User login
Dying Wish
Most Americans surveyed about their preferred place of death say they want to die at home.1 Nevertheless, many dying people are not able to realize this wish. One 2003 study found that nearly 90% of terminally ill cancer patients asked to choose where they would prefer to die cited their homes. Only one-third of those patients were able to make this desire a reality.2
The reasons behind the divergence between preference and actual place of death are complicated, says Rachelle Bernacki, MD, MS, assistant clinical professor, Geriatrics and Palliative Care, and a palliative care specialist with the University of California, San Francisco Medical Center Hospitalist Service. “I think most people envision … [dying] at home, but sometimes that’s just not feasible, for multiple reasons. When the reality sets in, there has to be a good plan in place at home—meaning, enough people and resources to keep that person at home.”
Is Death Imminent?
Dr. Bernacki points out that many studies on dying preferences are conducted when the patient is not ill or actively dying. The scenario becomes much more complex when patients are in crisis or on an end-of-life trajectory. In initial assessments, hospitalists should try not only to ascertain the patient’s health status but also to ask respectfully about their goals for care.
“It might not be appropriate [to ask] every patient, ‘Where do you want to die?’ ” suggests Dr. Bernacki. It can be appropriate, though, to ask patients about their experiences with their current illness and to talk about some of the goals they hope to achieve in the next week or month.
Although it is not possible to predict exactly how long a person will survive, the signs of critical illness can provide an appropriate window in which the physician can ask a patient, “If you were to die, where would you want to be, and what is most important to you?”
—Rachelle Bernacki, MD, MS, assistant clinical professor, Geriatrics and Palliative Care, UCSF Medical Center Hospitalist Service
Practitioners skilled in end-of-life care cite several attributes characteristic of patients who are actively dying, such as:
- Refusal of food and liquids;
- Decreased level of awareness;
- Dyspnea (shortness of breath), including erratic breathing patterns;
- Mottled skin that is colder to the touch, along with blue toes; and
- Abnormal breathing sounds due to secretions in the lungs.
Honor Their Choices
Researchers cite many factors that determine whether a terminally ill cancer patient dies in the home or in an institution, including gender, race, marital status, income level, and available health system resources. In a Yale (New Haven, Conn.) epidemiological study, men, unmarried people, and those living in low-income areas were at higher risk for institutionalized deaths.3
Dr. Bernacki has found that the two most important determinants of whether a patient will go home to die are the patient’s condition and their resources at home. Sometimes transporting a patient is not practical because the patient may be so close to dying that there is a risk of death en route. Or the patient’s symptoms may not be controlled with oral pain medications and may require frequent IV dosing, in which case discharge is not feasible. Barriers at the home site include the lack of an identified primary caregiver and the unavailability of qualified hospice personnel and/or medical supplies.
For in-depth learning about palliative care topics, be sure to visit these sessions at the upcoming SHM Annual Meeting in Dallas, May 23-25:
- Palliative Pain Management: Thurs., May 24, 10:35-11:50;
- Non-Pain Symptom Management: Thurs., May 24, 1:10-2:25;
- Ethical and Legal Considerations of Palliative Care and End-of-Life Care: Thurs., May 24, 2:45-4:00;
- Prognostication and PC Management of the Non-Cancer Diagnosis: Fri., May 25, 10:15-11:35; and
- Communication Skills and How to Conduct Family/Care Conferences: Fri., May 25, 1:35-2:55.
When the Hospital Is Preferred
In some situations, says Dr. Bernacki, “some family members feel very uncomfortable with the thought of their loved one dying at home.” Sometimes the disease process advances so quickly that the palliative care team cannot titrate the pain medicines to the right amount to allow discharge. Family members can become alarmed and may feel ill-prepared to handle difficult symptoms of the dying patient, such as uncontrolled nausea or dyspnea.
“So we have to just make an educated guess as to how long we think they have and how important it is to that patient or that family to be at home.” Often, the care team and family realize that it makes more sense not to move the patient but rather to try and make everything as comfortable as possible in the hospital.
The UCSF Palliative Care Service team, established by Steve Pantilat, MD, associate professor of clinical medicine, Department of Medicine, University of California, San Francisco, has access to two in-hospital comfort care suites, where family members can stay with their loved ones at all times.4 Dr. Pantilat is also the past-president of SHM and the Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at UCSF.
In all cases, says Dr. Bernacki, hospitalists dealing with dying patients should remain cognizant that they are treating not only the patients but the family members as well. “Part of palliative care is making sure that the daughters, sons, and spouses are all well cared for,” she emphasizes. Ascertaining goals and negotiating what’s possible are the keys to good palliative care. TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Tang ST, McCorkle R, Bradley EH. Determinants of death in an inpatient hospice for terminally ill cancer patients. Palliat Support Care. 2004 Dec;2(4):361-370.
- Tang ST, McCorkle R. Determinants of congruence between the preferred and actual place of death for terminally ill cancer patients. J Palliat Care. 2003;19:230-237.
- Gallo WT, Baker MJ, Bradley EH. Factors associated with home versus institutional death among cancer patients in Connecticut. J Am Geriatr Soc. 2001 Jun;49(6):771-777. Comment in J Am Geriatr Soc. 2001 Jun; 49(6):831-832.
- Auerbach AD, Pantilat SZ. End-of-life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
Most Americans surveyed about their preferred place of death say they want to die at home.1 Nevertheless, many dying people are not able to realize this wish. One 2003 study found that nearly 90% of terminally ill cancer patients asked to choose where they would prefer to die cited their homes. Only one-third of those patients were able to make this desire a reality.2
The reasons behind the divergence between preference and actual place of death are complicated, says Rachelle Bernacki, MD, MS, assistant clinical professor, Geriatrics and Palliative Care, and a palliative care specialist with the University of California, San Francisco Medical Center Hospitalist Service. “I think most people envision … [dying] at home, but sometimes that’s just not feasible, for multiple reasons. When the reality sets in, there has to be a good plan in place at home—meaning, enough people and resources to keep that person at home.”
Is Death Imminent?
Dr. Bernacki points out that many studies on dying preferences are conducted when the patient is not ill or actively dying. The scenario becomes much more complex when patients are in crisis or on an end-of-life trajectory. In initial assessments, hospitalists should try not only to ascertain the patient’s health status but also to ask respectfully about their goals for care.
“It might not be appropriate [to ask] every patient, ‘Where do you want to die?’ ” suggests Dr. Bernacki. It can be appropriate, though, to ask patients about their experiences with their current illness and to talk about some of the goals they hope to achieve in the next week or month.
Although it is not possible to predict exactly how long a person will survive, the signs of critical illness can provide an appropriate window in which the physician can ask a patient, “If you were to die, where would you want to be, and what is most important to you?”
—Rachelle Bernacki, MD, MS, assistant clinical professor, Geriatrics and Palliative Care, UCSF Medical Center Hospitalist Service
Practitioners skilled in end-of-life care cite several attributes characteristic of patients who are actively dying, such as:
- Refusal of food and liquids;
- Decreased level of awareness;
- Dyspnea (shortness of breath), including erratic breathing patterns;
- Mottled skin that is colder to the touch, along with blue toes; and
- Abnormal breathing sounds due to secretions in the lungs.
Honor Their Choices
Researchers cite many factors that determine whether a terminally ill cancer patient dies in the home or in an institution, including gender, race, marital status, income level, and available health system resources. In a Yale (New Haven, Conn.) epidemiological study, men, unmarried people, and those living in low-income areas were at higher risk for institutionalized deaths.3
Dr. Bernacki has found that the two most important determinants of whether a patient will go home to die are the patient’s condition and their resources at home. Sometimes transporting a patient is not practical because the patient may be so close to dying that there is a risk of death en route. Or the patient’s symptoms may not be controlled with oral pain medications and may require frequent IV dosing, in which case discharge is not feasible. Barriers at the home site include the lack of an identified primary caregiver and the unavailability of qualified hospice personnel and/or medical supplies.
For in-depth learning about palliative care topics, be sure to visit these sessions at the upcoming SHM Annual Meeting in Dallas, May 23-25:
- Palliative Pain Management: Thurs., May 24, 10:35-11:50;
- Non-Pain Symptom Management: Thurs., May 24, 1:10-2:25;
- Ethical and Legal Considerations of Palliative Care and End-of-Life Care: Thurs., May 24, 2:45-4:00;
- Prognostication and PC Management of the Non-Cancer Diagnosis: Fri., May 25, 10:15-11:35; and
- Communication Skills and How to Conduct Family/Care Conferences: Fri., May 25, 1:35-2:55.
When the Hospital Is Preferred
In some situations, says Dr. Bernacki, “some family members feel very uncomfortable with the thought of their loved one dying at home.” Sometimes the disease process advances so quickly that the palliative care team cannot titrate the pain medicines to the right amount to allow discharge. Family members can become alarmed and may feel ill-prepared to handle difficult symptoms of the dying patient, such as uncontrolled nausea or dyspnea.
“So we have to just make an educated guess as to how long we think they have and how important it is to that patient or that family to be at home.” Often, the care team and family realize that it makes more sense not to move the patient but rather to try and make everything as comfortable as possible in the hospital.
The UCSF Palliative Care Service team, established by Steve Pantilat, MD, associate professor of clinical medicine, Department of Medicine, University of California, San Francisco, has access to two in-hospital comfort care suites, where family members can stay with their loved ones at all times.4 Dr. Pantilat is also the past-president of SHM and the Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at UCSF.
In all cases, says Dr. Bernacki, hospitalists dealing with dying patients should remain cognizant that they are treating not only the patients but the family members as well. “Part of palliative care is making sure that the daughters, sons, and spouses are all well cared for,” she emphasizes. Ascertaining goals and negotiating what’s possible are the keys to good palliative care. TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Tang ST, McCorkle R, Bradley EH. Determinants of death in an inpatient hospice for terminally ill cancer patients. Palliat Support Care. 2004 Dec;2(4):361-370.
- Tang ST, McCorkle R. Determinants of congruence between the preferred and actual place of death for terminally ill cancer patients. J Palliat Care. 2003;19:230-237.
- Gallo WT, Baker MJ, Bradley EH. Factors associated with home versus institutional death among cancer patients in Connecticut. J Am Geriatr Soc. 2001 Jun;49(6):771-777. Comment in J Am Geriatr Soc. 2001 Jun; 49(6):831-832.
- Auerbach AD, Pantilat SZ. End-of-life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
Most Americans surveyed about their preferred place of death say they want to die at home.1 Nevertheless, many dying people are not able to realize this wish. One 2003 study found that nearly 90% of terminally ill cancer patients asked to choose where they would prefer to die cited their homes. Only one-third of those patients were able to make this desire a reality.2
The reasons behind the divergence between preference and actual place of death are complicated, says Rachelle Bernacki, MD, MS, assistant clinical professor, Geriatrics and Palliative Care, and a palliative care specialist with the University of California, San Francisco Medical Center Hospitalist Service. “I think most people envision … [dying] at home, but sometimes that’s just not feasible, for multiple reasons. When the reality sets in, there has to be a good plan in place at home—meaning, enough people and resources to keep that person at home.”
Is Death Imminent?
Dr. Bernacki points out that many studies on dying preferences are conducted when the patient is not ill or actively dying. The scenario becomes much more complex when patients are in crisis or on an end-of-life trajectory. In initial assessments, hospitalists should try not only to ascertain the patient’s health status but also to ask respectfully about their goals for care.
“It might not be appropriate [to ask] every patient, ‘Where do you want to die?’ ” suggests Dr. Bernacki. It can be appropriate, though, to ask patients about their experiences with their current illness and to talk about some of the goals they hope to achieve in the next week or month.
Although it is not possible to predict exactly how long a person will survive, the signs of critical illness can provide an appropriate window in which the physician can ask a patient, “If you were to die, where would you want to be, and what is most important to you?”
—Rachelle Bernacki, MD, MS, assistant clinical professor, Geriatrics and Palliative Care, UCSF Medical Center Hospitalist Service
Practitioners skilled in end-of-life care cite several attributes characteristic of patients who are actively dying, such as:
- Refusal of food and liquids;
- Decreased level of awareness;
- Dyspnea (shortness of breath), including erratic breathing patterns;
- Mottled skin that is colder to the touch, along with blue toes; and
- Abnormal breathing sounds due to secretions in the lungs.
Honor Their Choices
Researchers cite many factors that determine whether a terminally ill cancer patient dies in the home or in an institution, including gender, race, marital status, income level, and available health system resources. In a Yale (New Haven, Conn.) epidemiological study, men, unmarried people, and those living in low-income areas were at higher risk for institutionalized deaths.3
Dr. Bernacki has found that the two most important determinants of whether a patient will go home to die are the patient’s condition and their resources at home. Sometimes transporting a patient is not practical because the patient may be so close to dying that there is a risk of death en route. Or the patient’s symptoms may not be controlled with oral pain medications and may require frequent IV dosing, in which case discharge is not feasible. Barriers at the home site include the lack of an identified primary caregiver and the unavailability of qualified hospice personnel and/or medical supplies.
For in-depth learning about palliative care topics, be sure to visit these sessions at the upcoming SHM Annual Meeting in Dallas, May 23-25:
- Palliative Pain Management: Thurs., May 24, 10:35-11:50;
- Non-Pain Symptom Management: Thurs., May 24, 1:10-2:25;
- Ethical and Legal Considerations of Palliative Care and End-of-Life Care: Thurs., May 24, 2:45-4:00;
- Prognostication and PC Management of the Non-Cancer Diagnosis: Fri., May 25, 10:15-11:35; and
- Communication Skills and How to Conduct Family/Care Conferences: Fri., May 25, 1:35-2:55.
When the Hospital Is Preferred
In some situations, says Dr. Bernacki, “some family members feel very uncomfortable with the thought of their loved one dying at home.” Sometimes the disease process advances so quickly that the palliative care team cannot titrate the pain medicines to the right amount to allow discharge. Family members can become alarmed and may feel ill-prepared to handle difficult symptoms of the dying patient, such as uncontrolled nausea or dyspnea.
“So we have to just make an educated guess as to how long we think they have and how important it is to that patient or that family to be at home.” Often, the care team and family realize that it makes more sense not to move the patient but rather to try and make everything as comfortable as possible in the hospital.
The UCSF Palliative Care Service team, established by Steve Pantilat, MD, associate professor of clinical medicine, Department of Medicine, University of California, San Francisco, has access to two in-hospital comfort care suites, where family members can stay with their loved ones at all times.4 Dr. Pantilat is also the past-president of SHM and the Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at UCSF.
In all cases, says Dr. Bernacki, hospitalists dealing with dying patients should remain cognizant that they are treating not only the patients but the family members as well. “Part of palliative care is making sure that the daughters, sons, and spouses are all well cared for,” she emphasizes. Ascertaining goals and negotiating what’s possible are the keys to good palliative care. TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Tang ST, McCorkle R, Bradley EH. Determinants of death in an inpatient hospice for terminally ill cancer patients. Palliat Support Care. 2004 Dec;2(4):361-370.
- Tang ST, McCorkle R. Determinants of congruence between the preferred and actual place of death for terminally ill cancer patients. J Palliat Care. 2003;19:230-237.
- Gallo WT, Baker MJ, Bradley EH. Factors associated with home versus institutional death among cancer patients in Connecticut. J Am Geriatr Soc. 2001 Jun;49(6):771-777. Comment in J Am Geriatr Soc. 2001 Jun; 49(6):831-832.
- Auerbach AD, Pantilat SZ. End-of-life care in a voluntary hospitalist model: effects on communication, processes of care, and patient symptoms. Am J Med. 2004 May 15;116(10):669-675.
Palliative Care Patience
As hospital-based palliative care programs continue to grow, palliative care specialists are eager to dispel misconceptions about their work.1 Quality palliative care management at the end of life is often mistakenly perceived as synonymous with adequate pain control, but controlling pain is just one of the facets of effectively moderating the intensity of patients’ and families’ suffering.
The cases narrated here illustrate some of the other common themes of good palliative care management at the end of life: aggressive symptom management, interdisciplinary teamwork, and attention to patients’ and families’ spiritual concerns. Active, respectful listening can help to identify and alleviate obstacles to a more humane end-of-life journey.
Time to Process the Big Picture
State-of-the-art medical therapy does not always address dying patients’ suffering, says Melissa Mahoney, MD, assistant professor of medicine at Emory University and co-director of the Palliative Care Consult Service at Emory Crawford Long Hospital in Atlanta. She experienced this firsthand with a request to consult with a 60-year-old woman who had been in and out of sub-acute rehabilitation facilities seeking pain relief for her spinal stenosis. During a recent rehab facility stay, she had become septic and was transferred to the hospital for dialysis and other treatments. When Dr. Mahoney met the patient, the woman had been saying that she wanted to die, and her family was supportive of her wishes.
During her first conversation with the patient, however, Dr. Mahoney was able to discern that when she said she wanted to die, the patient meant, “I’m in so much pain that I don’t want to live this way.” The first step for the palliative care team was to begin patient-controlled analgesia (PCA) with IV hydromorphone hydrochloride in an attempt to control her pain. The PCA worked—dramatically.
“The next day,” recalls Dr. Mahoney, “she was like a new person. She was able to cope with the idea of dialysis and was able to talk with her family and put things in perspective.”
The palliative care team followed the woman for months, as she continued a cycle of readmissions to both the sub-acute facility and the hospital. The difference from the previous scenario, however, was that the team could offer aggressive symptom management while encouraging the patient and her family to revisit quality of life issues. She eventually died in the hospital, but Dr. Mahoney believes that the palliative care team’s interventions and emphasis on communication helped the patient and her family to cope with the situation more effectively.
With pain under control, patients can begin to address such questions as What’s important to me now? How do I want to spend my days? Who would I want to speak for me if I can’t speak for myself? What are my end-of-life wishes?’
“None of those higher-level discussions can take place until someone can physically handle them,” emphasizes Dr. Mahoney. “The palliative care approach puts the focus back on the patient and on the family and away from the disease. It seeks to treat the person and hopefully ease suffering through the illness.”
Goals of Care Change with Time
Howard R. Epstein, MD, medical director, Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and a member of the SHM Palliative Care Task Force, notes that good palliative care incorporates ongoing discussions about patients’ and families’ goals of care. “Following diagnosis of a life-threatening illness, the initial goal might be ‘I want to be cured,’ ” he says. “But, if the disease progresses, then you need to have another discussion about goals of care. Hopefully, this is part of the process all along.”
Dr. Epstein participated in a particularly memorable case last fall, consulting with a patient who had metastatic renal cancer. Surgery had left him with an abdominal abscess, which surgeons were proposing to address with another procedure in order to prevent a potentially fatal infection. The palliative care team was called in to help Mr. A, who was only 50, decide on a care plan. During the care conference, says Dr. Epstein, Mr. A was alert and joking with his wife and indicated that he would rather go home with hospice care than undergo another surgery.
The team asked Mr. A about his goals. “He didn’t know how much time he had left,” recalls Dr. Epstein, “although he had a specific goal in mind: One of his four sons was getting married, and he wanted to be there for that. They were a very close-knit family.” Mr. A had been intensely engaged as a father all through his sons’ school years. They ranged in age from 19 to 30, and Mr. A was determined to remain close with them throughout his dying process.
The care team facilitated his return home with a PCA pump for pain and a link with a visiting hospice nurse and social worker. The case was followed by a reporter from the St. Paul Pioneer Press, and it was in those articles that Dr. Epstein learned more of Mr. A’s story. For instance, extended family members were pitching in to remodel the house; Mrs. A would have to sell it to cover her husband’s medical bills after he died. The engaged son later had to tell his father that his fiancée had canceled the wedding. Mr. A was able to allay his son’s guilt and fear about the canceled wedding and to be the kind of supportive father he had always been.
Because his goal of living until the wedding had changed, Mr. A was then able to focus on his other goal: having family with him as he died at home. And, indeed, Mr. A died a peaceful death a few weeks later surrounded by his whole family.
A Ship without a Captain
Pediatric hospitalists who handle palliative care recognize that, unlike adults’ end-of-life trajectories, which are usually a straight line, the trajectories of children with complex medical conditions tend to be more erratic between diagnosis and cure or death. As a result, their families spend a longer time relating to the medical system. The job of the palliative care team is to acknowledge the family’s experience and reframe that experience into a more egalitarian and satisfying one, including a comprehensive plan of care, says Margaret Hood, MD, senior pediatric hospitalist at MultiCare’s Mary Bridge Children’s Hospital in Tacoma, Wash. Thus, the interdisciplinary team at Mary Bridge meets with the family around a round table, where everyone’s input is given equal respect and weight.
Dr. Hood recalls one case that was brought to her attention by a social worker. Amy (not her real name) had been born prematurely and had endured many medical problems in her first four years. Then, at age four, she started walking and talking; by age seven, she was reading at the fifth grade level. From ages seven to 10, Amy had minor problems, but she began deteriorating at age 10, when it was found that she had mitochondrial disease. The family had taken her to many specialists without any resolution to her problem and had been charging medical treatments to their credit cards. The social worker was concerned that the family would be devastated by bankruptcy.
The palliative care team organized a care conference attended by Amy’s primary care physician, palliative care team members, and other specialists. Although the care conference resulted in small adjustments to her care plan—a change in medication and the addition of one diagnostic test—the true change came when Amy’s mother turned to Dr. Hood and said, “You know, I thought you’d given up on us.”
That’s when it occurred to Dr. Hood that families like these, visiting specialist after specialist for their child’s complex medical conditions, are “on ‘a ship without a captain.’ Whether or not their children have life-limiting illnesses, they need a captain of the ship to help them navigate their journey,” she says.
Amy’s mother had been under the impression that the physicians were telling her there was nothing else to hope for. “You don’t give up hope,” asserts Dr. Hood. “You just change what you’re hoping for.”
Amy died three months after the palliative care conference, but took a Make-A-Wish Foundation trip to Disneyland and celebrated Christmas at home with her family. Her last wish, after Christmas, was to avoid re-entering the hospital, and this was honored as well.
There May Be More Time to Live
Attention to nuances embedded in patients’ stated wishes can sometimes result in a reversal of expectations about end of life. Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, was called by the hospitalist service last year to help facilitate transfer of a patient to hospice care.
In her 70s, the active woman had come to the hospital because a tumor mass was eroding through her breast tissue. The woman was avoiding treatment, including a biopsy, and appeared to be resolved to her fate. Based on her conversation with the emergency department (ED) attending, hospice was discussed and recommended; the patient was admitted primarily for IV antibiotics and care of her wound. In discussing goals of care with the patient, however, Dr. Grossman was able to elicit her reasons for refusing treatment. Ten years earlier, the patient had watched her daughter suffer with aggressive chemotherapy and radiation for her breast cancer. She told Dr. Grossman, “I’ve lived my life; I don’t want to go through all that.”
Knowing that breast cancer treatments have evolved in the past decade, Dr. Grossman asked the woman whether she would agree to a consultation with an oncologist to find out about less toxic treatment, including hormonal therapy. Subsequently, the patient decided to undergo a lumpectomy to increase her options. Dr. Grossman also prescribed a mild pain reliever for the woman, who had expressed fears about becoming addicted to pain medication (a common misperception in elderly patients). Upon discharge, the patient was feeling better physically, and she was optimistic about her future.
Despite the perceptions of the ED staff, the patient had not been hospice-appropriate. “No one had ever offered her the alternatives. In her mind, she saw chemotherapy as this terrible thing, and she just didn’t want to have that,” says Dr. Grossman. “So by listening to her we found out why she didn’t want chemotherapy, and we were able to encourage her to talk with the oncologist and the surgeon.”
I’m Afraid of What Comes after This Life
“Sometimes you find that patients and families are making decisions purely in a spiritual context,” notes Dr. Mahoney. “Until you know that, you can deliver clear and concise medical information and opinions and they won’t hear it. They may respect your opinion, but they will not take that into consideration when they’re making the decisions about themselves or a loved one because their spiritual belief system supersedes that factual information.”
Last year, Dr. Mahoney encountered a woman her late 50s with metastatic cancer. Her mother had died young of the same disease. The patient knew her disease was advanced and that she was facing the same thing her mother had faced. She, too, was leaving behind her daughters.
The patient, recalls Dr. Mahoney, had not filled out an advance directive and was having a difficult time talking with her family about her situation. It is Dr. Mahoney’s practice in such settings to ask people about their hopes and their fears, “because you can really gauge how someone sees their illness by asking those questions.”
The woman responded that she was very afraid of dying. “When I hear that answer, my next question is, ‘What do you fear? Do you fear that you might suffer?’ She said, ‘Oh no, no, I’m not afraid of that at all. Actually, I’ve sinned a lot in my life, and I’m afraid of what comes after this life.’ ”
Realizing that the woman was suffering spiritually, Dr. Mahoney called in her team’s chaplain to meet with the patient. During that meeting, the patient revealed to Chaplain Sandra Schaap that she had been the one to remove her mother from life support (her mother had not left an advance directive either). She was plagued by the fear of how she would be judged for that act. The chaplain was able to offer some comfort by sharing a benediction, which stated (among other things) that Christ would complete what we have left undone in this life.
“That conversation helped the patient see that she needed to complete her own advance directive so that her daughters wouldn’t go through the same thing that she had with her own mother,” says Dr. Mahoney.
Although Dr. Mahoney did not see the woman again, “I think we certainly set the framework for her and her family to be able to cope with what was coming. In the traditional medical model of disease treatment, I’m not sure that kind of detail would have come out. This woman would have left the hospital still carrying around that burden and [would have] had a very different life from that point,” she says.
Conclusion
“Every patient and family has a story of their illness and how it has impacted their lives,” Dr. Mahoney emphasizes. “Many times people are in the hospital for an acute problem, but they’ve suffered with an illness for years. There is a real opportunity to allow patients and families to tell their stories. People are often relieved when someone listens and can help put things in perspective. Palliative care specialists, by actively listening to patient and family concerns, can help relieve suffering on a physical, spiritual, and emotional level even when cure is not possible.” TH
In this issue Gretchen Henkel also writes about hospitalists who are overcommitted.
Reference
- Center to Advance Palliative Care. The case for hospital-based palliative care. Available at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Accessed on February 20, 2007.
As hospital-based palliative care programs continue to grow, palliative care specialists are eager to dispel misconceptions about their work.1 Quality palliative care management at the end of life is often mistakenly perceived as synonymous with adequate pain control, but controlling pain is just one of the facets of effectively moderating the intensity of patients’ and families’ suffering.
The cases narrated here illustrate some of the other common themes of good palliative care management at the end of life: aggressive symptom management, interdisciplinary teamwork, and attention to patients’ and families’ spiritual concerns. Active, respectful listening can help to identify and alleviate obstacles to a more humane end-of-life journey.
Time to Process the Big Picture
State-of-the-art medical therapy does not always address dying patients’ suffering, says Melissa Mahoney, MD, assistant professor of medicine at Emory University and co-director of the Palliative Care Consult Service at Emory Crawford Long Hospital in Atlanta. She experienced this firsthand with a request to consult with a 60-year-old woman who had been in and out of sub-acute rehabilitation facilities seeking pain relief for her spinal stenosis. During a recent rehab facility stay, she had become septic and was transferred to the hospital for dialysis and other treatments. When Dr. Mahoney met the patient, the woman had been saying that she wanted to die, and her family was supportive of her wishes.
During her first conversation with the patient, however, Dr. Mahoney was able to discern that when she said she wanted to die, the patient meant, “I’m in so much pain that I don’t want to live this way.” The first step for the palliative care team was to begin patient-controlled analgesia (PCA) with IV hydromorphone hydrochloride in an attempt to control her pain. The PCA worked—dramatically.
“The next day,” recalls Dr. Mahoney, “she was like a new person. She was able to cope with the idea of dialysis and was able to talk with her family and put things in perspective.”
The palliative care team followed the woman for months, as she continued a cycle of readmissions to both the sub-acute facility and the hospital. The difference from the previous scenario, however, was that the team could offer aggressive symptom management while encouraging the patient and her family to revisit quality of life issues. She eventually died in the hospital, but Dr. Mahoney believes that the palliative care team’s interventions and emphasis on communication helped the patient and her family to cope with the situation more effectively.
With pain under control, patients can begin to address such questions as What’s important to me now? How do I want to spend my days? Who would I want to speak for me if I can’t speak for myself? What are my end-of-life wishes?’
“None of those higher-level discussions can take place until someone can physically handle them,” emphasizes Dr. Mahoney. “The palliative care approach puts the focus back on the patient and on the family and away from the disease. It seeks to treat the person and hopefully ease suffering through the illness.”
Goals of Care Change with Time
Howard R. Epstein, MD, medical director, Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and a member of the SHM Palliative Care Task Force, notes that good palliative care incorporates ongoing discussions about patients’ and families’ goals of care. “Following diagnosis of a life-threatening illness, the initial goal might be ‘I want to be cured,’ ” he says. “But, if the disease progresses, then you need to have another discussion about goals of care. Hopefully, this is part of the process all along.”
Dr. Epstein participated in a particularly memorable case last fall, consulting with a patient who had metastatic renal cancer. Surgery had left him with an abdominal abscess, which surgeons were proposing to address with another procedure in order to prevent a potentially fatal infection. The palliative care team was called in to help Mr. A, who was only 50, decide on a care plan. During the care conference, says Dr. Epstein, Mr. A was alert and joking with his wife and indicated that he would rather go home with hospice care than undergo another surgery.
The team asked Mr. A about his goals. “He didn’t know how much time he had left,” recalls Dr. Epstein, “although he had a specific goal in mind: One of his four sons was getting married, and he wanted to be there for that. They were a very close-knit family.” Mr. A had been intensely engaged as a father all through his sons’ school years. They ranged in age from 19 to 30, and Mr. A was determined to remain close with them throughout his dying process.
The care team facilitated his return home with a PCA pump for pain and a link with a visiting hospice nurse and social worker. The case was followed by a reporter from the St. Paul Pioneer Press, and it was in those articles that Dr. Epstein learned more of Mr. A’s story. For instance, extended family members were pitching in to remodel the house; Mrs. A would have to sell it to cover her husband’s medical bills after he died. The engaged son later had to tell his father that his fiancée had canceled the wedding. Mr. A was able to allay his son’s guilt and fear about the canceled wedding and to be the kind of supportive father he had always been.
Because his goal of living until the wedding had changed, Mr. A was then able to focus on his other goal: having family with him as he died at home. And, indeed, Mr. A died a peaceful death a few weeks later surrounded by his whole family.
A Ship without a Captain
Pediatric hospitalists who handle palliative care recognize that, unlike adults’ end-of-life trajectories, which are usually a straight line, the trajectories of children with complex medical conditions tend to be more erratic between diagnosis and cure or death. As a result, their families spend a longer time relating to the medical system. The job of the palliative care team is to acknowledge the family’s experience and reframe that experience into a more egalitarian and satisfying one, including a comprehensive plan of care, says Margaret Hood, MD, senior pediatric hospitalist at MultiCare’s Mary Bridge Children’s Hospital in Tacoma, Wash. Thus, the interdisciplinary team at Mary Bridge meets with the family around a round table, where everyone’s input is given equal respect and weight.
Dr. Hood recalls one case that was brought to her attention by a social worker. Amy (not her real name) had been born prematurely and had endured many medical problems in her first four years. Then, at age four, she started walking and talking; by age seven, she was reading at the fifth grade level. From ages seven to 10, Amy had minor problems, but she began deteriorating at age 10, when it was found that she had mitochondrial disease. The family had taken her to many specialists without any resolution to her problem and had been charging medical treatments to their credit cards. The social worker was concerned that the family would be devastated by bankruptcy.
The palliative care team organized a care conference attended by Amy’s primary care physician, palliative care team members, and other specialists. Although the care conference resulted in small adjustments to her care plan—a change in medication and the addition of one diagnostic test—the true change came when Amy’s mother turned to Dr. Hood and said, “You know, I thought you’d given up on us.”
That’s when it occurred to Dr. Hood that families like these, visiting specialist after specialist for their child’s complex medical conditions, are “on ‘a ship without a captain.’ Whether or not their children have life-limiting illnesses, they need a captain of the ship to help them navigate their journey,” she says.
