User login
Why neutrophils have conflicting roles in cancer

Credit: Volker Brinkmann
New research has revealed distinct subpopulations of neutrophils that have conflicting functions when it comes to cancer.
Investigators identified a population of “normal,” high-density neutrophils (HDNs) that have anti-tumor properties and a population of low-density
neutrophils (LDNs) that exhibit pro-tumor activity.
They also found that the ratio of HDNs to LDNs determines whether the neutrophils have a pro- or anti-cancer effect overall.
This suggests we may be able to fight cancers by increasing the proportion of the anti-tumor HDNs while limiting the pro-tumor LDNs, according to Zvika Granot, PhD, of Hebrew University Medical School in Jerusalem, Israel.
“The novel distinction between harmful and beneficial neutrophils opens up new diagnostic and therapeutic opportunities,” Dr Granot said. “We are currently evaluating the effects of boosting the helpful anti-tumor neutrophil population, while limiting the tumor-promoting neutrophil population, on progression of the disease. If successful, this therapeutic strategy may take us closer to developing effective new therapies for cancer.”
Dr Granot and his colleagues described their discovery of LDNs and HDNs in Cell Reports.
The investigators found that LDNs were rare in healthy control subjects, but they accumulated in tumor-bearing mice and in cancer patients. HDNs exhibited cytotoxicity toward cancer cells and retarded tumor growth, but LDNs did not.
LDNs had impaired neutrophil function and immunosuppressive properties. They consisted of immature myeloid-derived suppressor cells and mature cells that were derived from HDNs.
HDNs transformed into LDNs in a TGF-β-dependent fashion, losing their anti-tumor properties and gaining immunosuppressive properties.
In the early stages of cancer development, HDNs prevailed. But as cancer progressed, the LDNs took over, and the overall neutrophil contribution became tumor-promoting.
The investigators noted that the expansion of LDNs was a relatively late event. So although these neutrophils likely contribute to tumor growth and progression, it’s less likely that they contribute to tumor initiation.
Regardless, this research challenges the concept that mature neutrophils are limited in their ability to change. It shows that neutrophils are not a homogeneous population of cells and may consist of multiple subtypes. And it provides a mechanistic explanation for the controversy surrounding neutrophil function in cancer. ![]()
Credit: Volker Brinkmann
New research has revealed distinct subpopulations of neutrophils that have conflicting functions when it comes to cancer.
Investigators identified a population of “normal,” high-density neutrophils (HDNs) that have anti-tumor properties and a population of low-density
neutrophils (LDNs) that exhibit pro-tumor activity.
They also found that the ratio of HDNs to LDNs determines whether the neutrophils have a pro- or anti-cancer effect overall.
This suggests we may be able to fight cancers by increasing the proportion of the anti-tumor HDNs while limiting the pro-tumor LDNs, according to Zvika Granot, PhD, of Hebrew University Medical School in Jerusalem, Israel.
“The novel distinction between harmful and beneficial neutrophils opens up new diagnostic and therapeutic opportunities,” Dr Granot said. “We are currently evaluating the effects of boosting the helpful anti-tumor neutrophil population, while limiting the tumor-promoting neutrophil population, on progression of the disease. If successful, this therapeutic strategy may take us closer to developing effective new therapies for cancer.”
Dr Granot and his colleagues described their discovery of LDNs and HDNs in Cell Reports.
The investigators found that LDNs were rare in healthy control subjects, but they accumulated in tumor-bearing mice and in cancer patients. HDNs exhibited cytotoxicity toward cancer cells and retarded tumor growth, but LDNs did not.
LDNs had impaired neutrophil function and immunosuppressive properties. They consisted of immature myeloid-derived suppressor cells and mature cells that were derived from HDNs.
HDNs transformed into LDNs in a TGF-β-dependent fashion, losing their anti-tumor properties and gaining immunosuppressive properties.
In the early stages of cancer development, HDNs prevailed. But as cancer progressed, the LDNs took over, and the overall neutrophil contribution became tumor-promoting.
The investigators noted that the expansion of LDNs was a relatively late event. So although these neutrophils likely contribute to tumor growth and progression, it’s less likely that they contribute to tumor initiation.
Regardless, this research challenges the concept that mature neutrophils are limited in their ability to change. It shows that neutrophils are not a homogeneous population of cells and may consist of multiple subtypes. And it provides a mechanistic explanation for the controversy surrounding neutrophil function in cancer. ![]()
Credit: Volker Brinkmann
New research has revealed distinct subpopulations of neutrophils that have conflicting functions when it comes to cancer.
Investigators identified a population of “normal,” high-density neutrophils (HDNs) that have anti-tumor properties and a population of low-density
neutrophils (LDNs) that exhibit pro-tumor activity.
They also found that the ratio of HDNs to LDNs determines whether the neutrophils have a pro- or anti-cancer effect overall.
This suggests we may be able to fight cancers by increasing the proportion of the anti-tumor HDNs while limiting the pro-tumor LDNs, according to Zvika Granot, PhD, of Hebrew University Medical School in Jerusalem, Israel.
“The novel distinction between harmful and beneficial neutrophils opens up new diagnostic and therapeutic opportunities,” Dr Granot said. “We are currently evaluating the effects of boosting the helpful anti-tumor neutrophil population, while limiting the tumor-promoting neutrophil population, on progression of the disease. If successful, this therapeutic strategy may take us closer to developing effective new therapies for cancer.”
Dr Granot and his colleagues described their discovery of LDNs and HDNs in Cell Reports.
The investigators found that LDNs were rare in healthy control subjects, but they accumulated in tumor-bearing mice and in cancer patients. HDNs exhibited cytotoxicity toward cancer cells and retarded tumor growth, but LDNs did not.
LDNs had impaired neutrophil function and immunosuppressive properties. They consisted of immature myeloid-derived suppressor cells and mature cells that were derived from HDNs.
HDNs transformed into LDNs in a TGF-β-dependent fashion, losing their anti-tumor properties and gaining immunosuppressive properties.
In the early stages of cancer development, HDNs prevailed. But as cancer progressed, the LDNs took over, and the overall neutrophil contribution became tumor-promoting.
The investigators noted that the expansion of LDNs was a relatively late event. So although these neutrophils likely contribute to tumor growth and progression, it’s less likely that they contribute to tumor initiation.
Regardless, this research challenges the concept that mature neutrophils are limited in their ability to change. It shows that neutrophils are not a homogeneous population of cells and may consist of multiple subtypes. And it provides a mechanistic explanation for the controversy surrounding neutrophil function in cancer. ![]()
Group creates detailed map of proteins in human body
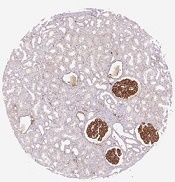
in the renal glomeruli,
the network responsible
for filtering the blood
Credit: Human Protein Atlas
Scientists say they’ve completed the first major analysis based on the Human Protein Atlas, providing a detailed picture of proteins linked to cancer, the number of proteins present in the bloodstream, and all proteins targeted by drugs.
The group described their work in Science.
The Human Protein Atlas, a multinational research project, recently launched an open-source, tissue-based, interactive map of the human proteome.
In the Science article, researchers described how they studied the human proteome. The group analyzed samples representing the 44 major tissues and organs in the human body.
They used 24,028 antibodies, corresponding to 16,975 protein-encoding genes, to produce more than 13 million tissue-based immunohistochemistry images. They complemented this analysis with RNA-sequencing data for 32 of the 44 tissue types.
In this way, the scientists mapped the distribution of proteins in all major tissues and organs in the human body. They identified proteins restricted to certain tissues—such as the brain, heart, or liver—and those present throughout the body.
Almost half of the nearly 17,000 protein-encoding genes are expressed in all the tissues the researchers analyzed. The group also found that 3171 proteins are secreted from cells, and 5570 are located in the membrane systems of cells.
“This is important information for the pharmaceutical industry,” said study author Mathias Uhlén, PhD, a professor at the KTH Royal Institute of Technology in Stockholm, Sweden, and the director of the Human Protein Atlas program.
“We show that 70% of the current targets for approved pharmaceutical drugs are either secreted or membrane-bound proteins. Interestingly, 30% of these protein targets are found in all analyzed tissues and organs. This could help explain some side effects of drugs and, thus, might have consequences for future drug development.” ![]()
in the renal glomeruli,
the network responsible
for filtering the blood
Credit: Human Protein Atlas
Scientists say they’ve completed the first major analysis based on the Human Protein Atlas, providing a detailed picture of proteins linked to cancer, the number of proteins present in the bloodstream, and all proteins targeted by drugs.
The group described their work in Science.
The Human Protein Atlas, a multinational research project, recently launched an open-source, tissue-based, interactive map of the human proteome.
In the Science article, researchers described how they studied the human proteome. The group analyzed samples representing the 44 major tissues and organs in the human body.
They used 24,028 antibodies, corresponding to 16,975 protein-encoding genes, to produce more than 13 million tissue-based immunohistochemistry images. They complemented this analysis with RNA-sequencing data for 32 of the 44 tissue types.
