User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
What’s the future of microbiome therapies in C. diff, cancer?
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
REPORTING FROM GMFH 2022
Excess weight over lifetime hikes risk for colorectal cancer
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.

Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
FROM JAMA ONCOLOGY
Ways to lessen toxic effects of chemo in older adults
Age-related changes that potentiate adverse drug reactions include alterations in absorption, distribution, metabolism, and excretion. As such, older patients often require adjustments in medications to optimize safety and use. Medication adjustment is especially important for older patients on complex medication regimens for multiple conditions, such as those undergoing cancer treatment. Three recent high-quality randomized trials evaluated the use of geriatric assessment (GA) in older adults with cancer.1-3
Interdisciplinary GA can identify aging-related conditions associated with poor outcomes in older patients with cancer (e.g., toxic effects of chemotherapy) and provide recommendations aimed at improving health outcomes. The results of these trials suggest that interdisciplinary GA can improve care outcomes and oncologists’ communication for older adults with cancer, and should be considered an emerging standard of care.
Geriatric assessment and chemotherapy-related toxic effects
A cluster randomized trial1 at City of Hope National Medical Center conducted between August 2015 and February 2019 enrolled 613 participants and randomly assigned them to receive a GA-guided intervention or usual standard of care in a 2-to-1 ratio. Participants were eligible for the study if they were aged ≥65 years; had a diagnosis of solid malignant neoplasm of any stage; were starting a new chemotherapy regimen; and were fluent in English, Spanish, or Chinese.
The intervention included a GA at baseline followed by assessments focused on six common areas: sleep problems, problems with eating and feeding, incontinence, confusion, evidence of falls, and skin breakdown. An interdisciplinary team (oncologist, nurse practitioner, pharmacist, physical therapist, occupational therapist, social worker, and nutritionist) performed the assessment and developed a plan of care. Interventions were multifactorial and could include referral to specialists; recommendations for medication changes; symptom management; nutritional intervention with diet recommendations and supplementation; and interventions targeting social, spiritual, and functional well-being. Follow-up by a nurse practitioner continued until completion of chemotherapy or 6 months after starting chemotherapy, whichever was earlier.
The primary outcome was grade 3 or higher chemotherapy-related toxic effects using National Cancer Institute criteria, and secondary outcomes were advance directive completion, emergency room visits and unplanned hospitalizations, and survival up to 12 months. Results showed a 10% absolute reduction in the incidence of grade 3 or higher toxic effects (P = .02), with a number needed to treat of 10. Advance directive completion also increased by 15%, but no differences were observed for other outcomes. This study offers high-quality evidence that a GA-based intervention can reduce toxic effects of chemotherapy regimens for older adults with cancer.
Geriatric assessment in community oncology practices
A recent study by Supriya G. Mohile, MD, and colleagues2 is the first nationwide multicenter clinical trial to demonstrate the effects of GA and GA-guided management. This study was conducted in 40 oncology practices from the University of Rochester National Cancer Institute Community Oncology Research Program network. Centers were randomly assigned to intervention or usual care (362 patients treated by 68 oncologists in the intervention group and 371 patients treated by 91 oncologists in the usual-care group). Eligibility criteria were age ≥70 years; impairment in at least one GA domain other than polypharmacy; incurable advanced solid tumor or lymphoma with a plan to start new cancer treatment with a high risk for toxic effects within 4 weeks; and English language fluency. Both study groups underwent a baseline GA that assessed patients’ physical performance, functional status, comorbidity, cognition, nutrition, social support, polypharmacy, and psychological status. For the intervention group, a summary and management recommendations were provided to the treating oncologists.
The primary outcome was grade 3 or higher toxic effects within 3 months of starting a new regimen; secondary outcomes included treatment intensity and survival and GA outcomes within 3 months. A smaller proportion of patients in the intervention group experienced toxicity (51% vs. 71%), with an absolute risk reduction of 20%. Patients in the intervention group also had fewer falls and a greater reduction in medications used; there were no other differences in secondary outcomes. This study offers very strong and generalizable evidence that incorporating GA in the care of older adults with cancer at risk for toxicity can reduce toxicity as well as improve other outcomes, such as falls and polypharmacy.
Geriatric assessment and oncologist-patient communication
A secondary analysis3 of data from Dr. Mohile and colleagues2 evaluated the effect of GA-guided recommendations on oncologist-patient communication regarding comorbidities. Patients (n = 541) included in this analysis were 76.6 years of age on average and had 3.2 (standard deviation, 1.9) comorbid conditions. All patients underwent GA, but only oncologists in the intervention arm received GA-based recommendations. Clinical encounters between oncologist and patient immediately following the GA were audio recorded and analyzed to examine communication between oncologists and participants as it relates to chronic comorbid conditions.
In the intervention arm, more discussions regarding comorbidities took place, and more participants’ concerns about comorbidities were acknowledged. More importantly, participants in the intervention group were 2.4 times more likely to have their concerns about comorbidities addressed through referral or education, compared with the usual-care group (P = .004). Moreover, 41% of oncologists in the intervention arm modified dosage or cancer treatment schedule because of concern about tolerability or comorbidities. This study demonstrates beneficial effects of GA in increasing communication and perhaps consideration of comorbidities of older adults when planning cancer treatment.
Dr. Hung is professor of geriatrics and palliative care at Mount Sinai Hospital, New York. He disclosed no relevant conflicts of interest.
References
1. Li D et al. JAMA Oncol. 2021;7:e214158.
2. Mohile SG et al. Lancet. 2021;398:1894-1904.
3. Kleckner AS et al. JCO Oncol Pract. 2022;18:e9-19.
A version of this article first appeared on Medscape.com.
Age-related changes that potentiate adverse drug reactions include alterations in absorption, distribution, metabolism, and excretion. As such, older patients often require adjustments in medications to optimize safety and use. Medication adjustment is especially important for older patients on complex medication regimens for multiple conditions, such as those undergoing cancer treatment. Three recent high-quality randomized trials evaluated the use of geriatric assessment (GA) in older adults with cancer.1-3
Interdisciplinary GA can identify aging-related conditions associated with poor outcomes in older patients with cancer (e.g., toxic effects of chemotherapy) and provide recommendations aimed at improving health outcomes. The results of these trials suggest that interdisciplinary GA can improve care outcomes and oncologists’ communication for older adults with cancer, and should be considered an emerging standard of care.
Geriatric assessment and chemotherapy-related toxic effects
A cluster randomized trial1 at City of Hope National Medical Center conducted between August 2015 and February 2019 enrolled 613 participants and randomly assigned them to receive a GA-guided intervention or usual standard of care in a 2-to-1 ratio. Participants were eligible for the study if they were aged ≥65 years; had a diagnosis of solid malignant neoplasm of any stage; were starting a new chemotherapy regimen; and were fluent in English, Spanish, or Chinese.
The intervention included a GA at baseline followed by assessments focused on six common areas: sleep problems, problems with eating and feeding, incontinence, confusion, evidence of falls, and skin breakdown. An interdisciplinary team (oncologist, nurse practitioner, pharmacist, physical therapist, occupational therapist, social worker, and nutritionist) performed the assessment and developed a plan of care. Interventions were multifactorial and could include referral to specialists; recommendations for medication changes; symptom management; nutritional intervention with diet recommendations and supplementation; and interventions targeting social, spiritual, and functional well-being. Follow-up by a nurse practitioner continued until completion of chemotherapy or 6 months after starting chemotherapy, whichever was earlier.
The primary outcome was grade 3 or higher chemotherapy-related toxic effects using National Cancer Institute criteria, and secondary outcomes were advance directive completion, emergency room visits and unplanned hospitalizations, and survival up to 12 months. Results showed a 10% absolute reduction in the incidence of grade 3 or higher toxic effects (P = .02), with a number needed to treat of 10. Advance directive completion also increased by 15%, but no differences were observed for other outcomes. This study offers high-quality evidence that a GA-based intervention can reduce toxic effects of chemotherapy regimens for older adults with cancer.
Geriatric assessment in community oncology practices
A recent study by Supriya G. Mohile, MD, and colleagues2 is the first nationwide multicenter clinical trial to demonstrate the effects of GA and GA-guided management. This study was conducted in 40 oncology practices from the University of Rochester National Cancer Institute Community Oncology Research Program network. Centers were randomly assigned to intervention or usual care (362 patients treated by 68 oncologists in the intervention group and 371 patients treated by 91 oncologists in the usual-care group). Eligibility criteria were age ≥70 years; impairment in at least one GA domain other than polypharmacy; incurable advanced solid tumor or lymphoma with a plan to start new cancer treatment with a high risk for toxic effects within 4 weeks; and English language fluency. Both study groups underwent a baseline GA that assessed patients’ physical performance, functional status, comorbidity, cognition, nutrition, social support, polypharmacy, and psychological status. For the intervention group, a summary and management recommendations were provided to the treating oncologists.
The primary outcome was grade 3 or higher toxic effects within 3 months of starting a new regimen; secondary outcomes included treatment intensity and survival and GA outcomes within 3 months. A smaller proportion of patients in the intervention group experienced toxicity (51% vs. 71%), with an absolute risk reduction of 20%. Patients in the intervention group also had fewer falls and a greater reduction in medications used; there were no other differences in secondary outcomes. This study offers very strong and generalizable evidence that incorporating GA in the care of older adults with cancer at risk for toxicity can reduce toxicity as well as improve other outcomes, such as falls and polypharmacy.
Geriatric assessment and oncologist-patient communication
A secondary analysis3 of data from Dr. Mohile and colleagues2 evaluated the effect of GA-guided recommendations on oncologist-patient communication regarding comorbidities. Patients (n = 541) included in this analysis were 76.6 years of age on average and had 3.2 (standard deviation, 1.9) comorbid conditions. All patients underwent GA, but only oncologists in the intervention arm received GA-based recommendations. Clinical encounters between oncologist and patient immediately following the GA were audio recorded and analyzed to examine communication between oncologists and participants as it relates to chronic comorbid conditions.
In the intervention arm, more discussions regarding comorbidities took place, and more participants’ concerns about comorbidities were acknowledged. More importantly, participants in the intervention group were 2.4 times more likely to have their concerns about comorbidities addressed through referral or education, compared with the usual-care group (P = .004). Moreover, 41% of oncologists in the intervention arm modified dosage or cancer treatment schedule because of concern about tolerability or comorbidities. This study demonstrates beneficial effects of GA in increasing communication and perhaps consideration of comorbidities of older adults when planning cancer treatment.
Dr. Hung is professor of geriatrics and palliative care at Mount Sinai Hospital, New York. He disclosed no relevant conflicts of interest.
References
1. Li D et al. JAMA Oncol. 2021;7:e214158.
2. Mohile SG et al. Lancet. 2021;398:1894-1904.
3. Kleckner AS et al. JCO Oncol Pract. 2022;18:e9-19.
A version of this article first appeared on Medscape.com.