Amy’s mother had been under the impression that the physicians were telling her there was nothing else to hope for. “You don’t give up hope,” asserts Dr. Hood. “You just change what you’re hoping for.”
Amy died three months after the palliative care conference, but took a Make-A-Wish Foundation trip to Disneyland and celebrated Christmas at home with her family. Her last wish, after Christmas, was to avoid re-entering the hospital, and this was honored as well.
There May Be More Time to Live
Attention to nuances embedded in patients’ stated wishes can sometimes result in a reversal of expectations about end of life. Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, was called by the hospitalist service last year to help facilitate transfer of a patient to hospice care.
In her 70s, the active woman had come to the hospital because a tumor mass was eroding through her breast tissue. The woman was avoiding treatment, including a biopsy, and appeared to be resolved to her fate. Based on her conversation with the emergency department (ED) attending, hospice was discussed and recommended; the patient was admitted primarily for IV antibiotics and care of her wound. In discussing goals of care with the patient, however, Dr. Grossman was able to elicit her reasons for refusing treatment. Ten years earlier, the patient had watched her daughter suffer with aggressive chemotherapy and radiation for her breast cancer. She told Dr. Grossman, “I’ve lived my life; I don’t want to go through all that.”
Knowing that breast cancer treatments have evolved in the past decade, Dr. Grossman asked the woman whether she would agree to a consultation with an oncologist to find out about less toxic treatment, including hormonal therapy. Subsequently, the patient decided to undergo a lumpectomy to increase her options. Dr. Grossman also prescribed a mild pain reliever for the woman, who had expressed fears about becoming addicted to pain medication (a common misperception in elderly patients). Upon discharge, the patient was feeling better physically, and she was optimistic about her future.
Despite the perceptions of the ED staff, the patient had not been hospice-appropriate. “No one had ever offered her the alternatives. In her mind, she saw chemotherapy as this terrible thing, and she just didn’t want to have that,” says Dr. Grossman. “So by listening to her we found out why she didn’t want chemotherapy, and we were able to encourage her to talk with the oncologist and the surgeon.”
I’m Afraid of What Comes after This Life
“Sometimes you find that patients and families are making decisions purely in a spiritual context,” notes Dr. Mahoney. “Until you know that, you can deliver clear and concise medical information and opinions and they won’t hear it. They may respect your opinion, but they will not take that into consideration when they’re making the decisions about themselves or a loved one because their spiritual belief system supersedes that factual information.”
Last year, Dr. Mahoney encountered a woman her late 50s with metastatic cancer. Her mother had died young of the same disease. The patient knew her disease was advanced and that she was facing the same thing her mother had faced. She, too, was leaving behind her daughters.
The patient, recalls Dr. Mahoney, had not filled out an advance directive and was having a difficult time talking with her family about her situation. It is Dr. Mahoney’s practice in such settings to ask people about their hopes and their fears, “because you can really gauge how someone sees their illness by asking those questions.”
The woman responded that she was very afraid of dying. “When I hear that answer, my next question is, ‘What do you fear? Do you fear that you might suffer?’ She said, ‘Oh no, no, I’m not afraid of that at all. Actually, I’ve sinned a lot in my life, and I’m afraid of what comes after this life.’ ”
Realizing that the woman was suffering spiritually, Dr. Mahoney called in her team’s chaplain to meet with the patient. During that meeting, the patient revealed to Chaplain Sandra Schaap that she had been the one to remove her mother from life support (her mother had not left an advance directive either). She was plagued by the fear of how she would be judged for that act. The chaplain was able to offer some comfort by sharing a benediction, which stated (among other things) that Christ would complete what we have left undone in this life.
“That conversation helped the patient see that she needed to complete her own advance directive so that her daughters wouldn’t go through the same thing that she had with her own mother,” says Dr. Mahoney.
Although Dr. Mahoney did not see the woman again, “I think we certainly set the framework for her and her family to be able to cope with what was coming. In the traditional medical model of disease treatment, I’m not sure that kind of detail would have come out. This woman would have left the hospital still carrying around that burden and [would have] had a very different life from that point,” she says.
Conclusion
“Every patient and family has a story of their illness and how it has impacted their lives,” Dr. Mahoney emphasizes. “Many times people are in the hospital for an acute problem, but they’ve suffered with an illness for years. There is a real opportunity to allow patients and families to tell their stories. People are often relieved when someone listens and can help put things in perspective. Palliative care specialists, by actively listening to patient and family concerns, can help relieve suffering on a physical, spiritual, and emotional level even when cure is not possible.” TH
In this issue Gretchen Henkel also writes about hospitalists who are overcommitted.
Reference
- Center to Advance Palliative Care. The case for hospital-based palliative care. Available at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Accessed on February 20, 2007.
As hospital-based palliative care programs continue to grow, palliative care specialists are eager to dispel misconceptions about their work.1 Quality palliative care management at the end of life is often mistakenly perceived as synonymous with adequate pain control, but controlling pain is just one of the facets of effectively moderating the intensity of patients’ and families’ suffering.
The cases narrated here illustrate some of the other common themes of good palliative care management at the end of life: aggressive symptom management, interdisciplinary teamwork, and attention to patients’ and families’ spiritual concerns. Active, respectful listening can help to identify and alleviate obstacles to a more humane end-of-life journey.
Time to Process the Big Picture
State-of-the-art medical therapy does not always address dying patients’ suffering, says Melissa Mahoney, MD, assistant professor of medicine at Emory University and co-director of the Palliative Care Consult Service at Emory Crawford Long Hospital in Atlanta. She experienced this firsthand with a request to consult with a 60-year-old woman who had been in and out of sub-acute rehabilitation facilities seeking pain relief for her spinal stenosis. During a recent rehab facility stay, she had become septic and was transferred to the hospital for dialysis and other treatments. When Dr. Mahoney met the patient, the woman had been saying that she wanted to die, and her family was supportive of her wishes.
During her first conversation with the patient, however, Dr. Mahoney was able to discern that when she said she wanted to die, the patient meant, “I’m in so much pain that I don’t want to live this way.” The first step for the palliative care team was to begin patient-controlled analgesia (PCA) with IV hydromorphone hydrochloride in an attempt to control her pain. The PCA worked—dramatically.
“The next day,” recalls Dr. Mahoney, “she was like a new person. She was able to cope with the idea of dialysis and was able to talk with her family and put things in perspective.”
The palliative care team followed the woman for months, as she continued a cycle of readmissions to both the sub-acute facility and the hospital. The difference from the previous scenario, however, was that the team could offer aggressive symptom management while encouraging the patient and her family to revisit quality of life issues. She eventually died in the hospital, but Dr. Mahoney believes that the palliative care team’s interventions and emphasis on communication helped the patient and her family to cope with the situation more effectively.
With pain under control, patients can begin to address such questions as What’s important to me now? How do I want to spend my days? Who would I want to speak for me if I can’t speak for myself? What are my end-of-life wishes?’
“None of those higher-level discussions can take place until someone can physically handle them,” emphasizes Dr. Mahoney. “The palliative care approach puts the focus back on the patient and on the family and away from the disease. It seeks to treat the person and hopefully ease suffering through the illness.”
Goals of Care Change with Time
Howard R. Epstein, MD, medical director, Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and a member of the SHM Palliative Care Task Force, notes that good palliative care incorporates ongoing discussions about patients’ and families’ goals of care. “Following diagnosis of a life-threatening illness, the initial goal might be ‘I want to be cured,’ ” he says. “But, if the disease progresses, then you need to have another discussion about goals of care. Hopefully, this is part of the process all along.”
Dr. Epstein participated in a particularly memorable case last fall, consulting with a patient who had metastatic renal cancer. Surgery had left him with an abdominal abscess, which surgeons were proposing to address with another procedure in order to prevent a potentially fatal infection. The palliative care team was called in to help Mr. A, who was only 50, decide on a care plan. During the care conference, says Dr. Epstein, Mr. A was alert and joking with his wife and indicated that he would rather go home with hospice care than undergo another surgery.
The team asked Mr. A about his goals. “He didn’t know how much time he had left,” recalls Dr. Epstein, “although he had a specific goal in mind: One of his four sons was getting married, and he wanted to be there for that. They were a very close-knit family.” Mr. A had been intensely engaged as a father all through his sons’ school years. They ranged in age from 19 to 30, and Mr. A was determined to remain close with them throughout his dying process.
The care team facilitated his return home with a PCA pump for pain and a link with a visiting hospice nurse and social worker. The case was followed by a reporter from the St. Paul Pioneer Press, and it was in those articles that Dr. Epstein learned more of Mr. A’s story. For instance, extended family members were pitching in to remodel the house; Mrs. A would have to sell it to cover her husband’s medical bills after he died. The engaged son later had to tell his father that his fiancée had canceled the wedding. Mr. A was able to allay his son’s guilt and fear about the canceled wedding and to be the kind of supportive father he had always been.
Because his goal of living until the wedding had changed, Mr. A was then able to focus on his other goal: having family with him as he died at home. And, indeed, Mr. A died a peaceful death a few weeks later surrounded by his whole family.
A Ship without a Captain
Pediatric hospitalists who handle palliative care recognize that, unlike adults’ end-of-life trajectories, which are usually a straight line, the trajectories of children with complex medical conditions tend to be more erratic between diagnosis and cure or death. As a result, their families spend a longer time relating to the medical system. The job of the palliative care team is to acknowledge the family’s experience and reframe that experience into a more egalitarian and satisfying one, including a comprehensive plan of care, says Margaret Hood, MD, senior pediatric hospitalist at MultiCare’s Mary Bridge Children’s Hospital in Tacoma, Wash. Thus, the interdisciplinary team at Mary Bridge meets with the family around a round table, where everyone’s input is given equal respect and weight.
Dr. Hood recalls one case that was brought to her attention by a social worker. Amy (not her real name) had been born prematurely and had endured many medical problems in her first four years. Then, at age four, she started walking and talking; by age seven, she was reading at the fifth grade level. From ages seven to 10, Amy had minor problems, but she began deteriorating at age 10, when it was found that she had mitochondrial disease. The family had taken her to many specialists without any resolution to her problem and had been charging medical treatments to their credit cards. The social worker was concerned that the family would be devastated by bankruptcy.
The palliative care team organized a care conference attended by Amy’s primary care physician, palliative care team members, and other specialists. Although the care conference resulted in small adjustments to her care plan—a change in medication and the addition of one diagnostic test—the true change came when Amy’s mother turned to Dr. Hood and said, “You know, I thought you’d given up on us.”
That’s when it occurred to Dr. Hood that families like these, visiting specialist after specialist for their child’s complex medical conditions, are “on ‘a ship without a captain.’ Whether or not their children have life-limiting illnesses, they need a captain of the ship to help them navigate their journey,” she says.
Amy’s mother had been under the impression that the physicians were telling her there was nothing else to hope for. “You don’t give up hope,” asserts Dr. Hood. “You just change what you’re hoping for.”
Amy died three months after the palliative care conference, but took a Make-A-Wish Foundation trip to Disneyland and celebrated Christmas at home with her family. Her last wish, after Christmas, was to avoid re-entering the hospital, and this was honored as well.
There May Be More Time to Live
Attention to nuances embedded in patients’ stated wishes can sometimes result in a reversal of expectations about end of life. Stephanie Grossman, MD, assistant professor of medicine and co-director of the Palliative Care Program for Emory University Hospital and Emory Crawford Long Hospital in Atlanta, was called by the hospitalist service last year to help facilitate transfer of a patient to hospice care.
In her 70s, the active woman had come to the hospital because a tumor mass was eroding through her breast tissue. The woman was avoiding treatment, including a biopsy, and appeared to be resolved to her fate. Based on her conversation with the emergency department (ED) attending, hospice was discussed and recommended; the patient was admitted primarily for IV antibiotics and care of her wound. In discussing goals of care with the patient, however, Dr. Grossman was able to elicit her reasons for refusing treatment. Ten years earlier, the patient had watched her daughter suffer with aggressive chemotherapy and radiation for her breast cancer. She told Dr. Grossman, “I’ve lived my life; I don’t want to go through all that.”
Knowing that breast cancer treatments have evolved in the past decade, Dr. Grossman asked the woman whether she would agree to a consultation with an oncologist to find out about less toxic treatment, including hormonal therapy. Subsequently, the patient decided to undergo a lumpectomy to increase her options. Dr. Grossman also prescribed a mild pain reliever for the woman, who had expressed fears about becoming addicted to pain medication (a common misperception in elderly patients). Upon discharge, the patient was feeling better physically, and she was optimistic about her future.
Despite the perceptions of the ED staff, the patient had not been hospice-appropriate. “No one had ever offered her the alternatives. In her mind, she saw chemotherapy as this terrible thing, and she just didn’t want to have that,” says Dr. Grossman. “So by listening to her we found out why she didn’t want chemotherapy, and we were able to encourage her to talk with the oncologist and the surgeon.”
I’m Afraid of What Comes after This Life
“Sometimes you find that patients and families are making decisions purely in a spiritual context,” notes Dr. Mahoney. “Until you know that, you can deliver clear and concise medical information and opinions and they won’t hear it. They may respect your opinion, but they will not take that into consideration when they’re making the decisions about themselves or a loved one because their spiritual belief system supersedes that factual information.”
Last year, Dr. Mahoney encountered a woman her late 50s with metastatic cancer. Her mother had died young of the same disease. The patient knew her disease was advanced and that she was facing the same thing her mother had faced. She, too, was leaving behind her daughters.
The patient, recalls Dr. Mahoney, had not filled out an advance directive and was having a difficult time talking with her family about her situation. It is Dr. Mahoney’s practice in such settings to ask people about their hopes and their fears, “because you can really gauge how someone sees their illness by asking those questions.”
The woman responded that she was very afraid of dying. “When I hear that answer, my next question is, ‘What do you fear? Do you fear that you might suffer?’ She said, ‘Oh no, no, I’m not afraid of that at all. Actually, I’ve sinned a lot in my life, and I’m afraid of what comes after this life.’ ”
Realizing that the woman was suffering spiritually, Dr. Mahoney called in her team’s chaplain to meet with the patient. During that meeting, the patient revealed to Chaplain Sandra Schaap that she had been the one to remove her mother from life support (her mother had not left an advance directive either). She was plagued by the fear of how she would be judged for that act. The chaplain was able to offer some comfort by sharing a benediction, which stated (among other things) that Christ would complete what we have left undone in this life.
“That conversation helped the patient see that she needed to complete her own advance directive so that her daughters wouldn’t go through the same thing that she had with her own mother,” says Dr. Mahoney.
Although Dr. Mahoney did not see the woman again, “I think we certainly set the framework for her and her family to be able to cope with what was coming. In the traditional medical model of disease treatment, I’m not sure that kind of detail would have come out. This woman would have left the hospital still carrying around that burden and [would have] had a very different life from that point,” she says.
Conclusion
“Every patient and family has a story of their illness and how it has impacted their lives,” Dr. Mahoney emphasizes. “Many times people are in the hospital for an acute problem, but they’ve suffered with an illness for years. There is a real opportunity to allow patients and families to tell their stories. People are often relieved when someone listens and can help put things in perspective. Palliative care specialists, by actively listening to patient and family concerns, can help relieve suffering on a physical, spiritual, and emotional level even when cure is not possible.” TH
In this issue Gretchen Henkel also writes about hospitalists who are overcommitted.
Reference
- Center to Advance Palliative Care. The case for hospital-based palliative care. Available at: www.capc.org/building-a-hospital-based-palliative-care-program/case/support-from-capc/capc_publications/making-the-case.pdf. Accessed on February 20, 2007.
Don't Commit to Overcommit
There is never enough time, unless you’re serving it. —Malcolm Forbes (1919-1990)
Has this ever happened to you? You agree—months in advance—to write an article for The Hospitalist, thinking you will have plenty of time to research and write it. You hurriedly enter the item on your calendar and turn back to all your current commitments. Later, as the date approaches, you realize that you’re running out of time to do justice to the article to which you had committed.
Psychologists have explored the common human problem of overbooking and have found many contributing dynamics. A 2005 study in the Journal of Experimental Psychology suggested one explanation: Most of us, when accepting invitations weeks or months in advance, tend to view the future as more open and less busy than the present. “The nature of time fools us and we ‘forget’ about how things fill our days,” comment study authors Gal Zauberman and John Lynch.1
How do hospitalists weigh competing demands on their time? For answers to this question, naturally we asked several already-busy hospitalists to discuss the issue. They shared some lessons learned and a few strategies for managing their most precious commodity.
No Mystery
“Many things take longer than they’re supposed to,” points out S. Trent Rosenbloom, MD, MPH, a former hospitalist and currently assistant professor in the departments of Biomedical Informatics, Internal Medicine and Pediatrics, and the School of Nursing at Vanderbilt University Medical Center in Nashville, Tenn.
His situation on the morning of our interview necessitated a reschedule due to a longer-than-anticipated smog check the afternoon before. “I told myself, next year, I’ll take care of this before the deadline,” he says. “But I always end up doing this at the last minute because everything else gets in the way.”
“This interview is another example: overcommitting once more,” writes Michael J. Hovan, MD, when he agrees via e-mail to a telephone interview about the problem of overscheduling. Like most hospitalists, Dr. Hovan works with a perpetually full plate. He is inpatient director for the Hospital Family Medicine Service and assistant professor at Mayo Medical School in the Division of Family and Community Medicine at the Mayo Clinic in Scottsdale/Phoenix. Like his colleagues, Dr. Hovan has had to struggle with juggling multiple roles.
“The hospital is a far different practice environment than it was just a few years ago,” he remarks. The high intensity of patient management is now coupled with increasing administrative complexities due to a more heavily regulated environment.
As a relatively new specialty, hospital medicine requires more attention in order to establish its visibility and viability. Dr. Hovan feels this pressure keenly because, as a family medicine hospitalist, he’s in a minority position. (The majority of hospitalists trained in internal medicine, according to SHM’s 2006 Annual Survey.2)
“It’s even more important for my department, in a tertiary academic center, to maintain a visible presence on particular committees,” he says. The result of all these necessary roles? “There really are no weekends or defined time off,” says Dr. Hovan. “I’d estimate that 20% of what I do is done ‘off the clock.’ I have taken the Mayo computers to Hawaii, to family ski vacations, and [to] far less exotic locales away from the hospital setting.”
“Medicine Is Stressful”
Mary A. Dallas, MD, formerly medical director of the hospitalist service and currently medical information officer for Presbyterian Healthcare Services, an integrated healthcare delivery network in Albuquerque, N.M., noticed certain trends when she was creating schedules with the hospitalist group.
“Things sound really good on paper,” she says. “The reality is, the intensity of work is high, and sometimes you forget about that when you’re creating schedules. You might have set yourself up for three overnight shifts in order to compress work hours and expand off-time, and by the end of the second shift, you are really tired.”
Another factor is that employers expect hospitalists to see patients until the end of their shifts, and that’s when the off the clock paperwork occurs. A 40-hour workweek can easily balloon into 50 hours or more.
Physicians may also neglect to build in the emotional toll of their jobs when blocking in future schedules. “Medicine is stressful,” comments Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston. “It’s stressful to see people suffer and to deal with families who are stressed and sometimes not perfectly functional.”
In addition, she says, “Excellence in teaching and excellence in patient care require communication, and communication takes time. If physicians are up all night taking calls and then working all day so that there is continuity in patient care, you have to grapple with the issue of physician fatigue.”
And Then There Are Committees
Even though committee participation is technically considered “volunteer” time, physicians who are elected chiefs of their hospital sections are automatically expected to participate. It behooves hospitalists to participate in committee work at their institutions, believes Dr. Dallas, because this is often where governance decisions are made about how they will practice in the hospital.
Tom Baudendistel, MD, is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health. The hospitalists in his group are very involved in committee work. “The committees are important, and we want the administration to match our faces to our names, especially when it comes to budget negotiation time,” he explains. “That is a direct benefit of being visible participants in committees.”
Committee participation may be handled differently in purely academic settings. The time Dr. Rosenbloom spends in committees related to department support is credited to his work schedule. The problem comes when, once again, that participation takes more time than expected. One of his weekly committees routinely runs a half hour longer than its one-and-a-half hour time slot and requires five to eight hours of preparatory work. As is common with his peers, Dr. Rosenbloom has sometimes used his allotted consulting time to cover extra commitments related to his primary job.
Temptations to Say Yes
Invitations to participate in extra administrative or educational duties often naturally flow to productive people, observes Dr. Dallas. “You may be dragged into a lot of different work that you didn’t necessarily need to be into,” she says. “You just have to step back periodically and ask, ‘Is this right for me? Am I the right person to be involved? Are there other people who can do this? And then, say no. Really, that’s OK!” (See “Triage What’s Important,” p. 15, for tips.]
“It’s easy to get overloaded,” admits Dr. Baudendistel. “I certainly found myself overextended more often earlier in my career.” Saying yes to additional commitments can be related to workplace power dynamics, he believes. “When people who are in positions above you approach you about a project that is going to take time—whether or not it’s your passion or skill set—there is pressure to want to please that person. Saying no is a skill, and if you say ‘absolutely not’ early on in your career, you will not be asked to do other things. You may be shooting yourself in the foot.”
Defining Trails
It’s natural enough for hospitalists to feel optimistic about the openness of the future, says Dr. Hovan. Hospitalists may feel that the time investments they make now to nurture their profession within their institutions are temporary and may not always be as intense. The hope is that “the specialty is going to be more mature and [will] become more self-sustaining in the near future. Yet you glimpse over the horizon, and that’s not really true,” he says ruefully. “Everything in hospital medicine has nascency about it. There are no established trails. When we define one role, another one emerges.”
Many hospitalist services, for example, are now expanding beyond the medical floor to the surgical floor to perform consults to provide post-surgical management of medical issues.
Dr. McKean sees the “overwhelming demand for service” as one of hospital medicine’s trickiest challenges. “Basically, because hospitalists are young and energetic and wanting to please, it’s very easy for them to feel like they have to meet all the service obligations.” But this propensity can derail the overall mission of and vision for the hospitalist service if physicians do not set clear goals for themselves and their groups.
Physician, Know Thyself
Building in time to set and re-examine career goals is a skill that hospitalists should practice regularly, says Dr. McKean: “I learned the hard way that a hospitalist’s most important strategy is to be very self-reflective.”
She confesses that, in the past, she has often said yes to the point that her obligations became unmanageable. She advises young hospitalists to reflect on what is important to them and also “to recognize that during different times in their lives, they’re going to either have less free time or more free time, depending upon their families and other demands. So what might seem like a great opportunity might be an unrealistic one when you have three children under the age of five.” On the other hand, someone who is single might set a goal to make as much money as possible in the short term by taking on additional work shifts.
Dr. McKean also suggests that young hospitalists seek out not just one but multiple mentors. For example, “someone who wants to be a superstar in hospital medicine relating to quality improvement might naturally pick as a mentor somebody who is already doing quality improvement.”
A person who is having difficulty juggling family roles in addition to intensive work schedules might want to seek out someone who has … grappled successfully with those issues. Hospitalists should also consider seeking mentors outside the discipline of medicine—those in business, for instance, can contribute valuable insights to someone seeking a career in hospital administration.
Given the nature of hospital medicine, guarding one’s time will always be a concern, agree most of those interviewed for this article. “I think the juggling act is always there,” says Dr. Baudendistel. “There are usually up to six or more balls that you can simultaneously be juggling: administrative duties, family obligations, society commitments, teaching duties, your own academic agenda, and your professional agenda. You just have to know which ones are your priorities. And, sometimes, you have to acknowledge that maybe it’s time to say no or to stop doing one of those things.” TH
Contributing Writer Gretchen Henkel thanks the hospitalists who reshuffled their commitments in order to discuss overbooking with her and thanks her editor, Lisa Dionne, for the two extensions that allowed her to complete this assignment.
References
- Zauberman G, Lynch JG Jr. Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen. 2005 Feb;134(1):23-37.
- Society of Hospital Medicine 2005-2006 Survey: State of the Hospital Medicine Movement. 2006. Available at: www.hospitalmedicine.org. Last accessed February 19, 2007.
There is never enough time, unless you’re serving it. —Malcolm Forbes (1919-1990)
Has this ever happened to you? You agree—months in advance—to write an article for The Hospitalist, thinking you will have plenty of time to research and write it. You hurriedly enter the item on your calendar and turn back to all your current commitments. Later, as the date approaches, you realize that you’re running out of time to do justice to the article to which you had committed.
Psychologists have explored the common human problem of overbooking and have found many contributing dynamics. A 2005 study in the Journal of Experimental Psychology suggested one explanation: Most of us, when accepting invitations weeks or months in advance, tend to view the future as more open and less busy than the present. “The nature of time fools us and we ‘forget’ about how things fill our days,” comment study authors Gal Zauberman and John Lynch.1
How do hospitalists weigh competing demands on their time? For answers to this question, naturally we asked several already-busy hospitalists to discuss the issue. They shared some lessons learned and a few strategies for managing their most precious commodity.
No Mystery
“Many things take longer than they’re supposed to,” points out S. Trent Rosenbloom, MD, MPH, a former hospitalist and currently assistant professor in the departments of Biomedical Informatics, Internal Medicine and Pediatrics, and the School of Nursing at Vanderbilt University Medical Center in Nashville, Tenn.
His situation on the morning of our interview necessitated a reschedule due to a longer-than-anticipated smog check the afternoon before. “I told myself, next year, I’ll take care of this before the deadline,” he says. “But I always end up doing this at the last minute because everything else gets in the way.”
“This interview is another example: overcommitting once more,” writes Michael J. Hovan, MD, when he agrees via e-mail to a telephone interview about the problem of overscheduling. Like most hospitalists, Dr. Hovan works with a perpetually full plate. He is inpatient director for the Hospital Family Medicine Service and assistant professor at Mayo Medical School in the Division of Family and Community Medicine at the Mayo Clinic in Scottsdale/Phoenix. Like his colleagues, Dr. Hovan has had to struggle with juggling multiple roles.
“The hospital is a far different practice environment than it was just a few years ago,” he remarks. The high intensity of patient management is now coupled with increasing administrative complexities due to a more heavily regulated environment.
As a relatively new specialty, hospital medicine requires more attention in order to establish its visibility and viability. Dr. Hovan feels this pressure keenly because, as a family medicine hospitalist, he’s in a minority position. (The majority of hospitalists trained in internal medicine, according to SHM’s 2006 Annual Survey.2)
“It’s even more important for my department, in a tertiary academic center, to maintain a visible presence on particular committees,” he says. The result of all these necessary roles? “There really are no weekends or defined time off,” says Dr. Hovan. “I’d estimate that 20% of what I do is done ‘off the clock.’ I have taken the Mayo computers to Hawaii, to family ski vacations, and [to] far less exotic locales away from the hospital setting.”
“Medicine Is Stressful”
Mary A. Dallas, MD, formerly medical director of the hospitalist service and currently medical information officer for Presbyterian Healthcare Services, an integrated healthcare delivery network in Albuquerque, N.M., noticed certain trends when she was creating schedules with the hospitalist group.
“Things sound really good on paper,” she says. “The reality is, the intensity of work is high, and sometimes you forget about that when you’re creating schedules. You might have set yourself up for three overnight shifts in order to compress work hours and expand off-time, and by the end of the second shift, you are really tired.”
Another factor is that employers expect hospitalists to see patients until the end of their shifts, and that’s when the off the clock paperwork occurs. A 40-hour workweek can easily balloon into 50 hours or more.
Physicians may also neglect to build in the emotional toll of their jobs when blocking in future schedules. “Medicine is stressful,” comments Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston. “It’s stressful to see people suffer and to deal with families who are stressed and sometimes not perfectly functional.”
In addition, she says, “Excellence in teaching and excellence in patient care require communication, and communication takes time. If physicians are up all night taking calls and then working all day so that there is continuity in patient care, you have to grapple with the issue of physician fatigue.”
And Then There Are Committees
Even though committee participation is technically considered “volunteer” time, physicians who are elected chiefs of their hospital sections are automatically expected to participate. It behooves hospitalists to participate in committee work at their institutions, believes Dr. Dallas, because this is often where governance decisions are made about how they will practice in the hospital.
Tom Baudendistel, MD, is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health. The hospitalists in his group are very involved in committee work. “The committees are important, and we want the administration to match our faces to our names, especially when it comes to budget negotiation time,” he explains. “That is a direct benefit of being visible participants in committees.”
Committee participation may be handled differently in purely academic settings. The time Dr. Rosenbloom spends in committees related to department support is credited to his work schedule. The problem comes when, once again, that participation takes more time than expected. One of his weekly committees routinely runs a half hour longer than its one-and-a-half hour time slot and requires five to eight hours of preparatory work. As is common with his peers, Dr. Rosenbloom has sometimes used his allotted consulting time to cover extra commitments related to his primary job.
Temptations to Say Yes
Invitations to participate in extra administrative or educational duties often naturally flow to productive people, observes Dr. Dallas. “You may be dragged into a lot of different work that you didn’t necessarily need to be into,” she says. “You just have to step back periodically and ask, ‘Is this right for me? Am I the right person to be involved? Are there other people who can do this? And then, say no. Really, that’s OK!” (See “Triage What’s Important,” p. 15, for tips.]
“It’s easy to get overloaded,” admits Dr. Baudendistel. “I certainly found myself overextended more often earlier in my career.” Saying yes to additional commitments can be related to workplace power dynamics, he believes. “When people who are in positions above you approach you about a project that is going to take time—whether or not it’s your passion or skill set—there is pressure to want to please that person. Saying no is a skill, and if you say ‘absolutely not’ early on in your career, you will not be asked to do other things. You may be shooting yourself in the foot.”
Defining Trails
It’s natural enough for hospitalists to feel optimistic about the openness of the future, says Dr. Hovan. Hospitalists may feel that the time investments they make now to nurture their profession within their institutions are temporary and may not always be as intense. The hope is that “the specialty is going to be more mature and [will] become more self-sustaining in the near future. Yet you glimpse over the horizon, and that’s not really true,” he says ruefully. “Everything in hospital medicine has nascency about it. There are no established trails. When we define one role, another one emerges.”
Many hospitalist services, for example, are now expanding beyond the medical floor to the surgical floor to perform consults to provide post-surgical management of medical issues.
Dr. McKean sees the “overwhelming demand for service” as one of hospital medicine’s trickiest challenges. “Basically, because hospitalists are young and energetic and wanting to please, it’s very easy for them to feel like they have to meet all the service obligations.” But this propensity can derail the overall mission of and vision for the hospitalist service if physicians do not set clear goals for themselves and their groups.
Physician, Know Thyself
Building in time to set and re-examine career goals is a skill that hospitalists should practice regularly, says Dr. McKean: “I learned the hard way that a hospitalist’s most important strategy is to be very self-reflective.”
She confesses that, in the past, she has often said yes to the point that her obligations became unmanageable. She advises young hospitalists to reflect on what is important to them and also “to recognize that during different times in their lives, they’re going to either have less free time or more free time, depending upon their families and other demands. So what might seem like a great opportunity might be an unrealistic one when you have three children under the age of five.” On the other hand, someone who is single might set a goal to make as much money as possible in the short term by taking on additional work shifts.
Dr. McKean also suggests that young hospitalists seek out not just one but multiple mentors. For example, “someone who wants to be a superstar in hospital medicine relating to quality improvement might naturally pick as a mentor somebody who is already doing quality improvement.”
A person who is having difficulty juggling family roles in addition to intensive work schedules might want to seek out someone who has … grappled successfully with those issues. Hospitalists should also consider seeking mentors outside the discipline of medicine—those in business, for instance, can contribute valuable insights to someone seeking a career in hospital administration.
Given the nature of hospital medicine, guarding one’s time will always be a concern, agree most of those interviewed for this article. “I think the juggling act is always there,” says Dr. Baudendistel. “There are usually up to six or more balls that you can simultaneously be juggling: administrative duties, family obligations, society commitments, teaching duties, your own academic agenda, and your professional agenda. You just have to know which ones are your priorities. And, sometimes, you have to acknowledge that maybe it’s time to say no or to stop doing one of those things.” TH
Contributing Writer Gretchen Henkel thanks the hospitalists who reshuffled their commitments in order to discuss overbooking with her and thanks her editor, Lisa Dionne, for the two extensions that allowed her to complete this assignment.
