User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
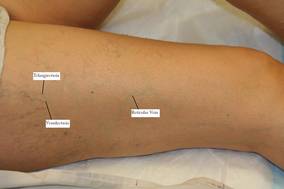
SDEF: Leg Vein Treatment Requires Algorithmic Approach
Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.

"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.
Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.
"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.
Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.
"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Critical Care Phase in HLHS Extends Through Transfer From ICU to Floor
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
Expert Analysis From The Annual International Congenital Heart Disease Symposium
Critical Care Phase in HLHS Extends Through Transfer From ICU to Floor
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
Expert Analysis From The Annual International Congenital Heart Disease Symposium
Critical Care Phase in HLHS Extends Through Transfer From ICU to Floor
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
ST. PETERSBURG, FLA. – Critical care phases for patients with hypoplastic left heart syndrome include both the immediate postoperative period and the recovery period prior to discharge, according to Dr. Peter C. Laussen.
In the immediate postoperative course, critical care largely comes down to a fundamental concern for all critical care patients: the balance between oxygen delivery and oxygen consumption, he said at the Annual International Congenital Heart Disease Symposium.
This is true regardless of the surgical approach to HLHS – which can have its own unique critical care considerations.
“We need to optimize oxygen delivery and minimize oxygen consumption; we need to get that balance correct,” said Dr. Laussen of Children’s Hospital Boston.
This requires continuous monitoring, integration, and interpretation of data – particularly in the rate of change, he added.
Careful attention should be paid during the transfer from the operating room to the cardiac intensive care unit, which is a critical period, he said, noting that surgeons do an important job of “setting the patient up” for the transition, such as by ensuring ultrafiltration in the operating room, peritoneal dialysis catheter placement, electively leaving the sternum open, and providing access via an internal jugular line for the short term and/or a double-lumen right atrium Broviac catheter for the longer term.
“Then we’re left to use indirect measurement to really determine the balance between supply and demand,” he said.
These measurements include:
- Clinical examination, because “continued review of clinical findings is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse width, which needs to be followed very closely, Dr. Laussen said, adding that this is a variable that often isn’t paid enough attention.
- Mixed venous oxygen saturation, which should be used if there is a catheter. Data show that continuous monitoring is associated with improved early survival and lower incidence of end-organ failure.
- End-tidal CO2, which is mandatory on every ventilated patient, he said, adding that the gradient must be known because it provides an index of what is happening with pulmonary blood flow.
- Serum lactate, which is routinely measured in these patients. The rate of change over time has been shown to be positively correlated with predictive value of mortality and morbidity.
- Cerebral and somatic near infrared spectroscopy, which is becoming a standard of care in this group of patients, he said. Findings need to be interpreted in light of all other findings in the patient, with careful attention to the rate of change, which is the critical finding, he noted.
- Clinical examination, because “continual updating of clinical examinations is absolutely vital and a skill that needs to be reinforced and continually taught,” he said.
- Pulse oximetry. This is the most common continuous, yet indirect, variable that everybody tracks and utilizes to make management decisions, Dr. Laussen said.
Once again, interpreting change is most important. There can be a great deal of variability in oxygen saturation following stage I palliation in these patients with functional single ventricular physiology, and it is “very critical to appreciate” the variability, he said.
Changes in SpO2 may be due to one of three things: alteration in pulmonary blood flow, pulmonary venous desaturation, and change in arterial oxygen content, he said.
Minimizing oxygen demand is a very important part of the equation, he said, noting that dopamine has been reported to increase myocardial oxygen consumption secondary to the associated increase in heart rate in these patients, and termination of dopamine is associated with improved oxygen consumption/oxygen delivery balance.
“This has changed our practice. We still use dopamine as our first-line inotrope, but go no higher than 10 [mcg/kg per minute], prefer to stay around 5 [mcg/kg per minute], and go very early to epinephrine,” he said, explaining that epinephrine is a very good inotrope and does not have the detrimental effects seen with dopamine.
As for the “recovery prior to discharge” period in these patients, this should also be considered a critical care phase, he said. This is a time of transfer to the floor, where a new team takes over. There’s a different thought process, and the new team has not seen what has transpired in the prior 1-2 weeks. Additionally, many changes take place in the management of the patient: Monitoring and surveillance may be reduced, efforts are made to advance nutrition, dosages (such as in diuretics) are changed, and anticoagulation practices are variable, he said, noting that “it’s very easy to unravel these patients” during this period.
“We have to be paying close attention to how we continue to follow these patients to avoid readmission to the ICU and the sudden untoward event that can still occur on the floor prior to discharge,” he said.
Dr. Laussen said he had no disclosures.
Expert Analysis From The Annual International Congenital Heart Disease Symposium
Thigh Proves Acceptable Injection Site for Fifth DTaP Dose
Children receiving the fifth dose of the DTaP vaccine are significantly less likely to experience a local injection site reaction if they receive the injection in the thigh rather than the arm.
Of 233,616 children aged 4-6 years who received a diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccination in 2002-2006, only 1,017 (0.4%) experienced a local reaction that required medical attention, but the rate of reactions was 47.4 vs. 32.1 per 10,000 vaccinations for arm vs. thigh injections, respectively, Dr. Lisa A. Jackson of the Group Health Research Institute, Seattle, and her colleagues from the Vaccine Safety Datalink (VSD) team reported in the March issue of Pediatrics.
After adjustment for age, sex, and study site, the risk of a local reaction requiring medical attention was 78% higher with arm vs. thigh injections, the investigators found (Pediatrics 2011;127:e581-7).
In children with a valid body mass index measurement, injection in the arm was associated with a 2.3-fold higher risk of a local reaction, and in that model, BMI also was shown to be an independent risk factor for a reaction. After adjustment for age, sex, and managed care organization site, similar associations of higher BMI and greater risk for a local injection-site reaction persisted among those who received an arm injection and in those vaccinated in the thigh, Dr. Jackson and her associates said, noting that the factors contributing to this association are unclear, but might be a result of an increased likelihood of inadequate intramuscular injection in larger children.
Children included in the study were from the VSD population; VSD is a collaborative project between the Centers for Disease Control and Prevention and a group of eight managed care organizations in the United States that was established in 1991 to monitor and evaluate vaccine safety. Injection-site reactions were identified by using administrative data, and were confirmed by a medical records review.
The findings confirm those from a previous prospective study of 1,315 children, who also had less redness and swelling at the injections site with thigh vs. arm injections, the investigators noted.
According to current recommendations from ACIP (the CDC’s Advisory Committee on Immunization Practices) and the American Academy of Pediatrics, the deltoid muscle in the arm is the preferred site for intramuscular injections in children older than age 1 year, but those recommendations were based on data from 18-month-old children, and reflected an increased likelihood of discomfort and difficulty with movement of the extremity when thigh injections were used.
Indeed, in the current study, nearly 14% of children with a medically attended local reaction following thigh vaccination were noted to have had difficulty walking as a result, which raises the question of whether the lower risk of a reaction with a thigh injection is counterbalanced by the risk of problems with ambulation.
However, the current data do not bear this out.
"If it is assumed that reactions resulting in a medical visit are reactions of greater concern to the parent, for whatever reason, it can be argued that, on balance, the risk of a concerning reaction is lower with thigh injections than with deltoid injections," Dr. Jackson and her colleagues said.
The risk of a medically attended reaction is very low (less than 0.5%) with both approaches; thus, although the findings do not indicate that arm vaccination is contraindicated in this age group, they do suggest that the thigh should be considered an acceptable site of injection for the fifth DTaP vaccination, the authors concluded.
Dr. Jackson received research funding (unrelated to DTaP vaccine) from Sanofi Pasteur and served as a consultant for GlaxoSmithKline. Coauthor Jennifer C. Nelson, Ph.D., reported serving as a statistical consultant to GlaxoSmithKline, and coauthor Dr. Roger Baxter reported receiving research grants from Sanofi Pasteur. The study received funding from the CDC through America’s Health Insurance Plans.
Children receiving the fifth dose of the DTaP vaccine are significantly less likely to experience a local injection site reaction if they receive the injection in the thigh rather than the arm.
Of 233,616 children aged 4-6 years who received a diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccination in 2002-2006, only 1,017 (0.4%) experienced a local reaction that required medical attention, but the rate of reactions was 47.4 vs. 32.1 per 10,000 vaccinations for arm vs. thigh injections, respectively, Dr. Lisa A. Jackson of the Group Health Research Institute, Seattle, and her colleagues from the Vaccine Safety Datalink (VSD) team reported in the March issue of Pediatrics.
After adjustment for age, sex, and study site, the risk of a local reaction requiring medical attention was 78% higher with arm vs. thigh injections, the investigators found (Pediatrics 2011;127:e581-7).
In children with a valid body mass index measurement, injection in the arm was associated with a 2.3-fold higher risk of a local reaction, and in that model, BMI also was shown to be an independent risk factor for a reaction. After adjustment for age, sex, and managed care organization site, similar associations of higher BMI and greater risk for a local injection-site reaction persisted among those who received an arm injection and in those vaccinated in the thigh, Dr. Jackson and her associates said, noting that the factors contributing to this association are unclear, but might be a result of an increased likelihood of inadequate intramuscular injection in larger children.
Children included in the study were from the VSD population; VSD is a collaborative project between the Centers for Disease Control and Prevention and a group of eight managed care organizations in the United States that was established in 1991 to monitor and evaluate vaccine safety. Injection-site reactions were identified by using administrative data, and were confirmed by a medical records review.
The findings confirm those from a previous prospective study of 1,315 children, who also had less redness and swelling at the injections site with thigh vs. arm injections, the investigators noted.
According to current recommendations from ACIP (the CDC’s Advisory Committee on Immunization Practices) and the American Academy of Pediatrics, the deltoid muscle in the arm is the preferred site for intramuscular injections in children older than age 1 year, but those recommendations were based on data from 18-month-old children, and reflected an increased likelihood of discomfort and difficulty with movement of the extremity when thigh injections were used.
