User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
New guidance on palliative care for neurologic disorders
Palliative care includes much more than hospice services, lead author of the new position statement Lynne P. Taylor, MD, University of Washington, Seattle, and a fellow of the AAN, said in a press release.
“Neurologists provide palliative care to people living with life-altering neurologic illnesses not just at the end of life but throughout the course of a disease, improving their lives with symptom control,” Dr. Taylor added.
The position paper, developed by a joint committee of the AAN, American Neurological Association, and Child Neurology Society, was published online March 8 in Neurology.
Guidance across the lifespan
The new paper, an update of previous position statements, includes palliative care guidance for different neurologic disorders across the lifespan. For example, neuropalliative care for neonates deserves “extra consideration,” because one-third of pediatric deaths occur during the neonatal period, most often in the neonatal intensive care unit, and after withdrawal of life-sustaining interventions, the authors note.
For older children, neuropalliative care consultation benefits families trying to maximize the quality of the remainder of their child’s life. Decisionmaking must consider the child’s cognitive abilities, the diagnosis, the perceived level of suffering, parental values, and the family’s understanding of the prognosis, the authors note.
They note that discussions about prognosis are often difficult but critical. Previous research “supports that patients desire prognostic information even when prognosis is uncertain and appreciate when their physicians disclose the presence of that uncertainty,” the authors note.
Also important is engaging in shared decisionmaking with patients and families. “This approach requires the physician to elicit a patient’s goals, make recommendations based on whether medical treatments are likely to achieve those goals, and work with patients and families to finalize a treatment plan,” according to the new guidance.
Ethical considerations
When treatments are physiologically futile, clinicians need to explain why interventions that may cause harm and have no benefit are not offered.
The authors cite cardiopulmonary resuscitation in the setting of cardiac arrest from irreversible herniation as an example of futility in the context of neurologic disease.
When life-prolonging care is no longer an option, clinicians have an obligation to shift the focus of care to preserving quality of life and comfort as much as possible, they add.
Hospices, which provide comfort-focused medical care as well as psychosocial and spiritual support, are reserved for patients believed to be in the last 6 months of their life if their disease follows the expected course.
The investigators also broached ethical considerations for individual neurologic conditions. Concerns for disorders of consciousness include misdiagnosis or inaccurate prognostication, and serial examinations are needed to re-evaluate levels of cognition, psychological state, decisionmaking capacity, and disease trajectory.
In patients with locked-in syndrome, a state of irreversible paralysis, often with respiratory and vocal paralysis, consciousness may range from a chronic minimally conscious state to intact cognition.
Without careful examination, patients with preserved consciousness may be mistaken as having a disorder of consciousness and risk their decisional capacity being ignored, the researchers note.
These patients may need assistance from speech pathologists to identify techniques to enhance communication, such as careful “yes/no” questioning, communication boards, or advanced eye-gaze technology, they add.
Stroke, dementia, Parkinson’s guidance
For stroke, the guidance suggests neurologists encourage patients with retained decisionmaking capacity to complete advance care planning given the risk of recurrent stroke and loss of capacity in the future.
For dementia, a proper and timely diagnosis can help patients and their families prepare for the consequences of cognitive dysfunction and loss of autonomy while respecting their identified values, the authors write.
They note that for Parkinson’s disease, which is marked by slow functional and cognitive decline, neurologists must aim to anticipate and treat symptoms, address psychosocial and spiritual distress and caregiver burden, and engage patients and families in advance care planning before onset of cognitive impairment.
For patients with amyotrophic lateral sclerosis (ALS) and related disorders, clinicians should aim to document goals and treatment preferences prior to extreme weakness and aphonia.
It is also important to anticipate patient preferences for future disability-specific decisions, such as those related to feeding tubes and mechanical ventilation, and to identify the patient’s minimal acceptable outcome from these life-sustaining interventions.
On the topic of withdrawal of treatment, the paper notes that competent patients have the right to refuse life-prolonging therapies, including artificial nutrition, hydration, mechanical ventilation, and antibiotics. If physicians have a moral objection to removing life-support systems, they are obligated to transfer the care of the patient to another physician, the authors add.
Once a decision is made to forgo life-sustaining treatment, physicians should minimize subsequent suffering. The investigators note most symptoms at the end of life can be managed without sedation.
In broaching the “gap” in neurology training programs, the statement referred to a survey of 49 neurology residency programs. Results showed that 42% of respondents reported being dissatisfied with their palliative care education.
Well-timed update
Kate T. Brizzi, MD, a Boston neurologist with experience in hospice and palliative care, said the updated position statement is “well-timed” as neuropalliative care has evolved dramatically over the last decade.
“In the last several years, I’ve witnessed a significant increase in trainee interest in the field, and there is growing recognition of how a palliative care approach can improve patient care and hopefully outcomes,” said Dr. Brizzi.
She praised the authors for doing “an excellent job” in highlighting the ethical challenges facing the neurology provider, particularly as it relates to prognostication in an uncertain setting.
Dr. Brizzi noted communication tools that help facilitate discussions around shared decisionmaking “have enhanced our ability to meet the palliative care needs of our patients and can be incorporated by any provider.”
However, she added that the paper only briefly comments on the role of the neurologist in “lawful physician-hastened death.”
“I anticipate that this will be an area of further discussion in the neurology and palliative care community in the future, as requests for hastened death are frequently encountered from patients with serious neurologic illness,” she said.
Dr. Brizzi also noted the importance of understanding the reasons behind the request – and addressing patient worries related to end-of-life care, which can frequently help alleviate distress.
There was no targeted funding for this paper. Coauthor Salvador Cruz-Flores, MD, department of neurology, Texas Tech University Center, El Paso, reported participation on member adjudication committees for clinical trials for Novo Nordisk, Sunovion, and Galapagos. The remaining authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Palliative care includes much more than hospice services, lead author of the new position statement Lynne P. Taylor, MD, University of Washington, Seattle, and a fellow of the AAN, said in a press release.
“Neurologists provide palliative care to people living with life-altering neurologic illnesses not just at the end of life but throughout the course of a disease, improving their lives with symptom control,” Dr. Taylor added.
The position paper, developed by a joint committee of the AAN, American Neurological Association, and Child Neurology Society, was published online March 8 in Neurology.
Guidance across the lifespan
The new paper, an update of previous position statements, includes palliative care guidance for different neurologic disorders across the lifespan. For example, neuropalliative care for neonates deserves “extra consideration,” because one-third of pediatric deaths occur during the neonatal period, most often in the neonatal intensive care unit, and after withdrawal of life-sustaining interventions, the authors note.
For older children, neuropalliative care consultation benefits families trying to maximize the quality of the remainder of their child’s life. Decisionmaking must consider the child’s cognitive abilities, the diagnosis, the perceived level of suffering, parental values, and the family’s understanding of the prognosis, the authors note.
They note that discussions about prognosis are often difficult but critical. Previous research “supports that patients desire prognostic information even when prognosis is uncertain and appreciate when their physicians disclose the presence of that uncertainty,” the authors note.
Also important is engaging in shared decisionmaking with patients and families. “This approach requires the physician to elicit a patient’s goals, make recommendations based on whether medical treatments are likely to achieve those goals, and work with patients and families to finalize a treatment plan,” according to the new guidance.
Ethical considerations
When treatments are physiologically futile, clinicians need to explain why interventions that may cause harm and have no benefit are not offered.
The authors cite cardiopulmonary resuscitation in the setting of cardiac arrest from irreversible herniation as an example of futility in the context of neurologic disease.
When life-prolonging care is no longer an option, clinicians have an obligation to shift the focus of care to preserving quality of life and comfort as much as possible, they add.
Hospices, which provide comfort-focused medical care as well as psychosocial and spiritual support, are reserved for patients believed to be in the last 6 months of their life if their disease follows the expected course.
The investigators also broached ethical considerations for individual neurologic conditions. Concerns for disorders of consciousness include misdiagnosis or inaccurate prognostication, and serial examinations are needed to re-evaluate levels of cognition, psychological state, decisionmaking capacity, and disease trajectory.
In patients with locked-in syndrome, a state of irreversible paralysis, often with respiratory and vocal paralysis, consciousness may range from a chronic minimally conscious state to intact cognition.
Without careful examination, patients with preserved consciousness may be mistaken as having a disorder of consciousness and risk their decisional capacity being ignored, the researchers note.
These patients may need assistance from speech pathologists to identify techniques to enhance communication, such as careful “yes/no” questioning, communication boards, or advanced eye-gaze technology, they add.
Stroke, dementia, Parkinson’s guidance
For stroke, the guidance suggests neurologists encourage patients with retained decisionmaking capacity to complete advance care planning given the risk of recurrent stroke and loss of capacity in the future.
For dementia, a proper and timely diagnosis can help patients and their families prepare for the consequences of cognitive dysfunction and loss of autonomy while respecting their identified values, the authors write.
They note that for Parkinson’s disease, which is marked by slow functional and cognitive decline, neurologists must aim to anticipate and treat symptoms, address psychosocial and spiritual distress and caregiver burden, and engage patients and families in advance care planning before onset of cognitive impairment.
For patients with amyotrophic lateral sclerosis (ALS) and related disorders, clinicians should aim to document goals and treatment preferences prior to extreme weakness and aphonia.
It is also important to anticipate patient preferences for future disability-specific decisions, such as those related to feeding tubes and mechanical ventilation, and to identify the patient’s minimal acceptable outcome from these life-sustaining interventions.
On the topic of withdrawal of treatment, the paper notes that competent patients have the right to refuse life-prolonging therapies, including artificial nutrition, hydration, mechanical ventilation, and antibiotics. If physicians have a moral objection to removing life-support systems, they are obligated to transfer the care of the patient to another physician, the authors add.
Once a decision is made to forgo life-sustaining treatment, physicians should minimize subsequent suffering. The investigators note most symptoms at the end of life can be managed without sedation.
In broaching the “gap” in neurology training programs, the statement referred to a survey of 49 neurology residency programs. Results showed that 42% of respondents reported being dissatisfied with their palliative care education.
Well-timed update
Kate T. Brizzi, MD, a Boston neurologist with experience in hospice and palliative care, said the updated position statement is “well-timed” as neuropalliative care has evolved dramatically over the last decade.
“In the last several years, I’ve witnessed a significant increase in trainee interest in the field, and there is growing recognition of how a palliative care approach can improve patient care and hopefully outcomes,” said Dr. Brizzi.
She praised the authors for doing “an excellent job” in highlighting the ethical challenges facing the neurology provider, particularly as it relates to prognostication in an uncertain setting.
Dr. Brizzi noted communication tools that help facilitate discussions around shared decisionmaking “have enhanced our ability to meet the palliative care needs of our patients and can be incorporated by any provider.”
However, she added that the paper only briefly comments on the role of the neurologist in “lawful physician-hastened death.”
“I anticipate that this will be an area of further discussion in the neurology and palliative care community in the future, as requests for hastened death are frequently encountered from patients with serious neurologic illness,” she said.
Dr. Brizzi also noted the importance of understanding the reasons behind the request – and addressing patient worries related to end-of-life care, which can frequently help alleviate distress.
There was no targeted funding for this paper. Coauthor Salvador Cruz-Flores, MD, department of neurology, Texas Tech University Center, El Paso, reported participation on member adjudication committees for clinical trials for Novo Nordisk, Sunovion, and Galapagos. The remaining authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Palliative care includes much more than hospice services, lead author of the new position statement Lynne P. Taylor, MD, University of Washington, Seattle, and a fellow of the AAN, said in a press release.
“Neurologists provide palliative care to people living with life-altering neurologic illnesses not just at the end of life but throughout the course of a disease, improving their lives with symptom control,” Dr. Taylor added.
The position paper, developed by a joint committee of the AAN, American Neurological Association, and Child Neurology Society, was published online March 8 in Neurology.