In this way, the scientists mapped the distribution of proteins in all major tissues and organs in the human body. They identified proteins restricted to certain tissues—such as the brain, heart, or liver—and those present throughout the body.
Almost half of the nearly 17,000 protein-encoding genes are expressed in all the tissues the researchers analyzed. The group also found that 3171 proteins are secreted from cells, and 5570 are located in the membrane systems of cells.
“This is important information for the pharmaceutical industry,” said study author Mathias Uhlén, PhD, a professor at the KTH Royal Institute of Technology in Stockholm, Sweden, and the director of the Human Protein Atlas program.
“We show that 70% of the current targets for approved pharmaceutical drugs are either secreted or membrane-bound proteins. Interestingly, 30% of these protein targets are found in all analyzed tissues and organs. This could help explain some side effects of drugs and, thus, might have consequences for future drug development.” ![]()
in the renal glomeruli,
the network responsible
for filtering the blood
Credit: Human Protein Atlas
Scientists say they’ve completed the first major analysis based on the Human Protein Atlas, providing a detailed picture of proteins linked to cancer, the number of proteins present in the bloodstream, and all proteins targeted by drugs.
The group described their work in Science.
The Human Protein Atlas, a multinational research project, recently launched an open-source, tissue-based, interactive map of the human proteome.
In the Science article, researchers described how they studied the human proteome. The group analyzed samples representing the 44 major tissues and organs in the human body.
They used 24,028 antibodies, corresponding to 16,975 protein-encoding genes, to produce more than 13 million tissue-based immunohistochemistry images. They complemented this analysis with RNA-sequencing data for 32 of the 44 tissue types.
In this way, the scientists mapped the distribution of proteins in all major tissues and organs in the human body. They identified proteins restricted to certain tissues—such as the brain, heart, or liver—and those present throughout the body.
Almost half of the nearly 17,000 protein-encoding genes are expressed in all the tissues the researchers analyzed. The group also found that 3171 proteins are secreted from cells, and 5570 are located in the membrane systems of cells.
“This is important information for the pharmaceutical industry,” said study author Mathias Uhlén, PhD, a professor at the KTH Royal Institute of Technology in Stockholm, Sweden, and the director of the Human Protein Atlas program.
“We show that 70% of the current targets for approved pharmaceutical drugs are either secreted or membrane-bound proteins. Interestingly, 30% of these protein targets are found in all analyzed tissues and organs. This could help explain some side effects of drugs and, thus, might have consequences for future drug development.” ![]()
CO2 tells malaria-carrying mosquitoes when to land

working on an experiment
involving a wind tunnel
Credit: Carrie Rosema
House-dwelling, malaria-carrying mosquitoes can detect minute changes in concentrations of exhaled carbon dioxide to determine when humans are present, according to research published in the Journal of Chemical Ecology.
Anopheles gambiae mosquitoes spend much of their adult lives indoors, where they are constantly exposed to human odor, even when people are absent.
But researchers found these mosquitoes respond very weakly to human skin odor alone.
Experiments showed that mosquitoes were more likely to a land on a source of skin odor if carbon dioxide was also present, even at very low levels.
“Responding strongly to human skin odor alone once inside a dwelling where human odor is ubiquitous is a highly inefficient means for the mosquito of locating a feeding site,” said study author Ring Cardé, PhD, of the University of California, Riverside.
“We already know that mosquitoes will readily fly upwind towards human skin odor, but landing, the final stage of host location, which typically takes place indoors, does not occur unless a fluctuating concentration of carbon dioxide indicates that a human host is present.”
Dr Cardé and his colleagues discovered the importance of carbon dioxide in mosquitoes’ landing patterns by studying Anopheles gambiae mosquitoes collected in Cameroon.
The researchers collected skin odor by using pieces of white polyester gauze worn by one of the study authors in a cotton sock for 4 to 6 hours before the experiments began. The team then recorded the mosquitoes’ landing behavior with a video camera equipped with night vision.
The landing behavior “dramatically increased” with the addition of carbon dioxide at a range of concentrations above ambient. This was true even when the carbon dioxide level was just 0.015% above ambient within the assay cage.
These results suggest the mosquitoes use a “sit-and-wait” ambush strategy during which they ignore persistent human odor until a living human is present.
One take-home message from this work is that researchers investigating which human odors mediate host-finding and which compounds are good mosquito repellents need to precisely control exposure to carbon dioxide. A researcher entering an assay room quickly elevates the level of carbon dioxide, thereby altering the mosquitoes’ behavior.
“It also would be useful next to see if mosquitoes’ response to skin odor is similarly affected by carbon dioxide in outdoor situations and how these interactions play out in human dwellings,” Dr Cardé noted. ![]()
working on an experiment
involving a wind tunnel
Credit: Carrie Rosema
House-dwelling, malaria-carrying mosquitoes can detect minute changes in concentrations of exhaled carbon dioxide to determine when humans are present, according to research published in the Journal of Chemical Ecology.
Anopheles gambiae mosquitoes spend much of their adult lives indoors, where they are constantly exposed to human odor, even when people are absent.
But researchers found these mosquitoes respond very weakly to human skin odor alone.
Experiments showed that mosquitoes were more likely to a land on a source of skin odor if carbon dioxide was also present, even at very low levels.
“Responding strongly to human skin odor alone once inside a dwelling where human odor is ubiquitous is a highly inefficient means for the mosquito of locating a feeding site,” said study author Ring Cardé, PhD, of the University of California, Riverside.
“We already know that mosquitoes will readily fly upwind towards human skin odor, but landing, the final stage of host location, which typically takes place indoors, does not occur unless a fluctuating concentration of carbon dioxide indicates that a human host is present.”
Dr Cardé and his colleagues discovered the importance of carbon dioxide in mosquitoes’ landing patterns by studying Anopheles gambiae mosquitoes collected in Cameroon.
The researchers collected skin odor by using pieces of white polyester gauze worn by one of the study authors in a cotton sock for 4 to 6 hours before the experiments began. The team then recorded the mosquitoes’ landing behavior with a video camera equipped with night vision.
The landing behavior “dramatically increased” with the addition of carbon dioxide at a range of concentrations above ambient. This was true even when the carbon dioxide level was just 0.015% above ambient within the assay cage.
These results suggest the mosquitoes use a “sit-and-wait” ambush strategy during which they ignore persistent human odor until a living human is present.
One take-home message from this work is that researchers investigating which human odors mediate host-finding and which compounds are good mosquito repellents need to precisely control exposure to carbon dioxide. A researcher entering an assay room quickly elevates the level of carbon dioxide, thereby altering the mosquitoes’ behavior.
“It also would be useful next to see if mosquitoes’ response to skin odor is similarly affected by carbon dioxide in outdoor situations and how these interactions play out in human dwellings,” Dr Cardé noted. ![]()
working on an experiment
involving a wind tunnel
Credit: Carrie Rosema
House-dwelling, malaria-carrying mosquitoes can detect minute changes in concentrations of exhaled carbon dioxide to determine when humans are present, according to research published in the Journal of Chemical Ecology.
Anopheles gambiae mosquitoes spend much of their adult lives indoors, where they are constantly exposed to human odor, even when people are absent.
But researchers found these mosquitoes respond very weakly to human skin odor alone.
Experiments showed that mosquitoes were more likely to a land on a source of skin odor if carbon dioxide was also present, even at very low levels.
“Responding strongly to human skin odor alone once inside a dwelling where human odor is ubiquitous is a highly inefficient means for the mosquito of locating a feeding site,” said study author Ring Cardé, PhD, of the University of California, Riverside.
“We already know that mosquitoes will readily fly upwind towards human skin odor, but landing, the final stage of host location, which typically takes place indoors, does not occur unless a fluctuating concentration of carbon dioxide indicates that a human host is present.”
Dr Cardé and his colleagues discovered the importance of carbon dioxide in mosquitoes’ landing patterns by studying Anopheles gambiae mosquitoes collected in Cameroon.
The researchers collected skin odor by using pieces of white polyester gauze worn by one of the study authors in a cotton sock for 4 to 6 hours before the experiments began. The team then recorded the mosquitoes’ landing behavior with a video camera equipped with night vision.
The landing behavior “dramatically increased” with the addition of carbon dioxide at a range of concentrations above ambient. This was true even when the carbon dioxide level was just 0.015% above ambient within the assay cage.
These results suggest the mosquitoes use a “sit-and-wait” ambush strategy during which they ignore persistent human odor until a living human is present.
One take-home message from this work is that researchers investigating which human odors mediate host-finding and which compounds are good mosquito repellents need to precisely control exposure to carbon dioxide. A researcher entering an assay room quickly elevates the level of carbon dioxide, thereby altering the mosquitoes’ behavior.