Indeed, in the current study, nearly 14% of children with a medically attended local reaction following thigh vaccination were noted to have had difficulty walking as a result, which raises the question of whether the lower risk of a reaction with a thigh injection is counterbalanced by the risk of problems with ambulation.
However, the current data do not bear this out.
"If it is assumed that reactions resulting in a medical visit are reactions of greater concern to the parent, for whatever reason, it can be argued that, on balance, the risk of a concerning reaction is lower with thigh injections than with deltoid injections," Dr. Jackson and her colleagues said.
The risk of a medically attended reaction is very low (less than 0.5%) with both approaches; thus, although the findings do not indicate that arm vaccination is contraindicated in this age group, they do suggest that the thigh should be considered an acceptable site of injection for the fifth DTaP vaccination, the authors concluded.
Dr. Jackson received research funding (unrelated to DTaP vaccine) from Sanofi Pasteur and served as a consultant for GlaxoSmithKline. Coauthor Jennifer C. Nelson, Ph.D., reported serving as a statistical consultant to GlaxoSmithKline, and coauthor Dr. Roger Baxter reported receiving research grants from Sanofi Pasteur. The study received funding from the CDC through America’s Health Insurance Plans.
Children receiving the fifth dose of the DTaP vaccine are significantly less likely to experience a local injection site reaction if they receive the injection in the thigh rather than the arm.
Of 233,616 children aged 4-6 years who received a diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccination in 2002-2006, only 1,017 (0.4%) experienced a local reaction that required medical attention, but the rate of reactions was 47.4 vs. 32.1 per 10,000 vaccinations for arm vs. thigh injections, respectively, Dr. Lisa A. Jackson of the Group Health Research Institute, Seattle, and her colleagues from the Vaccine Safety Datalink (VSD) team reported in the March issue of Pediatrics.
After adjustment for age, sex, and study site, the risk of a local reaction requiring medical attention was 78% higher with arm vs. thigh injections, the investigators found (Pediatrics 2011;127:e581-7).
In children with a valid body mass index measurement, injection in the arm was associated with a 2.3-fold higher risk of a local reaction, and in that model, BMI also was shown to be an independent risk factor for a reaction. After adjustment for age, sex, and managed care organization site, similar associations of higher BMI and greater risk for a local injection-site reaction persisted among those who received an arm injection and in those vaccinated in the thigh, Dr. Jackson and her associates said, noting that the factors contributing to this association are unclear, but might be a result of an increased likelihood of inadequate intramuscular injection in larger children.
Children included in the study were from the VSD population; VSD is a collaborative project between the Centers for Disease Control and Prevention and a group of eight managed care organizations in the United States that was established in 1991 to monitor and evaluate vaccine safety. Injection-site reactions were identified by using administrative data, and were confirmed by a medical records review.
The findings confirm those from a previous prospective study of 1,315 children, who also had less redness and swelling at the injections site with thigh vs. arm injections, the investigators noted.
According to current recommendations from ACIP (the CDC’s Advisory Committee on Immunization Practices) and the American Academy of Pediatrics, the deltoid muscle in the arm is the preferred site for intramuscular injections in children older than age 1 year, but those recommendations were based on data from 18-month-old children, and reflected an increased likelihood of discomfort and difficulty with movement of the extremity when thigh injections were used.
Indeed, in the current study, nearly 14% of children with a medically attended local reaction following thigh vaccination were noted to have had difficulty walking as a result, which raises the question of whether the lower risk of a reaction with a thigh injection is counterbalanced by the risk of problems with ambulation.
However, the current data do not bear this out.
"If it is assumed that reactions resulting in a medical visit are reactions of greater concern to the parent, for whatever reason, it can be argued that, on balance, the risk of a concerning reaction is lower with thigh injections than with deltoid injections," Dr. Jackson and her colleagues said.
The risk of a medically attended reaction is very low (less than 0.5%) with both approaches; thus, although the findings do not indicate that arm vaccination is contraindicated in this age group, they do suggest that the thigh should be considered an acceptable site of injection for the fifth DTaP vaccination, the authors concluded.
Dr. Jackson received research funding (unrelated to DTaP vaccine) from Sanofi Pasteur and served as a consultant for GlaxoSmithKline. Coauthor Jennifer C. Nelson, Ph.D., reported serving as a statistical consultant to GlaxoSmithKline, and coauthor Dr. Roger Baxter reported receiving research grants from Sanofi Pasteur. The study received funding from the CDC through America’s Health Insurance Plans.
FROM PEDIATRICS
Major Finding: Only 1,017 patients (0.4%) experienced a local reaction requiring medical attention, and the rate of reactions was 47.4 vs. 32.1 per 10,000 vaccinations for arm vs. thigh injections, respectively.
Data Source: A retrospective cohort study of 233,616 children aged 4-6 years who received DTaP vaccination in 2002-2006.
Disclosures: Dr. Jackson received research funding (unrelated to DTaP vaccine) from Sanofi Pasteur and served as a consultant for GlaxoSmithKline. Coauthor Jennifer C. Nelson, Ph.D., reported serving as a statistical consultant to GlaxoSmithKline, and coauthor Dr. Roger Baxter reported receiving research grants from Sanofi Pasteur. The study received funding from the CDC through America’s Health Insurance Plans.
Reduced Vaccination Coverage Result of "Unclear" Recommendations During Hib Shortage
Despite interim recommendations that the Hib – Haemophilus influenzae type b – vaccination be deferred only among children who were not at high risk for disease, and that the primary series normally given during the first year of life be provided as usual during the 2008-2009 Hib vaccine shortage, data indicate that vaccination coverage for the primary series was significantly decreased at numerous sites across the United States during that period.
Data from eight Immunization Information System (IIS) sentinel sites across the United States, which included nearly 123,000 children, showed that compared with coverage of two other vaccines given at similar ages – the PCV7 (7-valent pneumococcal conjugate) vaccine and the DTaP (diphtheria, tetanus, and acellular pertussis) vaccine – completion of the primary Hib series by 9 months of age was 7.8-10.3 percentage points lower in seven of the eight sentinel sites during the shortage period, Karen E. White of the Minnesota Department of Health, St. Paul, and her colleagues reported in the March issue of Pediatrics.
Specifically, the percentage point differences in coverage between the Hib and PCV7/DTaP vaccines were –8.6, –7.8, –9.7, –9.1, –10.1, –9.5, and –10.3 at the sentinel sites in Colorado, Michigan, Minnesota, New York City, North Dakota, Oregon, and Wisconsin, respectively, the investigators found (Pediatrics 2011;127:e707-12).
Only the Arizona sentinel site had no significant difference in the vaccination rates, they said.
A comparison of the coverage data during the 2008-2009 shortage vs. coverage data from the prior year (2006-2207) in each of the seven sentinel sites that had lower Hib coverage in 2008-2009 showed that Hib coverage previously was better than, or similar to, coverage for PCV7/DTaP in five of the seven sites, with percentage point differences ranging from +1.3 to +6.1. In the remaining two sites (Oregon and Wisconsin), Hib coverage previously was less than coverage for the other vaccines, but the magnitude of the difference was less during 2006-2007 than what was observed during the shortage (–3.5 vs. –9.5 and –1.7 vs. –10.3 percentage points, respectively).
This study was undertaken after public health officials in Minnesota observed low Hib vaccination coverage of the primary series there during the shortage. The findings, although not generalizable to the entire United States, do suggest that the reduced coverage was not isolated to Minnesota.
Possible explanations for the reduced coverage include limited availability of vaccine to specific provider practices at certain times, challenges in incorporating the combination vaccine product into provider practices, and differences in the availability of Hib vaccine between private and public vaccine stocks, Ms. White and her associates said.
Also, despite widespread efforts by the public health community to disseminate information about the interim recommendations through a variety of publications and media outlets, a "significant minority" of clinicians considered the recommendations to be unclear, they noted.
The findings from the IIS – a collaborative project between the Centers for Disease Control and Prevention and several city- and state-based information systems that is designed to evaluate immunization programs and estimate vaccine coverage – underscore the importance of the processes of sharing clear recommendations during vaccine shortages and providing public health support to vaccine providers to carry out the recommendations, they concluded.
Ms. White and her associates stated that they had no relevant financial disclosures.
Despite interim recommendations that the Hib – Haemophilus influenzae type b – vaccination be deferred only among children who were not at high risk for disease, and that the primary series normally given during the first year of life be provided as usual during the 2008-2009 Hib vaccine shortage, data indicate that vaccination coverage for the primary series was significantly decreased at numerous sites across the United States during that period.
Data from eight Immunization Information System (IIS) sentinel sites across the United States, which included nearly 123,000 children, showed that compared with coverage of two other vaccines given at similar ages – the PCV7 (7-valent pneumococcal conjugate) vaccine and the DTaP (diphtheria, tetanus, and acellular pertussis) vaccine – completion of the primary Hib series by 9 months of age was 7.8-10.3 percentage points lower in seven of the eight sentinel sites during the shortage period, Karen E. White of the Minnesota Department of Health, St. Paul, and her colleagues reported in the March issue of Pediatrics.
Specifically, the percentage point differences in coverage between the Hib and PCV7/DTaP vaccines were –8.6, –7.8, –9.7, –9.1, –10.1, –9.5, and –10.3 at the sentinel sites in Colorado, Michigan, Minnesota, New York City, North Dakota, Oregon, and Wisconsin, respectively, the investigators found (Pediatrics 2011;127:e707-12).
Only the Arizona sentinel site had no significant difference in the vaccination rates, they said.