Age-related changes that potentiate adverse drug reactions include alterations in absorption, distribution, metabolism, and excretion. As such, older patients often require adjustments in medications to optimize safety and use. Medication adjustment is especially important for older patients on complex medication regimens for multiple conditions, such as those undergoing cancer treatment. Three recent high-quality randomized trials evaluated the use of geriatric assessment (GA) in older adults with cancer.1-3
Interdisciplinary GA can identify aging-related conditions associated with poor outcomes in older patients with cancer (e.g., toxic effects of chemotherapy) and provide recommendations aimed at improving health outcomes. The results of these trials suggest that interdisciplinary GA can improve care outcomes and oncologists’ communication for older adults with cancer, and should be considered an emerging standard of care.
Geriatric assessment and chemotherapy-related toxic effects
A cluster randomized trial1 at City of Hope National Medical Center conducted between August 2015 and February 2019 enrolled 613 participants and randomly assigned them to receive a GA-guided intervention or usual standard of care in a 2-to-1 ratio. Participants were eligible for the study if they were aged ≥65 years; had a diagnosis of solid malignant neoplasm of any stage; were starting a new chemotherapy regimen; and were fluent in English, Spanish, or Chinese.
The intervention included a GA at baseline followed by assessments focused on six common areas: sleep problems, problems with eating and feeding, incontinence, confusion, evidence of falls, and skin breakdown. An interdisciplinary team (oncologist, nurse practitioner, pharmacist, physical therapist, occupational therapist, social worker, and nutritionist) performed the assessment and developed a plan of care. Interventions were multifactorial and could include referral to specialists; recommendations for medication changes; symptom management; nutritional intervention with diet recommendations and supplementation; and interventions targeting social, spiritual, and functional well-being. Follow-up by a nurse practitioner continued until completion of chemotherapy or 6 months after starting chemotherapy, whichever was earlier.
The primary outcome was grade 3 or higher chemotherapy-related toxic effects using National Cancer Institute criteria, and secondary outcomes were advance directive completion, emergency room visits and unplanned hospitalizations, and survival up to 12 months. Results showed a 10% absolute reduction in the incidence of grade 3 or higher toxic effects (P = .02), with a number needed to treat of 10. Advance directive completion also increased by 15%, but no differences were observed for other outcomes. This study offers high-quality evidence that a GA-based intervention can reduce toxic effects of chemotherapy regimens for older adults with cancer.
Geriatric assessment in community oncology practices
A recent study by Supriya G. Mohile, MD, and colleagues2 is the first nationwide multicenter clinical trial to demonstrate the effects of GA and GA-guided management. This study was conducted in 40 oncology practices from the University of Rochester National Cancer Institute Community Oncology Research Program network. Centers were randomly assigned to intervention or usual care (362 patients treated by 68 oncologists in the intervention group and 371 patients treated by 91 oncologists in the usual-care group). Eligibility criteria were age ≥70 years; impairment in at least one GA domain other than polypharmacy; incurable advanced solid tumor or lymphoma with a plan to start new cancer treatment with a high risk for toxic effects within 4 weeks; and English language fluency. Both study groups underwent a baseline GA that assessed patients’ physical performance, functional status, comorbidity, cognition, nutrition, social support, polypharmacy, and psychological status. For the intervention group, a summary and management recommendations were provided to the treating oncologists.
The primary outcome was grade 3 or higher toxic effects within 3 months of starting a new regimen; secondary outcomes included treatment intensity and survival and GA outcomes within 3 months. A smaller proportion of patients in the intervention group experienced toxicity (51% vs. 71%), with an absolute risk reduction of 20%. Patients in the intervention group also had fewer falls and a greater reduction in medications used; there were no other differences in secondary outcomes. This study offers very strong and generalizable evidence that incorporating GA in the care of older adults with cancer at risk for toxicity can reduce toxicity as well as improve other outcomes, such as falls and polypharmacy.
Geriatric assessment and oncologist-patient communication
A secondary analysis3 of data from Dr. Mohile and colleagues2 evaluated the effect of GA-guided recommendations on oncologist-patient communication regarding comorbidities. Patients (n = 541) included in this analysis were 76.6 years of age on average and had 3.2 (standard deviation, 1.9) comorbid conditions. All patients underwent GA, but only oncologists in the intervention arm received GA-based recommendations. Clinical encounters between oncologist and patient immediately following the GA were audio recorded and analyzed to examine communication between oncologists and participants as it relates to chronic comorbid conditions.
In the intervention arm, more discussions regarding comorbidities took place, and more participants’ concerns about comorbidities were acknowledged. More importantly, participants in the intervention group were 2.4 times more likely to have their concerns about comorbidities addressed through referral or education, compared with the usual-care group (P = .004). Moreover, 41% of oncologists in the intervention arm modified dosage or cancer treatment schedule because of concern about tolerability or comorbidities. This study demonstrates beneficial effects of GA in increasing communication and perhaps consideration of comorbidities of older adults when planning cancer treatment.
Dr. Hung is professor of geriatrics and palliative care at Mount Sinai Hospital, New York. He disclosed no relevant conflicts of interest.
References
1. Li D et al. JAMA Oncol. 2021;7:e214158.
2. Mohile SG et al. Lancet. 2021;398:1894-1904.
3. Kleckner AS et al. JCO Oncol Pract. 2022;18:e9-19.
A version of this article first appeared on Medscape.com.
Hematocrit, White Blood Cells, and Thrombotic Events in the Veteran Population With Polycythemia Vera
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
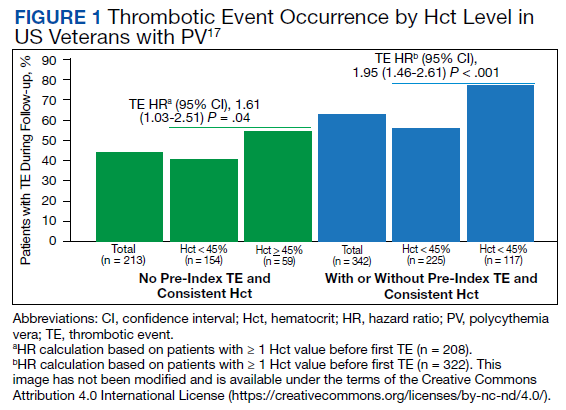
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
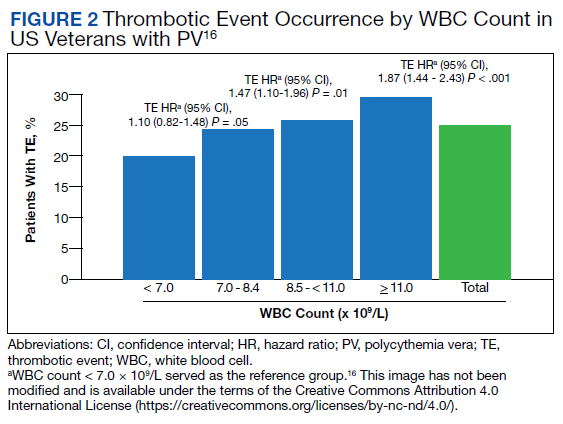
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
Cancer increases patients’ risk for cardiovascular deaths
and irrespective of cancer type, according to a population-based study.
The retrospective analysis, which included data from more than 200,000 patients with cancer, found that a new cancer diagnosis significantly increased the risk of cardiovascular (CV) death (hazard ratio [HR], 1.33) as well as other CV events, including stroke (HR, 1.44), heart failure (HR, 1.62) and pulmonary embolism (HR, 3.43).
From the results, the researchers concluded that a “new cancer diagnosis is independently associated with a significantly increased risk for cardiovascular death and nonfatal morbidity regardless of cancer site.”
The findings were published in the Journal of the American College of Cardiology: CardioOncology (2022 Mar;4[1]:85-94).
Patients with cancer and cancer survivors are known to have an increased risk for heart failure, but evidence on the risk for other CV outcomes remains less clear. In addition, the authors noted, many cancer therapies – including chest irradiation and chemotherapy – can increase a person’s risk of incident CV disease during treatment and after, but data on the long-term CV risk among cancer survivors conflict.
D. Ian Paterson, MD, of the University of Alberta, Edmonton, and coauthors wanted to clarify how a new cancer diagnosis at various sites and stages might affect a person’s risk for fatal and nonfatal CV events over the long term.
The current analysis included data from 224,016 patients with a new cancer diagnosis identified from an administrative database of more than 4.5 million adults residing in Alberta. The researcher identified 73,360 CV deaths and 470,481 nonfatal CV events between April 2007 and December 2018.
Comparing CV events in those with and in those without cancer, the authors found that patients with cancer had a 33% increased risk for CV mortality over the 12-year study follow-up, after adjusting for sociodemographic data and comorbidities (HR, 1.33; 95% confidence interval [CI], 1.29-1.37). Patients with cancer also had an increased risk for stroke (HR, 1.44), heart failure (HR, 1.62) and pulmonary embolism (HR, 3.43), though not myocardial infarction (HR, 1.01; 95% CI, 0.97 – 1.05), compared to those without cancer.
The extent of the risk varied somewhat by cancer stage, time from diagnosis, and cancer type.
A new cancer diagnosis put patients at a significantly higher risk of CV mortality, heart failure, stroke, or pulmonary embolism, regardless of the cancer site, but the risk of CV events was highest for patients with genitourinary, gastrointestinal, thoracic, nervous system, and hematologic malignancies. These patients accounted for more than half of the cancer cohort and more than 70% of the incident CV burden.
Patients with more advanced cancer were at the highest risk for poor CV outcomes, but even those with very early-stage disease faced an elevated risk.
The risk for CV events was greatest in the first year following a cancer diagnosis for all outcomes (HRs, 1.24-8.36) but remained significantly elevated for CV death, heart failure, and pulmonary embolism a decade later.
Overall, the authors concluded that “patients with cancer constitute a high-risk population for CV disease” over the long term and suggested that those with cancer “may benefit from comanagement that includes cardiologists as well as stroke and thrombosis specialists.”
In an accompanying editorial, Hiroshi Ohtsu of Juntendo University in Tokyo, and colleagues concluded that the work “has remarkable strengths” and important clinical implications. However, they said that additional steps may be warranted before translating these findings to clinical practice.
For example, the study is limited by its retrospective population-based design and the lack of data on cancer therapy as well as on several patient factors, including ethnicity, smoking, and physical activity.
The study authors agreed, noting that future work should evaluate how cancer therapies and other potential contributors to poor CV outcomes influence patients’ risk.
“Such work would potentially lead to better prediction of CV risk for patients with cancer and survivors and improved prevention and treatment strategies,” they wrote.
The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors have disclosed no relevant financial relationships. The editorial was supported in part by funding to individual authors from the Japan Society for the Promotion of Science/Ministry of Education, Culture, Sports, Science and Technology, the Ministry of Health, Labour and Welfare, and the Agency for Medical Research and Development.