“It also would be useful next to see if mosquitoes’ response to skin odor is similarly affected by carbon dioxide in outdoor situations and how these interactions play out in human dwellings,” Dr Cardé noted. ![]()
Theorem helps pinpoint start of patient recovery

Credit: CDC
The 2500-year-old Pythagorean theorem could be the most effective way to identify the point at which a patient’s health begins to improve, a new study suggests.
Researchers made the discovery while examining receiver operating characteristic (ROC) curves, which are used to measure changes in a patient’s health status.
“It all comes down to choosing a point on a curve to determine when recovery has occurred,” said study author Rob Froud, PhD, of the University of Warwick in Coventry, UK.
“For many chronic conditions, epidemiologists agree that the correct point to choose is that which is closest to the top-left corner of the plot containing the curve. As we stopped to think about it, it struck us as obvious that the way to choose this point was by using Pythagoras’s theorem.”
The theorem states that, in a right-angled triangle, the sum of the squares of the 2 right-angled sides is equal to the square of the hypotenuse (the longer diagonal that joins the 2 right-angled sides).
With this formula (a2+b2=c2), a person can determine the length of the hypotenuse when given the length of the other 2 sides.
“We set about exploring the implications of this and how it might change conclusions in research,” Dr Froud said. “We conducted several experiments using real trial data, and it seems using Pythagoras’s theorem makes a material difference.”
“It helps to identify the point at which a patient has improved with more consistency and accuracy than other methods commonly used. The moral of the story is that, before you throw out the old stuff in the attic, just go through it one last time, as there may be something in there that is still relevant and useful.”
Dr Froud and his colleague Gary Abel, PhD, of the University of Cambridge in the UK, described this research in PLOS ONE. ![]()
Credit: CDC
The 2500-year-old Pythagorean theorem could be the most effective way to identify the point at which a patient’s health begins to improve, a new study suggests.
Researchers made the discovery while examining receiver operating characteristic (ROC) curves, which are used to measure changes in a patient’s health status.
“It all comes down to choosing a point on a curve to determine when recovery has occurred,” said study author Rob Froud, PhD, of the University of Warwick in Coventry, UK.
“For many chronic conditions, epidemiologists agree that the correct point to choose is that which is closest to the top-left corner of the plot containing the curve. As we stopped to think about it, it struck us as obvious that the way to choose this point was by using Pythagoras’s theorem.”
The theorem states that, in a right-angled triangle, the sum of the squares of the 2 right-angled sides is equal to the square of the hypotenuse (the longer diagonal that joins the 2 right-angled sides).
With this formula (a2+b2=c2), a person can determine the length of the hypotenuse when given the length of the other 2 sides.
“We set about exploring the implications of this and how it might change conclusions in research,” Dr Froud said. “We conducted several experiments using real trial data, and it seems using Pythagoras’s theorem makes a material difference.”
“It helps to identify the point at which a patient has improved with more consistency and accuracy than other methods commonly used. The moral of the story is that, before you throw out the old stuff in the attic, just go through it one last time, as there may be something in there that is still relevant and useful.”
Dr Froud and his colleague Gary Abel, PhD, of the University of Cambridge in the UK, described this research in PLOS ONE. ![]()
Credit: CDC
The 2500-year-old Pythagorean theorem could be the most effective way to identify the point at which a patient’s health begins to improve, a new study suggests.
Researchers made the discovery while examining receiver operating characteristic (ROC) curves, which are used to measure changes in a patient’s health status.
“It all comes down to choosing a point on a curve to determine when recovery has occurred,” said study author Rob Froud, PhD, of the University of Warwick in Coventry, UK.
“For many chronic conditions, epidemiologists agree that the correct point to choose is that which is closest to the top-left corner of the plot containing the curve. As we stopped to think about it, it struck us as obvious that the way to choose this point was by using Pythagoras’s theorem.”
The theorem states that, in a right-angled triangle, the sum of the squares of the 2 right-angled sides is equal to the square of the hypotenuse (the longer diagonal that joins the 2 right-angled sides).
With this formula (a2+b2=c2), a person can determine the length of the hypotenuse when given the length of the other 2 sides.
“We set about exploring the implications of this and how it might change conclusions in research,” Dr Froud said. “We conducted several experiments using real trial data, and it seems using Pythagoras’s theorem makes a material difference.”
“It helps to identify the point at which a patient has improved with more consistency and accuracy than other methods commonly used. The moral of the story is that, before you throw out the old stuff in the attic, just go through it one last time, as there may be something in there that is still relevant and useful.”
Dr Froud and his colleague Gary Abel, PhD, of the University of Cambridge in the UK, described this research in PLOS ONE. ![]()
Gains in CLL are ‘Advance of the Year’

Credit: NIH
The “transformation” of treatment for chronic lymphocytic leukemia (CLL) is the “Advance of the Year” for 2015, according to a report by the American Society of Clinical Oncology (ASCO).
The report said 4 therapies that were recently approved in the US fill a major unmet need for CLL patients—obinutuzumab and ofatumumab for patients with previously untreated CLL and idelalisib and ibrutinib for patients with relapsed or refractory CLL.
“For many older patients, especially, these drugs essentially offer the first chance at effective treatment, since the side effects of earlier options were simply too toxic for many to handle,” said Gregory Masters, MD, ASCO expert and co-executive editor of the report.
The report, “Clinical Cancer Advances 2015: ASCO’s Annual Report on Progress Against Cancer,” is available in the Journal of Clinical Oncology and on ASCO’s cancer research advocacy website, CancerProgress.net.
The report was developed under the direction of an 18-person editorial board of experts from a wide range of oncology specialties. It features:
- The top cancer research advances of the past year: Identifying major trends in cancer prevention and screening, treatment, quality of life, survivorship, and tumor biology
- A Decade in Review: Recounting improvements in cancer care since the first issue of Clinical Cancer Advances
- The 10-Year Horizon: Previewing trends likely to shape the next decade of cancer care, including genomic technology, nanomedicine, and health information technologies
- Progress in Rare Cancers: Highlighting promising early achievements in treating certain uncommon but devastating cancers.
“This has truly been a banner year for CLL and for clinical cancer research as a whole,” said ASCO President Peter P. Yu, MD. “Advances in cancer prevention and care, especially those in precision medicine, are offering stunning new possibilities for patients.” ![]()
Credit: NIH
The “transformation” of treatment for chronic lymphocytic leukemia (CLL) is the “Advance of the Year” for 2015, according to a report by the American Society of Clinical Oncology (ASCO).
The report said 4 therapies that were recently approved in the US fill a major unmet need for CLL patients—obinutuzumab and ofatumumab for patients with previously untreated CLL and idelalisib and ibrutinib for patients with relapsed or refractory CLL.
“For many older patients, especially, these drugs essentially offer the first chance at effective treatment, since the side effects of earlier options were simply too toxic for many to handle,” said Gregory Masters, MD, ASCO expert and co-executive editor of the report.
The report, “Clinical Cancer Advances 2015: ASCO’s Annual Report on Progress Against Cancer,” is available in the Journal of Clinical Oncology and on ASCO’s cancer research advocacy website, CancerProgress.net.
The report was developed under the direction of an 18-person editorial board of experts from a wide range of oncology specialties. It features:
- The top cancer research advances of the past year: Identifying major trends in cancer prevention and screening, treatment, quality of life, survivorship, and tumor biology
- A Decade in Review: Recounting improvements in cancer care since the first issue of Clinical Cancer Advances
- The 10-Year Horizon: Previewing trends likely to shape the next decade of cancer care, including genomic technology, nanomedicine, and health information technologies
- Progress in Rare Cancers: Highlighting promising early achievements in treating certain uncommon but devastating cancers.
“This has truly been a banner year for CLL and for clinical cancer research as a whole,” said ASCO President Peter P. Yu, MD. “Advances in cancer prevention and care, especially those in precision medicine, are offering stunning new possibilities for patients.” ![]()
Credit: NIH
The “transformation” of treatment for chronic lymphocytic leukemia (CLL) is the “Advance of the Year” for 2015, according to a report by the American Society of Clinical Oncology (ASCO).
The report said 4 therapies that were recently approved in the US fill a major unmet need for CLL patients—obinutuzumab and ofatumumab for patients with previously untreated CLL and idelalisib and ibrutinib for patients with relapsed or refractory CLL.
“For many older patients, especially, these drugs essentially offer the first chance at effective treatment, since the side effects of earlier options were simply too toxic for many to handle,” said Gregory Masters, MD, ASCO expert and co-executive editor of the report.
The report, “Clinical Cancer Advances 2015: ASCO’s Annual Report on Progress Against Cancer,” is available in the Journal of Clinical Oncology and on ASCO’s cancer research advocacy website, CancerProgress.net.
The report was developed under the direction of an 18-person editorial board of experts from a wide range of oncology specialties. It features:
- The top cancer research advances of the past year: Identifying major trends in cancer prevention and screening, treatment, quality of life, survivorship, and tumor biology
- A Decade in Review: Recounting improvements in cancer care since the first issue of Clinical Cancer Advances
- The 10-Year Horizon: Previewing trends likely to shape the next decade of cancer care, including genomic technology, nanomedicine, and health information technologies
- Progress in Rare Cancers: Highlighting promising early achievements in treating certain uncommon but devastating cancers.