References
- Zauberman G, Lynch JG Jr. Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen. 2005 Feb;134(1):23-37.
- Society of Hospital Medicine 2005-2006 Survey: State of the Hospital Medicine Movement. 2006. Available at: www.hospitalmedicine.org. Last accessed February 19, 2007.
There is never enough time, unless you’re serving it. —Malcolm Forbes (1919-1990)
Has this ever happened to you? You agree—months in advance—to write an article for The Hospitalist, thinking you will have plenty of time to research and write it. You hurriedly enter the item on your calendar and turn back to all your current commitments. Later, as the date approaches, you realize that you’re running out of time to do justice to the article to which you had committed.
Psychologists have explored the common human problem of overbooking and have found many contributing dynamics. A 2005 study in the Journal of Experimental Psychology suggested one explanation: Most of us, when accepting invitations weeks or months in advance, tend to view the future as more open and less busy than the present. “The nature of time fools us and we ‘forget’ about how things fill our days,” comment study authors Gal Zauberman and John Lynch.1
How do hospitalists weigh competing demands on their time? For answers to this question, naturally we asked several already-busy hospitalists to discuss the issue. They shared some lessons learned and a few strategies for managing their most precious commodity.
No Mystery
“Many things take longer than they’re supposed to,” points out S. Trent Rosenbloom, MD, MPH, a former hospitalist and currently assistant professor in the departments of Biomedical Informatics, Internal Medicine and Pediatrics, and the School of Nursing at Vanderbilt University Medical Center in Nashville, Tenn.
His situation on the morning of our interview necessitated a reschedule due to a longer-than-anticipated smog check the afternoon before. “I told myself, next year, I’ll take care of this before the deadline,” he says. “But I always end up doing this at the last minute because everything else gets in the way.”
“This interview is another example: overcommitting once more,” writes Michael J. Hovan, MD, when he agrees via e-mail to a telephone interview about the problem of overscheduling. Like most hospitalists, Dr. Hovan works with a perpetually full plate. He is inpatient director for the Hospital Family Medicine Service and assistant professor at Mayo Medical School in the Division of Family and Community Medicine at the Mayo Clinic in Scottsdale/Phoenix. Like his colleagues, Dr. Hovan has had to struggle with juggling multiple roles.
“The hospital is a far different practice environment than it was just a few years ago,” he remarks. The high intensity of patient management is now coupled with increasing administrative complexities due to a more heavily regulated environment.
As a relatively new specialty, hospital medicine requires more attention in order to establish its visibility and viability. Dr. Hovan feels this pressure keenly because, as a family medicine hospitalist, he’s in a minority position. (The majority of hospitalists trained in internal medicine, according to SHM’s 2006 Annual Survey.2)
“It’s even more important for my department, in a tertiary academic center, to maintain a visible presence on particular committees,” he says. The result of all these necessary roles? “There really are no weekends or defined time off,” says Dr. Hovan. “I’d estimate that 20% of what I do is done ‘off the clock.’ I have taken the Mayo computers to Hawaii, to family ski vacations, and [to] far less exotic locales away from the hospital setting.”
“Medicine Is Stressful”
Mary A. Dallas, MD, formerly medical director of the hospitalist service and currently medical information officer for Presbyterian Healthcare Services, an integrated healthcare delivery network in Albuquerque, N.M., noticed certain trends when she was creating schedules with the hospitalist group.
“Things sound really good on paper,” she says. “The reality is, the intensity of work is high, and sometimes you forget about that when you’re creating schedules. You might have set yourself up for three overnight shifts in order to compress work hours and expand off-time, and by the end of the second shift, you are really tired.”
Another factor is that employers expect hospitalists to see patients until the end of their shifts, and that’s when the off the clock paperwork occurs. A 40-hour workweek can easily balloon into 50 hours or more.
Physicians may also neglect to build in the emotional toll of their jobs when blocking in future schedules. “Medicine is stressful,” comments Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston. “It’s stressful to see people suffer and to deal with families who are stressed and sometimes not perfectly functional.”
In addition, she says, “Excellence in teaching and excellence in patient care require communication, and communication takes time. If physicians are up all night taking calls and then working all day so that there is continuity in patient care, you have to grapple with the issue of physician fatigue.”
And Then There Are Committees
Even though committee participation is technically considered “volunteer” time, physicians who are elected chiefs of their hospital sections are automatically expected to participate. It behooves hospitalists to participate in committee work at their institutions, believes Dr. Dallas, because this is often where governance decisions are made about how they will practice in the hospital.
Tom Baudendistel, MD, is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health. The hospitalists in his group are very involved in committee work. “The committees are important, and we want the administration to match our faces to our names, especially when it comes to budget negotiation time,” he explains. “That is a direct benefit of being visible participants in committees.”
Committee participation may be handled differently in purely academic settings. The time Dr. Rosenbloom spends in committees related to department support is credited to his work schedule. The problem comes when, once again, that participation takes more time than expected. One of his weekly committees routinely runs a half hour longer than its one-and-a-half hour time slot and requires five to eight hours of preparatory work. As is common with his peers, Dr. Rosenbloom has sometimes used his allotted consulting time to cover extra commitments related to his primary job.
Temptations to Say Yes
Invitations to participate in extra administrative or educational duties often naturally flow to productive people, observes Dr. Dallas. “You may be dragged into a lot of different work that you didn’t necessarily need to be into,” she says. “You just have to step back periodically and ask, ‘Is this right for me? Am I the right person to be involved? Are there other people who can do this? And then, say no. Really, that’s OK!” (See “Triage What’s Important,” p. 15, for tips.]
“It’s easy to get overloaded,” admits Dr. Baudendistel. “I certainly found myself overextended more often earlier in my career.” Saying yes to additional commitments can be related to workplace power dynamics, he believes. “When people who are in positions above you approach you about a project that is going to take time—whether or not it’s your passion or skill set—there is pressure to want to please that person. Saying no is a skill, and if you say ‘absolutely not’ early on in your career, you will not be asked to do other things. You may be shooting yourself in the foot.”
Defining Trails
It’s natural enough for hospitalists to feel optimistic about the openness of the future, says Dr. Hovan. Hospitalists may feel that the time investments they make now to nurture their profession within their institutions are temporary and may not always be as intense. The hope is that “the specialty is going to be more mature and [will] become more self-sustaining in the near future. Yet you glimpse over the horizon, and that’s not really true,” he says ruefully. “Everything in hospital medicine has nascency about it. There are no established trails. When we define one role, another one emerges.”
Many hospitalist services, for example, are now expanding beyond the medical floor to the surgical floor to perform consults to provide post-surgical management of medical issues.
Dr. McKean sees the “overwhelming demand for service” as one of hospital medicine’s trickiest challenges. “Basically, because hospitalists are young and energetic and wanting to please, it’s very easy for them to feel like they have to meet all the service obligations.” But this propensity can derail the overall mission of and vision for the hospitalist service if physicians do not set clear goals for themselves and their groups.
Physician, Know Thyself
Building in time to set and re-examine career goals is a skill that hospitalists should practice regularly, says Dr. McKean: “I learned the hard way that a hospitalist’s most important strategy is to be very self-reflective.”
She confesses that, in the past, she has often said yes to the point that her obligations became unmanageable. She advises young hospitalists to reflect on what is important to them and also “to recognize that during different times in their lives, they’re going to either have less free time or more free time, depending upon their families and other demands. So what might seem like a great opportunity might be an unrealistic one when you have three children under the age of five.” On the other hand, someone who is single might set a goal to make as much money as possible in the short term by taking on additional work shifts.
Dr. McKean also suggests that young hospitalists seek out not just one but multiple mentors. For example, “someone who wants to be a superstar in hospital medicine relating to quality improvement might naturally pick as a mentor somebody who is already doing quality improvement.”
A person who is having difficulty juggling family roles in addition to intensive work schedules might want to seek out someone who has … grappled successfully with those issues. Hospitalists should also consider seeking mentors outside the discipline of medicine—those in business, for instance, can contribute valuable insights to someone seeking a career in hospital administration.
Given the nature of hospital medicine, guarding one’s time will always be a concern, agree most of those interviewed for this article. “I think the juggling act is always there,” says Dr. Baudendistel. “There are usually up to six or more balls that you can simultaneously be juggling: administrative duties, family obligations, society commitments, teaching duties, your own academic agenda, and your professional agenda. You just have to know which ones are your priorities. And, sometimes, you have to acknowledge that maybe it’s time to say no or to stop doing one of those things.” TH
Contributing Writer Gretchen Henkel thanks the hospitalists who reshuffled their commitments in order to discuss overbooking with her and thanks her editor, Lisa Dionne, for the two extensions that allowed her to complete this assignment.
References
- Zauberman G, Lynch JG Jr. Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen. 2005 Feb;134(1):23-37.
- Society of Hospital Medicine 2005-2006 Survey: State of the Hospital Medicine Movement. 2006. Available at: www.hospitalmedicine.org. Last accessed February 19, 2007.
Perfect Pain Control
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
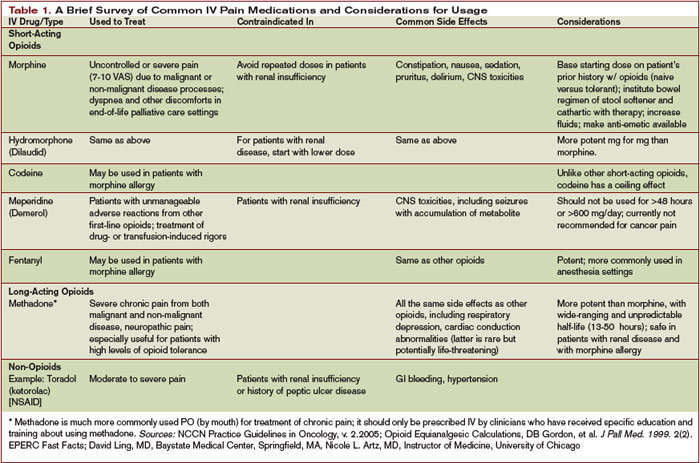
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
An Academic Hurdle
As clinicians and educators, academic hospitalists function within several arenas: They are role models and teachers in the inpatient arena, but they also feel pressure from hospital administration to meet throughput and capacity goals. In addition, hospitalist clinician-educators are expected to be leaders in quality improvement.
But are the rewards for academic hospitalists commensurate with the demands placed upon them? Even as hospitalists prove their worth to hospital administrators, many clinician-educators find themselves pulled between time spent on service and time for the academic pursuits necessary to improve resident education and merit faculty promotions.
“In my current situation, there is difficulty in fitting in the prep work time for teaching rounds,” says Elizabeth A. Schultz, MD, who practices with the Adult Hospitalist Team at Swedish Medical Center in Seattle and is also affiliated with the University of Washington School of Medicine. “There’s really no time for that, other than time on my own—and I’m actually in a really good situation right now where my boss has capped the number of patients I see in a day and afforded me the ability to go to conferences, do teaching rounds, and to really focus on resident and medical student education.”
Dr. Schultz is not alone in struggling to balance clinical and educational duties. Many hospital medicine leaders wrestle with these concerns, aware that growing clinical responsibilities impinge on teaching time and that the sustainability of hospital medicine as a career is at stake.
Confront the Dilemma
An October 2006 survey by the University HealthSystem Consortium confirmed that hospitalists have improved the educational process for residents and medical students, but it also identified impediments to the continuation and growth of hospitalist programs. (The Benchmarking Study, “Role of the Hospitalist,” is available online to University HealthSystem Consortium (UHC) members and registered website users at www.uhc.edu.) The most common barrier is the difficulty in attracting and retaining quality candidates, given the ratio of salary to workload, the potential for burnout, and undefined career paths.
“There is a significant amount of demand on one small group of physicians, and we haven’t necessarily found a way to compensate them for the different roles they play,” reflects Alpesh Amin, MD, MBA, FACP, associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California at Irvine (UCI), where he founded the UCI hospitalist program in 1998 and serves as its executive director. “These three arenas that hospitalists have to constantly keep moving in are not always complementary. How do you spend more time facilitating the teaching mission versus time facilitating the throughput mission or the expanding clinical mission?”
Meeting goals for academic appointments adds yet another layer of role conflict, he notes.
Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston and chair of SHM’s Career Satisfaction Task Force, also acknowledges the tensions between clinical duties and academic pursuits. “If you have 20 patients to see and discharge and yet you also have a grant to write, guess what’s not going to get done?”
To be fair, academic hospitalists experience their situations in different ways. Kathleen Bradford, MD, the inpatient director of the University of North Carolina (UNC) Children’s Hospital, director of the Pediatric Hospitalist Program, and assistant residency director for the Division of General Pediatrics at UNC in Chapel Hill, N.C., has not experienced a huge conflict between her teaching and clinical duties, but she has noticed that there are fewer opportunities for teaching, given the increased clinical demands on physicians and the decreased availability of residents.
“I’ve always felt that medicine—and especially medical teaching—is like an apprenticeship,” she explains. “There are many, many opportunities to teach while doing in an apprenticeship-like fashion. The demands of taking care of patients and [reduced] resident work hours have certainly decreased the ability to do more formal and didactic or classroom-type teaching. However, the opportunities for spontaneous or ‘teach as you go’ education still exist.”
Solutions to the Time Crunch
Dr. Schultz, a member of the Swedish Medical Center’s teaching service who leads a teaching team every month, admits she has no answers to the time crunch academic hospitalists experience. “There just isn’t enough manpower,” she says. “The hospital doesn’t get paid for people to teach, and to pay people to have dedicated time to pursue academic research or prepare lectures just isn’t feasible for most hospitals, as they are already struggling to make ends meet.”
Many hospitals employ both non-teaching and teaching services to ensure night and weekend coverage. But this can create other dilemmas for the academic hospitalist. For instance, Dr. Schultz says her teaching service gets the more complicated and critically ill patients who require more of her time, thus squeezing out, again, the opportunity to prepare lecture notes or conduct research.
At UNC Children’s Hospital, the pediatric hospitalist program is in its infancy, having launched in fall 2006, and the new service is mostly a non-teaching service. Dr. Bradford reports that the teaching and the hospitalist service are assigning patients on a case-by-case basis. “There is [teaching] value in all patients and all cases,” says Dr. Bradford, “but it’s really hard to say which ones have the most value: Should it be the patient who has a short stay with a common illness or a patient who has been chronically ill and in the hospital for 100 days? It’s hard to know.”
At Brigham and Women’s Hospital, Dr. McKean reports the hospitalist group did not want to institute a two-tiered [teaching and non-teaching] hospitalist program, so one of their hospitalists, Chris Roy, MD, created a Physician Assistant Clinician Educator (PACE) service, with a hospitalist supervising two PAs during daytime hours; it’s supplemented by moonlighters at night. Members of this service have teaching responsibilities and are involved in curriculum development for physician assistants and students. Additional research is needed to examine outcomes of educational efforts directed toward the multidisciplinary team in the core competency areas elaborated by the Accreditation Council for Graduate Medical Education, explains Dr. McKean.
Proactive Strategies
Whatever strategies are used to address case workloads, effecting real change for academic hospitalists—ensuring protected time as well as rewards for educational and research pursuits—will require clear-sighted planning from hospitalist leaders. “The bottom line is to proactively manage the program’s direction and growth,” asserts Dr. McKean. “Instead of being everybody’s Band-Aid and being everything to everybody, it’s important to have a strategic plan. You can’t necessarily plan for five years, but you can plan for three, and you could do things in a step-wise manner to increase the academic and research presence.”
This is precisely where SHM’s emphasis on networking and mentoring can come in, believes SHM’s Education Committee Chair Preetha Basaviah, MD, clinical associate professor of medicine and associate course director, Practice of Medicine, at Stanford University School of Medicine, California. SHM has led many initiatives, such as the publication of the Core Competencies and the creation of Web-based quality improvement resource rooms, which help provide curriculum support.
“What we’ve done as an education committee is to help provide some of the resources, support, and advocacy that our members need so that they can go back to their programs and say, ‘These are the national standards and resources provided by an organization that advocates for us.’ ” says Dr. Basaviah.
Creating a network of hospitalists, both regionally and nationally, provides opportunities to gain protected time for research pursuits and recognition from one’s peers, Dr. Basaviah continues. “I think what we’ve done for clinician educators is to promote thinking proactively about your short-term and long-term career goals, including developing an area of expertise, before you take on commitments,” she says.
Input with Curricular Design
Dr. Amin’s role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his role on the Core Competencies Task Force. He believes it is through such initiatives that hospitalists can become leaders in their institutions, participating in curriculum development as well as quality and performance improvement efforts.
“I don’t view myself as just working for the hospital or … for the School [of Medicine]. I view myself as working for the enterprise,” he says. As a result his hospitalist group has taken the lead in designing various residency inpatient curricula. “If you do it right, you could actually design curricula to educate residents about heart failure—teaching them about the pathophysiology and disease management—but then also teach them about core measures, outcomes, and systems-based practice in heart failure,” he says. “When all that comes together, I think you’re making some progress.”
Jeffrey G. Wiese, MD, vice chairman and director of the Internal Medicine Residency Program at Tulane University, New Orleans, is the leader of the SHM Task Force for Integrating Core Competencies into Residency Education. He points to the SHM Academic Task Force’s idea of developing an EVU, or educational value unit, that would define and compensate for amounts of time invested in educational pursuits. He would also like to see SHM take a role in developing standards and recommendations for promotion criteria. These are tools that academic hospitalists could use to “make their case” to medical schools’ residency programs about the value they offer to the institution.
Dr. Wiese is excited about train-the-trainer pre-courses now being designed for SHM’s 2008 annual meeting. These courses, he says, will train academic hospitalists to teach issues that are not only important to residency programs but “right up the alley of the hospitalist: namely, systems of care and practice-based learning.” In this way, he explains, academic hospitalists could have an “exponential effect” on furthering the profession.
Recruitment and Retention
Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine in Atlanta, is “significantly concerned” about attracting academic hospitalists. The 60+ hospitalists in his group staff five community hospitals (two of which have teaching services) in addition to the system’s tertiary care center. At that hospital, he says, patient acuity is appreciably higher, which means hospitalists must spend more time caring for patients and relating to their family members—time that does not translate into more billable relative value units (RVUs). This type of work environment is definitely “a difficult sell” to potential new hires, he notes. “There is … a balance between patient care and teaching in an academic environment, and maintaining that ‘right balance’ is always a challenge.”
System changes to reward educational prep time, such as the EVU Dr. Wiese mentioned, may be one solution to achieving a patient care/teaching time balance, agrees Dr. Dressler. “I think it’s an excellent idea to have some sort of measure that you can utilize to help reward physicians for putting an emphasis on education—actually promoting and executing educational efforts,” he says. Emory’s program is piloting a mechanism that would objectively measure clinicians’ self-identified efforts to set educational standards. Rewards (e.g., financial recognition or awards for “best teacher” and so on) could be built into the effort, he says.
Hospitalists face an uphill battle to secure funding for research, admits Dr. Wiese: “There is not the same level of NIH [National Institutes of Health] funding for quality improvement that there is for basic science research. And the QI funding that is available does not bring the same salary coverage that the basic science researchers are bringing to the department.”
Hospitalists need to be creative in defining their research agenda and funding streams. Dr. Basaviah says that if hospital medicine leaders emphasize the value of their systems-based quality improvement efforts, they may be able to secure funding for QI research efforts from “the hospital/medical center administration, Department of Medicine, QI group/division, or from residency programs, depending on where their efforts are going to be the most closely aligned.”
Avert Burnout
Tapping into SHM’s resources can foster community and allow younger hospitalists a method for charting a career path. Dr. McKean’s Career Satisfaction Task Force will soon release a white paper relating to the four pillars of career satisfaction: control/autonomy, reward/recognition, workload/schedule, and community environment. Questionnaires for individual hospitalists and physician leaders will help both groups identify the best job for an individual or the most appropriate person for a position. Included in the group’s analysis of career sustainability and satisfaction are organizational, system, professional development, and marketing-relationship strategies to help hospitalists assess job satisfaction. It is the task force’s hope that the document can be a useful tool in interactions with hospital administrators as well, to demonstrate the elements necessary for staff satisfaction and retention.
“A surgeon would never operate without a multidisciplinary team in the operating room,” says Dr. McKean. “And yet, because they’ve done order entry, they’ve done resident-level duties, hospitalists across the country are expected to step up without any resources to meet service demands relating to a shortage of residents and high census conditions. Performing residency-level duties not only undermines job satisfaction but also [affects] how efficiently hospitalists can care for a large number of patients. Hospitalists need to be given the tools to be efficient and improve the quality of care in the hospital.”
Fulfillment of Teaching
When asked what keeps him in academics despite lower remuneration rates, Dr. Wiese expresses the same sentiment as his colleagues: “It’s all about fulfillment. I like interacting with people and seeing them get better. If you train residents in the right way and then train them to train others, then suddenly your affect in improving quality of care and education has an exponential effect around the country.”
Dr. Dressler agrees. “Obviously, not everyone wants to do academic medicine, and you must have some interest in teaching and training others,” he says. But more important than financial remuneration, he notes, is “overall job satisfaction and being happy with the people you work with, as well as the patients you’re taking care of and the teaching that you’re doing.” That’s why hospitalists and faculty should work toward building recognition into the system. Hospitalist leaders can advocate for the mechanisms necessary, “to make sure that physicians also have time to have a life, to relax, and to enjoy their profession,” says Dr. Dressler.
“When I hire hospitalists, my goal is to hire people interested not only in good quality, efficient inpatient care but also in teaching,” said Dr. Amin. “I will easily tell them that they can probably make more money and have a better lifestyle working as a community hospitalist if they don’t want to deal with this other mission [of teaching].”
“I think if we view our work as just a job rather than as a career or profession that can be fulfilling, we may be led to paths of potential burnout,” said Dr. Basaviah. “Many of us view the healthcare profession with a notion of service and a vision for a satisfying career. I think that it’s important for all of us to facilitate the ability of our colleagues to thrive in these careers.” TH
Gretchen Henkel has written for The Hospitalist since 2005.
As clinicians and educators, academic hospitalists function within several arenas: They are role models and teachers in the inpatient arena, but they also feel pressure from hospital administration to meet throughput and capacity goals. In addition, hospitalist clinician-educators are expected to be leaders in quality improvement.
But are the rewards for academic hospitalists commensurate with the demands placed upon them? Even as hospitalists prove their worth to hospital administrators, many clinician-educators find themselves pulled between time spent on service and time for the academic pursuits necessary to improve resident education and merit faculty promotions.
“In my current situation, there is difficulty in fitting in the prep work time for teaching rounds,” says Elizabeth A. Schultz, MD, who practices with the Adult Hospitalist Team at Swedish Medical Center in Seattle and is also affiliated with the University of Washington School of Medicine. “There’s really no time for that, other than time on my own—and I’m actually in a really good situation right now where my boss has capped the number of patients I see in a day and afforded me the ability to go to conferences, do teaching rounds, and to really focus on resident and medical student education.”
Dr. Schultz is not alone in struggling to balance clinical and educational duties. Many hospital medicine leaders wrestle with these concerns, aware that growing clinical responsibilities impinge on teaching time and that the sustainability of hospital medicine as a career is at stake.
Confront the Dilemma
An October 2006 survey by the University HealthSystem Consortium confirmed that hospitalists have improved the educational process for residents and medical students, but it also identified impediments to the continuation and growth of hospitalist programs. (The Benchmarking Study, “Role of the Hospitalist,” is available online to University HealthSystem Consortium (UHC) members and registered website users at www.uhc.edu.) The most common barrier is the difficulty in attracting and retaining quality candidates, given the ratio of salary to workload, the potential for burnout, and undefined career paths.
“There is a significant amount of demand on one small group of physicians, and we haven’t necessarily found a way to compensate them for the different roles they play,” reflects Alpesh Amin, MD, MBA, FACP, associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California at Irvine (UCI), where he founded the UCI hospitalist program in 1998 and serves as its executive director. “These three arenas that hospitalists have to constantly keep moving in are not always complementary. How do you spend more time facilitating the teaching mission versus time facilitating the throughput mission or the expanding clinical mission?”
Meeting goals for academic appointments adds yet another layer of role conflict, he notes.
Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston and chair of SHM’s Career Satisfaction Task Force, also acknowledges the tensions between clinical duties and academic pursuits. “If you have 20 patients to see and discharge and yet you also have a grant to write, guess what’s not going to get done?”
To be fair, academic hospitalists experience their situations in different ways. Kathleen Bradford, MD, the inpatient director of the University of North Carolina (UNC) Children’s Hospital, director of the Pediatric Hospitalist Program, and assistant residency director for the Division of General Pediatrics at UNC in Chapel Hill, N.C., has not experienced a huge conflict between her teaching and clinical duties, but she has noticed that there are fewer opportunities for teaching, given the increased clinical demands on physicians and the decreased availability of residents.
“I’ve always felt that medicine—and especially medical teaching—is like an apprenticeship,” she explains. “There are many, many opportunities to teach while doing in an apprenticeship-like fashion. The demands of taking care of patients and [reduced] resident work hours have certainly decreased the ability to do more formal and didactic or classroom-type teaching. However, the opportunities for spontaneous or ‘teach as you go’ education still exist.”
Solutions to the Time Crunch
Dr. Schultz, a member of the Swedish Medical Center’s teaching service who leads a teaching team every month, admits she has no answers to the time crunch academic hospitalists experience. “There just isn’t enough manpower,” she says. “The hospital doesn’t get paid for people to teach, and to pay people to have dedicated time to pursue academic research or prepare lectures just isn’t feasible for most hospitals, as they are already struggling to make ends meet.”
Many hospitals employ both non-teaching and teaching services to ensure night and weekend coverage. But this can create other dilemmas for the academic hospitalist. For instance, Dr. Schultz says her teaching service gets the more complicated and critically ill patients who require more of her time, thus squeezing out, again, the opportunity to prepare lecture notes or conduct research.
At UNC Children’s Hospital, the pediatric hospitalist program is in its infancy, having launched in fall 2006, and the new service is mostly a non-teaching service. Dr. Bradford reports that the teaching and the hospitalist service are assigning patients on a case-by-case basis. “There is [teaching] value in all patients and all cases,” says Dr. Bradford, “but it’s really hard to say which ones have the most value: Should it be the patient who has a short stay with a common illness or a patient who has been chronically ill and in the hospital for 100 days? It’s hard to know.”
At Brigham and Women’s Hospital, Dr. McKean reports the hospitalist group did not want to institute a two-tiered [teaching and non-teaching] hospitalist program, so one of their hospitalists, Chris Roy, MD, created a Physician Assistant Clinician Educator (PACE) service, with a hospitalist supervising two PAs during daytime hours; it’s supplemented by moonlighters at night. Members of this service have teaching responsibilities and are involved in curriculum development for physician assistants and students. Additional research is needed to examine outcomes of educational efforts directed toward the multidisciplinary team in the core competency areas elaborated by the Accreditation Council for Graduate Medical Education, explains Dr. McKean.
Proactive Strategies
Whatever strategies are used to address case workloads, effecting real change for academic hospitalists—ensuring protected time as well as rewards for educational and research pursuits—will require clear-sighted planning from hospitalist leaders. “The bottom line is to proactively manage the program’s direction and growth,” asserts Dr. McKean. “Instead of being everybody’s Band-Aid and being everything to everybody, it’s important to have a strategic plan. You can’t necessarily plan for five years, but you can plan for three, and you could do things in a step-wise manner to increase the academic and research presence.”
This is precisely where SHM’s emphasis on networking and mentoring can come in, believes SHM’s Education Committee Chair Preetha Basaviah, MD, clinical associate professor of medicine and associate course director, Practice of Medicine, at Stanford University School of Medicine, California. SHM has led many initiatives, such as the publication of the Core Competencies and the creation of Web-based quality improvement resource rooms, which help provide curriculum support.
“What we’ve done as an education committee is to help provide some of the resources, support, and advocacy that our members need so that they can go back to their programs and say, ‘These are the national standards and resources provided by an organization that advocates for us.’ ” says Dr. Basaviah.
Creating a network of hospitalists, both regionally and nationally, provides opportunities to gain protected time for research pursuits and recognition from one’s peers, Dr. Basaviah continues. “I think what we’ve done for clinician educators is to promote thinking proactively about your short-term and long-term career goals, including developing an area of expertise, before you take on commitments,” she says.
Input with Curricular Design
Dr. Amin’s role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his role on the Core Competencies Task Force. He believes it is through such initiatives that hospitalists can become leaders in their institutions, participating in curriculum development as well as quality and performance improvement efforts.
“I don’t view myself as just working for the hospital or … for the School [of Medicine]. I view myself as working for the enterprise,” he says. As a result his hospitalist group has taken the lead in designing various residency inpatient curricula. “If you do it right, you could actually design curricula to educate residents about heart failure—teaching them about the pathophysiology and disease management—but then also teach them about core measures, outcomes, and systems-based practice in heart failure,” he says. “When all that comes together, I think you’re making some progress.”
Jeffrey G. Wiese, MD, vice chairman and director of the Internal Medicine Residency Program at Tulane University, New Orleans, is the leader of the SHM Task Force for Integrating Core Competencies into Residency Education. He points to the SHM Academic Task Force’s idea of developing an EVU, or educational value unit, that would define and compensate for amounts of time invested in educational pursuits. He would also like to see SHM take a role in developing standards and recommendations for promotion criteria. These are tools that academic hospitalists could use to “make their case” to medical schools’ residency programs about the value they offer to the institution.
Dr. Wiese is excited about train-the-trainer pre-courses now being designed for SHM’s 2008 annual meeting. These courses, he says, will train academic hospitalists to teach issues that are not only important to residency programs but “right up the alley of the hospitalist: namely, systems of care and practice-based learning.” In this way, he explains, academic hospitalists could have an “exponential effect” on furthering the profession.
Recruitment and Retention
Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine in Atlanta, is “significantly concerned” about attracting academic hospitalists. The 60+ hospitalists in his group staff five community hospitals (two of which have teaching services) in addition to the system’s tertiary care center. At that hospital, he says, patient acuity is appreciably higher, which means hospitalists must spend more time caring for patients and relating to their family members—time that does not translate into more billable relative value units (RVUs). This type of work environment is definitely “a difficult sell” to potential new hires, he notes. “There is … a balance between patient care and teaching in an academic environment, and maintaining that ‘right balance’ is always a challenge.”
System changes to reward educational prep time, such as the EVU Dr. Wiese mentioned, may be one solution to achieving a patient care/teaching time balance, agrees Dr. Dressler. “I think it’s an excellent idea to have some sort of measure that you can utilize to help reward physicians for putting an emphasis on education—actually promoting and executing educational efforts,” he says. Emory’s program is piloting a mechanism that would objectively measure clinicians’ self-identified efforts to set educational standards. Rewards (e.g., financial recognition or awards for “best teacher” and so on) could be built into the effort, he says.
Hospitalists face an uphill battle to secure funding for research, admits Dr. Wiese: “There is not the same level of NIH [National Institutes of Health] funding for quality improvement that there is for basic science research. And the QI funding that is available does not bring the same salary coverage that the basic science researchers are bringing to the department.”
Hospitalists need to be creative in defining their research agenda and funding streams. Dr. Basaviah says that if hospital medicine leaders emphasize the value of their systems-based quality improvement efforts, they may be able to secure funding for QI research efforts from “the hospital/medical center administration, Department of Medicine, QI group/division, or from residency programs, depending on where their efforts are going to be the most closely aligned.”
Avert Burnout
Tapping into SHM’s resources can foster community and allow younger hospitalists a method for charting a career path. Dr. McKean’s Career Satisfaction Task Force will soon release a white paper relating to the four pillars of career satisfaction: control/autonomy, reward/recognition, workload/schedule, and community environment. Questionnaires for individual hospitalists and physician leaders will help both groups identify the best job for an individual or the most appropriate person for a position. Included in the group’s analysis of career sustainability and satisfaction are organizational, system, professional development, and marketing-relationship strategies to help hospitalists assess job satisfaction. It is the task force’s hope that the document can be a useful tool in interactions with hospital administrators as well, to demonstrate the elements necessary for staff satisfaction and retention.