A version of this article first appeared on Medscape.com.
and irrespective of cancer type, according to a population-based study.
The retrospective analysis, which included data from more than 200,000 patients with cancer, found that a new cancer diagnosis significantly increased the risk of cardiovascular (CV) death (hazard ratio [HR], 1.33) as well as other CV events, including stroke (HR, 1.44), heart failure (HR, 1.62) and pulmonary embolism (HR, 3.43).
From the results, the researchers concluded that a “new cancer diagnosis is independently associated with a significantly increased risk for cardiovascular death and nonfatal morbidity regardless of cancer site.”
The findings were published in the Journal of the American College of Cardiology: CardioOncology (2022 Mar;4[1]:85-94).
Patients with cancer and cancer survivors are known to have an increased risk for heart failure, but evidence on the risk for other CV outcomes remains less clear. In addition, the authors noted, many cancer therapies – including chest irradiation and chemotherapy – can increase a person’s risk of incident CV disease during treatment and after, but data on the long-term CV risk among cancer survivors conflict.
D. Ian Paterson, MD, of the University of Alberta, Edmonton, and coauthors wanted to clarify how a new cancer diagnosis at various sites and stages might affect a person’s risk for fatal and nonfatal CV events over the long term.
The current analysis included data from 224,016 patients with a new cancer diagnosis identified from an administrative database of more than 4.5 million adults residing in Alberta. The researcher identified 73,360 CV deaths and 470,481 nonfatal CV events between April 2007 and December 2018.
Comparing CV events in those with and in those without cancer, the authors found that patients with cancer had a 33% increased risk for CV mortality over the 12-year study follow-up, after adjusting for sociodemographic data and comorbidities (HR, 1.33; 95% confidence interval [CI], 1.29-1.37). Patients with cancer also had an increased risk for stroke (HR, 1.44), heart failure (HR, 1.62) and pulmonary embolism (HR, 3.43), though not myocardial infarction (HR, 1.01; 95% CI, 0.97 – 1.05), compared to those without cancer.
The extent of the risk varied somewhat by cancer stage, time from diagnosis, and cancer type.
A new cancer diagnosis put patients at a significantly higher risk of CV mortality, heart failure, stroke, or pulmonary embolism, regardless of the cancer site, but the risk of CV events was highest for patients with genitourinary, gastrointestinal, thoracic, nervous system, and hematologic malignancies. These patients accounted for more than half of the cancer cohort and more than 70% of the incident CV burden.
Patients with more advanced cancer were at the highest risk for poor CV outcomes, but even those with very early-stage disease faced an elevated risk.
The risk for CV events was greatest in the first year following a cancer diagnosis for all outcomes (HRs, 1.24-8.36) but remained significantly elevated for CV death, heart failure, and pulmonary embolism a decade later.
Overall, the authors concluded that “patients with cancer constitute a high-risk population for CV disease” over the long term and suggested that those with cancer “may benefit from comanagement that includes cardiologists as well as stroke and thrombosis specialists.”
In an accompanying editorial, Hiroshi Ohtsu of Juntendo University in Tokyo, and colleagues concluded that the work “has remarkable strengths” and important clinical implications. However, they said that additional steps may be warranted before translating these findings to clinical practice.
For example, the study is limited by its retrospective population-based design and the lack of data on cancer therapy as well as on several patient factors, including ethnicity, smoking, and physical activity.
The study authors agreed, noting that future work should evaluate how cancer therapies and other potential contributors to poor CV outcomes influence patients’ risk.
“Such work would potentially lead to better prediction of CV risk for patients with cancer and survivors and improved prevention and treatment strategies,” they wrote.
The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors have disclosed no relevant financial relationships. The editorial was supported in part by funding to individual authors from the Japan Society for the Promotion of Science/Ministry of Education, Culture, Sports, Science and Technology, the Ministry of Health, Labour and Welfare, and the Agency for Medical Research and Development.
A version of this article first appeared on Medscape.com.
and irrespective of cancer type, according to a population-based study.
The retrospective analysis, which included data from more than 200,000 patients with cancer, found that a new cancer diagnosis significantly increased the risk of cardiovascular (CV) death (hazard ratio [HR], 1.33) as well as other CV events, including stroke (HR, 1.44), heart failure (HR, 1.62) and pulmonary embolism (HR, 3.43).
From the results, the researchers concluded that a “new cancer diagnosis is independently associated with a significantly increased risk for cardiovascular death and nonfatal morbidity regardless of cancer site.”
The findings were published in the Journal of the American College of Cardiology: CardioOncology (2022 Mar;4[1]:85-94).
Patients with cancer and cancer survivors are known to have an increased risk for heart failure, but evidence on the risk for other CV outcomes remains less clear. In addition, the authors noted, many cancer therapies – including chest irradiation and chemotherapy – can increase a person’s risk of incident CV disease during treatment and after, but data on the long-term CV risk among cancer survivors conflict.
D. Ian Paterson, MD, of the University of Alberta, Edmonton, and coauthors wanted to clarify how a new cancer diagnosis at various sites and stages might affect a person’s risk for fatal and nonfatal CV events over the long term.
The current analysis included data from 224,016 patients with a new cancer diagnosis identified from an administrative database of more than 4.5 million adults residing in Alberta. The researcher identified 73,360 CV deaths and 470,481 nonfatal CV events between April 2007 and December 2018.
Comparing CV events in those with and in those without cancer, the authors found that patients with cancer had a 33% increased risk for CV mortality over the 12-year study follow-up, after adjusting for sociodemographic data and comorbidities (HR, 1.33; 95% confidence interval [CI], 1.29-1.37). Patients with cancer also had an increased risk for stroke (HR, 1.44), heart failure (HR, 1.62) and pulmonary embolism (HR, 3.43), though not myocardial infarction (HR, 1.01; 95% CI, 0.97 – 1.05), compared to those without cancer.
The extent of the risk varied somewhat by cancer stage, time from diagnosis, and cancer type.
A new cancer diagnosis put patients at a significantly higher risk of CV mortality, heart failure, stroke, or pulmonary embolism, regardless of the cancer site, but the risk of CV events was highest for patients with genitourinary, gastrointestinal, thoracic, nervous system, and hematologic malignancies. These patients accounted for more than half of the cancer cohort and more than 70% of the incident CV burden.
Patients with more advanced cancer were at the highest risk for poor CV outcomes, but even those with very early-stage disease faced an elevated risk.
The risk for CV events was greatest in the first year following a cancer diagnosis for all outcomes (HRs, 1.24-8.36) but remained significantly elevated for CV death, heart failure, and pulmonary embolism a decade later.
Overall, the authors concluded that “patients with cancer constitute a high-risk population for CV disease” over the long term and suggested that those with cancer “may benefit from comanagement that includes cardiologists as well as stroke and thrombosis specialists.”
In an accompanying editorial, Hiroshi Ohtsu of Juntendo University in Tokyo, and colleagues concluded that the work “has remarkable strengths” and important clinical implications. However, they said that additional steps may be warranted before translating these findings to clinical practice.
For example, the study is limited by its retrospective population-based design and the lack of data on cancer therapy as well as on several patient factors, including ethnicity, smoking, and physical activity.
The study authors agreed, noting that future work should evaluate how cancer therapies and other potential contributors to poor CV outcomes influence patients’ risk.
“Such work would potentially lead to better prediction of CV risk for patients with cancer and survivors and improved prevention and treatment strategies,” they wrote.
The study was supported by a foundation grant from the Canadian Institutes of Health Research. The authors have disclosed no relevant financial relationships. The editorial was supported in part by funding to individual authors from the Japan Society for the Promotion of Science/Ministry of Education, Culture, Sports, Science and Technology, the Ministry of Health, Labour and Welfare, and the Agency for Medical Research and Development.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
FDA approves first PARP inhibitor for early BRCA+ breast cancer
BRCA+ breast cancer
Specifically, the new approval is for the adjuvant treatment of adult patients with high-risk early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The FDA also approved BRACAnalysis CDx (Myriad Genetics), a companion diagnostic test to identify patients who may benefit from olaparib.
The latest approval was based on phase 3 OlympiA trial results, which showed a 42% improvement in invasive and distant disease-free survival with olaparib in comparison with placebo. Data from OlympiaA and other clinical studies also confirm BRACAnalysis CDx as “an effective test for patients deciding on their best treatment options,” Myriad Genetics noted in a press release.
The OlympiA results, as reported by this news organization, were presented during the plenary session of the American Society of Clinical Oncology 2021 annual meeting and were published in the New England Journal of Medicine.
Those findings prompted an ASCO “rapid recommendation” updating of ASCO’s 2020 guidelines for the management of hereditary breast cancer.
The latest results from OlympiA show that olaparib reduced the risk of death by 32% (hazard ratio, 0.68) in comparison with placebo, according to a company press release announcing the approval. Overall survival data are slated for presentation at a European Society for Medical Oncology Virtual Plenary session on March 16, 2022.
A version of this article first appeared on Medscape.com.
Specifically, the new approval is for the adjuvant treatment of adult patients with high-risk early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The FDA also approved BRACAnalysis CDx (Myriad Genetics), a companion diagnostic test to identify patients who may benefit from olaparib.
The latest approval was based on phase 3 OlympiA trial results, which showed a 42% improvement in invasive and distant disease-free survival with olaparib in comparison with placebo. Data from OlympiaA and other clinical studies also confirm BRACAnalysis CDx as “an effective test for patients deciding on their best treatment options,” Myriad Genetics noted in a press release.
The OlympiA results, as reported by this news organization, were presented during the plenary session of the American Society of Clinical Oncology 2021 annual meeting and were published in the New England Journal of Medicine.
Those findings prompted an ASCO “rapid recommendation” updating of ASCO’s 2020 guidelines for the management of hereditary breast cancer.
The latest results from OlympiA show that olaparib reduced the risk of death by 32% (hazard ratio, 0.68) in comparison with placebo, according to a company press release announcing the approval. Overall survival data are slated for presentation at a European Society for Medical Oncology Virtual Plenary session on March 16, 2022.
A version of this article first appeared on Medscape.com.
Specifically, the new approval is for the adjuvant treatment of adult patients with high-risk early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The FDA also approved BRACAnalysis CDx (Myriad Genetics), a companion diagnostic test to identify patients who may benefit from olaparib.
The latest approval was based on phase 3 OlympiA trial results, which showed a 42% improvement in invasive and distant disease-free survival with olaparib in comparison with placebo. Data from OlympiaA and other clinical studies also confirm BRACAnalysis CDx as “an effective test for patients deciding on their best treatment options,” Myriad Genetics noted in a press release.
The OlympiA results, as reported by this news organization, were presented during the plenary session of the American Society of Clinical Oncology 2021 annual meeting and were published in the New England Journal of Medicine.
Those findings prompted an ASCO “rapid recommendation” updating of ASCO’s 2020 guidelines for the management of hereditary breast cancer.
