 1660 patients found that only 58% of those with a positive D-dimer had the requisite CTA, as did 7% of patients with a negative D-dimer.2
Physicians should not be concerned about ruling out a PE in the setting of a negative D-dimer, as a meta-analysis found that this diagnostic approach has a negative predictive value (NPV) of 99.7%.2 It is important to note that the NPV is significantly affected by the sensitivity of the D-dimer assay used. If the D-dimer assay is highly sensitive, a negative result in combination with a low, moderate, or unlikely probability Wells score rules out the diagnosis of PE. If the assay is moderately sensitive, however, only a low or unlikely probability Wells score rules out PE.10
The inappropriate work-up of this group of patients is significant and extends beyond the ultimate goal of preventing morbidity and mortality. The unnecessary use of pulmonary CTA is extremely expensive, exposes patients to unnecessary radiation, and results in contrast nephrotoxicity in about 4% of patients.9 Although pulmonary CTA is the standard diagnostic test for PE, other imaging modalities are more appropriate in some cases (TABLE 2).
TABLE 2
Alternative imaging modalities for diagnosing PE1,4,7,11
| Modality | Indication |
|---|---|
| Ventilation-perfusion scanning | Patients with contrast allergies or renal failure; test of choice for diagnosing chronic PE due to limited sensitivity of CT |
| Venous compression ultrasonography | Patients with symptoms of PE and signs/symptoms of DVT |
| Pulmonary angiography | Most invasive test. Should be used only in patients with high probability of PE who may need vascular intervention |
| CT, computed tomography; DVT, deep venous thrombosis; PE, pulmonary embolism. | |
The bottom line
This case report illustrates the importance of using sound clinical judgment when diagnosing a PE. Although our patient initially had a moderate probability Wells score and a negative D-dimer, her symptoms persisted. Her history of OCP use, persistent dyspnea, and new symptoms of a DVT prompted us to reinitiate the diagnostic algorithm and eventually diagnose a PE.
It is always essential to treat the patient and not simply react to laboratory values. To avoid unnecessary testing, however, adhering to the algorithm is equally important.
CORRESPONDENCE
Michael S. Kelleher, MD, University of Connecticut School of Medicine, 263 Farmington Avenue, Farmington, CT 06030; mkelleher@student.uchc.edu
1. Meyer G, Roy PM, Gilberg S, et al. Pulmonary embolism. BMJ. 2010;340:1421.-
2. Pasha SM, Kiok FA, Snoep JD, et al. Safety of excluding acute pulmonary embolism based on an unlikely clinical probability by the Wells rule and normal D-dimer concentration: a meta-analysis. Thromb Res. 2010;125:e123-e127.
3. Taira T, Taira BR, Carmen M, et al. Risk of venous thromboembolism in patients with borderline quantitative D-dimer levels. Am J Emerg Med. 2010;28:450-453.
4. Bounameaux H, Perrier A, Righini M. Diagnosis of venous thromboembolism: an update. Vasc Med. 2010;15:399-406.
5. Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350:2257-2264.
6. Agnelli G, Becattini C. Acute pulmonary embolism. N Engl J Med. 2010;363:266-274.
7. Gandara E, Wells PS. Diagnosis: use of clinical probability algorithms. Clin Chest Med. 2010;31:629-639.
8. Drescher FS, Chandrika S, Weir ID, et al. Effectiveness and acceptability of a computerized decision support system using modified wells criteria for evaluation of suspected pulmonary embolism. Ann Emerg Med. 2011;57:613-621.
9. Gimber LH, Travis RI, Takahashi JM, et al. Computed tomography angiography in patients evaluated for acute pulmonary embolism with low serum D-dimer levels: a prospective study. Perm J. 2009;13:4-10.
10. Agency for Healthcare Research and Quality. Guidelines on the diagnosis and management of acute pulmonary embolism. Available at: http://www.guideline.gov/content.aspx?id=13410#Section420. Accessed February 12, 2011.
11. Kim NH. Chronic thromboembolic pulmonary hypertension: diagnosis. Medscape. Available at: http://www.medscape.org/viewarticle/556058_3. Accessed May 9, 2011.
A 44-year-old woman sought care at the emergency department (ED) because she was having difficulty breathing and felt faint. She had been fine until that morning. Three days earlier the patient, who had a history of high blood pressure and elevated cholesterol levels, had driven from Connecticut to New York and back, spending a total of 4 hours in her car. The patient indicated that she’d been taking oral contraceptives (OCPs) for several years, but she did not smoke. There was no history of hemoptysis, recent surgery, or trauma. Neither blood clots nor cancer were part of her or her family’s history.
In the ED, the patient did not have any signs or symptoms of a deep venous thrombosis (DVT). She was obese, with a body mass index of 40.3 kg/m2; other vitals were: blood pressure (BP), 134/88 mm Hg; heart rate (HR), 64 beats per minute (bpm); respiratory rate (RR), 12; and O2 saturation, 99% with ambulation.
The ED physician strongly suspected a pulmonary embolism (PE), but the patient’s score on a clinical probability algorithm (using the Wells criteria) was a 3, indicating only “moderate probability“ of a PE (TABLE 1). (She scored a 3 because an “alternative diagnosis [was] less likely than PE.”) In addition, her D-dimer level was 160 ng/mL using the Triage D-Dimer Test by Biosite, Inc (normal <400 ng/mL), which ruled out a PE. (Many ED physicians at our institution are more cautious when using this D-dimer assay and use a lower cutoff value.)
Given these results, the ED physician did not order imaging studies because the expense and radiation exposure outweighed the probability of the patient having a PE. A subsequent coronary work-up was also negative. The patient was discharged to home and advised to follow up with her primary care physician a few days later.
Two days later we saw the patient at our office. Not only had her dyspnea gotten worse while the presyncope remained, but she now had left-sided pleuritic chest pain. She also reported mild pain in her right calf. On examination, the patient’s BP was 126/86 mm Hg, HR was 82 bpm, RR was 12, and O2 saturation was 96% with ambulation. Her Wells score was now 6, still a moderate probability for PE. (She received another 3 points for the new DVT symptoms—“clinically suspected DVT.”)
Although the patient did not also have signs of a DVT, her additional symptoms along with the original symptoms’ persistence and the existence of other risk factors (OCP use and obesity) led us to reconsider a PE diagnosis. These suspicions prompted us to send the patient back to the ED, where a Doppler ultrasound of the right lower extremity was negative, but the D-dimer was positive at 565 ng/mL.
A pulmonary computed tomography angiogram (CTA) showed 2 small pulmonary emboli within the distal left upper lobe pulmonary arteries.
The patient was treated with heparin and warfarin and discharged without complications.
TABLE 1
Calculating and interpreting the Wells score4,5,7,9,10
| Clinical parameter | Points |
|---|---|
| Clinically suspected DVT | 3.0 |
| Alternative diagnosis less likely than PE | 3.0 |
| Tachycardia | 1.5 |
| Immobilization/surgery (within 4 weeks) | 1.5 |
| History of DVT or PE | 1.5 |
| Hemoptysis | 1.0 |
| Malignancy (treatment within 6 months, palliative) | 1.0 |
| TOTAL | |
| Score | Traditional interpretation |
| <2.0 | Low probability of PE |
| 2.0-6.0 | Moderate probability of PE |
| >6.0 | High probability of PE |
| Score | Alternative classification scheme |
| ≤4.0 | PE unlikely |
| >4.0 | PE likely |
| DVT, deep venous thrombosis; PE, pulmonary embolism. | |
Discussion
The incidence of PE in the United States varies significantly: Individuals younger than 40 have a risk of 1 in 10,000 compared with 1 in 100 for those older than 80.1 Mortality associated with undiagnosed PE varies widely, from 9.2% to 51%.2 This percentage is significant given that half of all PEs go undiagnosed.3 In addition, when left untreated, PE will recur in 30% to 50% of patients, with a fatality rate of 10% to 45%.1 Further, up to 4% of patients with acute PE develop chronic PE and subsequent pulmonary hypertension.4,5 Given the consequences of failing to diagnose a PE, clinicians must consider this condition in patients who present with unexplained hypotension, dyspnea, or chest pain.6
Not an easy diagnosis
This case report demonstrates the inherent difficulty in diagnosing a PE. Still, certain clinical symptoms/signs can aid in the decision-making process. Fever, crackles, and wheezes decrease the probability of PE, whereas syncope, hemodynamic shock, leg edema, and hemoptysis increase its likelihood.7 Despite the many commonly reported risk factors for PE, only malignancy, recent surgery, or a history of DVT/PE significantly increase the risk of developing a clot.8
The Wells criteria. This scoring system groups patients according to the probability of having a PE: low (score: <2), moderate (score: 2-6), and high (score: >6).6 An alternative classification scheme divides patients into 2 groups: likely to have a PE (score: >4) or unlikely to have a PE (score: ≤4).8
This case report illustrates a key problem with the Wells criteria—the somewhat subjective nature of the scoring. Some physicians find it questionable to award 3 points for “alternative diagnosis less likely than PE,” for example.4 Similarly, with respect to immobilization, some clinicians might have awarded our patient 1.5 points for her recent car trip to New York. We did not think that riding in a car for 2 uninterrupted hours for each leg of the trip was significant enough. However, awarding this patient 1.5 points could have made an important difference in her clinical management if the alternative classification scheme was used. Instead of having a score of 3, the patient would have had a score of 4.5, placing her in the “likely to have a PE” group and prompting us to perform a CTA sooner (FIGURE).
FIGURE
Diagnostic algorithm for pulmonary embolism6,7,10
CTA, computed tomography angiogram; PE, pulmonary embolism.