Guidance across the lifespan
The new paper, an update of previous position statements, includes palliative care guidance for different neurologic disorders across the lifespan. For example, neuropalliative care for neonates deserves “extra consideration,” because one-third of pediatric deaths occur during the neonatal period, most often in the neonatal intensive care unit, and after withdrawal of life-sustaining interventions, the authors note.
For older children, neuropalliative care consultation benefits families trying to maximize the quality of the remainder of their child’s life. Decisionmaking must consider the child’s cognitive abilities, the diagnosis, the perceived level of suffering, parental values, and the family’s understanding of the prognosis, the authors note.
They note that discussions about prognosis are often difficult but critical. Previous research “supports that patients desire prognostic information even when prognosis is uncertain and appreciate when their physicians disclose the presence of that uncertainty,” the authors note.
Also important is engaging in shared decisionmaking with patients and families. “This approach requires the physician to elicit a patient’s goals, make recommendations based on whether medical treatments are likely to achieve those goals, and work with patients and families to finalize a treatment plan,” according to the new guidance.
Ethical considerations
When treatments are physiologically futile, clinicians need to explain why interventions that may cause harm and have no benefit are not offered.
The authors cite cardiopulmonary resuscitation in the setting of cardiac arrest from irreversible herniation as an example of futility in the context of neurologic disease.
When life-prolonging care is no longer an option, clinicians have an obligation to shift the focus of care to preserving quality of life and comfort as much as possible, they add.
Hospices, which provide comfort-focused medical care as well as psychosocial and spiritual support, are reserved for patients believed to be in the last 6 months of their life if their disease follows the expected course.
The investigators also broached ethical considerations for individual neurologic conditions. Concerns for disorders of consciousness include misdiagnosis or inaccurate prognostication, and serial examinations are needed to re-evaluate levels of cognition, psychological state, decisionmaking capacity, and disease trajectory.
In patients with locked-in syndrome, a state of irreversible paralysis, often with respiratory and vocal paralysis, consciousness may range from a chronic minimally conscious state to intact cognition.
Without careful examination, patients with preserved consciousness may be mistaken as having a disorder of consciousness and risk their decisional capacity being ignored, the researchers note.
These patients may need assistance from speech pathologists to identify techniques to enhance communication, such as careful “yes/no” questioning, communication boards, or advanced eye-gaze technology, they add.
Stroke, dementia, Parkinson’s guidance
For stroke, the guidance suggests neurologists encourage patients with retained decisionmaking capacity to complete advance care planning given the risk of recurrent stroke and loss of capacity in the future.
For dementia, a proper and timely diagnosis can help patients and their families prepare for the consequences of cognitive dysfunction and loss of autonomy while respecting their identified values, the authors write.
They note that for Parkinson’s disease, which is marked by slow functional and cognitive decline, neurologists must aim to anticipate and treat symptoms, address psychosocial and spiritual distress and caregiver burden, and engage patients and families in advance care planning before onset of cognitive impairment.
For patients with amyotrophic lateral sclerosis (ALS) and related disorders, clinicians should aim to document goals and treatment preferences prior to extreme weakness and aphonia.
It is also important to anticipate patient preferences for future disability-specific decisions, such as those related to feeding tubes and mechanical ventilation, and to identify the patient’s minimal acceptable outcome from these life-sustaining interventions.
On the topic of withdrawal of treatment, the paper notes that competent patients have the right to refuse life-prolonging therapies, including artificial nutrition, hydration, mechanical ventilation, and antibiotics. If physicians have a moral objection to removing life-support systems, they are obligated to transfer the care of the patient to another physician, the authors add.
Once a decision is made to forgo life-sustaining treatment, physicians should minimize subsequent suffering. The investigators note most symptoms at the end of life can be managed without sedation.
In broaching the “gap” in neurology training programs, the statement referred to a survey of 49 neurology residency programs. Results showed that 42% of respondents reported being dissatisfied with their palliative care education.
Well-timed update
Kate T. Brizzi, MD, a Boston neurologist with experience in hospice and palliative care, said the updated position statement is “well-timed” as neuropalliative care has evolved dramatically over the last decade.
“In the last several years, I’ve witnessed a significant increase in trainee interest in the field, and there is growing recognition of how a palliative care approach can improve patient care and hopefully outcomes,” said Dr. Brizzi.
She praised the authors for doing “an excellent job” in highlighting the ethical challenges facing the neurology provider, particularly as it relates to prognostication in an uncertain setting.
Dr. Brizzi noted communication tools that help facilitate discussions around shared decisionmaking “have enhanced our ability to meet the palliative care needs of our patients and can be incorporated by any provider.”
However, she added that the paper only briefly comments on the role of the neurologist in “lawful physician-hastened death.”
“I anticipate that this will be an area of further discussion in the neurology and palliative care community in the future, as requests for hastened death are frequently encountered from patients with serious neurologic illness,” she said.
Dr. Brizzi also noted the importance of understanding the reasons behind the request – and addressing patient worries related to end-of-life care, which can frequently help alleviate distress.
There was no targeted funding for this paper. Coauthor Salvador Cruz-Flores, MD, department of neurology, Texas Tech University Center, El Paso, reported participation on member adjudication committees for clinical trials for Novo Nordisk, Sunovion, and Galapagos. The remaining authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From Neurology
FDA approves first PARP inhibitor for early BRCA+ breast cancer
BRCA+ breast cancer
Specifically, the new approval is for the adjuvant treatment of adult patients with high-risk early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The FDA also approved BRACAnalysis CDx (Myriad Genetics), a companion diagnostic test to identify patients who may benefit from olaparib.
The latest approval was based on phase 3 OlympiA trial results, which showed a 42% improvement in invasive and distant disease-free survival with olaparib in comparison with placebo. Data from OlympiaA and other clinical studies also confirm BRACAnalysis CDx as “an effective test for patients deciding on their best treatment options,” Myriad Genetics noted in a press release.
The OlympiA results, as reported by this news organization, were presented during the plenary session of the American Society of Clinical Oncology 2021 annual meeting and were published in the New England Journal of Medicine.
Those findings prompted an ASCO “rapid recommendation” updating of ASCO’s 2020 guidelines for the management of hereditary breast cancer.
The latest results from OlympiA show that olaparib reduced the risk of death by 32% (hazard ratio, 0.68) in comparison with placebo, according to a company press release announcing the approval. Overall survival data are slated for presentation at a European Society for Medical Oncology Virtual Plenary session on March 16, 2022.
A version of this article first appeared on Medscape.com.
Specifically, the new approval is for the adjuvant treatment of adult patients with high-risk early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The FDA also approved BRACAnalysis CDx (Myriad Genetics), a companion diagnostic test to identify patients who may benefit from olaparib.
The latest approval was based on phase 3 OlympiA trial results, which showed a 42% improvement in invasive and distant disease-free survival with olaparib in comparison with placebo. Data from OlympiaA and other clinical studies also confirm BRACAnalysis CDx as “an effective test for patients deciding on their best treatment options,” Myriad Genetics noted in a press release.
The OlympiA results, as reported by this news organization, were presented during the plenary session of the American Society of Clinical Oncology 2021 annual meeting and were published in the New England Journal of Medicine.
Those findings prompted an ASCO “rapid recommendation” updating of ASCO’s 2020 guidelines for the management of hereditary breast cancer.
The latest results from OlympiA show that olaparib reduced the risk of death by 32% (hazard ratio, 0.68) in comparison with placebo, according to a company press release announcing the approval. Overall survival data are slated for presentation at a European Society for Medical Oncology Virtual Plenary session on March 16, 2022.
A version of this article first appeared on Medscape.com.
Specifically, the new approval is for the adjuvant treatment of adult patients with high-risk early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The FDA also approved BRACAnalysis CDx (Myriad Genetics), a companion diagnostic test to identify patients who may benefit from olaparib.
The latest approval was based on phase 3 OlympiA trial results, which showed a 42% improvement in invasive and distant disease-free survival with olaparib in comparison with placebo. Data from OlympiaA and other clinical studies also confirm BRACAnalysis CDx as “an effective test for patients deciding on their best treatment options,” Myriad Genetics noted in a press release.
The OlympiA results, as reported by this news organization, were presented during the plenary session of the American Society of Clinical Oncology 2021 annual meeting and were published in the New England Journal of Medicine.
Those findings prompted an ASCO “rapid recommendation” updating of ASCO’s 2020 guidelines for the management of hereditary breast cancer.
The latest results from OlympiA show that olaparib reduced the risk of death by 32% (hazard ratio, 0.68) in comparison with placebo, according to a company press release announcing the approval. Overall survival data are slated for presentation at a European Society for Medical Oncology Virtual Plenary session on March 16, 2022.
A version of this article first appeared on Medscape.com.
BRCA+ breast cancer
BRCA+ breast cancer
Registry data support lowering CRC screening age to 45
Approximately one-third of people between 45 and 49 years of age who undergo colonoscopies have neoplastic colorectal pathology, according to a retrospective analysis.
According to the researchers, led by Parth Trivedi, MD, of the Icahn School of Medicine at Mount Sinai, New York, there has progressively been a “disturbing” rise in early-onset colorectal cancer (CRC) in the United States, which has prompted guidelines from the American Cancer Society to the U.S. Preventive Services Task Force to recommend lowering the CRC screening starting age to 45 years old for average-risk individuals. Despite these recommendations, little research to date has fully characterized the prevalence of colorectal neoplasia in individuals younger than the currently recommended CRC onset screening age of 50 years.
Dr. Trivedi and colleagues, who published their study findings in Gastroenterology, retrospectively reviewed colonoscopy data recorded in the Gastrointestinal Quality Improvement Consortium Registry to address the current knowledge gaps on early-onset CRC. Collected data were for procedures conducted at 123 AMSURG ambulatory endoscopy centers across 29 states between January 2014 and February 2021. In total, 2,921,816 colonoscopies during the study period among patients aged 18-54 years were recorded by AMSURG-associated endoscopists; of these, 562,559 met inclusion criteria for high-quality screening or diagnostic colonoscopy procedures.
The researchers pooled a young-onset age group, including patients between the ages of 18 and 49 years old, in whom 145,998 procedures were performed, including 79,934 procedures in patients aged 45-49 years. A comparator group with 336,627 procedures in patients aged 50-54 years was also included in the study. The findings were categorized into CRC, advanced premalignant lesions (APL), and “any neoplasia,” the latter of which included all adenomas, sessile serrated polyps, and CRC.
Among patients aged 18-44 years, the most frequent indications were “diagnostic-other” (45.6%) as well as “diagnostic-bleeding” (39.4%). Among patients between 45 and 49 years of age, the most frequent indications were “screening” (41.4%) and “diagnostic-other” (30.7%). Nearly all (90%) procedures among those aged 50-54 years were for screening.
A multivariable logistic regression identified 5 variables predictive of either APL or CRC in patients between 18 and 49 years of age: increasing age (odds ratio, 1.08; 95% confidence interval, 1.07-1.08; P <0.01), male sex (OR = 1.67; 95% CI, 1.63-1.70; P <0.01), White race (vs. African American: OR = 0.76; 95% CI, 0.73-0.79, P <0.01; vs. Asian: OR = 0.89; 95% CI, 0.84-0.94, P <0.01), family history of CRC (OR = 1.21; 95% CI, 1.16-1.26; P <0.01) and polyps (OR = 1.33; 95% CI, 1.24-1.43; P <0.01), and examinations for bleeding (OR = 1.15; 95% CI, 1.12-1.18; P <0.01) or screening (OR = 1.20; 95% CI, 1.16-1.24; P <0.01).
The prevalence of neoplastic findings in the young-onset age-group increased with increasing age for the categories of any neoplasia, APLs, and CRC. Among patients aged 40-44, 26.59% had any neoplasia, 5.76% had APL, and 0.53% had CRC. In those aged 45-49 years, around 32% had any neoplasia, approximately 7.5% had APLs, and nearly 0.58% had CRC. In the 50- to 54-year-old group, the prevalences of any neoplasia, APL, and CRC were 37.72%, 9.48%, and 0.32%, respectively.