“This has truly been a banner year for CLL and for clinical cancer research as a whole,” said ASCO President Peter P. Yu, MD. “Advances in cancer prevention and care, especially those in precision medicine, are offering stunning new possibilities for patients.” ![]()
FDA puts drug on fast track to treat secondary AML

The US Food and Drug Administration (FDA) has granted fast track designation for CPX-351, a fixed-ratio combination of cytarabine and daunorubicin inside a lipid vesicle, to treat elderly patients with secondary acute myeloid leukemia (AML).
In a phase 2 study of elderly AML patients, there was no significant difference in response or survival rates between patients who received CPX-351 and those who received cytarabine and daunorubicin.
However, CPX-351 conferred a significant response benefit among patients with poor cytogenetics and a significant survival benefit in patients with secondary AML.
“We are pleased that FDA has granted fast track status for CPX-351 for the treatment of elderly patients with secondary AML,” said Scott Jackson, Chief Executive Officer of Celator Pharmaceuticals, the company developing CPX-351.
“Our ongoing phase 3 study in these patients has completed enrollment, and we expect induction response rate data to be available in the second quarter of this year, and to have overall survival data, the primary endpoint of the study, in the first quarter of 2016.”
“If our phase 3 study comparing CPX-351 to the current standard of care is successful, the fast track designation may provide an added benefit of facilitating the [new drug application] review process.”
The FDA established the fast track designation process to expedite the review of drugs that are intended to treat serious or life-threatening conditions and that demonstrate the potential to address unmet medical needs.
The designation allows a drug’s developer to submit sections of a new drug application (NDA) on a rolling basis, so the FDA can review portions of the NDA as they are received instead of waiting for the entire NDA submission. A fast-track-designated product could be eligible for priority review if supported by clinical data at the time of NDA submission.
Phase 2 trial
In an article published in Blood last April, researchers reported results with CPX-351 in elderly patients with newly diagnosed AML. The study enrolled 126 patients who were 60 to 75 years of age.
They were randomized to receive CPX-351 (n=85) or “control” treatment consisting of cytarabine and daunorubicin (n=41). The treatment groups were well-balanced for disease and patient characteristics at baseline.
Overall, the response rate was 66.7% in the CPX-351 arm and 51.2% in the control arm (P=0.07). Among patients with adverse cytogenetics, the response rates were 77.3% and 38.5%, respectively (P=0.03). And among patients with secondary AML, response rates were 57.6% and 31.6%, respectively (P=0.06).
The median overall survival was 14.7 months in the CPX-351 arm and 12.9 months in the control arm. The median event-free survival was 6.5 months and 2.0 months, respectively. These differences were not statistically significant.
However, secondary AML patients treated with CPX-351 had significantly better overall survival than secondary AML patients in the control arm. The median overall survival was 12.1 months and 6.1 months, respectively (P=0.01). The median event-free survival was 4.5 months and 1.3 months, respectively (P=0.08).
Common adverse events included febrile neutropenia, infection, rash, diarrhea, nausea, edema, and constipation. There were minimal differences between the treatment arms in the incidence of these events.
The median time to neutrophil recovery was longer in the CPX-351 arm than in the control arm—36 days and 32 days, respectively. And the same was true for platelet recovery—37 days and 28 days, respectively.
Patients in the CPX-351 arm had a higher incidence of grade 3-4 infection than controls—70.6% and 43.9%, respectively—but not infection-related deaths—3.5% and 7.3%, respectively.
By day 60, 4.7% of patients in the CPX-351 arm and 14.6% of patients in the control arm had died. All of these deaths occurred in high-risk patients, particularly those with secondary AML. ![]()
The US Food and Drug Administration (FDA) has granted fast track designation for CPX-351, a fixed-ratio combination of cytarabine and daunorubicin inside a lipid vesicle, to treat elderly patients with secondary acute myeloid leukemia (AML).
In a phase 2 study of elderly AML patients, there was no significant difference in response or survival rates between patients who received CPX-351 and those who received cytarabine and daunorubicin.
However, CPX-351 conferred a significant response benefit among patients with poor cytogenetics and a significant survival benefit in patients with secondary AML.
“We are pleased that FDA has granted fast track status for CPX-351 for the treatment of elderly patients with secondary AML,” said Scott Jackson, Chief Executive Officer of Celator Pharmaceuticals, the company developing CPX-351.
“Our ongoing phase 3 study in these patients has completed enrollment, and we expect induction response rate data to be available in the second quarter of this year, and to have overall survival data, the primary endpoint of the study, in the first quarter of 2016.”
“If our phase 3 study comparing CPX-351 to the current standard of care is successful, the fast track designation may provide an added benefit of facilitating the [new drug application] review process.”
The FDA established the fast track designation process to expedite the review of drugs that are intended to treat serious or life-threatening conditions and that demonstrate the potential to address unmet medical needs.
The designation allows a drug’s developer to submit sections of a new drug application (NDA) on a rolling basis, so the FDA can review portions of the NDA as they are received instead of waiting for the entire NDA submission. A fast-track-designated product could be eligible for priority review if supported by clinical data at the time of NDA submission.
Phase 2 trial
In an article published in Blood last April, researchers reported results with CPX-351 in elderly patients with newly diagnosed AML. The study enrolled 126 patients who were 60 to 75 years of age.
They were randomized to receive CPX-351 (n=85) or “control” treatment consisting of cytarabine and daunorubicin (n=41). The treatment groups were well-balanced for disease and patient characteristics at baseline.
Overall, the response rate was 66.7% in the CPX-351 arm and 51.2% in the control arm (P=0.07). Among patients with adverse cytogenetics, the response rates were 77.3% and 38.5%, respectively (P=0.03). And among patients with secondary AML, response rates were 57.6% and 31.6%, respectively (P=0.06).
The median overall survival was 14.7 months in the CPX-351 arm and 12.9 months in the control arm. The median event-free survival was 6.5 months and 2.0 months, respectively. These differences were not statistically significant.
However, secondary AML patients treated with CPX-351 had significantly better overall survival than secondary AML patients in the control arm. The median overall survival was 12.1 months and 6.1 months, respectively (P=0.01). The median event-free survival was 4.5 months and 1.3 months, respectively (P=0.08).
Common adverse events included febrile neutropenia, infection, rash, diarrhea, nausea, edema, and constipation. There were minimal differences between the treatment arms in the incidence of these events.
The median time to neutrophil recovery was longer in the CPX-351 arm than in the control arm—36 days and 32 days, respectively. And the same was true for platelet recovery—37 days and 28 days, respectively.
Patients in the CPX-351 arm had a higher incidence of grade 3-4 infection than controls—70.6% and 43.9%, respectively—but not infection-related deaths—3.5% and 7.3%, respectively.
By day 60, 4.7% of patients in the CPX-351 arm and 14.6% of patients in the control arm had died. All of these deaths occurred in high-risk patients, particularly those with secondary AML. ![]()
The US Food and Drug Administration (FDA) has granted fast track designation for CPX-351, a fixed-ratio combination of cytarabine and daunorubicin inside a lipid vesicle, to treat elderly patients with secondary acute myeloid leukemia (AML).
In a phase 2 study of elderly AML patients, there was no significant difference in response or survival rates between patients who received CPX-351 and those who received cytarabine and daunorubicin.
However, CPX-351 conferred a significant response benefit among patients with poor cytogenetics and a significant survival benefit in patients with secondary AML.
“We are pleased that FDA has granted fast track status for CPX-351 for the treatment of elderly patients with secondary AML,” said Scott Jackson, Chief Executive Officer of Celator Pharmaceuticals, the company developing CPX-351.
“Our ongoing phase 3 study in these patients has completed enrollment, and we expect induction response rate data to be available in the second quarter of this year, and to have overall survival data, the primary endpoint of the study, in the first quarter of 2016.”
“If our phase 3 study comparing CPX-351 to the current standard of care is successful, the fast track designation may provide an added benefit of facilitating the [new drug application] review process.”
The FDA established the fast track designation process to expedite the review of drugs that are intended to treat serious or life-threatening conditions and that demonstrate the potential to address unmet medical needs.
The designation allows a drug’s developer to submit sections of a new drug application (NDA) on a rolling basis, so the FDA can review portions of the NDA as they are received instead of waiting for the entire NDA submission. A fast-track-designated product could be eligible for priority review if supported by clinical data at the time of NDA submission.
Phase 2 trial
In an article published in Blood last April, researchers reported results with CPX-351 in elderly patients with newly diagnosed AML. The study enrolled 126 patients who were 60 to 75 years of age.
They were randomized to receive CPX-351 (n=85) or “control” treatment consisting of cytarabine and daunorubicin (n=41). The treatment groups were well-balanced for disease and patient characteristics at baseline.
