User login
Epilepsy
Multiday Seizure Cycles May Be Common
Tracking seizure cycles could facilitate personalized medicine and improve seizure reduction.
Multiday epileptic seizure cycles may occur in many individuals with epilepsy, according to a retrospective cohort study published online ahead of print September 12 in Lancet Neurology.
About 80% of patients in the study showed circadian modulation of their seizure rates, and more than 20% had strong circaseptan (ie, seven-day) rhythms, said Mark J. Cook, MD, a neurologist at St. Vincent’s Hospital in Melbourne, and colleagues.

The high prevalence of multiday seizure cycles could present an opportunity to improve treatment through the development of patient-specific chronotherapy (ie, the administration of medication when seizures are most likely). “Even without fully understanding the mechanisms of seizure cycles, temporal patterns can be incorporated into patient management plans,” said Dr. Cook.
The investigators based their study on two seizure datasets. One was a US cohort of 1,118 patients who reported at least 100 seizures through the SeizureTracker website or mobile app. The other was an Australian cohort of 12 patients with focal epilepsy who had at least 30 seizures recorded by an implanted electrocorticography device during follow-up that ranged between six months and three years.
In the US cohort, 86% of participants had at least one significant cycle in their seizure times, and 64% had more than one cycle. Most of the cycles (80%) were circadian, while 21% of people had significant circaseptan cycles in one analysis using the Hodges-Ajne test, a statistical method used to test for circular uniformity. “Many patients also showed some evidence of cycles lasting up to a month,” said the authors.
A confirmatory analysis using Monte Carlo simulation found that 7% of people, or 77 individuals, had significant circaseptan cycles. “The probability that 77 patients would randomly share a specific cycle is infinitesimal,” said the authors.
In the Australian study, 11 of 12 patients had strong rhythms at 24 hours, one had a significant cycle of exactly one week, and two others had cycles of approximately one week.
“Some people had stronger rhythms at time scales longer than 24 hours, which suggests that circadian regulation was not necessarily the strongest modulating factor of epileptic activity,” said the investigators. The cause of longer seizure cycles remains unclear, though peak seizure times might be linked to varying stress levels, seasonal changes in sleep quality, or biologic cycles such as menstruation.
—Andrew D. Bowser
Suggested Reading
Karoly PJ, Goldenholz DM, Freestone DR, et al. Circadian and circaseptan rhythms in human epilepsy: a retrospective cohort study. Lancet Neurol. 2018 Sep 12 [Epub ahead of print].
Tracking seizure cycles could facilitate personalized medicine and improve seizure reduction.
Tracking seizure cycles could facilitate personalized medicine and improve seizure reduction.
Multiday epileptic seizure cycles may occur in many individuals with epilepsy, according to a retrospective cohort study published online ahead of print September 12 in Lancet Neurology.
About 80% of patients in the study showed circadian modulation of their seizure rates, and more than 20% had strong circaseptan (ie, seven-day) rhythms, said Mark J. Cook, MD, a neurologist at St. Vincent’s Hospital in Melbourne, and colleagues.
The high prevalence of multiday seizure cycles could present an opportunity to improve treatment through the development of patient-specific chronotherapy (ie, the administration of medication when seizures are most likely). “Even without fully understanding the mechanisms of seizure cycles, temporal patterns can be incorporated into patient management plans,” said Dr. Cook.
The investigators based their study on two seizure datasets. One was a US cohort of 1,118 patients who reported at least 100 seizures through the SeizureTracker website or mobile app. The other was an Australian cohort of 12 patients with focal epilepsy who had at least 30 seizures recorded by an implanted electrocorticography device during follow-up that ranged between six months and three years.
In the US cohort, 86% of participants had at least one significant cycle in their seizure times, and 64% had more than one cycle. Most of the cycles (80%) were circadian, while 21% of people had significant circaseptan cycles in one analysis using the Hodges-Ajne test, a statistical method used to test for circular uniformity. “Many patients also showed some evidence of cycles lasting up to a month,” said the authors.
A confirmatory analysis using Monte Carlo simulation found that 7% of people, or 77 individuals, had significant circaseptan cycles. “The probability that 77 patients would randomly share a specific cycle is infinitesimal,” said the authors.
In the Australian study, 11 of 12 patients had strong rhythms at 24 hours, one had a significant cycle of exactly one week, and two others had cycles of approximately one week.
“Some people had stronger rhythms at time scales longer than 24 hours, which suggests that circadian regulation was not necessarily the strongest modulating factor of epileptic activity,” said the investigators. The cause of longer seizure cycles remains unclear, though peak seizure times might be linked to varying stress levels, seasonal changes in sleep quality, or biologic cycles such as menstruation.
—Andrew D. Bowser
Suggested Reading
Karoly PJ, Goldenholz DM, Freestone DR, et al. Circadian and circaseptan rhythms in human epilepsy: a retrospective cohort study. Lancet Neurol. 2018 Sep 12 [Epub ahead of print].
Multiday epileptic seizure cycles may occur in many individuals with epilepsy, according to a retrospective cohort study published online ahead of print September 12 in Lancet Neurology.
About 80% of patients in the study showed circadian modulation of their seizure rates, and more than 20% had strong circaseptan (ie, seven-day) rhythms, said Mark J. Cook, MD, a neurologist at St. Vincent’s Hospital in Melbourne, and colleagues.
The high prevalence of multiday seizure cycles could present an opportunity to improve treatment through the development of patient-specific chronotherapy (ie, the administration of medication when seizures are most likely). “Even without fully understanding the mechanisms of seizure cycles, temporal patterns can be incorporated into patient management plans,” said Dr. Cook.
The investigators based their study on two seizure datasets. One was a US cohort of 1,118 patients who reported at least 100 seizures through the SeizureTracker website or mobile app. The other was an Australian cohort of 12 patients with focal epilepsy who had at least 30 seizures recorded by an implanted electrocorticography device during follow-up that ranged between six months and three years.
In the US cohort, 86% of participants had at least one significant cycle in their seizure times, and 64% had more than one cycle. Most of the cycles (80%) were circadian, while 21% of people had significant circaseptan cycles in one analysis using the Hodges-Ajne test, a statistical method used to test for circular uniformity. “Many patients also showed some evidence of cycles lasting up to a month,” said the authors.
A confirmatory analysis using Monte Carlo simulation found that 7% of people, or 77 individuals, had significant circaseptan cycles. “The probability that 77 patients would randomly share a specific cycle is infinitesimal,” said the authors.
In the Australian study, 11 of 12 patients had strong rhythms at 24 hours, one had a significant cycle of exactly one week, and two others had cycles of approximately one week.
“Some people had stronger rhythms at time scales longer than 24 hours, which suggests that circadian regulation was not necessarily the strongest modulating factor of epileptic activity,” said the investigators. The cause of longer seizure cycles remains unclear, though peak seizure times might be linked to varying stress levels, seasonal changes in sleep quality, or biologic cycles such as menstruation.
—Andrew D. Bowser
Suggested Reading
Karoly PJ, Goldenholz DM, Freestone DR, et al. Circadian and circaseptan rhythms in human epilepsy: a retrospective cohort study. Lancet Neurol. 2018 Sep 12 [Epub ahead of print].
Long-Term Data Suggest Benefits of Adjunctive CBD in Treatment-Resistant Epilepsies
The drug promotes sustained reductions in seizure frequency and contributes to seizure freedom for some patients.
Pooled data from an expanded-access program provide further evidence that adjunctive cannabidiol (CBD) provides meaningful reductions in seizure frequency in patients with treatment-resistant epilepsies. The data were published in the August issue of Epilepsia.
Studies have recently indicated that adjunctive CBD effectively reduces seizures associated with Lennox-Gastaut syndrome and Dravet syndrome. An expanded-access program was created in January 2014 to offer CBD to patients with treatment-resistant epilepsies. Data on safety, tolerability, and efficacy during the first year of the study have been reported. Jerzy P. Szaflarski, MD, PhD, Professor of Neurology at the University of Alabama at Birmingham, and colleagues examined results for safety outcomes at 144 weeks and efficacy outcomes at 96 weeks.

An Expanded-Access Program
All participants in the program had treatment-resistant epilepsy and were receiving stable doses of antiepileptic drugs (AEDs) for at least four weeks before enrollment. During a four-week baseline period, parents and caregivers kept diaries of all countable seizure types. Participants subsequently received a plant-based oral pharmaceutical formulation of CBD (100 mg/mL). Treatment was initiated at a dose of 2–10 mg/kg/day and was titrated to a maximum dose of 25–50 mg/kg/day.