Across all age groups, a family history of CRC was associated with a higher prevalence of any neoplasia and APL. In addition, the rates of any APL and neoplasia in patients with a family history of CRC were comparable to patients who were 5 years older but had no family history of the disease. Across most young-onset age group, individuals with a positive family history had a lower CRC prevalence versus patients with no family history.
The researchers noted that their population data are derived from ambulatory endoscopy centers, which may introduce bias associated with insurance coverage or patient preference to attend specific endoscopic centers. Additionally, the investigators stated that many records on race and ethnicity were missing, further limiting the findings.
“The present analysis of neoplastic colorectal pathology among individuals younger than age 50 suggests that lowering the screening age to 45 for men and women of all races and ethnicities will likely detect important pathology rather frequently,” they concluded. In addition, the researchers noted that the study results “underscore the importance of early messaging to patients and providers in the years leading up to age 45.” Ultimately, improved “awareness of pathology prevalence in individuals younger than age 45 can help guide clinicians in the clinical management of CRC risk,” the researchers wrote.
Several of the researchers reported conflicts of interest with Exact Sciences Corp and Freenome. The study received no industry funding.
Approximately one-third of people between 45 and 49 years of age who undergo colonoscopies have neoplastic colorectal pathology, according to a retrospective analysis.
According to the researchers, led by Parth Trivedi, MD, of the Icahn School of Medicine at Mount Sinai, New York, there has progressively been a “disturbing” rise in early-onset colorectal cancer (CRC) in the United States, which has prompted guidelines from the American Cancer Society to the U.S. Preventive Services Task Force to recommend lowering the CRC screening starting age to 45 years old for average-risk individuals. Despite these recommendations, little research to date has fully characterized the prevalence of colorectal neoplasia in individuals younger than the currently recommended CRC onset screening age of 50 years.
Dr. Trivedi and colleagues, who published their study findings in Gastroenterology, retrospectively reviewed colonoscopy data recorded in the Gastrointestinal Quality Improvement Consortium Registry to address the current knowledge gaps on early-onset CRC. Collected data were for procedures conducted at 123 AMSURG ambulatory endoscopy centers across 29 states between January 2014 and February 2021. In total, 2,921,816 colonoscopies during the study period among patients aged 18-54 years were recorded by AMSURG-associated endoscopists; of these, 562,559 met inclusion criteria for high-quality screening or diagnostic colonoscopy procedures.
The researchers pooled a young-onset age group, including patients between the ages of 18 and 49 years old, in whom 145,998 procedures were performed, including 79,934 procedures in patients aged 45-49 years. A comparator group with 336,627 procedures in patients aged 50-54 years was also included in the study. The findings were categorized into CRC, advanced premalignant lesions (APL), and “any neoplasia,” the latter of which included all adenomas, sessile serrated polyps, and CRC.
Among patients aged 18-44 years, the most frequent indications were “diagnostic-other” (45.6%) as well as “diagnostic-bleeding” (39.4%). Among patients between 45 and 49 years of age, the most frequent indications were “screening” (41.4%) and “diagnostic-other” (30.7%). Nearly all (90%) procedures among those aged 50-54 years were for screening.
A multivariable logistic regression identified 5 variables predictive of either APL or CRC in patients between 18 and 49 years of age: increasing age (odds ratio, 1.08; 95% confidence interval, 1.07-1.08; P <0.01), male sex (OR = 1.67; 95% CI, 1.63-1.70; P <0.01), White race (vs. African American: OR = 0.76; 95% CI, 0.73-0.79, P <0.01; vs. Asian: OR = 0.89; 95% CI, 0.84-0.94, P <0.01), family history of CRC (OR = 1.21; 95% CI, 1.16-1.26; P <0.01) and polyps (OR = 1.33; 95% CI, 1.24-1.43; P <0.01), and examinations for bleeding (OR = 1.15; 95% CI, 1.12-1.18; P <0.01) or screening (OR = 1.20; 95% CI, 1.16-1.24; P <0.01).
The prevalence of neoplastic findings in the young-onset age-group increased with increasing age for the categories of any neoplasia, APLs, and CRC. Among patients aged 40-44, 26.59% had any neoplasia, 5.76% had APL, and 0.53% had CRC. In those aged 45-49 years, around 32% had any neoplasia, approximately 7.5% had APLs, and nearly 0.58% had CRC. In the 50- to 54-year-old group, the prevalences of any neoplasia, APL, and CRC were 37.72%, 9.48%, and 0.32%, respectively.
Across all age groups, a family history of CRC was associated with a higher prevalence of any neoplasia and APL. In addition, the rates of any APL and neoplasia in patients with a family history of CRC were comparable to patients who were 5 years older but had no family history of the disease. Across most young-onset age group, individuals with a positive family history had a lower CRC prevalence versus patients with no family history.
The researchers noted that their population data are derived from ambulatory endoscopy centers, which may introduce bias associated with insurance coverage or patient preference to attend specific endoscopic centers. Additionally, the investigators stated that many records on race and ethnicity were missing, further limiting the findings.
“The present analysis of neoplastic colorectal pathology among individuals younger than age 50 suggests that lowering the screening age to 45 for men and women of all races and ethnicities will likely detect important pathology rather frequently,” they concluded. In addition, the researchers noted that the study results “underscore the importance of early messaging to patients and providers in the years leading up to age 45.” Ultimately, improved “awareness of pathology prevalence in individuals younger than age 45 can help guide clinicians in the clinical management of CRC risk,” the researchers wrote.
Several of the researchers reported conflicts of interest with Exact Sciences Corp and Freenome. The study received no industry funding.
Approximately one-third of people between 45 and 49 years of age who undergo colonoscopies have neoplastic colorectal pathology, according to a retrospective analysis.
According to the researchers, led by Parth Trivedi, MD, of the Icahn School of Medicine at Mount Sinai, New York, there has progressively been a “disturbing” rise in early-onset colorectal cancer (CRC) in the United States, which has prompted guidelines from the American Cancer Society to the U.S. Preventive Services Task Force to recommend lowering the CRC screening starting age to 45 years old for average-risk individuals. Despite these recommendations, little research to date has fully characterized the prevalence of colorectal neoplasia in individuals younger than the currently recommended CRC onset screening age of 50 years.
Dr. Trivedi and colleagues, who published their study findings in Gastroenterology, retrospectively reviewed colonoscopy data recorded in the Gastrointestinal Quality Improvement Consortium Registry to address the current knowledge gaps on early-onset CRC. Collected data were for procedures conducted at 123 AMSURG ambulatory endoscopy centers across 29 states between January 2014 and February 2021. In total, 2,921,816 colonoscopies during the study period among patients aged 18-54 years were recorded by AMSURG-associated endoscopists; of these, 562,559 met inclusion criteria for high-quality screening or diagnostic colonoscopy procedures.
The researchers pooled a young-onset age group, including patients between the ages of 18 and 49 years old, in whom 145,998 procedures were performed, including 79,934 procedures in patients aged 45-49 years. A comparator group with 336,627 procedures in patients aged 50-54 years was also included in the study. The findings were categorized into CRC, advanced premalignant lesions (APL), and “any neoplasia,” the latter of which included all adenomas, sessile serrated polyps, and CRC.
Among patients aged 18-44 years, the most frequent indications were “diagnostic-other” (45.6%) as well as “diagnostic-bleeding” (39.4%). Among patients between 45 and 49 years of age, the most frequent indications were “screening” (41.4%) and “diagnostic-other” (30.7%). Nearly all (90%) procedures among those aged 50-54 years were for screening.
A multivariable logistic regression identified 5 variables predictive of either APL or CRC in patients between 18 and 49 years of age: increasing age (odds ratio, 1.08; 95% confidence interval, 1.07-1.08; P <0.01), male sex (OR = 1.67; 95% CI, 1.63-1.70; P <0.01), White race (vs. African American: OR = 0.76; 95% CI, 0.73-0.79, P <0.01; vs. Asian: OR = 0.89; 95% CI, 0.84-0.94, P <0.01), family history of CRC (OR = 1.21; 95% CI, 1.16-1.26; P <0.01) and polyps (OR = 1.33; 95% CI, 1.24-1.43; P <0.01), and examinations for bleeding (OR = 1.15; 95% CI, 1.12-1.18; P <0.01) or screening (OR = 1.20; 95% CI, 1.16-1.24; P <0.01).
The prevalence of neoplastic findings in the young-onset age-group increased with increasing age for the categories of any neoplasia, APLs, and CRC. Among patients aged 40-44, 26.59% had any neoplasia, 5.76% had APL, and 0.53% had CRC. In those aged 45-49 years, around 32% had any neoplasia, approximately 7.5% had APLs, and nearly 0.58% had CRC. In the 50- to 54-year-old group, the prevalences of any neoplasia, APL, and CRC were 37.72%, 9.48%, and 0.32%, respectively.
Across all age groups, a family history of CRC was associated with a higher prevalence of any neoplasia and APL. In addition, the rates of any APL and neoplasia in patients with a family history of CRC were comparable to patients who were 5 years older but had no family history of the disease. Across most young-onset age group, individuals with a positive family history had a lower CRC prevalence versus patients with no family history.
The researchers noted that their population data are derived from ambulatory endoscopy centers, which may introduce bias associated with insurance coverage or patient preference to attend specific endoscopic centers. Additionally, the investigators stated that many records on race and ethnicity were missing, further limiting the findings.
“The present analysis of neoplastic colorectal pathology among individuals younger than age 50 suggests that lowering the screening age to 45 for men and women of all races and ethnicities will likely detect important pathology rather frequently,” they concluded. In addition, the researchers noted that the study results “underscore the importance of early messaging to patients and providers in the years leading up to age 45.” Ultimately, improved “awareness of pathology prevalence in individuals younger than age 45 can help guide clinicians in the clinical management of CRC risk,” the researchers wrote.
Several of the researchers reported conflicts of interest with Exact Sciences Corp and Freenome. The study received no industry funding.
FROM GASTROENTEROLOGY
Children and COVID: Decline in new cases reaches 7th week
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.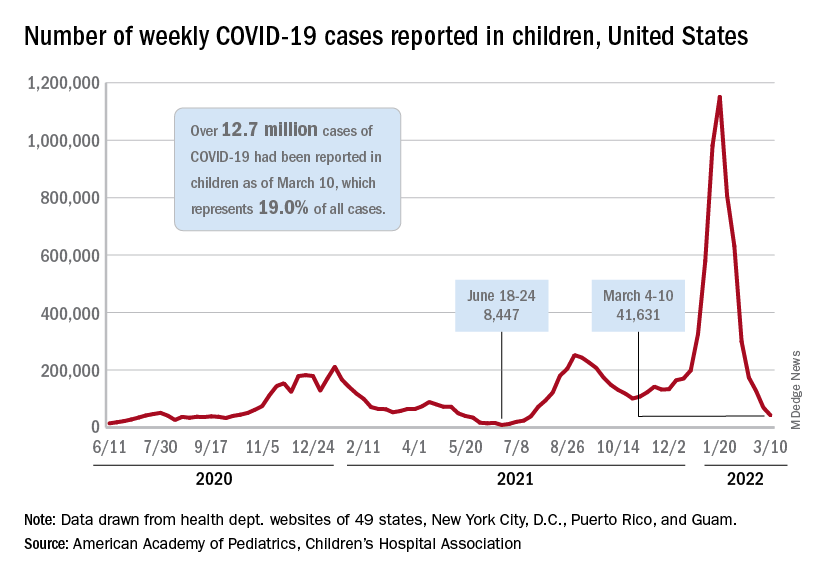
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
New cases of COVID-19 in U.S. children have fallen to their lowest level since the beginning of the Delta surge in July of 2021, according to the American Academy of Pediatrics and the Children’s Hospital Association.
. Over those 7 weeks, new cases dropped over 96% from the 1.15 million reported for Jan. 14-20, based on data collected by the AAP and CHA from state and territorial health departments.