“A surgeon would never operate without a multidisciplinary team in the operating room,” says Dr. McKean. “And yet, because they’ve done order entry, they’ve done resident-level duties, hospitalists across the country are expected to step up without any resources to meet service demands relating to a shortage of residents and high census conditions. Performing residency-level duties not only undermines job satisfaction but also [affects] how efficiently hospitalists can care for a large number of patients. Hospitalists need to be given the tools to be efficient and improve the quality of care in the hospital.”
Fulfillment of Teaching
When asked what keeps him in academics despite lower remuneration rates, Dr. Wiese expresses the same sentiment as his colleagues: “It’s all about fulfillment. I like interacting with people and seeing them get better. If you train residents in the right way and then train them to train others, then suddenly your affect in improving quality of care and education has an exponential effect around the country.”
Dr. Dressler agrees. “Obviously, not everyone wants to do academic medicine, and you must have some interest in teaching and training others,” he says. But more important than financial remuneration, he notes, is “overall job satisfaction and being happy with the people you work with, as well as the patients you’re taking care of and the teaching that you’re doing.” That’s why hospitalists and faculty should work toward building recognition into the system. Hospitalist leaders can advocate for the mechanisms necessary, “to make sure that physicians also have time to have a life, to relax, and to enjoy their profession,” says Dr. Dressler.
“When I hire hospitalists, my goal is to hire people interested not only in good quality, efficient inpatient care but also in teaching,” said Dr. Amin. “I will easily tell them that they can probably make more money and have a better lifestyle working as a community hospitalist if they don’t want to deal with this other mission [of teaching].”
“I think if we view our work as just a job rather than as a career or profession that can be fulfilling, we may be led to paths of potential burnout,” said Dr. Basaviah. “Many of us view the healthcare profession with a notion of service and a vision for a satisfying career. I think that it’s important for all of us to facilitate the ability of our colleagues to thrive in these careers.” TH
Gretchen Henkel has written for The Hospitalist since 2005.
As clinicians and educators, academic hospitalists function within several arenas: They are role models and teachers in the inpatient arena, but they also feel pressure from hospital administration to meet throughput and capacity goals. In addition, hospitalist clinician-educators are expected to be leaders in quality improvement.
But are the rewards for academic hospitalists commensurate with the demands placed upon them? Even as hospitalists prove their worth to hospital administrators, many clinician-educators find themselves pulled between time spent on service and time for the academic pursuits necessary to improve resident education and merit faculty promotions.
“In my current situation, there is difficulty in fitting in the prep work time for teaching rounds,” says Elizabeth A. Schultz, MD, who practices with the Adult Hospitalist Team at Swedish Medical Center in Seattle and is also affiliated with the University of Washington School of Medicine. “There’s really no time for that, other than time on my own—and I’m actually in a really good situation right now where my boss has capped the number of patients I see in a day and afforded me the ability to go to conferences, do teaching rounds, and to really focus on resident and medical student education.”
Dr. Schultz is not alone in struggling to balance clinical and educational duties. Many hospital medicine leaders wrestle with these concerns, aware that growing clinical responsibilities impinge on teaching time and that the sustainability of hospital medicine as a career is at stake.
Confront the Dilemma
An October 2006 survey by the University HealthSystem Consortium confirmed that hospitalists have improved the educational process for residents and medical students, but it also identified impediments to the continuation and growth of hospitalist programs. (The Benchmarking Study, “Role of the Hospitalist,” is available online to University HealthSystem Consortium (UHC) members and registered website users at www.uhc.edu.) The most common barrier is the difficulty in attracting and retaining quality candidates, given the ratio of salary to workload, the potential for burnout, and undefined career paths.
“There is a significant amount of demand on one small group of physicians, and we haven’t necessarily found a way to compensate them for the different roles they play,” reflects Alpesh Amin, MD, MBA, FACP, associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California at Irvine (UCI), where he founded the UCI hospitalist program in 1998 and serves as its executive director. “These three arenas that hospitalists have to constantly keep moving in are not always complementary. How do you spend more time facilitating the teaching mission versus time facilitating the throughput mission or the expanding clinical mission?”
Meeting goals for academic appointments adds yet another layer of role conflict, he notes.
Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston and chair of SHM’s Career Satisfaction Task Force, also acknowledges the tensions between clinical duties and academic pursuits. “If you have 20 patients to see and discharge and yet you also have a grant to write, guess what’s not going to get done?”
To be fair, academic hospitalists experience their situations in different ways. Kathleen Bradford, MD, the inpatient director of the University of North Carolina (UNC) Children’s Hospital, director of the Pediatric Hospitalist Program, and assistant residency director for the Division of General Pediatrics at UNC in Chapel Hill, N.C., has not experienced a huge conflict between her teaching and clinical duties, but she has noticed that there are fewer opportunities for teaching, given the increased clinical demands on physicians and the decreased availability of residents.
“I’ve always felt that medicine—and especially medical teaching—is like an apprenticeship,” she explains. “There are many, many opportunities to teach while doing in an apprenticeship-like fashion. The demands of taking care of patients and [reduced] resident work hours have certainly decreased the ability to do more formal and didactic or classroom-type teaching. However, the opportunities for spontaneous or ‘teach as you go’ education still exist.”
Solutions to the Time Crunch
Dr. Schultz, a member of the Swedish Medical Center’s teaching service who leads a teaching team every month, admits she has no answers to the time crunch academic hospitalists experience. “There just isn’t enough manpower,” she says. “The hospital doesn’t get paid for people to teach, and to pay people to have dedicated time to pursue academic research or prepare lectures just isn’t feasible for most hospitals, as they are already struggling to make ends meet.”
Many hospitals employ both non-teaching and teaching services to ensure night and weekend coverage. But this can create other dilemmas for the academic hospitalist. For instance, Dr. Schultz says her teaching service gets the more complicated and critically ill patients who require more of her time, thus squeezing out, again, the opportunity to prepare lecture notes or conduct research.
At UNC Children’s Hospital, the pediatric hospitalist program is in its infancy, having launched in fall 2006, and the new service is mostly a non-teaching service. Dr. Bradford reports that the teaching and the hospitalist service are assigning patients on a case-by-case basis. “There is [teaching] value in all patients and all cases,” says Dr. Bradford, “but it’s really hard to say which ones have the most value: Should it be the patient who has a short stay with a common illness or a patient who has been chronically ill and in the hospital for 100 days? It’s hard to know.”
At Brigham and Women’s Hospital, Dr. McKean reports the hospitalist group did not want to institute a two-tiered [teaching and non-teaching] hospitalist program, so one of their hospitalists, Chris Roy, MD, created a Physician Assistant Clinician Educator (PACE) service, with a hospitalist supervising two PAs during daytime hours; it’s supplemented by moonlighters at night. Members of this service have teaching responsibilities and are involved in curriculum development for physician assistants and students. Additional research is needed to examine outcomes of educational efforts directed toward the multidisciplinary team in the core competency areas elaborated by the Accreditation Council for Graduate Medical Education, explains Dr. McKean.
Proactive Strategies
Whatever strategies are used to address case workloads, effecting real change for academic hospitalists—ensuring protected time as well as rewards for educational and research pursuits—will require clear-sighted planning from hospitalist leaders. “The bottom line is to proactively manage the program’s direction and growth,” asserts Dr. McKean. “Instead of being everybody’s Band-Aid and being everything to everybody, it’s important to have a strategic plan. You can’t necessarily plan for five years, but you can plan for three, and you could do things in a step-wise manner to increase the academic and research presence.”
This is precisely where SHM’s emphasis on networking and mentoring can come in, believes SHM’s Education Committee Chair Preetha Basaviah, MD, clinical associate professor of medicine and associate course director, Practice of Medicine, at Stanford University School of Medicine, California. SHM has led many initiatives, such as the publication of the Core Competencies and the creation of Web-based quality improvement resource rooms, which help provide curriculum support.
“What we’ve done as an education committee is to help provide some of the resources, support, and advocacy that our members need so that they can go back to their programs and say, ‘These are the national standards and resources provided by an organization that advocates for us.’ ” says Dr. Basaviah.
Creating a network of hospitalists, both regionally and nationally, provides opportunities to gain protected time for research pursuits and recognition from one’s peers, Dr. Basaviah continues. “I think what we’ve done for clinician educators is to promote thinking proactively about your short-term and long-term career goals, including developing an area of expertise, before you take on commitments,” she says.
Input with Curricular Design
Dr. Amin’s role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his role on the Core Competencies Task Force. He believes it is through such initiatives that hospitalists can become leaders in their institutions, participating in curriculum development as well as quality and performance improvement efforts.
“I don’t view myself as just working for the hospital or … for the School [of Medicine]. I view myself as working for the enterprise,” he says. As a result his hospitalist group has taken the lead in designing various residency inpatient curricula. “If you do it right, you could actually design curricula to educate residents about heart failure—teaching them about the pathophysiology and disease management—but then also teach them about core measures, outcomes, and systems-based practice in heart failure,” he says. “When all that comes together, I think you’re making some progress.”
Jeffrey G. Wiese, MD, vice chairman and director of the Internal Medicine Residency Program at Tulane University, New Orleans, is the leader of the SHM Task Force for Integrating Core Competencies into Residency Education. He points to the SHM Academic Task Force’s idea of developing an EVU, or educational value unit, that would define and compensate for amounts of time invested in educational pursuits. He would also like to see SHM take a role in developing standards and recommendations for promotion criteria. These are tools that academic hospitalists could use to “make their case” to medical schools’ residency programs about the value they offer to the institution.
Dr. Wiese is excited about train-the-trainer pre-courses now being designed for SHM’s 2008 annual meeting. These courses, he says, will train academic hospitalists to teach issues that are not only important to residency programs but “right up the alley of the hospitalist: namely, systems of care and practice-based learning.” In this way, he explains, academic hospitalists could have an “exponential effect” on furthering the profession.
Recruitment and Retention
Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine in Atlanta, is “significantly concerned” about attracting academic hospitalists. The 60+ hospitalists in his group staff five community hospitals (two of which have teaching services) in addition to the system’s tertiary care center. At that hospital, he says, patient acuity is appreciably higher, which means hospitalists must spend more time caring for patients and relating to their family members—time that does not translate into more billable relative value units (RVUs). This type of work environment is definitely “a difficult sell” to potential new hires, he notes. “There is … a balance between patient care and teaching in an academic environment, and maintaining that ‘right balance’ is always a challenge.”
System changes to reward educational prep time, such as the EVU Dr. Wiese mentioned, may be one solution to achieving a patient care/teaching time balance, agrees Dr. Dressler. “I think it’s an excellent idea to have some sort of measure that you can utilize to help reward physicians for putting an emphasis on education—actually promoting and executing educational efforts,” he says. Emory’s program is piloting a mechanism that would objectively measure clinicians’ self-identified efforts to set educational standards. Rewards (e.g., financial recognition or awards for “best teacher” and so on) could be built into the effort, he says.
Hospitalists face an uphill battle to secure funding for research, admits Dr. Wiese: “There is not the same level of NIH [National Institutes of Health] funding for quality improvement that there is for basic science research. And the QI funding that is available does not bring the same salary coverage that the basic science researchers are bringing to the department.”
Hospitalists need to be creative in defining their research agenda and funding streams. Dr. Basaviah says that if hospital medicine leaders emphasize the value of their systems-based quality improvement efforts, they may be able to secure funding for QI research efforts from “the hospital/medical center administration, Department of Medicine, QI group/division, or from residency programs, depending on where their efforts are going to be the most closely aligned.”
Avert Burnout
Tapping into SHM’s resources can foster community and allow younger hospitalists a method for charting a career path. Dr. McKean’s Career Satisfaction Task Force will soon release a white paper relating to the four pillars of career satisfaction: control/autonomy, reward/recognition, workload/schedule, and community environment. Questionnaires for individual hospitalists and physician leaders will help both groups identify the best job for an individual or the most appropriate person for a position. Included in the group’s analysis of career sustainability and satisfaction are organizational, system, professional development, and marketing-relationship strategies to help hospitalists assess job satisfaction. It is the task force’s hope that the document can be a useful tool in interactions with hospital administrators as well, to demonstrate the elements necessary for staff satisfaction and retention.
“A surgeon would never operate without a multidisciplinary team in the operating room,” says Dr. McKean. “And yet, because they’ve done order entry, they’ve done resident-level duties, hospitalists across the country are expected to step up without any resources to meet service demands relating to a shortage of residents and high census conditions. Performing residency-level duties not only undermines job satisfaction but also [affects] how efficiently hospitalists can care for a large number of patients. Hospitalists need to be given the tools to be efficient and improve the quality of care in the hospital.”
Fulfillment of Teaching
When asked what keeps him in academics despite lower remuneration rates, Dr. Wiese expresses the same sentiment as his colleagues: “It’s all about fulfillment. I like interacting with people and seeing them get better. If you train residents in the right way and then train them to train others, then suddenly your affect in improving quality of care and education has an exponential effect around the country.”
Dr. Dressler agrees. “Obviously, not everyone wants to do academic medicine, and you must have some interest in teaching and training others,” he says. But more important than financial remuneration, he notes, is “overall job satisfaction and being happy with the people you work with, as well as the patients you’re taking care of and the teaching that you’re doing.” That’s why hospitalists and faculty should work toward building recognition into the system. Hospitalist leaders can advocate for the mechanisms necessary, “to make sure that physicians also have time to have a life, to relax, and to enjoy their profession,” says Dr. Dressler.
“When I hire hospitalists, my goal is to hire people interested not only in good quality, efficient inpatient care but also in teaching,” said Dr. Amin. “I will easily tell them that they can probably make more money and have a better lifestyle working as a community hospitalist if they don’t want to deal with this other mission [of teaching].”
“I think if we view our work as just a job rather than as a career or profession that can be fulfilling, we may be led to paths of potential burnout,” said Dr. Basaviah. “Many of us view the healthcare profession with a notion of service and a vision for a satisfying career. I think that it’s important for all of us to facilitate the ability of our colleagues to thrive in these careers.” TH
Gretchen Henkel has written for The Hospitalist since 2005.
Charts to Screens
Federal policy makers have set 2014 as the target year for all Americans to have an electronic health record. While researchers claim that health information technology (IT) holds great promise to improve the quality and efficiency of healthcare delivery, the path to effecting the transition to computer-based documentation systems is fraught with obstacles. In addition to large initial capital investments for upgraded hardware and software, hospitals face other barriers to IT adoption. The challenges experienced by hospitals making this change include steep learning curves, workflow disruptions, and time delays.

—Richard Todd, MD
Advancements and Glitches
A 2005 American Hospital Association (AHA) survey of 900 community hospitals found a wide range of IT usage. Some hospitals have completed installation of bar coding for medication management, while a small minority are using advanced computerized physician order entry (CPOE) systems.1 Typical of many hospitals in the AHA survey, Abbott Northwestern Hospital in Minneapolis chose an incremental IT implementation approach.
Academic hospitalist Debra L. Burgy, MD, is the lead physician in Abbott Northwestern General Medicine Associates Group, affiliated with the internal medicine program at the University of Minnesota (Minneapolis), where she is also adjunct assistant professor of medicine. Hers was the first group of physicians to go live with the hospital’s electronic documentation system 16 months ago, in July of 2005.
“We went up on July 1 because we thought it might be an advantage to have a long weekend with a lower census,” she recalls. As it turned out, her group of academic hospitalists was caught short-staffed on the holiday weekend, having to adjust to their new IT roles, take care of patients, and orient the brand-new interns.
“It was kind of a sad weekend for me,” she remarks wryly.
Of the launch in July 2005, Dr. Burgy observes that the learning curve “was longer than I expected, but once you achieve it and you’re adept at most of the functions I do find [electronic documentation] better overall in many ways.”
One advantage: As an academic hospitalist, she consults with her residents and emergency department admitting physicians in real time by pulling up patients’ charts from any location.
Dr. Burgy and her colleagues still find the time required to enter the narrative part of the patient’s history of present illness difficult, as well as the discharge notes. Another bug: The system is designed to prompt the physician to complete medication reconciliation (Medication Administration Record, or MAR) at admission, transfer, and discharge. Because the medications are not organized in alphabetical order or side by side, however, the logistics of reconciling more than a few medications can be frustrating.
“Most of us end up printing out the current MAR, which seems to defeat the purpose of the computerized record,” says Dr. Burgy.
A Staged Approach

According to Mary A. Dallas, MD, chief medical information officer for Presbyterian Healthcare Services (PHS), an integrated healthcare delivery network in Albuquerque, N.M., PHS launched CPOE in the main hospital’s inpatient services area as the final step in the pharmacy automation process designed to improve patient safety and prevent medication errors.
Five years ago, the main hospital began the process of developing a closed-loop pharmacy order system. Now, with this system in place, medication orders go directly from the physician’s fingertips to a pharmacy work queue. The verified drug order is then messaged to the pharmacy robot for packaging. On the floor, nurses’ hand-held devices flash a message that the drug order is ready. Upon delivery to the floor, a nurse scans the bar code on the packaged medication, matches it to the patient’s bracelet bar code, and scans his or her badge before administering the medication. This verifies the 5 “Rs” of medication safety: right medication, right dose, right route, right patient, and right time, as well as concurrently creating the electronic MAR.
As the former medical director of the hospital’s Adult Hospitalist Service, Dr. Dallas understands the physician’s point of view. When launching the hospital’s CPOE, she was aware that, “especially in the hospitalist arena, we were adding some extra learning curve to their day.”
She also admits, “It does take longer to log onto a computer system and wait for the program to boot than it does to just scribble a medication order on paper. There’s no way to avoid that.”
As she has worked to build order sets tailored for various specialties, however, Dr. Dallas has been sensitive to challenges that can be softened. Automatic prompts at the point of order entry are carefully monitored, she points out because “surplus of medication” alert pop-ups can sometimes produce physician “alert fatigue,” and doctors may begin to ignore—rather than address—the alerts. “You have to start light and then work to get more stringent as people tolerate and get used to that system,” she says.
Getting Physician Buy-In
The launch of the CPOE system at Presbyterian Hospital in Albuquerque was the fourth such experience for Richard Todd, MD, medical director of the hospital’s Adult Hospitalist Group. He sees speed—or the lack thereof—as a major barrier to physician adoption of computerized documentation systems. He has observed that some hospitals don’t invest in the appropriate hardware required to handle such technically demanding software. As a result, a user may have to wait 25 or 30 seconds for an order entry system to boot up.
“That is an eternity in computing time,” he says, and a physician who experiences this difficulty more than twice may no longer have the patience to work with the system.

—Richard H. Bailey, MD
Physicians should be part of the IT design and selection process, Dr. Todd believes. “To get a successful adoption by physicians, the engineers need to come to the physicians’ table and not the other way around,” he says, pointing to the success of Wiz Order, Vanderbilt University School of Medicine’s order-entry system, which is part of an electronic medical record custom-built with input from doctors.
“The biggest mistake you can make is to have physicians feel that you’re forcing something down their throats that slows them down,” says Dr. Todd. “Every physician is under tremendous time pressure to get the primary job done, so if you do anything that even makes them perceive that it’s going to make them less efficient, you’re not going to get buy-in.”
S. Trent Rosenbloom, MD, MPH, trained as an internist and pediatrician and spent some time as a hospitalist early in his career. Currently, he is assistant professor in the departments of Biomedical Informatics, Internal Medicine, and Pediatrics, and in the School of Nursing at Vanderbilt University Medical Center. He and his research colleagues have investigated the factors which influence providers’ perceptions of clinical documentation tools.2
“The key issue is not so much time, but the perception of time and work flow,” he explains. “It [a computerized documentation system] could be twice as fast, but if I have to go out of my way to do it, then I might perceive it as taking more effort and more time.”
For instance, writing a drug order on paper can appear to be a faster process than finding a computer, sitting down, logging on to the system, finding the patient in the menu, opening the patient file, and then entering a drug order. Dr. Rosenbloom points out that when physicians think about these two processes, however, they may not factor in the other time factors for the paper order, such as walking to the chart, finding the chart, turning to the right page, and entering the drug order. And although computer systems are not error-free, CPOE tends to reduce transcription and other errors that in themselves can be time-consuming, if not life threatening, for the patient.
Keys to Success
Sources agreed that IT adoption by physicians increases in direct proportion to their participation in the process. “[Hospitalists and other physicians] need to make sure that their hospital includes physicians in every step of the due diligence process: looking through systems, going to the sales, actually banging on the product, and making sure that they perceive it as meeting their needs,” advises Dr. Rosenbloom.
Vendors differ in their methods for bringing client hospitals online. “A staged approach is probably best, based on what we know currently,” he suggests.
Finally, flexibility is key—for vendors and users. Dr. Rosenbloom advises teams to “expect to fail, and learn from that.” It’s important to recognize, he says, “that even if you’re putting in a computer system that has been implemented in 50% of hospitals—which hasn’t yet happened—there are idiosyncrasies and differences in your own center that will cause the implementation process to be different.”
Given hospitalists’ interest in hospital processes, leading the IT adoption effort is a natural role for hospitalist leaders, believes Richard H. Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital in Weston, Wis. “I was one of the most computer illiterate people I knew,” he relates. “But somehow, I got thrown into the role. We took a potential lemon, embraced it early on, and made lemonade.” TH
Gretchen Henkel also writes about benchmarking hospital medicine programs in this issue.
References
- American Hospital Association. Forward momentum: hospital use of information technology. October 2005. Available at: www.aha.org/aha/research-and-trends/AHA-policy-research/2005.html. Last accessed November 29, 2006.
- Rosenbloom ST, Crow AN, Blackford JU, et al. Cognitive factors influencing perceptions of clinical documentation tools. J Biomed Inform. 2006 Jul 8; [Epub ahead of print].
Federal policy makers have set 2014 as the target year for all Americans to have an electronic health record. While researchers claim that health information technology (IT) holds great promise to improve the quality and efficiency of healthcare delivery, the path to effecting the transition to computer-based documentation systems is fraught with obstacles. In addition to large initial capital investments for upgraded hardware and software, hospitals face other barriers to IT adoption. The challenges experienced by hospitals making this change include steep learning curves, workflow disruptions, and time delays.
—Richard Todd, MD
Advancements and Glitches
A 2005 American Hospital Association (AHA) survey of 900 community hospitals found a wide range of IT usage. Some hospitals have completed installation of bar coding for medication management, while a small minority are using advanced computerized physician order entry (CPOE) systems.1 Typical of many hospitals in the AHA survey, Abbott Northwestern Hospital in Minneapolis chose an incremental IT implementation approach.
Academic hospitalist Debra L. Burgy, MD, is the lead physician in Abbott Northwestern General Medicine Associates Group, affiliated with the internal medicine program at the University of Minnesota (Minneapolis), where she is also adjunct assistant professor of medicine. Hers was the first group of physicians to go live with the hospital’s electronic documentation system 16 months ago, in July of 2005.
“We went up on July 1 because we thought it might be an advantage to have a long weekend with a lower census,” she recalls. As it turned out, her group of academic hospitalists was caught short-staffed on the holiday weekend, having to adjust to their new IT roles, take care of patients, and orient the brand-new interns.
“It was kind of a sad weekend for me,” she remarks wryly.
Of the launch in July 2005, Dr. Burgy observes that the learning curve “was longer than I expected, but once you achieve it and you’re adept at most of the functions I do find [electronic documentation] better overall in many ways.”
One advantage: As an academic hospitalist, she consults with her residents and emergency department admitting physicians in real time by pulling up patients’ charts from any location.
Dr. Burgy and her colleagues still find the time required to enter the narrative part of the patient’s history of present illness difficult, as well as the discharge notes. Another bug: The system is designed to prompt the physician to complete medication reconciliation (Medication Administration Record, or MAR) at admission, transfer, and discharge. Because the medications are not organized in alphabetical order or side by side, however, the logistics of reconciling more than a few medications can be frustrating.
“Most of us end up printing out the current MAR, which seems to defeat the purpose of the computerized record,” says Dr. Burgy.
A Staged Approach
According to Mary A. Dallas, MD, chief medical information officer for Presbyterian Healthcare Services (PHS), an integrated healthcare delivery network in Albuquerque, N.M., PHS launched CPOE in the main hospital’s inpatient services area as the final step in the pharmacy automation process designed to improve patient safety and prevent medication errors.
Five years ago, the main hospital began the process of developing a closed-loop pharmacy order system. Now, with this system in place, medication orders go directly from the physician’s fingertips to a pharmacy work queue. The verified drug order is then messaged to the pharmacy robot for packaging. On the floor, nurses’ hand-held devices flash a message that the drug order is ready. Upon delivery to the floor, a nurse scans the bar code on the packaged medication, matches it to the patient’s bracelet bar code, and scans his or her badge before administering the medication. This verifies the 5 “Rs” of medication safety: right medication, right dose, right route, right patient, and right time, as well as concurrently creating the electronic MAR.
As the former medical director of the hospital’s Adult Hospitalist Service, Dr. Dallas understands the physician’s point of view. When launching the hospital’s CPOE, she was aware that, “especially in the hospitalist arena, we were adding some extra learning curve to their day.”
She also admits, “It does take longer to log onto a computer system and wait for the program to boot than it does to just scribble a medication order on paper. There’s no way to avoid that.”
As she has worked to build order sets tailored for various specialties, however, Dr. Dallas has been sensitive to challenges that can be softened. Automatic prompts at the point of order entry are carefully monitored, she points out because “surplus of medication” alert pop-ups can sometimes produce physician “alert fatigue,” and doctors may begin to ignore—rather than address—the alerts. “You have to start light and then work to get more stringent as people tolerate and get used to that system,” she says.
Getting Physician Buy-In
The launch of the CPOE system at Presbyterian Hospital in Albuquerque was the fourth such experience for Richard Todd, MD, medical director of the hospital’s Adult Hospitalist Group. He sees speed—or the lack thereof—as a major barrier to physician adoption of computerized documentation systems. He has observed that some hospitals don’t invest in the appropriate hardware required to handle such technically demanding software. As a result, a user may have to wait 25 or 30 seconds for an order entry system to boot up.
“That is an eternity in computing time,” he says, and a physician who experiences this difficulty more than twice may no longer have the patience to work with the system.
—Richard H. Bailey, MD
Physicians should be part of the IT design and selection process, Dr. Todd believes. “To get a successful adoption by physicians, the engineers need to come to the physicians’ table and not the other way around,” he says, pointing to the success of Wiz Order, Vanderbilt University School of Medicine’s order-entry system, which is part of an electronic medical record custom-built with input from doctors.
“The biggest mistake you can make is to have physicians feel that you’re forcing something down their throats that slows them down,” says Dr. Todd. “Every physician is under tremendous time pressure to get the primary job done, so if you do anything that even makes them perceive that it’s going to make them less efficient, you’re not going to get buy-in.”
S. Trent Rosenbloom, MD, MPH, trained as an internist and pediatrician and spent some time as a hospitalist early in his career. Currently, he is assistant professor in the departments of Biomedical Informatics, Internal Medicine, and Pediatrics, and in the School of Nursing at Vanderbilt University Medical Center. He and his research colleagues have investigated the factors which influence providers’ perceptions of clinical documentation tools.2
“The key issue is not so much time, but the perception of time and work flow,” he explains. “It [a computerized documentation system] could be twice as fast, but if I have to go out of my way to do it, then I might perceive it as taking more effort and more time.”
For instance, writing a drug order on paper can appear to be a faster process than finding a computer, sitting down, logging on to the system, finding the patient in the menu, opening the patient file, and then entering a drug order. Dr. Rosenbloom points out that when physicians think about these two processes, however, they may not factor in the other time factors for the paper order, such as walking to the chart, finding the chart, turning to the right page, and entering the drug order. And although computer systems are not error-free, CPOE tends to reduce transcription and other errors that in themselves can be time-consuming, if not life threatening, for the patient.
Keys to Success
Sources agreed that IT adoption by physicians increases in direct proportion to their participation in the process. “[Hospitalists and other physicians] need to make sure that their hospital includes physicians in every step of the due diligence process: looking through systems, going to the sales, actually banging on the product, and making sure that they perceive it as meeting their needs,” advises Dr. Rosenbloom.
Vendors differ in their methods for bringing client hospitals online. “A staged approach is probably best, based on what we know currently,” he suggests.
Finally, flexibility is key—for vendors and users. Dr. Rosenbloom advises teams to “expect to fail, and learn from that.” It’s important to recognize, he says, “that even if you’re putting in a computer system that has been implemented in 50% of hospitals—which hasn’t yet happened—there are idiosyncrasies and differences in your own center that will cause the implementation process to be different.”
Given hospitalists’ interest in hospital processes, leading the IT adoption effort is a natural role for hospitalist leaders, believes Richard H. Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital in Weston, Wis. “I was one of the most computer illiterate people I knew,” he relates. “But somehow, I got thrown into the role. We took a potential lemon, embraced it early on, and made lemonade.” TH
Gretchen Henkel also writes about benchmarking hospital medicine programs in this issue.
References
- American Hospital Association. Forward momentum: hospital use of information technology. October 2005. Available at: www.aha.org/aha/research-and-trends/AHA-policy-research/2005.html. Last accessed November 29, 2006.
- Rosenbloom ST, Crow AN, Blackford JU, et al. Cognitive factors influencing perceptions of clinical documentation tools. J Biomed Inform. 2006 Jul 8; [Epub ahead of print].
Federal policy makers have set 2014 as the target year for all Americans to have an electronic health record. While researchers claim that health information technology (IT) holds great promise to improve the quality and efficiency of healthcare delivery, the path to effecting the transition to computer-based documentation systems is fraught with obstacles. In addition to large initial capital investments for upgraded hardware and software, hospitals face other barriers to IT adoption. The challenges experienced by hospitals making this change include steep learning curves, workflow disruptions, and time delays.
—Richard Todd, MD
Advancements and Glitches
A 2005 American Hospital Association (AHA) survey of 900 community hospitals found a wide range of IT usage. Some hospitals have completed installation of bar coding for medication management, while a small minority are using advanced computerized physician order entry (CPOE) systems.1 Typical of many hospitals in the AHA survey, Abbott Northwestern Hospital in Minneapolis chose an incremental IT implementation approach.
Academic hospitalist Debra L. Burgy, MD, is the lead physician in Abbott Northwestern General Medicine Associates Group, affiliated with the internal medicine program at the University of Minnesota (Minneapolis), where she is also adjunct assistant professor of medicine. Hers was the first group of physicians to go live with the hospital’s electronic documentation system 16 months ago, in July of 2005.
“We went up on July 1 because we thought it might be an advantage to have a long weekend with a lower census,” she recalls. As it turned out, her group of academic hospitalists was caught short-staffed on the holiday weekend, having to adjust to their new IT roles, take care of patients, and orient the brand-new interns.
“It was kind of a sad weekend for me,” she remarks wryly.
Of the launch in July 2005, Dr. Burgy observes that the learning curve “was longer than I expected, but once you achieve it and you’re adept at most of the functions I do find [electronic documentation] better overall in many ways.”
One advantage: As an academic hospitalist, she consults with her residents and emergency department admitting physicians in real time by pulling up patients’ charts from any location.
Dr. Burgy and her colleagues still find the time required to enter the narrative part of the patient’s history of present illness difficult, as well as the discharge notes. Another bug: The system is designed to prompt the physician to complete medication reconciliation (Medication Administration Record, or MAR) at admission, transfer, and discharge. Because the medications are not organized in alphabetical order or side by side, however, the logistics of reconciling more than a few medications can be frustrating.
“Most of us end up printing out the current MAR, which seems to defeat the purpose of the computerized record,” says Dr. Burgy.
A Staged Approach
According to Mary A. Dallas, MD, chief medical information officer for Presbyterian Healthcare Services (PHS), an integrated healthcare delivery network in Albuquerque, N.M., PHS launched CPOE in the main hospital’s inpatient services area as the final step in the pharmacy automation process designed to improve patient safety and prevent medication errors.
