User login
Answer
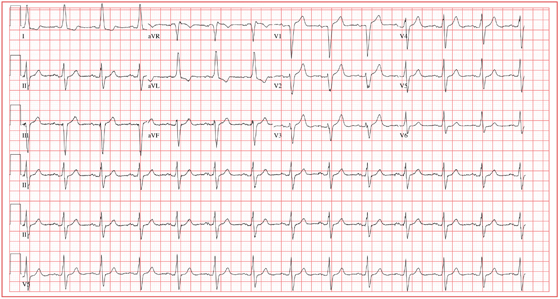
This ECG demonstrates normal sinus rhythm with left-axis deviation and left ventricular hypertrophy with QRS widening and repolarization abnormality, with no evidence of ischemia. Left-axis deviation is defined by an R-wave axis of less than –30° and is determined by examining leads III, aVF, and II. If leads III, aVF, and II are all negative, left-axis deviation is present. In this example, leads III and aVF are negative, while lead II is isoelectric or slightly negative.
Left ventricular hypertrophy is defined by high voltages in the limb leads (R wave in lead I plus S wave in lead III ≥ 25 mm) or in the precordial leads (S wave in V1 plus R wave in V5 or V6 ≥ 35 mm). The QRS duration, measured from the first deflection of the QRS from baseline to its return to baseline, is normal if ≤ 100 ms (0.10 sec). In this example, the QRS is widened (130 ms) in the absence of a bundle branch block. The delayed depolarization of both ventricles in the presence of left ventricular hypertrophy results in delayed repolarization—hence the repolarization abnormality.
This patient underwent cardiac catheterization, which revealed extensive three-vessel coronary artery disease with 99% stenosis of the proximal left anterior descending coronary artery. This case illustrates that severe coronary artery disease can present without ECG evidence of ischemia, particularly in women and in patients with diabetes.
Answer
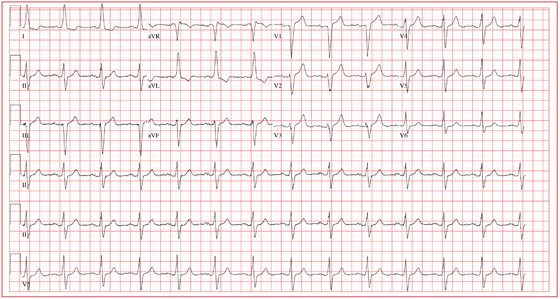
This ECG demonstrates normal sinus rhythm with left-axis deviation and left ventricular hypertrophy with QRS widening and repolarization abnormality, with no evidence of ischemia. Left-axis deviation is defined by an R-wave axis of less than –30° and is determined by examining leads III, aVF, and II. If leads III, aVF, and II are all negative, left-axis deviation is present. In this example, leads III and aVF are negative, while lead II is isoelectric or slightly negative.
Left ventricular hypertrophy is defined by high voltages in the limb leads (R wave in lead I plus S wave in lead III ≥ 25 mm) or in the precordial leads (S wave in V1 plus R wave in V5 or V6 ≥ 35 mm). The QRS duration, measured from the first deflection of the QRS from baseline to its return to baseline, is normal if ≤ 100 ms (0.10 sec). In this example, the QRS is widened (130 ms) in the absence of a bundle branch block. The delayed depolarization of both ventricles in the presence of left ventricular hypertrophy results in delayed repolarization—hence the repolarization abnormality.
This patient underwent cardiac catheterization, which revealed extensive three-vessel coronary artery disease with 99% stenosis of the proximal left anterior descending coronary artery. This case illustrates that severe coronary artery disease can present without ECG evidence of ischemia, particularly in women and in patients with diabetes.
Answer
This ECG demonstrates normal sinus rhythm with left-axis deviation and left ventricular hypertrophy with QRS widening and repolarization abnormality, with no evidence of ischemia. Left-axis deviation is defined by an R-wave axis of less than –30° and is determined by examining leads III, aVF, and II. If leads III, aVF, and II are all negative, left-axis deviation is present. In this example, leads III and aVF are negative, while lead II is isoelectric or slightly negative.
Left ventricular hypertrophy is defined by high voltages in the limb leads (R wave in lead I plus S wave in lead III ≥ 25 mm) or in the precordial leads (S wave in V1 plus R wave in V5 or V6 ≥ 35 mm). The QRS duration, measured from the first deflection of the QRS from baseline to its return to baseline, is normal if ≤ 100 ms (0.10 sec). In this example, the QRS is widened (130 ms) in the absence of a bundle branch block. The delayed depolarization of both ventricles in the presence of left ventricular hypertrophy results in delayed repolarization—hence the repolarization abnormality.
This patient underwent cardiac catheterization, which revealed extensive three-vessel coronary artery disease with 99% stenosis of the proximal left anterior descending coronary artery. This case illustrates that severe coronary artery disease can present without ECG evidence of ischemia, particularly in women and in patients with diabetes.
For two weeks, a Spanish-speaking woman, 60, has experienced substernal chest pain and shortness of breath. The pain began while she was visiting family in Mexico. She was seen by a local physician, who prescribed a medication that helped but did not relieve the pain completely. She exhausted her supply of this medication shortly after returning from vacation, and her chest pain worsened. The patient’s daughter transported her to your clinic, concerned that her mother may be having a heart attack. According to the daughter, who is interpreting, the pain is described as grade IV/X, intermittent, radiating to the back, and lasting for approximately 10 minutes before subsiding. It is exacerbated with activity, particularly climbing stairs, and resolves when the woman is at rest. She has been awakened by this pain on two occasions. The patient denies fever, chills, nausea, vomiting, dizziness, or syncope. Medical history is remarkable for hypertension, diabetes, and asthma. She has worked most of her life as a farm worker and as a cook. She does not use alcohol and has a 20–pack-year history of tobacco use. The patient’s medications include aspirin, metformin, pravastatin, telmisartan, verapamil, and a salmeterol inhaler. She is allergic to penicillin. Review of symptoms is remarkable for diarrhea that is resolving and headaches. Physical examination reveals a well-developed, obese woman who is comfortable, alert, and oriented. Her height is 5’3”; weight, 211 lb; blood pressure, 106/40 mm Hg; pulse, 80 beats/min; respiratory rate, 14 breaths/min; and temperature, 99.2°F. The cardiovascular exam reveals a normal rate and rhythm with no murmurs, rubs, or extra heart sounds. There are no carotid bruits or peripheral edema. The lungs are remarkable for scattered expiratory wheezes in both bases, with the right greater than the left. The abdomen is large but soft with good bowel tones in all quadrants. There are no palpable bruits or organomegaly. The neurologic exam shows no gross neural deficits. The serum glucose level is 148 mg/dL; hemoglobin, 10.6 g/dL; and troponin, 0.02 ng/mL. All other lab values are within normal limits. An ECG shows the following: a ventricular rate of 80 beats/min; PR interval, 168 ms; QRS duration, 130 ms; QT/QTc, 384/442 ms; P axis, 29°; R axis, –34°; and T axis, 96°. What is your interpretation of this ECG, and is there any evidence of ongoing ischemia?