Patients were examined every two to four weeks until the 16th week, and every two to 12 weeks after that point. The efficacy outcomes included the percentage change from baseline in median monthly convulsive seizure frequency and total seizure frequency, and the percentages of patients with at least 50%, at least 75%, and 100% reductions in seizures, compared with baseline. Investigators documented adverse events at each visit.
CBD Was Well Tolerated
The safety analysis included 607 patients, and the efficacy analysis included 580 patients. Among patients included in the safety analysis, 24% withdrew from the study. The most common reasons for withdrawal were lack of efficacy (15%) and adverse events (5%). Participants’ mean age was 13, and 52% of patients were male. The median number of concomitant AEDs was three, the median dose of CBD was 25 mg/kg/day, and the median treatment duration was 48 weeks.
At 12 weeks, adjunctive CBD was associated with a 51% reduction in median monthly convulsive seizures and a 48% reduction in total seizures. Reductions in these seizure types were similar through 96 weeks. At 12 weeks, 52% of patients had a reduction in convulsive seizures of at least 50%, 31% had a reduction of at least 75%, and 11% had a 100% reduction. These response rates were similar through 96 weeks of treatment.
CBD was generally well tolerated. The most common adverse events were diarrhea (29%) and somnolence (22%). About 10% of patients had abnormal liver adverse events, and 75% of them were taking valproate. Among patients taking concomitant clobazam, 38% had somnolence, compared with 14% of patients not taking concomitant clobazam.
The expanded-access program is not placebo-controlled, and neither patients nor investigators are blinded. Furthermore, reporting methods varied between study sites. Despite these limitations, the data indicate that adjunctive CBD significantly reduces seizure frequency, according to the authors.
The data support the results of double-blind, placebo-controlled trials that found that add-on CBD reduces seizure frequency, compared with placebo. The FDA in June approved Epidiolex, the formulation of CBD used in the expanded-access program, for the treatment of seizures associated with Dravet syndrome and Lennox-Gastaut syndrome.
—Erik Greb
Suggested Reading
Szaflarski JP, Bebin EM, Comi AM, et al. Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: Expanded access program results. Epilepsia. 2018;59(8):1540-1548.
The drug promotes sustained reductions in seizure frequency and contributes to seizure freedom for some patients.
The drug promotes sustained reductions in seizure frequency and contributes to seizure freedom for some patients.
Pooled data from an expanded-access program provide further evidence that adjunctive cannabidiol (CBD) provides meaningful reductions in seizure frequency in patients with treatment-resistant epilepsies. The data were published in the August issue of Epilepsia.
Studies have recently indicated that adjunctive CBD effectively reduces seizures associated with Lennox-Gastaut syndrome and Dravet syndrome. An expanded-access program was created in January 2014 to offer CBD to patients with treatment-resistant epilepsies. Data on safety, tolerability, and efficacy during the first year of the study have been reported. Jerzy P. Szaflarski, MD, PhD, Professor of Neurology at the University of Alabama at Birmingham, and colleagues examined results for safety outcomes at 144 weeks and efficacy outcomes at 96 weeks.
An Expanded-Access Program
All participants in the program had treatment-resistant epilepsy and were receiving stable doses of antiepileptic drugs (AEDs) for at least four weeks before enrollment. During a four-week baseline period, parents and caregivers kept diaries of all countable seizure types. Participants subsequently received a plant-based oral pharmaceutical formulation of CBD (100 mg/mL). Treatment was initiated at a dose of 2–10 mg/kg/day and was titrated to a maximum dose of 25–50 mg/kg/day.
Patients were examined every two to four weeks until the 16th week, and every two to 12 weeks after that point. The efficacy outcomes included the percentage change from baseline in median monthly convulsive seizure frequency and total seizure frequency, and the percentages of patients with at least 50%, at least 75%, and 100% reductions in seizures, compared with baseline. Investigators documented adverse events at each visit.
CBD Was Well Tolerated
The safety analysis included 607 patients, and the efficacy analysis included 580 patients. Among patients included in the safety analysis, 24% withdrew from the study. The most common reasons for withdrawal were lack of efficacy (15%) and adverse events (5%). Participants’ mean age was 13, and 52% of patients were male. The median number of concomitant AEDs was three, the median dose of CBD was 25 mg/kg/day, and the median treatment duration was 48 weeks.
At 12 weeks, adjunctive CBD was associated with a 51% reduction in median monthly convulsive seizures and a 48% reduction in total seizures. Reductions in these seizure types were similar through 96 weeks. At 12 weeks, 52% of patients had a reduction in convulsive seizures of at least 50%, 31% had a reduction of at least 75%, and 11% had a 100% reduction. These response rates were similar through 96 weeks of treatment.
CBD was generally well tolerated. The most common adverse events were diarrhea (29%) and somnolence (22%). About 10% of patients had abnormal liver adverse events, and 75% of them were taking valproate. Among patients taking concomitant clobazam, 38% had somnolence, compared with 14% of patients not taking concomitant clobazam.
The expanded-access program is not placebo-controlled, and neither patients nor investigators are blinded. Furthermore, reporting methods varied between study sites. Despite these limitations, the data indicate that adjunctive CBD significantly reduces seizure frequency, according to the authors.
The data support the results of double-blind, placebo-controlled trials that found that add-on CBD reduces seizure frequency, compared with placebo. The FDA in June approved Epidiolex, the formulation of CBD used in the expanded-access program, for the treatment of seizures associated with Dravet syndrome and Lennox-Gastaut syndrome.
—Erik Greb
Suggested Reading
Szaflarski JP, Bebin EM, Comi AM, et al. Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: Expanded access program results. Epilepsia. 2018;59(8):1540-1548.
Pooled data from an expanded-access program provide further evidence that adjunctive cannabidiol (CBD) provides meaningful reductions in seizure frequency in patients with treatment-resistant epilepsies. The data were published in the August issue of Epilepsia.
Studies have recently indicated that adjunctive CBD effectively reduces seizures associated with Lennox-Gastaut syndrome and Dravet syndrome. An expanded-access program was created in January 2014 to offer CBD to patients with treatment-resistant epilepsies. Data on safety, tolerability, and efficacy during the first year of the study have been reported. Jerzy P. Szaflarski, MD, PhD, Professor of Neurology at the University of Alabama at Birmingham, and colleagues examined results for safety outcomes at 144 weeks and efficacy outcomes at 96 weeks.
An Expanded-Access Program
All participants in the program had treatment-resistant epilepsy and were receiving stable doses of antiepileptic drugs (AEDs) for at least four weeks before enrollment. During a four-week baseline period, parents and caregivers kept diaries of all countable seizure types. Participants subsequently received a plant-based oral pharmaceutical formulation of CBD (100 mg/mL). Treatment was initiated at a dose of 2–10 mg/kg/day and was titrated to a maximum dose of 25–50 mg/kg/day.
Patients were examined every two to four weeks until the 16th week, and every two to 12 weeks after that point. The efficacy outcomes included the percentage change from baseline in median monthly convulsive seizure frequency and total seizure frequency, and the percentages of patients with at least 50%, at least 75%, and 100% reductions in seizures, compared with baseline. Investigators documented adverse events at each visit.
CBD Was Well Tolerated
The safety analysis included 607 patients, and the efficacy analysis included 580 patients. Among patients included in the safety analysis, 24% withdrew from the study. The most common reasons for withdrawal were lack of efficacy (15%) and adverse events (5%). Participants’ mean age was 13, and 52% of patients were male. The median number of concomitant AEDs was three, the median dose of CBD was 25 mg/kg/day, and the median treatment duration was 48 weeks.
At 12 weeks, adjunctive CBD was associated with a 51% reduction in median monthly convulsive seizures and a 48% reduction in total seizures. Reductions in these seizure types were similar through 96 weeks. At 12 weeks, 52% of patients had a reduction in convulsive seizures of at least 50%, 31% had a reduction of at least 75%, and 11% had a 100% reduction. These response rates were similar through 96 weeks of treatment.
CBD was generally well tolerated. The most common adverse events were diarrhea (29%) and somnolence (22%). About 10% of patients had abnormal liver adverse events, and 75% of them were taking valproate. Among patients taking concomitant clobazam, 38% had somnolence, compared with 14% of patients not taking concomitant clobazam.
The expanded-access program is not placebo-controlled, and neither patients nor investigators are blinded. Furthermore, reporting methods varied between study sites. Despite these limitations, the data indicate that adjunctive CBD significantly reduces seizure frequency, according to the authors.