A comparison of the coverage data during the 2008-2009 shortage vs. coverage data from the prior year (2006-2207) in each of the seven sentinel sites that had lower Hib coverage in 2008-2009 showed that Hib coverage previously was better than, or similar to, coverage for PCV7/DTaP in five of the seven sites, with percentage point differences ranging from +1.3 to +6.1. In the remaining two sites (Oregon and Wisconsin), Hib coverage previously was less than coverage for the other vaccines, but the magnitude of the difference was less during 2006-2007 than what was observed during the shortage (–3.5 vs. –9.5 and –1.7 vs. –10.3 percentage points, respectively).
This study was undertaken after public health officials in Minnesota observed low Hib vaccination coverage of the primary series there during the shortage. The findings, although not generalizable to the entire United States, do suggest that the reduced coverage was not isolated to Minnesota.
Possible explanations for the reduced coverage include limited availability of vaccine to specific provider practices at certain times, challenges in incorporating the combination vaccine product into provider practices, and differences in the availability of Hib vaccine between private and public vaccine stocks, Ms. White and her associates said.
Also, despite widespread efforts by the public health community to disseminate information about the interim recommendations through a variety of publications and media outlets, a "significant minority" of clinicians considered the recommendations to be unclear, they noted.
The findings from the IIS – a collaborative project between the Centers for Disease Control and Prevention and several city- and state-based information systems that is designed to evaluate immunization programs and estimate vaccine coverage – underscore the importance of the processes of sharing clear recommendations during vaccine shortages and providing public health support to vaccine providers to carry out the recommendations, they concluded.
Ms. White and her associates stated that they had no relevant financial disclosures.
Despite interim recommendations that the Hib – Haemophilus influenzae type b – vaccination be deferred only among children who were not at high risk for disease, and that the primary series normally given during the first year of life be provided as usual during the 2008-2009 Hib vaccine shortage, data indicate that vaccination coverage for the primary series was significantly decreased at numerous sites across the United States during that period.
Data from eight Immunization Information System (IIS) sentinel sites across the United States, which included nearly 123,000 children, showed that compared with coverage of two other vaccines given at similar ages – the PCV7 (7-valent pneumococcal conjugate) vaccine and the DTaP (diphtheria, tetanus, and acellular pertussis) vaccine – completion of the primary Hib series by 9 months of age was 7.8-10.3 percentage points lower in seven of the eight sentinel sites during the shortage period, Karen E. White of the Minnesota Department of Health, St. Paul, and her colleagues reported in the March issue of Pediatrics.
Specifically, the percentage point differences in coverage between the Hib and PCV7/DTaP vaccines were –8.6, –7.8, –9.7, –9.1, –10.1, –9.5, and –10.3 at the sentinel sites in Colorado, Michigan, Minnesota, New York City, North Dakota, Oregon, and Wisconsin, respectively, the investigators found (Pediatrics 2011;127:e707-12).
Only the Arizona sentinel site had no significant difference in the vaccination rates, they said.
A comparison of the coverage data during the 2008-2009 shortage vs. coverage data from the prior year (2006-2207) in each of the seven sentinel sites that had lower Hib coverage in 2008-2009 showed that Hib coverage previously was better than, or similar to, coverage for PCV7/DTaP in five of the seven sites, with percentage point differences ranging from +1.3 to +6.1. In the remaining two sites (Oregon and Wisconsin), Hib coverage previously was less than coverage for the other vaccines, but the magnitude of the difference was less during 2006-2007 than what was observed during the shortage (–3.5 vs. –9.5 and –1.7 vs. –10.3 percentage points, respectively).
This study was undertaken after public health officials in Minnesota observed low Hib vaccination coverage of the primary series there during the shortage. The findings, although not generalizable to the entire United States, do suggest that the reduced coverage was not isolated to Minnesota.
Possible explanations for the reduced coverage include limited availability of vaccine to specific provider practices at certain times, challenges in incorporating the combination vaccine product into provider practices, and differences in the availability of Hib vaccine between private and public vaccine stocks, Ms. White and her associates said.
Also, despite widespread efforts by the public health community to disseminate information about the interim recommendations through a variety of publications and media outlets, a "significant minority" of clinicians considered the recommendations to be unclear, they noted.
The findings from the IIS – a collaborative project between the Centers for Disease Control and Prevention and several city- and state-based information systems that is designed to evaluate immunization programs and estimate vaccine coverage – underscore the importance of the processes of sharing clear recommendations during vaccine shortages and providing public health support to vaccine providers to carry out the recommendations, they concluded.
Ms. White and her associates stated that they had no relevant financial disclosures.
Major Finding: Compared with coverage of two other vaccines given at similar ages –PCV7 and DTaP – completion of the primary Hib series by 9 months of age was 7.8-10.3 percentage points lower in seven of the eight sentinel sites during the 2008-2009 Hib shortage.
Data Source: An analysis of vaccination data from eight IIS sentinel sites involving 122,956 children.
Disclosures: Ms. White and her associates stated that they had no relevant financial disclosures.
SDEF: Psoriasis Comorbidities Carry Implications for Disease Management
Studies show that severe psoriasis is associated with a 50% increased risk of mortality and up to 5 years of life lost, according to Dr. Joel M. Gelfand.
The leading causes of death in psoriasis patients are cardiovascular disease, infection, and cancer, which account for 34%, 22%, and 21% of deaths, respectively (Br. J. Dermatol. 2010;163:586-92), Dr. Gelfand said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).

Although there are not yet enough data to confirm a causal effect between psoriasis and these leading causes of death, the findings do have implications for managing patients with psoriasis, he said. Data have consistently demonstrated an association between psoriasis and cardiovascular disease, with numerous published studies linking the two conditions.
Taken together, findings from several of these studies suggest that patients with psoriasis are at increased risk of myocardial infarction, stroke, and cardiovascular death, and that those with severe psoriasis have the greatest risks, said Dr. Gelfand of the department of dermatology at the University of Pennsylvania in Philadelphia.
The clinical significance of these findings is striking; patients with severe psoriasis, for example, are 15 times more likely to die prematurely as a result of cardiovascular disease attributable to psoriasis than they are to develop a melanoma, he said.
One study demonstrated a link between psoriasis and several cardiovascular risk factors, including smoking, obesity, dyslipidemia, hypertension, and diabetes, said Dr. Gelfand, who was one of the authors of the study (J. Am. Acad. Dermatol. 2006;55;829-35).
Furthermore, a population-based cohort study involving more than 130,000 psoriasis patients – including more than 3,800 with severe psoriasis - and up to 5 controls per patient, suggested that psoriasis confers an independent risk for myocardial infarction, particularly in young patients with severe psoriasis. The adjusted relative risk of MI in a 30-year-old patient with mild psoriasis was 1.29, and in a 30-year-old with severe psoriasis was 3.01. The adjusted relative risk of MI in a 60-year old with mild psoriasis was 1.08, and in a 60-year-old with severe psoriasis was 1.36, Dr. Gelfand and his colleagues reported (JAMA 2006;296:1735-41).
That study was conducted using the General Practice Research Database of medical records in the United Kingdom, which includes more than 9 million patients and more than 40 million person-years of follow-up data from 1987 to 2002, he said, adding that at least 12 papers have confirmed an association between psoriasis and cardiovascular disease independent of traditional risk factors for cardiovascular disease.
Although the available data on psoriasis and cardiovascular disease demonstrate the biologic credibility of an association, as well as a plausible time sequence suggesting causation, dose response has been demonstrated in only a few studies, and the strength of the study design has been variable, Dr. Gelfand said.
Although most studies have found an effect – along with a modest but clinically important strength of association similar to the association seen in heart disease, hypertension, and diabetes – data from a randomized controlled trial are needed before a causal relationship between psoriasis and cardiovascular disease can be confirmed, and before a link between aggressive treatment of psoriasis and a reduced risk of cardiovascular disease can be demonstrated, he said in an interview, adding that it currently remains unclear whether aggressive treatment will lower cardiovascular disease risk.
However, the U.S. Preventive Services Task Force, the American Diabetes Association, and the National Cholesterol Education Program recommend that severe psoriasis patients over age 21 years undergo blood pressure screening at each office visit; that those aged 45 years and older undergo fasting blood glucose testing every 3 years (unless they have diabetes risk factors, in which case they should undergo screening earlier and more often); and that those aged 20 years and older undergo cholesterol screening every 5 years.
Existing data also support recommendations for addressing concerns about infection and cancer risk in patients with psoriasis, Dr. Gelfand said.
Patients with severe psoriasis are 65% more likely to die of an infection than are those without psoriasis (Br. J. Dermatol. 2010;163:586-92). Specifically, studies have shown that streptococcal pharyngitis is a risk factor for guttate psoriasis, and that HIV is a risk factor for severe psoriasis, he said, noting that it is recommended that patients be screened for streptococcal infection with guttate flares, and that they be screened for HIV if they have severe psoriasis.
It is also important that patients with psoriasis be routinely vaccinated – prior to initiation of immunosuppressive therapy – against influenza and pneumonia. Vaccination against hepatitis B in patients at risk for infection should also be considered, as well as vaccination against zoster in patients aged 60 and older.
As for cancer, it is a concern in psoriasis patients because of the chronic use of immunosuppressive therapies, comorbid behaviors, and chronic inflammation, Dr. Gelfand said. Patients with severe psoriasis are 41% more likely to die of cancer than are those without psoriasis.
Studies have shown – although not consistently – that psoriasis may be linked with lung, liver, pancreatic, breast, colon, bladder, and kidney cancer. Lymphoma is also a particular concern, with cutaneous T-cell lymphoma having the strongest association.
As with cardiovascular disease, however, findings are not strong or consistent enough to confirm a causal effect of psoriasis on cancer risk, or to clarify whether any association is a disease effect or treatment effect.
Still, the available findings are concerning enough that biopsy should be considered in severe disease, especially if clinical features are not classic, and in those who fail to respond to treatment, because cutaneous T-cell lymphoma may progress rapidly in those on immunosuppressive therapy.