Inappropriate work-ups are common
Some physicians ignore algorithms when working up a PE and simply order a CTA. In fact, a large multicenter trial showed that 43% of patients suspected of having a PE were inappropriately managed diagnostically.9 Similarly, a meta-analysis of 4 studies including 1660 patients found that only 58% of those with a positive D-dimer had the requisite CTA, as did 7% of patients with a negative D-dimer.2
Physicians should not be concerned about ruling out a PE in the setting of a negative D-dimer, as a meta-analysis found that this diagnostic approach has a negative predictive value (NPV) of 99.7%.2 It is important to note that the NPV is significantly affected by the sensitivity of the D-dimer assay used. If the D-dimer assay is highly sensitive, a negative result in combination with a low, moderate, or unlikely probability Wells score rules out the diagnosis of PE. If the assay is moderately sensitive, however, only a low or unlikely probability Wells score rules out PE.10
The inappropriate work-up of this group of patients is significant and extends beyond the ultimate goal of preventing morbidity and mortality. The unnecessary use of pulmonary CTA is extremely expensive, exposes patients to unnecessary radiation, and results in contrast nephrotoxicity in about 4% of patients.9 Although pulmonary CTA is the standard diagnostic test for PE, other imaging modalities are more appropriate in some cases (TABLE 2).
TABLE 2
Alternative imaging modalities for diagnosing PE1,4,7,11
| Modality | Indication |
|---|---|
| Ventilation-perfusion scanning | Patients with contrast allergies or renal failure; test of choice for diagnosing chronic PE due to limited sensitivity of CT |
| Venous compression ultrasonography | Patients with symptoms of PE and signs/symptoms of DVT |
| Pulmonary angiography | Most invasive test. Should be used only in patients with high probability of PE who may need vascular intervention |
| CT, computed tomography; DVT, deep venous thrombosis; PE, pulmonary embolism. | |
The bottom line
This case report illustrates the importance of using sound clinical judgment when diagnosing a PE. Although our patient initially had a moderate probability Wells score and a negative D-dimer, her symptoms persisted. Her history of OCP use, persistent dyspnea, and new symptoms of a DVT prompted us to reinitiate the diagnostic algorithm and eventually diagnose a PE.
It is always essential to treat the patient and not simply react to laboratory values. To avoid unnecessary testing, however, adhering to the algorithm is equally important.
CORRESPONDENCE
Michael S. Kelleher, MD, University of Connecticut School of Medicine, 263 Farmington Avenue, Farmington, CT 06030; mkelleher@student.uchc.edu
A 44-year-old woman sought care at the emergency department (ED) because she was having difficulty breathing and felt faint. She had been fine until that morning. Three days earlier the patient, who had a history of high blood pressure and elevated cholesterol levels, had driven from Connecticut to New York and back, spending a total of 4 hours in her car. The patient indicated that she’d been taking oral contraceptives (OCPs) for several years, but she did not smoke. There was no history of hemoptysis, recent surgery, or trauma. Neither blood clots nor cancer were part of her or her family’s history.
In the ED, the patient did not have any signs or symptoms of a deep venous thrombosis (DVT). She was obese, with a body mass index of 40.3 kg/m2; other vitals were: blood pressure (BP), 134/88 mm Hg; heart rate (HR), 64 beats per minute (bpm); respiratory rate (RR), 12; and O2 saturation, 99% with ambulation.
The ED physician strongly suspected a pulmonary embolism (PE), but the patient’s score on a clinical probability algorithm (using the Wells criteria) was a 3, indicating only “moderate probability“ of a PE (TABLE 1). (She scored a 3 because an “alternative diagnosis [was] less likely than PE.”) In addition, her D-dimer level was 160 ng/mL using the Triage D-Dimer Test by Biosite, Inc (normal <400 ng/mL), which ruled out a PE. (Many ED physicians at our institution are more cautious when using this D-dimer assay and use a lower cutoff value.)
Given these results, the ED physician did not order imaging studies because the expense and radiation exposure outweighed the probability of the patient having a PE. A subsequent coronary work-up was also negative. The patient was discharged to home and advised to follow up with her primary care physician a few days later.
Two days later we saw the patient at our office. Not only had her dyspnea gotten worse while the presyncope remained, but she now had left-sided pleuritic chest pain. She also reported mild pain in her right calf. On examination, the patient’s BP was 126/86 mm Hg, HR was 82 bpm, RR was 12, and O2 saturation was 96% with ambulation. Her Wells score was now 6, still a moderate probability for PE. (She received another 3 points for the new DVT symptoms—“clinically suspected DVT.”)
Although the patient did not also have signs of a DVT, her additional symptoms along with the original symptoms’ persistence and the existence of other risk factors (OCP use and obesity) led us to reconsider a PE diagnosis. These suspicions prompted us to send the patient back to the ED, where a Doppler ultrasound of the right lower extremity was negative, but the D-dimer was positive at 565 ng/mL.
A pulmonary computed tomography angiogram (CTA) showed 2 small pulmonary emboli within the distal left upper lobe pulmonary arteries.
The patient was treated with heparin and warfarin and discharged without complications.
TABLE 1
Calculating and interpreting the Wells score4,5,7,9,10
| Clinical parameter | Points |
|---|---|
| Clinically suspected DVT | 3.0 |
| Alternative diagnosis less likely than PE | 3.0 |
| Tachycardia | 1.5 |
| Immobilization/surgery (within 4 weeks) | 1.5 |
| History of DVT or PE | 1.5 |
| Hemoptysis | 1.0 |
| Malignancy (treatment within 6 months, palliative) | 1.0 |
| TOTAL | |
| Score | Traditional interpretation |
| <2.0 | Low probability of PE |
| 2.0-6.0 | Moderate probability of PE |
| >6.0 | High probability of PE |
| Score | Alternative classification scheme |
| ≤4.0 | PE unlikely |
| >4.0 | PE likely |
| DVT, deep venous thrombosis; PE, pulmonary embolism. | |
Discussion
The incidence of PE in the United States varies significantly: Individuals younger than 40 have a risk of 1 in 10,000 compared with 1 in 100 for those older than 80.1 Mortality associated with undiagnosed PE varies widely, from 9.2% to 51%.2 This percentage is significant given that half of all PEs go undiagnosed.3 In addition, when left untreated, PE will recur in 30% to 50% of patients, with a fatality rate of 10% to 45%.1 Further, up to 4% of patients with acute PE develop chronic PE and subsequent pulmonary hypertension.4,5 Given the consequences of failing to diagnose a PE, clinicians must consider this condition in patients who present with unexplained hypotension, dyspnea, or chest pain.6
Not an easy diagnosis
This case report demonstrates the inherent difficulty in diagnosing a PE. Still, certain clinical symptoms/signs can aid in the decision-making process. Fever, crackles, and wheezes decrease the probability of PE, whereas syncope, hemodynamic shock, leg edema, and hemoptysis increase its likelihood.7 Despite the many commonly reported risk factors for PE, only malignancy, recent surgery, or a history of DVT/PE significantly increase the risk of developing a clot.8
The Wells criteria. This scoring system groups patients according to the probability of having a PE: low (score: <2), moderate (score: 2-6), and high (score: >6).6 An alternative classification scheme divides patients into 2 groups: likely to have a PE (score: >4) or unlikely to have a PE (score: ≤4).8
This case report illustrates a key problem with the Wells criteria—the somewhat subjective nature of the scoring. Some physicians find it questionable to award 3 points for “alternative diagnosis less likely than PE,” for example.4 Similarly, with respect to immobilization, some clinicians might have awarded our patient 1.5 points for her recent car trip to New York. We did not think that riding in a car for 2 uninterrupted hours for each leg of the trip was significant enough. However, awarding this patient 1.5 points could have made an important difference in her clinical management if the alternative classification scheme was used. Instead of having a score of 3, the patient would have had a score of 4.5, placing her in the “likely to have a PE” group and prompting us to perform a CTA sooner (FIGURE).
FIGURE
Diagnostic algorithm for pulmonary embolism6,7,10
CTA, computed tomography angiogram; PE, pulmonary embolism.
Inappropriate work-ups are common
Some physicians ignore algorithms when working up a PE and simply order a CTA. In fact, a large multicenter trial showed that 43% of patients suspected of having a PE were inappropriately managed diagnostically.9 Similarly, a meta-analysis of 4 studies including 1660 patients found that only 58% of those with a positive D-dimer had the requisite CTA, as did 7% of patients with a negative D-dimer.2
Physicians should not be concerned about ruling out a PE in the setting of a negative D-dimer, as a meta-analysis found that this diagnostic approach has a negative predictive value (NPV) of 99.7%.2 It is important to note that the NPV is significantly affected by the sensitivity of the D-dimer assay used. If the D-dimer assay is highly sensitive, a negative result in combination with a low, moderate, or unlikely probability Wells score rules out the diagnosis of PE. If the assay is moderately sensitive, however, only a low or unlikely probability Wells score rules out PE.10
The inappropriate work-up of this group of patients is significant and extends beyond the ultimate goal of preventing morbidity and mortality. The unnecessary use of pulmonary CTA is extremely expensive, exposes patients to unnecessary radiation, and results in contrast nephrotoxicity in about 4% of patients.9 Although pulmonary CTA is the standard diagnostic test for PE, other imaging modalities are more appropriate in some cases (TABLE 2).
