User login
Aggressive Crystalloid Resuscitation Ups Morbidity
NAPLES, FLA. - A rising crystalloid-to–packed red blood cell ratio increases the risk of morbidity in patients requiring massive transfusion, with high ratios of more than 1.5:1 showing the most dramatic increase in risk.
The finding is based on a secondary analysis of 452 blunt trauma patients who were transfused with a median of 17 L of crystalloid (C) resuscitation and a median of 16 units of packed red blood cells (PRBC) within the first 24 hours of admission. Overall mortality and multiple organ failure rates for the multicenter prospective cohort were 21% and 65%, respectively. Their median Injury Severity Score (ISS) was 34.
The secondary analysis divided the cohort at its median C:PRBC ratio, with 225 patients defined as having a high C:PRBC ratio and 227 patients as having a low C:PRBC ratio.
Logistic regression analysis revealed that the 24-hour C:PRBC ratio was significantly associated with a greater independent risk of multiple organ failure (MOF), acute respiratory distress syndrome (ARDS), and abdominal compartment syndrome (ACS). There was no significant association with mortality or nosocomial infection. Dr. Matthew D. Neal, a general surgery resident at the University of Pittsburgh, presented the study results at the annual meeting of the Eastern Association for the Surgery of Trauma.
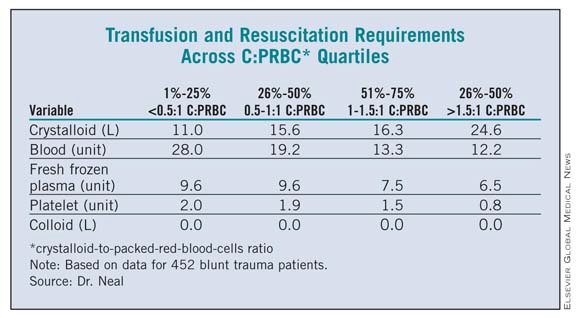
The researchers then conducted a dose-response analysis, dividing the cohort into four quartiles based on C:PRBC ratios. (See box below.) Interestingly, patients in the highest quartile (those with a C:PRBC ratio greater than 1.5:1) received by far the most crystalloid and the least amount of blood and blood products, said Dr. Neal. They also had a significant, more-than-twofold-higher independent risk of MOF (odds ratio, 2.6) and ARDS (OR, 2.5) and a nearly a fourfold higher risk of ACS (OR, 3.6).
Appropriate ratios of blood and blood products in massive transfusion protocols have been the focus of much research, but crystalloid has yet to be studied in a ratio-based manner, despite its being a mainstay of resuscitation since the 1950s, Dr. Neal said. There are recommendations in the hemostatic resuscitation literature to minimize its use because of the cellular and inflammatory disturbances associated with crystalloid infusion in the setting of trauma and hemorrhagic shock, but no specific guidelines exist.
Crystalloid use decreased over the study period of 2003-2008, according to an additional analysis that divided the cohort at its median into early and late time points. The mean total volume of crystalloid administered was significantly lower in the late group (12 L) than in the early group (16 L), Dr. Neal said. Patients treated with the high volumes of crystalloid for early resuscitation had a dramatically increased risk of ARDS and ACS – but not MOF – despite having lower ISS scores.
"Further high-level research is needed to see if crystalloid-to–packed red blood cell ratio should be incorporated into massive transfusion protocols," he said.
Invited discussant Dr. Jeffrey Kerby of the University of Alabama at Birmingham said that the analysis is based on the assumption that resuscitation ratios are fixed and stable; yet, in fact, they are dynamic and can change from hour to hour. Thus, patients could shift back and forth between C:PRBC groups, which could have a significant impact on outcomes. By excluding patients who died within the first 24 hours, he added, the analysis could have excluded a large number of patients and the genuine possibility of the findings.
Nonetheless, Dr. Kerby said he enjoyed the paper and asked what fluid the authors would recommend for use during the initial 24 hours.
Dr. Neal responded, "I think that we’re all still stuck with crystalloid for better or for worse until something better emerges, but I think our new literature is guiding us as to what the right outcomes are to measure – intravascular depletion and hypotension."
Dr. Neal’s paper won the 2011 Raymond H. Alexander, M.D., Resident Paper Competition of the EAST Foundation.
Dr. Neal disclosed a Glue Grant from the Inflammation and the Host Response to Injury research program. Dr. Kerby reported no conflicts of interest.
NAPLES, FLA. - A rising crystalloid-to–packed red blood cell ratio increases the risk of morbidity in patients requiring massive transfusion, with high ratios of more than 1.5:1 showing the most dramatic increase in risk.
The finding is based on a secondary analysis of 452 blunt trauma patients who were transfused with a median of 17 L of crystalloid (C) resuscitation and a median of 16 units of packed red blood cells (PRBC) within the first 24 hours of admission. Overall mortality and multiple organ failure rates for the multicenter prospective cohort were 21% and 65%, respectively. Their median Injury Severity Score (ISS) was 34.
The secondary analysis divided the cohort at its median C:PRBC ratio, with 225 patients defined as having a high C:PRBC ratio and 227 patients as having a low C:PRBC ratio.
Logistic regression analysis revealed that the 24-hour C:PRBC ratio was significantly associated with a greater independent risk of multiple organ failure (MOF), acute respiratory distress syndrome (ARDS), and abdominal compartment syndrome (ACS). There was no significant association with mortality or nosocomial infection. Dr. Matthew D. Neal, a general surgery resident at the University of Pittsburgh, presented the study results at the annual meeting of the Eastern Association for the Surgery of Trauma.
The researchers then conducted a dose-response analysis, dividing the cohort into four quartiles based on C:PRBC ratios. (See box below.) Interestingly, patients in the highest quartile (those with a C:PRBC ratio greater than 1.5:1) received by far the most crystalloid and the least amount of blood and blood products, said Dr. Neal. They also had a significant, more-than-twofold-higher independent risk of MOF (odds ratio, 2.6) and ARDS (OR, 2.5) and a nearly a fourfold higher risk of ACS (OR, 3.6).
Appropriate ratios of blood and blood products in massive transfusion protocols have been the focus of much research, but crystalloid has yet to be studied in a ratio-based manner, despite its being a mainstay of resuscitation since the 1950s, Dr. Neal said. There are recommendations in the hemostatic resuscitation literature to minimize its use because of the cellular and inflammatory disturbances associated with crystalloid infusion in the setting of trauma and hemorrhagic shock, but no specific guidelines exist.
Crystalloid use decreased over the study period of 2003-2008, according to an additional analysis that divided the cohort at its median into early and late time points. The mean total volume of crystalloid administered was significantly lower in the late group (12 L) than in the early group (16 L), Dr. Neal said. Patients treated with the high volumes of crystalloid for early resuscitation had a dramatically increased risk of ARDS and ACS – but not MOF – despite having lower ISS scores.
"Further high-level research is needed to see if crystalloid-to–packed red blood cell ratio should be incorporated into massive transfusion protocols," he said.
Invited discussant Dr. Jeffrey Kerby of the University of Alabama at Birmingham said that the analysis is based on the assumption that resuscitation ratios are fixed and stable; yet, in fact, they are dynamic and can change from hour to hour. Thus, patients could shift back and forth between C:PRBC groups, which could have a significant impact on outcomes. By excluding patients who died within the first 24 hours, he added, the analysis could have excluded a large number of patients and the genuine possibility of the findings.
Nonetheless, Dr. Kerby said he enjoyed the paper and asked what fluid the authors would recommend for use during the initial 24 hours.
Dr. Neal responded, "I think that we’re all still stuck with crystalloid for better or for worse until something better emerges, but I think our new literature is guiding us as to what the right outcomes are to measure – intravascular depletion and hypotension."
Dr. Neal’s paper won the 2011 Raymond H. Alexander, M.D., Resident Paper Competition of the EAST Foundation.
Dr. Neal disclosed a Glue Grant from the Inflammation and the Host Response to Injury research program. Dr. Kerby reported no conflicts of interest.
NAPLES, FLA. - A rising crystalloid-to–packed red blood cell ratio increases the risk of morbidity in patients requiring massive transfusion, with high ratios of more than 1.5:1 showing the most dramatic increase in risk.