The data support the results of double-blind, placebo-controlled trials that found that add-on CBD reduces seizure frequency, compared with placebo. The FDA in June approved Epidiolex, the formulation of CBD used in the expanded-access program, for the treatment of seizures associated with Dravet syndrome and Lennox-Gastaut syndrome.
—Erik Greb
Suggested Reading
Szaflarski JP, Bebin EM, Comi AM, et al. Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: Expanded access program results. Epilepsia. 2018;59(8):1540-1548.
Self-Management Intervention for Epilepsy Improves Health
The intervention appears to ameliorate mood and quality of life in people with a history of negative health events.
Self-management of epilepsy using a group-format, remote intervention improves mood, quality of life, and health functioning in high-risk individuals, according to a randomized, controlled trial published in the September issue of Epilepsia.
In the six-month trial, 120 individuals with epilepsy who had experienced at least one epilepsy-related negative health event in the previous six months were randomized to a wait-list control group or a novel self‐management intervention.
The eight-session intervention, known as SMART, focused on modifiable factors that can be addressed with self-management, such as stress, substance abuse, routine, nutrition, and social support. It was delivered remotely during eight to 10 weeks, either by telephone or online, after an initial in-person session.
“SMART combines the portability and low cost of a Web‐based intervention with the personally salient components of behavior modeling obtained by interacting with individuals who have walked the walk in living with epilepsy,” said Martha Sajatovic, MD, Professor of Psychiatry at Case Western Reserve University in Cleveland, and her colleagues.

During the six-month follow-up period, individuals randomized to the intervention had a mean of 10.16 fewer negative health events, compared with a mean of 1.93 fewer events in the control group.
When the authors examined subcategories of negative health event counts (eg, past three-day seizure count or past six‐month emergency department and hospitalization count), the differences between groups were not significant. There was also no difference between groups in seizure severity.
The study showed significant improvements in participants’ self-rated depressive symptom severity, observer-rated depressive symptom severity, quality of life, and physical and mental health functioning, compared with controls. The intervention group also reported significant improvements on the Epilepsy Self-Efficacy and Epilepsy Self-Management scales.
Most participants (94.2%) said that the intervention was useful and addressed their most important issues. Approximately 92% said that the benefits of the SMART intervention were worth the effort.
“It is possible that SMART, which uses people with epilepsy as guides to help others learn to cope with the challenges of living with this common chronic neurologic condition, may help to alleviate some of the factors that prevent people with epilepsy from optimizing their quality of life.”
—Bianca Nogrady
Suggested Reading
Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. Epilepsia. 2018;59(9):1684-1695.
The intervention appears to ameliorate mood and quality of life in people with a history of negative health events.
The intervention appears to ameliorate mood and quality of life in people with a history of negative health events.
Self-management of epilepsy using a group-format, remote intervention improves mood, quality of life, and health functioning in high-risk individuals, according to a randomized, controlled trial published in the September issue of Epilepsia.
In the six-month trial, 120 individuals with epilepsy who had experienced at least one epilepsy-related negative health event in the previous six months were randomized to a wait-list control group or a novel self‐management intervention.
The eight-session intervention, known as SMART, focused on modifiable factors that can be addressed with self-management, such as stress, substance abuse, routine, nutrition, and social support. It was delivered remotely during eight to 10 weeks, either by telephone or online, after an initial in-person session.
“SMART combines the portability and low cost of a Web‐based intervention with the personally salient components of behavior modeling obtained by interacting with individuals who have walked the walk in living with epilepsy,” said Martha Sajatovic, MD, Professor of Psychiatry at Case Western Reserve University in Cleveland, and her colleagues.
During the six-month follow-up period, individuals randomized to the intervention had a mean of 10.16 fewer negative health events, compared with a mean of 1.93 fewer events in the control group.
When the authors examined subcategories of negative health event counts (eg, past three-day seizure count or past six‐month emergency department and hospitalization count), the differences between groups were not significant. There was also no difference between groups in seizure severity.
The study showed significant improvements in participants’ self-rated depressive symptom severity, observer-rated depressive symptom severity, quality of life, and physical and mental health functioning, compared with controls. The intervention group also reported significant improvements on the Epilepsy Self-Efficacy and Epilepsy Self-Management scales.
Most participants (94.2%) said that the intervention was useful and addressed their most important issues. Approximately 92% said that the benefits of the SMART intervention were worth the effort.
“It is possible that SMART, which uses people with epilepsy as guides to help others learn to cope with the challenges of living with this common chronic neurologic condition, may help to alleviate some of the factors that prevent people with epilepsy from optimizing their quality of life.”
—Bianca Nogrady
Suggested Reading
Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. Epilepsia. 2018;59(9):1684-1695.
Self-management of epilepsy using a group-format, remote intervention improves mood, quality of life, and health functioning in high-risk individuals, according to a randomized, controlled trial published in the September issue of Epilepsia.
In the six-month trial, 120 individuals with epilepsy who had experienced at least one epilepsy-related negative health event in the previous six months were randomized to a wait-list control group or a novel self‐management intervention.
The eight-session intervention, known as SMART, focused on modifiable factors that can be addressed with self-management, such as stress, substance abuse, routine, nutrition, and social support. It was delivered remotely during eight to 10 weeks, either by telephone or online, after an initial in-person session.
“SMART combines the portability and low cost of a Web‐based intervention with the personally salient components of behavior modeling obtained by interacting with individuals who have walked the walk in living with epilepsy,” said Martha Sajatovic, MD, Professor of Psychiatry at Case Western Reserve University in Cleveland, and her colleagues.
During the six-month follow-up period, individuals randomized to the intervention had a mean of 10.16 fewer negative health events, compared with a mean of 1.93 fewer events in the control group.
When the authors examined subcategories of negative health event counts (eg, past three-day seizure count or past six‐month emergency department and hospitalization count), the differences between groups were not significant. There was also no difference between groups in seizure severity.
The study showed significant improvements in participants’ self-rated depressive symptom severity, observer-rated depressive symptom severity, quality of life, and physical and mental health functioning, compared with controls. The intervention group also reported significant improvements on the Epilepsy Self-Efficacy and Epilepsy Self-Management scales.
Most participants (94.2%) said that the intervention was useful and addressed their most important issues. Approximately 92% said that the benefits of the SMART intervention were worth the effort.
“It is possible that SMART, which uses people with epilepsy as guides to help others learn to cope with the challenges of living with this common chronic neurologic condition, may help to alleviate some of the factors that prevent people with epilepsy from optimizing their quality of life.”
—Bianca Nogrady
Suggested Reading
Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. Epilepsia. 2018;59(9):1684-1695.
Risk Factors for Epilepsy after Traumatic Brain Injury
Among patients who have experienced a traumatic brain injury (TBI), the likelihood of developing post-traumatic epilepsy (PTE) increases with age, the early onset of seizures, and the severity of the brain injury, according to an analysis of insurance claims from 2004 to 2014.
- There were approximately 2.8 million emergency room visits, hospitalizations and deaths from traumatic brain injuries in the US in 2013.
- Early seizures occurred in 0.5% of patients with TBI.
- Over a 9 year period, the incidence of post-traumatic epilepsy (PTE) increased from 1 to 4% in this population.
- Early onset of seizures, older age, and TBI severity increased the likelihood of PTE.
- Prophylactic acetazolamide seemed to reduce the risk of PTE, when compared to patients who had received no anti-epilepsy drugs.
DeGrauw X, Thurman D, Xu L, et al. Epidemiology of traumatic brain injury-associated epilepsy and early use of anti-epilepsy drugs: An analysis of insurance claims data, 2004-2014. [Published online ahead of print July 23, 2018] Epilepsy Res. doi: 10.1016/j.eplepsyres.2018.07.012
Among patients who have experienced a traumatic brain injury (TBI), the likelihood of developing post-traumatic epilepsy (PTE) increases with age, the early onset of seizures, and the severity of the brain injury, according to an analysis of insurance claims from 2004 to 2014.
- There were approximately 2.8 million emergency room visits, hospitalizations and deaths from traumatic brain injuries in the US in 2013.
- Early seizures occurred in 0.5% of patients with TBI.
- Over a 9 year period, the incidence of post-traumatic epilepsy (PTE) increased from 1 to 4% in this population.
- Early onset of seizures, older age, and TBI severity increased the likelihood of PTE.
- Prophylactic acetazolamide seemed to reduce the risk of PTE, when compared to patients who had received no anti-epilepsy drugs.