TABLE 2
Alternative imaging modalities for diagnosing PE1,4,7,11
| Modality | Indication |
|---|---|
| Ventilation-perfusion scanning | Patients with contrast allergies or renal failure; test of choice for diagnosing chronic PE due to limited sensitivity of CT |
| Venous compression ultrasonography | Patients with symptoms of PE and signs/symptoms of DVT |
| Pulmonary angiography | Most invasive test. Should be used only in patients with high probability of PE who may need vascular intervention |
| CT, computed tomography; DVT, deep venous thrombosis; PE, pulmonary embolism. | |
The bottom line
This case report illustrates the importance of using sound clinical judgment when diagnosing a PE. Although our patient initially had a moderate probability Wells score and a negative D-dimer, her symptoms persisted. Her history of OCP use, persistent dyspnea, and new symptoms of a DVT prompted us to reinitiate the diagnostic algorithm and eventually diagnose a PE.
It is always essential to treat the patient and not simply react to laboratory values. To avoid unnecessary testing, however, adhering to the algorithm is equally important.
CORRESPONDENCE
Michael S. Kelleher, MD, University of Connecticut School of Medicine, 263 Farmington Avenue, Farmington, CT 06030; mkelleher@student.uchc.edu
1. Meyer G, Roy PM, Gilberg S, et al. Pulmonary embolism. BMJ. 2010;340:1421.-
2. Pasha SM, Kiok FA, Snoep JD, et al. Safety of excluding acute pulmonary embolism based on an unlikely clinical probability by the Wells rule and normal D-dimer concentration: a meta-analysis. Thromb Res. 2010;125:e123-e127.
3. Taira T, Taira BR, Carmen M, et al. Risk of venous thromboembolism in patients with borderline quantitative D-dimer levels. Am J Emerg Med. 2010;28:450-453.
4. Bounameaux H, Perrier A, Righini M. Diagnosis of venous thromboembolism: an update. Vasc Med. 2010;15:399-406.
5. Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350:2257-2264.
6. Agnelli G, Becattini C. Acute pulmonary embolism. N Engl J Med. 2010;363:266-274.
7. Gandara E, Wells PS. Diagnosis: use of clinical probability algorithms. Clin Chest Med. 2010;31:629-639.
8. Drescher FS, Chandrika S, Weir ID, et al. Effectiveness and acceptability of a computerized decision support system using modified wells criteria for evaluation of suspected pulmonary embolism. Ann Emerg Med. 2011;57:613-621.
9. Gimber LH, Travis RI, Takahashi JM, et al. Computed tomography angiography in patients evaluated for acute pulmonary embolism with low serum D-dimer levels: a prospective study. Perm J. 2009;13:4-10.
10. Agency for Healthcare Research and Quality. Guidelines on the diagnosis and management of acute pulmonary embolism. Available at: http://www.guideline.gov/content.aspx?id=13410#Section420. Accessed February 12, 2011.
11. Kim NH. Chronic thromboembolic pulmonary hypertension: diagnosis. Medscape. Available at: http://www.medscape.org/viewarticle/556058_3. Accessed May 9, 2011.
1. Meyer G, Roy PM, Gilberg S, et al. Pulmonary embolism. BMJ. 2010;340:1421.-
2. Pasha SM, Kiok FA, Snoep JD, et al. Safety of excluding acute pulmonary embolism based on an unlikely clinical probability by the Wells rule and normal D-dimer concentration: a meta-analysis. Thromb Res. 2010;125:e123-e127.
3. Taira T, Taira BR, Carmen M, et al. Risk of venous thromboembolism in patients with borderline quantitative D-dimer levels. Am J Emerg Med. 2010;28:450-453.
4. Bounameaux H, Perrier A, Righini M. Diagnosis of venous thromboembolism: an update. Vasc Med. 2010;15:399-406.
5. Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350:2257-2264.
6. Agnelli G, Becattini C. Acute pulmonary embolism. N Engl J Med. 2010;363:266-274.
7. Gandara E, Wells PS. Diagnosis: use of clinical probability algorithms. Clin Chest Med. 2010;31:629-639.
8. Drescher FS, Chandrika S, Weir ID, et al. Effectiveness and acceptability of a computerized decision support system using modified wells criteria for evaluation of suspected pulmonary embolism. Ann Emerg Med. 2011;57:613-621.
9. Gimber LH, Travis RI, Takahashi JM, et al. Computed tomography angiography in patients evaluated for acute pulmonary embolism with low serum D-dimer levels: a prospective study. Perm J. 2009;13:4-10.
10. Agency for Healthcare Research and Quality. Guidelines on the diagnosis and management of acute pulmonary embolism. Available at: http://www.guideline.gov/content.aspx?id=13410#Section420. Accessed February 12, 2011.
11. Kim NH. Chronic thromboembolic pulmonary hypertension: diagnosis. Medscape. Available at: http://www.medscape.org/viewarticle/556058_3. Accessed May 9, 2011.
CT Screening Cuts Lung Cancer Mortality; Raises Policy Questions
Final results from the National Lung Screening Trial show a significant reduction in lung cancer mortality with the use of annual low-dose CT screening, compared with standard chest x-rays among former heavy smokers at high risk for lung cancer.
Low-dose CT screening led to a relative reduction of 20% in the rate of death from lung cancer, according to findings released online by the New England Journal of Medicine on June 29 (doi: 10.1056/NEJMoa1102873).The number needed to screen with low-dose CT to prevent one death from lung cancer was 320.
Although preliminary study results were announced in November 2010, the article by the National Lung Screening Trial (NLST) research team marks the first time that the results appear in a peer-reviewed journal. Acknowledging that the earlier announcement has led to calls for lung cancer screening, the authors urge rigorous analysis of cost-effectiveness before public policy recommendations are made.
"The reduction in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote.
In the study, 53,454 men and women aged 55-74 years – who were current or former smokers with a smoking history of at least 30 pack-years – were recruited at 33 U.S. medical centers. A total of 26,722 participants were randomized to receive three annual screens with low-dose helical CT; 26,732 were randomized to three annual screens using chest x-ray. The two groups were virtually identical in demographics and smoking history.
In all three screening rounds, positive screening tests were substantially more common in the low-dose CT group than in the radiography group (27.3% vs. 9.2% in the first round; 27.9% vs. 6.2% in the second; and 16.8% vs. 5% in the third). All told, 39.1% of the CT group and 16% of the radiography group had at least one positive result.
The percentage of screening tests that identified a clinically significant abnormality -- other than an abnormality suspicious for lung cancer – also was more than three times as high in the low-dose CT group as in the radiography group (7.5% vs. 2.1%).
More than 90% of positive screenings in the first round of the study led to a diagnostic evaluation, though the follow-up rates were lower in the later rounds. Diagnostic evaluation most often consisted of additional imaging with invasive procedures being performed infrequently.
Across the three screenings, most of the positive results were false positives – 96.4% in the CT group and 94.5% in the radiography group. Of the total number of low-dose CT screening tests, 24.2% were classified as positive and 23.4% had false-positive results; of the total number of radiographic screening tests, 6.9% were classified as positive and 6.5% were false-positive results.
In all, 1,060 lung cancers were diagnosed in the low-dose CT group (645/100,000 person-years) vs. 941 in the radiography group (572/100,000 person-years). Of these cancers, 649 in the low-dose CT group were diagnosed after a positive screening test and 44 were diagnosed after a negative screening test. In the radiography group, 279 cancers were diagnosed after a positive screening test and 137 were diagnosed after a negative screening test.
In both groups, the remaining cases were among participants who missed screening or were diagnosed after their trial screening phase was over
Analysis of lung cancer-specific mortality showed that in the CT group 356 lung cancer deaths occurred after 144,103 person-years; in the radiography group 443 lung cancer deaths occurred after 143,368 person-years. This corresponded to 247 and 309 lung cancer deaths, respectively, per 100,000 person-years in the CT and radiography groups.
There were 1,877 and 2,000 deaths from all causes in the CT and radiography groups, respectively, "representing a significant reduction with low-dose CT screening of 6.7% ... in the rate of death from any cause," the investigators wrote. While lung cancer accounted for 24.1% of all the deaths in the trial, 60.3% of the excess deaths in the radiography group were due to lung cancer.
The authors concluded that "although some agencies and organizations are contemplating the establishment of lung-cancer screening recommendations on the basis of the findings of the NLST, the current NLST data alone are, in our opinion, insufficient to fully inform such important decisions."
They noted that "The observation that low-dose CT screening can reduce the rate of death from lung cancer has generated many questions." Among these they listed: Will populations with different risk profiles benefit from screening? Could less frequent screening programs be equally effective? Would the use of different criteria for a positive screening result translate to similar benefit? For how long should people be screened?
In an accompanying editorial, Dr. Harold C. Sox, professor of medicine at the Dartmouth Institute in Hanover, N. H., agreed with the investigators’ reservations. In particular, the cost effectiveness of low-dose CT screening for lung cancer must be analyzed, he said: "Policy makers should wait for cost-effectiveness analyses to determine the amount of overdiagnosis in the NLST, and, perhaps identification of biologic markers of cancers that do not progress."
In addition, "it may be possible to define subgroups of smokers who are at higher or lower risk for lung cancer and tailor the screening strategy accordingly," he said. "The findings of the NLST regarding lung-cancer mortality signal the beginning of the end of one era of research on lung-cancer screening and the start of another. The focus will shift to informing the difficult patient-centered and policy decisions that are yet to come."
Dr. Sox also noted that "overdiagnosis is a problem because predicting which early-stage cancers will not progress is in an early stage of development, so that everyone with screen-detected cancer receives treatment that some do not need," he wrote in an accompanying editorial (doi: 10.1056/NEJME1103776).
All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan D. Clap reported having financial interest in Human Genome Sciences. Constantine Gatsonis, Ph.D., is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
This is an exciting
study that does show an impact on mortality, which has not been a screening
result from previous studies. What it doesn’t tell us exactly is: What does
this mean from a policy standpoint?