The finding is based on a secondary analysis of 452 blunt trauma patients who were transfused with a median of 17 L of crystalloid (C) resuscitation and a median of 16 units of packed red blood cells (PRBC) within the first 24 hours of admission. Overall mortality and multiple organ failure rates for the multicenter prospective cohort were 21% and 65%, respectively. Their median Injury Severity Score (ISS) was 34.
The secondary analysis divided the cohort at its median C:PRBC ratio, with 225 patients defined as having a high C:PRBC ratio and 227 patients as having a low C:PRBC ratio.
Logistic regression analysis revealed that the 24-hour C:PRBC ratio was significantly associated with a greater independent risk of multiple organ failure (MOF), acute respiratory distress syndrome (ARDS), and abdominal compartment syndrome (ACS). There was no significant association with mortality or nosocomial infection. Dr. Matthew D. Neal, a general surgery resident at the University of Pittsburgh, presented the study results at the annual meeting of the Eastern Association for the Surgery of Trauma.
The researchers then conducted a dose-response analysis, dividing the cohort into four quartiles based on C:PRBC ratios. (See box below.) Interestingly, patients in the highest quartile (those with a C:PRBC ratio greater than 1.5:1) received by far the most crystalloid and the least amount of blood and blood products, said Dr. Neal. They also had a significant, more-than-twofold-higher independent risk of MOF (odds ratio, 2.6) and ARDS (OR, 2.5) and a nearly a fourfold higher risk of ACS (OR, 3.6).
Appropriate ratios of blood and blood products in massive transfusion protocols have been the focus of much research, but crystalloid has yet to be studied in a ratio-based manner, despite its being a mainstay of resuscitation since the 1950s, Dr. Neal said. There are recommendations in the hemostatic resuscitation literature to minimize its use because of the cellular and inflammatory disturbances associated with crystalloid infusion in the setting of trauma and hemorrhagic shock, but no specific guidelines exist.
Crystalloid use decreased over the study period of 2003-2008, according to an additional analysis that divided the cohort at its median into early and late time points. The mean total volume of crystalloid administered was significantly lower in the late group (12 L) than in the early group (16 L), Dr. Neal said. Patients treated with the high volumes of crystalloid for early resuscitation had a dramatically increased risk of ARDS and ACS – but not MOF – despite having lower ISS scores.
"Further high-level research is needed to see if crystalloid-to–packed red blood cell ratio should be incorporated into massive transfusion protocols," he said.
Invited discussant Dr. Jeffrey Kerby of the University of Alabama at Birmingham said that the analysis is based on the assumption that resuscitation ratios are fixed and stable; yet, in fact, they are dynamic and can change from hour to hour. Thus, patients could shift back and forth between C:PRBC groups, which could have a significant impact on outcomes. By excluding patients who died within the first 24 hours, he added, the analysis could have excluded a large number of patients and the genuine possibility of the findings.
Nonetheless, Dr. Kerby said he enjoyed the paper and asked what fluid the authors would recommend for use during the initial 24 hours.
Dr. Neal responded, "I think that we’re all still stuck with crystalloid for better or for worse until something better emerges, but I think our new literature is guiding us as to what the right outcomes are to measure – intravascular depletion and hypotension."
Dr. Neal’s paper won the 2011 Raymond H. Alexander, M.D., Resident Paper Competition of the EAST Foundation.
Dr. Neal disclosed a Glue Grant from the Inflammation and the Host Response to Injury research program. Dr. Kerby reported no conflicts of interest.
Prophylactic Levetiracetam Fails to Reduce Post-TBI Seizures
NAPLES, FLA. – Early seizure rates after traumatic brain injury were nearly identical whether patients did or did not receive levetiracetam prophylaxis in a retrospective analysis of 5,551 patients.
The seizure rate during the first 7 days post injury was 1.9% among 208 patients given prophylactic levetiracetam (Keppra) vs. 2% among the 5,343 patients who were not (P = .92).
Seizure rates with and without prophylactic phenytoin (Dilantin) were 4.5% vs. 1.8% (P = .053), and 0% vs. 2% with and without prophylactic fosphenytoin (Cerebyx) (P = .75), Dr. Terence O’Keeffe and his colleagues reported in a poster at the Eastern Association for the Surgery of Trauma.
Although a 7-day course of phenytoin is the current standard of care, the authors note that neurosurgeons are substituting levetiracetam, even though data are lacking to show the efficacy of this approach. Levetiracetam is an attractive alternative because, unlike phenytoin, it has predictable pharmacokinetics, does not require serum drug monitoring to ensure that therapeutic levels are achieved and has a low propensity for drug interactions.
The 2010 updated Brain Trauma Foundation guidelines on the management of severe traumatic brain injury recommend anticonvulsants to reduce the incidence of posttraumatic seizures within 7 days of injury, but not thereafter.
The seizure rate in the entire cohort was 0.7%, and the median time to seizure post injury was 3 days. Seven patients had seizures in the emergency department (ED). Seizures were 25 times more likely in patients with severe TBI than in those with mild TBI (2% vs. 0.08%, odds ratio 25.6), according to Dr. O’Keeffe, director of the surgical and trauma ICU at the University of Arizona, Tucson, and his colleagues.
When the 208 levetiracetam patients were propensity matched 1:1 using an 11-variable algorithm with 208 patients who did not receive levetiracetam, seizure rates remained statistically similar at 1.9% with levetiracetam vs. 3.4% without.
"Keppra is ineffective for seizure prophylaxis in a trauma population with a low incidence of post-TBI seizures," the authors wrote.
Based on their data, the authors questioned the need for seizure prophylaxis following TBI, as the seizure rate was so much lower than had been previously reported.
"The incidence is so low in mild TBI as to not merit treatment in my mind," Dr. O’Keeffe said in an interview. "I think we should develop protocols that target high-risk populations, for example penetrating TBI, and that the vast majority of patients need no prophylaxis."
The first study to evaluate levetiracetam for seizure prophylaxis in severe TBI found no difference in seizure rates among 32 patients given levetiracetam and a historical cohort of 41 patients given phenytoin, although levetiracetam was associated with an increased seizure tendency on electroencephalographic (EEG) analysis (Neurosurg. Focus 2008;25:E3). The implication of the EEG finding is unclear, and the study has been criticized for using only 1 hour of EEG monitoring.
The first randomized trial of the two drugs published last year in 52 patients with severe TBI (89%) or subarachnoid hemorrhage reported that patients receiving levetiracetam experienced better long-term outcomes than did those on phenytoin and identified no differences between groups in seizure occurrence during continuous EEG monitoring for the initial 72 hours (Neurocrit. Care 2010;12:165-72).
The current analysis included all patients treated for TBI from January 2007 to December 2009 at a level I, urban trauma center. Patients were stratified by injury severity. Of the 5,551 patients, 3,756 had a mild TBI, defined by a Head Abbreviated Injury Scale (AIS) score of 1 or 2, and 1,795 had severe TBI, defined by a Head AIS score of 3-5.
In multivariate regression analysis, only head AIS and ED heart rate were predictive of seizure. In the severe TBI group, the type of injury (that is, skull fracture, subdural, etc.) was not predictive of seizures. As for why the seizure rate was higher with prophylactic phenytoin than without, Dr. O’Keeffe said it may be the patients receiving the drug as treatment rather than as prophylaxis.
Dr. O’Keeffe and his colleagues acknowledge that propensity scores cannot remove all selection bias, that seizure data were obtained from patient chart/registry review, and that there was no standard prophylaxis over the study period. Possible future areas of study are 2010 data with standardized prophylaxis regimens and a multicenter trial looking at the Extended Glasgow Outcome Scale benefit of levetiracetam vs. placebo.
Balancing the Costs
Phenytoin is more cost-effective in reducing the risk of early posttraumatic seizures than is levetiracetam at all reasonable prices.
"In fact, for levetiracetam to reach cost effectiveness vs. phenytoin, this newer antiepileptic would have to prevent 100% of posttrauma seizures and be less than $400 for a week of therapy," Dr. Bryan Cotton and his colleagues reported in a separate cost-utility analysis at the same meeting.
Based on current data, the cost of a 7-day course of phenytoin (Dilantin) was $37.50 vs. $480 for a 7-day course of levetiracetam (Keppra).
The cost-utility analysis was conducted from the perspective of a university, level 1 urban trauma center, assuming that all patients with traumatic brain injury survived to receive 7 days of either agent to prevent posttraumatic seizures.