DeGrauw X, Thurman D, Xu L, et al. Epidemiology of traumatic brain injury-associated epilepsy and early use of anti-epilepsy drugs: An analysis of insurance claims data, 2004-2014. [Published online ahead of print July 23, 2018] Epilepsy Res. doi: 10.1016/j.eplepsyres.2018.07.012
Among patients who have experienced a traumatic brain injury (TBI), the likelihood of developing post-traumatic epilepsy (PTE) increases with age, the early onset of seizures, and the severity of the brain injury, according to an analysis of insurance claims from 2004 to 2014.
- There were approximately 2.8 million emergency room visits, hospitalizations and deaths from traumatic brain injuries in the US in 2013.
- Early seizures occurred in 0.5% of patients with TBI.
- Over a 9 year period, the incidence of post-traumatic epilepsy (PTE) increased from 1 to 4% in this population.
- Early onset of seizures, older age, and TBI severity increased the likelihood of PTE.
- Prophylactic acetazolamide seemed to reduce the risk of PTE, when compared to patients who had received no anti-epilepsy drugs.
DeGrauw X, Thurman D, Xu L, et al. Epidemiology of traumatic brain injury-associated epilepsy and early use of anti-epilepsy drugs: An analysis of insurance claims data, 2004-2014. [Published online ahead of print July 23, 2018] Epilepsy Res. doi: 10.1016/j.eplepsyres.2018.07.012
Is It Possible to Predict Seizures?
Conventional medical wisdom insists that it is not possible to predict the onset of seizures with any certainty, but recent research suggests otherwise, according to a review published in Nature Reviews Neurology.
- An influential 2007 review of the medical literature concluded that there was insufficient evidence to foresee the onset of seizures.
- However, an international team of experts summarized several recent advances that suggest seizure prediction may be possible.
- The new review discusses a small experiment in which intracranial EEGs were used prospectively to predict seizures.
- Additional advances include EEG databases, seizure prediction competitions, and a better understanding of the mechanism of action behind seizures.
Kuhlmann L, Lehnertz K, Richardson MP, et al. Seizure prediction - ready for a new era. [Published online ahead of print August 21, 2018] Nat Rev Neurol. doi: 10.1038/s41582-018-0055-2
Conventional medical wisdom insists that it is not possible to predict the onset of seizures with any certainty, but recent research suggests otherwise, according to a review published in Nature Reviews Neurology.
- An influential 2007 review of the medical literature concluded that there was insufficient evidence to foresee the onset of seizures.
- However, an international team of experts summarized several recent advances that suggest seizure prediction may be possible.
- The new review discusses a small experiment in which intracranial EEGs were used prospectively to predict seizures.
- Additional advances include EEG databases, seizure prediction competitions, and a better understanding of the mechanism of action behind seizures.
Kuhlmann L, Lehnertz K, Richardson MP, et al. Seizure prediction - ready for a new era. [Published online ahead of print August 21, 2018] Nat Rev Neurol. doi: 10.1038/s41582-018-0055-2
Conventional medical wisdom insists that it is not possible to predict the onset of seizures with any certainty, but recent research suggests otherwise, according to a review published in Nature Reviews Neurology.
- An influential 2007 review of the medical literature concluded that there was insufficient evidence to foresee the onset of seizures.
- However, an international team of experts summarized several recent advances that suggest seizure prediction may be possible.
- The new review discusses a small experiment in which intracranial EEGs were used prospectively to predict seizures.
- Additional advances include EEG databases, seizure prediction competitions, and a better understanding of the mechanism of action behind seizures.
Kuhlmann L, Lehnertz K, Richardson MP, et al. Seizure prediction - ready for a new era. [Published online ahead of print August 21, 2018] Nat Rev Neurol. doi: 10.1038/s41582-018-0055-2
Managing Sleep Disorders in Epilepsy
Understanding the relationship between epilepsy and sleep disorders can help clinicians improve the management of both disorders according to a recent review in Epilepsy Research.
- Sleep apnea, insomnia, restless legs syndrome and parasomnias often occur in patients with epilepsy.
- Researchers from Brigham and Women’s Hospital in Boston and Mayo Clinic reviewed the symptoms and diagnosis of these sleep disorders to help clinicians screen patients with epilepsy at risk for these problems.
- The review also explores treatment options and several case reports that illustrate the consequences of said sleep disorders in those with epilepsy.
- Latreille et al believe that employing the latest diagnostic and treatment approaches to co-morbid sleep disorders may improve patients’ functional status, alertness, quality of life and seizure burden.
Latreille V, St. Louis EK, Pavlova M. Co-morbid sleep disorders and epilepsy: A narrative review and case examples. Epilepsy Res. 2018; 145:185-197. https://doi.org/10.1016/j.eplepsyres.2018.07.005
Understanding the relationship between epilepsy and sleep disorders can help clinicians improve the management of both disorders according to a recent review in Epilepsy Research.
- Sleep apnea, insomnia, restless legs syndrome and parasomnias often occur in patients with epilepsy.
- Researchers from Brigham and Women’s Hospital in Boston and Mayo Clinic reviewed the symptoms and diagnosis of these sleep disorders to help clinicians screen patients with epilepsy at risk for these problems.
- The review also explores treatment options and several case reports that illustrate the consequences of said sleep disorders in those with epilepsy.
- Latreille et al believe that employing the latest diagnostic and treatment approaches to co-morbid sleep disorders may improve patients’ functional status, alertness, quality of life and seizure burden.
Latreille V, St. Louis EK, Pavlova M. Co-morbid sleep disorders and epilepsy: A narrative review and case examples. Epilepsy Res. 2018; 145:185-197. https://doi.org/10.1016/j.eplepsyres.2018.07.005
Understanding the relationship between epilepsy and sleep disorders can help clinicians improve the management of both disorders according to a recent review in Epilepsy Research.
- Sleep apnea, insomnia, restless legs syndrome and parasomnias often occur in patients with epilepsy.
- Researchers from Brigham and Women’s Hospital in Boston and Mayo Clinic reviewed the symptoms and diagnosis of these sleep disorders to help clinicians screen patients with epilepsy at risk for these problems.
- The review also explores treatment options and several case reports that illustrate the consequences of said sleep disorders in those with epilepsy.
- Latreille et al believe that employing the latest diagnostic and treatment approaches to co-morbid sleep disorders may improve patients’ functional status, alertness, quality of life and seizure burden.
Latreille V, St. Louis EK, Pavlova M. Co-morbid sleep disorders and epilepsy: A narrative review and case examples. Epilepsy Res. 2018; 145:185-197. https://doi.org/10.1016/j.eplepsyres.2018.07.005
SMART Self-Management Program Enhances Epilepsy Care
A self-management program called SMART can help patients with epilepsy reduce the risk of negative health events according to researchers at Case Western Reserve University School of Medicine.
- A 6-month randomized controlled trial of the community-based program included 60 adult patients and was compared to 60 control patients on a waitlist.
- The experiment monitored a variety of events, including seizures, accidents, attempts at self-harm, emergency department visits, and hospitalizations.
- The average patient in this trial was about 41 years old, about 70% were African American, 74% were unemployed.
- Patients who were randomized to the SMART program had fewer negative health events by 6 months compared to controls.
- SMART was also linked to improved scores on the Patient Health Questionnaire (P=.002), the 10 item Quality of Life in Epilepsy Inventory, and the Short Form Health Survey.
Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. [Published online ahead of print August 10, 2018]. Epilepsia. https://doi.org/10.1111/epi.14527.
A self-management program called SMART can help patients with epilepsy reduce the risk of negative health events according to researchers at Case Western Reserve University School of Medicine.
- A 6-month randomized controlled trial of the community-based program included 60 adult patients and was compared to 60 control patients on a waitlist.
- The experiment monitored a variety of events, including seizures, accidents, attempts at self-harm, emergency department visits, and hospitalizations.
- The average patient in this trial was about 41 years old, about 70% were African American, 74% were unemployed.
- Patients who were randomized to the SMART program had fewer negative health events by 6 months compared to controls.
- SMART was also linked to improved scores on the Patient Health Questionnaire (P=.002), the 10 item Quality of Life in Epilepsy Inventory, and the Short Form Health Survey.
Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. [Published online ahead of print August 10, 2018]. Epilepsia. https://doi.org/10.1111/epi.14527.
A self-management program called SMART can help patients with epilepsy reduce the risk of negative health events according to researchers at Case Western Reserve University School of Medicine.
- A 6-month randomized controlled trial of the community-based program included 60 adult patients and was compared to 60 control patients on a waitlist.
- The experiment monitored a variety of events, including seizures, accidents, attempts at self-harm, emergency department visits, and hospitalizations.
- The average patient in this trial was about 41 years old, about 70% were African American, 74% were unemployed.