We need to look at a lot
more to see what’s the best model with this kind of screening and when this is
screening appropriate. I think the authors of this study were right to say that
this is a very positive result and it’s helpful … but that the best way to
implement this in day-to-day practice still is not completely resolved. There’s
a lot more work to be done in that regard.
One message that is still
very clear is that if you don’t want to die from lung cancer, you need to stop
smoking or never start smoking. This still has to be foremost in our public
health preventative message.
The study results do help
by saying that screening can have a role in day-to-day practice. The fact that
these patients were treated in a community setting showed that … the process
for diagnosing lung cancer can be handled by community physicians. I’m a
pulmonary physician. So when I sit down with patients who have the risk of
smoking, and we talk about what is the role of getting a low-dose CT scan for
screening, I think I have a lot more information to help both me and the
patient to decide whether this is beneficial to them versus a risk.
In the past, with CT
screening there was certainly risk from the radiation and risks for having
unnecessary procedures done, but no real proven benefit that we were going to
impact mortality if we found an early cancer. The study results do add value on
a day-to-day basis.
We just don’t know whether
it’s something that should be applied to everybody. Another question is whether
there are there markers that might help in this group of individuals to
identify who is at high risk for fast-growing tumors or for slow-growing tumors
Are there biologic markers that we can find with a blood test that might add to
this information to help us sort out who would benefit from screening or not?
[Other questions to
answer] from these data or from other ongoing studies include: Are there
subgroups of this 55- to 74-year-old population that are at higher risk? Are
there individuals who with less frequent screening can do just as well? Are
there individuals for whom more screening is necessary? The population looked
at [in the study] was a narrow window of high-risk individuals … It represents
about 7 million people out of the 94 million current and former smokers that we
have in this country.
We may even be able to
look at genetic markers at some point in the near future to determine who is at
higher risk and that will help us better identify who needs to be screened. I
think biomarkers and genetic markers all could be added to the formula when
we’re trying to decide what the best risk population to be screened is.
Screening tools work best when the screening population is well defined.
So now we have evidence
that screening in general can have an impact on disease. Unfortunately, prior
to this, lung cancer was diagnosed too late to make a big impact for most
patients. In lung cancer, an earlier diagnosis hopefully impacts mortality.
Lung cancer could become a curable disease if it’s found early enough to be
completely resected.
Dr. Albert A. Rizzo is
chair-elect of the American Lung Association board and chief of Christiana
Care’s pulmonary and critical care medicine section in Newark, Del.
He has no conflicts of interest.
This is an exciting
study that does show an impact on mortality, which has not been a screening
result from previous studies. What it doesn’t tell us exactly is: What does
this mean from a policy standpoint?
We need to look at a lot
more to see what’s the best model with this kind of screening and when this is
screening appropriate. I think the authors of this study were right to say that
this is a very positive result and it’s helpful … but that the best way to
implement this in day-to-day practice still is not completely resolved. There’s
a lot more work to be done in that regard.
One message that is still
very clear is that if you don’t want to die from lung cancer, you need to stop
smoking or never start smoking. This still has to be foremost in our public
health preventative message.
The study results do help
by saying that screening can have a role in day-to-day practice. The fact that
these patients were treated in a community setting showed that … the process
for diagnosing lung cancer can be handled by community physicians. I’m a
pulmonary physician. So when I sit down with patients who have the risk of
smoking, and we talk about what is the role of getting a low-dose CT scan for
screening, I think I have a lot more information to help both me and the
patient to decide whether this is beneficial to them versus a risk.
In the past, with CT
screening there was certainly risk from the radiation and risks for having
unnecessary procedures done, but no real proven benefit that we were going to
impact mortality if we found an early cancer. The study results do add value on
a day-to-day basis.
We just don’t know whether
it’s something that should be applied to everybody. Another question is whether
there are there markers that might help in this group of individuals to
identify who is at high risk for fast-growing tumors or for slow-growing tumors
Are there biologic markers that we can find with a blood test that might add to
this information to help us sort out who would benefit from screening or not?
[Other questions to
answer] from these data or from other ongoing studies include: Are there
subgroups of this 55- to 74-year-old population that are at higher risk? Are
there individuals who with less frequent screening can do just as well? Are
there individuals for whom more screening is necessary? The population looked
at [in the study] was a narrow window of high-risk individuals … It represents
about 7 million people out of the 94 million current and former smokers that we
have in this country.
We may even be able to
look at genetic markers at some point in the near future to determine who is at
higher risk and that will help us better identify who needs to be screened. I
think biomarkers and genetic markers all could be added to the formula when
we’re trying to decide what the best risk population to be screened is.
Screening tools work best when the screening population is well defined.
So now we have evidence
that screening in general can have an impact on disease. Unfortunately, prior
to this, lung cancer was diagnosed too late to make a big impact for most
patients. In lung cancer, an earlier diagnosis hopefully impacts mortality.
Lung cancer could become a curable disease if it’s found early enough to be
completely resected.
Dr. Albert A. Rizzo is
chair-elect of the American Lung Association board and chief of Christiana
Care’s pulmonary and critical care medicine section in Newark, Del.
He has no conflicts of interest.
This is an exciting
study that does show an impact on mortality, which has not been a screening
result from previous studies. What it doesn’t tell us exactly is: What does
this mean from a policy standpoint?
We need to look at a lot
more to see what’s the best model with this kind of screening and when this is
screening appropriate. I think the authors of this study were right to say that
this is a very positive result and it’s helpful … but that the best way to
implement this in day-to-day practice still is not completely resolved. There’s
a lot more work to be done in that regard.
One message that is still
very clear is that if you don’t want to die from lung cancer, you need to stop
smoking or never start smoking. This still has to be foremost in our public
health preventative message.
The study results do help
by saying that screening can have a role in day-to-day practice. The fact that
these patients were treated in a community setting showed that … the process
for diagnosing lung cancer can be handled by community physicians. I’m a
pulmonary physician. So when I sit down with patients who have the risk of
smoking, and we talk about what is the role of getting a low-dose CT scan for
screening, I think I have a lot more information to help both me and the
patient to decide whether this is beneficial to them versus a risk.
In the past, with CT
screening there was certainly risk from the radiation and risks for having
unnecessary procedures done, but no real proven benefit that we were going to
impact mortality if we found an early cancer. The study results do add value on
a day-to-day basis.
We just don’t know whether
it’s something that should be applied to everybody. Another question is whether
there are there markers that might help in this group of individuals to
identify who is at high risk for fast-growing tumors or for slow-growing tumors
Are there biologic markers that we can find with a blood test that might add to
this information to help us sort out who would benefit from screening or not?
[Other questions to
answer] from these data or from other ongoing studies include: Are there
subgroups of this 55- to 74-year-old population that are at higher risk? Are
there individuals who with less frequent screening can do just as well? Are
there individuals for whom more screening is necessary? The population looked
at [in the study] was a narrow window of high-risk individuals … It represents
about 7 million people out of the 94 million current and former smokers that we
have in this country.
We may even be able to
look at genetic markers at some point in the near future to determine who is at
higher risk and that will help us better identify who needs to be screened. I
think biomarkers and genetic markers all could be added to the formula when
we’re trying to decide what the best risk population to be screened is.
Screening tools work best when the screening population is well defined.
So now we have evidence
that screening in general can have an impact on disease. Unfortunately, prior
to this, lung cancer was diagnosed too late to make a big impact for most
patients. In lung cancer, an earlier diagnosis hopefully impacts mortality.
Lung cancer could become a curable disease if it’s found early enough to be
completely resected.
Dr. Albert A. Rizzo is
chair-elect of the American Lung Association board and chief of Christiana
Care’s pulmonary and critical care medicine section in Newark, Del.
He has no conflicts of interest.
Final results from the National Lung Screening Trial show a significant reduction in lung cancer mortality with the use of annual low-dose CT screening, compared with standard chest x-rays among former heavy smokers at high risk for lung cancer.
Low-dose CT screening led to a relative reduction of 20% in the rate of death from lung cancer, according to findings released online by the New England Journal of Medicine on June 29 (doi: 10.1056/NEJMoa1102873).The number needed to screen with low-dose CT to prevent one death from lung cancer was 320.
Although preliminary study results were announced in November 2010, the article by the National Lung Screening Trial (NLST) research team marks the first time that the results appear in a peer-reviewed journal. Acknowledging that the earlier announcement has led to calls for lung cancer screening, the authors urge rigorous analysis of cost-effectiveness before public policy recommendations are made.
"The reduction in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote.
In the study, 53,454 men and women aged 55-74 years – who were current or former smokers with a smoking history of at least 30 pack-years – were recruited at 33 U.S. medical centers. A total of 26,722 participants were randomized to receive three annual screens with low-dose helical CT; 26,732 were randomized to three annual screens using chest x-ray. The two groups were virtually identical in demographics and smoking history.
In all three screening rounds, positive screening tests were substantially more common in the low-dose CT group than in the radiography group (27.3% vs. 9.2% in the first round; 27.9% vs. 6.2% in the second; and 16.8% vs. 5% in the third). All told, 39.1% of the CT group and 16% of the radiography group had at least one positive result.
The percentage of screening tests that identified a clinically significant abnormality -- other than an abnormality suspicious for lung cancer – also was more than three times as high in the low-dose CT group as in the radiography group (7.5% vs. 2.1%).
More than 90% of positive screenings in the first round of the study led to a diagnostic evaluation, though the follow-up rates were lower in the later rounds. Diagnostic evaluation most often consisted of additional imaging with invasive procedures being performed infrequently.
Across the three screenings, most of the positive results were false positives – 96.4% in the CT group and 94.5% in the radiography group. Of the total number of low-dose CT screening tests, 24.2% were classified as positive and 23.4% had false-positive results; of the total number of radiographic screening tests, 6.9% were classified as positive and 6.5% were false-positive results.