Base case assumptions were that all phenytoin patients would receive 1 g fosphenytoin (Cerebyx) intravenous load on day 0 plus 3 days of 100 mg phenytoin every 8 hours and that all levetiracetam patients would receive 500-mg load IV on day 0, followed by 7 days of 500 mg every 12 hours IV. Phenytoin patients would have a free phenytoin level drawn on day 3, with therapeutic patients receiving 100 mg phenytoin every 8 hours from post injury days 4 through 7 and subtherapeutic patients receiving an increased dose of phenytoin 200 mg every 8 hours from days 4 through 7.
The authors pointed out that they chose the smallest, least-expensive intravenous dosing for the levetiracetam arm and the most-expensive intravenous dosing for the phenytoin arm.
Quality-adjusted life years (QALY) were 23.6 for phenytoin and 23.2 for levetiracetam. As a result, the cost/effectiveness ratios were $1.58/QALY for phenytoin and $20.72/QALY for levetiracetam, according to Dr. Cotton, with the University of Texas at Houston, and his colleagues.
Dr. Terence O’Keeffe and his colleagues reported no conflicts of interest.
Dr. Cotton disclosed grant/research support from Haemonetics Corp. for a multicenter trial of rapid thrombelastography.
NAPLES, FLA. – Early seizure rates after traumatic brain injury were nearly identical whether patients did or did not receive levetiracetam prophylaxis in a retrospective analysis of 5,551 patients.
The seizure rate during the first 7 days post injury was 1.9% among 208 patients given prophylactic levetiracetam (Keppra) vs. 2% among the 5,343 patients who were not (P = .92).
Seizure rates with and without prophylactic phenytoin (Dilantin) were 4.5% vs. 1.8% (P = .053), and 0% vs. 2% with and without prophylactic fosphenytoin (Cerebyx) (P = .75), Dr. Terence O’Keeffe and his colleagues reported in a poster at the Eastern Association for the Surgery of Trauma.
Although a 7-day course of phenytoin is the current standard of care, the authors note that neurosurgeons are substituting levetiracetam, even though data are lacking to show the efficacy of this approach. Levetiracetam is an attractive alternative because, unlike phenytoin, it has predictable pharmacokinetics, does not require serum drug monitoring to ensure that therapeutic levels are achieved and has a low propensity for drug interactions.
The 2010 updated Brain Trauma Foundation guidelines on the management of severe traumatic brain injury recommend anticonvulsants to reduce the incidence of posttraumatic seizures within 7 days of injury, but not thereafter.
The seizure rate in the entire cohort was 0.7%, and the median time to seizure post injury was 3 days. Seven patients had seizures in the emergency department (ED). Seizures were 25 times more likely in patients with severe TBI than in those with mild TBI (2% vs. 0.08%, odds ratio 25.6), according to Dr. O’Keeffe, director of the surgical and trauma ICU at the University of Arizona, Tucson, and his colleagues.
When the 208 levetiracetam patients were propensity matched 1:1 using an 11-variable algorithm with 208 patients who did not receive levetiracetam, seizure rates remained statistically similar at 1.9% with levetiracetam vs. 3.4% without.
"Keppra is ineffective for seizure prophylaxis in a trauma population with a low incidence of post-TBI seizures," the authors wrote.
Based on their data, the authors questioned the need for seizure prophylaxis following TBI, as the seizure rate was so much lower than had been previously reported.
"The incidence is so low in mild TBI as to not merit treatment in my mind," Dr. O’Keeffe said in an interview. "I think we should develop protocols that target high-risk populations, for example penetrating TBI, and that the vast majority of patients need no prophylaxis."
The first study to evaluate levetiracetam for seizure prophylaxis in severe TBI found no difference in seizure rates among 32 patients given levetiracetam and a historical cohort of 41 patients given phenytoin, although levetiracetam was associated with an increased seizure tendency on electroencephalographic (EEG) analysis (Neurosurg. Focus 2008;25:E3). The implication of the EEG finding is unclear, and the study has been criticized for using only 1 hour of EEG monitoring.
The first randomized trial of the two drugs published last year in 52 patients with severe TBI (89%) or subarachnoid hemorrhage reported that patients receiving levetiracetam experienced better long-term outcomes than did those on phenytoin and identified no differences between groups in seizure occurrence during continuous EEG monitoring for the initial 72 hours (Neurocrit. Care 2010;12:165-72).
The current analysis included all patients treated for TBI from January 2007 to December 2009 at a level I, urban trauma center. Patients were stratified by injury severity. Of the 5,551 patients, 3,756 had a mild TBI, defined by a Head Abbreviated Injury Scale (AIS) score of 1 or 2, and 1,795 had severe TBI, defined by a Head AIS score of 3-5.
In multivariate regression analysis, only head AIS and ED heart rate were predictive of seizure. In the severe TBI group, the type of injury (that is, skull fracture, subdural, etc.) was not predictive of seizures. As for why the seizure rate was higher with prophylactic phenytoin than without, Dr. O’Keeffe said it may be the patients receiving the drug as treatment rather than as prophylaxis.
Dr. O’Keeffe and his colleagues acknowledge that propensity scores cannot remove all selection bias, that seizure data were obtained from patient chart/registry review, and that there was no standard prophylaxis over the study period. Possible future areas of study are 2010 data with standardized prophylaxis regimens and a multicenter trial looking at the Extended Glasgow Outcome Scale benefit of levetiracetam vs. placebo.
Balancing the Costs
Phenytoin is more cost-effective in reducing the risk of early posttraumatic seizures than is levetiracetam at all reasonable prices.
"In fact, for levetiracetam to reach cost effectiveness vs. phenytoin, this newer antiepileptic would have to prevent 100% of posttrauma seizures and be less than $400 for a week of therapy," Dr. Bryan Cotton and his colleagues reported in a separate cost-utility analysis at the same meeting.
Based on current data, the cost of a 7-day course of phenytoin (Dilantin) was $37.50 vs. $480 for a 7-day course of levetiracetam (Keppra).
The cost-utility analysis was conducted from the perspective of a university, level 1 urban trauma center, assuming that all patients with traumatic brain injury survived to receive 7 days of either agent to prevent posttraumatic seizures.
Base case assumptions were that all phenytoin patients would receive 1 g fosphenytoin (Cerebyx) intravenous load on day 0 plus 3 days of 100 mg phenytoin every 8 hours and that all levetiracetam patients would receive 500-mg load IV on day 0, followed by 7 days of 500 mg every 12 hours IV. Phenytoin patients would have a free phenytoin level drawn on day 3, with therapeutic patients receiving 100 mg phenytoin every 8 hours from post injury days 4 through 7 and subtherapeutic patients receiving an increased dose of phenytoin 200 mg every 8 hours from days 4 through 7.
The authors pointed out that they chose the smallest, least-expensive intravenous dosing for the levetiracetam arm and the most-expensive intravenous dosing for the phenytoin arm.
Quality-adjusted life years (QALY) were 23.6 for phenytoin and 23.2 for levetiracetam. As a result, the cost/effectiveness ratios were $1.58/QALY for phenytoin and $20.72/QALY for levetiracetam, according to Dr. Cotton, with the University of Texas at Houston, and his colleagues.
Dr. Terence O’Keeffe and his colleagues reported no conflicts of interest.
Dr. Cotton disclosed grant/research support from Haemonetics Corp. for a multicenter trial of rapid thrombelastography.
NAPLES, FLA. – Early seizure rates after traumatic brain injury were nearly identical whether patients did or did not receive levetiracetam prophylaxis in a retrospective analysis of 5,551 patients.
The seizure rate during the first 7 days post injury was 1.9% among 208 patients given prophylactic levetiracetam (Keppra) vs. 2% among the 5,343 patients who were not (P = .92).
Seizure rates with and without prophylactic phenytoin (Dilantin) were 4.5% vs. 1.8% (P = .053), and 0% vs. 2% with and without prophylactic fosphenytoin (Cerebyx) (P = .75), Dr. Terence O’Keeffe and his colleagues reported in a poster at the Eastern Association for the Surgery of Trauma.
Although a 7-day course of phenytoin is the current standard of care, the authors note that neurosurgeons are substituting levetiracetam, even though data are lacking to show the efficacy of this approach. Levetiracetam is an attractive alternative because, unlike phenytoin, it has predictable pharmacokinetics, does not require serum drug monitoring to ensure that therapeutic levels are achieved and has a low propensity for drug interactions.