Five years ago, the main hospital began the process of developing a closed-loop pharmacy order system. Now, with this system in place, medication orders go directly from the physician’s fingertips to a pharmacy work queue. The verified drug order is then messaged to the pharmacy robot for packaging. On the floor, nurses’ hand-held devices flash a message that the drug order is ready. Upon delivery to the floor, a nurse scans the bar code on the packaged medication, matches it to the patient’s bracelet bar code, and scans his or her badge before administering the medication. This verifies the 5 “Rs” of medication safety: right medication, right dose, right route, right patient, and right time, as well as concurrently creating the electronic MAR.
As the former medical director of the hospital’s Adult Hospitalist Service, Dr. Dallas understands the physician’s point of view. When launching the hospital’s CPOE, she was aware that, “especially in the hospitalist arena, we were adding some extra learning curve to their day.”
She also admits, “It does take longer to log onto a computer system and wait for the program to boot than it does to just scribble a medication order on paper. There’s no way to avoid that.”
As she has worked to build order sets tailored for various specialties, however, Dr. Dallas has been sensitive to challenges that can be softened. Automatic prompts at the point of order entry are carefully monitored, she points out because “surplus of medication” alert pop-ups can sometimes produce physician “alert fatigue,” and doctors may begin to ignore—rather than address—the alerts. “You have to start light and then work to get more stringent as people tolerate and get used to that system,” she says.
Getting Physician Buy-In
The launch of the CPOE system at Presbyterian Hospital in Albuquerque was the fourth such experience for Richard Todd, MD, medical director of the hospital’s Adult Hospitalist Group. He sees speed—or the lack thereof—as a major barrier to physician adoption of computerized documentation systems. He has observed that some hospitals don’t invest in the appropriate hardware required to handle such technically demanding software. As a result, a user may have to wait 25 or 30 seconds for an order entry system to boot up.
“That is an eternity in computing time,” he says, and a physician who experiences this difficulty more than twice may no longer have the patience to work with the system.
—Richard H. Bailey, MD
Physicians should be part of the IT design and selection process, Dr. Todd believes. “To get a successful adoption by physicians, the engineers need to come to the physicians’ table and not the other way around,” he says, pointing to the success of Wiz Order, Vanderbilt University School of Medicine’s order-entry system, which is part of an electronic medical record custom-built with input from doctors.
“The biggest mistake you can make is to have physicians feel that you’re forcing something down their throats that slows them down,” says Dr. Todd. “Every physician is under tremendous time pressure to get the primary job done, so if you do anything that even makes them perceive that it’s going to make them less efficient, you’re not going to get buy-in.”
S. Trent Rosenbloom, MD, MPH, trained as an internist and pediatrician and spent some time as a hospitalist early in his career. Currently, he is assistant professor in the departments of Biomedical Informatics, Internal Medicine, and Pediatrics, and in the School of Nursing at Vanderbilt University Medical Center. He and his research colleagues have investigated the factors which influence providers’ perceptions of clinical documentation tools.2
“The key issue is not so much time, but the perception of time and work flow,” he explains. “It [a computerized documentation system] could be twice as fast, but if I have to go out of my way to do it, then I might perceive it as taking more effort and more time.”
For instance, writing a drug order on paper can appear to be a faster process than finding a computer, sitting down, logging on to the system, finding the patient in the menu, opening the patient file, and then entering a drug order. Dr. Rosenbloom points out that when physicians think about these two processes, however, they may not factor in the other time factors for the paper order, such as walking to the chart, finding the chart, turning to the right page, and entering the drug order. And although computer systems are not error-free, CPOE tends to reduce transcription and other errors that in themselves can be time-consuming, if not life threatening, for the patient.
Keys to Success
Sources agreed that IT adoption by physicians increases in direct proportion to their participation in the process. “[Hospitalists and other physicians] need to make sure that their hospital includes physicians in every step of the due diligence process: looking through systems, going to the sales, actually banging on the product, and making sure that they perceive it as meeting their needs,” advises Dr. Rosenbloom.
Vendors differ in their methods for bringing client hospitals online. “A staged approach is probably best, based on what we know currently,” he suggests.
Finally, flexibility is key—for vendors and users. Dr. Rosenbloom advises teams to “expect to fail, and learn from that.” It’s important to recognize, he says, “that even if you’re putting in a computer system that has been implemented in 50% of hospitals—which hasn’t yet happened—there are idiosyncrasies and differences in your own center that will cause the implementation process to be different.”
Given hospitalists’ interest in hospital processes, leading the IT adoption effort is a natural role for hospitalist leaders, believes Richard H. Bailey, MD, medical director of Inpatient Care and Hospitalist Services at Saint Clare’s Hospital in Weston, Wis. “I was one of the most computer illiterate people I knew,” he relates. “But somehow, I got thrown into the role. We took a potential lemon, embraced it early on, and made lemonade.” TH
Gretchen Henkel also writes about benchmarking hospital medicine programs in this issue.
References
- American Hospital Association. Forward momentum: hospital use of information technology. October 2005. Available at: www.aha.org/aha/research-and-trends/AHA-policy-research/2005.html. Last accessed November 29, 2006.
- Rosenbloom ST, Crow AN, Blackford JU, et al. Cognitive factors influencing perceptions of clinical documentation tools. J Biomed Inform. 2006 Jul 8; [Epub ahead of print].
A Stake in the Sand
Productivity and compensation benchmarks can be useful when negotiating with hospital administrators for increased reimbursements and support resources, when recruiting hospitalists, and when conducting self-evaluations. For many of these processes, hospitalists—and, indeed, hospital administrators—turn to the information contained in the voluminous SHM 2005-2006 Survey, “The Authoritative Source on the State of the Hospital Medicine Movement.” (See “For More Information,” p. 32.)
With a response rate of 26%, the survey represents some 2,550 hospitalists across the nation, and its variables present a more comprehensive aerial view of hospital medicine than did previous surveys. But on the ground and in the trenches, hospital medicine groups must be careful to look at the survey’s metrics with a discerning eye.
When applying the survey metrics to one’s own practice, there can be benefits as well as pitfalls, cautions Joe Miller, SHM senior vice president and principal analyst of the survey data. He emphasizes the great variation among hospital medicine groups and warns against looking at survey medians as representing a “typical” hospital medicine practice.
“When you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” he quips. In several recent conversations, hospital medicine group leaders and SHM leaders involved in compiling the survey discussed the survey’s strengths and limitations as a benchmarking tool.
Healthy to Negotiate
According to the survey 97% of hospitalist programs receive some type of financial support. “Virtually every program in the country is challenged to defend the amount of money [they receive] or to negotiate for support dollars,” says Miller, who believes that negotiation can be a healthy dynamic. “There is a sense of equality of both sides of the table, a mutual respect between hospitalists and the hospital.” In the process of such negotiations, it will be important not to pin one’s position entirely to the survey metrics.
John Nelson, MD, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, a columnist for The Hospitalist (“Practice Management”), and a co-founder and past president of SHM, believes that some hospitalists mistakenly view the survey as SHM’s position on what a hospitalist should make. “The survey is the best information we have about what hospitalists do make—there is no better source—but it’s still a survey.”
Using compensation medians as yardsticks for actual salaries and compensation packages is analogous to “learning the average weight of an American and deciding that’s what we all should weigh—and that’s a big mistake,” he says. “If you hold up the survey as the governing document, then each party will use it to their advantage.”
Because the survey is regarded as the most authoritative existing source on hospitalists’ compensation and productivity, it nevertheless ends up being used as a benchmark, says Robin L. Dauterive, assistant director of the clinical hospitalist service at Massachusetts General Hospital in Boston.
“Whenever I’m preparing billings reports or dashboard measures—anything that shows my group’s workload—sooner or later, I always have to include something in there that states, ‘This is what other people are doing,’ ” says Dauterive. “It’s something that you can’t get away from, unfortunately, in medicine.”
She realizes that the survey does not purport to set any national standards, and yet, “all administrations want comparisons.” Dr. Nelson has also noted this phenomenon with the survey. In the absence of additional guidance, hospital executives and hospitalists often find that they’re just arguing about the survey. “And that’s unfortunate,” he says. “It means they’ve lost sight of the unique attributes of a given practice that might support higher or lower incomes and higher or lower workloads.”
View in Context
Hospitalists reading the survey for the first time might first seek to analyze the metrics regarding billings and collections. Here it is especially important not to view the reported numbers in isolation, says Dr. Nelson. For instance, to learn how a hospitalist’s annual gross charges (billings) compare with others across the country (question 12 of the Individual Hospitalist questionnaire—p. 87, Appendix 2), details on pages 251 and 252 supply pertinent variables. For instance, in comparing the four regions of the country, Table 056-A shows that the median annual gross charges for physicians in the south are highest, at $354,000. Hospitalists compensated by a 100% incentive method report higher charges per year ($392,000) than those who are on a 100% salary or a mix of the two methods of payment. Turning to Table 056-B, on page 252 of the published survey, hospitalists can find annual gross charges according to practitioner type, specialty, and employment model. Hospitalists should not stop their reading there, however, as a comparison of others’ annual gross collections might give a more complete picture.
Still, the SHM Survey does not reference all possible explanatory variables. Collections can be influenced by location and payer mix. Hospitalists practicing in a large urban hospital are likely to see more indigent patients for whom the hospital is not reimbursed. A careful reading of the survey should include the questionnaire and the tables supporting chapter conclusions, and the reader must recognize the survey’s limitations.
Apples to Oranges
IPC–The Hospitalist Company participates in the SHM survey and also uses it as a recruitment tool, reports IPC Vice President of Physician Staffing Timothy Lary. “We look at the income averages, and we’re able to demonstrate how our averages are, for the most part, higher than the averages,” he explains. “We also look at the survey from an internal viewpoint, but oftentimes you are comparing apples to oranges.”
Like individual hospitalists, hospital medicine group leaders seek comparisons when they read the survey. For her part, Dr. Dauterive has found the data on starting salaries for new hospitalists useful. For example, page 259, detailed table 060-A on hospitalists’ compensation by category and total, breaks out median yearly income by years as a hospitalist, from less than a year to six or more years. (Many of the detailed “A” tables in Chapter 8 on compensation include the “years as a hospitalist” category.) Dr. Dauterive praises the wealth of data in the survey, pointing to examples of the many variables she was surprised to learn. One of those factors was that 48% of surveyed hospitalist programs were at non-teaching hospitals. (See page 7 of the survey, Executive Summary, “Teaching status of affiliated hospital.”)
Those interviewed for this article agree that productivity data are probably more telling about the day-to-day clinical realities for hospitalists. Productivity metrics figure prominently in Dr. Dauterive’s uses for the survey. Accordingly, the annual number of billable patient encounters seen by the hospitalist (Table 58-B, page 256) and the annual number of work relative value units (RVUs) worked by the hospitalist (Table 59-B, page 258) caught her interest.
Still, Dr. Dauterive found herself wanting more data to shed light on those numbers. In negotiations for resources with hospital administrators, Dr. Dauterive would like to be able to pinpoint the reasons behind reported numbers of clinical encounters seen by the hospitalist. If the median number of billable patient encounters seen by the hospitalist in a teaching service was 1,668 (based on 107 responses; page 256, Detailed Table 058-B), what were some of the influences on this number? What was the acuity level of patients? Did the hospitalist have group resources, such as physician extenders, to help with patient admissions and rounds?
“For groups that have low lengths of stay, it would be important for me to know why,” she says. “Did they have extra supports? Do their [doctors] use Palm Pilots? You don’t always know from looking at the numbers how to apply them, make the connection, and justify the resources you’re trying to achieve,” she says.
No Perfect Measure
The ideal survey for Dr. Dauterive would include specific structured models, providing links between categories so that she could compare characteristics that more closely align with her group’s situation.
“Our program is very mixed, so it would be helpful for me to know how work RVUs were being reported,” she says. Pointing to results showing higher productivity (work RVUs) in practices compensated by 100% incentive (Table 060-A, page 259 of the survey), Dr. Dauterive wonders what factors drive these results. While the 100% incentive might appear to be the most important factor, perhaps these groups also have physician extenders or are located in a geographic location that boosts their productivity.
“I’m in a nonprofit hospital, in a clinical hospitalist service, and I want to be able to approach the administration and say, ‘If you want us to see the most patients, these are the kinds of services that see the most patients,’ ”says Dr. Dauterive. “But, if you are more interested in physician retention and work/life, then these are the characteristics of those successful programs.”
This level of detail can be difficult to interpolate from the survey, agrees Dr. Nelson. Patient acuity, for instance, is not specifically queried in the survey questionnaire. “I agree, in the ideal world, this is all information that you would want to know,” he says. Answers to the following questions could help refine product metrics:
- Does your group have teaching responsibilities for residents?
- Do you take a lot of calls from home, or do you have a separate night shift?
- Do you cover more than one physical hospital on the same day?
- Does your group do more than the typical amount of committee and administrative work?
“All these factors,” notes Dr. Nelson, “would influence productivity. There is no perfect way to know the answer to any of those things.” And, he adds, the survey already comprises 292 pages, including numerous detailed tables of data. To include all pertinent variables would entail a longer questionnaire, which might affect the response rate.
Healthcare Delivery Is Local
In his consultations with hospitalist groups, Dr. Nelson always emphasizes that the survey is “a starting point” and not the goal of what hospitalists should make. He favors adjunctive methods for benchmarking practices: “I think that when you’re benchmarking your practice, it’s as important to gather as much local and regional data as you can—in addition to the SHM survey.” He tries to network with other Seattle hospitalist programs to learn about their patterns of work hours, patient loads, and the like.
Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, notes that regional markets differ widely. The healthcare market in the Northern California Bay area is very different from the one in Los Angeles in terms of financial remuneration and incentivization.
“The survey,” he says, “gives a global gestalt of the regional flavor of hospital medicine” and reveals general ballpark medians that can be a good starting point for practice benchmarking. “I think what our administration [at California Pacific Medical Center] wants to see is our data compared to the people across the street and down the road, because that’s a closer comparison in terms of payer mix and insurance reimbursements.”
IPC’s Lary agrees. “When I compete, I don’t compete against people across the country; I compete with people across the street,” he says. “As large as IPC is, we realize that healthcare is delivered locally. What we try to do [with the survey] is take the information and, to the best or our ability, figure out how it applies to our individual settings and [to the] different markets that we are in.”
A Stake in the Sand
“I think the benchmarks we have in the survey are just a piece of information—[the survey] is a context, it’s a stake in the sand,” concludes Miller. “We do have variations by type of program, by size of hospital, by geographic location, by size of program. There are numbers for each one of those, and you can clue in as to what some of the more important variations are. We could list probably 25 to 50 variables that would affect hospitalists’ productivity in one way or the other—and that’s not taking into account the individual styles of hospitalists.”
For instance, some hospitalists want to work and earn as much money as possible, while others are searching for a work/life balance that will allow them time with their families.
The survey, says Lary, supplies a piece of information in a complex puzzle about a highly variable profession. “There are so many different ways this business is being conducted right now,” he says. “One medical community may be willing to subsidize a hospital medicine program, and another may not be willing.”
Hospitalists’ professional goals vary widely as well. As far as Dr. Nelson is concerned, the bottom line for hospitalists is to structure independent practices tailored to fit their goals. This means that hospitalists are connected to the economic consequences of their staffing and workload decisions. In that way, he says, rather than approaching administrators about hiring more physicians, the practice itself can decide whether it is worth the decrease in individual hospitalists’ incomes to hire another doctor.
Because their specialty is still evolving, hospitalists will find themselves educating their clients about the profession’s services and advantages. And for that process, the survey can be a helpful adjunct. Miller agrees that the use of the survey requires a certain amount of interpolation on the part of hospitalist leaders. They should be careful, he emphasizes, not to lose sight of the individuality of their own practices.
“If you hold up the survey as the governing document when you negotiate with your hospital, then each party will use it to their advantage,” says Dr. Nelson. “This can push you towards being ‘average’ when that might not be appropriate for your practice.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
Productivity and compensation benchmarks can be useful when negotiating with hospital administrators for increased reimbursements and support resources, when recruiting hospitalists, and when conducting self-evaluations. For many of these processes, hospitalists—and, indeed, hospital administrators—turn to the information contained in the voluminous SHM 2005-2006 Survey, “The Authoritative Source on the State of the Hospital Medicine Movement.” (See “For More Information,” p. 32.)
With a response rate of 26%, the survey represents some 2,550 hospitalists across the nation, and its variables present a more comprehensive aerial view of hospital medicine than did previous surveys. But on the ground and in the trenches, hospital medicine groups must be careful to look at the survey’s metrics with a discerning eye.
When applying the survey metrics to one’s own practice, there can be benefits as well as pitfalls, cautions Joe Miller, SHM senior vice president and principal analyst of the survey data. He emphasizes the great variation among hospital medicine groups and warns against looking at survey medians as representing a “typical” hospital medicine practice.
“When you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” he quips. In several recent conversations, hospital medicine group leaders and SHM leaders involved in compiling the survey discussed the survey’s strengths and limitations as a benchmarking tool.
Healthy to Negotiate
According to the survey 97% of hospitalist programs receive some type of financial support. “Virtually every program in the country is challenged to defend the amount of money [they receive] or to negotiate for support dollars,” says Miller, who believes that negotiation can be a healthy dynamic. “There is a sense of equality of both sides of the table, a mutual respect between hospitalists and the hospital.” In the process of such negotiations, it will be important not to pin one’s position entirely to the survey metrics.
John Nelson, MD, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, a columnist for The Hospitalist (“Practice Management”), and a co-founder and past president of SHM, believes that some hospitalists mistakenly view the survey as SHM’s position on what a hospitalist should make. “The survey is the best information we have about what hospitalists do make—there is no better source—but it’s still a survey.”
Using compensation medians as yardsticks for actual salaries and compensation packages is analogous to “learning the average weight of an American and deciding that’s what we all should weigh—and that’s a big mistake,” he says. “If you hold up the survey as the governing document, then each party will use it to their advantage.”
Because the survey is regarded as the most authoritative existing source on hospitalists’ compensation and productivity, it nevertheless ends up being used as a benchmark, says Robin L. Dauterive, assistant director of the clinical hospitalist service at Massachusetts General Hospital in Boston.
“Whenever I’m preparing billings reports or dashboard measures—anything that shows my group’s workload—sooner or later, I always have to include something in there that states, ‘This is what other people are doing,’ ” says Dauterive. “It’s something that you can’t get away from, unfortunately, in medicine.”
She realizes that the survey does not purport to set any national standards, and yet, “all administrations want comparisons.” Dr. Nelson has also noted this phenomenon with the survey. In the absence of additional guidance, hospital executives and hospitalists often find that they’re just arguing about the survey. “And that’s unfortunate,” he says. “It means they’ve lost sight of the unique attributes of a given practice that might support higher or lower incomes and higher or lower workloads.”
View in Context
Hospitalists reading the survey for the first time might first seek to analyze the metrics regarding billings and collections. Here it is especially important not to view the reported numbers in isolation, says Dr. Nelson. For instance, to learn how a hospitalist’s annual gross charges (billings) compare with others across the country (question 12 of the Individual Hospitalist questionnaire—p. 87, Appendix 2), details on pages 251 and 252 supply pertinent variables. For instance, in comparing the four regions of the country, Table 056-A shows that the median annual gross charges for physicians in the south are highest, at $354,000. Hospitalists compensated by a 100% incentive method report higher charges per year ($392,000) than those who are on a 100% salary or a mix of the two methods of payment. Turning to Table 056-B, on page 252 of the published survey, hospitalists can find annual gross charges according to practitioner type, specialty, and employment model. Hospitalists should not stop their reading there, however, as a comparison of others’ annual gross collections might give a more complete picture.
Still, the SHM Survey does not reference all possible explanatory variables. Collections can be influenced by location and payer mix. Hospitalists practicing in a large urban hospital are likely to see more indigent patients for whom the hospital is not reimbursed. A careful reading of the survey should include the questionnaire and the tables supporting chapter conclusions, and the reader must recognize the survey’s limitations.
Apples to Oranges
IPC–The Hospitalist Company participates in the SHM survey and also uses it as a recruitment tool, reports IPC Vice President of Physician Staffing Timothy Lary. “We look at the income averages, and we’re able to demonstrate how our averages are, for the most part, higher than the averages,” he explains. “We also look at the survey from an internal viewpoint, but oftentimes you are comparing apples to oranges.”
Like individual hospitalists, hospital medicine group leaders seek comparisons when they read the survey. For her part, Dr. Dauterive has found the data on starting salaries for new hospitalists useful. For example, page 259, detailed table 060-A on hospitalists’ compensation by category and total, breaks out median yearly income by years as a hospitalist, from less than a year to six or more years. (Many of the detailed “A” tables in Chapter 8 on compensation include the “years as a hospitalist” category.) Dr. Dauterive praises the wealth of data in the survey, pointing to examples of the many variables she was surprised to learn. One of those factors was that 48% of surveyed hospitalist programs were at non-teaching hospitals. (See page 7 of the survey, Executive Summary, “Teaching status of affiliated hospital.”)
Those interviewed for this article agree that productivity data are probably more telling about the day-to-day clinical realities for hospitalists. Productivity metrics figure prominently in Dr. Dauterive’s uses for the survey. Accordingly, the annual number of billable patient encounters seen by the hospitalist (Table 58-B, page 256) and the annual number of work relative value units (RVUs) worked by the hospitalist (Table 59-B, page 258) caught her interest.
Still, Dr. Dauterive found herself wanting more data to shed light on those numbers. In negotiations for resources with hospital administrators, Dr. Dauterive would like to be able to pinpoint the reasons behind reported numbers of clinical encounters seen by the hospitalist. If the median number of billable patient encounters seen by the hospitalist in a teaching service was 1,668 (based on 107 responses; page 256, Detailed Table 058-B), what were some of the influences on this number? What was the acuity level of patients? Did the hospitalist have group resources, such as physician extenders, to help with patient admissions and rounds?
“For groups that have low lengths of stay, it would be important for me to know why,” she says. “Did they have extra supports? Do their [doctors] use Palm Pilots? You don’t always know from looking at the numbers how to apply them, make the connection, and justify the resources you’re trying to achieve,” she says.
No Perfect Measure
The ideal survey for Dr. Dauterive would include specific structured models, providing links between categories so that she could compare characteristics that more closely align with her group’s situation.
“Our program is very mixed, so it would be helpful for me to know how work RVUs were being reported,” she says. Pointing to results showing higher productivity (work RVUs) in practices compensated by 100% incentive (Table 060-A, page 259 of the survey), Dr. Dauterive wonders what factors drive these results. While the 100% incentive might appear to be the most important factor, perhaps these groups also have physician extenders or are located in a geographic location that boosts their productivity.
“I’m in a nonprofit hospital, in a clinical hospitalist service, and I want to be able to approach the administration and say, ‘If you want us to see the most patients, these are the kinds of services that see the most patients,’ ”says Dr. Dauterive. “But, if you are more interested in physician retention and work/life, then these are the characteristics of those successful programs.”
This level of detail can be difficult to interpolate from the survey, agrees Dr. Nelson. Patient acuity, for instance, is not specifically queried in the survey questionnaire. “I agree, in the ideal world, this is all information that you would want to know,” he says. Answers to the following questions could help refine product metrics:
- Does your group have teaching responsibilities for residents?
- Do you take a lot of calls from home, or do you have a separate night shift?
- Do you cover more than one physical hospital on the same day?
- Does your group do more than the typical amount of committee and administrative work?
“All these factors,” notes Dr. Nelson, “would influence productivity. There is no perfect way to know the answer to any of those things.” And, he adds, the survey already comprises 292 pages, including numerous detailed tables of data. To include all pertinent variables would entail a longer questionnaire, which might affect the response rate.
Healthcare Delivery Is Local
In his consultations with hospitalist groups, Dr. Nelson always emphasizes that the survey is “a starting point” and not the goal of what hospitalists should make. He favors adjunctive methods for benchmarking practices: “I think that when you’re benchmarking your practice, it’s as important to gather as much local and regional data as you can—in addition to the SHM survey.” He tries to network with other Seattle hospitalist programs to learn about their patterns of work hours, patient loads, and the like.
Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, notes that regional markets differ widely. The healthcare market in the Northern California Bay area is very different from the one in Los Angeles in terms of financial remuneration and incentivization.
“The survey,” he says, “gives a global gestalt of the regional flavor of hospital medicine” and reveals general ballpark medians that can be a good starting point for practice benchmarking. “I think what our administration [at California Pacific Medical Center] wants to see is our data compared to the people across the street and down the road, because that’s a closer comparison in terms of payer mix and insurance reimbursements.”
IPC’s Lary agrees. “When I compete, I don’t compete against people across the country; I compete with people across the street,” he says. “As large as IPC is, we realize that healthcare is delivered locally. What we try to do [with the survey] is take the information and, to the best or our ability, figure out how it applies to our individual settings and [to the] different markets that we are in.”
A Stake in the Sand
“I think the benchmarks we have in the survey are just a piece of information—[the survey] is a context, it’s a stake in the sand,” concludes Miller. “We do have variations by type of program, by size of hospital, by geographic location, by size of program. There are numbers for each one of those, and you can clue in as to what some of the more important variations are. We could list probably 25 to 50 variables that would affect hospitalists’ productivity in one way or the other—and that’s not taking into account the individual styles of hospitalists.”
For instance, some hospitalists want to work and earn as much money as possible, while others are searching for a work/life balance that will allow them time with their families.
The survey, says Lary, supplies a piece of information in a complex puzzle about a highly variable profession. “There are so many different ways this business is being conducted right now,” he says. “One medical community may be willing to subsidize a hospital medicine program, and another may not be willing.”
Hospitalists’ professional goals vary widely as well. As far as Dr. Nelson is concerned, the bottom line for hospitalists is to structure independent practices tailored to fit their goals. This means that hospitalists are connected to the economic consequences of their staffing and workload decisions. In that way, he says, rather than approaching administrators about hiring more physicians, the practice itself can decide whether it is worth the decrease in individual hospitalists’ incomes to hire another doctor.
Because their specialty is still evolving, hospitalists will find themselves educating their clients about the profession’s services and advantages. And for that process, the survey can be a helpful adjunct. Miller agrees that the use of the survey requires a certain amount of interpolation on the part of hospitalist leaders. They should be careful, he emphasizes, not to lose sight of the individuality of their own practices.
“If you hold up the survey as the governing document when you negotiate with your hospital, then each party will use it to their advantage,” says Dr. Nelson. “This can push you towards being ‘average’ when that might not be appropriate for your practice.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
Productivity and compensation benchmarks can be useful when negotiating with hospital administrators for increased reimbursements and support resources, when recruiting hospitalists, and when conducting self-evaluations. For many of these processes, hospitalists—and, indeed, hospital administrators—turn to the information contained in the voluminous SHM 2005-2006 Survey, “The Authoritative Source on the State of the Hospital Medicine Movement.” (See “For More Information,” p. 32.)
With a response rate of 26%, the survey represents some 2,550 hospitalists across the nation, and its variables present a more comprehensive aerial view of hospital medicine than did previous surveys. But on the ground and in the trenches, hospital medicine groups must be careful to look at the survey’s metrics with a discerning eye.
When applying the survey metrics to one’s own practice, there can be benefits as well as pitfalls, cautions Joe Miller, SHM senior vice president and principal analyst of the survey data. He emphasizes the great variation among hospital medicine groups and warns against looking at survey medians as representing a “typical” hospital medicine practice.
“When you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” he quips. In several recent conversations, hospital medicine group leaders and SHM leaders involved in compiling the survey discussed the survey’s strengths and limitations as a benchmarking tool.
Healthy to Negotiate
According to the survey 97% of hospitalist programs receive some type of financial support. “Virtually every program in the country is challenged to defend the amount of money [they receive] or to negotiate for support dollars,” says Miller, who believes that negotiation can be a healthy dynamic. “There is a sense of equality of both sides of the table, a mutual respect between hospitalists and the hospital.” In the process of such negotiations, it will be important not to pin one’s position entirely to the survey metrics.
John Nelson, MD, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., a consultant for hospitalist practices with Nelson/Flores Associates, a columnist for The Hospitalist (“Practice Management”), and a co-founder and past president of SHM, believes that some hospitalists mistakenly view the survey as SHM’s position on what a hospitalist should make. “The survey is the best information we have about what hospitalists do make—there is no better source—but it’s still a survey.”
Using compensation medians as yardsticks for actual salaries and compensation packages is analogous to “learning the average weight of an American and deciding that’s what we all should weigh—and that’s a big mistake,” he says. “If you hold up the survey as the governing document, then each party will use it to their advantage.”
Because the survey is regarded as the most authoritative existing source on hospitalists’ compensation and productivity, it nevertheless ends up being used as a benchmark, says Robin L. Dauterive, assistant director of the clinical hospitalist service at Massachusetts General Hospital in Boston.
“Whenever I’m preparing billings reports or dashboard measures—anything that shows my group’s workload—sooner or later, I always have to include something in there that states, ‘This is what other people are doing,’ ” says Dauterive. “It’s something that you can’t get away from, unfortunately, in medicine.”
She realizes that the survey does not purport to set any national standards, and yet, “all administrations want comparisons.” Dr. Nelson has also noted this phenomenon with the survey. In the absence of additional guidance, hospital executives and hospitalists often find that they’re just arguing about the survey. “And that’s unfortunate,” he says. “It means they’ve lost sight of the unique attributes of a given practice that might support higher or lower incomes and higher or lower workloads.”
View in Context
Hospitalists reading the survey for the first time might first seek to analyze the metrics regarding billings and collections. Here it is especially important not to view the reported numbers in isolation, says Dr. Nelson. For instance, to learn how a hospitalist’s annual gross charges (billings) compare with others across the country (question 12 of the Individual Hospitalist questionnaire—p. 87, Appendix 2), details on pages 251 and 252 supply pertinent variables. For instance, in comparing the four regions of the country, Table 056-A shows that the median annual gross charges for physicians in the south are highest, at $354,000. Hospitalists compensated by a 100% incentive method report higher charges per year ($392,000) than those who are on a 100% salary or a mix of the two methods of payment. Turning to Table 056-B, on page 252 of the published survey, hospitalists can find annual gross charges according to practitioner type, specialty, and employment model. Hospitalists should not stop their reading there, however, as a comparison of others’ annual gross collections might give a more complete picture.
Still, the SHM Survey does not reference all possible explanatory variables. Collections can be influenced by location and payer mix. Hospitalists practicing in a large urban hospital are likely to see more indigent patients for whom the hospital is not reimbursed. A careful reading of the survey should include the questionnaire and the tables supporting chapter conclusions, and the reader must recognize the survey’s limitations.
Apples to Oranges
IPC–The Hospitalist Company participates in the SHM survey and also uses it as a recruitment tool, reports IPC Vice President of Physician Staffing Timothy Lary. “We look at the income averages, and we’re able to demonstrate how our averages are, for the most part, higher than the averages,” he explains. “We also look at the survey from an internal viewpoint, but oftentimes you are comparing apples to oranges.”
Like individual hospitalists, hospital medicine group leaders seek comparisons when they read the survey. For her part, Dr. Dauterive has found the data on starting salaries for new hospitalists useful. For example, page 259, detailed table 060-A on hospitalists’ compensation by category and total, breaks out median yearly income by years as a hospitalist, from less than a year to six or more years. (Many of the detailed “A” tables in Chapter 8 on compensation include the “years as a hospitalist” category.) Dr. Dauterive praises the wealth of data in the survey, pointing to examples of the many variables she was surprised to learn. One of those factors was that 48% of surveyed hospitalist programs were at non-teaching hospitals. (See page 7 of the survey, Executive Summary, “Teaching status of affiliated hospital.”)
Those interviewed for this article agree that productivity data are probably more telling about the day-to-day clinical realities for hospitalists. Productivity metrics figure prominently in Dr. Dauterive’s uses for the survey. Accordingly, the annual number of billable patient encounters seen by the hospitalist (Table 58-B, page 256) and the annual number of work relative value units (RVUs) worked by the hospitalist (Table 59-B, page 258) caught her interest.