The latest results from OlympiA show that olaparib reduced the risk of death by 32% (hazard ratio, 0.68) in comparison with placebo, according to a company press release announcing the approval. Overall survival data are slated for presentation at a European Society for Medical Oncology Virtual Plenary session on March 16, 2022.
A version of this article first appeared on Medscape.com.
BRCA+ breast cancer
BRCA+ breast cancer
Registry data support lowering CRC screening age to 45
Approximately one-third of people between 45 and 49 years of age who undergo colonoscopies have neoplastic colorectal pathology, according to a retrospective analysis.
According to the researchers, led by Parth Trivedi, MD, of the Icahn School of Medicine at Mount Sinai, New York, there has progressively been a “disturbing” rise in early-onset colorectal cancer (CRC) in the United States, which has prompted guidelines from the American Cancer Society to the U.S. Preventive Services Task Force to recommend lowering the CRC screening starting age to 45 years old for average-risk individuals. Despite these recommendations, little research to date has fully characterized the prevalence of colorectal neoplasia in individuals younger than the currently recommended CRC onset screening age of 50 years.
Dr. Trivedi and colleagues, who published their study findings in Gastroenterology, retrospectively reviewed colonoscopy data recorded in the Gastrointestinal Quality Improvement Consortium Registry to address the current knowledge gaps on early-onset CRC. Collected data were for procedures conducted at 123 AMSURG ambulatory endoscopy centers across 29 states between January 2014 and February 2021. In total, 2,921,816 colonoscopies during the study period among patients aged 18-54 years were recorded by AMSURG-associated endoscopists; of these, 562,559 met inclusion criteria for high-quality screening or diagnostic colonoscopy procedures.
The researchers pooled a young-onset age group, including patients between the ages of 18 and 49 years old, in whom 145,998 procedures were performed, including 79,934 procedures in patients aged 45-49 years. A comparator group with 336,627 procedures in patients aged 50-54 years was also included in the study. The findings were categorized into CRC, advanced premalignant lesions (APL), and “any neoplasia,” the latter of which included all adenomas, sessile serrated polyps, and CRC.
Among patients aged 18-44 years, the most frequent indications were “diagnostic-other” (45.6%) as well as “diagnostic-bleeding” (39.4%). Among patients between 45 and 49 years of age, the most frequent indications were “screening” (41.4%) and “diagnostic-other” (30.7%). Nearly all (90%) procedures among those aged 50-54 years were for screening.
A multivariable logistic regression identified 5 variables predictive of either APL or CRC in patients between 18 and 49 years of age: increasing age (odds ratio, 1.08; 95% confidence interval, 1.07-1.08; P <0.01), male sex (OR = 1.67; 95% CI, 1.63-1.70; P <0.01), White race (vs. African American: OR = 0.76; 95% CI, 0.73-0.79, P <0.01; vs. Asian: OR = 0.89; 95% CI, 0.84-0.94, P <0.01), family history of CRC (OR = 1.21; 95% CI, 1.16-1.26; P <0.01) and polyps (OR = 1.33; 95% CI, 1.24-1.43; P <0.01), and examinations for bleeding (OR = 1.15; 95% CI, 1.12-1.18; P <0.01) or screening (OR = 1.20; 95% CI, 1.16-1.24; P <0.01).
The prevalence of neoplastic findings in the young-onset age-group increased with increasing age for the categories of any neoplasia, APLs, and CRC. Among patients aged 40-44, 26.59% had any neoplasia, 5.76% had APL, and 0.53% had CRC. In those aged 45-49 years, around 32% had any neoplasia, approximately 7.5% had APLs, and nearly 0.58% had CRC. In the 50- to 54-year-old group, the prevalences of any neoplasia, APL, and CRC were 37.72%, 9.48%, and 0.32%, respectively.
Across all age groups, a family history of CRC was associated with a higher prevalence of any neoplasia and APL. In addition, the rates of any APL and neoplasia in patients with a family history of CRC were comparable to patients who were 5 years older but had no family history of the disease. Across most young-onset age group, individuals with a positive family history had a lower CRC prevalence versus patients with no family history.
The researchers noted that their population data are derived from ambulatory endoscopy centers, which may introduce bias associated with insurance coverage or patient preference to attend specific endoscopic centers. Additionally, the investigators stated that many records on race and ethnicity were missing, further limiting the findings.
“The present analysis of neoplastic colorectal pathology among individuals younger than age 50 suggests that lowering the screening age to 45 for men and women of all races and ethnicities will likely detect important pathology rather frequently,” they concluded. In addition, the researchers noted that the study results “underscore the importance of early messaging to patients and providers in the years leading up to age 45.” Ultimately, improved “awareness of pathology prevalence in individuals younger than age 45 can help guide clinicians in the clinical management of CRC risk,” the researchers wrote.
Several of the researchers reported conflicts of interest with Exact Sciences Corp and Freenome. The study received no industry funding.
Approximately one-third of people between 45 and 49 years of age who undergo colonoscopies have neoplastic colorectal pathology, according to a retrospective analysis.
According to the researchers, led by Parth Trivedi, MD, of the Icahn School of Medicine at Mount Sinai, New York, there has progressively been a “disturbing” rise in early-onset colorectal cancer (CRC) in the United States, which has prompted guidelines from the American Cancer Society to the U.S. Preventive Services Task Force to recommend lowering the CRC screening starting age to 45 years old for average-risk individuals. Despite these recommendations, little research to date has fully characterized the prevalence of colorectal neoplasia in individuals younger than the currently recommended CRC onset screening age of 50 years.
Dr. Trivedi and colleagues, who published their study findings in Gastroenterology, retrospectively reviewed colonoscopy data recorded in the Gastrointestinal Quality Improvement Consortium Registry to address the current knowledge gaps on early-onset CRC. Collected data were for procedures conducted at 123 AMSURG ambulatory endoscopy centers across 29 states between January 2014 and February 2021. In total, 2,921,816 colonoscopies during the study period among patients aged 18-54 years were recorded by AMSURG-associated endoscopists; of these, 562,559 met inclusion criteria for high-quality screening or diagnostic colonoscopy procedures.
The researchers pooled a young-onset age group, including patients between the ages of 18 and 49 years old, in whom 145,998 procedures were performed, including 79,934 procedures in patients aged 45-49 years. A comparator group with 336,627 procedures in patients aged 50-54 years was also included in the study. The findings were categorized into CRC, advanced premalignant lesions (APL), and “any neoplasia,” the latter of which included all adenomas, sessile serrated polyps, and CRC.
Among patients aged 18-44 years, the most frequent indications were “diagnostic-other” (45.6%) as well as “diagnostic-bleeding” (39.4%). Among patients between 45 and 49 years of age, the most frequent indications were “screening” (41.4%) and “diagnostic-other” (30.7%). Nearly all (90%) procedures among those aged 50-54 years were for screening.
A multivariable logistic regression identified 5 variables predictive of either APL or CRC in patients between 18 and 49 years of age: increasing age (odds ratio, 1.08; 95% confidence interval, 1.07-1.08; P <0.01), male sex (OR = 1.67; 95% CI, 1.63-1.70; P <0.01), White race (vs. African American: OR = 0.76; 95% CI, 0.73-0.79, P <0.01; vs. Asian: OR = 0.89; 95% CI, 0.84-0.94, P <0.01), family history of CRC (OR = 1.21; 95% CI, 1.16-1.26; P <0.01) and polyps (OR = 1.33; 95% CI, 1.24-1.43; P <0.01), and examinations for bleeding (OR = 1.15; 95% CI, 1.12-1.18; P <0.01) or screening (OR = 1.20; 95% CI, 1.16-1.24; P <0.01).
The prevalence of neoplastic findings in the young-onset age-group increased with increasing age for the categories of any neoplasia, APLs, and CRC. Among patients aged 40-44, 26.59% had any neoplasia, 5.76% had APL, and 0.53% had CRC. In those aged 45-49 years, around 32% had any neoplasia, approximately 7.5% had APLs, and nearly 0.58% had CRC. In the 50- to 54-year-old group, the prevalences of any neoplasia, APL, and CRC were 37.72%, 9.48%, and 0.32%, respectively.
Across all age groups, a family history of CRC was associated with a higher prevalence of any neoplasia and APL. In addition, the rates of any APL and neoplasia in patients with a family history of CRC were comparable to patients who were 5 years older but had no family history of the disease. Across most young-onset age group, individuals with a positive family history had a lower CRC prevalence versus patients with no family history.
The researchers noted that their population data are derived from ambulatory endoscopy centers, which may introduce bias associated with insurance coverage or patient preference to attend specific endoscopic centers. Additionally, the investigators stated that many records on race and ethnicity were missing, further limiting the findings.
“The present analysis of neoplastic colorectal pathology among individuals younger than age 50 suggests that lowering the screening age to 45 for men and women of all races and ethnicities will likely detect important pathology rather frequently,” they concluded. In addition, the researchers noted that the study results “underscore the importance of early messaging to patients and providers in the years leading up to age 45.” Ultimately, improved “awareness of pathology prevalence in individuals younger than age 45 can help guide clinicians in the clinical management of CRC risk,” the researchers wrote.
Several of the researchers reported conflicts of interest with Exact Sciences Corp and Freenome. The study received no industry funding.
Approximately one-third of people between 45 and 49 years of age who undergo colonoscopies have neoplastic colorectal pathology, according to a retrospective analysis.
According to the researchers, led by Parth Trivedi, MD, of the Icahn School of Medicine at Mount Sinai, New York, there has progressively been a “disturbing” rise in early-onset colorectal cancer (CRC) in the United States, which has prompted guidelines from the American Cancer Society to the U.S. Preventive Services Task Force to recommend lowering the CRC screening starting age to 45 years old for average-risk individuals. Despite these recommendations, little research to date has fully characterized the prevalence of colorectal neoplasia in individuals younger than the currently recommended CRC onset screening age of 50 years.
Dr. Trivedi and colleagues, who published their study findings in Gastroenterology, retrospectively reviewed colonoscopy data recorded in the Gastrointestinal Quality Improvement Consortium Registry to address the current knowledge gaps on early-onset CRC. Collected data were for procedures conducted at 123 AMSURG ambulatory endoscopy centers across 29 states between January 2014 and February 2021. In total, 2,921,816 colonoscopies during the study period among patients aged 18-54 years were recorded by AMSURG-associated endoscopists; of these, 562,559 met inclusion criteria for high-quality screening or diagnostic colonoscopy procedures.
The researchers pooled a young-onset age group, including patients between the ages of 18 and 49 years old, in whom 145,998 procedures were performed, including 79,934 procedures in patients aged 45-49 years. A comparator group with 336,627 procedures in patients aged 50-54 years was also included in the study. The findings were categorized into CRC, advanced premalignant lesions (APL), and “any neoplasia,” the latter of which included all adenomas, sessile serrated polyps, and CRC.