The 2010 updated Brain Trauma Foundation guidelines on the management of severe traumatic brain injury recommend anticonvulsants to reduce the incidence of posttraumatic seizures within 7 days of injury, but not thereafter.
The seizure rate in the entire cohort was 0.7%, and the median time to seizure post injury was 3 days. Seven patients had seizures in the emergency department (ED). Seizures were 25 times more likely in patients with severe TBI than in those with mild TBI (2% vs. 0.08%, odds ratio 25.6), according to Dr. O’Keeffe, director of the surgical and trauma ICU at the University of Arizona, Tucson, and his colleagues.
When the 208 levetiracetam patients were propensity matched 1:1 using an 11-variable algorithm with 208 patients who did not receive levetiracetam, seizure rates remained statistically similar at 1.9% with levetiracetam vs. 3.4% without.
"Keppra is ineffective for seizure prophylaxis in a trauma population with a low incidence of post-TBI seizures," the authors wrote.
Based on their data, the authors questioned the need for seizure prophylaxis following TBI, as the seizure rate was so much lower than had been previously reported.
"The incidence is so low in mild TBI as to not merit treatment in my mind," Dr. O’Keeffe said in an interview. "I think we should develop protocols that target high-risk populations, for example penetrating TBI, and that the vast majority of patients need no prophylaxis."
The first study to evaluate levetiracetam for seizure prophylaxis in severe TBI found no difference in seizure rates among 32 patients given levetiracetam and a historical cohort of 41 patients given phenytoin, although levetiracetam was associated with an increased seizure tendency on electroencephalographic (EEG) analysis (Neurosurg. Focus 2008;25:E3). The implication of the EEG finding is unclear, and the study has been criticized for using only 1 hour of EEG monitoring.
The first randomized trial of the two drugs published last year in 52 patients with severe TBI (89%) or subarachnoid hemorrhage reported that patients receiving levetiracetam experienced better long-term outcomes than did those on phenytoin and identified no differences between groups in seizure occurrence during continuous EEG monitoring for the initial 72 hours (Neurocrit. Care 2010;12:165-72).
The current analysis included all patients treated for TBI from January 2007 to December 2009 at a level I, urban trauma center. Patients were stratified by injury severity. Of the 5,551 patients, 3,756 had a mild TBI, defined by a Head Abbreviated Injury Scale (AIS) score of 1 or 2, and 1,795 had severe TBI, defined by a Head AIS score of 3-5.
In multivariate regression analysis, only head AIS and ED heart rate were predictive of seizure. In the severe TBI group, the type of injury (that is, skull fracture, subdural, etc.) was not predictive of seizures. As for why the seizure rate was higher with prophylactic phenytoin than without, Dr. O’Keeffe said it may be the patients receiving the drug as treatment rather than as prophylaxis.
Dr. O’Keeffe and his colleagues acknowledge that propensity scores cannot remove all selection bias, that seizure data were obtained from patient chart/registry review, and that there was no standard prophylaxis over the study period. Possible future areas of study are 2010 data with standardized prophylaxis regimens and a multicenter trial looking at the Extended Glasgow Outcome Scale benefit of levetiracetam vs. placebo.
Balancing the Costs
Phenytoin is more cost-effective in reducing the risk of early posttraumatic seizures than is levetiracetam at all reasonable prices.
"In fact, for levetiracetam to reach cost effectiveness vs. phenytoin, this newer antiepileptic would have to prevent 100% of posttrauma seizures and be less than $400 for a week of therapy," Dr. Bryan Cotton and his colleagues reported in a separate cost-utility analysis at the same meeting.
Based on current data, the cost of a 7-day course of phenytoin (Dilantin) was $37.50 vs. $480 for a 7-day course of levetiracetam (Keppra).
The cost-utility analysis was conducted from the perspective of a university, level 1 urban trauma center, assuming that all patients with traumatic brain injury survived to receive 7 days of either agent to prevent posttraumatic seizures.
Base case assumptions were that all phenytoin patients would receive 1 g fosphenytoin (Cerebyx) intravenous load on day 0 plus 3 days of 100 mg phenytoin every 8 hours and that all levetiracetam patients would receive 500-mg load IV on day 0, followed by 7 days of 500 mg every 12 hours IV. Phenytoin patients would have a free phenytoin level drawn on day 3, with therapeutic patients receiving 100 mg phenytoin every 8 hours from post injury days 4 through 7 and subtherapeutic patients receiving an increased dose of phenytoin 200 mg every 8 hours from days 4 through 7.
The authors pointed out that they chose the smallest, least-expensive intravenous dosing for the levetiracetam arm and the most-expensive intravenous dosing for the phenytoin arm.
Quality-adjusted life years (QALY) were 23.6 for phenytoin and 23.2 for levetiracetam. As a result, the cost/effectiveness ratios were $1.58/QALY for phenytoin and $20.72/QALY for levetiracetam, according to Dr. Cotton, with the University of Texas at Houston, and his colleagues.
Dr. Terence O’Keeffe and his colleagues reported no conflicts of interest.
Dr. Cotton disclosed grant/research support from Haemonetics Corp. for a multicenter trial of rapid thrombelastography.
FROM THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Major Finding: Posttraumatic seizure rates were 1.9% with prophylactic levetiracetam and 2.0% without the anticonvulsant.
Data Source: Retrospective and propensity score matched cohort analyses of 5,551 patients with mild and severe traumatic brain injury.
Disclosures: The authors report no conflicts of interest.
Prophylactic Levetiracetam Fails to Reduce Post-TBI Seizures
NAPLES, FLA. – Early seizure rates after traumatic brain injury were nearly identical whether patients did or did not receive levetiracetam prophylaxis in a retrospective analysis of 5,551 patients.
The seizure rate during the first 7 days post injury was 1.9% among 208 patients given prophylactic levetiracetam (Keppra) vs. 2% among the 5,343 patients who were not (P = .92).
Seizure rates with and without prophylactic phenytoin (Dilantin) were 4.5% vs. 1.8% (P = .053), and 0% vs. 2% with and without prophylactic fosphenytoin (Cerebyx) (P = .75), Dr. Terence O’Keeffe and his colleagues reported in a poster at the Eastern Association for the Surgery of Trauma.
Although a 7-day course of phenytoin is the current standard of care, the authors note that neurosurgeons are substituting levetiracetam, even though data are lacking to show the efficacy of this approach. Levetiracetam is an attractive alternative because, unlike phenytoin, it has predictable pharmacokinetics, does not require serum drug monitoring to ensure that therapeutic levels are achieved and has a low propensity for drug interactions.
The 2010 updated Brain Trauma Foundation guidelines on the management of severe traumatic brain injury recommend anticonvulsants to reduce the incidence of posttraumatic seizures within 7 days of injury, but not thereafter.
The seizure rate in the entire cohort was 0.7%, and the median time to seizure post injury was 3 days. Seven patients had seizures in the emergency department (ED). Seizures were 25 times more likely in patients with severe TBI than in those with mild TBI (2% vs. 0.08%, odds ratio 25.6), according to Dr. O’Keeffe, director of the surgical and trauma ICU at the University of Arizona, Tucson, and his colleagues.
When the 208 levetiracetam patients were propensity matched 1:1 using an 11-variable algorithm with 208 patients who did not receive levetiracetam, seizure rates remained statistically similar at 1.9% with levetiracetam vs. 3.4% without.
"Keppra is ineffective for seizure prophylaxis in a trauma population with a low incidence of post-TBI seizures," the authors wrote.
Based on their data, the authors questioned the need for seizure prophylaxis following TBI, as the seizure rate was so much lower than had been previously reported.
"The incidence is so low in mild TBI as to not merit treatment in my mind," Dr. O’Keeffe said in an interview. "I think we should develop protocols that target high-risk populations, for example penetrating TBI, and that the vast majority of patients need no prophylaxis."
The first study to evaluate levetiracetam for seizure prophylaxis in severe TBI found no difference in seizure rates among 32 patients given levetiracetam and a historical cohort of 41 patients given phenytoin, although levetiracetam was associated with an increased seizure tendency on electroencephalographic (EEG) analysis (Neurosurg. Focus 2008;25:E3). The implication of the EEG finding is unclear, and the study has been criticized for using only 1 hour of EEG monitoring.