Overall, the response rate was 66.7% in the CPX-351 arm and 51.2% in the control arm (P=0.07). Among patients with adverse cytogenetics, the response rates were 77.3% and 38.5%, respectively (P=0.03). And among patients with secondary AML, response rates were 57.6% and 31.6%, respectively (P=0.06).
The median overall survival was 14.7 months in the CPX-351 arm and 12.9 months in the control arm. The median event-free survival was 6.5 months and 2.0 months, respectively. These differences were not statistically significant.
However, secondary AML patients treated with CPX-351 had significantly better overall survival than secondary AML patients in the control arm. The median overall survival was 12.1 months and 6.1 months, respectively (P=0.01). The median event-free survival was 4.5 months and 1.3 months, respectively (P=0.08).
Common adverse events included febrile neutropenia, infection, rash, diarrhea, nausea, edema, and constipation. There were minimal differences between the treatment arms in the incidence of these events.
The median time to neutrophil recovery was longer in the CPX-351 arm than in the control arm—36 days and 32 days, respectively. And the same was true for platelet recovery—37 days and 28 days, respectively.
Patients in the CPX-351 arm had a higher incidence of grade 3-4 infection than controls—70.6% and 43.9%, respectively—but not infection-related deaths—3.5% and 7.3%, respectively.
By day 60, 4.7% of patients in the CPX-351 arm and 14.6% of patients in the control arm had died. All of these deaths occurred in high-risk patients, particularly those with secondary AML. ![]()
Nanoparticle could enable ‘hypermodal’ imaging
Credit: Jonathan Lovell
A new type of nanoparticle can be used with 6 different imaging techniques, according to research published in Advanced Materials.
Investigators found they could detect these nanoparticles via CT and PET scans, as well as photoacoustic, fluorescence, upconversion, and Cerenkov luminescence imaging.
A machine capable of performing all 6 imaging techniques at once has not yet been invented, to the researchers’ knowledge.
But they hope the creation of their nanoparticles and related work will spur the development of such technology.
That way, patients could receive a single injection of the nanoparticles and have several types of imaging done, which would provide a clearer picture of organs and tissues than a single imaging method alone.
For instance, when the investigators used their nanoparticles to examine the lymph nodes of mice, they found that CT and PET scans provided the
deepest tissue penetration, while the photoacoustic imaging showed blood vessel details the first 2 techniques missed.
“This nanoparticle may open the door for new ‘hypermodal’ imaging systems that allow a lot of new information to be obtained using just one contrast agent,” said study author Jonathan Lovell, PhD, of the University of Buffalo in New York.
“Once such systems are developed, a patient could theoretically go in for one scan with one machine instead of multiple scans with multiple machines.”
Dr Lovell and his colleagues designed their nanoparticles to have 2 components: a core that glows blue when struck by near-infrared light and an outer fabric of porphyrin-phospholipids (PoP) that wraps around the core.
Each part has unique characteristics that make it ideal for certain types of imaging.
The core, initially designed for upconversion imaging, is made from sodium, ytterbium, fluorine, yttrium, and thulium. The ytterbium is dense in electrons—a property that facilitates detection by CT scans.
The PoP wrapper has biophotonic qualities that make it a great match for fluorescence and photoacoustic imagining. The PoP layer is also adept at attracting copper, which is used in PET and Cerenkov luminescence imaging.
“Combining these 2 biocompatible components into a single nanoparticle could give tomorrow’s doctors a powerful new tool for medical imaging,” said Paras Prasad, PhD, also of the University of Buffalo.
“More studies would have to be done to determine whether the nanoparticle is safe to use for such purposes, but it does not contain toxic metals, such as cadmium, that are known to pose potential risks and are found in some other nanoparticles.”
“Another advantage of this core/shell imaging contrast agent is that it could enable biomedical imaging at multiple scales, from single-molecule to cell imaging, as well as from vascular and organ imaging to whole-body bioimaging,” added Guanying Chen, PhD, of the University of Buffalo and Harbin Institute of Technology in China.
Dr Lovell said the next step for this research is to explore additional uses for the technology.
For example, it might be possible to attach a targeting molecule to the PoP surface that would enable cancer cells to take up the particles, something that photoacoustic and fluorescence imaging can detect due to the properties of the smart PoP coating. This would enable doctors to better see where tumors begin and end. ![]()
Credit: Jonathan Lovell
A new type of nanoparticle can be used with 6 different imaging techniques, according to research published in Advanced Materials.
Investigators found they could detect these nanoparticles via CT and PET scans, as well as photoacoustic, fluorescence, upconversion, and Cerenkov luminescence imaging.
A machine capable of performing all 6 imaging techniques at once has not yet been invented, to the researchers’ knowledge.
But they hope the creation of their nanoparticles and related work will spur the development of such technology.
That way, patients could receive a single injection of the nanoparticles and have several types of imaging done, which would provide a clearer picture of organs and tissues than a single imaging method alone.
For instance, when the investigators used their nanoparticles to examine the lymph nodes of mice, they found that CT and PET scans provided the
deepest tissue penetration, while the photoacoustic imaging showed blood vessel details the first 2 techniques missed.
“This nanoparticle may open the door for new ‘hypermodal’ imaging systems that allow a lot of new information to be obtained using just one contrast agent,” said study author Jonathan Lovell, PhD, of the University of Buffalo in New York.
“Once such systems are developed, a patient could theoretically go in for one scan with one machine instead of multiple scans with multiple machines.”
Dr Lovell and his colleagues designed their nanoparticles to have 2 components: a core that glows blue when struck by near-infrared light and an outer fabric of porphyrin-phospholipids (PoP) that wraps around the core.
Each part has unique characteristics that make it ideal for certain types of imaging.
The core, initially designed for upconversion imaging, is made from sodium, ytterbium, fluorine, yttrium, and thulium. The ytterbium is dense in electrons—a property that facilitates detection by CT scans.
The PoP wrapper has biophotonic qualities that make it a great match for fluorescence and photoacoustic imagining. The PoP layer is also adept at attracting copper, which is used in PET and Cerenkov luminescence imaging.
“Combining these 2 biocompatible components into a single nanoparticle could give tomorrow’s doctors a powerful new tool for medical imaging,” said Paras Prasad, PhD, also of the University of Buffalo.
“More studies would have to be done to determine whether the nanoparticle is safe to use for such purposes, but it does not contain toxic metals, such as cadmium, that are known to pose potential risks and are found in some other nanoparticles.”
“Another advantage of this core/shell imaging contrast agent is that it could enable biomedical imaging at multiple scales, from single-molecule to cell imaging, as well as from vascular and organ imaging to whole-body bioimaging,” added Guanying Chen, PhD, of the University of Buffalo and Harbin Institute of Technology in China.
Dr Lovell said the next step for this research is to explore additional uses for the technology.
For example, it might be possible to attach a targeting molecule to the PoP surface that would enable cancer cells to take up the particles, something that photoacoustic and fluorescence imaging can detect due to the properties of the smart PoP coating. This would enable doctors to better see where tumors begin and end. ![]()
Credit: Jonathan Lovell
A new type of nanoparticle can be used with 6 different imaging techniques, according to research published in Advanced Materials.
Investigators found they could detect these nanoparticles via CT and PET scans, as well as photoacoustic, fluorescence, upconversion, and Cerenkov luminescence imaging.
A machine capable of performing all 6 imaging techniques at once has not yet been invented, to the researchers’ knowledge.
But they hope the creation of their nanoparticles and related work will spur the development of such technology.
That way, patients could receive a single injection of the nanoparticles and have several types of imaging done, which would provide a clearer picture of organs and tissues than a single imaging method alone.
For instance, when the investigators used their nanoparticles to examine the lymph nodes of mice, they found that CT and PET scans provided the
deepest tissue penetration, while the photoacoustic imaging showed blood vessel details the first 2 techniques missed.
“This nanoparticle may open the door for new ‘hypermodal’ imaging systems that allow a lot of new information to be obtained using just one contrast agent,” said study author Jonathan Lovell, PhD, of the University of Buffalo in New York.
“Once such systems are developed, a patient could theoretically go in for one scan with one machine instead of multiple scans with multiple machines.”
Dr Lovell and his colleagues designed their nanoparticles to have 2 components: a core that glows blue when struck by near-infrared light and an outer fabric of porphyrin-phospholipids (PoP) that wraps around the core.
Each part has unique characteristics that make it ideal for certain types of imaging.
The core, initially designed for upconversion imaging, is made from sodium, ytterbium, fluorine, yttrium, and thulium. The ytterbium is dense in electrons—a property that facilitates detection by CT scans.
The PoP wrapper has biophotonic qualities that make it a great match for fluorescence and photoacoustic imagining. The PoP layer is also adept at attracting copper, which is used in PET and Cerenkov luminescence imaging.
“Combining these 2 biocompatible components into a single nanoparticle could give tomorrow’s doctors a powerful new tool for medical imaging,” said Paras Prasad, PhD, also of the University of Buffalo.