"Always consider a skin biopsy in patients with atypical features of psoriasis and those not responding to treatment," Dr. Gelfand said.
Also, encourage patients to stay up to date on age-appropriate cancer screening. According to Centers for Disease Control guidelines, women aged 21-70 years should undergo cervical cancer screening every 2-3 years, women aged 50-74 years should undergo screening for breast cancer by mammography every 2 years, and men and women aged 50-75 years should undergo screening for colon cancer by fecal occult blood testing every year, by flexible sigmoidoscopy every 5 years, and by colonoscopy every 10 years, he said.
Dr. Gelfand has been an investigator and/or consultant for Amgen, Abbott, Centocor, Pfizer, Celgene, Novartis, and Genentech. He reported having no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
Studies show that severe psoriasis is associated with a 50% increased risk of mortality and up to 5 years of life lost, according to Dr. Joel M. Gelfand.
The leading causes of death in psoriasis patients are cardiovascular disease, infection, and cancer, which account for 34%, 22%, and 21% of deaths, respectively (Br. J. Dermatol. 2010;163:586-92), Dr. Gelfand said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Although there are not yet enough data to confirm a causal effect between psoriasis and these leading causes of death, the findings do have implications for managing patients with psoriasis, he said. Data have consistently demonstrated an association between psoriasis and cardiovascular disease, with numerous published studies linking the two conditions.
Taken together, findings from several of these studies suggest that patients with psoriasis are at increased risk of myocardial infarction, stroke, and cardiovascular death, and that those with severe psoriasis have the greatest risks, said Dr. Gelfand of the department of dermatology at the University of Pennsylvania in Philadelphia.
The clinical significance of these findings is striking; patients with severe psoriasis, for example, are 15 times more likely to die prematurely as a result of cardiovascular disease attributable to psoriasis than they are to develop a melanoma, he said.
One study demonstrated a link between psoriasis and several cardiovascular risk factors, including smoking, obesity, dyslipidemia, hypertension, and diabetes, said Dr. Gelfand, who was one of the authors of the study (J. Am. Acad. Dermatol. 2006;55;829-35).
Furthermore, a population-based cohort study involving more than 130,000 psoriasis patients – including more than 3,800 with severe psoriasis - and up to 5 controls per patient, suggested that psoriasis confers an independent risk for myocardial infarction, particularly in young patients with severe psoriasis. The adjusted relative risk of MI in a 30-year-old patient with mild psoriasis was 1.29, and in a 30-year-old with severe psoriasis was 3.01. The adjusted relative risk of MI in a 60-year old with mild psoriasis was 1.08, and in a 60-year-old with severe psoriasis was 1.36, Dr. Gelfand and his colleagues reported (JAMA 2006;296:1735-41).
That study was conducted using the General Practice Research Database of medical records in the United Kingdom, which includes more than 9 million patients and more than 40 million person-years of follow-up data from 1987 to 2002, he said, adding that at least 12 papers have confirmed an association between psoriasis and cardiovascular disease independent of traditional risk factors for cardiovascular disease.
Although the available data on psoriasis and cardiovascular disease demonstrate the biologic credibility of an association, as well as a plausible time sequence suggesting causation, dose response has been demonstrated in only a few studies, and the strength of the study design has been variable, Dr. Gelfand said.
Although most studies have found an effect – along with a modest but clinically important strength of association similar to the association seen in heart disease, hypertension, and diabetes – data from a randomized controlled trial are needed before a causal relationship between psoriasis and cardiovascular disease can be confirmed, and before a link between aggressive treatment of psoriasis and a reduced risk of cardiovascular disease can be demonstrated, he said in an interview, adding that it currently remains unclear whether aggressive treatment will lower cardiovascular disease risk.
However, the U.S. Preventive Services Task Force, the American Diabetes Association, and the National Cholesterol Education Program recommend that severe psoriasis patients over age 21 years undergo blood pressure screening at each office visit; that those aged 45 years and older undergo fasting blood glucose testing every 3 years (unless they have diabetes risk factors, in which case they should undergo screening earlier and more often); and that those aged 20 years and older undergo cholesterol screening every 5 years.
Existing data also support recommendations for addressing concerns about infection and cancer risk in patients with psoriasis, Dr. Gelfand said.
Patients with severe psoriasis are 65% more likely to die of an infection than are those without psoriasis (Br. J. Dermatol. 2010;163:586-92). Specifically, studies have shown that streptococcal pharyngitis is a risk factor for guttate psoriasis, and that HIV is a risk factor for severe psoriasis, he said, noting that it is recommended that patients be screened for streptococcal infection with guttate flares, and that they be screened for HIV if they have severe psoriasis.
It is also important that patients with psoriasis be routinely vaccinated – prior to initiation of immunosuppressive therapy – against influenza and pneumonia. Vaccination against hepatitis B in patients at risk for infection should also be considered, as well as vaccination against zoster in patients aged 60 and older.
As for cancer, it is a concern in psoriasis patients because of the chronic use of immunosuppressive therapies, comorbid behaviors, and chronic inflammation, Dr. Gelfand said. Patients with severe psoriasis are 41% more likely to die of cancer than are those without psoriasis.
Studies have shown – although not consistently – that psoriasis may be linked with lung, liver, pancreatic, breast, colon, bladder, and kidney cancer. Lymphoma is also a particular concern, with cutaneous T-cell lymphoma having the strongest association.
As with cardiovascular disease, however, findings are not strong or consistent enough to confirm a causal effect of psoriasis on cancer risk, or to clarify whether any association is a disease effect or treatment effect.
Still, the available findings are concerning enough that biopsy should be considered in severe disease, especially if clinical features are not classic, and in those who fail to respond to treatment, because cutaneous T-cell lymphoma may progress rapidly in those on immunosuppressive therapy.
"Always consider a skin biopsy in patients with atypical features of psoriasis and those not responding to treatment," Dr. Gelfand said.
Also, encourage patients to stay up to date on age-appropriate cancer screening. According to Centers for Disease Control guidelines, women aged 21-70 years should undergo cervical cancer screening every 2-3 years, women aged 50-74 years should undergo screening for breast cancer by mammography every 2 years, and men and women aged 50-75 years should undergo screening for colon cancer by fecal occult blood testing every year, by flexible sigmoidoscopy every 5 years, and by colonoscopy every 10 years, he said.
Dr. Gelfand has been an investigator and/or consultant for Amgen, Abbott, Centocor, Pfizer, Celgene, Novartis, and Genentech. He reported having no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
Studies show that severe psoriasis is associated with a 50% increased risk of mortality and up to 5 years of life lost, according to Dr. Joel M. Gelfand.
The leading causes of death in psoriasis patients are cardiovascular disease, infection, and cancer, which account for 34%, 22%, and 21% of deaths, respectively (Br. J. Dermatol. 2010;163:586-92), Dr. Gelfand said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Although there are not yet enough data to confirm a causal effect between psoriasis and these leading causes of death, the findings do have implications for managing patients with psoriasis, he said. Data have consistently demonstrated an association between psoriasis and cardiovascular disease, with numerous published studies linking the two conditions.
Taken together, findings from several of these studies suggest that patients with psoriasis are at increased risk of myocardial infarction, stroke, and cardiovascular death, and that those with severe psoriasis have the greatest risks, said Dr. Gelfand of the department of dermatology at the University of Pennsylvania in Philadelphia.
The clinical significance of these findings is striking; patients with severe psoriasis, for example, are 15 times more likely to die prematurely as a result of cardiovascular disease attributable to psoriasis than they are to develop a melanoma, he said.
One study demonstrated a link between psoriasis and several cardiovascular risk factors, including smoking, obesity, dyslipidemia, hypertension, and diabetes, said Dr. Gelfand, who was one of the authors of the study (J. Am. Acad. Dermatol. 2006;55;829-35).
Furthermore, a population-based cohort study involving more than 130,000 psoriasis patients – including more than 3,800 with severe psoriasis - and up to 5 controls per patient, suggested that psoriasis confers an independent risk for myocardial infarction, particularly in young patients with severe psoriasis. The adjusted relative risk of MI in a 30-year-old patient with mild psoriasis was 1.29, and in a 30-year-old with severe psoriasis was 3.01. The adjusted relative risk of MI in a 60-year old with mild psoriasis was 1.08, and in a 60-year-old with severe psoriasis was 1.36, Dr. Gelfand and his colleagues reported (JAMA 2006;296:1735-41).
That study was conducted using the General Practice Research Database of medical records in the United Kingdom, which includes more than 9 million patients and more than 40 million person-years of follow-up data from 1987 to 2002, he said, adding that at least 12 papers have confirmed an association between psoriasis and cardiovascular disease independent of traditional risk factors for cardiovascular disease.
Although the available data on psoriasis and cardiovascular disease demonstrate the biologic credibility of an association, as well as a plausible time sequence suggesting causation, dose response has been demonstrated in only a few studies, and the strength of the study design has been variable, Dr. Gelfand said.
Although most studies have found an effect – along with a modest but clinically important strength of association similar to the association seen in heart disease, hypertension, and diabetes – data from a randomized controlled trial are needed before a causal relationship between psoriasis and cardiovascular disease can be confirmed, and before a link between aggressive treatment of psoriasis and a reduced risk of cardiovascular disease can be demonstrated, he said in an interview, adding that it currently remains unclear whether aggressive treatment will lower cardiovascular disease risk.
However, the U.S. Preventive Services Task Force, the American Diabetes Association, and the National Cholesterol Education Program recommend that severe psoriasis patients over age 21 years undergo blood pressure screening at each office visit; that those aged 45 years and older undergo fasting blood glucose testing every 3 years (unless they have diabetes risk factors, in which case they should undergo screening earlier and more often); and that those aged 20 years and older undergo cholesterol screening every 5 years.
Existing data also support recommendations for addressing concerns about infection and cancer risk in patients with psoriasis, Dr. Gelfand said.