The first randomized trial of the two drugs published last year in 52 patients with severe TBI (89%) or subarachnoid hemorrhage reported that patients receiving levetiracetam experienced better long-term outcomes than did those on phenytoin and identified no differences between groups in seizure occurrence during continuous EEG monitoring for the initial 72 hours (Neurocrit. Care 2010;12:165-72).
The current analysis included all patients treated for TBI from January 2007 to December 2009 at a level I, urban trauma center. Patients were stratified by injury severity. Of the 5,551 patients, 3,756 had a mild TBI, defined by a Head Abbreviated Injury Scale (AIS) score of 1 or 2, and 1,795 had severe TBI, defined by a Head AIS score of 3-5.
In multivariate regression analysis, only head AIS and ED heart rate were predictive of seizure. In the severe TBI group, the type of injury (that is, skull fracture, subdural, etc.) was not predictive of seizures. As for why the seizure rate was higher with prophylactic phenytoin than without, Dr. O’Keeffe said it may be the patients receiving the drug as treatment rather than as prophylaxis.
Dr. O’Keeffe and his colleagues acknowledge that propensity scores cannot remove all selection bias, that seizure data were obtained from patient chart/registry review, and that there was no standard prophylaxis over the study period. Possible future areas of study are 2010 data with standardized prophylaxis regimens and a multicenter trial looking at the Extended Glasgow Outcome Scale benefit of levetiracetam vs. placebo.
Balancing the Costs
Phenytoin is more cost-effective in reducing the risk of early posttraumatic seizures than is levetiracetam at all reasonable prices.
"In fact, for levetiracetam to reach cost effectiveness vs. phenytoin, this newer antiepileptic would have to prevent 100% of posttrauma seizures and be less than $400 for a week of therapy," Dr. Bryan Cotton and his colleagues reported in a separate cost-utility analysis at the same meeting.
Based on current data, the cost of a 7-day course of phenytoin (Dilantin) was $37.50 vs. $480 for a 7-day course of levetiracetam (Keppra).
The cost-utility analysis was conducted from the perspective of a university, level 1 urban trauma center, assuming that all patients with traumatic brain injury survived to receive 7 days of either agent to prevent posttraumatic seizures.
Base case assumptions were that all phenytoin patients would receive 1 g fosphenytoin (Cerebyx) intravenous load on day 0 plus 3 days of 100 mg phenytoin every 8 hours and that all levetiracetam patients would receive 500-mg load IV on day 0, followed by 7 days of 500 mg every 12 hours IV. Phenytoin patients would have a free phenytoin level drawn on day 3, with therapeutic patients receiving 100 mg phenytoin every 8 hours from post injury days 4 through 7 and subtherapeutic patients receiving an increased dose of phenytoin 200 mg every 8 hours from days 4 through 7.
The authors pointed out that they chose the smallest, least-expensive intravenous dosing for the levetiracetam arm and the most-expensive intravenous dosing for the phenytoin arm.
Quality-adjusted life years (QALY) were 23.6 for phenytoin and 23.2 for levetiracetam. As a result, the cost/effectiveness ratios were $1.58/QALY for phenytoin and $20.72/QALY for levetiracetam, according to Dr. Cotton, with the University of Texas at Houston, and his colleagues.
Dr. Terence O’Keeffe and his colleagues reported no conflicts of interest.
Dr. Cotton disclosed grant/research support from Haemonetics Corp. for a multicenter trial of rapid thrombelastography.
NAPLES, FLA. – Early seizure rates after traumatic brain injury were nearly identical whether patients did or did not receive levetiracetam prophylaxis in a retrospective analysis of 5,551 patients.
The seizure rate during the first 7 days post injury was 1.9% among 208 patients given prophylactic levetiracetam (Keppra) vs. 2% among the 5,343 patients who were not (P = .92).
Seizure rates with and without prophylactic phenytoin (Dilantin) were 4.5% vs. 1.8% (P = .053), and 0% vs. 2% with and without prophylactic fosphenytoin (Cerebyx) (P = .75), Dr. Terence O’Keeffe and his colleagues reported in a poster at the Eastern Association for the Surgery of Trauma.
Although a 7-day course of phenytoin is the current standard of care, the authors note that neurosurgeons are substituting levetiracetam, even though data are lacking to show the efficacy of this approach. Levetiracetam is an attractive alternative because, unlike phenytoin, it has predictable pharmacokinetics, does not require serum drug monitoring to ensure that therapeutic levels are achieved and has a low propensity for drug interactions.
The 2010 updated Brain Trauma Foundation guidelines on the management of severe traumatic brain injury recommend anticonvulsants to reduce the incidence of posttraumatic seizures within 7 days of injury, but not thereafter.
The seizure rate in the entire cohort was 0.7%, and the median time to seizure post injury was 3 days. Seven patients had seizures in the emergency department (ED). Seizures were 25 times more likely in patients with severe TBI than in those with mild TBI (2% vs. 0.08%, odds ratio 25.6), according to Dr. O’Keeffe, director of the surgical and trauma ICU at the University of Arizona, Tucson, and his colleagues.
When the 208 levetiracetam patients were propensity matched 1:1 using an 11-variable algorithm with 208 patients who did not receive levetiracetam, seizure rates remained statistically similar at 1.9% with levetiracetam vs. 3.4% without.
"Keppra is ineffective for seizure prophylaxis in a trauma population with a low incidence of post-TBI seizures," the authors wrote.
Based on their data, the authors questioned the need for seizure prophylaxis following TBI, as the seizure rate was so much lower than had been previously reported.
"The incidence is so low in mild TBI as to not merit treatment in my mind," Dr. O’Keeffe said in an interview. "I think we should develop protocols that target high-risk populations, for example penetrating TBI, and that the vast majority of patients need no prophylaxis."
The first study to evaluate levetiracetam for seizure prophylaxis in severe TBI found no difference in seizure rates among 32 patients given levetiracetam and a historical cohort of 41 patients given phenytoin, although levetiracetam was associated with an increased seizure tendency on electroencephalographic (EEG) analysis (Neurosurg. Focus 2008;25:E3). The implication of the EEG finding is unclear, and the study has been criticized for using only 1 hour of EEG monitoring.
The first randomized trial of the two drugs published last year in 52 patients with severe TBI (89%) or subarachnoid hemorrhage reported that patients receiving levetiracetam experienced better long-term outcomes than did those on phenytoin and identified no differences between groups in seizure occurrence during continuous EEG monitoring for the initial 72 hours (Neurocrit. Care 2010;12:165-72).
The current analysis included all patients treated for TBI from January 2007 to December 2009 at a level I, urban trauma center. Patients were stratified by injury severity. Of the 5,551 patients, 3,756 had a mild TBI, defined by a Head Abbreviated Injury Scale (AIS) score of 1 or 2, and 1,795 had severe TBI, defined by a Head AIS score of 3-5.
In multivariate regression analysis, only head AIS and ED heart rate were predictive of seizure. In the severe TBI group, the type of injury (that is, skull fracture, subdural, etc.) was not predictive of seizures. As for why the seizure rate was higher with prophylactic phenytoin than without, Dr. O’Keeffe said it may be the patients receiving the drug as treatment rather than as prophylaxis.
Dr. O’Keeffe and his colleagues acknowledge that propensity scores cannot remove all selection bias, that seizure data were obtained from patient chart/registry review, and that there was no standard prophylaxis over the study period. Possible future areas of study are 2010 data with standardized prophylaxis regimens and a multicenter trial looking at the Extended Glasgow Outcome Scale benefit of levetiracetam vs. placebo.
Balancing the Costs
Phenytoin is more cost-effective in reducing the risk of early posttraumatic seizures than is levetiracetam at all reasonable prices.
"In fact, for levetiracetam to reach cost effectiveness vs. phenytoin, this newer antiepileptic would have to prevent 100% of posttrauma seizures and be less than $400 for a week of therapy," Dr. Bryan Cotton and his colleagues reported in a separate cost-utility analysis at the same meeting.
Based on current data, the cost of a 7-day course of phenytoin (Dilantin) was $37.50 vs. $480 for a 7-day course of levetiracetam (Keppra).
The cost-utility analysis was conducted from the perspective of a university, level 1 urban trauma center, assuming that all patients with traumatic brain injury survived to receive 7 days of either agent to prevent posttraumatic seizures.