In all, 1,060 lung cancers were diagnosed in the low-dose CT group (645/100,000 person-years) vs. 941 in the radiography group (572/100,000 person-years). Of these cancers, 649 in the low-dose CT group were diagnosed after a positive screening test and 44 were diagnosed after a negative screening test. In the radiography group, 279 cancers were diagnosed after a positive screening test and 137 were diagnosed after a negative screening test.
In both groups, the remaining cases were among participants who missed screening or were diagnosed after their trial screening phase was over
Analysis of lung cancer-specific mortality showed that in the CT group 356 lung cancer deaths occurred after 144,103 person-years; in the radiography group 443 lung cancer deaths occurred after 143,368 person-years. This corresponded to 247 and 309 lung cancer deaths, respectively, per 100,000 person-years in the CT and radiography groups.
There were 1,877 and 2,000 deaths from all causes in the CT and radiography groups, respectively, "representing a significant reduction with low-dose CT screening of 6.7% ... in the rate of death from any cause," the investigators wrote. While lung cancer accounted for 24.1% of all the deaths in the trial, 60.3% of the excess deaths in the radiography group were due to lung cancer.
The authors concluded that "although some agencies and organizations are contemplating the establishment of lung-cancer screening recommendations on the basis of the findings of the NLST, the current NLST data alone are, in our opinion, insufficient to fully inform such important decisions."
They noted that "The observation that low-dose CT screening can reduce the rate of death from lung cancer has generated many questions." Among these they listed: Will populations with different risk profiles benefit from screening? Could less frequent screening programs be equally effective? Would the use of different criteria for a positive screening result translate to similar benefit? For how long should people be screened?
In an accompanying editorial, Dr. Harold C. Sox, professor of medicine at the Dartmouth Institute in Hanover, N. H., agreed with the investigators’ reservations. In particular, the cost effectiveness of low-dose CT screening for lung cancer must be analyzed, he said: "Policy makers should wait for cost-effectiveness analyses to determine the amount of overdiagnosis in the NLST, and, perhaps identification of biologic markers of cancers that do not progress."
In addition, "it may be possible to define subgroups of smokers who are at higher or lower risk for lung cancer and tailor the screening strategy accordingly," he said. "The findings of the NLST regarding lung-cancer mortality signal the beginning of the end of one era of research on lung-cancer screening and the start of another. The focus will shift to informing the difficult patient-centered and policy decisions that are yet to come."
Dr. Sox also noted that "overdiagnosis is a problem because predicting which early-stage cancers will not progress is in an early stage of development, so that everyone with screen-detected cancer receives treatment that some do not need," he wrote in an accompanying editorial (doi: 10.1056/NEJME1103776).
All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan D. Clap reported having financial interest in Human Genome Sciences. Constantine Gatsonis, Ph.D., is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
Final results from the National Lung Screening Trial show a significant reduction in lung cancer mortality with the use of annual low-dose CT screening, compared with standard chest x-rays among former heavy smokers at high risk for lung cancer.
Low-dose CT screening led to a relative reduction of 20% in the rate of death from lung cancer, according to findings released online by the New England Journal of Medicine on June 29 (doi: 10.1056/NEJMoa1102873).The number needed to screen with low-dose CT to prevent one death from lung cancer was 320.
Although preliminary study results were announced in November 2010, the article by the National Lung Screening Trial (NLST) research team marks the first time that the results appear in a peer-reviewed journal. Acknowledging that the earlier announcement has led to calls for lung cancer screening, the authors urge rigorous analysis of cost-effectiveness before public policy recommendations are made.
"The reduction in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote.
In the study, 53,454 men and women aged 55-74 years – who were current or former smokers with a smoking history of at least 30 pack-years – were recruited at 33 U.S. medical centers. A total of 26,722 participants were randomized to receive three annual screens with low-dose helical CT; 26,732 were randomized to three annual screens using chest x-ray. The two groups were virtually identical in demographics and smoking history.
In all three screening rounds, positive screening tests were substantially more common in the low-dose CT group than in the radiography group (27.3% vs. 9.2% in the first round; 27.9% vs. 6.2% in the second; and 16.8% vs. 5% in the third). All told, 39.1% of the CT group and 16% of the radiography group had at least one positive result.
The percentage of screening tests that identified a clinically significant abnormality -- other than an abnormality suspicious for lung cancer – also was more than three times as high in the low-dose CT group as in the radiography group (7.5% vs. 2.1%).
More than 90% of positive screenings in the first round of the study led to a diagnostic evaluation, though the follow-up rates were lower in the later rounds. Diagnostic evaluation most often consisted of additional imaging with invasive procedures being performed infrequently.
Across the three screenings, most of the positive results were false positives – 96.4% in the CT group and 94.5% in the radiography group. Of the total number of low-dose CT screening tests, 24.2% were classified as positive and 23.4% had false-positive results; of the total number of radiographic screening tests, 6.9% were classified as positive and 6.5% were false-positive results.
In all, 1,060 lung cancers were diagnosed in the low-dose CT group (645/100,000 person-years) vs. 941 in the radiography group (572/100,000 person-years). Of these cancers, 649 in the low-dose CT group were diagnosed after a positive screening test and 44 were diagnosed after a negative screening test. In the radiography group, 279 cancers were diagnosed after a positive screening test and 137 were diagnosed after a negative screening test.
In both groups, the remaining cases were among participants who missed screening or were diagnosed after their trial screening phase was over
Analysis of lung cancer-specific mortality showed that in the CT group 356 lung cancer deaths occurred after 144,103 person-years; in the radiography group 443 lung cancer deaths occurred after 143,368 person-years. This corresponded to 247 and 309 lung cancer deaths, respectively, per 100,000 person-years in the CT and radiography groups.
There were 1,877 and 2,000 deaths from all causes in the CT and radiography groups, respectively, "representing a significant reduction with low-dose CT screening of 6.7% ... in the rate of death from any cause," the investigators wrote. While lung cancer accounted for 24.1% of all the deaths in the trial, 60.3% of the excess deaths in the radiography group were due to lung cancer.
The authors concluded that "although some agencies and organizations are contemplating the establishment of lung-cancer screening recommendations on the basis of the findings of the NLST, the current NLST data alone are, in our opinion, insufficient to fully inform such important decisions."
They noted that "The observation that low-dose CT screening can reduce the rate of death from lung cancer has generated many questions." Among these they listed: Will populations with different risk profiles benefit from screening? Could less frequent screening programs be equally effective? Would the use of different criteria for a positive screening result translate to similar benefit? For how long should people be screened?
In an accompanying editorial, Dr. Harold C. Sox, professor of medicine at the Dartmouth Institute in Hanover, N. H., agreed with the investigators’ reservations. In particular, the cost effectiveness of low-dose CT screening for lung cancer must be analyzed, he said: "Policy makers should wait for cost-effectiveness analyses to determine the amount of overdiagnosis in the NLST, and, perhaps identification of biologic markers of cancers that do not progress."
In addition, "it may be possible to define subgroups of smokers who are at higher or lower risk for lung cancer and tailor the screening strategy accordingly," he said. "The findings of the NLST regarding lung-cancer mortality signal the beginning of the end of one era of research on lung-cancer screening and the start of another. The focus will shift to informing the difficult patient-centered and policy decisions that are yet to come."
Dr. Sox also noted that "overdiagnosis is a problem because predicting which early-stage cancers will not progress is in an early stage of development, so that everyone with screen-detected cancer receives treatment that some do not need," he wrote in an accompanying editorial (doi: 10.1056/NEJME1103776).
All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan D. Clap reported having financial interest in Human Genome Sciences. Constantine Gatsonis, Ph.D., is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Low-dose CT screening reduced the relative rate of death from lung cancer by 20%, compared with chest x-ray screening.
Data Source: A study of 53,454 Americans aged 55-74 years, who were current or former smokers with a smoking history of at least 30 pack-years.
Disclosures: All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan Clap reported having financial interest in Human Genome Sciences Inc. Constantine Gatsonis is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health, and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
CT Screening Cuts Lung Cancer Mortality; Raises Policy Questions
Final results from the National Lung Screening Trial show a significant reduction in lung cancer mortality with the use of annual low-dose CT screening, compared with standard chest x-rays among former heavy smokers at high risk for lung cancer.
Low-dose CT screening led to a relative reduction of 20% in the rate of death from lung cancer, according to findings released online by the New England Journal of Medicine on June 29 (doi: 10.1056/NEJMoa1102873).The number needed to screen with low-dose CT to prevent one death from lung cancer was 320.
Although preliminary study results were announced in November 2010, the article by the National Lung Screening Trial (NLST) research team marks the first time that the results appear in a peer-reviewed journal. Acknowledging that the earlier announcement has led to calls for lung cancer screening, the authors urge rigorous analysis of cost-effectiveness before public policy recommendations are made.
"The reduction in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote.
In the study, 53,454 men and women aged 55-74 years – who were current or former smokers with a smoking history of at least 30 pack-years – were recruited at 33 U.S. medical centers. A total of 26,722 participants were randomized to receive three annual screens with low-dose helical CT; 26,732 were randomized to three annual screens using chest x-ray. The two groups were virtually identical in demographics and smoking history.
In all three screening rounds, positive screening tests were substantially more common in the low-dose CT group than in the radiography group (27.3% vs. 9.2% in the first round; 27.9% vs. 6.2% in the second; and 16.8% vs. 5% in the third). All told, 39.1% of the CT group and 16% of the radiography group had at least one positive result.
The percentage of screening tests that identified a clinically significant abnormality -- other than an abnormality suspicious for lung cancer – also was more than three times as high in the low-dose CT group as in the radiography group (7.5% vs. 2.1%).