Patients with severe psoriasis are 65% more likely to die of an infection than are those without psoriasis (Br. J. Dermatol. 2010;163:586-92). Specifically, studies have shown that streptococcal pharyngitis is a risk factor for guttate psoriasis, and that HIV is a risk factor for severe psoriasis, he said, noting that it is recommended that patients be screened for streptococcal infection with guttate flares, and that they be screened for HIV if they have severe psoriasis.
It is also important that patients with psoriasis be routinely vaccinated – prior to initiation of immunosuppressive therapy – against influenza and pneumonia. Vaccination against hepatitis B in patients at risk for infection should also be considered, as well as vaccination against zoster in patients aged 60 and older.
As for cancer, it is a concern in psoriasis patients because of the chronic use of immunosuppressive therapies, comorbid behaviors, and chronic inflammation, Dr. Gelfand said. Patients with severe psoriasis are 41% more likely to die of cancer than are those without psoriasis.
Studies have shown – although not consistently – that psoriasis may be linked with lung, liver, pancreatic, breast, colon, bladder, and kidney cancer. Lymphoma is also a particular concern, with cutaneous T-cell lymphoma having the strongest association.
As with cardiovascular disease, however, findings are not strong or consistent enough to confirm a causal effect of psoriasis on cancer risk, or to clarify whether any association is a disease effect or treatment effect.
Still, the available findings are concerning enough that biopsy should be considered in severe disease, especially if clinical features are not classic, and in those who fail to respond to treatment, because cutaneous T-cell lymphoma may progress rapidly in those on immunosuppressive therapy.
"Always consider a skin biopsy in patients with atypical features of psoriasis and those not responding to treatment," Dr. Gelfand said.
Also, encourage patients to stay up to date on age-appropriate cancer screening. According to Centers for Disease Control guidelines, women aged 21-70 years should undergo cervical cancer screening every 2-3 years, women aged 50-74 years should undergo screening for breast cancer by mammography every 2 years, and men and women aged 50-75 years should undergo screening for colon cancer by fecal occult blood testing every year, by flexible sigmoidoscopy every 5 years, and by colonoscopy every 10 years, he said.
Dr. Gelfand has been an investigator and/or consultant for Amgen, Abbott, Centocor, Pfizer, Celgene, Novartis, and Genentech. He reported having no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Similar Outcomes for Bidirectional Cavopulmonary Shunt and. Hemi-Fontan
ST. PETERSBURG, FLA. – Both the bidirectional cavopulmonary shunt and the hemi-Fontan procedure have been used in children with hypoplastic left heart syndrome. Is one better than the other?
Dr. Tom Karl, deputy director of pediatric cardiac surgery at Mater Children’s Hospital in South Brisbane, Queensland, sought to answer this question at the annual International Congenital Heart Disease Symposium.
One potential benefit of the bidirectional cavopulmonary shunt (also called the bidirectional Glenn shunt), he said, is decreased tricuspid insufficiency as the right ventricle’s geometry normalizes from volume unloading.
Other potential benefits include avoidance of later hypertrophy and subendocardial ischemic damage. General hemodynamic stability is promoted by improvement in effective systemic output – with reduced interstage mortality, better somatic growth, and the opportunity to correct associated abnormalities out of the neonatal period, he added.
But is the bidirectional cavopulmonary shunt better than the hemi-Fontan procedure when it is used as the second stage in the typical three-stage treatment sequence (between neonatal palliation, such as the Norwood procedure, and a Fontan operation) for the univentricular heart?
It does have some advantages: It is technically simpler; it can be performed on a beating heart at normothermia, and off pump in many cases; and it requires no prosthetic material. It also is a very good setup for an extracardiac variant of the Fontan operation.
"On the other hand, there is some potential for stenosis, and there is probably some asymmetry of flow in many cases," said Dr. Karl.
The hemi-Fontan doesn’t have asymmetry of flow; there is actually very good flow to the left lung, he said. Also, there is a long, favorable history of this type of anastomosis specifically in hypoplastic left heart syndrome, and the hemi-Fontan provides a good setup for a lateral tunnel Fontan completion. Stenosis risk is minimal.
However, the hemi-Fontan is technically more complex. It requires cardiopulmonary bypass, which some surgeons choose to do using deep hypothermic circulatory arrest, and it may pose greater risk to the sinoatrial node. The hemi-Fontan also requires a considerable load of prosthetic material, but this is not seen as a disadvantage if the procedure follows a Norwood procedure, Dr. Karl noted.
Sinus node dysfunction, which has been examined in detail by investigators at the Children’s Hospital of Philadelphia, is a common problem in the early postoperative period following a hemi-Fontan procedure (J. Thorac. Cardiovasc. Surg. 2001:121:582-3).
The investigators found that on postoperative day 1, sinus node dysfunction occurred in 9.8% of 51 patients undergoing bidirectional cavopulmonary shunt, compared with 36% of 79 hemi-Fontan patients.
"But these differences are amortized by the time the patient is discharged – 6% and 8%, respectively, had sinus node dysfunction at discharge – and in any case, most (81%) of the sinus nodes recover during the interstage period," Dr. Karl said.
Also, the incidence of sinus node dysfunction after a lateral tunnel and an extracardiac Fontan seems to be about the same, at 13% in each group, he noted.
"So what is the best anastomosis strategy for the cavopulmonary connection? Based on recent studies using computational flow modeling and MRI studies, it seems that the key factor ... relates mostly to the cross-sectional area of the anastomosis, and some of the other geometric factors don’t have as much effect as we had predicted earlier. So I think this comes down to surgeon’s choice or institutional choice, and both procedures work quite well," he said.
Dr. Karl declared he had no conflicts of interest.
ST. PETERSBURG, FLA. – Both the bidirectional cavopulmonary shunt and the hemi-Fontan procedure have been used in children with hypoplastic left heart syndrome. Is one better than the other?
Dr. Tom Karl, deputy director of pediatric cardiac surgery at Mater Children’s Hospital in South Brisbane, Queensland, sought to answer this question at the annual International Congenital Heart Disease Symposium.
One potential benefit of the bidirectional cavopulmonary shunt (also called the bidirectional Glenn shunt), he said, is decreased tricuspid insufficiency as the right ventricle’s geometry normalizes from volume unloading.
Other potential benefits include avoidance of later hypertrophy and subendocardial ischemic damage. General hemodynamic stability is promoted by improvement in effective systemic output – with reduced interstage mortality, better somatic growth, and the opportunity to correct associated abnormalities out of the neonatal period, he added.
But is the bidirectional cavopulmonary shunt better than the hemi-Fontan procedure when it is used as the second stage in the typical three-stage treatment sequence (between neonatal palliation, such as the Norwood procedure, and a Fontan operation) for the univentricular heart?
It does have some advantages: It is technically simpler; it can be performed on a beating heart at normothermia, and off pump in many cases; and it requires no prosthetic material. It also is a very good setup for an extracardiac variant of the Fontan operation.
"On the other hand, there is some potential for stenosis, and there is probably some asymmetry of flow in many cases," said Dr. Karl.
The hemi-Fontan doesn’t have asymmetry of flow; there is actually very good flow to the left lung, he said. Also, there is a long, favorable history of this type of anastomosis specifically in hypoplastic left heart syndrome, and the hemi-Fontan provides a good setup for a lateral tunnel Fontan completion. Stenosis risk is minimal.
However, the hemi-Fontan is technically more complex. It requires cardiopulmonary bypass, which some surgeons choose to do using deep hypothermic circulatory arrest, and it may pose greater risk to the sinoatrial node. The hemi-Fontan also requires a considerable load of prosthetic material, but this is not seen as a disadvantage if the procedure follows a Norwood procedure, Dr. Karl noted.
Sinus node dysfunction, which has been examined in detail by investigators at the Children’s Hospital of Philadelphia, is a common problem in the early postoperative period following a hemi-Fontan procedure (J. Thorac. Cardiovasc. Surg. 2001:121:582-3).
The investigators found that on postoperative day 1, sinus node dysfunction occurred in 9.8% of 51 patients undergoing bidirectional cavopulmonary shunt, compared with 36% of 79 hemi-Fontan patients.
"But these differences are amortized by the time the patient is discharged – 6% and 8%, respectively, had sinus node dysfunction at discharge – and in any case, most (81%) of the sinus nodes recover during the interstage period," Dr. Karl said.
Also, the incidence of sinus node dysfunction after a lateral tunnel and an extracardiac Fontan seems to be about the same, at 13% in each group, he noted.
"So what is the best anastomosis strategy for the cavopulmonary connection? Based on recent studies using computational flow modeling and MRI studies, it seems that the key factor ... relates mostly to the cross-sectional area of the anastomosis, and some of the other geometric factors don’t have as much effect as we had predicted earlier. So I think this comes down to surgeon’s choice or institutional choice, and both procedures work quite well," he said.
Dr. Karl declared he had no conflicts of interest.
ST. PETERSBURG, FLA. – Both the bidirectional cavopulmonary shunt and the hemi-Fontan procedure have been used in children with hypoplastic left heart syndrome. Is one better than the other?
Dr. Tom Karl, deputy director of pediatric cardiac surgery at Mater Children’s Hospital in South Brisbane, Queensland, sought to answer this question at the annual International Congenital Heart Disease Symposium.
One potential benefit of the bidirectional cavopulmonary shunt (also called the bidirectional Glenn shunt), he said, is decreased tricuspid insufficiency as the right ventricle’s geometry normalizes from volume unloading.
Other potential benefits include avoidance of later hypertrophy and subendocardial ischemic damage. General hemodynamic stability is promoted by improvement in effective systemic output – with reduced interstage mortality, better somatic growth, and the opportunity to correct associated abnormalities out of the neonatal period, he added.
But is the bidirectional cavopulmonary shunt better than the hemi-Fontan procedure when it is used as the second stage in the typical three-stage treatment sequence (between neonatal palliation, such as the Norwood procedure, and a Fontan operation) for the univentricular heart?
