User login
Experts Recommend Medication for Pediatric MASLD Management
, according to a new joint perspective paper.
Pediatric MASLD is the number-one cause of chronic liver disease in children and the number-one reason for liver transplant listing in young adults aged 18-40 years, said corresponding author Jennifer A. Panganiban, MD, Children’s Hospital of Philadelphia, Philadelphia.
The paper, published in Obesity Pillars, represents “a call to action that has been long overdue,” Panganiban told GI & Hepatology News.
The goal of the authors was to bring global awareness to the recent changes in the pediatric MASLD landscape — especially in medication use — and to empower clinicians treating the disease, she explained.
The recommendations are based on a combination of the latest published evidence and clinical expertise from eight hepatologists/gastroenterologists and two physicians from the Obesity Medicine Association, Centennial, Colorado.
One of the major barriers to MASLD management in children is suboptimal screening resulting in underdiagnosis, said Panganiban. “Unfortunately, only up to 30% of children are being screened in their pediatrician’s office.”
The new guideline outlines the patient care process from screening, referral to a subspecialist, and workup; however, the primary focus is on treatment with medication options that were previously not available or underutilized, she said.
Successful and Sustainable Weight Loss
Adiposity and weight gain make MASLD worse, but weight reduction has been shown to improve the condition, the authors noted. Previous strategies for curbing MASLD in children with obesity have focused mainly on lifestyle changes, but with limited success.
Nevertheless, the authors recommend continuing physical activity and nutrition as treatments for MASLD in children, with a plan tailored specifically to the patient.
In addition, however, they suggest that anti-obesity medications started early in the disease may help reduce costs and improve future outcomes.
Although glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have not yet been studied specifically for pediatric MASLD, data from studies of pediatric obesity, diabetes, and other retrospective studies are encouraging, the authors wrote.
The GLP-1 RAs liraglutide and semaglutide are both approved by the US Food and Drug Administration (FDA) for managing obesity in children and adolescents aged 12 years or older, they noted. And a recent phase 3a randomized trial showed that liraglutide, not yet approved for children younger than 12 years, led to a mean change in body mass index of 5.8% from baseline to 56 weeks in children aged 6-11 years with obesity.
GLP-1 RAs not only are effective for weight management but also improve other metabolic dysfunction indicators including cholesterol and blood pressure, which makes these medications an even more beneficial option for individuals with obesity and MASLD, Panganiban and colleagues wrote.
For example, a recent single-center study of 111 children with MASLD (mean age, 15 years) showed a significant improvement in alanine aminotransferase levels with the use of GLP-1 RAs, although body mass index and weight were unchanged.
Regaining weight after discontinuing GLP-1 RAs is the main barrier to their use for MASLD, the authors noted. In addition, GLP-1 RAs are contraindicated in some situations, such as in those with a history of serious hypersensitivity, and in patients with a personal or family history of either medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 based on animal studies showing an association with the medications and thyroid C–cell tumors.
Other FDA-approved medication options for obesity in children include metformin, topiramate, and phentermine, as well as bupropion, lisdexamfetamine, and setmelanotide, the authors said.
Resmetirom, a thyroid hormone receptor-beta agonist, which is another significant breakthrough in MASLD for adults, has not yet been tested or approved for pediatric use.
In addition to medications, metabolic bariatric surgery has shown effectiveness in children with obesity and/or MASLD by reducing liver fat and reversing fibrosis, as shown in the Teen-LABS study, the authors wrote. However, long-term data on fibrosis reversal are limited, and cost and access remain barriers.
More Research Needed
The joint expert review is intended as an educational tool that may require updates and should not be interpreted as rules for individual patient care, the authors cautioned. And physical activity and nutrition remain the primary treatment of MASLD and should be continued in conjunction with other treatment modalities, they emphasized.
Looking ahead, research is needed to develop accurate and reliable noninvasive biomarkers to diagnose and assess obesity treatment efficacy, Panganiban told GI & Hepatology News.
Also needed are multicenter randomized control trials in children with obesity involving different medications that have been successful in the treatment of metabolic dysfunction–associated steatohepatitis/fibrosis in adults, such as GLP-1 RAs or resmetirom, she added.
Educating Clinicians on Early Identification
When obesity occurs in childhood, it starts a process of additional complications that arise in earlier ages in adults, said Saul J. Karpen, MD, chief scientific officer at the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health, Virginia Commonwealth University, Richmond, Virginia, in an interview.“Given the epidemic of obesity, altered diets, and reduced physical activities during younger ages, it is not easy to identify which children are at greater risk of MASLD,” said Karpen.
“It requires insight from the care providers and often imaging, a blood test, or a referral to a pediatric hepatologist, and not every region has easy access to such expertise,” Karpen said.
The new review is important because it highlights the fact that obesity and its consequences are not limited to adulthood, and that educated clinicians are in a position to get an early start on treatment in children, Karpen noted.
The guideline received no outside funding. Panganiban and Karpen had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
, according to a new joint perspective paper.
Pediatric MASLD is the number-one cause of chronic liver disease in children and the number-one reason for liver transplant listing in young adults aged 18-40 years, said corresponding author Jennifer A. Panganiban, MD, Children’s Hospital of Philadelphia, Philadelphia.
The paper, published in Obesity Pillars, represents “a call to action that has been long overdue,” Panganiban told GI & Hepatology News.
The goal of the authors was to bring global awareness to the recent changes in the pediatric MASLD landscape — especially in medication use — and to empower clinicians treating the disease, she explained.
The recommendations are based on a combination of the latest published evidence and clinical expertise from eight hepatologists/gastroenterologists and two physicians from the Obesity Medicine Association, Centennial, Colorado.
One of the major barriers to MASLD management in children is suboptimal screening resulting in underdiagnosis, said Panganiban. “Unfortunately, only up to 30% of children are being screened in their pediatrician’s office.”
The new guideline outlines the patient care process from screening, referral to a subspecialist, and workup; however, the primary focus is on treatment with medication options that were previously not available or underutilized, she said.
Successful and Sustainable Weight Loss
Adiposity and weight gain make MASLD worse, but weight reduction has been shown to improve the condition, the authors noted. Previous strategies for curbing MASLD in children with obesity have focused mainly on lifestyle changes, but with limited success.
Nevertheless, the authors recommend continuing physical activity and nutrition as treatments for MASLD in children, with a plan tailored specifically to the patient.
In addition, however, they suggest that anti-obesity medications started early in the disease may help reduce costs and improve future outcomes.
Although glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have not yet been studied specifically for pediatric MASLD, data from studies of pediatric obesity, diabetes, and other retrospective studies are encouraging, the authors wrote.
The GLP-1 RAs liraglutide and semaglutide are both approved by the US Food and Drug Administration (FDA) for managing obesity in children and adolescents aged 12 years or older, they noted. And a recent phase 3a randomized trial showed that liraglutide, not yet approved for children younger than 12 years, led to a mean change in body mass index of 5.8% from baseline to 56 weeks in children aged 6-11 years with obesity.
GLP-1 RAs not only are effective for weight management but also improve other metabolic dysfunction indicators including cholesterol and blood pressure, which makes these medications an even more beneficial option for individuals with obesity and MASLD, Panganiban and colleagues wrote.
For example, a recent single-center study of 111 children with MASLD (mean age, 15 years) showed a significant improvement in alanine aminotransferase levels with the use of GLP-1 RAs, although body mass index and weight were unchanged.
Regaining weight after discontinuing GLP-1 RAs is the main barrier to their use for MASLD, the authors noted. In addition, GLP-1 RAs are contraindicated in some situations, such as in those with a history of serious hypersensitivity, and in patients with a personal or family history of either medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 based on animal studies showing an association with the medications and thyroid C–cell tumors.
Other FDA-approved medication options for obesity in children include metformin, topiramate, and phentermine, as well as bupropion, lisdexamfetamine, and setmelanotide, the authors said.
Resmetirom, a thyroid hormone receptor-beta agonist, which is another significant breakthrough in MASLD for adults, has not yet been tested or approved for pediatric use.
In addition to medications, metabolic bariatric surgery has shown effectiveness in children with obesity and/or MASLD by reducing liver fat and reversing fibrosis, as shown in the Teen-LABS study, the authors wrote. However, long-term data on fibrosis reversal are limited, and cost and access remain barriers.
More Research Needed
The joint expert review is intended as an educational tool that may require updates and should not be interpreted as rules for individual patient care, the authors cautioned. And physical activity and nutrition remain the primary treatment of MASLD and should be continued in conjunction with other treatment modalities, they emphasized.
Looking ahead, research is needed to develop accurate and reliable noninvasive biomarkers to diagnose and assess obesity treatment efficacy, Panganiban told GI & Hepatology News.
Also needed are multicenter randomized control trials in children with obesity involving different medications that have been successful in the treatment of metabolic dysfunction–associated steatohepatitis/fibrosis in adults, such as GLP-1 RAs or resmetirom, she added.
Educating Clinicians on Early Identification
When obesity occurs in childhood, it starts a process of additional complications that arise in earlier ages in adults, said Saul J. Karpen, MD, chief scientific officer at the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health, Virginia Commonwealth University, Richmond, Virginia, in an interview.“Given the epidemic of obesity, altered diets, and reduced physical activities during younger ages, it is not easy to identify which children are at greater risk of MASLD,” said Karpen.
“It requires insight from the care providers and often imaging, a blood test, or a referral to a pediatric hepatologist, and not every region has easy access to such expertise,” Karpen said.
The new review is important because it highlights the fact that obesity and its consequences are not limited to adulthood, and that educated clinicians are in a position to get an early start on treatment in children, Karpen noted.
The guideline received no outside funding. Panganiban and Karpen had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
, according to a new joint perspective paper.
Pediatric MASLD is the number-one cause of chronic liver disease in children and the number-one reason for liver transplant listing in young adults aged 18-40 years, said corresponding author Jennifer A. Panganiban, MD, Children’s Hospital of Philadelphia, Philadelphia.
The paper, published in Obesity Pillars, represents “a call to action that has been long overdue,” Panganiban told GI & Hepatology News.
The goal of the authors was to bring global awareness to the recent changes in the pediatric MASLD landscape — especially in medication use — and to empower clinicians treating the disease, she explained.
The recommendations are based on a combination of the latest published evidence and clinical expertise from eight hepatologists/gastroenterologists and two physicians from the Obesity Medicine Association, Centennial, Colorado.
One of the major barriers to MASLD management in children is suboptimal screening resulting in underdiagnosis, said Panganiban. “Unfortunately, only up to 30% of children are being screened in their pediatrician’s office.”
The new guideline outlines the patient care process from screening, referral to a subspecialist, and workup; however, the primary focus is on treatment with medication options that were previously not available or underutilized, she said.
Successful and Sustainable Weight Loss
Adiposity and weight gain make MASLD worse, but weight reduction has been shown to improve the condition, the authors noted. Previous strategies for curbing MASLD in children with obesity have focused mainly on lifestyle changes, but with limited success.
Nevertheless, the authors recommend continuing physical activity and nutrition as treatments for MASLD in children, with a plan tailored specifically to the patient.
In addition, however, they suggest that anti-obesity medications started early in the disease may help reduce costs and improve future outcomes.
Although glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have not yet been studied specifically for pediatric MASLD, data from studies of pediatric obesity, diabetes, and other retrospective studies are encouraging, the authors wrote.
The GLP-1 RAs liraglutide and semaglutide are both approved by the US Food and Drug Administration (FDA) for managing obesity in children and adolescents aged 12 years or older, they noted. And a recent phase 3a randomized trial showed that liraglutide, not yet approved for children younger than 12 years, led to a mean change in body mass index of 5.8% from baseline to 56 weeks in children aged 6-11 years with obesity.
GLP-1 RAs not only are effective for weight management but also improve other metabolic dysfunction indicators including cholesterol and blood pressure, which makes these medications an even more beneficial option for individuals with obesity and MASLD, Panganiban and colleagues wrote.
For example, a recent single-center study of 111 children with MASLD (mean age, 15 years) showed a significant improvement in alanine aminotransferase levels with the use of GLP-1 RAs, although body mass index and weight were unchanged.
Regaining weight after discontinuing GLP-1 RAs is the main barrier to their use for MASLD, the authors noted. In addition, GLP-1 RAs are contraindicated in some situations, such as in those with a history of serious hypersensitivity, and in patients with a personal or family history of either medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 based on animal studies showing an association with the medications and thyroid C–cell tumors.
Other FDA-approved medication options for obesity in children include metformin, topiramate, and phentermine, as well as bupropion, lisdexamfetamine, and setmelanotide, the authors said.
Resmetirom, a thyroid hormone receptor-beta agonist, which is another significant breakthrough in MASLD for adults, has not yet been tested or approved for pediatric use.
In addition to medications, metabolic bariatric surgery has shown effectiveness in children with obesity and/or MASLD by reducing liver fat and reversing fibrosis, as shown in the Teen-LABS study, the authors wrote. However, long-term data on fibrosis reversal are limited, and cost and access remain barriers.
More Research Needed
The joint expert review is intended as an educational tool that may require updates and should not be interpreted as rules for individual patient care, the authors cautioned. And physical activity and nutrition remain the primary treatment of MASLD and should be continued in conjunction with other treatment modalities, they emphasized.
Looking ahead, research is needed to develop accurate and reliable noninvasive biomarkers to diagnose and assess obesity treatment efficacy, Panganiban told GI & Hepatology News.
Also needed are multicenter randomized control trials in children with obesity involving different medications that have been successful in the treatment of metabolic dysfunction–associated steatohepatitis/fibrosis in adults, such as GLP-1 RAs or resmetirom, she added.
Educating Clinicians on Early Identification
When obesity occurs in childhood, it starts a process of additional complications that arise in earlier ages in adults, said Saul J. Karpen, MD, chief scientific officer at the Stravitz-Sanyal Institute for Liver Disease and Metabolic Health, Virginia Commonwealth University, Richmond, Virginia, in an interview.“Given the epidemic of obesity, altered diets, and reduced physical activities during younger ages, it is not easy to identify which children are at greater risk of MASLD,” said Karpen.
“It requires insight from the care providers and often imaging, a blood test, or a referral to a pediatric hepatologist, and not every region has easy access to such expertise,” Karpen said.
The new review is important because it highlights the fact that obesity and its consequences are not limited to adulthood, and that educated clinicians are in a position to get an early start on treatment in children, Karpen noted.
The guideline received no outside funding. Panganiban and Karpen had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Key Blood Proteins Predict MASLD Up to 16 Years in Advance
SAN DIEGO –
“This represents the first high-performance, ultra-early (16 years) predictive model for MASLD,” said first author Shiyi Yu, MD, resident physician in the department of gastroenterology, Guangdong Provincial People’s Hospital in China.
“The findings could be a game-changer for how we screen for and intervene in liver disease,” Yu said at a press briefing for Digestive Disease Week® (DDW) 2025.
“Instead of waiting for symptoms or irreversible damage, we can [identify] high-risk individuals early and take steps to prevent MASLD from developing, which is particularly important because MASLD often progresses silently until advanced stages,” she added.
MASLD is the most common liver disorder in the world and carries a high risk of morbidity and mortality, with a mortality rate that is doubled compared with those without MASLD.
To identify any long-term predictive markers that could be used in simple predictive models, Yu and colleagues evaluated data on 52,952 participants enrolled in the UK Biobank between 2006 and 2010 who did not have MASLD at baseline and were followed up for up to 16.6 years.
Overall, 782 participants were diagnosed with MASLD over the course of the study.
A total of 2,737 blood proteins were analyzed, and among them, the five that emerged as being robust predictive biomarkers for development of MASLD within 5 years included CDHR2 (area under the curve [AUC] = 0.825), FUOM (AUC = 0.815), KRT18 (AUC = 0.810), ACY1 (AUC = 0.803), and GGT1 (AUC = 0.797).
Deviations of the proteins in plasma concentrations were observed up to 16 years prior to MASLD onset, with higher levels of the proteins at baseline associated with up to a nearly 10-times higher risk of MASLD (hazard ratios, 7.05-9.81).
A combination of the five proteins was predictive of incident MASLD at all time frames, including at 5-years (AUC = 0.857), 10-years (AUC = 0.775), and at all time points (AUC = 0.758).
The combined proteins gained even stronger predictive performance when added to key clinical biomarkers such as BMI and daily exercise, with an accuracy of 90.4% at 5 years and 82.2% at 16 years, “surpassing all existing short-term prediction models,” Yu reported.
Similar results were observed with the predictive model in a separate, smaller cohort of 100 participants in China, “further supporting the robustness of the model and showing it can be effective across diverse populations,” she noted in the press briefing.
Potential for Interventions ‘Years Before’ Damage Begins
Yu underscored the potential benefits of informing patients of their risk of MASLD.
“Too often, people do not find out they are at risk for liver disease before they are diagnosed and coping with symptoms,” she said.
A protein-based risk score could “profoundly transform early intervention strategies, triggering personalized lifestyle interventions for high-risk individuals” she said.
With obesity, type 2 diabetes, and high cholesterol levels among key risk factors for MASLD, such personalized interventions could include “counseling on diet, physical activity, and other factors years before liver damage begins, potentially averting disease progression altogether,” Yu noted.
Instead of waiting for abnormal liver function tests or imaging findings, patients could receive more frequent monitoring with annual elastography or ultrasound, for example, she explained.
In addition, “knowing one’s individualized protein-based risk may be more effective than abstract measures such as BMI or liver enzymes in motivating patients, facilitating better patient engagement and adherence,” Yu said.While noting that more work is needed to understand the biology behind the biomarkers, Yu underscored that “this is a big step toward personalized prevention.”
“By finding at-risk patients early, we hope to help stop MASLD before it starts,” she concluded.
Predictive Performance Impressive
Commenting on the study at the press briefing, Loren A. Laine, MD, AGAF, professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine, New Haven, Conn., and council chair of DDW 2025, noted that — as far as AUCs go — even a ranking in the 80% range is considered good. “So, for this to have an accuracy up to the 90s indicates a really excellent [predictive] performance,” he explained.
Laine agreed that the study findings have “the potential value to identify individuals at increased risk,” allowing for early monitoring and interventions.
The interventions “could be either general, such as things like diet and lifestyle, or more specific,” based on the function of these proteins, he added.
Rotonya Carr, MD, the division head of gastroenterology at the University of Washington, Seattle, further highlighted the pressing need for better predictive tools in MASLD.
“The predictions are that if we don’t do anything, as many as 122 million people will be impacted by MASLD” in the US by 2050, she told GI & Hepatology News.
“So, I am very excited about this work because we really don’t have anything right now that predicts who is going to get MASLD,” she said. “We are going to need tools like this, where people have information about their future health in order to make decisions.”
MASLD is known to be a significant risk factor for cardiovascular disease (CVD), and Carr speculated that the findings could lead to the types of predictive tools already available for CVD.
“I see this as being akin to what cardiology has had for quite some time, where they have cardiovascular risk disease calculators in which patients or their physicians can enter data and then estimate their risk of developing cardiovascular disease over, for instance, 10 years,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer. Carr’s disclosures include relationships with Intercept and Novo Nordisk and research funding from Merck.
A version of this article appeared on Medscape.com.
SAN DIEGO –
“This represents the first high-performance, ultra-early (16 years) predictive model for MASLD,” said first author Shiyi Yu, MD, resident physician in the department of gastroenterology, Guangdong Provincial People’s Hospital in China.
“The findings could be a game-changer for how we screen for and intervene in liver disease,” Yu said at a press briefing for Digestive Disease Week® (DDW) 2025.
“Instead of waiting for symptoms or irreversible damage, we can [identify] high-risk individuals early and take steps to prevent MASLD from developing, which is particularly important because MASLD often progresses silently until advanced stages,” she added.
MASLD is the most common liver disorder in the world and carries a high risk of morbidity and mortality, with a mortality rate that is doubled compared with those without MASLD.
To identify any long-term predictive markers that could be used in simple predictive models, Yu and colleagues evaluated data on 52,952 participants enrolled in the UK Biobank between 2006 and 2010 who did not have MASLD at baseline and were followed up for up to 16.6 years.
Overall, 782 participants were diagnosed with MASLD over the course of the study.
A total of 2,737 blood proteins were analyzed, and among them, the five that emerged as being robust predictive biomarkers for development of MASLD within 5 years included CDHR2 (area under the curve [AUC] = 0.825), FUOM (AUC = 0.815), KRT18 (AUC = 0.810), ACY1 (AUC = 0.803), and GGT1 (AUC = 0.797).
Deviations of the proteins in plasma concentrations were observed up to 16 years prior to MASLD onset, with higher levels of the proteins at baseline associated with up to a nearly 10-times higher risk of MASLD (hazard ratios, 7.05-9.81).
A combination of the five proteins was predictive of incident MASLD at all time frames, including at 5-years (AUC = 0.857), 10-years (AUC = 0.775), and at all time points (AUC = 0.758).
The combined proteins gained even stronger predictive performance when added to key clinical biomarkers such as BMI and daily exercise, with an accuracy of 90.4% at 5 years and 82.2% at 16 years, “surpassing all existing short-term prediction models,” Yu reported.
Similar results were observed with the predictive model in a separate, smaller cohort of 100 participants in China, “further supporting the robustness of the model and showing it can be effective across diverse populations,” she noted in the press briefing.
Potential for Interventions ‘Years Before’ Damage Begins
Yu underscored the potential benefits of informing patients of their risk of MASLD.
“Too often, people do not find out they are at risk for liver disease before they are diagnosed and coping with symptoms,” she said.
A protein-based risk score could “profoundly transform early intervention strategies, triggering personalized lifestyle interventions for high-risk individuals” she said.
With obesity, type 2 diabetes, and high cholesterol levels among key risk factors for MASLD, such personalized interventions could include “counseling on diet, physical activity, and other factors years before liver damage begins, potentially averting disease progression altogether,” Yu noted.
Instead of waiting for abnormal liver function tests or imaging findings, patients could receive more frequent monitoring with annual elastography or ultrasound, for example, she explained.