Still, Dr. Dauterive found herself wanting more data to shed light on those numbers. In negotiations for resources with hospital administrators, Dr. Dauterive would like to be able to pinpoint the reasons behind reported numbers of clinical encounters seen by the hospitalist. If the median number of billable patient encounters seen by the hospitalist in a teaching service was 1,668 (based on 107 responses; page 256, Detailed Table 058-B), what were some of the influences on this number? What was the acuity level of patients? Did the hospitalist have group resources, such as physician extenders, to help with patient admissions and rounds?
“For groups that have low lengths of stay, it would be important for me to know why,” she says. “Did they have extra supports? Do their [doctors] use Palm Pilots? You don’t always know from looking at the numbers how to apply them, make the connection, and justify the resources you’re trying to achieve,” she says.
No Perfect Measure
The ideal survey for Dr. Dauterive would include specific structured models, providing links between categories so that she could compare characteristics that more closely align with her group’s situation.
“Our program is very mixed, so it would be helpful for me to know how work RVUs were being reported,” she says. Pointing to results showing higher productivity (work RVUs) in practices compensated by 100% incentive (Table 060-A, page 259 of the survey), Dr. Dauterive wonders what factors drive these results. While the 100% incentive might appear to be the most important factor, perhaps these groups also have physician extenders or are located in a geographic location that boosts their productivity.
“I’m in a nonprofit hospital, in a clinical hospitalist service, and I want to be able to approach the administration and say, ‘If you want us to see the most patients, these are the kinds of services that see the most patients,’ ”says Dr. Dauterive. “But, if you are more interested in physician retention and work/life, then these are the characteristics of those successful programs.”
This level of detail can be difficult to interpolate from the survey, agrees Dr. Nelson. Patient acuity, for instance, is not specifically queried in the survey questionnaire. “I agree, in the ideal world, this is all information that you would want to know,” he says. Answers to the following questions could help refine product metrics:
- Does your group have teaching responsibilities for residents?
- Do you take a lot of calls from home, or do you have a separate night shift?
- Do you cover more than one physical hospital on the same day?
- Does your group do more than the typical amount of committee and administrative work?
“All these factors,” notes Dr. Nelson, “would influence productivity. There is no perfect way to know the answer to any of those things.” And, he adds, the survey already comprises 292 pages, including numerous detailed tables of data. To include all pertinent variables would entail a longer questionnaire, which might affect the response rate.
Healthcare Delivery Is Local
In his consultations with hospitalist groups, Dr. Nelson always emphasizes that the survey is “a starting point” and not the goal of what hospitalists should make. He favors adjunctive methods for benchmarking practices: “I think that when you’re benchmarking your practice, it’s as important to gather as much local and regional data as you can—in addition to the SHM survey.” He tries to network with other Seattle hospitalist programs to learn about their patterns of work hours, patient loads, and the like.
Thomas Baudendistel, MD, FACP, associate program director of the Internal Medicine Residency Program at Sutter Health’s California Pacific Medical Center in San Francisco, notes that regional markets differ widely. The healthcare market in the Northern California Bay area is very different from the one in Los Angeles in terms of financial remuneration and incentivization.
“The survey,” he says, “gives a global gestalt of the regional flavor of hospital medicine” and reveals general ballpark medians that can be a good starting point for practice benchmarking. “I think what our administration [at California Pacific Medical Center] wants to see is our data compared to the people across the street and down the road, because that’s a closer comparison in terms of payer mix and insurance reimbursements.”
IPC’s Lary agrees. “When I compete, I don’t compete against people across the country; I compete with people across the street,” he says. “As large as IPC is, we realize that healthcare is delivered locally. What we try to do [with the survey] is take the information and, to the best or our ability, figure out how it applies to our individual settings and [to the] different markets that we are in.”
A Stake in the Sand
“I think the benchmarks we have in the survey are just a piece of information—[the survey] is a context, it’s a stake in the sand,” concludes Miller. “We do have variations by type of program, by size of hospital, by geographic location, by size of program. There are numbers for each one of those, and you can clue in as to what some of the more important variations are. We could list probably 25 to 50 variables that would affect hospitalists’ productivity in one way or the other—and that’s not taking into account the individual styles of hospitalists.”
For instance, some hospitalists want to work and earn as much money as possible, while others are searching for a work/life balance that will allow them time with their families.
The survey, says Lary, supplies a piece of information in a complex puzzle about a highly variable profession. “There are so many different ways this business is being conducted right now,” he says. “One medical community may be willing to subsidize a hospital medicine program, and another may not be willing.”
Hospitalists’ professional goals vary widely as well. As far as Dr. Nelson is concerned, the bottom line for hospitalists is to structure independent practices tailored to fit their goals. This means that hospitalists are connected to the economic consequences of their staffing and workload decisions. In that way, he says, rather than approaching administrators about hiring more physicians, the practice itself can decide whether it is worth the decrease in individual hospitalists’ incomes to hire another doctor.
Because their specialty is still evolving, hospitalists will find themselves educating their clients about the profession’s services and advantages. And for that process, the survey can be a helpful adjunct. Miller agrees that the use of the survey requires a certain amount of interpolation on the part of hospitalist leaders. They should be careful, he emphasizes, not to lose sight of the individuality of their own practices.
“If you hold up the survey as the governing document when you negotiate with your hospital, then each party will use it to their advantage,” says Dr. Nelson. “This can push you towards being ‘average’ when that might not be appropriate for your practice.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
X-Ray Has Left the Building
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Medical outsourcing is a growing trend in American hospitals, driven by shortages of on-call radiologists and intensivists, economic pressures, and advances in telemedicine. Hospitalists will likely encounter—if they haven’t already—outsourced services that range from off-site medical transcription and language interpreters to long-distance radiology and, increasingly, electronic intensivist services.1 What are the implications for quality patient care and collegial interface when hospitals contract with outsourced providers? What are the advantages, possible disadvantages, and opportunities for hospitalists as teleradiology and eICUs become facts of life?
A Variety of Configurations
According to Rick Wade, senior vice president for strategic communications for the American Hospital Association (Chicago), it’s difficult to quantify the extent to which outsourcing is currently being used in U.S. hospitals. VISICU, Inc., a leader in the provision of eICU services, currently has 150 client hospitals. Eight hospitalists contacted at community and university hospitals in Colo., Fla., Maine, Minn., Ga. and N.M. reported that they were not directly involved with outsourcing other than with transcription services.
Robert M. Wachter, MD, professor and associate chairman, Department of Medicine, and chief of the Medical Service at the University of California at San Francisco (UCSF), whose “Perspective” piece on medical outsourcing appeared in the February 16 New England Journal of Medicine, is intrigued by the implications of outsourcing trends for medicine: “I think medicine has been peculiarly insulated from [the globalization of services], and it’s just very interesting and exciting—and troubling as well.”1
Off-Site X-Ray Reads Common
According to the American College of Radiology, teleradiology has become a fixture in most practices and hospitals.2,3 Some institutions have retained their own radiologists, who take advantage of teleradiology by reading digitized radiographs and CT scans from home instead of within the hospital building. A shortage of radiologists has led others to contract with off-site providers of teleradiology services. Those who provide services at night are sometimes called “nighthawk” companies.1 Outsourcing of radiology, Dr. Wachter believes, is a logical step due to technological advances, though he admits that visiting the radiology department in his hospital often yields educational and collegial opportunities that online X-ray reading does not.
At Saint Clare’s Hospital in Weston/Wasau, Wis., a new, 107-bed state-of-the-art facility built by Ministry Health Care, Richard Bailey, MD, is medical director of Inpatient Care and Hospitalist Services. Radiology and other ancillary specialist services are provided by the Diagnostic and Treatment Center (DTC), jointly owned by Ministry Health Care and the Marshfield Clinic. The DTC, through a relationship with a radiology group in Hawaii, provides night coverage for full reads of radiographs and scans from 5 p.m. to 5 a.m. The interactions are virtually seamless, according to Dr. Bailey. “We don’t even notice they’re in Hawaii” when conferring with radiologists on the phone, he reports.
Off-site radiology also created an opportunity for his hospitalist group, Dr. Bailey says. Saint Clare’s hospitalist group provides supervision of contrast administration when needed during night and weekend coverage times. “This is one more way our hospitalist program supports the hospital and provides value beyond just seeing patients,” he says.
Overseas Outsourcing a ‘Hot Button’
Using an overseas teleradiology company provides many advantages, says Sunita Maheshwari, MD, a consulting pediatric cardiologist and director of Teleradiology Solutions, a four-year-old teleradiology company located in Bangalore, India. The company’s radiologists do mostly preliminary night-reads but also do final-reads on approximately 20% of their cases. If contrast must be administered for an imaging study at the client hospital, a local tech, emergency department physician, or resident usually handles the procedure, with the Teleradiology Solutions radiologist in constant voice contact.
“The time zone advantage is huge,” says Dr. Maheshwari. With the 12.5-hour time difference between the United States and India, Teleradiology Solutions’ radiologists work regular day shifts and are able to cover 10-20 hospitals simultaneously, depending on how busy their client hospitals are.
“You don’t have to have one radiologist who stays up all night to be able to read two CT scans and one X-ray, who will [then] be groggy the next morning for his [or her] regular day shift,” she says. It makes a lot of sense from the standpoint of human resource efficiency to not waste several nights of several doctors covering multiple hospitals.” Dr. Maheshwari reports that American hospital staff are often pleasantly surprised to find a “cheerful, awake” radiologist on the other end of the phone line.
Despite these benefits, however, Dr. Maheshwari and her colleagues have noticed a political backlash stemming from the outsourcing of U.S. jobs to Asia that colors Americans’ reactions to overseas teleradiology. In her company’s first two years, some physicians questioned the company’s level of quality and lashed out because it is located in India, reports Dr. Maheshwari.
“Our work speaks for itself,” she says. “We have not lost a client, and, in fact, our hospitals have managed to grow because they have been able to take their radiologists off the night shift, and they take on more day work.”
Like several overseas teleradiology companies, Teleradiology Solutions retains a staff of U.S.-trained radiologists and goes through the same licensing and credentialing (they are JCAHO-accredited) as American companies.
The company now has 40 U.S. hospitals as clients and includes in its client mix some remote hospitals in India and Singapore, where the Ministry of Health is experiencing a similar shortage of radiologists.
Filling an ICU Gap
Shortages of specialists—and federal mandates to improve access to care—have spurred the growth of telemedicine in remote rural areas. Wade notes that multi-hospital systems are now installing remote electronic ICU care programs, where intensivists simultaneously monitor ICU patients in several hospitals from a central location. Preliminary studies have demonstrated both improved clinical outcomes and heightened hospital performance with programs such as VISICU Inc.’s eCare Manager software, which features built-in online decision support, adverse events alerts, and outcomes tracking. One 2004 study documented a 27% reduction in severity-adjusted hospital mortality for ICU patients, a 17% reduction in ICU length of stay, and a savings of $2,150 per patient, even after accounting for initial capital outlays to install the eICU system.4
SHM President Mary Jo Gorman, MD, MBA, is now chief executive officer for Advanced ICU Care, headquartered in St. Louis, Mo. Using VISICU’s patented software platform, the new company currently contracts with two community-based Midwestern hospitals to deliver real-time intensivist rounding and decision-making support.
Saint Clare’s Hospital, located in north central Wisconsin, was opened by Ministry Health Care in October 2005 with the intention of creating a tertiary referral center, says Dr. Bailey. To be competitive in the market, the hospital needed to provide a full-service intensive care unit. He explains, “[Unfortunately,] we are in an area that is suffering from the same kind of recruitment drought in pulmonary and critical care medicine as everyone else—and ours is accentuated because we are not in a large city, and we are not a teaching hospital.”
Advanced ICU proved a good fit for addressing the hospital’s ICU needs. The hospital “went live” with eICU in January and no longer has to send patients to sister hospitals with on-site intensivist coverage, says Dr. Bailey. Saint Clare’s staff intensivist works regular day shifts, and the hospitalist group co-manages the ICU with Advanced ICU’s staff the rest of the time, providing 24/7 coverage. ICU mortality, after adjusting for Acute Physiology and Chronic Health Evaluation (APACHE) scores and other severity indices, is also below predicted numbers.
Patient and Staff Acceptance
Does the notion of real-time video surveillance coupled with real-time data feeds on vital signs, lab work, and medications present problems for patients or staff? Patients are “very accepting and feel it’s an extra sort of security” knowing that Advanced ICU intensivists are on the job, says Dr. Gorman: “One patient referred to us as a ‘guardian angel’ looking over them.
“The nursing staff has been extremely accepting because it reduces their stress about making a determination of whether to interrupt the attending doctor during his office hours or at night,” she continues. “We’re really a partner to the local medical staff. We all know that to reduce medical errors, the bedside caregiver needs to recognize the problem, be able to contact somebody, address the problem, and then see if that intervention is the right one for the problem described. With eICU, you just move past all of those points of failure to get the patient right to the doctor in a very timely manner.”
Janet Pestle, RN, MSN, director of the Cardiovascular Program at SSM Health Care’s St. Mary’s Hospital and Medical Center in Jefferson City, Mo., echoes Dr. Gorman’s assessment. Encountering the same intensivist drought as other hospitals outside of metropolitan areas, St. Mary’s also contracted with Advanced ICU.
“I’d have a fist fight if I ever wanted to take [the eICU] away from the nurses and staff on the night shift,” declares Pestle. “I think there is definitely some guilt associated with healthcare workers having to wake up a doctor who may have been working all day. They love being able to push a button and have a physician there.”
Dr. Bailey believes the eICU offers many advantages for Saint Clare’s six-member hospitalist group. Although hospitalists have a large presence in the ICU, “ … we shouldn’t expect them to be intensivists,” he insists. “Given that the typical hospitalist is very young, I was concerned about setting up hospitalists for failure by not giving them the resources to help them provide high quality care and to be successful.”
Partnering with Advanced ICU has also helped recruitment of younger hospitalists, he says, noting that hospitalists have chosen Saint Clare’s over other hospitals because of the eICU presence. “Our hospitalists get very concerned about being pulled in too many directions,” says Dr. Bailey. “Advanced ICU frees up our hospitalists, giving them a high degree of comfort and confidence that they can handle multiple cases at once.”
To ensure continuity between the ICU and the medical floor, all admissions are still handled by the hospitalists. The eCare Manager software used by Advanced ICU also provides another layer of attention to quality indicators, with built-in decision support and alerts.
Outsourcing Opens the Box
Dr. Bailey visited Advanced ICU’s command center and was impressed with the frequency with which the company’s intensivists were virtually “rounding” on Saint Clare’s patients. “It’s very exciting if you think about it,” he says. “Intensivists in Missouri can talk with a radiologist in Hawaii about a patient in Wisconsin. This is certainly improving our quality of care.”
“The eICU is really mind-blowing,” agrees Dr. Wachter. Once services are no longer located in the building, “there’s not much difference between 30 miles and 10,000 miles away, and this just opens up the box in some very interesting ways.” Service providers operating from different countries under different sets of laws and value systems, he notes in his New England Journal of Medicine article, can, however, “create opportunities for new kinds of mischief.”
Asked for an example of this, he explains that his institution’s initial foray into medical outsourcing was a bit of a cautionary tale. Unbeknownst to UCSF, their domestic medical transcription company sub-contracted with a transcription company in Pakistan. Administrators discovered this fact when a Pakistani transcriptionist contacted the university, threatening to put all the medical records she had transcribed on the Web if she did not get a raise. This would have constituted a breach of HIPAA and would have created multiple liability issues for UCSF. Contractors dealing with the medical center now have to guarantee, in writing, that they will use only domestic subcontractors, says Dr. Wachter.
Future Directions
Because of the “high-touch” nature of hospital medicine, Dr. Wachter does not think that hospitalists’ services are feasible candidates for outsourcing.
“I guess one could conceive of a robotic hospitalist running around the building being controlled by a joystick in Singapore, but that’s science fiction and not a real risk,” he quips.
Still, relationships with specialists such as radiologists and intensivists may more likely be formed over the telephone, through video conferencing, and in online interactions—phenomena with which younger physicians may be much more comfortable.
Dr. Maheshwari, who, like the company’s founder Arjun Kalyanpur, MD, trained at Yale University in New Haven, Conn., expects that Teleradiology Solution’s business will continue to grow and that, over time, “the world will truly be flat—hopefully!”
Wade admits that the need for outsourced services is not going to diminish. “Our need to be able to harness technology to provide [a high] level of intensive care to patients, no matter where they are, is going to be very strong,” he says. “So I think we will see more of this [outsourcing]. But I also think we’ll see a much greater emphasis on trying to train new physicians. Outsourcing is part of the same phenomenon as medical tourism. Hospitals that go this route are going to have a responsibility to demand high-quality physicians, demand Joint Commission certification, and demand to know the background and training of these [outsourced] physicians, because the patients and families are going to have questions. That’s part of the doctor-patient relationship that the hospital is going to create.” TH
Gretchen Henkel is a frequent contributor to The Hospitalist.
References
- Wachter RM. The “dis-location” of U.S. medicine – the implications of medical outsourcing. N Engl J Med. 2006; 354(7):661-665.
- Larson DB, Cypel YS, Forman HP, et al. A comprehensive portrait of teleradiology in radiology practices: results from the American College of Radiology’s 1999 Survey. AJR Am J Roentgenol. 2005 Jul;185(1):24-35.
- Dimmick SL, Ignatova KD. The diffusion of a medical innovation: where teleradiology is and where it is going. J Telemed Telecare. 2006;12 Suppl 2:S51-58.
- Breslow MJ, Rosenfeld BA, Doerfler M, et al. Effect of a multiple-site intensive care unit telemedicine program on clinical and economic outcomes: an alternative paradigm for intensivist staffing. Crit Care Med. 2004 Jan;32(1):31-38.
Crucial Contact
If the secret to successful real estate investing is “location, location, location,” the key to maintaining good relationships with referring physicians is “communication, communication, communication.” While this may seem simplistic, the complexities of interpersonal communications can pose challenges even in the most straightforward of physician interchanges.
Recent studies and hospitalists consulted for this report maintain that hospitalists’ communications with referring physicians must be examined, practiced, and fine-tuned continually to ensure satisfaction for doctors—and their patients.
“It’s all about the communication,” says Bruce Becker, MD, chief medical officer at Medical Center Hospital in Odessa, Texas, and a family physician and professor of medicine for more than 20 years. “It’s sometimes not what you say, but how you say it.”
According to John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospital medicine groups with Nelson/Flores Associates and a columnist for The Hospitalist (“Practice Management”), it is key for hospitalists to examine and revise oral and written communication processes—especially at critical points during patient handoffs—rather than to assume that good communication will just happen naturally.
Gaining Acceptance
Some primary care physicians (PCPs) are more willing than others to refer patients to a hospitalist. Initially, new programs may have to work hard to gain acceptance with referring physicians. Some referring physicians may not be ready to give up hospital visits and may want to maintain collegiality and control. On the other hand, some family physicians are “ready to step away from hospital practice,” says Dr. Becker, citing diminishing reimbursements due to diagnosis-related groups (DRGs) and managed care.
John A. Bolinger, DO, FACP, medical director of the Hospitalist Program at Terre Haute (Ind.) Regional Hospital, believes that one way to promote a hospitalist program to PCPs is to emphasize hospitalists’ levels of training and efficiency.
“I try to make them aware of how [our hospitalist program] can be advantageous to them,” he explains. “Even if they have only one patient in the hospital, by the time they drive there, get the chart, make the rounds, make their notes, and do the required paperwork, it may take them an hour to see one patient. It makes good economic sense for them to stay in their offices, where they can see a minimum of four patients in the same amount of time for equal or better reimbursements.”
When primary care physicians voice resistance to using a hospitalist program, Dr. Bolinger says he tries to impress upon them the fact that hospitalists do not have outside practices, they will “never try to steal patients,” they stay within referral patterns, and they will make sure that PCPs get pertinent records as soon as possible. Dr. Bolinger believes referring physicians’ biggest concern when dealing with hospitalists is that they “don’t want to lose control.” The way to address those fears is to make sure referring physicians are always kept in the communications loop regarding their patients’ progress.
The policy for Dr. Bolinger’s hospitalist program is to make sure all dictated reports are transcribed and faxed immediately to the referring physician’s office. All scheduled follow-up appointments and medication changes are included in discharge summaries. “If need be,” says Dr. Bolinger, “we will even hand deliver information to physicians’ offices, which we have done multiple times.”
Become User-Friendly
The methods Dr. Bolinger describes often result in referring physicians’ satisfaction with hospitalist services, followed by increased referrals. Hospitalists can ensure continued referrals from their PCPs if they remember hospital medicine’s cardinal rules of availability and prompt, thorough reporting, says Dr. Nelson. It can help to view the interface with the hospitalist service from the PCP’s point of view.
For instance, how can physicians quickly reach the hospitalist service? “If you’re a referring doctor and you’ve got a patient in your office whom you think should be admitted today, who do you call? This can actually be a little tricky for most practices,” says Dr. Nelson. “Every practice should give some thought to making that contact as easy for the referring doctors as possible.”
Some important questions to ask: When trying to reach a hospitalist, is it best to call the group’s main number? Will a voicemail message be returned within an hour? Two hours? Is it better to call the hospital operator and have the hospitalist paged? Or do PCPs have access to hospitalists’ cell phone numbers?
Dr. Nelson suggests that hospitalist groups also give thought to standardizing admission and discharge reports, as well as other forms. Often, individual members of a hospitalist group use slightly different formats for reporting to referring physicians. He points out that this can be less user friendly for the reader, who may have a harder time scanning the document quickly to find a particular piece of important information. Other useful suggestions for making reports user friendly: Use similar headings on all reports; avoid dense text; list pending tests in a prominent place in the report document; and consider highlighting or underlining key words.
Preference for In-Person Contact
For a new hospitalist practice, telephone communication between the hospitalist and the primary physician is valuable, and the hospitalist should “pick up the phone liberally,” says Dr. Nelson.
Dr. Becker believes the best way for physicians to communicate is one on one—in person. “Too often,” he says, “we get used to communicating through a third party—usually a unit clerk, a nurse, or a resident. I believe that physician-to-physician communication is the ideal. If the attending physician and the consultant [hospitalist or subspecialist] speak in person, they can explain their thinking to each other, and “within one minute of precious time, figure out which way to go.”
In this way, without wasting time, the physician gives the consultant guidance as to the appropriate track to take and can also listen to the consultant’s suggestions.
“I feel that medicine has perhaps gotten a little bit away from that communication link,” continues Dr. Becker. “When we get further away from that direct communication—whether it is between doctors and consultants, nurses and doctors, or doctors and family members—you take that little bit of risk that there will be a missed step, either on the part of the communicator or on the receiving end as the listener.”
In a study exploring barriers to effective patient handoffs, Solet and colleagues focused on the communication between physicians as a vital link in patient care continuity. The authors concluded that, regardless of the method of managing patient handoffs (e.g., computer-assisted or paper-based), the best way to ensure effective handoffs of hospitalized patients was “precise, unambiguous, face-to-face communication.”1
In a 2001 study by Hruby, Pantilat, and colleagues at UCSF, the authors found that, for the most part, hospitalized patients with PCPs wanted contact with their primary physicians even while in the hospital. Approximately half of the surveyed patients also believed that the PCP, rather than an inpatient physician, should be the first to discuss with them serious diagnoses or disease management choices.2 Preferences such as those expressed in this study may play into referring physicians’ reluctance to make use of hospitalist services, says Dr. Bolinger. They may fear that patients will feel abandoned by the primary physician. Dr. Bolinger’s response to those sentiments: “Initially, some patients [in our hospital] were a little guarded and were not sure what to expect. But after a day or two of having us there, they are generally very, very pleased to have us on board. We are part of their medical team now.”
A Need for Marketing?
Dr. Becker has been actively developing a hospital medicine program at Medical Center Hospital for the past two years and joined SHM as part of that effort. Familiarizing himself with the tenets of hospital medicine, he discovered that, as a family doctor, “unknowingly, I was actually practicing hospital medicine for 20 years!”
As part of the hospital medicine program development process, he has solicited input from local physicians as well as patients. A simple survey to assess interest in a hospitalist program asked potential referring physicians, Would you use a hospitalist? Would you use a hospitalist after waiting a while to see how the process goes? Or, would you not consider using a hospitalist?
In two years, says Dr. Becker, response from the referring physician community has changed from “bah, humbug” to one of readiness for the program.
A mass mailing can serve to introduce a hospital medicine program in a community. Dr. Bolinger’s group used this method and, in his experience, local subspecialists—orthopedists, cardiologists, endocrinologists, pulmonologists—have proved the biggest source of referrals to their program. But PCPs are starting to use the hospitalist service for vacations and call-coverage issues and are beginning to value hospitalists’ services. “Physicians like coming to the hospital, but they’re starting to realize that the hospitalist program is a better system,” says Dr. Bolinger.
Dr. Nelson has been a hospitalist for 18 years. For most of that time he has had no shortage of referred patients. In fact, the bigger problem has been finding enough doctors to join the group and handle the existing referral volume. In that situation, it has not made sense to undertake marketing with the goal of increasing referrals. However, he advises, “It is always worth spending time and energy trying to maintain good relationships with physicians with whom you regularly share patients, and perhaps this could be called ‘marketing.’”
To maintain good relationships with referring physicians, his group conducts a survey on a yearly basis. A survey, he suggests, should be very short, consisting of only a few key questions, such as:
- Do we send reports promptly to your practice?
- Are your patients satisfied with the care they receive from us?
- Do you have any comments or feedback for our group?
Although his group gains information from these surveys, Dr. Nelson notes that the greater value of conducting such surveys may be in building public relations capital. By conducting a survey, hospitalists demonstrate that they care enough to ask for their referring physicians’ input.
Another good marketing tool is a patient education brochure, given to referring physicians, that explains hospitalists and hospitalist care. These brochures can help referring physicians prepare their patients for seeing a hospitalist in the inpatient setting, thus easing the initial reluctance patients sometimes experience when encountering a new physician.
Conclusion
On the cusp of launching his medical center’s hospital medicine program, Dr. Becker sees that good communication between referring physicians and hospitalists will ensure the program’s success. He advises physicians to remember their classes in communication as third-year medical students, when most participate in videotaped patient encounters. It’s always instructive, he says, to see how we come across to others in conversation.
Both verbal and nonverbal cues play a part in good communication. A 2003 study by Griffith and colleagues concluded that better nonverbal communication skills are associated with greater patient satisfaction, and that formal instruction in nonverbal communication can be a good addition to residency training.3
“I find that doctors talk to each other, in general, very easily,” says Dr. Becker. Sometimes [good communication] is just a matter of opening that door and essentially keeping the former attending, the PCP, apprised of what is going on.”
When hospitalists attend to thorough communication and promptly deliver complete discharge summaries, family physicians can report to their patients that they know what happened in the hospital and poll their patients about their experiences in the hospital. In this way, hospitalists and referring physicians can cement their relationship as team members for the patient. The success of any hospitalist program, Dr. Becker believes, lies in “making sure you fulfill the promise of what hospital medicine generates, and that is a continuity of care … , obtaining front-end communication so that patients get the best care throughout their [hospital] stay, and then follow up with discharge summaries to the primary physician’s office.” TH
Gretchen Henkel is a regular contributor to The Hospitalist.
References
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12): 1094-1099.
- Hruby M, Pantilat SZ, Lo B. How do patients view the role of the primary care physician in inpatient care? Am J Med. 2001;21;111(9B):21S-25S.
- Griffith CH III, Wilson JF, Langer S, et al. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003 Mar;18(3):170-174.
If the secret to successful real estate investing is “location, location, location,” the key to maintaining good relationships with referring physicians is “communication, communication, communication.” While this may seem simplistic, the complexities of interpersonal communications can pose challenges even in the most straightforward of physician interchanges.
Recent studies and hospitalists consulted for this report maintain that hospitalists’ communications with referring physicians must be examined, practiced, and fine-tuned continually to ensure satisfaction for doctors—and their patients.
“It’s all about the communication,” says Bruce Becker, MD, chief medical officer at Medical Center Hospital in Odessa, Texas, and a family physician and professor of medicine for more than 20 years. “It’s sometimes not what you say, but how you say it.”
According to John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospital medicine groups with Nelson/Flores Associates and a columnist for The Hospitalist (“Practice Management”), it is key for hospitalists to examine and revise oral and written communication processes—especially at critical points during patient handoffs—rather than to assume that good communication will just happen naturally.
Gaining Acceptance
Some primary care physicians (PCPs) are more willing than others to refer patients to a hospitalist. Initially, new programs may have to work hard to gain acceptance with referring physicians. Some referring physicians may not be ready to give up hospital visits and may want to maintain collegiality and control. On the other hand, some family physicians are “ready to step away from hospital practice,” says Dr. Becker, citing diminishing reimbursements due to diagnosis-related groups (DRGs) and managed care.
John A. Bolinger, DO, FACP, medical director of the Hospitalist Program at Terre Haute (Ind.) Regional Hospital, believes that one way to promote a hospitalist program to PCPs is to emphasize hospitalists’ levels of training and efficiency.
“I try to make them aware of how [our hospitalist program] can be advantageous to them,” he explains. “Even if they have only one patient in the hospital, by the time they drive there, get the chart, make the rounds, make their notes, and do the required paperwork, it may take them an hour to see one patient. It makes good economic sense for them to stay in their offices, where they can see a minimum of four patients in the same amount of time for equal or better reimbursements.”
When primary care physicians voice resistance to using a hospitalist program, Dr. Bolinger says he tries to impress upon them the fact that hospitalists do not have outside practices, they will “never try to steal patients,” they stay within referral patterns, and they will make sure that PCPs get pertinent records as soon as possible. Dr. Bolinger believes referring physicians’ biggest concern when dealing with hospitalists is that they “don’t want to lose control.” The way to address those fears is to make sure referring physicians are always kept in the communications loop regarding their patients’ progress.
The policy for Dr. Bolinger’s hospitalist program is to make sure all dictated reports are transcribed and faxed immediately to the referring physician’s office. All scheduled follow-up appointments and medication changes are included in discharge summaries. “If need be,” says Dr. Bolinger, “we will even hand deliver information to physicians’ offices, which we have done multiple times.”
Become User-Friendly
The methods Dr. Bolinger describes often result in referring physicians’ satisfaction with hospitalist services, followed by increased referrals. Hospitalists can ensure continued referrals from their PCPs if they remember hospital medicine’s cardinal rules of availability and prompt, thorough reporting, says Dr. Nelson. It can help to view the interface with the hospitalist service from the PCP’s point of view.
For instance, how can physicians quickly reach the hospitalist service? “If you’re a referring doctor and you’ve got a patient in your office whom you think should be admitted today, who do you call? This can actually be a little tricky for most practices,” says Dr. Nelson. “Every practice should give some thought to making that contact as easy for the referring doctors as possible.”
Some important questions to ask: When trying to reach a hospitalist, is it best to call the group’s main number? Will a voicemail message be returned within an hour? Two hours? Is it better to call the hospital operator and have the hospitalist paged? Or do PCPs have access to hospitalists’ cell phone numbers?
Dr. Nelson suggests that hospitalist groups also give thought to standardizing admission and discharge reports, as well as other forms. Often, individual members of a hospitalist group use slightly different formats for reporting to referring physicians. He points out that this can be less user friendly for the reader, who may have a harder time scanning the document quickly to find a particular piece of important information. Other useful suggestions for making reports user friendly: Use similar headings on all reports; avoid dense text; list pending tests in a prominent place in the report document; and consider highlighting or underlining key words.
Preference for In-Person Contact
For a new hospitalist practice, telephone communication between the hospitalist and the primary physician is valuable, and the hospitalist should “pick up the phone liberally,” says Dr. Nelson.
Dr. Becker believes the best way for physicians to communicate is one on one—in person. “Too often,” he says, “we get used to communicating through a third party—usually a unit clerk, a nurse, or a resident. I believe that physician-to-physician communication is the ideal. If the attending physician and the consultant [hospitalist or subspecialist] speak in person, they can explain their thinking to each other, and “within one minute of precious time, figure out which way to go.”
In this way, without wasting time, the physician gives the consultant guidance as to the appropriate track to take and can also listen to the consultant’s suggestions.