The last time that the weekly count was below 42,000 was July 16-22, 2021, when almost 39,000 cases were reported in the midst of the Delta upsurge. That was shortly after cases had reached their lowest point, 8,447, since the early stages of the pandemic in 2020, the AAP/CHA data show.
The cumulative number of pediatric cases is now up to 12.7 million, while the overall proportion of cases occurring in children held steady at 19.0% for the 4th week in a row, the AAP and CHA said in their weekly COVID-19 report. The Centers for Disease Control and Prevention, using an age range of 0-18 versus the states’ variety of ages, puts total cases at 11.7 million and deaths at 1,656 as of March 14.
Data from the CDC’s COVID-19–Associated Hospitalization Surveillance Network show that hospitalizations with laboratory-confirmed infection were down by 50% in children aged 0-4 years, by 63% among 5- to 11-year-olds, and by 58% in those aged 12-17 years for the week of Feb. 27 to March 5, compared with the week before.
The pace of vaccination continues to follow a similar trend, as the declines seen through February have continued into March. Cumulatively, 33.7% of children aged 5-11 have received at least one dose, and 26.8% are fully vaccinated, with corresponding numbers of 68.0% and 58.0% for children aged 12-17, the CDC reported on its COVID Data Tracker.
State-level data show that children aged 5-11 in Vermont, with a rate of 65%, are the most likely to have received at least one dose of COVID vaccine, while just 15% of 5- to 11-year-olds in Alabama, Louisiana, and Mississippi have gotten their first dose. Among children aged 12-17, that rate ranges from 40% in Wyoming to 94% in Hawaii, Massachusetts, and Rhode Island, the AAP said in a separate report based on CDC data.
In a recent report involving 1,364 children aged 5-15 years, two doses of the COVID-19 vaccine reduced the risk of infection from the Omicron variant by 31% in children aged 5-11 years and by 59% among children aged 12-15 years, said Ashley L. Fowlkes, ScD, of the CDC’s COVID-19 Emergency Response Team, and associates (MMWR 2022 Mar 11;71).
CPAP has only small effect on metabolic syndrome
Continuous positive airway pressure (CPAP) may be only modestly effective for ameliorating metabolic syndrome in patients with moderate to severe obstructive sleep apnea (OSA).
That conclusion comes from investigators in a randomized controlled, trial, who found that, among 100 patients with OSA and a recent diagnosis of metabolic syndrome (MS), 18% of those assigned to use CPAP at night had a reversal of MS at 6 months of follow-up, compared with 4% of controls who were assigned to use nasal strips at night (P = .04).
The majority of patients assigned to CPAP still retained their MS diagnoses at 6 months, and CPAP did not significantly reduce individual components of the syndrome. Use of CPAP was, however, associated with small reductions in visceral fat and improvement in endothelial function, reported Sara Q.C. Giampa, PhD, from the University of São Paulo, and colleagues.
“Despite a significant rate of MS reversibility after CPAP therapy, most of the patients maintained the MS diagnosis. The modest effects of CPAP on MS reversibility underscore the need for combined therapy with CPAP, aiming to maximize metabolic syndrome recovery in parallel with improvements in OSA severity and related symptoms,” according to their study, reported in the journal CHEST®.
Asked whether he still recommends CPAP to patients with OSA and the metabolic syndrome, given the findings, corresponding author Luciano F. Drager, MD, PhD, replied “yes, definitely.”
“Despite the modest rate in reversing metabolic syndrome after CPAP, the rate was 5-fold higher than non-effective treatment (18% vs. 4%),” he said in an interview.
Dr. Drager noted that studies of other single interventions such as physical exercise to reverse MS in patients with OSA also had modest results.
A researcher who studies the relationship between sleep, circadian rhythms, and metabolism commented that, although the patients in the CPAP group were compliant with the assigned equipment and had both reductions in apneic events and improvement in oxygen saturation, the effect of CPAP on the metabolic syndrome was rather small.
“The CPAP was doing what we thought it was supposed to do, but it didn’t have the magnitude of effect on the metabolic syndrome as I expected or I think as the authors expected,” said Deanna Arble, PhD, assistant professor of biological science at Marquette University, Milwaukee.
She noted that the study also failed to detect a significant improvement in the blood pressure component of metabolic syndrome.
“In my experience and my review of the literature, blood pressure tends to be the one that’s improved most dramatically with CPAP,” she said.
Dr. Arble was not involved in the study.
Study details
In the trial, titled TREATOSA-MS, the investigators enrolled 100 patients with a recent diagnosis of metabolic syndrome and moderate to severe OSA, defined as 15 or more apnea-hypopnea index events per hour. The patients were stratified by body mass index and then randomized to undergo therapeutic CPAP or to use nasal strips for 6 months.
At baseline and at the end of each intervention investigators measured anthropometric variables, blood pressure, glucose, and lipid profiles. They also leptin and adiponectin, body composition, food intake, physical activity, subcutaneous and abdominal fat (visceral and hepatic), and endothelial function to control for potential confounders.
As noted previously, they found that after 6 months “most patients with OSA randomized to CPAP retained the MS diagnosis, but the rate of MS reversibility was higher than observed in the placebo group.” The difference in metabolic syndrome reversal, 18% with CPAP versus 4% with nasal strips, translated into a hazard ratio favoring CPAP of 5.27 (P = .04).
Also as noted, in analyses adjusted for baseline values, CPAP did not significantly improve either weight, liver fat, lip profiles, or the adiposity biomarkers leptin and adiponectin, but did have “very modest” influence on reducing visceral fat and improving endothelial function.
Rigorous study
Dr. Arble said that most studies of the association between OSA and metabolic syndrome have focused on only one or two of the parameters that were included in the TREATOSA-MS study, giving the findings additional weight.
“This could potentially be a very good, carefully controlled first insight into how obstructive sleep apnea is related to the metabolic syndrome,” she said.
The study was funded by grants Fundação de Amparo Q22 à Pesquisa do Estado de São Paulo and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors and Dr. Arble reported having no conflicts of interest to disclose.
Continuous positive airway pressure (CPAP) may be only modestly effective for ameliorating metabolic syndrome in patients with moderate to severe obstructive sleep apnea (OSA).
That conclusion comes from investigators in a randomized controlled, trial, who found that, among 100 patients with OSA and a recent diagnosis of metabolic syndrome (MS), 18% of those assigned to use CPAP at night had a reversal of MS at 6 months of follow-up, compared with 4% of controls who were assigned to use nasal strips at night (P = .04).
The majority of patients assigned to CPAP still retained their MS diagnoses at 6 months, and CPAP did not significantly reduce individual components of the syndrome. Use of CPAP was, however, associated with small reductions in visceral fat and improvement in endothelial function, reported Sara Q.C. Giampa, PhD, from the University of São Paulo, and colleagues.
“Despite a significant rate of MS reversibility after CPAP therapy, most of the patients maintained the MS diagnosis. The modest effects of CPAP on MS reversibility underscore the need for combined therapy with CPAP, aiming to maximize metabolic syndrome recovery in parallel with improvements in OSA severity and related symptoms,” according to their study, reported in the journal CHEST®.
Asked whether he still recommends CPAP to patients with OSA and the metabolic syndrome, given the findings, corresponding author Luciano F. Drager, MD, PhD, replied “yes, definitely.”
“Despite the modest rate in reversing metabolic syndrome after CPAP, the rate was 5-fold higher than non-effective treatment (18% vs. 4%),” he said in an interview.
Dr. Drager noted that studies of other single interventions such as physical exercise to reverse MS in patients with OSA also had modest results.
A researcher who studies the relationship between sleep, circadian rhythms, and metabolism commented that, although the patients in the CPAP group were compliant with the assigned equipment and had both reductions in apneic events and improvement in oxygen saturation, the effect of CPAP on the metabolic syndrome was rather small.
“The CPAP was doing what we thought it was supposed to do, but it didn’t have the magnitude of effect on the metabolic syndrome as I expected or I think as the authors expected,” said Deanna Arble, PhD, assistant professor of biological science at Marquette University, Milwaukee.
She noted that the study also failed to detect a significant improvement in the blood pressure component of metabolic syndrome.
“In my experience and my review of the literature, blood pressure tends to be the one that’s improved most dramatically with CPAP,” she said.
Dr. Arble was not involved in the study.
Study details
In the trial, titled TREATOSA-MS, the investigators enrolled 100 patients with a recent diagnosis of metabolic syndrome and moderate to severe OSA, defined as 15 or more apnea-hypopnea index events per hour. The patients were stratified by body mass index and then randomized to undergo therapeutic CPAP or to use nasal strips for 6 months.
At baseline and at the end of each intervention investigators measured anthropometric variables, blood pressure, glucose, and lipid profiles. They also leptin and adiponectin, body composition, food intake, physical activity, subcutaneous and abdominal fat (visceral and hepatic), and endothelial function to control for potential confounders.
As noted previously, they found that after 6 months “most patients with OSA randomized to CPAP retained the MS diagnosis, but the rate of MS reversibility was higher than observed in the placebo group.” The difference in metabolic syndrome reversal, 18% with CPAP versus 4% with nasal strips, translated into a hazard ratio favoring CPAP of 5.27 (P = .04).
Also as noted, in analyses adjusted for baseline values, CPAP did not significantly improve either weight, liver fat, lip profiles, or the adiposity biomarkers leptin and adiponectin, but did have “very modest” influence on reducing visceral fat and improving endothelial function.
Rigorous study
Dr. Arble said that most studies of the association between OSA and metabolic syndrome have focused on only one or two of the parameters that were included in the TREATOSA-MS study, giving the findings additional weight.
“This could potentially be a very good, carefully controlled first insight into how obstructive sleep apnea is related to the metabolic syndrome,” she said.
The study was funded by grants Fundação de Amparo Q22 à Pesquisa do Estado de São Paulo and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors and Dr. Arble reported having no conflicts of interest to disclose.
Continuous positive airway pressure (CPAP) may be only modestly effective for ameliorating metabolic syndrome in patients with moderate to severe obstructive sleep apnea (OSA).
That conclusion comes from investigators in a randomized controlled, trial, who found that, among 100 patients with OSA and a recent diagnosis of metabolic syndrome (MS), 18% of those assigned to use CPAP at night had a reversal of MS at 6 months of follow-up, compared with 4% of controls who were assigned to use nasal strips at night (P = .04).
The majority of patients assigned to CPAP still retained their MS diagnoses at 6 months, and CPAP did not significantly reduce individual components of the syndrome. Use of CPAP was, however, associated with small reductions in visceral fat and improvement in endothelial function, reported Sara Q.C. Giampa, PhD, from the University of São Paulo, and colleagues.
“Despite a significant rate of MS reversibility after CPAP therapy, most of the patients maintained the MS diagnosis. The modest effects of CPAP on MS reversibility underscore the need for combined therapy with CPAP, aiming to maximize metabolic syndrome recovery in parallel with improvements in OSA severity and related symptoms,” according to their study, reported in the journal CHEST®.
Asked whether he still recommends CPAP to patients with OSA and the metabolic syndrome, given the findings, corresponding author Luciano F. Drager, MD, PhD, replied “yes, definitely.”
“Despite the modest rate in reversing metabolic syndrome after CPAP, the rate was 5-fold higher than non-effective treatment (18% vs. 4%),” he said in an interview.
Dr. Drager noted that studies of other single interventions such as physical exercise to reverse MS in patients with OSA also had modest results.
A researcher who studies the relationship between sleep, circadian rhythms, and metabolism commented that, although the patients in the CPAP group were compliant with the assigned equipment and had both reductions in apneic events and improvement in oxygen saturation, the effect of CPAP on the metabolic syndrome was rather small.
“The CPAP was doing what we thought it was supposed to do, but it didn’t have the magnitude of effect on the metabolic syndrome as I expected or I think as the authors expected,” said Deanna Arble, PhD, assistant professor of biological science at Marquette University, Milwaukee.