It does have some advantages: It is technically simpler; it can be performed on a beating heart at normothermia, and off pump in many cases; and it requires no prosthetic material. It also is a very good setup for an extracardiac variant of the Fontan operation.
"On the other hand, there is some potential for stenosis, and there is probably some asymmetry of flow in many cases," said Dr. Karl.
The hemi-Fontan doesn’t have asymmetry of flow; there is actually very good flow to the left lung, he said. Also, there is a long, favorable history of this type of anastomosis specifically in hypoplastic left heart syndrome, and the hemi-Fontan provides a good setup for a lateral tunnel Fontan completion. Stenosis risk is minimal.
However, the hemi-Fontan is technically more complex. It requires cardiopulmonary bypass, which some surgeons choose to do using deep hypothermic circulatory arrest, and it may pose greater risk to the sinoatrial node. The hemi-Fontan also requires a considerable load of prosthetic material, but this is not seen as a disadvantage if the procedure follows a Norwood procedure, Dr. Karl noted.
Sinus node dysfunction, which has been examined in detail by investigators at the Children’s Hospital of Philadelphia, is a common problem in the early postoperative period following a hemi-Fontan procedure (J. Thorac. Cardiovasc. Surg. 2001:121:582-3).
The investigators found that on postoperative day 1, sinus node dysfunction occurred in 9.8% of 51 patients undergoing bidirectional cavopulmonary shunt, compared with 36% of 79 hemi-Fontan patients.
"But these differences are amortized by the time the patient is discharged – 6% and 8%, respectively, had sinus node dysfunction at discharge – and in any case, most (81%) of the sinus nodes recover during the interstage period," Dr. Karl said.
Also, the incidence of sinus node dysfunction after a lateral tunnel and an extracardiac Fontan seems to be about the same, at 13% in each group, he noted.
"So what is the best anastomosis strategy for the cavopulmonary connection? Based on recent studies using computational flow modeling and MRI studies, it seems that the key factor ... relates mostly to the cross-sectional area of the anastomosis, and some of the other geometric factors don’t have as much effect as we had predicted earlier. So I think this comes down to surgeon’s choice or institutional choice, and both procedures work quite well," he said.
Dr. Karl declared he had no conflicts of interest.
Diabetes Linked With Risk of Premature Death
Diabetes is independently associated with premature death from numerous causes, including several nonvascular causes, according to findings from an analysis of individual-participant data from 97 prospective studies.
The risk of death from any cause was increased in 40,116 patients with diabetes, compared with 674,945 without diabetes (hazard ratio, 1.80), after adjustment for age, sex, smoking status, and body mass index. Similarly, the patients with diabetes also had increased risks of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and deaths of unknown or ill-defined causes (HR, 1.88), investigators reported in the March 3 issue of the New England Journal of Medicine.
Specific cancers that were found in this study to be moderately associated with premature death in diabetes patients vs. nondiabetes patients were liver, pancreas, ovary, colorectum, bladder, lung, and breast cancer (HRs, 2.16, 1.51, 1.45, 1.40, 1.40, 1.27 and 1.25, respectively), reported Dr. Sreenivasa Rao Kondapally Seshasai of the University of Cambridge (England) and colleagues from the Emerging Risk Factors Collaboration (ERFC).
"Other" causes of death in diabetes patients vs. nondiabetes patients included renal disease; liver disease; pneumonia and other infectious diseases; mental disorders; nonhepatic digestive diseases; external causes; intentional self-harm; nervous-system disorders; and chronic obstructive pulmonary disease, the investigators found (N. Engl. J. Med. 2011;364:829-41).
"These hazard ratios were not appreciably reduced after additional adjustment for systolic blood pressure, lipid levels, C-reactive protein levels, fibrinogen levels, alcohol use, estimated glomerular filtration rate, or indicators of socioeconomic status," the investigators said.
The hazard ratios were, however, reduced considerably after adjustment for fasting glucose or glycated hemoglobin levels, they noted.
Fasting glucose levels exceeding 100 mg/dL – but not levels of 70-100 mg/dL – were associated with excess risk of mortality.
In this study, middle-aged adults with diabetes but without known vascular disease at the time of enrollment generally died earlier than did those without diabetes.
"At 40, 50, and 60 years of age, men with diabetes but without a history of vascular disease would incur about 6.3, 5.8, and 4.5 years of life lost, respectively. The corresponding years of life lost for women with diabetes in middle age were 6.8, 6.4, and 5.4 years, respectively," the investigators wrote. They noted that about 58%, 9%, and 30% of the survival difference at 50 years between those with and without diabetes was attributable to excess vascular, cancer, and noncancer nonvascular deaths, respectively. The number of years of life lost because of diabetes was close to the 7-year reduction in life expectancy among long-term cigarette smokers.
About 40% of the years of life lost as a result of diabetes were attributable to nonvascular conditions, including about 10% attributable to cancer-related death, they said.
The finding of "generally continuous associations" between fasting glucose levels above 100 mg/dL and death suggests that hyperglycemia or a similar factor has direct relevance to the association between diabetes and premature death from these various causes – a finding that is also supported by the "substantial attenuation observed in hazard ratios for death from diabetes after adjustment for markers of glycemia," they added.
In contrast, other risk factors (such as blood pressure, adiposity, inflammation, insulin, and renal function) do not appear to be major mediators of the excess risk of death.
The ERFC is a collaboration that has previously published reports on the associations between lipids, lipoproteins, and inflammatory markers and the risk of vascular disease and cause-specific death. In 2009, the group extended its focus to include analyses of diabetes and other metabolic markers as they relate to incident vascular disease outcomes and cause-specific death. For the current study, the collaboration analyzed individual-participant data from prospective studies with information on diabetes diagnosis or fasting baseline blood-glucose levels. Studies included in the analysis did not select participants on the basis of having previous chronic disease; they did, however, record cause-specific death classified according to clearly defined criteria, and accrued more than 1 year of follow-up data.
The current analysis included 820,900 participants from those studies, of whom 123,205 died. The average age of participants was 55 years, and 48% were women.
The findings of this study have several implications, the investigators said.
For example, the association that was observed between diabetes and deaths resulting from mental and neurologic disease requires further study, with investigation into the possible link between diabetes and onset of depression (especially in light of the association between diabetes and death resulting from intentional self-harm). The findings also reinforce the need for people with diabetes to seek appropriate cancer screenings.
"Future studies are warranted to investigate additional (and potentially more specific) risk factors that may link diabetes and chronic disease, to study non-Western populations, and to explain associations observed between very low glucose levels and vascular death in people without diabetes," they said, concluding that the findings of the study underscore the need for better understanding and prevention of the multisystem consequences of diabetes.
This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.
Diabetes is independently associated with premature death from numerous causes, including several nonvascular causes, according to findings from an analysis of individual-participant data from 97 prospective studies.
The risk of death from any cause was increased in 40,116 patients with diabetes, compared with 674,945 without diabetes (hazard ratio, 1.80), after adjustment for age, sex, smoking status, and body mass index. Similarly, the patients with diabetes also had increased risks of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and deaths of unknown or ill-defined causes (HR, 1.88), investigators reported in the March 3 issue of the New England Journal of Medicine.
Specific cancers that were found in this study to be moderately associated with premature death in diabetes patients vs. nondiabetes patients were liver, pancreas, ovary, colorectum, bladder, lung, and breast cancer (HRs, 2.16, 1.51, 1.45, 1.40, 1.40, 1.27 and 1.25, respectively), reported Dr. Sreenivasa Rao Kondapally Seshasai of the University of Cambridge (England) and colleagues from the Emerging Risk Factors Collaboration (ERFC).
"Other" causes of death in diabetes patients vs. nondiabetes patients included renal disease; liver disease; pneumonia and other infectious diseases; mental disorders; nonhepatic digestive diseases; external causes; intentional self-harm; nervous-system disorders; and chronic obstructive pulmonary disease, the investigators found (N. Engl. J. Med. 2011;364:829-41).
"These hazard ratios were not appreciably reduced after additional adjustment for systolic blood pressure, lipid levels, C-reactive protein levels, fibrinogen levels, alcohol use, estimated glomerular filtration rate, or indicators of socioeconomic status," the investigators said.
The hazard ratios were, however, reduced considerably after adjustment for fasting glucose or glycated hemoglobin levels, they noted.
Fasting glucose levels exceeding 100 mg/dL – but not levels of 70-100 mg/dL – were associated with excess risk of mortality.
In this study, middle-aged adults with diabetes but without known vascular disease at the time of enrollment generally died earlier than did those without diabetes.
"At 40, 50, and 60 years of age, men with diabetes but without a history of vascular disease would incur about 6.3, 5.8, and 4.5 years of life lost, respectively. The corresponding years of life lost for women with diabetes in middle age were 6.8, 6.4, and 5.4 years, respectively," the investigators wrote. They noted that about 58%, 9%, and 30% of the survival difference at 50 years between those with and without diabetes was attributable to excess vascular, cancer, and noncancer nonvascular deaths, respectively. The number of years of life lost because of diabetes was close to the 7-year reduction in life expectancy among long-term cigarette smokers.
About 40% of the years of life lost as a result of diabetes were attributable to nonvascular conditions, including about 10% attributable to cancer-related death, they said.
The finding of "generally continuous associations" between fasting glucose levels above 100 mg/dL and death suggests that hyperglycemia or a similar factor has direct relevance to the association between diabetes and premature death from these various causes – a finding that is also supported by the "substantial attenuation observed in hazard ratios for death from diabetes after adjustment for markers of glycemia," they added.
In contrast, other risk factors (such as blood pressure, adiposity, inflammation, insulin, and renal function) do not appear to be major mediators of the excess risk of death.