In addition, “knowing one’s individualized protein-based risk may be more effective than abstract measures such as BMI or liver enzymes in motivating patients, facilitating better patient engagement and adherence,” Yu said.While noting that more work is needed to understand the biology behind the biomarkers, Yu underscored that “this is a big step toward personalized prevention.”
“By finding at-risk patients early, we hope to help stop MASLD before it starts,” she concluded.
Predictive Performance Impressive
Commenting on the study at the press briefing, Loren A. Laine, MD, AGAF, professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine, New Haven, Conn., and council chair of DDW 2025, noted that — as far as AUCs go — even a ranking in the 80% range is considered good. “So, for this to have an accuracy up to the 90s indicates a really excellent [predictive] performance,” he explained.
Laine agreed that the study findings have “the potential value to identify individuals at increased risk,” allowing for early monitoring and interventions.
The interventions “could be either general, such as things like diet and lifestyle, or more specific,” based on the function of these proteins, he added.
Rotonya Carr, MD, the division head of gastroenterology at the University of Washington, Seattle, further highlighted the pressing need for better predictive tools in MASLD.
“The predictions are that if we don’t do anything, as many as 122 million people will be impacted by MASLD” in the US by 2050, she told GI & Hepatology News.
“So, I am very excited about this work because we really don’t have anything right now that predicts who is going to get MASLD,” she said. “We are going to need tools like this, where people have information about their future health in order to make decisions.”
MASLD is known to be a significant risk factor for cardiovascular disease (CVD), and Carr speculated that the findings could lead to the types of predictive tools already available for CVD.
“I see this as being akin to what cardiology has had for quite some time, where they have cardiovascular risk disease calculators in which patients or their physicians can enter data and then estimate their risk of developing cardiovascular disease over, for instance, 10 years,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer. Carr’s disclosures include relationships with Intercept and Novo Nordisk and research funding from Merck.
A version of this article appeared on Medscape.com.
SAN DIEGO –
“This represents the first high-performance, ultra-early (16 years) predictive model for MASLD,” said first author Shiyi Yu, MD, resident physician in the department of gastroenterology, Guangdong Provincial People’s Hospital in China.
“The findings could be a game-changer for how we screen for and intervene in liver disease,” Yu said at a press briefing for Digestive Disease Week® (DDW) 2025.
“Instead of waiting for symptoms or irreversible damage, we can [identify] high-risk individuals early and take steps to prevent MASLD from developing, which is particularly important because MASLD often progresses silently until advanced stages,” she added.
MASLD is the most common liver disorder in the world and carries a high risk of morbidity and mortality, with a mortality rate that is doubled compared with those without MASLD.
To identify any long-term predictive markers that could be used in simple predictive models, Yu and colleagues evaluated data on 52,952 participants enrolled in the UK Biobank between 2006 and 2010 who did not have MASLD at baseline and were followed up for up to 16.6 years.
Overall, 782 participants were diagnosed with MASLD over the course of the study.
A total of 2,737 blood proteins were analyzed, and among them, the five that emerged as being robust predictive biomarkers for development of MASLD within 5 years included CDHR2 (area under the curve [AUC] = 0.825), FUOM (AUC = 0.815), KRT18 (AUC = 0.810), ACY1 (AUC = 0.803), and GGT1 (AUC = 0.797).
Deviations of the proteins in plasma concentrations were observed up to 16 years prior to MASLD onset, with higher levels of the proteins at baseline associated with up to a nearly 10-times higher risk of MASLD (hazard ratios, 7.05-9.81).
A combination of the five proteins was predictive of incident MASLD at all time frames, including at 5-years (AUC = 0.857), 10-years (AUC = 0.775), and at all time points (AUC = 0.758).
The combined proteins gained even stronger predictive performance when added to key clinical biomarkers such as BMI and daily exercise, with an accuracy of 90.4% at 5 years and 82.2% at 16 years, “surpassing all existing short-term prediction models,” Yu reported.
Similar results were observed with the predictive model in a separate, smaller cohort of 100 participants in China, “further supporting the robustness of the model and showing it can be effective across diverse populations,” she noted in the press briefing.
Potential for Interventions ‘Years Before’ Damage Begins
Yu underscored the potential benefits of informing patients of their risk of MASLD.
“Too often, people do not find out they are at risk for liver disease before they are diagnosed and coping with symptoms,” she said.
A protein-based risk score could “profoundly transform early intervention strategies, triggering personalized lifestyle interventions for high-risk individuals” she said.
With obesity, type 2 diabetes, and high cholesterol levels among key risk factors for MASLD, such personalized interventions could include “counseling on diet, physical activity, and other factors years before liver damage begins, potentially averting disease progression altogether,” Yu noted.
Instead of waiting for abnormal liver function tests or imaging findings, patients could receive more frequent monitoring with annual elastography or ultrasound, for example, she explained.
In addition, “knowing one’s individualized protein-based risk may be more effective than abstract measures such as BMI or liver enzymes in motivating patients, facilitating better patient engagement and adherence,” Yu said.While noting that more work is needed to understand the biology behind the biomarkers, Yu underscored that “this is a big step toward personalized prevention.”
“By finding at-risk patients early, we hope to help stop MASLD before it starts,” she concluded.
Predictive Performance Impressive
Commenting on the study at the press briefing, Loren A. Laine, MD, AGAF, professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine, New Haven, Conn., and council chair of DDW 2025, noted that — as far as AUCs go — even a ranking in the 80% range is considered good. “So, for this to have an accuracy up to the 90s indicates a really excellent [predictive] performance,” he explained.
Laine agreed that the study findings have “the potential value to identify individuals at increased risk,” allowing for early monitoring and interventions.
The interventions “could be either general, such as things like diet and lifestyle, or more specific,” based on the function of these proteins, he added.
Rotonya Carr, MD, the division head of gastroenterology at the University of Washington, Seattle, further highlighted the pressing need for better predictive tools in MASLD.
“The predictions are that if we don’t do anything, as many as 122 million people will be impacted by MASLD” in the US by 2050, she told GI & Hepatology News.
“So, I am very excited about this work because we really don’t have anything right now that predicts who is going to get MASLD,” she said. “We are going to need tools like this, where people have information about their future health in order to make decisions.”
MASLD is known to be a significant risk factor for cardiovascular disease (CVD), and Carr speculated that the findings could lead to the types of predictive tools already available for CVD.
“I see this as being akin to what cardiology has had for quite some time, where they have cardiovascular risk disease calculators in which patients or their physicians can enter data and then estimate their risk of developing cardiovascular disease over, for instance, 10 years,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer. Carr’s disclosures include relationships with Intercept and Novo Nordisk and research funding from Merck.
A version of this article appeared on Medscape.com.
FROM DDW 2025
A Practical Approach to Diagnosis and Management of Eosinophilic Esophagitis
Eosinophilic esophagitis (EoE) can be considered a “young” disease, with initial case series reported only about 30 years ago. Since that time, it has become a commonly encountered condition in both emergency and clinic settings. The most recent prevalence study estimates that 1 in 700 people in the U.S. have EoE,1 the volume of EoE-associated ED visits tripped between 2009 and 2019 and is projected to double again by 2030,2 and “new” gastroenterologists undoubtedly have learned about and seen this condition. As a chronic disease, EoE necessitates longitudinal follow-up and optimization of care to prevent complications. With increasing diagnostic delay, EoE progresses in most, but not all, patients from an inflammatory- to fibrostenotic-predominant condition.3
Diagnosis of EoE
The most likely area that you will encounter EoE is during an emergent middle-of-the-night endoscopy for food impaction. If called in for this, EoE will be the cause in more than 50% of patients.4 However, the diagnosis can only be made if esophageal biopsies are obtained at the time of the procedure. This is a critical time to decrease diagnostic delay, as half of patients are lost to follow-up after a food impaction.5 Unfortunately, although taking biopsies during index food impaction is guideline-recommended, a quality metric, and safe to obtain after the food bolus is cleared, this is infrequently done in practice.6, 7
The next most likely area for EoE detection is in the endoscopy suite where 15-23% of patients with dysphagia and 5-7% of patients undergoing upper endoscopy for any indication will have EoE.4 Sometimes EoE will be detected “incidentally” during an open-access case (for example, in a patient with diarrhea undergoing evaluation for celiac). In these cases, it is important to perform a careful history (as noted below) as subtle EoE symptoms can frequently be identified. Finally, when patients are seen in clinic for solid food dysphagia, EoE is clearly on the differential. A few percent of patients with refractory heartburn or chest pain will have EoE causing the symptoms rather than reflux,4 and all patients under consideration for antireflux surgery should have an endoscopy to assess for EoE.
When talking to patients with known or suspected EoE, the history must go beyond general questions about dysphagia or trouble swallowing. Many patients with EoE have overtly or subconsciously modified their eating behaviors over many years to minimize symptoms, may have adapted to chronic dysphagia, and will answer “no” when asked if they have trouble swallowing. Instead, use the acronym “IMPACT” to delve deeper into possible symptoms.8 Do they “Imbibe” fluids or liquids between each bite to help get food down? Do they “Modify” the way they eat (cut food into small bites; puree foods)? Do they “Prolong” mealtimes? Do they “Avoid” certain foods that stick? Do they “Chew’ until their food is a mush to get it down? And do they “Turn away” tablets or pills? Pill dysphagia is often a subtle symptom, and sometimes the only symptom elicited.
Additionally, it may be important to ask a partner or family member (if present) about their observations. They may provide insight (e.g. “yes – he chokes with every bite but never says it bothers him”) that the patient might not otherwise provide. The suspicion for EoE should also be increased in patients with concomitant atopic diseases and in those with a family history of dysphagia or who have family members needing esophageal dilation. It is important to remember that EoE can be seen across all ages, sexes, and races/ethnicities.
Diagnosis of EoE is based on the AGREE consensus,9 which is also echoed in the recently updated American College of Gastroenterology (ACG) guidelines.10 Diagnosis requires three steps. First, symptoms of esophageal dysfunction must be present. This will most typically be dysphagia in adolescents and adults, but symptoms are non-specific in children (e.g. poor growth and feeding, abdominal pain, vomiting, regurgitation, heartburn).
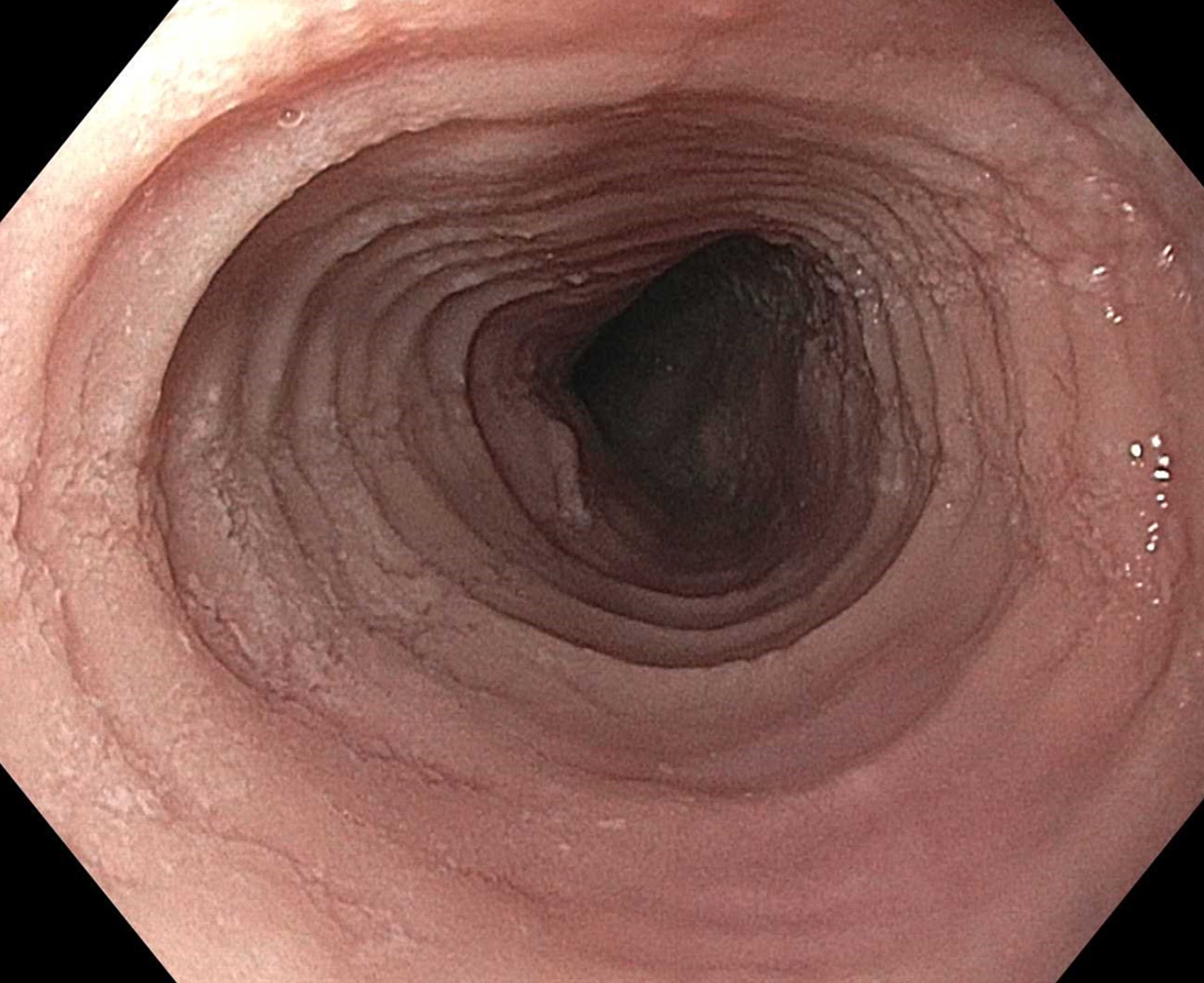
Second, at least 15 eosinophils per high-power field (eos/hpf) are required on esophageal biopsy, which implies that an endoscopy be performed. A high-quality endoscopic exam in EoE is of the utmost importance. The approach has been described elsewhere,11 but enough time on insertion should be taken to fully insufflate and examine the esophagus, including the areas of the gastroesophageal junction and upper esophageal sphincter where strictures can be missed, to gently wash debris, and to assess the endoscopic findings of EoE. Endoscopic findings should be reported using the validated EoE Endoscopy Reference Score (EREFS),12 which grades five key features. EREFS is reproducible, is responsive to treatment, and is guideline-recommended (see Figure 1).6, 10 The features are edema (present=1), rings (mild=1; moderate=2; severe=3), exudates (mild=1; severe=2), furrows (mild=1; severe=2), and stricture (present=1; also estimate diameter in mm) and are incorporated into many endoscopic reporting programs. Additionally, diffuse luminal narrowing and mucosal fragility (“crepe-paper” mucosa) should be assessed.
After this, biopsies should be obtained with at least 6 biopsy fragments from different locations in the esophagus. Any visible endoscopic abnormalities should be targeted (the highest yield is in exudates and furrows). The rationale is that EoE is patchy and at least 6 biopsies will maximize diagnostic yield.10 Ideally the initial endoscopy for EoE should be done off of treatments (like PPI or diet restriction) as these could mask the diagnosis. If a patient with suspected EoE has an endoscopy while on PPI, and the endoscopy is normal, a diagnosis of EoE cannot be made. In this case, consideration should be given as to stopping the PPI, allowing a wash out period (at least 1-2 months), and then repeating the endoscopy to confirm the diagnosis. This is important as EoE is a chronic condition necessitating life-long treatment and monitoring, so a definitive diagnosis is critical.
The third and final step in diagnosis is assessing for other conditions that could cause esophageal eosinophilia.9 The most common differential diagnosis is gastroesophageal reflux disease (GERD). In some cases, EoE and GERD overlap or can have a complex relationship.13 Unfortunately the location of the eosinophilia (i.e. distal only) and the level of the eosinophil counts are not useful in making this distinction, so all clinical features (symptoms, presence of erosive esophagitis, or a hiatal hernia endoscopically), and ancillary reflex testing when indicated may be required prior to a formal EoE diagnosis. After the diagnosis is established, there should be direct communication with the patient to review the diagnosis and select treatments. While it is possible to convey results electronically in a messaging portal or with a letter, a more formal interaction, such as a clinic visit, is recommended because this is a new diagnosis of a chronic condition. Similarly, a new diagnosis of inflammatory bowel disease would never be made in a pathology follow-up letter alone.
Treatment of EoE
When it comes to treatment, the new guidelines emphasize several points.10 First, there is the concept that anti-inflammatory treatment should be paired with assessment of fibrostenosis and esophageal dilation; to do either in isolation is incomplete treatment. It is safe to perform dilation both prior to anti-inflammatory treatment (for example, with a critical stricture in a patient with dysphagia) and after anti-inflammatory treatment has been prescribed (for example, during an endoscopy to assess treatment response).
Second, proton pump inhibitors (PPIs), swallowed topical corticosteroids (tCS), or dietary elimination are all acceptable first-line treatment options for EoE. A shared decision-making framework should be used for this discussion. If dietary elimination is selected,14 based on new clinical trial data, guidelines recommend using empiric elimination and starting with a less restrictive diet (either a one-food elimination diet with dairy alone or a two-food elimination with dairy and wheat elimination). If PPIs are selected, the dose should be double the standard reflux dose. Data are mixed as to whether to use twice daily dosing (i.e., omeprazole 20 mg twice daily) or once a day dosing (i.e., omeprazole 40 mg daily), but total dose and adherence may be more important than frequency.10
For tCS use, either budesonide or fluticasone can be selected, but budesonide oral suspension is the only FDA-approved tCS for EoE.15 Initial treatment length is usually 6-8 weeks for diet elimination and, 12 weeks for PPI and tCS. In general, it is best to pick a single treatment to start, and reserve combining therapies for patients who do not have a complete response to a single modality as there are few data to support combination therapy.
After initial treatment, it is critical to assess for treatment response.16 Goals of EoE treatment include improvement in symptoms, but also improvement in endoscopic and histologic features to prevent complications. Symptoms in EoE do not always correlate with underlying biologic disease activity: patients can minimize symptoms with careful eating; they may perceive no difference in symptoms despite histologic improvement if a stricture persists; and they may have minimal symptoms after esophageal dilation despite ongoing inflammation. Because of this, performing a follow-up endoscopy after initial treatment is guideline-recommended.10, 17 This allows assessing for endoscopic improvement, re-assessing for fibrostenosis and performing dilation if indicated, and obtaining esophageal biopsies. If there is non-response, options include switching between other first line treatments or considering “stepping-up” to dupilumab which is also an FDA-approved option for EoE that is recommended in the guidelines.10, 18 In some cases where patients have multiple severe atopic conditions such as asthma or eczema that would warrant dupilumab use, or if patients are intolerant to PPIs or tCS, dupilumab could be considered as an earlier treatment for EoE.
Long-Term Maintenance
If a patient has a good response (for example, improved symptoms, improved endoscopic features, and <15 eos/hpf on biopsy), treatment can be maintained long-term. In almost all cases, if treatment is stopped, EoE disease activity recurs.19 Patients could be seen back in clinic in 6-12 months, and then a discussion can be conducted about a follow-up endoscopy, with timing to be determined based on their individual disease features and severity.17
Patients with more severe strictures, however, may have to be seen in endoscopy for serial dilations. Continued follow-up is essential for optimal care. Just as patients can progress in their disease course with diagnostic delay, there are data that show they can also progress after diagnosis when there are gaps in care without regular follow-up.20 Unlike other chronic esophageal disorders such as GERD and Barrett’s esophagus and other chronic GI inflammatory conditions like inflammatory bowel disease, however, EoE is not associated with an increased risk of esophageal cancer.21, 22
Given its increasing frequency, EoE will be commonly encountered by gastroenterologists both new and established. Having a systematic approach for diagnosis, understanding how to elicit subtle symptoms, implementing a shared decision-making framework for treatment with a structured algorithm for assessing response, performing follow-up, maintaining treatment, and monitoring patients long-term will allow the large majority of EoE patients to be successfully managed.
Dr. Dellon is based at the Center for Esophageal Diseases and Swallowing, Center for Gastrointestinal Biology and Disease, Division of Gastroenterology and Hepatology, University of North Carolina School of Medicine, Chapel Hill. He disclosed research funding, consultant fees, and educational grants from multiple companies.
References
1. Thel HL, et al. Prevalence and Costs of Eosinophilic Esophagitis in the United States. Clin Gastroenterol Hepatol. 2025 Feb. doi: 10.1016/j.cgh.2024.09.031.
2. Lam AY, et al. Epidemiologic Burden and Projections for Eosinophilic Esophagitis-Associated Emergency Department Visits in the United States: 2009-2030. Clin Gastroenterol Hepatol. 2023 Nov. doi: 10.1016/j.cgh.2023.04.028.
3. Schoepfer AM, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013 Dec. doi: 10.1053/j.gastro.2013.08.015.
4. Dellon ES, Hirano I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology. 2018 Jan. doi: 10.1053/j.gastro.2017.06.067.
5. Chang JW, et al. Loss to follow-up after food impaction among patients with and without eosinophilic esophagitis. Dis Esophagus. 2019 Dec. doi: 10.1093/dote/doz056.
6. Aceves SS, et al. Endoscopic approach to eosinophilic esophagitis: American Society for Gastrointestinal Endoscopy Consensus Conference. Gastrointest Endosc. 2022 Aug. doi: 10.1016/j.gie.2022.05.013.
7. Leiman DA, et al. Quality Indicators for the Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2023 Jun. doi: 10.14309/ajg.0000000000002138.
8. Hirano I, Furuta GT. Approaches and Challenges to Management of Pediatric and Adult Patients With Eosinophilic Esophagitis. Gastroenterology. 2020 Mar. doi: 10.1053/j.gastro.2019.09.052.
9. Dellon ES, et al. Updated international consensus diagnostic criteria for eosinophilic esophagitis: Proceedings of the AGREE conference. Gastroenterology. 2018 Oct. doi: 10.1053/j.gastro.2018.07.009.