More than 90% of positive screenings in the first round of the study led to a diagnostic evaluation, though the follow-up rates were lower in the later rounds. Diagnostic evaluation most often consisted of additional imaging with invasive procedures being performed infrequently.
Across the three screenings, most of the positive results were false positives – 96.4% in the CT group and 94.5% in the radiography group. Of the total number of low-dose CT screening tests, 24.2% were classified as positive and 23.4% had false-positive results; of the total number of radiographic screening tests, 6.9% were classified as positive and 6.5% were false-positive results.
In all, 1,060 lung cancers were diagnosed in the low-dose CT group (645/100,000 person-years) vs. 941 in the radiography group (572/100,000 person-years). Of these cancers, 649 in the low-dose CT group were diagnosed after a positive screening test and 44 were diagnosed after a negative screening test. In the radiography group, 279 cancers were diagnosed after a positive screening test and 137 were diagnosed after a negative screening test.
In both groups, the remaining cases were among participants who missed screening or were diagnosed after their trial screening phase was over
Analysis of lung cancer-specific mortality showed that in the CT group 356 lung cancer deaths occurred after 144,103 person-years; in the radiography group 443 lung cancer deaths occurred after 143,368 person-years. This corresponded to 247 and 309 lung cancer deaths, respectively, per 100,000 person-years in the CT and radiography groups.
There were 1,877 and 2,000 deaths from all causes in the CT and radiography groups, respectively, "representing a significant reduction with low-dose CT screening of 6.7% ... in the rate of death from any cause," the investigators wrote. While lung cancer accounted for 24.1% of all the deaths in the trial, 60.3% of the excess deaths in the radiography group were due to lung cancer.
The authors concluded that "although some agencies and organizations are contemplating the establishment of lung-cancer screening recommendations on the basis of the findings of the NLST, the current NLST data alone are, in our opinion, insufficient to fully inform such important decisions."
They noted that "The observation that low-dose CT screening can reduce the rate of death from lung cancer has generated many questions." Among these they listed: Will populations with different risk profiles benefit from screening? Could less frequent screening programs be equally effective? Would the use of different criteria for a positive screening result translate to similar benefit? For how long should people be screened?
In an accompanying editorial, Dr. Harold C. Sox, professor of medicine at the Dartmouth Institute in Hanover, N. H., agreed with the investigators’ reservations. In particular, the cost effectiveness of low-dose CT screening for lung cancer must be analyzed, he said: "Policy makers should wait for cost-effectiveness analyses to determine the amount of overdiagnosis in the NLST, and, perhaps identification of biologic markers of cancers that do not progress."
In addition, "it may be possible to define subgroups of smokers who are at higher or lower risk for lung cancer and tailor the screening strategy accordingly," he said. "The findings of the NLST regarding lung-cancer mortality signal the beginning of the end of one era of research on lung-cancer screening and the start of another. The focus will shift to informing the difficult patient-centered and policy decisions that are yet to come."
Dr. Sox also noted that "overdiagnosis is a problem because predicting which early-stage cancers will not progress is in an early stage of development, so that everyone with screen-detected cancer receives treatment that some do not need," he wrote in an accompanying editorial (doi: 10.1056/NEJME1103776).
All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan D. Clap reported having financial interest in Human Genome Sciences. Constantine Gatsonis, Ph.D., is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
This is an exciting
study that does show an impact on mortality, which has not been a screening
result from previous studies. What it doesn’t tell us exactly is: What does
this mean from a policy standpoint?
We need to look at a lot
more to see what’s the best model with this kind of screening and when this is
screening appropriate. I think the authors of this study were right to say that
this is a very positive result and it’s helpful … but that the best way to
implement this in day-to-day practice still is not completely resolved. There’s
a lot more work to be done in that regard.
One message that is still
very clear is that if you don’t want to die from lung cancer, you need to stop
smoking or never start smoking. This still has to be foremost in our public
health preventative message.
The study results do help
by saying that screening can have a role in day-to-day practice. The fact that
these patients were treated in a community setting showed that … the process
for diagnosing lung cancer can be handled by community physicians. I’m a
pulmonary physician. So when I sit down with patients who have the risk of
smoking, and we talk about what is the role of getting a low-dose CT scan for
screening, I think I have a lot more information to help both me and the
patient to decide whether this is beneficial to them versus a risk.
In the past, with CT
screening there was certainly risk from the radiation and risks for having
unnecessary procedures done, but no real proven benefit that we were going to
impact mortality if we found an early cancer. The study results do add value on
a day-to-day basis.
We just don’t know whether
it’s something that should be applied to everybody. Another question is whether
there are there markers that might help in this group of individuals to
identify who is at high risk for fast-growing tumors or for slow-growing tumors
Are there biologic markers that we can find with a blood test that might add to
this information to help us sort out who would benefit from screening or not?
[Other questions to
answer] from these data or from other ongoing studies include: Are there
subgroups of this 55- to 74-year-old population that are at higher risk? Are
there individuals who with less frequent screening can do just as well? Are
there individuals for whom more screening is necessary? The population looked
at [in the study] was a narrow window of high-risk individuals … It represents
about 7 million people out of the 94 million current and former smokers that we
have in this country.
We may even be able to
look at genetic markers at some point in the near future to determine who is at
higher risk and that will help us better identify who needs to be screened. I
think biomarkers and genetic markers all could be added to the formula when
we’re trying to decide what the best risk population to be screened is.
Screening tools work best when the screening population is well defined.
So now we have evidence
that screening in general can have an impact on disease. Unfortunately, prior
to this, lung cancer was diagnosed too late to make a big impact for most
patients. In lung cancer, an earlier diagnosis hopefully impacts mortality.
Lung cancer could become a curable disease if it’s found early enough to be
completely resected.
Dr. Albert A. Rizzo is
chair-elect of the American Lung Association board and chief of Christiana
Care’s pulmonary and critical care medicine section in Newark, Del.
He has no conflicts of interest.
This is an exciting
study that does show an impact on mortality, which has not been a screening
result from previous studies. What it doesn’t tell us exactly is: What does
this mean from a policy standpoint?
We need to look at a lot
more to see what’s the best model with this kind of screening and when this is
screening appropriate. I think the authors of this study were right to say that
this is a very positive result and it’s helpful … but that the best way to
implement this in day-to-day practice still is not completely resolved. There’s
a lot more work to be done in that regard.
One message that is still
very clear is that if you don’t want to die from lung cancer, you need to stop
smoking or never start smoking. This still has to be foremost in our public
health preventative message.
The study results do help
by saying that screening can have a role in day-to-day practice. The fact that
these patients were treated in a community setting showed that … the process
for diagnosing lung cancer can be handled by community physicians. I’m a
pulmonary physician. So when I sit down with patients who have the risk of
smoking, and we talk about what is the role of getting a low-dose CT scan for
screening, I think I have a lot more information to help both me and the
patient to decide whether this is beneficial to them versus a risk.
In the past, with CT
screening there was certainly risk from the radiation and risks for having
unnecessary procedures done, but no real proven benefit that we were going to
impact mortality if we found an early cancer. The study results do add value on
a day-to-day basis.
We just don’t know whether
it’s something that should be applied to everybody. Another question is whether
there are there markers that might help in this group of individuals to
identify who is at high risk for fast-growing tumors or for slow-growing tumors
Are there biologic markers that we can find with a blood test that might add to
this information to help us sort out who would benefit from screening or not?
[Other questions to
answer] from these data or from other ongoing studies include: Are there
subgroups of this 55- to 74-year-old population that are at higher risk? Are
there individuals who with less frequent screening can do just as well? Are
there individuals for whom more screening is necessary? The population looked
at [in the study] was a narrow window of high-risk individuals … It represents
about 7 million people out of the 94 million current and former smokers that we
have in this country.
We may even be able to
look at genetic markers at some point in the near future to determine who is at
higher risk and that will help us better identify who needs to be screened. I
think biomarkers and genetic markers all could be added to the formula when
we’re trying to decide what the best risk population to be screened is.
Screening tools work best when the screening population is well defined.
So now we have evidence
that screening in general can have an impact on disease. Unfortunately, prior
to this, lung cancer was diagnosed too late to make a big impact for most
patients. In lung cancer, an earlier diagnosis hopefully impacts mortality.
Lung cancer could become a curable disease if it’s found early enough to be
completely resected.
Dr. Albert A. Rizzo is
chair-elect of the American Lung Association board and chief of Christiana
Care’s pulmonary and critical care medicine section in Newark, Del.
He has no conflicts of interest.
This is an exciting
study that does show an impact on mortality, which has not been a screening
result from previous studies. What it doesn’t tell us exactly is: What does
this mean from a policy standpoint?
We need to look at a lot
more to see what’s the best model with this kind of screening and when this is
screening appropriate. I think the authors of this study were right to say that
this is a very positive result and it’s helpful … but that the best way to
implement this in day-to-day practice still is not completely resolved. There’s
a lot more work to be done in that regard.
One message that is still
very clear is that if you don’t want to die from lung cancer, you need to stop
smoking or never start smoking. This still has to be foremost in our public
health preventative message.
The study results do help
by saying that screening can have a role in day-to-day practice. The fact that
these patients were treated in a community setting showed that … the process
for diagnosing lung cancer can be handled by community physicians. I’m a
pulmonary physician. So when I sit down with patients who have the risk of
smoking, and we talk about what is the role of getting a low-dose CT scan for
screening, I think I have a lot more information to help both me and the
patient to decide whether this is beneficial to them versus a risk.
In the past, with CT
screening there was certainly risk from the radiation and risks for having
unnecessary procedures done, but no real proven benefit that we were going to
impact mortality if we found an early cancer. The study results do add value on
a day-to-day basis.