Among patients aged 18-44 years, the most frequent indications were “diagnostic-other” (45.6%) as well as “diagnostic-bleeding” (39.4%). Among patients between 45 and 49 years of age, the most frequent indications were “screening” (41.4%) and “diagnostic-other” (30.7%). Nearly all (90%) procedures among those aged 50-54 years were for screening.
A multivariable logistic regression identified 5 variables predictive of either APL or CRC in patients between 18 and 49 years of age: increasing age (odds ratio, 1.08; 95% confidence interval, 1.07-1.08; P <0.01), male sex (OR = 1.67; 95% CI, 1.63-1.70; P <0.01), White race (vs. African American: OR = 0.76; 95% CI, 0.73-0.79, P <0.01; vs. Asian: OR = 0.89; 95% CI, 0.84-0.94, P <0.01), family history of CRC (OR = 1.21; 95% CI, 1.16-1.26; P <0.01) and polyps (OR = 1.33; 95% CI, 1.24-1.43; P <0.01), and examinations for bleeding (OR = 1.15; 95% CI, 1.12-1.18; P <0.01) or screening (OR = 1.20; 95% CI, 1.16-1.24; P <0.01).
The prevalence of neoplastic findings in the young-onset age-group increased with increasing age for the categories of any neoplasia, APLs, and CRC. Among patients aged 40-44, 26.59% had any neoplasia, 5.76% had APL, and 0.53% had CRC. In those aged 45-49 years, around 32% had any neoplasia, approximately 7.5% had APLs, and nearly 0.58% had CRC. In the 50- to 54-year-old group, the prevalences of any neoplasia, APL, and CRC were 37.72%, 9.48%, and 0.32%, respectively.
Across all age groups, a family history of CRC was associated with a higher prevalence of any neoplasia and APL. In addition, the rates of any APL and neoplasia in patients with a family history of CRC were comparable to patients who were 5 years older but had no family history of the disease. Across most young-onset age group, individuals with a positive family history had a lower CRC prevalence versus patients with no family history.
The researchers noted that their population data are derived from ambulatory endoscopy centers, which may introduce bias associated with insurance coverage or patient preference to attend specific endoscopic centers. Additionally, the investigators stated that many records on race and ethnicity were missing, further limiting the findings.
“The present analysis of neoplastic colorectal pathology among individuals younger than age 50 suggests that lowering the screening age to 45 for men and women of all races and ethnicities will likely detect important pathology rather frequently,” they concluded. In addition, the researchers noted that the study results “underscore the importance of early messaging to patients and providers in the years leading up to age 45.” Ultimately, improved “awareness of pathology prevalence in individuals younger than age 45 can help guide clinicians in the clinical management of CRC risk,” the researchers wrote.
Several of the researchers reported conflicts of interest with Exact Sciences Corp and Freenome. The study received no industry funding.
FROM GASTROENTEROLOGY
Can green tea extract protect against colorectal adenomas?
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
RFA has long-lasting protective effects in esophageal cancer
Radiofrequency ablation (RFA) is effective and long lasting in preventing esophageal adenocarcinoma, new data suggest.
Researchers, led by Paul Wolfson, MBBS, from the Wellcome/EPSRC (Engineering and Physical Sciences Research Council) Centre for Interventional & Surgical Sciences, University College London also found that most treatment relapses happen early and can be re-treated successfully.
Findings were published in a final 10-year report from the United Kingdom National Halo Radiofrequency Ablation Registry and in Gastrointestinal Endoscopy. Because RFA has been used in mainstream clinical practice only since 2005, long-term data of more than 5 years has been lacking.
Multiple studies have shown that RFA is effective in preventing esophageal cancer, but data have been lacking on how long RFA is effective in preventing esophageal adenocarcinoma in patients with dysplastic Barrett’s esophagus (BE). A significant number of patients with dysplastic BE do not initially have visible lesions. For instance, the U.S. RFA Patient Registry reported an average 2.7-year follow up of 4,982 patients, but only 1,305 had dysplasia, the authors of the U.K. report note.
“It is well-established that endoscopic treatment of dysplastic BE is initially successful in up to 90% of patients,” the authors wrote. “What is less well understood is how long that benefit lasts and if this contributes to a substantial reduction in progression to cancer.”
Researchers prospectively gathered data from 2,535 patients from 28 U.K. specialist centers who underwent RFA therapy for BE (average length 5.2cm, range 1-20 cm). Among the group, 20% had low-grade dysplasia, 54% had high-grade dysplasia, and 26% had intramucosal carcinoma.
They looked at rates of invasive cancer and analyzed data for 1,175 patients to assess clearance rates of dysplasia (CR-D) and intestinal metaplasia (CR-IM) within 2 years of starting RFA, then looked at relapses and rates of return to CR-D and CR-IM after more therapy.
One year after RFA therapy, the Kaplan Meier (KM) rate of invasive cancer in the 2,535 patients was 0.5%. Ten years after starting treatment, the KM cancer rate was 4.1%, with a crude incidence rate of 0.52 per 100 patient-years. After 2 years of RFA, CR-D was 88% and CR-IM was 62.6%.
At 8 years, the KM relapse rates were 5.9% from CR-D and 18.7% from CR-IM. Most relapses happened in the first 2 years.
“Our study confirms durable reversal of dysplasia and BE with RFA, which reduces cancer risk by more than 90% compared to historical control data of 6-19% per annum,” the authors wrote.
Despite advances in diagnosis and treatment for esophageal adenocarcinoma, there has been only small improvement in 5-year survival over the past 40 years, the authors note. Meanwhile, the incidence of continues to rise in the Western world.
Researchers look for minimally invasive solutions
Surgery removing the esophagus and lymph node clearance had been the standard for high-grade dysplasia, the authors wrote. It is still the intervention of choice for patients with locoregional disease, but it comes with high morbidity and mortality rates.
This has spurred researchers to look for a minimally invasive solution focused on organ preservation to treat early disease and avoid surgical side effects but also to deliver a cure, according to the authors.
Shria Kumar, MD, assistant professor in the Division of Digestive and Liver Diseases at University of Miami Miller School of Medicine, told this publication, “Endoscopic ablation of dysplasia or intramucosal cancer is a mainstay of Barrett’s treatment.”
She noted the importance of the 10-year time period as the initial studies that established ablation evaluated outcomes within 1-3 years, and more recent data shows 5-year favorable outcomes.
Citing a study from the New England Journal of Medicine, Dr. Kumar said, “The present study’s cohort developed cancer at rates similar to one of the earlier U.S.-based cohorts of Barrett’s patients, suggesting that we can draw some parallels.”
She pointed out notable characteristics in the U.K. cohort: “The majority of participants were male and Caucasian; 80% of had high-grade dysplasia or early cancer upon enrollment and long-segment Barrett’s.”
That difference is important when thinking about how this applies to a more diverse U.S. population, she said, or even patients who don’t have high-grade dysplasia or early cancer when they enroll.
“It’s also important to point out are that individuals with low-grade dysplasia were included in this U.K.-based study. There has been evidence that persons in Europe with low-grade dysplasia have higher rates of progression than persons in the U.S. with low-grade dysplasia.”
Dr. Kumar said this may be attributable to differences in the way pathologists practice in the two countries or in endoscopists’ treatment patterns. U.S. guidelines agree that ablation can be used in select persons with low-grade dysplasia, she said, but it’s an area that needs further study.
“Overall, though, this is a really important study of real-time data showing that ablation is impacting cancer rates in a positive way and that in select patients, we can really decrease the risk of invasive cancer by endoscopic eradication therapies,” Dr. Kumar said.
Two coauthors have received grants from Medtronic and Pentax Medical. The other authors have declared no relevant financial relationships. Dr. Kumar reports no relevant financial relationships.
Radiofrequency ablation (RFA) is effective and long lasting in preventing esophageal adenocarcinoma, new data suggest.
Researchers, led by Paul Wolfson, MBBS, from the Wellcome/EPSRC (Engineering and Physical Sciences Research Council) Centre for Interventional & Surgical Sciences, University College London also found that most treatment relapses happen early and can be re-treated successfully.
Findings were published in a final 10-year report from the United Kingdom National Halo Radiofrequency Ablation Registry and in Gastrointestinal Endoscopy. Because RFA has been used in mainstream clinical practice only since 2005, long-term data of more than 5 years has been lacking.
Multiple studies have shown that RFA is effective in preventing esophageal cancer, but data have been lacking on how long RFA is effective in preventing esophageal adenocarcinoma in patients with dysplastic Barrett’s esophagus (BE). A significant number of patients with dysplastic BE do not initially have visible lesions. For instance, the U.S. RFA Patient Registry reported an average 2.7-year follow up of 4,982 patients, but only 1,305 had dysplasia, the authors of the U.K. report note.
“It is well-established that endoscopic treatment of dysplastic BE is initially successful in up to 90% of patients,” the authors wrote. “What is less well understood is how long that benefit lasts and if this contributes to a substantial reduction in progression to cancer.”
Researchers prospectively gathered data from 2,535 patients from 28 U.K. specialist centers who underwent RFA therapy for BE (average length 5.2cm, range 1-20 cm). Among the group, 20% had low-grade dysplasia, 54% had high-grade dysplasia, and 26% had intramucosal carcinoma.
They looked at rates of invasive cancer and analyzed data for 1,175 patients to assess clearance rates of dysplasia (CR-D) and intestinal metaplasia (CR-IM) within 2 years of starting RFA, then looked at relapses and rates of return to CR-D and CR-IM after more therapy.
One year after RFA therapy, the Kaplan Meier (KM) rate of invasive cancer in the 2,535 patients was 0.5%. Ten years after starting treatment, the KM cancer rate was 4.1%, with a crude incidence rate of 0.52 per 100 patient-years. After 2 years of RFA, CR-D was 88% and CR-IM was 62.6%.
At 8 years, the KM relapse rates were 5.9% from CR-D and 18.7% from CR-IM. Most relapses happened in the first 2 years.
“Our study confirms durable reversal of dysplasia and BE with RFA, which reduces cancer risk by more than 90% compared to historical control data of 6-19% per annum,” the authors wrote.
Despite advances in diagnosis and treatment for esophageal adenocarcinoma, there has been only small improvement in 5-year survival over the past 40 years, the authors note. Meanwhile, the incidence of continues to rise in the Western world.
Researchers look for minimally invasive solutions
Surgery removing the esophagus and lymph node clearance had been the standard for high-grade dysplasia, the authors wrote. It is still the intervention of choice for patients with locoregional disease, but it comes with high morbidity and mortality rates.
This has spurred researchers to look for a minimally invasive solution focused on organ preservation to treat early disease and avoid surgical side effects but also to deliver a cure, according to the authors.
Shria Kumar, MD, assistant professor in the Division of Digestive and Liver Diseases at University of Miami Miller School of Medicine, told this publication, “Endoscopic ablation of dysplasia or intramucosal cancer is a mainstay of Barrett’s treatment.”