10. Dellon ES, et al. ACG Clinical Guideline: Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2025 Jan. doi: 10.14309/ajg.0000000000003194.
11. Dellon ES. Optimizing the Endoscopic Examination in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2021 Dec. doi: 10.1016/j.cgh.2021.07.011.
12. Hirano I, et al. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2012 May. doi: 10.1136/gutjnl-2011-301817.
13. Spechler SJ, et al. Thoughts on the complex relationship between gastroesophageal reflux disease and eosinophilic esophagitis. Am J Gastroenterol. 2007 Jun. doi: 10.1111/j.1572-0241.2007.01179.x.
14. Chang JW, et al. Development of a Practical Guide to Implement and Monitor Diet Therapy for Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2023 Jul. doi: 10.1016/j.cgh.2023.03.006.
15. Hirano I, et al. Budesonide Oral Suspension Improves Outcomes in Patients With Eosinophilic Esophagitis: Results from a Phase 3 Trial. Clin Gastroenterol Hepatol. 2022 Mar. doi: 10.1016/j.cgh.2021.04.022.
16. Dellon ES, Gupta SK. A conceptual approach to understanding treatment response in eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2019 Oct. doi: 10.1016/j.cgh.2019.01.030.
17. von Arnim U, et al. Monitoring Patients With Eosinophilic Esophagitis in Routine Clinical Practice - International Expert Recommendations. Clin Gastroenterol Hepatol. 2023 Sep. doi: 10.1016/j.cgh.2022.12.018.
18. Dellon ES, et al. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N Engl J Med. 2022 Dec. doi: 10.1056/NEJMoa220598.
19. Dellon ES, et al. Rapid Recurrence of Eosinophilic Esophagitis Activity After Successful Treatment in the Observation Phase of a Randomized, Double-Blind, Double-Dummy Trial. Clin Gastroenterol Hepatol. 2020 Jun. doi: 10.1016/j.cgh.2019.08.050.
20. Chang NC, et al. A Gap in Care Leads to Progression of Fibrosis in Eosinophilic Esophagitis Patients. Clin Gastroenterol Hepatol. 2022 Aug. doi: 10.1016/j.cgh.2021.10.028.
21. Syed A, et al. The relationship between eosinophilic esophagitis and esophageal cancer. Dis Esophagus. 2017 Jul. doi: 10.1093/dote/dox050.
22. Albaneze N, et al. No Association Between Eosinophilic Oesophagitis and Oesophageal Cancer in US Adults: A Case-Control Study. Aliment Pharmacol Ther. 2025 Jan. doi: 10.1111/apt.18431.
Eosinophilic esophagitis (EoE) can be considered a “young” disease, with initial case series reported only about 30 years ago. Since that time, it has become a commonly encountered condition in both emergency and clinic settings. The most recent prevalence study estimates that 1 in 700 people in the U.S. have EoE,1 the volume of EoE-associated ED visits tripped between 2009 and 2019 and is projected to double again by 2030,2 and “new” gastroenterologists undoubtedly have learned about and seen this condition. As a chronic disease, EoE necessitates longitudinal follow-up and optimization of care to prevent complications. With increasing diagnostic delay, EoE progresses in most, but not all, patients from an inflammatory- to fibrostenotic-predominant condition.3
Diagnosis of EoE
The most likely area that you will encounter EoE is during an emergent middle-of-the-night endoscopy for food impaction. If called in for this, EoE will be the cause in more than 50% of patients.4 However, the diagnosis can only be made if esophageal biopsies are obtained at the time of the procedure. This is a critical time to decrease diagnostic delay, as half of patients are lost to follow-up after a food impaction.5 Unfortunately, although taking biopsies during index food impaction is guideline-recommended, a quality metric, and safe to obtain after the food bolus is cleared, this is infrequently done in practice.6, 7
The next most likely area for EoE detection is in the endoscopy suite where 15-23% of patients with dysphagia and 5-7% of patients undergoing upper endoscopy for any indication will have EoE.4 Sometimes EoE will be detected “incidentally” during an open-access case (for example, in a patient with diarrhea undergoing evaluation for celiac). In these cases, it is important to perform a careful history (as noted below) as subtle EoE symptoms can frequently be identified. Finally, when patients are seen in clinic for solid food dysphagia, EoE is clearly on the differential. A few percent of patients with refractory heartburn or chest pain will have EoE causing the symptoms rather than reflux,4 and all patients under consideration for antireflux surgery should have an endoscopy to assess for EoE.
When talking to patients with known or suspected EoE, the history must go beyond general questions about dysphagia or trouble swallowing. Many patients with EoE have overtly or subconsciously modified their eating behaviors over many years to minimize symptoms, may have adapted to chronic dysphagia, and will answer “no” when asked if they have trouble swallowing. Instead, use the acronym “IMPACT” to delve deeper into possible symptoms.8 Do they “Imbibe” fluids or liquids between each bite to help get food down? Do they “Modify” the way they eat (cut food into small bites; puree foods)? Do they “Prolong” mealtimes? Do they “Avoid” certain foods that stick? Do they “Chew’ until their food is a mush to get it down? And do they “Turn away” tablets or pills? Pill dysphagia is often a subtle symptom, and sometimes the only symptom elicited.
Additionally, it may be important to ask a partner or family member (if present) about their observations. They may provide insight (e.g. “yes – he chokes with every bite but never says it bothers him”) that the patient might not otherwise provide. The suspicion for EoE should also be increased in patients with concomitant atopic diseases and in those with a family history of dysphagia or who have family members needing esophageal dilation. It is important to remember that EoE can be seen across all ages, sexes, and races/ethnicities.
Diagnosis of EoE is based on the AGREE consensus,9 which is also echoed in the recently updated American College of Gastroenterology (ACG) guidelines.10 Diagnosis requires three steps. First, symptoms of esophageal dysfunction must be present. This will most typically be dysphagia in adolescents and adults, but symptoms are non-specific in children (e.g. poor growth and feeding, abdominal pain, vomiting, regurgitation, heartburn).
Second, at least 15 eosinophils per high-power field (eos/hpf) are required on esophageal biopsy, which implies that an endoscopy be performed. A high-quality endoscopic exam in EoE is of the utmost importance. The approach has been described elsewhere,11 but enough time on insertion should be taken to fully insufflate and examine the esophagus, including the areas of the gastroesophageal junction and upper esophageal sphincter where strictures can be missed, to gently wash debris, and to assess the endoscopic findings of EoE. Endoscopic findings should be reported using the validated EoE Endoscopy Reference Score (EREFS),12 which grades five key features. EREFS is reproducible, is responsive to treatment, and is guideline-recommended (see Figure 1).6, 10 The features are edema (present=1), rings (mild=1; moderate=2; severe=3), exudates (mild=1; severe=2), furrows (mild=1; severe=2), and stricture (present=1; also estimate diameter in mm) and are incorporated into many endoscopic reporting programs. Additionally, diffuse luminal narrowing and mucosal fragility (“crepe-paper” mucosa) should be assessed.
After this, biopsies should be obtained with at least 6 biopsy fragments from different locations in the esophagus. Any visible endoscopic abnormalities should be targeted (the highest yield is in exudates and furrows). The rationale is that EoE is patchy and at least 6 biopsies will maximize diagnostic yield.10 Ideally the initial endoscopy for EoE should be done off of treatments (like PPI or diet restriction) as these could mask the diagnosis. If a patient with suspected EoE has an endoscopy while on PPI, and the endoscopy is normal, a diagnosis of EoE cannot be made. In this case, consideration should be given as to stopping the PPI, allowing a wash out period (at least 1-2 months), and then repeating the endoscopy to confirm the diagnosis. This is important as EoE is a chronic condition necessitating life-long treatment and monitoring, so a definitive diagnosis is critical.
The third and final step in diagnosis is assessing for other conditions that could cause esophageal eosinophilia.9 The most common differential diagnosis is gastroesophageal reflux disease (GERD). In some cases, EoE and GERD overlap or can have a complex relationship.13 Unfortunately the location of the eosinophilia (i.e. distal only) and the level of the eosinophil counts are not useful in making this distinction, so all clinical features (symptoms, presence of erosive esophagitis, or a hiatal hernia endoscopically), and ancillary reflex testing when indicated may be required prior to a formal EoE diagnosis. After the diagnosis is established, there should be direct communication with the patient to review the diagnosis and select treatments. While it is possible to convey results electronically in a messaging portal or with a letter, a more formal interaction, such as a clinic visit, is recommended because this is a new diagnosis of a chronic condition. Similarly, a new diagnosis of inflammatory bowel disease would never be made in a pathology follow-up letter alone.
Treatment of EoE
When it comes to treatment, the new guidelines emphasize several points.10 First, there is the concept that anti-inflammatory treatment should be paired with assessment of fibrostenosis and esophageal dilation; to do either in isolation is incomplete treatment. It is safe to perform dilation both prior to anti-inflammatory treatment (for example, with a critical stricture in a patient with dysphagia) and after anti-inflammatory treatment has been prescribed (for example, during an endoscopy to assess treatment response).
Second, proton pump inhibitors (PPIs), swallowed topical corticosteroids (tCS), or dietary elimination are all acceptable first-line treatment options for EoE. A shared decision-making framework should be used for this discussion. If dietary elimination is selected,14 based on new clinical trial data, guidelines recommend using empiric elimination and starting with a less restrictive diet (either a one-food elimination diet with dairy alone or a two-food elimination with dairy and wheat elimination). If PPIs are selected, the dose should be double the standard reflux dose. Data are mixed as to whether to use twice daily dosing (i.e., omeprazole 20 mg twice daily) or once a day dosing (i.e., omeprazole 40 mg daily), but total dose and adherence may be more important than frequency.10
For tCS use, either budesonide or fluticasone can be selected, but budesonide oral suspension is the only FDA-approved tCS for EoE.15 Initial treatment length is usually 6-8 weeks for diet elimination and, 12 weeks for PPI and tCS. In general, it is best to pick a single treatment to start, and reserve combining therapies for patients who do not have a complete response to a single modality as there are few data to support combination therapy.
After initial treatment, it is critical to assess for treatment response.16 Goals of EoE treatment include improvement in symptoms, but also improvement in endoscopic and histologic features to prevent complications. Symptoms in EoE do not always correlate with underlying biologic disease activity: patients can minimize symptoms with careful eating; they may perceive no difference in symptoms despite histologic improvement if a stricture persists; and they may have minimal symptoms after esophageal dilation despite ongoing inflammation. Because of this, performing a follow-up endoscopy after initial treatment is guideline-recommended.10, 17 This allows assessing for endoscopic improvement, re-assessing for fibrostenosis and performing dilation if indicated, and obtaining esophageal biopsies. If there is non-response, options include switching between other first line treatments or considering “stepping-up” to dupilumab which is also an FDA-approved option for EoE that is recommended in the guidelines.10, 18 In some cases where patients have multiple severe atopic conditions such as asthma or eczema that would warrant dupilumab use, or if patients are intolerant to PPIs or tCS, dupilumab could be considered as an earlier treatment for EoE.
Long-Term Maintenance
If a patient has a good response (for example, improved symptoms, improved endoscopic features, and <15 eos/hpf on biopsy), treatment can be maintained long-term. In almost all cases, if treatment is stopped, EoE disease activity recurs.19 Patients could be seen back in clinic in 6-12 months, and then a discussion can be conducted about a follow-up endoscopy, with timing to be determined based on their individual disease features and severity.17
Patients with more severe strictures, however, may have to be seen in endoscopy for serial dilations. Continued follow-up is essential for optimal care. Just as patients can progress in their disease course with diagnostic delay, there are data that show they can also progress after diagnosis when there are gaps in care without regular follow-up.20 Unlike other chronic esophageal disorders such as GERD and Barrett’s esophagus and other chronic GI inflammatory conditions like inflammatory bowel disease, however, EoE is not associated with an increased risk of esophageal cancer.21, 22
Given its increasing frequency, EoE will be commonly encountered by gastroenterologists both new and established. Having a systematic approach for diagnosis, understanding how to elicit subtle symptoms, implementing a shared decision-making framework for treatment with a structured algorithm for assessing response, performing follow-up, maintaining treatment, and monitoring patients long-term will allow the large majority of EoE patients to be successfully managed.
Dr. Dellon is based at the Center for Esophageal Diseases and Swallowing, Center for Gastrointestinal Biology and Disease, Division of Gastroenterology and Hepatology, University of North Carolina School of Medicine, Chapel Hill. He disclosed research funding, consultant fees, and educational grants from multiple companies.
References
1. Thel HL, et al. Prevalence and Costs of Eosinophilic Esophagitis in the United States. Clin Gastroenterol Hepatol. 2025 Feb. doi: 10.1016/j.cgh.2024.09.031.
2. Lam AY, et al. Epidemiologic Burden and Projections for Eosinophilic Esophagitis-Associated Emergency Department Visits in the United States: 2009-2030. Clin Gastroenterol Hepatol. 2023 Nov. doi: 10.1016/j.cgh.2023.04.028.
3. Schoepfer AM, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013 Dec. doi: 10.1053/j.gastro.2013.08.015.
4. Dellon ES, Hirano I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology. 2018 Jan. doi: 10.1053/j.gastro.2017.06.067.
5. Chang JW, et al. Loss to follow-up after food impaction among patients with and without eosinophilic esophagitis. Dis Esophagus. 2019 Dec. doi: 10.1093/dote/doz056.
6. Aceves SS, et al. Endoscopic approach to eosinophilic esophagitis: American Society for Gastrointestinal Endoscopy Consensus Conference. Gastrointest Endosc. 2022 Aug. doi: 10.1016/j.gie.2022.05.013.
7. Leiman DA, et al. Quality Indicators for the Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2023 Jun. doi: 10.14309/ajg.0000000000002138.
8. Hirano I, Furuta GT. Approaches and Challenges to Management of Pediatric and Adult Patients With Eosinophilic Esophagitis. Gastroenterology. 2020 Mar. doi: 10.1053/j.gastro.2019.09.052.
9. Dellon ES, et al. Updated international consensus diagnostic criteria for eosinophilic esophagitis: Proceedings of the AGREE conference. Gastroenterology. 2018 Oct. doi: 10.1053/j.gastro.2018.07.009.
10. Dellon ES, et al. ACG Clinical Guideline: Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2025 Jan. doi: 10.14309/ajg.0000000000003194.
11. Dellon ES. Optimizing the Endoscopic Examination in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2021 Dec. doi: 10.1016/j.cgh.2021.07.011.
12. Hirano I, et al. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2012 May. doi: 10.1136/gutjnl-2011-301817.
13. Spechler SJ, et al. Thoughts on the complex relationship between gastroesophageal reflux disease and eosinophilic esophagitis. Am J Gastroenterol. 2007 Jun. doi: 10.1111/j.1572-0241.2007.01179.x.
14. Chang JW, et al. Development of a Practical Guide to Implement and Monitor Diet Therapy for Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2023 Jul. doi: 10.1016/j.cgh.2023.03.006.
15. Hirano I, et al. Budesonide Oral Suspension Improves Outcomes in Patients With Eosinophilic Esophagitis: Results from a Phase 3 Trial. Clin Gastroenterol Hepatol. 2022 Mar. doi: 10.1016/j.cgh.2021.04.022.
16. Dellon ES, Gupta SK. A conceptual approach to understanding treatment response in eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2019 Oct. doi: 10.1016/j.cgh.2019.01.030.
17. von Arnim U, et al. Monitoring Patients With Eosinophilic Esophagitis in Routine Clinical Practice - International Expert Recommendations. Clin Gastroenterol Hepatol. 2023 Sep. doi: 10.1016/j.cgh.2022.12.018.
18. Dellon ES, et al. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N Engl J Med. 2022 Dec. doi: 10.1056/NEJMoa220598.
19. Dellon ES, et al. Rapid Recurrence of Eosinophilic Esophagitis Activity After Successful Treatment in the Observation Phase of a Randomized, Double-Blind, Double-Dummy Trial. Clin Gastroenterol Hepatol. 2020 Jun. doi: 10.1016/j.cgh.2019.08.050.
20. Chang NC, et al. A Gap in Care Leads to Progression of Fibrosis in Eosinophilic Esophagitis Patients. Clin Gastroenterol Hepatol. 2022 Aug. doi: 10.1016/j.cgh.2021.10.028.
21. Syed A, et al. The relationship between eosinophilic esophagitis and esophageal cancer. Dis Esophagus. 2017 Jul. doi: 10.1093/dote/dox050.
22. Albaneze N, et al. No Association Between Eosinophilic Oesophagitis and Oesophageal Cancer in US Adults: A Case-Control Study. Aliment Pharmacol Ther. 2025 Jan. doi: 10.1111/apt.18431.
Eosinophilic esophagitis (EoE) can be considered a “young” disease, with initial case series reported only about 30 years ago. Since that time, it has become a commonly encountered condition in both emergency and clinic settings. The most recent prevalence study estimates that 1 in 700 people in the U.S. have EoE,1 the volume of EoE-associated ED visits tripped between 2009 and 2019 and is projected to double again by 2030,2 and “new” gastroenterologists undoubtedly have learned about and seen this condition. As a chronic disease, EoE necessitates longitudinal follow-up and optimization of care to prevent complications. With increasing diagnostic delay, EoE progresses in most, but not all, patients from an inflammatory- to fibrostenotic-predominant condition.3
Diagnosis of EoE
The most likely area that you will encounter EoE is during an emergent middle-of-the-night endoscopy for food impaction. If called in for this, EoE will be the cause in more than 50% of patients.4 However, the diagnosis can only be made if esophageal biopsies are obtained at the time of the procedure. This is a critical time to decrease diagnostic delay, as half of patients are lost to follow-up after a food impaction.5 Unfortunately, although taking biopsies during index food impaction is guideline-recommended, a quality metric, and safe to obtain after the food bolus is cleared, this is infrequently done in practice.6, 7
The next most likely area for EoE detection is in the endoscopy suite where 15-23% of patients with dysphagia and 5-7% of patients undergoing upper endoscopy for any indication will have EoE.4 Sometimes EoE will be detected “incidentally” during an open-access case (for example, in a patient with diarrhea undergoing evaluation for celiac). In these cases, it is important to perform a careful history (as noted below) as subtle EoE symptoms can frequently be identified. Finally, when patients are seen in clinic for solid food dysphagia, EoE is clearly on the differential. A few percent of patients with refractory heartburn or chest pain will have EoE causing the symptoms rather than reflux,4 and all patients under consideration for antireflux surgery should have an endoscopy to assess for EoE.
When talking to patients with known or suspected EoE, the history must go beyond general questions about dysphagia or trouble swallowing. Many patients with EoE have overtly or subconsciously modified their eating behaviors over many years to minimize symptoms, may have adapted to chronic dysphagia, and will answer “no” when asked if they have trouble swallowing. Instead, use the acronym “IMPACT” to delve deeper into possible symptoms.8 Do they “Imbibe” fluids or liquids between each bite to help get food down? Do they “Modify” the way they eat (cut food into small bites; puree foods)? Do they “Prolong” mealtimes? Do they “Avoid” certain foods that stick? Do they “Chew’ until their food is a mush to get it down? And do they “Turn away” tablets or pills? Pill dysphagia is often a subtle symptom, and sometimes the only symptom elicited.
Additionally, it may be important to ask a partner or family member (if present) about their observations. They may provide insight (e.g. “yes – he chokes with every bite but never says it bothers him”) that the patient might not otherwise provide. The suspicion for EoE should also be increased in patients with concomitant atopic diseases and in those with a family history of dysphagia or who have family members needing esophageal dilation. It is important to remember that EoE can be seen across all ages, sexes, and races/ethnicities.
Diagnosis of EoE is based on the AGREE consensus,9 which is also echoed in the recently updated American College of Gastroenterology (ACG) guidelines.10 Diagnosis requires three steps. First, symptoms of esophageal dysfunction must be present. This will most typically be dysphagia in adolescents and adults, but symptoms are non-specific in children (e.g. poor growth and feeding, abdominal pain, vomiting, regurgitation, heartburn).
Second, at least 15 eosinophils per high-power field (eos/hpf) are required on esophageal biopsy, which implies that an endoscopy be performed. A high-quality endoscopic exam in EoE is of the utmost importance. The approach has been described elsewhere,11 but enough time on insertion should be taken to fully insufflate and examine the esophagus, including the areas of the gastroesophageal junction and upper esophageal sphincter where strictures can be missed, to gently wash debris, and to assess the endoscopic findings of EoE. Endoscopic findings should be reported using the validated EoE Endoscopy Reference Score (EREFS),12 which grades five key features. EREFS is reproducible, is responsive to treatment, and is guideline-recommended (see Figure 1).6, 10 The features are edema (present=1), rings (mild=1; moderate=2; severe=3), exudates (mild=1; severe=2), furrows (mild=1; severe=2), and stricture (present=1; also estimate diameter in mm) and are incorporated into many endoscopic reporting programs. Additionally, diffuse luminal narrowing and mucosal fragility (“crepe-paper” mucosa) should be assessed.
After this, biopsies should be obtained with at least 6 biopsy fragments from different locations in the esophagus. Any visible endoscopic abnormalities should be targeted (the highest yield is in exudates and furrows). The rationale is that EoE is patchy and at least 6 biopsies will maximize diagnostic yield.10 Ideally the initial endoscopy for EoE should be done off of treatments (like PPI or diet restriction) as these could mask the diagnosis. If a patient with suspected EoE has an endoscopy while on PPI, and the endoscopy is normal, a diagnosis of EoE cannot be made. In this case, consideration should be given as to stopping the PPI, allowing a wash out period (at least 1-2 months), and then repeating the endoscopy to confirm the diagnosis. This is important as EoE is a chronic condition necessitating life-long treatment and monitoring, so a definitive diagnosis is critical.