She noted that the study also failed to detect a significant improvement in the blood pressure component of metabolic syndrome.
“In my experience and my review of the literature, blood pressure tends to be the one that’s improved most dramatically with CPAP,” she said.
Dr. Arble was not involved in the study.
Study details
In the trial, titled TREATOSA-MS, the investigators enrolled 100 patients with a recent diagnosis of metabolic syndrome and moderate to severe OSA, defined as 15 or more apnea-hypopnea index events per hour. The patients were stratified by body mass index and then randomized to undergo therapeutic CPAP or to use nasal strips for 6 months.
At baseline and at the end of each intervention investigators measured anthropometric variables, blood pressure, glucose, and lipid profiles. They also leptin and adiponectin, body composition, food intake, physical activity, subcutaneous and abdominal fat (visceral and hepatic), and endothelial function to control for potential confounders.
As noted previously, they found that after 6 months “most patients with OSA randomized to CPAP retained the MS diagnosis, but the rate of MS reversibility was higher than observed in the placebo group.” The difference in metabolic syndrome reversal, 18% with CPAP versus 4% with nasal strips, translated into a hazard ratio favoring CPAP of 5.27 (P = .04).
Also as noted, in analyses adjusted for baseline values, CPAP did not significantly improve either weight, liver fat, lip profiles, or the adiposity biomarkers leptin and adiponectin, but did have “very modest” influence on reducing visceral fat and improving endothelial function.
Rigorous study
Dr. Arble said that most studies of the association between OSA and metabolic syndrome have focused on only one or two of the parameters that were included in the TREATOSA-MS study, giving the findings additional weight.
“This could potentially be a very good, carefully controlled first insight into how obstructive sleep apnea is related to the metabolic syndrome,” she said.
The study was funded by grants Fundação de Amparo Q22 à Pesquisa do Estado de São Paulo and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors and Dr. Arble reported having no conflicts of interest to disclose.
FROM CHEST
Can green tea extract protect against colorectal adenomas?
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Guidance seeks to improve statin treatment adherence
International experts have created recommendations on ways to improve adherence to statin therapy by offering doctors guidance on how to distinguish between true side effects of statins and those arising due to patients’ expectations of side effects.
A position paper from the International Lipid Expert Panel (ILEP), a group of over 70 experts worldwide, provides a step-by-step approach to diagnosing and managing symptoms, such as muscle aches, and encourages patients to continue the statin therapy they have been prescribed.
The authors described in their paper, published in the Journal of Cachexia, Sarcopenia, and Muscle, how statins are among the most commonly prescribed drugs globally, with “strong and unambiguous evidence” that statin treatment makes a significant difference in preventing cardiovascular disease and dying from it.
They said how, although a recent meta-analysis showed the prevalence of statin intolerance is less than 10%, “as many as 1 in 2 patients stop taking statins, reduce the dose, or take them irregularly because they believe they are responsible for side effects.”
In addition to misattribution of aches and pains, a substantial proportion of statin-associated muscle symptoms (SAMS) result from the action of taking medicines and the expectation that medicines cause side effects. A systematic review of trials estimated that between 38% and 78% of SAMS-related statin intolerance could be attributed to expectation alone.
Nocebo/drucebo effect
President of the ILEP, Professor Maciej Banach, of the Medical University of Lodz and the University of Zielona Góra, both in Poland, who originated these recommendations, said: “There is an enormous worldwide problem with diagnosing statin intolerance correctly. In addition, we know that most diagnosed statin side effects should not, in fact, be attributed to statin therapy.”
He highlighted how as much as 70% of statin side effect symptoms may be due to a psychological phenomenon called the “nocebo” or “drucebo” effect.
“The ‘nocebo/drucebo’ effect is when patients’ expectations that they will experience side effects from the statins result in them actually experiencing these symptoms,” Professor Banach explained. Knowledge gained from the internet, leaflets, friends and family, and other sources, for example, about the most common side effects – muscle pain and liver complaints – can “result in them discontinuing their therapy and, therefore, increasing their risk of heart problems, stroke, and death,” he cautioned.
First author of the paper, Dr. Peter Penson, a reader in Cardiovascular Pharmacology at Liverpool John Moores University, England, said “the benefits of statins are not seen immediately by patients, whilst the associated adverse effects are more tangible, and so many patients stop taking statins, thereby putting themselves at risk of serious illness or death.”
A practical evidence-based guide
The authors expressed hope that their recommendations would help doctors improve patient-centered care for those patients at risk of cardiovascular disease and help these patients understand the reason for their treatment, the benefits, including that statins may prolong their lives, and the potential harms, thus enabling the patient to “make a fully informed decision about commencing and continuing therapy.”
The recommendations include:
- That health care professionals should consider the nocebo/drucebo effect when they first prescribe statins and provide information to patients about the rationale and benefits of the therapy
- The Personalized Lipid Intervention Plan (PLIP) should be used to help this process. It estimates the patient’s 10-year risk of cardiovascular disease with and without statin therapy, as well as providing clear information on adverse side effects, including that muscle symptoms are common but rarely caused by statins
- How to effectively diagnose statin intolerance and exclude nocebo/drucebo effect
- Routine follow-up to check the safety and efficacy of the therapy is recommended, and strategies for managing patients with complete statin intolerance are provided, within the recommendations. Also offered is advice about improving adherence to statin therapy and suggestions for the identification and management of the “relatively small number of patients who have true statin intolerance.”
Dr. Penson emphasized how this was the first paper to deal explicitly with the nocebo/drucebo effect and offers “practical and evidence-based suggestions” to help support individuals who are at risk of cardiovascular disease but who experience adverse effects attributable to their medicines. He added how the PLIP summarizes important lifestyle advice to help patients reduce their risk of heart attacks and strokes and also discusses the evidence for non-statin drugs that can be used to lower cholesterol.
Dr. Penson pointed out how “the vast majority of patients can take statins safely and that the benefits greatly outweigh the potential risk of side effects” and, therefore, an individual’s risk of heart problems, stroke, and death, can be reduced.
A version of this article first appeared on Medscape.com.
International experts have created recommendations on ways to improve adherence to statin therapy by offering doctors guidance on how to distinguish between true side effects of statins and those arising due to patients’ expectations of side effects.
A position paper from the International Lipid Expert Panel (ILEP), a group of over 70 experts worldwide, provides a step-by-step approach to diagnosing and managing symptoms, such as muscle aches, and encourages patients to continue the statin therapy they have been prescribed.
The authors described in their paper, published in the Journal of Cachexia, Sarcopenia, and Muscle, how statins are among the most commonly prescribed drugs globally, with “strong and unambiguous evidence” that statin treatment makes a significant difference in preventing cardiovascular disease and dying from it.
They said how, although a recent meta-analysis showed the prevalence of statin intolerance is less than 10%, “as many as 1 in 2 patients stop taking statins, reduce the dose, or take them irregularly because they believe they are responsible for side effects.”
In addition to misattribution of aches and pains, a substantial proportion of statin-associated muscle symptoms (SAMS) result from the action of taking medicines and the expectation that medicines cause side effects. A systematic review of trials estimated that between 38% and 78% of SAMS-related statin intolerance could be attributed to expectation alone.
Nocebo/drucebo effect
President of the ILEP, Professor Maciej Banach, of the Medical University of Lodz and the University of Zielona Góra, both in Poland, who originated these recommendations, said: “There is an enormous worldwide problem with diagnosing statin intolerance correctly. In addition, we know that most diagnosed statin side effects should not, in fact, be attributed to statin therapy.”
He highlighted how as much as 70% of statin side effect symptoms may be due to a psychological phenomenon called the “nocebo” or “drucebo” effect.
“The ‘nocebo/drucebo’ effect is when patients’ expectations that they will experience side effects from the statins result in them actually experiencing these symptoms,” Professor Banach explained. Knowledge gained from the internet, leaflets, friends and family, and other sources, for example, about the most common side effects – muscle pain and liver complaints – can “result in them discontinuing their therapy and, therefore, increasing their risk of heart problems, stroke, and death,” he cautioned.
First author of the paper, Dr. Peter Penson, a reader in Cardiovascular Pharmacology at Liverpool John Moores University, England, said “the benefits of statins are not seen immediately by patients, whilst the associated adverse effects are more tangible, and so many patients stop taking statins, thereby putting themselves at risk of serious illness or death.”
A practical evidence-based guide
The authors expressed hope that their recommendations would help doctors improve patient-centered care for those patients at risk of cardiovascular disease and help these patients understand the reason for their treatment, the benefits, including that statins may prolong their lives, and the potential harms, thus enabling the patient to “make a fully informed decision about commencing and continuing therapy.”
The recommendations include:
- That health care professionals should consider the nocebo/drucebo effect when they first prescribe statins and provide information to patients about the rationale and benefits of the therapy
- The Personalized Lipid Intervention Plan (PLIP) should be used to help this process. It estimates the patient’s 10-year risk of cardiovascular disease with and without statin therapy, as well as providing clear information on adverse side effects, including that muscle symptoms are common but rarely caused by statins
- How to effectively diagnose statin intolerance and exclude nocebo/drucebo effect
- Routine follow-up to check the safety and efficacy of the therapy is recommended, and strategies for managing patients with complete statin intolerance are provided, within the recommendations. Also offered is advice about improving adherence to statin therapy and suggestions for the identification and management of the “relatively small number of patients who have true statin intolerance.”
Dr. Penson emphasized how this was the first paper to deal explicitly with the nocebo/drucebo effect and offers “practical and evidence-based suggestions” to help support individuals who are at risk of cardiovascular disease but who experience adverse effects attributable to their medicines. He added how the PLIP summarizes important lifestyle advice to help patients reduce their risk of heart attacks and strokes and also discusses the evidence for non-statin drugs that can be used to lower cholesterol.
Dr. Penson pointed out how “the vast majority of patients can take statins safely and that the benefits greatly outweigh the potential risk of side effects” and, therefore, an individual’s risk of heart problems, stroke, and death, can be reduced.
A version of this article first appeared on Medscape.com.
International experts have created recommendations on ways to improve adherence to statin therapy by offering doctors guidance on how to distinguish between true side effects of statins and those arising due to patients’ expectations of side effects.
A position paper from the International Lipid Expert Panel (ILEP), a group of over 70 experts worldwide, provides a step-by-step approach to diagnosing and managing symptoms, such as muscle aches, and encourages patients to continue the statin therapy they have been prescribed.
The authors described in their paper, published in the Journal of Cachexia, Sarcopenia, and Muscle, how statins are among the most commonly prescribed drugs globally, with “strong and unambiguous evidence” that statin treatment makes a significant difference in preventing cardiovascular disease and dying from it.
They said how, although a recent meta-analysis showed the prevalence of statin intolerance is less than 10%, “as many as 1 in 2 patients stop taking statins, reduce the dose, or take them irregularly because they believe they are responsible for side effects.”
In addition to misattribution of aches and pains, a substantial proportion of statin-associated muscle symptoms (SAMS) result from the action of taking medicines and the expectation that medicines cause side effects. A systematic review of trials estimated that between 38% and 78% of SAMS-related statin intolerance could be attributed to expectation alone.
Nocebo/drucebo effect
President of the ILEP, Professor Maciej Banach, of the Medical University of Lodz and the University of Zielona Góra, both in Poland, who originated these recommendations, said: “There is an enormous worldwide problem with diagnosing statin intolerance correctly. In addition, we know that most diagnosed statin side effects should not, in fact, be attributed to statin therapy.”
He highlighted how as much as 70% of statin side effect symptoms may be due to a psychological phenomenon called the “nocebo” or “drucebo” effect.
“The ‘nocebo/drucebo’ effect is when patients’ expectations that they will experience side effects from the statins result in them actually experiencing these symptoms,” Professor Banach explained. Knowledge gained from the internet, leaflets, friends and family, and other sources, for example, about the most common side effects – muscle pain and liver complaints – can “result in them discontinuing their therapy and, therefore, increasing their risk of heart problems, stroke, and death,” he cautioned.