The ERFC is a collaboration that has previously published reports on the associations between lipids, lipoproteins, and inflammatory markers and the risk of vascular disease and cause-specific death. In 2009, the group extended its focus to include analyses of diabetes and other metabolic markers as they relate to incident vascular disease outcomes and cause-specific death. For the current study, the collaboration analyzed individual-participant data from prospective studies with information on diabetes diagnosis or fasting baseline blood-glucose levels. Studies included in the analysis did not select participants on the basis of having previous chronic disease; they did, however, record cause-specific death classified according to clearly defined criteria, and accrued more than 1 year of follow-up data.
The current analysis included 820,900 participants from those studies, of whom 123,205 died. The average age of participants was 55 years, and 48% were women.
The findings of this study have several implications, the investigators said.
For example, the association that was observed between diabetes and deaths resulting from mental and neurologic disease requires further study, with investigation into the possible link between diabetes and onset of depression (especially in light of the association between diabetes and death resulting from intentional self-harm). The findings also reinforce the need for people with diabetes to seek appropriate cancer screenings.
"Future studies are warranted to investigate additional (and potentially more specific) risk factors that may link diabetes and chronic disease, to study non-Western populations, and to explain associations observed between very low glucose levels and vascular death in people without diabetes," they said, concluding that the findings of the study underscore the need for better understanding and prevention of the multisystem consequences of diabetes.
This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.
Diabetes is independently associated with premature death from numerous causes, including several nonvascular causes, according to findings from an analysis of individual-participant data from 97 prospective studies.
The risk of death from any cause was increased in 40,116 patients with diabetes, compared with 674,945 without diabetes (hazard ratio, 1.80), after adjustment for age, sex, smoking status, and body mass index. Similarly, the patients with diabetes also had increased risks of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and deaths of unknown or ill-defined causes (HR, 1.88), investigators reported in the March 3 issue of the New England Journal of Medicine.
Specific cancers that were found in this study to be moderately associated with premature death in diabetes patients vs. nondiabetes patients were liver, pancreas, ovary, colorectum, bladder, lung, and breast cancer (HRs, 2.16, 1.51, 1.45, 1.40, 1.40, 1.27 and 1.25, respectively), reported Dr. Sreenivasa Rao Kondapally Seshasai of the University of Cambridge (England) and colleagues from the Emerging Risk Factors Collaboration (ERFC).
"Other" causes of death in diabetes patients vs. nondiabetes patients included renal disease; liver disease; pneumonia and other infectious diseases; mental disorders; nonhepatic digestive diseases; external causes; intentional self-harm; nervous-system disorders; and chronic obstructive pulmonary disease, the investigators found (N. Engl. J. Med. 2011;364:829-41).
"These hazard ratios were not appreciably reduced after additional adjustment for systolic blood pressure, lipid levels, C-reactive protein levels, fibrinogen levels, alcohol use, estimated glomerular filtration rate, or indicators of socioeconomic status," the investigators said.
The hazard ratios were, however, reduced considerably after adjustment for fasting glucose or glycated hemoglobin levels, they noted.
Fasting glucose levels exceeding 100 mg/dL – but not levels of 70-100 mg/dL – were associated with excess risk of mortality.
In this study, middle-aged adults with diabetes but without known vascular disease at the time of enrollment generally died earlier than did those without diabetes.
"At 40, 50, and 60 years of age, men with diabetes but without a history of vascular disease would incur about 6.3, 5.8, and 4.5 years of life lost, respectively. The corresponding years of life lost for women with diabetes in middle age were 6.8, 6.4, and 5.4 years, respectively," the investigators wrote. They noted that about 58%, 9%, and 30% of the survival difference at 50 years between those with and without diabetes was attributable to excess vascular, cancer, and noncancer nonvascular deaths, respectively. The number of years of life lost because of diabetes was close to the 7-year reduction in life expectancy among long-term cigarette smokers.
About 40% of the years of life lost as a result of diabetes were attributable to nonvascular conditions, including about 10% attributable to cancer-related death, they said.
The finding of "generally continuous associations" between fasting glucose levels above 100 mg/dL and death suggests that hyperglycemia or a similar factor has direct relevance to the association between diabetes and premature death from these various causes – a finding that is also supported by the "substantial attenuation observed in hazard ratios for death from diabetes after adjustment for markers of glycemia," they added.
In contrast, other risk factors (such as blood pressure, adiposity, inflammation, insulin, and renal function) do not appear to be major mediators of the excess risk of death.
The ERFC is a collaboration that has previously published reports on the associations between lipids, lipoproteins, and inflammatory markers and the risk of vascular disease and cause-specific death. In 2009, the group extended its focus to include analyses of diabetes and other metabolic markers as they relate to incident vascular disease outcomes and cause-specific death. For the current study, the collaboration analyzed individual-participant data from prospective studies with information on diabetes diagnosis or fasting baseline blood-glucose levels. Studies included in the analysis did not select participants on the basis of having previous chronic disease; they did, however, record cause-specific death classified according to clearly defined criteria, and accrued more than 1 year of follow-up data.
The current analysis included 820,900 participants from those studies, of whom 123,205 died. The average age of participants was 55 years, and 48% were women.
The findings of this study have several implications, the investigators said.
For example, the association that was observed between diabetes and deaths resulting from mental and neurologic disease requires further study, with investigation into the possible link between diabetes and onset of depression (especially in light of the association between diabetes and death resulting from intentional self-harm). The findings also reinforce the need for people with diabetes to seek appropriate cancer screenings.
"Future studies are warranted to investigate additional (and potentially more specific) risk factors that may link diabetes and chronic disease, to study non-Western populations, and to explain associations observed between very low glucose levels and vascular death in people without diabetes," they said, concluding that the findings of the study underscore the need for better understanding and prevention of the multisystem consequences of diabetes.
This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.
Major Finding: After adjustment for age, sex, smoking status, and body mass index, the risk of death from any cause was increased in patients with diabetes, compared with those without diabetes (HR, 1.80), as was the risk of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and unknown or ill-defined causes (HR, 1.88).
Data Source: An analysis of individual-participant data from 97 prospective studies.
Disclosures: This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.
Diabetes Linked With Risk of Premature Death
Diabetes is independently associated with premature death from numerous causes, including several nonvascular causes, according to findings from an analysis of individual-participant data from 97 prospective studies.
The risk of death from any cause was increased in 40,116 patients with diabetes, compared with 674,945 without diabetes (hazard ratio, 1.80), after adjustment for age, sex, smoking status, and body mass index. Similarly, the patients with diabetes also had increased risks of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and deaths of unknown or ill-defined causes (HR, 1.88), investigators reported in the March 3 issue of the New England Journal of Medicine.
Specific cancers that were found in this study to be moderately associated with premature death in diabetes patients vs. nondiabetes patients were liver, pancreas, ovary, colorectum, bladder, lung, and breast cancer (HRs, 2.16, 1.51, 1.45, 1.40, 1.40, 1.27 and 1.25, respectively), reported Dr. Sreenivasa Rao Kondapally Seshasai of the University of Cambridge (England) and colleagues from the Emerging Risk Factors Collaboration (ERFC).
"Other" causes of death in diabetes patients vs. nondiabetes patients included renal disease; liver disease; pneumonia and other infectious diseases; mental disorders; nonhepatic digestive diseases; external causes; intentional self-harm; nervous-system disorders; and chronic obstructive pulmonary disease, the investigators found (N. Engl. J. Med. 2011;364:829-41).
"These hazard ratios were not appreciably reduced after additional adjustment for systolic blood pressure, lipid levels, C-reactive protein levels, fibrinogen levels, alcohol use, estimated glomerular filtration rate, or indicators of socioeconomic status," the investigators said.
The hazard ratios were, however, reduced considerably after adjustment for fasting glucose or glycated hemoglobin levels, they noted.
Fasting glucose levels exceeding 100 mg/dL – but not levels of 70-100 mg/dL – were associated with excess risk of mortality.
In this study, middle-aged adults with diabetes but without known vascular disease at the time of enrollment generally died earlier than did those without diabetes.
"At 40, 50, and 60 years of age, men with diabetes but without a history of vascular disease would incur about 6.3, 5.8, and 4.5 years of life lost, respectively. The corresponding years of life lost for women with diabetes in middle age were 6.8, 6.4, and 5.4 years, respectively," the investigators wrote. They noted that about 58%, 9%, and 30% of the survival difference at 50 years between those with and without diabetes was attributable to excess vascular, cancer, and noncancer nonvascular deaths, respectively. The number of years of life lost because of diabetes was close to the 7-year reduction in life expectancy among long-term cigarette smokers.
About 40% of the years of life lost as a result of diabetes were attributable to nonvascular conditions, including about 10% attributable to cancer-related death, they said.
The finding of "generally continuous associations" between fasting glucose levels above 100 mg/dL and death suggests that hyperglycemia or a similar factor has direct relevance to the association between diabetes and premature death from these various causes – a finding that is also supported by the "substantial attenuation observed in hazard ratios for death from diabetes after adjustment for markers of glycemia," they added.
In contrast, other risk factors (such as blood pressure, adiposity, inflammation, insulin, and renal function) do not appear to be major mediators of the excess risk of death.
The ERFC is a collaboration that has previously published reports on the associations between lipids, lipoproteins, and inflammatory markers and the risk of vascular disease and cause-specific death. In 2009, the group extended its focus to include analyses of diabetes and other metabolic markers as they relate to incident vascular disease outcomes and cause-specific death. For the current study, the collaboration analyzed individual-participant data from prospective studies with information on diabetes diagnosis or fasting baseline blood-glucose levels. Studies included in the analysis did not select participants on the basis of having previous chronic disease; they did, however, record cause-specific death classified according to clearly defined criteria, and accrued more than 1 year of follow-up data.
The current analysis included 820,900 participants from those studies, of whom 123,205 died. The average age of participants was 55 years, and 48% were women.
The findings of this study have several implications, the investigators said.