We just don’t know whether
it’s something that should be applied to everybody. Another question is whether
there are there markers that might help in this group of individuals to
identify who is at high risk for fast-growing tumors or for slow-growing tumors
Are there biologic markers that we can find with a blood test that might add to
this information to help us sort out who would benefit from screening or not?
[Other questions to
answer] from these data or from other ongoing studies include: Are there
subgroups of this 55- to 74-year-old population that are at higher risk? Are
there individuals who with less frequent screening can do just as well? Are
there individuals for whom more screening is necessary? The population looked
at [in the study] was a narrow window of high-risk individuals … It represents
about 7 million people out of the 94 million current and former smokers that we
have in this country.
We may even be able to
look at genetic markers at some point in the near future to determine who is at
higher risk and that will help us better identify who needs to be screened. I
think biomarkers and genetic markers all could be added to the formula when
we’re trying to decide what the best risk population to be screened is.
Screening tools work best when the screening population is well defined.
So now we have evidence
that screening in general can have an impact on disease. Unfortunately, prior
to this, lung cancer was diagnosed too late to make a big impact for most
patients. In lung cancer, an earlier diagnosis hopefully impacts mortality.
Lung cancer could become a curable disease if it’s found early enough to be
completely resected.
Dr. Albert A. Rizzo is
chair-elect of the American Lung Association board and chief of Christiana
Care’s pulmonary and critical care medicine section in Newark, Del.
He has no conflicts of interest.
Final results from the National Lung Screening Trial show a significant reduction in lung cancer mortality with the use of annual low-dose CT screening, compared with standard chest x-rays among former heavy smokers at high risk for lung cancer.
Low-dose CT screening led to a relative reduction of 20% in the rate of death from lung cancer, according to findings released online by the New England Journal of Medicine on June 29 (doi: 10.1056/NEJMoa1102873).The number needed to screen with low-dose CT to prevent one death from lung cancer was 320.
Although preliminary study results were announced in November 2010, the article by the National Lung Screening Trial (NLST) research team marks the first time that the results appear in a peer-reviewed journal. Acknowledging that the earlier announcement has led to calls for lung cancer screening, the authors urge rigorous analysis of cost-effectiveness before public policy recommendations are made.
"The reduction in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote.
In the study, 53,454 men and women aged 55-74 years – who were current or former smokers with a smoking history of at least 30 pack-years – were recruited at 33 U.S. medical centers. A total of 26,722 participants were randomized to receive three annual screens with low-dose helical CT; 26,732 were randomized to three annual screens using chest x-ray. The two groups were virtually identical in demographics and smoking history.
In all three screening rounds, positive screening tests were substantially more common in the low-dose CT group than in the radiography group (27.3% vs. 9.2% in the first round; 27.9% vs. 6.2% in the second; and 16.8% vs. 5% in the third). All told, 39.1% of the CT group and 16% of the radiography group had at least one positive result.
The percentage of screening tests that identified a clinically significant abnormality -- other than an abnormality suspicious for lung cancer – also was more than three times as high in the low-dose CT group as in the radiography group (7.5% vs. 2.1%).
More than 90% of positive screenings in the first round of the study led to a diagnostic evaluation, though the follow-up rates were lower in the later rounds. Diagnostic evaluation most often consisted of additional imaging with invasive procedures being performed infrequently.
Across the three screenings, most of the positive results were false positives – 96.4% in the CT group and 94.5% in the radiography group. Of the total number of low-dose CT screening tests, 24.2% were classified as positive and 23.4% had false-positive results; of the total number of radiographic screening tests, 6.9% were classified as positive and 6.5% were false-positive results.
In all, 1,060 lung cancers were diagnosed in the low-dose CT group (645/100,000 person-years) vs. 941 in the radiography group (572/100,000 person-years). Of these cancers, 649 in the low-dose CT group were diagnosed after a positive screening test and 44 were diagnosed after a negative screening test. In the radiography group, 279 cancers were diagnosed after a positive screening test and 137 were diagnosed after a negative screening test.
In both groups, the remaining cases were among participants who missed screening or were diagnosed after their trial screening phase was over
Analysis of lung cancer-specific mortality showed that in the CT group 356 lung cancer deaths occurred after 144,103 person-years; in the radiography group 443 lung cancer deaths occurred after 143,368 person-years. This corresponded to 247 and 309 lung cancer deaths, respectively, per 100,000 person-years in the CT and radiography groups.
There were 1,877 and 2,000 deaths from all causes in the CT and radiography groups, respectively, "representing a significant reduction with low-dose CT screening of 6.7% ... in the rate of death from any cause," the investigators wrote. While lung cancer accounted for 24.1% of all the deaths in the trial, 60.3% of the excess deaths in the radiography group were due to lung cancer.
The authors concluded that "although some agencies and organizations are contemplating the establishment of lung-cancer screening recommendations on the basis of the findings of the NLST, the current NLST data alone are, in our opinion, insufficient to fully inform such important decisions."
They noted that "The observation that low-dose CT screening can reduce the rate of death from lung cancer has generated many questions." Among these they listed: Will populations with different risk profiles benefit from screening? Could less frequent screening programs be equally effective? Would the use of different criteria for a positive screening result translate to similar benefit? For how long should people be screened?
In an accompanying editorial, Dr. Harold C. Sox, professor of medicine at the Dartmouth Institute in Hanover, N. H., agreed with the investigators’ reservations. In particular, the cost effectiveness of low-dose CT screening for lung cancer must be analyzed, he said: "Policy makers should wait for cost-effectiveness analyses to determine the amount of overdiagnosis in the NLST, and, perhaps identification of biologic markers of cancers that do not progress."
In addition, "it may be possible to define subgroups of smokers who are at higher or lower risk for lung cancer and tailor the screening strategy accordingly," he said. "The findings of the NLST regarding lung-cancer mortality signal the beginning of the end of one era of research on lung-cancer screening and the start of another. The focus will shift to informing the difficult patient-centered and policy decisions that are yet to come."
Dr. Sox also noted that "overdiagnosis is a problem because predicting which early-stage cancers will not progress is in an early stage of development, so that everyone with screen-detected cancer receives treatment that some do not need," he wrote in an accompanying editorial (doi: 10.1056/NEJME1103776).
All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan D. Clap reported having financial interest in Human Genome Sciences. Constantine Gatsonis, Ph.D., is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
Final results from the National Lung Screening Trial show a significant reduction in lung cancer mortality with the use of annual low-dose CT screening, compared with standard chest x-rays among former heavy smokers at high risk for lung cancer.
Low-dose CT screening led to a relative reduction of 20% in the rate of death from lung cancer, according to findings released online by the New England Journal of Medicine on June 29 (doi: 10.1056/NEJMoa1102873).The number needed to screen with low-dose CT to prevent one death from lung cancer was 320.
Although preliminary study results were announced in November 2010, the article by the National Lung Screening Trial (NLST) research team marks the first time that the results appear in a peer-reviewed journal. Acknowledging that the earlier announcement has led to calls for lung cancer screening, the authors urge rigorous analysis of cost-effectiveness before public policy recommendations are made.
"The reduction in lung-cancer mortality must be weighed against the harms from positive screening results and overdiagnosis, as well as the costs," they wrote.
In the study, 53,454 men and women aged 55-74 years – who were current or former smokers with a smoking history of at least 30 pack-years – were recruited at 33 U.S. medical centers. A total of 26,722 participants were randomized to receive three annual screens with low-dose helical CT; 26,732 were randomized to three annual screens using chest x-ray. The two groups were virtually identical in demographics and smoking history.
In all three screening rounds, positive screening tests were substantially more common in the low-dose CT group than in the radiography group (27.3% vs. 9.2% in the first round; 27.9% vs. 6.2% in the second; and 16.8% vs. 5% in the third). All told, 39.1% of the CT group and 16% of the radiography group had at least one positive result.
The percentage of screening tests that identified a clinically significant abnormality -- other than an abnormality suspicious for lung cancer – also was more than three times as high in the low-dose CT group as in the radiography group (7.5% vs. 2.1%).
More than 90% of positive screenings in the first round of the study led to a diagnostic evaluation, though the follow-up rates were lower in the later rounds. Diagnostic evaluation most often consisted of additional imaging with invasive procedures being performed infrequently.
Across the three screenings, most of the positive results were false positives – 96.4% in the CT group and 94.5% in the radiography group. Of the total number of low-dose CT screening tests, 24.2% were classified as positive and 23.4% had false-positive results; of the total number of radiographic screening tests, 6.9% were classified as positive and 6.5% were false-positive results.
In all, 1,060 lung cancers were diagnosed in the low-dose CT group (645/100,000 person-years) vs. 941 in the radiography group (572/100,000 person-years). Of these cancers, 649 in the low-dose CT group were diagnosed after a positive screening test and 44 were diagnosed after a negative screening test. In the radiography group, 279 cancers were diagnosed after a positive screening test and 137 were diagnosed after a negative screening test.
In both groups, the remaining cases were among participants who missed screening or were diagnosed after their trial screening phase was over
Analysis of lung cancer-specific mortality showed that in the CT group 356 lung cancer deaths occurred after 144,103 person-years; in the radiography group 443 lung cancer deaths occurred after 143,368 person-years. This corresponded to 247 and 309 lung cancer deaths, respectively, per 100,000 person-years in the CT and radiography groups.
There were 1,877 and 2,000 deaths from all causes in the CT and radiography groups, respectively, "representing a significant reduction with low-dose CT screening of 6.7% ... in the rate of death from any cause," the investigators wrote. While lung cancer accounted for 24.1% of all the deaths in the trial, 60.3% of the excess deaths in the radiography group were due to lung cancer.