The third and final step in diagnosis is assessing for other conditions that could cause esophageal eosinophilia.9 The most common differential diagnosis is gastroesophageal reflux disease (GERD). In some cases, EoE and GERD overlap or can have a complex relationship.13 Unfortunately the location of the eosinophilia (i.e. distal only) and the level of the eosinophil counts are not useful in making this distinction, so all clinical features (symptoms, presence of erosive esophagitis, or a hiatal hernia endoscopically), and ancillary reflex testing when indicated may be required prior to a formal EoE diagnosis. After the diagnosis is established, there should be direct communication with the patient to review the diagnosis and select treatments. While it is possible to convey results electronically in a messaging portal or with a letter, a more formal interaction, such as a clinic visit, is recommended because this is a new diagnosis of a chronic condition. Similarly, a new diagnosis of inflammatory bowel disease would never be made in a pathology follow-up letter alone.
Treatment of EoE
When it comes to treatment, the new guidelines emphasize several points.10 First, there is the concept that anti-inflammatory treatment should be paired with assessment of fibrostenosis and esophageal dilation; to do either in isolation is incomplete treatment. It is safe to perform dilation both prior to anti-inflammatory treatment (for example, with a critical stricture in a patient with dysphagia) and after anti-inflammatory treatment has been prescribed (for example, during an endoscopy to assess treatment response).
Second, proton pump inhibitors (PPIs), swallowed topical corticosteroids (tCS), or dietary elimination are all acceptable first-line treatment options for EoE. A shared decision-making framework should be used for this discussion. If dietary elimination is selected,14 based on new clinical trial data, guidelines recommend using empiric elimination and starting with a less restrictive diet (either a one-food elimination diet with dairy alone or a two-food elimination with dairy and wheat elimination). If PPIs are selected, the dose should be double the standard reflux dose. Data are mixed as to whether to use twice daily dosing (i.e., omeprazole 20 mg twice daily) or once a day dosing (i.e., omeprazole 40 mg daily), but total dose and adherence may be more important than frequency.10
For tCS use, either budesonide or fluticasone can be selected, but budesonide oral suspension is the only FDA-approved tCS for EoE.15 Initial treatment length is usually 6-8 weeks for diet elimination and, 12 weeks for PPI and tCS. In general, it is best to pick a single treatment to start, and reserve combining therapies for patients who do not have a complete response to a single modality as there are few data to support combination therapy.
After initial treatment, it is critical to assess for treatment response.16 Goals of EoE treatment include improvement in symptoms, but also improvement in endoscopic and histologic features to prevent complications. Symptoms in EoE do not always correlate with underlying biologic disease activity: patients can minimize symptoms with careful eating; they may perceive no difference in symptoms despite histologic improvement if a stricture persists; and they may have minimal symptoms after esophageal dilation despite ongoing inflammation. Because of this, performing a follow-up endoscopy after initial treatment is guideline-recommended.10, 17 This allows assessing for endoscopic improvement, re-assessing for fibrostenosis and performing dilation if indicated, and obtaining esophageal biopsies. If there is non-response, options include switching between other first line treatments or considering “stepping-up” to dupilumab which is also an FDA-approved option for EoE that is recommended in the guidelines.10, 18 In some cases where patients have multiple severe atopic conditions such as asthma or eczema that would warrant dupilumab use, or if patients are intolerant to PPIs or tCS, dupilumab could be considered as an earlier treatment for EoE.
Long-Term Maintenance
If a patient has a good response (for example, improved symptoms, improved endoscopic features, and <15 eos/hpf on biopsy), treatment can be maintained long-term. In almost all cases, if treatment is stopped, EoE disease activity recurs.19 Patients could be seen back in clinic in 6-12 months, and then a discussion can be conducted about a follow-up endoscopy, with timing to be determined based on their individual disease features and severity.17
Patients with more severe strictures, however, may have to be seen in endoscopy for serial dilations. Continued follow-up is essential for optimal care. Just as patients can progress in their disease course with diagnostic delay, there are data that show they can also progress after diagnosis when there are gaps in care without regular follow-up.20 Unlike other chronic esophageal disorders such as GERD and Barrett’s esophagus and other chronic GI inflammatory conditions like inflammatory bowel disease, however, EoE is not associated with an increased risk of esophageal cancer.21, 22
Given its increasing frequency, EoE will be commonly encountered by gastroenterologists both new and established. Having a systematic approach for diagnosis, understanding how to elicit subtle symptoms, implementing a shared decision-making framework for treatment with a structured algorithm for assessing response, performing follow-up, maintaining treatment, and monitoring patients long-term will allow the large majority of EoE patients to be successfully managed.
Dr. Dellon is based at the Center for Esophageal Diseases and Swallowing, Center for Gastrointestinal Biology and Disease, Division of Gastroenterology and Hepatology, University of North Carolina School of Medicine, Chapel Hill. He disclosed research funding, consultant fees, and educational grants from multiple companies.
References
1. Thel HL, et al. Prevalence and Costs of Eosinophilic Esophagitis in the United States. Clin Gastroenterol Hepatol. 2025 Feb. doi: 10.1016/j.cgh.2024.09.031.
2. Lam AY, et al. Epidemiologic Burden and Projections for Eosinophilic Esophagitis-Associated Emergency Department Visits in the United States: 2009-2030. Clin Gastroenterol Hepatol. 2023 Nov. doi: 10.1016/j.cgh.2023.04.028.
3. Schoepfer AM, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013 Dec. doi: 10.1053/j.gastro.2013.08.015.
4. Dellon ES, Hirano I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology. 2018 Jan. doi: 10.1053/j.gastro.2017.06.067.
5. Chang JW, et al. Loss to follow-up after food impaction among patients with and without eosinophilic esophagitis. Dis Esophagus. 2019 Dec. doi: 10.1093/dote/doz056.
6. Aceves SS, et al. Endoscopic approach to eosinophilic esophagitis: American Society for Gastrointestinal Endoscopy Consensus Conference. Gastrointest Endosc. 2022 Aug. doi: 10.1016/j.gie.2022.05.013.
7. Leiman DA, et al. Quality Indicators for the Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2023 Jun. doi: 10.14309/ajg.0000000000002138.
8. Hirano I, Furuta GT. Approaches and Challenges to Management of Pediatric and Adult Patients With Eosinophilic Esophagitis. Gastroenterology. 2020 Mar. doi: 10.1053/j.gastro.2019.09.052.
9. Dellon ES, et al. Updated international consensus diagnostic criteria for eosinophilic esophagitis: Proceedings of the AGREE conference. Gastroenterology. 2018 Oct. doi: 10.1053/j.gastro.2018.07.009.
10. Dellon ES, et al. ACG Clinical Guideline: Diagnosis and Management of Eosinophilic Esophagitis. Am J Gastroenterol. 2025 Jan. doi: 10.14309/ajg.0000000000003194.
11. Dellon ES. Optimizing the Endoscopic Examination in Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2021 Dec. doi: 10.1016/j.cgh.2021.07.011.
12. Hirano I, et al. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2012 May. doi: 10.1136/gutjnl-2011-301817.
13. Spechler SJ, et al. Thoughts on the complex relationship between gastroesophageal reflux disease and eosinophilic esophagitis. Am J Gastroenterol. 2007 Jun. doi: 10.1111/j.1572-0241.2007.01179.x.
14. Chang JW, et al. Development of a Practical Guide to Implement and Monitor Diet Therapy for Eosinophilic Esophagitis. Clin Gastroenterol Hepatol. 2023 Jul. doi: 10.1016/j.cgh.2023.03.006.
15. Hirano I, et al. Budesonide Oral Suspension Improves Outcomes in Patients With Eosinophilic Esophagitis: Results from a Phase 3 Trial. Clin Gastroenterol Hepatol. 2022 Mar. doi: 10.1016/j.cgh.2021.04.022.
16. Dellon ES, Gupta SK. A conceptual approach to understanding treatment response in eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2019 Oct. doi: 10.1016/j.cgh.2019.01.030.
17. von Arnim U, et al. Monitoring Patients With Eosinophilic Esophagitis in Routine Clinical Practice - International Expert Recommendations. Clin Gastroenterol Hepatol. 2023 Sep. doi: 10.1016/j.cgh.2022.12.018.
18. Dellon ES, et al. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N Engl J Med. 2022 Dec. doi: 10.1056/NEJMoa220598.
19. Dellon ES, et al. Rapid Recurrence of Eosinophilic Esophagitis Activity After Successful Treatment in the Observation Phase of a Randomized, Double-Blind, Double-Dummy Trial. Clin Gastroenterol Hepatol. 2020 Jun. doi: 10.1016/j.cgh.2019.08.050.
20. Chang NC, et al. A Gap in Care Leads to Progression of Fibrosis in Eosinophilic Esophagitis Patients. Clin Gastroenterol Hepatol. 2022 Aug. doi: 10.1016/j.cgh.2021.10.028.
21. Syed A, et al. The relationship between eosinophilic esophagitis and esophageal cancer. Dis Esophagus. 2017 Jul. doi: 10.1093/dote/dox050.
22. Albaneze N, et al. No Association Between Eosinophilic Oesophagitis and Oesophageal Cancer in US Adults: A Case-Control Study. Aliment Pharmacol Ther. 2025 Jan. doi: 10.1111/apt.18431.
Four Key Genes Linked to Worse Gastric Cancer Outcomes
SAN DIEGO – that potentially paves the way for precision oncology and improved targeting of therapies.
“About a third of patients with gastric cancer in our study had somatic mutations or variants of uncertain significance in [one of] four key genes,” lead author Ulysses Ribeiro, MD, PhD, a professor of digestive system surgery at the University of São Paulo School of Medicine in São Paulo, Brazil, said in a press briefing for the study, presented at Digestive Disease Week® (DDW) 2025.
“These patients were more likely to have their cancer come back or to die from the disease, even after surgery and the best chemotherapy and immunotherapy regimens,” said Ribeiro. While treatment strategies in gastric cancer have improved in recent years, resistance to multiple drugs continues, and the 5-year overall survival rate remains low — about 36% — underscoring the critical need for targeted therapies.
In an effort to identify genetic alterations that could have prognostic value, Ribeiro and his colleagues used next-generation DNA sequencing to analyze 21 genes in the tumor samples of 87 patients with gastric cancer who had undergone curative surgery and chemotherapy at the Sao Paulo Cancer Institute, São Paulo, Brazil.
Using Cox regression analysis, they found pathogenic variants or variants of uncertain significance in the following four genes: BRCA2, CDH1, RHOA, and TP53. “We found that 33% of patients carried at least one of these four genes,” Ribeiro told GI & Hepatology News.
Individually, each of the four genes with pathogenic variants or variants of uncertain significance had significantly or near-significantly higher risks in a survival analysis vs wild-type or benign variants, including BRCA2 (hazard ratio [HR], 4.33; P = .030); CDH1 (HR, 7.54; P = .004); RHOA (HR, 29.24; P < .001); and TP53 (HR, 2.82; P = .07).
A further multivariate analysis adjusting for key confounders showed that, when combined, carriers of the genes had lower disease-free survival (P = .005) and worse overall survival (P = .009) than those with none of the mutations.
“Individually, all four genes were related to prognosis in our gastric cancer patients, and when combined, the genes had even a higher difference in prognosis, varying from 2 to 28 times higher,” Ribeiro said.
Overall, factors such as having a more advanced tumor, node, metastasis stage, pathological stage, and the presence of a pathogenic mutation or a variant of uncertain significance in the four genes in the model were independently associated with worse disease-free survival.
Familiar Genes
Some of these genes are highly familiar. BRCA2 is well-known for its role in increasing the risk for breast and ovarian cancers, and CDH1 is known to be associated with hereditary diffuse gastric cancer, which is the most common hereditary cancer syndrome linked to gastric cancer.
TP53, also known as the “guardian of the genome,” is the most commonly altered gene in human cancers, while RHOA is known to be involved in encoding the GTPase protein RhoA, which is key in the regulation of cell shape, motility, and other essential cellular processes.
“This is the first time that these four genes have been shown to strongly relate to these gastric cancer outcomes,” said Ribeiro. This suggests that there’s more than one pathway by which stomach cancer forms and that some stomach cancers are much more aggressive than others.
He noted that “patients without these high-risk mutations” could be given “less aggressive treatment, in some cases sparing them from unnecessary side effects.”
Speaking during the press briefing, Loren A. Laine, MD, AGAF, who is a professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine in New Haven, Connecticut, and council chair of DDW 2025, agreed that “certainly, if these genetic factors, along with other factors, predict risk, this also has implications in practice with respect to the level of monitoring during the follow-up and determining the need for therapy.”
In addition, “it will be interesting to see how much this adds to other known risk factors, such as pathologic stage,” said Laine.
A strength of this study, “which I think is unique, is that it looks at a Western population,” whereas data on gastric as well as esophageal cancer is heavily biased to Eastern regions like China and East Asia, where the rates are much higher than in the West, Alia Qureshi, MD, an associate professor of esophageal and gastric cancer surgery at Oregon Health & Science University in Portland, Oregon, told GI & Hepatology News.
While noting the limitation of the relatively small sample size, Qureshi said the study is nevertheless “exciting and moving the direction we want to go, specifically towards precision medicine [and] precision oncology.”
The study “builds on existing understanding, especially with regard to TP53 and CDH1, and it points to the opportunity to use this data in a way to direct patient care or possibly therapeutic intervention,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept Pharmaceuticals, Merck, and Pfizer. Qureshi had no disclosures to report.
A version of this article appeared on Medscape.com.
SAN DIEGO – that potentially paves the way for precision oncology and improved targeting of therapies.
“About a third of patients with gastric cancer in our study had somatic mutations or variants of uncertain significance in [one of] four key genes,” lead author Ulysses Ribeiro, MD, PhD, a professor of digestive system surgery at the University of São Paulo School of Medicine in São Paulo, Brazil, said in a press briefing for the study, presented at Digestive Disease Week® (DDW) 2025.
“These patients were more likely to have their cancer come back or to die from the disease, even after surgery and the best chemotherapy and immunotherapy regimens,” said Ribeiro. While treatment strategies in gastric cancer have improved in recent years, resistance to multiple drugs continues, and the 5-year overall survival rate remains low — about 36% — underscoring the critical need for targeted therapies.
In an effort to identify genetic alterations that could have prognostic value, Ribeiro and his colleagues used next-generation DNA sequencing to analyze 21 genes in the tumor samples of 87 patients with gastric cancer who had undergone curative surgery and chemotherapy at the Sao Paulo Cancer Institute, São Paulo, Brazil.
Using Cox regression analysis, they found pathogenic variants or variants of uncertain significance in the following four genes: BRCA2, CDH1, RHOA, and TP53. “We found that 33% of patients carried at least one of these four genes,” Ribeiro told GI & Hepatology News.
Individually, each of the four genes with pathogenic variants or variants of uncertain significance had significantly or near-significantly higher risks in a survival analysis vs wild-type or benign variants, including BRCA2 (hazard ratio [HR], 4.33; P = .030); CDH1 (HR, 7.54; P = .004); RHOA (HR, 29.24; P < .001); and TP53 (HR, 2.82; P = .07).
A further multivariate analysis adjusting for key confounders showed that, when combined, carriers of the genes had lower disease-free survival (P = .005) and worse overall survival (P = .009) than those with none of the mutations.
“Individually, all four genes were related to prognosis in our gastric cancer patients, and when combined, the genes had even a higher difference in prognosis, varying from 2 to 28 times higher,” Ribeiro said.
Overall, factors such as having a more advanced tumor, node, metastasis stage, pathological stage, and the presence of a pathogenic mutation or a variant of uncertain significance in the four genes in the model were independently associated with worse disease-free survival.
Familiar Genes
Some of these genes are highly familiar. BRCA2 is well-known for its role in increasing the risk for breast and ovarian cancers, and CDH1 is known to be associated with hereditary diffuse gastric cancer, which is the most common hereditary cancer syndrome linked to gastric cancer.
TP53, also known as the “guardian of the genome,” is the most commonly altered gene in human cancers, while RHOA is known to be involved in encoding the GTPase protein RhoA, which is key in the regulation of cell shape, motility, and other essential cellular processes.
“This is the first time that these four genes have been shown to strongly relate to these gastric cancer outcomes,” said Ribeiro. This suggests that there’s more than one pathway by which stomach cancer forms and that some stomach cancers are much more aggressive than others.
He noted that “patients without these high-risk mutations” could be given “less aggressive treatment, in some cases sparing them from unnecessary side effects.”
Speaking during the press briefing, Loren A. Laine, MD, AGAF, who is a professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine in New Haven, Connecticut, and council chair of DDW 2025, agreed that “certainly, if these genetic factors, along with other factors, predict risk, this also has implications in practice with respect to the level of monitoring during the follow-up and determining the need for therapy.”
In addition, “it will be interesting to see how much this adds to other known risk factors, such as pathologic stage,” said Laine.
A strength of this study, “which I think is unique, is that it looks at a Western population,” whereas data on gastric as well as esophageal cancer is heavily biased to Eastern regions like China and East Asia, where the rates are much higher than in the West, Alia Qureshi, MD, an associate professor of esophageal and gastric cancer surgery at Oregon Health & Science University in Portland, Oregon, told GI & Hepatology News.
While noting the limitation of the relatively small sample size, Qureshi said the study is nevertheless “exciting and moving the direction we want to go, specifically towards precision medicine [and] precision oncology.”
The study “builds on existing understanding, especially with regard to TP53 and CDH1, and it points to the opportunity to use this data in a way to direct patient care or possibly therapeutic intervention,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept Pharmaceuticals, Merck, and Pfizer. Qureshi had no disclosures to report.
A version of this article appeared on Medscape.com.
SAN DIEGO – that potentially paves the way for precision oncology and improved targeting of therapies.
“About a third of patients with gastric cancer in our study had somatic mutations or variants of uncertain significance in [one of] four key genes,” lead author Ulysses Ribeiro, MD, PhD, a professor of digestive system surgery at the University of São Paulo School of Medicine in São Paulo, Brazil, said in a press briefing for the study, presented at Digestive Disease Week® (DDW) 2025.
“These patients were more likely to have their cancer come back or to die from the disease, even after surgery and the best chemotherapy and immunotherapy regimens,” said Ribeiro. While treatment strategies in gastric cancer have improved in recent years, resistance to multiple drugs continues, and the 5-year overall survival rate remains low — about 36% — underscoring the critical need for targeted therapies.
In an effort to identify genetic alterations that could have prognostic value, Ribeiro and his colleagues used next-generation DNA sequencing to analyze 21 genes in the tumor samples of 87 patients with gastric cancer who had undergone curative surgery and chemotherapy at the Sao Paulo Cancer Institute, São Paulo, Brazil.
Using Cox regression analysis, they found pathogenic variants or variants of uncertain significance in the following four genes: BRCA2, CDH1, RHOA, and TP53. “We found that 33% of patients carried at least one of these four genes,” Ribeiro told GI & Hepatology News.
Individually, each of the four genes with pathogenic variants or variants of uncertain significance had significantly or near-significantly higher risks in a survival analysis vs wild-type or benign variants, including BRCA2 (hazard ratio [HR], 4.33; P = .030); CDH1 (HR, 7.54; P = .004); RHOA (HR, 29.24; P < .001); and TP53 (HR, 2.82; P = .07).
A further multivariate analysis adjusting for key confounders showed that, when combined, carriers of the genes had lower disease-free survival (P = .005) and worse overall survival (P = .009) than those with none of the mutations.
“Individually, all four genes were related to prognosis in our gastric cancer patients, and when combined, the genes had even a higher difference in prognosis, varying from 2 to 28 times higher,” Ribeiro said.
Overall, factors such as having a more advanced tumor, node, metastasis stage, pathological stage, and the presence of a pathogenic mutation or a variant of uncertain significance in the four genes in the model were independently associated with worse disease-free survival.
Familiar Genes
Some of these genes are highly familiar. BRCA2 is well-known for its role in increasing the risk for breast and ovarian cancers, and CDH1 is known to be associated with hereditary diffuse gastric cancer, which is the most common hereditary cancer syndrome linked to gastric cancer.
TP53, also known as the “guardian of the genome,” is the most commonly altered gene in human cancers, while RHOA is known to be involved in encoding the GTPase protein RhoA, which is key in the regulation of cell shape, motility, and other essential cellular processes.
“This is the first time that these four genes have been shown to strongly relate to these gastric cancer outcomes,” said Ribeiro. This suggests that there’s more than one pathway by which stomach cancer forms and that some stomach cancers are much more aggressive than others.
He noted that “patients without these high-risk mutations” could be given “less aggressive treatment, in some cases sparing them from unnecessary side effects.”
Speaking during the press briefing, Loren A. Laine, MD, AGAF, who is a professor of medicine and chief of the Section of Digestive Diseases at the Yale School of Medicine in New Haven, Connecticut, and council chair of DDW 2025, agreed that “certainly, if these genetic factors, along with other factors, predict risk, this also has implications in practice with respect to the level of monitoring during the follow-up and determining the need for therapy.”
In addition, “it will be interesting to see how much this adds to other known risk factors, such as pathologic stage,” said Laine.
A strength of this study, “which I think is unique, is that it looks at a Western population,” whereas data on gastric as well as esophageal cancer is heavily biased to Eastern regions like China and East Asia, where the rates are much higher than in the West, Alia Qureshi, MD, an associate professor of esophageal and gastric cancer surgery at Oregon Health & Science University in Portland, Oregon, told GI & Hepatology News.
While noting the limitation of the relatively small sample size, Qureshi said the study is nevertheless “exciting and moving the direction we want to go, specifically towards precision medicine [and] precision oncology.”
The study “builds on existing understanding, especially with regard to TP53 and CDH1, and it points to the opportunity to use this data in a way to direct patient care or possibly therapeutic intervention,” she said.
Laine’s disclosures include consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept Pharmaceuticals, Merck, and Pfizer. Qureshi had no disclosures to report.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Targeted CRC Outreach Doubles Screening Rates, Cuts Deaths by Half
SAN DIEGO — A 20-year initiative by Kaiser Permanente Northern California that assessed colorectal cancer (CRC) screening status and offered flexible options for screening has made a huge difference in CRC incidence, deaths, and racial disparities, an analysis showed.
“The program promptly doubled the proportion of people up to date with screening,” reported lead investigator Douglas A. Corley, MD, PhD, AGAF, a research scientist with Kaiser’s Division of Research, at a press briefing held on April 24, ahead of a presentation at the Digestive Disease Week® (DDW) 2025.