- Patients who were randomized to the SMART program had fewer negative health events by 6 months compared to controls.
- SMART was also linked to improved scores on the Patient Health Questionnaire (P=.002), the 10 item Quality of Life in Epilepsy Inventory, and the Short Form Health Survey.
Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. [Published online ahead of print August 10, 2018]. Epilepsia. https://doi.org/10.1111/epi.14527.
Don’t Ignore Sleep Complaints in PNES Patients
Patients with psychogenic nonepileptic seizures (PNES) are more likely to suffer from sleep complaints than are patients with epilepsy according to an analysis conducted by clinicians at the Brigham and Women’s Hospital.
- 149 patients with PNES and 82 patients with epilepsy completed the Beck Depression Inventory and the Quality of Life in Epilepsy Inventory-10.
- By analyzing item 16 on the Beck Depression Inventory, which looks at changes in sleep patterns, the investigators found that PNES patients were more likely to report moderate to severe changes in sleep patterns, including waking up too early, sleeping less than usual, and having trouble falling back to sleep.
- The sleep complaints were associated with poorer quality of life, suggesting that they need to be addressed more closely in PNES patients.
Latreille V, Baslet G, Sarkis R, et al. Sleep in psychogenic nonepileptic seizures: time to raise a red flag. Epilepsy Behav. 2018;86:6-8.
Patients with psychogenic nonepileptic seizures (PNES) are more likely to suffer from sleep complaints than are patients with epilepsy according to an analysis conducted by clinicians at the Brigham and Women’s Hospital.
- 149 patients with PNES and 82 patients with epilepsy completed the Beck Depression Inventory and the Quality of Life in Epilepsy Inventory-10.
- By analyzing item 16 on the Beck Depression Inventory, which looks at changes in sleep patterns, the investigators found that PNES patients were more likely to report moderate to severe changes in sleep patterns, including waking up too early, sleeping less than usual, and having trouble falling back to sleep.
- The sleep complaints were associated with poorer quality of life, suggesting that they need to be addressed more closely in PNES patients.
Latreille V, Baslet G, Sarkis R, et al. Sleep in psychogenic nonepileptic seizures: time to raise a red flag. Epilepsy Behav. 2018;86:6-8.
Patients with psychogenic nonepileptic seizures (PNES) are more likely to suffer from sleep complaints than are patients with epilepsy according to an analysis conducted by clinicians at the Brigham and Women’s Hospital.
- 149 patients with PNES and 82 patients with epilepsy completed the Beck Depression Inventory and the Quality of Life in Epilepsy Inventory-10.
- By analyzing item 16 on the Beck Depression Inventory, which looks at changes in sleep patterns, the investigators found that PNES patients were more likely to report moderate to severe changes in sleep patterns, including waking up too early, sleeping less than usual, and having trouble falling back to sleep.
- The sleep complaints were associated with poorer quality of life, suggesting that they need to be addressed more closely in PNES patients.
Latreille V, Baslet G, Sarkis R, et al. Sleep in psychogenic nonepileptic seizures: time to raise a red flag. Epilepsy Behav. 2018;86:6-8.
Analysis of Epilepsy Self-Management Skills
Although patients with epilepsy can benefit from self-management programs, a recent analysis from the Centers for Disease Control and Prevention has found that competency in self-management skills varies considerably across behavioral domains.
- Data from the Prevention Managing Epilepsy Well Network found that competencies in information and lifestyle management were considerably weaker than competencies in medication, safety, and seizure management.
- The Managing Epilepsy Well database analysis included 436 patients with epilepsy from 5 studies in the United States.
- Self-management behavioral skills were stronger in females and among patients with less education.
- The same skills were weaker in patients with depression and in those who reported a lower quality of life.
Begley C, Shegog R, Liu H, et al. Correlates of epilepsy self-management in MEW Network participants: From the Centers for Disease Control and Prevention Managing Epilepsy Well Network. Epilepsy Behav. 2018;85:243-247.
Although patients with epilepsy can benefit from self-management programs, a recent analysis from the Centers for Disease Control and Prevention has found that competency in self-management skills varies considerably across behavioral domains.
- Data from the Prevention Managing Epilepsy Well Network found that competencies in information and lifestyle management were considerably weaker than competencies in medication, safety, and seizure management.
- The Managing Epilepsy Well database analysis included 436 patients with epilepsy from 5 studies in the United States.
- Self-management behavioral skills were stronger in females and among patients with less education.
- The same skills were weaker in patients with depression and in those who reported a lower quality of life.
Begley C, Shegog R, Liu H, et al. Correlates of epilepsy self-management in MEW Network participants: From the Centers for Disease Control and Prevention Managing Epilepsy Well Network. Epilepsy Behav. 2018;85:243-247.
Although patients with epilepsy can benefit from self-management programs, a recent analysis from the Centers for Disease Control and Prevention has found that competency in self-management skills varies considerably across behavioral domains.
- Data from the Prevention Managing Epilepsy Well Network found that competencies in information and lifestyle management were considerably weaker than competencies in medication, safety, and seizure management.
- The Managing Epilepsy Well database analysis included 436 patients with epilepsy from 5 studies in the United States.
- Self-management behavioral skills were stronger in females and among patients with less education.
- The same skills were weaker in patients with depression and in those who reported a lower quality of life.
Begley C, Shegog R, Liu H, et al. Correlates of epilepsy self-management in MEW Network participants: From the Centers for Disease Control and Prevention Managing Epilepsy Well Network. Epilepsy Behav. 2018;85:243-247.
Status Epilepticus in Pregnancy
Andrew N. Wilner, MD, FAAN, FACP
Angels Neurological Centers
Abington, MA
Clinical History
A 37-year-old pregnant African American woman with a history of epilepsy and polysubstance abuse was found unresponsive in a hotel room. She had four convulsions en route to the hospital. In transit, she received levetiracetam and phenytoin, resulting in the cessation of the clinical seizures.
According to her mother, seizures began at age 16 during her first pregnancy, which was complicated by hypertension. She was prescribed medications for hypertension and phenytoin for seizures. The patient provided a different history, claiming that her seizures began 2 years ago. She denied taking medication for seizures or other health problems.
The patient has two children, ages 22 and 11 years. Past medical history is otherwise unremarkable. She has no allergies. Social history includes cigarette smoking, and alcohol and substance abuse. She lives with her boyfriend and does not work. She is 25 weeks pregnant. Family history was notable only for migraine in her mother and grandmother.
Physical Examination
In the emergency department, blood pressure was 135/65, pulse 121 beats per minute, and oxygen saturation was 97%. She was oriented only to self and did not follow commands. Pupils were equal and reactive. There was no facial asymmetry. She moved all 4 extremities spontaneously. Reflexes were brisk. Oral mucosa was dry. She had no edema in the lower extremities.
Laboratories
Chest x-ray was normal. EKG revealed tachycardia and nonspecific ST changes. Hemoglobin was 11.1 g/dl, hematocrit 32%, white blood cell count 10,900, and platelets 181,000. Electrolytes were normal except for a low sodium of 132 mmol/l (135-145) and bicarbonate of 17 mmol/l (21-31). Glucose was initially 67 mg/dl and dropped to 46 mg/dl. Total protein was 6 g/dl (6.7-8.2) and albumin was 2.7 g/dl (3.2-5.5). Metabolic panel was otherwise normal. Urinalysis was positive for glucose, ketones, and a small amount of blood and protein. There were no bacteria. Blood and urine cultures were negative. Phenytoin level was undetectable. Urine drug screen was positive for cannabinoids and cocaine.