For example, the association that was observed between diabetes and deaths resulting from mental and neurologic disease requires further study, with investigation into the possible link between diabetes and onset of depression (especially in light of the association between diabetes and death resulting from intentional self-harm). The findings also reinforce the need for people with diabetes to seek appropriate cancer screenings.
"Future studies are warranted to investigate additional (and potentially more specific) risk factors that may link diabetes and chronic disease, to study non-Western populations, and to explain associations observed between very low glucose levels and vascular death in people without diabetes," they said, concluding that the findings of the study underscore the need for better understanding and prevention of the multisystem consequences of diabetes.
This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.
Diabetes is independently associated with premature death from numerous causes, including several nonvascular causes, according to findings from an analysis of individual-participant data from 97 prospective studies.
The risk of death from any cause was increased in 40,116 patients with diabetes, compared with 674,945 without diabetes (hazard ratio, 1.80), after adjustment for age, sex, smoking status, and body mass index. Similarly, the patients with diabetes also had increased risks of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and deaths of unknown or ill-defined causes (HR, 1.88), investigators reported in the March 3 issue of the New England Journal of Medicine.
Specific cancers that were found in this study to be moderately associated with premature death in diabetes patients vs. nondiabetes patients were liver, pancreas, ovary, colorectum, bladder, lung, and breast cancer (HRs, 2.16, 1.51, 1.45, 1.40, 1.40, 1.27 and 1.25, respectively), reported Dr. Sreenivasa Rao Kondapally Seshasai of the University of Cambridge (England) and colleagues from the Emerging Risk Factors Collaboration (ERFC).
"Other" causes of death in diabetes patients vs. nondiabetes patients included renal disease; liver disease; pneumonia and other infectious diseases; mental disorders; nonhepatic digestive diseases; external causes; intentional self-harm; nervous-system disorders; and chronic obstructive pulmonary disease, the investigators found (N. Engl. J. Med. 2011;364:829-41).
"These hazard ratios were not appreciably reduced after additional adjustment for systolic blood pressure, lipid levels, C-reactive protein levels, fibrinogen levels, alcohol use, estimated glomerular filtration rate, or indicators of socioeconomic status," the investigators said.
The hazard ratios were, however, reduced considerably after adjustment for fasting glucose or glycated hemoglobin levels, they noted.
Fasting glucose levels exceeding 100 mg/dL – but not levels of 70-100 mg/dL – were associated with excess risk of mortality.
In this study, middle-aged adults with diabetes but without known vascular disease at the time of enrollment generally died earlier than did those without diabetes.
"At 40, 50, and 60 years of age, men with diabetes but without a history of vascular disease would incur about 6.3, 5.8, and 4.5 years of life lost, respectively. The corresponding years of life lost for women with diabetes in middle age were 6.8, 6.4, and 5.4 years, respectively," the investigators wrote. They noted that about 58%, 9%, and 30% of the survival difference at 50 years between those with and without diabetes was attributable to excess vascular, cancer, and noncancer nonvascular deaths, respectively. The number of years of life lost because of diabetes was close to the 7-year reduction in life expectancy among long-term cigarette smokers.
About 40% of the years of life lost as a result of diabetes were attributable to nonvascular conditions, including about 10% attributable to cancer-related death, they said.
The finding of "generally continuous associations" between fasting glucose levels above 100 mg/dL and death suggests that hyperglycemia or a similar factor has direct relevance to the association between diabetes and premature death from these various causes – a finding that is also supported by the "substantial attenuation observed in hazard ratios for death from diabetes after adjustment for markers of glycemia," they added.
In contrast, other risk factors (such as blood pressure, adiposity, inflammation, insulin, and renal function) do not appear to be major mediators of the excess risk of death.
The ERFC is a collaboration that has previously published reports on the associations between lipids, lipoproteins, and inflammatory markers and the risk of vascular disease and cause-specific death. In 2009, the group extended its focus to include analyses of diabetes and other metabolic markers as they relate to incident vascular disease outcomes and cause-specific death. For the current study, the collaboration analyzed individual-participant data from prospective studies with information on diabetes diagnosis or fasting baseline blood-glucose levels. Studies included in the analysis did not select participants on the basis of having previous chronic disease; they did, however, record cause-specific death classified according to clearly defined criteria, and accrued more than 1 year of follow-up data.
The current analysis included 820,900 participants from those studies, of whom 123,205 died. The average age of participants was 55 years, and 48% were women.
The findings of this study have several implications, the investigators said.
For example, the association that was observed between diabetes and deaths resulting from mental and neurologic disease requires further study, with investigation into the possible link between diabetes and onset of depression (especially in light of the association between diabetes and death resulting from intentional self-harm). The findings also reinforce the need for people with diabetes to seek appropriate cancer screenings.
"Future studies are warranted to investigate additional (and potentially more specific) risk factors that may link diabetes and chronic disease, to study non-Western populations, and to explain associations observed between very low glucose levels and vascular death in people without diabetes," they said, concluding that the findings of the study underscore the need for better understanding and prevention of the multisystem consequences of diabetes.
This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.
Diabetes is independently associated with premature death from numerous causes, including several nonvascular causes, according to findings from an analysis of individual-participant data from 97 prospective studies.
The risk of death from any cause was increased in 40,116 patients with diabetes, compared with 674,945 without diabetes (hazard ratio, 1.80), after adjustment for age, sex, smoking status, and body mass index. Similarly, the patients with diabetes also had increased risks of death from cancer (HR, 1.25), vascular causes (HR, 2.32), "other" nonvascular causes not attributed to cancer (HR, 1.73), and deaths of unknown or ill-defined causes (HR, 1.88), investigators reported in the March 3 issue of the New England Journal of Medicine.
Specific cancers that were found in this study to be moderately associated with premature death in diabetes patients vs. nondiabetes patients were liver, pancreas, ovary, colorectum, bladder, lung, and breast cancer (HRs, 2.16, 1.51, 1.45, 1.40, 1.40, 1.27 and 1.25, respectively), reported Dr. Sreenivasa Rao Kondapally Seshasai of the University of Cambridge (England) and colleagues from the Emerging Risk Factors Collaboration (ERFC).
"Other" causes of death in diabetes patients vs. nondiabetes patients included renal disease; liver disease; pneumonia and other infectious diseases; mental disorders; nonhepatic digestive diseases; external causes; intentional self-harm; nervous-system disorders; and chronic obstructive pulmonary disease, the investigators found (N. Engl. J. Med. 2011;364:829-41).
"These hazard ratios were not appreciably reduced after additional adjustment for systolic blood pressure, lipid levels, C-reactive protein levels, fibrinogen levels, alcohol use, estimated glomerular filtration rate, or indicators of socioeconomic status," the investigators said.
The hazard ratios were, however, reduced considerably after adjustment for fasting glucose or glycated hemoglobin levels, they noted.
Fasting glucose levels exceeding 100 mg/dL – but not levels of 70-100 mg/dL – were associated with excess risk of mortality.
In this study, middle-aged adults with diabetes but without known vascular disease at the time of enrollment generally died earlier than did those without diabetes.
"At 40, 50, and 60 years of age, men with diabetes but without a history of vascular disease would incur about 6.3, 5.8, and 4.5 years of life lost, respectively. The corresponding years of life lost for women with diabetes in middle age were 6.8, 6.4, and 5.4 years, respectively," the investigators wrote. They noted that about 58%, 9%, and 30% of the survival difference at 50 years between those with and without diabetes was attributable to excess vascular, cancer, and noncancer nonvascular deaths, respectively. The number of years of life lost because of diabetes was close to the 7-year reduction in life expectancy among long-term cigarette smokers.
About 40% of the years of life lost as a result of diabetes were attributable to nonvascular conditions, including about 10% attributable to cancer-related death, they said.
The finding of "generally continuous associations" between fasting glucose levels above 100 mg/dL and death suggests that hyperglycemia or a similar factor has direct relevance to the association between diabetes and premature death from these various causes – a finding that is also supported by the "substantial attenuation observed in hazard ratios for death from diabetes after adjustment for markers of glycemia," they added.
In contrast, other risk factors (such as blood pressure, adiposity, inflammation, insulin, and renal function) do not appear to be major mediators of the excess risk of death.
The ERFC is a collaboration that has previously published reports on the associations between lipids, lipoproteins, and inflammatory markers and the risk of vascular disease and cause-specific death. In 2009, the group extended its focus to include analyses of diabetes and other metabolic markers as they relate to incident vascular disease outcomes and cause-specific death. For the current study, the collaboration analyzed individual-participant data from prospective studies with information on diabetes diagnosis or fasting baseline blood-glucose levels. Studies included in the analysis did not select participants on the basis of having previous chronic disease; they did, however, record cause-specific death classified according to clearly defined criteria, and accrued more than 1 year of follow-up data.
The current analysis included 820,900 participants from those studies, of whom 123,205 died. The average age of participants was 55 years, and 48% were women.
The findings of this study have several implications, the investigators said.
For example, the association that was observed between diabetes and deaths resulting from mental and neurologic disease requires further study, with investigation into the possible link between diabetes and onset of depression (especially in light of the association between diabetes and death resulting from intentional self-harm). The findings also reinforce the need for people with diabetes to seek appropriate cancer screenings.
"Future studies are warranted to investigate additional (and potentially more specific) risk factors that may link diabetes and chronic disease, to study non-Western populations, and to explain associations observed between very low glucose levels and vascular death in people without diabetes," they said, concluding that the findings of the study underscore the need for better understanding and prevention of the multisystem consequences of diabetes.
This study was supported by grants from the British Heart Foundation, the U.K. Medical Research Council, Pfizer, the Gates Cambridge Trust Scholarship, an Overseas Research Studentship Award, and an Addenbrooke’s Charitable Trust Clinical Research Fellowship to the EFRC and/or individual EFRC members. Members’ specific disclosures are available with the full text of the EFRC article at NEJM.com.