Additionally, , he said.
“Ten years ago, there were big gaps in cancer risk and death, especially among our Black patients. Now, those differences are nearly gone,” Corley said.
Closing the Gap
A systematic CRC screening program was implemented across Kaiser Permanente Northern California. The program included proactive outreach to members who were overdue for screening and mailing them fecal immunochemical test (FIT) kits for at-home use.
Corley and colleagues tracked screening status and CRC incidence and mortality annually from 2000 to 2019 among about 1.1 million members aged 50-75 years across 22 medical centers of the integrated healthcare system. The cohort included American Indian or Alaska Native, Asian, Black, Hispanic, Native Hawaiian or Pacific Islander, and White members.
Screening rates via FIT, colonoscopy, or sigmoidoscopy more than doubled after starting the program, from about 37% in the early years to about 80% within a few years, and it stayed that high through 2019, Corley reported.
“Importantly, these large increases occurred across the whole population with only small differences,” he said.
For example, about 76% of Hispanic members, 77% of Black members, 82% of White members, and 83% of Asian members were up to date in the later years and through 2019.
“This shows that systematic, comparable outreach can provide a level playing field for completion of preventive care,” Corley said.
After an expected early uptick in CRC incidence due to early detection, incidence later declined and by 2019 had dropped approximately 30% across the groups.
Long-Standing Disparities Erased
CRC deaths also fell by about 50% across all groups, with the largest decline among Black members, Corley noted.
Racial and ethnic disparities in both CRC incidence and mortality have long existed, with Black patients in particular experiencing higher risks and worse outcomes, likely from a mixture of risk factors and healthcare utilization, Corley said.
Offering outreach and equal access to screening in the Kaiser program erased those long-standing disparities.
“It’s remarkable that some of these large differences in mortality by race and ethnicity that we saw two decades ago, and which are found throughout the United States, are now similar to small chance variation in the population,” Corley said.
Flexibility was key to getting more people screened, he noted. “It’s about reaching people at their homes and offering a choice to patients. It’s an astonishingly simple concept.”
It’s important to note that these findings stem from a large, integrated healthcare system, which may differ from other settings, although similar outreach strategies have succeeded in safety net clinics and smaller practices, Corley added.
By boosting screening rates to 80%, the health system reached the level that’s essentially been defined in the past as our goal of screening programs, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Connecticut, and chair of this year’s DDW.

“It shows that if health systems institute programmatic screening for all their covered individuals, they could markedly increase screening, said Laine, who also served as moderator of the press briefing.
“Most importantly, of course, [screening] was associated with a reduction in colorectal cancer incidence and deaths,” he said.
The study had no commercial funding. Corley reported having no relevant conflicts of interest.
Laine’s disclosures included consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer.
A version of this article appeared on Medscape.com.
SAN DIEGO — A 20-year initiative by Kaiser Permanente Northern California that assessed colorectal cancer (CRC) screening status and offered flexible options for screening has made a huge difference in CRC incidence, deaths, and racial disparities, an analysis showed.
“The program promptly doubled the proportion of people up to date with screening,” reported lead investigator Douglas A. Corley, MD, PhD, AGAF, a research scientist with Kaiser’s Division of Research, at a press briefing held on April 24, ahead of a presentation at the Digestive Disease Week® (DDW) 2025.
Additionally, , he said.
“Ten years ago, there were big gaps in cancer risk and death, especially among our Black patients. Now, those differences are nearly gone,” Corley said.
Closing the Gap
A systematic CRC screening program was implemented across Kaiser Permanente Northern California. The program included proactive outreach to members who were overdue for screening and mailing them fecal immunochemical test (FIT) kits for at-home use.
Corley and colleagues tracked screening status and CRC incidence and mortality annually from 2000 to 2019 among about 1.1 million members aged 50-75 years across 22 medical centers of the integrated healthcare system. The cohort included American Indian or Alaska Native, Asian, Black, Hispanic, Native Hawaiian or Pacific Islander, and White members.
Screening rates via FIT, colonoscopy, or sigmoidoscopy more than doubled after starting the program, from about 37% in the early years to about 80% within a few years, and it stayed that high through 2019, Corley reported.
“Importantly, these large increases occurred across the whole population with only small differences,” he said.
For example, about 76% of Hispanic members, 77% of Black members, 82% of White members, and 83% of Asian members were up to date in the later years and through 2019.
“This shows that systematic, comparable outreach can provide a level playing field for completion of preventive care,” Corley said.
After an expected early uptick in CRC incidence due to early detection, incidence later declined and by 2019 had dropped approximately 30% across the groups.
Long-Standing Disparities Erased
CRC deaths also fell by about 50% across all groups, with the largest decline among Black members, Corley noted.
Racial and ethnic disparities in both CRC incidence and mortality have long existed, with Black patients in particular experiencing higher risks and worse outcomes, likely from a mixture of risk factors and healthcare utilization, Corley said.
Offering outreach and equal access to screening in the Kaiser program erased those long-standing disparities.
“It’s remarkable that some of these large differences in mortality by race and ethnicity that we saw two decades ago, and which are found throughout the United States, are now similar to small chance variation in the population,” Corley said.
Flexibility was key to getting more people screened, he noted. “It’s about reaching people at their homes and offering a choice to patients. It’s an astonishingly simple concept.”
It’s important to note that these findings stem from a large, integrated healthcare system, which may differ from other settings, although similar outreach strategies have succeeded in safety net clinics and smaller practices, Corley added.
By boosting screening rates to 80%, the health system reached the level that’s essentially been defined in the past as our goal of screening programs, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Connecticut, and chair of this year’s DDW.
“It shows that if health systems institute programmatic screening for all their covered individuals, they could markedly increase screening, said Laine, who also served as moderator of the press briefing.
“Most importantly, of course, [screening] was associated with a reduction in colorectal cancer incidence and deaths,” he said.
The study had no commercial funding. Corley reported having no relevant conflicts of interest.
Laine’s disclosures included consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer.
A version of this article appeared on Medscape.com.
SAN DIEGO — A 20-year initiative by Kaiser Permanente Northern California that assessed colorectal cancer (CRC) screening status and offered flexible options for screening has made a huge difference in CRC incidence, deaths, and racial disparities, an analysis showed.
“The program promptly doubled the proportion of people up to date with screening,” reported lead investigator Douglas A. Corley, MD, PhD, AGAF, a research scientist with Kaiser’s Division of Research, at a press briefing held on April 24, ahead of a presentation at the Digestive Disease Week® (DDW) 2025.
Additionally, , he said.
“Ten years ago, there were big gaps in cancer risk and death, especially among our Black patients. Now, those differences are nearly gone,” Corley said.
Closing the Gap
A systematic CRC screening program was implemented across Kaiser Permanente Northern California. The program included proactive outreach to members who were overdue for screening and mailing them fecal immunochemical test (FIT) kits for at-home use.
Corley and colleagues tracked screening status and CRC incidence and mortality annually from 2000 to 2019 among about 1.1 million members aged 50-75 years across 22 medical centers of the integrated healthcare system. The cohort included American Indian or Alaska Native, Asian, Black, Hispanic, Native Hawaiian or Pacific Islander, and White members.
Screening rates via FIT, colonoscopy, or sigmoidoscopy more than doubled after starting the program, from about 37% in the early years to about 80% within a few years, and it stayed that high through 2019, Corley reported.
“Importantly, these large increases occurred across the whole population with only small differences,” he said.
For example, about 76% of Hispanic members, 77% of Black members, 82% of White members, and 83% of Asian members were up to date in the later years and through 2019.
“This shows that systematic, comparable outreach can provide a level playing field for completion of preventive care,” Corley said.
After an expected early uptick in CRC incidence due to early detection, incidence later declined and by 2019 had dropped approximately 30% across the groups.
Long-Standing Disparities Erased
CRC deaths also fell by about 50% across all groups, with the largest decline among Black members, Corley noted.
Racial and ethnic disparities in both CRC incidence and mortality have long existed, with Black patients in particular experiencing higher risks and worse outcomes, likely from a mixture of risk factors and healthcare utilization, Corley said.
Offering outreach and equal access to screening in the Kaiser program erased those long-standing disparities.
“It’s remarkable that some of these large differences in mortality by race and ethnicity that we saw two decades ago, and which are found throughout the United States, are now similar to small chance variation in the population,” Corley said.
Flexibility was key to getting more people screened, he noted. “It’s about reaching people at their homes and offering a choice to patients. It’s an astonishingly simple concept.”
It’s important to note that these findings stem from a large, integrated healthcare system, which may differ from other settings, although similar outreach strategies have succeeded in safety net clinics and smaller practices, Corley added.
By boosting screening rates to 80%, the health system reached the level that’s essentially been defined in the past as our goal of screening programs, said Loren Laine, MD, AGAF, professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Connecticut, and chair of this year’s DDW.
“It shows that if health systems institute programmatic screening for all their covered individuals, they could markedly increase screening, said Laine, who also served as moderator of the press briefing.
“Most importantly, of course, [screening] was associated with a reduction in colorectal cancer incidence and deaths,” he said.
The study had no commercial funding. Corley reported having no relevant conflicts of interest.
Laine’s disclosures included consulting and/or relationships with Medtronic, Phathom Pharmaceuticals, Biohaven, Celgene, Intercept, Merck, and Pfizer.
A version of this article appeared on Medscape.com.
FROM DDW 2025
Salvage Rendezvous Technique on Par With Precut Sphincterotomy for Tough Biliary Access
, new data suggest.
Selective deep cannulation of the common bile duct remains the key rate-limiting step in successful endoscopic retrograde cholangiopancreatography (ERCP), especially in benign biliary disease.
In cases of difficult cannulation, the traditional fallback has been precut sphincterotomy. Recently, EUS-RV has emerged as an alternative. However, head-to-head comparisons of these salvage techniques in homogeneous patient populations have been lacking, until now.
A team led by Arup Choudhury, MD, DM, with Department of Gastroenterology, Postgraduate Institute of Medical Education and Research, Chandigarh, India, compared the two salvage techniques in a single-center, randomized controlled trial of 100 patients with benign biliary disease and difficult bile duct cannulation.
There were 50 patients in each group. When one technique failed, patients were crossed over to the other technique.
The technical success rate for achieving deep biliary, the primary outcome measure, was similar with EUS-RV and precut sphincterotomy (92% and 90%, respectively; P = 1.00; relative risk [RR], 1.02), the authors reported in Annals of Internal Medicine.
Median procedure time was also comparable (10.1 minutes with EUS-RV and 9.75 minutes with precut sphincterotomy). As expected, radiation exposure was notably higher in the EUS-RV group (median, 200.2 vs 67.8 mGy).
There was no difference in overall complication rates (12% and 10%, respectively; RR, 1.20).
Five patients in each group (10%) developed post-ERCP pancreatitis (PEP); one patient in the EUS-RV had moderately severe pancreatitis, whereas the rest had mild pancreatitis.
In an exploratory analysis of the subcohort of 72 patients who did not have 1 or more inadvertent pancreatic duct cannulation, two (5.6%) patients in the precut sphincterotomy group had PEP, whereas none of the patients in the EUS-RV had PEP (RR, 0.21). The investigators caution that a larger, multicenter, randomized controlled trial would be required to evaluate the “probable benefit” of lower PEP in the EUS-RV approach.
None of the patients had bleeding or perforation, but two (4%) patients in the EUS-RV group had an infection after the intervention. One required repeated ERCP due to post procedure cholangitis, whereas the other developed lower respiratory tract infection with transient acute lung injury and sputum showing gram-negative organism. None of the patients required surgical intervention.
“Interestingly,” said the investigators, on crossover from one salvage technique to the other, all of the cases could be successfully cannulated, suggesting the two salvage techniques are “complementary to each other and can help achieve successful cannulation in all cases when used in any sequence.”
Summing up, they said it appears from this head-to-head comparison that both EUS-RV and precut sphincterotomy can be considered effective salvage techniques in expert centers with similar safety and success profiles.
Limitations included the single-center design with both procedures performed by expert operators. EUS-RV entailed additional cost of needle and use of a separate scope, and a cost-efficacy analysis was not done.
This study had no specific funding. Disclosures for the authors are available with the original article.
A version of this article appeared on Medscape.com.
, new data suggest.
Selective deep cannulation of the common bile duct remains the key rate-limiting step in successful endoscopic retrograde cholangiopancreatography (ERCP), especially in benign biliary disease.
In cases of difficult cannulation, the traditional fallback has been precut sphincterotomy. Recently, EUS-RV has emerged as an alternative. However, head-to-head comparisons of these salvage techniques in homogeneous patient populations have been lacking, until now.
A team led by Arup Choudhury, MD, DM, with Department of Gastroenterology, Postgraduate Institute of Medical Education and Research, Chandigarh, India, compared the two salvage techniques in a single-center, randomized controlled trial of 100 patients with benign biliary disease and difficult bile duct cannulation.
There were 50 patients in each group. When one technique failed, patients were crossed over to the other technique.
The technical success rate for achieving deep biliary, the primary outcome measure, was similar with EUS-RV and precut sphincterotomy (92% and 90%, respectively; P = 1.00; relative risk [RR], 1.02), the authors reported in Annals of Internal Medicine.
Median procedure time was also comparable (10.1 minutes with EUS-RV and 9.75 minutes with precut sphincterotomy). As expected, radiation exposure was notably higher in the EUS-RV group (median, 200.2 vs 67.8 mGy).
There was no difference in overall complication rates (12% and 10%, respectively; RR, 1.20).
Five patients in each group (10%) developed post-ERCP pancreatitis (PEP); one patient in the EUS-RV had moderately severe pancreatitis, whereas the rest had mild pancreatitis.
In an exploratory analysis of the subcohort of 72 patients who did not have 1 or more inadvertent pancreatic duct cannulation, two (5.6%) patients in the precut sphincterotomy group had PEP, whereas none of the patients in the EUS-RV had PEP (RR, 0.21). The investigators caution that a larger, multicenter, randomized controlled trial would be required to evaluate the “probable benefit” of lower PEP in the EUS-RV approach.
None of the patients had bleeding or perforation, but two (4%) patients in the EUS-RV group had an infection after the intervention. One required repeated ERCP due to post procedure cholangitis, whereas the other developed lower respiratory tract infection with transient acute lung injury and sputum showing gram-negative organism. None of the patients required surgical intervention.
“Interestingly,” said the investigators, on crossover from one salvage technique to the other, all of the cases could be successfully cannulated, suggesting the two salvage techniques are “complementary to each other and can help achieve successful cannulation in all cases when used in any sequence.”
Summing up, they said it appears from this head-to-head comparison that both EUS-RV and precut sphincterotomy can be considered effective salvage techniques in expert centers with similar safety and success profiles.
Limitations included the single-center design with both procedures performed by expert operators. EUS-RV entailed additional cost of needle and use of a separate scope, and a cost-efficacy analysis was not done.
This study had no specific funding. Disclosures for the authors are available with the original article.
A version of this article appeared on Medscape.com.
, new data suggest.
Selective deep cannulation of the common bile duct remains the key rate-limiting step in successful endoscopic retrograde cholangiopancreatography (ERCP), especially in benign biliary disease.
In cases of difficult cannulation, the traditional fallback has been precut sphincterotomy. Recently, EUS-RV has emerged as an alternative. However, head-to-head comparisons of these salvage techniques in homogeneous patient populations have been lacking, until now.
A team led by Arup Choudhury, MD, DM, with Department of Gastroenterology, Postgraduate Institute of Medical Education and Research, Chandigarh, India, compared the two salvage techniques in a single-center, randomized controlled trial of 100 patients with benign biliary disease and difficult bile duct cannulation.
There were 50 patients in each group. When one technique failed, patients were crossed over to the other technique.
The technical success rate for achieving deep biliary, the primary outcome measure, was similar with EUS-RV and precut sphincterotomy (92% and 90%, respectively; P = 1.00; relative risk [RR], 1.02), the authors reported in Annals of Internal Medicine.
Median procedure time was also comparable (10.1 minutes with EUS-RV and 9.75 minutes with precut sphincterotomy). As expected, radiation exposure was notably higher in the EUS-RV group (median, 200.2 vs 67.8 mGy).
There was no difference in overall complication rates (12% and 10%, respectively; RR, 1.20).
Five patients in each group (10%) developed post-ERCP pancreatitis (PEP); one patient in the EUS-RV had moderately severe pancreatitis, whereas the rest had mild pancreatitis.
In an exploratory analysis of the subcohort of 72 patients who did not have 1 or more inadvertent pancreatic duct cannulation, two (5.6%) patients in the precut sphincterotomy group had PEP, whereas none of the patients in the EUS-RV had PEP (RR, 0.21). The investigators caution that a larger, multicenter, randomized controlled trial would be required to evaluate the “probable benefit” of lower PEP in the EUS-RV approach.
None of the patients had bleeding or perforation, but two (4%) patients in the EUS-RV group had an infection after the intervention. One required repeated ERCP due to post procedure cholangitis, whereas the other developed lower respiratory tract infection with transient acute lung injury and sputum showing gram-negative organism. None of the patients required surgical intervention.
“Interestingly,” said the investigators, on crossover from one salvage technique to the other, all of the cases could be successfully cannulated, suggesting the two salvage techniques are “complementary to each other and can help achieve successful cannulation in all cases when used in any sequence.”
Summing up, they said it appears from this head-to-head comparison that both EUS-RV and precut sphincterotomy can be considered effective salvage techniques in expert centers with similar safety and success profiles.
Limitations included the single-center design with both procedures performed by expert operators. EUS-RV entailed additional cost of needle and use of a separate scope, and a cost-efficacy analysis was not done.
This study had no specific funding. Disclosures for the authors are available with the original article.
A version of this article appeared on Medscape.com.
Clinicians Should Have Private Spaces for Telehealth According to VA Memo
US Department of Veterans Affairs (VA) officials are insisting that when remote telehealth clinicians return to an office setting, they must have private workspaces “that foster trusted, confidential, and therapeutic relationships with veterans,” according to an April internal memo reported on by NPR.
The return-to-office mandate followed a Trump Administration executive order in February indicated that mental health clinicians at the US Department of Veterans Affairs (VA) must physically return to their workplace by May 5. For some, the deadline came as early as April 14; however, that order, like many others, may now be being revised or reconsidered due to concerns that have been raised. Many mental health clinicians were hired specifically to work remotely. They worried there would simply not be enough space for them, particularly to provide confidential counseling.
Millions of veterans use telehealth to access VA care. More than 98% of VA mental health clinicians have conducted ≥ 1 video visit to screen and treat patients for anxiety, depression, posttraumatic stress disorder, and more. Telehealth has been particularly important for veterans living in rural communities.
The April VA memo stipulated that “spaces used to deliver synchronous telehealth services should offer the same level of privacy and therapeutic environment applicable to an in-person visit in the same space.”
Therapists, patients, advocacy groups, and lawmakers have expressed concern about the potential impacts the policy change could have on patient care for veterans and, above all, about what it could mean for privacy. On Mar. 27, the American Psychological Association issued a statement noting that the change “resulted in providers being asked to conduct sensitive therapy sessions in open office environments, cubicles, or shared spaces that fail to meet basic confidentiality and privacy requirements for the delivery of mental health care services.”
Twenty Democrats in the House of Representatives sent a letter to VA Secretary Doug Collins expressing concern with the return to office policy. According to the letter a VA social worker supervisor reported managing their caseload while sharing a 100 ft2 shower space with another supervisor. It also reported that Clinical Resource Hub employees were being told to report to buildings where federal employees from other agencies work. “We have heard from countless stakeholders, veterans, and Department of Veterans Affairs (VA) employees that by carrying out President Trump’s blanket return-to-office policy your administration is damaging veteran and employee trust in VA, disrupting and impeding veterans’ access to care, and creating untenable and inefficient conditions for both veterans and the VA workforce,” the letter stated.
“This is a clear violation of veterans’ privacy and VA’s obligation to protect veterans’ private health information, and risks violation of the Health Insurance Portability and Accountability Act (HIPAA),” the letter added.
The lawmakers noted that, as of March 10, the VA was exempting Veterans Crisis Line workers, most of whom had been working remotely for the past 5 years, responding to more than 10 million calls, texts, and chats. That move, they said, indicated “that you understand there will be negative impacts to veterans’ care due to the return-to-office order and that these must be mitigated.”
VA spokesperson Peter Kasperowicz called the privacy concerns “nonsensical” and blamed “fear mongering from the media.” The VA, he said, “is no longer a place where the status quo for employees is to simply phone it in from home.” He also claimed that “the small number of employees who are desperate to avoid returning to the office will do more to drive away staff and patients than VA’s commonsense return-to-office policy ever will.”
VA care, he said, would continue uninterrupted and the “VA will ensure that employees have a workspace that is appropriate for the work they do.”
US Department of Veterans Affairs (VA) officials are insisting that when remote telehealth clinicians return to an office setting, they must have private workspaces “that foster trusted, confidential, and therapeutic relationships with veterans,” according to an April internal memo reported on by NPR.
The return-to-office mandate followed a Trump Administration executive order in February indicated that mental health clinicians at the US Department of Veterans Affairs (VA) must physically return to their workplace by May 5. For some, the deadline came as early as April 14; however, that order, like many others, may now be being revised or reconsidered due to concerns that have been raised. Many mental health clinicians were hired specifically to work remotely. They worried there would simply not be enough space for them, particularly to provide confidential counseling.
Millions of veterans use telehealth to access VA care. More than 98% of VA mental health clinicians have conducted ≥ 1 video visit to screen and treat patients for anxiety, depression, posttraumatic stress disorder, and more. Telehealth has been particularly important for veterans living in rural communities.
The April VA memo stipulated that “spaces used to deliver synchronous telehealth services should offer the same level of privacy and therapeutic environment applicable to an in-person visit in the same space.”