Hospital Course
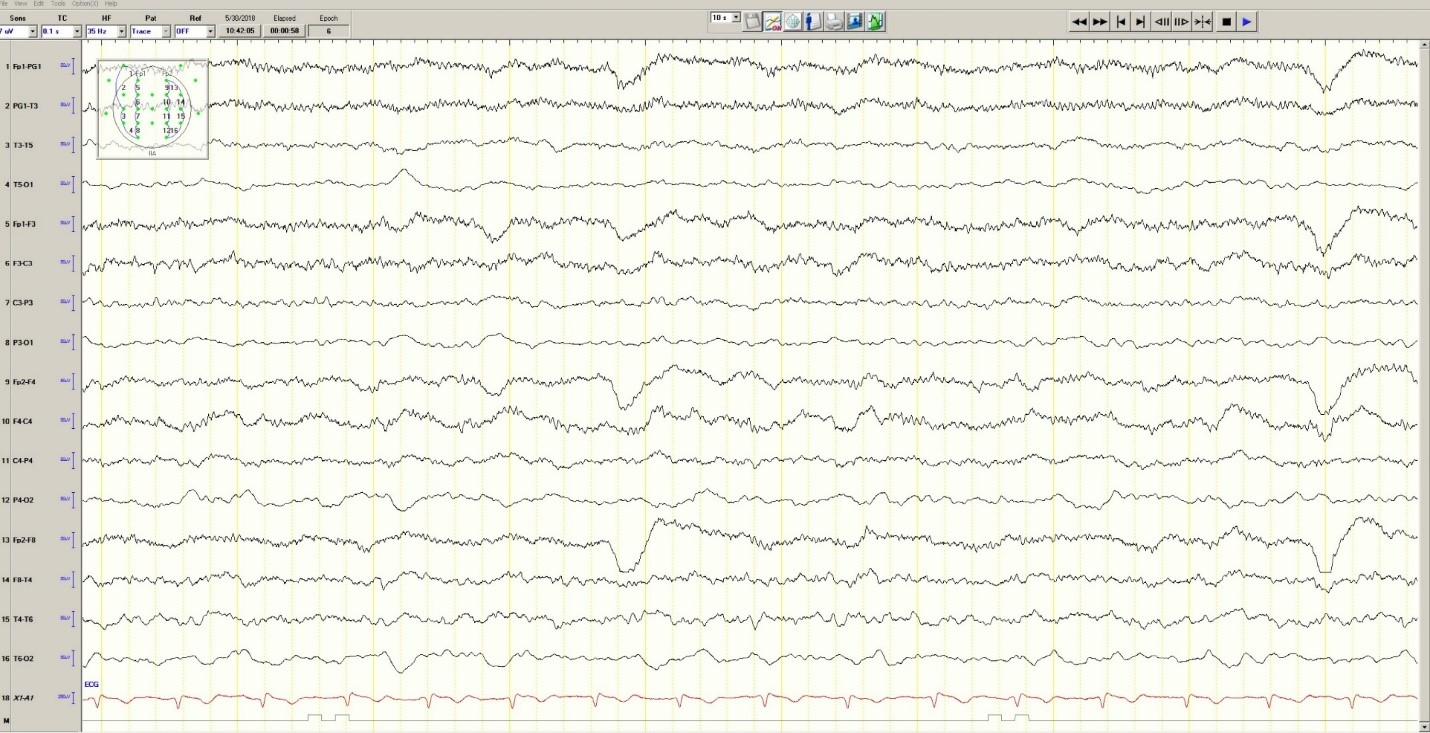
Hypoglycemia was treated with an ampule of D50 and intravenous fluids. On the obstetrics ward, nurses observed several episodes of head and eye deviation to the right accompanied by decreased responsiveness that lasted approximately 30 seconds. The patient was sent to the electrophysiology lab where an EEG revealed a diffusely slow background (Figure 1).
Figure 1. Generalized Slowing
During the 20-minute EEG recording, the patient had six clinical seizures similar to those described by the nurses. These events correlated with an ictal pattern consisting of 11 HZ_sharp activity in the right occipital temporal region that spread to the right parietal and left occipital temporal regions (Figure 2). Head CT revealed mild generalized atrophy and an enlarged right occipital horn, but no acute lesions (Figure 3).
Figure 2. Partial seizure originating in right occipital temporal region
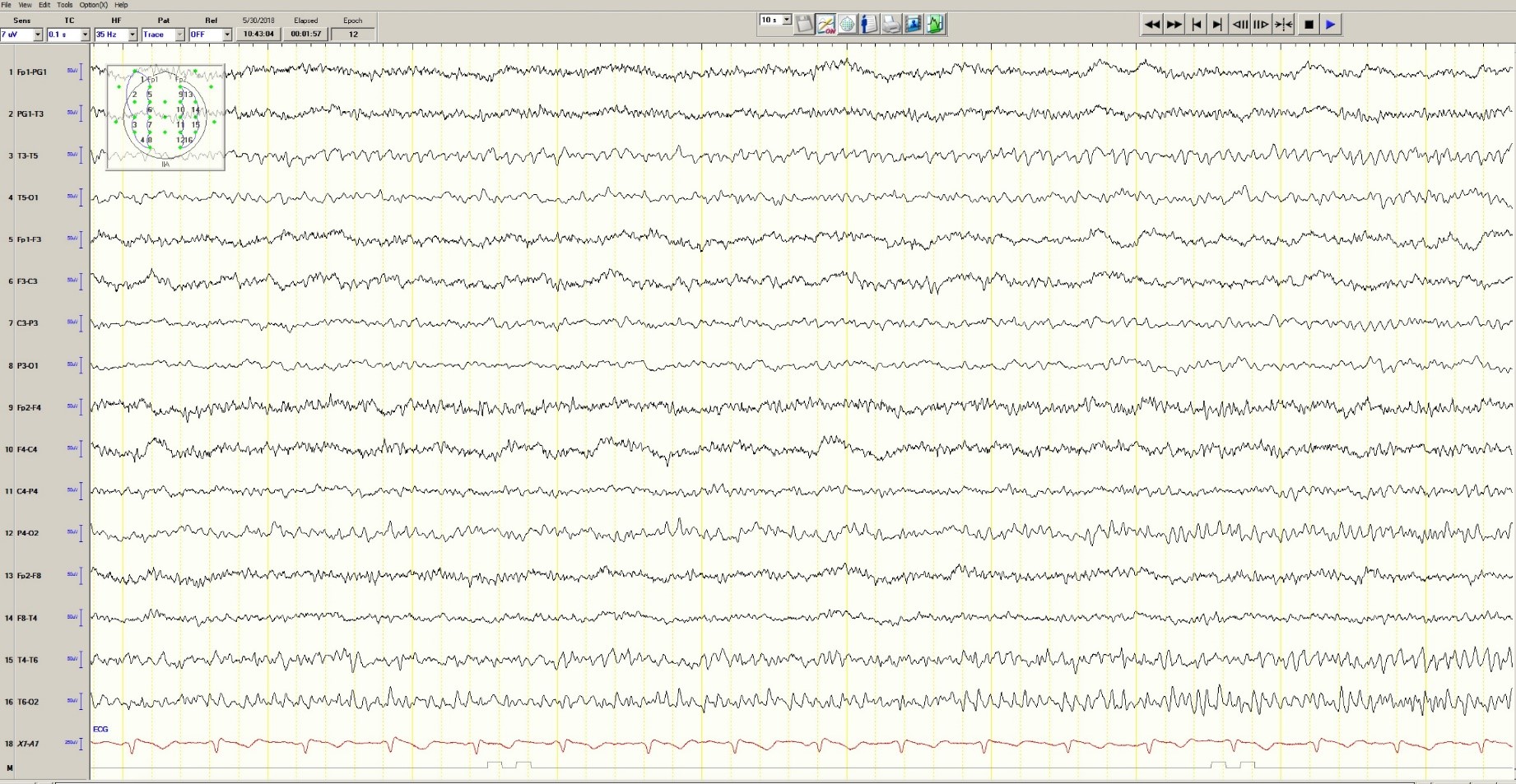
Figure 3. Mild generalized arophy, greater in right hemisphere

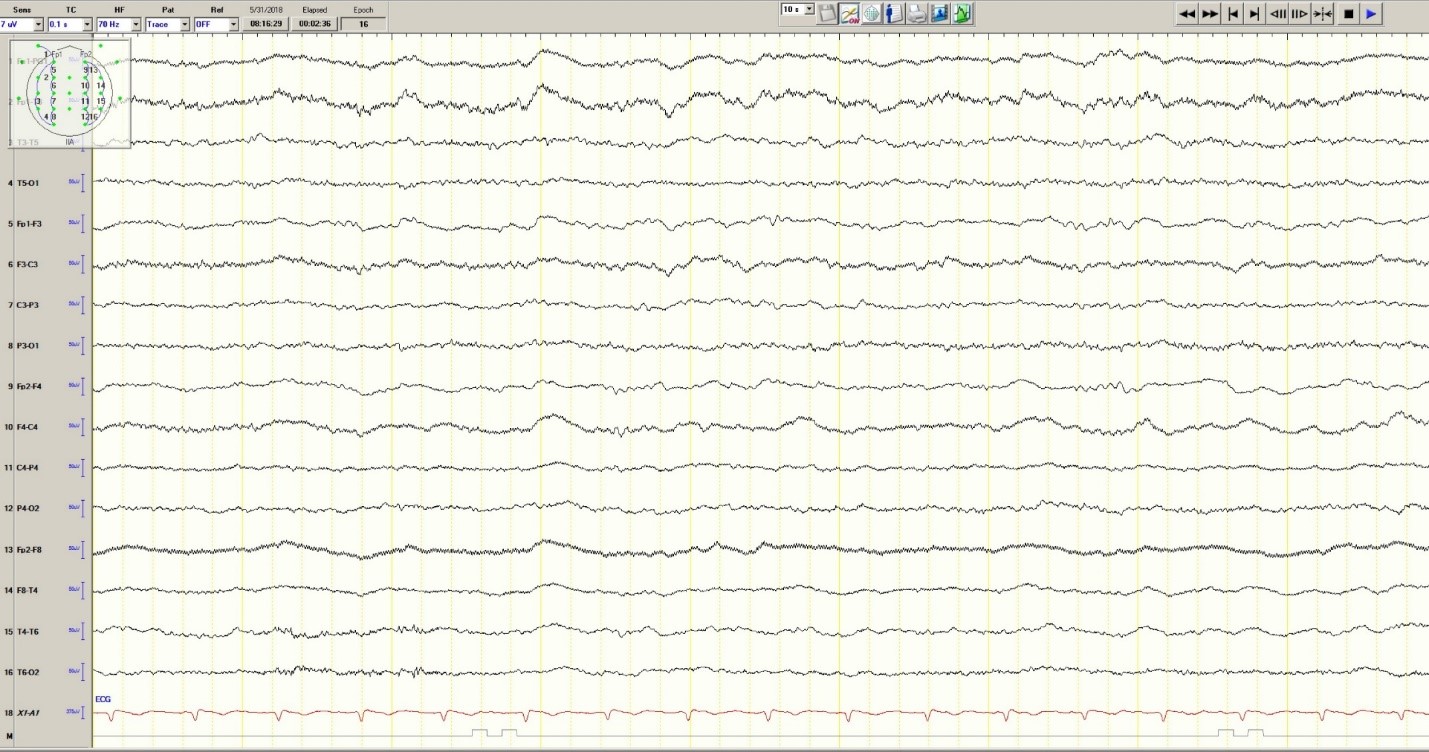
The patient was transferred to intensive care and received fosphenytoin. No further clinical and /or electrographic seizures were identified. The following day, an EEG revealed diffuse slowing without focal seizures (Figure 4). The patient gradually became more alert and cooperative over the next 24 hours. However, the next day no fetal heartbeat was detected. Labor was induced and a stillborn baby delivered. The pathology report indicated that the placenta was between the 5th and 10th percentile for gestational age.