First author of the paper, Dr. Peter Penson, a reader in Cardiovascular Pharmacology at Liverpool John Moores University, England, said “the benefits of statins are not seen immediately by patients, whilst the associated adverse effects are more tangible, and so many patients stop taking statins, thereby putting themselves at risk of serious illness or death.”
A practical evidence-based guide
The authors expressed hope that their recommendations would help doctors improve patient-centered care for those patients at risk of cardiovascular disease and help these patients understand the reason for their treatment, the benefits, including that statins may prolong their lives, and the potential harms, thus enabling the patient to “make a fully informed decision about commencing and continuing therapy.”
The recommendations include:
- That health care professionals should consider the nocebo/drucebo effect when they first prescribe statins and provide information to patients about the rationale and benefits of the therapy
- The Personalized Lipid Intervention Plan (PLIP) should be used to help this process. It estimates the patient’s 10-year risk of cardiovascular disease with and without statin therapy, as well as providing clear information on adverse side effects, including that muscle symptoms are common but rarely caused by statins
- How to effectively diagnose statin intolerance and exclude nocebo/drucebo effect
- Routine follow-up to check the safety and efficacy of the therapy is recommended, and strategies for managing patients with complete statin intolerance are provided, within the recommendations. Also offered is advice about improving adherence to statin therapy and suggestions for the identification and management of the “relatively small number of patients who have true statin intolerance.”
Dr. Penson emphasized how this was the first paper to deal explicitly with the nocebo/drucebo effect and offers “practical and evidence-based suggestions” to help support individuals who are at risk of cardiovascular disease but who experience adverse effects attributable to their medicines. He added how the PLIP summarizes important lifestyle advice to help patients reduce their risk of heart attacks and strokes and also discusses the evidence for non-statin drugs that can be used to lower cholesterol.
Dr. Penson pointed out how “the vast majority of patients can take statins safely and that the benefits greatly outweigh the potential risk of side effects” and, therefore, an individual’s risk of heart problems, stroke, and death, can be reduced.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CACHEXIA, SARCOPENIA, AND MUSCLE
B-cell depletion overkill?
The results, drawn from a retrospective analysis, provide support for clinical trials to rest longer re-infusion intervals.

The study appeared online Jan. 21 in the journal Multiple Sclerosis and Related Disorders, presented by lead author Mahmoud AbdelRazek, MD, at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Both drugs were approved based on clinical trials that investigated 6-month doses, but previous studies have suggested depletion can last longer, including a range of 9-26 months in the case of rituximab.
The initial rationale for monitoring B cell depletion was to prevent a relapse by re-infusing a patient if B cells levels rise, but the researchers noted a pattern of sustained depletion, especially in patients who had a delayed infusion for some reason – they often still had low B cell counts at the time of the next drug infusion. “That became not an unusual finding,” said Dr. AbdelRazek in an interview. He is an instructor of neurology at Harvard Medical School.
Patients also found the delay appealing, in part because they often felt unwell in the days following an infusion, and delays could mean fewer infections and other adverse effects. “Most of my patients I’ve discussed this with would be very appreciative of that delay,” said Dr. AbdelRazek. “There’s obviously an economic benefit as well,” said Dr. AbdelRazek.
The final answer?
The retrospective nature of the study is a key weakness, and the rationale to delay infusions based on continuing B cell depletion assumes that B cell depletion is in fact the mechanism of action for countering MS. “That is a critical question,” said Mark Gudesblatt, MD, who was asked to comment on the study. But if that is indeed the way the drugs work, then it would make sense to identify patients who repopulate B cells more slowly and tailor drug regimens. “It’s not one size fits all and blindly just re-dosing. The upsides are good: You come in less frequently for dosing, the cost to payers is less. But the bad is, maybe there are other markers. This is the putative mechanism, but what we believe may not be the final answer. There may be more to the story,” said Dr. Gutesblatt, who is Medical Director at South Shore Neurologic Associates, Patchogue, New York.
Dr. AbdelRazek also noted the study’s limitation. “I think a clinical trial is going to be warranted to really have this translated into clinical practice,” he said. His group is planning to conduct just such a trial, pending confirmation of a funding source.
B cell depletion beyond 6 months
The researchers analyzed data from 178 patients with MS and 10 patients with NMOSD who received ocrelizumab (n = 111) or rituximab (n = 53), or both (n = 24) at two Harvard Medical School teaching hospitals between 2010 and 2020. The data included 800 infusions and 1,054 CD19 measurements.
The researchers defined B cell depletion as an absolute count of 20 cells/uL or less, a B cell percentage of 2% or less, or if B cells were 5% or less of total lymphocytes.
Among the patient population, B cell depletion that met all 3 criteria occurred as long as 13.8 months after an initial ocrelizumab infusion cycle, and 22.8 months after second or more cycles of ocrelizumab. Following rituximab, the researchers noted B cell depletions. Following 500 mg of rituximab, B cell depletion defined by the first, second, or third criteria occurred as far out as 22.3, 26.2, and 28.5 months. For 1,000 mg doses of rituximab, B cell depletion occurred as long as 18.3, 18.3, and 29.1 months after a dose.
Examining 90 B cell measurements conducted at least 8 months after an ocrelizumab infusion, 50% were depleted by the first definition and 54% by the second definition. At 13 months, the figures were 58% and 62% among 26 B-cell measurements. Eight months or more after rituximab, 113 B-cell measurements showed rates of 43% and 52% B-cell depletion by the first two criteria.
Dr. AbdelRazek and Dr. Gudesblatt have no relevant financial disclosures.
The results, drawn from a retrospective analysis, provide support for clinical trials to rest longer re-infusion intervals.
The study appeared online Jan. 21 in the journal Multiple Sclerosis and Related Disorders, presented by lead author Mahmoud AbdelRazek, MD, at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Both drugs were approved based on clinical trials that investigated 6-month doses, but previous studies have suggested depletion can last longer, including a range of 9-26 months in the case of rituximab.
The initial rationale for monitoring B cell depletion was to prevent a relapse by re-infusing a patient if B cells levels rise, but the researchers noted a pattern of sustained depletion, especially in patients who had a delayed infusion for some reason – they often still had low B cell counts at the time of the next drug infusion. “That became not an unusual finding,” said Dr. AbdelRazek in an interview. He is an instructor of neurology at Harvard Medical School.
Patients also found the delay appealing, in part because they often felt unwell in the days following an infusion, and delays could mean fewer infections and other adverse effects. “Most of my patients I’ve discussed this with would be very appreciative of that delay,” said Dr. AbdelRazek. “There’s obviously an economic benefit as well,” said Dr. AbdelRazek.
The final answer?
The retrospective nature of the study is a key weakness, and the rationale to delay infusions based on continuing B cell depletion assumes that B cell depletion is in fact the mechanism of action for countering MS. “That is a critical question,” said Mark Gudesblatt, MD, who was asked to comment on the study. But if that is indeed the way the drugs work, then it would make sense to identify patients who repopulate B cells more slowly and tailor drug regimens. “It’s not one size fits all and blindly just re-dosing. The upsides are good: You come in less frequently for dosing, the cost to payers is less. But the bad is, maybe there are other markers. This is the putative mechanism, but what we believe may not be the final answer. There may be more to the story,” said Dr. Gutesblatt, who is Medical Director at South Shore Neurologic Associates, Patchogue, New York.
Dr. AbdelRazek also noted the study’s limitation. “I think a clinical trial is going to be warranted to really have this translated into clinical practice,” he said. His group is planning to conduct just such a trial, pending confirmation of a funding source.
B cell depletion beyond 6 months
The researchers analyzed data from 178 patients with MS and 10 patients with NMOSD who received ocrelizumab (n = 111) or rituximab (n = 53), or both (n = 24) at two Harvard Medical School teaching hospitals between 2010 and 2020. The data included 800 infusions and 1,054 CD19 measurements.
The researchers defined B cell depletion as an absolute count of 20 cells/uL or less, a B cell percentage of 2% or less, or if B cells were 5% or less of total lymphocytes.
Among the patient population, B cell depletion that met all 3 criteria occurred as long as 13.8 months after an initial ocrelizumab infusion cycle, and 22.8 months after second or more cycles of ocrelizumab. Following rituximab, the researchers noted B cell depletions. Following 500 mg of rituximab, B cell depletion defined by the first, second, or third criteria occurred as far out as 22.3, 26.2, and 28.5 months. For 1,000 mg doses of rituximab, B cell depletion occurred as long as 18.3, 18.3, and 29.1 months after a dose.
Examining 90 B cell measurements conducted at least 8 months after an ocrelizumab infusion, 50% were depleted by the first definition and 54% by the second definition. At 13 months, the figures were 58% and 62% among 26 B-cell measurements. Eight months or more after rituximab, 113 B-cell measurements showed rates of 43% and 52% B-cell depletion by the first two criteria.
Dr. AbdelRazek and Dr. Gudesblatt have no relevant financial disclosures.
The results, drawn from a retrospective analysis, provide support for clinical trials to rest longer re-infusion intervals.
The study appeared online Jan. 21 in the journal Multiple Sclerosis and Related Disorders, presented by lead author Mahmoud AbdelRazek, MD, at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS).
Both drugs were approved based on clinical trials that investigated 6-month doses, but previous studies have suggested depletion can last longer, including a range of 9-26 months in the case of rituximab.
The initial rationale for monitoring B cell depletion was to prevent a relapse by re-infusing a patient if B cells levels rise, but the researchers noted a pattern of sustained depletion, especially in patients who had a delayed infusion for some reason – they often still had low B cell counts at the time of the next drug infusion. “That became not an unusual finding,” said Dr. AbdelRazek in an interview. He is an instructor of neurology at Harvard Medical School.
Patients also found the delay appealing, in part because they often felt unwell in the days following an infusion, and delays could mean fewer infections and other adverse effects. “Most of my patients I’ve discussed this with would be very appreciative of that delay,” said Dr. AbdelRazek. “There’s obviously an economic benefit as well,” said Dr. AbdelRazek.
The final answer?
The retrospective nature of the study is a key weakness, and the rationale to delay infusions based on continuing B cell depletion assumes that B cell depletion is in fact the mechanism of action for countering MS. “That is a critical question,” said Mark Gudesblatt, MD, who was asked to comment on the study. But if that is indeed the way the drugs work, then it would make sense to identify patients who repopulate B cells more slowly and tailor drug regimens. “It’s not one size fits all and blindly just re-dosing. The upsides are good: You come in less frequently for dosing, the cost to payers is less. But the bad is, maybe there are other markers. This is the putative mechanism, but what we believe may not be the final answer. There may be more to the story,” said Dr. Gutesblatt, who is Medical Director at South Shore Neurologic Associates, Patchogue, New York.
Dr. AbdelRazek also noted the study’s limitation. “I think a clinical trial is going to be warranted to really have this translated into clinical practice,” he said. His group is planning to conduct just such a trial, pending confirmation of a funding source.
B cell depletion beyond 6 months
The researchers analyzed data from 178 patients with MS and 10 patients with NMOSD who received ocrelizumab (n = 111) or rituximab (n = 53), or both (n = 24) at two Harvard Medical School teaching hospitals between 2010 and 2020. The data included 800 infusions and 1,054 CD19 measurements.
The researchers defined B cell depletion as an absolute count of 20 cells/uL or less, a B cell percentage of 2% or less, or if B cells were 5% or less of total lymphocytes.
Among the patient population, B cell depletion that met all 3 criteria occurred as long as 13.8 months after an initial ocrelizumab infusion cycle, and 22.8 months after second or more cycles of ocrelizumab. Following rituximab, the researchers noted B cell depletions. Following 500 mg of rituximab, B cell depletion defined by the first, second, or third criteria occurred as far out as 22.3, 26.2, and 28.5 months. For 1,000 mg doses of rituximab, B cell depletion occurred as long as 18.3, 18.3, and 29.1 months after a dose.