Therapists, patients, advocacy groups, and lawmakers have expressed concern about the potential impacts the policy change could have on patient care for veterans and, above all, about what it could mean for privacy. On Mar. 27, the American Psychological Association issued a statement noting that the change “resulted in providers being asked to conduct sensitive therapy sessions in open office environments, cubicles, or shared spaces that fail to meet basic confidentiality and privacy requirements for the delivery of mental health care services.”
Twenty Democrats in the House of Representatives sent a letter to VA Secretary Doug Collins expressing concern with the return to office policy. According to the letter a VA social worker supervisor reported managing their caseload while sharing a 100 ft2 shower space with another supervisor. It also reported that Clinical Resource Hub employees were being told to report to buildings where federal employees from other agencies work. “We have heard from countless stakeholders, veterans, and Department of Veterans Affairs (VA) employees that by carrying out President Trump’s blanket return-to-office policy your administration is damaging veteran and employee trust in VA, disrupting and impeding veterans’ access to care, and creating untenable and inefficient conditions for both veterans and the VA workforce,” the letter stated.
“This is a clear violation of veterans’ privacy and VA’s obligation to protect veterans’ private health information, and risks violation of the Health Insurance Portability and Accountability Act (HIPAA),” the letter added.
The lawmakers noted that, as of March 10, the VA was exempting Veterans Crisis Line workers, most of whom had been working remotely for the past 5 years, responding to more than 10 million calls, texts, and chats. That move, they said, indicated “that you understand there will be negative impacts to veterans’ care due to the return-to-office order and that these must be mitigated.”
VA spokesperson Peter Kasperowicz called the privacy concerns “nonsensical” and blamed “fear mongering from the media.” The VA, he said, “is no longer a place where the status quo for employees is to simply phone it in from home.” He also claimed that “the small number of employees who are desperate to avoid returning to the office will do more to drive away staff and patients than VA’s commonsense return-to-office policy ever will.”
VA care, he said, would continue uninterrupted and the “VA will ensure that employees have a workspace that is appropriate for the work they do.”
US Department of Veterans Affairs (VA) officials are insisting that when remote telehealth clinicians return to an office setting, they must have private workspaces “that foster trusted, confidential, and therapeutic relationships with veterans,” according to an April internal memo reported on by NPR.
The return-to-office mandate followed a Trump Administration executive order in February indicated that mental health clinicians at the US Department of Veterans Affairs (VA) must physically return to their workplace by May 5. For some, the deadline came as early as April 14; however, that order, like many others, may now be being revised or reconsidered due to concerns that have been raised. Many mental health clinicians were hired specifically to work remotely. They worried there would simply not be enough space for them, particularly to provide confidential counseling.
Millions of veterans use telehealth to access VA care. More than 98% of VA mental health clinicians have conducted ≥ 1 video visit to screen and treat patients for anxiety, depression, posttraumatic stress disorder, and more. Telehealth has been particularly important for veterans living in rural communities.
The April VA memo stipulated that “spaces used to deliver synchronous telehealth services should offer the same level of privacy and therapeutic environment applicable to an in-person visit in the same space.”
Therapists, patients, advocacy groups, and lawmakers have expressed concern about the potential impacts the policy change could have on patient care for veterans and, above all, about what it could mean for privacy. On Mar. 27, the American Psychological Association issued a statement noting that the change “resulted in providers being asked to conduct sensitive therapy sessions in open office environments, cubicles, or shared spaces that fail to meet basic confidentiality and privacy requirements for the delivery of mental health care services.”
Twenty Democrats in the House of Representatives sent a letter to VA Secretary Doug Collins expressing concern with the return to office policy. According to the letter a VA social worker supervisor reported managing their caseload while sharing a 100 ft2 shower space with another supervisor. It also reported that Clinical Resource Hub employees were being told to report to buildings where federal employees from other agencies work. “We have heard from countless stakeholders, veterans, and Department of Veterans Affairs (VA) employees that by carrying out President Trump’s blanket return-to-office policy your administration is damaging veteran and employee trust in VA, disrupting and impeding veterans’ access to care, and creating untenable and inefficient conditions for both veterans and the VA workforce,” the letter stated.
“This is a clear violation of veterans’ privacy and VA’s obligation to protect veterans’ private health information, and risks violation of the Health Insurance Portability and Accountability Act (HIPAA),” the letter added.
The lawmakers noted that, as of March 10, the VA was exempting Veterans Crisis Line workers, most of whom had been working remotely for the past 5 years, responding to more than 10 million calls, texts, and chats. That move, they said, indicated “that you understand there will be negative impacts to veterans’ care due to the return-to-office order and that these must be mitigated.”
VA spokesperson Peter Kasperowicz called the privacy concerns “nonsensical” and blamed “fear mongering from the media.” The VA, he said, “is no longer a place where the status quo for employees is to simply phone it in from home.” He also claimed that “the small number of employees who are desperate to avoid returning to the office will do more to drive away staff and patients than VA’s commonsense return-to-office policy ever will.”
VA care, he said, would continue uninterrupted and the “VA will ensure that employees have a workspace that is appropriate for the work they do.”

Auto-Brewery Syndrome Explained: New Patient Cohort Identifies Culprit Bacteria, Fermentation
WASHINGTON — When a published case of auto-brewery syndrome (ABS) in China — caused by Klebsiella pneumoniae — received widespread publicity in 2019, patients reacted, sending emails to lead author Jing Yuan, in Beijing, China. Many of these inquiries were from patients in the United States who believed they might have ABS.
“Can you check to see if I have ABS?” patients asked Yuan.
For help, Yuan contacted Bernd Schnabl, MD, AGAF, at the University of California, San Diego, whose research was addressing alcohol-associated liver disease and who was also interested in the gut-liver axis and the role of gut microbiome–derived ethanol in metabolic dysfunction–associated steatotic liver disease (MASLD).
“She asked me, ‘Are you interested in looking into ABS?” Schnabl recalled at the Gut Microbiota for Health (GMFH) World Summit 2025. He dug in and formed what may be the largest research cohort thus far of patients with ABS — a group of 22 patients with their diagnosis confirmed through observed glucose challenge.
His soon-to-be-published
ABS is considered a rare condition, but “I’d argue that it’s rarely diagnosed because many physicians don’t know of the diagnosis, and many are actually very skeptical about the disease,” Schnabl said at the meeting, convened by AGA and the European Society of Neurogastroenterology and Motility.
Patients experience symptoms of intoxication when ethanol produced by dysregulated gut microbiota exceeds the capacity of the liver to metabolize it and accumulates in the blood, he explained.
“Patients constantly talk about brain fog; they can’t concentrate, and it can be very severe,” he said. “They don’t get a firm diagnosis and go from one medical center to another, and they also suffer from complications of alcohol use disorder including serious family, social, and legal problems.”
Advancing Knowledge, Findings From the Cohort
The phenomenon of ethanol production by gut microbiota has been known for over a century, Schnabl wrote with two co-authors in a 2024 review in Nature Reviews Gastroenterology & Hepatology of “endogenous ethanol production in health and disease.”
And in recent decades, he said at the meeting, research has linked endogenous ethanol production to MASLD, positioning it as a potential contributor to disease pathogenesis. In one of the most recently published studies, patients with MASLD had higher concentrations of ethanol in their systemic circulation after a mixed meal test than did healthy controls — and even higher ethanol concentrations in their portal vein blood, “suggesting that this ethanol is coming from the gut microbiome,” Schnabl said.
The paper from China that led Schnabl to establish his cohort was spurred on by a patient with both ABS and MASLD cirrhosis. The patient was found to have strains of high alcohol–producing K pneumoniae in the gut microbiome. When the researchers transplanted these strains into mice via fecal microbiota transplantation (FMT), the mice developed MASLD.
Schnabl’s study focused just on ABS, which is alternatively sometimes called gut fermentation syndrome. The 22 patients in his ABS cohort — each of whom provided stool samples corresponding to remission or flare of ABS symptoms — had a median age of 45 years and were predominantly men, slightly overweight and not obese, and without liver disease. (About 48 patients with suspected ABS were screened, and 20 were excluded after an observed glucose challenge failed to establish a diagnosis; 6 withdrew from the study.)
During remission (no symptoms), patients’ mean blood alcohol content (BAC) level was zero, but during a flare, the mean BAC level was 136 mg/dL. “To put it into perspective, the legal limit for driving in the US is 80 mg/dL,” Schnabl said. Within a mean of 4 hours after the oral glucose load used for diagnosis, patients’ mean BAC level was 73 mg/dL, he noted.
To assess ethanol production by the patients’ microbiota, Schnabl and his team cultured the stool samples — anaerobically adding glucose and measuring ethanol production — and compared the results with findings from stool samples collected from household partners who generally were of the opposite sex. Among their findings: cultures of stool from patients experiencing a flare produced significantly more ethanol than stool from household partners and samples from patients in remission.
To assess whether ethanol was produced by bacteria or fungi, the researchers measured ethanol production in cultures treated with either the antifungal amphotericin B or the antibiotic chloramphenicol. “Chloramphenicol clearly decreased the ethanol production,” Schnabl said. “So at least in this culture test, bacteria produced most of the alcohol in our patients.”
Taxonomic profiling, moreover, revealed “significantly elevated levels” of proteobacteria — with relative abundance of Escherichia coli and K pneumoniae — in patients who were flaring, he said. And functional profiling of the fecal microbiota showed much higher activity of fermentation pathways during patients’ flares than in household partners or healthy controls. (Healthy controls were incorporated into the taxonomic and functional profiling parts of the research.)
A Clinical Approach to ABS
Schnabl said at the meeting that stool cultures of both household partners and patients in long-term remission “all produced some low amount of ethanol, which was initially puzzling to us” but became less surprising as he and his colleagues reviewed more of the literature.
Asked during a discussion period whether ABS could explain chronic fatigue, a commonly reported chronic symptom in populations, Schnabl said it’s possible. And in an interview after the meeting, he elaborated. “The literature clearly says ABS is a rare disease, but I argue that more patients may have ABS; they just don’t know it. And I suspect some may have mild symptoms, like brain fog, feeling tired,” he said. “But at this point, this is complete speculation.”
Physicians should “be aware that if a patient has unexplained symptoms that could be aligned with ABS, checking the blood alcohol level” may be warranted, he said in the interview. A PEth (phosphatidylethanol) test — a biomarker test used to check for longer-term alcohol consumption — is an option, but it is important to appreciate it will not discriminate between exogenous alcohol drinking and endogenous ethanol production.
There are no standardized diagnostic tests for ABS, but at the meeting, Schnabl outlined a clinical approach, starting with a standardized oral glucose tolerance challenge test to detect elevated ethanol concentrations.
A fecal yeast test is warranted for diagnosed patients on the basis of some case reports in which ABS symptoms have improved with antifungal treatments. When the fecal yeast test is negative, “ideally you want to identify the ethanol-producing intestinal bacteria in the patient,” he said, using cultures and fecal metagenomics sequencing.
Treatment could then be tailored to the identified microbial strain, with options being selective antibiotics, probiotics and/or prebiotics, and — likely in the future — phages or FMT, he said. (These options, all aimed at restoring gut homeostasis, are also discussed in his 2024 review.)
Schnabl and his team recently performed FMT in a patient with ABS in whom E coli was determined to be producing excessive ethanol. The FMT, performed after antibiotic pretreatment, resulted in decreases in the relative abundance of proteobacteria and E coli levels, lower blood alcohol levels and fermentation enrichment pathways, and normalized liver enzymes.
After 6 months, however, the patient relapsed, and the measurements reversed. “We decided to do FMT every month, and we treated the patient for 6 months,” Schnabl said, noting that ABS had rendered the patient dysfunctional and unable to work. “He has been out of treatment for over a year now and is not flaring any longer.”
Schnabl and Elizabeth Hohmann, MD, at Massachusetts General Hospital, Boston, are currently recruiting patients with confirmed ABS for a National Institutes of Health–funded phase 1 safety and tolerability study of FMT for ABS.
Schnabl disclosed serving as an external scientific advisor/consultant to Ambys Medicines, Boehringer Ingelheim, Gelesis, Mabwell Therapeutics, Surrozen, and Takeda; and as the founder/BOD/BEO of Nterica Bio.
A version of this article appeared on Medscape.com.
WASHINGTON — When a published case of auto-brewery syndrome (ABS) in China — caused by Klebsiella pneumoniae — received widespread publicity in 2019, patients reacted, sending emails to lead author Jing Yuan, in Beijing, China. Many of these inquiries were from patients in the United States who believed they might have ABS.
“Can you check to see if I have ABS?” patients asked Yuan.
For help, Yuan contacted Bernd Schnabl, MD, AGAF, at the University of California, San Diego, whose research was addressing alcohol-associated liver disease and who was also interested in the gut-liver axis and the role of gut microbiome–derived ethanol in metabolic dysfunction–associated steatotic liver disease (MASLD).
“She asked me, ‘Are you interested in looking into ABS?” Schnabl recalled at the Gut Microbiota for Health (GMFH) World Summit 2025. He dug in and formed what may be the largest research cohort thus far of patients with ABS — a group of 22 patients with their diagnosis confirmed through observed glucose challenge.
His soon-to-be-published
ABS is considered a rare condition, but “I’d argue that it’s rarely diagnosed because many physicians don’t know of the diagnosis, and many are actually very skeptical about the disease,” Schnabl said at the meeting, convened by AGA and the European Society of Neurogastroenterology and Motility.
Patients experience symptoms of intoxication when ethanol produced by dysregulated gut microbiota exceeds the capacity of the liver to metabolize it and accumulates in the blood, he explained.
“Patients constantly talk about brain fog; they can’t concentrate, and it can be very severe,” he said. “They don’t get a firm diagnosis and go from one medical center to another, and they also suffer from complications of alcohol use disorder including serious family, social, and legal problems.”
Advancing Knowledge, Findings From the Cohort
The phenomenon of ethanol production by gut microbiota has been known for over a century, Schnabl wrote with two co-authors in a 2024 review in Nature Reviews Gastroenterology & Hepatology of “endogenous ethanol production in health and disease.”
And in recent decades, he said at the meeting, research has linked endogenous ethanol production to MASLD, positioning it as a potential contributor to disease pathogenesis. In one of the most recently published studies, patients with MASLD had higher concentrations of ethanol in their systemic circulation after a mixed meal test than did healthy controls — and even higher ethanol concentrations in their portal vein blood, “suggesting that this ethanol is coming from the gut microbiome,” Schnabl said.
The paper from China that led Schnabl to establish his cohort was spurred on by a patient with both ABS and MASLD cirrhosis. The patient was found to have strains of high alcohol–producing K pneumoniae in the gut microbiome. When the researchers transplanted these strains into mice via fecal microbiota transplantation (FMT), the mice developed MASLD.
Schnabl’s study focused just on ABS, which is alternatively sometimes called gut fermentation syndrome. The 22 patients in his ABS cohort — each of whom provided stool samples corresponding to remission or flare of ABS symptoms — had a median age of 45 years and were predominantly men, slightly overweight and not obese, and without liver disease. (About 48 patients with suspected ABS were screened, and 20 were excluded after an observed glucose challenge failed to establish a diagnosis; 6 withdrew from the study.)
During remission (no symptoms), patients’ mean blood alcohol content (BAC) level was zero, but during a flare, the mean BAC level was 136 mg/dL. “To put it into perspective, the legal limit for driving in the US is 80 mg/dL,” Schnabl said. Within a mean of 4 hours after the oral glucose load used for diagnosis, patients’ mean BAC level was 73 mg/dL, he noted.
To assess ethanol production by the patients’ microbiota, Schnabl and his team cultured the stool samples — anaerobically adding glucose and measuring ethanol production — and compared the results with findings from stool samples collected from household partners who generally were of the opposite sex. Among their findings: cultures of stool from patients experiencing a flare produced significantly more ethanol than stool from household partners and samples from patients in remission.
To assess whether ethanol was produced by bacteria or fungi, the researchers measured ethanol production in cultures treated with either the antifungal amphotericin B or the antibiotic chloramphenicol. “Chloramphenicol clearly decreased the ethanol production,” Schnabl said. “So at least in this culture test, bacteria produced most of the alcohol in our patients.”
Taxonomic profiling, moreover, revealed “significantly elevated levels” of proteobacteria — with relative abundance of Escherichia coli and K pneumoniae — in patients who were flaring, he said. And functional profiling of the fecal microbiota showed much higher activity of fermentation pathways during patients’ flares than in household partners or healthy controls. (Healthy controls were incorporated into the taxonomic and functional profiling parts of the research.)
A Clinical Approach to ABS
Schnabl said at the meeting that stool cultures of both household partners and patients in long-term remission “all produced some low amount of ethanol, which was initially puzzling to us” but became less surprising as he and his colleagues reviewed more of the literature.
Asked during a discussion period whether ABS could explain chronic fatigue, a commonly reported chronic symptom in populations, Schnabl said it’s possible. And in an interview after the meeting, he elaborated. “The literature clearly says ABS is a rare disease, but I argue that more patients may have ABS; they just don’t know it. And I suspect some may have mild symptoms, like brain fog, feeling tired,” he said. “But at this point, this is complete speculation.”
Physicians should “be aware that if a patient has unexplained symptoms that could be aligned with ABS, checking the blood alcohol level” may be warranted, he said in the interview. A PEth (phosphatidylethanol) test — a biomarker test used to check for longer-term alcohol consumption — is an option, but it is important to appreciate it will not discriminate between exogenous alcohol drinking and endogenous ethanol production.
There are no standardized diagnostic tests for ABS, but at the meeting, Schnabl outlined a clinical approach, starting with a standardized oral glucose tolerance challenge test to detect elevated ethanol concentrations.
A fecal yeast test is warranted for diagnosed patients on the basis of some case reports in which ABS symptoms have improved with antifungal treatments. When the fecal yeast test is negative, “ideally you want to identify the ethanol-producing intestinal bacteria in the patient,” he said, using cultures and fecal metagenomics sequencing.
Treatment could then be tailored to the identified microbial strain, with options being selective antibiotics, probiotics and/or prebiotics, and — likely in the future — phages or FMT, he said. (These options, all aimed at restoring gut homeostasis, are also discussed in his 2024 review.)
Schnabl and his team recently performed FMT in a patient with ABS in whom E coli was determined to be producing excessive ethanol. The FMT, performed after antibiotic pretreatment, resulted in decreases in the relative abundance of proteobacteria and E coli levels, lower blood alcohol levels and fermentation enrichment pathways, and normalized liver enzymes.
After 6 months, however, the patient relapsed, and the measurements reversed. “We decided to do FMT every month, and we treated the patient for 6 months,” Schnabl said, noting that ABS had rendered the patient dysfunctional and unable to work. “He has been out of treatment for over a year now and is not flaring any longer.”
Schnabl and Elizabeth Hohmann, MD, at Massachusetts General Hospital, Boston, are currently recruiting patients with confirmed ABS for a National Institutes of Health–funded phase 1 safety and tolerability study of FMT for ABS.
Schnabl disclosed serving as an external scientific advisor/consultant to Ambys Medicines, Boehringer Ingelheim, Gelesis, Mabwell Therapeutics, Surrozen, and Takeda; and as the founder/BOD/BEO of Nterica Bio.
A version of this article appeared on Medscape.com.
WASHINGTON — When a published case of auto-brewery syndrome (ABS) in China — caused by Klebsiella pneumoniae — received widespread publicity in 2019, patients reacted, sending emails to lead author Jing Yuan, in Beijing, China. Many of these inquiries were from patients in the United States who believed they might have ABS.
“Can you check to see if I have ABS?” patients asked Yuan.
For help, Yuan contacted Bernd Schnabl, MD, AGAF, at the University of California, San Diego, whose research was addressing alcohol-associated liver disease and who was also interested in the gut-liver axis and the role of gut microbiome–derived ethanol in metabolic dysfunction–associated steatotic liver disease (MASLD).
“She asked me, ‘Are you interested in looking into ABS?” Schnabl recalled at the Gut Microbiota for Health (GMFH) World Summit 2025. He dug in and formed what may be the largest research cohort thus far of patients with ABS — a group of 22 patients with their diagnosis confirmed through observed glucose challenge.
His soon-to-be-published
ABS is considered a rare condition, but “I’d argue that it’s rarely diagnosed because many physicians don’t know of the diagnosis, and many are actually very skeptical about the disease,” Schnabl said at the meeting, convened by AGA and the European Society of Neurogastroenterology and Motility.
Patients experience symptoms of intoxication when ethanol produced by dysregulated gut microbiota exceeds the capacity of the liver to metabolize it and accumulates in the blood, he explained.
“Patients constantly talk about brain fog; they can’t concentrate, and it can be very severe,” he said. “They don’t get a firm diagnosis and go from one medical center to another, and they also suffer from complications of alcohol use disorder including serious family, social, and legal problems.”
Advancing Knowledge, Findings From the Cohort
The phenomenon of ethanol production by gut microbiota has been known for over a century, Schnabl wrote with two co-authors in a 2024 review in Nature Reviews Gastroenterology & Hepatology of “endogenous ethanol production in health and disease.”
And in recent decades, he said at the meeting, research has linked endogenous ethanol production to MASLD, positioning it as a potential contributor to disease pathogenesis. In one of the most recently published studies, patients with MASLD had higher concentrations of ethanol in their systemic circulation after a mixed meal test than did healthy controls — and even higher ethanol concentrations in their portal vein blood, “suggesting that this ethanol is coming from the gut microbiome,” Schnabl said.
The paper from China that led Schnabl to establish his cohort was spurred on by a patient with both ABS and MASLD cirrhosis. The patient was found to have strains of high alcohol–producing K pneumoniae in the gut microbiome. When the researchers transplanted these strains into mice via fecal microbiota transplantation (FMT), the mice developed MASLD.
Schnabl’s study focused just on ABS, which is alternatively sometimes called gut fermentation syndrome. The 22 patients in his ABS cohort — each of whom provided stool samples corresponding to remission or flare of ABS symptoms — had a median age of 45 years and were predominantly men, slightly overweight and not obese, and without liver disease. (About 48 patients with suspected ABS were screened, and 20 were excluded after an observed glucose challenge failed to establish a diagnosis; 6 withdrew from the study.)