“More studies would have to be done to determine whether the nanoparticle is safe to use for such purposes, but it does not contain toxic metals, such as cadmium, that are known to pose potential risks and are found in some other nanoparticles.”
“Another advantage of this core/shell imaging contrast agent is that it could enable biomedical imaging at multiple scales, from single-molecule to cell imaging, as well as from vascular and organ imaging to whole-body bioimaging,” added Guanying Chen, PhD, of the University of Buffalo and Harbin Institute of Technology in China.
Dr Lovell said the next step for this research is to explore additional uses for the technology.
For example, it might be possible to attach a targeting molecule to the PoP surface that would enable cancer cells to take up the particles, something that photoacoustic and fluorescence imaging can detect due to the properties of the smart PoP coating. This would enable doctors to better see where tumors begin and end.
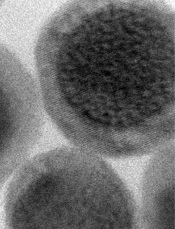
Study reveals genetic changes driving artemisinin resistance

Plasmodium falciparum
Credit: CDC/Mae Melvin
Researchers say they’ve uncovered the complex genetic architecture that enables the malaria parasite Plasmodium falciparum to develop resistance to the antimalarial drug artemisinin.
The team found evidence to suggest that 20 mutations in a single gene work with background mutations in 4 other genes to promote resistance.
The group believes their findings, published in Nature Genetics, could help improve early detection of emerging artemisinin resistance.
To make their discovery, the researchers analyzed 1612 samples from subjects at 15 locations in Southeast Asia and Africa. The team performed P falciparum genome sequencing and genotype calling at more than 600,000 single-nucleotide polymorphism positions on all samples.
The work revealed 20 mutations in the kelch13 gene, a known artemisinin resistance marker, that appear to work in concert with a set of background mutations in 4 other genes—fd, arps10, mdr2, and crt—to support artemisinin resistance.
“Our findings suggest that these background mutations emerged with limited impact on artemisinin resistance—until mutations occurred in the kelch13 gene,” said Roberto Amato, PhD, of the Wellcome Trust Sanger Institute in Oxford, UK.
“It’s similar to what we see with precancerous cells, which accumulate genetic changes but only become malignant when they acquire critical driver mutations that kick off growth.”
The variety of kelch13 mutations associated with artemisinin resistance makes it difficult to use this gene alone as a marker for genetic surveillance.
Monitoring parasite populations for a specific genetic background—in this case, a fixed set of 4 well-defined mutations in fd, arps10, mdr2, and crt—could allow researchers to assess the likelihood of new resistance-causing mutations emerging in different locations, helping to target high-risk regions before resistant parasites take hold.
“We are at a pivotal point for malaria control,” said Nick Day, MBBS, of the Mahidol-Oxford Tropical Medicine Research Unit (MORU) in Bangkok, Thailand.
“While malaria deaths have been halved, this progress is at risk if artemisinin ceases to be effective. We need to use every tool at our disposal to protect this drug. Monitoring parasites for background mutations could provide an early warning system to identify areas at risk for artemisinin resistance.”
The researchers also uncovered new clues about how artemisinin resistance has evolved in Southeast Asia. By comparing parasites from Cambodia, Vietnam, Laos, Thailand, Myanmar, and Bangladesh, the team found that the distribution of different kelch13 mutations is localized within relatively well-defined geographical areas.
Although artemisinin-resistant parasites appear to have migrated across national borders, this only happened on a limited scale. In fact, the most widespread kelch13 mutation, C580Y, seems to have emerged independently on several occasions.
Parasites along the Thailand-Myanmar border appear to have acquired C580Y separately from those in Cambodia and Vietnam. But parasite populations in both regions possess the genetic background mutations, even though they are clearly genetically distinct.
“We don’t yet know the role of these background mutations,” said Olivo Miotto, PhD, also of MORU. “Some may not affect drug resistance directly but, rather, provide an environment where drug-resistance mutations are tolerated.”
“Since kelch13 has hardly changed in 50 million years of Plasmodium evolution, we can assume that this gene is essential to parasite survival. Therefore, kelch13 mutations may severely handicap mutant parasites, compromising their survival unless some other change can counteract this negative effect.”
Mutations in the kelch13 gene were present, yet rare, in Africa. But they weren’t associated with artemisinin resistance and lacked the genetic background present in artemisinin-resistant parasites in Southeast Asia. This provides some reassurance for public health authorities working to prevent the spread of artemisinin resistance to Africa, where most malaria deaths occur.
“These data serve as a reminder of how crucial surveillance and elimination programs are,” said Dominic Kwiatkowski, MBBS, of the Wellcome Trust Sanger Institute.
“At present, artemisinin resistance appears to be largely confined to Southeast Asia, but the situation might change as the parasite population continues to evolve. By linking genomic data with clinical data, we’re developing a better understanding of the multiple genetic factors involved in the emergence of resistance, and that is starting to provide vital clues about how to prevent its spread.”
Plasmodium falciparum
Credit: CDC/Mae Melvin
Researchers say they’ve uncovered the complex genetic architecture that enables the malaria parasite Plasmodium falciparum to develop resistance to the antimalarial drug artemisinin.
The team found evidence to suggest that 20 mutations in a single gene work with background mutations in 4 other genes to promote resistance.
The group believes their findings, published in Nature Genetics, could help improve early detection of emerging artemisinin resistance.
To make their discovery, the researchers analyzed 1612 samples from subjects at 15 locations in Southeast Asia and Africa. The team performed P falciparum genome sequencing and genotype calling at more than 600,000 single-nucleotide polymorphism positions on all samples.
The work revealed 20 mutations in the kelch13 gene, a known artemisinin resistance marker, that appear to work in concert with a set of background mutations in 4 other genes—fd, arps10, mdr2, and crt—to support artemisinin resistance.
“Our findings suggest that these background mutations emerged with limited impact on artemisinin resistance—until mutations occurred in the kelch13 gene,” said Roberto Amato, PhD, of the Wellcome Trust Sanger Institute in Oxford, UK.
“It’s similar to what we see with precancerous cells, which accumulate genetic changes but only become malignant when they acquire critical driver mutations that kick off growth.”
The variety of kelch13 mutations associated with artemisinin resistance makes it difficult to use this gene alone as a marker for genetic surveillance.
Monitoring parasite populations for a specific genetic background—in this case, a fixed set of 4 well-defined mutations in fd, arps10, mdr2, and crt—could allow researchers to assess the likelihood of new resistance-causing mutations emerging in different locations, helping to target high-risk regions before resistant parasites take hold.
“We are at a pivotal point for malaria control,” said Nick Day, MBBS, of the Mahidol-Oxford Tropical Medicine Research Unit (MORU) in Bangkok, Thailand.
“While malaria deaths have been halved, this progress is at risk if artemisinin ceases to be effective. We need to use every tool at our disposal to protect this drug. Monitoring parasites for background mutations could provide an early warning system to identify areas at risk for artemisinin resistance.”
The researchers also uncovered new clues about how artemisinin resistance has evolved in Southeast Asia. By comparing parasites from Cambodia, Vietnam, Laos, Thailand, Myanmar, and Bangladesh, the team found that the distribution of different kelch13 mutations is localized within relatively well-defined geographical areas.
Although artemisinin-resistant parasites appear to have migrated across national borders, this only happened on a limited scale. In fact, the most widespread kelch13 mutation, C580Y, seems to have emerged independently on several occasions.
Parasites along the Thailand-Myanmar border appear to have acquired C580Y separately from those in Cambodia and Vietnam. But parasite populations in both regions possess the genetic background mutations, even though they are clearly genetically distinct.
“We don’t yet know the role of these background mutations,” said Olivo Miotto, PhD, also of MORU. “Some may not affect drug resistance directly but, rather, provide an environment where drug-resistance mutations are tolerated.”
“Since kelch13 has hardly changed in 50 million years of Plasmodium evolution, we can assume that this gene is essential to parasite survival. Therefore, kelch13 mutations may severely handicap mutant parasites, compromising their survival unless some other change can counteract this negative effect.”
Mutations in the kelch13 gene were present, yet rare, in Africa. But they weren’t associated with artemisinin resistance and lacked the genetic background present in artemisinin-resistant parasites in Southeast Asia. This provides some reassurance for public health authorities working to prevent the spread of artemisinin resistance to Africa, where most malaria deaths occur.
“These data serve as a reminder of how crucial surveillance and elimination programs are,” said Dominic Kwiatkowski, MBBS, of the Wellcome Trust Sanger Institute.
“At present, artemisinin resistance appears to be largely confined to Southeast Asia, but the situation might change as the parasite population continues to evolve. By linking genomic data with clinical data, we’re developing a better understanding of the multiple genetic factors involved in the emergence of resistance, and that is starting to provide vital clues about how to prevent its spread.”
Plasmodium falciparum
Credit: CDC/Mae Melvin
Researchers say they’ve uncovered the complex genetic architecture that enables the malaria parasite Plasmodium falciparum to develop resistance to the antimalarial drug artemisinin.