Examining 90 B cell measurements conducted at least 8 months after an ocrelizumab infusion, 50% were depleted by the first definition and 54% by the second definition. At 13 months, the figures were 58% and 62% among 26 B-cell measurements. Eight months or more after rituximab, 113 B-cell measurements showed rates of 43% and 52% B-cell depletion by the first two criteria.
Dr. AbdelRazek and Dr. Gudesblatt have no relevant financial disclosures.
FROM ACTRIMS FORUM 2022
Big missed opportunities for BP control in premenopausal women
A new report shows considerable gaps in the awareness, treatment, and control of hypertension in premenopausal women in the United States, with a key driver being regular access to health care.
In a nationally representative sample of women ages 35-54 with no prior cardiovascular disease, the prevalence of hypertension increased 8% from an estimated 15.2 million women between 2011 and 2014 to 16.4 million women between 2015 and 2018.
What’s more, the percentage of women with controlled hypertension dropped over the two time periods from 55% to 50%, which is well below the government’s Million Hearts target of 70%.
Missed opportunities for hypertension control in these premenopausal women were a lack of awareness of their hypertension in 23%, ineffective treatment in 34%, and a lack of health care access in 43%; increasing to 51% in non-Hispanic Black patients and 56% in Hispanic patients.
Notably, lack of health care access affected an estimated 3.1 million women (45%) in 2011-2014 and 3.5 million women (43%) in 2015-2018.
Equally stubborn over the two time periods was the lack of effective treatment, affecting 2.1 million (31%) versus 2.8 million (34%) women, and lack of awareness, affecting 1.6 million (24%) versus 1.9 million (23%) women.
“There’s been no improvement over the past decade, and there is evidence of race/ethnic disparities,” study author Susan Hennessy, PhD, said at the recent Epidemiology, Prevention/Lifestyle & Cardiometabolic Health (EPI|Lifestyle) 2022 conference sponsored by the American Heart Association.
The prevalence of uncontrolled hypertension among non-Hispanic Whites was less than that of the U.S. population, at 44%, and most of the missed opportunities were due to uncontrolled blood pressure (BP), noted Dr. Hennessy, a researcher with the University of California, San Francisco School of Medicine.
However, the uncontrolled prevalence was 54% in non-Hispanic Black women and 66% in Hispanic women. “In both of these subgroups, over half of the missed opportunities occur because these women have no regular access to health care,” she said.
In women who identified as “other,” which includes non-Hispanic Asian and mixed-race populations, the uncontrolled prevalence reached 70%, and the biggest missed opportunity was in those who were untreated.
Raising awareness, empowering women, and delivery of guideline-concordant care will help premenopausal women gain control of their blood pressure, Dr. Hennessy said. “But underpinning all of this is ensuring equitable health care access, because if we fail to get women into the system, then we have no opportunity to help them lower their blood pressure.”
She reminded the audience that cardiovascular disease (CVD) is the number one killer of women in the United States and that CVD risk, mediated through hypertension, increases after menopause. Thus, managing hypertension prior to this life event is an important element of primary prevention of CVD and should be a priority.
Session moderator Sadiya S. Khan, MD, Northwestern University Feinberg School of Medicine, Chicago, told this news organization that the findings should raise “alarm and concern that hypertension is not just a disease of the old but very prevalent in younger women, particularly around the time of pregnancy. And this is a clear driver of maternal morbidity and mortality as well.”
“This idea that patients should ‘Know Your Numbers’ is really important, and we talk a lot about that for hypertension, but if you don’t have a doctor, if you don’t have someone to go to, it’s very hard to know or understand what your numbers mean,” she said. “I think that’s really the main message.”
Speaking to this news organization, Dr. Hennessy said there’s no simple solution to the problem, given that some women are not even in the system, whereas others are not being treated effectively, but that increasing opportunities to screen BP would be a start. That could be through community programs, similar to the Barbershop Hypertension trial, or by making BP devices available for home monitoring.
“Again, this is about empowering ourselves to take some level of control, but, as a system, we have to be able to make it equitable for everyone and make sure they have the right equipment, the right cuff size,” she said. “The disparities arise because of the social determinants of health, so if these women are struggling to put food on the table, they aren’t going to be able to afford a blood pressure cuff.”
During a discussion of the findings, audience members noted that the National Health and Nutrition Examination Survey (NHANES) data used for the analysis were somewhat dated. Dr. Hennessy also pointed out that NHANES blood pressure is measured up to three times during a single visit, which differs from clinical practice, and that responses were based on self-report and thus subject to recall bias.
The sample included 3,343 women aged 35-54 years with no prior cardiovascular disease, representing an estimated 31.6 million American women. Hypertension was defined by a systolic BP of at least 140 mm Hg or a diastolic BP of at least 90 mm Hg or current BP medication use.
The authors and Dr. Khan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new report shows considerable gaps in the awareness, treatment, and control of hypertension in premenopausal women in the United States, with a key driver being regular access to health care.
In a nationally representative sample of women ages 35-54 with no prior cardiovascular disease, the prevalence of hypertension increased 8% from an estimated 15.2 million women between 2011 and 2014 to 16.4 million women between 2015 and 2018.
What’s more, the percentage of women with controlled hypertension dropped over the two time periods from 55% to 50%, which is well below the government’s Million Hearts target of 70%.
Missed opportunities for hypertension control in these premenopausal women were a lack of awareness of their hypertension in 23%, ineffective treatment in 34%, and a lack of health care access in 43%; increasing to 51% in non-Hispanic Black patients and 56% in Hispanic patients.
Notably, lack of health care access affected an estimated 3.1 million women (45%) in 2011-2014 and 3.5 million women (43%) in 2015-2018.
Equally stubborn over the two time periods was the lack of effective treatment, affecting 2.1 million (31%) versus 2.8 million (34%) women, and lack of awareness, affecting 1.6 million (24%) versus 1.9 million (23%) women.
“There’s been no improvement over the past decade, and there is evidence of race/ethnic disparities,” study author Susan Hennessy, PhD, said at the recent Epidemiology, Prevention/Lifestyle & Cardiometabolic Health (EPI|Lifestyle) 2022 conference sponsored by the American Heart Association.
The prevalence of uncontrolled hypertension among non-Hispanic Whites was less than that of the U.S. population, at 44%, and most of the missed opportunities were due to uncontrolled blood pressure (BP), noted Dr. Hennessy, a researcher with the University of California, San Francisco School of Medicine.
However, the uncontrolled prevalence was 54% in non-Hispanic Black women and 66% in Hispanic women. “In both of these subgroups, over half of the missed opportunities occur because these women have no regular access to health care,” she said.
In women who identified as “other,” which includes non-Hispanic Asian and mixed-race populations, the uncontrolled prevalence reached 70%, and the biggest missed opportunity was in those who were untreated.
Raising awareness, empowering women, and delivery of guideline-concordant care will help premenopausal women gain control of their blood pressure, Dr. Hennessy said. “But underpinning all of this is ensuring equitable health care access, because if we fail to get women into the system, then we have no opportunity to help them lower their blood pressure.”
She reminded the audience that cardiovascular disease (CVD) is the number one killer of women in the United States and that CVD risk, mediated through hypertension, increases after menopause. Thus, managing hypertension prior to this life event is an important element of primary prevention of CVD and should be a priority.
Session moderator Sadiya S. Khan, MD, Northwestern University Feinberg School of Medicine, Chicago, told this news organization that the findings should raise “alarm and concern that hypertension is not just a disease of the old but very prevalent in younger women, particularly around the time of pregnancy. And this is a clear driver of maternal morbidity and mortality as well.”
“This idea that patients should ‘Know Your Numbers’ is really important, and we talk a lot about that for hypertension, but if you don’t have a doctor, if you don’t have someone to go to, it’s very hard to know or understand what your numbers mean,” she said. “I think that’s really the main message.”
Speaking to this news organization, Dr. Hennessy said there’s no simple solution to the problem, given that some women are not even in the system, whereas others are not being treated effectively, but that increasing opportunities to screen BP would be a start. That could be through community programs, similar to the Barbershop Hypertension trial, or by making BP devices available for home monitoring.
“Again, this is about empowering ourselves to take some level of control, but, as a system, we have to be able to make it equitable for everyone and make sure they have the right equipment, the right cuff size,” she said. “The disparities arise because of the social determinants of health, so if these women are struggling to put food on the table, they aren’t going to be able to afford a blood pressure cuff.”
During a discussion of the findings, audience members noted that the National Health and Nutrition Examination Survey (NHANES) data used for the analysis were somewhat dated. Dr. Hennessy also pointed out that NHANES blood pressure is measured up to three times during a single visit, which differs from clinical practice, and that responses were based on self-report and thus subject to recall bias.
The sample included 3,343 women aged 35-54 years with no prior cardiovascular disease, representing an estimated 31.6 million American women. Hypertension was defined by a systolic BP of at least 140 mm Hg or a diastolic BP of at least 90 mm Hg or current BP medication use.
The authors and Dr. Khan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new report shows considerable gaps in the awareness, treatment, and control of hypertension in premenopausal women in the United States, with a key driver being regular access to health care.
In a nationally representative sample of women ages 35-54 with no prior cardiovascular disease, the prevalence of hypertension increased 8% from an estimated 15.2 million women between 2011 and 2014 to 16.4 million women between 2015 and 2018.
What’s more, the percentage of women with controlled hypertension dropped over the two time periods from 55% to 50%, which is well below the government’s Million Hearts target of 70%.
Missed opportunities for hypertension control in these premenopausal women were a lack of awareness of their hypertension in 23%, ineffective treatment in 34%, and a lack of health care access in 43%; increasing to 51% in non-Hispanic Black patients and 56% in Hispanic patients.
Notably, lack of health care access affected an estimated 3.1 million women (45%) in 2011-2014 and 3.5 million women (43%) in 2015-2018.
Equally stubborn over the two time periods was the lack of effective treatment, affecting 2.1 million (31%) versus 2.8 million (34%) women, and lack of awareness, affecting 1.6 million (24%) versus 1.9 million (23%) women.
“There’s been no improvement over the past decade, and there is evidence of race/ethnic disparities,” study author Susan Hennessy, PhD, said at the recent Epidemiology, Prevention/Lifestyle & Cardiometabolic Health (EPI|Lifestyle) 2022 conference sponsored by the American Heart Association.
The prevalence of uncontrolled hypertension among non-Hispanic Whites was less than that of the U.S. population, at 44%, and most of the missed opportunities were due to uncontrolled blood pressure (BP), noted Dr. Hennessy, a researcher with the University of California, San Francisco School of Medicine.
However, the uncontrolled prevalence was 54% in non-Hispanic Black women and 66% in Hispanic women. “In both of these subgroups, over half of the missed opportunities occur because these women have no regular access to health care,” she said.
In women who identified as “other,” which includes non-Hispanic Asian and mixed-race populations, the uncontrolled prevalence reached 70%, and the biggest missed opportunity was in those who were untreated.
Raising awareness, empowering women, and delivery of guideline-concordant care will help premenopausal women gain control of their blood pressure, Dr. Hennessy said. “But underpinning all of this is ensuring equitable health care access, because if we fail to get women into the system, then we have no opportunity to help them lower their blood pressure.”
She reminded the audience that cardiovascular disease (CVD) is the number one killer of women in the United States and that CVD risk, mediated through hypertension, increases after menopause. Thus, managing hypertension prior to this life event is an important element of primary prevention of CVD and should be a priority.
Session moderator Sadiya S. Khan, MD, Northwestern University Feinberg School of Medicine, Chicago, told this news organization that the findings should raise “alarm and concern that hypertension is not just a disease of the old but very prevalent in younger women, particularly around the time of pregnancy. And this is a clear driver of maternal morbidity and mortality as well.”
