User login
More than half of patients with noninfectious acute anterior uveitis seen in ophthalmology clinics in a new cross-sectional study were found by rheumatologists to have spondyloarthritis (SpA), prompting the researchers to recommend referring “all patients with AAU reporting musculoskeletal symptoms to rheumatologists.”
The results also suggest that “rheumatologists should consider that SpA in AAU patients might present ‘atypically’ with no or mild back pain starting after the age of 45 years and lasting shorter than 3 months,” according to first author Judith Rademacher, MD, and colleagues at Charité–Universitätsmedizin Berlin, who published their work online in Arthritis & Rheumatology.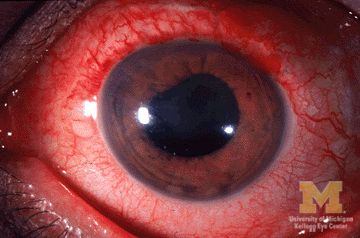
During July 2017–April 2021, the study team prospectively assessed 189 consecutive adult patients with noninfectious AAU at ophthalmology clinics in the Berlin area. The patients had rheumatologic examinations and underwent pelvic x-ray if they had back pain as well as MRI of sacroiliac joints regardless of back pain unless there was a contraindication. The patients had a mean age of nearly 41 years, and 54.5% were male.
Of the 189 patients with AAU, the researchers diagnosed SpA in 106, including 74 (70%) who had been previously undiagnosed. A total of 99 (93%) had predominately axial SpA, and 7 (7%) had peripheral SpA.
A multivariable logistic regression assessment found that male sex (odds ratio, 2.1; 95% confidence interval, 1.1-4.2), HLA-B27 positivity (OR, 6.3; 95% CI, 2.4-16.4), elevated C-reactive protein (OR, 4.8; 95% CI, 1.9-12.4), and psoriasis (OR, 12.5; 95% CI, 1.3-120.2) were significantly associated with SpA in patients with AAU. No ophthalmologic factors were significantly associated with SpA.
Among all patients, an adaptation of the Assessment of SpondyloArthritis International Society (ASAS) referral tool demonstrated lower specificity for SpA recognition than did the Dublin Uveitis Evaluation Tool (28% vs. 42%). The ASAS referral took had a slightly greater sensitivity than the Dublin Uveitis Evaluation Tool (80% vs. 78%).
“Taking into account only AAU patients without prior diagnosis of SpA, a rheumatologist would have to see 2.1 patients fulfilling the ASAS tool or 1.9 patients fulfilling the DUET to diagnose one patient with SpA. However, with both referral strategies more than 20% of SpA patients would have been missed,” the researchers wrote. “This might be due to an ‘unusual presentation’ of SpA in those patients as their back pain started more often after the age of 45 years, lasted shorter than 3 months and thus, ASAS classification criteria were less frequently fulfilled.”
The researchers acknowledged possible selection bias because 15 patients with an incomplete rheumatologic evaluation were excluded. MRI also was routinely done for sacroiliac joints alone, although it was possible for clinician to order spinal MRI. In addition, the researchers allowed patients with AAU into the study regardless of their current treatment, meaning that it may have been possible for some patients receiving biologic disease-modifying antirheumatic drugs to not be correctly identified as having SpA if the treatment improved their musculoskeletal symptoms.
Expert commentary
There are a number of diseases associated with SpA, including AAU, noted Kristine Kuhn, MD, PhD, an associate professor of medicine at the University of Colorado at Denver, Aurora, who was not involved in the study.
“As a rheumatologist, we are quite aware of [uveitis] as an association, and we are usually asking our patients about eye symptoms because of this association,” Dr. Kuhn said in an interview.
While just over half of the patients with AAU also met the criteria for SpA, “that doesn’t necessarily mean diagnosis per se because classification criteria are based on a series of features to homogenize a group of people for clinical research studies. So it doesn’t always align 100% with diagnosis, but it does give us an indication that a little of over half of people with anterior uveitis will have underlying spondyloarthritis and should be evaluated by a rheumatologist.”
Dr. Kuhn also highlighted the associations of male sex, HLA-B27 positivity, and concomitant presence of psoriasis. “I bring those up because I find those to be interesting associations. We have known those for years to be associated with axial spondyloarthritis, but when you look at the actual data, I would just put a little bit of caution to those conclusions.”
She pointed out that, although the link of male sex to SpA in patients with AAU was statistically significant, it is not a clinically meaningful association.
Dr. Kuhn also noted that caution should be used when interpreting the HLA-B27 positivity data. “The caution that I put there is that this was conducted in Germany, and we know that Northern European populations tend to be more enriched for HLA-B27 genes, so what that association would be in a more diverse population is unknown.
“I think ophthalmologists are really good when they see a patient with [acute]-onset anterior uveitis; they have a suspicion that there’s probably another systemic disease that they should be looking at. What this tells us as a physician community is that maybe we should lower the threshold for getting patients into rheumatology and looking at whether or not the patient has underlying spondyloarthritis,” she said.