During remission (no symptoms), patients’ mean blood alcohol content (BAC) level was zero, but during a flare, the mean BAC level was 136 mg/dL. “To put it into perspective, the legal limit for driving in the US is 80 mg/dL,” Schnabl said. Within a mean of 4 hours after the oral glucose load used for diagnosis, patients’ mean BAC level was 73 mg/dL, he noted.
To assess ethanol production by the patients’ microbiota, Schnabl and his team cultured the stool samples — anaerobically adding glucose and measuring ethanol production — and compared the results with findings from stool samples collected from household partners who generally were of the opposite sex. Among their findings: cultures of stool from patients experiencing a flare produced significantly more ethanol than stool from household partners and samples from patients in remission.
To assess whether ethanol was produced by bacteria or fungi, the researchers measured ethanol production in cultures treated with either the antifungal amphotericin B or the antibiotic chloramphenicol. “Chloramphenicol clearly decreased the ethanol production,” Schnabl said. “So at least in this culture test, bacteria produced most of the alcohol in our patients.”
Taxonomic profiling, moreover, revealed “significantly elevated levels” of proteobacteria — with relative abundance of Escherichia coli and K pneumoniae — in patients who were flaring, he said. And functional profiling of the fecal microbiota showed much higher activity of fermentation pathways during patients’ flares than in household partners or healthy controls. (Healthy controls were incorporated into the taxonomic and functional profiling parts of the research.)
A Clinical Approach to ABS
Schnabl said at the meeting that stool cultures of both household partners and patients in long-term remission “all produced some low amount of ethanol, which was initially puzzling to us” but became less surprising as he and his colleagues reviewed more of the literature.
Asked during a discussion period whether ABS could explain chronic fatigue, a commonly reported chronic symptom in populations, Schnabl said it’s possible. And in an interview after the meeting, he elaborated. “The literature clearly says ABS is a rare disease, but I argue that more patients may have ABS; they just don’t know it. And I suspect some may have mild symptoms, like brain fog, feeling tired,” he said. “But at this point, this is complete speculation.”
Physicians should “be aware that if a patient has unexplained symptoms that could be aligned with ABS, checking the blood alcohol level” may be warranted, he said in the interview. A PEth (phosphatidylethanol) test — a biomarker test used to check for longer-term alcohol consumption — is an option, but it is important to appreciate it will not discriminate between exogenous alcohol drinking and endogenous ethanol production.
There are no standardized diagnostic tests for ABS, but at the meeting, Schnabl outlined a clinical approach, starting with a standardized oral glucose tolerance challenge test to detect elevated ethanol concentrations.
A fecal yeast test is warranted for diagnosed patients on the basis of some case reports in which ABS symptoms have improved with antifungal treatments. When the fecal yeast test is negative, “ideally you want to identify the ethanol-producing intestinal bacteria in the patient,” he said, using cultures and fecal metagenomics sequencing.
Treatment could then be tailored to the identified microbial strain, with options being selective antibiotics, probiotics and/or prebiotics, and — likely in the future — phages or FMT, he said. (These options, all aimed at restoring gut homeostasis, are also discussed in his 2024 review.)
Schnabl and his team recently performed FMT in a patient with ABS in whom E coli was determined to be producing excessive ethanol. The FMT, performed after antibiotic pretreatment, resulted in decreases in the relative abundance of proteobacteria and E coli levels, lower blood alcohol levels and fermentation enrichment pathways, and normalized liver enzymes.
After 6 months, however, the patient relapsed, and the measurements reversed. “We decided to do FMT every month, and we treated the patient for 6 months,” Schnabl said, noting that ABS had rendered the patient dysfunctional and unable to work. “He has been out of treatment for over a year now and is not flaring any longer.”
Schnabl and Elizabeth Hohmann, MD, at Massachusetts General Hospital, Boston, are currently recruiting patients with confirmed ABS for a National Institutes of Health–funded phase 1 safety and tolerability study of FMT for ABS.
Schnabl disclosed serving as an external scientific advisor/consultant to Ambys Medicines, Boehringer Ingelheim, Gelesis, Mabwell Therapeutics, Surrozen, and Takeda; and as the founder/BOD/BEO of Nterica Bio.
A version of this article appeared on Medscape.com.
FROM GMFH 2025
Early Warning Signs: Catching Gastric Cancer in Time
Hello. I’m Dr. David Johnson, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School and Old Dominion University in Norfolk, Virginia.
The American College of Gastroenterology (ACG) recently issued a clinical guideline on the diagnosis and management of gastric premalignant conditions.
Coincidentally, earlier this year, the ACG and the American Society for Gastrointestinal Endoscopy (ASGE) collaborated to issue recommendations on quality indicators for upper endoscopy.
In this overview, I’ll focus on gastric premalignant conditions while drawing upon some of the quality indicators from ACG/ASGE. Together, these publications highlight several things that we may be overlooking and clearly need to do better at addressing, given the emerging data in this area.
Gastric Premalignant Conditions: Increased Risk for Progression
Gastric premalignant conditions are common and include atrophic gastritis, gastric intestinal metaplasia, dysplasia, and certain gastric epithelial polyps.
The increased risk for progression to gastric adenocarcinoma in the United States is quite striking. It also reveals an important cancer disparity in certain high-risk groups.
The incidence rates of gastric cancer are two- to 13-fold greater in non-White individuals, particularly among immigrants from high-risk areas. The rates exceed those for esophageal cancer and approach those for colorectal cancer. We have had a dramatic oversight in recognizing the risk for gastric carcinoma in underserved areas.
Gastric carcinoma is not a good diagnosis. The 5-year survival rate is 36%. Approximately 40% of cases are metastatic at the time of diagnosis; only about 15% are caught at a curable early stage.
These rates are in far contrast to Asia and areas that do programmatic screening, where the numbers are dramatically reduced. However, in the United States, we’re simply not there yet.
Endoscopic Evaluation
There are three phases of endoscopic evaluation for gastric premalignant conditions on which I’d like to focus: pre-endoscopy, intra-endoscopy, and post-endoscopy.
Pre-endoscopy — that is, before you even put in the endoscope — it’s important to assess patients’ potential risk for certain conditions, regardless of the reason for performing the endoscopy.
Gastric carcinoma is in the top eight leading causes of cancer death in the United States, with the risk being particularly high in Hispanics and Asians.
According to 2020 data, 40 million people living in the United States were born in another country, with over 70% coming from areas that have a high incidence of gastric carcinoma.
Accounting for the increased risk in these groups will become even more important. By 2065, it is projected that Asian and Hispanic individuals — the immigrant groups with the highest risk for gastric cancer — will comprise 70% of the US population. Therefore, we need to do a better job on pre-endoscopic assessment if we want to address this major cancer disparity in the United States.
However, it’s a potentially fixable problem because, in most cases, gastric carcinoma is preceded by a typical asymptomatic precancerous cascade known as the “Correa’s cascade.” It is analogous to what we see in Barrett’s esophagus or even in colorectal neoplasia as it evolves.
This histologic cascade is important to recognize in patients before they get to the stage of progression. Doing so is highly dependent on the assessment prior to the endoscopy.
You should also be thinking about high-risk groups before a pre-endoscopy evaluation.
During intra-endoscopy, it’s important to plan your actions while performing the procedure, even if you are not specifically screening for gastric carcinoma. We must be held accountable to established recommendations, standards, and best practices for accurately defining observations, determining appropriate actions, and effectively implementing screening protocols.
A high-quality evaluation of the gastric mucosa is critically important, as an estimated 5%-11% of neoplastic lesions are missed on upper endoscopy completed within 3 years of a gastric cancer diagnosis. With less-experienced endoscopists, the rate of missed neoplastic lesions may be as high as 25%.
A quality endoscopy begins (as it would in the colon) with mucosal cleaning. This may not be achieved by water alone and requires the use of mucolytic and defoaming agents, such as simethicone or N-acetylcysteine, which can be inordinately helpful.
Complete mucosal evaluation entails using insufflation to adequately distend the gastric folds.
Atrophic gastritis is observed in a high percentage of patients, and I’m always on the lookout for it when performing endoscopies. One way to identify atrophic gastritis is to look for the loss of gastric folds, which has an approximate sensitivity of 67% and specificity of 85%. The increased visibility of the submucosal venules is another sign of atrophic gastritis, although its sensitivity and specificity are relatively lower at 48% and 87%, respectively.
Full photo documentation of the gastric mucosa should be included. It is an important part of the intra-endoscopy procedure and also is mentioned as part of the recently published quality indicators for upper endoscopy from ACG/ASGE.
Recognizing which patients require a biopsy is important. Appropriate biopsy samples should be obtained in patients with recognizable abnormalities. We’re often looking for changes that may be quite subtle. Dysplasia and even adenocarcinoma in the stomach sometimes just cannot be appreciated based on pure endoscopic evaluation.
When it comes to the biopsy protocol, the recommendation is to follow the Sydney system, which was developed in the 1990s. Simply put, this protocol calls for the biopsy samples to be obtained and placed in two separate jars. You look at the greater and lesser curvature of the antrum and the incisura (jar one), and the greater and lesser curvature of the corpus (jar two) in any identified incidental focused biopsy. This is what we do in the colon and the esophagus.
You should do this after you appropriately clean the mucosa and distend the gastric lumen, ideally using CO2, to avoid the retention of gas.
Time is another important quality measure. This is similar to the colon, where we see that withdrawal times have increased from 6 minutes to 8-9 minutes. In the stomach, there were initial data about a minimum of 2-3 minutes. However, more recent data in the ACG guideline and the ACG/ASGE quality indicators indicate that detection rates increase after mucosal clearance and dissension when the gastric evaluation is 6-7 minutes. These are numbers we need to pay attention to. The ACG guideline notes that a 2- to 3-minute withdrawal time for upper endoscopy is substandard and not acceptable. If you’re still at that level, then you’re below the standard of care.
Again, consider time and photo documentation while examining four to six specific areas of both the greater and lesser curvature of the antrum and corpus, and the incisura angularis. It is ideal to use high-definition endoscopy along with the available virtual imaging enhancers. This is the basic requirement for achieving high-quality assessments.
When it comes to post-endoscopy, it’s essential to talk to your pathologist about using validated instruments of reporting what gastric precancerous lesions involve. There are two different systems: the Operative Link for Gastritis Assessment (OLGA) and the Operative Link on Gastric Intestinal Metaplasia (OLGIM). Although not routinely used in the United States, they are the best recommendations we have for validated histologic scoring systems.
Your pathologist needs to be up to speed on understanding how to report the extent of intestinal metaplasia (complete, incomplete, and mixed) and identifying the areas of focality or abnormalities. It defines what the subsequent surveillance recommendations should be.
Know What’s Required
Let’s review what’s required when it comes to diagnosing and managing gastric premalignant conditions.
First, pre-endoscopy must involve the assessment of risk. Before we put in the endoscope, it’s critical to know, regardless of why the patient is there, who needs to be assessed for gastric premalignant conditions.
Second, during the intra-endoscopy phase, don’t forget the assessments and documentation. If you’re assessing for gastric intestinal metaplasia, use the Sydney system.
Time is a big component. Withdrawal times are discussed much more frequently now, with the takeaway being that longer is better. Aiming for 6-7 minutes is best, according to recommendations from international endoscopy societies and quality measures from the United States. The ACG guideline says that withdrawal times of 2-3 minutes are not best practice and fall short of standard of care.
For post-endoscopy, talk to your pathologist to ensure better communication and understanding. Make sure that you have a quality gastrointestinal pathologist interpreting these lesions so patients can either enter surveillance or discontinue surveillance after potentially two exams negative for evidence of progressive change.
To do better, we need to understand these guidelines, which are all applicable now.
I’m Dr. David Johnson. Thanks for listening. See you next time.
David A. Johnson, MD, a regular contributor to Medscape, is professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, Virginia, and a past president of the American College of Gastroenterology. His primary focus is the clinical practice of gastroenterology. He has published extensively in the internal medicine/gastroenterology literature, with principal research interests in esophageal and colon disease, and more recently in sleep and microbiome effects on gastrointestinal health and disease.
He has disclosed the relevant financial relationships: Advisor to ISOTHRIVE.
A version of this article first appeared on Medscape.com.
Hello. I’m Dr. David Johnson, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School and Old Dominion University in Norfolk, Virginia.
The American College of Gastroenterology (ACG) recently issued a clinical guideline on the diagnosis and management of gastric premalignant conditions.
Coincidentally, earlier this year, the ACG and the American Society for Gastrointestinal Endoscopy (ASGE) collaborated to issue recommendations on quality indicators for upper endoscopy.
In this overview, I’ll focus on gastric premalignant conditions while drawing upon some of the quality indicators from ACG/ASGE. Together, these publications highlight several things that we may be overlooking and clearly need to do better at addressing, given the emerging data in this area.
Gastric Premalignant Conditions: Increased Risk for Progression
Gastric premalignant conditions are common and include atrophic gastritis, gastric intestinal metaplasia, dysplasia, and certain gastric epithelial polyps.
The increased risk for progression to gastric adenocarcinoma in the United States is quite striking. It also reveals an important cancer disparity in certain high-risk groups.
The incidence rates of gastric cancer are two- to 13-fold greater in non-White individuals, particularly among immigrants from high-risk areas. The rates exceed those for esophageal cancer and approach those for colorectal cancer. We have had a dramatic oversight in recognizing the risk for gastric carcinoma in underserved areas.
Gastric carcinoma is not a good diagnosis. The 5-year survival rate is 36%. Approximately 40% of cases are metastatic at the time of diagnosis; only about 15% are caught at a curable early stage.
These rates are in far contrast to Asia and areas that do programmatic screening, where the numbers are dramatically reduced. However, in the United States, we’re simply not there yet.
Endoscopic Evaluation
There are three phases of endoscopic evaluation for gastric premalignant conditions on which I’d like to focus: pre-endoscopy, intra-endoscopy, and post-endoscopy.
Pre-endoscopy — that is, before you even put in the endoscope — it’s important to assess patients’ potential risk for certain conditions, regardless of the reason for performing the endoscopy.
Gastric carcinoma is in the top eight leading causes of cancer death in the United States, with the risk being particularly high in Hispanics and Asians.
According to 2020 data, 40 million people living in the United States were born in another country, with over 70% coming from areas that have a high incidence of gastric carcinoma.
Accounting for the increased risk in these groups will become even more important. By 2065, it is projected that Asian and Hispanic individuals — the immigrant groups with the highest risk for gastric cancer — will comprise 70% of the US population. Therefore, we need to do a better job on pre-endoscopic assessment if we want to address this major cancer disparity in the United States.
However, it’s a potentially fixable problem because, in most cases, gastric carcinoma is preceded by a typical asymptomatic precancerous cascade known as the “Correa’s cascade.” It is analogous to what we see in Barrett’s esophagus or even in colorectal neoplasia as it evolves.
This histologic cascade is important to recognize in patients before they get to the stage of progression. Doing so is highly dependent on the assessment prior to the endoscopy.
You should also be thinking about high-risk groups before a pre-endoscopy evaluation.
During intra-endoscopy, it’s important to plan your actions while performing the procedure, even if you are not specifically screening for gastric carcinoma. We must be held accountable to established recommendations, standards, and best practices for accurately defining observations, determining appropriate actions, and effectively implementing screening protocols.
A high-quality evaluation of the gastric mucosa is critically important, as an estimated 5%-11% of neoplastic lesions are missed on upper endoscopy completed within 3 years of a gastric cancer diagnosis. With less-experienced endoscopists, the rate of missed neoplastic lesions may be as high as 25%.
A quality endoscopy begins (as it would in the colon) with mucosal cleaning. This may not be achieved by water alone and requires the use of mucolytic and defoaming agents, such as simethicone or N-acetylcysteine, which can be inordinately helpful.
Complete mucosal evaluation entails using insufflation to adequately distend the gastric folds.
Atrophic gastritis is observed in a high percentage of patients, and I’m always on the lookout for it when performing endoscopies. One way to identify atrophic gastritis is to look for the loss of gastric folds, which has an approximate sensitivity of 67% and specificity of 85%. The increased visibility of the submucosal venules is another sign of atrophic gastritis, although its sensitivity and specificity are relatively lower at 48% and 87%, respectively.
Full photo documentation of the gastric mucosa should be included. It is an important part of the intra-endoscopy procedure and also is mentioned as part of the recently published quality indicators for upper endoscopy from ACG/ASGE.
Recognizing which patients require a biopsy is important. Appropriate biopsy samples should be obtained in patients with recognizable abnormalities. We’re often looking for changes that may be quite subtle. Dysplasia and even adenocarcinoma in the stomach sometimes just cannot be appreciated based on pure endoscopic evaluation.
When it comes to the biopsy protocol, the recommendation is to follow the Sydney system, which was developed in the 1990s. Simply put, this protocol calls for the biopsy samples to be obtained and placed in two separate jars. You look at the greater and lesser curvature of the antrum and the incisura (jar one), and the greater and lesser curvature of the corpus (jar two) in any identified incidental focused biopsy. This is what we do in the colon and the esophagus.
You should do this after you appropriately clean the mucosa and distend the gastric lumen, ideally using CO2, to avoid the retention of gas.
Time is another important quality measure. This is similar to the colon, where we see that withdrawal times have increased from 6 minutes to 8-9 minutes. In the stomach, there were initial data about a minimum of 2-3 minutes. However, more recent data in the ACG guideline and the ACG/ASGE quality indicators indicate that detection rates increase after mucosal clearance and dissension when the gastric evaluation is 6-7 minutes. These are numbers we need to pay attention to. The ACG guideline notes that a 2- to 3-minute withdrawal time for upper endoscopy is substandard and not acceptable. If you’re still at that level, then you’re below the standard of care.
Again, consider time and photo documentation while examining four to six specific areas of both the greater and lesser curvature of the antrum and corpus, and the incisura angularis. It is ideal to use high-definition endoscopy along with the available virtual imaging enhancers. This is the basic requirement for achieving high-quality assessments.
When it comes to post-endoscopy, it’s essential to talk to your pathologist about using validated instruments of reporting what gastric precancerous lesions involve. There are two different systems: the Operative Link for Gastritis Assessment (OLGA) and the Operative Link on Gastric Intestinal Metaplasia (OLGIM). Although not routinely used in the United States, they are the best recommendations we have for validated histologic scoring systems.
Your pathologist needs to be up to speed on understanding how to report the extent of intestinal metaplasia (complete, incomplete, and mixed) and identifying the areas of focality or abnormalities. It defines what the subsequent surveillance recommendations should be.
Know What’s Required
Let’s review what’s required when it comes to diagnosing and managing gastric premalignant conditions.
First, pre-endoscopy must involve the assessment of risk. Before we put in the endoscope, it’s critical to know, regardless of why the patient is there, who needs to be assessed for gastric premalignant conditions.
Second, during the intra-endoscopy phase, don’t forget the assessments and documentation. If you’re assessing for gastric intestinal metaplasia, use the Sydney system.
Time is a big component. Withdrawal times are discussed much more frequently now, with the takeaway being that longer is better. Aiming for 6-7 minutes is best, according to recommendations from international endoscopy societies and quality measures from the United States. The ACG guideline says that withdrawal times of 2-3 minutes are not best practice and fall short of standard of care.
For post-endoscopy, talk to your pathologist to ensure better communication and understanding. Make sure that you have a quality gastrointestinal pathologist interpreting these lesions so patients can either enter surveillance or discontinue surveillance after potentially two exams negative for evidence of progressive change.
To do better, we need to understand these guidelines, which are all applicable now.
I’m Dr. David Johnson. Thanks for listening. See you next time.
David A. Johnson, MD, a regular contributor to Medscape, is professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, Virginia, and a past president of the American College of Gastroenterology. His primary focus is the clinical practice of gastroenterology. He has published extensively in the internal medicine/gastroenterology literature, with principal research interests in esophageal and colon disease, and more recently in sleep and microbiome effects on gastrointestinal health and disease.
He has disclosed the relevant financial relationships: Advisor to ISOTHRIVE.
A version of this article first appeared on Medscape.com.
Hello. I’m Dr. David Johnson, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School and Old Dominion University in Norfolk, Virginia.
The American College of Gastroenterology (ACG) recently issued a clinical guideline on the diagnosis and management of gastric premalignant conditions.
Coincidentally, earlier this year, the ACG and the American Society for Gastrointestinal Endoscopy (ASGE) collaborated to issue recommendations on quality indicators for upper endoscopy.
In this overview, I’ll focus on gastric premalignant conditions while drawing upon some of the quality indicators from ACG/ASGE. Together, these publications highlight several things that we may be overlooking and clearly need to do better at addressing, given the emerging data in this area.
Gastric Premalignant Conditions: Increased Risk for Progression
Gastric premalignant conditions are common and include atrophic gastritis, gastric intestinal metaplasia, dysplasia, and certain gastric epithelial polyps.
The increased risk for progression to gastric adenocarcinoma in the United States is quite striking. It also reveals an important cancer disparity in certain high-risk groups.
The incidence rates of gastric cancer are two- to 13-fold greater in non-White individuals, particularly among immigrants from high-risk areas. The rates exceed those for esophageal cancer and approach those for colorectal cancer. We have had a dramatic oversight in recognizing the risk for gastric carcinoma in underserved areas.
Gastric carcinoma is not a good diagnosis. The 5-year survival rate is 36%. Approximately 40% of cases are metastatic at the time of diagnosis; only about 15% are caught at a curable early stage.
These rates are in far contrast to Asia and areas that do programmatic screening, where the numbers are dramatically reduced. However, in the United States, we’re simply not there yet.
Endoscopic Evaluation
There are three phases of endoscopic evaluation for gastric premalignant conditions on which I’d like to focus: pre-endoscopy, intra-endoscopy, and post-endoscopy.
Pre-endoscopy — that is, before you even put in the endoscope — it’s important to assess patients’ potential risk for certain conditions, regardless of the reason for performing the endoscopy.
Gastric carcinoma is in the top eight leading causes of cancer death in the United States, with the risk being particularly high in Hispanics and Asians.