“This idea that patients should ‘Know Your Numbers’ is really important, and we talk a lot about that for hypertension, but if you don’t have a doctor, if you don’t have someone to go to, it’s very hard to know or understand what your numbers mean,” she said. “I think that’s really the main message.”
Speaking to this news organization, Dr. Hennessy said there’s no simple solution to the problem, given that some women are not even in the system, whereas others are not being treated effectively, but that increasing opportunities to screen BP would be a start. That could be through community programs, similar to the Barbershop Hypertension trial, or by making BP devices available for home monitoring.
“Again, this is about empowering ourselves to take some level of control, but, as a system, we have to be able to make it equitable for everyone and make sure they have the right equipment, the right cuff size,” she said. “The disparities arise because of the social determinants of health, so if these women are struggling to put food on the table, they aren’t going to be able to afford a blood pressure cuff.”
During a discussion of the findings, audience members noted that the National Health and Nutrition Examination Survey (NHANES) data used for the analysis were somewhat dated. Dr. Hennessy also pointed out that NHANES blood pressure is measured up to three times during a single visit, which differs from clinical practice, and that responses were based on self-report and thus subject to recall bias.
The sample included 3,343 women aged 35-54 years with no prior cardiovascular disease, representing an estimated 31.6 million American women. Hypertension was defined by a systolic BP of at least 140 mm Hg or a diastolic BP of at least 90 mm Hg or current BP medication use.
The authors and Dr. Khan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Overwhelming’ need to study COVID vaccine–associated tinnitus
It’s now known that tinnitus may be an unexpected side effect of SARS-CoV-2 vaccination, and there is an urgent need to understand the precise mechanisms and best treatment for vaccine-associated tinnitus, researchers say.
As of mid-September 2021, 12,247 cases of tinnitus, or ringing in the ears, following COVID-19 vaccination had been reported to the Vaccine Adverse Event Reporting System of the U.S. Centers for Disease Control and Prevention.
“Despite several cases of tinnitus being reported following SARS-CoV-2 vaccination, the precise pathophysiology is still not clear,” write Syed Hassan Ahmed, 3rd-year MBBS student, Dow University of Health Sciences, Karachi, Pakistan, and coauthors.
The researchers review what is known and unknown about SARS-CoV-2 vaccine-associated tinnitus in an article published online Feb. 11 in Annals of Medicine and Surgery.
Molecular mimicry?
The researchers say cross-reactivity between anti-spike SARS-CoV-2 antibodies and otologic antigens is one possibility, based on the mechanisms behind other COVID-19 vaccine–induced disorders and the phenomenon of molecular mimicry.
“The heptapeptide resemblance between coronavirus spike glycoprotein and numerous human proteins further supports molecular mimicry as a potential mechanism behind such vaccine-induced disorders,” they write.
Anti-spike antibodies may react with antigens anywhere along the auditory pathway and fuel an inflammatory reaction, they point out.
“Therefore, understanding the phenomenon of cross-reactivity and molecular mimicry may be helpful in postulating potential treatment behind not only tinnitus but also the rare events of vaccination associated hearing loss and other otologic manifestations,” the authors say.
Genetic predispositions and associated conditions may also play a significant role in determining whether an individual develops vaccine-induced tinnitus.
Stress and anxiety following COVID vaccination may also play a role, inasmuch as anxiety-related adverse events following vaccination have been reported. Vaccine-related anxiety as a potential cause of tinnitus developing after vaccination needs to be explored, they write.
Jury out on best management
How best to manage COVID vaccine-associated tinnitus also remains unclear, but it starts with a well-established diagnosis, the authors say.
A well-focused and detailed history and examination are essential, with particular emphasis placed on preexisting health conditions, specifically, autoimmune diseases, such as Hashimoto thyroiditis; otologic conditions, such as sensorineural hearing loss; glaucoma; and psychological well-being. According to the review, patients often present with a history of one or more of these disorders.
“However, any such association has not yet been established and requires further investigation to be concluded as potential risk factors for vaccine-induced tinnitus,” they caution.
Routine cranial nerve examination, otoscopy, Weber test, and Rinne test, which are used for tinnitus diagnosis in general, may be helpful for confirmation of vaccine-associated tinnitus.
Owing to the significant association between tinnitus and hearing impairment, audiology should also performed, the authors say.
Although treatments for non–vaccine-induced tinnitus vary significantly, corticosteroids are the top treatment choice for SARS-CoV-2 vaccine-induced tinnitus reported in the literature.
Trials of other drug and nondrug interventions that may uniquely help with vaccine-associated tinnitus are urgently needed, the authors say.
Summing up, the reviewers say, “Although the incidence of COVID-19 vaccine-associated tinnitus is rare, there is an overwhelming need to discern the precise pathophysiology and clinical management as a better understanding of adverse events may help in encountering vaccine hesitancy and hence fostering the COVID-19 global vaccination program.
“Despite the incidence of adverse events, the benefits of the SARS-CoV-2 vaccine in reducing hospitalization and deaths continue to outweigh the rare ramifications,” they conclude.
The research had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It’s now known that tinnitus may be an unexpected side effect of SARS-CoV-2 vaccination, and there is an urgent need to understand the precise mechanisms and best treatment for vaccine-associated tinnitus, researchers say.
As of mid-September 2021, 12,247 cases of tinnitus, or ringing in the ears, following COVID-19 vaccination had been reported to the Vaccine Adverse Event Reporting System of the U.S. Centers for Disease Control and Prevention.
“Despite several cases of tinnitus being reported following SARS-CoV-2 vaccination, the precise pathophysiology is still not clear,” write Syed Hassan Ahmed, 3rd-year MBBS student, Dow University of Health Sciences, Karachi, Pakistan, and coauthors.
The researchers review what is known and unknown about SARS-CoV-2 vaccine-associated tinnitus in an article published online Feb. 11 in Annals of Medicine and Surgery.
Molecular mimicry?
The researchers say cross-reactivity between anti-spike SARS-CoV-2 antibodies and otologic antigens is one possibility, based on the mechanisms behind other COVID-19 vaccine–induced disorders and the phenomenon of molecular mimicry.
“The heptapeptide resemblance between coronavirus spike glycoprotein and numerous human proteins further supports molecular mimicry as a potential mechanism behind such vaccine-induced disorders,” they write.
Anti-spike antibodies may react with antigens anywhere along the auditory pathway and fuel an inflammatory reaction, they point out.
“Therefore, understanding the phenomenon of cross-reactivity and molecular mimicry may be helpful in postulating potential treatment behind not only tinnitus but also the rare events of vaccination associated hearing loss and other otologic manifestations,” the authors say.
Genetic predispositions and associated conditions may also play a significant role in determining whether an individual develops vaccine-induced tinnitus.
Stress and anxiety following COVID vaccination may also play a role, inasmuch as anxiety-related adverse events following vaccination have been reported. Vaccine-related anxiety as a potential cause of tinnitus developing after vaccination needs to be explored, they write.
Jury out on best management
How best to manage COVID vaccine-associated tinnitus also remains unclear, but it starts with a well-established diagnosis, the authors say.
A well-focused and detailed history and examination are essential, with particular emphasis placed on preexisting health conditions, specifically, autoimmune diseases, such as Hashimoto thyroiditis; otologic conditions, such as sensorineural hearing loss; glaucoma; and psychological well-being. According to the review, patients often present with a history of one or more of these disorders.
“However, any such association has not yet been established and requires further investigation to be concluded as potential risk factors for vaccine-induced tinnitus,” they caution.
Routine cranial nerve examination, otoscopy, Weber test, and Rinne test, which are used for tinnitus diagnosis in general, may be helpful for confirmation of vaccine-associated tinnitus.
Owing to the significant association between tinnitus and hearing impairment, audiology should also performed, the authors say.
Although treatments for non–vaccine-induced tinnitus vary significantly, corticosteroids are the top treatment choice for SARS-CoV-2 vaccine-induced tinnitus reported in the literature.
Trials of other drug and nondrug interventions that may uniquely help with vaccine-associated tinnitus are urgently needed, the authors say.
Summing up, the reviewers say, “Although the incidence of COVID-19 vaccine-associated tinnitus is rare, there is an overwhelming need to discern the precise pathophysiology and clinical management as a better understanding of adverse events may help in encountering vaccine hesitancy and hence fostering the COVID-19 global vaccination program.
“Despite the incidence of adverse events, the benefits of the SARS-CoV-2 vaccine in reducing hospitalization and deaths continue to outweigh the rare ramifications,” they conclude.
The research had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It’s now known that tinnitus may be an unexpected side effect of SARS-CoV-2 vaccination, and there is an urgent need to understand the precise mechanisms and best treatment for vaccine-associated tinnitus, researchers say.
As of mid-September 2021, 12,247 cases of tinnitus, or ringing in the ears, following COVID-19 vaccination had been reported to the Vaccine Adverse Event Reporting System of the U.S. Centers for Disease Control and Prevention.
“Despite several cases of tinnitus being reported following SARS-CoV-2 vaccination, the precise pathophysiology is still not clear,” write Syed Hassan Ahmed, 3rd-year MBBS student, Dow University of Health Sciences, Karachi, Pakistan, and coauthors.
The researchers review what is known and unknown about SARS-CoV-2 vaccine-associated tinnitus in an article published online Feb. 11 in Annals of Medicine and Surgery.
Molecular mimicry?
The researchers say cross-reactivity between anti-spike SARS-CoV-2 antibodies and otologic antigens is one possibility, based on the mechanisms behind other COVID-19 vaccine–induced disorders and the phenomenon of molecular mimicry.
“The heptapeptide resemblance between coronavirus spike glycoprotein and numerous human proteins further supports molecular mimicry as a potential mechanism behind such vaccine-induced disorders,” they write.
Anti-spike antibodies may react with antigens anywhere along the auditory pathway and fuel an inflammatory reaction, they point out.
“Therefore, understanding the phenomenon of cross-reactivity and molecular mimicry may be helpful in postulating potential treatment behind not only tinnitus but also the rare events of vaccination associated hearing loss and other otologic manifestations,” the authors say.
Genetic predispositions and associated conditions may also play a significant role in determining whether an individual develops vaccine-induced tinnitus.
Stress and anxiety following COVID vaccination may also play a role, inasmuch as anxiety-related adverse events following vaccination have been reported. Vaccine-related anxiety as a potential cause of tinnitus developing after vaccination needs to be explored, they write.
Jury out on best management
How best to manage COVID vaccine-associated tinnitus also remains unclear, but it starts with a well-established diagnosis, the authors say.
A well-focused and detailed history and examination are essential, with particular emphasis placed on preexisting health conditions, specifically, autoimmune diseases, such as Hashimoto thyroiditis; otologic conditions, such as sensorineural hearing loss; glaucoma; and psychological well-being. According to the review, patients often present with a history of one or more of these disorders.
“However, any such association has not yet been established and requires further investigation to be concluded as potential risk factors for vaccine-induced tinnitus,” they caution.
Routine cranial nerve examination, otoscopy, Weber test, and Rinne test, which are used for tinnitus diagnosis in general, may be helpful for confirmation of vaccine-associated tinnitus.
Owing to the significant association between tinnitus and hearing impairment, audiology should also performed, the authors say.
Although treatments for non–vaccine-induced tinnitus vary significantly, corticosteroids are the top treatment choice for SARS-CoV-2 vaccine-induced tinnitus reported in the literature.
Trials of other drug and nondrug interventions that may uniquely help with vaccine-associated tinnitus are urgently needed, the authors say.
Summing up, the reviewers say, “Although the incidence of COVID-19 vaccine-associated tinnitus is rare, there is an overwhelming need to discern the precise pathophysiology and clinical management as a better understanding of adverse events may help in encountering vaccine hesitancy and hence fostering the COVID-19 global vaccination program.
“Despite the incidence of adverse events, the benefits of the SARS-CoV-2 vaccine in reducing hospitalization and deaths continue to outweigh the rare ramifications,” they conclude.
The research had no specific funding. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF MEDICINE AND SURGERY