The team found evidence to suggest that 20 mutations in a single gene work with background mutations in 4 other genes to promote resistance.
The group believes their findings, published in Nature Genetics, could help improve early detection of emerging artemisinin resistance.
To make their discovery, the researchers analyzed 1612 samples from subjects at 15 locations in Southeast Asia and Africa. The team performed P falciparum genome sequencing and genotype calling at more than 600,000 single-nucleotide polymorphism positions on all samples.
The work revealed 20 mutations in the kelch13 gene, a known artemisinin resistance marker, that appear to work in concert with a set of background mutations in 4 other genes—fd, arps10, mdr2, and crt—to support artemisinin resistance.
“Our findings suggest that these background mutations emerged with limited impact on artemisinin resistance—until mutations occurred in the kelch13 gene,” said Roberto Amato, PhD, of the Wellcome Trust Sanger Institute in Oxford, UK.
“It’s similar to what we see with precancerous cells, which accumulate genetic changes but only become malignant when they acquire critical driver mutations that kick off growth.”
The variety of kelch13 mutations associated with artemisinin resistance makes it difficult to use this gene alone as a marker for genetic surveillance.
Monitoring parasite populations for a specific genetic background—in this case, a fixed set of 4 well-defined mutations in fd, arps10, mdr2, and crt—could allow researchers to assess the likelihood of new resistance-causing mutations emerging in different locations, helping to target high-risk regions before resistant parasites take hold.
“We are at a pivotal point for malaria control,” said Nick Day, MBBS, of the Mahidol-Oxford Tropical Medicine Research Unit (MORU) in Bangkok, Thailand.
“While malaria deaths have been halved, this progress is at risk if artemisinin ceases to be effective. We need to use every tool at our disposal to protect this drug. Monitoring parasites for background mutations could provide an early warning system to identify areas at risk for artemisinin resistance.”
The researchers also uncovered new clues about how artemisinin resistance has evolved in Southeast Asia. By comparing parasites from Cambodia, Vietnam, Laos, Thailand, Myanmar, and Bangladesh, the team found that the distribution of different kelch13 mutations is localized within relatively well-defined geographical areas.
Although artemisinin-resistant parasites appear to have migrated across national borders, this only happened on a limited scale. In fact, the most widespread kelch13 mutation, C580Y, seems to have emerged independently on several occasions.
Parasites along the Thailand-Myanmar border appear to have acquired C580Y separately from those in Cambodia and Vietnam. But parasite populations in both regions possess the genetic background mutations, even though they are clearly genetically distinct.
“We don’t yet know the role of these background mutations,” said Olivo Miotto, PhD, also of MORU. “Some may not affect drug resistance directly but, rather, provide an environment where drug-resistance mutations are tolerated.”
“Since kelch13 has hardly changed in 50 million years of Plasmodium evolution, we can assume that this gene is essential to parasite survival. Therefore, kelch13 mutations may severely handicap mutant parasites, compromising their survival unless some other change can counteract this negative effect.”
Mutations in the kelch13 gene were present, yet rare, in Africa. But they weren’t associated with artemisinin resistance and lacked the genetic background present in artemisinin-resistant parasites in Southeast Asia. This provides some reassurance for public health authorities working to prevent the spread of artemisinin resistance to Africa, where most malaria deaths occur.
“These data serve as a reminder of how crucial surveillance and elimination programs are,” said Dominic Kwiatkowski, MBBS, of the Wellcome Trust Sanger Institute.
“At present, artemisinin resistance appears to be largely confined to Southeast Asia, but the situation might change as the parasite population continues to evolve. By linking genomic data with clinical data, we’re developing a better understanding of the multiple genetic factors involved in the emergence of resistance, and that is starting to provide vital clues about how to prevent its spread.”
Studies shed new light on HSPC mobilization

in the bone marrow
Two new studies have revealed elements that are key to hematopoietic stem and progenitor cell (HSPC) mobilization.
In one study, investigators discovered that elevated levels of the peptide hormone angiotensin II increases HSPC mobilization in the context of vasculopathy and sickle cell disease (SCD).
In the other study, researchers found that p62, an autophagy regulator and signal organizer, is required to maintain HSPC retention in the bone marrow.
Jose Cancelas, MD, PhD, of the University of Cincinnati College of Medicine in Ohio, is the corresponding author on both studies.
In the first paper, published in Nature Communications, Dr Cancelas and his colleagues noted that patients with vasculopathies have an increase in circulating HSPCs.
“This phenomenon may represent a stress response contributing to vascular damage repair,” he said. “So the question becomes, how can we learn from these patients?”
Using mouse models of vasculopathy and vasculopathy-associated SCD, Dr Cancelas and his colleagues showed that acute and chronic elevated levels of angiotensin II resulted in an increased pool of HSPCs.
And when the researchers administered anti-angiotensin therapy, the pool of HSPCs decreased in mice and humans with SCD.
“These results indicate a new role for angiotensin in hematopoietic stem and progenitor cell trafficking under pathological conditions and define the hematopoietic consequences of anti-angiotensin therapy in vascular disease and sickle cell disease,” Dr Cancelas said.
“Every year, millions of patients receive anti-angiotensin therapies due to the harmful effects associated with chronic hyperangiotensinemia in cardiac, renal, or liver failure. Our study shows that this anti-angiotensin therapy modulates the levels of circulating stem cells and progenitors.”
In the second paper, published in Cell Reports, Dr Cancelas and his colleagues examined the role that p62 plays in HSPC mobilization.
The investigators found that, when p62 is lost in osteoblasts, mice develop a condition similar to osteoporosis in humans.
The osteoblasts cannot degrade inflammatory signals coming from macrophages. And as a consequence, the deficient osteoblasts secrete inflammatory signals that impair the retention of HSPCs in the bone marrow and allow their escape to the circulation.
Specifically, the team found that macrophages activate osteoblastic NF-kB, which results in osteopenia and HSPC egress. And p62 negatively regulates osteoblastic NF-kB activation.
Dr Cancelas noted that patients with inflammatory diseases often have osteopenia. So this research may provide insight into that phenomenon and help explain why patients with chronic inflammatory diseases have higher levels of circulating HSPCs.
in the bone marrow
Two new studies have revealed elements that are key to hematopoietic stem and progenitor cell (HSPC) mobilization.
In one study, investigators discovered that elevated levels of the peptide hormone angiotensin II increases HSPC mobilization in the context of vasculopathy and sickle cell disease (SCD).
In the other study, researchers found that p62, an autophagy regulator and signal organizer, is required to maintain HSPC retention in the bone marrow.
Jose Cancelas, MD, PhD, of the University of Cincinnati College of Medicine in Ohio, is the corresponding author on both studies.
In the first paper, published in Nature Communications, Dr Cancelas and his colleagues noted that patients with vasculopathies have an increase in circulating HSPCs.
“This phenomenon may represent a stress response contributing to vascular damage repair,” he said. “So the question becomes, how can we learn from these patients?”
Using mouse models of vasculopathy and vasculopathy-associated SCD, Dr Cancelas and his colleagues showed that acute and chronic elevated levels of angiotensin II resulted in an increased pool of HSPCs.
And when the researchers administered anti-angiotensin therapy, the pool of HSPCs decreased in mice and humans with SCD.
“These results indicate a new role for angiotensin in hematopoietic stem and progenitor cell trafficking under pathological conditions and define the hematopoietic consequences of anti-angiotensin therapy in vascular disease and sickle cell disease,” Dr Cancelas said.
“Every year, millions of patients receive anti-angiotensin therapies due to the harmful effects associated with chronic hyperangiotensinemia in cardiac, renal, or liver failure. Our study shows that this anti-angiotensin therapy modulates the levels of circulating stem cells and progenitors.”
In the second paper, published in Cell Reports, Dr Cancelas and his colleagues examined the role that p62 plays in HSPC mobilization.
The investigators found that, when p62 is lost in osteoblasts, mice develop a condition similar to osteoporosis in humans.
The osteoblasts cannot degrade inflammatory signals coming from macrophages. And as a consequence, the deficient osteoblasts secrete inflammatory signals that impair the retention of HSPCs in the bone marrow and allow their escape to the circulation.
Specifically, the team found that macrophages activate osteoblastic NF-kB, which results in osteopenia and HSPC egress. And p62 negatively regulates osteoblastic NF-kB activation.
Dr Cancelas noted that patients with inflammatory diseases often have osteopenia. So this research may provide insight into that phenomenon and help explain why patients with chronic inflammatory diseases have higher levels of circulating HSPCs.
in the bone marrow
Two new studies have revealed elements that are key to hematopoietic stem and progenitor cell (HSPC) mobilization.
In one study, investigators discovered that elevated levels of the peptide hormone angiotensin II increases HSPC mobilization in the context of vasculopathy and sickle cell disease (SCD).
In the other study, researchers found that p62, an autophagy regulator and signal organizer, is required to maintain HSPC retention in the bone marrow.