Base case assumptions were that all phenytoin patients would receive 1 g fosphenytoin (Cerebyx) intravenous load on day 0 plus 3 days of 100 mg phenytoin every 8 hours and that all levetiracetam patients would receive 500-mg load IV on day 0, followed by 7 days of 500 mg every 12 hours IV. Phenytoin patients would have a free phenytoin level drawn on day 3, with therapeutic patients receiving 100 mg phenytoin every 8 hours from post injury days 4 through 7 and subtherapeutic patients receiving an increased dose of phenytoin 200 mg every 8 hours from days 4 through 7.
The authors pointed out that they chose the smallest, least-expensive intravenous dosing for the levetiracetam arm and the most-expensive intravenous dosing for the phenytoin arm.
Quality-adjusted life years (QALY) were 23.6 for phenytoin and 23.2 for levetiracetam. As a result, the cost/effectiveness ratios were $1.58/QALY for phenytoin and $20.72/QALY for levetiracetam, according to Dr. Cotton, with the University of Texas at Houston, and his colleagues.
Dr. Terence O’Keeffe and his colleagues reported no conflicts of interest.
Dr. Cotton disclosed grant/research support from Haemonetics Corp. for a multicenter trial of rapid thrombelastography.
NAPLES, FLA. – Early seizure rates after traumatic brain injury were nearly identical whether patients did or did not receive levetiracetam prophylaxis in a retrospective analysis of 5,551 patients.
The seizure rate during the first 7 days post injury was 1.9% among 208 patients given prophylactic levetiracetam (Keppra) vs. 2% among the 5,343 patients who were not (P = .92).
Seizure rates with and without prophylactic phenytoin (Dilantin) were 4.5% vs. 1.8% (P = .053), and 0% vs. 2% with and without prophylactic fosphenytoin (Cerebyx) (P = .75), Dr. Terence O’Keeffe and his colleagues reported in a poster at the Eastern Association for the Surgery of Trauma.
Although a 7-day course of phenytoin is the current standard of care, the authors note that neurosurgeons are substituting levetiracetam, even though data are lacking to show the efficacy of this approach. Levetiracetam is an attractive alternative because, unlike phenytoin, it has predictable pharmacokinetics, does not require serum drug monitoring to ensure that therapeutic levels are achieved and has a low propensity for drug interactions.
The 2010 updated Brain Trauma Foundation guidelines on the management of severe traumatic brain injury recommend anticonvulsants to reduce the incidence of posttraumatic seizures within 7 days of injury, but not thereafter.
The seizure rate in the entire cohort was 0.7%, and the median time to seizure post injury was 3 days. Seven patients had seizures in the emergency department (ED). Seizures were 25 times more likely in patients with severe TBI than in those with mild TBI (2% vs. 0.08%, odds ratio 25.6), according to Dr. O’Keeffe, director of the surgical and trauma ICU at the University of Arizona, Tucson, and his colleagues.
When the 208 levetiracetam patients were propensity matched 1:1 using an 11-variable algorithm with 208 patients who did not receive levetiracetam, seizure rates remained statistically similar at 1.9% with levetiracetam vs. 3.4% without.
"Keppra is ineffective for seizure prophylaxis in a trauma population with a low incidence of post-TBI seizures," the authors wrote.
Based on their data, the authors questioned the need for seizure prophylaxis following TBI, as the seizure rate was so much lower than had been previously reported.
"The incidence is so low in mild TBI as to not merit treatment in my mind," Dr. O’Keeffe said in an interview. "I think we should develop protocols that target high-risk populations, for example penetrating TBI, and that the vast majority of patients need no prophylaxis."
The first study to evaluate levetiracetam for seizure prophylaxis in severe TBI found no difference in seizure rates among 32 patients given levetiracetam and a historical cohort of 41 patients given phenytoin, although levetiracetam was associated with an increased seizure tendency on electroencephalographic (EEG) analysis (Neurosurg. Focus 2008;25:E3). The implication of the EEG finding is unclear, and the study has been criticized for using only 1 hour of EEG monitoring.
The first randomized trial of the two drugs published last year in 52 patients with severe TBI (89%) or subarachnoid hemorrhage reported that patients receiving levetiracetam experienced better long-term outcomes than did those on phenytoin and identified no differences between groups in seizure occurrence during continuous EEG monitoring for the initial 72 hours (Neurocrit. Care 2010;12:165-72).
The current analysis included all patients treated for TBI from January 2007 to December 2009 at a level I, urban trauma center. Patients were stratified by injury severity. Of the 5,551 patients, 3,756 had a mild TBI, defined by a Head Abbreviated Injury Scale (AIS) score of 1 or 2, and 1,795 had severe TBI, defined by a Head AIS score of 3-5.
In multivariate regression analysis, only head AIS and ED heart rate were predictive of seizure. In the severe TBI group, the type of injury (that is, skull fracture, subdural, etc.) was not predictive of seizures. As for why the seizure rate was higher with prophylactic phenytoin than without, Dr. O’Keeffe said it may be the patients receiving the drug as treatment rather than as prophylaxis.
Dr. O’Keeffe and his colleagues acknowledge that propensity scores cannot remove all selection bias, that seizure data were obtained from patient chart/registry review, and that there was no standard prophylaxis over the study period. Possible future areas of study are 2010 data with standardized prophylaxis regimens and a multicenter trial looking at the Extended Glasgow Outcome Scale benefit of levetiracetam vs. placebo.
Balancing the Costs
Phenytoin is more cost-effective in reducing the risk of early posttraumatic seizures than is levetiracetam at all reasonable prices.
"In fact, for levetiracetam to reach cost effectiveness vs. phenytoin, this newer antiepileptic would have to prevent 100% of posttrauma seizures and be less than $400 for a week of therapy," Dr. Bryan Cotton and his colleagues reported in a separate cost-utility analysis at the same meeting.
Based on current data, the cost of a 7-day course of phenytoin (Dilantin) was $37.50 vs. $480 for a 7-day course of levetiracetam (Keppra).
The cost-utility analysis was conducted from the perspective of a university, level 1 urban trauma center, assuming that all patients with traumatic brain injury survived to receive 7 days of either agent to prevent posttraumatic seizures.
Base case assumptions were that all phenytoin patients would receive 1 g fosphenytoin (Cerebyx) intravenous load on day 0 plus 3 days of 100 mg phenytoin every 8 hours and that all levetiracetam patients would receive 500-mg load IV on day 0, followed by 7 days of 500 mg every 12 hours IV. Phenytoin patients would have a free phenytoin level drawn on day 3, with therapeutic patients receiving 100 mg phenytoin every 8 hours from post injury days 4 through 7 and subtherapeutic patients receiving an increased dose of phenytoin 200 mg every 8 hours from days 4 through 7.
The authors pointed out that they chose the smallest, least-expensive intravenous dosing for the levetiracetam arm and the most-expensive intravenous dosing for the phenytoin arm.
Quality-adjusted life years (QALY) were 23.6 for phenytoin and 23.2 for levetiracetam. As a result, the cost/effectiveness ratios were $1.58/QALY for phenytoin and $20.72/QALY for levetiracetam, according to Dr. Cotton, with the University of Texas at Houston, and his colleagues.
Dr. Terence O’Keeffe and his colleagues reported no conflicts of interest.
Dr. Cotton disclosed grant/research support from Haemonetics Corp. for a multicenter trial of rapid thrombelastography.
FROM THE EASTERN ASSOCIATION FOR THE SURGERY OF TRAUMA
Major Finding: Posttraumatic seizure rates were 1.9% with prophylactic levetiracetam and 2.0% without the anticonvulsant.
Data Source: Retrospective and propensity score matched cohort analyses of 5,551 patients with mild and severe traumatic brain injury.
Disclosures: The authors report no conflicts of interest.
Lung Debris May Help Identify Surgical Margins
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
Microscopic Vascular Invasion Emerging as a Powerful Prognosticator in Early Lung Cancer
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
Lung Debris May Help Identify Surgical Margins
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
Microscopic Vascular Invasion Emerging as a Powerful Prognosticator in Early Lung Cancer
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
Lung Debris May Help Identify Surgical Margins
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
CHICAGO - A novel technique utilizing stapled lung debris could help determine adequate and inadequate surgical margins in resected non-small cell lung cancer, results of a prospective study suggest.