“I feel that medicine has perhaps gotten a little bit away from that communication link,” continues Dr. Becker. “When we get further away from that direct communication—whether it is between doctors and consultants, nurses and doctors, or doctors and family members—you take that little bit of risk that there will be a missed step, either on the part of the communicator or on the receiving end as the listener.”
In a study exploring barriers to effective patient handoffs, Solet and colleagues focused on the communication between physicians as a vital link in patient care continuity. The authors concluded that, regardless of the method of managing patient handoffs (e.g., computer-assisted or paper-based), the best way to ensure effective handoffs of hospitalized patients was “precise, unambiguous, face-to-face communication.”1
In a 2001 study by Hruby, Pantilat, and colleagues at UCSF, the authors found that, for the most part, hospitalized patients with PCPs wanted contact with their primary physicians even while in the hospital. Approximately half of the surveyed patients also believed that the PCP, rather than an inpatient physician, should be the first to discuss with them serious diagnoses or disease management choices.2 Preferences such as those expressed in this study may play into referring physicians’ reluctance to make use of hospitalist services, says Dr. Bolinger. They may fear that patients will feel abandoned by the primary physician. Dr. Bolinger’s response to those sentiments: “Initially, some patients [in our hospital] were a little guarded and were not sure what to expect. But after a day or two of having us there, they are generally very, very pleased to have us on board. We are part of their medical team now.”
A Need for Marketing?
Dr. Becker has been actively developing a hospital medicine program at Medical Center Hospital for the past two years and joined SHM as part of that effort. Familiarizing himself with the tenets of hospital medicine, he discovered that, as a family doctor, “unknowingly, I was actually practicing hospital medicine for 20 years!”
As part of the hospital medicine program development process, he has solicited input from local physicians as well as patients. A simple survey to assess interest in a hospitalist program asked potential referring physicians, Would you use a hospitalist? Would you use a hospitalist after waiting a while to see how the process goes? Or, would you not consider using a hospitalist?
In two years, says Dr. Becker, response from the referring physician community has changed from “bah, humbug” to one of readiness for the program.
A mass mailing can serve to introduce a hospital medicine program in a community. Dr. Bolinger’s group used this method and, in his experience, local subspecialists—orthopedists, cardiologists, endocrinologists, pulmonologists—have proved the biggest source of referrals to their program. But PCPs are starting to use the hospitalist service for vacations and call-coverage issues and are beginning to value hospitalists’ services. “Physicians like coming to the hospital, but they’re starting to realize that the hospitalist program is a better system,” says Dr. Bolinger.
Dr. Nelson has been a hospitalist for 18 years. For most of that time he has had no shortage of referred patients. In fact, the bigger problem has been finding enough doctors to join the group and handle the existing referral volume. In that situation, it has not made sense to undertake marketing with the goal of increasing referrals. However, he advises, “It is always worth spending time and energy trying to maintain good relationships with physicians with whom you regularly share patients, and perhaps this could be called ‘marketing.’”
To maintain good relationships with referring physicians, his group conducts a survey on a yearly basis. A survey, he suggests, should be very short, consisting of only a few key questions, such as:
- Do we send reports promptly to your practice?
- Are your patients satisfied with the care they receive from us?
- Do you have any comments or feedback for our group?
Although his group gains information from these surveys, Dr. Nelson notes that the greater value of conducting such surveys may be in building public relations capital. By conducting a survey, hospitalists demonstrate that they care enough to ask for their referring physicians’ input.
Another good marketing tool is a patient education brochure, given to referring physicians, that explains hospitalists and hospitalist care. These brochures can help referring physicians prepare their patients for seeing a hospitalist in the inpatient setting, thus easing the initial reluctance patients sometimes experience when encountering a new physician.
Conclusion
On the cusp of launching his medical center’s hospital medicine program, Dr. Becker sees that good communication between referring physicians and hospitalists will ensure the program’s success. He advises physicians to remember their classes in communication as third-year medical students, when most participate in videotaped patient encounters. It’s always instructive, he says, to see how we come across to others in conversation.
Both verbal and nonverbal cues play a part in good communication. A 2003 study by Griffith and colleagues concluded that better nonverbal communication skills are associated with greater patient satisfaction, and that formal instruction in nonverbal communication can be a good addition to residency training.3
“I find that doctors talk to each other, in general, very easily,” says Dr. Becker. Sometimes [good communication] is just a matter of opening that door and essentially keeping the former attending, the PCP, apprised of what is going on.”
When hospitalists attend to thorough communication and promptly deliver complete discharge summaries, family physicians can report to their patients that they know what happened in the hospital and poll their patients about their experiences in the hospital. In this way, hospitalists and referring physicians can cement their relationship as team members for the patient. The success of any hospitalist program, Dr. Becker believes, lies in “making sure you fulfill the promise of what hospital medicine generates, and that is a continuity of care … , obtaining front-end communication so that patients get the best care throughout their [hospital] stay, and then follow up with discharge summaries to the primary physician’s office.” TH
Gretchen Henkel is a regular contributor to The Hospitalist.
References
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12): 1094-1099.
- Hruby M, Pantilat SZ, Lo B. How do patients view the role of the primary care physician in inpatient care? Am J Med. 2001;21;111(9B):21S-25S.
- Griffith CH III, Wilson JF, Langer S, et al. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003 Mar;18(3):170-174.
If the secret to successful real estate investing is “location, location, location,” the key to maintaining good relationships with referring physicians is “communication, communication, communication.” While this may seem simplistic, the complexities of interpersonal communications can pose challenges even in the most straightforward of physician interchanges.
Recent studies and hospitalists consulted for this report maintain that hospitalists’ communications with referring physicians must be examined, practiced, and fine-tuned continually to ensure satisfaction for doctors—and their patients.
“It’s all about the communication,” says Bruce Becker, MD, chief medical officer at Medical Center Hospital in Odessa, Texas, and a family physician and professor of medicine for more than 20 years. “It’s sometimes not what you say, but how you say it.”
According to John Nelson, MD, medical director of the Hospitalist Practice at Overlake Hospital in Bellevue, Wash., a consultant for hospital medicine groups with Nelson/Flores Associates and a columnist for The Hospitalist (“Practice Management”), it is key for hospitalists to examine and revise oral and written communication processes—especially at critical points during patient handoffs—rather than to assume that good communication will just happen naturally.
Gaining Acceptance
Some primary care physicians (PCPs) are more willing than others to refer patients to a hospitalist. Initially, new programs may have to work hard to gain acceptance with referring physicians. Some referring physicians may not be ready to give up hospital visits and may want to maintain collegiality and control. On the other hand, some family physicians are “ready to step away from hospital practice,” says Dr. Becker, citing diminishing reimbursements due to diagnosis-related groups (DRGs) and managed care.
John A. Bolinger, DO, FACP, medical director of the Hospitalist Program at Terre Haute (Ind.) Regional Hospital, believes that one way to promote a hospitalist program to PCPs is to emphasize hospitalists’ levels of training and efficiency.
“I try to make them aware of how [our hospitalist program] can be advantageous to them,” he explains. “Even if they have only one patient in the hospital, by the time they drive there, get the chart, make the rounds, make their notes, and do the required paperwork, it may take them an hour to see one patient. It makes good economic sense for them to stay in their offices, where they can see a minimum of four patients in the same amount of time for equal or better reimbursements.”
When primary care physicians voice resistance to using a hospitalist program, Dr. Bolinger says he tries to impress upon them the fact that hospitalists do not have outside practices, they will “never try to steal patients,” they stay within referral patterns, and they will make sure that PCPs get pertinent records as soon as possible. Dr. Bolinger believes referring physicians’ biggest concern when dealing with hospitalists is that they “don’t want to lose control.” The way to address those fears is to make sure referring physicians are always kept in the communications loop regarding their patients’ progress.
The policy for Dr. Bolinger’s hospitalist program is to make sure all dictated reports are transcribed and faxed immediately to the referring physician’s office. All scheduled follow-up appointments and medication changes are included in discharge summaries. “If need be,” says Dr. Bolinger, “we will even hand deliver information to physicians’ offices, which we have done multiple times.”
Become User-Friendly
The methods Dr. Bolinger describes often result in referring physicians’ satisfaction with hospitalist services, followed by increased referrals. Hospitalists can ensure continued referrals from their PCPs if they remember hospital medicine’s cardinal rules of availability and prompt, thorough reporting, says Dr. Nelson. It can help to view the interface with the hospitalist service from the PCP’s point of view.
For instance, how can physicians quickly reach the hospitalist service? “If you’re a referring doctor and you’ve got a patient in your office whom you think should be admitted today, who do you call? This can actually be a little tricky for most practices,” says Dr. Nelson. “Every practice should give some thought to making that contact as easy for the referring doctors as possible.”
Some important questions to ask: When trying to reach a hospitalist, is it best to call the group’s main number? Will a voicemail message be returned within an hour? Two hours? Is it better to call the hospital operator and have the hospitalist paged? Or do PCPs have access to hospitalists’ cell phone numbers?
Dr. Nelson suggests that hospitalist groups also give thought to standardizing admission and discharge reports, as well as other forms. Often, individual members of a hospitalist group use slightly different formats for reporting to referring physicians. He points out that this can be less user friendly for the reader, who may have a harder time scanning the document quickly to find a particular piece of important information. Other useful suggestions for making reports user friendly: Use similar headings on all reports; avoid dense text; list pending tests in a prominent place in the report document; and consider highlighting or underlining key words.
Preference for In-Person Contact
For a new hospitalist practice, telephone communication between the hospitalist and the primary physician is valuable, and the hospitalist should “pick up the phone liberally,” says Dr. Nelson.
Dr. Becker believes the best way for physicians to communicate is one on one—in person. “Too often,” he says, “we get used to communicating through a third party—usually a unit clerk, a nurse, or a resident. I believe that physician-to-physician communication is the ideal. If the attending physician and the consultant [hospitalist or subspecialist] speak in person, they can explain their thinking to each other, and “within one minute of precious time, figure out which way to go.”
In this way, without wasting time, the physician gives the consultant guidance as to the appropriate track to take and can also listen to the consultant’s suggestions.
“I feel that medicine has perhaps gotten a little bit away from that communication link,” continues Dr. Becker. “When we get further away from that direct communication—whether it is between doctors and consultants, nurses and doctors, or doctors and family members—you take that little bit of risk that there will be a missed step, either on the part of the communicator or on the receiving end as the listener.”
In a study exploring barriers to effective patient handoffs, Solet and colleagues focused on the communication between physicians as a vital link in patient care continuity. The authors concluded that, regardless of the method of managing patient handoffs (e.g., computer-assisted or paper-based), the best way to ensure effective handoffs of hospitalized patients was “precise, unambiguous, face-to-face communication.”1
In a 2001 study by Hruby, Pantilat, and colleagues at UCSF, the authors found that, for the most part, hospitalized patients with PCPs wanted contact with their primary physicians even while in the hospital. Approximately half of the surveyed patients also believed that the PCP, rather than an inpatient physician, should be the first to discuss with them serious diagnoses or disease management choices.2 Preferences such as those expressed in this study may play into referring physicians’ reluctance to make use of hospitalist services, says Dr. Bolinger. They may fear that patients will feel abandoned by the primary physician. Dr. Bolinger’s response to those sentiments: “Initially, some patients [in our hospital] were a little guarded and were not sure what to expect. But after a day or two of having us there, they are generally very, very pleased to have us on board. We are part of their medical team now.”
A Need for Marketing?
Dr. Becker has been actively developing a hospital medicine program at Medical Center Hospital for the past two years and joined SHM as part of that effort. Familiarizing himself with the tenets of hospital medicine, he discovered that, as a family doctor, “unknowingly, I was actually practicing hospital medicine for 20 years!”
As part of the hospital medicine program development process, he has solicited input from local physicians as well as patients. A simple survey to assess interest in a hospitalist program asked potential referring physicians, Would you use a hospitalist? Would you use a hospitalist after waiting a while to see how the process goes? Or, would you not consider using a hospitalist?
In two years, says Dr. Becker, response from the referring physician community has changed from “bah, humbug” to one of readiness for the program.
A mass mailing can serve to introduce a hospital medicine program in a community. Dr. Bolinger’s group used this method and, in his experience, local subspecialists—orthopedists, cardiologists, endocrinologists, pulmonologists—have proved the biggest source of referrals to their program. But PCPs are starting to use the hospitalist service for vacations and call-coverage issues and are beginning to value hospitalists’ services. “Physicians like coming to the hospital, but they’re starting to realize that the hospitalist program is a better system,” says Dr. Bolinger.
Dr. Nelson has been a hospitalist for 18 years. For most of that time he has had no shortage of referred patients. In fact, the bigger problem has been finding enough doctors to join the group and handle the existing referral volume. In that situation, it has not made sense to undertake marketing with the goal of increasing referrals. However, he advises, “It is always worth spending time and energy trying to maintain good relationships with physicians with whom you regularly share patients, and perhaps this could be called ‘marketing.’”
To maintain good relationships with referring physicians, his group conducts a survey on a yearly basis. A survey, he suggests, should be very short, consisting of only a few key questions, such as:
- Do we send reports promptly to your practice?
- Are your patients satisfied with the care they receive from us?
- Do you have any comments or feedback for our group?
Although his group gains information from these surveys, Dr. Nelson notes that the greater value of conducting such surveys may be in building public relations capital. By conducting a survey, hospitalists demonstrate that they care enough to ask for their referring physicians’ input.
Another good marketing tool is a patient education brochure, given to referring physicians, that explains hospitalists and hospitalist care. These brochures can help referring physicians prepare their patients for seeing a hospitalist in the inpatient setting, thus easing the initial reluctance patients sometimes experience when encountering a new physician.
Conclusion
On the cusp of launching his medical center’s hospital medicine program, Dr. Becker sees that good communication between referring physicians and hospitalists will ensure the program’s success. He advises physicians to remember their classes in communication as third-year medical students, when most participate in videotaped patient encounters. It’s always instructive, he says, to see how we come across to others in conversation.
Both verbal and nonverbal cues play a part in good communication. A 2003 study by Griffith and colleagues concluded that better nonverbal communication skills are associated with greater patient satisfaction, and that formal instruction in nonverbal communication can be a good addition to residency training.3
“I find that doctors talk to each other, in general, very easily,” says Dr. Becker. Sometimes [good communication] is just a matter of opening that door and essentially keeping the former attending, the PCP, apprised of what is going on.”
When hospitalists attend to thorough communication and promptly deliver complete discharge summaries, family physicians can report to their patients that they know what happened in the hospital and poll their patients about their experiences in the hospital. In this way, hospitalists and referring physicians can cement their relationship as team members for the patient. The success of any hospitalist program, Dr. Becker believes, lies in “making sure you fulfill the promise of what hospital medicine generates, and that is a continuity of care … , obtaining front-end communication so that patients get the best care throughout their [hospital] stay, and then follow up with discharge summaries to the primary physician’s office.” TH
Gretchen Henkel is a regular contributor to The Hospitalist.
References
- Solet DJ, Norvell JM, Rutan GH, et al. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005 Dec;80(12): 1094-1099.
- Hruby M, Pantilat SZ, Lo B. How do patients view the role of the primary care physician in inpatient care? Am J Med. 2001;21;111(9B):21S-25S.
- Griffith CH III, Wilson JF, Langer S, et al. House staff nonverbal communication skills and standardized patient satisfaction. J Gen Intern Med. 2003 Mar;18(3):170-174.
Massachusetts Healthcare Reform
Like the community organizations that must increase outreach efforts to formerly disenfranchised healthcare consumers, the administrators who fulfill the law’s mandates, and citizens who will be comparing new health plans, hospitalists may find themselves working harder once the law is implemented.
Massachusetts’ lawmakers garnered huge headlines across the nation in April when the Democratic-dominated state legislature passed a health insurance reform bill nearly unanimously, and Republican Governor Mitt Romney signed the bill into law. This summer, health policy experts are hard at work implementing the first of many mandated stages of the legislation. Other states will watch Massachusetts in the next year as administrators hammer out details of the much-heralded bipartisan statute. Much remains to be done, however, and effects of the statute on patients, hospitals, and physicians remain unclear.
The hope is that the state can ensure nearly universal health insurance coverage for its estimated 500,000 citizens who currently have none. The Massachusetts statute aims to accomplish this feat by offering subsidized insurance coverage to those earning up to 300% of the federal poverty level (facilitated by a Medicaid waiver now being finalized between the state and CMS); assessing $295 per employee from businesses with 11 or more employees who do not provide coverage; and requiring purchase of affordable individual insurance products by those to whom such products are available.
Can the complex, market-driven compromise work? If all staged implementations go into effect as planned, will they be sustainable? Once in place, how might these reforms play out for the practice of hospital medicine? The Hospitalist recently solicited opinions from several hospitalists, physicians, a network president, and health policy experts to get some idea of what the future may hold for healthcare delivery in Massachusetts.
Key Features of the Legislation
As the number of uninsured Americans continues to grow, and reform at the federal level has stalled, many states have been working on their own plans to increase access to insurance and healthcare. The linchpin of individuals’ and businesses’ shared responsibility, health policy experts say, was key to the bipartisan support shown for the Massachusetts insurance reform bill. As of July 1, 2007, every citizen over 18 will be required to obtain health insurance. Businesses with 11 or more employees must pay $295 per employee if they do not offer coverage. (This provision was vetoed by Governor Romney when he signed the bill, but it was subsequently overridden by the legislature.)
The legislation—hundreds of pages long—stipulates an approximate two-year timeline for implementing all phases of the plan, and includes state tax penalties for individuals who don’t comply with the requirement to obtain insurance. The law also creates a state authority, The Commonwealth Health Insurance Connector, to set eligibility standards for subsidized policies, expand Medicaid enrollment, determine affordability guidelines, and approve of plans submitted by private insurers to be offered to consumers. It is anticipated that The Connector (its nickname) will act as a clearinghouse, linking individuals and small businesses with choices of affordable health plans paid for with pretax dollars.
Some of the features lauded by most—even critics—include expansion of Medicaid enrollment; policies with no to low premiums and no deductibles, on a sliding scale, for individuals and families earning up to 300% of the federal poverty line ($29,400 for individuals and $60,000 for families in the contiguous 48 states); and portability of the policies. In addition, young adults can remain covered through their parents’ policies until they become independent or reach age 25. Other specially designed low cost, limited coverage plans will be offered to young adults between ages 19 and 26.
In the press, the statute has been touted as providing “universal care,” but critics doubt that the coverage will be truly universal. For instance, they claim, based on U.S. Census data, that the number of uninsured in Massachusetts is closer to 714,000—not the 500,000 that resulted from bilingual telephone surveys used by those who drafted the bill. Those who espouse a single-payer solution to the insurance crisis, such as Physicians for a National Health Policy and Mass-Care (the statewide coalition of organizations that back single-payer healthcare), argue that mandating purchase of individual plans will shut many working families out of the market. Even administrators and physicians interviewed for this article admit that to generate affordable policies, insurers may have to limit networks and benefits. And increasing the number of insured citizens may have no effect on the rising tide of healthcare delivery costs. With so many unknowns, and a complicated administrative system to initiate, the task of fulfilling the statute’s mandate is daunting.
Where It Is Now
Reached in mid-July between meetings, Jon M. Kingsdale, PhD, newly appointed executive director of the Commonwealth Health Insurance Connector Authority, reported that his board had met five times since June 7. Included in its busy schedule: generating a plan of operations and a budget and hiring staff. The Connector also met its first legislative deadline, which was to develop and issue regulations and criteria by July 1, 2006, for contracting with health plans for the Commonwealth Care Health Insurance Program, or C-CHIP. This is the state-subsidized health plan for people earning up to 300% of the federal poverty line that will begin on October 1, 2006. Key features of C-CHIP and other components of the Massachusetts health reform include no premiums for those who earn less than 100% of the federal poverty line, increased coverage for children, and increased Medicaid reimbursement rates for providers (a good thing for hospitals). Premiums for those earning 100%-300% of the federal poverty line will be set according to a sliding scale, but none of the C-CHIP plans include deductibles. Funding for this plan will come from federal and state matching Medicaid funds made possible by a waiver currently being negotiated between Massachusetts and CMS. (Formal approval had not yet been granted by CMS as of July 21.)
As to the insurance products for those earning above 300% of the federal poverty level, Dr. Kingsdale says The Connector board will address affordability criteria once C-CHIP deadlines have been met. The legislation calls for The Connector to provide its seal of approval for plans that are offered and make determinations about continuing or withdrawing approval. After two years, the agency will formally evaluate the program and make recommendations for changes.
Reactions to the Plan
Joseph Li, MD, assistant professor of medicine at Harvard Medical School and director of the Hospital Medicine Program at Beth Israel Deaconess Medical Center in Boston, admits that his excitement about the insurance statute is somewhat tempered. His personal opinion, which does not reflect his group’s or hospital’s opinion—is that he will “believe it when it’s truly enacted.”
Massachusetts has passed healthcare care reform bills in the past: Witness the 1988 legislation under Governor Michael Dukakis that was later repealed. Nevertheless, Dr. Li says, “I’m glad to see it happen. A lot of people have been wondering how we are going to address the issue of the 45 million uninsured in this country. This is one step toward that, but there are really a lot of ifs, ands, and buts on whether it will truly be pulled off in a year or two.”
Shortly after the ceremonial signing of the bill in early April, Nancy C. Turnbull, president of the Blue Cross Blue Shield of Massachusetts Foundation, co-wrote an editorial with Philip W. Johnston, calling the legislation a “bold insurance experiment.” Both Turnbull and Johnston were part of the Dukakis team that helped create that administration’s 1988 healthcare reform bill, which was later repealed. In their 4/16/06 Boston Globe editorial, the authors noted that the consensus for passing the April legislation bodes well for the plan. Recently, Turnbull said she was still optimistic about the workability of the reform.
Praising The Connector’s “aggressive implementation schedule” (for the expanded Medicaid coverage and the C-CHIP), Turnbull points out that outreach and public education will be key to the success of the plan’s subsidized coverage components. To that end, she anticipates that the Foundation will fund grants to community-based organizations to help them with the “significant new responsibilities” of community outreach to enroll those eligible.
What’s “Affordable?”
The individual mandate deadline is July 1, 2007, and before that date The Connector is charged with making determinations about affordability standards. “Over the next six months,” explains Turnbull, “they will have to decide what portion of household income it is reasonable to expect people to contribute toward health coverage.”
People such as Steffie Woolhandler, MD, MPH, a primary care physician in the Department of Medicine, Cambridge Hospital and Harvard Medical School (Boston) and a co-founder of Physicians for a National Health Program, which favors a single-payer system, worry that insurers will rely on high deductibles and co-pays to make premiums affordable.
“Consumer-directed healthcare is terrible for patients,” says Dr. Woolhandler. And under the payment structure of high-deductible insurance policies, “payment is terrible for docs because most of what we bill is in that early part of spending before the deductible [is met].
“I’m a primary care doc,” she continues, “and most patients who come to my office would be paying out of pocket in that consumer-directed healthcare situation.”
Calling the statute a hoax, Dr. Woolhandler maintains that it won’t achieve universal healthcare, and, in fact, will financially penalize working families.
Turnbull acknowledges that concerns such as those voiced by Dr. Woolhandler are well-founded because insurers and employers have traditionally resorted to increased cost-sharing to regulate premiums. However, she says, “If we don’t find ways to make good coverage more affordable, then the individual mandate will not go into effect for many people.”
Asked what he would say to critics who do not think private insurance companies can structure products that are both affordable and of good quality, Dr. Kingsdale says, “It’s up to them [the insurance companies] to prove you wrong. A well-functioning market with a lot of good information, which is what this reform calls for, can improve upon the plans available to what is perhaps the least well-functioning part of the existing insurance market: the non-group and small-group insurance market.”
Determination of good quality, affordable benefit packages will be a difficult decision. “In my personal view, I think we will have failed if, as a result of the mandate, we succeed only in requiring people to purchase coverage that is not adequate,” says Turnbull, “because then we will have traded ‘un-insurance’ for underinsurance, and that’s not a good policy outcome either.”

—Joseph Li, MD
Some Likely Effects
For his hospitalist group at University of Massachusetts (UMass) Memorial Medical Center in Worcester, the new legislation “will not represent any new change in our mission or change in the composition of our typical patient panels,” says Glenn Allison, MD, chief of the Division of Hospital Medicine.
Hospitalists, in general, are accustomed to and adept at caring for unassigned patients included in the uncompensated pool, he notes, and at UMass, caring for these patients is a major mission of the hospital. Dr. Allison is hopeful that the legislation holds promise for bringing many previously marginalized and uninsured people into the healthcare system.
Thomas H. Lee, MD, MPH, network president of Partners HealthCare System, Inc, Boston, believes everyone in Massachusetts wants the healthcare reform to work. All stakeholders must “face reality,” he says, and realize that lowering the cost of healthcare is imperative. “It’s clear that the whole healthcare system must become more efficient. The imperative for that was present before this legislation was passed, and I’m not sure the pressures for that imperative are going to change qualitatively.”
One change Dr. Lee does foresee due to the legislation’s dependence on market reforms is that resulting insurance products will “spend a lot less money on patients than existing ones do. There are going to be a variety of pressures on doctors and hospitals to either be much more efficient or take less money for what they do,” he says. “Given that choice, most of us would rather become more efficient.”
Another consequence of affordable insurance products may be a narrowing of provider networks. And a narrow network product, says Sylvia C.W. McKean, MD, FACP, medical director of the BWH/Faulkner Hospitalist Service at Brigham and Women’s Hospital in Boston, “might result in a reduced number of patients going to tertiary care hospitals, which currently care for a large number of indigent patients.”
Even though standards of affordability and details of insurance products have yet to be generated by The Connector and insurers, Dr. Lee also believes that narrowing of benefits and networks will be one likely consequence of the legislation. This will entail some difficult choices about the range of services hospitals and physicians can offer. But, he says, “I think it’s worth doing painful, difficult stuff, and making painful, ugly choices in order for everyone to have necessary catastrophic care and to have access to basic preventive care. We should be willing to live with some of that ugly stuff because it will, in Massachusetts, at least, give us a chance of preventing the need for even uglier outcomes, which is, 10% of our population not having any coverage at all.”
Dr. Lee believes that hospitalists will be critical to the success of hospital efficiency. “To the extent that institutions can use hospitalists and other systems to become much more efficient and reduce readmissions, it’s going to mitigate the need for the narrowing of benefits and networks,” he says.

—Glenn Allison, MD
Upshot for Hospitalists
Unknowns about the workability of and funding for the legislation abound. It’s not clear whether shifting costs to individuals (by mandating they purchase private insurance) and employers (via the $295 per employee fee) can bridge current deficits in compensation and care. Dr. Lee points out that “it’s still an open question of whether there is going to be enough money. But clearly, there are going to be insurance products that spend a lot less money on patients than existing ones do.”
Dr. Li does not believe these funding questions will affect the bottom line for his hospitalist group because their compensation is based on productivity, as measured by relative value units (RVUs).
The next 10 months or so leading up to the July 1, 2007, deadline for purchase of individual health insurance policies will be revealing for consumers and physicians alike. Although the devil will be in the details, Dr. Lee notes, “The big picture is not uncertain. We know there is going to be more transparency, more data, on quality and efficiency.”
That means that hospitals’ delivery of care will endure more scrutiny, and that pay for performance will become commonplace.
The influx of patients into the healthcare system, which legislators hope will be a consequence of greater access to care, will necessitate some consciousness-raising for hospitalists, Dr. Allison maintains. While hospitalists already work closely with other providers on the multidisciplinary team (social workers, case managers, and primary care physicians), they will have to strengthen those collaborations to ensure that patients don’t fall through the cracks. Community outreach may become part of the hospitalists’ job description.
For example, he explains, many preventive or follow-up services that are now being performed in the hospital because patients have no primary care physicians can now be referred to outpatient sites. “Now that these people will have doctors and will be tied into the healthcare system, these services can be performed in the right setting, instead of using more expensive inpatient resources,” he says.
Steering patients to community-based preventive services, such as early cardiac and cancer screenings, will fall to hospitalists, who will be “on the frontlines seeing these patients and referring them appropriately as they leave the hospital,” says Dr. Allison. Hospitalists and all providers will also be evaluated by how well they deliver culturally competent care—another mandate of the statute. To steer through these changes, hospitalists must become much more conscious, he says, of costs, communications, referrals, and resources. “That, as far as I can see, has not been a major emphasis of hospitalist literature or debate.”
A Role to Play
Dr. McKean and others contend that by virtue of their skill set and core mission, hospitalists will have much to contribute toward moderating the costs of healthcare. “The good news for hospitalists,” says Turnbull, “is that if we’re successful in providing health coverage to many people who are now uninsured and if that coverage is adequate there should be more people receiving primary and preventive care and services. This should prevent them from needing to go to the hospital in the first place. We should also be able to create more rational systems of care for people, so that when patients are in the hospital, they need to be there, and they can take full advantage of the talents and contributions that hospitalists make.”
Dr. Kingsdale agrees with the assessment that hospitalists will have a potentially significant role to play in improving the delivery, efficiency, and quality of care, as well as reducing medical errors. He hopes the new insurance products generated by companies will include financial incentives for hospitals and other providers who will be doing “the difficult work of changing their systems of care.”
“The healthcare system really has to improve,” asserts Dr. Lee. “In our organization, we say that we need both an industrial revolution and a cultural revolution, where we develop and use systems that reduce errors. There are electronic records and other industrial systems, and then there are human-ware systems, like hospitalists and disease management programs.”
Like the community organizations that must increase outreach efforts to formerly disenfranchised healthcare consumers, the administrators who fulfill the law’s mandates, and citizens who will be comparing new health plans, hospitalists may find themselves working harder once the law is implemented. The April legislation “elevates the stakes for delivering effective, quality inpatient care,” says Dr. Allison. “I don’t want to over-inflate our importance, but I do think in a system where so many of our healthcare dollars are expended on the inpatient side, we’ve got to be extremely conscious of what we do.” This may mean shifting hospitalists’ implicit skills into the explicit realm, he says: “For instance, everyone talks about guidelines and how helpful they are, but we don’t do a good enough job when it comes to using them. We need to do better with vaccination, with discharge instructions, and with communicating and coordinating care.
“I think the care coordination piece is going to be the key to success,” concludes Dr. Allison. “I think we need to take what we do now, but do more of it, and do a better job of it. That is something that will make a tough job even tougher. But I think if we fail in this, the whole effort may collapse.” TH
Gretchen Henkel is coauthor of Marketing Your Clinical Practice—Ethically, Effectively, Economically.
Resources
- Altman SH, Doonan M. “Can Massachusetts lead the way in health care reform?” N Engl J Med. 2006 May;354(20):2093-2095.
- Steinbrook R. Health care reform in Massachusetts—a work in progress. N Engl J Med. 2006 May;354(20): 2095-2098.
- The 184th General Court of the Commonwealth of Massachusetts. Chapter 58 of the Acts of 2006, an act providing access to affordable, quality, accountable health care. Available at: www.mass.gov/legis/summary.pdf). Last accessed June 12, 2006.
- Johnston PW, Turnbull NC. A bold insurance experiment. The Boston Globe. April 16, 2006. Available at: www.boston.com. Last accessed June 26, 2006.
- McCormick D, Himmelstein DU, Woolhandler S, et al. Single-payer national health insurance. Physicians’ views. Arch Intern Med. 2004 Feb 9;164(3):300-304.
- “Massachusetts Health Reform Bill: A False Promise of Universal Coverage.” Statement by Steffie Woolhandler, MD, MPH and David U. Himmelstein, MD. Available at www.pnhp.org/news/2006/april/massachusetts_health.php. Last accessed June 26, 2006.
Like the community organizations that must increase outreach efforts to formerly disenfranchised healthcare consumers, the administrators who fulfill the law’s mandates, and citizens who will be comparing new health plans, hospitalists may find themselves working harder once the law is implemented.
Massachusetts’ lawmakers garnered huge headlines across the nation in April when the Democratic-dominated state legislature passed a health insurance reform bill nearly unanimously, and Republican Governor Mitt Romney signed the bill into law. This summer, health policy experts are hard at work implementing the first of many mandated stages of the legislation. Other states will watch Massachusetts in the next year as administrators hammer out details of the much-heralded bipartisan statute. Much remains to be done, however, and effects of the statute on patients, hospitals, and physicians remain unclear.