AbbVie supported the study with an unrestricted research grant but had no role in the study design or in the collection, analysis, or interpretation of the data, the writing of the manuscript, or the decision to submit the manuscript for publication. Of the study’s 12 authors, 2 reported having no financial disclosures. All others reported financial relationships with pharmaceutical companies, including AbbVie.
More than half of patients with noninfectious acute anterior uveitis seen in ophthalmology clinics in a new cross-sectional study were found by rheumatologists to have spondyloarthritis (SpA), prompting the researchers to recommend referring “all patients with AAU reporting musculoskeletal symptoms to rheumatologists.”
The results also suggest that “rheumatologists should consider that SpA in AAU patients might present ‘atypically’ with no or mild back pain starting after the age of 45 years and lasting shorter than 3 months,” according to first author Judith Rademacher, MD, and colleagues at Charité–Universitätsmedizin Berlin, who published their work online in Arthritis & Rheumatology.
During July 2017–April 2021, the study team prospectively assessed 189 consecutive adult patients with noninfectious AAU at ophthalmology clinics in the Berlin area. The patients had rheumatologic examinations and underwent pelvic x-ray if they had back pain as well as MRI of sacroiliac joints regardless of back pain unless there was a contraindication. The patients had a mean age of nearly 41 years, and 54.5% were male.
Of the 189 patients with AAU, the researchers diagnosed SpA in 106, including 74 (70%) who had been previously undiagnosed. A total of 99 (93%) had predominately axial SpA, and 7 (7%) had peripheral SpA.
A multivariable logistic regression assessment found that male sex (odds ratio, 2.1; 95% confidence interval, 1.1-4.2), HLA-B27 positivity (OR, 6.3; 95% CI, 2.4-16.4), elevated C-reactive protein (OR, 4.8; 95% CI, 1.9-12.4), and psoriasis (OR, 12.5; 95% CI, 1.3-120.2) were significantly associated with SpA in patients with AAU. No ophthalmologic factors were significantly associated with SpA.
Among all patients, an adaptation of the Assessment of SpondyloArthritis International Society (ASAS) referral tool demonstrated lower specificity for SpA recognition than did the Dublin Uveitis Evaluation Tool (28% vs. 42%). The ASAS referral took had a slightly greater sensitivity than the Dublin Uveitis Evaluation Tool (80% vs. 78%).
“Taking into account only AAU patients without prior diagnosis of SpA, a rheumatologist would have to see 2.1 patients fulfilling the ASAS tool or 1.9 patients fulfilling the DUET to diagnose one patient with SpA. However, with both referral strategies more than 20% of SpA patients would have been missed,” the researchers wrote. “This might be due to an ‘unusual presentation’ of SpA in those patients as their back pain started more often after the age of 45 years, lasted shorter than 3 months and thus, ASAS classification criteria were less frequently fulfilled.”
The researchers acknowledged possible selection bias because 15 patients with an incomplete rheumatologic evaluation were excluded. MRI also was routinely done for sacroiliac joints alone, although it was possible for clinician to order spinal MRI. In addition, the researchers allowed patients with AAU into the study regardless of their current treatment, meaning that it may have been possible for some patients receiving biologic disease-modifying antirheumatic drugs to not be correctly identified as having SpA if the treatment improved their musculoskeletal symptoms.
Expert commentary
There are a number of diseases associated with SpA, including AAU, noted Kristine Kuhn, MD, PhD, an associate professor of medicine at the University of Colorado at Denver, Aurora, who was not involved in the study.
“As a rheumatologist, we are quite aware of [uveitis] as an association, and we are usually asking our patients about eye symptoms because of this association,” Dr. Kuhn said in an interview.
While just over half of the patients with AAU also met the criteria for SpA, “that doesn’t necessarily mean diagnosis per se because classification criteria are based on a series of features to homogenize a group of people for clinical research studies. So it doesn’t always align 100% with diagnosis, but it does give us an indication that a little of over half of people with anterior uveitis will have underlying spondyloarthritis and should be evaluated by a rheumatologist.”
Dr. Kuhn also highlighted the associations of male sex, HLA-B27 positivity, and concomitant presence of psoriasis. “I bring those up because I find those to be interesting associations. We have known those for years to be associated with axial spondyloarthritis, but when you look at the actual data, I would just put a little bit of caution to those conclusions.”
She pointed out that, although the link of male sex to SpA in patients with AAU was statistically significant, it is not a clinically meaningful association.
Dr. Kuhn also noted that caution should be used when interpreting the HLA-B27 positivity data. “The caution that I put there is that this was conducted in Germany, and we know that Northern European populations tend to be more enriched for HLA-B27 genes, so what that association would be in a more diverse population is unknown.
“I think ophthalmologists are really good when they see a patient with [acute]-onset anterior uveitis; they have a suspicion that there’s probably another systemic disease that they should be looking at. What this tells us as a physician community is that maybe we should lower the threshold for getting patients into rheumatology and looking at whether or not the patient has underlying spondyloarthritis,” she said.
AbbVie supported the study with an unrestricted research grant but had no role in the study design or in the collection, analysis, or interpretation of the data, the writing of the manuscript, or the decision to submit the manuscript for publication. Of the study’s 12 authors, 2 reported having no financial disclosures. All others reported financial relationships with pharmaceutical companies, including AbbVie.