Jose Cancelas, MD, PhD, of the University of Cincinnati College of Medicine in Ohio, is the corresponding author on both studies.
In the first paper, published in Nature Communications, Dr Cancelas and his colleagues noted that patients with vasculopathies have an increase in circulating HSPCs.
“This phenomenon may represent a stress response contributing to vascular damage repair,” he said. “So the question becomes, how can we learn from these patients?”
Using mouse models of vasculopathy and vasculopathy-associated SCD, Dr Cancelas and his colleagues showed that acute and chronic elevated levels of angiotensin II resulted in an increased pool of HSPCs.
And when the researchers administered anti-angiotensin therapy, the pool of HSPCs decreased in mice and humans with SCD.
“These results indicate a new role for angiotensin in hematopoietic stem and progenitor cell trafficking under pathological conditions and define the hematopoietic consequences of anti-angiotensin therapy in vascular disease and sickle cell disease,” Dr Cancelas said.
“Every year, millions of patients receive anti-angiotensin therapies due to the harmful effects associated with chronic hyperangiotensinemia in cardiac, renal, or liver failure. Our study shows that this anti-angiotensin therapy modulates the levels of circulating stem cells and progenitors.”
In the second paper, published in Cell Reports, Dr Cancelas and his colleagues examined the role that p62 plays in HSPC mobilization.
The investigators found that, when p62 is lost in osteoblasts, mice develop a condition similar to osteoporosis in humans.
The osteoblasts cannot degrade inflammatory signals coming from macrophages. And as a consequence, the deficient osteoblasts secrete inflammatory signals that impair the retention of HSPCs in the bone marrow and allow their escape to the circulation.
Specifically, the team found that macrophages activate osteoblastic NF-kB, which results in osteopenia and HSPC egress. And p62 negatively regulates osteoblastic NF-kB activation.
Dr Cancelas noted that patients with inflammatory diseases often have osteopenia. So this research may provide insight into that phenomenon and help explain why patients with chronic inflammatory diseases have higher levels of circulating HSPCs.
EC supports continued use of ponatinib

Credit: Rhoda Baer
The European Commission (EC) has concluded that ponatinib (Iclusig) should continue to be prescribed in accordance with its already approved indications.
After trial results suggested the drug poses an increased risk of thrombotic events, the European Medicines Agency’s (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) conducted a review of available ponatinib data.
Results of that review suggested the benefits of ponatinib outweigh the risks. So the committee said the drug should be prescribed as indicated.
The EMA’s Committee for Medicinal Products for Human Use (CHMP) recently endorsed this recommendation, and, now, the EC has followed suit. The EC’s decision is legally binding.
Ponatinib is approved in the European Union to treat adults with chronic phase, accelerated phase, or blast phase chronic myeloid leukemia who are resistant to dasatinib or nilotinib, who are intolerant to dasatinib or nilotinib and for whom subsequent treatment with imatinib is not clinically appropriate, or who have the T315I mutation.
The drug is also approved to treat adults with Philadelphia-chromosome positive acute lymphoblastic leukemia who are resistant to dasatinib, who cannot tolerate dasatinib and subsequent treatment with imatinib is not clinically appropriate, or who have the T315I mutation.
In October 2013, extended follow-up data from the PACE trial revealed that ponatinib-treated patients had a higher incidence of arterial and venous thrombotic events than was observed when the drug first gained approval. So one ponatinib trial was discontinued, and the rest were placed on partial clinical hold.
Soon after, ponatinib was pulled from the US market. The drug ultimately returned to the marketplace with new recommendations designed to decrease the risk of thrombotic events.
The EMA also revised its recommendations for ponatinib—discouraging use of the drug in certain patients, providing advice for managing comorbidities, and suggesting patient monitoring—but kept the drug on the market.
In October 2014, the PRAC concluded its 11-month review of ponatinib data, confirming that the benefit-risk profile of the drug was favorable in its approved indications and recommending that the indications remain unchanged.
However, the PRAC also said the risk of vascular occlusive events with ponatinib is likely dose-related. So the committee recommended that healthcare professionals monitor ponatinib-treated patients and consider dose reductions or discontinuing the drug in certain patients.
The CHMP endorsed these recommendations, and, now, the EC has as well. This is a legally binding decision for ponatinib to continue to be prescribed in Europe in accordance with its already approved indications.
Ponatinib is being developed by ARIAD Pharmaceuticals, Inc.
Credit: Rhoda Baer
The European Commission (EC) has concluded that ponatinib (Iclusig) should continue to be prescribed in accordance with its already approved indications.
After trial results suggested the drug poses an increased risk of thrombotic events, the European Medicines Agency’s (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) conducted a review of available ponatinib data.
Results of that review suggested the benefits of ponatinib outweigh the risks. So the committee said the drug should be prescribed as indicated.
The EMA’s Committee for Medicinal Products for Human Use (CHMP) recently endorsed this recommendation, and, now, the EC has followed suit. The EC’s decision is legally binding.
Ponatinib is approved in the European Union to treat adults with chronic phase, accelerated phase, or blast phase chronic myeloid leukemia who are resistant to dasatinib or nilotinib, who are intolerant to dasatinib or nilotinib and for whom subsequent treatment with imatinib is not clinically appropriate, or who have the T315I mutation.
The drug is also approved to treat adults with Philadelphia-chromosome positive acute lymphoblastic leukemia who are resistant to dasatinib, who cannot tolerate dasatinib and subsequent treatment with imatinib is not clinically appropriate, or who have the T315I mutation.
In October 2013, extended follow-up data from the PACE trial revealed that ponatinib-treated patients had a higher incidence of arterial and venous thrombotic events than was observed when the drug first gained approval. So one ponatinib trial was discontinued, and the rest were placed on partial clinical hold.
Soon after, ponatinib was pulled from the US market. The drug ultimately returned to the marketplace with new recommendations designed to decrease the risk of thrombotic events.
The EMA also revised its recommendations for ponatinib—discouraging use of the drug in certain patients, providing advice for managing comorbidities, and suggesting patient monitoring—but kept the drug on the market.
In October 2014, the PRAC concluded its 11-month review of ponatinib data, confirming that the benefit-risk profile of the drug was favorable in its approved indications and recommending that the indications remain unchanged.
However, the PRAC also said the risk of vascular occlusive events with ponatinib is likely dose-related. So the committee recommended that healthcare professionals monitor ponatinib-treated patients and consider dose reductions or discontinuing the drug in certain patients.
The CHMP endorsed these recommendations, and, now, the EC has as well. This is a legally binding decision for ponatinib to continue to be prescribed in Europe in accordance with its already approved indications.
Ponatinib is being developed by ARIAD Pharmaceuticals, Inc.
Credit: Rhoda Baer
The European Commission (EC) has concluded that ponatinib (Iclusig) should continue to be prescribed in accordance with its already approved indications.
After trial results suggested the drug poses an increased risk of thrombotic events, the European Medicines Agency’s (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) conducted a review of available ponatinib data.
Results of that review suggested the benefits of ponatinib outweigh the risks. So the committee said the drug should be prescribed as indicated.
The EMA’s Committee for Medicinal Products for Human Use (CHMP) recently endorsed this recommendation, and, now, the EC has followed suit. The EC’s decision is legally binding.
Ponatinib is approved in the European Union to treat adults with chronic phase, accelerated phase, or blast phase chronic myeloid leukemia who are resistant to dasatinib or nilotinib, who are intolerant to dasatinib or nilotinib and for whom subsequent treatment with imatinib is not clinically appropriate, or who have the T315I mutation.
The drug is also approved to treat adults with Philadelphia-chromosome positive acute lymphoblastic leukemia who are resistant to dasatinib, who cannot tolerate dasatinib and subsequent treatment with imatinib is not clinically appropriate, or who have the T315I mutation.
In October 2013, extended follow-up data from the PACE trial revealed that ponatinib-treated patients had a higher incidence of arterial and venous thrombotic events than was observed when the drug first gained approval. So one ponatinib trial was discontinued, and the rest were placed on partial clinical hold.
Soon after, ponatinib was pulled from the US market. The drug ultimately returned to the marketplace with new recommendations designed to decrease the risk of thrombotic events.
The EMA also revised its recommendations for ponatinib—discouraging use of the drug in certain patients, providing advice for managing comorbidities, and suggesting patient monitoring—but kept the drug on the market.
In October 2014, the PRAC concluded its 11-month review of ponatinib data, confirming that the benefit-risk profile of the drug was favorable in its approved indications and recommending that the indications remain unchanged.
However, the PRAC also said the risk of vascular occlusive events with ponatinib is likely dose-related. So the committee recommended that healthcare professionals monitor ponatinib-treated patients and consider dose reductions or discontinuing the drug in certain patients.
The CHMP endorsed these recommendations, and, now, the EC has as well. This is a legally binding decision for ponatinib to continue to be prescribed in Europe in accordance with its already approved indications.
Ponatinib is being developed by ARIAD Pharmaceuticals, Inc.