She noted the importance of the 10-year time period as the initial studies that established ablation evaluated outcomes within 1-3 years, and more recent data shows 5-year favorable outcomes.
Citing a study from the New England Journal of Medicine, Dr. Kumar said, “The present study’s cohort developed cancer at rates similar to one of the earlier U.S.-based cohorts of Barrett’s patients, suggesting that we can draw some parallels.”
She pointed out notable characteristics in the U.K. cohort: “The majority of participants were male and Caucasian; 80% of had high-grade dysplasia or early cancer upon enrollment and long-segment Barrett’s.”
That difference is important when thinking about how this applies to a more diverse U.S. population, she said, or even patients who don’t have high-grade dysplasia or early cancer when they enroll.
“It’s also important to point out are that individuals with low-grade dysplasia were included in this U.K.-based study. There has been evidence that persons in Europe with low-grade dysplasia have higher rates of progression than persons in the U.S. with low-grade dysplasia.”
Dr. Kumar said this may be attributable to differences in the way pathologists practice in the two countries or in endoscopists’ treatment patterns. U.S. guidelines agree that ablation can be used in select persons with low-grade dysplasia, she said, but it’s an area that needs further study.
“Overall, though, this is a really important study of real-time data showing that ablation is impacting cancer rates in a positive way and that in select patients, we can really decrease the risk of invasive cancer by endoscopic eradication therapies,” Dr. Kumar said.
Two coauthors have received grants from Medtronic and Pentax Medical. The other authors have declared no relevant financial relationships. Dr. Kumar reports no relevant financial relationships.
Radiofrequency ablation (RFA) is effective and long lasting in preventing esophageal adenocarcinoma, new data suggest.
Researchers, led by Paul Wolfson, MBBS, from the Wellcome/EPSRC (Engineering and Physical Sciences Research Council) Centre for Interventional & Surgical Sciences, University College London also found that most treatment relapses happen early and can be re-treated successfully.
Findings were published in a final 10-year report from the United Kingdom National Halo Radiofrequency Ablation Registry and in Gastrointestinal Endoscopy. Because RFA has been used in mainstream clinical practice only since 2005, long-term data of more than 5 years has been lacking.
Multiple studies have shown that RFA is effective in preventing esophageal cancer, but data have been lacking on how long RFA is effective in preventing esophageal adenocarcinoma in patients with dysplastic Barrett’s esophagus (BE). A significant number of patients with dysplastic BE do not initially have visible lesions. For instance, the U.S. RFA Patient Registry reported an average 2.7-year follow up of 4,982 patients, but only 1,305 had dysplasia, the authors of the U.K. report note.
“It is well-established that endoscopic treatment of dysplastic BE is initially successful in up to 90% of patients,” the authors wrote. “What is less well understood is how long that benefit lasts and if this contributes to a substantial reduction in progression to cancer.”
Researchers prospectively gathered data from 2,535 patients from 28 U.K. specialist centers who underwent RFA therapy for BE (average length 5.2cm, range 1-20 cm). Among the group, 20% had low-grade dysplasia, 54% had high-grade dysplasia, and 26% had intramucosal carcinoma.
They looked at rates of invasive cancer and analyzed data for 1,175 patients to assess clearance rates of dysplasia (CR-D) and intestinal metaplasia (CR-IM) within 2 years of starting RFA, then looked at relapses and rates of return to CR-D and CR-IM after more therapy.
One year after RFA therapy, the Kaplan Meier (KM) rate of invasive cancer in the 2,535 patients was 0.5%. Ten years after starting treatment, the KM cancer rate was 4.1%, with a crude incidence rate of 0.52 per 100 patient-years. After 2 years of RFA, CR-D was 88% and CR-IM was 62.6%.
At 8 years, the KM relapse rates were 5.9% from CR-D and 18.7% from CR-IM. Most relapses happened in the first 2 years.
“Our study confirms durable reversal of dysplasia and BE with RFA, which reduces cancer risk by more than 90% compared to historical control data of 6-19% per annum,” the authors wrote.
Despite advances in diagnosis and treatment for esophageal adenocarcinoma, there has been only small improvement in 5-year survival over the past 40 years, the authors note. Meanwhile, the incidence of continues to rise in the Western world.
Researchers look for minimally invasive solutions
Surgery removing the esophagus and lymph node clearance had been the standard for high-grade dysplasia, the authors wrote. It is still the intervention of choice for patients with locoregional disease, but it comes with high morbidity and mortality rates.
This has spurred researchers to look for a minimally invasive solution focused on organ preservation to treat early disease and avoid surgical side effects but also to deliver a cure, according to the authors.
Shria Kumar, MD, assistant professor in the Division of Digestive and Liver Diseases at University of Miami Miller School of Medicine, told this publication, “Endoscopic ablation of dysplasia or intramucosal cancer is a mainstay of Barrett’s treatment.”
She noted the importance of the 10-year time period as the initial studies that established ablation evaluated outcomes within 1-3 years, and more recent data shows 5-year favorable outcomes.
Citing a study from the New England Journal of Medicine, Dr. Kumar said, “The present study’s cohort developed cancer at rates similar to one of the earlier U.S.-based cohorts of Barrett’s patients, suggesting that we can draw some parallels.”
She pointed out notable characteristics in the U.K. cohort: “The majority of participants were male and Caucasian; 80% of had high-grade dysplasia or early cancer upon enrollment and long-segment Barrett’s.”
That difference is important when thinking about how this applies to a more diverse U.S. population, she said, or even patients who don’t have high-grade dysplasia or early cancer when they enroll.
“It’s also important to point out are that individuals with low-grade dysplasia were included in this U.K.-based study. There has been evidence that persons in Europe with low-grade dysplasia have higher rates of progression than persons in the U.S. with low-grade dysplasia.”
Dr. Kumar said this may be attributable to differences in the way pathologists practice in the two countries or in endoscopists’ treatment patterns. U.S. guidelines agree that ablation can be used in select persons with low-grade dysplasia, she said, but it’s an area that needs further study.
“Overall, though, this is a really important study of real-time data showing that ablation is impacting cancer rates in a positive way and that in select patients, we can really decrease the risk of invasive cancer by endoscopic eradication therapies,” Dr. Kumar said.
Two coauthors have received grants from Medtronic and Pentax Medical. The other authors have declared no relevant financial relationships. Dr. Kumar reports no relevant financial relationships.
FROM GASTROINTESTINAL ENDOSCOPY
Free now to speak, nine oncologists spill the beans over firing
Last year, nine oncologists filed a lawsuit against the Anne Arundel Medical Center (AAMC), in Annapolis, Md., alleging that the hospital had fired them and had refused to allow them privileges to see their patients.
The oncologists said that the hospital chose profit over the needs of cancer patients, as it slashed oncology care services to cut costs.
The hospital denied any wrongdoing and alleged that the oncologists were not fired but that they had quit because they had been offered a more profitable opportunity.
At that time, the oncologists were not free to respond because of the ongoing litigation. But now that the lawsuit is over and the dust has settled, they are free to speak, and they contacted this news organization to tell their side of the story.
AAMC is a private, not-for-profit corporation that operates a large acute care hospital in Annapolis. It is affiliated with Luminis Health, the parent company of the medical center. Until October 23, 2020, the nine oncologists were employed by the AA Physician Group.
The doctors are Jason Taksey, MD, Benjamin Bridges, MD, Ravin Garg, MD, Adam Goldrich, MD, Carol Tweed, MD, Peter Graze, MD, Stuart Selonick, MD, David Weng, MD, and Jeanine Werner, MD.
They are all “highly respected, board certified oncologists and hematologists, with regional and, for some, national reputations in their medical specialty. The oncologists have had privileges at AAMC for many years and their capability as physicians is unquestioned,” according to the court filing made on behalf of the oncologists.
“Most of us have been in this town for decades,” said Dr. Tweed, who served as the unofficial spokesperson for the group. “Some of us are faculty members at Johns Hopkins, and this hospital’s oncology service was historically defined by our group.”
AAMC has a good reputation for providing high-quality medicine, “which is what brought many of us there in the first place,” Dr. Tweed said in an interview.
Triggered by cost cutting
The situation began when the hospital began cutting services to curtail costs, which directly affected the delivery of oncology care, Dr. Tweed explained. “They were also creating a very toxic and difficult interpersonal work environment, and that made it difficult to do patient care,” she said. “We would go to them and let them know that we were having difficulty delivering optimal patient care because we didn’t have enough staff or the resources we needed for safety — and it got to the point where we were being ignored and our input was no longer welcome.”
Dr. Tweed explained that the administrators announced which patient-care services would be cut without asking for their input as to the safety of those decisions. “Perhaps the most notorious was when they shut down the oncology lab,” she said. “That lab to an oncologist/hematologist is like a scalpel to a surgeon. I need lab results immediately — I need to know if I can give chemotherapy right now, or do I need to hold a dose. The lab is intrinsic to oncology care anywhere.”
There was a continuing cascade of events, and the oncology group mulled over some ideas as to how to provide optimal patient care in this increasingly difficult environment. The decision they reached was to discuss running their own practice with the hospital administrators as a means of making up for the gaps that they were now having to contend with. “As physicians, we do a lot of non-billable work, such as patient education, nighttime rounds for our cancer patients, and so on, and we told them that we would continue doing that,” said Dr. Tweed. “They said that they would talk to us, but they didn’t.”
Within a week of sending their proposal for setting up their own practice, all nine physicians were fired. “Instead of arranging a discussion, we received termination letters,” she explained. “We were terminated without cause.”
As physicians, Dr. Tweed explained that they were by contract obligated to arbitrate. It dragged on for weeks and months, to the tune of hundreds of thousands of dollars in legal fees.
“The only thing we wanted was to be able to practice in this town,” said Dr. Tweed. “And what is important to know is that it was never for money, and that was never our motivation for wanting to form our own practice.”
Dr. Tweed was referring to the hospital’s allegations that the oncologists had left their employment for monetary gain. A statement given to this news organization by the Luminis Health Anne Arundel Medical Center at the time stated that “this dispute started after nine oncologists left their employment to join a for-profit organization. We tried repeatedly to remain aligned with them.”
The oncologists had resigned during the height of the coronavirus pandemic to “pursue lucrative contracts” with a “major pharmaceutical distribution,” according to Todd M. Reinecker, attorney for Luminis Health, as reported by the Capital Gazette (this news organization reached out to Mr. Reinecker at that time but did not receive a response).
This was not the case, Dr. Tweed emphasized. “We took a great financial risk in doing this for patient care. It was pretty disgusting that was in print from the hospital’s lawyer.”
“The doctors anticipated Luminis Health would be unable to recruit new physicians and be forced to continue to use their services,” Mr. Reinecker maintained.
In fact, the medical center hired seven new oncologists to replace them.