The authors concluded that "although some agencies and organizations are contemplating the establishment of lung-cancer screening recommendations on the basis of the findings of the NLST, the current NLST data alone are, in our opinion, insufficient to fully inform such important decisions."
They noted that "The observation that low-dose CT screening can reduce the rate of death from lung cancer has generated many questions." Among these they listed: Will populations with different risk profiles benefit from screening? Could less frequent screening programs be equally effective? Would the use of different criteria for a positive screening result translate to similar benefit? For how long should people be screened?
In an accompanying editorial, Dr. Harold C. Sox, professor of medicine at the Dartmouth Institute in Hanover, N. H., agreed with the investigators’ reservations. In particular, the cost effectiveness of low-dose CT screening for lung cancer must be analyzed, he said: "Policy makers should wait for cost-effectiveness analyses to determine the amount of overdiagnosis in the NLST, and, perhaps identification of biologic markers of cancers that do not progress."
In addition, "it may be possible to define subgroups of smokers who are at higher or lower risk for lung cancer and tailor the screening strategy accordingly," he said. "The findings of the NLST regarding lung-cancer mortality signal the beginning of the end of one era of research on lung-cancer screening and the start of another. The focus will shift to informing the difficult patient-centered and policy decisions that are yet to come."
Dr. Sox also noted that "overdiagnosis is a problem because predicting which early-stage cancers will not progress is in an early stage of development, so that everyone with screen-detected cancer receives treatment that some do not need," he wrote in an accompanying editorial (doi: 10.1056/NEJME1103776).
All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan D. Clap reported having financial interest in Human Genome Sciences. Constantine Gatsonis, Ph.D., is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Low-dose CT screening reduced the relative rate of death from lung cancer by 20%, compared with chest x-ray screening.
Data Source: A study of 53,454 Americans aged 55-74 years, who were current or former smokers with a smoking history of at least 30 pack-years.
Disclosures: All but two of the NLST study authors reported that they have no relevant financial relationships. Jonathan Clap reported having financial interest in Human Genome Sciences Inc. Constantine Gatsonis is a consultant for Wilex AG, Mela Sciences, and Endocyte Inc., has received speaker fees from Bayer Health, and payment for education development by the Radiologic Society of North America. He also has invested in the Vanguard Health Fund. Dr. Sox had no conflicts.
FDA Advisory Panel Supports Hereditary Angioedema Drug
A Food and Drug Administration advisory panel has backed the approval of the hereditary angioedema drug icatibant, to be marketed as Firazyr.
Firazyr’s manufacturer, Shire, will enter discussions with the FDA on labeling for the drug, with backing from the panel for a claim to allow patients to self-administer the product, which is delivered through subcutaneous injection.
The Pulmonary-Allergy Drugs Advisory Committee voted 11-1, with one abstention, on June 23 that data for the bradykinin B2 receptor antagonist support self-injection of the drug, which is proposed to treat acute attacks of HAE in adults at a dose of 30 mg.
The panel supported approval of Firazyr by a vote of 12-1, following votes of 12-1 that data provide substantial and convincing evidence that it has a clinically meaningful benefit in acute HAE attacks, and 11-1, with one abstention, that its safety has been adequately addressed.
The "real benefit of this medication that I see will be self-medication," said Dr. Thomas Alexander Platts-Mills of the University of Virginia, Charlottesville.
It will put patients in control, enabling them to get therapy more quickly and to reduce the anxiety of seeking treatment from an emergency department that may or may not be equipped to treat the disease, he noted.
Fully half of hospitals do not have on hand a treatment for HAE acute attacks, and most will not administer a drug brought in by a patient, said Dr. Jay Portnoy of Children’s Mercy Hospitals and Clinics in Kansas City, Mo., so patients with HAE should be equipped to treat themselves, much as epinephrine can be self-administered. Firazyr will probably be used off label for self-administration anyway, he added.
The company is "very gratified" by the committee’s comments in support of self-administration, Suzanne Bruhn, Ph.D., senior vice president for strategic planning and program management for Shire Human Genetic Therapies, told reporters following the meeting.
The self-administration claim would distinguish Firazyr from competitors that are already in the U.S. market for acute HAE attacks. For example, Dyax Corp.’s Kalbitor (ecallantide) is delivered subcutaneously, but because of the potential for anaphylaxis, it must be administered by a health care professional. CSL Behring’s Berinert, which is used only for attacks affecting the face and abdominal area, is delivered intravenously.
Firazyr already is approved for self-administration in Europe and Australia.
Shire HGT would launch the drug within a few weeks of approval, using the experience and infrastructure built up to market its other orphan products, Dr. Bruhn said. Firazyr has an Aug. 25 Prescription Drug User Fee Act date.
This coverage is provided courtesy of "The Pink Sheet." This news organization and "The Pink Sheet" are owned by Elsevier.
A Food and Drug Administration advisory panel has backed the approval of the hereditary angioedema drug icatibant, to be marketed as Firazyr.
Firazyr’s manufacturer, Shire, will enter discussions with the FDA on labeling for the drug, with backing from the panel for a claim to allow patients to self-administer the product, which is delivered through subcutaneous injection.
The Pulmonary-Allergy Drugs Advisory Committee voted 11-1, with one abstention, on June 23 that data for the bradykinin B2 receptor antagonist support self-injection of the drug, which is proposed to treat acute attacks of HAE in adults at a dose of 30 mg.
The panel supported approval of Firazyr by a vote of 12-1, following votes of 12-1 that data provide substantial and convincing evidence that it has a clinically meaningful benefit in acute HAE attacks, and 11-1, with one abstention, that its safety has been adequately addressed.
The "real benefit of this medication that I see will be self-medication," said Dr. Thomas Alexander Platts-Mills of the University of Virginia, Charlottesville.
It will put patients in control, enabling them to get therapy more quickly and to reduce the anxiety of seeking treatment from an emergency department that may or may not be equipped to treat the disease, he noted.
Fully half of hospitals do not have on hand a treatment for HAE acute attacks, and most will not administer a drug brought in by a patient, said Dr. Jay Portnoy of Children’s Mercy Hospitals and Clinics in Kansas City, Mo., so patients with HAE should be equipped to treat themselves, much as epinephrine can be self-administered. Firazyr will probably be used off label for self-administration anyway, he added.
The company is "very gratified" by the committee’s comments in support of self-administration, Suzanne Bruhn, Ph.D., senior vice president for strategic planning and program management for Shire Human Genetic Therapies, told reporters following the meeting.
The self-administration claim would distinguish Firazyr from competitors that are already in the U.S. market for acute HAE attacks. For example, Dyax Corp.’s Kalbitor (ecallantide) is delivered subcutaneously, but because of the potential for anaphylaxis, it must be administered by a health care professional. CSL Behring’s Berinert, which is used only for attacks affecting the face and abdominal area, is delivered intravenously.
Firazyr already is approved for self-administration in Europe and Australia.
Shire HGT would launch the drug within a few weeks of approval, using the experience and infrastructure built up to market its other orphan products, Dr. Bruhn said. Firazyr has an Aug. 25 Prescription Drug User Fee Act date.
This coverage is provided courtesy of "The Pink Sheet." This news organization and "The Pink Sheet" are owned by Elsevier.
A Food and Drug Administration advisory panel has backed the approval of the hereditary angioedema drug icatibant, to be marketed as Firazyr.
Firazyr’s manufacturer, Shire, will enter discussions with the FDA on labeling for the drug, with backing from the panel for a claim to allow patients to self-administer the product, which is delivered through subcutaneous injection.
The Pulmonary-Allergy Drugs Advisory Committee voted 11-1, with one abstention, on June 23 that data for the bradykinin B2 receptor antagonist support self-injection of the drug, which is proposed to treat acute attacks of HAE in adults at a dose of 30 mg.
The panel supported approval of Firazyr by a vote of 12-1, following votes of 12-1 that data provide substantial and convincing evidence that it has a clinically meaningful benefit in acute HAE attacks, and 11-1, with one abstention, that its safety has been adequately addressed.
The "real benefit of this medication that I see will be self-medication," said Dr. Thomas Alexander Platts-Mills of the University of Virginia, Charlottesville.
It will put patients in control, enabling them to get therapy more quickly and to reduce the anxiety of seeking treatment from an emergency department that may or may not be equipped to treat the disease, he noted.
Fully half of hospitals do not have on hand a treatment for HAE acute attacks, and most will not administer a drug brought in by a patient, said Dr. Jay Portnoy of Children’s Mercy Hospitals and Clinics in Kansas City, Mo., so patients with HAE should be equipped to treat themselves, much as epinephrine can be self-administered. Firazyr will probably be used off label for self-administration anyway, he added.
The company is "very gratified" by the committee’s comments in support of self-administration, Suzanne Bruhn, Ph.D., senior vice president for strategic planning and program management for Shire Human Genetic Therapies, told reporters following the meeting.
The self-administration claim would distinguish Firazyr from competitors that are already in the U.S. market for acute HAE attacks. For example, Dyax Corp.’s Kalbitor (ecallantide) is delivered subcutaneously, but because of the potential for anaphylaxis, it must be administered by a health care professional. CSL Behring’s Berinert, which is used only for attacks affecting the face and abdominal area, is delivered intravenously.
Firazyr already is approved for self-administration in Europe and Australia.
Shire HGT would launch the drug within a few weeks of approval, using the experience and infrastructure built up to market its other orphan products, Dr. Bruhn said. Firazyr has an Aug. 25 Prescription Drug User Fee Act date.
This coverage is provided courtesy of "The Pink Sheet." This news organization and "The Pink Sheet" are owned by Elsevier.
FDA Unveils Graphic Cigarette Packaging Intended to Deter Smoking
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings