User login
Certain cancers primarily result from ‘bad luck’
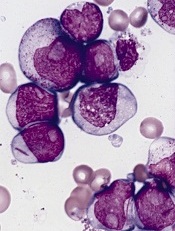
in the bone marrow
Scientists have created a statistical model that measures the proportion of cancer incidence, across many tissue types, caused mainly by random mutations that occur when stem cells divide.
By their measure, two-thirds of adult cancers—including certain leukemias—can be explained primarily by “bad luck,” when these random mutations occur in genes that can drive cancer growth.
The remaining third are due to environmental factors and inherited genes.
“All cancers are caused by a combination of bad luck, the environment, and heredity, and we’ve created a model that may help quantify how much of these three factors contribute to cancer development,” said Bert Vogelstein, MD, of the Johns Hopkins University School of Medicine.
Dr Vogelstein and Cristian Tomasetti, PhD, also of the Johns Hopkins University School of Medicine, detailed these findings in Science.
The pair came to their conclusions by searching the scientific literature for information on the cumulative number of stem cell divisions in 31 tissue types during an average individual’s lifetime.
The researchers knew that cancer arises when tissue-specific stem cells make random mistakes, or mutations. But the actual contribution of these random mistakes to cancer incidence, in comparison to the contribution of hereditary or environmental factors, was unclear.
To sort out the role of random mutations in cancer risk, the team charted the number of stem cell divisions in 31 tissues and compared these rates with the lifetime risks of cancer in the same tissues among Americans.
From this data scatterplot, Drs Tomasetti and Vogelstein determined the correlation between the total number of stem cell divisions and cancer risk to be 0.804. Mathematically, the closer this value is to 1, the more stem cell divisions and cancer risk are correlated.
“Our study shows, in general, that a change in the number of stem cell divisions in a tissue type is highly correlated with a change in the incidence of cancer in that same tissue,” Dr Vogelstein said.
One example is in colon tissue, which undergoes 4 times more stem cell divisions than small intestine tissue in humans. Likewise, colon cancer is much more prevalent than small intestinal cancer.
“You could argue that the colon is exposed to more environmental factors than the small intestine, which increases the potential rate of acquired mutations,” Dr Tomasetti said.
However, the scientists observed the opposite in mouse colons, which had a lower number of stem cell divisions than in their small intestines. In mice, cancer incidence is lower in the colon than in the small intestine. The researchers believe this supports the role of the total number of stem cell divisions in the development of cancer.
Using statistical theory, the pair calculated how much of the variation in cancer risk can be explained by the number of stem cell divisions, which is 0.804 squared, or, in percentage form, approximately 65%.
Finally, the scientists classified the types of cancers they studied into two groups. They calculated which cancer types had an incidence predicted by the number of stem cell divisions and which had higher incidence.
They found that 22 cancer types—including acute myeloid leukemia and chronic lymphocytic leukemia—could be largely explained by the “bad luck” factor of random DNA mutations during cell division.
The other 9 cancer types had incidences higher than predicted by “bad luck” and were presumably due to a combination of bad luck plus environmental or inherited factors.
“We found that the types of cancer that had higher risk than predicted by the number of stem cell divisions were precisely the ones you’d expect, including lung cancer, which is linked to smoking; skin cancer, linked to sun exposure; and forms of cancers associated with hereditary syndromes,” Dr Vogelstein said.
“This study shows that you can add to your risk of getting cancers by smoking or other poor lifestyle factors. However, many forms of cancer are due largely to the bad luck of acquiring a mutation in a cancer driver gene regardless of lifestyle and heredity factors. The best way to eradicate these cancers will be through early detection, when they are still curable by surgery.”
The researchers noted that some cancers, such as breast and prostate cancer, were not included in the report because the team was unable to find reliable stem cell division rates in the scientific literature.
They hope other scientists will help refine their statistical model by finding more precise stem cell division rates. ![]()
in the bone marrow
Scientists have created a statistical model that measures the proportion of cancer incidence, across many tissue types, caused mainly by random mutations that occur when stem cells divide.
By their measure, two-thirds of adult cancers—including certain leukemias—can be explained primarily by “bad luck,” when these random mutations occur in genes that can drive cancer growth.
The remaining third are due to environmental factors and inherited genes.
“All cancers are caused by a combination of bad luck, the environment, and heredity, and we’ve created a model that may help quantify how much of these three factors contribute to cancer development,” said Bert Vogelstein, MD, of the Johns Hopkins University School of Medicine.
Dr Vogelstein and Cristian Tomasetti, PhD, also of the Johns Hopkins University School of Medicine, detailed these findings in Science.
The pair came to their conclusions by searching the scientific literature for information on the cumulative number of stem cell divisions in 31 tissue types during an average individual’s lifetime.
The researchers knew that cancer arises when tissue-specific stem cells make random mistakes, or mutations. But the actual contribution of these random mistakes to cancer incidence, in comparison to the contribution of hereditary or environmental factors, was unclear.
To sort out the role of random mutations in cancer risk, the team charted the number of stem cell divisions in 31 tissues and compared these rates with the lifetime risks of cancer in the same tissues among Americans.
From this data scatterplot, Drs Tomasetti and Vogelstein determined the correlation between the total number of stem cell divisions and cancer risk to be 0.804. Mathematically, the closer this value is to 1, the more stem cell divisions and cancer risk are correlated.
“Our study shows, in general, that a change in the number of stem cell divisions in a tissue type is highly correlated with a change in the incidence of cancer in that same tissue,” Dr Vogelstein said.
One example is in colon tissue, which undergoes 4 times more stem cell divisions than small intestine tissue in humans. Likewise, colon cancer is much more prevalent than small intestinal cancer.
“You could argue that the colon is exposed to more environmental factors than the small intestine, which increases the potential rate of acquired mutations,” Dr Tomasetti said.
However, the scientists observed the opposite in mouse colons, which had a lower number of stem cell divisions than in their small intestines. In mice, cancer incidence is lower in the colon than in the small intestine. The researchers believe this supports the role of the total number of stem cell divisions in the development of cancer.
Using statistical theory, the pair calculated how much of the variation in cancer risk can be explained by the number of stem cell divisions, which is 0.804 squared, or, in percentage form, approximately 65%.
Finally, the scientists classified the types of cancers they studied into two groups. They calculated which cancer types had an incidence predicted by the number of stem cell divisions and which had higher incidence.
They found that 22 cancer types—including acute myeloid leukemia and chronic lymphocytic leukemia—could be largely explained by the “bad luck” factor of random DNA mutations during cell division.
The other 9 cancer types had incidences higher than predicted by “bad luck” and were presumably due to a combination of bad luck plus environmental or inherited factors.
“We found that the types of cancer that had higher risk than predicted by the number of stem cell divisions were precisely the ones you’d expect, including lung cancer, which is linked to smoking; skin cancer, linked to sun exposure; and forms of cancers associated with hereditary syndromes,” Dr Vogelstein said.
“This study shows that you can add to your risk of getting cancers by smoking or other poor lifestyle factors. However, many forms of cancer are due largely to the bad luck of acquiring a mutation in a cancer driver gene regardless of lifestyle and heredity factors. The best way to eradicate these cancers will be through early detection, when they are still curable by surgery.”
The researchers noted that some cancers, such as breast and prostate cancer, were not included in the report because the team was unable to find reliable stem cell division rates in the scientific literature.
They hope other scientists will help refine their statistical model by finding more precise stem cell division rates. ![]()
in the bone marrow
Scientists have created a statistical model that measures the proportion of cancer incidence, across many tissue types, caused mainly by random mutations that occur when stem cells divide.
By their measure, two-thirds of adult cancers—including certain leukemias—can be explained primarily by “bad luck,” when these random mutations occur in genes that can drive cancer growth.
The remaining third are due to environmental factors and inherited genes.
“All cancers are caused by a combination of bad luck, the environment, and heredity, and we’ve created a model that may help quantify how much of these three factors contribute to cancer development,” said Bert Vogelstein, MD, of the Johns Hopkins University School of Medicine.
Dr Vogelstein and Cristian Tomasetti, PhD, also of the Johns Hopkins University School of Medicine, detailed these findings in Science.
The pair came to their conclusions by searching the scientific literature for information on the cumulative number of stem cell divisions in 31 tissue types during an average individual’s lifetime.
The researchers knew that cancer arises when tissue-specific stem cells make random mistakes, or mutations. But the actual contribution of these random mistakes to cancer incidence, in comparison to the contribution of hereditary or environmental factors, was unclear.
To sort out the role of random mutations in cancer risk, the team charted the number of stem cell divisions in 31 tissues and compared these rates with the lifetime risks of cancer in the same tissues among Americans.
From this data scatterplot, Drs Tomasetti and Vogelstein determined the correlation between the total number of stem cell divisions and cancer risk to be 0.804. Mathematically, the closer this value is to 1, the more stem cell divisions and cancer risk are correlated.
“Our study shows, in general, that a change in the number of stem cell divisions in a tissue type is highly correlated with a change in the incidence of cancer in that same tissue,” Dr Vogelstein said.
One example is in colon tissue, which undergoes 4 times more stem cell divisions than small intestine tissue in humans. Likewise, colon cancer is much more prevalent than small intestinal cancer.
“You could argue that the colon is exposed to more environmental factors than the small intestine, which increases the potential rate of acquired mutations,” Dr Tomasetti said.
However, the scientists observed the opposite in mouse colons, which had a lower number of stem cell divisions than in their small intestines. In mice, cancer incidence is lower in the colon than in the small intestine. The researchers believe this supports the role of the total number of stem cell divisions in the development of cancer.
Using statistical theory, the pair calculated how much of the variation in cancer risk can be explained by the number of stem cell divisions, which is 0.804 squared, or, in percentage form, approximately 65%.
Finally, the scientists classified the types of cancers they studied into two groups. They calculated which cancer types had an incidence predicted by the number of stem cell divisions and which had higher incidence.
They found that 22 cancer types—including acute myeloid leukemia and chronic lymphocytic leukemia—could be largely explained by the “bad luck” factor of random DNA mutations during cell division.
The other 9 cancer types had incidences higher than predicted by “bad luck” and were presumably due to a combination of bad luck plus environmental or inherited factors.
“We found that the types of cancer that had higher risk than predicted by the number of stem cell divisions were precisely the ones you’d expect, including lung cancer, which is linked to smoking; skin cancer, linked to sun exposure; and forms of cancers associated with hereditary syndromes,” Dr Vogelstein said.
“This study shows that you can add to your risk of getting cancers by smoking or other poor lifestyle factors. However, many forms of cancer are due largely to the bad luck of acquiring a mutation in a cancer driver gene regardless of lifestyle and heredity factors. The best way to eradicate these cancers will be through early detection, when they are still curable by surgery.”
The researchers noted that some cancers, such as breast and prostate cancer, were not included in the report because the team was unable to find reliable stem cell division rates in the scientific literature.
They hope other scientists will help refine their statistical model by finding more precise stem cell division rates. ![]()
CARs come in different makes and models

Credit: NIAID
SAN FRANCISCO—CTL019, a chimeric antigen receptor (CAR) T cell targeting CD19, is not the only CAR in the production line.
Investigators at the National Cancer Institute in Bethesda, Maryland, and Memorial Sloan Kettering Cancer Center (MSKCC) in New York City are also pursuing CAR T-cell therapy.
These groups are using a retroviral platform to transduce the T cells rather than a lentiviral one, as is the case with CTL019.
Investigators reported progress to date on these makes of CARs at the 2014 ASH Annual Meeting.
Daniel W. Lee III, MD, of the National Cancer Institute, reported on a phase 1 study of CD19 CAR T cells in children and young adults with CD19+ acute lymphoblastic leukemia or non-Hodgkin lymphoma.
And Jae H. Park, MD, of MSKCC, presented data from a trial of JCAR015—autologous T cells genetically modified to express a 19-28z CAR targeting CD19—in patients with B-cell acute lymphoblastic leukemia.
The study is sponsored by MSKCC, but JCAR015 is a product of Juno Therapeutics. ![]()
Credit: NIAID
SAN FRANCISCO—CTL019, a chimeric antigen receptor (CAR) T cell targeting CD19, is not the only CAR in the production line.
Investigators at the National Cancer Institute in Bethesda, Maryland, and Memorial Sloan Kettering Cancer Center (MSKCC) in New York City are also pursuing CAR T-cell therapy.
These groups are using a retroviral platform to transduce the T cells rather than a lentiviral one, as is the case with CTL019.
Investigators reported progress to date on these makes of CARs at the 2014 ASH Annual Meeting.
Daniel W. Lee III, MD, of the National Cancer Institute, reported on a phase 1 study of CD19 CAR T cells in children and young adults with CD19+ acute lymphoblastic leukemia or non-Hodgkin lymphoma.
And Jae H. Park, MD, of MSKCC, presented data from a trial of JCAR015—autologous T cells genetically modified to express a 19-28z CAR targeting CD19—in patients with B-cell acute lymphoblastic leukemia.
The study is sponsored by MSKCC, but JCAR015 is a product of Juno Therapeutics. ![]()
Credit: NIAID
SAN FRANCISCO—CTL019, a chimeric antigen receptor (CAR) T cell targeting CD19, is not the only CAR in the production line.
Investigators at the National Cancer Institute in Bethesda, Maryland, and Memorial Sloan Kettering Cancer Center (MSKCC) in New York City are also pursuing CAR T-cell therapy.
These groups are using a retroviral platform to transduce the T cells rather than a lentiviral one, as is the case with CTL019.
Investigators reported progress to date on these makes of CARs at the 2014 ASH Annual Meeting.
Daniel W. Lee III, MD, of the National Cancer Institute, reported on a phase 1 study of CD19 CAR T cells in children and young adults with CD19+ acute lymphoblastic leukemia or non-Hodgkin lymphoma.
And Jae H. Park, MD, of MSKCC, presented data from a trial of JCAR015—autologous T cells genetically modified to express a 19-28z CAR targeting CD19—in patients with B-cell acute lymphoblastic leukemia.
The study is sponsored by MSKCC, but JCAR015 is a product of Juno Therapeutics. ![]()
CAR is feasible in majority of ALL patients, team says

Credit: Bill Branson
SAN FRANCISCO—A chimeric antigen receptor (CAR) T-cell therapy is feasible in 90% of heavily pretreated or transplanted patients with acute lymphoblastic leukemia (ALL) and can serve as a bridge to transplant, according to investigators.
Daniel W. Lee III, MD, of the National Cancer Institute in Bethesda, Maryland, reported on a phase 1 study of this CD19 CAR T-cell therapy in children and young adults with CD19+ ALL or non-Hodgkin lymphoma at the 2014 ASH Annual Meeting (abstract 381*).
Twenty-one patients were enrolled on the trial. They had a preparative regimen of fludarabine and cyclophosphamide and were infused with CAR T cells 11 days after the peripheral blood mononuclear cells were collected.
Dose levels were 1 x 106 CAR+ T cells/kg, 3 x 106 CAR+ T cells/kg, or the maximum number of cells generated if below either one of these levels. Two patients received less than the dose assigned and were not evaluated for toxicity.
Patients were a median age of 13 years (range, 5 to 27). Fourteen were male, 20 had ALL, and 1 had diffuse large B-cell lymphoma.
All had detectable disease, and 2 were CNS2 at the time of T-cell infusion. Six had primary refractory disease, 8 had at least 1 prior stem cell transplant, and 4 had prior immunotherapy.
The investigators determined that the maximally tolerated dose was 1 x 106 CAR+ T cells/kg. The dose-limiting toxicities were related to cytokine release syndrome (CRS), which was reversible if managed appropriately with tocilizumab, with or without steroids.
Grade 3 adverse events possibly related to therapy included fever (47%), febrile neutropenia (37%), electrolyte disturbance (29%), CRS (16%), hypotension (11%), transaminitis (16%), and 5% each for hypertension, prolonged QTc, dysphasia, LV systolic dysfunction, multiorgan failure, hypoxia, and pulmonary edema.
Grade 4 events possibly related to treatment included electrolyte disturbance (5%), CRS (16%), hypotension (11%), cardiac arrest (5%), and hypoxia (5%). There was no evidence of graft-vs-host disease.
The complete response (CR) rate was 67% in the intent-to-treat population and 70% in patients with ALL.
“Those patients who responded tended to have some degree of cytokine release syndrome, whereas those patients who did not respond or had stable disease did not have any CRS,” Dr Lee said. “But, also, it’s important to note that you don’t have to have severe grade 3 or grade 4 CRS in order to have significant response.”
Dr Lee also pointed out that in vivo CAR T-cell expansion significantly correlated with response (P=0.0028). And CRS severity correlated with IL-6 (P=0.0002), INF-γ (P=0.0002), C-reactive protein (P=0.0015), and CAR (P=0.0011).
At a median follow-up of 10 months, minimal residual disease-negative patients had a 79% leukemia-free survival. Overall survival was 52% for all patients enrolled. Two patients had CD19-negative relapses.
The investigators also found that CAR T cells can eliminate CNS leukemia, with 11 of 17 patients (65%) having CAR T cells detectable in their cerebrospinal fluid.
The team concluded that this therapy is feasible in 90% of heavily pretreated or transplanted ALL patients and can serve as a bridge to transplant. ![]()
*Information in the abstract differs from that presented at the meeting.
Credit: Bill Branson
SAN FRANCISCO—A chimeric antigen receptor (CAR) T-cell therapy is feasible in 90% of heavily pretreated or transplanted patients with acute lymphoblastic leukemia (ALL) and can serve as a bridge to transplant, according to investigators.
Daniel W. Lee III, MD, of the National Cancer Institute in Bethesda, Maryland, reported on a phase 1 study of this CD19 CAR T-cell therapy in children and young adults with CD19+ ALL or non-Hodgkin lymphoma at the 2014 ASH Annual Meeting (abstract 381*).
Twenty-one patients were enrolled on the trial. They had a preparative regimen of fludarabine and cyclophosphamide and were infused with CAR T cells 11 days after the peripheral blood mononuclear cells were collected.
Dose levels were 1 x 106 CAR+ T cells/kg, 3 x 106 CAR+ T cells/kg, or the maximum number of cells generated if below either one of these levels. Two patients received less than the dose assigned and were not evaluated for toxicity.
Patients were a median age of 13 years (range, 5 to 27). Fourteen were male, 20 had ALL, and 1 had diffuse large B-cell lymphoma.
All had detectable disease, and 2 were CNS2 at the time of T-cell infusion. Six had primary refractory disease, 8 had at least 1 prior stem cell transplant, and 4 had prior immunotherapy.
The investigators determined that the maximally tolerated dose was 1 x 106 CAR+ T cells/kg. The dose-limiting toxicities were related to cytokine release syndrome (CRS), which was reversible if managed appropriately with tocilizumab, with or without steroids.
Grade 3 adverse events possibly related to therapy included fever (47%), febrile neutropenia (37%), electrolyte disturbance (29%), CRS (16%), hypotension (11%), transaminitis (16%), and 5% each for hypertension, prolonged QTc, dysphasia, LV systolic dysfunction, multiorgan failure, hypoxia, and pulmonary edema.
Grade 4 events possibly related to treatment included electrolyte disturbance (5%), CRS (16%), hypotension (11%), cardiac arrest (5%), and hypoxia (5%). There was no evidence of graft-vs-host disease.
The complete response (CR) rate was 67% in the intent-to-treat population and 70% in patients with ALL.
“Those patients who responded tended to have some degree of cytokine release syndrome, whereas those patients who did not respond or had stable disease did not have any CRS,” Dr Lee said. “But, also, it’s important to note that you don’t have to have severe grade 3 or grade 4 CRS in order to have significant response.”
Dr Lee also pointed out that in vivo CAR T-cell expansion significantly correlated with response (P=0.0028). And CRS severity correlated with IL-6 (P=0.0002), INF-γ (P=0.0002), C-reactive protein (P=0.0015), and CAR (P=0.0011).
At a median follow-up of 10 months, minimal residual disease-negative patients had a 79% leukemia-free survival. Overall survival was 52% for all patients enrolled. Two patients had CD19-negative relapses.
The investigators also found that CAR T cells can eliminate CNS leukemia, with 11 of 17 patients (65%) having CAR T cells detectable in their cerebrospinal fluid.
The team concluded that this therapy is feasible in 90% of heavily pretreated or transplanted ALL patients and can serve as a bridge to transplant. ![]()
*Information in the abstract differs from that presented at the meeting.
Credit: Bill Branson
SAN FRANCISCO—A chimeric antigen receptor (CAR) T-cell therapy is feasible in 90% of heavily pretreated or transplanted patients with acute lymphoblastic leukemia (ALL) and can serve as a bridge to transplant, according to investigators.
Daniel W. Lee III, MD, of the National Cancer Institute in Bethesda, Maryland, reported on a phase 1 study of this CD19 CAR T-cell therapy in children and young adults with CD19+ ALL or non-Hodgkin lymphoma at the 2014 ASH Annual Meeting (abstract 381*).
Twenty-one patients were enrolled on the trial. They had a preparative regimen of fludarabine and cyclophosphamide and were infused with CAR T cells 11 days after the peripheral blood mononuclear cells were collected.
Dose levels were 1 x 106 CAR+ T cells/kg, 3 x 106 CAR+ T cells/kg, or the maximum number of cells generated if below either one of these levels. Two patients received less than the dose assigned and were not evaluated for toxicity.
Patients were a median age of 13 years (range, 5 to 27). Fourteen were male, 20 had ALL, and 1 had diffuse large B-cell lymphoma.
All had detectable disease, and 2 were CNS2 at the time of T-cell infusion. Six had primary refractory disease, 8 had at least 1 prior stem cell transplant, and 4 had prior immunotherapy.
The investigators determined that the maximally tolerated dose was 1 x 106 CAR+ T cells/kg. The dose-limiting toxicities were related to cytokine release syndrome (CRS), which was reversible if managed appropriately with tocilizumab, with or without steroids.
Grade 3 adverse events possibly related to therapy included fever (47%), febrile neutropenia (37%), electrolyte disturbance (29%), CRS (16%), hypotension (11%), transaminitis (16%), and 5% each for hypertension, prolonged QTc, dysphasia, LV systolic dysfunction, multiorgan failure, hypoxia, and pulmonary edema.
Grade 4 events possibly related to treatment included electrolyte disturbance (5%), CRS (16%), hypotension (11%), cardiac arrest (5%), and hypoxia (5%). There was no evidence of graft-vs-host disease.
The complete response (CR) rate was 67% in the intent-to-treat population and 70% in patients with ALL.
“Those patients who responded tended to have some degree of cytokine release syndrome, whereas those patients who did not respond or had stable disease did not have any CRS,” Dr Lee said. “But, also, it’s important to note that you don’t have to have severe grade 3 or grade 4 CRS in order to have significant response.”
Dr Lee also pointed out that in vivo CAR T-cell expansion significantly correlated with response (P=0.0028). And CRS severity correlated with IL-6 (P=0.0002), INF-γ (P=0.0002), C-reactive protein (P=0.0015), and CAR (P=0.0011).
At a median follow-up of 10 months, minimal residual disease-negative patients had a 79% leukemia-free survival. Overall survival was 52% for all patients enrolled. Two patients had CD19-negative relapses.
The investigators also found that CAR T cells can eliminate CNS leukemia, with 11 of 17 patients (65%) having CAR T cells detectable in their cerebrospinal fluid.
The team concluded that this therapy is feasible in 90% of heavily pretreated or transplanted ALL patients and can serve as a bridge to transplant. ![]()
*Information in the abstract differs from that presented at the meeting.
CAR produces durable responses in B-cell ALL

Credit: Charles Haymond
SAN FRANCISCO—JCAR015, a chimeric antigen receptor (CAR) T-cell therapy, can produce durable responses in patients with B-cell acute lymphoblastic leukemia (ALL) who do not undergo subsequent hematopoietic stem cell transplant (HSCT), new research suggests.
JCAR015 consists of autologous T cells genetically modified to express 19-28z chimeric antigen receptor (19-28z CAR) targeting CD19.
Jae H. Park, MD, of Memorial Sloan Kettering Cancer Center in New York, presented data on JCAR015 at the 2014 ASH Annual Meeting (abstract 382).* The study is sponsored by Memorial Sloan Kettering, but funding has also been provided by Juno Therapeutics, the company developing JCAR015.
JCAR015 was tested at a dose of 1 - 3 x 106 CAR cells/kg in 33 adults with relapsed/refractory B-cell ALL. Twenty-eight patients were evaluable for toxicity, 27 for response, and 5 patients were too early in their treatment to evaluate at the time of data cutoff.
Twenty-one patients were male, and the median age was 55 (range, 23 to 74).
Thirteen patients (46%) had minimal disease (<5% blasts) immediately prior to T-cell infusion, and 15 patients (54%) had morphologic disease of 5% to 100% blasts (median 63%).
Eighteen patients (64%) had received 2 prior lines of therapy, and 5 (18%) each had 3 or more prior lines.
Eight patients (29%) underwent prior allogeneic HSCT, 9 patients (32%) were Philadelphia chromosome positive (Ph+), and 3 (11%) had the T315I mutation.
The overall complete response (CR) rate was 89%, and the minimal residual disease-negative CR rate was 88%. The median time to CR was 22.5 days (range, 9 to 33).
The investigators performed a subgroup analysis and found that 100% of the 13 patients with minimal disease before therapy achieved a CR, compared to 79% of patients with morphologic disease.
Eighty-six percent (6/7) of patients who had a prior HSCT and 90% (18/20) without a prior HSCT achieved a CR. Eighty-nine percent (8/9) of Ph+ patients achieved a CR, and 89% (16/18) of Philadelphia-negative patients (89%) achieved a CR.
At a median follow-up of 6 months (range, 1 to 38 months), 12 patients remained disease-free, including 7 patients who had more than a year of follow-up. Seven patients are disease-free without a subsequent HSCT.
Nine patients relapsed during a follow-up of 3 to 8 months, and 10 patients proceeded to HSCT. Two relapses occurred after HSCT, one in a patient who had CD19-negative blasts, and 7 relapses occurred without HSCT.
The overall survival rate at 6 months was 57%, and the median survival was 8.5 months.
For those patients who had a transplant after CAR therapy, the median survival was 10.8 months, and the survival rate at 6 months was 68%.
Dr Park pointed out that maximum T-cell expansion occurred between days 7 and 14 and correlated with the occurrence of cytokine release syndrome (CRS). The T cells persisted for 1 to 3 months following infusion.
The main adverse events were those associated with CRS and neurologic changes. Severe CRS requiring vasopressors or mechanical ventilation occurred in 5 patients (18%) overall and in 5 patients (33%) with morphologic disease before therapy. Severe CRS did not occur in any patient with minimal disease before therapy.
Grade 3 or 4 neurotoxicity occurred in 7 patients (25%) overall, in 6 patients (40%) with morphologic disease, and in 1 with minimal disease (8%) before therapy.
The investigators observed no graft-vs-host disease exacerbation, and CRS was managed with an IL-6R inhibitor, steroids, or both.
Dr Park noted that the neurologic symptoms are reversible and can occur independently of CRS.
He also pointed out that CR rates were similar regardless of different disease risk factors, and that durable responses have been achieved in patients who did not have a subsequent HSCT. ![]()
*Information in the abstract differs from that presented at the meeting.
Credit: Charles Haymond
SAN FRANCISCO—JCAR015, a chimeric antigen receptor (CAR) T-cell therapy, can produce durable responses in patients with B-cell acute lymphoblastic leukemia (ALL) who do not undergo subsequent hematopoietic stem cell transplant (HSCT), new research suggests.
JCAR015 consists of autologous T cells genetically modified to express 19-28z chimeric antigen receptor (19-28z CAR) targeting CD19.
Jae H. Park, MD, of Memorial Sloan Kettering Cancer Center in New York, presented data on JCAR015 at the 2014 ASH Annual Meeting (abstract 382).* The study is sponsored by Memorial Sloan Kettering, but funding has also been provided by Juno Therapeutics, the company developing JCAR015.
JCAR015 was tested at a dose of 1 - 3 x 106 CAR cells/kg in 33 adults with relapsed/refractory B-cell ALL. Twenty-eight patients were evaluable for toxicity, 27 for response, and 5 patients were too early in their treatment to evaluate at the time of data cutoff.
Twenty-one patients were male, and the median age was 55 (range, 23 to 74).
Thirteen patients (46%) had minimal disease (<5% blasts) immediately prior to T-cell infusion, and 15 patients (54%) had morphologic disease of 5% to 100% blasts (median 63%).
Eighteen patients (64%) had received 2 prior lines of therapy, and 5 (18%) each had 3 or more prior lines.
Eight patients (29%) underwent prior allogeneic HSCT, 9 patients (32%) were Philadelphia chromosome positive (Ph+), and 3 (11%) had the T315I mutation.
The overall complete response (CR) rate was 89%, and the minimal residual disease-negative CR rate was 88%. The median time to CR was 22.5 days (range, 9 to 33).
The investigators performed a subgroup analysis and found that 100% of the 13 patients with minimal disease before therapy achieved a CR, compared to 79% of patients with morphologic disease.
Eighty-six percent (6/7) of patients who had a prior HSCT and 90% (18/20) without a prior HSCT achieved a CR. Eighty-nine percent (8/9) of Ph+ patients achieved a CR, and 89% (16/18) of Philadelphia-negative patients (89%) achieved a CR.
At a median follow-up of 6 months (range, 1 to 38 months), 12 patients remained disease-free, including 7 patients who had more than a year of follow-up. Seven patients are disease-free without a subsequent HSCT.
Nine patients relapsed during a follow-up of 3 to 8 months, and 10 patients proceeded to HSCT. Two relapses occurred after HSCT, one in a patient who had CD19-negative blasts, and 7 relapses occurred without HSCT.
The overall survival rate at 6 months was 57%, and the median survival was 8.5 months.
For those patients who had a transplant after CAR therapy, the median survival was 10.8 months, and the survival rate at 6 months was 68%.
Dr Park pointed out that maximum T-cell expansion occurred between days 7 and 14 and correlated with the occurrence of cytokine release syndrome (CRS). The T cells persisted for 1 to 3 months following infusion.
The main adverse events were those associated with CRS and neurologic changes. Severe CRS requiring vasopressors or mechanical ventilation occurred in 5 patients (18%) overall and in 5 patients (33%) with morphologic disease before therapy. Severe CRS did not occur in any patient with minimal disease before therapy.
Grade 3 or 4 neurotoxicity occurred in 7 patients (25%) overall, in 6 patients (40%) with morphologic disease, and in 1 with minimal disease (8%) before therapy.
The investigators observed no graft-vs-host disease exacerbation, and CRS was managed with an IL-6R inhibitor, steroids, or both.
Dr Park noted that the neurologic symptoms are reversible and can occur independently of CRS.
He also pointed out that CR rates were similar regardless of different disease risk factors, and that durable responses have been achieved in patients who did not have a subsequent HSCT. ![]()
*Information in the abstract differs from that presented at the meeting.
Credit: Charles Haymond
SAN FRANCISCO—JCAR015, a chimeric antigen receptor (CAR) T-cell therapy, can produce durable responses in patients with B-cell acute lymphoblastic leukemia (ALL) who do not undergo subsequent hematopoietic stem cell transplant (HSCT), new research suggests.
JCAR015 consists of autologous T cells genetically modified to express 19-28z chimeric antigen receptor (19-28z CAR) targeting CD19.
Jae H. Park, MD, of Memorial Sloan Kettering Cancer Center in New York, presented data on JCAR015 at the 2014 ASH Annual Meeting (abstract 382).* The study is sponsored by Memorial Sloan Kettering, but funding has also been provided by Juno Therapeutics, the company developing JCAR015.
JCAR015 was tested at a dose of 1 - 3 x 106 CAR cells/kg in 33 adults with relapsed/refractory B-cell ALL. Twenty-eight patients were evaluable for toxicity, 27 for response, and 5 patients were too early in their treatment to evaluate at the time of data cutoff.
Twenty-one patients were male, and the median age was 55 (range, 23 to 74).
Thirteen patients (46%) had minimal disease (<5% blasts) immediately prior to T-cell infusion, and 15 patients (54%) had morphologic disease of 5% to 100% blasts (median 63%).
Eighteen patients (64%) had received 2 prior lines of therapy, and 5 (18%) each had 3 or more prior lines.
Eight patients (29%) underwent prior allogeneic HSCT, 9 patients (32%) were Philadelphia chromosome positive (Ph+), and 3 (11%) had the T315I mutation.
The overall complete response (CR) rate was 89%, and the minimal residual disease-negative CR rate was 88%. The median time to CR was 22.5 days (range, 9 to 33).
The investigators performed a subgroup analysis and found that 100% of the 13 patients with minimal disease before therapy achieved a CR, compared to 79% of patients with morphologic disease.
Eighty-six percent (6/7) of patients who had a prior HSCT and 90% (18/20) without a prior HSCT achieved a CR. Eighty-nine percent (8/9) of Ph+ patients achieved a CR, and 89% (16/18) of Philadelphia-negative patients (89%) achieved a CR.
At a median follow-up of 6 months (range, 1 to 38 months), 12 patients remained disease-free, including 7 patients who had more than a year of follow-up. Seven patients are disease-free without a subsequent HSCT.
Nine patients relapsed during a follow-up of 3 to 8 months, and 10 patients proceeded to HSCT. Two relapses occurred after HSCT, one in a patient who had CD19-negative blasts, and 7 relapses occurred without HSCT.
The overall survival rate at 6 months was 57%, and the median survival was 8.5 months.
For those patients who had a transplant after CAR therapy, the median survival was 10.8 months, and the survival rate at 6 months was 68%.
Dr Park pointed out that maximum T-cell expansion occurred between days 7 and 14 and correlated with the occurrence of cytokine release syndrome (CRS). The T cells persisted for 1 to 3 months following infusion.
The main adverse events were those associated with CRS and neurologic changes. Severe CRS requiring vasopressors or mechanical ventilation occurred in 5 patients (18%) overall and in 5 patients (33%) with morphologic disease before therapy. Severe CRS did not occur in any patient with minimal disease before therapy.
Grade 3 or 4 neurotoxicity occurred in 7 patients (25%) overall, in 6 patients (40%) with morphologic disease, and in 1 with minimal disease (8%) before therapy.
The investigators observed no graft-vs-host disease exacerbation, and CRS was managed with an IL-6R inhibitor, steroids, or both.
Dr Park noted that the neurologic symptoms are reversible and can occur independently of CRS.
He also pointed out that CR rates were similar regardless of different disease risk factors, and that durable responses have been achieved in patients who did not have a subsequent HSCT. ![]()
*Information in the abstract differs from that presented at the meeting.
Combo shows promise for rel/ref MM

Credit: Linda Bartlett
SAN FRANCISCO—Combination therapy involving a novel monoclonal antibody (mAb) produces encouraging activity in relapsed or refractory multiple myeloma (MM), according to researchers.
The team conducted a phase 1b trial testing the IgG1 mAb SAR650984 in combination with lenalidomide and dexamethasone (SAR-len-dex).
The treatment produced an overall response rate (ORR) of 58% and a higher ORR among patients who received the highest dose of SAR.
Furthermore, the combination had a “very manageable safety profile,” according to study investigator Thomas Martin, MD, of the University of California at San Francisco.
“The safety findings are really consistent with those of the individual drugs,” he said.
Dr Martin presented these findings at the 2014 ASH Annual Meeting as abstract 83.* The trial was sponsored by Sanofi (the company developing SAR), but investigators also received research funding from Karyopharm, Bristol Myers Squibb, Millennium, and Celgene.
Dr Martin explained that SAR is a humanized IgG1 mAb that binds selectively to a unique epitope on the human CD38 receptor, and it has 4 potential mechanisms of action: antibody-dependent cellular cytotoxicity, complement-dependent cytotoxicity, direct apoptosis without crosslinking, and inhibition of CD38 enzyme activity.
He said there is “ample evidence” to suggest that SAR-len-dex would be active in MM. First, both lenalidomide and SAR have demonstrated single-agent activity in MM. Second, lenalidomide can increase IL-2 production, which leads to enhanced antibody-dependent cellular cytotoxicity. And finally, SAR and lenalidomide showed additive effects in a mouse model of MM.
With that in mind, Dr Martin and his colleagues decided to test SAR-len-dex in patients with relapsed or refractory MM.
The team enrolled 31 patients and administered SAR at 3 different dose levels. Patients received 3 mg/kg (n=4), 5 mg/kg (n=3), or 10 mg/kg (n=24) every 2 weeks. They received lenalidomide at 25 mg on days 1-21 per 28-day cycle and dexamethasone at 40 mg once a week on days 1, 8, 15, and 22.
The patients’ median age was 59 (range, 45-74), the median time since diagnosis was 4 years (range, 1-12), the median number of prior treatment regimens was 7 (range, 2-14), and the median number of prior lines of therapy was 4 (range, 1-11).
“The median time from the last lenalidomide-containing regimen was 9 months,” Dr Martin noted. “Ninety-four percent of the patients had prior lenalidomide, and 74% of these patients were lenalidomide refractory.”
Of the 29% of patients who had received prior pomalidomide, all were refractory to it. The same was true of the 48% of patients who received carfilzomib. And of the 94% of patients who received prior bortezomib, 52% were refractory to it.
Adverse events
The maximum-tolerated dose of SAR was not reached. Treatment-emergent adverse events occurring in 30% of patients or more included anemia, neutropenia, thrombocytopenia, febrile neutropenia, diarrhea, fatigue, insomnia, muscle spasms, nausea, pneumonia, pyrexia, and upper respiratory tract infections.
Grade 3/4 events occurring in 5% of patients or more included anemia, neutropenia, thrombocytopenia, febrile neutropenia, fatigue, insomnia, and pneumonia.
“All of these events are commonly associated with the backbone treatment of lenalidomide and dexamethasone, and no unexpected or untoward adverse events were seen,” Dr Martin noted.
The most common SAR-associated adverse events were infusion reactions. About 35% of patients experienced an infusion reaction in cycle 1, and 10% did so in cycle 2.
Most reactions were grade 1 and 2 and did not lead to treatment discontinuation. Two patients did discontinue treatment due to grade 3 infusion reactions, but both events were ultimately resolved.
Response and survival
The ORR was 58% (n=18), and the clinical benefit rate was 65% (n=20). Two patients had a stringent complete response, 7 had a very good partial response, 9 had a partial response, 2 had a minimal response, 6 had stable disease, 4 progressed, and 1 was not evaluable.
Responses were seen at all dose levels, but the best responses occurred in patients who received the highest dose of SAR. Among patients who received the highest dose, the ORR was 68%, and the clinical benefit rate was 65%.
The ORR was 50% in patients who were refractory to prior treatment with an immunomodulatory drug, 40% in patients who were refractory to carfilzomib, and 33% in patients who were refractory to pomalidomide.
At 9 months of follow-up, the median progression-free survival was 6.2 months. The median progression-free survival was not reached for patients who had received 1 to 2 prior lines of therapy, and it was 5.8 months for patients who had received 3 or more prior lines of therapy.
“SAR in combination with lenalidomide/dexamethasone showed encouraging activity in this heavily pretreated population,” Dr Martin said in closing, adding that the combination compares favorably to other treatments tested in patients who received the same number of prior lines of therapy. ![]()
*Information in the abstract differs from that presented at the meeting.
Credit: Linda Bartlett
SAN FRANCISCO—Combination therapy involving a novel monoclonal antibody (mAb) produces encouraging activity in relapsed or refractory multiple myeloma (MM), according to researchers.
The team conducted a phase 1b trial testing the IgG1 mAb SAR650984 in combination with lenalidomide and dexamethasone (SAR-len-dex).
The treatment produced an overall response rate (ORR) of 58% and a higher ORR among patients who received the highest dose of SAR.
Furthermore, the combination had a “very manageable safety profile,” according to study investigator Thomas Martin, MD, of the University of California at San Francisco.
“The safety findings are really consistent with those of the individual drugs,” he said.
Dr Martin presented these findings at the 2014 ASH Annual Meeting as abstract 83.* The trial was sponsored by Sanofi (the company developing SAR), but investigators also received research funding from Karyopharm, Bristol Myers Squibb, Millennium, and Celgene.
Dr Martin explained that SAR is a humanized IgG1 mAb that binds selectively to a unique epitope on the human CD38 receptor, and it has 4 potential mechanisms of action: antibody-dependent cellular cytotoxicity, complement-dependent cytotoxicity, direct apoptosis without crosslinking, and inhibition of CD38 enzyme activity.
He said there is “ample evidence” to suggest that SAR-len-dex would be active in MM. First, both lenalidomide and SAR have demonstrated single-agent activity in MM. Second, lenalidomide can increase IL-2 production, which leads to enhanced antibody-dependent cellular cytotoxicity. And finally, SAR and lenalidomide showed additive effects in a mouse model of MM.
With that in mind, Dr Martin and his colleagues decided to test SAR-len-dex in patients with relapsed or refractory MM.
The team enrolled 31 patients and administered SAR at 3 different dose levels. Patients received 3 mg/kg (n=4), 5 mg/kg (n=3), or 10 mg/kg (n=24) every 2 weeks. They received lenalidomide at 25 mg on days 1-21 per 28-day cycle and dexamethasone at 40 mg once a week on days 1, 8, 15, and 22.
The patients’ median age was 59 (range, 45-74), the median time since diagnosis was 4 years (range, 1-12), the median number of prior treatment regimens was 7 (range, 2-14), and the median number of prior lines of therapy was 4 (range, 1-11).
“The median time from the last lenalidomide-containing regimen was 9 months,” Dr Martin noted. “Ninety-four percent of the patients had prior lenalidomide, and 74% of these patients were lenalidomide refractory.”
Of the 29% of patients who had received prior pomalidomide, all were refractory to it. The same was true of the 48% of patients who received carfilzomib. And of the 94% of patients who received prior bortezomib, 52% were refractory to it.
Adverse events
The maximum-tolerated dose of SAR was not reached. Treatment-emergent adverse events occurring in 30% of patients or more included anemia, neutropenia, thrombocytopenia, febrile neutropenia, diarrhea, fatigue, insomnia, muscle spasms, nausea, pneumonia, pyrexia, and upper respiratory tract infections.
Grade 3/4 events occurring in 5% of patients or more included anemia, neutropenia, thrombocytopenia, febrile neutropenia, fatigue, insomnia, and pneumonia.
“All of these events are commonly associated with the backbone treatment of lenalidomide and dexamethasone, and no unexpected or untoward adverse events were seen,” Dr Martin noted.
The most common SAR-associated adverse events were infusion reactions. About 35% of patients experienced an infusion reaction in cycle 1, and 10% did so in cycle 2.
Most reactions were grade 1 and 2 and did not lead to treatment discontinuation. Two patients did discontinue treatment due to grade 3 infusion reactions, but both events were ultimately resolved.
Response and survival
The ORR was 58% (n=18), and the clinical benefit rate was 65% (n=20). Two patients had a stringent complete response, 7 had a very good partial response, 9 had a partial response, 2 had a minimal response, 6 had stable disease, 4 progressed, and 1 was not evaluable.
Responses were seen at all dose levels, but the best responses occurred in patients who received the highest dose of SAR. Among patients who received the highest dose, the ORR was 68%, and the clinical benefit rate was 65%.
The ORR was 50% in patients who were refractory to prior treatment with an immunomodulatory drug, 40% in patients who were refractory to carfilzomib, and 33% in patients who were refractory to pomalidomide.
At 9 months of follow-up, the median progression-free survival was 6.2 months. The median progression-free survival was not reached for patients who had received 1 to 2 prior lines of therapy, and it was 5.8 months for patients who had received 3 or more prior lines of therapy.
“SAR in combination with lenalidomide/dexamethasone showed encouraging activity in this heavily pretreated population,” Dr Martin said in closing, adding that the combination compares favorably to other treatments tested in patients who received the same number of prior lines of therapy. ![]()
*Information in the abstract differs from that presented at the meeting.
Credit: Linda Bartlett
SAN FRANCISCO—Combination therapy involving a novel monoclonal antibody (mAb) produces encouraging activity in relapsed or refractory multiple myeloma (MM), according to researchers.
The team conducted a phase 1b trial testing the IgG1 mAb SAR650984 in combination with lenalidomide and dexamethasone (SAR-len-dex).
The treatment produced an overall response rate (ORR) of 58% and a higher ORR among patients who received the highest dose of SAR.
Furthermore, the combination had a “very manageable safety profile,” according to study investigator Thomas Martin, MD, of the University of California at San Francisco.
“The safety findings are really consistent with those of the individual drugs,” he said.
Dr Martin presented these findings at the 2014 ASH Annual Meeting as abstract 83.* The trial was sponsored by Sanofi (the company developing SAR), but investigators also received research funding from Karyopharm, Bristol Myers Squibb, Millennium, and Celgene.
Dr Martin explained that SAR is a humanized IgG1 mAb that binds selectively to a unique epitope on the human CD38 receptor, and it has 4 potential mechanisms of action: antibody-dependent cellular cytotoxicity, complement-dependent cytotoxicity, direct apoptosis without crosslinking, and inhibition of CD38 enzyme activity.
He said there is “ample evidence” to suggest that SAR-len-dex would be active in MM. First, both lenalidomide and SAR have demonstrated single-agent activity in MM. Second, lenalidomide can increase IL-2 production, which leads to enhanced antibody-dependent cellular cytotoxicity. And finally, SAR and lenalidomide showed additive effects in a mouse model of MM.
With that in mind, Dr Martin and his colleagues decided to test SAR-len-dex in patients with relapsed or refractory MM.
The team enrolled 31 patients and administered SAR at 3 different dose levels. Patients received 3 mg/kg (n=4), 5 mg/kg (n=3), or 10 mg/kg (n=24) every 2 weeks. They received lenalidomide at 25 mg on days 1-21 per 28-day cycle and dexamethasone at 40 mg once a week on days 1, 8, 15, and 22.
The patients’ median age was 59 (range, 45-74), the median time since diagnosis was 4 years (range, 1-12), the median number of prior treatment regimens was 7 (range, 2-14), and the median number of prior lines of therapy was 4 (range, 1-11).
“The median time from the last lenalidomide-containing regimen was 9 months,” Dr Martin noted. “Ninety-four percent of the patients had prior lenalidomide, and 74% of these patients were lenalidomide refractory.”
Of the 29% of patients who had received prior pomalidomide, all were refractory to it. The same was true of the 48% of patients who received carfilzomib. And of the 94% of patients who received prior bortezomib, 52% were refractory to it.
Adverse events
The maximum-tolerated dose of SAR was not reached. Treatment-emergent adverse events occurring in 30% of patients or more included anemia, neutropenia, thrombocytopenia, febrile neutropenia, diarrhea, fatigue, insomnia, muscle spasms, nausea, pneumonia, pyrexia, and upper respiratory tract infections.
Grade 3/4 events occurring in 5% of patients or more included anemia, neutropenia, thrombocytopenia, febrile neutropenia, fatigue, insomnia, and pneumonia.
“All of these events are commonly associated with the backbone treatment of lenalidomide and dexamethasone, and no unexpected or untoward adverse events were seen,” Dr Martin noted.
The most common SAR-associated adverse events were infusion reactions. About 35% of patients experienced an infusion reaction in cycle 1, and 10% did so in cycle 2.
Most reactions were grade 1 and 2 and did not lead to treatment discontinuation. Two patients did discontinue treatment due to grade 3 infusion reactions, but both events were ultimately resolved.
Response and survival
The ORR was 58% (n=18), and the clinical benefit rate was 65% (n=20). Two patients had a stringent complete response, 7 had a very good partial response, 9 had a partial response, 2 had a minimal response, 6 had stable disease, 4 progressed, and 1 was not evaluable.
Responses were seen at all dose levels, but the best responses occurred in patients who received the highest dose of SAR. Among patients who received the highest dose, the ORR was 68%, and the clinical benefit rate was 65%.
The ORR was 50% in patients who were refractory to prior treatment with an immunomodulatory drug, 40% in patients who were refractory to carfilzomib, and 33% in patients who were refractory to pomalidomide.
At 9 months of follow-up, the median progression-free survival was 6.2 months. The median progression-free survival was not reached for patients who had received 1 to 2 prior lines of therapy, and it was 5.8 months for patients who had received 3 or more prior lines of therapy.
“SAR in combination with lenalidomide/dexamethasone showed encouraging activity in this heavily pretreated population,” Dr Martin said in closing, adding that the combination compares favorably to other treatments tested in patients who received the same number of prior lines of therapy. ![]()
*Information in the abstract differs from that presented at the meeting.
New data added to obinutuzumab label

Credit: Bill Branson
The US Food and Drug Administration (FDA) has approved a supplemental biologics license application for obinutuzumab (Gazyva) in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia (CLL).
The approval adds to the drug’s label data from stage 2 of the CLL11 study, which showed that obinutuzumab plus chlorambucil offers significant clinical improvements when compared head-to-head with rituximab plus chlorambucil.
This includes progression-free survival (PFS), complete response (CR), and minimal residual disease (MRD) data from stage 2 of the study. In addition, overall survival data was added from stage 1, in which researchers compared obinutuzumab plus chlorambucil to chlorambucil alone.
The label now reflects that obinutuzumab plus chlorambucil improved PFS compared to rituximab plus chlorambucil. The median PFS was 26.7 months and 14.9 months, respectively (hazard ratio=0.42, P<0.0001).
Additionally, obinutuzumab plus chlorambucil nearly tripled the CR rate when compared to rituximab plus chlorambucil. The CR rates were 26.1% and 8.8%, respectively.
Of the patients who achieved a CR with or without complete recovery from abnormal blood cell counts, 19% (18/94) of patients in the obinutuzumab arm and 6% (2/34) in the rituximab arm were MRD negative in the bone marrow.
Forty-one percent (39/94) of patients in the obinutuzumab arm and 12% (4/34) in the rituximab arm were MRD-negative in the peripheral blood.
At nearly 2 years, the rate of death was 9% (22/238) for patients who received obinutuzumab plus chlorambucil and 20% (24/118) for those who received chlorambucil alone (hazard ratio=0.41). The median overall survival has not yet been reached.
About obinutuzumab
Obinutuzumab is an engineered monoclonal antibody designed to attach to CD20 on B cells. The drug attacks targeted cells both directly and together with the body’s immune system.
The prescribing information for obinutuzumab includes warnings that the drug can cause serious or life-threatening side effects. These include hepatitis B reactivation, progressive multifocal leukoencephalopathy, infusion reactions, tumor lysis syndrome, infections, and neutropenia.
The most common side effects of the drug are infusion reactions, neutropenia, thrombocytopenia, anemia, fever, cough, nausea, and diarrhea.
Obinutuzumab was FDA-approved for use in combination with chlorambucil to treat previously untreated CLL in November 2013. The drug (which is known as Gazyvaro in Europe) was approved by the European Commission for the same indication in July 2014.
Obinutuzumab was discovered by Roche Glycart AG, an independent research unit of Roche. In the US, the drug is part of a collaboration between Genentech and Biogen Idec.![]()
Credit: Bill Branson
The US Food and Drug Administration (FDA) has approved a supplemental biologics license application for obinutuzumab (Gazyva) in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia (CLL).
The approval adds to the drug’s label data from stage 2 of the CLL11 study, which showed that obinutuzumab plus chlorambucil offers significant clinical improvements when compared head-to-head with rituximab plus chlorambucil.
This includes progression-free survival (PFS), complete response (CR), and minimal residual disease (MRD) data from stage 2 of the study. In addition, overall survival data was added from stage 1, in which researchers compared obinutuzumab plus chlorambucil to chlorambucil alone.
The label now reflects that obinutuzumab plus chlorambucil improved PFS compared to rituximab plus chlorambucil. The median PFS was 26.7 months and 14.9 months, respectively (hazard ratio=0.42, P<0.0001).
Additionally, obinutuzumab plus chlorambucil nearly tripled the CR rate when compared to rituximab plus chlorambucil. The CR rates were 26.1% and 8.8%, respectively.
Of the patients who achieved a CR with or without complete recovery from abnormal blood cell counts, 19% (18/94) of patients in the obinutuzumab arm and 6% (2/34) in the rituximab arm were MRD negative in the bone marrow.
Forty-one percent (39/94) of patients in the obinutuzumab arm and 12% (4/34) in the rituximab arm were MRD-negative in the peripheral blood.
At nearly 2 years, the rate of death was 9% (22/238) for patients who received obinutuzumab plus chlorambucil and 20% (24/118) for those who received chlorambucil alone (hazard ratio=0.41). The median overall survival has not yet been reached.
About obinutuzumab
Obinutuzumab is an engineered monoclonal antibody designed to attach to CD20 on B cells. The drug attacks targeted cells both directly and together with the body’s immune system.
The prescribing information for obinutuzumab includes warnings that the drug can cause serious or life-threatening side effects. These include hepatitis B reactivation, progressive multifocal leukoencephalopathy, infusion reactions, tumor lysis syndrome, infections, and neutropenia.
The most common side effects of the drug are infusion reactions, neutropenia, thrombocytopenia, anemia, fever, cough, nausea, and diarrhea.
Obinutuzumab was FDA-approved for use in combination with chlorambucil to treat previously untreated CLL in November 2013. The drug (which is known as Gazyvaro in Europe) was approved by the European Commission for the same indication in July 2014.
Obinutuzumab was discovered by Roche Glycart AG, an independent research unit of Roche. In the US, the drug is part of a collaboration between Genentech and Biogen Idec.![]()
Credit: Bill Branson
The US Food and Drug Administration (FDA) has approved a supplemental biologics license application for obinutuzumab (Gazyva) in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia (CLL).
The approval adds to the drug’s label data from stage 2 of the CLL11 study, which showed that obinutuzumab plus chlorambucil offers significant clinical improvements when compared head-to-head with rituximab plus chlorambucil.
This includes progression-free survival (PFS), complete response (CR), and minimal residual disease (MRD) data from stage 2 of the study. In addition, overall survival data was added from stage 1, in which researchers compared obinutuzumab plus chlorambucil to chlorambucil alone.
The label now reflects that obinutuzumab plus chlorambucil improved PFS compared to rituximab plus chlorambucil. The median PFS was 26.7 months and 14.9 months, respectively (hazard ratio=0.42, P<0.0001).
Additionally, obinutuzumab plus chlorambucil nearly tripled the CR rate when compared to rituximab plus chlorambucil. The CR rates were 26.1% and 8.8%, respectively.
Of the patients who achieved a CR with or without complete recovery from abnormal blood cell counts, 19% (18/94) of patients in the obinutuzumab arm and 6% (2/34) in the rituximab arm were MRD negative in the bone marrow.
Forty-one percent (39/94) of patients in the obinutuzumab arm and 12% (4/34) in the rituximab arm were MRD-negative in the peripheral blood.
At nearly 2 years, the rate of death was 9% (22/238) for patients who received obinutuzumab plus chlorambucil and 20% (24/118) for those who received chlorambucil alone (hazard ratio=0.41). The median overall survival has not yet been reached.
About obinutuzumab
Obinutuzumab is an engineered monoclonal antibody designed to attach to CD20 on B cells. The drug attacks targeted cells both directly and together with the body’s immune system.
The prescribing information for obinutuzumab includes warnings that the drug can cause serious or life-threatening side effects. These include hepatitis B reactivation, progressive multifocal leukoencephalopathy, infusion reactions, tumor lysis syndrome, infections, and neutropenia.
The most common side effects of the drug are infusion reactions, neutropenia, thrombocytopenia, anemia, fever, cough, nausea, and diarrhea.
Obinutuzumab was FDA-approved for use in combination with chlorambucil to treat previously untreated CLL in November 2013. The drug (which is known as Gazyvaro in Europe) was approved by the European Commission for the same indication in July 2014.
Obinutuzumab was discovered by Roche Glycart AG, an independent research unit of Roche. In the US, the drug is part of a collaboration between Genentech and Biogen Idec.![]()
Extended anticoagulation offers transient benefit

SAN FRANCISCO—New research indicates that extending anticoagulant therapy to 2 years can reduce the risk of recurrent venous thromboembolism (VTE) without increasing major bleeding, but this benefit only lasts while patients are receiving the therapy.
In the PADIS-PE study, patients with a first episode of symptomatic, unprovoked pulmonary embolism (PE) received 6 months of treatment with a vitamin K antagonist (VKA), followed by 18 months of warfarin or placebo.
Patients who received warfarin had a 77% reduction in the relative risk of recurrent VTE or major bleeding while they received treatment. But an additional 2 years of follow-up showed that this benefit was lost once patients stopped anticoagulation.
Francis Couturaud, MD, PhD, of the Brest University Hospital Center in Brest, France, presented these data at the 2014 ASH Annual Meeting as LBA-3.*
He and his colleagues randomized patients to receive warfarin (n=184) or placebo (n=187) for 18 months after their intial VKA treatment. Patients were followed for an additional 24 months after treatment ended.
Most baseline characteristics were similar between the treatment arms, although there was a significantly higher percentage of females in the warfarin arm.
“[Overall,] the mean age was below 60, [and] the mean BMI [body mass index] was below 30,” Dr Couturaud noted. “About 4% of patients had previous cancer [that had been] resolved for more than 2 years, 8% had previous distal DVT [deep vein thrombosis] or superficial venous thrombosis, a quarter of women were on estrogen-containing pills, and about one-third had an associated proximal DVT at the time of PE diagnosis.”
“Before the randomization, the mean duration of VKA [therapy] was 6 months, and the mean percentage of time within the therapeutic range was 70. At inclusion, about one-third of patients had residual perfusion defect, about 15% had residual DVT, the mean D-dimer level was below 500 μg/L, and about 27% had thrombophilia.”
Results
The study’s primary outcome was the composite of recurrent VTE or major bleeding during the 18-month treatment period. Significantly fewer patients met this endpoint in the warfarin arm than in the placebo arm—6 (3.3%) and 25 (13.5%), respectively (hazard ratio [HR]=0.23, P=0.0004).
Likewise, the number of patients with recurrent VTE at 18 months was significantly lower in the warfarin arm than in the placebo arm—3 (1.7%) and 25 (13.5%), respectively (HR=0.11, P<0.0001).
On the other hand, there was no significant difference in the rate of major bleeding between the treatment arms at 18 months. Four patients (2.2%) had major bleeding in the warfarin arm, as did 1 (0.5%) in the placebo arm (HR=4.07, P=0.18).
At 42 months, there was no significant difference between the treatment arms with regard to the composite outcome, the rate of recurrent VTE, or the rate of major bleeding.
The composite outcome occurred in 33 (20.8%) patients in the warfarin arm and 42 (24%) in the placebo arm (HR=0.74, P=0.19). Recurrent VTE occurred in 28 (17.9%) and 39 patients (22.1%), respectively (HR=0.67, P=0.10). And major bleeding occurred in 6 (3.5%) and 5 patients (3%), respectively (HR=1.12, P=0.71).
“[E]xtending anticoagulation for 18 additional months was associated with a major relative risk reduction of 77% of recurrent VTE or major bleeding during the treatment period,” Dr Couturaud said in summary. “However, this benefit was lost during a long-term follow-up of 2 years after stopping anticoagulation.”
“In addition, recurrent VTE occurred in 80% of cases as recurrent PE and in 90% of cases as unprovoked VTE. So additional investigations are needed to identify subgroups of patients at lower risk who may not need indefinite anticoagulation.”
This study was sponsored by Brest University Hospital. Investigators received research funding from Actelion Pharmaceuticals, GlaxoSmithKline, Bristol-Myers Squibb, Boehringer Ingelheim, Sanofi, LEO Pharma, and Bayer. ![]()
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—New research indicates that extending anticoagulant therapy to 2 years can reduce the risk of recurrent venous thromboembolism (VTE) without increasing major bleeding, but this benefit only lasts while patients are receiving the therapy.
In the PADIS-PE study, patients with a first episode of symptomatic, unprovoked pulmonary embolism (PE) received 6 months of treatment with a vitamin K antagonist (VKA), followed by 18 months of warfarin or placebo.
Patients who received warfarin had a 77% reduction in the relative risk of recurrent VTE or major bleeding while they received treatment. But an additional 2 years of follow-up showed that this benefit was lost once patients stopped anticoagulation.
Francis Couturaud, MD, PhD, of the Brest University Hospital Center in Brest, France, presented these data at the 2014 ASH Annual Meeting as LBA-3.*
He and his colleagues randomized patients to receive warfarin (n=184) or placebo (n=187) for 18 months after their intial VKA treatment. Patients were followed for an additional 24 months after treatment ended.
Most baseline characteristics were similar between the treatment arms, although there was a significantly higher percentage of females in the warfarin arm.
“[Overall,] the mean age was below 60, [and] the mean BMI [body mass index] was below 30,” Dr Couturaud noted. “About 4% of patients had previous cancer [that had been] resolved for more than 2 years, 8% had previous distal DVT [deep vein thrombosis] or superficial venous thrombosis, a quarter of women were on estrogen-containing pills, and about one-third had an associated proximal DVT at the time of PE diagnosis.”
“Before the randomization, the mean duration of VKA [therapy] was 6 months, and the mean percentage of time within the therapeutic range was 70. At inclusion, about one-third of patients had residual perfusion defect, about 15% had residual DVT, the mean D-dimer level was below 500 μg/L, and about 27% had thrombophilia.”
Results
The study’s primary outcome was the composite of recurrent VTE or major bleeding during the 18-month treatment period. Significantly fewer patients met this endpoint in the warfarin arm than in the placebo arm—6 (3.3%) and 25 (13.5%), respectively (hazard ratio [HR]=0.23, P=0.0004).
Likewise, the number of patients with recurrent VTE at 18 months was significantly lower in the warfarin arm than in the placebo arm—3 (1.7%) and 25 (13.5%), respectively (HR=0.11, P<0.0001).
On the other hand, there was no significant difference in the rate of major bleeding between the treatment arms at 18 months. Four patients (2.2%) had major bleeding in the warfarin arm, as did 1 (0.5%) in the placebo arm (HR=4.07, P=0.18).
At 42 months, there was no significant difference between the treatment arms with regard to the composite outcome, the rate of recurrent VTE, or the rate of major bleeding.
The composite outcome occurred in 33 (20.8%) patients in the warfarin arm and 42 (24%) in the placebo arm (HR=0.74, P=0.19). Recurrent VTE occurred in 28 (17.9%) and 39 patients (22.1%), respectively (HR=0.67, P=0.10). And major bleeding occurred in 6 (3.5%) and 5 patients (3%), respectively (HR=1.12, P=0.71).
“[E]xtending anticoagulation for 18 additional months was associated with a major relative risk reduction of 77% of recurrent VTE or major bleeding during the treatment period,” Dr Couturaud said in summary. “However, this benefit was lost during a long-term follow-up of 2 years after stopping anticoagulation.”
“In addition, recurrent VTE occurred in 80% of cases as recurrent PE and in 90% of cases as unprovoked VTE. So additional investigations are needed to identify subgroups of patients at lower risk who may not need indefinite anticoagulation.”
This study was sponsored by Brest University Hospital. Investigators received research funding from Actelion Pharmaceuticals, GlaxoSmithKline, Bristol-Myers Squibb, Boehringer Ingelheim, Sanofi, LEO Pharma, and Bayer. ![]()
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—New research indicates that extending anticoagulant therapy to 2 years can reduce the risk of recurrent venous thromboembolism (VTE) without increasing major bleeding, but this benefit only lasts while patients are receiving the therapy.
In the PADIS-PE study, patients with a first episode of symptomatic, unprovoked pulmonary embolism (PE) received 6 months of treatment with a vitamin K antagonist (VKA), followed by 18 months of warfarin or placebo.
Patients who received warfarin had a 77% reduction in the relative risk of recurrent VTE or major bleeding while they received treatment. But an additional 2 years of follow-up showed that this benefit was lost once patients stopped anticoagulation.
Francis Couturaud, MD, PhD, of the Brest University Hospital Center in Brest, France, presented these data at the 2014 ASH Annual Meeting as LBA-3.*
He and his colleagues randomized patients to receive warfarin (n=184) or placebo (n=187) for 18 months after their intial VKA treatment. Patients were followed for an additional 24 months after treatment ended.
Most baseline characteristics were similar between the treatment arms, although there was a significantly higher percentage of females in the warfarin arm.
“[Overall,] the mean age was below 60, [and] the mean BMI [body mass index] was below 30,” Dr Couturaud noted. “About 4% of patients had previous cancer [that had been] resolved for more than 2 years, 8% had previous distal DVT [deep vein thrombosis] or superficial venous thrombosis, a quarter of women were on estrogen-containing pills, and about one-third had an associated proximal DVT at the time of PE diagnosis.”
“Before the randomization, the mean duration of VKA [therapy] was 6 months, and the mean percentage of time within the therapeutic range was 70. At inclusion, about one-third of patients had residual perfusion defect, about 15% had residual DVT, the mean D-dimer level was below 500 μg/L, and about 27% had thrombophilia.”
Results
The study’s primary outcome was the composite of recurrent VTE or major bleeding during the 18-month treatment period. Significantly fewer patients met this endpoint in the warfarin arm than in the placebo arm—6 (3.3%) and 25 (13.5%), respectively (hazard ratio [HR]=0.23, P=0.0004).
Likewise, the number of patients with recurrent VTE at 18 months was significantly lower in the warfarin arm than in the placebo arm—3 (1.7%) and 25 (13.5%), respectively (HR=0.11, P<0.0001).
On the other hand, there was no significant difference in the rate of major bleeding between the treatment arms at 18 months. Four patients (2.2%) had major bleeding in the warfarin arm, as did 1 (0.5%) in the placebo arm (HR=4.07, P=0.18).
At 42 months, there was no significant difference between the treatment arms with regard to the composite outcome, the rate of recurrent VTE, or the rate of major bleeding.
The composite outcome occurred in 33 (20.8%) patients in the warfarin arm and 42 (24%) in the placebo arm (HR=0.74, P=0.19). Recurrent VTE occurred in 28 (17.9%) and 39 patients (22.1%), respectively (HR=0.67, P=0.10). And major bleeding occurred in 6 (3.5%) and 5 patients (3%), respectively (HR=1.12, P=0.71).
“[E]xtending anticoagulation for 18 additional months was associated with a major relative risk reduction of 77% of recurrent VTE or major bleeding during the treatment period,” Dr Couturaud said in summary. “However, this benefit was lost during a long-term follow-up of 2 years after stopping anticoagulation.”
“In addition, recurrent VTE occurred in 80% of cases as recurrent PE and in 90% of cases as unprovoked VTE. So additional investigations are needed to identify subgroups of patients at lower risk who may not need indefinite anticoagulation.”
This study was sponsored by Brest University Hospital. Investigators received research funding from Actelion Pharmaceuticals, GlaxoSmithKline, Bristol-Myers Squibb, Boehringer Ingelheim, Sanofi, LEO Pharma, and Bayer.
*Information in the abstract differs from that presented at the meeting.
FDA releases warning about IV solutions
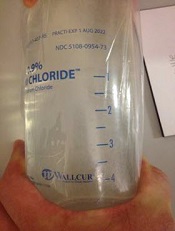
The US Food and Drug Administration (FDA) is alerting healthcare professionals not to use Wallcur, LLC, simulated intravenous (IV) products in human or animal patients, as the products are for training purposes only.
The FDA has become aware that some Wallcur training IV products have been distributed to healthcare facilities and administered to patients.
There have been reports of serious adverse events associated with some of these products, such as Practi IV Solution Bags.
Before administering IV solutions to patients, healthcare providers should carefully check the labels to ensure that products are not training products.
Wallcur’s training products, which may bear the words “for clinical simulation,” are not to be administered to patients.
If you suspect that any Wallcur training IV products may have been administered to a patient, whether or not the incident has resulted in an adverse event, please report the incident to the FDA’s MedWatch Adverse Event Reporting Program.
The FDA said it will continue to investigate and monitor this issue. The agency is also working with the Centers for Disease Control and Prevention to inform healthcare professionals and state health departments.
The US Food and Drug Administration (FDA) is alerting healthcare professionals not to use Wallcur, LLC, simulated intravenous (IV) products in human or animal patients, as the products are for training purposes only.
The FDA has become aware that some Wallcur training IV products have been distributed to healthcare facilities and administered to patients.
There have been reports of serious adverse events associated with some of these products, such as Practi IV Solution Bags.
Before administering IV solutions to patients, healthcare providers should carefully check the labels to ensure that products are not training products.
Wallcur’s training products, which may bear the words “for clinical simulation,” are not to be administered to patients.
If you suspect that any Wallcur training IV products may have been administered to a patient, whether or not the incident has resulted in an adverse event, please report the incident to the FDA’s MedWatch Adverse Event Reporting Program.
The FDA said it will continue to investigate and monitor this issue. The agency is also working with the Centers for Disease Control and Prevention to inform healthcare professionals and state health departments.
The US Food and Drug Administration (FDA) is alerting healthcare professionals not to use Wallcur, LLC, simulated intravenous (IV) products in human or animal patients, as the products are for training purposes only.
The FDA has become aware that some Wallcur training IV products have been distributed to healthcare facilities and administered to patients.
There have been reports of serious adverse events associated with some of these products, such as Practi IV Solution Bags.
Before administering IV solutions to patients, healthcare providers should carefully check the labels to ensure that products are not training products.
Wallcur’s training products, which may bear the words “for clinical simulation,” are not to be administered to patients.
If you suspect that any Wallcur training IV products may have been administered to a patient, whether or not the incident has resulted in an adverse event, please report the incident to the FDA’s MedWatch Adverse Event Reporting Program.
The FDA said it will continue to investigate and monitor this issue. The agency is also working with the Centers for Disease Control and Prevention to inform healthcare professionals and state health departments.
Teams map paths to drug resistance in cancers, MPNs

Researchers say they’ve discovered key events that prompt drug resistance in myeloproliferative neoplasms (MPNs) and certain solid tumor malignancies.
By mapping the steps that myelofibrosis, melanoma, and breast cancer cells use to become resistant to drugs, the investigators believe they have identified better targets for blocking those pathways to ensure current therapies are effective.
The groups reported these findings in two papers published in Science Signaling.
“In our studies, we developed a screening technology that allows us to quickly identify the routes cells can use to become resistant, and, using that information, we were able to show that these mechanisms seen in the laboratory are actually also occurring in patients’ tumors,” said Kris Wood, PhD, an assistant professor at Duke University in Durham, North Carolina, and senior author of both studies.
In the first study, Dr Wood and his colleagues conducted a broad survey of the known cell-signaling pathways that, when activated, have the potential to trigger drug resistance.
Using this screening technology, the researchers were able to corroborate the results of earlier drug-resistance studies, while also finding pathways that had not previously been described.
The team identified the MAPK and PI3K pathways, which are known to mediate drug resistance. But they also found that activation of the Notch1 pathway caused drug resistance, and inhibiting Notch1 signaling restored drug efficacy.
“Interestingly, the mechanisms are quite similar among all 3 of the cancer types,” Dr Wood noted. “In breast cancer and melanoma, our findings suggest the same Notch1 pathway as a potential driver of resistance to a wide array of targeted therapies—a role that has not been widely acknowledged previously.”
The investigators found that Notch signaling mediated drug resistance to an estrogen receptor-targeted therapy used in breast cancer and to a kinase-targeted therapy used in melanoma. And tumors from some patients with relapsed breast cancer or melanoma had increased markers of Notch1 signaling.
In the second study, the researchers used the aforementioned pathway-centric screen to track a pair of separate signaling pathways downstream of RAS, a protein frequently activated in MPNs.
The team found the pathway mediated by RAS promoted drug resistance in hematopoietic cell lines containing an activating mutation in JAK2. And RAS signaling led to the phosphorylation-mediated inactivation of the pro-apoptotic protein BAD, which enabled cell survival.
Combining JAK inhibitors with inhibitors of kinases downstream of RAS signaling prompted apoptosis in cell lines that were resistant to JAK inhibitors. This suggests such combinations may be effective for treating drug-resistant MPNs.
“Together, these findings improve our ability to stratify patients into groups more and less likely to respond to therapy and design drug combinations that work together to block or delay resistance,” Dr Wood concluded.
Researchers say they’ve discovered key events that prompt drug resistance in myeloproliferative neoplasms (MPNs) and certain solid tumor malignancies.
By mapping the steps that myelofibrosis, melanoma, and breast cancer cells use to become resistant to drugs, the investigators believe they have identified better targets for blocking those pathways to ensure current therapies are effective.
The groups reported these findings in two papers published in Science Signaling.
“In our studies, we developed a screening technology that allows us to quickly identify the routes cells can use to become resistant, and, using that information, we were able to show that these mechanisms seen in the laboratory are actually also occurring in patients’ tumors,” said Kris Wood, PhD, an assistant professor at Duke University in Durham, North Carolina, and senior author of both studies.
In the first study, Dr Wood and his colleagues conducted a broad survey of the known cell-signaling pathways that, when activated, have the potential to trigger drug resistance.
Using this screening technology, the researchers were able to corroborate the results of earlier drug-resistance studies, while also finding pathways that had not previously been described.
The team identified the MAPK and PI3K pathways, which are known to mediate drug resistance. But they also found that activation of the Notch1 pathway caused drug resistance, and inhibiting Notch1 signaling restored drug efficacy.
“Interestingly, the mechanisms are quite similar among all 3 of the cancer types,” Dr Wood noted. “In breast cancer and melanoma, our findings suggest the same Notch1 pathway as a potential driver of resistance to a wide array of targeted therapies—a role that has not been widely acknowledged previously.”
The investigators found that Notch signaling mediated drug resistance to an estrogen receptor-targeted therapy used in breast cancer and to a kinase-targeted therapy used in melanoma. And tumors from some patients with relapsed breast cancer or melanoma had increased markers of Notch1 signaling.
In the second study, the researchers used the aforementioned pathway-centric screen to track a pair of separate signaling pathways downstream of RAS, a protein frequently activated in MPNs.
The team found the pathway mediated by RAS promoted drug resistance in hematopoietic cell lines containing an activating mutation in JAK2. And RAS signaling led to the phosphorylation-mediated inactivation of the pro-apoptotic protein BAD, which enabled cell survival.
Combining JAK inhibitors with inhibitors of kinases downstream of RAS signaling prompted apoptosis in cell lines that were resistant to JAK inhibitors. This suggests such combinations may be effective for treating drug-resistant MPNs.
“Together, these findings improve our ability to stratify patients into groups more and less likely to respond to therapy and design drug combinations that work together to block or delay resistance,” Dr Wood concluded.
Researchers say they’ve discovered key events that prompt drug resistance in myeloproliferative neoplasms (MPNs) and certain solid tumor malignancies.
By mapping the steps that myelofibrosis, melanoma, and breast cancer cells use to become resistant to drugs, the investigators believe they have identified better targets for blocking those pathways to ensure current therapies are effective.
The groups reported these findings in two papers published in Science Signaling.
“In our studies, we developed a screening technology that allows us to quickly identify the routes cells can use to become resistant, and, using that information, we were able to show that these mechanisms seen in the laboratory are actually also occurring in patients’ tumors,” said Kris Wood, PhD, an assistant professor at Duke University in Durham, North Carolina, and senior author of both studies.
In the first study, Dr Wood and his colleagues conducted a broad survey of the known cell-signaling pathways that, when activated, have the potential to trigger drug resistance.
Using this screening technology, the researchers were able to corroborate the results of earlier drug-resistance studies, while also finding pathways that had not previously been described.
The team identified the MAPK and PI3K pathways, which are known to mediate drug resistance. But they also found that activation of the Notch1 pathway caused drug resistance, and inhibiting Notch1 signaling restored drug efficacy.
“Interestingly, the mechanisms are quite similar among all 3 of the cancer types,” Dr Wood noted. “In breast cancer and melanoma, our findings suggest the same Notch1 pathway as a potential driver of resistance to a wide array of targeted therapies—a role that has not been widely acknowledged previously.”
The investigators found that Notch signaling mediated drug resistance to an estrogen receptor-targeted therapy used in breast cancer and to a kinase-targeted therapy used in melanoma. And tumors from some patients with relapsed breast cancer or melanoma had increased markers of Notch1 signaling.
In the second study, the researchers used the aforementioned pathway-centric screen to track a pair of separate signaling pathways downstream of RAS, a protein frequently activated in MPNs.
The team found the pathway mediated by RAS promoted drug resistance in hematopoietic cell lines containing an activating mutation in JAK2. And RAS signaling led to the phosphorylation-mediated inactivation of the pro-apoptotic protein BAD, which enabled cell survival.
Combining JAK inhibitors with inhibitors of kinases downstream of RAS signaling prompted apoptosis in cell lines that were resistant to JAK inhibitors. This suggests such combinations may be effective for treating drug-resistant MPNs.
“Together, these findings improve our ability to stratify patients into groups more and less likely to respond to therapy and design drug combinations that work together to block or delay resistance,” Dr Wood concluded.
Drug combats complications of SCD

SAN FRANCISCO—Pharmaceutical-grade L-glutamine can reduce the risk of complications in patients with sickle cell disease (SCD), according to new research.
In a phase 3 study of more than 200 patients, those who received L-glutamine saw a reduction in sickle cell crises, hospitalizations, and the incidence of acute chest syndrome (ACS) when compared to patients who received placebo.
In addition, L-glutamine appeared to have a synergistic effect with hydroxyurea.
Yutaka Niihara, MD, of Emmaus Medical, Inc., in Torrance, California, presented these results at the 2014 ASH Annual Meeting (abstract 86*). Emmaus Medical produced the pharmaceutical-grade L-glutamine used in the study.
Dr Niihara noted that nicotinamide adenine dinucleotide (NAD) is an important physiological antioxidant in red blood cells. But in sickled red blood cells, NAD redox potential is significantly compromised.
So he and his colleagues hypothesized that glutamine, a precursor for NAD, can improve NAD redox potential and modify the destructive effect of increased oxidation and the pathophysiology of SCD. They also theorized that glutamine will decrease the frequency of vaso-occlusive crises.
To test their theories, the researchers enrolled 230 patients from 31 different sites on a phase 3 trial. Patients had sickle cell anemia (SS) or sickle B0 thalassemia. They were 5 years of age or older, and some were receiving hydroxyurea.
Patients were randomized 2:1 to receive L-glutamine at 0.3 g/kg twice daily (maximum 30 g/day) or placebo (maltodextrin) at 0.3 g/kg twice daily for 48 weeks. The researchers had discovered high variation in the quality of over-the-counter L-glutamine, so they used pharmaceutical-grade L-glutamine only.
In all, 152 patients received L-glutamine, and 78 received placebo. Demographics and baseline characteristics were similar between the two treatment arms.
The median age was 19 (range, 5-57) in the L-glutamine arm and 17 (range, 5-58) in the placebo arm. There were more females than males in both arms—52% and 57.7%, respectively. And most patients in both arms had sickle cell anemia—89.5% and 91%, respectively.
Safety and efficacy
Dr Niihara said there were no serious adverse events attributable to L-glutamine and no dose modifications due to toxicity.
There were more gastrointestinal events (such as constipation and flatulence) in the L-glutamine arm (8.6%) than in the placebo arm (5.2%). But there was no difference in other adverse events between the two arms.
The study’s primary endpoint was the frequency of painful sickle cell crises. Patients in the L-glutamine arm had 25% fewer crises than patients in the placebo arm (P=0.008).
In patients aged 18 and younger, the median number of sickle cell crises was 3 in the L-glutamine arm and 4 in the placebo arm (P<0.001). The numbers were the same in patients older than 18 (P<0.001) and among patients receiving hydroxyurea (P<0.001).
“Those patients, even though they were on hydroxyurea, they have shown improvements [with L-glutamine],” Dr Niihara said. “And it appears there is some synergistic effect . . ., certainly more than just an additive effect.”
Dr Niihara also noted that patients who received placebo took less than 2 months to experience a first sickle cell crisis, but, for patients on L-glutamine, it took almost 3 months before they had a first crisis. The time to a first crisis was a median of 87 days in the L-glutamine arm and 54 days in the placebo arm (P=0.010).
The study’s secondary endpoint was the frequency of hospitalizations. Compared to patients in the placebo arm, those in the L-glutamine arm had a 33% reduction in hospitalizations (P=0.005) and a 41% reduction in the length of hospital stay (P=0.022).
The researchers also looked at the incidence of ACS and found that L-glutamine was associated with a 58% reduction in ACS. The incidence was 26.9% in the placebo arm and 11.9% in the L-glutamine arm (P=0.006).
“We observed this cascade improvement [with L-glutamine],” Dr Niihara noted. “And what we mean [by that] is that, with glutamine, there is less chance of having painful crises, but if patients have to have crises, they have less chance of being hospitalized. And if they have to be hospitalized, their stays in the hospital are shorter. And, again, if they have to be hospitalized, there’s less chance of them going to the ICU with acute chest syndrome.”
Dr Niihara said the researchers’ next steps are to investigate L-glutamine in a clinical setting, in patients younger than 5 years old, in pregnant women, and as part of combination therapy.
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—Pharmaceutical-grade L-glutamine can reduce the risk of complications in patients with sickle cell disease (SCD), according to new research.
In a phase 3 study of more than 200 patients, those who received L-glutamine saw a reduction in sickle cell crises, hospitalizations, and the incidence of acute chest syndrome (ACS) when compared to patients who received placebo.
In addition, L-glutamine appeared to have a synergistic effect with hydroxyurea.
Yutaka Niihara, MD, of Emmaus Medical, Inc., in Torrance, California, presented these results at the 2014 ASH Annual Meeting (abstract 86*). Emmaus Medical produced the pharmaceutical-grade L-glutamine used in the study.
Dr Niihara noted that nicotinamide adenine dinucleotide (NAD) is an important physiological antioxidant in red blood cells. But in sickled red blood cells, NAD redox potential is significantly compromised.
So he and his colleagues hypothesized that glutamine, a precursor for NAD, can improve NAD redox potential and modify the destructive effect of increased oxidation and the pathophysiology of SCD. They also theorized that glutamine will decrease the frequency of vaso-occlusive crises.
To test their theories, the researchers enrolled 230 patients from 31 different sites on a phase 3 trial. Patients had sickle cell anemia (SS) or sickle B0 thalassemia. They were 5 years of age or older, and some were receiving hydroxyurea.
Patients were randomized 2:1 to receive L-glutamine at 0.3 g/kg twice daily (maximum 30 g/day) or placebo (maltodextrin) at 0.3 g/kg twice daily for 48 weeks. The researchers had discovered high variation in the quality of over-the-counter L-glutamine, so they used pharmaceutical-grade L-glutamine only.
In all, 152 patients received L-glutamine, and 78 received placebo. Demographics and baseline characteristics were similar between the two treatment arms.
The median age was 19 (range, 5-57) in the L-glutamine arm and 17 (range, 5-58) in the placebo arm. There were more females than males in both arms—52% and 57.7%, respectively. And most patients in both arms had sickle cell anemia—89.5% and 91%, respectively.
Safety and efficacy
Dr Niihara said there were no serious adverse events attributable to L-glutamine and no dose modifications due to toxicity.
There were more gastrointestinal events (such as constipation and flatulence) in the L-glutamine arm (8.6%) than in the placebo arm (5.2%). But there was no difference in other adverse events between the two arms.
The study’s primary endpoint was the frequency of painful sickle cell crises. Patients in the L-glutamine arm had 25% fewer crises than patients in the placebo arm (P=0.008).
In patients aged 18 and younger, the median number of sickle cell crises was 3 in the L-glutamine arm and 4 in the placebo arm (P<0.001). The numbers were the same in patients older than 18 (P<0.001) and among patients receiving hydroxyurea (P<0.001).
“Those patients, even though they were on hydroxyurea, they have shown improvements [with L-glutamine],” Dr Niihara said. “And it appears there is some synergistic effect . . ., certainly more than just an additive effect.”
Dr Niihara also noted that patients who received placebo took less than 2 months to experience a first sickle cell crisis, but, for patients on L-glutamine, it took almost 3 months before they had a first crisis. The time to a first crisis was a median of 87 days in the L-glutamine arm and 54 days in the placebo arm (P=0.010).
The study’s secondary endpoint was the frequency of hospitalizations. Compared to patients in the placebo arm, those in the L-glutamine arm had a 33% reduction in hospitalizations (P=0.005) and a 41% reduction in the length of hospital stay (P=0.022).
The researchers also looked at the incidence of ACS and found that L-glutamine was associated with a 58% reduction in ACS. The incidence was 26.9% in the placebo arm and 11.9% in the L-glutamine arm (P=0.006).
“We observed this cascade improvement [with L-glutamine],” Dr Niihara noted. “And what we mean [by that] is that, with glutamine, there is less chance of having painful crises, but if patients have to have crises, they have less chance of being hospitalized. And if they have to be hospitalized, their stays in the hospital are shorter. And, again, if they have to be hospitalized, there’s less chance of them going to the ICU with acute chest syndrome.”
Dr Niihara said the researchers’ next steps are to investigate L-glutamine in a clinical setting, in patients younger than 5 years old, in pregnant women, and as part of combination therapy.
*Information in the abstract differs from that presented at the meeting.
SAN FRANCISCO—Pharmaceutical-grade L-glutamine can reduce the risk of complications in patients with sickle cell disease (SCD), according to new research.
In a phase 3 study of more than 200 patients, those who received L-glutamine saw a reduction in sickle cell crises, hospitalizations, and the incidence of acute chest syndrome (ACS) when compared to patients who received placebo.
In addition, L-glutamine appeared to have a synergistic effect with hydroxyurea.
Yutaka Niihara, MD, of Emmaus Medical, Inc., in Torrance, California, presented these results at the 2014 ASH Annual Meeting (abstract 86*). Emmaus Medical produced the pharmaceutical-grade L-glutamine used in the study.
Dr Niihara noted that nicotinamide adenine dinucleotide (NAD) is an important physiological antioxidant in red blood cells. But in sickled red blood cells, NAD redox potential is significantly compromised.
So he and his colleagues hypothesized that glutamine, a precursor for NAD, can improve NAD redox potential and modify the destructive effect of increased oxidation and the pathophysiology of SCD. They also theorized that glutamine will decrease the frequency of vaso-occlusive crises.
To test their theories, the researchers enrolled 230 patients from 31 different sites on a phase 3 trial. Patients had sickle cell anemia (SS) or sickle B0 thalassemia. They were 5 years of age or older, and some were receiving hydroxyurea.
Patients were randomized 2:1 to receive L-glutamine at 0.3 g/kg twice daily (maximum 30 g/day) or placebo (maltodextrin) at 0.3 g/kg twice daily for 48 weeks. The researchers had discovered high variation in the quality of over-the-counter L-glutamine, so they used pharmaceutical-grade L-glutamine only.
In all, 152 patients received L-glutamine, and 78 received placebo. Demographics and baseline characteristics were similar between the two treatment arms.
The median age was 19 (range, 5-57) in the L-glutamine arm and 17 (range, 5-58) in the placebo arm. There were more females than males in both arms—52% and 57.7%, respectively. And most patients in both arms had sickle cell anemia—89.5% and 91%, respectively.
Safety and efficacy
Dr Niihara said there were no serious adverse events attributable to L-glutamine and no dose modifications due to toxicity.
There were more gastrointestinal events (such as constipation and flatulence) in the L-glutamine arm (8.6%) than in the placebo arm (5.2%). But there was no difference in other adverse events between the two arms.
The study’s primary endpoint was the frequency of painful sickle cell crises. Patients in the L-glutamine arm had 25% fewer crises than patients in the placebo arm (P=0.008).
In patients aged 18 and younger, the median number of sickle cell crises was 3 in the L-glutamine arm and 4 in the placebo arm (P<0.001). The numbers were the same in patients older than 18 (P<0.001) and among patients receiving hydroxyurea (P<0.001).
“Those patients, even though they were on hydroxyurea, they have shown improvements [with L-glutamine],” Dr Niihara said. “And it appears there is some synergistic effect . . ., certainly more than just an additive effect.”
Dr Niihara also noted that patients who received placebo took less than 2 months to experience a first sickle cell crisis, but, for patients on L-glutamine, it took almost 3 months before they had a first crisis. The time to a first crisis was a median of 87 days in the L-glutamine arm and 54 days in the placebo arm (P=0.010).
The study’s secondary endpoint was the frequency of hospitalizations. Compared to patients in the placebo arm, those in the L-glutamine arm had a 33% reduction in hospitalizations (P=0.005) and a 41% reduction in the length of hospital stay (P=0.022).
The researchers also looked at the incidence of ACS and found that L-glutamine was associated with a 58% reduction in ACS. The incidence was 26.9% in the placebo arm and 11.9% in the L-glutamine arm (P=0.006).
“We observed this cascade improvement [with L-glutamine],” Dr Niihara noted. “And what we mean [by that] is that, with glutamine, there is less chance of having painful crises, but if patients have to have crises, they have less chance of being hospitalized. And if they have to be hospitalized, their stays in the hospital are shorter. And, again, if they have to be hospitalized, there’s less chance of them going to the ICU with acute chest syndrome.”
Dr Niihara said the researchers’ next steps are to investigate L-glutamine in a clinical setting, in patients younger than 5 years old, in pregnant women, and as part of combination therapy.
*Information in the abstract differs from that presented at the meeting.