According to 2020 data, 40 million people living in the United States were born in another country, with over 70% coming from areas that have a high incidence of gastric carcinoma.
Accounting for the increased risk in these groups will become even more important. By 2065, it is projected that Asian and Hispanic individuals — the immigrant groups with the highest risk for gastric cancer — will comprise 70% of the US population. Therefore, we need to do a better job on pre-endoscopic assessment if we want to address this major cancer disparity in the United States.
However, it’s a potentially fixable problem because, in most cases, gastric carcinoma is preceded by a typical asymptomatic precancerous cascade known as the “Correa’s cascade.” It is analogous to what we see in Barrett’s esophagus or even in colorectal neoplasia as it evolves.
This histologic cascade is important to recognize in patients before they get to the stage of progression. Doing so is highly dependent on the assessment prior to the endoscopy.
You should also be thinking about high-risk groups before a pre-endoscopy evaluation.
During intra-endoscopy, it’s important to plan your actions while performing the procedure, even if you are not specifically screening for gastric carcinoma. We must be held accountable to established recommendations, standards, and best practices for accurately defining observations, determining appropriate actions, and effectively implementing screening protocols.
A high-quality evaluation of the gastric mucosa is critically important, as an estimated 5%-11% of neoplastic lesions are missed on upper endoscopy completed within 3 years of a gastric cancer diagnosis. With less-experienced endoscopists, the rate of missed neoplastic lesions may be as high as 25%.
A quality endoscopy begins (as it would in the colon) with mucosal cleaning. This may not be achieved by water alone and requires the use of mucolytic and defoaming agents, such as simethicone or N-acetylcysteine, which can be inordinately helpful.
Complete mucosal evaluation entails using insufflation to adequately distend the gastric folds.
Atrophic gastritis is observed in a high percentage of patients, and I’m always on the lookout for it when performing endoscopies. One way to identify atrophic gastritis is to look for the loss of gastric folds, which has an approximate sensitivity of 67% and specificity of 85%. The increased visibility of the submucosal venules is another sign of atrophic gastritis, although its sensitivity and specificity are relatively lower at 48% and 87%, respectively.
Full photo documentation of the gastric mucosa should be included. It is an important part of the intra-endoscopy procedure and also is mentioned as part of the recently published quality indicators for upper endoscopy from ACG/ASGE.
Recognizing which patients require a biopsy is important. Appropriate biopsy samples should be obtained in patients with recognizable abnormalities. We’re often looking for changes that may be quite subtle. Dysplasia and even adenocarcinoma in the stomach sometimes just cannot be appreciated based on pure endoscopic evaluation.
When it comes to the biopsy protocol, the recommendation is to follow the Sydney system, which was developed in the 1990s. Simply put, this protocol calls for the biopsy samples to be obtained and placed in two separate jars. You look at the greater and lesser curvature of the antrum and the incisura (jar one), and the greater and lesser curvature of the corpus (jar two) in any identified incidental focused biopsy. This is what we do in the colon and the esophagus.
You should do this after you appropriately clean the mucosa and distend the gastric lumen, ideally using CO2, to avoid the retention of gas.
Time is another important quality measure. This is similar to the colon, where we see that withdrawal times have increased from 6 minutes to 8-9 minutes. In the stomach, there were initial data about a minimum of 2-3 minutes. However, more recent data in the ACG guideline and the ACG/ASGE quality indicators indicate that detection rates increase after mucosal clearance and dissension when the gastric evaluation is 6-7 minutes. These are numbers we need to pay attention to. The ACG guideline notes that a 2- to 3-minute withdrawal time for upper endoscopy is substandard and not acceptable. If you’re still at that level, then you’re below the standard of care.
Again, consider time and photo documentation while examining four to six specific areas of both the greater and lesser curvature of the antrum and corpus, and the incisura angularis. It is ideal to use high-definition endoscopy along with the available virtual imaging enhancers. This is the basic requirement for achieving high-quality assessments.
When it comes to post-endoscopy, it’s essential to talk to your pathologist about using validated instruments of reporting what gastric precancerous lesions involve. There are two different systems: the Operative Link for Gastritis Assessment (OLGA) and the Operative Link on Gastric Intestinal Metaplasia (OLGIM). Although not routinely used in the United States, they are the best recommendations we have for validated histologic scoring systems.
Your pathologist needs to be up to speed on understanding how to report the extent of intestinal metaplasia (complete, incomplete, and mixed) and identifying the areas of focality or abnormalities. It defines what the subsequent surveillance recommendations should be.
Know What’s Required
Let’s review what’s required when it comes to diagnosing and managing gastric premalignant conditions.
First, pre-endoscopy must involve the assessment of risk. Before we put in the endoscope, it’s critical to know, regardless of why the patient is there, who needs to be assessed for gastric premalignant conditions.
Second, during the intra-endoscopy phase, don’t forget the assessments and documentation. If you’re assessing for gastric intestinal metaplasia, use the Sydney system.
Time is a big component. Withdrawal times are discussed much more frequently now, with the takeaway being that longer is better. Aiming for 6-7 minutes is best, according to recommendations from international endoscopy societies and quality measures from the United States. The ACG guideline says that withdrawal times of 2-3 minutes are not best practice and fall short of standard of care.
For post-endoscopy, talk to your pathologist to ensure better communication and understanding. Make sure that you have a quality gastrointestinal pathologist interpreting these lesions so patients can either enter surveillance or discontinue surveillance after potentially two exams negative for evidence of progressive change.
To do better, we need to understand these guidelines, which are all applicable now.
I’m Dr. David Johnson. Thanks for listening. See you next time.
David A. Johnson, MD, a regular contributor to Medscape, is professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, Virginia, and a past president of the American College of Gastroenterology. His primary focus is the clinical practice of gastroenterology. He has published extensively in the internal medicine/gastroenterology literature, with principal research interests in esophageal and colon disease, and more recently in sleep and microbiome effects on gastrointestinal health and disease.
He has disclosed the relevant financial relationships: Advisor to ISOTHRIVE.
A version of this article first appeared on Medscape.com.
Can a Polygenic Risk Score Turn the Tide on Prostate Cancer Screening?
Incorporating a polygenic risk score into prostate cancer screening could enhance the detection of clinically significant prostate cancer that conventional screening may miss, according to results of the BARCODE 1 clinical trial conducted in the United Kingdom.
The study found that about 72% of participants with high polygenic risk scores were diagnosed with clinically significant prostate cancers, which would not have been detected with prostate-specific antigen (PSA) testing or MRI.
“With this test, it could be possible to turn the tide on prostate cancer,” study author Ros Eeles, PhD, professor of oncogenetics at The Institute of Cancer Research, London, England, said in a statement following the publication of the analysis in The New England Journal of Medicine.
Prostate cancer remains the second most commonly diagnosed cancer among men. As a screening tool, PSA testing has been criticized for leading to a high rate of false positive results and overdiagnosis — defined as a screen-detected cancer that would take longer to progress to clinical cancer than the patient’s lifetime. Both issues can result in overtreatment.
Given prostate cancer’s high heritability and the proliferation of genome-wide association studies identifying common genetic variants, there has been growing interest in using polygenic risk scores to improve risk stratification and guide screening.
“Building on decades of research into the genetic markers of prostate cancer, our study shows that the theory does work in practice — we can identify men at risk of aggressive cancers who need further tests and spare the men who are at lower risk from unnecessary treatments,” said Eeles.
An Adjunct to Screening?
The BARCODE 1 study, conducted in the United Kingdom, tested the clinical utility of a polygenic risk score as an adjunct to screening.
The researchers recruited men aged 55-69 years from primary care centers in the United Kingdom. Using germline DNA extracted from saliva, they derived polygenic risk scores from 130 genetic variants known to be associated with an increased risk for prostate cancer.
Among a total of 6393 men who had their scores calculated, 745 (12%) had a score in the top 10% of genetic risk (≥ 90th percentile) and were invited to undergo further screening.
Of these, 468 (63%) accepted the invite and underwent multiparametric MRI and transperineal prostate biopsy, irrespective of the PSA level. Overall, 187 (40%) were diagnosed with prostate cancer following biopsy. Of the 187 men with prostate cancer, 55% (n = 103) had disease classified as intermediate or high risk (Gleason score ≥ 7) per National Comprehensive Cancer Network criteria and therefore warranted further treatment.
Researchers then compared screening that incorporated polygenic risk scores with standard screening with PSA levels and MRI.
When participants’ risk was stratified by their polygenic risk score, 103 patients (55%) with prostate cancer could be classified as intermediate or higher risk, thus warranting treatment. Overall, 74 (71.8%) of those cancers would have been missed using the standard diagnostic pathway in the United Kingdom, which requires patients to have a high PSA level (> 3.0 μg/L) as well as a positive MRI result. These 74 patients either had PSA levels ≤ 3.0 μg/L or negative MRIs, which would mean these patients would typically fall below the action threshold for further testing.
Of the 103 participants warranting treatment, 40 of these men would have been classified as unfavorable intermediate, high, or very high risk, which would require radical treatment. Among this group, roughly 43% would have been missed using the UK diagnostic pathway.
However, the investigators estimated a rate of overdiagnosis with the use of polygenic risk scores of 16%-21%, similar to the overdiagnosis estimates in two prior PSA-based screening studies, signaling that the addition of polygenic risk scores does not necessarily reduce the risk for overdiagnosis.
Overall, “this study is the strongest evidence to date on the clinical utility of a polygenic score for prostate cancer screening,” commented Michael Inouye, professor of systems genomics & population health, University of Cambridge, Cambridge, England, in a statement from the UK nonprofit Science Media Centre (SMC).
“I suspect we will look back on this as a landmark study that really made the clinical case for polygenic scores as a new tool that moved health systems from disease management to early detection and prevention,” said Inouye, who was not involved in the study.
However, other experts were more cautious about the findings.
Dusko Ilic, MD, professor of stem cell sciences, King’s College London, London, England, said the results are “promising, especially in identifying significant cancers that would otherwise be missed,” but cautioned that “there is no direct evidence yet that using [polygenic risk scores] improves long-term outcomes such as mortality or quality-adjusted life years.”
“Modeling suggests benefit, but empirical confirmation is needed,” Ilic said in the SMC statement.
The hope is that the recently launched TRANSFORM trial will help answer some of these outstanding questions.
The current study suggests that polygenic risk scores for prostate cancer “would be a useful component of a multimodality screening program that assesses age, family history of prostate cancer, PSA, and MRI results as triage tools before biopsy is recommended,” David Hunter, MPH, ScD, with Harvard T. H. Chan School of Public Health, Boston, and University of Oxford, Oxford, England, wrote in an editorial accompanying the study.
“To make this integrated program a reality, however, changes to infrastructure would be needed to make running and analyzing a regulated genome array as easy as requesting a PSA level or ordering an MRI. Clearly, we are far from that future,” Hunter cautioned.
“A possible first step that would require less infrastructure could be to order a polygenic risk score only for men with a positive PSA result, then use the polygenic risk score to determine who should undergo an MRI, and then use all the information to determine whether biopsy is recommended,” Hunter said.
In his view, the current study is a “first step on a long road to evaluating new components of any disease screening pathway.”
The research received funding from the European Research Council, the Bob Willis Fund, Cancer Research UK, the Peacock Trust, and the National Institute for Health and Care Research Biomedical Research Centre at The Royal Marsden and The Institute of Cancer Research. Disclosures for authors and editorialists are available with the original article. Inouye and Ilic reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Incorporating a polygenic risk score into prostate cancer screening could enhance the detection of clinically significant prostate cancer that conventional screening may miss, according to results of the BARCODE 1 clinical trial conducted in the United Kingdom.
The study found that about 72% of participants with high polygenic risk scores were diagnosed with clinically significant prostate cancers, which would not have been detected with prostate-specific antigen (PSA) testing or MRI.
“With this test, it could be possible to turn the tide on prostate cancer,” study author Ros Eeles, PhD, professor of oncogenetics at The Institute of Cancer Research, London, England, said in a statement following the publication of the analysis in The New England Journal of Medicine.
Prostate cancer remains the second most commonly diagnosed cancer among men. As a screening tool, PSA testing has been criticized for leading to a high rate of false positive results and overdiagnosis — defined as a screen-detected cancer that would take longer to progress to clinical cancer than the patient’s lifetime. Both issues can result in overtreatment.
Given prostate cancer’s high heritability and the proliferation of genome-wide association studies identifying common genetic variants, there has been growing interest in using polygenic risk scores to improve risk stratification and guide screening.
“Building on decades of research into the genetic markers of prostate cancer, our study shows that the theory does work in practice — we can identify men at risk of aggressive cancers who need further tests and spare the men who are at lower risk from unnecessary treatments,” said Eeles.
An Adjunct to Screening?
The BARCODE 1 study, conducted in the United Kingdom, tested the clinical utility of a polygenic risk score as an adjunct to screening.
The researchers recruited men aged 55-69 years from primary care centers in the United Kingdom. Using germline DNA extracted from saliva, they derived polygenic risk scores from 130 genetic variants known to be associated with an increased risk for prostate cancer.
Among a total of 6393 men who had their scores calculated, 745 (12%) had a score in the top 10% of genetic risk (≥ 90th percentile) and were invited to undergo further screening.
Of these, 468 (63%) accepted the invite and underwent multiparametric MRI and transperineal prostate biopsy, irrespective of the PSA level. Overall, 187 (40%) were diagnosed with prostate cancer following biopsy. Of the 187 men with prostate cancer, 55% (n = 103) had disease classified as intermediate or high risk (Gleason score ≥ 7) per National Comprehensive Cancer Network criteria and therefore warranted further treatment.
Researchers then compared screening that incorporated polygenic risk scores with standard screening with PSA levels and MRI.
When participants’ risk was stratified by their polygenic risk score, 103 patients (55%) with prostate cancer could be classified as intermediate or higher risk, thus warranting treatment. Overall, 74 (71.8%) of those cancers would have been missed using the standard diagnostic pathway in the United Kingdom, which requires patients to have a high PSA level (> 3.0 μg/L) as well as a positive MRI result. These 74 patients either had PSA levels ≤ 3.0 μg/L or negative MRIs, which would mean these patients would typically fall below the action threshold for further testing.
Of the 103 participants warranting treatment, 40 of these men would have been classified as unfavorable intermediate, high, or very high risk, which would require radical treatment. Among this group, roughly 43% would have been missed using the UK diagnostic pathway.
However, the investigators estimated a rate of overdiagnosis with the use of polygenic risk scores of 16%-21%, similar to the overdiagnosis estimates in two prior PSA-based screening studies, signaling that the addition of polygenic risk scores does not necessarily reduce the risk for overdiagnosis.
Overall, “this study is the strongest evidence to date on the clinical utility of a polygenic score for prostate cancer screening,” commented Michael Inouye, professor of systems genomics & population health, University of Cambridge, Cambridge, England, in a statement from the UK nonprofit Science Media Centre (SMC).
“I suspect we will look back on this as a landmark study that really made the clinical case for polygenic scores as a new tool that moved health systems from disease management to early detection and prevention,” said Inouye, who was not involved in the study.
However, other experts were more cautious about the findings.
Dusko Ilic, MD, professor of stem cell sciences, King’s College London, London, England, said the results are “promising, especially in identifying significant cancers that would otherwise be missed,” but cautioned that “there is no direct evidence yet that using [polygenic risk scores] improves long-term outcomes such as mortality or quality-adjusted life years.”
“Modeling suggests benefit, but empirical confirmation is needed,” Ilic said in the SMC statement.
The hope is that the recently launched TRANSFORM trial will help answer some of these outstanding questions.
The current study suggests that polygenic risk scores for prostate cancer “would be a useful component of a multimodality screening program that assesses age, family history of prostate cancer, PSA, and MRI results as triage tools before biopsy is recommended,” David Hunter, MPH, ScD, with Harvard T. H. Chan School of Public Health, Boston, and University of Oxford, Oxford, England, wrote in an editorial accompanying the study.
“To make this integrated program a reality, however, changes to infrastructure would be needed to make running and analyzing a regulated genome array as easy as requesting a PSA level or ordering an MRI. Clearly, we are far from that future,” Hunter cautioned.
“A possible first step that would require less infrastructure could be to order a polygenic risk score only for men with a positive PSA result, then use the polygenic risk score to determine who should undergo an MRI, and then use all the information to determine whether biopsy is recommended,” Hunter said.
In his view, the current study is a “first step on a long road to evaluating new components of any disease screening pathway.”
The research received funding from the European Research Council, the Bob Willis Fund, Cancer Research UK, the Peacock Trust, and the National Institute for Health and Care Research Biomedical Research Centre at The Royal Marsden and The Institute of Cancer Research. Disclosures for authors and editorialists are available with the original article. Inouye and Ilic reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Incorporating a polygenic risk score into prostate cancer screening could enhance the detection of clinically significant prostate cancer that conventional screening may miss, according to results of the BARCODE 1 clinical trial conducted in the United Kingdom.
The study found that about 72% of participants with high polygenic risk scores were diagnosed with clinically significant prostate cancers, which would not have been detected with prostate-specific antigen (PSA) testing or MRI.
“With this test, it could be possible to turn the tide on prostate cancer,” study author Ros Eeles, PhD, professor of oncogenetics at The Institute of Cancer Research, London, England, said in a statement following the publication of the analysis in The New England Journal of Medicine.
Prostate cancer remains the second most commonly diagnosed cancer among men. As a screening tool, PSA testing has been criticized for leading to a high rate of false positive results and overdiagnosis — defined as a screen-detected cancer that would take longer to progress to clinical cancer than the patient’s lifetime. Both issues can result in overtreatment.
Given prostate cancer’s high heritability and the proliferation of genome-wide association studies identifying common genetic variants, there has been growing interest in using polygenic risk scores to improve risk stratification and guide screening.
“Building on decades of research into the genetic markers of prostate cancer, our study shows that the theory does work in practice — we can identify men at risk of aggressive cancers who need further tests and spare the men who are at lower risk from unnecessary treatments,” said Eeles.
An Adjunct to Screening?
The BARCODE 1 study, conducted in the United Kingdom, tested the clinical utility of a polygenic risk score as an adjunct to screening.
The researchers recruited men aged 55-69 years from primary care centers in the United Kingdom. Using germline DNA extracted from saliva, they derived polygenic risk scores from 130 genetic variants known to be associated with an increased risk for prostate cancer.
Among a total of 6393 men who had their scores calculated, 745 (12%) had a score in the top 10% of genetic risk (≥ 90th percentile) and were invited to undergo further screening.
Of these, 468 (63%) accepted the invite and underwent multiparametric MRI and transperineal prostate biopsy, irrespective of the PSA level. Overall, 187 (40%) were diagnosed with prostate cancer following biopsy. Of the 187 men with prostate cancer, 55% (n = 103) had disease classified as intermediate or high risk (Gleason score ≥ 7) per National Comprehensive Cancer Network criteria and therefore warranted further treatment.
Researchers then compared screening that incorporated polygenic risk scores with standard screening with PSA levels and MRI.
When participants’ risk was stratified by their polygenic risk score, 103 patients (55%) with prostate cancer could be classified as intermediate or higher risk, thus warranting treatment. Overall, 74 (71.8%) of those cancers would have been missed using the standard diagnostic pathway in the United Kingdom, which requires patients to have a high PSA level (> 3.0 μg/L) as well as a positive MRI result. These 74 patients either had PSA levels ≤ 3.0 μg/L or negative MRIs, which would mean these patients would typically fall below the action threshold for further testing.
Of the 103 participants warranting treatment, 40 of these men would have been classified as unfavorable intermediate, high, or very high risk, which would require radical treatment. Among this group, roughly 43% would have been missed using the UK diagnostic pathway.
However, the investigators estimated a rate of overdiagnosis with the use of polygenic risk scores of 16%-21%, similar to the overdiagnosis estimates in two prior PSA-based screening studies, signaling that the addition of polygenic risk scores does not necessarily reduce the risk for overdiagnosis.
Overall, “this study is the strongest evidence to date on the clinical utility of a polygenic score for prostate cancer screening,” commented Michael Inouye, professor of systems genomics & population health, University of Cambridge, Cambridge, England, in a statement from the UK nonprofit Science Media Centre (SMC).
“I suspect we will look back on this as a landmark study that really made the clinical case for polygenic scores as a new tool that moved health systems from disease management to early detection and prevention,” said Inouye, who was not involved in the study.
However, other experts were more cautious about the findings.
Dusko Ilic, MD, professor of stem cell sciences, King’s College London, London, England, said the results are “promising, especially in identifying significant cancers that would otherwise be missed,” but cautioned that “there is no direct evidence yet that using [polygenic risk scores] improves long-term outcomes such as mortality or quality-adjusted life years.”
“Modeling suggests benefit, but empirical confirmation is needed,” Ilic said in the SMC statement.
The hope is that the recently launched TRANSFORM trial will help answer some of these outstanding questions.
The current study suggests that polygenic risk scores for prostate cancer “would be a useful component of a multimodality screening program that assesses age, family history of prostate cancer, PSA, and MRI results as triage tools before biopsy is recommended,” David Hunter, MPH, ScD, with Harvard T. H. Chan School of Public Health, Boston, and University of Oxford, Oxford, England, wrote in an editorial accompanying the study.
“To make this integrated program a reality, however, changes to infrastructure would be needed to make running and analyzing a regulated genome array as easy as requesting a PSA level or ordering an MRI. Clearly, we are far from that future,” Hunter cautioned.
“A possible first step that would require less infrastructure could be to order a polygenic risk score only for men with a positive PSA result, then use the polygenic risk score to determine who should undergo an MRI, and then use all the information to determine whether biopsy is recommended,” Hunter said.
In his view, the current study is a “first step on a long road to evaluating new components of any disease screening pathway.”
The research received funding from the European Research Council, the Bob Willis Fund, Cancer Research UK, the Peacock Trust, and the National Institute for Health and Care Research Biomedical Research Centre at The Royal Marsden and The Institute of Cancer Research. Disclosures for authors and editorialists are available with the original article. Inouye and Ilic reported no relevant disclosures.
A version of this article first appeared on Medscape.com.