Figure 4. Improved generalized slowing
Discussion
Status epilepticus is associated with significant morbidity and mortality (Claassen et al. 2002). This 37-year-old pregnant woman had an episode of focal status epilepticus with impaired awareness likely provoked by nonadherence to antiepileptic drugs (AEDs). Cocaine may have contributed to the episode of status epilepticus (Majlesi et al. 2010). The obstetric service did not diagnose preeclampsia.
The patient’s seizures started in the right occipital region, which was abnormal on neuroimaging. An MRI might have revealed more subtle structural abnormalities such as cortical dysplasia as the etiology of her epilepsy, but she refused the scan.
Women with epilepsy are at increased risk for adverse pregnancy outcomes such as preeclampsia, preterm labor, and stillbirth and should be considered high risk (MacDonald et al. 2015). Serum levels of AEDs such as lamotrigine, levetiracetam and phenytoin may decrease during pregnancy and contribute to breakthrough seizures. Accordingly, monthly measurements of serum levels of AEDs during the entire course of the pregnancy are strongly recommended. These measurements allow for a timely adjustment of AED doses to prevent significant drop in their serum concentrations and minimize the occurrence of breakthrough seizures. In the case of phenytoin, measurement of free and total serum concentrations are recommended. Supplementation with at least 0.4 mg/day to 1 mg /day of folic acid (and up to 4 mg /day) has been recommended (Harden et al. 2009a). Of note, there is no increase in the incidence of status epilepticus due to pregnancy per se (Harden et al. 2009b).
Although the patient survived this episode of status epilepticus, her fetus did not. Antiseizure drug nonadherence and polysubstance abuse probably contributed to fetal demise.
References
Claassen J, Lokin JK, Fitzsimons BFM et al. Predictors of functional disability and mortality after status epilepticus. Neurology. 2002;58:139-142.
Harden CL, Pennell PB, Koppel BS et al. Practice Parameter update: Management issues for women with epilepsy Focus on pregnancy (an evidence-based review): Vitamin K, folic acid, blood levels, and breastfeeding: Neurology 2009a;73:142-149.
Harden CL, Hopp J, Ting TY et al. Practice Parameter update: Management issues for women with epilepsy-focus on pregnancy (an evidence-based review): Obstetrical complications and change in seizure frequency. Neurology 2009b;50(5):1229-36.
MacDonald SC, Bateman BT, McElrath TF, Hernandez-Diaz S. Mortality and morbidity during delivery hospitalization among pregnant women with epilepsy in the United States. JAMA Neurol. 2015;72(9):981-988.
Majlesi N, Shih R, Fiesseler FW et al. Cocaine-associated seizures and incidence of status epilepticus. Western Journal of Emergency Medicine. 2010;XI(2):157-160.
Andrew N. Wilner, MD, FAAN, FACP
Angels Neurological Centers
Abington, MA
Clinical History
A 37-year-old pregnant African American woman with a history of epilepsy and polysubstance abuse was found unresponsive in a hotel room. She had four convulsions en route to the hospital. In transit, she received levetiracetam and phenytoin, resulting in the cessation of the clinical seizures.
According to her mother, seizures began at age 16 during her first pregnancy, which was complicated by hypertension. She was prescribed medications for hypertension and phenytoin for seizures. The patient provided a different history, claiming that her seizures began 2 years ago. She denied taking medication for seizures or other health problems.
The patient has two children, ages 22 and 11 years. Past medical history is otherwise unremarkable. She has no allergies. Social history includes cigarette smoking, and alcohol and substance abuse. She lives with her boyfriend and does not work. She is 25 weeks pregnant. Family history was notable only for migraine in her mother and grandmother.
Physical Examination
In the emergency department, blood pressure was 135/65, pulse 121 beats per minute, and oxygen saturation was 97%. She was oriented only to self and did not follow commands. Pupils were equal and reactive. There was no facial asymmetry. She moved all 4 extremities spontaneously. Reflexes were brisk. Oral mucosa was dry. She had no edema in the lower extremities.
Laboratories
Chest x-ray was normal. EKG revealed tachycardia and nonspecific ST changes. Hemoglobin was 11.1 g/dl, hematocrit 32%, white blood cell count 10,900, and platelets 181,000. Electrolytes were normal except for a low sodium of 132 mmol/l (135-145) and bicarbonate of 17 mmol/l (21-31). Glucose was initially 67 mg/dl and dropped to 46 mg/dl. Total protein was 6 g/dl (6.7-8.2) and albumin was 2.7 g/dl (3.2-5.5). Metabolic panel was otherwise normal. Urinalysis was positive for glucose, ketones, and a small amount of blood and protein. There were no bacteria. Blood and urine cultures were negative. Phenytoin level was undetectable. Urine drug screen was positive for cannabinoids and cocaine.
Hospital Course
Hypoglycemia was treated with an ampule of D50 and intravenous fluids. On the obstetrics ward, nurses observed several episodes of head and eye deviation to the right accompanied by decreased responsiveness that lasted approximately 30 seconds. The patient was sent to the electrophysiology lab where an EEG revealed a diffusely slow background (Figure 1).
Figure 1. Generalized Slowing
During the 20-minute EEG recording, the patient had six clinical seizures similar to those described by the nurses. These events correlated with an ictal pattern consisting of 11 HZ_sharp activity in the right occipital temporal region that spread to the right parietal and left occipital temporal regions (Figure 2). Head CT revealed mild generalized atrophy and an enlarged right occipital horn, but no acute lesions (Figure 3).
Figure 2. Partial seizure originating in right occipital temporal region
Figure 3. Mild generalized arophy, greater in right hemisphere
The patient was transferred to intensive care and received fosphenytoin. No further clinical and /or electrographic seizures were identified. The following day, an EEG revealed diffuse slowing without focal seizures (Figure 4). The patient gradually became more alert and cooperative over the next 24 hours. However, the next day no fetal heartbeat was detected. Labor was induced and a stillborn baby delivered. The pathology report indicated that the placenta was between the 5th and 10th percentile for gestational age.