Researchers at Albany (N.Y.) Medical College and the Hospital of St. Raphael in New Haven, Conn., are using cytology to analyze lung tissue taken from spent staple cartridges used during sublobar resection. The staple cartridge is simply mixed with 30 cc of normal saline and serves as the cytologic margin, Dr. Thomas Fabian explained at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
"People have [observed] that certain staples used through cancers can potentially contaminate new tissue planes, so that is how the idea was born," he said in an interview.
Dr. Fabian and his colleagues prospectively compared staple-line cytology with traditional histopathologic evaluation of surgical specimens taken from 97 patients undergoing diagnostic sublobar wedge resection between November 2007 and September 2009. Of the 98 specimens retrieved, 30 were benign and 68 were malignant.
Staple-line cytology was 100% accurate in the evaluation of benign lesions when compared with histology, he said.
In the 68 malignant nodules, initial blinded cytologic evaluation was positive in 7, surgical pathology was positive in 6, and both were positive in 4.
Subsequent unblinded review of both specimens changed the final pathologic interpretation in 4 (6%) of the 68 cases, said Dr. Fabian, chief of thoracic surgery at the Albany Medical Center. The interpretation changed from a negative margin to a positive margin in 3 surgical specimens (7%) and in 1 staple-line cytology specimen (2%).
According to analysis of the unblinded data, staple-line cytology demonstrated an overall accuracy of 96%, with 88% sensitivity, 97% specificity, 70% positive-predictive value, and 99% negative-predictive value.
Dr. Fabian described staple-line cytology as a simple technique that could serve as an adjunct to the gold standard of histopathology, which he said is prone to inaccuracies including both false positives and false negatives.
"We need to reevaluate the techniques that allow us to accurately assess surgical margins - particularly in the setting of sublobar resections, given the growing interest in this technique," according to Dr. Fabian.
"The cytologic technique appears to be sensitive, specific, and accurate, but it does need to be validated at other institutions and with additional studies," he added.
Dr. Fabian acknowledged that by design the study lacked clinical outcome data and said further evaluation is ongoing. The next step is to evaluate the technique in patients undergoing sublobar resection with curative intent.
Of the 68 malignant samples, 43 were diagnosed as adenocarcinoma, 7 as squamous cell carcinoma, 3 as large cell, 1 as small cell, 5 as carcinoid, and 9 as other histologies.
Dr. Fabian disclosed serving as a speaker for, and receiving research funding and honoraria from, Covidien. His coauthors reported no conflicts.
Microscopic Vascular Invasion Emerging as a Powerful Prognosticator in Early Lung Cancer
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
Subtle histologic markers have long been championed as a potential means to this ends, but historically gain little traction because essentially all are trumped by the presence of either metastic disease or regional lymph node involvement as important risks for recurrence. Consequently, the use of more sophisticated, but perhaps less reproduceable, pathologic markers is retricted to node-negative cancers, where T (of TNM) descriptors are important. This represents only about one-quarter of all lung cancers detected.
The authors have proposed microscopic vascular invasion (MVI) as an important factor that might be a reasonable addition to the T aspect of the new staging system. Their data demonstrate that MVI (found in a relatively small cohort of all node-negative patients in their study) appears to be an important risk for mortality. However, the road to the perfect staging system is paved with new histopathologic markers, and few are adopted because another one soon emerges and it is difficult for pathologists to keep up.
I think that molecular and radiologic characterization will eventually supplant all such subjective histopathologic markers and, within the next few years, will make the microscope something we'll be telling our grandkids about.
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
CHICAGO - New data suggest that microscopic vascular invasion may be a more powerful prognosticator in early lung cancer than are the tumor size-based categories suggested in the new TNM staging system.
Italian researchers used histologic and immunohistochemical techniques to identify microscopic vascular invasion (MVI), or the presence of neoplastic structures inside the lumen of a vessel, in one-third (154) of 512 patients with resected, pathologically staged T1a to T3 node-negative non-small cell lung cancer (NSCLC). The 2009 edition of the tumor, node, metastasis (TNM) staging system for lung tumors was used.
MVI was significantly correlated with the presence of tumor-infiltrating lymphocytes (odds ratio 1.65, P value = .03), adenocarcinoma histology (OR 1.32, P = .003), and increased tumor size (OR 1.13, P = .009).
Five-year overall survival was significantly lower for patients with MVI at 50% vs. those without MVI at 66% (P = .001), Dr. Enrico Ruffini said at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
The difference in survival remained significant even in those with squamous cell carcinoma (45% vs. 61%, P = .05), although it was more pronounced in those with adenocarcinoma (56% vs. 70%, P = .03).
"Microscopic vascular invasion is a significant independent negative prognostic factor," he said.
When patients with pT1a-T2b tumors were stratified by T-size category, the presence of MVI resulted in a one-category upstaging for each T category, said Dr. Ruffini of the division of thoracic surgery at the University of Torino (Italy). For example, T1a patients with MVI had a prognosis similar to that of patients with T1b tumors without MVI. The number of T3 cases was too small to stratify.
T size was prognostic of survival in the MVI-negative patients (P = .03) but was not a statistically significant factor in MVI-positive patients (P = .9), indicating that MVI is indeed a more powerful prognosticator, he said.
The 2009 TNM stresses the importance of tumor size as a major prognostic factor, but no TNM edition has so far included MVI as a major determinant in the staging of NSCLC.
In a multivariate survival analysis that included age, sex, histology, grading, T-size determinant, MVI, perineural invasion, and tumor-infiltrating lymphocytes, MVI was a stronger prognostic indicator (hazard ratio 1.43, P = .02) than T-size determinant (HR 1.06, P = .06), Dr. Ruffini said.
"The use of adjuvant chemotherapy in NSCLC patients with MVI may be considered," he said.
Invited discussant Dr. Mark Socinski pointed out that 88% of patients in the analysis had 5 cm or smaller tumors, a category of patients in which the role of adjuvant therapy has been discouraged. He highlighted the recent LACE meta-analysis of 4,584 NSCLC patients in five cisplatin-based adjuvant chemotherapy trials that showed an overall significant survival benefit of 4% at 5 years, but also a potentially negative effect in resected stage 1A (Ann. Oncol. 2010 Oct;21 Suppl. 7:vii196-vii198).
"We need to make sure [MVI] is easily reproducible amongst pathologists, and we also clearly need to demonstrate that adjuvant therapy can overcome the biologic impact of this histopathologic finding," said Dr. Socinski of the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
Dr. Ruffini acknowledged that bias could have been introduced into the study through its retrospective design, use of overall survival rather than disease-free survival as an outcome measure, and the long study period of January 1998 to August 2008. Prospective validation of MVI is underway using the prospective International Association for the Study of Lung Cancer database, he said.
The median tumor size among the 512 patients was 3.4 cm, with 164 classified as having T1a (less than 2 cm) tumors, 123 T1b (2-3 cm), 164 T2a (3-5 cm), 50 T2b (5-7 cm), and 11 T3 (greater than 7 cm) tumors.
The researchers and Dr. Socinski disclosed no relevant conflicts.
Pediatric HIV Admissions Decline Is Slowing
Minneapolis – Pediatric HIV admissions continue to decline, but less so than previously reported and mostly in older children, according to an analysis of two national data sets.
Researchers analyzed the Kids' Inpatient Database (KID) and Nationwide Inpatient Sample (NIS) from 2003 through 2007 for HIV trends across the years including hospitalization rates, changes in length of stay (LOS), and costs. The NIS data are annual; KID data are triennial.
Pediatric admissions for HIV as a primary diagnosis declined from 2003 by 32% in the 2006 KID and by 47% in the 2007 NIS. The decrease in admissions for HIV as the principal diagnosis plus secondary conditions, also known as the all-listed diagnosis, was lower at 23% for the 2006 KID and 38% for the 2007 NIS, Dr. Daniel Rauch reported in a poster presentation at the meeting.
“We've been very successful in identifying kids with HIV and preventing transmission, so that we're seeing an overall reduction in HIV in the United States,” he said. “The decreased admission volume is also partly due to successful management of HIV by multidisciplinary outpatient teams, which may serve as a model for chronic disease management. The outcome is that less and less children are being hospitalized.”
In New York City, just five infants were born with HIV last year, noted Dr. Rauch of Mount Sinai School of Medicine and associate director of pediatrics at Elmhurst Hospital Center, both in New York.
The pace of the decline is slower than previously reported. A similar analysis of NIS data documented a 71% decline in hospital use by HIV-infected children from 1994 to 2003, during the advent of highly active antiretroviral therapy (Pediatrics 2007;120:e236-43).