The hope is that the state can ensure nearly universal health insurance coverage for its estimated 500,000 citizens who currently have none. The Massachusetts statute aims to accomplish this feat by offering subsidized insurance coverage to those earning up to 300% of the federal poverty level (facilitated by a Medicaid waiver now being finalized between the state and CMS); assessing $295 per employee from businesses with 11 or more employees who do not provide coverage; and requiring purchase of affordable individual insurance products by those to whom such products are available.
Can the complex, market-driven compromise work? If all staged implementations go into effect as planned, will they be sustainable? Once in place, how might these reforms play out for the practice of hospital medicine? The Hospitalist recently solicited opinions from several hospitalists, physicians, a network president, and health policy experts to get some idea of what the future may hold for healthcare delivery in Massachusetts.
Key Features of the Legislation
As the number of uninsured Americans continues to grow, and reform at the federal level has stalled, many states have been working on their own plans to increase access to insurance and healthcare. The linchpin of individuals’ and businesses’ shared responsibility, health policy experts say, was key to the bipartisan support shown for the Massachusetts insurance reform bill. As of July 1, 2007, every citizen over 18 will be required to obtain health insurance. Businesses with 11 or more employees must pay $295 per employee if they do not offer coverage. (This provision was vetoed by Governor Romney when he signed the bill, but it was subsequently overridden by the legislature.)
The legislation—hundreds of pages long—stipulates an approximate two-year timeline for implementing all phases of the plan, and includes state tax penalties for individuals who don’t comply with the requirement to obtain insurance. The law also creates a state authority, The Commonwealth Health Insurance Connector, to set eligibility standards for subsidized policies, expand Medicaid enrollment, determine affordability guidelines, and approve of plans submitted by private insurers to be offered to consumers. It is anticipated that The Connector (its nickname) will act as a clearinghouse, linking individuals and small businesses with choices of affordable health plans paid for with pretax dollars.
Some of the features lauded by most—even critics—include expansion of Medicaid enrollment; policies with no to low premiums and no deductibles, on a sliding scale, for individuals and families earning up to 300% of the federal poverty line ($29,400 for individuals and $60,000 for families in the contiguous 48 states); and portability of the policies. In addition, young adults can remain covered through their parents’ policies until they become independent or reach age 25. Other specially designed low cost, limited coverage plans will be offered to young adults between ages 19 and 26.
In the press, the statute has been touted as providing “universal care,” but critics doubt that the coverage will be truly universal. For instance, they claim, based on U.S. Census data, that the number of uninsured in Massachusetts is closer to 714,000—not the 500,000 that resulted from bilingual telephone surveys used by those who drafted the bill. Those who espouse a single-payer solution to the insurance crisis, such as Physicians for a National Health Policy and Mass-Care (the statewide coalition of organizations that back single-payer healthcare), argue that mandating purchase of individual plans will shut many working families out of the market. Even administrators and physicians interviewed for this article admit that to generate affordable policies, insurers may have to limit networks and benefits. And increasing the number of insured citizens may have no effect on the rising tide of healthcare delivery costs. With so many unknowns, and a complicated administrative system to initiate, the task of fulfilling the statute’s mandate is daunting.
Where It Is Now
Reached in mid-July between meetings, Jon M. Kingsdale, PhD, newly appointed executive director of the Commonwealth Health Insurance Connector Authority, reported that his board had met five times since June 7. Included in its busy schedule: generating a plan of operations and a budget and hiring staff. The Connector also met its first legislative deadline, which was to develop and issue regulations and criteria by July 1, 2006, for contracting with health plans for the Commonwealth Care Health Insurance Program, or C-CHIP. This is the state-subsidized health plan for people earning up to 300% of the federal poverty line that will begin on October 1, 2006. Key features of C-CHIP and other components of the Massachusetts health reform include no premiums for those who earn less than 100% of the federal poverty line, increased coverage for children, and increased Medicaid reimbursement rates for providers (a good thing for hospitals). Premiums for those earning 100%-300% of the federal poverty line will be set according to a sliding scale, but none of the C-CHIP plans include deductibles. Funding for this plan will come from federal and state matching Medicaid funds made possible by a waiver currently being negotiated between Massachusetts and CMS. (Formal approval had not yet been granted by CMS as of July 21.)
As to the insurance products for those earning above 300% of the federal poverty level, Dr. Kingsdale says The Connector board will address affordability criteria once C-CHIP deadlines have been met. The legislation calls for The Connector to provide its seal of approval for plans that are offered and make determinations about continuing or withdrawing approval. After two years, the agency will formally evaluate the program and make recommendations for changes.
Reactions to the Plan
Joseph Li, MD, assistant professor of medicine at Harvard Medical School and director of the Hospital Medicine Program at Beth Israel Deaconess Medical Center in Boston, admits that his excitement about the insurance statute is somewhat tempered. His personal opinion, which does not reflect his group’s or hospital’s opinion—is that he will “believe it when it’s truly enacted.”
Massachusetts has passed healthcare care reform bills in the past: Witness the 1988 legislation under Governor Michael Dukakis that was later repealed. Nevertheless, Dr. Li says, “I’m glad to see it happen. A lot of people have been wondering how we are going to address the issue of the 45 million uninsured in this country. This is one step toward that, but there are really a lot of ifs, ands, and buts on whether it will truly be pulled off in a year or two.”
Shortly after the ceremonial signing of the bill in early April, Nancy C. Turnbull, president of the Blue Cross Blue Shield of Massachusetts Foundation, co-wrote an editorial with Philip W. Johnston, calling the legislation a “bold insurance experiment.” Both Turnbull and Johnston were part of the Dukakis team that helped create that administration’s 1988 healthcare reform bill, which was later repealed. In their 4/16/06 Boston Globe editorial, the authors noted that the consensus for passing the April legislation bodes well for the plan. Recently, Turnbull said she was still optimistic about the workability of the reform.
Praising The Connector’s “aggressive implementation schedule” (for the expanded Medicaid coverage and the C-CHIP), Turnbull points out that outreach and public education will be key to the success of the plan’s subsidized coverage components. To that end, she anticipates that the Foundation will fund grants to community-based organizations to help them with the “significant new responsibilities” of community outreach to enroll those eligible.
What’s “Affordable?”
The individual mandate deadline is July 1, 2007, and before that date The Connector is charged with making determinations about affordability standards. “Over the next six months,” explains Turnbull, “they will have to decide what portion of household income it is reasonable to expect people to contribute toward health coverage.”
People such as Steffie Woolhandler, MD, MPH, a primary care physician in the Department of Medicine, Cambridge Hospital and Harvard Medical School (Boston) and a co-founder of Physicians for a National Health Program, which favors a single-payer system, worry that insurers will rely on high deductibles and co-pays to make premiums affordable.
“Consumer-directed healthcare is terrible for patients,” says Dr. Woolhandler. And under the payment structure of high-deductible insurance policies, “payment is terrible for docs because most of what we bill is in that early part of spending before the deductible [is met].
“I’m a primary care doc,” she continues, “and most patients who come to my office would be paying out of pocket in that consumer-directed healthcare situation.”
Calling the statute a hoax, Dr. Woolhandler maintains that it won’t achieve universal healthcare, and, in fact, will financially penalize working families.
Turnbull acknowledges that concerns such as those voiced by Dr. Woolhandler are well-founded because insurers and employers have traditionally resorted to increased cost-sharing to regulate premiums. However, she says, “If we don’t find ways to make good coverage more affordable, then the individual mandate will not go into effect for many people.”
Asked what he would say to critics who do not think private insurance companies can structure products that are both affordable and of good quality, Dr. Kingsdale says, “It’s up to them [the insurance companies] to prove you wrong. A well-functioning market with a lot of good information, which is what this reform calls for, can improve upon the plans available to what is perhaps the least well-functioning part of the existing insurance market: the non-group and small-group insurance market.”
Determination of good quality, affordable benefit packages will be a difficult decision. “In my personal view, I think we will have failed if, as a result of the mandate, we succeed only in requiring people to purchase coverage that is not adequate,” says Turnbull, “because then we will have traded ‘un-insurance’ for underinsurance, and that’s not a good policy outcome either.”
—Joseph Li, MD
Some Likely Effects
For his hospitalist group at University of Massachusetts (UMass) Memorial Medical Center in Worcester, the new legislation “will not represent any new change in our mission or change in the composition of our typical patient panels,” says Glenn Allison, MD, chief of the Division of Hospital Medicine.
Hospitalists, in general, are accustomed to and adept at caring for unassigned patients included in the uncompensated pool, he notes, and at UMass, caring for these patients is a major mission of the hospital. Dr. Allison is hopeful that the legislation holds promise for bringing many previously marginalized and uninsured people into the healthcare system.
Thomas H. Lee, MD, MPH, network president of Partners HealthCare System, Inc, Boston, believes everyone in Massachusetts wants the healthcare reform to work. All stakeholders must “face reality,” he says, and realize that lowering the cost of healthcare is imperative. “It’s clear that the whole healthcare system must become more efficient. The imperative for that was present before this legislation was passed, and I’m not sure the pressures for that imperative are going to change qualitatively.”
One change Dr. Lee does foresee due to the legislation’s dependence on market reforms is that resulting insurance products will “spend a lot less money on patients than existing ones do. There are going to be a variety of pressures on doctors and hospitals to either be much more efficient or take less money for what they do,” he says. “Given that choice, most of us would rather become more efficient.”
Another consequence of affordable insurance products may be a narrowing of provider networks. And a narrow network product, says Sylvia C.W. McKean, MD, FACP, medical director of the BWH/Faulkner Hospitalist Service at Brigham and Women’s Hospital in Boston, “might result in a reduced number of patients going to tertiary care hospitals, which currently care for a large number of indigent patients.”
Even though standards of affordability and details of insurance products have yet to be generated by The Connector and insurers, Dr. Lee also believes that narrowing of benefits and networks will be one likely consequence of the legislation. This will entail some difficult choices about the range of services hospitals and physicians can offer. But, he says, “I think it’s worth doing painful, difficult stuff, and making painful, ugly choices in order for everyone to have necessary catastrophic care and to have access to basic preventive care. We should be willing to live with some of that ugly stuff because it will, in Massachusetts, at least, give us a chance of preventing the need for even uglier outcomes, which is, 10% of our population not having any coverage at all.”
Dr. Lee believes that hospitalists will be critical to the success of hospital efficiency. “To the extent that institutions can use hospitalists and other systems to become much more efficient and reduce readmissions, it’s going to mitigate the need for the narrowing of benefits and networks,” he says.
—Glenn Allison, MD
Upshot for Hospitalists
Unknowns about the workability of and funding for the legislation abound. It’s not clear whether shifting costs to individuals (by mandating they purchase private insurance) and employers (via the $295 per employee fee) can bridge current deficits in compensation and care. Dr. Lee points out that “it’s still an open question of whether there is going to be enough money. But clearly, there are going to be insurance products that spend a lot less money on patients than existing ones do.”
Dr. Li does not believe these funding questions will affect the bottom line for his hospitalist group because their compensation is based on productivity, as measured by relative value units (RVUs).
The next 10 months or so leading up to the July 1, 2007, deadline for purchase of individual health insurance policies will be revealing for consumers and physicians alike. Although the devil will be in the details, Dr. Lee notes, “The big picture is not uncertain. We know there is going to be more transparency, more data, on quality and efficiency.”
That means that hospitals’ delivery of care will endure more scrutiny, and that pay for performance will become commonplace.
The influx of patients into the healthcare system, which legislators hope will be a consequence of greater access to care, will necessitate some consciousness-raising for hospitalists, Dr. Allison maintains. While hospitalists already work closely with other providers on the multidisciplinary team (social workers, case managers, and primary care physicians), they will have to strengthen those collaborations to ensure that patients don’t fall through the cracks. Community outreach may become part of the hospitalists’ job description.
For example, he explains, many preventive or follow-up services that are now being performed in the hospital because patients have no primary care physicians can now be referred to outpatient sites. “Now that these people will have doctors and will be tied into the healthcare system, these services can be performed in the right setting, instead of using more expensive inpatient resources,” he says.
Steering patients to community-based preventive services, such as early cardiac and cancer screenings, will fall to hospitalists, who will be “on the frontlines seeing these patients and referring them appropriately as they leave the hospital,” says Dr. Allison. Hospitalists and all providers will also be evaluated by how well they deliver culturally competent care—another mandate of the statute. To steer through these changes, hospitalists must become much more conscious, he says, of costs, communications, referrals, and resources. “That, as far as I can see, has not been a major emphasis of hospitalist literature or debate.”
A Role to Play
Dr. McKean and others contend that by virtue of their skill set and core mission, hospitalists will have much to contribute toward moderating the costs of healthcare. “The good news for hospitalists,” says Turnbull, “is that if we’re successful in providing health coverage to many people who are now uninsured and if that coverage is adequate there should be more people receiving primary and preventive care and services. This should prevent them from needing to go to the hospital in the first place. We should also be able to create more rational systems of care for people, so that when patients are in the hospital, they need to be there, and they can take full advantage of the talents and contributions that hospitalists make.”
Dr. Kingsdale agrees with the assessment that hospitalists will have a potentially significant role to play in improving the delivery, efficiency, and quality of care, as well as reducing medical errors. He hopes the new insurance products generated by companies will include financial incentives for hospitals and other providers who will be doing “the difficult work of changing their systems of care.”
“The healthcare system really has to improve,” asserts Dr. Lee. “In our organization, we say that we need both an industrial revolution and a cultural revolution, where we develop and use systems that reduce errors. There are electronic records and other industrial systems, and then there are human-ware systems, like hospitalists and disease management programs.”
Like the community organizations that must increase outreach efforts to formerly disenfranchised healthcare consumers, the administrators who fulfill the law’s mandates, and citizens who will be comparing new health plans, hospitalists may find themselves working harder once the law is implemented. The April legislation “elevates the stakes for delivering effective, quality inpatient care,” says Dr. Allison. “I don’t want to over-inflate our importance, but I do think in a system where so many of our healthcare dollars are expended on the inpatient side, we’ve got to be extremely conscious of what we do.” This may mean shifting hospitalists’ implicit skills into the explicit realm, he says: “For instance, everyone talks about guidelines and how helpful they are, but we don’t do a good enough job when it comes to using them. We need to do better with vaccination, with discharge instructions, and with communicating and coordinating care.
“I think the care coordination piece is going to be the key to success,” concludes Dr. Allison. “I think we need to take what we do now, but do more of it, and do a better job of it. That is something that will make a tough job even tougher. But I think if we fail in this, the whole effort may collapse.” TH
Gretchen Henkel is coauthor of Marketing Your Clinical Practice—Ethically, Effectively, Economically.
Resources
- Altman SH, Doonan M. “Can Massachusetts lead the way in health care reform?” N Engl J Med. 2006 May;354(20):2093-2095.
- Steinbrook R. Health care reform in Massachusetts—a work in progress. N Engl J Med. 2006 May;354(20): 2095-2098.
- The 184th General Court of the Commonwealth of Massachusetts. Chapter 58 of the Acts of 2006, an act providing access to affordable, quality, accountable health care. Available at: www.mass.gov/legis/summary.pdf). Last accessed June 12, 2006.
- Johnston PW, Turnbull NC. A bold insurance experiment. The Boston Globe. April 16, 2006. Available at: www.boston.com. Last accessed June 26, 2006.
- McCormick D, Himmelstein DU, Woolhandler S, et al. Single-payer national health insurance. Physicians’ views. Arch Intern Med. 2004 Feb 9;164(3):300-304.
- “Massachusetts Health Reform Bill: A False Promise of Universal Coverage.” Statement by Steffie Woolhandler, MD, MPH and David U. Himmelstein, MD. Available at www.pnhp.org/news/2006/april/massachusetts_health.php. Last accessed June 26, 2006.
Like the community organizations that must increase outreach efforts to formerly disenfranchised healthcare consumers, the administrators who fulfill the law’s mandates, and citizens who will be comparing new health plans, hospitalists may find themselves working harder once the law is implemented.
Massachusetts’ lawmakers garnered huge headlines across the nation in April when the Democratic-dominated state legislature passed a health insurance reform bill nearly unanimously, and Republican Governor Mitt Romney signed the bill into law. This summer, health policy experts are hard at work implementing the first of many mandated stages of the legislation. Other states will watch Massachusetts in the next year as administrators hammer out details of the much-heralded bipartisan statute. Much remains to be done, however, and effects of the statute on patients, hospitals, and physicians remain unclear.
The hope is that the state can ensure nearly universal health insurance coverage for its estimated 500,000 citizens who currently have none. The Massachusetts statute aims to accomplish this feat by offering subsidized insurance coverage to those earning up to 300% of the federal poverty level (facilitated by a Medicaid waiver now being finalized between the state and CMS); assessing $295 per employee from businesses with 11 or more employees who do not provide coverage; and requiring purchase of affordable individual insurance products by those to whom such products are available.
Can the complex, market-driven compromise work? If all staged implementations go into effect as planned, will they be sustainable? Once in place, how might these reforms play out for the practice of hospital medicine? The Hospitalist recently solicited opinions from several hospitalists, physicians, a network president, and health policy experts to get some idea of what the future may hold for healthcare delivery in Massachusetts.
Key Features of the Legislation
As the number of uninsured Americans continues to grow, and reform at the federal level has stalled, many states have been working on their own plans to increase access to insurance and healthcare. The linchpin of individuals’ and businesses’ shared responsibility, health policy experts say, was key to the bipartisan support shown for the Massachusetts insurance reform bill. As of July 1, 2007, every citizen over 18 will be required to obtain health insurance. Businesses with 11 or more employees must pay $295 per employee if they do not offer coverage. (This provision was vetoed by Governor Romney when he signed the bill, but it was subsequently overridden by the legislature.)
The legislation—hundreds of pages long—stipulates an approximate two-year timeline for implementing all phases of the plan, and includes state tax penalties for individuals who don’t comply with the requirement to obtain insurance. The law also creates a state authority, The Commonwealth Health Insurance Connector, to set eligibility standards for subsidized policies, expand Medicaid enrollment, determine affordability guidelines, and approve of plans submitted by private insurers to be offered to consumers. It is anticipated that The Connector (its nickname) will act as a clearinghouse, linking individuals and small businesses with choices of affordable health plans paid for with pretax dollars.
Some of the features lauded by most—even critics—include expansion of Medicaid enrollment; policies with no to low premiums and no deductibles, on a sliding scale, for individuals and families earning up to 300% of the federal poverty line ($29,400 for individuals and $60,000 for families in the contiguous 48 states); and portability of the policies. In addition, young adults can remain covered through their parents’ policies until they become independent or reach age 25. Other specially designed low cost, limited coverage plans will be offered to young adults between ages 19 and 26.
In the press, the statute has been touted as providing “universal care,” but critics doubt that the coverage will be truly universal. For instance, they claim, based on U.S. Census data, that the number of uninsured in Massachusetts is closer to 714,000—not the 500,000 that resulted from bilingual telephone surveys used by those who drafted the bill. Those who espouse a single-payer solution to the insurance crisis, such as Physicians for a National Health Policy and Mass-Care (the statewide coalition of organizations that back single-payer healthcare), argue that mandating purchase of individual plans will shut many working families out of the market. Even administrators and physicians interviewed for this article admit that to generate affordable policies, insurers may have to limit networks and benefits. And increasing the number of insured citizens may have no effect on the rising tide of healthcare delivery costs. With so many unknowns, and a complicated administrative system to initiate, the task of fulfilling the statute’s mandate is daunting.
Where It Is Now
Reached in mid-July between meetings, Jon M. Kingsdale, PhD, newly appointed executive director of the Commonwealth Health Insurance Connector Authority, reported that his board had met five times since June 7. Included in its busy schedule: generating a plan of operations and a budget and hiring staff. The Connector also met its first legislative deadline, which was to develop and issue regulations and criteria by July 1, 2006, for contracting with health plans for the Commonwealth Care Health Insurance Program, or C-CHIP. This is the state-subsidized health plan for people earning up to 300% of the federal poverty line that will begin on October 1, 2006. Key features of C-CHIP and other components of the Massachusetts health reform include no premiums for those who earn less than 100% of the federal poverty line, increased coverage for children, and increased Medicaid reimbursement rates for providers (a good thing for hospitals). Premiums for those earning 100%-300% of the federal poverty line will be set according to a sliding scale, but none of the C-CHIP plans include deductibles. Funding for this plan will come from federal and state matching Medicaid funds made possible by a waiver currently being negotiated between Massachusetts and CMS. (Formal approval had not yet been granted by CMS as of July 21.)
As to the insurance products for those earning above 300% of the federal poverty level, Dr. Kingsdale says The Connector board will address affordability criteria once C-CHIP deadlines have been met. The legislation calls for The Connector to provide its seal of approval for plans that are offered and make determinations about continuing or withdrawing approval. After two years, the agency will formally evaluate the program and make recommendations for changes.
Reactions to the Plan
Joseph Li, MD, assistant professor of medicine at Harvard Medical School and director of the Hospital Medicine Program at Beth Israel Deaconess Medical Center in Boston, admits that his excitement about the insurance statute is somewhat tempered. His personal opinion, which does not reflect his group’s or hospital’s opinion—is that he will “believe it when it’s truly enacted.”
Massachusetts has passed healthcare care reform bills in the past: Witness the 1988 legislation under Governor Michael Dukakis that was later repealed. Nevertheless, Dr. Li says, “I’m glad to see it happen. A lot of people have been wondering how we are going to address the issue of the 45 million uninsured in this country. This is one step toward that, but there are really a lot of ifs, ands, and buts on whether it will truly be pulled off in a year or two.”
Shortly after the ceremonial signing of the bill in early April, Nancy C. Turnbull, president of the Blue Cross Blue Shield of Massachusetts Foundation, co-wrote an editorial with Philip W. Johnston, calling the legislation a “bold insurance experiment.” Both Turnbull and Johnston were part of the Dukakis team that helped create that administration’s 1988 healthcare reform bill, which was later repealed. In their 4/16/06 Boston Globe editorial, the authors noted that the consensus for passing the April legislation bodes well for the plan. Recently, Turnbull said she was still optimistic about the workability of the reform.
Praising The Connector’s “aggressive implementation schedule” (for the expanded Medicaid coverage and the C-CHIP), Turnbull points out that outreach and public education will be key to the success of the plan’s subsidized coverage components. To that end, she anticipates that the Foundation will fund grants to community-based organizations to help them with the “significant new responsibilities” of community outreach to enroll those eligible.
What’s “Affordable?”
The individual mandate deadline is July 1, 2007, and before that date The Connector is charged with making determinations about affordability standards. “Over the next six months,” explains Turnbull, “they will have to decide what portion of household income it is reasonable to expect people to contribute toward health coverage.”
People such as Steffie Woolhandler, MD, MPH, a primary care physician in the Department of Medicine, Cambridge Hospital and Harvard Medical School (Boston) and a co-founder of Physicians for a National Health Program, which favors a single-payer system, worry that insurers will rely on high deductibles and co-pays to make premiums affordable.
“Consumer-directed healthcare is terrible for patients,” says Dr. Woolhandler. And under the payment structure of high-deductible insurance policies, “payment is terrible for docs because most of what we bill is in that early part of spending before the deductible [is met].
“I’m a primary care doc,” she continues, “and most patients who come to my office would be paying out of pocket in that consumer-directed healthcare situation.”
Calling the statute a hoax, Dr. Woolhandler maintains that it won’t achieve universal healthcare, and, in fact, will financially penalize working families.
Turnbull acknowledges that concerns such as those voiced by Dr. Woolhandler are well-founded because insurers and employers have traditionally resorted to increased cost-sharing to regulate premiums. However, she says, “If we don’t find ways to make good coverage more affordable, then the individual mandate will not go into effect for many people.”
Asked what he would say to critics who do not think private insurance companies can structure products that are both affordable and of good quality, Dr. Kingsdale says, “It’s up to them [the insurance companies] to prove you wrong. A well-functioning market with a lot of good information, which is what this reform calls for, can improve upon the plans available to what is perhaps the least well-functioning part of the existing insurance market: the non-group and small-group insurance market.”
Determination of good quality, affordable benefit packages will be a difficult decision. “In my personal view, I think we will have failed if, as a result of the mandate, we succeed only in requiring people to purchase coverage that is not adequate,” says Turnbull, “because then we will have traded ‘un-insurance’ for underinsurance, and that’s not a good policy outcome either.”
—Joseph Li, MD
Some Likely Effects
For his hospitalist group at University of Massachusetts (UMass) Memorial Medical Center in Worcester, the new legislation “will not represent any new change in our mission or change in the composition of our typical patient panels,” says Glenn Allison, MD, chief of the Division of Hospital Medicine.
Hospitalists, in general, are accustomed to and adept at caring for unassigned patients included in the uncompensated pool, he notes, and at UMass, caring for these patients is a major mission of the hospital. Dr. Allison is hopeful that the legislation holds promise for bringing many previously marginalized and uninsured people into the healthcare system.
Thomas H. Lee, MD, MPH, network president of Partners HealthCare System, Inc, Boston, believes everyone in Massachusetts wants the healthcare reform to work. All stakeholders must “face reality,” he says, and realize that lowering the cost of healthcare is imperative. “It’s clear that the whole healthcare system must become more efficient. The imperative for that was present before this legislation was passed, and I’m not sure the pressures for that imperative are going to change qualitatively.”
One change Dr. Lee does foresee due to the legislation’s dependence on market reforms is that resulting insurance products will “spend a lot less money on patients than existing ones do. There are going to be a variety of pressures on doctors and hospitals to either be much more efficient or take less money for what they do,” he says. “Given that choice, most of us would rather become more efficient.”
Another consequence of affordable insurance products may be a narrowing of provider networks. And a narrow network product, says Sylvia C.W. McKean, MD, FACP, medical director of the BWH/Faulkner Hospitalist Service at Brigham and Women’s Hospital in Boston, “might result in a reduced number of patients going to tertiary care hospitals, which currently care for a large number of indigent patients.”
Even though standards of affordability and details of insurance products have yet to be generated by The Connector and insurers, Dr. Lee also believes that narrowing of benefits and networks will be one likely consequence of the legislation. This will entail some difficult choices about the range of services hospitals and physicians can offer. But, he says, “I think it’s worth doing painful, difficult stuff, and making painful, ugly choices in order for everyone to have necessary catastrophic care and to have access to basic preventive care. We should be willing to live with some of that ugly stuff because it will, in Massachusetts, at least, give us a chance of preventing the need for even uglier outcomes, which is, 10% of our population not having any coverage at all.”
Dr. Lee believes that hospitalists will be critical to the success of hospital efficiency. “To the extent that institutions can use hospitalists and other systems to become much more efficient and reduce readmissions, it’s going to mitigate the need for the narrowing of benefits and networks,” he says.
—Glenn Allison, MD
Upshot for Hospitalists
Unknowns about the workability of and funding for the legislation abound. It’s not clear whether shifting costs to individuals (by mandating they purchase private insurance) and employers (via the $295 per employee fee) can bridge current deficits in compensation and care. Dr. Lee points out that “it’s still an open question of whether there is going to be enough money. But clearly, there are going to be insurance products that spend a lot less money on patients than existing ones do.”
Dr. Li does not believe these funding questions will affect the bottom line for his hospitalist group because their compensation is based on productivity, as measured by relative value units (RVUs).
The next 10 months or so leading up to the July 1, 2007, deadline for purchase of individual health insurance policies will be revealing for consumers and physicians alike. Although the devil will be in the details, Dr. Lee notes, “The big picture is not uncertain. We know there is going to be more transparency, more data, on quality and efficiency.”
That means that hospitals’ delivery of care will endure more scrutiny, and that pay for performance will become commonplace.
The influx of patients into the healthcare system, which legislators hope will be a consequence of greater access to care, will necessitate some consciousness-raising for hospitalists, Dr. Allison maintains. While hospitalists already work closely with other providers on the multidisciplinary team (social workers, case managers, and primary care physicians), they will have to strengthen those collaborations to ensure that patients don’t fall through the cracks. Community outreach may become part of the hospitalists’ job description.
For example, he explains, many preventive or follow-up services that are now being performed in the hospital because patients have no primary care physicians can now be referred to outpatient sites. “Now that these people will have doctors and will be tied into the healthcare system, these services can be performed in the right setting, instead of using more expensive inpatient resources,” he says.
Steering patients to community-based preventive services, such as early cardiac and cancer screenings, will fall to hospitalists, who will be “on the frontlines seeing these patients and referring them appropriately as they leave the hospital,” says Dr. Allison. Hospitalists and all providers will also be evaluated by how well they deliver culturally competent care—another mandate of the statute. To steer through these changes, hospitalists must become much more conscious, he says, of costs, communications, referrals, and resources. “That, as far as I can see, has not been a major emphasis of hospitalist literature or debate.”
A Role to Play
Dr. McKean and others contend that by virtue of their skill set and core mission, hospitalists will have much to contribute toward moderating the costs of healthcare. “The good news for hospitalists,” says Turnbull, “is that if we’re successful in providing health coverage to many people who are now uninsured and if that coverage is adequate there should be more people receiving primary and preventive care and services. This should prevent them from needing to go to the hospital in the first place. We should also be able to create more rational systems of care for people, so that when patients are in the hospital, they need to be there, and they can take full advantage of the talents and contributions that hospitalists make.”
Dr. Kingsdale agrees with the assessment that hospitalists will have a potentially significant role to play in improving the delivery, efficiency, and quality of care, as well as reducing medical errors. He hopes the new insurance products generated by companies will include financial incentives for hospitals and other providers who will be doing “the difficult work of changing their systems of care.”
“The healthcare system really has to improve,” asserts Dr. Lee. “In our organization, we say that we need both an industrial revolution and a cultural revolution, where we develop and use systems that reduce errors. There are electronic records and other industrial systems, and then there are human-ware systems, like hospitalists and disease management programs.”
Like the community organizations that must increase outreach efforts to formerly disenfranchised healthcare consumers, the administrators who fulfill the law’s mandates, and citizens who will be comparing new health plans, hospitalists may find themselves working harder once the law is implemented. The April legislation “elevates the stakes for delivering effective, quality inpatient care,” says Dr. Allison. “I don’t want to over-inflate our importance, but I do think in a system where so many of our healthcare dollars are expended on the inpatient side, we’ve got to be extremely conscious of what we do.” This may mean shifting hospitalists’ implicit skills into the explicit realm, he says: “For instance, everyone talks about guidelines and how helpful they are, but we don’t do a good enough job when it comes to using them. We need to do better with vaccination, with discharge instructions, and with communicating and coordinating care.
“I think the care coordination piece is going to be the key to success,” concludes Dr. Allison. “I think we need to take what we do now, but do more of it, and do a better job of it. That is something that will make a tough job even tougher. But I think if we fail in this, the whole effort may collapse.” TH
Gretchen Henkel is coauthor of Marketing Your Clinical Practice—Ethically, Effectively, Economically.
Resources
- Altman SH, Doonan M. “Can Massachusetts lead the way in health care reform?” N Engl J Med. 2006 May;354(20):2093-2095.
- Steinbrook R. Health care reform in Massachusetts—a work in progress. N Engl J Med. 2006 May;354(20): 2095-2098.
- The 184th General Court of the Commonwealth of Massachusetts. Chapter 58 of the Acts of 2006, an act providing access to affordable, quality, accountable health care. Available at: www.mass.gov/legis/summary.pdf). Last accessed June 12, 2006.
- Johnston PW, Turnbull NC. A bold insurance experiment. The Boston Globe. April 16, 2006. Available at: www.boston.com. Last accessed June 26, 2006.
- McCormick D, Himmelstein DU, Woolhandler S, et al. Single-payer national health insurance. Physicians’ views. Arch Intern Med. 2004 Feb 9;164(3):300-304.
- “Massachusetts Health Reform Bill: A False Promise of Universal Coverage.” Statement by Steffie Woolhandler, MD, MPH and David U. Himmelstein, MD. Available at www.pnhp.org/news/2006/april/massachusetts_health.php. Last accessed June 26, 2006.