Figure 4. Improved generalized slowing
Discussion
Status epilepticus is associated with significant morbidity and mortality (Claassen et al. 2002). This 37-year-old pregnant woman had an episode of focal status epilepticus with impaired awareness likely provoked by nonadherence to antiepileptic drugs (AEDs). Cocaine may have contributed to the episode of status epilepticus (Majlesi et al. 2010). The obstetric service did not diagnose preeclampsia.
The patient’s seizures started in the right occipital region, which was abnormal on neuroimaging. An MRI might have revealed more subtle structural abnormalities such as cortical dysplasia as the etiology of her epilepsy, but she refused the scan.
Women with epilepsy are at increased risk for adverse pregnancy outcomes such as preeclampsia, preterm labor, and stillbirth and should be considered high risk (MacDonald et al. 2015). Serum levels of AEDs such as lamotrigine, levetiracetam and phenytoin may decrease during pregnancy and contribute to breakthrough seizures. Accordingly, monthly measurements of serum levels of AEDs during the entire course of the pregnancy are strongly recommended. These measurements allow for a timely adjustment of AED doses to prevent significant drop in their serum concentrations and minimize the occurrence of breakthrough seizures. In the case of phenytoin, measurement of free and total serum concentrations are recommended. Supplementation with at least 0.4 mg/day to 1 mg /day of folic acid (and up to 4 mg /day) has been recommended (Harden et al. 2009a). Of note, there is no increase in the incidence of status epilepticus due to pregnancy per se (Harden et al. 2009b).
Although the patient survived this episode of status epilepticus, her fetus did not. Antiseizure drug nonadherence and polysubstance abuse probably contributed to fetal demise.
References
Claassen J, Lokin JK, Fitzsimons BFM et al. Predictors of functional disability and mortality after status epilepticus. Neurology. 2002;58:139-142.
Harden CL, Pennell PB, Koppel BS et al. Practice Parameter update: Management issues for women with epilepsy Focus on pregnancy (an evidence-based review): Vitamin K, folic acid, blood levels, and breastfeeding: Neurology 2009a;73:142-149.
Harden CL, Hopp J, Ting TY et al. Practice Parameter update: Management issues for women with epilepsy-focus on pregnancy (an evidence-based review): Obstetrical complications and change in seizure frequency. Neurology 2009b;50(5):1229-36.
MacDonald SC, Bateman BT, McElrath TF, Hernandez-Diaz S. Mortality and morbidity during delivery hospitalization among pregnant women with epilepsy in the United States. JAMA Neurol. 2015;72(9):981-988.
Majlesi N, Shih R, Fiesseler FW et al. Cocaine-associated seizures and incidence of status epilepticus. Western Journal of Emergency Medicine. 2010;XI(2):157-160.
Andrew N. Wilner, MD, FAAN, FACP
Angels Neurological Centers
Abington, MA
Clinical History
A 37-year-old pregnant African American woman with a history of epilepsy and polysubstance abuse was found unresponsive in a hotel room. She had four convulsions en route to the hospital. In transit, she received levetiracetam and phenytoin, resulting in the cessation of the clinical seizures.
According to her mother, seizures began at age 16 during her first pregnancy, which was complicated by hypertension. She was prescribed medications for hypertension and phenytoin for seizures. The patient provided a different history, claiming that her seizures began 2 years ago. She denied taking medication for seizures or other health problems.
The patient has two children, ages 22 and 11 years. Past medical history is otherwise unremarkable. She has no allergies. Social history includes cigarette smoking, and alcohol and substance abuse. She lives with her boyfriend and does not work. She is 25 weeks pregnant. Family history was notable only for migraine in her mother and grandmother.
Physical Examination
In the emergency department, blood pressure was 135/65, pulse 121 beats per minute, and oxygen saturation was 97%. She was oriented only to self and did not follow commands. Pupils were equal and reactive. There was no facial asymmetry. She moved all 4 extremities spontaneously. Reflexes were brisk. Oral mucosa was dry. She had no edema in the lower extremities.
Laboratories
Chest x-ray was normal. EKG revealed tachycardia and nonspecific ST changes. Hemoglobin was 11.1 g/dl, hematocrit 32%, white blood cell count 10,900, and platelets 181,000. Electrolytes were normal except for a low sodium of 132 mmol/l (135-145) and bicarbonate of 17 mmol/l (21-31). Glucose was initially 67 mg/dl and dropped to 46 mg/dl. Total protein was 6 g/dl (6.7-8.2) and albumin was 2.7 g/dl (3.2-5.5). Metabolic panel was otherwise normal. Urinalysis was positive for glucose, ketones, and a small amount of blood and protein. There were no bacteria. Blood and urine cultures were negative. Phenytoin level was undetectable. Urine drug screen was positive for cannabinoids and cocaine.
Hospital Course
Hypoglycemia was treated with an ampule of D50 and intravenous fluids. On the obstetrics ward, nurses observed several episodes of head and eye deviation to the right accompanied by decreased responsiveness that lasted approximately 30 seconds. The patient was sent to the electrophysiology lab where an EEG revealed a diffusely slow background (Figure 1).
Figure 1. Generalized Slowing
During the 20-minute EEG recording, the patient had six clinical seizures similar to those described by the nurses. These events correlated with an ictal pattern consisting of 11 HZ_sharp activity in the right occipital temporal region that spread to the right parietal and left occipital temporal regions (Figure 2). Head CT revealed mild generalized atrophy and an enlarged right occipital horn, but no acute lesions (Figure 3).
Figure 2. Partial seizure originating in right occipital temporal region
Figure 3. Mild generalized arophy, greater in right hemisphere
The patient was transferred to intensive care and received fosphenytoin. No further clinical and /or electrographic seizures were identified. The following day, an EEG revealed diffuse slowing without focal seizures (Figure 4). The patient gradually became more alert and cooperative over the next 24 hours. However, the next day no fetal heartbeat was detected. Labor was induced and a stillborn baby delivered. The pathology report indicated that the placenta was between the 5th and 10th percentile for gestational age.
Figure 4. Improved generalized slowing
Discussion
Status epilepticus is associated with significant morbidity and mortality (Claassen et al. 2002). This 37-year-old pregnant woman had an episode of focal status epilepticus with impaired awareness likely provoked by nonadherence to antiepileptic drugs (AEDs). Cocaine may have contributed to the episode of status epilepticus (Majlesi et al. 2010). The obstetric service did not diagnose preeclampsia.
The patient’s seizures started in the right occipital region, which was abnormal on neuroimaging. An MRI might have revealed more subtle structural abnormalities such as cortical dysplasia as the etiology of her epilepsy, but she refused the scan.
Women with epilepsy are at increased risk for adverse pregnancy outcomes such as preeclampsia, preterm labor, and stillbirth and should be considered high risk (MacDonald et al. 2015). Serum levels of AEDs such as lamotrigine, levetiracetam and phenytoin may decrease during pregnancy and contribute to breakthrough seizures. Accordingly, monthly measurements of serum levels of AEDs during the entire course of the pregnancy are strongly recommended. These measurements allow for a timely adjustment of AED doses to prevent significant drop in their serum concentrations and minimize the occurrence of breakthrough seizures. In the case of phenytoin, measurement of free and total serum concentrations are recommended. Supplementation with at least 0.4 mg/day to 1 mg /day of folic acid (and up to 4 mg /day) has been recommended (Harden et al. 2009a). Of note, there is no increase in the incidence of status epilepticus due to pregnancy per se (Harden et al. 2009b).
Although the patient survived this episode of status epilepticus, her fetus did not. Antiseizure drug nonadherence and polysubstance abuse probably contributed to fetal demise.
References
Claassen J, Lokin JK, Fitzsimons BFM et al. Predictors of functional disability and mortality after status epilepticus. Neurology. 2002;58:139-142.
Harden CL, Pennell PB, Koppel BS et al. Practice Parameter update: Management issues for women with epilepsy Focus on pregnancy (an evidence-based review): Vitamin K, folic acid, blood levels, and breastfeeding: Neurology 2009a;73:142-149.
Harden CL, Hopp J, Ting TY et al. Practice Parameter update: Management issues for women with epilepsy-focus on pregnancy (an evidence-based review): Obstetrical complications and change in seizure frequency. Neurology 2009b;50(5):1229-36.
MacDonald SC, Bateman BT, McElrath TF, Hernandez-Diaz S. Mortality and morbidity during delivery hospitalization among pregnant women with epilepsy in the United States. JAMA Neurol. 2015;72(9):981-988.
Majlesi N, Shih R, Fiesseler FW et al. Cocaine-associated seizures and incidence of status epilepticus. Western Journal of Emergency Medicine. 2010;XI(2):157-160.