This decrease was more marked among infants and children younger than 5 years (94% for boys, 92% for girls), compared with adolescents (47% decrease for boys, 23% increase for girls aged 15–18 years).
By contrast, the current KID data show decreased admissions were more from children older than 4 years, Dr. Rauch said. In this age group, admissions for HIV as a primary diagnosis and as an all-listed diagnosis were 24% and 33%, compared with 17% and 15%, respectively, among children youngerlthan 5.
The previously observed decrease in male admissions also has reversed and the male/female ratio now approaches 50%. Boys represented 38% of primary diagnoses in both the 2003 KID and NIS data sets, compared with 44% in the 2006 KID and 2007 NIS, said Dr. Rauch, who could offer no explanation for the finding.
“We have to stay vigilant,” he said. “We can't let it get away from us.”
For all years, HIV children are hospitalized overwhelmingly in teaching hospitals (more than 81%) and in metropolitan areas (more than 98%).
“The potential downfall there is that they're only presenting to a few centers now, so the overall skill set of taking care of a child that is HIV positive and is sick is being lost from the general community and only remains in a couple of centers,” he said at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Length of hospital stay for HIV as a primary diagnosis varied from 10.8 days in the 2003 NIS to 6.6 days in the 2005 NIS to 12.2 days in the 2007 NIS.
The average cost per admission increased from $15,015 in the 2003 KID to $20,936 in 2006 and from $18,493 in the 2003 NIS to $20,832 in the 2007 NIS. The lowest cost for admission was $13,448 in the 2005 NIS.
Cost per day increased from $1,706 in 2003 to $1,869 in 2006 in the KID data set, but stayed stable in the NIS data set at $1,712 in the 2003 vs. $1,707 in 2007.
Dr. Rauch reports serving as a consultant with Baxter.
Minneapolis – Pediatric HIV admissions continue to decline, but less so than previously reported and mostly in older children, according to an analysis of two national data sets.
Researchers analyzed the Kids' Inpatient Database (KID) and Nationwide Inpatient Sample (NIS) from 2003 through 2007 for HIV trends across the years including hospitalization rates, changes in length of stay (LOS), and costs. The NIS data are annual; KID data are triennial.
Pediatric admissions for HIV as a primary diagnosis declined from 2003 by 32% in the 2006 KID and by 47% in the 2007 NIS. The decrease in admissions for HIV as the principal diagnosis plus secondary conditions, also known as the all-listed diagnosis, was lower at 23% for the 2006 KID and 38% for the 2007 NIS, Dr. Daniel Rauch reported in a poster presentation at the meeting.
“We've been very successful in identifying kids with HIV and preventing transmission, so that we're seeing an overall reduction in HIV in the United States,” he said. “The decreased admission volume is also partly due to successful management of HIV by multidisciplinary outpatient teams, which may serve as a model for chronic disease management. The outcome is that less and less children are being hospitalized.”
In New York City, just five infants were born with HIV last year, noted Dr. Rauch of Mount Sinai School of Medicine and associate director of pediatrics at Elmhurst Hospital Center, both in New York.
The pace of the decline is slower than previously reported. A similar analysis of NIS data documented a 71% decline in hospital use by HIV-infected children from 1994 to 2003, during the advent of highly active antiretroviral therapy (Pediatrics 2007;120:e236-43).
This decrease was more marked among infants and children younger than 5 years (94% for boys, 92% for girls), compared with adolescents (47% decrease for boys, 23% increase for girls aged 15–18 years).
By contrast, the current KID data show decreased admissions were more from children older than 4 years, Dr. Rauch said. In this age group, admissions for HIV as a primary diagnosis and as an all-listed diagnosis were 24% and 33%, compared with 17% and 15%, respectively, among children youngerlthan 5.
The previously observed decrease in male admissions also has reversed and the male/female ratio now approaches 50%. Boys represented 38% of primary diagnoses in both the 2003 KID and NIS data sets, compared with 44% in the 2006 KID and 2007 NIS, said Dr. Rauch, who could offer no explanation for the finding.
“We have to stay vigilant,” he said. “We can't let it get away from us.”
For all years, HIV children are hospitalized overwhelmingly in teaching hospitals (more than 81%) and in metropolitan areas (more than 98%).
“The potential downfall there is that they're only presenting to a few centers now, so the overall skill set of taking care of a child that is HIV positive and is sick is being lost from the general community and only remains in a couple of centers,” he said at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Length of hospital stay for HIV as a primary diagnosis varied from 10.8 days in the 2003 NIS to 6.6 days in the 2005 NIS to 12.2 days in the 2007 NIS.
The average cost per admission increased from $15,015 in the 2003 KID to $20,936 in 2006 and from $18,493 in the 2003 NIS to $20,832 in the 2007 NIS. The lowest cost for admission was $13,448 in the 2005 NIS.
Cost per day increased from $1,706 in 2003 to $1,869 in 2006 in the KID data set, but stayed stable in the NIS data set at $1,712 in the 2003 vs. $1,707 in 2007.
Dr. Rauch reports serving as a consultant with Baxter.
Minneapolis – Pediatric HIV admissions continue to decline, but less so than previously reported and mostly in older children, according to an analysis of two national data sets.
Researchers analyzed the Kids' Inpatient Database (KID) and Nationwide Inpatient Sample (NIS) from 2003 through 2007 for HIV trends across the years including hospitalization rates, changes in length of stay (LOS), and costs. The NIS data are annual; KID data are triennial.
Pediatric admissions for HIV as a primary diagnosis declined from 2003 by 32% in the 2006 KID and by 47% in the 2007 NIS. The decrease in admissions for HIV as the principal diagnosis plus secondary conditions, also known as the all-listed diagnosis, was lower at 23% for the 2006 KID and 38% for the 2007 NIS, Dr. Daniel Rauch reported in a poster presentation at the meeting.
“We've been very successful in identifying kids with HIV and preventing transmission, so that we're seeing an overall reduction in HIV in the United States,” he said. “The decreased admission volume is also partly due to successful management of HIV by multidisciplinary outpatient teams, which may serve as a model for chronic disease management. The outcome is that less and less children are being hospitalized.”
In New York City, just five infants were born with HIV last year, noted Dr. Rauch of Mount Sinai School of Medicine and associate director of pediatrics at Elmhurst Hospital Center, both in New York.
The pace of the decline is slower than previously reported. A similar analysis of NIS data documented a 71% decline in hospital use by HIV-infected children from 1994 to 2003, during the advent of highly active antiretroviral therapy (Pediatrics 2007;120:e236-43).
This decrease was more marked among infants and children younger than 5 years (94% for boys, 92% for girls), compared with adolescents (47% decrease for boys, 23% increase for girls aged 15–18 years).
By contrast, the current KID data show decreased admissions were more from children older than 4 years, Dr. Rauch said. In this age group, admissions for HIV as a primary diagnosis and as an all-listed diagnosis were 24% and 33%, compared with 17% and 15%, respectively, among children youngerlthan 5.
The previously observed decrease in male admissions also has reversed and the male/female ratio now approaches 50%. Boys represented 38% of primary diagnoses in both the 2003 KID and NIS data sets, compared with 44% in the 2006 KID and 2007 NIS, said Dr. Rauch, who could offer no explanation for the finding.
“We have to stay vigilant,” he said. “We can't let it get away from us.”
For all years, HIV children are hospitalized overwhelmingly in teaching hospitals (more than 81%) and in metropolitan areas (more than 98%).
“The potential downfall there is that they're only presenting to a few centers now, so the overall skill set of taking care of a child that is HIV positive and is sick is being lost from the general community and only remains in a couple of centers,” he said at the meeting, which was sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
Length of hospital stay for HIV as a primary diagnosis varied from 10.8 days in the 2003 NIS to 6.6 days in the 2005 NIS to 12.2 days in the 2007 NIS.
The average cost per admission increased from $15,015 in the 2003 KID to $20,936 in 2006 and from $18,493 in the 2003 NIS to $20,832 in the 2007 NIS. The lowest cost for admission was $13,448 in the 2005 NIS.
Cost per day increased from $1,706 in 2003 to $1,869 in 2006 in the KID data set, but stayed stable in the NIS data set at $1,712 in the 2003 vs. $1,707 in 2007.
Dr. Rauch reports serving as a consultant with Baxter.