More than half of patients with noninfectious acute anterior uveitis seen in ophthalmology clinics in a new cross-sectional study were found by rheumatologists to have spondyloarthritis (SpA), prompting the researchers to recommend referring “all patients with AAU reporting musculoskeletal symptoms to rheumatologists.”
The results also suggest that “rheumatologists should consider that SpA in AAU patients might present ‘atypically’ with no or mild back pain starting after the age of 45 years and lasting shorter than 3 months,” according to first author Judith Rademacher, MD, and colleagues at Charité–Universitätsmedizin Berlin, who published their work online in Arthritis & Rheumatology.
During July 2017–April 2021, the study team prospectively assessed 189 consecutive adult patients with noninfectious AAU at ophthalmology clinics in the Berlin area. The patients had rheumatologic examinations and underwent pelvic x-ray if they had back pain as well as MRI of sacroiliac joints regardless of back pain unless there was a contraindication. The patients had a mean age of nearly 41 years, and 54.5% were male.
Of the 189 patients with AAU, the researchers diagnosed SpA in 106, including 74 (70%) who had been previously undiagnosed. A total of 99 (93%) had predominately axial SpA, and 7 (7%) had peripheral SpA.
A multivariable logistic regression assessment found that male sex (odds ratio, 2.1; 95% confidence interval, 1.1-4.2), HLA-B27 positivity (OR, 6.3; 95% CI, 2.4-16.4), elevated C-reactive protein (OR, 4.8; 95% CI, 1.9-12.4), and psoriasis (OR, 12.5; 95% CI, 1.3-120.2) were significantly associated with SpA in patients with AAU. No ophthalmologic factors were significantly associated with SpA.
Among all patients, an adaptation of the Assessment of SpondyloArthritis International Society (ASAS) referral tool demonstrated lower specificity for SpA recognition than did the Dublin Uveitis Evaluation Tool (28% vs. 42%). The ASAS referral took had a slightly greater sensitivity than the Dublin Uveitis Evaluation Tool (80% vs. 78%).
“Taking into account only AAU patients without prior diagnosis of SpA, a rheumatologist would have to see 2.1 patients fulfilling the ASAS tool or 1.9 patients fulfilling the DUET to diagnose one patient with SpA. However, with both referral strategies more than 20% of SpA patients would have been missed,” the researchers wrote. “This might be due to an ‘unusual presentation’ of SpA in those patients as their back pain started more often after the age of 45 years, lasted shorter than 3 months and thus, ASAS classification criteria were less frequently fulfilled.”
The researchers acknowledged possible selection bias because 15 patients with an incomplete rheumatologic evaluation were excluded. MRI also was routinely done for sacroiliac joints alone, although it was possible for clinician to order spinal MRI. In addition, the researchers allowed patients with AAU into the study regardless of their current treatment, meaning that it may have been possible for some patients receiving biologic disease-modifying antirheumatic drugs to not be correctly identified as having SpA if the treatment improved their musculoskeletal symptoms.
Expert commentary
There are a number of diseases associated with SpA, including AAU, noted Kristine Kuhn, MD, PhD, an associate professor of medicine at the University of Colorado at Denver, Aurora, who was not involved in the study.
“As a rheumatologist, we are quite aware of [uveitis] as an association, and we are usually asking our patients about eye symptoms because of this association,” Dr. Kuhn said in an interview.
While just over half of the patients with AAU also met the criteria for SpA, “that doesn’t necessarily mean diagnosis per se because classification criteria are based on a series of features to homogenize a group of people for clinical research studies. So it doesn’t always align 100% with diagnosis, but it does give us an indication that a little of over half of people with anterior uveitis will have underlying spondyloarthritis and should be evaluated by a rheumatologist.”
Dr. Kuhn also highlighted the associations of male sex, HLA-B27 positivity, and concomitant presence of psoriasis. “I bring those up because I find those to be interesting associations. We have known those for years to be associated with axial spondyloarthritis, but when you look at the actual data, I would just put a little bit of caution to those conclusions.”
She pointed out that, although the link of male sex to SpA in patients with AAU was statistically significant, it is not a clinically meaningful association.
Dr. Kuhn also noted that caution should be used when interpreting the HLA-B27 positivity data. “The caution that I put there is that this was conducted in Germany, and we know that Northern European populations tend to be more enriched for HLA-B27 genes, so what that association would be in a more diverse population is unknown.
“I think ophthalmologists are really good when they see a patient with [acute]-onset anterior uveitis; they have a suspicion that there’s probably another systemic disease that they should be looking at. What this tells us as a physician community is that maybe we should lower the threshold for getting patients into rheumatology and looking at whether or not the patient has underlying spondyloarthritis,” she said.
AbbVie supported the study with an unrestricted research grant but had no role in the study design or in the collection, analysis, or interpretation of the data, the writing of the manuscript, or the decision to submit the manuscript for publication. Of the study’s 12 authors, 2 reported having no financial disclosures. All others reported financial relationships with pharmaceutical companies, including AbbVie.
FROM ARTHRITIS & RHEUMATOLOGY