Noncompete covenant
In filing their lawsuit, the nine oncologists put before the arbitrator the issue of the enforceability of the noncompete provision in their employment agreement, which prohibited the oncologists from working in the geographic area that includes the hospital. Their position was that the agreement was overly broad and thus unenforceable.
“We sign noncompete restrictive covenant contracts and we’re told that they are nonenforceable, and that’s the general discourse,” said Dr. Tweed. “Some states don’t even allow them. Well, we found out that they are very enforceable.”
The arbitrator eventually determined that three of the oncologists, including Dr. Tweed, had enforceable noncompete contracts.
“During the year or so while this was all going on, I would say that 90% of my patients wanted to stay with me,” said Dr. Tweed. “Patients were looking all over the place for us because, in many cases, the hospital did not tell them where to find us. In fact, they told us that we couldn’t contact the patients — they said it was ‘solicitation of a patient.’ “
In addition, the hospital continued to put more restrictions on the doctors. Six of the nine oncologists were able to continue practicing in Annapolis, and the remaining three will be able to join them in October 2022 when their noncompete contracts expire.
Now that the hospital has seen that there was a new oncology practice in town, Dr. Tweed noted, they changed their bylaws, and they now forbid hospital privileges to every physician in that group.
“The new bylaws do not restrict all private oncologists, just specifically our group, which prevents us from being able to do rounds in the hospital,” said Dr. Tweed. “If I want to see any of my patients, I have to get a visitor badge.”
Dr. Tweed contends that this move was purely for financial and business reasons to keep the oncologists from their patients. This is the primary hospital where their patients would be admitted if they need hospital care. AAMC is the only hospital within a 15-mile radius, and it serves as the regional hospital for the greater Annapolis area and for many Eastern Shore communities, whose hospitals do not offer various specialty services, such as oncology care.
“This was done purely because they were finance focused and not patient care focused,” Dr. Tweed emphasized. “We basically had to bargain with the hospital to let us even transfuse our patients.”
Telemedicine added to the mix
Yet another restriction that surfaced during the arbitration involved telemedicine. Dr. Tweed explained that as soon as the hospital realized that the three oncologists planned to stay in town and that their patients wanted to continue receiving care with them, they put telemedicine on the chopping block.
As if the restrictions and removal of hospital privileges wasn’t enough, the hospital decided to go after telemedicine during arbitration, Dr. Tweed said. If patients lived in any of the restricted ZIP codes, they were forbidden to conduct virtual visits with them.
“This isn’t ethical, but they tried to do everything to keep us from seeing our patients,” she said. “This is patient choice, but they were telling patients that if you live in any of these ZIP codes, you cannot do telemedicine if you choose Carol Tweed as your doctor,” Dr. Tweed said.
Of course, a patient isn’t bound by the arbitration and can see any doctor, but Dr. Tweed explained that the hospital threatened to come after her with a lawsuit.
One of the other physicians, Stuart Selonick, MD, said in an interview that he wasn’t quite sure how the idea of prohibiting telemedicine even came up. “There is little precedence for telemedicine in the U.S.,” he said. “They’ve extended the restrictions to telemedicine, and this is a new legal boundary, and it was new to the judge. But they made it part of the definition of the restrictive covenant. But to fight it would mean another lawsuit,” he added.
A separate lawsuit had previously been filed in an effort to regain hospital privileges, but the decision was made not to continue, owing to the amount of litigation it would involve.
“We can’t spend a lifetime and millions on another legal battle,” said Dr. Tweed. “We don’t have the corporate legal pool that the hospital has, and they know it.”
Patients have written endless letters supporting the doctors, Dr. Tweed said, but to no avail, as the hospital did not change course.
Litigation is now completed, and in about 9 months, the remaining three physicians will be able to rejoin their colleagues and put this behind them as best they can.
“The hospital knows that they harmed patient care for financial gain -- that’s the tagline,” said Tweed.
Approached for a response, Justin McLeod, spokesperson for Luminis Health, said that they are “pleased with the outcome of the case and the resolution agreed to by both sides. This agreement ensures patient access and continuity of care for patients with cancer. These providers have access to their patients’ electronic medical records, can order outpatient services, and attend quarterly cancer committee meetings with other providers.
“Our focus is the future of cancer care for our community. Luminis Health Anne Arundel Medical Center is committed to providing patients with high quality, comprehensive cancer care that is accessible to all,” he added.
A version of this article first appeared on Medscape.com.
Last year, nine oncologists filed a lawsuit against the Anne Arundel Medical Center (AAMC), in Annapolis, Md., alleging that the hospital had fired them and had refused to allow them privileges to see their patients.
The oncologists said that the hospital chose profit over the needs of cancer patients, as it slashed oncology care services to cut costs.
The hospital denied any wrongdoing and alleged that the oncologists were not fired but that they had quit because they had been offered a more profitable opportunity.
At that time, the oncologists were not free to respond because of the ongoing litigation. But now that the lawsuit is over and the dust has settled, they are free to speak, and they contacted this news organization to tell their side of the story.
AAMC is a private, not-for-profit corporation that operates a large acute care hospital in Annapolis. It is affiliated with Luminis Health, the parent company of the medical center. Until October 23, 2020, the nine oncologists were employed by the AA Physician Group.
The doctors are Jason Taksey, MD, Benjamin Bridges, MD, Ravin Garg, MD, Adam Goldrich, MD, Carol Tweed, MD, Peter Graze, MD, Stuart Selonick, MD, David Weng, MD, and Jeanine Werner, MD.
They are all “highly respected, board certified oncologists and hematologists, with regional and, for some, national reputations in their medical specialty. The oncologists have had privileges at AAMC for many years and their capability as physicians is unquestioned,” according to the court filing made on behalf of the oncologists.
“Most of us have been in this town for decades,” said Dr. Tweed, who served as the unofficial spokesperson for the group. “Some of us are faculty members at Johns Hopkins, and this hospital’s oncology service was historically defined by our group.”
AAMC has a good reputation for providing high-quality medicine, “which is what brought many of us there in the first place,” Dr. Tweed said in an interview.
Triggered by cost cutting
The situation began when the hospital began cutting services to curtail costs, which directly affected the delivery of oncology care, Dr. Tweed explained. “They were also creating a very toxic and difficult interpersonal work environment, and that made it difficult to do patient care,” she said. “We would go to them and let them know that we were having difficulty delivering optimal patient care because we didn’t have enough staff or the resources we needed for safety — and it got to the point where we were being ignored and our input was no longer welcome.”
Dr. Tweed explained that the administrators announced which patient-care services would be cut without asking for their input as to the safety of those decisions. “Perhaps the most notorious was when they shut down the oncology lab,” she said. “That lab to an oncologist/hematologist is like a scalpel to a surgeon. I need lab results immediately — I need to know if I can give chemotherapy right now, or do I need to hold a dose. The lab is intrinsic to oncology care anywhere.”
There was a continuing cascade of events, and the oncology group mulled over some ideas as to how to provide optimal patient care in this increasingly difficult environment. The decision they reached was to discuss running their own practice with the hospital administrators as a means of making up for the gaps that they were now having to contend with. “As physicians, we do a lot of non-billable work, such as patient education, nighttime rounds for our cancer patients, and so on, and we told them that we would continue doing that,” said Dr. Tweed. “They said that they would talk to us, but they didn’t.”
Within a week of sending their proposal for setting up their own practice, all nine physicians were fired. “Instead of arranging a discussion, we received termination letters,” she explained. “We were terminated without cause.”
As physicians, Dr. Tweed explained that they were by contract obligated to arbitrate. It dragged on for weeks and months, to the tune of hundreds of thousands of dollars in legal fees.
“The only thing we wanted was to be able to practice in this town,” said Dr. Tweed. “And what is important to know is that it was never for money, and that was never our motivation for wanting to form our own practice.”
Dr. Tweed was referring to the hospital’s allegations that the oncologists had left their employment for monetary gain. A statement given to this news organization by the Luminis Health Anne Arundel Medical Center at the time stated that “this dispute started after nine oncologists left their employment to join a for-profit organization. We tried repeatedly to remain aligned with them.”
The oncologists had resigned during the height of the coronavirus pandemic to “pursue lucrative contracts” with a “major pharmaceutical distribution,” according to Todd M. Reinecker, attorney for Luminis Health, as reported by the Capital Gazette (this news organization reached out to Mr. Reinecker at that time but did not receive a response).
This was not the case, Dr. Tweed emphasized. “We took a great financial risk in doing this for patient care. It was pretty disgusting that was in print from the hospital’s lawyer.”
“The doctors anticipated Luminis Health would be unable to recruit new physicians and be forced to continue to use their services,” Mr. Reinecker maintained.
In fact, the medical center hired seven new oncologists to replace them.
Noncompete covenant
In filing their lawsuit, the nine oncologists put before the arbitrator the issue of the enforceability of the noncompete provision in their employment agreement, which prohibited the oncologists from working in the geographic area that includes the hospital. Their position was that the agreement was overly broad and thus unenforceable.
“We sign noncompete restrictive covenant contracts and we’re told that they are nonenforceable, and that’s the general discourse,” said Dr. Tweed. “Some states don’t even allow them. Well, we found out that they are very enforceable.”
The arbitrator eventually determined that three of the oncologists, including Dr. Tweed, had enforceable noncompete contracts.
“During the year or so while this was all going on, I would say that 90% of my patients wanted to stay with me,” said Dr. Tweed. “Patients were looking all over the place for us because, in many cases, the hospital did not tell them where to find us. In fact, they told us that we couldn’t contact the patients — they said it was ‘solicitation of a patient.’ “
In addition, the hospital continued to put more restrictions on the doctors. Six of the nine oncologists were able to continue practicing in Annapolis, and the remaining three will be able to join them in October 2022 when their noncompete contracts expire.
Now that the hospital has seen that there was a new oncology practice in town, Dr. Tweed noted, they changed their bylaws, and they now forbid hospital privileges to every physician in that group.
“The new bylaws do not restrict all private oncologists, just specifically our group, which prevents us from being able to do rounds in the hospital,” said Dr. Tweed. “If I want to see any of my patients, I have to get a visitor badge.”
Dr. Tweed contends that this move was purely for financial and business reasons to keep the oncologists from their patients. This is the primary hospital where their patients would be admitted if they need hospital care. AAMC is the only hospital within a 15-mile radius, and it serves as the regional hospital for the greater Annapolis area and for many Eastern Shore communities, whose hospitals do not offer various specialty services, such as oncology care.
“This was done purely because they were finance focused and not patient care focused,” Dr. Tweed emphasized. “We basically had to bargain with the hospital to let us even transfuse our patients.”
Telemedicine added to the mix
Yet another restriction that surfaced during the arbitration involved telemedicine. Dr. Tweed explained that as soon as the hospital realized that the three oncologists planned to stay in town and that their patients wanted to continue receiving care with them, they put telemedicine on the chopping block.
