User login
ANSWER
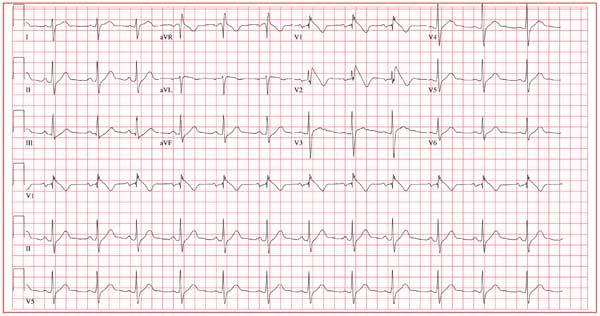
The ECG shows normal sinus rhythm, with a right-axis deviation (R wave axis > 90°) and a significant ST elevation noted in the anterior precordial leads consistent with a type 1 Brugada pattern. In this ECG, the elevated ST segment (≥ 2 mm) descends into an inverted T wave in leads V1 and V2.
The Brugada syndrome is due to a mutation in SCN5A, the alpha subunit of the cardiac sodium channel gene. Any clinical expression of the Brugada syndrome is related to ventricular arrhythmias, which are life-threatening.
Given his family history and his ECG, the patient is correct to be concerned. Genetic testing should be performed, and he should be referred for evaluation, including placement of an implantable defibrillator system for primary prevention of sudden cardiac death.
ANSWER
The ECG shows normal sinus rhythm, with a right-axis deviation (R wave axis > 90°) and a significant ST elevation noted in the anterior precordial leads consistent with a type 1 Brugada pattern. In this ECG, the elevated ST segment (≥ 2 mm) descends into an inverted T wave in leads V1 and V2.
The Brugada syndrome is due to a mutation in SCN5A, the alpha subunit of the cardiac sodium channel gene. Any clinical expression of the Brugada syndrome is related to ventricular arrhythmias, which are life-threatening.
Given his family history and his ECG, the patient is correct to be concerned. Genetic testing should be performed, and he should be referred for evaluation, including placement of an implantable defibrillator system for primary prevention of sudden cardiac death.
ANSWER
The ECG shows normal sinus rhythm, with a right-axis deviation (R wave axis > 90°) and a significant ST elevation noted in the anterior precordial leads consistent with a type 1 Brugada pattern. In this ECG, the elevated ST segment (≥ 2 mm) descends into an inverted T wave in leads V1 and V2.
The Brugada syndrome is due to a mutation in SCN5A, the alpha subunit of the cardiac sodium channel gene. Any clinical expression of the Brugada syndrome is related to ventricular arrhythmias, which are life-threatening.
Given his family history and his ECG, the patient is correct to be concerned. Genetic testing should be performed, and he should be referred for evaluation, including placement of an implantable defibrillator system for primary prevention of sudden cardiac death.
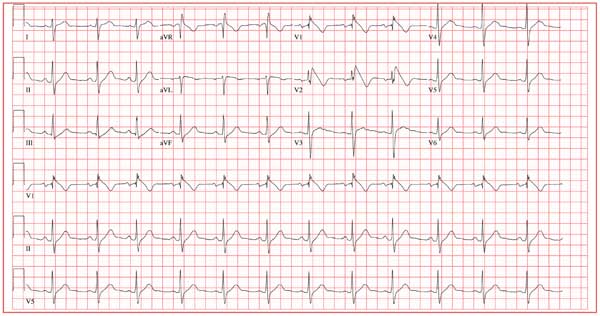
A 25-year-old Vietnamese man has lived in the United States since age 14. He was in his usual state of “excellent” health until one week ago, when he had an episode of syncope while walking along the shore of a lake with a friend. His friend told him that he lost consciousness without warning, fell to the ground, and promptly regained consciousness. He did not lose bowel or bladder control and did not injure himself. He attributed this episode to an insufficient intake of water on a hot, humid afternoon. Two days later, while talking to his father about the episode, he learned that he had a paternal uncle who died suddenly in his late 20s and a maternal aunt who died in her early 30s after similar episodes of syncope. Frightened that he may meet the same end, he presents to your clinic. He has no history of chest pain, palpitations, or dyspnea. Medical history is remarkable for an episode of pneumonia as a child. He has no known drug allergies and is currently taking no medications. He has smoked one pack of cigarettes per day since age 14, and he uses marijuana approximately twice a month. He drinks a six-pack of beer on weekends. He is married with no children and works in the IT department at a local community college. A detailed review of systems reveals no pertinent positive findings. He has had no loss of energy, trouble sleeping, or weight change (loss or gain). Physical examination reveals a blood pressure of 110/72 mm Hg; pulse, 70 beats/min and regular; and respiratory rate, 14 min-1. He is afebrile. His height is 68”, and his weight, 151 lb. He is well nourished and in no acute distress. The HEENT, neck, chest, cardiovascular, abdominal, musculoskeletal, and neurologic exams are all normal. Blood chemistries, complete blood count, lipid profile, liver profile, and thyroid function studies are all normal. You assure the patient that he is in excellent health. He remains concerned, however, and asks that you order an ECG—a request to which you reluctantly agree. The ECG reveals the following: a ventricular rate of 75 beats/min; PR interval, 168 ms; QRS duration, 88 ms; QT/QTc interval, 390/435 ms; P axis, 73°; R axis, 112°; and T axis, 63°. What is your interpretation—and does the patient have a legitimate concern regarding his risk for dying suddenly?