As if the restrictions and removal of hospital privileges wasn’t enough, the hospital decided to go after telemedicine during arbitration, Dr. Tweed said. If patients lived in any of the restricted ZIP codes, they were forbidden to conduct virtual visits with them.
“This isn’t ethical, but they tried to do everything to keep us from seeing our patients,” she said. “This is patient choice, but they were telling patients that if you live in any of these ZIP codes, you cannot do telemedicine if you choose Carol Tweed as your doctor,” Dr. Tweed said.
Of course, a patient isn’t bound by the arbitration and can see any doctor, but Dr. Tweed explained that the hospital threatened to come after her with a lawsuit.
One of the other physicians, Stuart Selonick, MD, said in an interview that he wasn’t quite sure how the idea of prohibiting telemedicine even came up. “There is little precedence for telemedicine in the U.S.,” he said. “They’ve extended the restrictions to telemedicine, and this is a new legal boundary, and it was new to the judge. But they made it part of the definition of the restrictive covenant. But to fight it would mean another lawsuit,” he added.
A separate lawsuit had previously been filed in an effort to regain hospital privileges, but the decision was made not to continue, owing to the amount of litigation it would involve.
“We can’t spend a lifetime and millions on another legal battle,” said Dr. Tweed. “We don’t have the corporate legal pool that the hospital has, and they know it.”
Patients have written endless letters supporting the doctors, Dr. Tweed said, but to no avail, as the hospital did not change course.
Litigation is now completed, and in about 9 months, the remaining three physicians will be able to rejoin their colleagues and put this behind them as best they can.
“The hospital knows that they harmed patient care for financial gain -- that’s the tagline,” said Tweed.
Approached for a response, Justin McLeod, spokesperson for Luminis Health, said that they are “pleased with the outcome of the case and the resolution agreed to by both sides. This agreement ensures patient access and continuity of care for patients with cancer. These providers have access to their patients’ electronic medical records, can order outpatient services, and attend quarterly cancer committee meetings with other providers.
“Our focus is the future of cancer care for our community. Luminis Health Anne Arundel Medical Center is committed to providing patients with high quality, comprehensive cancer care that is accessible to all,” he added.
A version of this article first appeared on Medscape.com.
Last year, nine oncologists filed a lawsuit against the Anne Arundel Medical Center (AAMC), in Annapolis, Md., alleging that the hospital had fired them and had refused to allow them privileges to see their patients.
The oncologists said that the hospital chose profit over the needs of cancer patients, as it slashed oncology care services to cut costs.
The hospital denied any wrongdoing and alleged that the oncologists were not fired but that they had quit because they had been offered a more profitable opportunity.
At that time, the oncologists were not free to respond because of the ongoing litigation. But now that the lawsuit is over and the dust has settled, they are free to speak, and they contacted this news organization to tell their side of the story.
AAMC is a private, not-for-profit corporation that operates a large acute care hospital in Annapolis. It is affiliated with Luminis Health, the parent company of the medical center. Until October 23, 2020, the nine oncologists were employed by the AA Physician Group.
The doctors are Jason Taksey, MD, Benjamin Bridges, MD, Ravin Garg, MD, Adam Goldrich, MD, Carol Tweed, MD, Peter Graze, MD, Stuart Selonick, MD, David Weng, MD, and Jeanine Werner, MD.
They are all “highly respected, board certified oncologists and hematologists, with regional and, for some, national reputations in their medical specialty. The oncologists have had privileges at AAMC for many years and their capability as physicians is unquestioned,” according to the court filing made on behalf of the oncologists.
“Most of us have been in this town for decades,” said Dr. Tweed, who served as the unofficial spokesperson for the group. “Some of us are faculty members at Johns Hopkins, and this hospital’s oncology service was historically defined by our group.”
AAMC has a good reputation for providing high-quality medicine, “which is what brought many of us there in the first place,” Dr. Tweed said in an interview.
Triggered by cost cutting
The situation began when the hospital began cutting services to curtail costs, which directly affected the delivery of oncology care, Dr. Tweed explained. “They were also creating a very toxic and difficult interpersonal work environment, and that made it difficult to do patient care,” she said. “We would go to them and let them know that we were having difficulty delivering optimal patient care because we didn’t have enough staff or the resources we needed for safety — and it got to the point where we were being ignored and our input was no longer welcome.”
Dr. Tweed explained that the administrators announced which patient-care services would be cut without asking for their input as to the safety of those decisions. “Perhaps the most notorious was when they shut down the oncology lab,” she said. “That lab to an oncologist/hematologist is like a scalpel to a surgeon. I need lab results immediately — I need to know if I can give chemotherapy right now, or do I need to hold a dose. The lab is intrinsic to oncology care anywhere.”
There was a continuing cascade of events, and the oncology group mulled over some ideas as to how to provide optimal patient care in this increasingly difficult environment. The decision they reached was to discuss running their own practice with the hospital administrators as a means of making up for the gaps that they were now having to contend with. “As physicians, we do a lot of non-billable work, such as patient education, nighttime rounds for our cancer patients, and so on, and we told them that we would continue doing that,” said Dr. Tweed. “They said that they would talk to us, but they didn’t.”
Within a week of sending their proposal for setting up their own practice, all nine physicians were fired. “Instead of arranging a discussion, we received termination letters,” she explained. “We were terminated without cause.”
As physicians, Dr. Tweed explained that they were by contract obligated to arbitrate. It dragged on for weeks and months, to the tune of hundreds of thousands of dollars in legal fees.
“The only thing we wanted was to be able to practice in this town,” said Dr. Tweed. “And what is important to know is that it was never for money, and that was never our motivation for wanting to form our own practice.”
Dr. Tweed was referring to the hospital’s allegations that the oncologists had left their employment for monetary gain. A statement given to this news organization by the Luminis Health Anne Arundel Medical Center at the time stated that “this dispute started after nine oncologists left their employment to join a for-profit organization. We tried repeatedly to remain aligned with them.”
The oncologists had resigned during the height of the coronavirus pandemic to “pursue lucrative contracts” with a “major pharmaceutical distribution,” according to Todd M. Reinecker, attorney for Luminis Health, as reported by the Capital Gazette (this news organization reached out to Mr. Reinecker at that time but did not receive a response).
This was not the case, Dr. Tweed emphasized. “We took a great financial risk in doing this for patient care. It was pretty disgusting that was in print from the hospital’s lawyer.”
“The doctors anticipated Luminis Health would be unable to recruit new physicians and be forced to continue to use their services,” Mr. Reinecker maintained.
In fact, the medical center hired seven new oncologists to replace them.
Noncompete covenant
In filing their lawsuit, the nine oncologists put before the arbitrator the issue of the enforceability of the noncompete provision in their employment agreement, which prohibited the oncologists from working in the geographic area that includes the hospital. Their position was that the agreement was overly broad and thus unenforceable.
“We sign noncompete restrictive covenant contracts and we’re told that they are nonenforceable, and that’s the general discourse,” said Dr. Tweed. “Some states don’t even allow them. Well, we found out that they are very enforceable.”
The arbitrator eventually determined that three of the oncologists, including Dr. Tweed, had enforceable noncompete contracts.
“During the year or so while this was all going on, I would say that 90% of my patients wanted to stay with me,” said Dr. Tweed. “Patients were looking all over the place for us because, in many cases, the hospital did not tell them where to find us. In fact, they told us that we couldn’t contact the patients — they said it was ‘solicitation of a patient.’ “
In addition, the hospital continued to put more restrictions on the doctors. Six of the nine oncologists were able to continue practicing in Annapolis, and the remaining three will be able to join them in October 2022 when their noncompete contracts expire.
Now that the hospital has seen that there was a new oncology practice in town, Dr. Tweed noted, they changed their bylaws, and they now forbid hospital privileges to every physician in that group.
“The new bylaws do not restrict all private oncologists, just specifically our group, which prevents us from being able to do rounds in the hospital,” said Dr. Tweed. “If I want to see any of my patients, I have to get a visitor badge.”
Dr. Tweed contends that this move was purely for financial and business reasons to keep the oncologists from their patients. This is the primary hospital where their patients would be admitted if they need hospital care. AAMC is the only hospital within a 15-mile radius, and it serves as the regional hospital for the greater Annapolis area and for many Eastern Shore communities, whose hospitals do not offer various specialty services, such as oncology care.
“This was done purely because they were finance focused and not patient care focused,” Dr. Tweed emphasized. “We basically had to bargain with the hospital to let us even transfuse our patients.”
Telemedicine added to the mix
Yet another restriction that surfaced during the arbitration involved telemedicine. Dr. Tweed explained that as soon as the hospital realized that the three oncologists planned to stay in town and that their patients wanted to continue receiving care with them, they put telemedicine on the chopping block.
As if the restrictions and removal of hospital privileges wasn’t enough, the hospital decided to go after telemedicine during arbitration, Dr. Tweed said. If patients lived in any of the restricted ZIP codes, they were forbidden to conduct virtual visits with them.
“This isn’t ethical, but they tried to do everything to keep us from seeing our patients,” she said. “This is patient choice, but they were telling patients that if you live in any of these ZIP codes, you cannot do telemedicine if you choose Carol Tweed as your doctor,” Dr. Tweed said.
Of course, a patient isn’t bound by the arbitration and can see any doctor, but Dr. Tweed explained that the hospital threatened to come after her with a lawsuit.
One of the other physicians, Stuart Selonick, MD, said in an interview that he wasn’t quite sure how the idea of prohibiting telemedicine even came up. “There is little precedence for telemedicine in the U.S.,” he said. “They’ve extended the restrictions to telemedicine, and this is a new legal boundary, and it was new to the judge. But they made it part of the definition of the restrictive covenant. But to fight it would mean another lawsuit,” he added.
A separate lawsuit had previously been filed in an effort to regain hospital privileges, but the decision was made not to continue, owing to the amount of litigation it would involve.
“We can’t spend a lifetime and millions on another legal battle,” said Dr. Tweed. “We don’t have the corporate legal pool that the hospital has, and they know it.”
Patients have written endless letters supporting the doctors, Dr. Tweed said, but to no avail, as the hospital did not change course.
Litigation is now completed, and in about 9 months, the remaining three physicians will be able to rejoin their colleagues and put this behind them as best they can.
“The hospital knows that they harmed patient care for financial gain -- that’s the tagline,” said Tweed.
Approached for a response, Justin McLeod, spokesperson for Luminis Health, said that they are “pleased with the outcome of the case and the resolution agreed to by both sides. This agreement ensures patient access and continuity of care for patients with cancer. These providers have access to their patients’ electronic medical records, can order outpatient services, and attend quarterly cancer committee meetings with other providers.
“Our focus is the future of cancer care for our community. Luminis Health Anne Arundel Medical Center is committed to providing patients with high quality, comprehensive cancer care that is accessible to all,” he added.
A version of this article first appeared on Medscape.com.